







Languages
Pages
Legal

Highlights of ACC-i2 2009; ACS/AMI:
What’s Hot and What’s Not Roxana Mehran, MD, FACC, FSCAI
Columbia University Medical CenterCardiovascular Research Foundation

DisclosuresDisclosures
Research support (significant) from: The Research support (significant) from: The Medicines Company, Boston Scientific, Medicines Company, Boston Scientific, CordisCordis, Medtronic Vascular, Abbott , Medtronic Vascular, Abbott Vascular, Vascular, SanofiSanofi/Aventis/Aventis
Consultant (Modest): Lilly/Consultant (Modest): Lilly/DiachiDiachi Sankyo, Sankyo, Medtronic Vascular, Abbott Vascular, Medtronic Vascular, Abbott Vascular, CordisCordis, , BraccoBracco, The Medicines Company, The Medicines Company

Early Glycoprotein IIb/IIIa Inhibition in Non-ST-segment Elevation Acute Coronary Syndrome: A Randomized, Double-blind, Placebo-Controlled Trial Evaluating the
Clinical Benefits of Early Front-loaded Eptifibatide in the Treatment of Patients with Non-ST-segment Elevation
Acute Coronary Syndromes
Early Glycoprotein IIb/IIIa Inhibition in Non-ST-segment Elevation Acute Coronary Syndrome: A Randomized, Double-blind, Placebo-Controlled Trial Evaluating the
Clinical Benefits of Early Front-loaded Eptifibatide in the Treatment of Patients with Non-ST-segment Elevation
Acute Coronary Syndromes
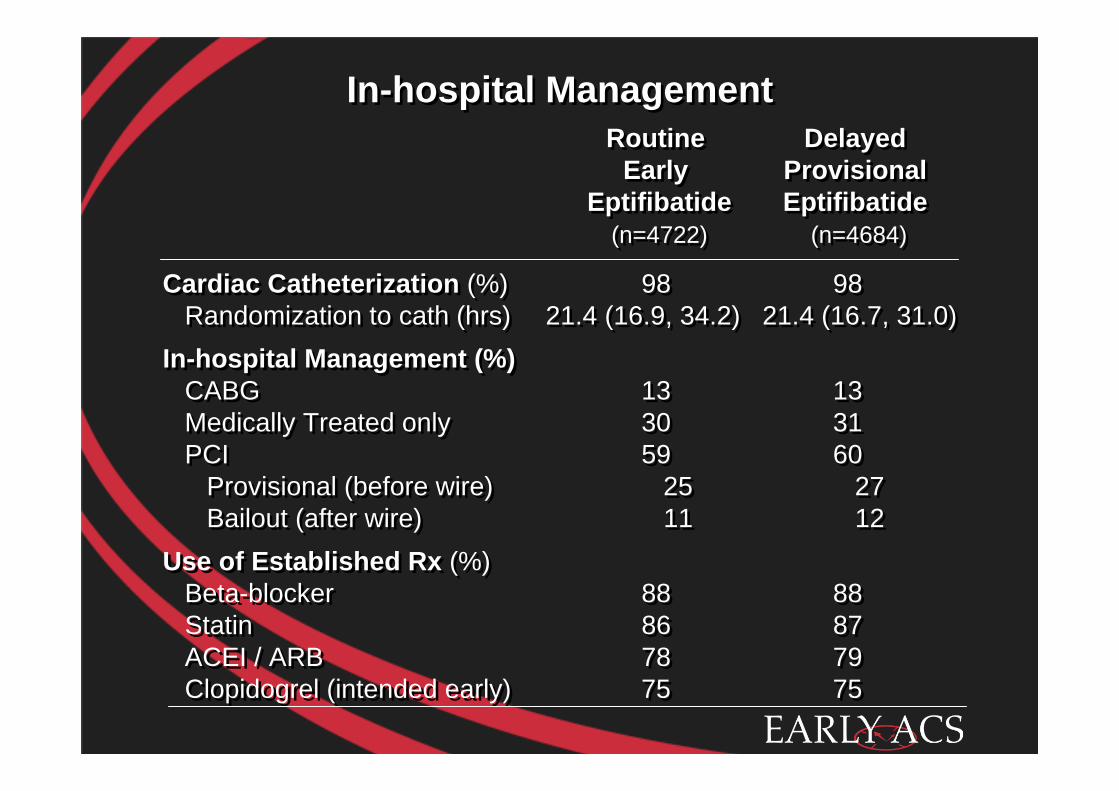
In-hospital ManagementIn-hospital Management
Cardiac Catheterization (%) 98 98Randomization to cath (hrs) 21.4 (16.9, 34.2) 21.4 (16.7, 31.0)
In-hospital Management (%)CABG 13 13Medically Treated only 30 31PCI 59 60
Provisional (before wire) 25 27Bailout (after wire) 11 12
Use of Established Rx (%)Beta-blocker 88 88Statin 86 87ACEI / ARB 78 79Clopidogrel (intended early) 75 75
Cardiac Catheterization (%) 98 98Randomization to cath (hrs) 21.4 (16.9, 34.2) 21.4 (16.7, 31.0)
In-hospital Management (%)CABG 13 13Medically Treated only 30 31PCI 59 60
Provisional (before wire) 25 27Bailout (after wire) 11 12
Use of Established Rx (%)Beta-blocker 88 88Statin 86 87ACEI / ARB 78 79Clopidogrel (intended early) 75 75
Routine Early
Eptifibatide(n=4722)
Routine Early
Eptifibatide(n=4722)
Delayed Provisional Eptifibatide
(n=4684)
Delayed Provisional Eptifibatide
(n=4684)
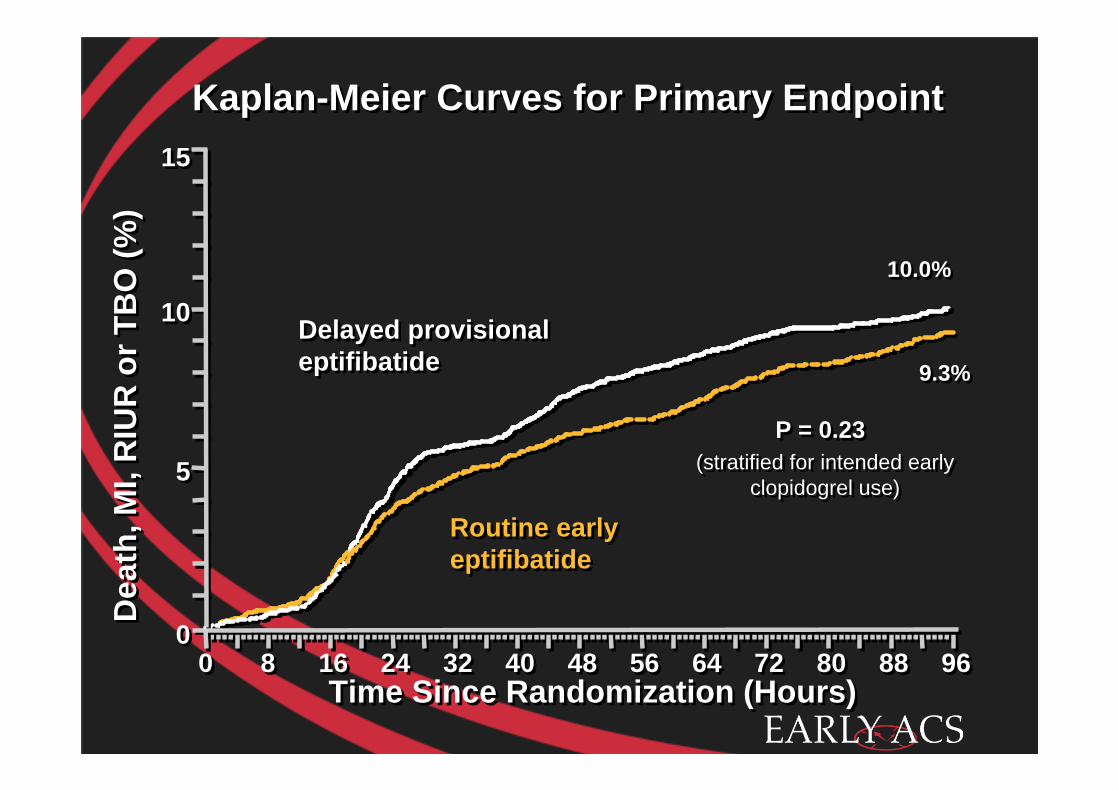
Kaplan-Meier Curves for Primary EndpointKaplan-Meier Curves for Primary EndpointD
eath
, MI,
RIU
R o
r TB
O (%
)D
eath
, MI,
RIU
R o
r TB
O (%
)
00
55
1010
1515
Time Since Randomization (Hours)Time Since Randomization (Hours)
10.0%10.0%
9.3%9.3%
P = 0.23P = 0.23(stratified for intended early
clopidogrel use)(stratified for intended early
clopidogrel use)
Delayed provisional eptifibatideDelayed provisional eptifibatide
Routine early eptifibatideRoutine early eptifibatide
00 88 1616 2424 3232 4040 4848 5656 6464 7272 8080 8888 9696

Kaplan-Meier Curves for 30-day Death or MIKaplan-Meier Curves for 30-day Death or MID
eath
or M
I (%
)D
eath
or M
I (%
)
00
55
1010
1515
Time Since Randomization (Days)Time Since Randomization (Days)00 22 44 66 88 1010 1212 1414 1616 1818 2020 2222 2424 2626 2828 3030
12.4%12.4%
11.2%11.2%
P = 0.079P = 0.079(stratified for intended early
clopidogrel use)(stratified for intended early
clopidogrel use)
Delayed provisional eptifibatideDelayed provisional eptifibatide
Routine early eptifibatideRoutine early eptifibatide

Safety Results (through 120 hours)Safety Results (through 120 hours)
Bleeding (all patients, %)TIMI major 2.6 1.8 1.42 (1.07-1.89) 0.015TIMI major or minor 5.8 3.4 1.75 (1.43-2.14) <0.001GUSTO severe 0.8 0.9 0.99 (0.64-1.55) 0.97GUSTO moderate or severe 7.6 5.1 1.52 (1.28-1.80) <0.001PRBC transfusion 8.6 6.7 1.31 (1.12-1.53) 0.001
Bleeding (CABG)Re-operation for bleeding (%) 6.0 8.4 0.70 (0.39-1.27) 0.24 Chest tube output (mL/24 H) 720 770 -- 0.41
Thrombocytopenia (<100K, %) 3.3 2.8 1.19 (0.93-1.51) 0.17Stroke (total, %) 0.6 0.8 0.79 (0.48-1.30) 0.36
Bleeding (all patients, %)TIMI major 2.6 1.8 1.42 (1.07-1.89) 0.015TIMI major or minor 5.8 3.4 1.75 (1.43-2.14) <0.001GUSTO severe 0.8 0.9 0.99 (0.64-1.55) 0.97GUSTO moderate or severe 7.6 5.1 1.52 (1.28-1.80) <0.001PRBC transfusion 8.6 6.7 1.31 (1.12-1.53) 0.001
Bleeding (CABG)Re-operation for bleeding (%) 6.0 8.4 0.70 (0.39-1.27) 0.24 Chest tube output (mL/24 H) 720 770 -- 0.41
Thrombocytopenia (<100K, %) 3.3 2.8 1.19 (0.93-1.51) 0.17Stroke (total, %) 0.6 0.8 0.79 (0.48-1.30) 0.36
DelayedProvisional Eptifibatide
(n=4643)
DelayedProvisional Eptifibatide
(n=4643)
Routine Early
Eptifibatide(n=4686)
Routine Early
Eptifibatide(n=4686)
OR(95% CI)
OR(95% CI)
PP

Small Molecule GP IIb/IIIa Inhibition in NSTE ACSSmall Molecule GP IIb/IIIa Inhibition in NSTE ACSPURSUITPURSUIT
PRISMPRISM
PRISM PLUSPRISM PLUS
PARAGON BPARAGON B
PARAGON APARAGON A
TherouxTheroux
0.25 0.50 1.0 2.0 4.0Odds Ratio for 30-day Death or MI Relative to ControlOdds Ratio for 30-day Death or MI Relative to Control
COMBINED 2009 (n = 42,666)COMBINED 2009 (n = 42,666)0.89 (0.84-0.95)0.89 (0.84-0.95)
COMBINED 1998 (n = 23,967)COMBINED 1998 (n = 23,967)0.88 (0.79-0.97)0.88 (0.79-0.97)
EARLY ACSEARLY ACS
ACUITY TimingACUITY Timing
EARLY ACS + ACUITYEARLY ACS + ACUITY0.92 (0.82-1.01)

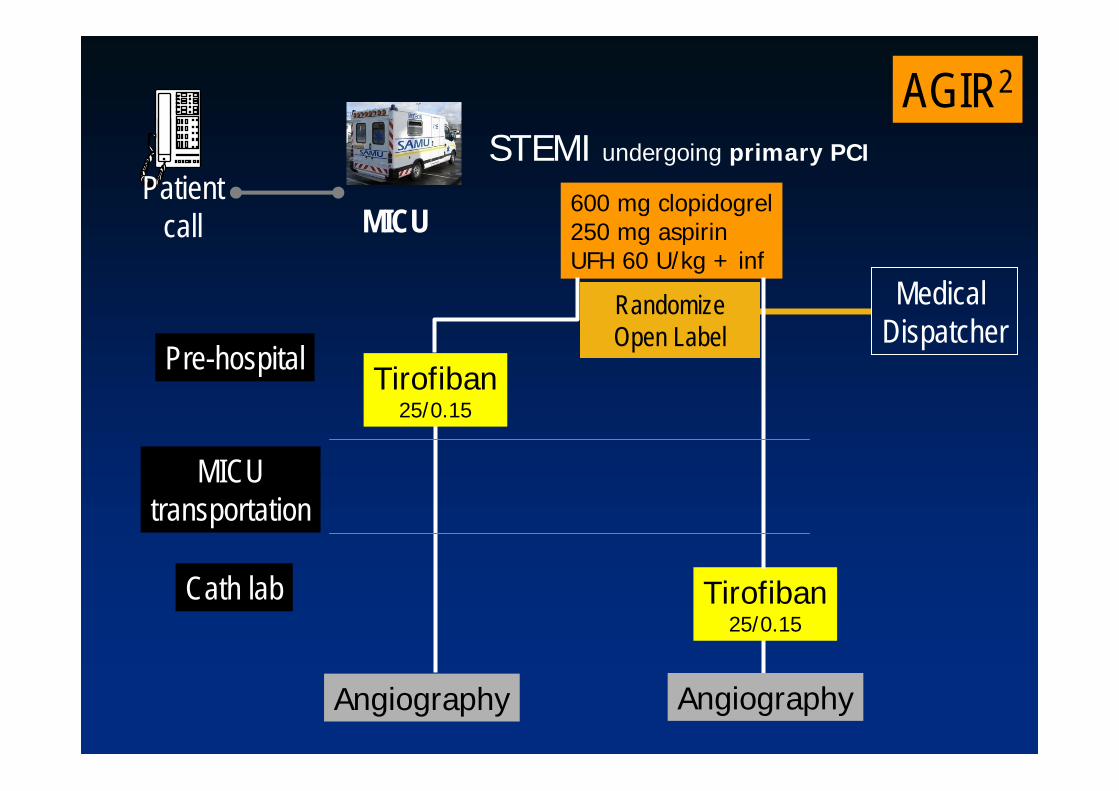
AGIR2
Comparison of Pre-hospital or Cath lab Administration of High Dose Tirofiban
in Patients Undergoing Primary AngioplastyThe AGIR2 Study
Eric Bonnefoyon behalf of AGIR2 investigators
and RESCUe and RESURCOR networksHospices Civils de Lyon, France
RESURCORRESURCOR
AGIR2
MICUPatient
call
STEMI undergoing primary PCI
600 mg clopidogrel250 mg aspirinUFH 60 U/kg + inf
Tirofiban25/0.15
Tirofiban25/0.15
AngiographyAngiography
Pre-hospital
MICUtransportation
Cath lab
Randomize Open Label
MedicalDispatcher

AGIR2
RESURCORRESURCOR
11 cath labs
17 MICU
20 miles
6 central triage centers(randomization)
Lyon
Annecy
Grenoble
Mont Blanc
Valence

AGIR2
End Points
Primary endpointTIMI grade 2-3 flow at initial angiographyKey secondary endpoints• Complete (>70%) ST segment resolution one
hour after procedure• Troponin I and CK peaks

AGIR2TIMI grade 2-3 flow
first angiography
Pre-hospitaltirofiban
39.7%44.2%P=0.42
Cath labtirofiban
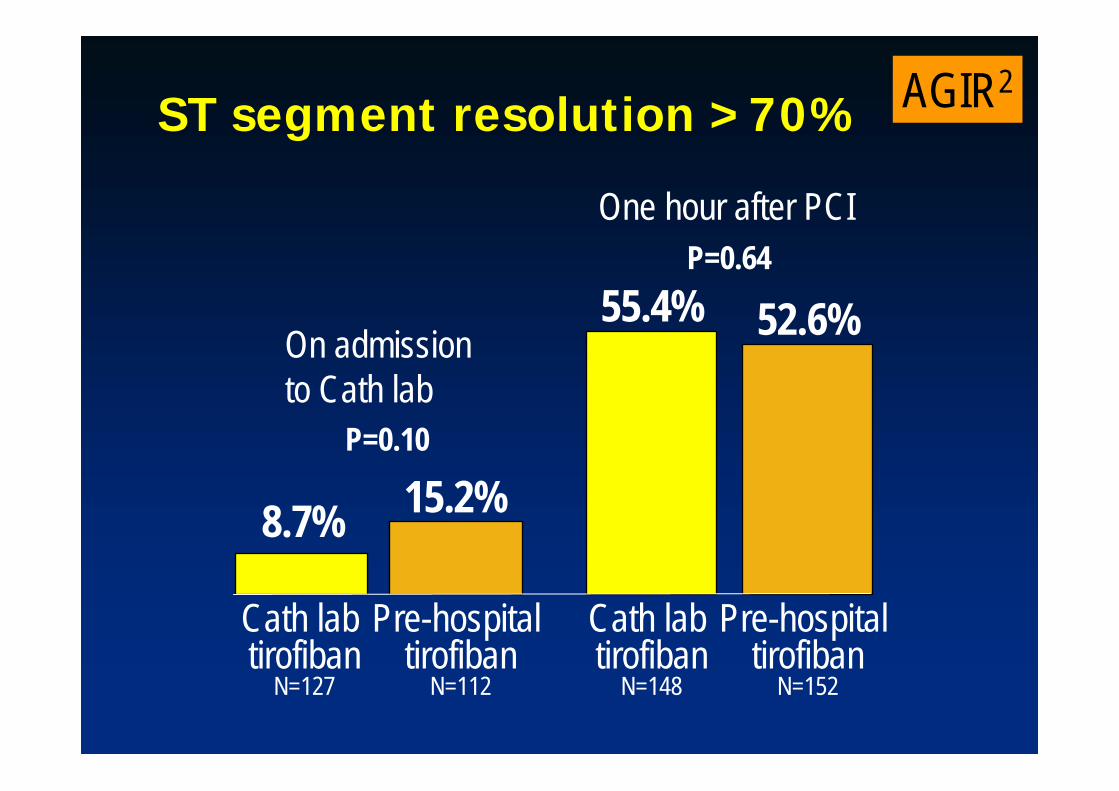
AGIR2ST segment resolution >70%
Cath labtirofiban
N=148
Pre-hospitaltirofiban
N=152
55.4% 52.6%P=0.64
Cath labtirofiban
N=127
Pre-hospitaltirofiban
N=112
8.7% 15.2%P=0.10
On admission to Cath lab
One hour after PCI
AGIR2
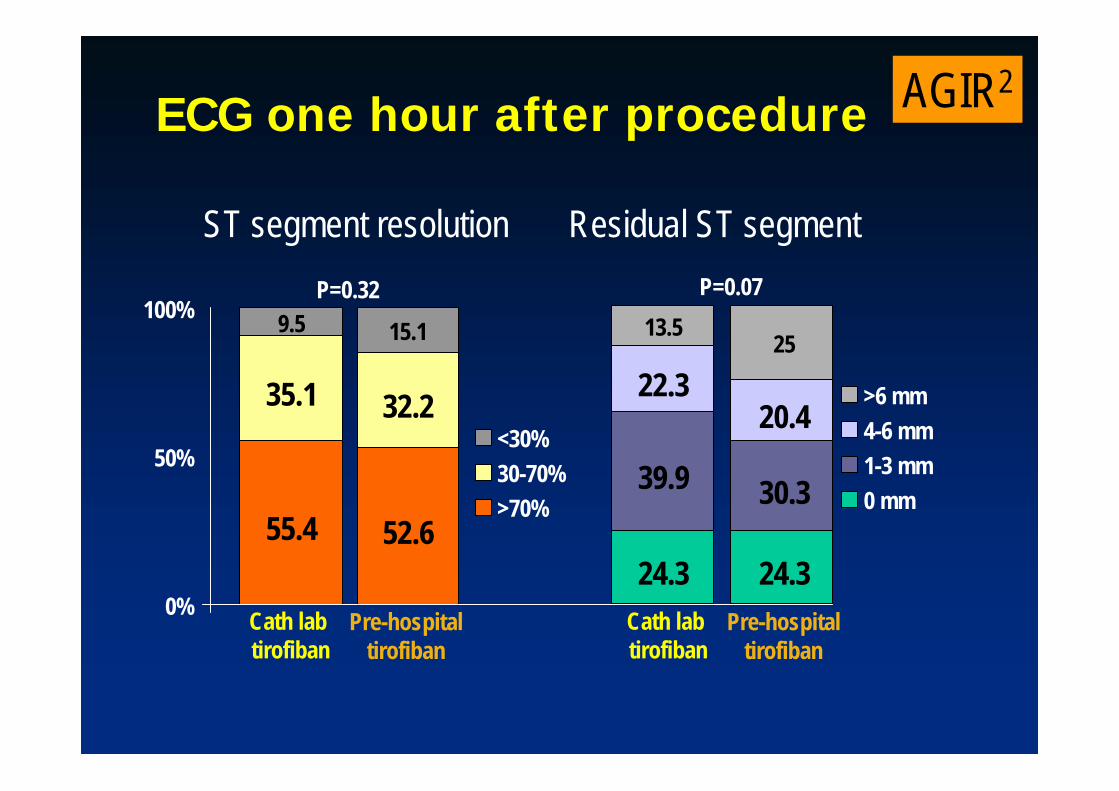
0%
50%
100%
Cath labtirofiban
Pre-hospitaltirofiban
<30%30-70%>70%
55.4 52.6
35.1 32.2
9.5 15.1P=0.32
24.3 24.3
39.9 30.3
22.320.4
13.5 25
P=0.07
>6 mm4-6 mm1-3 mm0 mm
Cath lab tirofiban
Pre-hospitaltirofiban
ST segment resolution Residual ST segment
ECG one hour after procedure

AGIR2
3.2
1.31.9
0.6
5.5
3.7
0.61.2
0
1
2
3
4
5
6
Death Severe Bleeding Acute stentthrombosis
Stroke
Cath lab tirofiban Pre-Hospital tirofiban% p=0.15
p=0.15
p=0.29p=0.26
In-hospital events

AGIR2Influence of treatment period tirofiban to angiography
p=0.15
p=0.11
33.0
63.8
46.0 49.345.5
54.3
0
10
20
30
40
50
60
70
TIMI 2-3 flow ST 60 min >70%
<10'10'-45'>45'
%
(terciles)

AGIR2
Conclusion
• Initiation of tirofiban in pre-hospital settings, prior to primary PCI and on top of a loading dose of clopidogrel, does not yield superior TIMI grade 2-3 flow in the culprit artery compared to initiation of tirofiban in the cardiac catheterization laboratory
• No beneficial effects on ST-segment resolution or peak troponin levels were found

Predictors of Acute, Subacute and Late Stent Thrombosis After Acute
MI Primary Angioplasty in the Horizons AMI Trial
George D. Dangas, Alexandra J. Lansky, Bruce R. Brodie, Bernhard Witzenbichler,
Giulio Guagliumi, Jan Z. Peruga, Dariusz Dudek, Martin Moeckel, Helen Parise, Roxana Mehran,
and Gregg W. Stone

HHarmonizing armonizing OOutcomes with utcomes with RRevascularevascularizizatiationon and and SStentstents in in AMIAMI
3602 pts with STEMI with symptom onset 3602 pts with STEMI with symptom onset ≤≤12 hours12 hours
Emergent angiography, followed by triage toEmergent angiography, followed by triage to……
Primary PCIPrimary PCICABGCABG –– Medical RxMedical Rx––
UFH + GP UFH + GP IIb/IIIaIIb/IIIa inhibitorinhibitor((abciximababciximab or or eptifibatideeptifibatide))
BivalirudinBivalirudin monotherapymonotherapy((±± provisional GP provisional GP IIb/IIIaIIb/IIIa))
Aspirin, Aspirin, thienopyridinethienopyridineR R
1:11:1
3006 pts eligible for 3006 pts eligible for stentstent randomizationrandomization R R 3:13:1
Bare metal EXPRESS Bare metal EXPRESS stentstentPaclitaxelPaclitaxel--eluting TAXUS eluting TAXUS stentstent
Clinical FU at 30 days, 6 months, 1 year, and thenyearly through 5 years; angio FU at 13 months
Clinical FU at 30 days, 6 months, 1 year, and thenClinical FU at 30 days, 6 months, 1 year, and thenyearly through 5 years; yearly through 5 years; angioangio FU at 13 monthsFU at 13 months
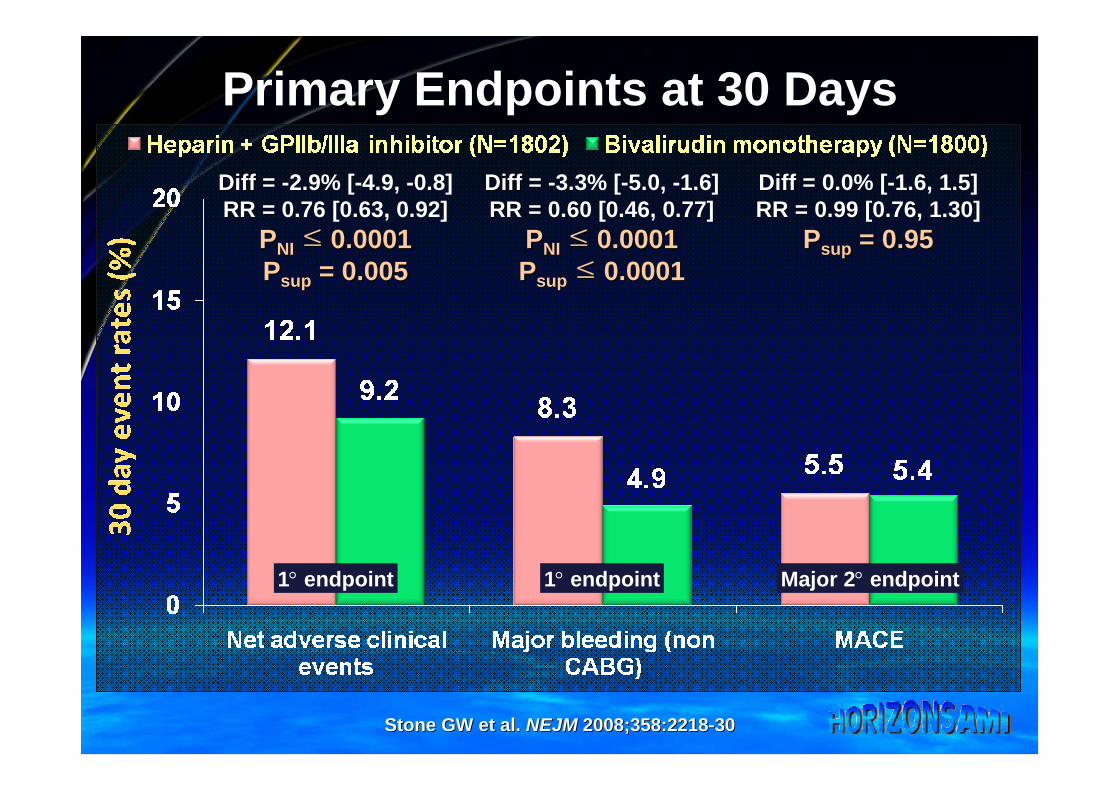
Diff = Diff = 0.0% [-1.6, 1.5]RR = 0.99RR = 0.99 [0.76, 1.30]
PPsupsup = 0.95= 0.95
Primary Endpoints at 30 Days
Diff = Diff = -3.3% [-5.0, -1.6]RR = RR = 0.60 [0.46, 0.77]
PPNINI ≤≤ 0.00010.0001PPsupsup ≤≤ 0.00010.0001
Diff = Diff = -2.9% [-4.9, -0.8]RR = RR = 0.76 [0.63, 0.92]
PPNINI ≤≤ 0.00010.0001PPsupsup = 0.005= 0.005
1° endpoint 1° endpoint
Stone GW et al. Stone GW et al. NEJMNEJM 2008;358:22182008;358:2218--3030
Major 2° endpoint

1-Year Mortality (All-Cause)
Number at riskBivalirudin aloneHeparin+GPIIb/IIIa
1800 1705 1684 1669 15201802 1679 1664 1647 1487
Mor
talit
y (%
)
0
1
2
3
4
5
Time in Months
0 1 2 3 4 5 6 7 8 9 10 11 12
Bivalirudin alone (n=1800)Heparin + GPIIb/IIIa (n=1802) 4.8%
3.4%
Diff [95%CI] = -1.4% [-2.7,-0.1]HR [95%CI] =
0.70 [0.51, 0.98] P=0.036P=0.036
3.1%
2.1%
Δ = 1.0%P=0.049
Δ = 1.4%

11--Year Year StentStent Thrombosis: Thrombosis: Impact of Impact of Implanted Implanted StentStent TypeType
3.3% 3.3% 3.4% 3.4%
HR [95%CI] =HR [95%CI] =0.98 [0.640.98 [0.64--1.51]1.51]
P = 0.93P = 0.93
22612261 21712171 21472147 21232123 20972097 19001900872872 832832 818818 805805 791791 720720
Number at riskNumber at riskAny DESAny DESBMS onlyBMS only
Def
/D
ef/ P
rob
Prob
Sten
tSt
ent T
hrom
bosi
s (%
)Th
rom
bosi
s (%
)
00
11
22
33
44
Time in daysTime in days00 3030 6060 9090 120120 150150 180180 210210 240240 270270 300300 330330 365365
Any DESAny DESBMS OnlyBMS Only

2.2% 2.2%
3.0% 3.0%
1.5%1.5%
0.3%0.3%
HR [95%CI] =HR [95%CI] =1.73 [0.471.73 [0.47--1.13]1.13]
P = 0.06P = 0.06
HR [95%CI] =HR [95%CI] =5.93 [2.065.93 [2.06--17.04]17.04]
P = 0.0002P = 0.0002
1611161115911591
16001600 15621562 15251525 15061506 14851485 1355135515871587 15211521 14951495 14761476 14571457 13151315
Number at riskNumber at riskBivalirudinBivalirudinUFH+GPIIb/IIIaUFH+GPIIb/IIIa
Def
/D
ef/ P
rob
Prob
Sten
tSt
ent T
hrom
bosi
s (%
)Th
rom
bosi
s (%
)
0.00.0
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
3.53.5
Time in DaysTime in Days00 11 3030 9090 180180 270270 365365
StentStent Thrombosis 1Thrombosis 1--Day Landmark Day Landmark Analysis:Analysis: Impact of Impact of AntithrombinAntithrombin
BivalirudinBivalirudin monotherapymonotherapyHeparin + Heparin + GPIIb/IIIaGPIIb/IIIa inhibitorinhibitor

Acute Acute StentStent Thrombosis:Thrombosis: Impact of Impact of PrePre--Randomization HeparinRandomization Heparin
10661066 10521052 10511051 10501050 10491049545545 531531 529529 528528 528528
Number at riskNumber at riskPP--R HeparinR HeparinNo PNo P--R HeparinR Heparin
Def
/D
ef/ P
rob
Prob
Sten
tSt
ent T
hrom
bosi
s (%
)Th
rom
bosi
s (%
)
0.00.0
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
3.53.5
Time in HoursTime in Hours00 66 1212 1818 2424
PrePre--Randomization HeparinRandomization HeparinNo PreNo Pre--Randomization HeparinRandomization Heparin
UFH+GPI UFH+GPI
UFH+GPIUFH+GPI
12111211 12081208 12071207 12071207 12071207378378 377377 375375 374374 374374
PP--R HeparinR HeparinNo PNo P--R HeparinR Heparin
BivalirudinBivalirudin
BivalirudinBivalirudin
0.1%0.1%
0.8%0.8%HR [95%CI] = 9.64 [1.00,92.70]HR [95%CI] = 9.64 [1.00,92.70]
P = 0.02P = 0.02
0.9%0.9%
2.6%2.6%
HR [95%CI] = HR [95%CI] = 3.07 [1.33,7.09]3.07 [1.33,7.09]
P = 0.006P = 0.006
PPintint antithrombinantithrombin x prex pre--rand rand hephep = 0.39= 0.39

1.6% 1.6%
3.4% 3.4%
1.5%1.5%
1.2%1.2%
HR [95%CI] =HR [95%CI] =1.30 [0.541.30 [0.54--3.16]3.16]
P = 0.56P = 0.56
HR [95%CI] =2.11 HR [95%CI] =2.11 [1.07,4.17][1.07,4.17]P = 0.03P = 0.03
10131013519519
10091009 990990 969969 957957 943943 863863514514 497497 486486 480480 474474 430430
Number at riskNumber at risk600 mg600 mg300 mg300 mg
Def
/D
ef/ P
rob
Prob
Sten
tSt
ent T
hrom
bosi
s (%
)Th
rom
bosi
s (%
)
00
11
22
33
44
55
Time in DaysTime in Days00 11 3030 9090 180180 270270 365365
StentStent Thrombosis 1Thrombosis 1--Day Landmark Analysis:Day Landmark Analysis:Impact of Impact of ClopidogrelClopidogrel Loading (Loading (BivalirudinBivalirudin))
600mg 600mg ClopidogrelClopidogrel300mg 300mg ClopidogrelClopidogrel

600mg 600mg ClopidogrelClopidogrel300mg 300mg ClopidogrelClopidogrel
2.8% 2.8% 2.9%2.9%
0.4%0.4%
0%0%
HR=0.21 HR=0.21 CI=0.01CI=0.01--3.883.88
P = 0.30P = 0.30
HR=1.08 HR=1.08 CI= [0.57,2.05]CI= [0.57,2.05]
P = 0.81P = 0.81
10351035559559
10341034 995995 977977 963963 951951 852852557557 537537 531531 528528 521521 482482
Number at riskNumber at risk600 mg600 mg300 mg300 mg
Def
/D
ef/ P
rob
Prob
Sten
tSt
ent T
hrom
bosi
s (%
)Th
rom
bosi
s (%
)
00
11
22
33
44
55
Time in DaysTime in Days00 11 3030 9090 180180 270270 365365
PPintint antithrombinantithrombin x x clopidogrelclopidogrel LD = 0.16LD = 0.16
StentStent Thrombosis 1Thrombosis 1--Day Landmark Analysis:Day Landmark Analysis:Impact of Impact of ClopidogrelClopidogrel Loading (UFH+GPI)Loading (UFH+GPI)

Independent Predictors of 1Independent Predictors of 1--Year ST Year ST (Cox Model)(Cox Model)
Variable HR [95% CI] P-value
Insulin-treated diabetes 3.42 [1.81, 6.47] 0.0002
Lesion ulceration 2.28 [0.99, 5.27] 0.05
Pre-PCI TIMI flow 0/1 2.22 [1.37, 3.61] 0.001
Current smoking 1.81 [1.20, 2.72] 0.005
Number of stents 1.31 [1.07, 1.60] 0.04
Clopidogrel loading dose 600mg 0.65 [0.44, 0.97] 0.04

In the primary results of the HORIZONSIn the primary results of the HORIZONS--AMI trial, AMI trial, bivalirudinbivalirudin monotherapymonotherapy resulted in less major bleeding, resulted in less major bleeding, comparable rates of ischemia and improved survival comparable rates of ischemia and improved survival compared to UFH+GPI at 30 days and 1compared to UFH+GPI at 30 days and 1--yearyearThe results of the present analysis suggest that The results of the present analysis suggest that optimizing adjunct pharmacology with optimizing adjunct pharmacology with bivalirudinbivalirudin during during primary PCI may further improve outcomes:primary PCI may further improve outcomes:–– PrePre--randomization UFH attenuated the risk of acute STrandomization UFH attenuated the risk of acute ST–– A 600 mg A 600 mg clopidogrelclopidogrel LD attenuated the risk of LD attenuated the risk of subacutesubacute STST
Whether a prolonged Whether a prolonged bivalirudinbivalirudin infusion (4infusion (4--6 hrs) post6 hrs) post--PCI and/or an even more potent and rapid acting PCI and/or an even more potent and rapid acting thienopyridinethienopyridine agent might further reduce early ST in pts agent might further reduce early ST in pts with STEMI treated with with STEMI treated with bivalirudinbivalirudin (without increasing (without increasing bleeding) warrants further studybleeding) warrants further study
ImplicationsImplications

Vascular Responses after Vascular Responses after PaclitaxelPaclitaxel--eluting eluting and Bare Metal and Bare Metal StentStent Implantation in Acute Implantation in Acute
Myocardial InfarctionMyocardial Infarction
-- The HORIZONSThe HORIZONS--AMI IVUS AMI IVUS SubstudySubstudy --
Akiko Maehara, Gary S. Mintz, Alexandra J. Lansky, Akiko Maehara, Gary S. Mintz, Alexandra J. Lansky, Bernhard Witzenbichler, Giulio Guagliumi, Bruce Brodie, Bernhard Witzenbichler, Giulio Guagliumi, Bruce Brodie,
Helen Parise, Roxana Mehran, and Gregg W. StoneHelen Parise, Roxana Mehran, and Gregg W. Stone
For the HORIZONFor the HORIZON--AMI IVUS AMI IVUS SubStudySubStudy InvestigatorsInvestigators
BackgroundNo consensus exists regarding efficacy and safety of drug-eluting stents (DES) in pts with STEMI undergoing primary PCI–The safety of implanting DES in thrombus
containing ruptured plaques with the potential for subsequent late acquired stent-vessel wall malapposition (positive remodeling, thrombus dissolution) has been questioned
No large-scale IVUS study has been performed to address the underlying vascular responses to bare metal or in this clinical setting
No consensus exists regarding efficacy and safety of drug-eluting stents (DES) in pts with STEMI undergoing primary PCI–The safety of implanting DES in thrombus
containing ruptured plaques with the potential for subsequent late acquired stent-vessel wall malapposition (positive remodeling, thrombus dissolution) has been questioned
No large-scale IVUS study has been performed to address the underlying vascular responses to bare metal or in this clinical setting

HHarmonizing armonizing OOutcomes with utcomes with RRevascularevascularizizatiationon and and SStentstents inin3602 pts with STEMI with symptoms onset3602 pts with STEMI with symptoms onset <12 hours<12 hours
UFH+GP UFH+GP IIb/IIIaIIb/IIIa inhibitorinhibitor((abciximababciximab or or eptifibatideeptifibatide))
BivalirudinBivalirudinmonotherapymonotherapy((±± provisional GP provisional GP IIb/IIIaIIb/IIIa))
R1:1
3006 eligible for Primary PCI with 3006 eligible for Primary PCI with stentstent
Paclitaxcel-eluting TAXUS stent
PaclitaxcelPaclitaxcel--eluting TAXUS eluting TAXUS stentstent
Bare metal EXPRESS stent
Bare metal EXPRESS Bare metal EXPRESS stentstent
R3:1
1800 eligible for 13 month 1800 eligible for 13 month angioangio followfollow--upup
294 TAXUS stent
294 TAXUS 294 TAXUS stentstent
95 BMS stent
95 BMS 95 BMS stentstent196 (67%) FU196 (67%) FU196 (67%) FU 62 (65%) FU62 (65%) FU62 (65%) FU
IVUSIVUSSubstudSubstudyy

IVUS SubStudy Inclusion
IVUS sites were pre-selected based on their desire to participate in this substudy and their agreement to perform baseline and follow-up IVUS on consecutive pts in the angiographic follow-up cohort until at least 300 consecutive IVUS caseswere completed.
Follow-up IVUS was performed at 13 months unless restenosis occurred earlier
IVUS sites were pre-selected based on their desire to participate in this substudy and their agreement to perform baseline and follow-up IVUS on consecutive pts in the angiographic follow-up cohort until at least 300 consecutive IVUS caseswere completed.
Follow-up IVUS was performed at 13 months unless restenosis occurred earlier

Change of EEM Volume
-1
-0.5
0
0.5
1
ProximalEdge
In-Stent Distal Edge
TAXUSBMS
p<0.0001
p=0.59
p=0.092
(mm3/mm2
)
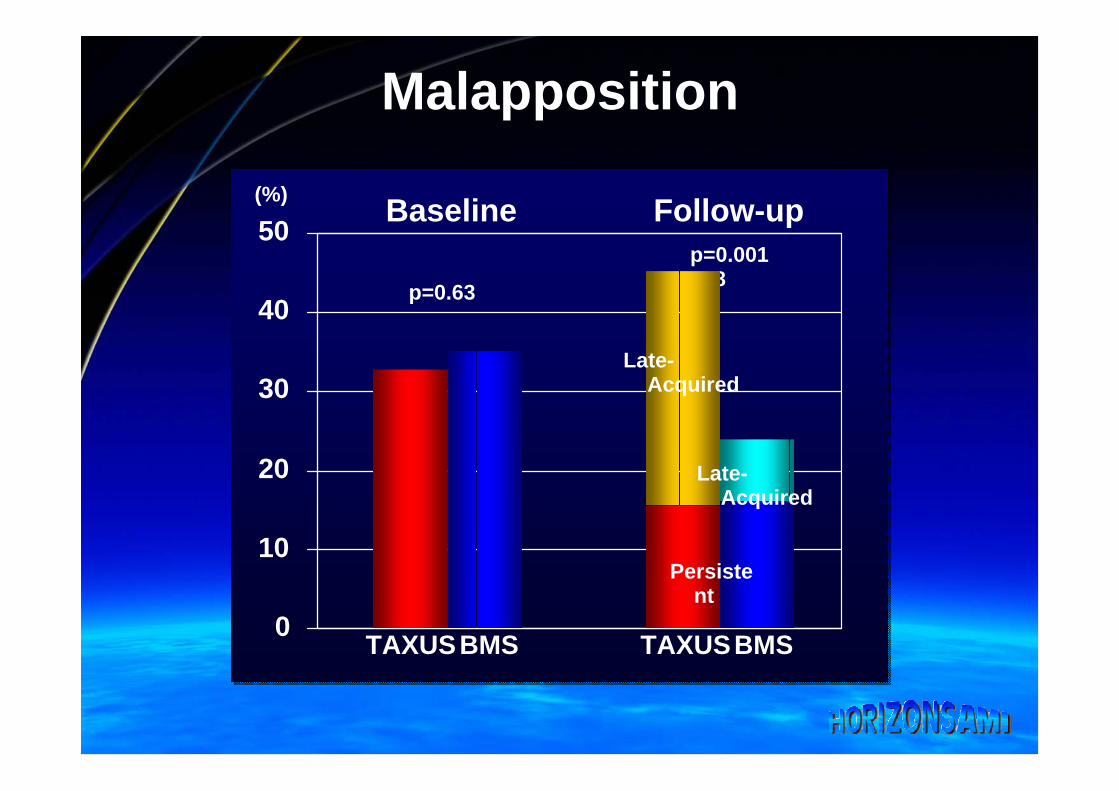
Malapposition
p=0.0018
Baseline Follow-up
0
10
20
30
40
50
p=0.63
Late-Acquired
Late-Acquired
Persistent
(%)
TAXUSBMS TAXUSBMS
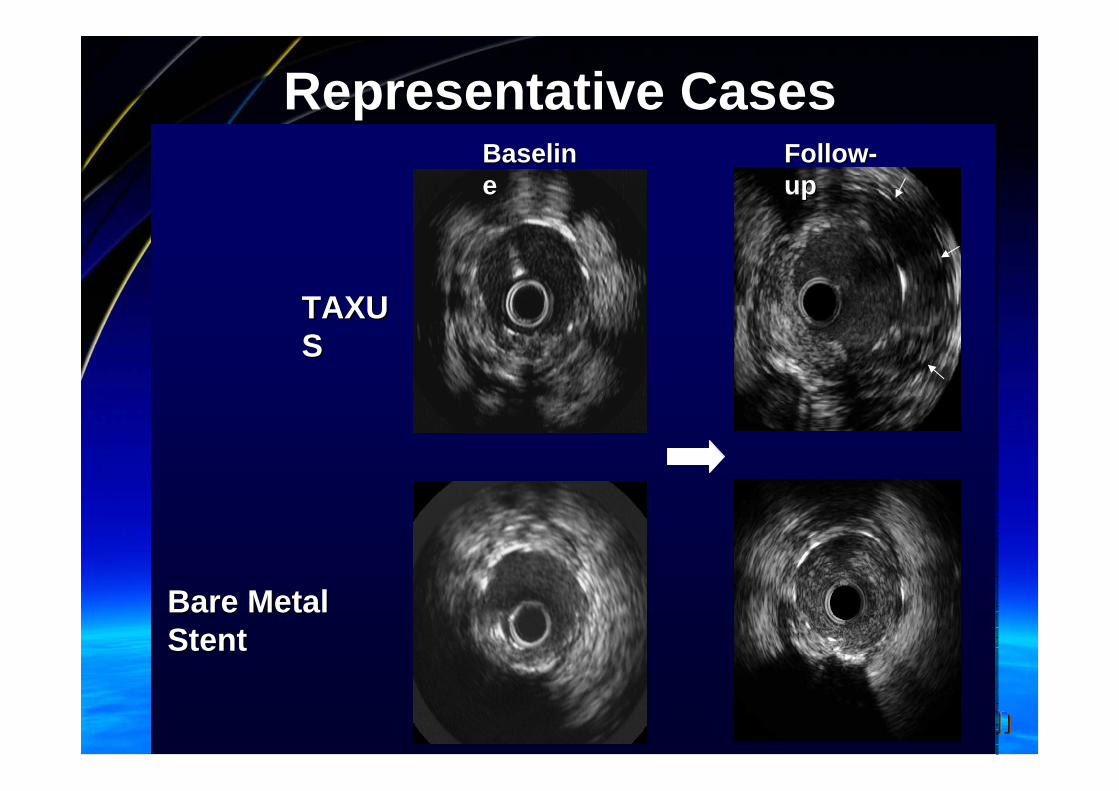
Representative CasesFollowFollow--upup
BaselinBaselinee
Bare Metal Bare Metal StentStent
TAXUTAXUSS

Conclusions
TAXUS significantly reduced 13TAXUS significantly reduced 13--month inmonth in--stentstentneointimalneointimal hyperplasia compared to BMS hyperplasia compared to BMS TAXUS had a higher incidence of lateTAXUS had a higher incidence of late--acquired acquired stentstent--vessel wall vessel wall malappositionmalapposition compared to compared to BMS due to positive remodelingBMS due to positive remodelingApproximately twoApproximately two--thirds of thirds of stentsstents had tissue had tissue protrusion or protrusion or intraluminalintraluminal thrombus thrombus immediately after immediately after stentstent implantation, almost all implantation, almost all of which resolved during followof which resolved during follow--upupNew aneurysm formation and New aneurysm formation and stentstent fracture fracture were uncommon, although seen only in TAXUS were uncommon, although seen only in TAXUS stentsstents

Conclusions
Ongoing long-term follow-up is required
to establish the clinical significance of
these findings
Ongoing longOngoing long--term followterm follow--up is required up is required
to establish the clinical significance of to establish the clinical significance of
these findingsthese findings
Top Related