


![Idiopathic granulomatous mastitis: a diagnostic dilemma for the … · 2017. 8. 29. · ulomatousinflammatoryresponse[4].Oralcontraceptivescan cause a chemically induced granulomatous](https://static.fdocuments.us/doc/165x107/6080908ddddf1618501e8d3d/idiopathic-granulomatous-mastitis-a-diagnostic-dilemma-for-the-2017-8-29-ulomatousinflammatoryresponse4oralcontraceptivescan.jpg)



Languages
Pages
Legal


MANAGEMENT OF IDIOPATHIC MANAGEMENT OF IDIOPATHIC GRANULOMATOUS MASTITISGRANULOMATOUS MASTITIS
Canon CHANCanon CHANDepartment of Surgery, North District Hospital. Department of Surgery, North District Hospital.
Hong Kong SARHong Kong SAR

Idiopathic Granulomatous Idiopathic Granulomatous Mastitis (IGM)Mastitis (IGM)
►Kessler and Wolloch 1972Kessler and Wolloch 1972►Cohen 1977Cohen 1977
Chronic granulomatous lobulitis Chronic granulomatous lobulitis Absence of an obvious etiologyAbsence of an obvious etiology
Kessler E, Wolloch Y. Am J Clin Pathol, 1972
Cohen C. S Afr Med J 1977

IntroductionIntroduction
►Rare inflammatory breast diseaseRare inflammatory breast disease►Unknown etiologyUnknown etiology►Women of childbearing ageWomen of childbearing age►Simulate breast cancer Simulate breast cancer
Breast massBreast mass Nipple retractionNipple retraction
Sakurai et al. Breast Cancer 2002
Cakir et al. Breast J 2002

IntroductionIntroduction
►Diagnosis is one of exclusionDiagnosis is one of exclusion Infectious and noninfectious causesInfectious and noninfectious causes Carcinoma/ carcinomatous mastitisCarcinoma/ carcinomatous mastitis Wegener granulomaWegener granuloma SarcoidosisSarcoidosis TuberculosisTuberculosis Histoplasmosis Histoplasmosis
Erhan et al. Breast 2000
Topic of interestTopic of interest
►The pathogenesis is not clear►Etiology unknownEtiology unknown►Treatment strategy controversialTreatment strategy controversial

Current argumentsCurrent arguments
► An etiology for an idiopathic disease?An etiology for an idiopathic disease? Oral contraceptive pillsOral contraceptive pills Pregnancy and lactationPregnancy and lactation InfectiveInfective Autoimmune processAutoimmune process Immune response to extravasated secretions Immune response to extravasated secretions
from lobulesfrom lobules
Kessler et al. Am J Clin Pathol. 1972
Cohen et al. S Afr Med J. 1977
Brown et al. Am J Surg. 1979
Imoto et al. Jpn J clin Oncol. 1997
Cserni et al. Breast J. 1999

IGM - PresentationIGM - Presentation
► PainPain► Swelling/ massSwelling/ mass► Discharge/ galactorrhoeaDischarge/ galactorrhoea► Nipple retractionNipple retraction► Skin ulcersSkin ulcers

IGM – Physical examinationIGM – Physical examination
► Skin ulcerationSkin ulceration► MassMass► IndurationInduration► AbscessAbscess► FistulaFistula► Enlarged lymph Enlarged lymph
nodenode Up to 15% of casesUp to 15% of cases
Asoglu et. al The Breast Journal. 2005

IGM - InvestigationsIGM - Investigations

IGM - investigationsIGM - investigations
►Manage as a breast massManage as a breast massMammography (MMG)/ Ultrasound (USG)/ Mammography (MMG)/ Ultrasound (USG)/ Magnetic Resonance Imaging (MRI)Magnetic Resonance Imaging (MRI)Fine needle aspiration cytology (FNAC)Fine needle aspiration cytology (FNAC)Core biopsyCore biopsy
Mammography in IGMMammography in IGM
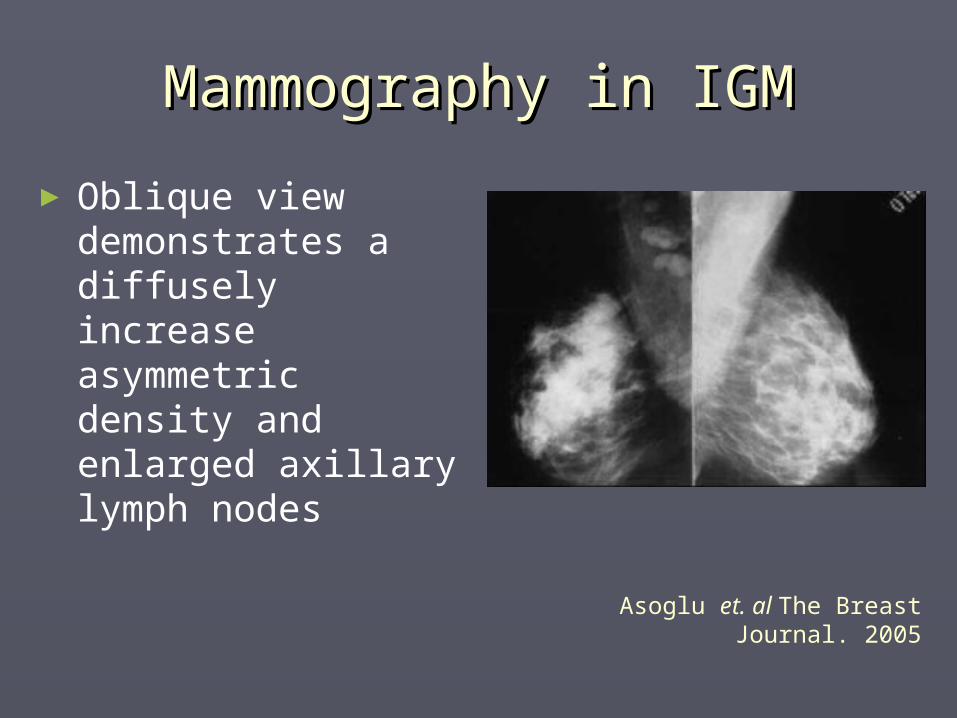
► Oblique view demonstrates a diffusely increase asymmetric density and enlarged axillary lymph nodes
Asoglu et. al The Breast Journal. 2005
Mammography and IGMMammography and IGM
► Small, multiple, ill-defined masses without microcalcification
► Most commonly reported finding of IGM is an asymmetrically increased density without a distinct margin or mass effect, though this is not specific
► Low sensitivity caused by dense breast tissue limits the value of MMG in this age group
► In patients having dense breast parenchyma, MMG may be negative
Memis A et al. Clin Radiol. 2002Han BK et al. AJR Am J Roentgenol.
1999

Ultrasound and IGMUltrasound and IGM
► Hypoechoic indistinctly bordered heterogeneous masses
► May be connected by a few tubular hypoechoic structures
Kocaoglu et al. J Comput Assist Tomogr. 2004

MRI and IGMMRI and IGM► Segmental heterogeneity
► Hypointense on precontrast T1-weighted images and hyperintense on T2-weighted sequences
► Postcontrast dynamic T1-weighted scans showed heterogeneously enhancing ring-like abscesses
► Abscess walls reveal a benign type time-signal intensity curve (gradual and progressive enhancement without washout)
Kocaoglu et al. J Comput Assist Tomogr. 2004

Imaging and IGMImaging and IGMNN USGUSG MMGMMG MRIMRI
Schelfout et al.2001
11 Asymmetric diffuse increaseddensity
Focal irregular homogeneouslyenhanced masses
Van Ongeval et al.
1997
11 Inhomogeneous hypoechoic lesion with posterior acoustic shadow
Bilateral diffuse increased density ofthe fibroglandular tissue
An irregular ring-shaped enhancedlesion
Cakir et al.2002
11 Inhomogeneous hypoechoic lesionwith posterior acoustic shadow
Unilateral diffuse increased density Heterogeneously enhanced irregularlesion and gradual and progressive
enhancement without washout
Sakurai et al.2002
11 Inhomogeneous hypoechoic lesionwith posterior acoustic shadow
Unilateral diffuse increased density Irregularly enhanced mass withoutcontrast washout
Memis et al.2002
1515 Irregular hypoechoic mass withtubular extensions
Asymmetric opacities
Kara et al.2003
11 Well-defined hypoechoic areas withtubular extensions
Asymmetric densities with skinthickening
Engin et al1999
1010 Heterogeneous hypoechoic masses,circumscribed opacities,
and abscess cavities with sinustracts
Circumscribed opacities asymmetric dense parenchyma,nodular opacities
parenchymal distortion ,and bilateral dense parenchyma
Yilmaz et al2001
1212 Heterogeneous hypoechoic areaswith/without tubular extensions, hypoechoic irregular mass, and
edematous breast withskin thickening
Focal asymmetric density withoutmass formation, irregular
masses, and negative
Han et al1999
99 Tubular hypoechoic lesionsand oval hypoechoic masses withhypoechoic tubular connections
Multiple small ill-defined masses and local asymmetric
density
Idiopathic granulomatous mastitis is rare; hence, the number of patients in these studies can not make generalizations
Biopsy still remains the golden method of definite diagnosis
IGM - FNACIGM - FNAC
► The cytological diagnosis is difficult and often does not deliver any diagnostic information ~30% can be diagnosed by FNAC only
► The absence of necrosis and a predominantly neutrophil infiltrate in the background favor the diagnosis these signs overlap with other etiologies:
Tuberculosis Azlina AF et al. World J Surg 2003Sakurai T et al. Breast Cancer. 2002Kumarasinghe MP Acta Cytol. 1997Imoto S et al. Jpn J Clin Oncol. 1997
IGM - BiopsyIGM - Biopsy
► Gold standard in diagnosis of IGMGold standard in diagnosis of IGM
► Histological featuresHistological features Granulomas (100%) Background of inflammatory infiltrate (88%) Foamy macrophages and multinucleated giant
cells (65%) Microabscesses The ducts appear normal without evidence of
malignancy or caseation Stains for fungi and acid-fast bacilli are negative
Ramachandram K et al. Pathology. 2004
Histological reviewHistological review
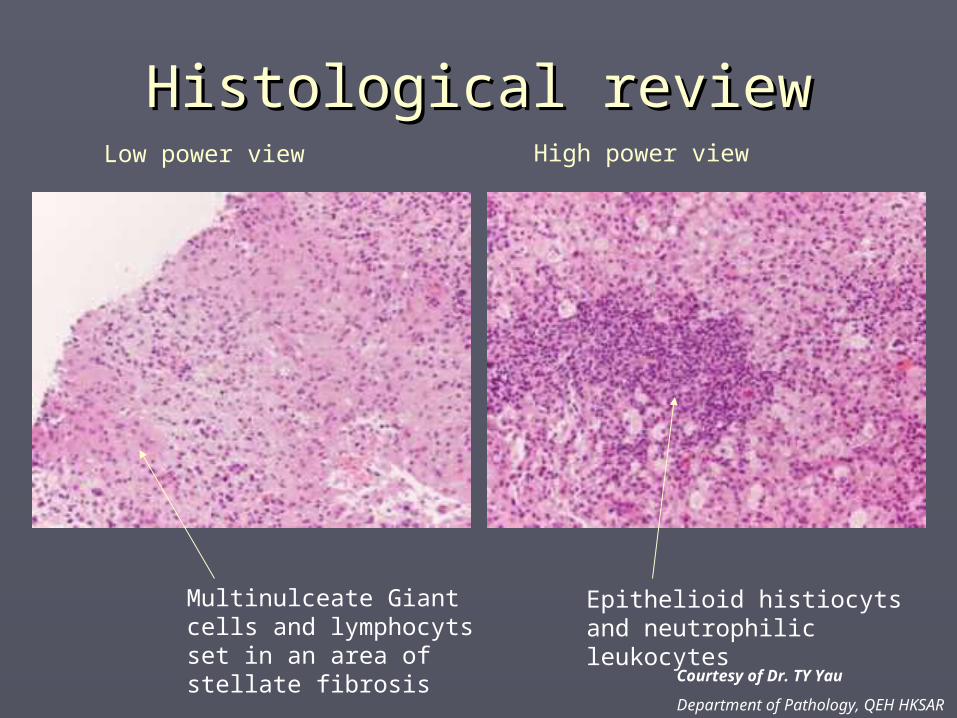
Multinulceate Giant cells and lymphocyts set in an area of stellate fibrosis
Epithelioid histiocyts and neutrophilic leukocytes
Low power view High power view
Courtesy of Dr. TY Yau
Department of Pathology, QEH HKSAR

IGM - TreatmentIGM - Treatment
Current ArgumentsCurrent Arguments
►Management optionsManagement options Surgical excisionSurgical excision
►Wide local excision +/- reconstructionWide local excision +/- reconstruction►Invasive procedure for a benign disease entityInvasive procedure for a benign disease entity
Systemic steroid/ immunosuppressantSystemic steroid/ immunosuppressant►Immune suppressionImmune suppression►Underlying infective cause renders its use a Underlying infective cause renders its use a
concernconcern

Surgical excisionSurgical excision
►Asoglu Asoglu et al.et al. The Breast J. 2005. The Breast J. 2005. 18 patients with IGM18 patients with IGM All underwent surgical excision with All underwent surgical excision with
negative marginsnegative margins Mean follow up 18 monthsMean follow up 18 months Recurrence rate 6%Recurrence rate 6%

Prednisolone managementPrednisolone management
► DeHertogh DeHertogh et al. et al. N. Eng. J. Med. 1980.N. Eng. J. Med. 1980. Short course high dose prednisoloneShort course high dose prednisolone Single patient case reportSingle patient case report Short follow up periodShort follow up period Recurrence was not reportedRecurrence was not reported
► Azlina Azlina et al.et al. World J Surg. 2003. World J Surg. 2003. 25 patients with mean follow up of 6.5 months25 patients with mean follow up of 6.5 months Recurrence up to 50% for steroid treatmentRecurrence up to 50% for steroid treatment Short follow up periodShort follow up period

Conservative ManagementConservative Management
►Lai Lai et al.et al. Breast Journal. 2005. Breast Journal. 2005. 9 women with mean followed up of 18.7 9 women with mean followed up of 18.7
monthsmonths 50% spontaneous complete resolution 50% spontaneous complete resolution
after 14.5 monthsafter 14.5 months
Small size reviewSmall size review

Conservative vs SurgeryConservative vs Surgery
►Al-Khaffaf et al. J Am Coll Surg. 2008
18 patients wth IGM 25 years retrospective review FU period not mentioned Steriod use/ antiobiotic/ surgical procedures compared
► Overall outcomes were not related to any combination of treatment options
► All patients spontaneously resolved regardless of treatment used, it may be best to let this condition “burn out.”
MANAGEMENT OF IDIOPATHIC GRANULOMATOUS MASTITIS
EXPERIENCE FROM A REGIONAL HOSPITAL
CANON CHAN, N. S. C HO, M. POON, M. T. CHEUNGDepartment of Surgery, Queen Elizabeth Hospital.
Hong Kong SAR
ObjectiveObjective
This study is aimed to This study is aimed to determine the best determine the best
treatment modality for treatment modality for IGMIGM

Queen Elizabeth HospitalQueen Elizabeth Hospital

MethodsMethods
► A retrospective review A retrospective review
► Twenty three women with histopathologic Twenty three women with histopathologic diagnosis of IGM between 1997 and 2006 diagnosis of IGM between 1997 and 2006 was performedwas performed
► The difference in presentation, recurrence The difference in presentation, recurrence and outcome between those treated by and outcome between those treated by surgical intervention and those managed surgical intervention and those managed conservatively were assessed conservatively were assessed
ResultsResults
► The women had a mean follow-up of 22.7 months The women had a mean follow-up of 22.7 months and a mean age of 40 years (range 22-55 years) and a mean age of 40 years (range 22-55 years)
► Clinically and radiologically, 13% of the women Clinically and radiologically, 13% of the women were suspected to have malignancy were suspected to have malignancy
► All patients had unilateral involvementsAll patients had unilateral involvements
► None of the patient were pregnant or lactatingNone of the patient were pregnant or lactating
► None of the patient were given systemic steroid None of the patient were given systemic steroid therapytherapy

ResultsResults
► PresentationPresentation
Mass(n=19)83%
Ulcer(n=1)4%
Abscess(n=3)13%
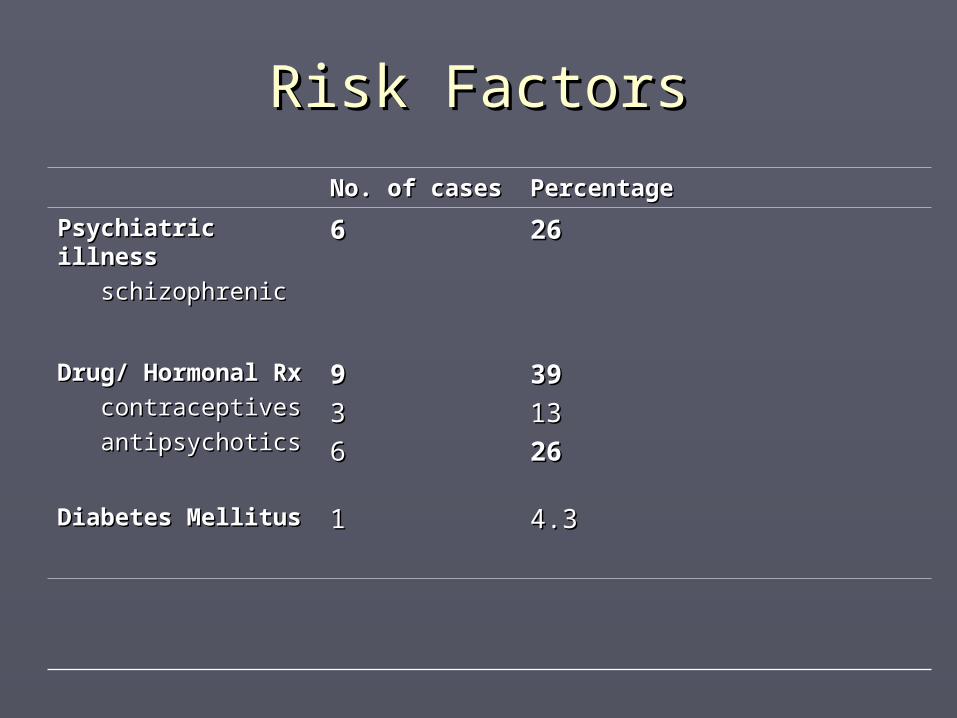
Risk FactorsRisk Factors
No. of casesNo. of cases PercentagePercentage
Psychiatric illnessPsychiatric illness
schizophrenicschizophrenic
66 2626
Drug/ Hormonal Drug/ Hormonal RxRx
contraceptivescontraceptives
antipsychoticsantipsychotics
99
33
66
3939
1313
2626
Diabetes MellitusDiabetes Mellitus 11 4.34.3
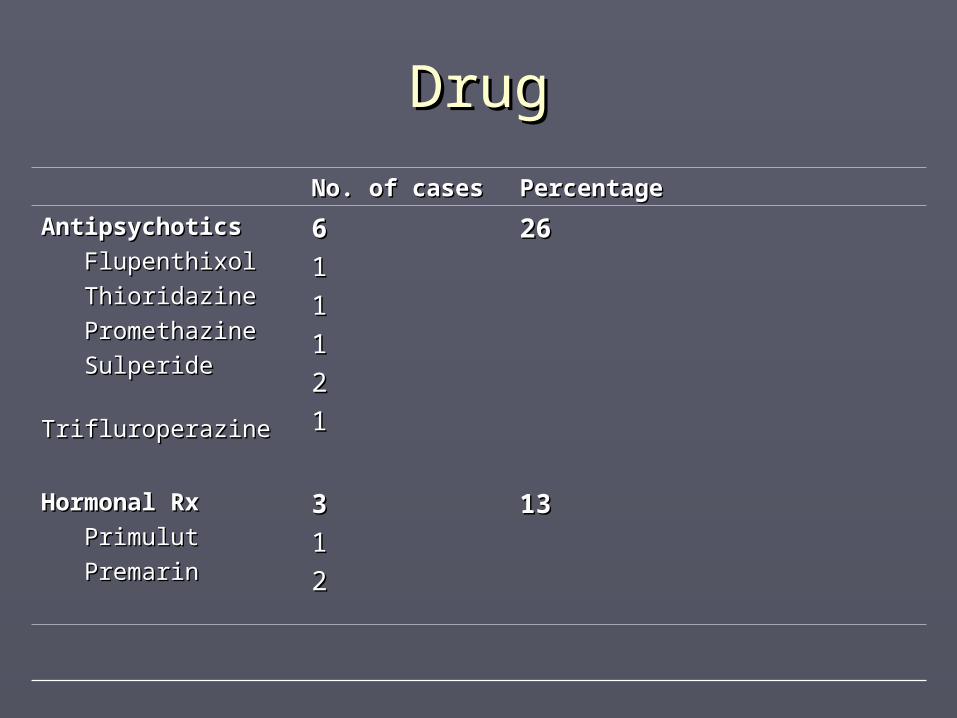
DrugDrug
No. of casesNo. of cases PercentagePercentage
AntipsychoticsAntipsychotics
FlupenthixolFlupenthixol
ThioridazineThioridazine
PromethazinePromethazine
SulperideSulperide
TrifluroperazineTrifluroperazine
66
11
11
11
22
11
2626
Hormonal RxHormonal Rx
PrimulutPrimulut
PremarinPremarin
33
11
22
1313

ResultsResults
► TreatmentTreatment
I&D17%
Lumpectomy35%
Expectant48%
Results – Expectant Results – Expectant managementmanagement
►91% of the patients had spontaneous 91% of the patients had spontaneous complete resolution of disease without complete resolution of disease without recurrencerecurrence
►Mean interval of 12 months. Mean interval of 12 months.
►Remaining patients had either Remaining patients had either recurrence (4.5%) or static disease recurrence (4.5%) or static disease (4.5%)(4.5%)
Results – Surgical treatmentResults – Surgical treatment
►85% of patients had resolution of 85% of patients had resolution of disease after either lumpectomy or disease after either lumpectomy or surgical drainage of abscesssurgical drainage of abscess
►Two patients (15%) had disease Two patients (15%) had disease recurred and one of them (7.5%) recurred and one of them (7.5%) eventually became static after eventually became static after followed up for 24 monthsfollowed up for 24 months
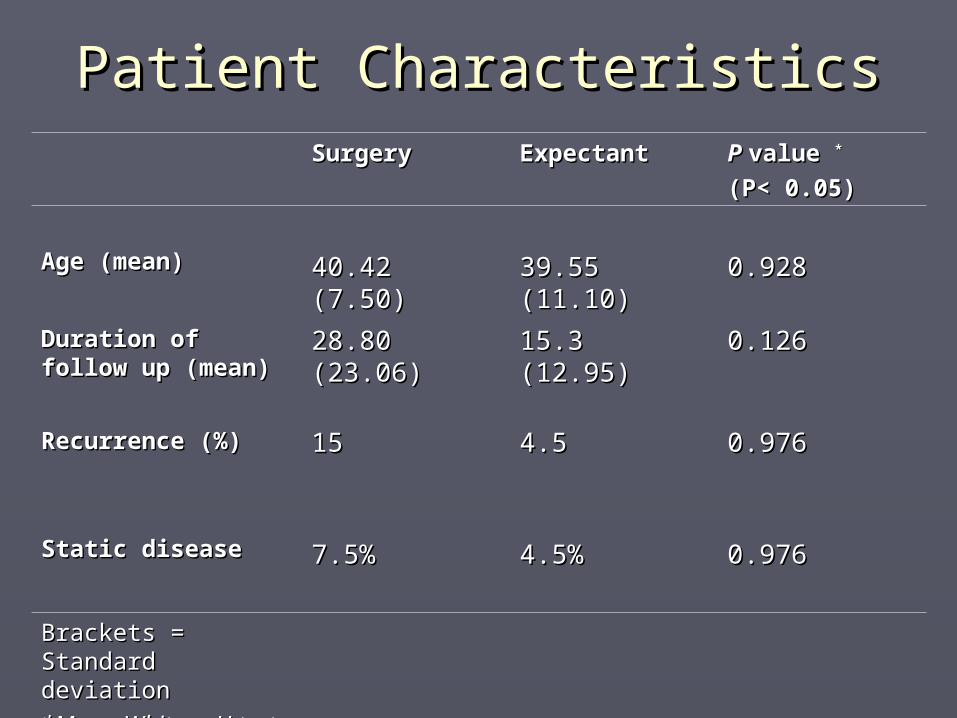
Patient CharacteristicsPatient CharacteristicsSurgerySurgery ExpectantExpectant P P value value **
(P< 0.05)(P< 0.05)
Age (mean)Age (mean) 40.42 (7.50)40.42 (7.50) 39.55 (11.10)39.55 (11.10) 0.9280.928
Duration of follow Duration of follow up (mean)up (mean)
28.80 (23.06)28.80 (23.06) 15.3 (12.95)15.3 (12.95) 0.1260.126
Recurrence (%)Recurrence (%) 1515 4.54.5 0.9760.976
Static diseaseStatic disease 7.5%7.5% 4.5%4.5% 0.9760.976
Brackets = Standard Brackets = Standard deviationdeviation
*Mann-Whitney U *Mann-Whitney U testtest
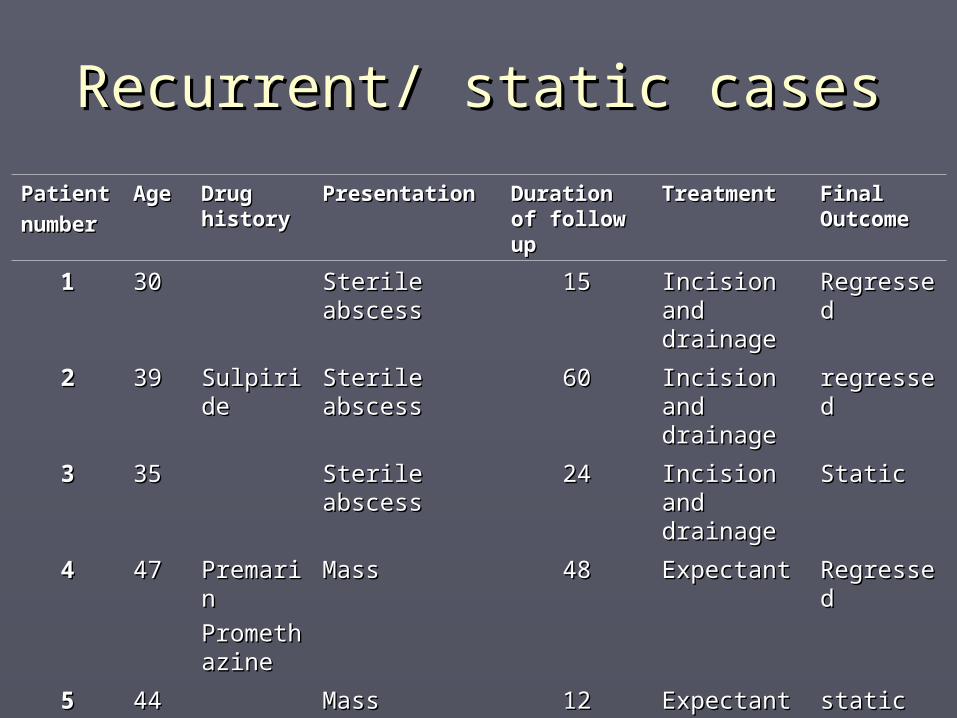
Recurrent/ static casesRecurrent/ static cases
PatientPatient
numbernumberAgeAge Drug Drug
historyhistoryPresentationPresentation Duration Duration
of follow of follow upup
TreatmentTreatment Final Final OutcomeOutcome
11 3030 Sterile Sterile abscessabscess
1515 Incision Incision and and drainagedrainage
RegresseRegressed d
22 3939 SulpiridSulpiridee
Sterile Sterile abscessabscess
6060 Incision Incision and and drainagedrainage
regresseregressedd
33 3535 Sterile Sterile abscessabscess
2424 Incision Incision and and drainagedrainage
Static Static
44 4747 PremariPremarinn
PromethPromethazineazine
MassMass 4848 ExpectantExpectant RegresseRegressedd
55 4444 MassMass 1212 Expectant Expectant staticstatic

ConclusionsConclusions
► It is important to exclude malignancy by It is important to exclude malignancy by histopathology in IGMhistopathology in IGM
► The presence of a breast mass in a woman The presence of a breast mass in a woman with history of hormonal therapy or with history of hormonal therapy or antipsychotic drug use should alert the antipsychotic drug use should alert the differential diagnosis of IGMdifferential diagnosis of IGM
► Our results suggest expectant management Our results suggest expectant management with close regular surveillance has an with close regular surveillance has an acceptable recurrence rate of 4.5% and it is acceptable recurrence rate of 4.5% and it is the treatment of choice for patients with IGM the treatment of choice for patients with IGM
Hyperprolactinaemia and Hyperprolactinaemia and IGM?IGM?
► Antipsychotics block D2 receptors on Antipsychotics block D2 receptors on lactotroph cells and remove inhibitory lactotroph cells and remove inhibitory influence on prolactin secretioninfluence on prolactin secretion
► Seen in 40-60% of antipsychotic usersSeen in 40-60% of antipsychotic users► Causes breast enlargement and Causes breast enlargement and
galactorrhoeagalactorrhoea► Baseline levels take up to 3 weeks to return Baseline levels take up to 3 weeks to return
to normalto normal
► No study has yet looked into the association No study has yet looked into the association between antipsychotic usage and IGMbetween antipsychotic usage and IGM
Wieck, A.et al. British Journal of Psychiatry. 2003.
Future studyFuture study
►Randomized controlled trialRandomized controlled trial Difficulty lies in the rarity of this disease Difficulty lies in the rarity of this disease
entityentity
►Relationship between antipsychotics Relationship between antipsychotics and IGMand IGM Elevated serum prolactin level?Elevated serum prolactin level?
Cserni G, Szajki K. Breast J., 1999
Rowe PM. Br. J. Clin. Pract. 1984

Thank youThank you
IGM in the male breastIGM in the male breast
Reddy et al. The Breast Journal. 2005
Top Related