







Languages
Pages
Legal

LUNGS AND RESPIRATORY SYSTEM

Lung Physical exam:1- Inspection2- Palpation
3- Percussion
4-Auscultation5- Egophony
INSPECTION• Deformities or asymetry• Abnormal retraction of the interpaces• Impairment in respiratory movement

Tactile Fremitus• Performed by : 1- placing ulnar side of hand or
palm against the patient posterior chest wall.• 2 – Have the patient say ninety-nine• Increased tactile fremitus =increased density
of the lungs (consolidation).• Decreased tactile fremitus =excess
subcutaneous tissue on the chest ,air or fluid
Percussion• Dull =increased density such as fluid in the
lungs , or lung cavity or consolidation• Tympanic = hollow air-containing structure• Resonant = structure of air within tissue• Hyperresonant = decreased density and more
air , such as in emphysema

Auscultation• Crackles :short discontinuous nonmusical
sounds heard mostly during inspiration• Wheezes :continuous , musical , high-pitched
heard mostly during expiration.• Rhonchi:lower-pitched lung sounds• Pleural rub :Sound produced by motion
pleura, heard best at end of inspiration /beginning of expiration

Lung auscultation
Egophony • Spoken words by the patient are increased in
intensity and take on different quality during auscultation.Patient says eeee”and will heard as “aaaa”in area of consolidation and in areas of compressed lung above a pleural effusion

PLEURAL EFFUSIONDefinition Transudate :1- increased hydrostatic pressure2- decreased oncotic pressure3- CHF, Cirrhosis, Nephrosis

Oxidative pleural effusion• Increased capillary permeability• Tumors, Trauma, Infection
Diagnosis criteria of exudate• Ratio of pleural to serum protein >0.5• Ratio of pleural to serum LDH >0.6• Pleural fluid LDH >2/3 upper normal limit
Para pneumonic effusion :• Pleural fluid leukocyte count >10,000/mm• Always exudates• WBC >100,000 =empyema• Empyema =pus in pleural space , positive
cultures, require chest tube

• Gross blood in pleural fluid:• Tumor (breast ,lung cancer, lymphoma)• Trauma• Pulmonary infarction• Aortic dissection
• Low glucose in pleural fluid is associated :• Empyema• Rheumatoid arthritis• Tumor• tuberculosis

• High amylase in pleural fluid is associated :• Pancreatitis• Renal failure• Tumor• Esophageal rupture

• PULMONARY FUNCTION TEST• Spirometry measures the rate at which the
lung changes during forced breathing• Forced vital capacity (FVC) :• Fev1 :the volume of air exhaled in the first
second of the FVC• Normal FEV1/FVC ratio=>0.7

Spirometry1
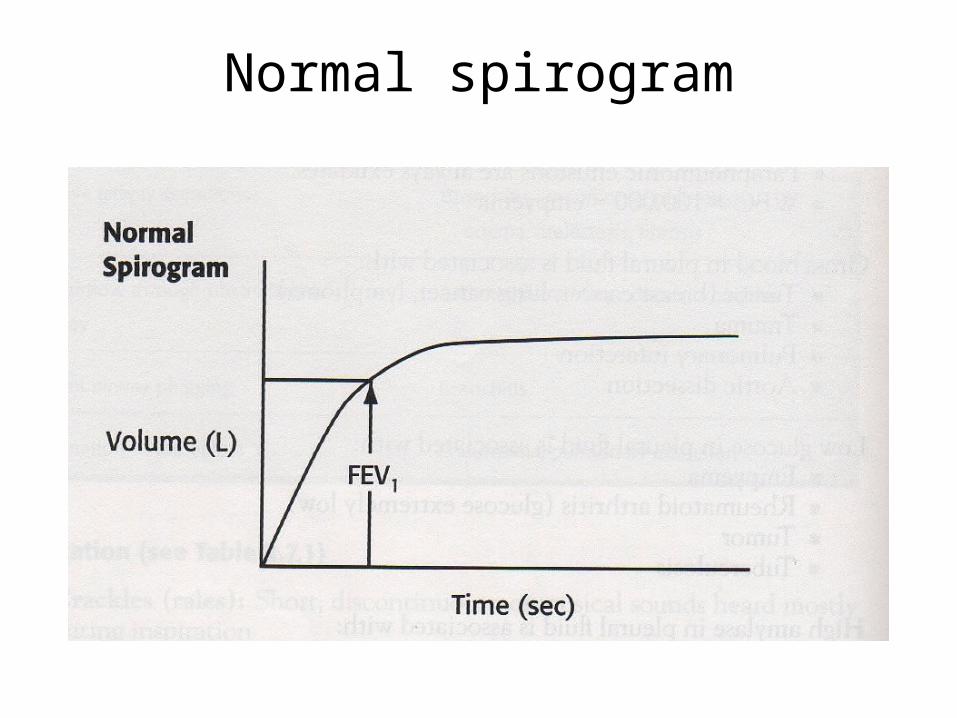
Normal spirogram

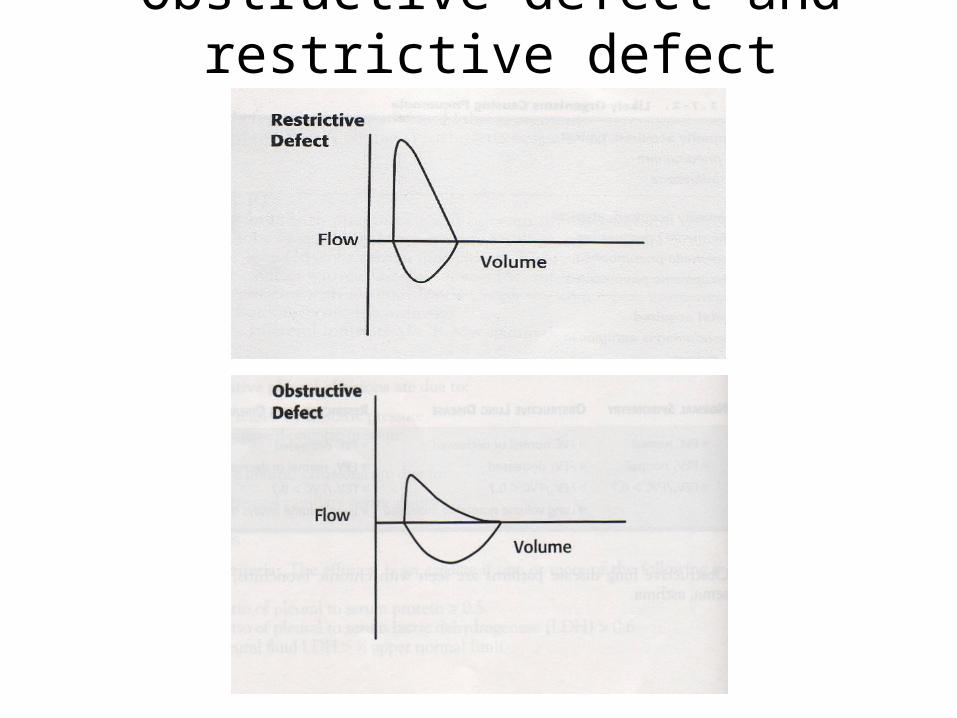
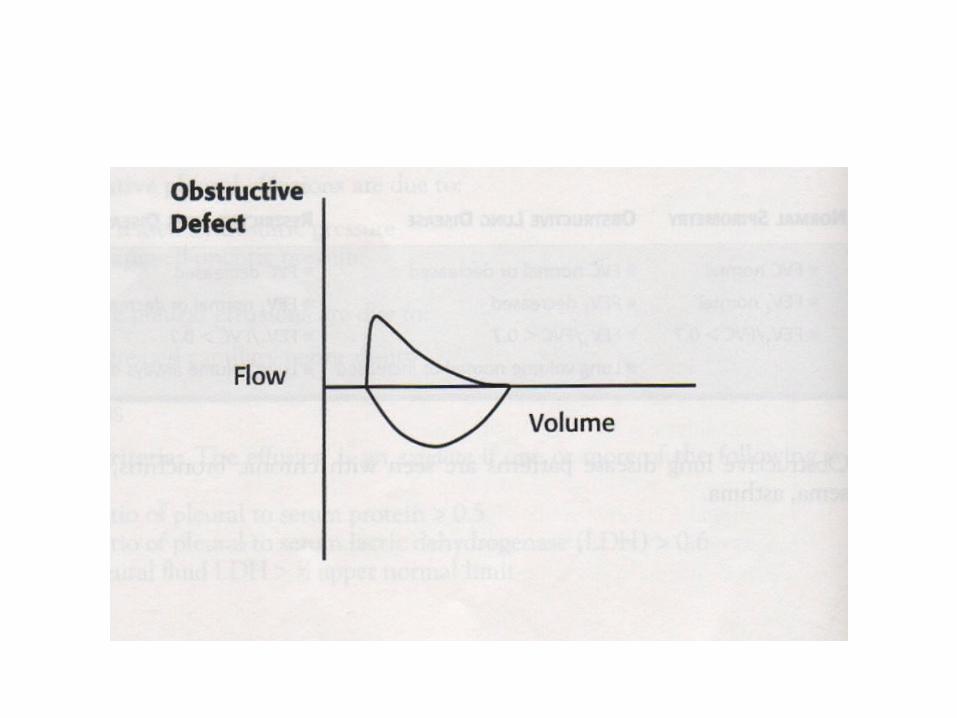
Obstructive defect and restrictive defect

Lung Infections • Pneumonia: infection of the lung parenchyma
by any microorganism.Etiology:• A- community acquired pneumonia• 1-S-Pneumonia• 2- H. influenzae

B- community acquired atypical• 1- chlamydia pneumoniae• 2- Legionella pneumophila• 3- Mycoplasma pneumonia
C- Hospital acquired• 1- pseudomonas aeruginosa• 2 S.Aureus• 3- Enteric organisms

Signs and Symptoms• A- Typical Symptoms• 1- Fever• 2- cough• 3- pleuritic chest pain
B- Atypical Symptoms• 1- Dry cough• 2-headache• 3- malaise• 4- Gastrointestinal symptoms
Physical exam• 1- Dullness to percussion• 2-Rales• 3- Tactiles fremitus• 4- Egophony (E to A changes ) with
stethoscope

Diagnosis• A – Chest Xray• 1- upper lobe infiltrate or consolidation• 2- small cavities w/o air-fluid levels( M.tb• 3- larges cavities with air-fluid levels (staph)• 4- diffuse bilateral infiltrate (PCP,
Mycoplasma)

Criteria for admission• 1- Age >50• 2-Nursing home residents• 3- underlying chronic disease• 4- change in mental status• 5- Tachypnea, tachycardia, or hypotension• 6- Pleural effusion

Scenario 1• A 19 y/o college student male c/o malaise, dry
cough for the last 10 days, denied fever and pleuritic chest pain .Physical unremarkable , CXR showed diffuse bilateral infiltrate.
• Scenario2A patient comes to the ER with consolidation
and pleural effusion on CXR. What is the most important test to determine admission/treatment.

Scenario 3• A 27 y/o White male brought to the ER c/o
productive cough, fever and pleuritic chest pain.Physical exam elicited tachypnea and crackles on R upper lobe .What other physical finding suggestive of typical pneumonia?

Obstructive Disorders
1. Chronic Obstructive pulmonary Disease: A-Chronic bronchitis :chronic expiratory airflow
obstruction accompanied by chronic productive cough for 3 or more months in each of 2 successive years

• Emphysema :chronic expiratory airflow obstruction accompanied by permanent enlargement of the airspace distal to the terminal bronchioles due destruction of alveolar septa.
• Pathophysiology of Emphysema• Centrilobular emphysema affects the
respiratory bronchioles.• Panlobular emphysema occurs in patients
with alpha-1 antitrypsin deficiency.• Distal acinar emphysema is associated with
spontaneous pneumothorax.
• Epidemiology 1- Higher prevalence in men2- Mortality rates are higher in whites3- Only 15 % of smokers develop COPD
• Risk Factors• Smoking• Alpha-1-antitrypsin deficiency
Diagnosis /Findings Chest xray: hyperinflated lungs, flattened
diaphragm. Physical exam: Barrel chest Pulmonary function tests: irreversible
obstructive pattern (low FEV1) Computed tomography: loss of alveolar walls

Symptoms Cough Dyspnea on exertion CO2 retention (chronic bronchitis) Weight loss (emphysema) tachypnea
treatment Smoking cessation Oxygen Maintain vaccination against influenza and
S.pneumoniae Beta agonist and ipratropium Steroid
Asthma A chronic condition characterized by: 1- airway inflammation 2- brochoconstriction 3- hypersecretion
PATHOPHYSIOLOGY • IgE mediated ,associated with histamine
release from mast cells(early phase)• The late phase is associated with cytokine
release
TRIGGERS• Exposure to pets, dust ,smoke ,carpets• Aggravation by exercise ,hot or cold weather• Seasonal changes

Signs and symptoms• Chest tightness• Wheezing• Shortness of breath• cough
Differential diagnosis of wheezing• Reactive airway disease• Congestive heart failure• Foreign body aspiration (most often in
children)• Asthma
Physical Exam• Wheezing on exhalation• Decreased air entry , increased expiratory
phase• Decreased peak flow and FEV1• Retractions of sternocleidomastoids

• Intercostal muscle use for breathing• Oxygen saturation <95%• Inability to speak full sentences

asthma classification and treatment

Top Related