







Languages
Pages
Legal


Department of Public Health and Caring sciences
Section of Caring Science
Knowledge and practices regarding foot care
among patients with Type 2 diabetes in Ho Chi
Minh City, Vietnam
A quantitative study
Authors: Supervisor:
Sofia Hellenberg Pranee Lundberg
Stina Thunberg Co- supervisor:
Nguyen Thi Phuong Lan
Examiner:
Clara Aarts
Thesis in Caring Sciences 15 ECTS credits
The Bachelor Programme of Science in Nursing 180 ECTS credits, 2013

1
ABSTRACT
Introduction: Previous research shows that knowledge and practice was low in type 2
diabetes patients and that women had better practice/self-care than men.
Aim: The aim of this study was to investigate the knowledge and practices regarding foot-
care among patients with type 2 diabetes in Ho Chi Minh City, Vietnam, and also investigate
if there was any difference between genders in knowledge and practicing of foot care.
Method: This study was a descriptive and cross-sectional design with quantitative method.
The data was collected at the out-patient clinic of the University Medical Center in Ho Chi
Minh City, Vietnam and 100 patients participated voluntarily to answer questionnaire. Orem’s
self-care theory was used as theoretical framework. Data were analysed by using statistics.
Result: The result shows that more than 70% of the patients had good knowledge of foot care
and no significant differences between the genders in the knowledge. Their foot care practices
were various. There was significant difference between men and women about using a hot
water bottle or heating pad on the feet, and more women than men did. For type of shoes,
there were differences between genders in wearing broad, round toes and shoes made of
leather or canvas, and more men than women did.
Conclusion: The knowledge of foot care was good, but the practice of foot care was low.
There was not found any significant difference between the genders in knowledge, but some
differences in the foot care practices. More information about foot care is needed to prevent
complications with type 2 diabetes.
Key words: Diabetes Mellitus, Knowledge, Foot Care, Gender, Ho Chi Minh City

2
SAMMANFATTNING
Introduktion: Tidigare forsknings resultat visar att kunskapen om egenvård och utförande av
fotvård hos patienter med diabetes typ 2 var låg. Kvinnorna var dock bättre på att utföra
egenvården än männen.
Syfte: Syftet med denna studie var att undersöka kunskapen och utförandet av egenvård hos
patienter med diabetes typ 2 i Ho Chi Minh City, Vietnam, samt att undersöka om det fanns
några skillnader mellan män och kvinnor i kunskapen om egenvård inom fotvård samt dess
utförande.
Metod: För att undersöka detta gjordes en kvantitativ tvärsnittsstudie med hjälp av enkäter.
Det var 100 patienter på en mottagning vid University Medical Center, Ho Chi Minh City,
Vietnam, som deltog frivilligt. Orems egenvård teori användes som teoretiskt ramverk i detta
arbete. Data analyserades av statistik.
Resultat: Resultatet i denna studie påvisar att mer än 70 % av patienternas visade god
kunskap och inga signifikanta skillnader fanns mellan kvinnor och män gällande
kunskapsnivån. Utförandes av fotvården visade sig dock vara varierande och det fanns
signifikanta skillnader mellan kvinnor och män gällande fotvården. Kvinnor använde sig
oftare av varma pads och flaskor på deras fötter än vad männen gjorde. Kvinnor och män
använde också olika typer av skor. Männen använde oftare breda skor med rundad tå, skor av
läder eller canvas skor än vad kvinnorna gjorde.
Slutsats: Kunskapen om fotvård hos diabetes patienter i Ho Chi Minh City var god, dock var
utförandet av fotvården varierande i denna studie. Det visades ingen signifikant skillnad
mellan kvinnor och män angående kunskapsnivån, dock fanns det skillnader angående
utförandet av fotvården. Det behövs fortsatt information om fotvård för att patienter med typ 2
diabetes ska förhindra komplikationer
Nyckelord: Diabetes Mellitus typ 2, Kunskap, Fotvård, Kön, Ho Chi Minh City

3
CONTENTS
1. Introduction 5
1.1 Type 2 diabetes mellitus 5
1.2 Prevalence of type 2 diabetes in the world 5
1.3 Type 2 diabetes in Vietnam 6
1.4 Risk factors 6
1.5 Complications 6
1.6 Foot ulcer 7
1.7 Self-care and treatment of diabetes 8
1.8 Knowledge about diabetes and foot care in type 2 diabetes patients 9
1.9 Practice of foot care in type 2 diabetes patients 10
2. Theoretical framework 11
3. Rationale of research 12
4. Aim 12
5. Research questions 12
6. Methods 13
6.1 Design 13
6.2 Settings 13
6.3 Sample 13
6.4 Data collection method 16
6.5 Procedure 16
6.6 Data analysis 17
7. Ethical considerations 18

4
8. Results 18
8.1 Demographic information 18
8.2 History of foot problems 19
8.3 Current foot or leg problems 19
8.4 Knowledge of foot care 19
8.5 Foot care practice 20
8.6 Foot care education 24
9. Discussion 25
9.1Results discussion 26
9.1.1 Knowledge of foot care among the patients with type 2 diabetes 26
9.1.2. Foot care practices among patients with type 2 diabetes. 26
9.1.3. Difference between genders in knowledge and practice of foot care 27
9.2 Method discussion 28
9.3 Theoretical framework discussion 29
9.4 Clinical implication 30
9.5 Further research study 30
9.6 Acknowledgement 31
10. References 32
Appendix 1 Questionnaire 36

5
1. INTRODUCTION
1.1 Type 2 diabetes mellitus
Type 2 diabetes is a chronic disease that develops when the pancreas does not produce enough
insulin, or when the body is unable to use the insulin it produces effectively. The hormone
insulin is regulating the blood sugar. If the blood sugar is too high over a long time it can lead
to serious damage on the body’s systems, especially the blood vessels and nerves (World
health organization, [WHO] 2013). Type 2 diabetes develops when the body fails to use its
own insulin. The most common reason is high body weight and/or inactivity (Almås, 2001).
Symptoms of type 2 diabetes are increased urination, thirst and fatigue mentally and
physically. Some people also get bad eyesight. The symptoms often develop very slowly and
some people do not get any symptoms at all, which makes it difficult to defect the disease
(FASS, 2011). The patient can be diagnosed in three ways: glycosylated hemoglobin test,
fasting glucose and oral glucose test. After the diagnosis is determined the patient have to do
home monitoring and do regular check up’s at the local nurse (Heart, 2012).
1.2Prevalence of type 2 diabetes mellitus in the World
About 347 million people around the world have diabetes and 90 % of the affected have
diabetes type 2 (WHO, 2013). In 1980 the prevalence of people with diabetes was 153 million
in the world. Reasons for the increase of type 2 diabetes are obesity, inactivity, urbanization,
adverse dietary and that people get older (Maruthur, 2013). The biggest increase is in Asia,
Middle East and in America (Insulin, 2011). Type 2 diabetes occurs in both high- and low-
income countries. However, the low-income countries are bearing the majority of the burden.
Increased supervision of the diabetes contributed to an increased prevalence of diabetes in
high income countries (Maruthur, 2013).
The prevalence of type 2 diabetes varies across regions. In 2008 the prevalence of diabetes
was highest in Oceania (>15 %). The lowest prevalence of diabetes was in the high-income
region of North America and of Asia-pacific region. Australia and Western Europe had also a
low prevalence (Maruthur, 2013). Globally more than 60 % of people with diabetes is in
Asian countries. The prevalence of diabetes and impaired glucose tolerance are high in all
Asian countries and are expected to increase further (Ramachandran, Snehalatha, Samith-
Shetty & Nanditha, 2012).

6
1.3 Type 2 diabetes in Vietnam
Type 2 diabetes is on it is rise in Vietnam. In 2000 the prevalence of people with diabetes in
Vietnam was 792,000 (WHO, 2000). In 2012 experts believed that approximately two million
people had diabetes in Vietnam. About 60 % of them are unaware of their condition and
remain undiagnosed (WHO, 2012). In 2004 the prevalence of type 2 diabetes was 3.8% in Ho
Chi Minh City, Vietnam. The people in Ho Chi Min City with a high level of education had a
lower prevalence of type 2 diabetes, compared to people with lower level of education (Duc
Son et al., 2004). In 2008 almost seven percent of the adults in age 30 – 69 years had diabetes
in Ho Chi Minh City (WHO, 2012).
1.4 Risk factors
Type 2 diabetes is a common disease which usually affects older people, however it is
beginning to be more common in younger ages. The disease often develops gradually and can
be inherited, but it can also be due to the lifestyle (Almås, 2001). A “key” risk factor for
developing type 2 diabetes is overweight and obesity. Other risk factors are ageing, genetics,
previous gestational diabetes and family history of type 2 diabetes (Mc Naughtun,
2013). Physical inactivity, stress and smoking are also risk factors for type 2 diabetes (Almås,
2001). In the study of Tomisaka et al. (2002) about risk factors for type 2 diabetes among
Asian women, they found that Vietnamese women were at high risk to develop type 2
diabetes because of their high obesity levels and their carbohydrate intake was higher than the
other Asian women in the study.
1.5 Complications
In 2004 three - four million people around the world died in complications of high blood
sugar and 80% of the deaths due to diabetes occur in low- and middle-income countries. In
the next ten years they are projected to rise about 50 % (WHO, 2013). High blood sugar
during a long time can results in a lot of complications for the patient. The acute
complications of diabetes mellitus are hyperglycemia, hypoglycemia and ketoacidosis.
Chronic complications of diabetes mellitus are angiopathy. This complication can give
cerebrovascular, cardiovascular, peripheral vascular disease, retinopathy, blindness,

7
neuropathy and nephropathy. Neuropathy means that the nerves are damaged, which affects
the sensitivity in the hands, feet or both, but it can also give the patients tingling, burning
and/or tearing in the outer extremity. This can lead to ulcers in the lower extremity. Diabetic
patients are also more susceptible to infections than other patients (Brown & Edwards. 2005).
1.6 Foot ulcers
Foot complications are common in type 2 diabetes patients. Diabetes may cause nerve
damage that can take away the feeling in the feet, which can make the patients unable to feel
stones in their shoes or blisters on their feet. The blood circulation to the feet can also be
reduced which can make it difficult for ulcers on the feet to heal. This complication can lead
to an infection or a non-healing ulcer, and in the worst case it can lead to amputation
(American College of Foot and Ankle Surgeons, [ACFAS] 2009). Sensory neuropathy and
peripheral vascular disease is the main reason for foot ulcers but also clotting abnormalities,
immune functions, smoking and neuropathy play an important role. Peripheral vascular
disease make it hard for the nutrition and oxygen to get to the ulcer making it hard for it to
heel and in the worst case it can lead to amputation (Brown and Edwards, 2005). Diabetic foot
ulcers can also have negative psychological and social effects. For example it can lead to
reduced social activities and employments. It can also have negative effects on the diabetes
patient mental health and at the relationship to family and friends (Goodridge, Trepman &
Embil, 2005).
In Fuller (2013) it is found that amputation related to foot ulcer is very common in Vietnam
and creeps lower in age. It often starts with a small scrape and develops to a hard treated
ulcer. The doctors believe that foot ulcers in type 2 diabetes patients are very common in
Vietnam because of lack of wearing shoes to protect their feet. It is more common to use
sandals, go barefoot or have flip-flops which do not protect the foot. The doctors in Ho Chi
Minh City mean that the situation in Vietnam is severe, however, it cannot be more specific
because it is a lack of data about diabetes and foot care which have been analyzed. One of the
doctors in Ho Chi Minh City said that it is getting worse every day and a pandemic is coming
in a few years. Diabetes is a result from a new urban lifestyle, no exercise, migration from the
countryside to the big cities and working in factories instead of the fields, but the normal
patient in Vietnam is not obese. They also point out that the symptoms emerges gradually, so

8
it is common to have the disease without knowing for many years, especially where health
care systems are rudimentary.
1.7 Self-care and treatment of diabetes
The primary treatment of type 2 diabetes is self-care because it improves the patients’ health
and prevents complications. Many of the risk factors can be prevented with changes of
lifestyle for people with high risk (Marques, Silva, Coutinho & Lopes, 2013). The lifestyle
changes involve eating healthy food, loss in weight for people with obesity, regular exercises,
foot care and meetings with health care providers regularly. The patients have to learn about
the disease, self-monitoring the glucose and how the treatment works (Almås, 2001). The
self-care is a partnership between the patient and the health care provider. The health care
provider gives information of self-care and mentoring in self-care to let the patient perform it
(Marques et al., 2013).
The health care provider’s education for the diabetes patient is important for their self-care of
the disease. If the information to the patient is not clear, the patient can forget it or may not
understand it, the patient can also miss out important facts. This can cause lack of the self-
care or ignorance of the healthy lifestyle for the patient (Tham, Ong, Tan &How, 2004).
Increased participation in decision-making about diabetes care is associated with an
increasing understanding of self-care in diabetes (Quinn et al., 2011). The competence of self-
care can decrease in elderly age. Marques et al. (2013) found that very few (6 %) of the
elderly with type 2 diabetes had the competence to provide their self-care. Low level of
education and bad eyesight was contributing factors and this group needs more help and
instruments for performing their self-care.
Medication may be needed if blood glucose is not adequately controlled with the primary
treatment. The aim of treatment is to lower the blood glucose levels and reduce the risk of
complications. Preventive measures to prevent foot problems should begin immediately after
diabetes diagnosis is established (Almås, 2001).
Mull, Nguyen and Mull (2001) found that many Vietnamese people used herbal medicine to
treat their type 2 diabetes. They thought herbal medicine was much safer than Western
medicine because herbal medicine cools the body and brings it back into balance, but if herbal
medicine did not work they would consider Western medicine. Three-quarters of the

9
Vietnamese patients have not achieved a good control of their diabetes and one reason is that
they do not have knowledge of how the insulin works and about their disease. There was a
strong aversion to use insulin injections among the Vietnamese people because the needle was
painful, the insulin created an imbalance in the body, gave blindness, was addictive and the
insulin showed that a person was seriously ill and had a chronic disease. In Helman (2001),
Vietnamese in USA and England said that their diabetes has their roots in psychological
emotions, like feeling sad and being stressed. They also thought the weather could be the
reason of their symptoms. They explained their disease with imbalance between the “hot” and
“cold” substance in their body. They thought that insulin is a “hot” substance and could lead
to substance illness; therefore, they prefer to use traditional Chinese medicine and herbs.
1.8 Knowledge of diabetes and foot care in Type 2 diabetes patients
The study of Pollock, Unwin & Connolly (2004) showed that the type 2 diabetes patients
knowledge was low. Those with high risk generally had better knowledge than the patients
that had lower risk for foot complications and amputation. Females had higher knowledge
than the males. The patients who had received information or advice previously had better
knowledge. Also the patients in the study of Khamseh, Vatankhah & Baradaran (2007) had
low knowledge about foot care practice. The patients who had a history of diabetes in ten
years or more had better knowledge about foot care practice than those who had diabetes less
than ten years and 70 % of the patients said that they had not received advice or information
about foot care.
Khamseh et al. (2007) and Quinn et al. (2011) showed that the type 2 diabetes patients with
higher education had better knowledge than those with lower education. Quinn et al. (2011)
also described that the patients with lower education needed more information about their
diagnosis. Tham et al. (2004) found that people with type 2 diabetes, which have been
educated in diabetes, have better knowledge about the disease and in changing practices in
their self-care. In addition, Kavanagh et al. (2010) found that lower education and income are
associated with higher levels of glucose, waist circumference and blood pressure when
compared to people with higher education and income. Kafaie., Rashidi., Sedigheh
Soheilikhah &Taghi (2004) investigated self-care among patients with type 2 diabetes and
helped them by training in self-care for diabetic ulcers. The results showed that the patients

10
had inadequate knowledge about foot-care. After completing the training most of the patients
(85 %) had sufficient information to be able to perform proper self-care of their own feet.
1.9 Foot care practice
Foot care is important for preventing foot ulcers among type 2 diabetes patients. The patients
have to inspect their feet daily and check for cuts, redness, blisters, swelling or nail problems
(ACFAS, 2009). They shall wash their feet daily with warm water and a mild soap, but it’s
important to test the water temperature before washing the feet. Finally the patients shall dry
their feet and especially between the toes (Brown & Edwards, 2005). The patient will use a
moisturizer after bath, but not between the toes because that could encourage a fungal
infection. The patients shall cut the nails straight across and file the edges and wear clean, dry
socks and change them daily and keep the feet dry and warm (ACFAS, 2009). Use warm
water and mild soap when cleaning the cuts on the feet and cover with clean dressing and
separate overlapping toes with cotton. The patient has to report skin infections or non-healing
sores to health care provider immediately. Avoid prolonged sitting, standing and crossing of
legs (Brown & Edwards, 2005). The patient shall not walk barefoot because the patient can
step on something or get a cut in the foot (ACFAS, 2009). The patient shall avoid open-toe,
open-heel and high-heel shoes. Leather shoes are preferred before plastic ones. Shake the shoe
before putting it on (Brown & Edwards, 2005).
Several studies have shown that the practice of good foot care is very low (Pollock et al.,
2004; Khamseh et al., 2007;Bhupendra, Anand, Sangram, Dilip & Ravinder, 2008). In the
study of Pollock et al. (2004) 83% of the patients failed to inspect their feet. Khamseh et al.
(2007) found that it was 60% who failed to inspect their feet and 42 % did not trim their nails.
Also the patients in the study of Bhupendra et al. (2008) did not inspect their feet in the right
way and 76,4 % did not wash their feet properly and 56,4 % walked barefoot outside and
inside.
In practice of foot care it showed that there was a difference between those with high
education and those with lower, but no difference in how long the patients have had type 2
diabetes. It was 70 % of the patients did not wear footwear after the hospitals guidelines
(Khamseh et al., 2007). The attitude regarding self-care of diabetic patients with foot ulcers
may be different for men and women. Women were more active in self-care and preventive
care and they searched for more information and tried to adapt to the situation. Men searched
11
more health care for acute foot ulcers problem. They showed a passive attitude and had a
more pessimistic view of the future (Goodridge et al., 2005).
2. THEORETICAL FRAMEWORK
Dorothea Orem´s theory of self-care and self-care deficit was used as theoretical framework
for this study. The theory highlights the importance of self-care and the goal is normal
function, development, health and well-being. The theory is based on two key concepts, self-
care and self-care deficit. The first key-point (self-care) is based on why and how people care
for themselves and the second key-point (self- care deficit) describes and explains why people
can be helped through nursing and a nurse.
Self-care depends on the health of the person, interest for maintaining living, function, well-
being etc. Self- care is affected by age, unable to perform the self-care well-being and interest
of performing the self-care that is needed
The nurse have to identify five methods to help the patient
“ Acting for or doing for another”
“Guiding and directing”
“Providing physical or psychological support”
“Providing and maintaining an environment that supports personal development”
“Teaching”
(Alligood & Tomey, 2009).
Dorothea Orem means that nursing-care is needed when the patient is affected of limitations
which make it difficult to practice their self-care of example on their feet. The nursing care
will give possibility for the patient to regain the capacity of self-care (Kirkevold, 2000).
Therefore, this theoretical framework was used to investigate if the patients with type 2
diabetes have the capacity to take care of their own feet.

12
3. RATIONALE OF RESARCH
In Ho Chi Minh City, type 2 diabetes has become more common and the disease is expanding
fast. Important determinants of the increased prevalence of the disease are industrialization,
development with sedentary lifestyles and shift of dietary habits with much carbohydrate
(Duc Son et al., 2004). Foot ulcers are complications due to diabetes, and foot-care is an
important prevention measure that should be concurrently started with the settling of the
diabetes diagnoses (Almås, 2001). High level of education increased the degree of self-care
and understanding of their diabetes diagnosis which makes it important to inform the patients
with diabetes (Tham et al., 2004). To prevent foot ulcers among type 2 diabetes patients in Ho
Chi Minh City, it is important to find out what their knowledge is and practice of foot care
and investigate if there are some differences between the genders regarding knowledge and
practice in foot care. The results of this study will provide more information in order to
develop an appropriate intervention program concerning foot care.
4. AIM
The purpose of this study was to investigate the knowledge and practices regarding foot-care
among patients with type 2 diabetes in Ho Chi Minh City, Vietnam.
5. RESEARCH QUESTIONS
1. What knowledge about foot care do the patients with Type 2 diabetes have?
2. How have they practiced their foot care?
3. Is there any difference between the genders regarding knowledge about foot care and its
practice?

13
6. METHOD
6.1 Design
The study was a descriptive and comparative cross-sectional design. This method was chosen
because it is time-effective and provides a lot of data (Eliasson, 2006).
6.2 Setting
The data for the project was collected at the outpatient department at the University Medical
Center, in Ho Chi Minh City, Vietnam. Ho Chi Minh City is set in the south part of Vietnam
and is the largest city in the country. The data was collected during one week in November,
2013. In one day around 150 – 180 patients are visit the outpatient department, 80 % (120 –
140 patients) of them had the diagnose type 2 diabetes. The most common reason for the type
2 diabetes patients to visit the outpatient clinic was to check up their diabetes.
6.3 Sample
A purposive sample was used for selecting the participants. The outpatients who could
participate in the study were the ones that met the inclusion criteria at the diabetic out-patient
clinic during the data collection period. 100 patients were asked to participant in this study
and all of them participated.
The inclusion criteria to participate were:
1. Patients with type 2 diabetes, both male and female, with an age over 18 years
2. They are able to write and read or can be helped to fill in the questionnaire
3. They are living in Ho Chi Minh City in Vietnam
4. They should not have any mental disease or dementia
5. They are willing to participate
14
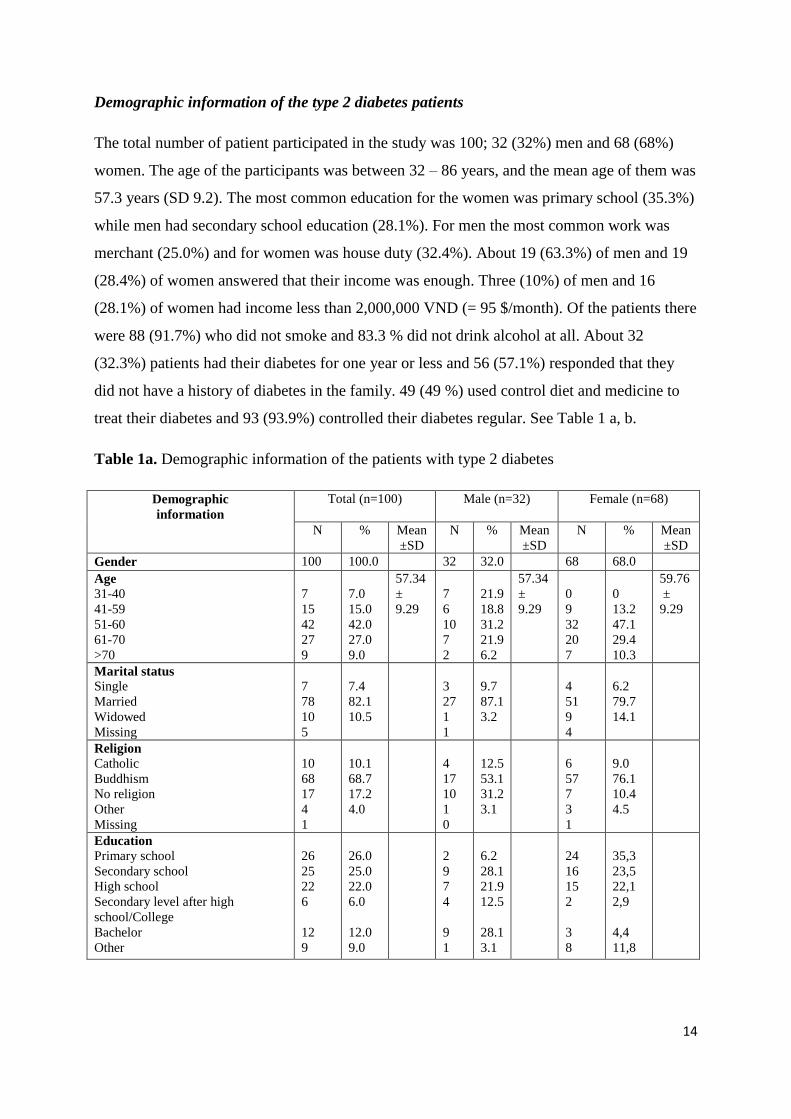
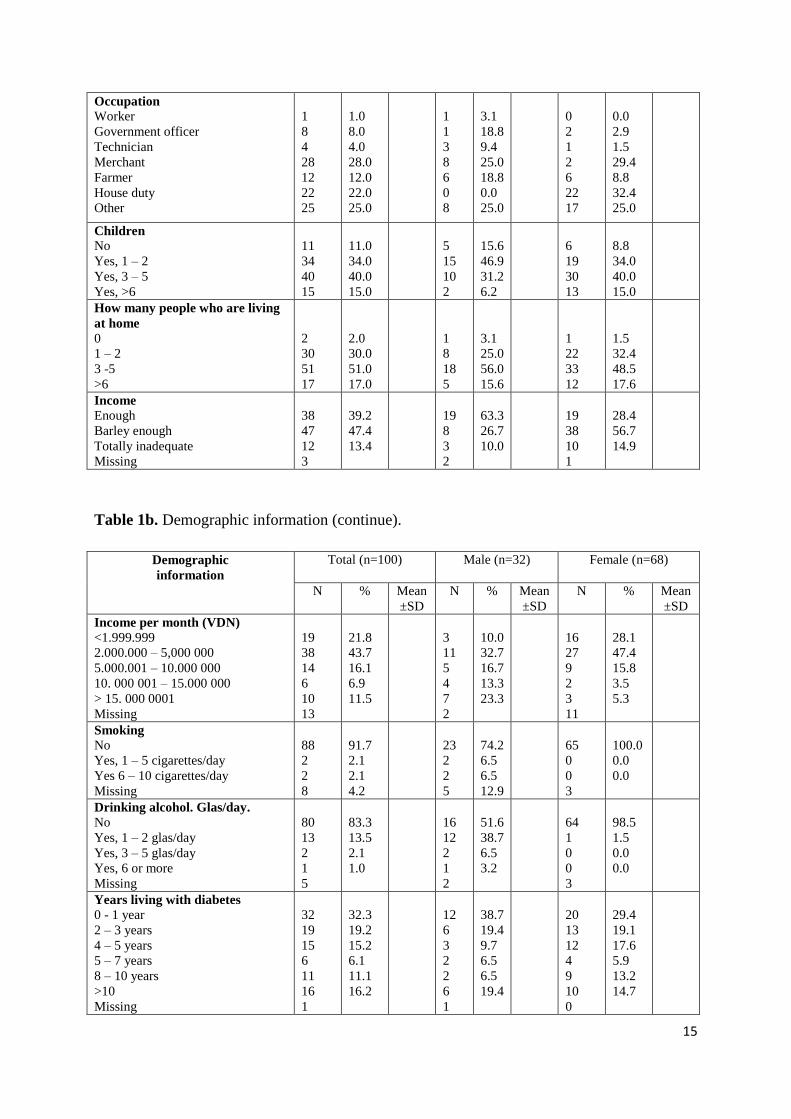
Demographic information of the type 2 diabetes patients
The total number of patient participated in the study was 100; 32 (32%) men and 68 (68%)
women. The age of the participants was between 32 – 86 years, and the mean age of them was
57.3 years (SD 9.2). The most common education for the women was primary school (35.3%)
while men had secondary school education (28.1%). For men the most common work was
merchant (25.0%) and for women was house duty (32.4%). About 19 (63.3%) of men and 19
(28.4%) of women answered that their income was enough. Three (10%) of men and 16
(28.1%) of women had income less than 2,000,000 VND (= 95 $/month). Of the patients there
were 88 (91.7%) who did not smoke and 83.3 % did not drink alcohol at all. About 32
(32.3%) patients had their diabetes for one year or less and 56 (57.1%) responded that they
did not have a history of diabetes in the family. 49 (49 %) used control diet and medicine to
treat their diabetes and 93 (93.9%) controlled their diabetes regular. See Table 1 a, b.
Table 1a. Demographic information of the patients with type 2 diabetes
Demographic
information
Total (n=100) Male (n=32) Female (n=68)
N % Mean
±SD
N % Mean
±SD
N % Mean
±SD
Gender 100 100.0 32 32.0 68 68.0
Age
31-40
41-59
51-60
61-70
>70
7
15
42
27
9
7.0
15.0
42.0
27.0
9.0
57.34
±
9.29
7
6
10
7
2
21.9
18.8
31.2
21.9
6.2
57.34
±
9.29
0
9
32
20
7
0
13.2
47.1
29.4
10.3
59.76
±
9.29
Marital status
Single
Married
Widowed
Missing
7
78
10
5
7.4
82.1
10.5
3
27
1
1
9.7
87.1
3.2
4
51
9
4
6.2
79.7
14.1
Religion
Catholic
Buddhism
No religion
Other
Missing
10
68
17
4
1
10.1
68.7
17.2
4.0
4
17
10
1
0
12.5
53.1
31.2
3.1
6
57
7
3
1
9.0
76.1
10.4
4.5
Education
Primary school
Secondary school
High school
Secondary level after high
school/College
Bachelor
Other
26
25
22
6
12
9
26.0
25.0
22.0
6.0
12.0
9.0
2
9
7
4
9
1
6.2
28.1
21.9
12.5
28.1
3.1
24
16
15
2
3
8
35,3
23,5
22,1
2,9
4,4
11,8
15
Occupation
Worker
Government officer
Technician
Merchant
Farmer
House duty
Other
1
8
4
28
12
22
25
1.0
8.0
4.0
28.0
12.0
22.0
25.0
1
1
3
8
6
0
8
3.1
18.8
9.4
25.0
18.8
0.0
25.0
0
2
1
2
6
22
17
0.0
2.9
1.5
29.4
8.8
32.4
25.0
Children
No
Yes, 1 – 2
Yes, 3 – 5
Yes, >6
11
34
40
15
11.0
34.0
40.0
15.0
5
15
10
2
15.6
46.9
31.2
6.2
6
19
30
13
8.8
34.0
40.0
15.0
How many people who are living
at home
0
1 – 2
3 -5
>6
2
30
51
17
2.0
30.0
51.0
17.0
1
8
18
5
3.1
25.0
56.0
15.6
1
22
33
12
1.5
32.4
48.5
17.6
Income
Enough
Barley enough
Totally inadequate
Missing
38
47
12
3
39.2
47.4
13.4
19
8
3
2
63.3
26.7
10.0
19
38
10
1
28.4
56.7
14.9
Table 1b. Demographic information (continue).
Demographic
information
Total (n=100) Male (n=32) Female (n=68)
N % Mean
±SD
N % Mean
±SD
N % Mean
±SD
Income per month (VDN)
<1.999.999
2.000.000 – 5,000 000
5.000.001 – 10.000 000
10. 000 001 – 15.000 000
> 15. 000 0001
Missing
19
38
14
6
10
13
21.8
43.7
16.1
6.9
11.5
3
11
5
4
7
2
10.0
32.7
16.7
13.3
23.3
16
27
9
2
3
11
28.1
47.4
15.8
3.5
5.3
Smoking
No
Yes, 1 – 5 cigarettes/day
Yes 6 – 10 cigarettes/day
Missing
88
2
2
8
91.7
2.1
2.1
4.2
23
2
2
5
74.2
6.5
6.5
12.9
65
0
0
3
100.0
0.0
0.0
Drinking alcohol. Glas/day.
No
Yes, 1 – 2 glas/day
Yes, 3 – 5 glas/day
Yes, 6 or more
Missing
80
13
2
1
5
83.3
13.5
2.1
1.0
16
12
2
1
2
51.6
38.7
6.5
3.2
64
1
0
0
3
98.5
1.5
0.0
0.0
Years living with diabetes
0 - 1 year
2 – 3 years
4 – 5 years
5 – 7 years
8 – 10 years
>10
Missing
32
19
15
6
11
16
1
32.3
19.2
15.2
6.1
11.1
16.2
12
6
3
2
2
6
1
38.7
19.4
9.7
6.5
6.5
19.4
20
13
12
4
9
10
0
29.4
19.1
17.6
5.9
13.2
14.7

16
Family History with diabetes
No
Yes
Missing
56
42
2
57.1
42.9
17
15
0
53.1
46.9
39
27
2
59.1
40.9
Treatment of diabetes
Control diet
Take medicine
Inject insulin
Other
Control diet and medicine
Take medicine and inject insulin
Control diabetes and inject insulin
Control diabetes, take medicine and
inject insulin
2
24
2
1
49
9
2
11
2.0
24.0
2.0
1.0
49.0
9.0
2.0
11.0
0
11
0
1
13
4
0
3
0.0
34.4
0.0
3,6
40.6
12.5
0.0
9.4
2
13
2
0
36
5
2
8
2.9
19.1
2.9
0.0
52.9
7.4
2.9
11.8
Regular follow up diabetes
treatment
No
Yes
Missing
6
93
1
6.1
93.9
3
29
0
9.4
90.6
3
64
1
4.5
95.5
Help with diabetes at home
Wife/husband
Children
My relative
No one
Wife/husband and children
Other
15
11
3
60
4
7
15.0
11.0
3.0
60.0
4.0
7.0
5
2
2
18
3
2
15.6
6.2
6.2
56.2
6.2
9.4
10
9
1
42
4
2
14.7
13.2
1.5
61.8
5.9
2.9
6.4 Data Collection Method
A questionnaire in English has been developed by Dr. Pranee Lundberg, Associate Professor,
at the Department of Public Health and Caring Sciences, Uppsala University and Ms Nguyen
Thi Phuong Lan, Nursing Lecturer, at the Department of Nursing, University of Medicine and
Pharmacy in Ho Chi Minh City (Appendix 1). The questionnaire was based on literature
(Bijoy et al., 2012; Pollock et al., 2004) and also adjusted to Vietnamese culture. The
questionnaire was translated to Vietnamese and then it was translated back and forth for face
validity of the questionnaire. The questionnaire was pilot tested by our co- supervisor Nguyen
Thi Phuong Lan in Ho Chi Ming City, before data collection.
The questionnaire consists of 46 questions which are divided into three parts: (1) Background,
(2) Knowledge of foot care and (3) Foot care practice including foot care education. The first
part in the questionnaire is divided into A, B and C part. The A part is about the participants’
demographic background such as age, gender, education, family, smoke and alcohol habits.
The B part is about the participant´s foot problem history and C part is questions about foot
and leg problem. The second part is about knowledge of foot care. Finally, the last part is
about how to practice foot care including foot care education.

17
6.5 Procedure
The project was the collaboration between the Department of Public Health and Caring
Sciences, Uppsala University, Sweden and the University of Medicine and Pharmacy in Ho
Chi Minh City, Vietnam, by Linnaeus-Palme Exchange Programme.
Our Co- supervisor, Nguyen Thi Phuong Lan, contacted the Director of the Medical Centre
for permission to carry out the study. The nurses at the clinic were informed about the study
and helped us to give information to the patients with type 2 Diabetes. The participants were
informed about the study and their rights to participate. The co-supervisor together with the
authors gave both oral and written information to the outpatients at the diabetes clinic about
the study and their right for participation. The patients who were interested to participate
received a questionnaire to answer during the waiting time at the clinic. The patients gave it
back after finishing. If some patients had problem to fill in the questionnaire or had questions
during answering the questionnaire, Ms. Nguyen Thi Phuong Lan and a few Vietnamese
lecturers helped the participants to fill in the questionnaire. It took around 15 – 20 minutes to
answer the questionnaire.
6.6 Data analysis
Analysis of data from the questionnaire was done using the statistic program, SPSS (The
Statistical Package of Social Science).
The answers about demographic information in Part I, A (questions 1 – 17) was coded into
numbers and then registered in the SPSS-program using descriptive statistic.
The B and C part (Questions 18 – 23) in Part one were based on a nominal scale and we used
numbers and percent to investigate the participant’s history of foot problems and current foot
problems.
To analyze research question 1, “What knowledge about foot care do the patients with Type 2
diabetes have?”, we analyzed the answers in part two about Knowledge (Question 25) with
numbers and percent. In part II the participant could answer true or false of 15 questions. The
“True” answer of all questions is the right answer. Fifteen questions were regarding
knowledge about foot care. Each correct answer was given one mark. Good knowledge: If

18
score is more than 70% (11-15), Satisfactory knowledge: If score is 50-70% (10-8), and Poor
knowledge: Scores less than 50% (<8)(Bijoy et al., 2012).
To analyze the research question 2, “How have they practiced their foot care?”, we analyzed
the answers in part III about practice (Questions 26 – 46) with numbers and percent.
To answer research question three, “Is there any difference between the genders regarding
knowledge about foot care and its practice?”, we analyzed the answer in part two about
knowledge (Question 25) and the answers in part three about practice (Questions 26 – 46) by
using Chi squared test.
The significant difference between men and women has a determined p-value ≤0.05. The
results were presented by using tables and text.
7. ETHICAL CONSIDERATIONS
The study has got approval from the ethical committee at the University of Medicine and
Pharmacy in Ho Chi Minh City. The participants were informed about the study and their
rights before they participated in the study. It was anonymous and voluntarily to participate
and the data was analyzed confidently. The participants could drop out any time without any
consequences. The International Council of nurses (ICN) code of ethics for nurses (2012) was
used in this study for ethical considerations concerning respect for customs, values and beliefs
for the individual, family and community and respect for the human rights. During the data
collection it was important to let the participant fill in the questionnaire in seclusion, because
the questionnaire could have some private questions.
19
8. RESULTS
8.2 History of foot problems
About 85 (85%) of the participants answered that they never have had a foot ulcer and 87
(87.9%) have never had a sore or cut on the leg or foot that took more than two weeks to heal.
Only one (1%) answered that they had amputated a leg or foot.
8.3 Current foot or leg problems
About 96 (96%) of the patients reported that they did not have an ulcer, sore or blister on the
feet at this moment. 58 (58%) answered that they had numbness, tingling, pins, needles or
itching on their feet.
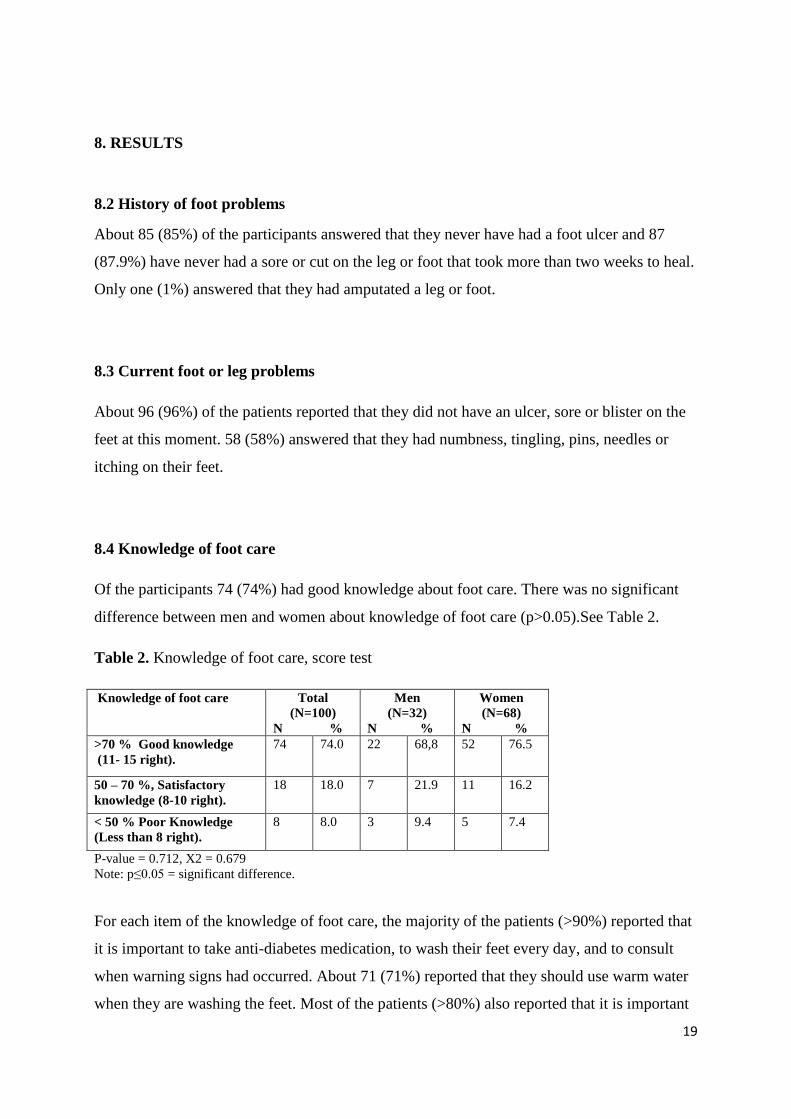
8.4 Knowledge of foot care
Of the participants 74 (74%) had good knowledge about foot care. There was no significant
difference between men and women about knowledge of foot care (p>0.05).See Table 2.
Table 2. Knowledge of foot care, score test
Knowledge of foot care Total
(N=100)
N %
Men
(N=32)
N %
Women
(N=68)
N % >70 % Good knowledge
(11- 15 right). 74 74.0 22 68,8 52 76.5
50 – 70 %, Satisfactory
knowledge (8-10 right).
18 18.0 7 21.9 11 16.2
< 50 % Poor Knowledge
(Less than 8 right).
8 8.0 3 9.4 5 7.4
P-value = 0.712, X2 = 0.679
Note: p≤0.05 = significant difference.
For each item of the knowledge of foot care, the majority of the patients (>90%) reported that
it is important to take anti-diabetes medication, to wash their feet every day, and to consult
when warning signs had occurred. About 71 (71%) reported that they should use warm water
when they are washing the feet. Most of the patients (>80%) also reported that it is important

20
to dry the feet, to keep the skin soft to prevent dryness, and to inspect the feet´s every day.
Half of the patients reported that they should not apply lotion in the interdigital spaces. There
were no significance differences between genders concerning the items of knowledge of foot
care. See Table 3.
Table 3.Knowledge of foot care among the patients with type 2 diabetes.
Knowledge of foot care Total (n=100) Male (n=32) Female (n=68) X2 p-value
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
Importance of taking anti-
diabetes treatment to
prevent complication
5
(5.0)
95
(95.0)
2
(6.2)
30
(93.8)
2
(6.2)
65
(95.6)
0.155 0.694
Daily washing the feet 4
(4.0)
96
(96.0)
2
(6.2)
30
(93.8)
2
(2.9)
66
(97.1)
0.620 0.431
Using warm water for
washing/bathing
29
(30.0)
71
(70.0)
12
(37.5)
20
(62.5)
17
(25.0)
51
(75.0)
0.651 0.199
Checking temperature of
water before using
37
(37.0)
63
(63.0)
13
(40.6)
19
(59.4)
24
(35,3)
44
(64,7)
1.625
0.607
Drying the feet after
washing
15
(15.0)
85
(85.0)
6
(18.8)
26
(81.2)
9
(13.2)
59
(86.8)
0.519
0.471
Talcum powder usage for
keeping interdigital spaces
dry
54
(54.0)
46
(46.0)
21
(65.6)
11
(34.4)
33
(48.5)
35
(51.5)
2.560
0.110
Keeping skin of the feet
soft to prevent dryness
16
(84.0)
84
(84.0)
5
(16.0)
27
(84.0)
11
(16.2)
57
(83.8)
0.005 0.944
Lotion not to be applied to
the interdigital spaces
50
(50.0)
50
(50.0)
15
(46.9)
17
(53.1)
35
(51.5)
33
(48.5)
0.184) 0.668)
Daily changes of socks 26
26.0)
74
(74.0)
10
(31.2)
22
(68.8)
16
(23.5)
52
(76.5)
0.674 0.412
Trimming nails of feet
straight with care
9
(9.0)
91
(91.0)
5
(14.6)
27
(84.4)
4
(9.0)
64
(91.0)
2.522 0.112
Inspection of feet once a
day by yourself
17
(17.0)
83
(83.0)
4
(14.6)
27
(84.4)
44
(17.6)
56
(82.4)
0.063 0.802
Wearing comfortable coat
shoes
9
(9.0)
91
(91.0)
1
(3.1)
31
(96.9)
2
(2,9)
66
(97.1)
0.003 0.960
Checking the shoes from
inside before wearing
15
(15.0)
85
(85.0)
5
(15.6)
27
(84.4)
10
(14.7)
58
(85.3)
0.014 0.901
Not walking bare foot 13
(13.0)
87
(87.0)
2
(6.2)
30
(93.8)
11
(16.2)
57
(83.8)
1.896 0.169
Warning signs for which
consultation is required
5
(5.0)
95
(95.0)
3
(9.4)
29
(90.6)
2
(2.9)
66
(97.1)
1.896 0.168
Note: p≤0.05 = significant difference.
8.5 Practice of foot care
There was a significant difference between men and women concerning the use of hot water
or heating pads on their feet (p=0.002).10 (14.7%) women used it on their feet and no men
reported that they did it. Of the participants 90 (90%) reported that they examine their feet and
72 (72.0 %) of them thought that they take care of their feet in a correct way. There were only
9.1 % who used moisturizing cream on their feet. There was 23(43.8%) of women and 5

21
(15.6%) of men who thought that they did not take care of their feet in correct way, but there
was no significant difference between genders. See Table 4.

22
Table 4. Foot care practices among patients with type 2 diabetes.
Foot care practices Total (n=100) Male (n=32) Female (n=68) X2 p-value
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
I can reach and see the
bottoms of my feet
(M=1 woman)
8
(8.1)
91
(91.9)
3
(9.4)
29
(90.6)
5
(5.4)
62
(61.6)
0.107 0.744
I examine my feet?
(M=0)
10
(10.0)
90
(90.0)
3
(9.4)
29
(90.6)
7
(10,3)
61
(89.7)
2.114 0.715
I wash my feet every day
(M=0)
6
(6.0)
94
(94.0)
2
(6.2)
30
(93.8)
4
(5.9)
64
(94.1)
0.005 0.942
Dry my toes
(M= 0)
35
(35.0)
65
(65.0)
12
(37.5)
20
(62.5)
23
(33.8)
33.8
(66.2)
0.129 0.719
I use a moisturizing cream
on my feet
(M=1 man)
90
(90.9)
9
(9.1)
29
(93.5)
2
(6.5)
61
(89.7)
7
(10.3)
0.380 0.537
I cut my own toenails
(M=0)
48
(48.0)
52
(52.0)
18
(56.2)
14
(43.8)
30
(44.1)
38
(55.9)
5.816 0.121
I ever soak my feet
M=1 woman)
78
(78.8)
21
(21.2)
27
(84.4)
5
(15.6)
51
(67.1)
16
(32,9)
0.883 0.347
I always test water
temperature before my
foot in
(M=1 woman)
78
(78.8)
20
(20,2)
27
(87.1)
4
(12.9)
52
(76.5)
16
(23.4)
1.491 0.222
I use medicated products
for warts, corns or calluses
M=0)
93
(93.0)
7
(7.0)
31
(96.9)
1
(3.1)
62
(91.2)
6
(8.8)
1.085 0.297
I put moisturizing creams
or lotions between my toes
(M=1 men)
92
(92.9)
7
(7.1)
29
(93.5)
2
(6.5)
63
(92.6)
5
(7.2)
0.026 0.871
I ever walk around in my
bare feet
(M=1 women)
69
(63.6)
36
(36.4)
21
(65.6)
11
(34.4)
42
(62.7)
25
(37.3)
0.081 0.776
I ever wear shoes without
wearing any socks
M=0)
67
(67.0)
33
(33.0)
20
(62.5)
12
(37.5)
47
(69.1)
21
(30.9)
0.431 0.511
I use a hot water bottle or
heating pad on my feet
(M=0)
90
(90.0)
10
(10.0)
32
(100.0)
0
(0.0)
58
(85.3)
10
(14.7)
5.229 0.002*
I sit with my leg crossed
(M=0)
31
(31.0)
69
(69.0)
9
(28.)
23
(71.9)
22
(32.4)
46
(67.6)
0.182 0.670
I think I have taken care
my feet in correct way
(M=0)
28
(28.0)
72
(72.0)
5
(15.6)
27
(84.4)
23
(43.8)
45
(66.2)
3.575 0.059
Note: p≤0.05 = significant difference., M= Missing, * = significant difference
92 (92%) of the participants used sandals and 37 (37, 0%) used cotton socks. There was a
significant difference between men and women concerning the use of shoes with round toes
(p=0.002). Nine (28.1%) men who used round toes shoes, but only three (4.4%) of the
women. There was also a significant difference between genders in using shoes of leather or
canvas (p=0.000). 11 (34.4%) of the men and two (2.9) women used leather or canvas shoes.
See Table 5.
Table 5.Types of shoes and socks which the patients with type 2 diabetes wear.

23
Types of shoes Total (n=100) Male (n=32) Female (n=68) X2 p-value
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
Pointed toes 90
(95.0)
5
(5.0)
29
(90.6)
3
(9.4)
66
(95.0)
2
(5.0)
1.896 0.168
Broad, round toes 88
(88.0)
12
(12.0)
23
(71.9)
9
(28.1)
65
(95.6)
3
(4.4)
11.587 0.001*
High heels 100
(100.0)
0
(0.0)
32
(100.0)
0
(0.0)
68
(100.0)
0
(0.0)
Sandals 8
(8.0)
92
(92.0)
2
(6.2)
30
(93.8)
6
(8.8)
62
(91.2)
0,196 0.658
Flip flops/thongs 12
(12.0)
88
(88.0)
6
(18.8)
26
(81.2)
6
(8.8)
62
(91.2)
2.030 0.154
Athletic/sneakers/runners 94
(94.0)
6
(6.0)
28
(87.5)
4
(12.5)
66
(97.1)
2
(2.9)
3.525 0.060
Shoes made of leather or
canvas
87
(87.0)
13
(13.0)
21
(65.6)
11
(34.4)
66
(97.1)
2
(2.9)
19.010 0.000*
Types of socks Total (n=100) Male (n=32) Female (n=68) X2 p-value
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
Cotton 63
(63.0)
37
(37.0)
17
(53.1)
15
(46.9)
46
(67.6)
22
(32.0)
1.969 0.161
Wool 99
(99.0)
1
(1.0)
32
(100.0)
0
(0.0)
67
(98.5)
1
(1.5)
0.475 0.491
Acrylic/synthetic 93
(93.0)
7
(7.0)
32
(100.0)
0
(0.0)
61
(87.7)
7
(10.3)
3.452 0.060
Knee highs 100
(100.0)
0
(0.0)
32
(100.0)
0
(0.0)
68
(100.0)
0
(0.0)
Prescription/compression 97
(97.0)
3
(3.0)
32
(100.0)
0
(0.0)
65
(95.6)
3
(3.0)
1.455 0.228
Not know 94
(94.0)
6
(6.0)
29
(90.6)
3
(9.4)
65
(95.6)
3
(4.4)
0.950 0.330
Others 54
(54.0)
46
(46.0)
18
(56.2)
14
(43.8)
36
(52.9)
32
(47.1)
0.096 0.757
Note: p≤0.05 = significant difference, * = significant difference.
8.6 Foot care education
For foot care education the majority of the patients reported that they had not attended a class
in foot care (93%) and that they had not read handouts about diabetes (83%). They (85%) also
reported that they would like to get handouts with information of foot care. There was no
significant difference between genders regarding foot care education. See Table 6.

24
Table 6. Foot care education among patients with type 2 diabetes.
Foot care education Total (n=100) Male (n=32) Female (n=68) X2 p-value
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
I have ever attended a
class on how to care for
my feet
93
(93)
7
(7)
30
(93.8)
2
(6.2)
63
(92.6)
4
(7.4)
0.041 0.840
I have ever read handouts
on foot care
80
(80)
20
(20)
24
(75)
8
(25)
56
(82.4)
12
(17.6)
0.735 0.391
I would like a handout on
how to care for my feet
15
(15)
85
(85)
6
(18.8)
26
(81.2)
9
(13.2)
59
(86.8)
0.519 0.471
Note: P≤0.05 = significant difference, * = significant difference.
Most patients 39 (39%) thought that media was the most effective way for increasing
knowledge and practice of foot care. There was no difference between genders concerning the
opinion about the most effective ways. See Table 7.
Table 7. The opinions of the patients about the most effective way for increasing knowledge
and practice of foot care.
Most effective ways for Total (n=100) Male (n=32) Female (n=68) X2 p-value
increasing knowledge and
practice
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
No
n (%)
Yes
n (%)
Receiving
handout/brochure
65
(65.0)
35
(35.0)
20
(62.5)
12
(37.5)
45
(66.2)
23
(33.8)
0.571 0.752
Health education in group 96
(96.0)
4
(4.0)
30
(93.8)
2
(6.2)
66
(97.1)
2
(2.9)
0.620 0.431
Individual health
education
78
(78.0)
22
(22.0)
24
(75.0)
8
(25.0)
54
(79.4)
14
(20.6)
0.247 0.619
Media such as TV, radio,
etc.
61
(61.0)
39
(39.0)
18
(56.2)
14
(43.8)
43
(62.2)
25
(36.8)
0.446 0.504
Others 93
(93.0)
7
(7.0)
29
(90.6)
3
(9.4)
64
(94.1)
4
(5.9)
0.408 0.523
Note: P≤0.05 = significant difference, * = significant difference.
9. DISCUSSION
Previous research shows that knowledge and practice is low in type 2 diabetes patients and
that women had better practice/self-care then the men. The results in this study showed that
the knowledge about foot care was high in the type 2 diabetes patients. There was 74.0 % who
had good knowledge and only 8.0 % had poor knowledge. There was no significant difference
between genders concerning knowledge. The result of foot care practice was more
varied and had some significant differences between men and women. The result of
knowledge was high but there is still lack in the practice of foot care.
25
9.1. Result discussion
9.1.1. Knowledge of foot care among the patients with type 2 diabetes
Of the type 2 diabetes patients who participated in the study 74.0 % had good knowledge in
foot care. This is a great number compared to several other studies where the type 2 diabetes
patients had poor knowledge in foot care (Pollock et al., 2004; Khamseh et al., 2007).
The patients who had received information or advice previously had better knowledge than
those who hadn´t got any information (Pollock et al., 2004). In this study the patients had
good knowledge even though the majority of the patients had not attended a class in foot care
or read handouts about diabetes. One possible reason for good knowledge about foot care can
be that the majority of patients mentioned that media was the best way for increasing
knowledge and practicing of foot care and maybe the patients can search information by
themselves through media. However, many of patients would like to have a handout about
foot care to improve their knowledge.
About 54% of the patients answered wrong concerning the use of talcum powder usage for
keeping interdigital spaces dry. Also 50.0 % answered that it was not right to apply lotion to
the interdigital spaces on the feet. This shows that half of the patients in this study still did not
know about correct foot care. Many patients had low education (primary school or secondary
school), and this can affect their understanding. Quinn et al. (2011) found that the patients
with low education need more information about their diagnosis, and also need to be educated
about diabetes (Tham et al. 2004).
9.1.2. Foot care practices among patients with type 2 diabetes.
The results of foot care practice among patients was varied and are in agreement with several
other studies (Pollock et al., 2004; Khamseh et al., 2007;Bhupendra et al., 2008) which
showed that the practice of foot care in type 2 diabetes is low.
In this study 90.0 % of the patients examined their feet. This is contrary to the results of
Pollock et al. (2004) that 83% of the patients failed to inspect their feet. It seems that patients
in this study have daily routines to inspect their feet and have searched for information in
practice of foot care.
26
It is important to test the water before washing the feet, but only 20.2 % reported that they did
so even if 60.0 % answered that they knew that. About 33.0 % reported that they walked
around barefoot while 87.0 % answered that it was not good to walk around barefoot. Only
9% used moisturizing cream on their feet and 69 % sit with their leg crossed even do it is not
good for the circulation (Brown and Edwards (2005). This can explain that the patients have
lack of motivation to change of their lifestyle and that health care professionals cannot
motivate, support and give feedback to the patients about self-care. Another reason may be
that the patient didn’t have relatives and friends to support for his/her foot care (Kneckt et al.,
2000). In addition, Rätsep, Oja, Kalda & Lember (2007) showed that economy can have an
important role of the lack in self-care.
The majority of the patients used sandals and flip-flops and only 13 % used shoes of leather.
Brown & Edwards (2005) recommend that the patient shall avoid open-toe and open-heel
shoes and use leather shoes. Contributing factors may be the hot weather in Vietnam which
makes it more convenient to us flip-flops and sandals than leather shoes. Leather shoes are
more expensive. Health care professionals should be aware of this when providing education
to the patients.
9.1.3. Difference between genders in knowledge and practice of foot care
In the study of Pollock et al. (2004) the women had higher knowledge about foot care than
men, and this is in contrast with the results of this study that there was no significant
difference between genders in knowledge of foot care. It may be due to that both male and
female have got good information about foot-care when they visited the doctors at the
hospital. Another reason can be that the participation group in this study is too small to show
differences between genders.
More women than men reported that they use hot water bottle or heating pad on their feet.
This makes it seem that women had low awareness of diabetes and complications as Rätsep et
al. (2007) found. It is important that knowledge of diabetes and practice of foot care should be
educated to patients (Tham et al. 2004) and they have more individual information about their
diagnosis (Quinn et al., 2011). To increase the practicing in correct way Pollock et al., (2004)
mean that there is a need to motivate health providers in educating the type 2 diabetes patients
about self-care and also let them practicing by themselves. Also countrywide network of

27
diabetes centers with implementation of primary prevention programs has to be developed to
prevent complications. It is important to increase the practicing of foot care in a correct way.
More men than women used shoes with round toes and leather/canvas shoes. The authors
believe that one possible reason may be that there were more men who worked as government
officers and merchants and they used this kind of shoes in their work.
Many of the type 2 diabetes patients had a low income and the women had generally lower
income than the men. Financing problems for the women can be a reason for the lack in their
practice of foot care (Rätsep et al., 2007). People in higher social classes have easier to adapt
and change their habits and lifestyle and that can be one reason for the difference between
genders (Chan et al., 2001). Another possible reason can be that the women had a lack of
motivation to change their life style (Rätsep et al., 2007).
More women participating in the study visited the clinic the days for data collection.
Goodridge et al. (2005) found that women was more active in their self-care and men
searched more health care for acute problems, and this can explain why there were more
women visiting the clinic these days.
9.2 Method discussion
Not much research is done about type 2 diabetes in Ho Chi Minh City, Vietnam, and more
research was needed. Therefore this quantitative study was used to investigate the knowledge
and practice in foot care among men and women with type 2 diabetes. The descriptive and
comparative cross- sectional design with questionnaires in suitable to use when the time is
limited and it can collect more data (Eliasson, 2006). Quantitative method was used because
of its strength of generalizability reliability and objectivity (Weinreich, 2006). A purposive
sample was used for this study. The sample method was chosen because of the small amount
of time.
The authors of this study verified the reliability of the data and the questionnaires were
reviewed twice by both the authors before it was entered in to SPSS. When the data was
entered into SPSS both of the authors checked the data two more times so the data were
entered correctly in order to be trustworthy and no data would be printed wrong. The
questionnaire was supposed to be answered in private and help could be supervised to the

28
patients who had a difficulty to fill in the questionnaire, but most of the patients needed help.
Many patients that thought the questionnaire was too long and complicated to fill in. Ms.
Nguyen Thi Phuong Lan interviewed them and filled in the answer for them. Therefore, it is
hard for the authors to know how the questions were read, if the patients answered truthfully,
and this may affect the results. The help to fill in the questionnaires could have harmed the
ethical considerations due to that the questioners have some sensitive questions, such as their
social status Due to the help the patients were given the reliability could have been decreased,
because the authors do not know if the data were trustworthy from the beginning. However,
the authors believe that the quantitative method was the most suitable method to answer the
research questions.
The validity of the questionnaires is high because it is based upon several studies (Bijoy et al.,
2012; Pollock et al., 2004) and a pilot study was done by Ms Nguyen Thi Phungon Lan. The
questionnaires was developed by the two supervisors (Appendix 1). The questionnaires were
also translated in to Vietnamese language by Ms Nguyen Thi Phuong Lan and were adjusted
to Vietnamese culture. A pilot test had also been done by the co- supervisor Nguyen Thi
Phuong Lan in Ho Chi Ming City, before the data collection.
The authors believe that the generalizability is low because of the small sample (100
questionnaires) and cannot be transferred to a larger group/population. The authors believe
that they could be objectivity to the result, even if they were interviewed, due to that they did
not be a big part of the data collection because of the language barrier. In the result there were
no missing data in the knowledge part. In the practices part there was four missing women
and two missing men. See table 4. The authors do not think that the missing data affect the
result. The reason for the missing could be that the patients might not understand the question
or that the questions did not have an answer that they agreed with.
9.3 Theoretical framework discussion
The patients in the study had good knowledge about foot care, but some did not practice their
foot care in a correct way. It means that they don’t have the capacity to perform their self-
care. Dorothea Orem means that the nurse should help the patient with practice of self-care

29
when they are affected of limitations and help them to give capacity to regain the self-care
(Kirkevold, 2000).
When the patients already have knowledge about foot care, it is important that the nurse
motivate the patients to practice their foot care (Rätsep et al., 2007). This agrees with
Dorothea Orem’s theory that nurses should guide and teach patient about self-care
management concerning foot care, give physical and psychological support, and empower
patient to increase his/her self-confidence so that patient can regain the capacity of self-care.
Orem also means that self-care depends on the health of the person, wellbeing, interest of
maintaining living and function and the age can affect the self-care (Alligood & Tomey,
2009).Type 2 diabetes often affects older people and many patients mentioned that economy
was an important role for their self-care. It is important that the nurse should be aware of this
when guiding and teaching patients.
9.4 Clinical implication
The results of this study can be used to increase understanding among health care
professionals to develop an intervention program of self-care management for type 2 diabetes
patients to provide knowledge and practice of foot care in Vietnam. This can be applied to
other developing countries. The study also provides an opportunity for information and
feedback to the nurses, doctors and other health professionals, all to improve the self- care of
type 2 diabetes foot care and prevent complications. Sweden is a multicultural society, the
results of this study can also be used to increase awareness of health care professionals when
provide health education to patients from different cultures.
9.5 Further research study
The aim of this study was to investigate what knowledge the patients had about foot care, how
they practice their foot care and if there was some gender differences. In further research it
would be interesting to investigate more about why patients with type 2 diabetes do not
practice their foot care and from where they were given the information about their
knowledge. It would also be interesting to investigate a correlation between the patients’
income and their foot care practice.

30
9.6 Acknowledgement
We would like to thank Swedish Council for Higher Education through its exchange
programme Linnaeus-Palme that made this study possible. We specially want to thank our
supervisor Dr. Pranee Lundberg, Associate Professor at the Department of Public Health. We
also want to thank our co-supervisor Ms Nguyen Thi Phuong Lan, Nursing Lecturer, at the
Department of Nursing, University of Medicine and to Pharmacy in Ho Chi Minh City, for all
help to hand out the questionnaires. Without her it would not been possible to write and
implement this study. We also thank to all patients who participated voluntarily in this study.
9.7 Conclusions
The knowledge of foot care was good, but the practice of foot care was poor among patients
with type 2 diabetes in this study. More information about the importance of foot care practice
is needed to prevent complications from type 2 diabetes in Ho Chi Minh City, Vietnam. The
poor foot care practice can not only be explained by poor information, and low income of the
patients. There was no significant difference between genders in knowledge but there were
some differences between genders concerning foot care practices. It is important to give
individual information to the patients and follow up their self-care of foot care.

31
10. REFERENCES
Alligood, M & Tomey,A (2009) Nursing Theorists and their work, Dorothe E. Orem: self-
care deicit theory of nursing (pp 265-285) Mosby Elsevier
American College of Foot and ankle surgeons. (2009). Foot health facts -healthy feet for an
active life. Collected 2010-03-13, from American College of Foot and ankle surgeons,
http://www.foothealthfacts.org/footankleinfo/diabetic-guidelines.htm
Bijoy, C.V., Feba, B., Vilkas, R.C., Dhaandapani, C., Geetha, K., & Vikayakumar, A. (2012).
Knowledge assessment and patient counseling on diabetic foot care. Indian Journal of
Pharmacy Practice 5(2), 11-15.
Bhupendra, R. M., Anand, P.T., Sangram S.K., Dilip, O.G., Ravinder, R.N. (2008).
Evaluation of foot problems among diabetes in rural population. Indian J. Surg. 70: 175 - 180.
Chan, J.C.N., Ng, M.C.Y., Critchley, J.A.J.H., Lee, S. –C. & Cockram, C.S. (2001). Diabetes
mellitus-a special medical challenge from a Chinese perspective. Diabetes Research and
Clinical practice 54 – supplement 1, 19-27.
Duc Son, L. E. N. T., Kusama, K., Hungt, N. T. K., Loant, T. T. H., Van Chuyen, N., Kunii.
(2004). Prevalence and risk factors for diabetes in Ho Chi Minh City, Vietnam.Diabetic
Medicine, 21, 371-376.
Eliasson, A. (2006). Kvantitativ metod från början. Studentlitteratur: Lund
Fass. (2011). Diabetes typ 2.Collected 2013 - 09 - 30 from
http://www.fass.se/LIF/illness/ViewIllness.action?documentId=d226df85-ba7f-409d-9a32-
b69c9781f9c8&docType=95&docTitle=Sjukdomar+%26amp%3B+besv%26auml%3Br
Fuller, T. (2013, June 4) Diabetes Is the Price Vietnam Pays for Progress. New Yorkers
Times. p 15.
32
Goodridge, D., Trepman, E., Embil, J.M., (2005). Health – related quality of life in diabetic
patients with foot ulcers. The Wound, Ostomy and Continence Nurses Society, 42(1) 368 –
376.
Hallbjorg, A. (2001). Klinisk omvårdnad del 2, 39.Omvårdnad vid förändringar i
bukspottkörtelns endokrina funktion. Stockholm: Liber.
Heart. (2012) Symptoms, Diagnosis & Monitoring of Diabetes. Collected 3 Ocktober 2013,
fromhttp://www.heart.org/HEARTORG/Conditions/Diabetes/SymptomsDiagnosisMonitoring
ofDiabetes/Symptoms-Diagnosis-Monitoring-of-Diabetes_UCM_002035_Article.jsp
Helman, C. (2001).Health beliefs about diabetes: patients versus doctors. West J Med
2001;175:312-313
Insulin. (2011). Förekomst. Collected 13 June 2013, from
http://www.insulin.se/Startsida_insulin/Typ-2-diabetes/Forekomst/
International Council of Nurses. (2012). The ICN Code of Ethics for Nurses. Geneva:
International Council of Nurses. 28 may 2013 from http://www.icn.ch/about-icn/code-of-
ethics-for-nurses/
Kafaie P., Rashidi., M,.Sedigheh Soheilikhah N., Taghi M,.(2012)
Evaluation of Patients' Education on Foot Self-Care Status in Diabetic Patient
Iranian Red Crescent medical journal. 829-32.
Khamseh, M.E., Vatankhah, N., Baradaran, H.R. (2007). Knowledge and practice of footcare
in Irainan people with type 2 diabetes, Int wound Journal. 4, 298 - 302.
Kavanagh, A., Bentley, R.J., Turrell, G., Jonathan, Shawc, J.,, Dunstan,.D.,
Kirkevold, M. (2000). Omvårdnadsteorier: Analys och utvärdering. Lund: Studentlitteratur.
Kneckt, M.C., Syrjälä, A-M. H. & Knuuttila, M.L.E. (2000). Attributions to dental and
diabetes health outcomes. Journal of Clinical Periodontology 27 (3), 205-211.

33
Marques, M.B., Silva, M.J., Coutinho J.F.V. & Lopes, M.V.O. (2003). Assessment of self-
care competence of elderly people with diabetes. Rev Esc Enferm USP 47(2), 409-14.
Mc Naughton, D. (2013). “Diabesity” down under overweigt and obesity as cultural signifies
for type 2 diabetes mellitus. Critical public health 23(3), 274 - 288.
Maruthur, N. M. (2013). The Growing Prevalence of Type 2 Diabetes: IncreasedIncidence or
Improved Survival? Curr Diab Rep. Published online 27 September 2013.
Migrationsverket, 2013. Statistik. 29 may 2013, from http://www.migrationsverket.se/
Mull, D.S., Nguyen, N., Mull, D. (2001) Vietnamese diabetic patients and their physicians.
West journal medicine 175(5), 307 - 311.
Pollock, R.D., Unwin, N.C., & Connolly, V. (2004). Knowledge and practice of foot care in
people with diabetes. Diabetes Research Clinical Practice 64, 117-122.
Quinn, C., Royak-Schaler, R., Lender, D., Steinle, N., Gadalla, S. & Zhan., M. (2011). Patient
Understanding of Diabetes Self-Management: Participatory Decision-Making in Diabetes
Care.J Diabetes Sci Technol, 5(3), 723–730.
Ramachandran, A., Snehalatha, C., Samith Shetty, A. & Nanditha, A. (2012). Trends in
prevalence of diabetes in Asian countries. World journal of Diabetes. 15; 3(6), 110-117.

34
Rätep, A., Oja, I., Kalda, R. & Lember, M. (2007). Faily doctors´s asessment of patient and
health care system-related factors constributing to non-adherence to diabetes mellitus
guidelines. Primary Care Diabetes 1(2): 93-97.
Subramanian, S.V. (2010). Socioeconomic position, gender, health behaviors and biomarkers
of cardiovascular disease and diabetes. Social Science & Medicine, 71. 1150-1160.
Tham, K.Y., Ong, J.J.Y., Tan, D.K.L. & How, K.Y. (2004). How much do Diabetic Patients
Know About Diabetes Mellitus and its Complications? Annals Academy of Medicine, 33(4),
503-509.
Tomisaka, K., Lako, J., Maruyama, C., Anh,N., Lien, D., Khoi, H.H., Van Chuyen, N (2002).
Dietary patterns and risk factors for Type 2 diabetes mellitus in Fijian, Japanese and
Vietnamese populations. Aisa Pacific Journal, 11(1), 8-12.
Weinreich, N.K. (1996). A more perfect union: Integrating quantitative and qualitative
methods in social marketing research. Social marketing Quarterly, 3(1), 53-58.
WHO. (2013). Diabetes. WHO Media centre: 15 mars 2013, from
http://www.who.int/mediacentre/factsheets/fs312/en/
WHO, Western pacific region. (2012). Vietnam. WHO Media centre: 15 September 2013,
from http://www.wpro.who.int/vietnam/mediacentre/features/feature_world_diabetes_day
2012_vietnam/en/index.html

35
Appendix 1 Questionnaire
Knowledge and practice of foot care in Vietnamese people with
Type 2 diabetes
Please mark (X) your answer for every question.
Part I: BACKGROUND
A. Demographic information
1. Gender 1. Man 2. Woman
2. Age __________ years
3. Marital status
1. Single 2. Married
3. Separated 4. Divorced
5. Widowed 6. Other, _____________________
4. What is your religion?
1. Catholic 2. Protestant
3. Buddhism 4 . Muslim
5. No religion 4 . Other (Specify)…………………
5. Education
1. Primary school 2. Secondary school
3. High school 4. Secondary level after high school/College 5.
Bachelor 6.Other, _____________________
6. Occupation
1.Worker 2.Government officer
3.Technician 4.Merchant
5.Farmer 7.House duty
8. Other, ______________________

36
7. Do you have children?
1. No 2. Yes
8. How many people do you live with at home? _____________
9. How adequate is your income to meet your daily living expenses?
1. Enough 2.Barely enough 3.Totally inadequate
10. How much income do you have per month? _______________________ VDN
11. Do you smoke? 1. No 2. Yes, how many cigarette/day? _______
12. Do you drink alcohol? 1. No 2. Yes, how much do you drink per day? _______
13. For how long have you been living with Diabetes? __________________
14. Does your family have any history of Diabetes?
1. No 2. Yes
15. What kinds of diabetes treatment do you use? (you can mark more than one)
1. Control diet 2. Take medicine
3. Inject insulin 4. Other (specify) ______________
16. Do you follow up regularly your diabetes treatment with the doctor?
1. No 2. Yes
17. Who is person to take care or help you about diabetes at home? (you can mark more than
one)
1. My wife/husband 2. My children 3. My relative
4. No one 5. Other (specify) _________________
B. History of foot problems
18. Have you ever had a foot ulcer?

37
1. No 2. Yes, How many? __________
19. Have you ever had a sore or cut on your foot or leg that took more than two weeks to
heal?
1. No 2. Yes, How many? __________
20. Have you ever had an amputation of a toe, foot, or leg?
1. No 2. Yes (If yes, when (date): _______
C. Current foot or leg problems
21. Do you have an ulcer, sore, or blister on your feet at this time?
1. No 2. Yes
22. Do you have blood or discharge on your socks?
1. No 2. Yes
23. Do you have any calluses on your feet?
1. No 2. Yes
24. Do you have any numbness, tingling, pins and needles, or itching sensation in your feet?
1. No 2. Yes

38
Part II: Knowledge of foot care
25. Please mark “X” for your answer in each item.
Items True False
Importance of taking antidiabetes treatment to prevent complications
Daily washing the feet
Using warm water for washing/bathing
Checking temperature of water before using
Drying the feet after washing
Talcum powder usage for keeping interdigital spaces dry
Keeping skin of the feet soft to prevent dryness
Lotion not to be applied in the interdigital spaces
Daily change of socks
Trimming nails of feet straight with care
Inspection of feet once a day by respondents
Wearing comfortable coat shoes
Checking the shoes from inside before wearing
Not walking bare foot
Warning signs for which consultation is required
Part III: Foot care practice
26. Can you reach and see the bottoms of your feet?
1. No 2. Yes
27. Do you examine your feet?
1. No 2. Yes

39
If yes, how often?
1. Every day 2. 2-6 times a week
3. Once a week or less 4. When I have a problem
28. Do you wash your feet every day? 1. No 2. Yes
29. Do you dry well between the toes? 1. No 2. Yes
30. Do you use a moisturizing cream on your feet? 1. No 2. Yes
31. Do you cut your own toenails? 1. No 2. Yes
If no, who does this for you?
1. Family member 2. Foot care nurse
3. Podiatrist 4. Other (specify): ______________
32. What kind of shoes do you wear? (Check all that apply)
1. Pointed toes 2. Broad, round toes
3. High heels 4. Sandals
5. Flip flops/thongs 6. Athletic/sneakers/runners
7. Shoes made of leather or canvas
33. What kind of socks do you wear? (Check all that apply)
1. Cotton 2.Wool
3.Acrylic/synthetic 4. Knee highs
5. Prescription/compression 6. Not know
7. Other (specify)………
34. Do you ever soak your feet?
1. No 2. Yes
35. Do you always test water temperature before your foot in?
1. No 2. Yes
36. Do you use medicated products for warts, corns or calluses?

40
1. No 2. Yes
37. Do you put moisturizing creams or lotions between your toes?
1. No 2. Yes
38. Do you ever walk around in your bare feet?
1. No 2. Yes
39. Do you ever wear shoes without wearing any socks?
1. No 2. Yes 3. Never use socks when wearing shoes
40. Do you use a hot water bottle or heating pad on your feet?
1. No 2. Yes
41. Do you sit with your legs crossed?
1. No 2. Yes
42. Do you think you have taken care your feet in correct way?
1. No 2. Yes
Foot care Education
43. Have you ever attended a class on how to care for your feet?
1. No 2. Yes
44. Have you ever read any handouts on foot care?
1. No 2. Yes
45. Would you like a handout on how to care for your feet?
1. No 2. Yes

41
46. What kind do you think is the most effective way for increasing your knowledge and
practice of foot care?
1. Receiving handout/brochure
2. Health education in group
3. Individual health education
4. Media such as TV, radio, etc.
5. Others (specify) ____________________________
Thank you for your answer!
Top Related