







Languages
Pages
Legal


Slide 1
David O’Neill MSc BSc RN NMP FHEA
Associate Lecturer (Non Medical Prescribing) Cardiff University
Advanced Nurse Practitioner Respiratory Medicine
ARTERIAL BLOOD GAS
INTERPRETATION
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2
David O'Neill
Learning Outcomes
• Understand Acid-base balance physiology
• Understand Buffer systems in acid base
balance
• Basic understanding of Oxygen dissociation
• Know normal ABG parameters
• To systematically analyse and interpret ABG
results
• Review Anion gap and its use
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3
David O'Neill
Acid base terminology
• Acids are substances which have a high
concentration of Hydrogen ions [H+]
– Which two bodily substances have high
concentration of hydrogen ions? (i.e. very acidic)
• Bases (or alkalis) are substances with low
concentration of hydrogen ions and high
concentration of bicarbonate ions [HCO3-]
– Which bodily substance has a high concentration
of bicarbonate ions (i.e. very alkaline)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 4
David O'Neill
pH of body fluids
Body Fluid pH
Gastric juices 1.0-3.0
Urine 5.0-6.0
Arterial blood 7.4
Venous blood 7.36
CSF 7.32
Pancreatic fluid 7.8-8.0
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5
David O'Neill
pH scale
• Hydrogen ion concentration is
expressed as the pH scale
(range 1 to 14)
• Logarithmic scale
• If pH changes by 1 unit (7.0 to 6.0)
Hydrogen ions increase by tenfold
• Greater [H+] lower pH and vice versa
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6
David O'Neill
Source of acids
• About 100mmols/day is formed as result of
end products of cellular metabolism of
protein, carbohydrates and fats
• It must be neutralised or excreted
• There are three main systems involved in
acid base balance – what are they?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 7
David O'Neill
Acid base balance
• Lungs
• Kidneys
• Bones
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8
David O'Neill
Acid base balance
• Systems interrelated
• Acid exists in two forms
– VOLATILE
• Eliminated as CO2 gas
– NON VOLATILE
• Are eliminated by the renal tubules
and regulated by HCO3-
• Lungs & Kidneys (assisted by buffers) are
main regulators of acid-base balance
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 9
David O'Neill
Carbonic acid
• Carbonic acid (H2CO3) is a weak acid
(Volatile)
• In presence of CARBONIC
ANHYDRASE (an enzyme)
• It easily breaks down into carbon
dioxide and water
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 10
David O'Neill
Respiratory equation
LUNGS KIDNEYS
• CO2 + H20 H2CO3 HCO3-+ H
+
This is a reversible reaction and can go both
ways
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11
David O'Neill
Bicarbonate in the blood
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12
David O'Neill
Oxygen dissociation curve
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 13
David O'Neill
Buffer systems 1
• Buffers:
– Absorb excessive H+
ions (Acids) or OH-
ions (Bases)
– Exist in ICF and ECF compartments
– FUNCTION AT DIFFERENT RATES
– Exist as buffer pairs of weak acid and
conjugate base
– Can associate and dissociate
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 14
David O'Neill
Buffer systems 2
• The most important PLASMA buffer
systems are:
– CARBONIC ACID-BICARBONATE
and
– HAEMOGLOBIN
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15
David O'Neill
Buffer systems 3
• The most important INTRACELLULAR
buffer systems are:
– PHOSPHATE
AND
– PROTEIN
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 16
David O'Neill
Buffer systems
Buffer
pair
Buffer
system
Reaction Rate
HCO3-
/H2CO3
Bicarbonate H++ HCO3
-= H2O + CO2 INSTANT
Hb-/HHb Haemoglobin HHb = H
++ Hb
-INSTANT
HPO42-
/H2PO4-
Phosphate H2PO4-
= H+
+
HPO4-
INSTANT
Pr-/HPr Plasma
proteins
HPr = H+
+ Pr-
INSTANT
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 17
David O'Neill
ORGAN SYSTEMS
ORGANS MECHANISM RATE
Lungs Regulates retention/elimination
of CO2 and hence H2CO3
Minutes-hours
Ionic shifts Exchange intracellular
potassium and sodium for
hydrogen
2-4 hours
Kidneys Bicarbonate reabsorption and
regeneration, ammonia
formation, phosphate buffering
Hours to days
Bone Exchange calcium, phosphate
and release of carbonate
Hours to days
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18
David O'Neill
Carbonic acid-Bicarbonate buffering
• The most important buffer.
• Operates in lungs AND kidney
• Lungs get rid of CO2 and retain H2O
• Kidneys reabsorb H2CO3-and water.
• Both systems work well together with
the lungs quickly adjusting acid
concentration and kidneys reabsorb or
regenerate H2CO3-
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 19
David O'Neill
Why is this important?
• All systems work together to maintain a NORMAL ph (7.35-7.45)
• Outside these parameters enzyme systems start to fail
• Deficit in any of these can affect acid base balance
• Adjustment of abnormal pH is called COMPENSATION but it can leave some abnormal values
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20
David O'Neill
Renal buffering 1
• Distal tubules:
– Secrete H+
into urine and reabsorbs HCO3-
– Phosphate (HPO42-
) and ammonia (NH3)
– HPO42-
(in tubule) combines with H+
to
create H2PO4-which is lipid insoluble and
hence excreted in urine
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21
David O'Neill
Renal buffering 2
– H+
combines with NH3 to form ammonium
ions (NH4 +) which are excreted in urine
– Buffering H+
requires use of CO2 and H2O
to form H2CO3-
– New H2CO3-
is added to plasma and H+
are excreted in urine resulting in more
alkaline plasma
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 22
David O'Neill
Normal ABG
• pH 7.35-7.45
• PaCO2 4.6 – 6 kPa (35-45mmHg*)
• PaO2 10.6- 14.6 kPa (80-110mmHg)
• HCO3 24-26mmols/l
• Base Excess -3 to + 3
*To convert kPa to mmHg multiply by 7.5
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23
David O'Neill
Base excess
• Derived variable
• Indicates acidity/alkalinity
• Highly NEGATIVE numbers are very ACIDIC(eg -15)
• Highly POSITIVE numbers are very ALKALINE (eg +15)
• It is calculated from how much acid or alkaline is required to return pH to normal at standard temperature and pressure
• It is an alternative to looking at the HCO3 value
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24
David O'Neill
ABG Interpretation Step 1.
Look at the pH
– Is it Low (equals ACIDIC)
– Is it High (equals ALKALINE)
– Is it Normal
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 25
David O'Neill
ABG Interpretation Step 2
• Look at the PaCO2
– Is it HIGH (equals ACIDIC)
– Is it LOW (equals ALKALINE)
– Is it NORMAL
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26
David O'Neill
ABG Interpretation Step 3
• Look at PaO2
– Is it HIGH
– Is it LOW
– Is it NORMAL
Does Oxygen have a direct impact on acid
base balance?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27
David O'Neill
ABG Interpretation Step 4
• Look at the HCO3 OR Base Excess
– Is it LOW (EQUALS ACIDIC)
– Is it HIGH (EQUALS ALKALINE)
– Is it NORMAL
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 28
David O'Neill
Examples
• pH 7.30
• ACIDIC
• PaCO2 7.3kPa (55mmHg)
• ACIDIC
• PaO2 12kPa (85mmHg)
• NORMAL
• HCO3 24mmols/l
• NORMAL
• Base Excess +1
• NORMAL
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 29
David O'Neill
Interpretation
• Its an ACIDOSIS
• The system causing the acidosis is
RESPIRATORY
(high CO2 causes acidosis)
• The pH is still deranged so its ACUTE
• The HCO3 and BE are still NORMAL so
there is NO COMPENSATION
• So its an ACUTE RESPIRATORY ACIDOSIS
(acute type II respiratory failure)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 30
David O'Neill
Example 2
• pH 7.37
• PaCO2 7.3kPa (55mmHg)
• PaO2 8.0kPa (60mmHg)
• HCO3 30mmols/l
• Base Excess +7
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 31
David O'Neill
Interpretation
• pH is NORMAL
• PaCO2 is HIGH (ACID)
• PaO2 is LOW (no effect on pH at this level)
• HCO3 is HIGH (ALKALINE)
• Base excess is HIGH (ALKALINE)
• Original disturbance was respiratory
• COMPENSATION has occurred returning pH to normal range
• Chronic Type II respiratory failure
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32
David O'Neill
Example 3
• pH 7.25
• PaCO2 10kPa (75mmHg)
• PaO2 7kPa (52.5mmHg)
• HCO3 30mmols/l
• Base Excess +6
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33
David O'Neill
Interpretation
• pH is deranged (Acidotic)
• Therefore ACUTE
• PaCO2 is HIGH therefore ACID
• PaO2 is LOW (no effect)
• HCO3 and Base Excess are HIGH and
therefore ALKALINE AND CHRONIC
• ACUTE ON CHRONIC TYPE II
RESPIRATORY FAILURE
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 34
David O'Neill
Example 4
• pH 7.10
• PaCO2 3kPa (22.5mmHg)
• PaO2 20kPa (150mmHg)
• HCO3 14mmols/l
• Base Excess -12
• Blood Glucose 30mmols/l
• Urine Ketones +++ Glucose +++
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35
David O'Neill
Interpretation
• pH is low therefore ACIDIC
• It is still deranged, therefore ACUTE
• PaCO2 is LOW (ALKALINE)
• PaO2 is high (probably too much O2)
• HCO3 is LOW therefore ACIDIC
• Base Excess is LOW therefore ACIDIC
• So its ACUTE METABOLIC ACIDOSIS with respiratory alkalosis (compensation)
• Given blood glucose and ketones in urine Diabetic Ketoacidosis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36
David O'Neill
Example 5
• pH 7.50
• PaCO2 6.6 kPa (50mmHg)
• PaO2 10kPa (75mmHg)
• HCO3 35mmols/l
• Base Excess +10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 37
David O'Neill
Interpretation
• pH is HIGH therefore ALKALINE
• It is still deranged therefore ACUTE
• PaCO2 is slightly High (ACIDOTIC) BUT it WON’T get any higher, WHY?
• HCO3 is HIGH (ALKALINE) as is the
• Base Excess (ALKALINE)
• Therefore its an ACUTE METABOLIC ALKALOSIS with respiratory acidosis as compensation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 38
David O'Neill
Example 6
• pH 7.10
• PaCO2 8kPa (60mmHg)
• PaO2 10kPa (75mmHg)
• HCO3 15mmols/l
• Base Excess -10
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 39
David O'Neill
Interpretation 1
• pH is LOW therefore ACID
• pH is still deranged, therefore ACUTE
• PaCO2 is HIGH therefore ACID
• PaO2 is ? Normal
• HCO3 is LOW therefore ACID
• Base Excess is LOW, therefore ACID
• So what’s going on?
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 40
David O'Neill
Interpretation 2
• It’s a MIXED ACIDOSIS,
• Predominantly METABOLIC IN ORIGIN
• Action would be to CORRECT THE
UNDERLYING METABOLIC COMPONENT
(DKA, renal Failure, Cardiac failure leading to
lactic acidosis)
• Then review the Pa CO2 which will probably
then have little effect on the pH
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 41
David O'Neill
Anion gap
• Is an estimate of unmeasured Anions
• It is the difference between:
• Cations (Na and K) and
• Anions (Cl and HCO3-
)
• NORMAL RANGE 10-18mols/l
• Eg Na + K – Cl + HCO3-
• (135 + 4.0) – (100 + 24) = 139 – 124 = 15
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 42
David O'Neill
Metabolic Acidosis with increased anion
gap
• Increased production of fixed or organic acids causes:
– HCO3-
to fall
– Unmeasured anions associated with the acids accumulate
• Caused by Increased Lactic acid (shock infection, hypoxia)
• Urea (renal failure)
• Ketones (diabetes, alcohol
• Drugs/toxins (salicylates, biguanides, ethylene glycol, methanol)
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 43
David O'Neill
Metabolic Acidosis with normal anion
gap
• Due to loss of bicarbonate or ingestion
of hydrogen ions (Cl-
) retained
– Caused by renal tubular acidosis
– Profuse diarrhoea
– Drugs (acetazolamide)
– Addisons disease
– Pancreatic fistula
– Ammonium chloride ingestion
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 44
David O'Neill
Questions
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 45
David O'Neill
References
• Longmore, M, Wilkinson, I, Torok, E (2001) Oxford Hnadbook of
Clinical Medicine Oxford Oxford University Press.
• McCance KL, Heuther, SE. (2006). Pathophysiology-The biologic
basis for disease in adults and children. St Louis. Elsevier-Mosby
• Parson PE Heffner JE. (2002) Pulmonary/Respiratory Therapy
Secrets (2nd Ed.) Philadelphia. Hanley & Belfus
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 46
David O'Neill
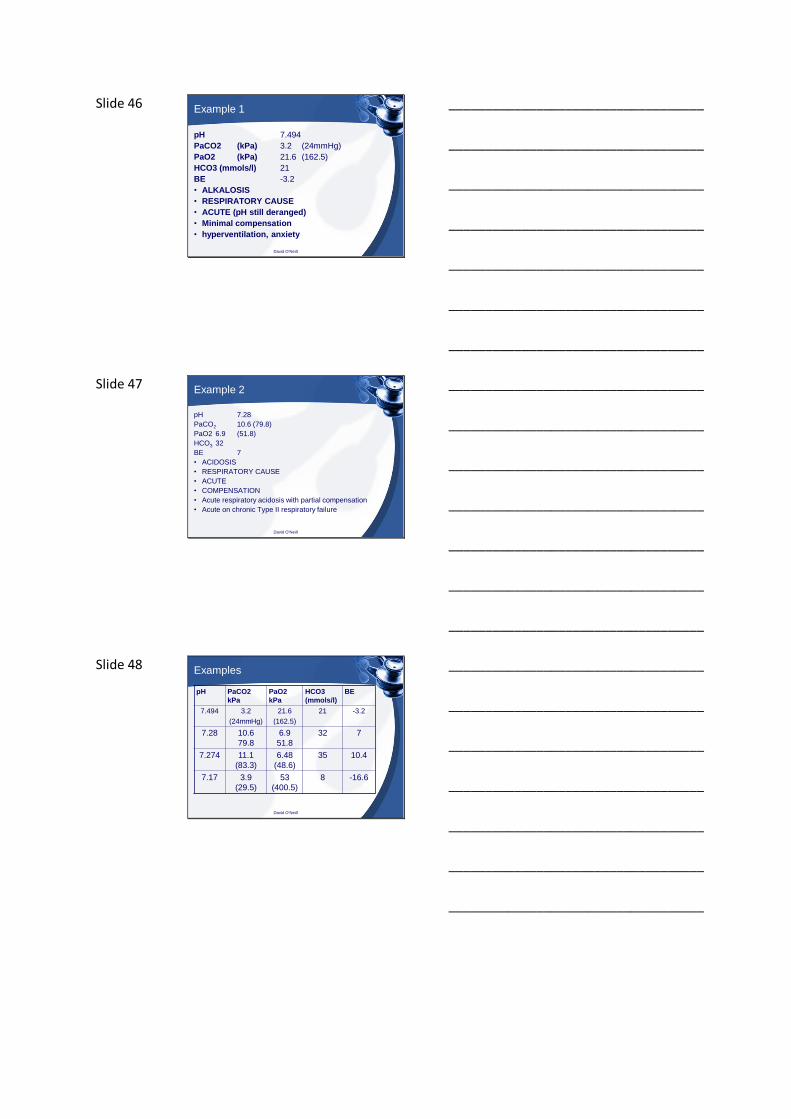
Example 1
pH 7.494
PaCO2 (kPa) 3.2 (24mmHg)
PaO2 (kPa) 21.6 (162.5)
HCO3 (mmols/l) 21
BE -3.2
• ALKALOSIS
• RESPIRATORY CAUSE
• ACUTE (pH still deranged)
• Minimal compensation
• hyperventilation, anxiety
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 47
David O'Neill
Example 2
pH 7.28
PaCO2 10.6 (79.8)
PaO2 6.9 (51.8)
HCO3 32
BE 7
• ACIDOSIS
• RESPIRATORY CAUSE
• ACUTE
• COMPENSATION
• Acute respiratory acidosis with partial compensation
• Acute on chronic Type II respiratory failure
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 48
David O'Neill
Examples
pH PaCO2
kPa
PaO2
kPa
HCO3
(mmols/l)
BE
7.494 3.2
(24mmHg)
21.6
(162.5)
21 -3.2
7.28 10.6
79.8
6.9
51.8
32 7
7.274 11.1
(83.3)
6.48
(48.6)
35 10.4
7.17 3.9
(29.5)
53
(400.5)
8 -16.6
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 49
David O'Neill
Examples
pH PaCO2
kPa
PaO2
kPa
HCO3
(mmols/l)
BE
7.278 5.2
(39.2)
8.1
(61.2)
16 -7.9
6.867 105.1 60.3 8 -16.6
7.335 12.2
(91.8)
10.5
(78.8)
16.7 -9
7.365 10.1
(76.9)
14.6
(110)
40 15.4
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Top Related