





Languages
Pages
Legal

9/2/2014
1
MANAGING THE DIABETIC FOOT ULCER
AND
PREVENTING RECURRENCE
Pamela ScarboroughPT, DPT, CDE, CWS, CEEAA
Director Public Policy & EducationAmerican Medical Technologies
Irvine, CA
Director of EducationPARKS InstituteWimberley, TX
2014 WOCN MIDEAST REGIONAL CONFERENCEPRESENTS
Objectives
• Identify multiple pathophysiological issues that can lead to diabetic foot disease
• Discuss structural and biomechanical issues contributing to formation of diabetic foot ulcers and recidivism of these wounds
• Describe intervention to create a healing environment for diabetic foot ulcers and to prevent recurrence of these wounds
9/2/2014
2
Ultimate Goal
3
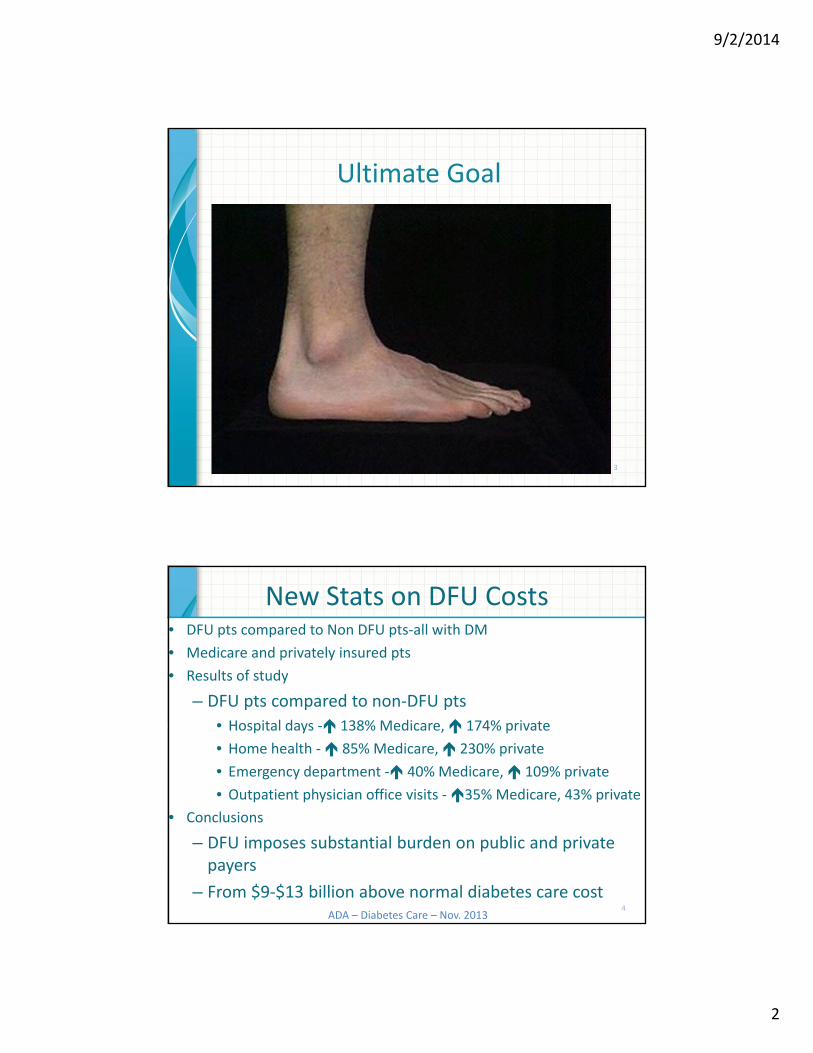
New Stats on DFU Costs• DFU pts compared to Non DFU pts‐all with DM
• Medicare and privately insured pts
• Results of study
– DFU pts compared to non‐DFU pts
• Hospital days ‐ 138% Medicare, 174% private
• Home health ‐ 85% Medicare, 230% private
• Emergency department ‐ 40% Medicare, 109% private
• Outpatient physician office visits ‐35% Medicare, 43% private
• Conclusions
– DFU imposes substantial burden on public and private payers
– From $9‐$13 billion above normal diabetes care cost4
ADA – Diabetes Care – Nov. 2013

9/2/2014
3
Good News!!!Drop in DM Related Amputation Rates
•CDC ‐ dramatic drop rate of diabetes‐relatedamputations in the U.S.
• CDC• Diabetes Care: February 2012
5
CDC Reports Amputation
Rates
65%
Since 1996
1996
11 / 1000 with DM 2008
4 / 1000 with DM
6

9/2/2014
4
Reason for Decreasein Amputation Rates
•Better management of risk factors
• Question: How many of you think risk factors are being better managed
and taught to your patients?
7
Stroke
Nephropathy
Peripheral Neuropathy
Autonomic Neuropathy
Retinopathy
Heart Disease
Chronic HyperglycemiaMulti‐Organ Dysfunction & Failure

9/2/2014
5
Road to Ulceration
Complicated
Multifactorial
Prevention NOT well reimbursed
Recurrence Common
9
#1 Condition leading to
Foot Ulcer?
#1 Condition leading to
Amputation?
Neuropathy Foot Ulcer
10
9/2/2014
6
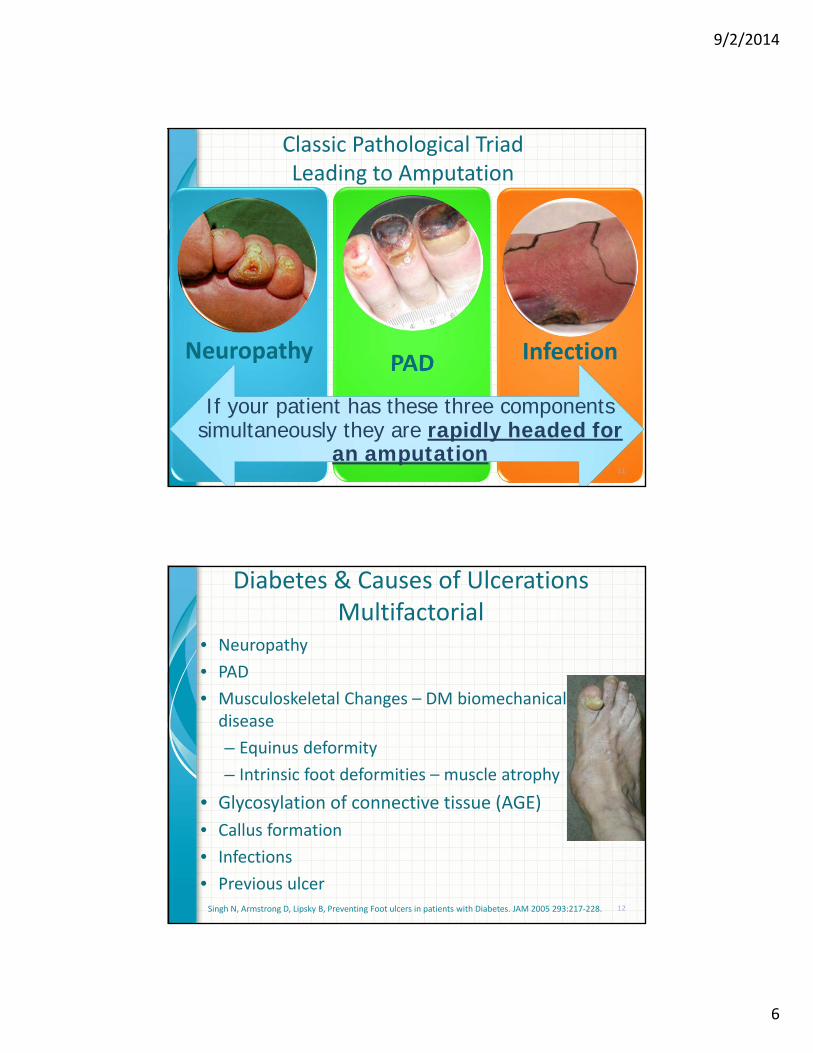
Classic Pathological TriadLeading to Amputation
Neuropathy PAD Infection
If your patient has these three components simultaneously they are rapidly headed for
an amputation11
Diabetes & Causes of Ulcerations Multifactorial
• Neuropathy
• PAD
• Musculoskeletal Changes – DM biomechanical disease
– Equinus deformity
– Intrinsic foot deformities – muscle atrophy
• Glycosylation of connective tissue (AGE)
• Callus formation
• Infections
• Previous ulcerSingh N, Armstrong D, Lipsky B, Preventing Foot ulcers in patients with Diabetes. JAM 2005 293:217‐228. 12

9/2/2014
7
Neuropathic Ulcers: Tri‐Neuropathy
Sensory
Motor
Autonomic
13
Peripheral Neuropathy and Ulcerations
• Loss of Protective Sensation (LOPS)
–Present in 50% of people with DM
–Present in 80% of people with DFUs
–7 Xs increase in ulceration
Boulton AJ, Kirsner RS, Vileikyte L Clinical Practice neuropathic diabetic foot ulcers N Eng Med 2004;351(1) 48‐55Singh N, Armstrong D, Lipsky B, Preventing Foot ulcers in patients with Diabetes. JAM 2005 293:217‐228. 14

9/2/2014
8
Sensory/Motor Neuropathy
• Single most common cause of LOPS
• Small fiber – touch, pain, temperature
• Large fiber – intrinsic changes of foot
–Weakness
–Musculoskeletal changes in foot/ankle
• Prominent metatarsal head/fat pad changes
• Leading to high foot pressures
Boulton AJ, Kirsner RS, Vileikyte L Clinical Practice neuropathic diabetic foot ulcers N Eng Med 2004;351(1) 48‐55Singh N, Armstrong D, Lipsky B, Preventing Foot ulcers in patients with Diabetes. JAM 2005 293:217‐228.
15
Cerebral Vascular Disease
Nephropathy
Peripheral Neuropathy
Autonomic Neuropathy
Retinopathy
Heart Disease
Peripheral Arterial DiseaseMicro/Macro
Remember: Diabetes is a
Systemic Disease!!!
Complications of Chronic HyperglycemiaMultiple Organ
Dysfunction & Failure

9/2/2014
9
Remember the Autonomic Nervous System Impairments from Diabetes
17
Autonomic Neuropathy• Affected structures: sympathetic parasympathetic ganglions
• S & S:
– Postural hypotension
– Cardiorespiratory arrest
– Anhidrosis
– Impotency
– Gastropathy
– Diarrhea
– Gustatory sweating
– Hypoglycemic unawareness18
9/2/2014
10
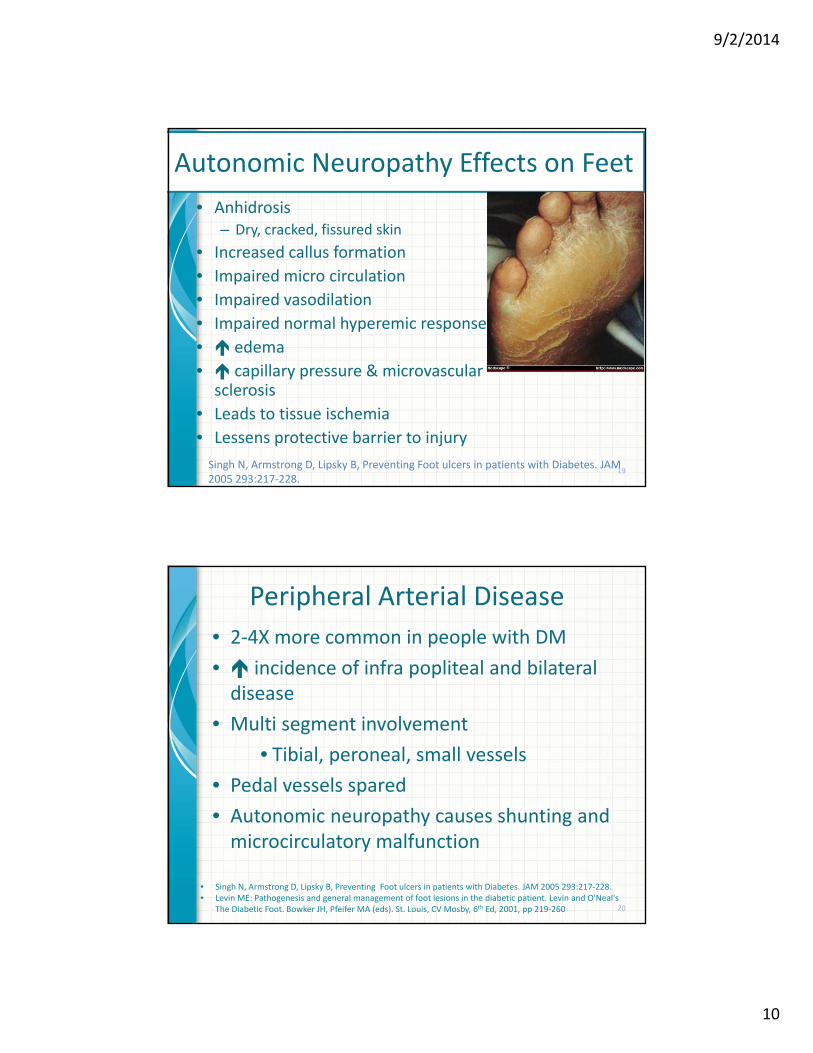
Autonomic Neuropathy Effects on Feet
• Anhidrosis– Dry, cracked, fissured skin
• Increased callus formation
• Impaired micro circulation
• Impaired vasodilation
• Impaired normal hyperemic response
• edema
• capillary pressure & microvascular sclerosis
• Leads to tissue ischemia
• Lessens protective barrier to injury
19Singh N, Armstrong D, Lipsky B, Preventing Foot ulcers in patients with Diabetes. JAM 2005 293:217‐228.
Peripheral Arterial Disease
• 2‐4X more common in people with DM
• incidence of infra popliteal and bilateral disease
• Multi segment involvement
• Tibial, peroneal, small vessels
• Pedal vessels spared
• Autonomic neuropathy causes shunting and microcirculatory malfunction
20
• Singh N, Armstrong D, Lipsky B, Preventing Foot ulcers in patients with Diabetes. JAM 2005 293:217‐228.• Levin ME: Pathogenesis and general management of foot lesions in the diabetic patient. Levin and O'Neal's
The Diabetic Foot. Bowker JH, Pfeifer MA (eds). St. Louis, CV Mosby, 6th Ed, 2001, pp 219‐260
9/2/2014
11
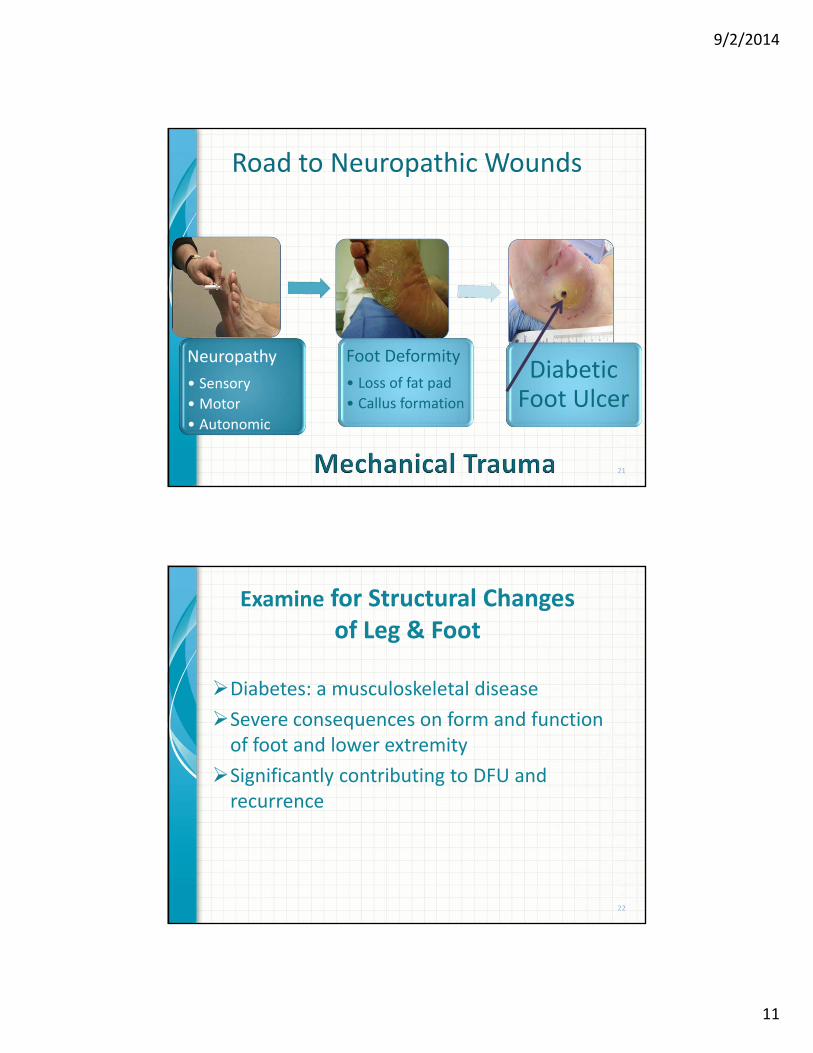
Road to Neuropathic Wounds
Neuropathy
• Sensory
• Motor
• Autonomic
Foot Deformity
• Loss of fat pad
• Callus formation
Diabetic Foot Ulcer
21
Examine for Structural Changes of Leg & Foot
Diabetes: a musculoskeletal disease
Severe consequences on form and function of foot and lower extremity
Significantly contributing to DFU and recurrence
22
9/2/2014
12
Advanced Glycosylation of End Products (AGE)
• Molecular glue ‐ chemical reaction between glucose & proteins
• Cross‐linking of proteins irreversible
• Changes in soft‐tissue extensibility and joint‐capsule mobility ‐ often manifest as decreased ROM
• Clinical marker of DM‐related complications
• Any joint can be affected by AGEs
• Reduction in ROM may be noticed when it interferes with functional activities including ambulation
• Seen in other areas of body…shoulder‐adhesive capsulitis23
Musculoskeletal Examination
Skeletal deformities
Range of motion
Muscle strength
Gait analysis
24

9/2/2014
13
Range of Motion Examination
• “Limited joint mobility in foot & ankle associated with higher plantar pressures.”
• Hallux Limitus‐Limited range of motion in the proximal great toe/Metatarsal‐phalangeal joint (MTP)
– Normal: 50‐70° dorsiflexion/extension
• Hallux Rigidus: Absence of ROM in IP joint of great toe
Normal ROM of MTP Jt Limited MTP &IP Jt ROM25
Ankle Equinus • Equinus‐ defined as ankle dorsiflexion measured at <0/neutral or
less
• Diabetes cohort, 16 of 43 patients (37.2%) equinus
• Compared with 9 of 59 nondiabetic participants (15.3%)
• Threefold risk of equinus in the diabetic population
• Equinus group had a history of ulceration in 52.0% compared with 20.8% of the nonequinus group
• Equinus imparted a fourfold risk of ulceration
• Found 2.8 times risk of equinus in patients with peripheral neuropathy
• CONCLUSIONS:
• “Equinus may be more prevalent in diabetic patients than previously reported. Study found a significant association between equinus and ulceration.” 26

9/2/2014
14
Ankle Equinus
Mild Equinus
Moderate Equinus
Severe Equinus 27
Ankle EquinusLimited Ankle Dorsiflexion
Actively
Knee Straight Knee Bent(gastrocnemius) (soleus)
28
• DuckworthT, Boulton A, Betts R, et al; Plantar pressure measurements and the prevention of ulceration in the diabetic foot. J Bone Joint Surg 67b 1985 p79‐85
• Lavery L, Armstrong D, Boulton A, Ankle equinus deformity and its relationship to high plantar pressure in a large population with diabetes mellitus JAPMA 92(9) 2002
9/2/2014
15
ROM Needed for Normal Gait Cycle
• Ankle – stance phase
– 0‐10° dorsiflexion
– 0‐20° plantarflexion for push‐off
– 0‐5° eversion at subtalar joint
• 1st Metatarsophalangeal joint
– 50‐60° of dorsiflexion during push off
– (deficiency is cause of shear stress in deep tissue)
• IP joint
– 10°
29
Objective ROM Testing
RangeOfMotionVL.flv
30
9/2/2014
16
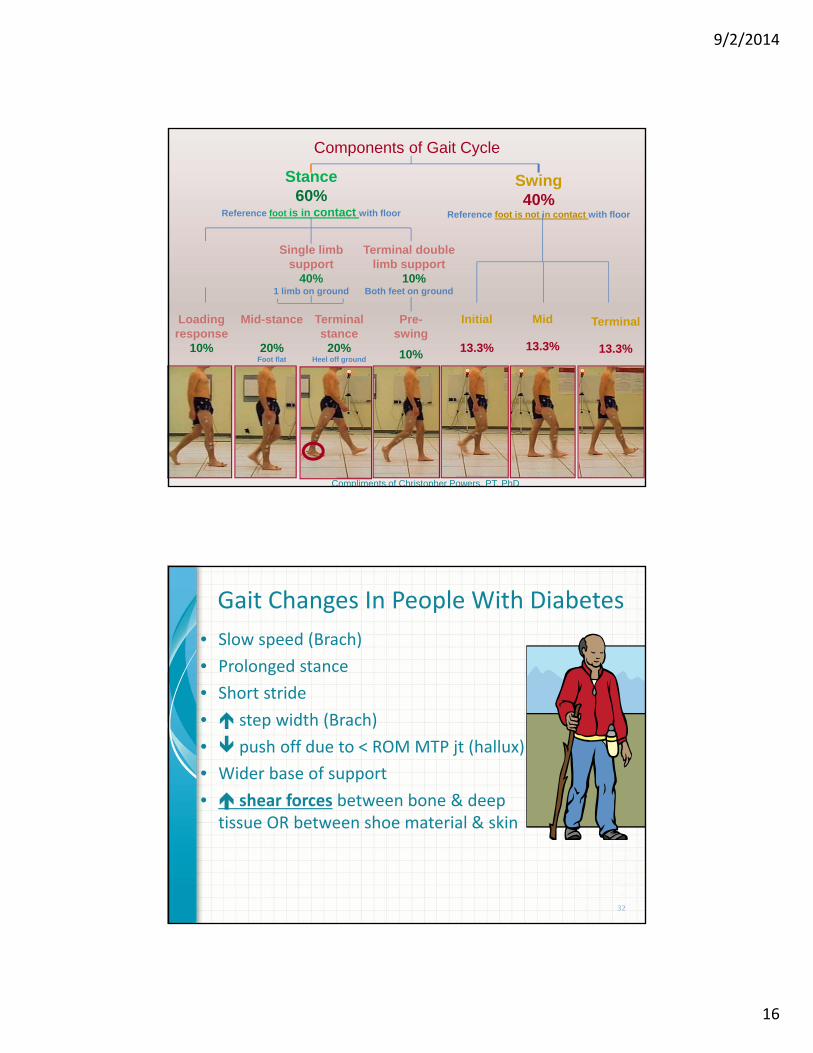
Components of Gait Cycle
Stance 60%
Reference foot is in contact with floor
Swing 40%
Reference foot is not in contact with floor
Single limb support
40%1 limb on ground
Terminal double limb support
10%Both feet on ground
Loading response
10%
Mid-stance
20%Foot flat
Terminal stance
20%Heel off ground
Pre-swing
10%
Initial
13.3%
Mid
13.3%
Terminal
13.3%
Compliments of Christopher Powers, PT, PhD
Gait Changes In People With Diabetes
• Slow speed (Brach)
• Prolonged stance
• Short stride
• step width (Brach)
• push off due to < ROM MTP jt (hallux)
• Wider base of support
• shear forces between bone & deep tissue OR between shoe material & skin
32

9/2/2014
17
Forces Measured by Force PlatformDuring Stance Phase of Gait
• Vertical forces
• Anteroposterior shear
• Mediolateral shear
Shear – what is its effect on deep tissue???
33Attribution: Rose Hamm, DPT, CWS
34

9/2/2014
18
Postural Changes in Peoplewith Diabetes
• Balance and postural awareness of body in space impaired
• Due to peripheral neuropathy & gastroc weakness due to ankle hypomobility
• More pronounced with diabetic retinopathy & decreased vision
• Increased sway with eyes open and head forward
• Unstable static balance
• Unstable dynamic balance
• Increased risk for falls 35
Common Cause of Mechanical Trauma
Poorly fitting shoes
36
Attribution: Rose Hamm, DPT, CWS
9/2/2014
19
What to Do???
37
Therapies to Improve Healing Opportunitiesin People with Diabetes
• Blood glucose control
• Wound bed preparation
– Debridement
– Infection/bioburden management
– Moisture management
– Edge
• Dressings – according to the characteristics of the wound
• Advanced wound dressings‐collagen, silver, honey
• Offloading38
9/2/2014
20
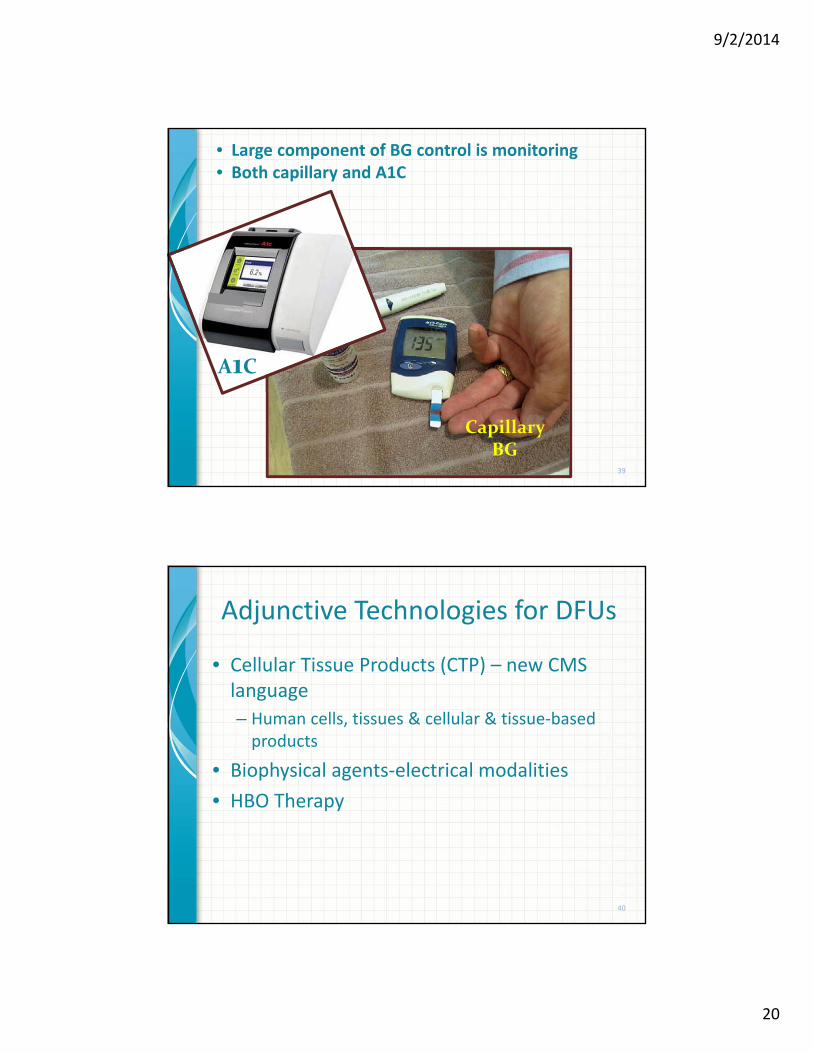
39
A1C
Capillary BG
• Large component of BG control is monitoring• Both capillary and A1C
Adjunctive Technologies for DFUs
• Cellular Tissue Products (CTP) – new CMS language
– Human cells, tissues & cellular & tissue‐based products
• Biophysical agents‐electrical modalities
• HBO Therapy
40
9/2/2014
21
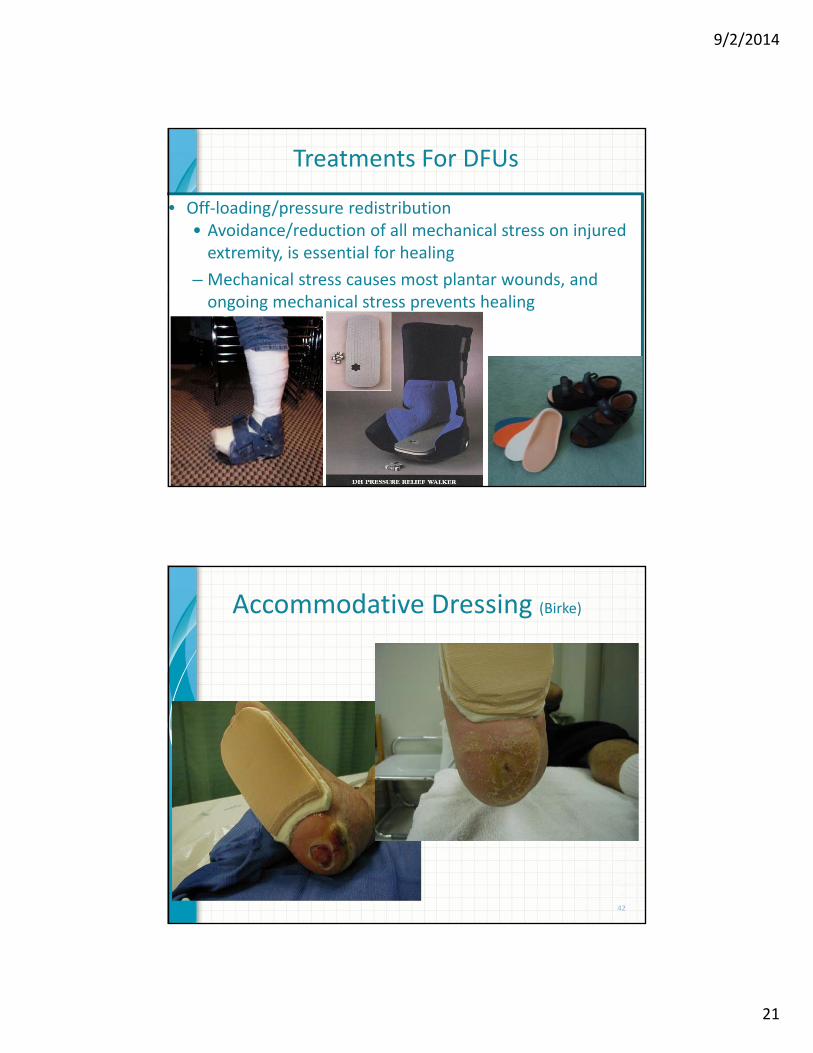
Treatments For DFUs
• Off‐loading/pressure redistribution• Avoidance/reduction of all mechanical stress on injured extremity, is essential for healing
– Mechanical stress causes most plantar wounds, and ongoing mechanical stress prevents healing
41
Accommodative Dressing (Birke)
42
9/2/2014
22
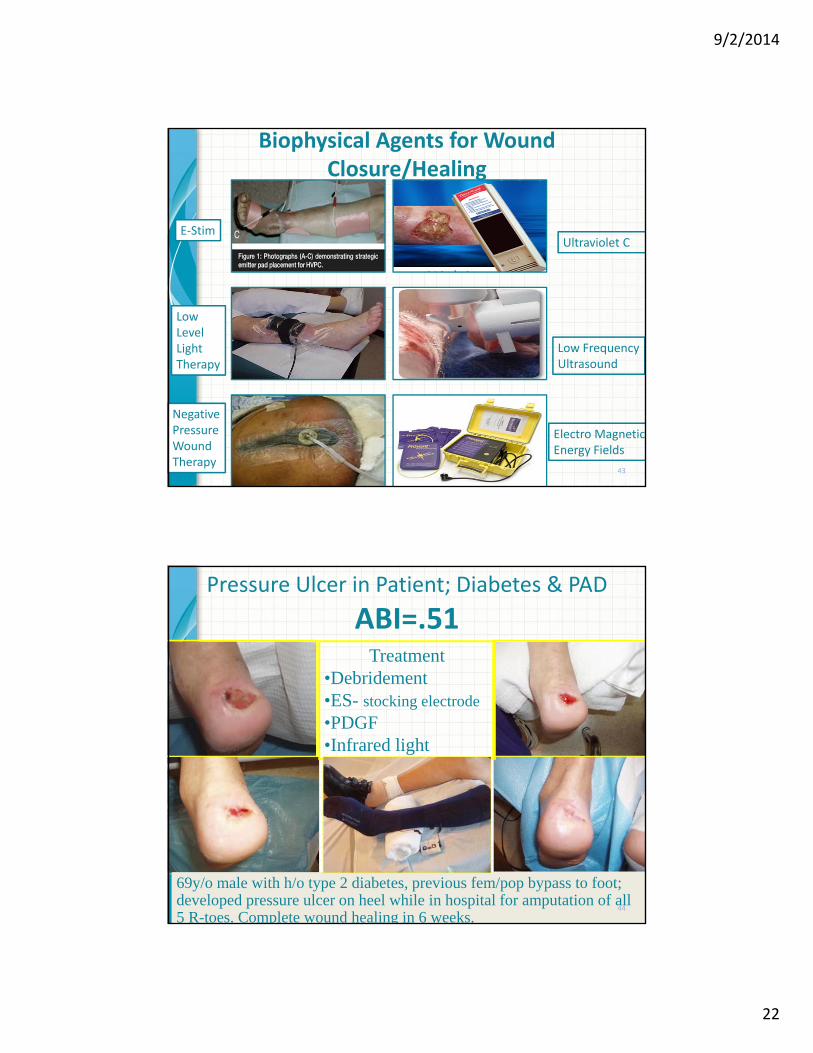
Biophysical Agents for Wound Closure/Healing
43
E‐Stim
LowLevelLightTherapy
NegativePressureWoundTherapy
Ultraviolet C
Low FrequencyUltrasound
Electro MagneticEnergy Fields
Pressure Ulcer in Patient; Diabetes & PAD
ABI=.51
69y/o male with h/o type 2 diabetes, previous fem/pop bypass to foot; developed pressure ulcer on heel while in hospital for amputation of all 5 R-toes. Complete wound healing in 6 weeks.
Treatment•Debridement•ES- stocking electrode
•PDGF•Infrared light
44
9/2/2014
23
10/08/01
45
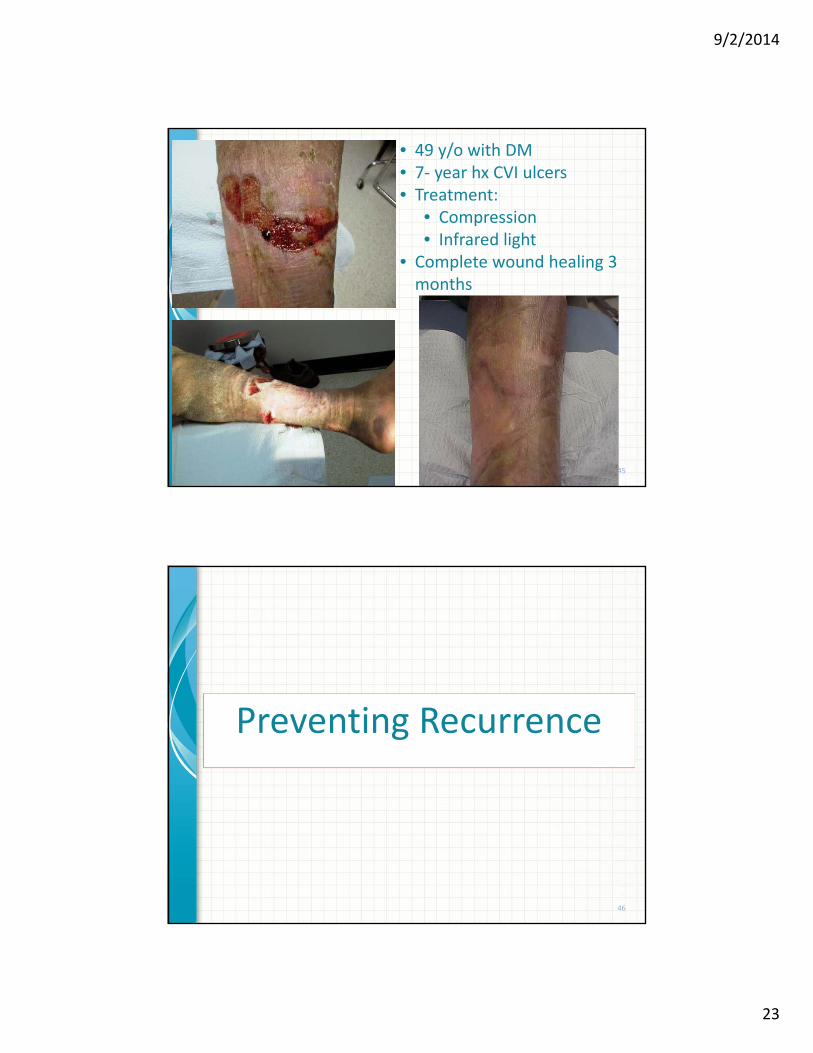
• 49 y/o with DM• 7‐ year hx CVI ulcers• Treatment:
• Compression• Infrared light
• Complete wound healing 3 months
Preventing Recurrence
46
9/2/2014
24
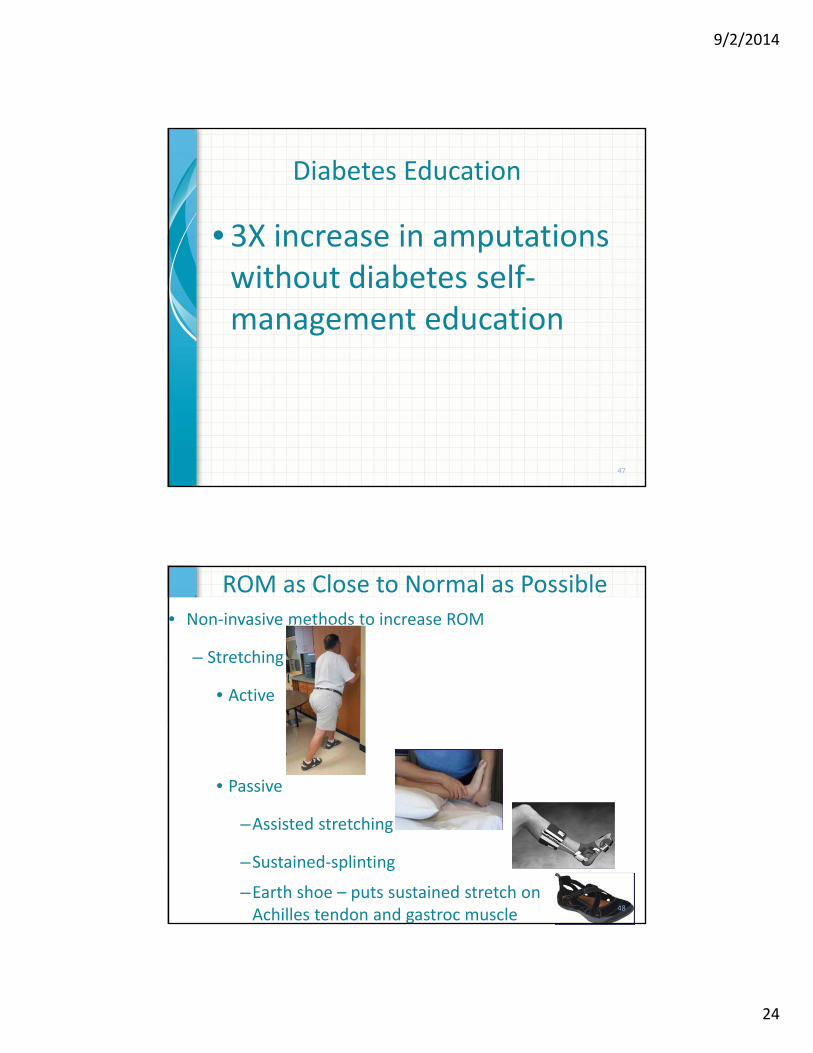
Diabetes Education
• 3X increase in amputations without diabetes self‐management education
47
ROM as Close to Normal as Possible• Non‐invasive methods to increase ROM
– Stretching
• Active
• Passive
–Assisted stretching
–Sustained‐splinting
–Earth shoe – puts sustained stretch on Achilles tendon and gastroc muscle
48
9/2/2014
25
Achilles Tendon Lengthening
• TCC 29 / 33 (88%) ulcers in healed (41=/‐ 28 days)
• Achilles Lengthening 30/30 ulcers (100%) healed (58+/‐ 47 days) (p >0.050)
• Recurrence of ulcer a 7 months (p = 0.001)– 16/27 (59%) in the total‐contact cast group
– 4/27 (15%) in the Achilles tendon lengthening group
• 2 year follow‐up Ulcer recurrence– 21/26 (81%) total‐contact cast group
– 10/26 (38%) Achilles tendon (p = 0.002)
49Mueller MJ, Sinacore DR, et al Effect of Achilles tendon lengthening on neuropathic plantar ulcers. A randomized clinical trial J Bone Joint Surg 2003 85 A(8) P 1436‐45
Attribution: Greg Bohn, MD
Footwear and Assistive Devices
50Courtesy: Rose Hamm, DPT, CWS

9/2/2014
26
Management of Post‐Healing Foot
• Medicare Therapeutic Shoe Bill
– Pays for diabetic shoes and inserts
– Patient must have diabetes, previous amputation, ulceration, pre‐ulcerative calluses, foot deformities, or poor circulation
– Must be under care of physician who is managing diabetes
51
Ensure Patients Get Shoes & Inserts
• Only small percentage of patients eligible for therapeutic shoes and insoles receive them
• Shoes and inserts decrease pressure, friction & shear
• Growing body of basic science work supports important role of friction and shear in ulcer development in insensate feet
• Patients wearing shear‐reducing insoles had fewer foot ulcers than patients with standard prevention therapy
• More research needed52
9/2/2014
27
Purpose of Footwear and Orthotics
• Redistribute pressure
• Optimize patient function
• Provide stability during gait/transfers
53
Is Shoe Gear Important???• Studies:
– 1st study: Patients in neuropathic group received therapeutic and custom shoes
• 26% had reulceration
• 83% reulceration ‐ wore their own footwear
– 2nd study: Randomized clinical trial of single style of shoe and insert for men and women was conducted in persons with prior foot ulcer at 2 study sites in Italy
• After 1 year, reulceration occurred in 28% of the therapeutic footwear group vs 58% in those wearing their own footwear.
54

9/2/2014
28
Educate Patients Exactly How to Perform a
Self‐Foot Exam
• Use adult learning principles
– Show ‐ visual
– Tell ‐ auditory
– Practice ‐ kinesthetic
• Provide follow‐up education
• Time for return demonstration
55
Evaluate Patient’s Ability to Perform Self‐Foot Exams
1. Assess knowledge of the
self‐exam
2. Assess vision
3. Assess flexibility
4. Assess skill using tools
1. Mirror 56
9/2/2014
29
Dermal Thermometer
57
CONCLUSIONS—Infrared temperature home monitoring, in serving as an “early warning sign,” appears to be a simple and useful adjunct in the prevention of diabetic foot ulcerations.
LAVERY LA, HIGGINS KR, LANCTOT DR: Preventing diabetic foot ulcer recurrence in high‐risk patients: Use of temperature monitoring as a self‐assessment tool. DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
ADA Guidelines for Foot Care in Patients With Diabetes
58

9/2/2014
30
ADA Guidelines for Foot Care in Patients With Diabetes (cont.)
59
Is Physician / Healthcare Provider Important???
• This study suggests that careful attention to foot care by health care professionals may be more important than therapeutic footwear
• But does not negate the possibility that special footwear is beneficial in persons with diabetes who do not receive such close attention to foot care by their health care providers or in individuals with severe foot deformities.
Reiber GE. Smith DG, Wallace C et al. Effect of Therapeutic Footwear on Foot Reulceration in Patients With Diabetes: JAMA. 2002;287(19):2552‐2558. 60

9/2/2014
31
A Component for Preventing Recidivism / RecurrenceScreen For Depression
• Studies show increased incidence of depression in people with diabetes
• Depression often causes decrease self‐care strategies
• Decreased self‐care creates increase incidence in complications including foot ulcers
J Am Podiatr Med Assoc 98(2): 130‐136, 2008 61
References• Luther C. Kloth, Joseph M. McCulloch:Wound Healing: Alternative in Management,
Contemporary Perspectives in Rehabilitation, 3rd edition 2001. F.A. Davis.• American Diabetes Association: Clinical Practice Recommendations 2012; Diabetes Care• Payne, CB, Biomechanics of the foot in diabetes mellitus. Some theoretical considerations.
J. Am Podiatric Medicine Association, 1998 June; 88(6): 285‐9• APhA Diabetic Foot Ulcer Protocol Panel: Management of Foot Ulcers in Patients with
Diabetes; APhA Drug Treatment Protocols, Journal of the American Pharmaceutical Association, 40(4): 467‐474, 2000
• Sussman, C, Bates‐Jensen, BM: Wound Care, A Collaborative Practice Manual for Health Professionals. Lippincott Williams & Wilkins, 2011
• A Core Curriculum for Diabetes Education, Fourth Edition, 2001, American Association of Diabetes Educators
• Diabetes Self‐Management Education Desk Reference‐Second Ed. AADE 2011.• Sanders LJ, Frykberg RG: Charcot Foot. In The Diabetic Foot. 5th ed. Levin ME, O’Neal LW,
Bowker JH, Eds. St. Louis, MO, Mosby, 1993, p. 149‐180• Zatouroff, M, Bouffler, LE: A Colour Atlas of The Foot in Clinical Diagnosis, Wolfe Publishing
Ltd, 1992, Aylesbury, England• Levin, ME, et al, The Diabetic Foot. 5th ed, Mosby St. Louis, MO 1993• Levin, LE: Preventing Amputation in the Patient with Diabetes, Diabetes Care, Vol 18, No
10, Oct 1995 p1383‐1394
62
9/2/2014
32
References
• Bowker, JH, Pfeifer MA. Levin and O’Neal’s The Diabetic Foot 6th Edition.2001, Mosby, St. Louis.
• Duffy, JC, Patout, CA: Management of the Insensitive Foot in Diabetes: Lessons Learned from Hansen’s Disease, Military Medicine, Vol. 155, p 575‐579, Dec. 1990
• Caputo, GM, Cavanagh, PR: Assessment and Management of Foot Disease in Patients with Diabetes, New Eng J of Med, 331:854‐860, Sept 29, 1994
• Fylling, CP: Wound healing: An update. Comprehensive Wound Management for prevention of amputation, Diabetes Spectrum, 1992; 5:358‐9
• Bild ED, Selby JV, et al: Lower extremity amputation in people with diabetes, epidemiology, and prevention, Diabetes Care 12: 1, 1989
• National Long Range Plan to Combat Diabetes 1987, National Diabetes Advisory Board, U.S. Department of Health and Human Services, 1987
• Brand PW: Repetitive stress in the development of diabetic foot ulcers, in The Diabetic Foot, 4th ed, Edited by Levin ME, O’Neal LW, St. Louis, CV Mosby Co, Inc, 83‐90 1988
• Sinacore DR, Total contact casting for diabetic neuropathic ulcers, Phys Ther, 1996, vol 76, 296‐301
63
References•Frykberg, Robert G., “The Diabetic Foot”; 61st Scientific Sessions of the American Diabetes Association; Day 1‐June 22, 2001.•Vinik, Aaron I., “Diabetic Neuropathy: A Small‐Fiber Disease” 61st Scientific Sessions of the American Diabetes Association, Day 1‐June 22, 2001•Vinik, Aaron I, “New Methods to Assess Diabetic Neuropathy for Clinical Research”, 60th Scientific Sessions of the American Diabetes Association, Day 4‐June 13, 2000•Suchkova VN, Baggs RB, et al. Ultrasound improves tissue perfusion in ischemic tissue through a nitric oxide dependent mechanism. ThrombHaemost 2002 Nov; 88(5): 865‐70.•Kavros SJ, Wagner SA, et al et al. Presented at SAWC 2002•Nichter LS, McDonald S, et al. Efficacy of debridement and primary closure of contaminated wounds: A comparison of methods. Ann Plast Surg 1989; 23: 224‐230.•Ukhov AI, Petrus VS, et al. Potentiation of the action of antibiotics by ultrasound. Antibiotiki i Meditsinskaia Biotekhnologiia 1985; 30(9): 684‐7.
64
9/2/2014
33
References
• Armstrong DG, Abu‐Ruman PL, Nixon BP, Boulton AJ. Continuous activity monitoring in persons at highrisk for diabetes‐related lower‐extremity amputation. Journal of the American Podiatric Association 2001;91(9):451‐455.
• Armstrong DG, Lavery LA, Wu S, Boulton AJ. Evaluation of removable and irremovable cast walkers in the healing of diabetic foot wounds: a randomized controlled trial. Diabetes Care 2005;28(3):551‐554.
• Birke JA, Lewis K, Penton A, Pittman D, Tucker A, Durand C. The effectiveness of a modified wedge shoe in reducing pressure at the area of previous great toe ulceration in individuals with diabetes mellitus. Wounds 2004;16(4). Retrieved from https://www.medscape.com/viewarticle/474841.
• Birke JA, Pavich MA, Patout CA, Horswell R. Comparison of forefoot ulcer healing using alternative off‐loading methods in patients with diabetes mellitus. Advances in Skin and Wound Care 2002;15(5):210‐215.
• Brach, JS, Talkowski JB, Strotmeyer ES, Newman AB. Diabetes Mellitus and gait dysfunction: possible explanatory causes. Physical Therapy 2008;88(11):1365‐1374.
65
References
McGuire J. Transitional off‐loading: an evidence‐based approach to pressure redistribution in the diabetic foot. Advances in Skin and Wound Care 2010;23:175‐188.
Nabuurs‐Franssen MH, Sleegers R, Huijberts MS, et al. Total contact casting of the diabetic foot in daily practice: a prospective follow‐up study. Diabetes Care 2000;19:213‐221.
Petrofsky J, Lee S, Bweir S. Gait characteristics in people with type 2 diabetes mellitus. European Journal of Applied Physiology 2005;93(5‐6):640‐647.
Rader AJ, Barry T. Football dressing for neuropathic forefoot ulcerations. Wounds 2006;18(4):85‐91.
Sacco IC, Amadio AC. Influence of the diabetic neuropathy on the behavior of electromyographic and sensorial responses in treadmill gait. Clinical Biomechanics 2003;18(5):426‐434.
Wrobel JS, Najafi B. Diabetic foot biomechanics and gait dysfunction. Journal of Diabetes Science and Technology 2010;4(4):833‐845.
66
Top Related