







Languages
Pages
Legal


11/16/2011
1
M24: ReThink Health: Leadership for System Innovation
An initiative of the Fannie E Rippel Foundation
To contact session faculty or to pursue questions,
please contact Sherry Immediato,
Chief Learning Officer, ReThink Health
Session Faculty• Elliott Fisher, MD, MPH - Director, Population Health and Policy, The Dartmouth
Institute for Health Policy and Clinical Practice; founding member ReThink Health
• Kate Hilton, MTS, JD - Director, Organizing for Health and Leading Change Project
at Harvard University
• Gary Hirsch, SM – Consultant, Gary B. Hirsch Consultant - Creator of Learning
Environments
• Sherry Immediato, MPP, MBA – Chief Learning Officer, ReThink Health
• Laura Landy, MBA - President & CEO, ReThink Health/The Fannie E. Rippel
Foundation
• Michael McGinnis, PhD - Director, Managing the Health Commons, and Director,
Workshop in Political Theory and Policy Analysis Indiana University-Bloomington
• Bobby Milstein, PhD, MPH - Director, Systems Strategy & Programs ReThink
Health/The Fannie E. Rippel Foundation
• Ruth Wageman, PhD – Director of Research, ReThink Health and Visiting Faculty
Harvard University-Harvard College

11/16/2011
2
Objectives
• Rethink what it takes to achieve the IHI Triple Aim in
your organization and community or region
• Distinguish between strategies designed to yield
incremental improvement and high-leverage
innovation
• Explore a suite of practical, relationship-based tools
to understand and lead health system
transformation
• Engage with colleagues who are re-orienting their
systems
Disclosures• Elliott Fisher: This presenter has nothing to disclose.
• Kate Hilton: This presenter has nothing to disclose.
• Gary Hirsch: This presentation will discuss software packages, but Gary Hirsch,
does NOT have a significant financial interest or other relationship with the
manufacturer of any of the software packages.
• Sherry Immediato: This presentation may mention the "Leading for Health"
program offered by the Society for Organizational Learning, Inc. and/or the Fannie
E. Rippel Foundation. Sherry Immediato is paid to lead these programs. Both
organizations are non-profit corporations.
• Laura Landy: This presenter has nothing to disclose.
• Michael McGinnis: This presenter has nothing to disclose.
• Bobby Milstein: This presenter has nothing to disclose.
• Ruth Wageman: This presenter has nothing to disclose.

11/16/2011
3
Session Agenda
1. Welcome – The ReThink Health Story
2. What do we need/want to rethink?
3. Our leadership stories – what calls us to leading for health?
4. Managing the Health Commons
5. Essential Competences for Collaborating
6. ReThink Health Dynamics –Using Simulations to Improve Decision Making
7. Organizing for Health –People, Power and Change
8. Building Collaborative Leadership Teams for Community Efforts
9. Laura - Evaluation – closing recap
Founded 1953
An Innovation Story
11/16/2011
4
Julius A. Rippel
• 1959 - Hospital facilities should be adapted to the
patients rather than the opposite.
• 1967 – To avoid becoming sick may be the greatest
health and medical challenge to contemporary society.
• 1968 – Sooner or later some group will find out how to
build, organize and operate a hospital which will be
better and more flexible than at present, and at a lower
cost.
• 1969 – We need to develop a “health care” system
which will be recognized as distinct from “medical
care”. This is a real key to solving our “medical
problem”.
Julius A. Rippel
• 1980 – It seems clear that we have been living in a period of
excesses which cannot continue unabated.
One thing seems inescapable. Some persons will suffer from
what is ahead – in spite of all our social and political concern.
The major problem will be to restrict the damage done to our
entire population.

11/16/2011
5
Acting Results
Values &
Expectations
ReThinking
Thinking
Catalytic
Methods
Reacting
Rethinking
Reflecting
A collaborative organization that works to build
capacity for transforming health and health care
with a goal of better population health,
improved access, excellent care and sustainable
costs.

11/16/2011
6
Don Berwick, CMS, IHI
Elliott Fisher, The Dartmouth Institute
Amory Lovins, Rocky Mountain Institute
Jay Ogilvy, Global Business Network
Celinda Lake, Lake Research
John Sterman, MIT System Dynamics
Group
Marshall Ganz, Leading Change, Harvard
Peter Senge, MIT and the Society for
Organizational Learning
Elinor Ostrom, Nobel Laureate in
Economics, Indiana University
Laura Landy, Rippel Foundation
Principles
• Health as a Commons
• Shared Vision
• A Third Way
• Systems Thinking
• Leadership
• Cross Sector Collaboration
• Public Narrative
• Local Action
• Triple Aim
11/16/2011
7
ReThink Health
• Managing the Health Commons
• Leading for Health
• ReThink Health Dynamics
• Organizing for Health
• ReThink Health Research
What do we want/need to rethink?
• In particular, what do you want to rethink today?
What is a question that has been on your mind
relative to your own leadership?
– “What would it take to … (a result you want)?”

11/16/2011
8
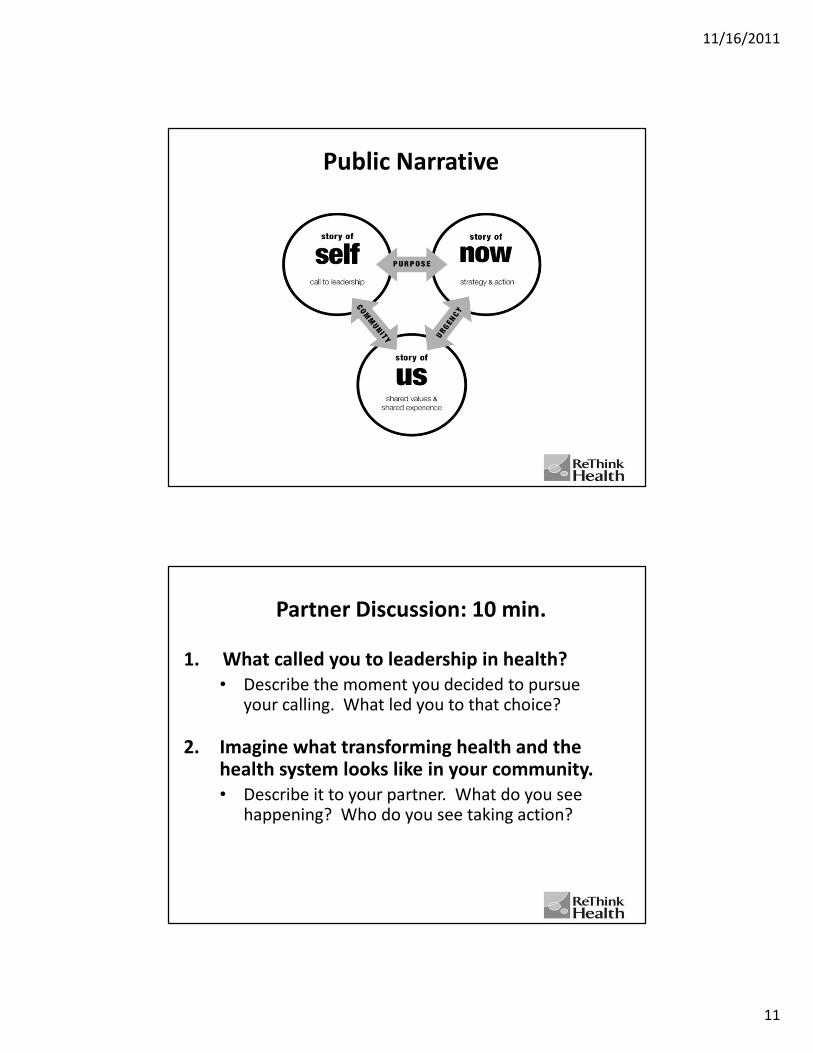
Public Narrative
A leadership practice through
which we motivate others to
join us in action
Public Narrative
11/16/2011
9
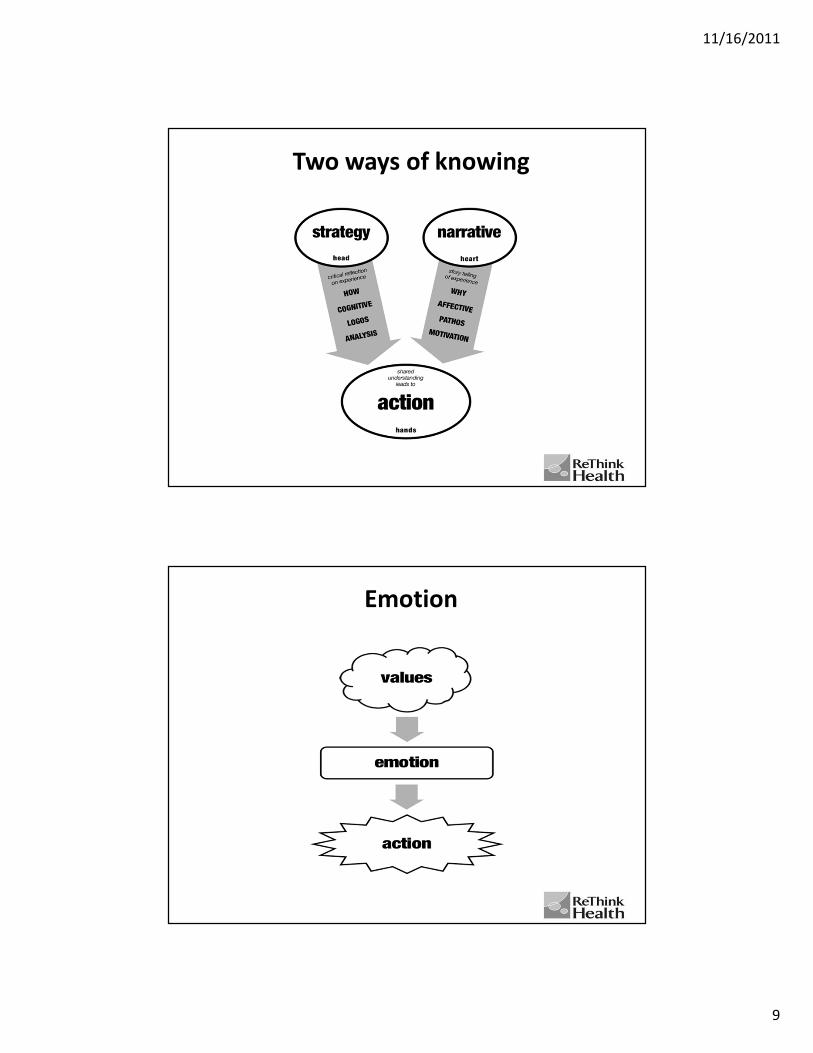
Two ways of knowing
Emotion

11/16/2011
10
Action Motivators
Challenge-Choice-Outcome
11/16/2011
11
Public Narrative
Partner Discussion: 10 min.
1. What called you to leadership in health?
• Describe the moment you decided to pursue your calling. What led you to that choice?
2. Imagine what transforming health and the health system looks like in your community.
• Describe it to your partner. What do you see happening? Who do you see taking action?

11/16/2011
12
Collaborative Stewardshipof a Health Commons:
Michael D. McGinnis, Ph.D.
ReThink Health, Fannie E. Rippel Foundation, and
Workshop in Political Theory and Policy Analysis, Indiana University
Presenter Disclosure Statement
Michael D. McGinnis
• Personal financial relationships with commercial
interests relevant to this presentation that existed
during the past 12 months: NO RELATIONSHIPS TO
DISCLOSE
• My presentation DOES NOT include discussion of
“off-label” use of any products.

11/16/2011
13
Acknowledgement of Research Collaborators
• This presentation draws on results generated by all members of the
Indiana University Managing the Health Commons (MHC) research
team, composed of myself and
– Elinor Ostrom, Ph.D., Distinguished Professor, Political Science
and Public and Environmental Affairs
– Joan Pong Linton, Ph.D., Associate Professor, English
– Claudia Brink, MBA, MPA, Ph.D. candidate in Public Policy, and
Assistant Director, Workshop
– Carrie Ann Lawrence, Ph.D. candidate in Health Behavior
– Ryan Conway, Ph.D. candidate in Political Science
• We has also benefited greatly from our interactions with other
research and research-action teams in the ReThink Health initiative,
funded by The Fannie E. Rippel Foundation.
A Regional Approach to Health Reform
• Health and medical care are intrinsically local or regional.
– Researchers have documented a wide range of regional
variation in costs and the overall quality of medical services.
– A reasonable presumption is that someone did something in
these communities that contributed to positive outcomes,
and our guess is that they developed informal mechanisms of
collaborative stewardship at the regional level.
26

11/16/2011
14
A Regional Approach to Health Reform, cont.
• We’re engaged in a research project to learn more about factors
that affect capacity for collective action regarding regional-level
stewardship of healthcare or medical services.
– We interviewed stakeholders in 3 communities to elicit
experiences (positive & negative) with multi-stakeholder
collaborations.
– We focus on collaborative stewardship among professionals,
but in long term, the active participation of ordinary citizens is
critical.
27
What is a Commons?
1. A resource or system of resources to which members of a group share
access, and which they either (a) consume jointly or (b) use as a
common pool from which they extract units for private consumption;
2. This common resource can be exhausted or degraded by over-use (of
resources) or under-investment (in resource replenishment and/or
contributions to public goods);
3. Efforts to replenish or maintain the relevant resources are costly;
4. And these costs will be paid only by someone with an incentive to
consider long-term consequences of current actions when they make
decisions regarding rules, regulations, & procedures.
Examples:
– Natural resource commons (fisheries, common grazing land, forests);
– Constructed commons (irrigation systems, technical infrastructures, information
systems, health commons)
28

11/16/2011
15
Health as a Commons (In Need of Self-Regulation)
1. Residents share access to local & regional resources for medical care:
1) trained healthcare professionals,
2) hospitals, clinics & test facilities,
3) financial support (insurance, government programs).
2. Congestion can be common and service degradation can be severe
because there is a limited number of clinicians, hospital beds,
emergency rooms, insurance programs, etc.
3. These resources can be reallocated to achieve more efficient or
equitable outcomes, but any significant reform will face resistance from
entrenched interests.
4. Research of Lin Ostrom & others on Commons Theory suggests that key
stakeholders can work together to craft, monitor, and enforce rules that
ensure the continued viability of common resources.
Who can act as stewards of
common resources in health?
29
The Usual Suspects: Key Local Stakeholder Groups
1. Physicians and Other Healthcare Professionals
2. Administrators of medical facilities
3. Insurers (Private and Public)
4. Employers (primarily as purchasers of insurance)
5. Public health officials (and program managers)
6. Health Information Exchanges (HIEs)
7. Community Service Organizations (CSOs)
8. Individual Citizens (critical for overall health but limited
influence over details of the medical services industry)
Note: Other categories of relevant actors have been excluded
to simplify initial analysis.
3
0

11/16/2011
16
Local Levers of Allocation and PowerImportant resource allocation decisions are made in local settings:
1. Choices by healthcare professionals concerning career paths or specializations;
2. Corporate decisions to build new facilities or to consolidate;
3. Negotiations between hospitals, physician groups, and insurance plans
regarding reimbursement levels and partnerships;
4. Procedures established within hospitals or physician groups (regarding quality
control, reducing medical errors, hospitalists, etc.);
5. Consultations among medical professionals (care coordination among
physicians-nurses-pharmacists-therapists);
6. Interactions between individual patients and clinicians (esp. regarding referrals
to specialists or testing facilities);
7. Interactions between patients and employers or government agencies offering
health insurance coverage or wellness plans;
8. Personal choices between healthy and unhealthy behaviors;
9. How personal choices are shaped by the natural and
built environment.
31
How often are these local resource allocation decisions guided by considerations of long-term effects or systemic stewardship?
Allocation of human capital
• Availability of primary care
• Physician training & recruitment
• Referral patterns (for specialty care)
• Hospital-physician relations
• Care transitions
Healthcare facilities & physical capital
• Coordination of emergency care
• Quality improvement and cost-cutting procedures (e.g., reducing medical errors)
• Facility construction
• Consolidation of hospital systems
• Market concentration; anti-trust
Financial issues
• Cost of chronic and end-of-life care
• Cost of care for uninsured patients
• Safety net for catastrophic bills
• Reimbursement and rates for care
Public/population health
• Emergency preparedness
• Preventive care
• Pre-natal care
• Dental care
• Mental health care
• Health promotion (tobacco, obesity, etc.)
• Improving the built environment
Information systems
• Quality monitoring
• Format for electronic records
• Privacy of personal health records
• Health information exchange networks
Other issues
• Employment & economic conditions
• Equity; urban/rural disparities
• Legal culture (malpractice, regulation)
32
11/16/2011
17
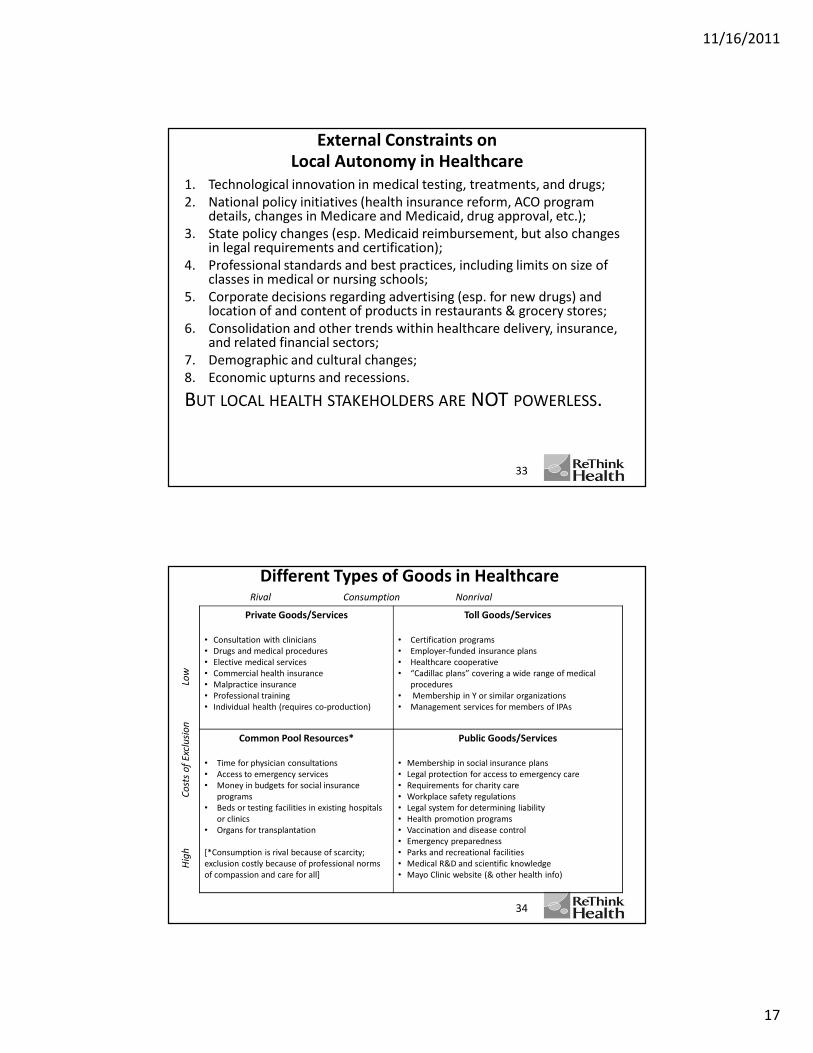
External Constraints on
Local Autonomy in Healthcare
1. Technological innovation in medical testing, treatments, and drugs;
2. National policy initiatives (health insurance reform, ACO program details, changes in Medicare and Medicaid, drug approval, etc.);
3. State policy changes (esp. Medicaid reimbursement, but also changes in legal requirements and certification);
4. Professional standards and best practices, including limits on size of classes in medical or nursing schools;
5. Corporate decisions regarding advertising (esp. for new drugs) and location of and content of products in restaurants & grocery stores;
6. Consolidation and other trends within healthcare delivery, insurance, and related financial sectors;
7. Demographic and cultural changes;
8. Economic upturns and recessions.
BUT LOCAL HEALTH STAKEHOLDERS ARE NOT POWERLESS.
33
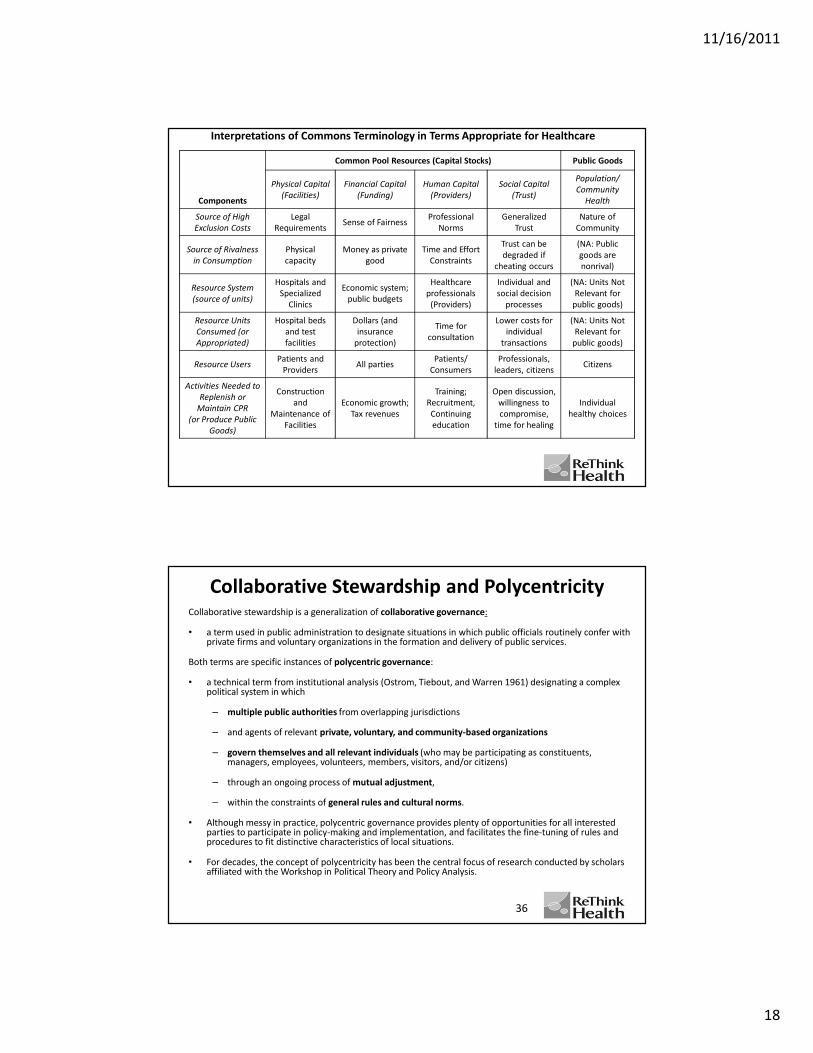
Different Types of Goods in Healthcare
Private Goods/Services
• Consultation with clinicians
• Drugs and medical procedures
• Elective medical services
• Commercial health insurance
• Malpractice insurance
• Professional training
• Individual health (requires co-production)
Toll Goods/Services
• Certification programs
• Employer-funded insurance plans
• Healthcare cooperative
• “Cadillac plans” covering a wide range of medical
procedures
• Membership in Y or similar organizations
• Management services for members of IPAs
Common Pool Resources*
• Time for physician consultations
• Access to emergency services
• Money in budgets for social insurance
programs
• Beds or testing facilities in existing hospitals
or clinics
• Organs for transplantation
[*Consumption is rival because of scarcity;
exclusion costly because of professional norms
of compassion and care for all]
Public Goods/Services
• Membership in social insurance plans
• Legal protection for access to emergency care
• Requirements for charity care
• Workplace safety regulations
• Legal system for determining liability
• Health promotion programs
• Vaccination and disease control
• Emergency preparedness
• Parks and recreational facilities
• Medical R&D and scientific knowledge
• Mayo Clinic website (& other health info)
Rival Consumption Nonrival
Hig
h
C
ost
s o
f E
xclu
sio
n
L
ow
34
11/16/2011
18
Interpretations of Commons Terminology in Terms Appropriate for Healthcare
Components
Common Pool Resources (Capital Stocks) Public Goods
Physical Capital
(Facilities)
Financial Capital
(Funding)
Human Capital
(Providers)
Social Capital
(Trust)
Population/
Community
Health
Source of High
Exclusion Costs
Legal
RequirementsSense of Fairness
Professional
Norms
Generalized
Trust
Nature of
Community
Source of Rivalness
in Consumption
Physical
capacity
Money as private
good
Time and Effort
Constraints
Trust can be
degraded if
cheating occurs
(NA: Public
goods are
nonrival)
Resource System
(source of units)
Hospitals and
Specialized
Clinics
Economic system;
public budgets
Healthcare
professionals
(Providers)
Individual and
social decision
processes
(NA: Units Not
Relevant for
public goods)
Resource Units
Consumed (or
Appropriated)
Hospital beds
and test
facilities
Dollars (and
insurance
protection)
Time for
consultation
Lower costs for
individual
transactions
(NA: Units Not
Relevant for
public goods)
Resource UsersPatients and
ProvidersAll parties
Patients/
Consumers
Professionals,
leaders, citizensCitizens
Activities Needed to
Replenish or
Maintain CPR
(or Produce Public
Goods)
Construction
and
Maintenance of
Facilities
Economic growth;
Tax revenues
Training;
Recruitment,
Continuing
education
Open discussion,
willingness to
compromise,
time for healing
Individual
healthy choices
Collaborative Stewardship and PolycentricityCollaborative stewardship is a generalization of collaborative governance:
• a term used in public administration to designate situations in which public officials routinely confer with private firms and voluntary organizations in the formation and delivery of public services.
Both terms are specific instances of polycentric governance:
• a technical term from institutional analysis (Ostrom, Tiebout, and Warren 1961) designating a complex political system in which
– multiple public authorities from overlapping jurisdictions
– and agents of relevant private, voluntary, and community-based organizations
– govern themselves and all relevant individuals (who may be participating as constituents, managers, employees, volunteers, members, visitors, and/or citizens)
– through an ongoing process of mutual adjustment,
– within the constraints of general rules and cultural norms.
• Although messy in practice, polycentric governance provides plenty of opportunities for all interested parties to participate in policy-making and implementation, and facilitates the fine-tuning of rules and procedures to fit distinctive characteristics of local situations.
• For decades, the concept of polycentricity has been the central focus of research conducted by scholars affiliated with the Workshop in Political Theory and Policy Analysis.
36

11/16/2011
19
Key References on Commons Theory, IAD, & Polycentric Governance
Aligica, Paul Dragos, and Peter Boettke. 2009. Challenging Institutional Analysis and Development: The
Bloomington School. Routledge.
Cox, Michael, Gwen Arnold, and Sergio Villamayor Tomás. 2010. “A Review of Design Principles for
Community-Based Natural Resource Management.” Ecology and Society 15(4):38
http://www.ecologyandsociety.org/vol15/iss4/art38/ES-2010-3704.pdf;
McGinnis, Michael D. 2011. “An Introduction to IAD and the Language of the Ostrom Workshop: A
Simple Guide to a Complex Framework,” Policy Studies Journal 39(1) (February 2011): 163-177.
[longer version: http://php.indiana.edu/~mcginnis/iad_guide.pdf].
Ostrom, Elinor. 1990. Governing the Commons: The Evolution of Institutions for Collective Action. New
York: Cambridge University Press.
_____. 2005. Understanding Institutional Diversity. Princeton, NJ: Princeton University Press.
_____. 2007. “Collective Action Theory.” In The Oxford Handbook of Comparative Politics, ed. Carles
Boix and Susan C. Stokes, 186–208. Oxford: Oxford University Press.
_____. 2010. “Beyond Markets and States: Polycentric Governance of Complex Economic Systems,”
American Economic Review, 100(3) (June 2010): 641–72.
_____. 2011. “Background on the Institutional Analysis and Development Framework.” Policy Studies
Journal 39(1) (February 2011): 7–27.
Ostrom, Vincent, Charles M. Tiebout, and Robert Warren. 1961. “The Organization of Government in
Metropolitan Areas: A Theoretical Inquiry.” American Political Science Review 55 (Dec.): 831-42.
Poteete, Amy, Marco Janssen, and Elinor Ostrom. 2010. Working Together: Collective Action, the
Commons, and Multiple Methods in Practice. Princeton, NJ: Princeton University Press.
37
Work-in-Progress
ReThink Health Dynamics
Seeding Innovation for Local Health System Change
Bobby Milstein & Gary Hirsch
Sponsors Advisors
11/16/2011
20
Healthier behaviors
Adherence to Guidelines
Insurance coverage
Post-Discharge Care
Socioeconomic disadvantage
Provider capacity
Provider income
Provider efficiency
Access to care
ER use
Environmental Hazards
Medical homes
Pay for Performance
Innovation Funding
Hospice
Coordinated Care
Mental Illness
Physical IllnessCrime
Benchmarks
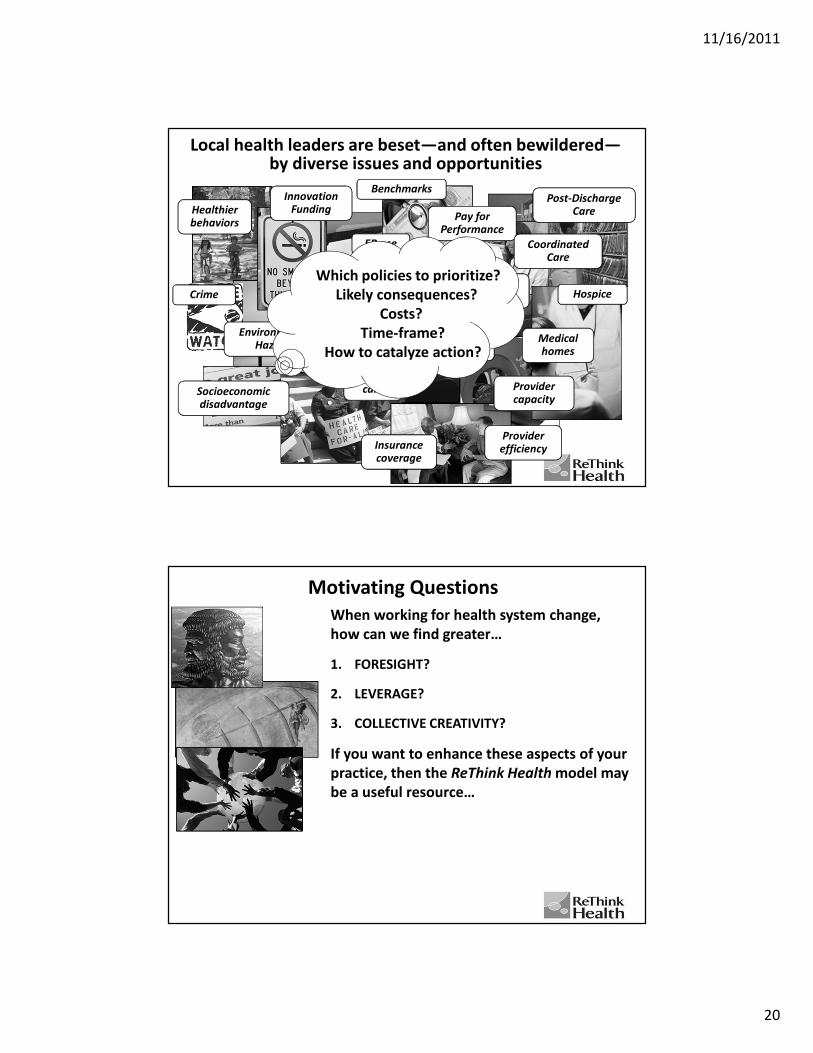
Local health leaders are beset—and often bewildered—by diverse issues and opportunities
Which policies to prioritize?
Likely consequences?
Costs?
Time-frame?
How to catalyze action?
Motivating Questions
When working for health system change,
how can we find greater…
1. FORESIGHT?
2. LEVERAGE?
3. COLLECTIVE CREATIVITY?
If you want to enhance these aspects of your
practice, then the ReThink Health model may
be a useful resource…
11/16/2011
21
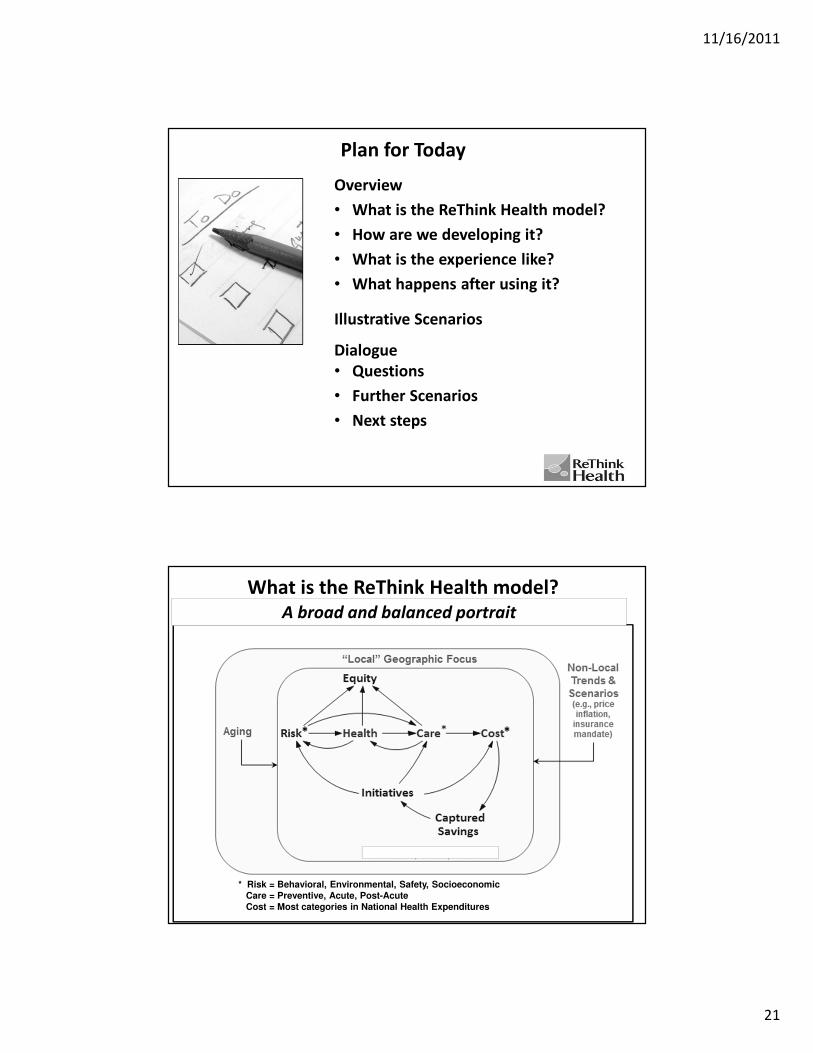
Plan for Today
Overview
• What is the ReThink Health model?
• How are we developing it?
• What is the experience like?
• What happens after using it?
Illustrative Scenarios
Dialogue
• Questions
• Further Scenarios
• Next steps
What is the ReThink Health model?
An imperfect, but realistic representation
* Risk = Behavioral, Environmental, Safety, Socioeconomic
Care = Preventive, Acute, Post-Acute
Cost = Most categories in National Health Expenditures
* *
A broad and balanced portrait

11/16/2011
22
What is the ReThink Health model?• Imperfect, but realistic representation
of local health and health care landscape
• Broad and balanced portrait, with vast policy scope
• Engaging way for planners to see and feel how things tend to change in response to different interventions
• Explicit analytic tool, anchored in dozens of databases and research literatures
– Foundation for sensitivity testing
• An extension of well-accepted prior models, now available at the local level
– A work-in-progress
How are we developing it?

11/16/2011
23
How are we developing it?• Persistent, iterative development
• Active collaboration with Triple Aim team in
Pueblo and Manchester
• Filtering details and assembling evidence on
essential processes and interventions that
affect risk, health, care, cost, equity, and
funding
– Testing in three more pilot sites
(Alameda, Contra Costa, Whatcom)
– Science advisors
– Formative evaluation and guidance
• Wider dialogues and alliances with
philanthropists, IHI, universities, ACO
designers, NNPHI, others…
What is the experience like?
First image of the
entire Earth - 1968
System dynamics operates from a “very particular distance”:
not so close to individual details, but not so far away as to be insensitive
to internal pressures and patterns.
-- Jay Forrester

11/16/2011
24
What is the experience like?
• New view of familiar terrain
• Experiments with structure and behavior
• Work together (in diverse teams) to create and play out scenarios
• Trace through and interpret system-wide performance metrics
• Compare, combine, and perhaps compete to find high-leverage strategies
– and understand how they work
• Dramatize the urgency for alignment and action, along with the stakes of inaction
Core Members
• Pueblo City County Health Department
• Pueblo City County Board of Health
• Pueblo Community Health Center
• Parkview Medical Center
• St. Mary Corwin Hospital
• Spanish Peaks Mental Health Center
• Kaiser Permanente
• Public Health Partners
Pueblo Triple Aim Team
ReThink Health opened our eyes. It offered perspective on big impact changes that might not pay off right away.
Executive Director, Pueblo City-County
Health Department
No one is interested in new programs. ReThink Health is helping us to align existing priorities and programs with more efficiency and effectiveness.
CEO, Pueblo Community Health Center

11/16/2011
25
Trends & Questions
2000 2010 2020 2030 2040
Deaths
Healthcare Costs
Care Quality
Seniors
Inequity
How far can you move
the system?
What cost?How long?Trade-offs?
Who decides?
Illustrative Scenarios
“More Care ≠ Better Care”
Coordinate Care
“Prevent and Control Chronic Illness”
Improve Care for Physical Illness
“Address the Behavioral Drivers”
Enable healthier behaviors
“Establish ACO Governance”
Capture and Reinvest Savings
“Harness Synergy and Alter Vulnerability”
Combos, plus Pathways to Advantage
“Pay for New Initiatives”
Establish an Innovation Fund

11/16/2011
26
What happens after using it?
“The future is not to be predicted, but created.”
-- Arthur C. Clarke
What happens after using it?
• Stakeholders must still decide and act
• Now equipped with
– sharper, common vocabulary
– deeper understanding of the conditions
that affect performance over time
– justifiable basis for goals and investments
• Convene others to test scenarios for themselves
– Set aside schemes unlikely to succeed
– Build support for the most promising strategies
• Streamline information systems
– Focus research on key uncertainties
• Help strengthen alignment and action
11/16/2011
27
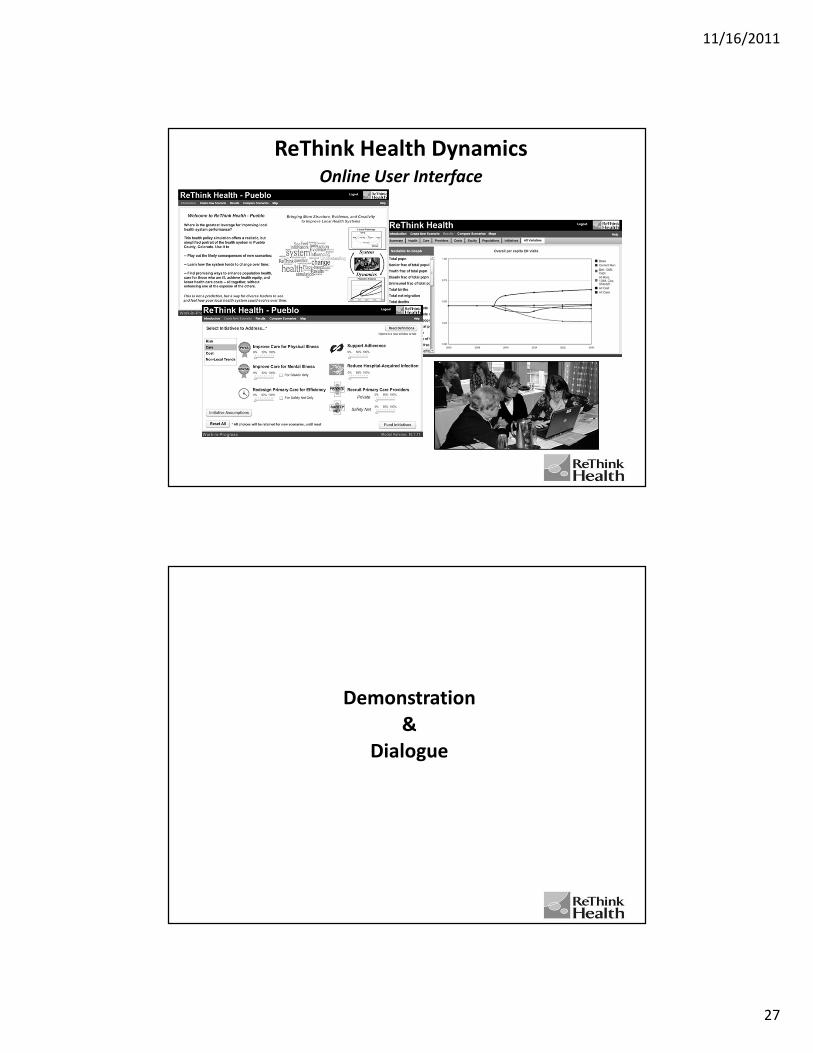
ReThink Health DynamicsOnline User Interface
Demonstration
&
Dialogue

11/16/2011
28
Science Underlying the ReThink Health Model
Integrating prior findings and local data
• On costs, prevalence, risk factors, inequity, utilization, insurance, workforce capacity, etc. (many databases and large literatures)
Using sound methodology
• Reflecting real-world accumulations, resource constraints, delays, behavioral feedback
Simplifying as appropriate
• Aggregated categories of chronic illness (physical: mild, severe; mental) and risk (behavioral, environmental)
• Ten population subgroups: by Age, Poverty, Insurance status
• 19 policy domainsUpstream, Downstream, Funding
• Trends that could affect policy conclusions Aging, PCP-per-capita decline, Price inflation, HAI non-reimbursement; possible 2014 Federal insurance mandate
56
Integrating Diverse Data SourcesLocal Sources
• Local/regional/state surveys
• Local/regional/state research reports
• Administrative data
• Ad hoc information gathering
Extracted/Adjusted from National Datasets
• Census
• Vital Statistics
• National Health Expenditure Accounts
• Consumer Price Indices (Bureau of Labor Statistics)
• National Health Interview Survey (NHIS)
• National Health and Nutrition Examination Survey (NHANES)
• Behavioral Risk Factor Surveillance System (BRFSS)
• National Ambulatory Medical Care Survey (NAMCS)
• National Hospital Ambulatory Medical Care Survey (NHAMCS)
• National Nursing Home Survey (NNHS)
• National Home Health Care Survey (NHHCS)
• Smoking-Attributable Mortality, Morbidity, and Economic Costs (SAMMEC)
• Medical Expenditure Panel Survey (MEPS)
• Dartmouth Atlas of Health Care
Publications
• Large professional literatures on health system as well as specific conditions and risk factors (see reference studies)
Prior Syntheses
• HealthBound (national health system)
• PRISM (multiple chronic diseases, risks, and interventions)
11/16/2011
29
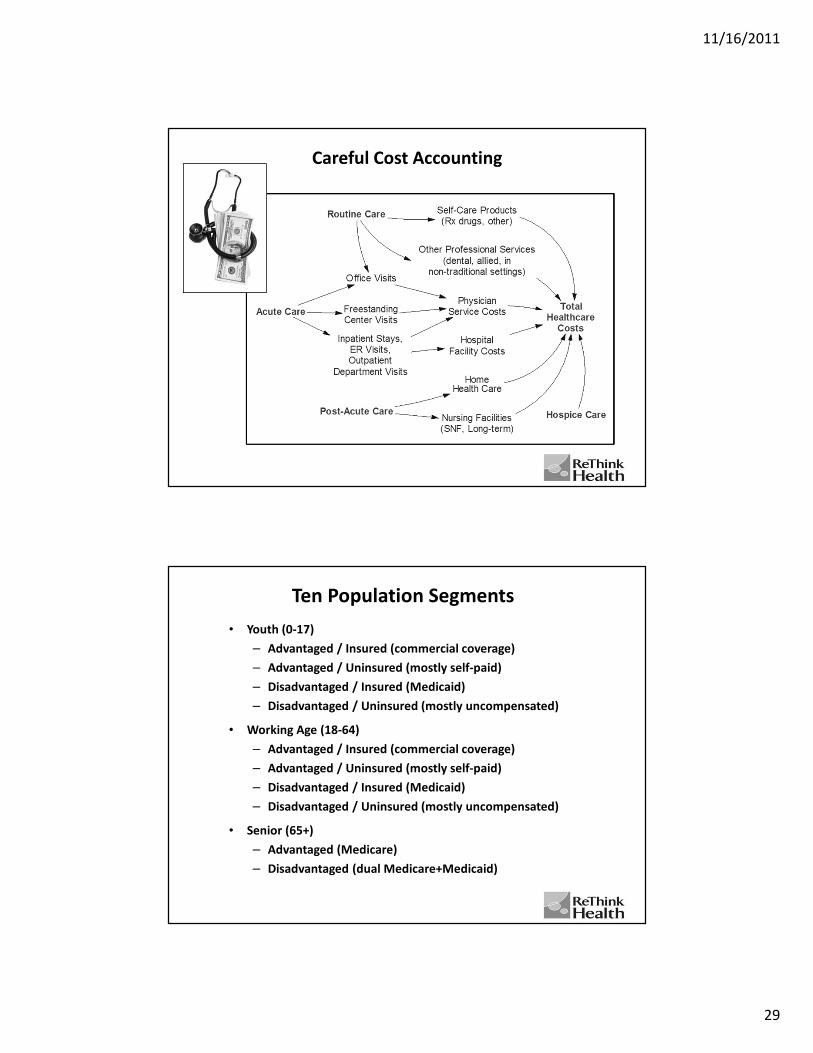
Careful Cost Accounting
Ten Population Segments
• Youth (0-17)
– Advantaged / Insured (commercial coverage)
– Advantaged / Uninsured (mostly self-paid)
– Disadvantaged / Insured (Medicaid)
– Disadvantaged / Uninsured (mostly uncompensated)
• Working Age (18-64)
– Advantaged / Insured (commercial coverage)
– Advantaged / Uninsured (mostly self-paid)
– Disadvantaged / Insured (Medicaid)
– Disadvantaged / Uninsured (mostly uncompensated)
• Senior (65+)
– Advantaged (Medicare)
– Disadvantaged (dual Medicare+Medicaid)
11/16/2011
30
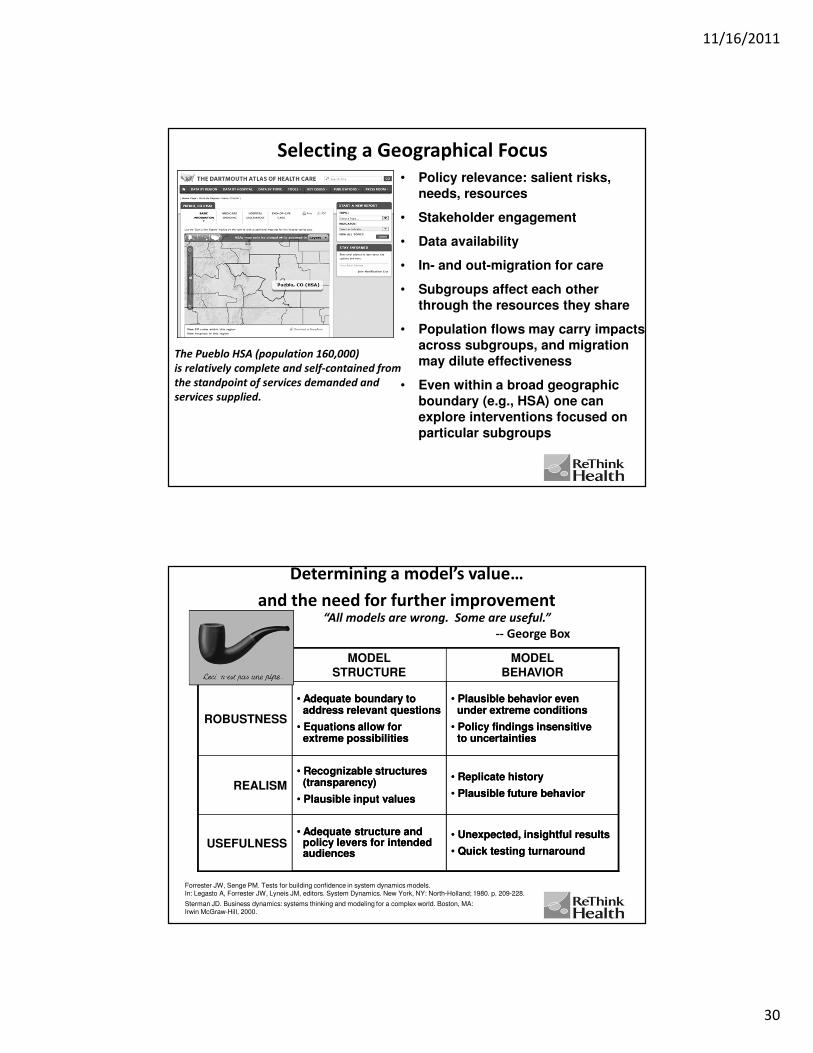
Selecting a Geographical Focus
• Policy relevance: salient risks,
needs, resources
• Stakeholder engagement
• Data availability
• In- and out-migration for care
• Subgroups affect each other
through the resources they share
• Population flows may carry impacts
across subgroups, and migration
may dilute effectiveness
• Even within a broad geographic
boundary (e.g., HSA) one can
explore interventions focused on
particular subgroups
The Pueblo HSA (population 160,000)
is relatively complete and self-contained from
the standpoint of services demanded and
services supplied.
Determining a model’s value…
and the need for further improvement
MODEL STRUCTURE
MODEL BEHAVIOR
ROBUSTNESS
• Adequate boundary to address relevant questions
• Equations allow for extreme possibilities
• Plausible behavior even under extreme conditions
• Policy findings insensitive to uncertainties
REALISM
• Recognizable structures (transparency)
• Plausible input values
• Replicate history
• Plausible future behavior
USEFULNESS• Adequate structure and
policy levers for intended audiences
• Unexpected, insightful results
• Quick testing turnaround
Forrester JW, Senge PM. Tests for building confidence in system dynamics models. In: Legasto A, Forrester JW, Lyneis JM, editors. System Dynamics. New York, NY: North-Holland; 1980. p. 209-228.
Sterman JD. Business dynamics: systems thinking and modeling for a complex world. Boston, MA: Irwin McGraw-Hill, 2000.
“All models are wrong. Some are useful.”
-- George Box
MODEL STRUCTURE
MODEL BEHAVIOR
ROBUSTNESS
• Adequate boundary to address relevant questions
• Equations allow for extreme possibilities
• Plausible behavior even under extreme conditions
• Policy findings insensitive to uncertainties
REALISM
• Recognizable structures (transparency)
• Plausible input values
• Replicate history
• Plausible future behavior
USEFULNESS• Adequate structure and
policy levers for intended audiences
• Unexpected, insightful results
• Quick testing turnaround
11/16/2011
31
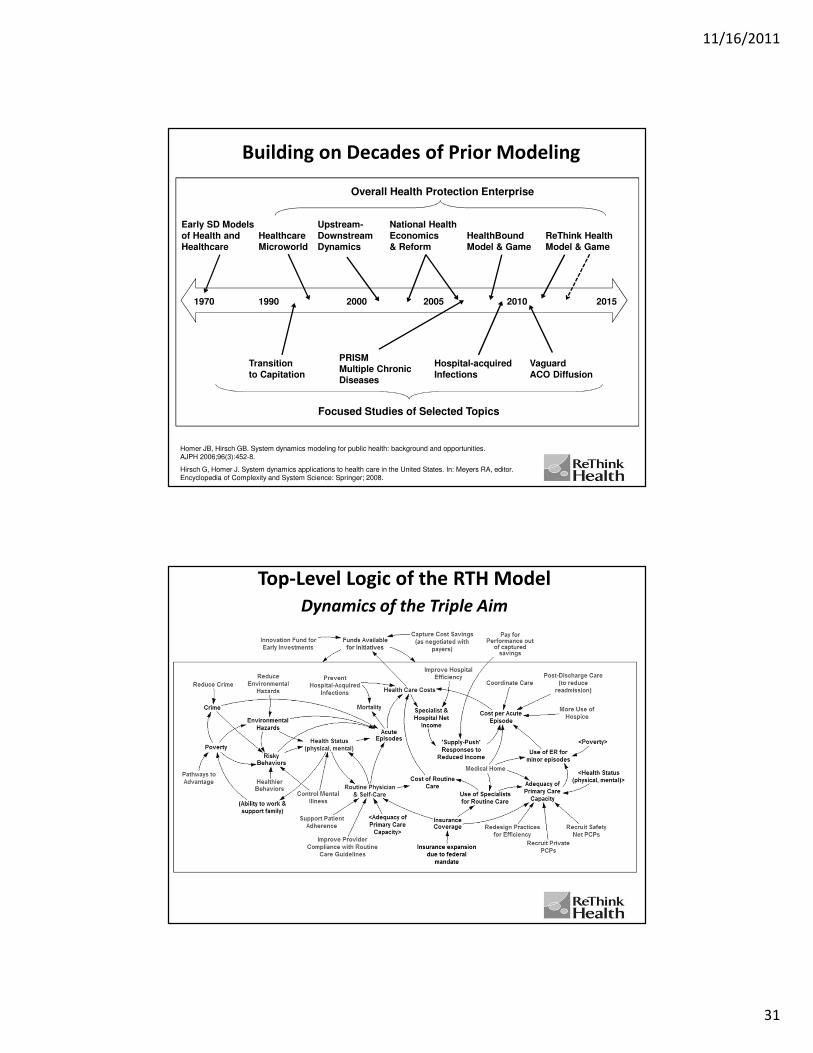
1970 1990 2000 2005 2010
Building on Decades of Prior Modeling
Early SD Models
of Health and
Healthcare
Upstream-
Downstream
Dynamics
Healthcare
Microworld
National Health
Economics
& Reform
HealthBound
Model & Game
Overall Health Protection Enterprise
2015
Homer JB, Hirsch GB. System dynamics modeling for public health: background and opportunities. AJPH 2006;96(3):452-8.
Hirsch G, Homer J. System dynamics applications to health care in the United States. In: Meyers RA, editor. Encyclopedia of Complexity and System Science: Springer; 2008.
ReThink Health
Model & Game
Focused Studies of Selected Topics
PRISM
Multiple Chronic
Diseases
Hospital-acquired
Infections
Transition
to Capitation
Vaguard
ACO Diffusion
Top-Level Logic of the RTH Model
Dynamics of the Triple Aim

11/16/2011
32
Intervention Options for Scenario Testing
* These interventions have the potential to dampen the “supply-push” backlash of
specialists and hospitals responding to cost reduction efforts that reduce their income.
What Is Organizing?People, Power and Change
The core principles of interdependent leadership
ORGANIZING FOR HEALTH
Kate Hilton

11/16/2011
33
‘Organizing is identifying, recruiting and
developing leaders; building community
around that leadership; and building power
out of that community.’
Organizing Theory of Change
Change = People + Power
What is organizing?
Theory of Change

11/16/2011
34
What Organizing is NOT• Information / training programs
– If only we acquire knowledge, we will change our behavior
– Example: If we train nurses in lean methodologies, they will implement those changes in their wards
• Awareness raising
– If only they were informed, they would change their behavior
– Example: If we remind people to wash their hands, they will
• Technological innovation (fix v. solution)
– If only we implement this innovation, it will “fix” the problem
– Example: If we build a more innovative facility, the community will use it
• Marketing
– If we “sell” our idea, people will take it up
– Example: If market this service to patients, they will want it
• Service (for others v. with others)
– If “we” act for others , they will benefit
– Example: If we offer a free diabetes screening or build a walking path, people will come
‘Organizing is identifying, recruiting and
developing leaders; building community
around that leadership; and building power
out of that community.’
Organizing Theory of Change
Change = People + Power
What is organizing?

11/16/2011
35
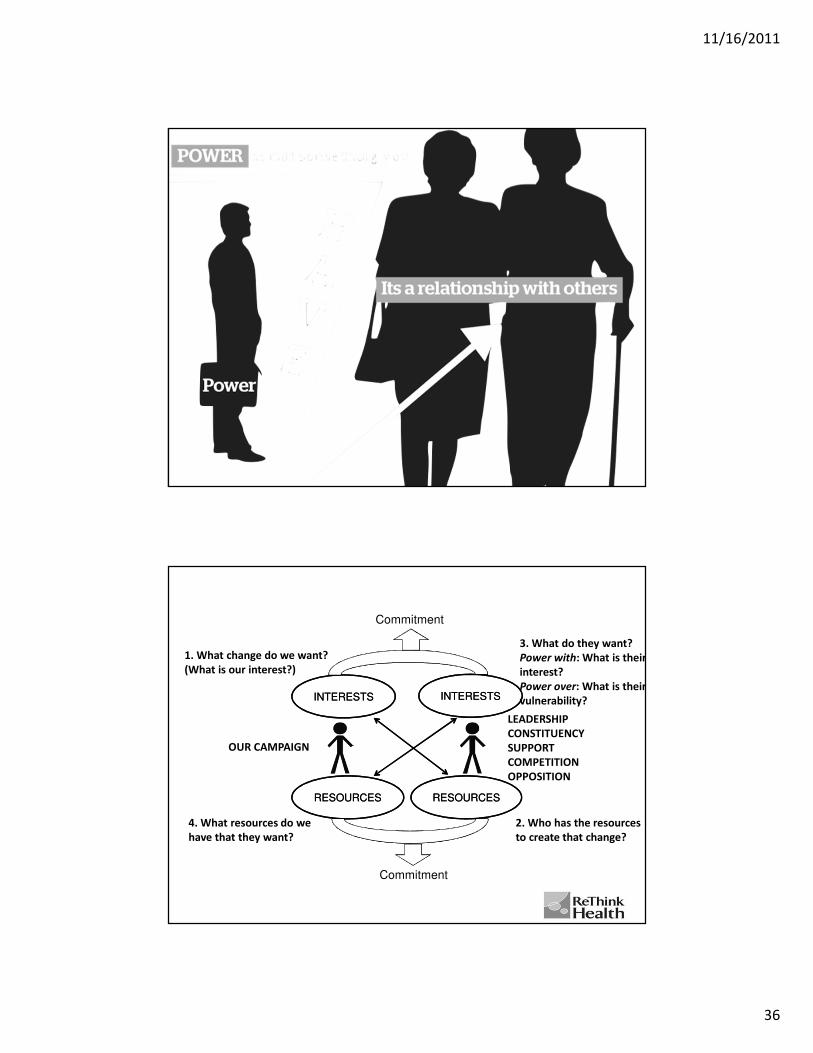
Map of Actors
POWER WITH POWER OVER
Power Analysis
11/16/2011
36
INTERESTSINTERESTS INTERESTSINTERESTS
RESOURCESRESOURCES RESOURCESRESOURCES
Commitment
Commitment
1. What change do we want?
(What is our interest?)
2. Who has the resources
to create that change?
3. What do they want?
Power with: What is their
interest?
Power over: What is their
vulnerability?
4. What resources do we
have that they want?
OUR CAMPAIGN
LEADERSHIP
CONSTITUENCY
SUPPORT
COMPETITION
OPPOSITION
11/16/2011
37
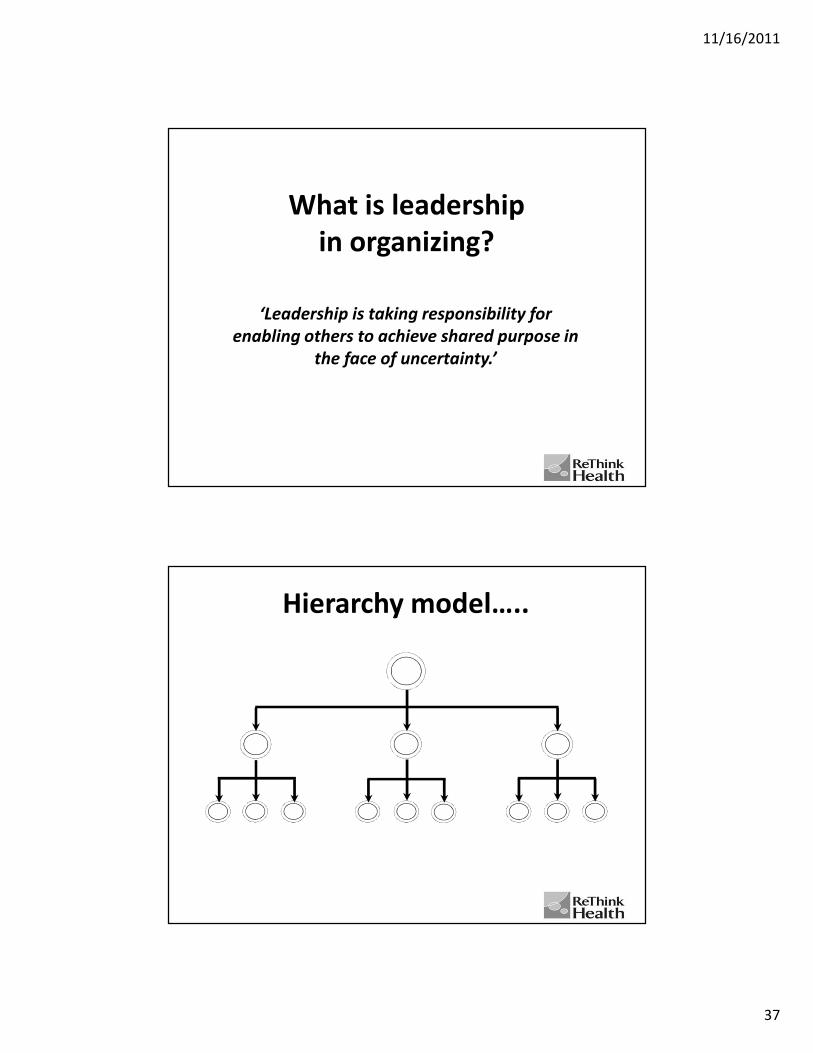
‘Leadership is taking responsibility for
enabling others to achieve shared purpose in
the face of uncertainty.’
What is leadership
in organizing?
Hierarchy model…..

11/16/2011
38
The ‘Lone Ranger’ leader…..
‘We’re all leaders’ model…..

11/16/2011
39
Interdependent leadership…..
‘Leadership is taking responsibility for
enabling others to achieve shared purpose
in the face of uncertainty.’
What is leadership
in organizing?

11/16/2011
40
‘Is equipping people (constituency)
with the power (resources) to make
change (real outcomes)’
Organizing…..
The Five Key Practices

11/16/2011
41
1. Creating a shared story
Relationship as Interest
Common Interests
New Interests
New Resources
Common Resources
Relationship as Resource
Interests
2. Creating shared relational commitment
Interests
Resources Resources

11/16/2011
42
3. Creating a shared structure
Turning the resources you have people
4. Creating a shared strategy
Into the resources you need power
To get the change you want change

11/16/2011
43
5. Creating shared action
Mobilise resources Deploy resources
Commitment
The five key practices create
DISORGANIZATION LEADERSHIP ORGANIZATION
Passive Shared Story Motivated
Divided Relational Commitments United
Drift Team Structure Purposeful
Reactive Creative Strategy Initiative
Inaction Effective Action Change
Interdependent Leadership
& Strong Organizational Capacity

11/16/2011
44
Map of Actors
INTERESTSINTERESTS INTERESTSINTERESTS
RESOURCESRESOURCES RESOURCESRESOURCES
Commitment
Commitment
1. What change do we want?
(What is our interest?)
2. Who has the resources
to create that change?
3. What do they want?
Power with: What is their
interest?
Power over: What is their
vulnerability?
4. What resources do we
have that they want?
OUR CAMPAIGN
LEADERSHIP
CONSTITUENCY
SUPPORT
COMPETITION
OPPOSITION
11/16/2011
45
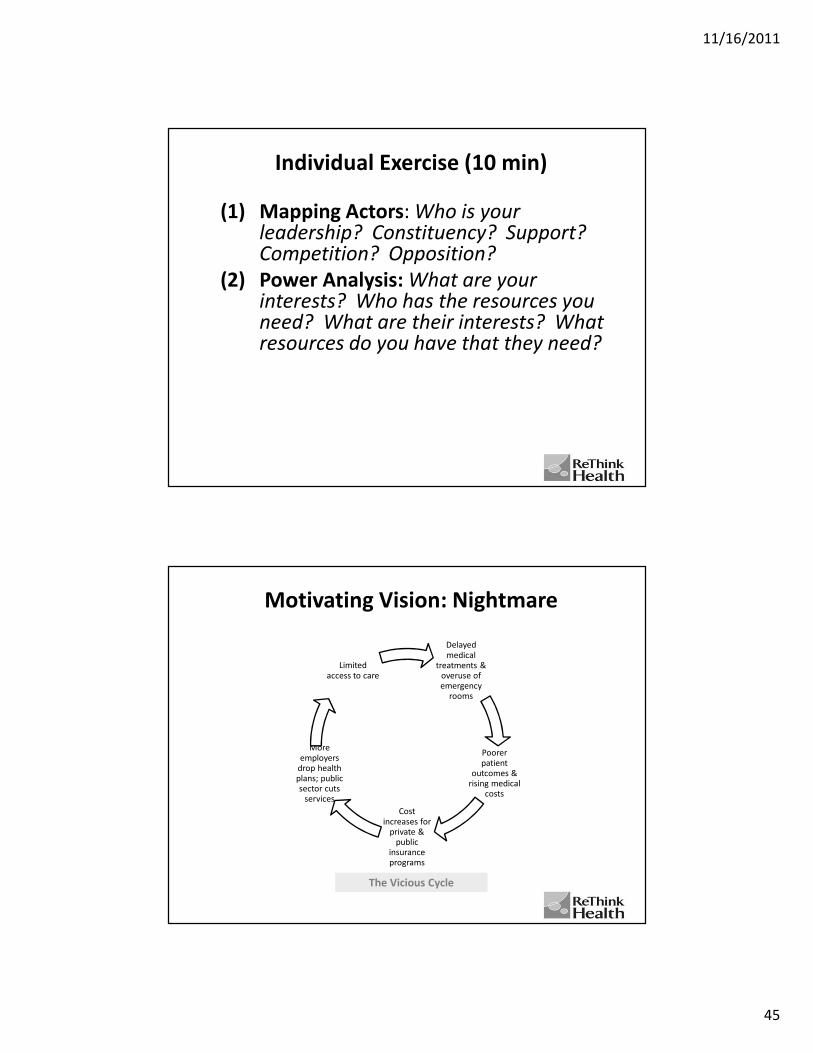
Individual Exercise (10 min)
(1) Mapping Actors: Who is your leadership? Constituency? Support? Competition? Opposition?
(2) Power Analysis: What are your interests? Who has the resources you need? What are their interests? What resources do you have that they need?
Motivating Vision: Nightmare
Delayed medical
treatments & overuse of emergency
rooms
Poorer patient
outcomes & rising medical
costs
Cost increases for
private & public
insurance programs
More employers
drop health plans; public sector cuts
services
Limited access to care
The Vicious Cycle
11/16/2011
46
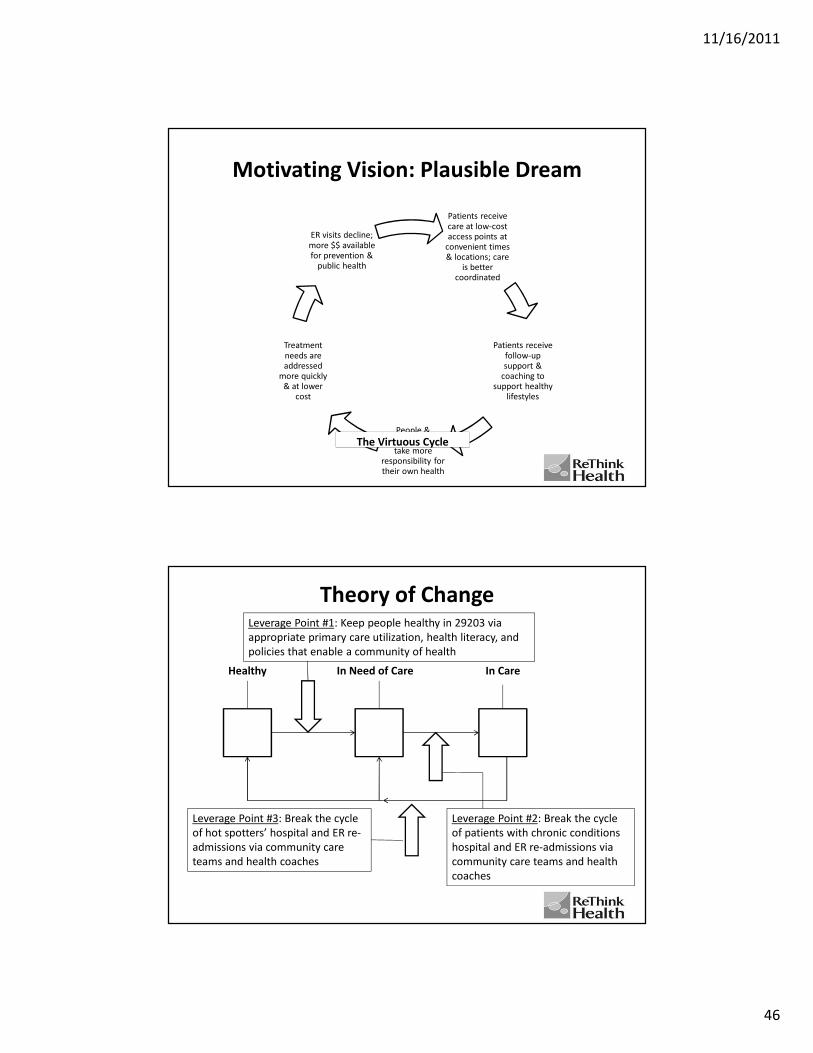
Motivating Vision: Plausible Dream
Patients receive care at low-cost access points at
convenient times & locations; care
is better coordinated
Patients receive follow-up support &
coaching to support healthy
lifestyles
People & communities
take more responsibility for their own health
Treatment needs are addressed
more quickly & at lower
cost
ER visits decline; more $$ available for prevention &
public health
The Virtuous Cycle
Theory of Change
In Need of CareHealthy In Care
Leverage Point #2: Break the cycle
of patients with chronic conditions
hospital and ER re-admissions via
community care teams and health
coaches
Leverage Point #3: Break the cycle
of hot spotters’ hospital and ER re-
admissions via community care
teams and health coaches
Leverage Point #1: Keep people healthy in 29203 via
appropriate primary care utilization, health literacy, and
policies that enable a community of health

11/16/2011
47
Theory of Change
POWER WITH POWER OVER
Power Analysis

11/16/2011
48
Campaign Goals
(1) Increase organizing and leadership skills among individuals and teams
(2) Increase access to and use of appropriate low-cost care in ways that are meaningful to 29203 community members
(3) Increase the community’s commitment to health and involvement in wellness policies and activities
(4) Make primary care more available in 29203
(5) Improve health outcomes
(6) Reduce costs
Constituencies
(1) Community members in 29203 and
Columbia
(2) Health care providers
(3) Volunteer health coaches
(4) Private and public insurers
(5) Students
11/16/2011
49
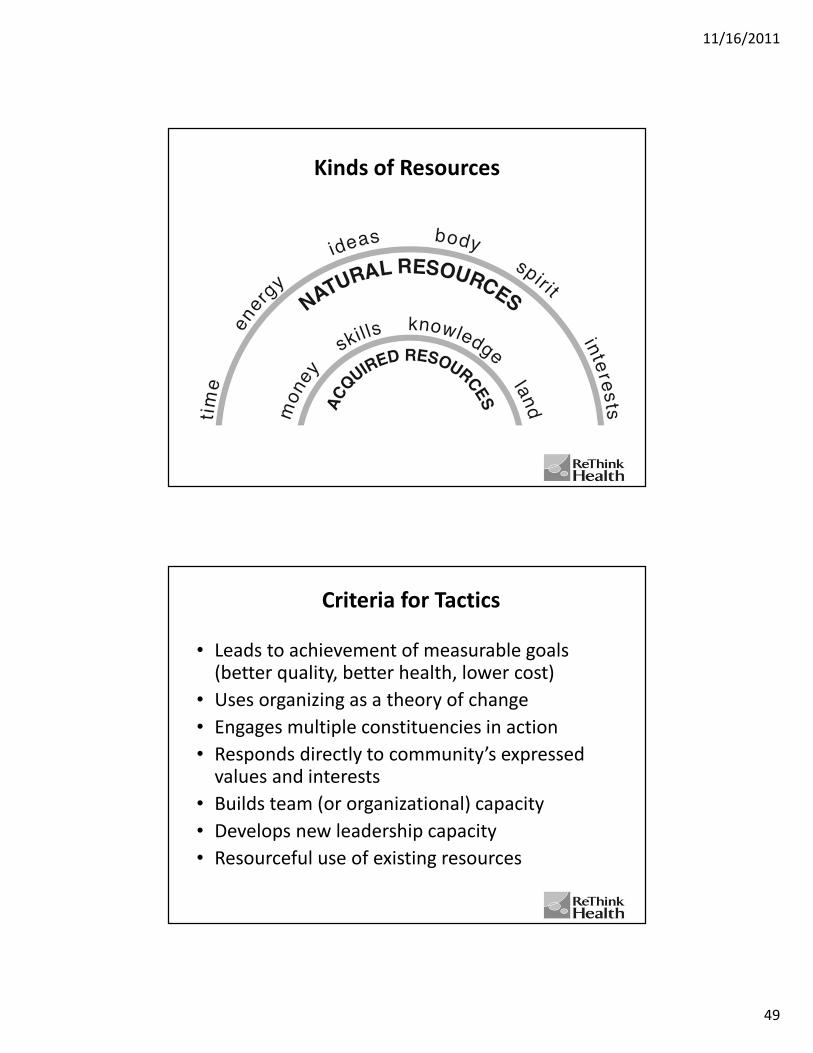
Kinds of Resources
Criteria for Tactics
• Leads to achievement of measurable goals (better quality, better health, lower cost)
• Uses organizing as a theory of change
• Engages multiple constituencies in action
• Responds directly to community’s expressed values and interests
• Builds team (or organizational) capacity
• Develops new leadership capacity
• Resourceful use of existing resources

11/16/2011
50
How will we grow our campaign?
Time
Healthy South Carolina
Campaign Chart 2011-2012
20 participants
Core Leadership
Team Training
July 13-14
Mission 2011
Aug. 3-4
60 participants
Leadership
Team Training
+
Launch of
House Meeting
Campaign
Sept 27-28
91 leaders
attend
Town Hall
Meeting
Aug. 16
Community Issues
Assembly
with decision-making
on campaign focus
November 16, 17 or 19
1,000 people
Official Campaign
Launch!
February 2012 Team Training
with 200 leaders
January 2012
11/16/2011
51
Building Collaborative Leadership Teams for Community Efforts
Ruth Wageman
Two real examples• A group of leaders convene to meet the HC needs of the disenfranchised
in 4 counties (<200K)
– 2 senior leaders from major employers, senior leaders from 2
hospitals, 2 primary care practices, major payer
– Mobilized volunteer HC workers, resulted in a new FQHC
– Different configurations of leaders have undertaken additional
collaborations, e.g., single sleep lab jointly owned by both hospitals;
community health needs assessment with 100 institutional partners,
Vision for Community Health 2020
• 8 leaders convened in a small city (<200K) to address how to provide care
to the underinsured
– 3 hospital CEOS, 1 senior leader from a mental health provider, from
children’s health center, 2 from public health, 1 from major private
insurer in the region
– Met monthly over 2 years, no change in access to care for the
uninsured, still meet but individuals largely attend so that no decisions
get made behind their backs
11/16/2011
52
Why the difference?
• Dream team… Scream team…
Research on leadership teams across sectors
• Three key challenges when teams of leaders
convene
• Conditions which can be put in place to address
those challenges
• Hypotheses about how to do that in the context of
community-level self-governing multi-stakeholder
teams whose purpose is to lead change

11/16/2011
53
Challenge 1: What is the purpose of the leadership team?
Why purposes can be very unclear:
• Who authorized them to do anything?
• Assume all “signed on” or view selves as a leadership group
• Teams are not good at defining clear purposes
– They sand down the sharp edges of a vision
– They assume consensus is needed on everything
3
3.5
4
4.5
5
Compelling purpose? The teams we studied….
Consequential Challenging Clear
11/16/2011
54
Condition 1: A Compelling Purpose
• Challenging: Has to engage the best of what people bring
• Consequential: Rooted in values, real impact on the lives of others
• Clear: We know what the community would look like if we were to achieve it
• How? Hypothesis:
– Facilitated and iterative process
– Individuals articulate, group selects
– Individual is authorized, group ratifies
Challenge 2: Wrong people are convening
• Assume high level leader
• Assume institutions must be ‘represented’
• No assessment of the individuals’ collaborative
abilities
11/16/2011
55
Condition 2: The Right People
• “Enterprise perspective,” in this case the community, not just the institution
• Systems understanding (conceptual skill)
• Empathy and integrity
– Recognize the concerns of others
– Act as one on group agreements
• Time to devote
• How? Hypothesis:
– Convene initial set. Ask that group to appoint the “right people” for continuing collaboration
Challenge 3: The meetings are a waste of time
• Not real leadership work
– Discussions rather than interdependent tasks
• Institutional cultures and norms vary
– Deciding independently not to appear
– Sending delegates
• Assume “we’re all grownups”

11/16/2011
56
3
3.5
4
4.5
Outstanding Leadership Teams
Have Enabling Structures
Poor Teams MediocreTeams
OutstandingTeams
Meaningful Tasks
Clear Norms
Condition 3: Enabling Structure
• Work on the agenda is strategic
– Problem solve and decide
– Members consult to one another about
challenges
• Norms of conduct are explicit
• How? Hypothesis:
– Authorize individual to prepare agenda
– Consider a facilitated process for norm
development and accountability structure

11/16/2011
57
Application
• Assess a key change leadership team in your own context:
– Overall “Grade” on each of the three conditions
– Choose one that is especially in need of work and consider potential interventions
• Choose a partner to exchange ideas about improving collaborative leadership
• Bring back a question, observation, or key lesson for larger group
Innovation
• Iterative
• Totally transformative
• Many have gone out of business
• Others have grown

11/16/2011
58
Conditions for Innovation
• Champion with will and passion
• Team
• Vision
• New mental models, system thinking
• Relationships
• Time and hard work
• Resourcefulness
• High tolerance for risk and uncertainty
• Community of learning and support
• Early adapters and supporters
Drivers of Innovation
• New technology
• New discoveries
• New questions
• New problem definitions
• Consumers
• Visionaries and leaders
• Advocates
• Competition(s)
• Urgency, crisis
• Capacity
• Regulations and policy
• Intrinsic and extrinsic rewards
• Open sourcing and new data
• Mandate efficiency
• Funders
• Supply chain
• Regulators (FDA)
• Health impact assessments
• Scenarios and visioning
• Total spending
• Coordinated investment
• Public health legislation
• Basic science
• Supply chain
11/16/2011
59
Thank you!
• Please join us in ReThinking Health!
http://www.rethinkhealth.org
• Join our online community:
http://leading4health.ning.com
Top Related