







Languages
Pages
Legal


International Pain School
type in your name
Assessing pain & taking a pain history
type in the name of your institution

Outline
• Why is it important to assess pain?
• Why should you use tools to evaluate pain?
• What are the components of the pain assessment process?
• How to optimize pain assessment
• Pain assessment in children & in patients with impaired
communication
• Pain evaluation tools which are practical for
low-resource settings
• Conclusion: Pearls

Case
• You are working in a small rural hospital when Parmanand,
a 17 year old male, is admitted after a motorcycle accident.
• He is awake, haemodynamically stable and seems to have
fractured his left leg. He is groaning.
The surgeon tries to carry out a physical examination, but
Parmanand resists.
• Do you need to assess Parmanand’s pain?
• How would you do it?
• How should you act once you have assessed
Parmanand’s pain?

Why is it important to assess pain?• Assessment of pain is the first step in planning
pain management.• Pain assessment should be repeated to
evaluate the efficacy of pain management• Tailor the assessment tool to the patient’s age,
condition, type of pain (acute vs chronic). • Evaluate the patient’s other symptoms,
functional status and general clinical status in
parallel with the pain assessment.

Timing of the pain assessment
Pain assessment should occur at:•Each clinical encounter•Regular intervals after initiation of treatment,
e.g. a suitable interval after pharmacologic or
non-pharmacologic intervention
[15–30 minutes after parenteral drug therapy & 1 hour
after oral administration]
•Each new report of pain

Components of taking a pain historyAsk about:
• Location
• Quality
• Intensity
• Duration
• Alleviating and aggravating factors [e.g., medicines/drugs,
alcohol, herbals, movement, positioning]
• Impact on patient’s life [e.g., daily activities, work performance,
social contacts]
• Medication related side effects
• Ask and assess for other symptoms [e.g., nausea, vomiting,
constipation, confusion, depression, dyspnoea].
of the pain

How to assess a patient’s pain history: the ‘PQRST’ approachP: Provokes and Palliates
•What causes the pain?
•What makes the pain better?
•What makes the pain worse?
Q: Quality
•What does the pain feel like?
•Sharp? Dull? Stabbing? Burning?
Crushing?
R: Region and Radiation
•Where is the pain located?
•Is it confined to one place?
• Does the pain radiate? If yes, where
to?
• Did it start elsewhere and now
loclized to one spot?
S: Severity
• How severe is the pain?
T: Time
• When did the pain start?
• Is it present all the time?
• Are you pain-free at night / day?
• Are you pain-free on movement?
• How long does the pain last?

Factors influencing perception of pain• The patient is an expert about his/her body,
his self-reported pain should be accepted as
accurate.• In communicating patients, rely on the patient’s
self report; it is affected by a variety of factors. • Factors influencing a person’s experience of pain:
–positive vs. negative expectations–mood (sense of hopelessness vs. optimism)–culturally acceptable levels of ‘complaining’–coping and adaptation abilities–meaning attached to the experience of pain

Communication between patient and caregiver: listen actively
• Caregivers should not wait for the patient to report
about pain, but actively and sensitively explore
this with the patient.
• Allow patients to describe their pain in their own
words.
• Consider, that patients may report their pain
experience in socially acceptable words.
• When patients feel uncomfortable describing their
pain, health care providers can suggest a sample of
relevant descriptors, they can be written on cards.

Communication of pain: locate the pain• Patients can be requested to
indicate primary site/s of
pain by shading relevant
areas on a figure of a human
body
[front and back] OR pointing
out on their own body.
• This can indicate the
direction of radiating or
referred pain
• Schematics such as these
are used for assessing
chronic pain conditions; not
typically carried out in acute
situations.
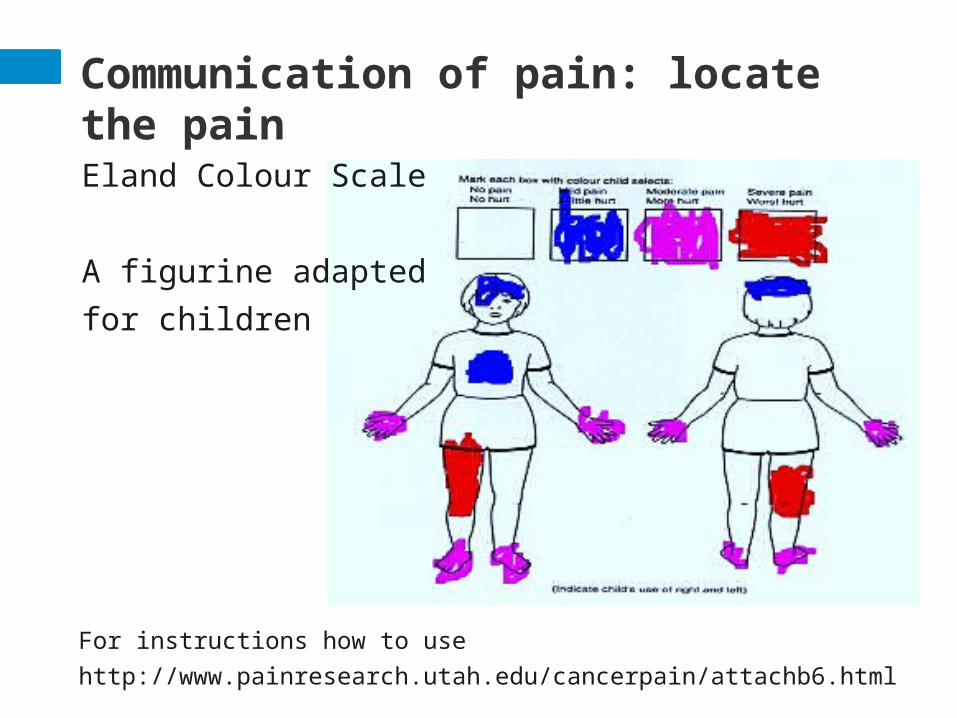
Communication of pain: locate the painEland Colour Scale
A figurine adapted for
children
For instructions how to use
http://www.painresearch.utah.edu/cancerpain/attachb6.html

Duration of pain assessment
•D
epends on the presenting problem/s and demands of
clinic time.

Patients with communication barriersPatients with barriers to communication can affect the pain
assessment.
These include:
• Pre-verbal children
• Individuals of advanced age
• Patients with dementia
• Patients with emotional or cognitive dysfunction
• Patient does not speak the same language as the care
provider
• Patients who are seriously ill

General approach to pain assessment
•A
llow sufficient time for the assessment.
•U
se interpreter if language of communication is
second language.
•G
ive the patient the opportunity to use a rating
scale or other tool appropriate for that
population.

General approach to pain assessment cont’d
•U
se pain indicators according to the following hierarchy of importance:•P
atient self-report•P
athological conditions or procedures known to be painful•P
ain-related behaviors (e.g., grimacing, restlessness, vocalization)•R
eports of pain by family members or caretakers•P
hysiological measures (vital signs)•R
eliance on behavioral or objective indicators of pain (e.g., vital signs)
only when no suitable alternative exists

Assessment in situations of acute pain
• Control of pain does not impede the accuracy
of diagnosis.
• Do not withhold pain management because of
ongoing or planned diagnostic procedures.
• A comfortable patient will tolerate diagnostic
procedures better and will be more cooperative.
• It is also a humane duty to ensure fast provision of
pain relief.
Pain assessment in children
• Children, even newborns, feel pain.
• ‘QUESTT’ approach
–Question the child if verbal, and the parent/guardian
in both the verbal and non-verbal child
–Use pain rating scales if appropriate
–Evaluate behavior and physiological changes
–Secure the parent’s involvement
–Take the cause of pain into account
–Take action and evaluate the results
When possible: carry out the assessment in the presence of family/guardian

Pain assessment in children
• Neonates: 0-1 month• Behavioral observation, done accompanied by
child’s family/guardian to discern between
‘normal’ and ‘abnormal’ behavior, is the only way
of assessment at this age• Lack of behavioral responses [facial expressions
e.g. crying, and discomforted movement] does
not always mean absence of pain• Behavioral responses are not necessarily
accurate indicators of the neonate’s level of pain

Pain assessment in children
Infants may exhibit the following when experiencing
pain:
•Body rigidity/thrashing
•Facial expression of pain [brows lowered and drawn
together, eyes tightly closed, mouth open and squared]
•Loud and intense cries
•Inconsolability, hypersensitivity / irritability
•Draw knees to chest
•Poor food intake, poor sleep
Infants: 1 month to 1 year

Pain assessment in children
Toddlers may exhibit the following when experiencing
pain:
• Verbal aggression, intense cries
• Regressive behavior / withdrawal
• Physical resistance, guard painful part of the body
• Poor sleep
• May require play and drawings to get an accurate
assessment of their pain
• Some may express their pain using simple language.
Toddlers: 1-2 years

Assessing behavioral signs of painFLACC Pain Scale (<2,5 years)

Assessing behavioral signs of pain
How to Use the FLACC
In patients who are awake:
Observe for 1 to 5 minutes or longer. Observe legs and body
uncovered. Reposition patient or observe activity. Assess body for
tenseness and tone. Initiate consoling interventions if needed.
In patients who are asleep:
Observe for 5 minutes or longer. Observe body and legs
uncovered. If possible, reposition the patient. Touch the body and
assess for tenseness and tone
FLACC Pain Scale (<2,5 years)

Assessing behavioral signs of pain
Interpreting the FLACC Score
Each category is scored on a 0–2 scale, which results in a
total score of 0–10.
0 -- Relaxed and comfortable
1–3 -- Mild discomfort
4–6 -- Moderate pain
7–10 -- Severe discomfort or pain or both
FLACC Pain Scale (<2,5 years)

Pain assessment in children
The pre-schooler may exhibit the following during pain:
•may verbalize his/her pain
•Thrash arms and legs, pushes stimuli away before they are
applied
•Be uncooperative, need physical restraint
•Cling to their parent/guardian, need emotional support [e.g.
hugs]
•Poor sleep
•Carry out the assessment using simple language and sympathetic
demeanor
Pre-school: 3-5 years

Self report
The OUCHER is a poster developed for children to help them communicate how much pain or hurt they feel.
There are two scales on the OUCHER: a number scale for older children and a picture scale for younger children.
OUCHER Scale (< 3 years)
It is possible to adapt the photos on the scale to different ethnicities (USA): •Caucasian•African American•Hispanic•Asian - Boy•Asian - Girl•First Nations (Canada- Boy•First Nations - Girl
For instructions how to use the scale: http://www.oucher.org/the_scales.html

Pain assessment in children
The school-age child may exhibit the following during pain:
•Verbalize their pain
•May even ask what causes their pain; may need age-sensitive
explanations: ‘You have pain in your stomach because you have a
lump there which is making it hurt.’
•Influenced by cultural beliefs, experience pain-related nightmares
•Stalling behaviors [e.g. ‘wait a minute’, ‘I’m not ready’]
•Muscular rigidity [e.g. clenched fists, white knuckles, gritted
teeth, contracted limbs, stiff body, closed eyes, wrinkled forehead]
•Reservation in fear of consequences [e.g. injection]
•All behaviors of pre-schoolers
School-age: 6-12 years

Age: > 6 years
Pain assessment in older children
• can also be used in
adults unable to use
numerical scales
verbal rating scale
Pain assessment in children
Adolescents may exhibit the following during pain:
•Verbalize their pain
•Peer pressure: deny pain in the presence of peers
•Changes in sleep pattern or appetite
•Health care provider
should avoid confrontation, engage conversation
focused on the adolescent rather than the problem
[informal questions about friends, school, hobbies,
family, soccer …]
Adolescents: 13-18 years

Pain assessment in adolescents and adults
0 – 3 OR no to mild pain = no change in therapy
4 – 7 OR moderate pain = initiate or change
therapy
8 – 10 OR severe pain = emergency treatment
Numerical and verbal rating scales (>12 years)
How to use the scale? Example of what to say to a
patient:
‘On a scale of 0 to 10, when ‘0’ represents NO PAIN and ’10’
represents the WORST PAIN IMAGINABLE, how much pain do you
have now?’
Pain assessment among the aged •T
he UN definition of ‘older people’ may not apply for sub-
Saharan Africa where complex and multi-dimensional socio-
cultural definitions exist [e.g. seniority status, number of
grandchildren]•I
t is challenging to assess pain among geriatric patients with
multi-morbidity, poli-pharmacy and dementia•V
isual and hearing impairment may be obstacles•U
se behavior-based proxies in non-communicative cases•I
n principle, for the geriatric patient: Ask for Pain

Pain evaluation tools practical for low-resource settings• One-dimensional tools can be practical because they:
take shorter time to administer
require lower levels of patient’s education
are validated in linguistically and culturally diverse
settings
• Examples include: African Palliative Outcome Scales
(APOS), Numerical Rating Scale [NRS], Verbal Descriptor
Scale [VDS], FLACC Behavioral Pain Scale, Wong-Baker
FACES Pain Rating Scale, the Pain Thermometer

Example for Multidimensional Pain Evaluation
Rated using the hand scale:
Clenched hand represents ‘no hurt’.
Five extended digits represents ‘overwhelming/worst’
Each extended digit indicates increasing level of pain.
APCA African Palliative Outcome Scale

Observe for 5 min
Interpretation: moderate pain = 4-6, severe pain = 7-10
Pain assessment in Dementia
Observational Scale: PAINAD
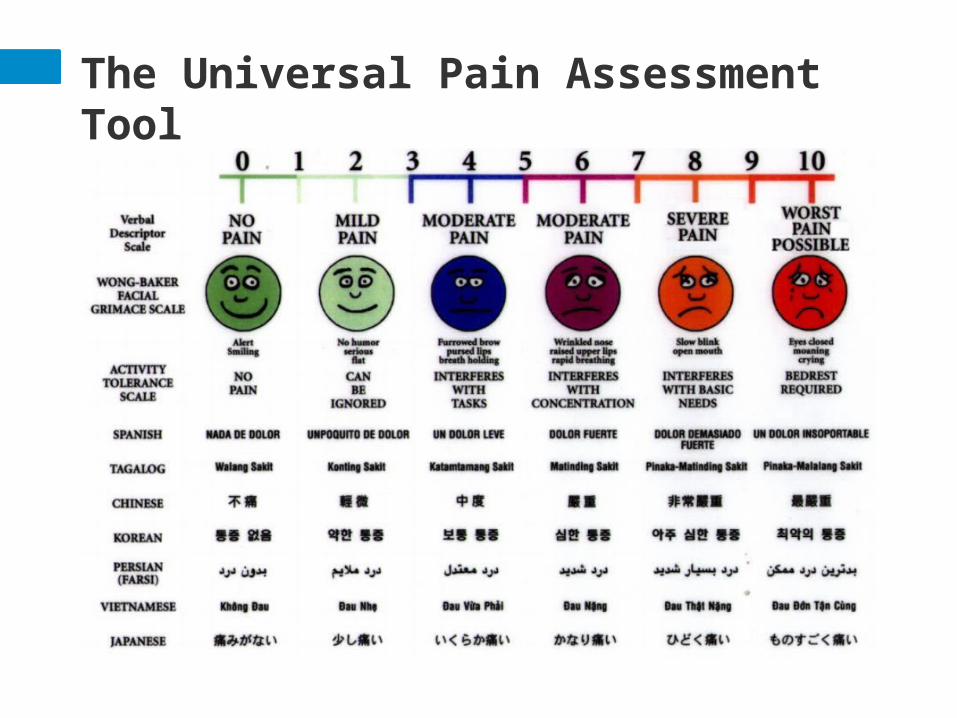
The Universal Pain Assessment Tool
Conclusion: Pearls I
• Pain assessment should be part of the daily
routine (“5th vital sign”). • Tailor the assessment to the patient [e.g. age,
cognitive ability, literacy level]. • Aim to use validated pain assessment tools –
this helps to standardize the process of
assessment. • Pain assessment is not an “academic
exercise”: assessment should be used planning
management of pain.

Conclusion: Pearls II
• Once you have made an assessment, interpret
it and carry out the relevant therapeutic
intervention: • ≤ 3/0-10 scale no change in therapy is
typically necessary• ≥ 3/0-10 scale typically analgesic therapy
should be administered or current regimen
changed• pain emergency, typically intensity of 9-
10/10 analgesic therapy should given
immediately & intravenously, if appropriate.

Conclusion: Pearls III
Interview the patient about which factors aggravate
or relieve the pain. Can help to identify the etiology of
pain, e.g.,
• pain worst at early morning hours: inflammation?• pain constant and severe: chronic pain disease?• pain decreases with movement: osteoarthritis?• pain worse on coughing/sneezing: radicular pain?• pain is alleviated with a cool pack: inflammation?• pain is alleviated with heat: muscular pain?

Conclusion: Pearls IV
• Pain descriptors help to differentiate the
aetiology of the pain and point to a therapeutic
strategy:• ‘burning’, ‘shooting’, ‘electrical’ -> think pain is
of neuropathic origin.• ‘dull’, ‘aching’, drilling, etc -> think pain is of
nociceptive origin.

Case study
• You are working in a small rural hospital when
Parmanand,
a 17 year old male, is admitted after a motorcycle
accident.
• He is awake, haemodynamically stable and seems to
have fractured his left leg. He is groaning.
The surgeon tries to carry out a physical examination,
but Parmanand resists.
• Do you need to assess Parmanand’s pain?
• How would you do it?
• How should you act once you have assessed
Parmanand’s pain?

Discussion of Case
• Permanand seems to be in intense pain and so it is
imperative to control his pain as quickly as possible.
• Permanand is of an age that he can verbalize his pain,
therefore, ask him to assess the intensity of his pain.
• Use verbal descriptor scale or numerical pain scale.
• If there is no acute volume loss, initiate analgesia before
further diagnostic procedures
• When the pain is severe, management should be
intravenous and opioid based.
• Using the body diagram in this acute situation
is not necessary.

This talk was originally prepared by:

Talks in the International Pain School include the following:
International Pain School
Physiology and pathophysiology of pain Nilesh Patel, PhD, Kenya
Assessment of pain & taking a pain historyYohannes Woubished, M.D, Addis Ababa, Ethiopia
Clinical pharmacology of analgesicsand non-pharmacological treatments
Ramani Vijayan, M.D. Kuala Lumpur, Malaysia
Postoperative – low technology treatment methodsDominique Fletcher, M.D, Garches & Xavier Lassalle, RN, MSF, Paris, France
Postoperative– high treatment technology methodsNarinder Rawal, M.D. PhD, FRCA(Hon), Orebro, Sweden
Cancer pain– low technology treatment methods Barbara Kleinmann, MD, Freiburg, Germany
Cancer pain– high technology treatment methodsJamie Laubisch MD, Justin Baker MD, Doralina Anghelescu MD, Memphis, USA
Palliative CareJamie Laubisch MD, Justin Baker MD, Memphis, USA
Neuropathic pain - low technology treatment methodsMaija Haanpää, MD, Helsinki & Aki Hietaharju, Tampere, Finland
Neuropathic pain – high technology treatment methodsMaija Haanpää, M.D., Helsinki & Aki Hietaharju, M.D., Tampere, Finland
Psychological aspects of managing pain Etleva Gjoni, Germany
Special Management Challenges: Chronic pain, addiction and dependence, old age and dementia, obstetrics and lactation
Debra Gordon, RN, DNP, FAAN, Seattle, USA

International Pain School
The project is supported by these organizations:
Top Related