





Languages
Pages
Legal

Lung Transplant for Interstitial Lung Disease
Isabel Neuringer, MD
Living with IPF Patient SymposiumSeptember 15, 2012
1
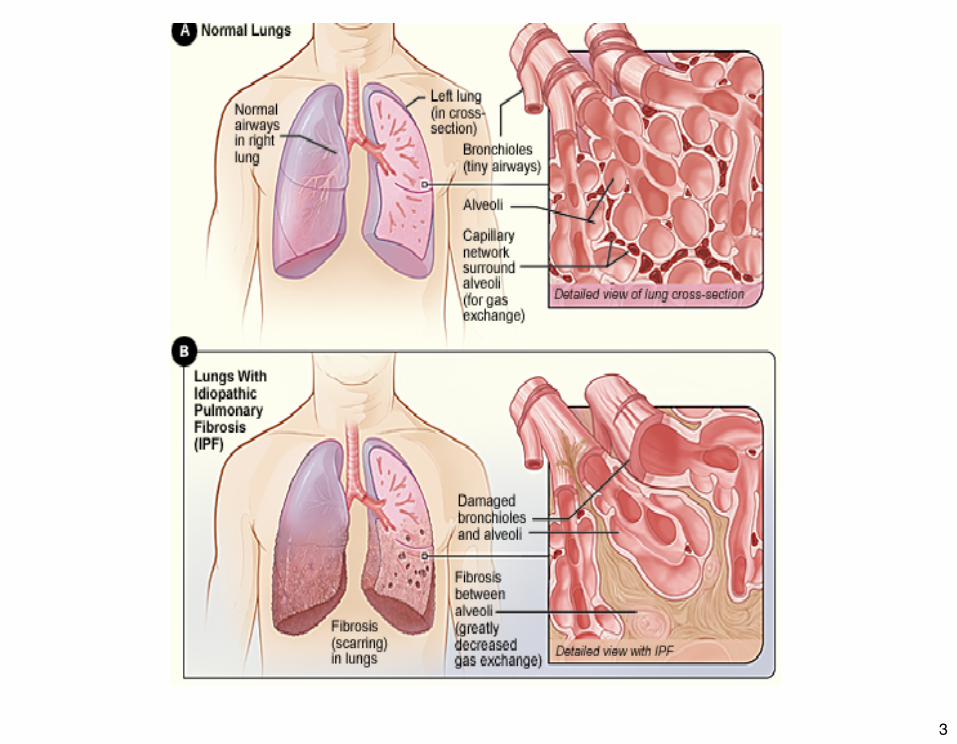
Diffuse Lung Parenchymal Diseases
• Heterogeneous disorders• Auto-immune disease, environmental/
exposure• 30-40% idiopathic• Prevalence ~ 70 per 100,000• Median survival ~ 3-5 years• If disease progresses – lung
transplantation remains an appropriate treatment
2
3
Lung Transplantation for ILD• 1983 Toronto Lung Transplant Group performed
1st single lung transplant on a patient with idiopathic pulmonary fibrosis
• Now ~ 3000 lung transplants performed per year for all end-stage lung diseases
• Lung transplant for IPF has been increasing• IPF and diffuse parenchymal diseases now >
50% of all transplants in US• ~ 7000 lung transplants performed for IPF
between 1995 - 2010
4
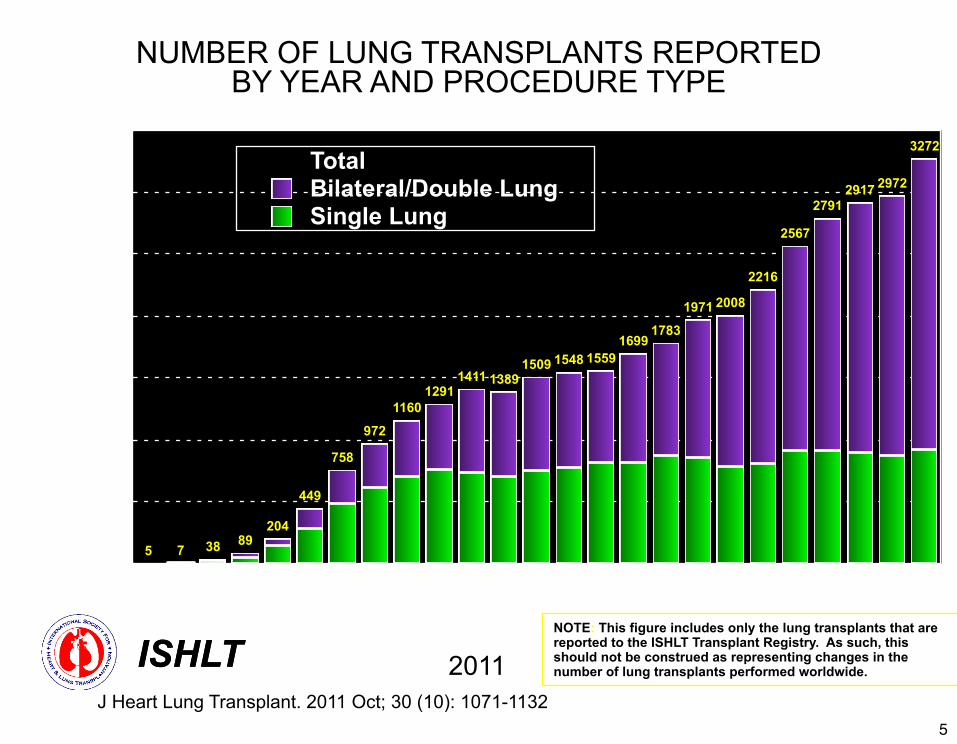
NUMBER OF LUNG TRANSPLANTS REPORTED BY YEAR AND PROCEDURE TYPE
0
500
1000
1500
2000
2500
3000
3500
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
3272
297229172791
2567
2216
20081971
17831699
15591548150913891411
12911160
972
758
449
204893875
Num
ber o
f tra
nspl
ants
Single LungBilateral/Double LungTotal
NOTE: This figure includes only the lung transplants that are reported to the ISHLT Transplant Registry. As such, this should not be construed as representing changes in the number of lung transplants performed worldwide.
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
5
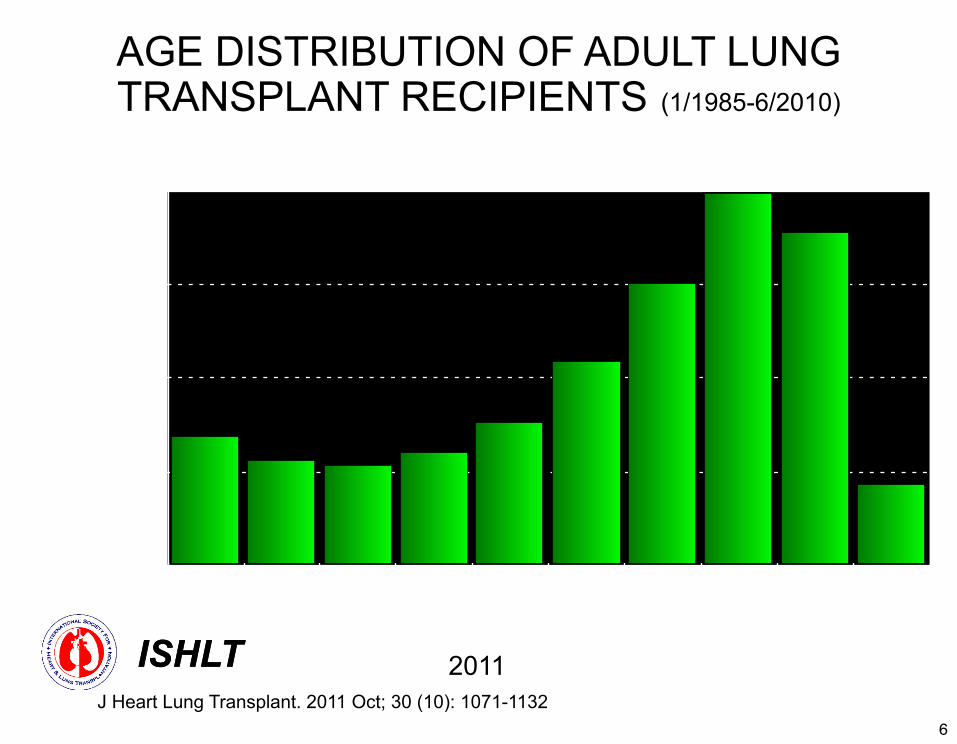
AGE DISTRIBUTION OF ADULT LUNG TRANSPLANT RECIPIENTS (1/1985-6/2010)
0
5.0000
10.0000
15.0000
20.0000
18-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-65 >65
% o
f tr
ansp
lant
s
Recipient Age
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
6
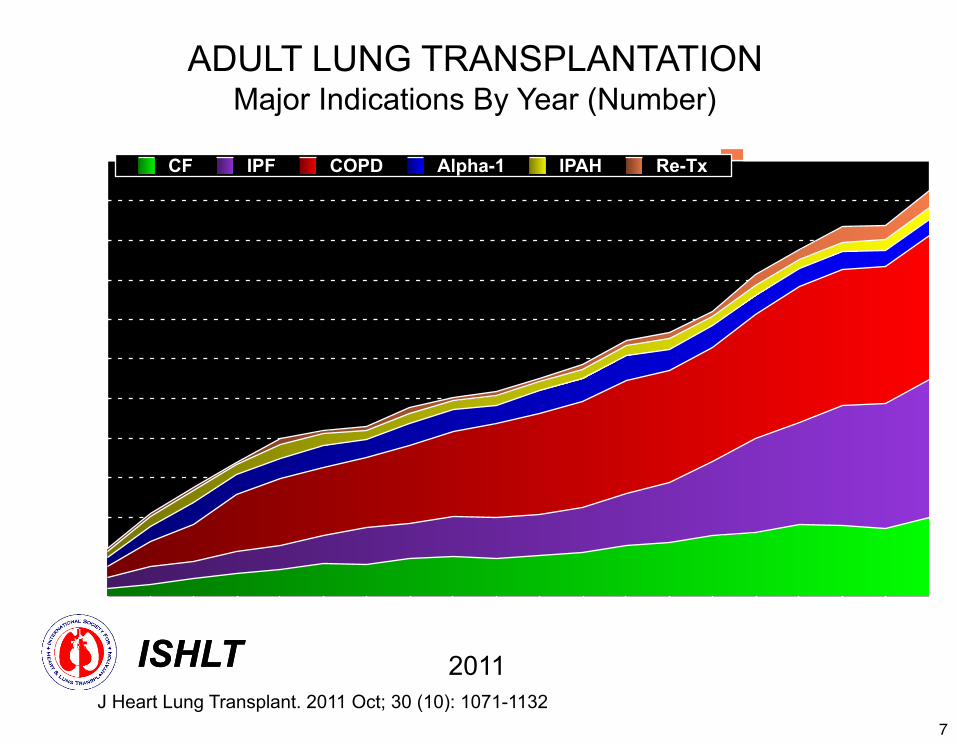
ADULT LUNG TRANSPLANTATIONMajor Indications By Year (Number)
0
17.50
35.00
52.50
70.00
Myopathy CAD
198219831984198519861987198819891990199119921993199419951996
0
250
500
750
1000
1250
1500
1750
2000
2250
2500
2750
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Num
ber o
f tra
nspl
ants
Transplant Year
CF IPF COPD Alpha-1 IPAH Re-Tx
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
7
Lung Transplantation for ILD
• 3 potential types of procedures: heart/lung, double lung, single lung
• Heart/lung transplantation 1980s now uncommon
• Double lung – if chronic suppurative infection or if pulmonary hypertension, will lessen graft dysfunction upon implantation
• Increasing trend for double lung transplant • Increased mortality on wait list
8
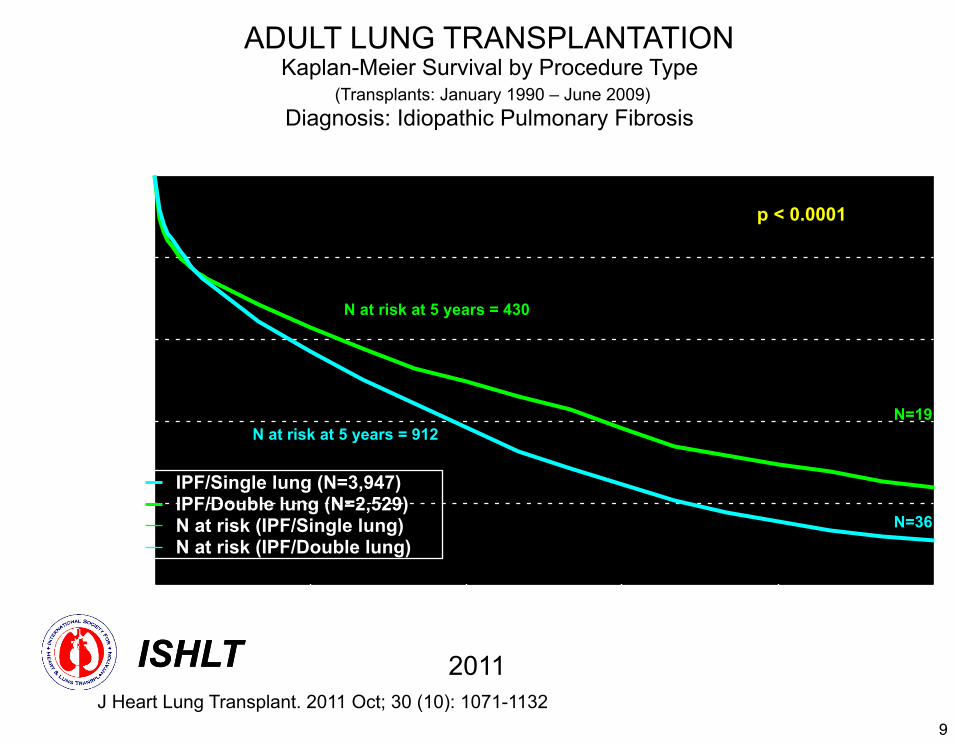
ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival by Procedure Type
(Transplants: January 1990 – June 2009)Diagnosis: Idiopathic Pulmonary Fibrosis
0
20.0000
40.0000
60.0000
80.0000
100.0000
0 3 6 9 12 15
Surv
ival
(%)
Years
IPF/Single lung (N=3,947)IPF/Double lung (N=2,529)N at risk (IPF/Single lung)N at risk (IPF/Double lung)
N=36
N=19
p < 0.0001
N at risk at 5 years = 430
N at risk at 5 years = 912
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
9
Contra-indications for Lung Transplantation
• Malignancy/cancer within 2 years• Untreatable dysfunction of other organ
system• Chronic incurable extra-pulmonary
infection• Chest deformity• Non-adherence• Substance addiction –tobacco, alcohol,
10
Relative Contra-indications for Lung Transplantation
• Age ? • Severely limited functional status• Colonization with resistant bacteria, fungi,
mycobacteria• Body mass index > 30 kg/m2• Mechanical ventilation• Other medical comorbidities – need to be
optimized – diabetes, hypertension, gastroesophageal reflux, coronary artery disease
11
Lung Transplantation for ILD
• Early evaluation • Progression of disease can be
unpredictable• More difficult to accomplish urgent/
emergent work-up when critically ill• Patients expected to participate in
pulmonary rehab program• Medical and psychosocial assessment
12
Lung Transplantation for ILD
• Risk factors and prognoses unique to ILD patients awaiting transplant– Fibrosis score on chest CT scan– Pulmonary function testing may not always
correlate with outcome– 10% decline forced vital capacity identifies
high risk – Drop in oxygen with exercise– “Acute exacerbations”
13

Lung Transplantation for ILD
14

Lung Transplantation for ILD
• Improved peri-operative outcomes• Improved donor management, operative
techniques, critical care • Cardiopulmonary techniques to manage
critically ill patients• Patients often sicker at time transplant in
current era
15
Lung Transplantation for ILD
• Lung allocated by blood group, size• Lung Allocation Score (LAS)
– DOB, height, weight– Diagnosis– Functional status, six minute walk distance– Diabetes, kidney tests– Ventilation, supplemental oxygen, breathing
tests, carbon dioxide– Pulmonary artery pressure
16
Lung Transplantation for ILD
• Transplant team members– surgeon (MD)– pulmonologist (MD)– coordinators (RN, NP, PA)– psychologist– social worker– infectious diseases (MD)– financial coordinator– transplant administrators
17

18
Lung Transplantation for ILD
• Extensive testing – blood counts – kidney and liver function – CT scan of chest and abdomen – perfusion scanning – right and left heart catheterization – serologies to common viruses – CMV, EBV– blood types, antibodies to donor proteins
19
20
21
Lung Transplantation for ILD
• Recovery – Intensive care unit (ICU) with breathing tube,
ventilator and chest tubes– Regular hospital ward – nutrition, airway
clearance, incentive spirometer, chest tubes– Education about medical regimen and active
learning about self-care– Length of stay may vary anticipate 14-21 days
22
Lung Transplantation for ILD
• Primary Graft Dysfunction– Early re-implantation and perfusion– Cold preservation solution to warm re-
perfusion– Reactive oxygen – Severity graded by oxygenation– Higher incidence in ILD and high pulmonary
circulation pressures
23
Lung Transplantation for ILD• Early events –
– Infection – hospitalization, donor, community– Anti-viral and anti-fungal prophylaxis
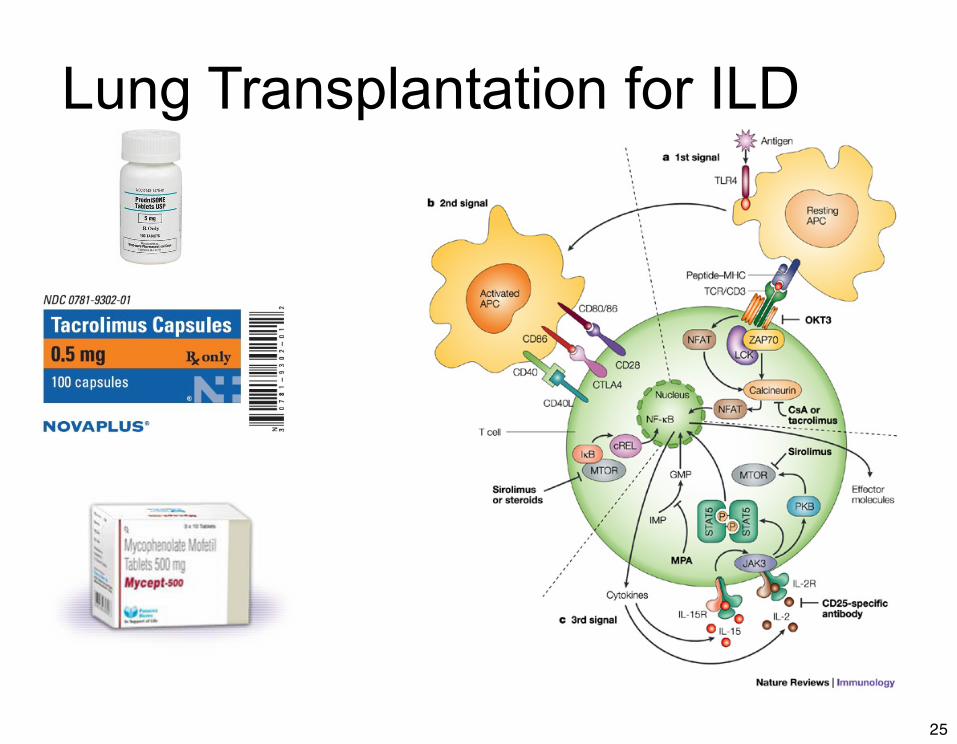
• Life-long immunosuppression– Deplete immune cells at the time of transplant– Steroids– Calcineurin inhibitor (tacrolimus or cyclosporin)– Anti-metabolite (azathioprine or mycophenolate
mofetil)
24
Lung Transplantation for ILD
25
Lung Transplantation for ILD
26
Lung Transplant for ILD• Acute rejection
– Present with cough, fatigue, shortness of breath– 30-40 % within 1st year– Acute rejection - foreign proteins on the donor lungs
and the recipient’s immune system response– Diagnosed with tissue sample read by pathologist– Treat acute rejection with steroids– If persistent, add stronger biological therapy to
deplete immune cells
27
Lung Transplant for ILD
• Chronic lung allograft dysfunction– Recipient response to donor lungs over time
causing scarring– ~ 45 % of patients develop by 5 years time– Diagnosed by following pulmonary function
testing– Multiple causes – repeated acute rejection,
antibodies to the donor lungs, chronic aspiration, responses to viral infections
28
Lung Transplantation for ILD
• Long term complications– Chronic lung allograft rejection– Kidney insufficiency and high blood pressure– Diabetes– Anemia– Skin cancers and post-transplant lymphoma– Osteoporosis
29

ADULT LUNG TRANSPLANTATIONKaplan-Meier Survival (Transplants: January 1994 - June 2009)
0
25.0000
50.0000
75.0000
100.0000
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
Bilateral/Double Lung (N=16,628)Single Lung (N=12,085)All Lungs (N= 28,727)Number at risk (bilateral/double)Number at risk (single)Number at risk(all)
Double lung: 1/2-life = 6.8 Years; Conditional 1/2-life = 9.3 YearsSingle lung: 1/2-life = 4.7 Years; Conditional 1/2-life = 6.5 YearsAll lungs: 1/2-life = 5.5 Years; Conditional 1/2-life = 7.8 Years
P < 0.0001
Surv
ival
(%)
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
30

ADULT LUNG TRANSPLANTATION Kaplan-Meier Survival by Age Group (Transplants: January 1990 – June 2009)
0
20.0000
40.0000
60.0000
80.0000
100.0000
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Years
18-34 (N = 5,523)35-49 (N = 7,980)50-59 (N = 11,389)60-65 (N = 5,685)>65 (N = 1,217)N at risk (18-34)N at risk (35-49)N at risk (50-59)N at risk (60-65)N at risk (66+)
Survival comparisonsAll p-values significant at p < 0.0001 except 18-34 vs. 35-49: p =0.1708
HALF-LIFE 18-34: 6.4 Years; 35-49: 6.7 Years; 50-59: 5.3 Years; 60-65: 4.4 Years; >65: 3.5 Years
Surv
ival
(%)
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
31
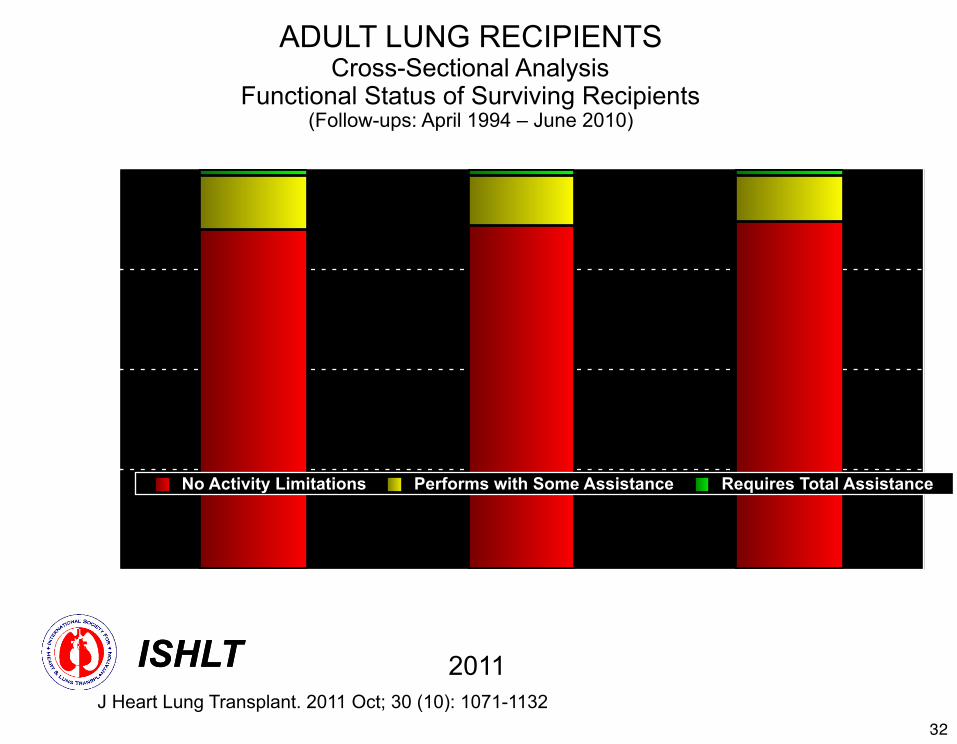
ADULT LUNG RECIPIENTSCross-Sectional Analysis
Functional Status of Surviving Recipients(Follow-ups: April 1994 – June 2010)
0%
25%
50%
75%
100%
1 Year (N = 6,882) 3 Year (N = 4,423) 5 Year (N = 2,544)
No Activity Limitations Performs with Some Assistance Requires Total Assistance
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132
32
Lung Transplantation for ILD• Heterogeneous disease• Difficult to predict timing of transplant• IPF now > 50 % of lung transplants• Early referral best• Keep in shape, wear oxygen, exercise, nutrition• Support groups• Education• THANK YOU !!
33
Top Related