HIV Medicine From Guidelines to Practice Kiat Ruxrungtham
Professor of Medicine, Chulalongkorn University; and HIV-NAT, Thai
Red Cross AIDS Research Center Kiat Ruxrungtham Professor of
Medicine, Chulalongkorn University; and HIV-NAT, Thai Red Cross
AIDS Research Center
Slide 2
Three Decades of HIV/AIDS Learning and the Future Mid 1990 1981
2012 - 2014 One/ two ARVs Improve survival One/ two ARVs Improve
survival 2020 Three ARVs (HAART) Durable undetectable VL Three ARVs
(HAART) Durable undetectable VL Earlier HAART non-AIDS death
Transmission New TB Earlier HAART non-AIDS death Transmission New
TB New strategies Long-acting ARV ? Cure ? New strategies
Long-acting ARV ? Cure ? late 1980 Few ARVs More toxicity Few ARVs
More toxicity More class ARVs More potent PIs But high pill burden
More class ARVs More potent PIs But high pill burden More new ARVs
More tolerable More OD options More FDC options Single tablet
regimens More new ARVs More tolerable More OD options More FDC
options Single tablet regimens Monthly ARV? Cure ? Monthly ARV?
Cure ? Evidences and developments Availability and treatment
options
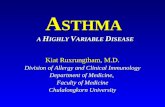
CD4 cell count Years After HIV Infection Clinical outcomes No
AIDS-complication + No non-AIDS-complication Clinical outcomes No
AIDS-complication + No non-AIDS-complication 500 350 200 ? CIPRA
HT001 START trial
Slide 6
Current Update on HIV Treatment 2014
Slide 7
When to start ART by guidelines GuidelinesCD4Note U.S. DHHS
2014All When the patient is ready and committed to treatment WHO
2013
What to start in Resource-rich settings? NtRTI or NRTI NtRTI or
NRTI NRTI Cytidine Analog NRTI Cytidine Analog NNRTI or bPI or
Integrase inh. NNRTI or bPI or Integrase inh. ++ TDF ABC* AZT TDF
ABC* AZT FTC 3TC FTC 3TC Three drug combination in Nave Patients 2
Nucleoside RT Inhibitors + NNRTI or Boosted PI or Integrase
inhibitor Efavirenz Atazanavir/r Darunaivr/r Raltegravir
Dolutegravir Evitegravir/cobi 1 Rilpivirine 2 Efavirenz
Atazanavir/r Darunaivr/r Raltegravir Dolutegravir Evitegravir/cobi
1 Rilpivirine 2 1 eGFR>70; 2 when VL
How to detect failure and DR? Time-course of HAART Failure
Clinical Started HAART 1 234 5 Non- Adherence Non- Adherence Viral
load Resistance CD4 drop Time (months years) Thai NHSO guidelines:
VL q 6 mo, until VL350, q 1 yr Thai NHSO guidelines: VL q 6 mo,
until VL350, q 1 yr
Slide 31
Viral Load and CD4 Tests
Slide 32
Virologic Failure The inability to achieve or maintain
suppression of viral replication SettingDHHS 2009DHHS 2011WHO 2009
Incomplete suppression after 24 weeks >400*>200*>5000**
Virologic Rebound >50>200***>5000 *High Baseline VL
(>100,000 c/ml) may take longer than low BL VL **Values of >5
000 copies/ml are associated with clinical progression and a
decline in the CD4 cell count ***>200 is associated with
evidence of viral evolution and drug-resistance mutation
accumulation
Slide 33
Slide 34
Second-line ART controlled studies
StudyNcomparatorsSitesSponsorsEnd point analysis HIV-STAR200
TDF/3TC +LPV/r LPV/r mono Thailand 10 sites HIVNAT, NHSO, Swiss
cohort Nov 2011 SECOND- LINE 550 2NRTI +LPV/r RAL +LPV/r All
continents 18 countries Kirby Insitute, Australia Sept 2012 ALISA
386 TDF/FTC +LPV/r TDF/3TC +ATV/r Africa SA, Tanzania French NIH
May 2013 2LADY 450 TDF/FTC +LPV/r ABC/ddI +LPV/r TDF/FTC +DRV/r
Africa Burkina Faso, Cammaroon, Senegal ANRS12169 Sep 2013 EARNEST
1277 2NRTIs +LPV/r RAL +LPV/r LPV/r mono Africa 5 countries MRC,
EDCTP Dec 2013 www.clinicaltrials.gov (assessed 22 Apr 2012)
Slide 35
HIV-STAR Results (HIVNAT, TRC-ARC, Thailand initiated trial)
Patients with baseline GSS 2 had a better % with VL< 50 c/ml at
48 weeks of treatment Bunupuradah T, et al,. Antiviral therapy 2012
Jul 2. doi: 10.3851
Slide 36
SECOND-LINE results
Slide 37
SECOND-LINE Study RAL/LPV/r NRTIs/LPV/r N= 270 N= 271 83% 81% %
patients with VL
Slide 38
Options after First-line Failure NRTI in the failing regimen
NRTI optionThird ARV option TDF failure Guided by resistance test
results, or Consider : AZT/3TC Preferred : Lopinavir/ritonavir
(LPV/r)* Alternative: Atazanavir/ritonavir (ATV/r),
darunavir/ritonavir (DRV/r) AZT or ABC failure Guided by resistance
test results, or Consider :TDF/FTC or TDF/3TC
Slide 39
boosted PI : WARNING Serious Drug Interaction 1.Ergotism:
ergotamine 2.Rhadomyolysis: statins (simvastatin, etc.)
Alternatives: pravastatin, fluvastatin and fibrate derivatives
3.Excessive sedation: benzodiazeoines (diazepam, alprazolam,
midazolam,..)except lorazepam 4.Hypotension: Ca-blockers
(amlodipine, nifedipine, felopdipine), beta-blockers 5.Cushing
syndrome, adrenal insufficiency: with fluticasone 6.Torsades de
Pointes (prolong QT and ventricular arrhythmia): cisapride,
pimozide; ditiazem; antiarrhythmic flecanide, amiodarone, quinidine
etc. 1.Ergotism: ergotamine 2.Rhadomyolysis: statins (simvastatin,
etc.) Alternatives: pravastatin, fluvastatin and fibrate
derivatives 3.Excessive sedation: benzodiazeoines (diazepam,
alprazolam, midazolam,..)except lorazepam 4.Hypotension:
Ca-blockers (amlodipine, nifedipine, felopdipine), beta-blockers
5.Cushing syndrome, adrenal insufficiency: with fluticasone
6.Torsades de Pointes (prolong QT and ventricular arrhythmia):
cisapride, pimozide; ditiazem; antiarrhythmic flecanide,
amiodarone, quinidine etc.
Slide 40
Ergotism and bPI is not common in patients who were well VL
control and on bPIs Thai report N=23 All had VL 250 20
hospitalization (4-20 days) 3 gangrene 2 Amputation 1death Thai
report N=23 All had VL 250 20 hospitalization (4-20 days) 3
gangrene 2 Amputation 1death Avihingsanond A. et al in submission
2012 a HCW casewas prescribed bPI as a PEP regimen bPI Ergotamine
AEs
Slide 41
Standard doses of boosted protease inhibitors (bPIs) associated
with a high exposure in Asian van der Lugt J, and Avinhingsanon A.
Asian Biomedicine Feb 2009
Slide 42
Cost Saving When Using a Lower Dose Atazanavir : from 300 to
200 mg 5 year savings = 6900 million Baht to treat 5000 cases with
a 5% cases increased/yr 5 year savings = 6900 million Baht to treat
5000 cases with a 5% cases increased/yr
Slide 43
ATV/r: atazanavor/ritonavir, PI: protease inhibitor, HAART:
highly active antiretroviral therapy, OD: once daily, TDF:
tenofovir Complete enrollment: Dec 2013, expected results by Jan
2015
Slide 44
Life Expectancy approaches normal in a High-income country
after HAART The Netherlands N = 17,580 person-year Median CD4 = 480
(24 wks of Dx) Life expectancy from 25 yo Men = 52.7 years Women
=57.8 years The Netherlands N = 17,580 person-year Median CD4 = 480
(24 wks of Dx) Life expectancy from 25 yo Men = 52.7 years Women
=57.8 years
Slide 45
Date of download: 8/25/2012 Copyright The American College of
Physicians. All rights reserved. From: Life Expectancy of Persons
Receiving Combination Antiretroviral Therapy in Low-Income
Countries: A Cohort Analysis From Uganda Ann Intern Med.
2011;155(4):209-216. doi:10.1059/0003-4819-155-4-201108160-00358
Uganda (N=22,315) Life expectancy at 30 yo CD4 150 = 40 years
Uganda (N=22,315) Life expectancy at 30 yo CD4 150 = 40 years The
life expectancy can be near normal with antiretroviral therapy,
especially when ART was initiated at CD4>150 cells
Slide 46
Thailand: Age and gender distribution HIV/AIDS statistic, BOE,
MOPH (data up to Nov 2011) Aging Future Trend Male Female
Slide 47
Reduced bone mineral density Renal dysfunction 30% of HIV+
patients have abnormal kidney function 1 Increased prevalence 63%
of HIV+ patients 2 Increased prevalence 63% of HIV+ patients 2
Emerging co-morbidities in HIV Gupta SK et al. Clin Infect Dis
2005;40:15591585.,Brown TT et al. J Clin Endocrinol Metab
2004;89(3):12001206, Clifford DB. Top HIV Med 2008;16(2):9498
Triant VA et al. J Clin Endocrinol Metab 2007;92:25062512, Patel P
et al. Ann Intern Med 2008;148:728736 Cardiovascular disease
Neurocognitive dysfunction Impairment present in 50% HIV+ patients
3 Cancer Increased risk of non-AIDS- defining cancers e.g. anal,
vaginal, liver, lung, melanoma, leukemia, colorectal and renal 5
Increased risk of non-AIDS- defining cancers e.g. anal, vaginal,
liver, lung, melanoma, leukemia, colorectal and renal 5 75%
increase in risk of acute MI 4
Slide 48
Drug Interactions with First-line ART and Lipid-Lowering
Therapy AntiretroviralContraindicatedTitrate Dose No Dose
Adjustment RPV [1] Atorvastatin EVG/COBI/TDF/ FTC [1] Lovastatin
Simvastatin Atorvastatin Rosuvastatin DTG [2] ATV/RTV [1]
Lovastatin Simvastatin Atorvastatin Rosuvastatin Pitavastatin
DRV/RTV [1] Lovastatin Simvastatin Atorvastatin Pravastatin
Rosuvastatin Pitavastatin EFV [1] Atorvastatin Simvastatin
Pravastatin Rosuvastatin RAL [1] 1. DHHS Adult Guidelines. February
2013. 2. Dolutegravir [package insert]. Kuritzkes D et al.
www.clinicaloptions.com
Slide 49
Drug Interactions With Oral Contraceptive Pills (OCPs)
AntiretroviralEffect on OCPDosing Recommendation RPV [1,2] Ethinyl
estradiol AUC 14% Norethindrone: no significant change No dose
adjustment EVG/COBI TDF/FTC [1,3] Ethinyl estradiol AUC 25%
Norgestimate Weigh the risks and benefits of norgestimate and
consider alternative contraceptive DTG [4] No clinically relevant
interactionNo dose adjustment ATV/RTV [1,2] Ethinyl estradiol AUC
Norgestimate OCP should contain 35 mcg ethinyl estradiol DRV/RTV
[1,2] Ethinyl estradiol AUC 44% Norethindrone AUC 14% Additional
methods of contraception recommended EFV [1,2] No effect on ethinyl
estradiol Active metabolites of norgestimate A reliable method of
barrier contraception must be used in addition to hormonal
contraceptives RAL [1,2] No clinically relevant interactionNo dose
adjustment 1. DHHS Adult Guidelines. February 2013. 2. DHHS
Perinatal Guidelines. July 2012. 3. TDF/FTC/EVG/COBI [package
insert]. 4. Dolutegravir [package insert]. Kuritzkes D et al.
www.clinicaloptions.com
Slide 50
DrugDrug Interactions Acid-Reducing Medications and Newer ARVs
ARVAntacids H2-Receptor Antagonists Proton Pump Inhibitors RPV [1]
Give antacids at least 2 hrs before or at least 4 hrs after RPV
Give H2-receptor antagonists at least 12 hrs before or at least 4
hrs after RPV Contraindicated EVG/COBI TDF/FTC [1] Separate
EVG/COBI/ FTC/TDF and antacid administration by > 2 hrs No
clinically relevant DTG [2] RAL DTG should be given 2 hrs before or
6 hrs after taking medications containing polyvalent cations No
clinically relevant 1. DHHS Adult Guidelines. February 2013. 2.
Dolutegravir [package insert]. Kuritzkes D et al.
www.clinicaloptions.com
Slide 51
Cardiologist Lifetime HIV care Requires an integrated
multidisciplinary approach Hepatologist Plastic surgeon
Nephrologist Neurologist Endocrinologist Nutritionalist Smoking
cessation Gynecologist Adpated From Anna Maria Geretti. London HIV
physician
Slide 52
Can we be the AIDS Free Generation?
Slide 53
Ending AIDS Policy How and When? Petchsri Sirinirund Advisor on
HIV/AIDS Policy and Programme Department of Disease Control,
Thailand ICAAP 11, 21 Nov 2013, Bangkok
Slide 54
50% reduction New Infection In 5 Years 50% reduction New
Infection In 5 Years End AIDS In 20 years End AIDS In 20 years
Ending AIDS Working Definition 1.New infection