







Languages
Pages
Legal


1 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
Mandatory Competency Assessment for Medicines Management (Not Injectable Medicines) for
Registered Practitioners
‘IN HOSPITAL’
Document Author Authorised Signature
Written by: Lead Pharmacist/Lead
Technician
Medicines Use and Safety Team,
Pharmacy Department
Date: September 2015
Authorised by: Head of Practice Education
and Development
Date: September 2015
Effective Date: October 2015
Review Date: October 2017
Approval at: Clinical Competency Group
and Mandatory Training Group
Date Approved: September 2015

2 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
DOCUMENT HISTORY
(Procedural document version numbering convention will follow the following format. Whole numbers for approved versions, e.g.
1.0, 2.0, 3.0 etc. With decimals being used to represent the current working draft version, e.g. 1.1, 1.2, 1.3, 1.4 etc. For example, when
writing a procedural document for the first time – the initial draft will be version 0.1)
Date of Issue Version
No.
Date
Approved
Person Responsible for
Change
Nature of
Change
Ratification /
Approval
October 2015 1.0 September
2015
Clinical
Competency
Group/Mandatory
Training Group
March 2016 1.1 Donna Baker Frequency
amended to
reflect the annual
assessment
component of the
Medicines Policy
3 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
‘Nursing staff in the best interests of their patients must know the therapeutic uses of the
medicine to be administered, normal dosage, side effects, precautions and contraindications.
They must have considered the dosage, method of administration, route and timing of the
administration in context of the patient’s condition, co-existing therapies and meals’ (NMC,
Standards for Medicines Management 2010).
The core mandatory assessment requirements for Medicines Management ‘IN HOSPITAL’
are applicable to the following practitioners:
NEW REGISTERED PRACTITIONERS OR EXISTING PRACTITIONERS WHERE MEDICINES
MANAGEMENT IS NEW TO THEIR ROLE ARE TO COMPLETE ALL THE REQUIRED ELEMENTS
BELOW PRIOR TO UNDERTAKING MEDICINES MANAGEMENT UNSUPERVISED.
EXISTING REGISTERED PRACTITIONERS WHERE MEDICINES MANAGEMENT IS PART OF
THEIR ROLE ARE TO COMPLETE THE REQUIRED ELEMENTS ON AN ANNUAL BASIS.
REQUIRED ELEMENTS:
1. Ward based ‘IN HOSPITAL’ Competency Assessment for Medicines Management (this document)
2. E Learning Training Tracker Module for Medicines Management
a) Clinical Medicines Scenarios – 100%
b) Maths and Medicines Calculations - 100%
IF REQUIRED
3. Electronic Prescribing and Medicines Administration system (EPMA) training
commonly referred to as “JAC” Medicines Management system, if in use on the
ward.
4. Electronic Medicines Storage Cabinet training (e.g. Omnicell and MDG Cabinet) if the
electronic medicines storage cabinet is in use on the ward.
4 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
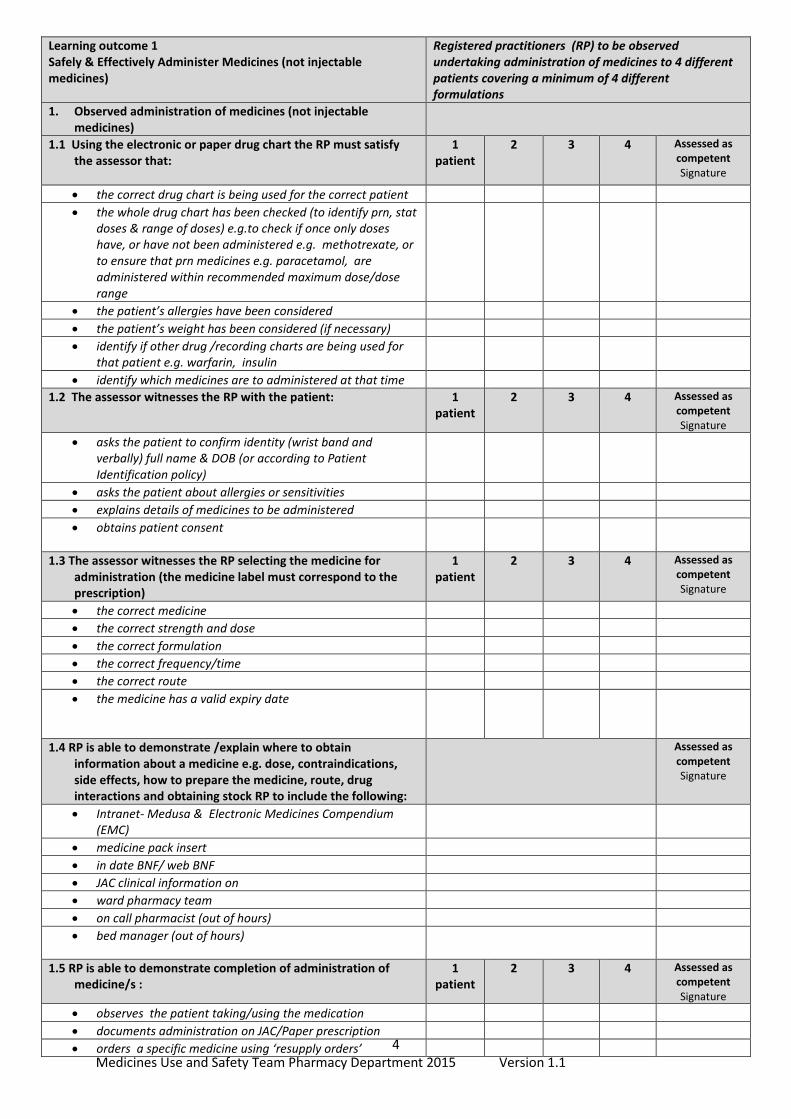
Learning outcome 1 Safely & Effectively Administer Medicines (not injectable medicines)
Registered practitioners (RP) to be observed undertaking administration of medicines to 4 different patients covering a minimum of 4 different formulations
1. Observed administration of medicines (not injectable medicines)
1.1 Using the electronic or paper drug chart the RP must satisfy the assessor that:
1 patient
2 3 4 Assessed as competent Signature
the correct drug chart is being used for the correct patient
the whole drug chart has been checked (to identify prn, stat doses & range of doses) e.g.to check if once only doses have, or have not been administered e.g. methotrexate, or to ensure that prn medicines e.g. paracetamol, are administered within recommended maximum dose/dose range
the patient’s allergies have been considered
the patient’s weight has been considered (if necessary)
identify if other drug /recording charts are being used for that patient e.g. warfarin, insulin
identify which medicines are to administered at that time
1.2 The assessor witnesses the RP with the patient: 1 patient
2 3 4 Assessed as competent Signature
asks the patient to confirm identity (wrist band and verbally) full name & DOB (or according to Patient Identification policy)
asks the patient about allergies or sensitivities
explains details of medicines to be administered
obtains patient consent
1.3 The assessor witnesses the RP selecting the medicine for administration (the medicine label must correspond to the prescription)
1 patient
2 3 4 Assessed as competent Signature
the correct medicine
the correct strength and dose
the correct formulation
the correct frequency/time
the correct route
the medicine has a valid expiry date
1.4 RP is able to demonstrate /explain where to obtain information about a medicine e.g. dose, contraindications, side effects, how to prepare the medicine, route, drug interactions and obtaining stock RP to include the following:
Assessed as competent Signature
Intranet- Medusa & Electronic Medicines Compendium (EMC)
medicine pack insert
in date BNF/ web BNF
JAC clinical information on
ward pharmacy team
on call pharmacist (out of hours)
bed manager (out of hours)
1.5 RP is able to demonstrate completion of administration of medicine/s :
1 patient
2 3 4 Assessed as competent Signature
observes the patient taking/using the medication
documents administration on JAC/Paper prescription
orders a specific medicine using ‘resupply orders’

5 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
can explain process when delaying or omitting a prescribed medicine
demonstrates disposal of equipment/waste medicines
1.6 RP is witnessed administering a selection of formulations during assessment; tick preparations/routes assessed *mandatory
1 patient
2 3 4 Assessed as competent Signature
Oral tablet
Dispersible tablets*
Liquid- oral syringe/spoon/medicine measure*
Inhalers*
Cream/ointment
Eye drops/ointment*
Rectal – suppositories
Vaginal - pessaries
patch
Nebules*
Sublingual
Others please state:
1.7 RP to explain what action to take if they are unable to administer a prescribed medicine to include:
Assessed as competent Signature
if a patient is unable to swallow (determine reason e.g. size of table, refer for SALT assessment, refer to doctor for review form of medication)
if a medicine is not available(contact pharmacy, bed manager- out of hours ,prescriber) there should be NO delay, especially with critical medicines)
patient unable to tolerate
nurse unable to give by prescribed route (contact prescriber without delay)
1.8 RP is witnessed administering a subcutaneous injection (tick boxes 1.1 – 1.8)
1 patient
2 3 4 Assessed as competent Signature
demonstrates ability to select appropriate equipment with rationale for us
prepares the medicine for injection appropriately
identifies correct patient, explains procedure, checks any contraindications, potential side effects and obtains valid consent
demonstrates ability to ensure correct administration technique of the medicine via the subcutaneous route in the prescribed site
demonstrates understanding of the anatomy and physiology of sites used for injection technique
1.9 RP is witnessed administering an intramuscular injection 1 patient
2 3 4 Assessed as competent Signature
demonstrates ability to select appropriate equipment with rationale for use
prepares the medicine for injection appropriately
identifies correct patient, explains procedure, checks any contraindications, potential side effects and obtains valid consent
6 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
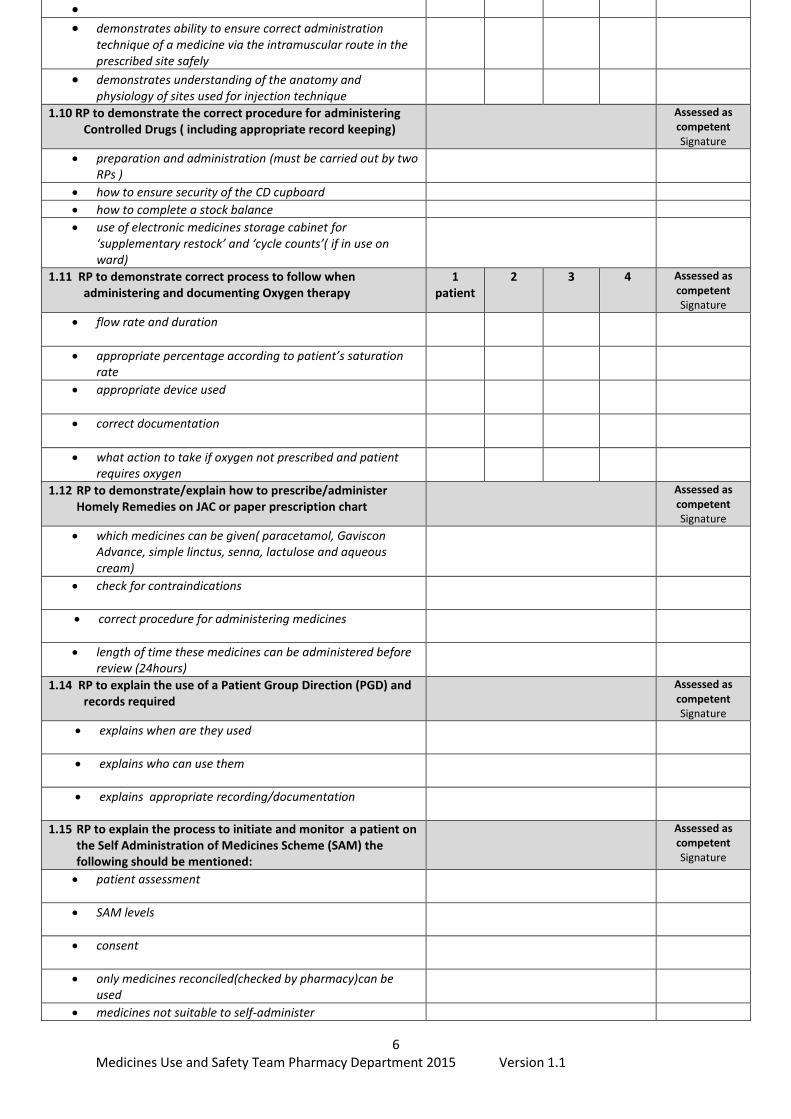
demonstrates ability to ensure correct administration technique of a medicine via the intramuscular route in the prescribed site safely
demonstrates understanding of the anatomy and physiology of sites used for injection technique
1.10 RP to demonstrate the correct procedure for administering Controlled Drugs ( including appropriate record keeping)
Assessed as competent Signature
preparation and administration (must be carried out by two RPs )
how to ensure security of the CD cupboard
how to complete a stock balance
use of electronic medicines storage cabinet for ‘supplementary restock’ and ‘cycle counts’( if in use on ward)
1.11 RP to demonstrate correct process to follow when administering and documenting Oxygen therapy
1 patient
2 3 4 Assessed as competent Signature
flow rate and duration
appropriate percentage according to patient’s saturation rate
appropriate device used
correct documentation
what action to take if oxygen not prescribed and patient requires oxygen
1.12 RP to demonstrate/explain how to prescribe/administer Homely Remedies on JAC or paper prescription chart
Assessed as competent Signature
which medicines can be given( paracetamol, Gaviscon Advance, simple linctus, senna, lactulose and aqueous cream)
check for contraindications
correct procedure for administering medicines
length of time these medicines can be administered before review (24hours)
1.14 RP to explain the use of a Patient Group Direction (PGD) and records required
Assessed as competent Signature
explains when are they used
explains who can use them
explains appropriate recording/documentation
1.15 RP to explain the process to initiate and monitor a patient on the Self Administration of Medicines Scheme (SAM) the following should be mentioned:
Assessed as competent Signature
patient assessment
SAM levels
consent
only medicines reconciled(checked by pharmacy)can be used
medicines not suitable to self-administer
7 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
key security
Medicines Information Card/JAC administration chart
where to store medicines
nurse responsibility for monitoring patient (mention deteriorating patient and withdrawal from scheme)

8 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
Learning outcome 2 Medicines Safety
2.0 Medication errors and patient safety
2.1 RP to define the following: Assessed as competent Signature
Medication errors: are incidents in which there has been an error in prescribing, dispensing, preparing, administering or monitoring, regardless of whether harm has occurred
Near miss: are incidents that did not cause harm but which are judged to have had the potential to cause harm
2.2 RP to explain what process to follow upon discovery of a medication error (including near miss)
complete incident on electronic incident report ‘Datix’
the ‘Management of medication related incidents’ protocol (see Intranet)must be followed
2.3 RP to explain how they would manage the following: Assessed as competent Signature
Adverse drug reaction(preventable and non-preventable)(MHRA- Yellow Card Scheme)
a missed dose
a patient sensitive to prescribed medicine (e.g. upset stomach)
no stock of the first dose antibiotic
incorrect stock balance of a Controlled Drug
a patient has been given two doses of Paracetamol within 1 hour by a colleague
a discovery of a ‘near miss’
you have given a medicine to the wrong patient

9 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
Learning outcome 3 Order, Receive, Store, Transfer and Dispose of Medicines
3.1 RP is able to demonstrate/explain the process for ordering, receiving and storage of urgent medicines used on the ward including : cardiac arrest, anaphylaxis, intubation boxes.
Assessed as competent Signature
which packs are stocked on your ward?
when are they used?
where are they stored?
how are they ordered?
3.2 RP can demonstrate/explain the correct process for ordering, receiving and storage of ward stock medicines
Assessed as competent Signature
urgent medicines for cardiac arrest , anaphylaxis, extravasation, intubation and neonatal resuscitation boxes
order a ward stock item for Top Up and Non Top up wards ( use stock item request form or green stock profile order folder)
request a new stock item by using the ‘New Stock Request’ form
receiving medicines on to a ward including signing transportation of medicines register
‘returning’, ‘supplementary re -stock ‘and ‘cycle count’ for medicines using the electronic medicines storage cabinet, if in use on ward
storage of the following ward stock:
Intravenous fluids - should be stored off the floor in their original containers in a designated area/electronic medicines storage cabinet
medicines for internal use
medicines for external use
diagnostic reagents
medical gases
3.3 RP to explain the correct storage and documentation requirements for refrigerated medicines:
Assessed as competent Signature
demonstrate/explain daily temperature monitoring and recording (using an electronic max/min thermometer to maintain temp between 2-8
0C or electronic display on
automated fridges) or web monitoring (electronic medicines storage cabinet)
action to be taken following disconnection of electrical supply or refrigerator breakdown
action following the discovery of medicines that have not been stored in recommended conditions

10 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
3.4 RP can demonstrate the process for ordering, receiving and storage of named patient medicines
Assessed as competent Signature
ordering medicines for named patients
receiving medicines in secure green pharmacy bag, checking and signing transportation of medicines register
storage of the following:
insulin
unopened eye drops
dosette box (patient’s own medicines)
oral tablets
3.5 RP can demonstrate/explain correct procedures for dealing with the following:
Assessed as competent Signature
Expired medicines
Lost/missing medicines
Returns to pharmacy
Disposal of medicines (see Trust Waste Policy)
Medicines on death of a patient
3.6 RP can demonstrate the process for ordering, receiving, returning and storage of Controlled Drugs to include:
Assessed as competent Signature
ordering a Controlled Drug for stock
receiving stock Controlled Drugs
storing and stock checking process for Controlled Drugs
returning Controlled drugs to Pharmacy including documentation
how to obtain supplies of Controlled drugs out of hours
explain the process for dealing with discrepancies in ward stock levels of Controlled Drugs
why a Controlled Drugs record book needs to be used on the ward (include requirements for documentation)
how to manage patient’s own Controlled Drugs brought into the hospital
process for managing Controlled Drugs when a ward or clinical area is closed or transferred to another clinical area
11 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
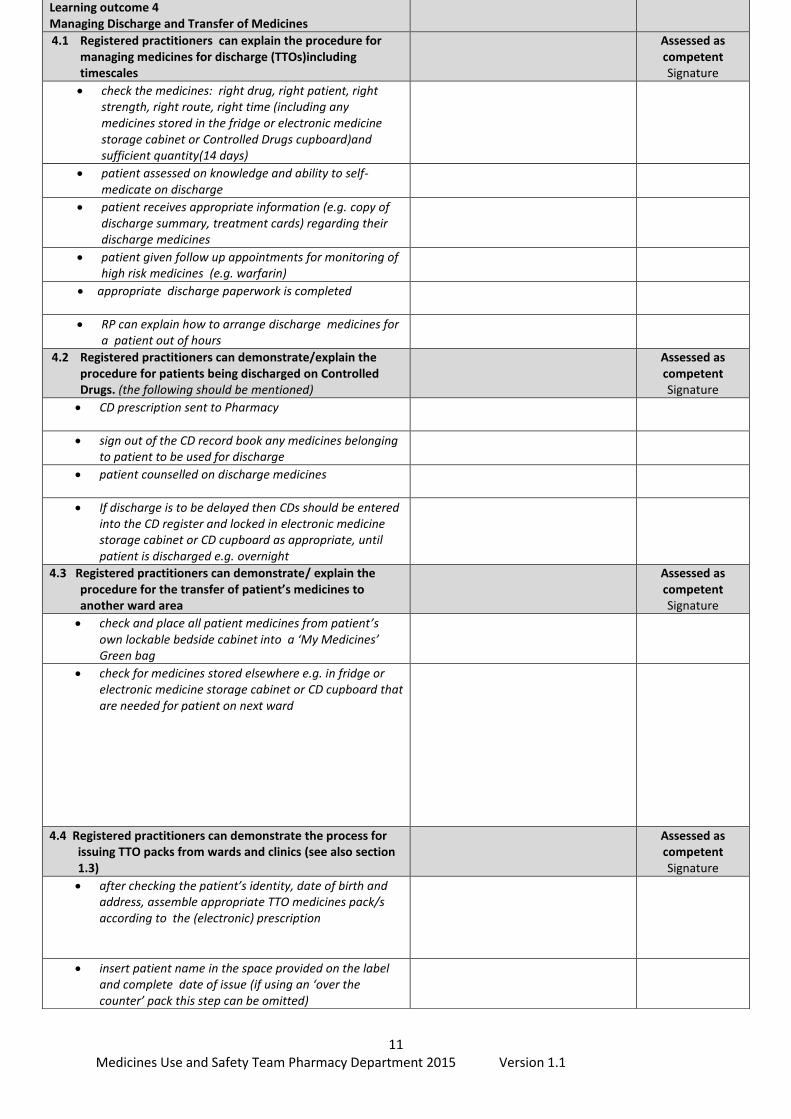
Learning outcome 4 Managing Discharge and Transfer of Medicines
4.1 Registered practitioners can explain the procedure for managing medicines for discharge (TTOs)including timescales
Assessed as competent Signature
check the medicines: right drug, right patient, right strength, right route, right time (including any medicines stored in the fridge or electronic medicine storage cabinet or Controlled Drugs cupboard)and sufficient quantity(14 days)
patient assessed on knowledge and ability to self-medicate on discharge
patient receives appropriate information (e.g. copy of discharge summary, treatment cards) regarding their discharge medicines
patient given follow up appointments for monitoring of high risk medicines (e.g. warfarin)
appropriate discharge paperwork is completed
RP can explain how to arrange discharge medicines for a patient out of hours
4.2 Registered practitioners can demonstrate/explain the procedure for patients being discharged on Controlled Drugs. (the following should be mentioned)
Assessed as competent Signature
CD prescription sent to Pharmacy
sign out of the CD record book any medicines belonging to patient to be used for discharge
patient counselled on discharge medicines
If discharge is to be delayed then CDs should be entered into the CD register and locked in electronic medicine storage cabinet or CD cupboard as appropriate, until patient is discharged e.g. overnight
4.3 Registered practitioners can demonstrate/ explain the procedure for the transfer of patient’s medicines to another ward area
Assessed as competent Signature
check and place all patient medicines from patient’s own lockable bedside cabinet into a ‘My Medicines’ Green bag
check for medicines stored elsewhere e.g. in fridge or electronic medicine storage cabinet or CD cupboard that are needed for patient on next ward
4.4 Registered practitioners can demonstrate the process for issuing TTO packs from wards and clinics (see also section 1.3)
Assessed as competent Signature
after checking the patient’s identity, date of birth and address, assemble appropriate TTO medicines pack/s according to the (electronic) prescription
insert patient name in the space provided on the label and complete date of issue (if using an ‘over the counter’ pack this step can be omitted)

12 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
insert administration instructions if not already present on the label according to the prescription
obtain second check from another RP
complete appropriate paperwork
complete identity checks, sensitivities and allergies before issuing the medicine
Give the patient full verbal instructions on taking the medicine and make patient aware of information leaflet inside the pack.
If paper prescription is used, place the pink copy of the triplicate form with GP’s letter and give to the patient.
Send completed paper prescription to Pharmacy for filing

13 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
Assessment Outcome – Please sign in relevant box
Rating Outcome Actions Assessor Signature and date Initial Assessment
Assessor Signature and date 2nd Assessment
Assessor Signature and date 3rd Assessment
Green Pass - All essential competencies evidenced.
No action required. Review annually at appraisal. Revisit any development learning points listed below as recommended by assessor.
Red Refer - One or more competencies not evidenced.
Clinical practice in relation to the specific competency not evidenced is to be supervised and reassessed within 2 weeks.
Learning points to revisit following successful competency assessment:
First Assessors Signature: Registered Practitioners Signature:
Date:
Inform [email protected] of PASS outcome to update individuals Mandatory Training Profile
14 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
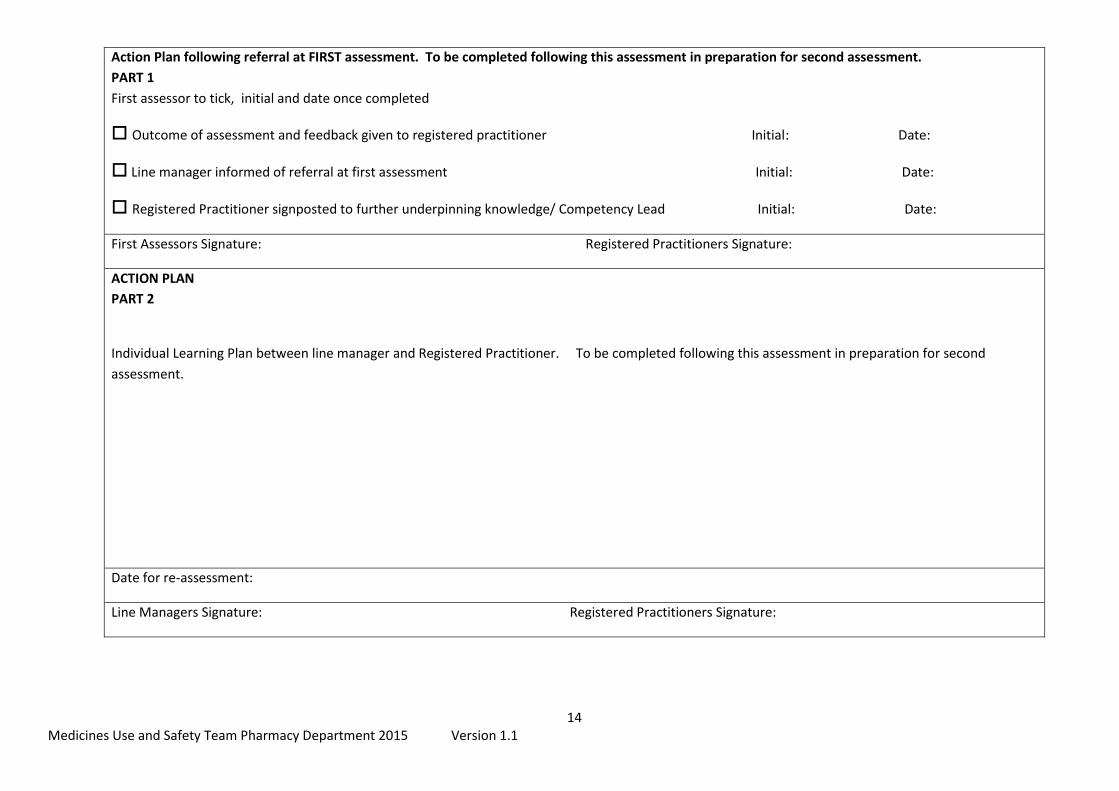
Action Plan following referral at FIRST assessment. To be completed following this assessment in preparation for second assessment.
PART 1
First assessor to tick, initial and date once completed
Outcome of assessment and feedback given to registered practitioner Initial: Date:
Line manager informed of referral at first assessment Initial: Date:
Registered Practitioner signposted to further underpinning knowledge/ Competency Lead Initial: Date:
First Assessors Signature: Registered Practitioners Signature:
ACTION PLAN
PART 2
Individual Learning Plan between line manager and Registered Practitioner. To be completed following this assessment in preparation for second
assessment.
Date for re-assessment:
Line Managers Signature: Registered Practitioners Signature:

15 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
Action Plan following referral at SECOND assessment. To be completed following this assessment in preparation for final assessment.
PART 1
Second Assessor to tick, initial and date once completed
Outcome of assessment and feedback given to registered practitioner Initial: Date:
Line manager informed of referral at first assessment Initial: Date:
Registered Practitioner signposted to further underpinning knowledge / competency Lead Initial: Date:
Second Assessors Signature: Registered Practitioners Signature:
ACTION PLAN
PART 2
Individual Learning Plan between line manager and Registered Practitioner. To be completed following this assessment in preparation for final
assessment
Date for Reassessment:
Line Managers Signature: Registered Practitioners Signature:

16 Medicines Use and Safety Team Pharmacy Department 2015 Version 1.1
Managing a referral at Summative Assessment
Referral following Final Assessment Referral at the final attempt may lead to further performance management in line with Trust policy. This will be discussed in confidence with the candidate and their line manager.
Referral following Second Assessment
The second assessor provides feedback to the candidate; documents the outcome and completes PART 2 of the action plan.
The assessor will refer the outcome to the candidate‘s line manager.
The line manager will complete an individual learning plan and arrange for the candidate to undertake further simulated / supervised practice in preparation for the final re-assessment.
The line manager will consider invoking formal capability.
Referral following Initial Assessment
The first assessor provides feedback to the candidate; documents the outcome and completes PART 1 of the action plan.
The assessor will refer the outcome to the candidate‘s line manager.
The line manager will complete an individual learning plan in preparation for the second re-assessment. A different assessor will be identified for the second assessment.
The line manager will consider invoking informal capability.
Top Related