






Languages
Pages
Legal

KKIINNGGDDOOMM OOFF CCAAMMBBOODDIIAA NNAATTIIOONN –– RREELLIIGGIIOONN ‐‐ KKIINNGG
MMiinniissttrryy ooff HHeeaalltthh
HHeeaalltthh FFaacciilliittyy SSuurrvveeyy iinn CCaammbbooddiiaa 22001100
SSuuppppoorrtteedd bbyy
WWoorrlldd HHeeaalltthh OOrrggaanniizzaattiioonn UUnniitteedd NNaattiioonnss CChhiillddrreenn’’ss FFuunndd
PPhhnnoomm PPeennhh,, MMaayy 22001100

Cambodia Health Facility Survey 2010
2
TABLE OF CONTENTS Preface ..................................................................................................................................................... 4
Study overview ........................................................................................................................................ 5
Glossary ................................................................................................................................................... 8
1. Background ...................................................................................................................................... 9
2. Survey Design .................................................................................................................................. 9
3. Purpose and Objectives ................................................................................................................... 9
4. Primary and secondary outcomes ................................................................................................. 10
5. Ethical review ................................................................................................................................ 10
6. Methods ......................................................................................................................................... 10
6.1. Sampling .............................................................................................................................. 10
Sampling frame ................................................................................................................... 10
Stratification ........................................................................................................................ 11
Definition of the strata ........................................................................................................ 11
Sample size .......................................................................................................................... 12
Randomization .................................................................................................................... 12
6.2. Data collection instruments ................................................................................................ 14
Observations of sick child management: ............................................................................ 14
Re‐examination of the sick child by the assessors: ............................................................. 14
Interviews with child caretakers: ........................................................................................ 14
Review of facility supports: ................................................................................................. 14
6.3 Data collection ..................................................................................................................... 15
6.4 Data Entry and Analysis ....................................................................................................... 15
7. Results ........................................................................................................................................... 16
7.1 Description of the sample ................................................................................................... 16
7.2 Facility supports for IMCI .................................................................................................... 17
Availability of essential drugs and supplies ......................................................................... 18
IMCI training status of health workers ................................................................................ 21
Supervision .......................................................................................................................... 23
Referral practices ................................................................................................................ 23
Administration ..................................................................................................................... 24
7.3 Management of the young infant 0‐2 months of age ......................................................... 27
Age at presentation ............................................................................................................. 27
Reason for presentation ...................................................................................................... 27
Performance of key tasks by the Health Worker ................................................................ 28
Assessment of the young infant .......................................................................................... 29
Classification of young infants ............................................................................................. 30
Treatment of young infants ................................................................................................. 31
Counseling of the mother .................................................................................................... 31
7.4. Management of children aged 2 to 59 months ................................................................... 34
Assessment of sick children ................................................................................................. 34
Index of integrated assessment .......................................................................................... 36
Feeding assessment for children under 2 years .................................................................. 37
Management of children with diarrhoea ............................................................................ 38
Management of children with pneumonia ......................................................................... 39
Cambodia Health Facility Survey 2010
3
General tasks ....................................................................................................................... 40
Questions to the mother ..................................................................................................... 41
8. Comparison of IMCI and IMCI ++ facilities .................................................................................... 43
9. Comparison of 2010 HFS and 2006 HFS ........................................................................................ 48
10. Conclusions .................................................................................................................................... 51
11. Draft Recommendations from findings of the Health Facility Survey 2010 .................................. 54
11.1. Specific recommendations: ................................................................................................. 54
IMCI Training ....................................................................................................................... 54
IMCI Implementation .......................................................................................................... 55
11.2. Further suggested operations researcH .............................................................................. 56
11.3. Acknowledgments .............................................................................................................. 57
Annex 1 ‐ Data Tables ............................................................................................................................ 58
Preliminary results: description of the sample ................................................................... 58
Supplemental measures ...................................................................................................... 66
Additional indicators and information ................................................................................ 68
Sick young infants ‐ summary results .................................................................................. 80
Annex 2: List of surveyors. Cambodia HFS, May 2010 ......................................................................... 85
Additional information available on request from WHO Cambodia:
1) Study Instruments
2) Sample size, precision and issues relating to clustering
3) Completed data tables
4) Final sample of facilities surveyed
5) Surveyor Training Workshop Agenda
6) List of participants
Cambodia Health Facility Survey 2010
PREFACE
The improvement of health care services delivered at health facilities and theenhancement of the public facility utilization is one of the major health priorities. TheIntegrated Management of Childhood Illness (IMCI) strategy was adopted by the Ministry ofHealth in 1996 in order to improve the quality of care for sick children delivered at first levelhealth facilities, and the early implementation of the IMCI strategy started in 2001 in twopilot operational districts. Currently, IMCI is implemented country-wide. Therefore, it is an
appropriate time to evaluate the results and quality of our efforts and to determine thestrategic direction for further investment.
Whilst waiting for the result of the Cambodia Demographic and Health Survey(CDHS) 2010 (data collection currently underway), which is expected to show progress
including the improvement in reducing maternal mortality as the result of the joint effortbetween the Ministry of Health and its health development partners, the Cambodia HealthFacility Survey (HFS) 2010 provides findings from an evaluation focusing on the quality ofcare provided by the first level health facilities. This is the second suryey with the first HFShaving been conducted in early 2006.
The results of the Cambodia HFS 2010 will serve as a basis for determiningpriorities and strategies for improving the quality of care delivered at health center level as
well as planning and strengthening clinical training for health staff responsible for providingcare for children. The findings will be used for continued improvement in implementing theintegrated approach in case management and the health system support to ensure the qualityand sustainability of the implementation at health facility level. f
Prof. Eng Huol
Secretary of State for Heal&

Cambodia Health Facility Survey 2010
5
STUDY OVERVIEW
Title Cambodia Health Facility Survey (HFS) 2010
Study design Facility-based cross sectional, national survey
Principal Investigator
Prof. San Chan Soeung, Deputy-Director General for Health, Chair, CSMC, Chair RMNCH Taskforce
Co-Investigators Dr Hong Rathmony, Deputy-Director, Communicable Disease Control Department, Ministry of Health
Dr Bun Sreng, Head, Communicable Disease Control and Prevention Bureau, CDC Department, Ministry of Health
Dr Sieng Nam, Health Officer, UNICEF, Cambodia
Dr Susan Jack, Medical Officer, WHO, Cambodia
Partners Ministry of Health, Department of Communicable Disease Control (CDC)
United Nations Children’s Fund
World Health Organization
Abstract
Study Design:
This cross sectional survey of 120 randomly selected health centres across Cambodia assessed the quality of care delivered to sick children at health centres (first level health facilities) using locally adapted standard instruments. The survey compared quality of care for sick children in facilities receiving financial incentives for IMCI implementation, facilities implementing IMCI with current level of health system support, and facilities not implementing IMCI. It was the first Health Facility Survey to include an assessment of care for infants younger than 2 months by case observation.
Findings:
IMCI training coverage is very high. Key health system supports such as essential medicines, equipment, and supervision are generally available, although there are deficiencies in supply of injectable antibiotics and drugs for obstetric emergencies. Health workers display an integrated approach to care and the quality of care provided to children is significantly better in IMCI facilities over non-IMCI facilities. The assessment, classification and treatment of young infants needs improvement – children with possible serious infections are often unrecognized and treated incorrectly. For older children, a number of case management tasks were done well by IMCI trained staff, including, classification of pneumonia and

Cambodia Health Facility Survey 2010
6
diarrhoea and treatment of diarrhoea with ORS.
Gaps were also noted in key areas, including limited assessments of danger signs and feeding, incorrect treatment of pneumonia and failure to use zinc to treat diarrhoea, and inadequate counseling of caretakers in several areas. Hand-washing was very rarely practiced. Missed opportunities to vaccinate children were common. Supervisory visits happen regularly but supportive supervision that includes case observation and problem solving is not usually done. Financial incentives for IMCI implementation resulted in considerably more sick children being managed using IMCI, and improvements in some elements of case management practice. Since the last health facility survey in 2006, health systems support has significantly improved, and IMCI has reached almost national coverage while quality of IMCI implementation has remained un-changed. Recommendations or further improving quality of care were outlined.
Summary of main findings – Cambodia HFS, May 2010
1) Key Health System’s supports for IMCI implementation are widely available although a few important gaps remain.
2) IMCI facilities provide better quality of care than non-IMCI facilities.
3) Incentivized IMCI facilities are more likely to use the IMCI approach when
seeing sick children, and perform better than standard IMCI facilities for some indicators.
4) Care for the young infant is suboptimal.
5) Assessment for danger signs is often not done.
6) Treatment practices for diarrhoea and pneumonia need improvement.
7) Counseling of mothers needs improvement, especially on danger signs
requiring immediate return to a health facility.
8) Supervision does not usually include observation of practice and problem solving.
9) Missed opportunities to vaccinate are common.
10) Hand-washing is rarely performed by health workers seeing sick children.
Cambodia Health Facility Survey 2010
8
GLOSSARY
CDHS Cambodia Demographic and Health Survey
HC Health Centre
HEFs Health Equity Fund(s)
HFS Health Facility Survey
HHS Maternal, Newborn and Child Health Household Survey
HW Health Worker
IMCI Integrated Management of Childhood Illness
IMCI++ Facility receiving (from an NGO) case-based incentives for practicing IMCI
MoH Ministry of Health
MPA Minimum Package of Activities (Health services required by MoH to be delivered by a facility)
OD Operational District
ORS Oral Rehydration Solution
PHD Provincial Health Department
SOA Special Operating Agency (contracted by MoH to deliver health services)
UNICEF United Nations Children’s Fund
WHO World Health Organization

Cambodia Health Facility Survey 2010
9
1. BACKGROUND
The integrated Management of Childhood Illness (IMCI) strategy was begun in Cambodia in 2001 and has been gradually expanded after the review of the early implementation in 2002. A health facility survey to evaluate quality of care provided by IMCI trained health workers was conducted in 2006. This survey found that facilities with IMCI trained health staff were performing better than those without IMCI training, and made several recommendations for further improving the quality of care, including strengthening drug supply and supervision.
IMCI is now being implemented in over 82% of first-level health facilities in the country. Since 2007 a new financial incentive mechanism is in place as part of a GAVI initiative (IMCI++). High coverage and the new financial incentive scheme prompted a re-assessment of quality integrated sick child care at first-level outpatient health facilities, to evaluate how well IMCI trained health workers are performing, and to assess whether the financial incentive scheme has improved performance.
2. SURVEY DESIGN
The survey was a nationally representative cross sectional survey of randomly selected health centres, designed to provide descriptive data about the quality of care delivered to sick children at first level health facilities in Cambodia.
3. PURPOSE AND OBJECTIVES
This survey was designed to provide Ministry of Health and health development partners data on the quality of care delivered to sick children attending health centres.
The purpose of the survey was to use data on quality of sick child care to:
1. Prioritize and plan strategies for improving the quality of care provided at the first level health facilities, including: case-management practices, drugs and supplies, supervisory practices, equipment needs, staffing and health centre organization.
2. Plan and strengthen IMCI training for health staff responsible for caring
for children. 3. Improve or develop strategies for supervision and monitoring of IMCI
implementation.
Cambodia Health Facility Survey 2010
10
The objectives of the survey were to assess:
1. Quality of health care services provided at health facilities for sick children under-5 years, including young infants 0-2 months of age, using IMCI technical standards.
2. Availability of key health system supports that are required for the
implementation of sick child services (drugs, vaccines, equipment, and supervision).
3. Barriers to effective integrated case management for sick children.
4. PRIMARY AND SECONDARY OUTCOMES
The primary outcome being evaluated was:
Is there a difference in the quality of care provided between IMCI versus non-IMCI
facilities?
The secondary outcomes being evaluated were:
Is there a difference in the quality of care provided between IMCI trained facilities
versus IMCI trained facilities receiving financial incentives for IMCI implementation?
What is the quality of newborn and young infant care in health centres?
5. ETHICAL REVIEW
The Human Research Ethics Committee of the Ministry of Health, Royal Government of Cambodia approved this survey, and permission to access health centres was granted by the Ministry. Verbal informed consent was provided by caregivers, and they were given a plain language statement explaining the survey.
6. METHODS
6.1. SAMPLING
Sampling frame
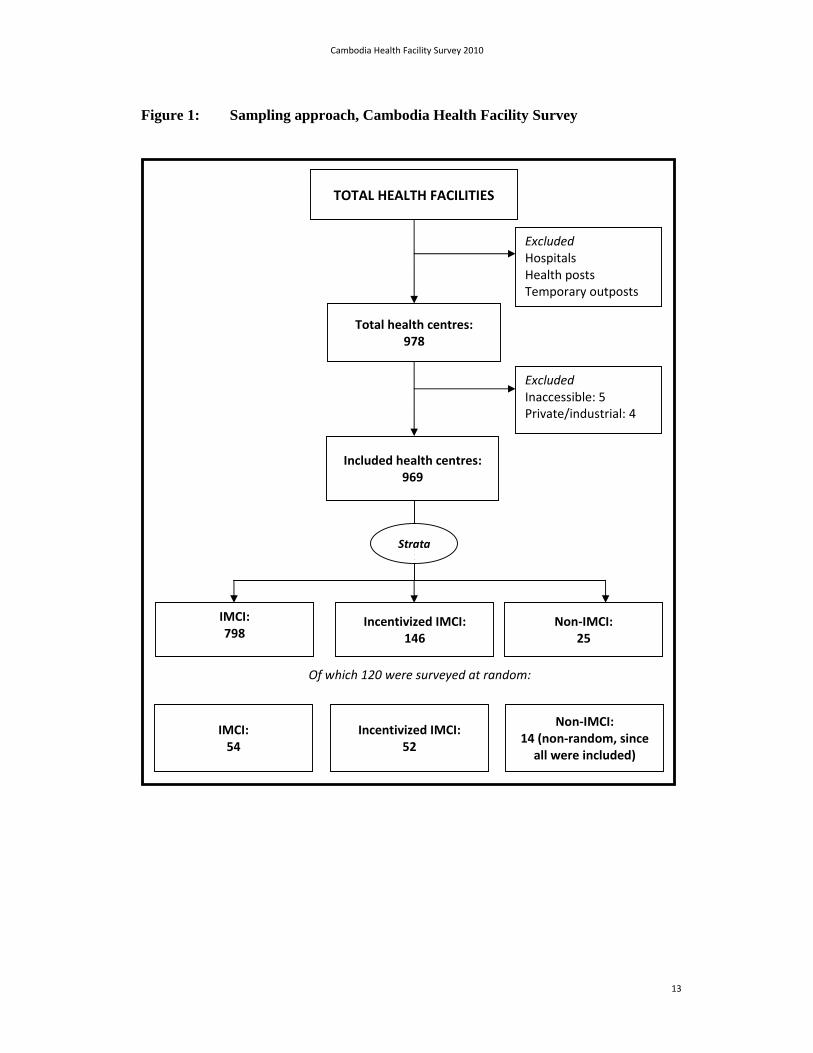
The sampling method is summarized in Figure 1. All functional health facilities in the country were listed. Hospitals, health posts and temporary outposts were then excluded.

Cambodia Health Facility Survey 2010
11
Health centres that could not be reached within a 1 day drive from any other health centre were also excluded; current accessibility was checked with local health centre staff. Five health centres were excluded on the basis of accessibility (1 health centre was on an offshore island, 1 a 6 hour drive from the nearest health centre, 1 accessible only to military vehicles, and 2 did not have road access and were accessible only by cross-country motorcycle). In addition, health centres run by industry (such as plantations) and privately run clinics, were excluded.
The Ministry of Health requires health centers to be capable of providing a Minimum Package of Activities (MPA). Health centers are classified as full MPA or not. This survey included all health centres, regardless of whether or not they were full MPA centres or not.
Stratification
Stratification of facilities was based on degree of IMCI support. Three strata were defined: IMCI, IMCI with incentives (henceforth IMCI++) and non-IMCI.
Definition of the strata
1. The definition of IMCI facilities were those where at least 2 health workers had been trained in IMCI. A facility in which only one health worker had been trained in IMCI was classified as a non-IMCI facility. Prior to the survey the MoH updated its list of non-IMCI facilities. During the survey, 11 facilities that had been classified as non-IMCI were found to have become IMCI practicing facilities. Although 25 non-IMCI facilities had been selected, the final sample contained only 14. Facilities that had been selected as a part of the non-IMCI group, but which were found to be practicing IMCI when visited, were excluded from the sample.
2. IMCI ++ facilities were IMCI facilities that in addition received specific financial incentives for IMCI implementation. In IMCI ++ facilities payments are received for each IMCI case reporting form completed. Other types of general financial support may be received by IMCI implementing facilities that is not specific for IMCI, such as Service Delivery Grants (SDGs) in areas with Special Operating Agencies (SOA’s) as well as standard support from the MoH or health development partners.
3. Non-IMCI facilities referred to facility with one or fewer IMCI trained health workers. For this reason, it was possible that children coming to facilities classified as non-IMCI were seen by IMCI trained health workers.

Cambodia Health Facility Survey 2010
12
Sample size
This survey was designed to detect differences between IMCI and non-IMCI facilities as the primary outcome, and to detect differences between IMCI and IMCI ++ facilities, as the secondary outcome. Rates for were estimated for all young infants combined. Some comparisons between IMCI (either type combined) and non-IMCI facilities were also possible for the subset of young infants.
The total estimated sample size was 120 facilities. This sample size assumed about 50 facilities in each IMCI group and about 20 non-IMCI facilities. Based on the HFS 2006 it was assumed that 3.5 children per facility would be seen. These assumptions had 80% power to detect a difference of 8 to 20% in specific indicators between IMCI and non-IMCI facilities with estimated proportions of 99% and 50% respectively. For the secondary outcome (differences between IMCI and incentivized IMCI facilities), it was calculated that 50 facilities of each type would allow a detectable difference of between 7 and 16% with estimated proportions of 99% and 50% respectively. For the secondary outcome of young infants, precise estimates were obtainable if at least 30 infants were included. No comparisons across strata were planned for young infants. The effect of stratification (clustering) was not considered in calculating sample size. This is because the strata were themselves the unit of comparison and any differences in variance would be accounted for in hypothesis testing. Logistics considerations also determined sample size – 120 facilities could be visited by twelve teams 3 surveyors in 2 weeks. Further details regarding sample size, precision and clustering are given in the HFS planning documents, available on request from MoH or WHO.
Randomization
Randomisation was performed separately for each stratum (IMCI, IMCI++, non-IMCI). Facilities in each strata were listed by district and selected using systematic random sampling.
Cambodia Health Facility Survey 2010
13
Figure 1: Sampling approach, Cambodia Health Facility Survey
Excluded Inaccessible: 5 Private/industrial: 4
TOTAL HEALTH FACILITIES
Excluded Hospitals Health posts Temporary outposts
Included health centres: 969
IMCI: 798
Incentivized IMCI: 146
Non‐IMCI: 25
IMCI: 54
Incentivized IMCI: 52
Non‐IMCI: 14 (non‐random, since all were included)
Of which 120 were surveyed at random:
Strata
Total health centres: 978

Cambodia Health Facility Survey 2010
14
6.2. DATA COLLECTION INSTRUMENTS
Study questionnaires were adapted from the Cambodia Health Facility Survey 2006 which was based on the WHO IMCI Health Facility Survey guidelines1. This survey method compares health worker practices against the IMCI clinical guidelines for first level-health facilities. In 2007 the Cambodia IMCI guidelines were revised to include the sick young infant 0-2 months, and for this survey, the young infant (0-2 months) assessment form was used when required. Some additional questions regarding water and sanitation and waste management were also added.
Data collection instruments are summarized below:
Observations of sick child management:
Health centre (HC) staff were observed managing sick children. Surveyors completed a structured observation questionnaire (form 1) which included information on the HC staff being observed; the sick child being observed; assessment, classification, treatment and counseling tasks completed by the health worker. Data were collected by surveyors who had been trained in the use of form 1.
Re-examination of the sick child by the assessors:
Clinical re-examination was done by an experienced IMCI trained physician using a structured questionnaire (form 3), to determine the ‘gold-standard’ classification of the child according to the IMCI clinical guidelines. This standard was used to check whether or not the health worker classified and treated the child correctly.
Interviews with child caretakers:
Surveyors conducted exit interviews with child caretakers using a structured questionnaire (form 2), to determine whether messages given by health workers were understood, and to collect information on caretaker satisfaction. Data from these interviews help determine how well counseling was conducted.
Review of facility supports:
Following interviews with HC staff, surveyors directly observed the availability of equipment and supplies, drugs and vaccines, facility services, and records (form 4).
1 WHO 2003. Health Facility Survey: Tool to evaluate the quality of care delivered to sick children attenting outpatients facilities (using IMCI clinical guidelines as best practices). WHO, Geneva.
Cambodia Health Facility Survey 2010
15
6.3 DATA COLLECTION
Surveyors were IMCI facilitators who had received IMCI refresher training with updated IMCI guidelines. Thirty-two survey staff were trained in Siem Reap between 17-21 May 2010. Training involved an explanation of survey objectives, survey procedures and instruments. Instruments were reviewed by the group. Surveyors reached consensus on how to interpret questions. IMCI clinical training was also reviewed. An inter-surveyor reliability of 96% on all survey instruments was achieved at the end of training. A list of surveyors is provided in Annex 2.
Twelve survey teams were deployed. Each team consisted of 3 members (2 surveyors and a supervisor). One member of each team was an experienced physician (usually a paediatrician) who performed the exit interview and clinical re-examination of each case. The other surveyor observed case management by the health worker. The supervisor was involved in identifying and recruiting eligible children, assessing availability of equipment and drugs and was responsible for data quality and completeness.
The duration of data collection was 10 working days. To minimize bias, surveyors were deployed to assess facilities away from their home province.
Health Centers were notified that an assessment would be conducted within a 2-week period, but were not given the exact date. Upon arrival at the centre, the health worker who was responsible for seeing sick children on that day was assessed regardless of whether that health worker was IMCI trained or not. Care was taken that surveyors observed routine practices, as they would normally take place.
6.4 DATA ENTRY AND ANALYSIS
Data entry and analysis were conducted using the Epi-Info version 3.5.1. Questionnaire data were entered and cleaned by an information technology expert at the Ministry of Health. At least 50% of the data were double entered for accuracy checking. Analysis was conducted at an analysis capacity building workshop by a group of previously trained data analysts under guidance of WHO technical facilitators.
Standard indicators were calculated. Analysis compared any IMCI versus non-IMCI facilities; and IMCI ++ versus standard IMCI facilities. Data on the young infant 0-2 months were pooled to provide coverage indicators for quality of young infant care, but comparisons across strata were not conducted.
Comparisons of means were performed with the 2-tailed t-test assuming unequal variances. Comparisons of proportions used the 2-test, except for young infants where the Fisher’s Exact test was used because of small numbers. Corrections for multiple testing were not performed. Only a limited number of comparisons were formally tested. Caution should be exercised when interpreting multiple hypothesis tests. This is
Cambodia Health Facility Survey 2010
16
discussed further in the results secion. Interval estimation for binomial proportions use Wilson confidence intervals2. Data tables are summarized in Annex 1.
7. RESULTS
7.1 DESCRIPTION OF THE SAMPLE
The final sampling frame was 969 primary health centres. One hundred and twenty health centres were visited for this survey. All non-IMCI facilities were selected (N=14). A total of 425 children 2 to 59 months of age were observed, and 34 infants 0-2 months. An average of 3.8 children were seen per facility, including young infants. The breakdown of the final sample is shown in Table 1.
Table 1: Final sample of health facilities and children, Cambodia HFS, May 2010
Facility type
Total IMCI IMCI++ non-IMCI
Health Centres 54 52 14 120
Children 2mth-5y 178 208 39 425
Infants <2mth 16 13 5 34
Ages of children seen at health facilities is shown in Figure 2. A high proportion of children seen were in their first 2 years of life. Relatively few neonates (infants in their first month of life) were seen, although there was a spike in visits by children at 2 months. The age histogram shows age-heaping at 6-month multiples. This is most likely to have resulted from recording child ages as reported by the caregiver (“18 months old”, “3 years old”, etc) rather than the actual date of birth. This has no impact on the analysis in this survey, and it could be assumed that age-heaped children would be normally distributed around the given age. If desired, the degree of age heaping can be assessed using the Whipple’s index or Myers’ blended index3.
2 See Brown LD, Cai TT and DasGupta A, Interval Estimation for a Binomial Proportion. Statistical Science 2001; 16:101 and associated commentary papers published there. 3 Siegel JS & Swanson DA The Methods and Materials of Demography, 2ed, Elsevier 2004, San Diego.

Cambodia Health Facility Survey 2010
17
Figure 2: Ages of children seen at health centres, Cambodia HFS, May 2010
7.2 FACILITY SUPPORTS FOR IMCI
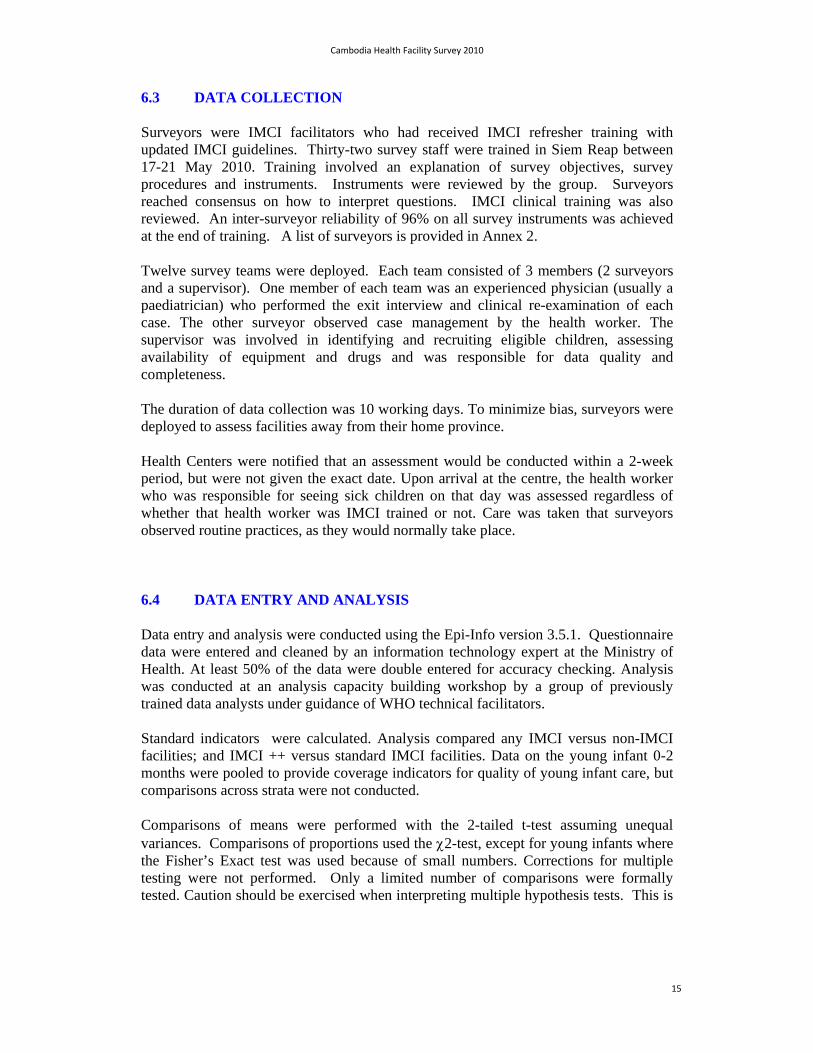
Findings on opening hours and number of children seen in the previous month are shown in Figures 3 and 4. Most facilities reported being open during the morning at least 5 days a week, and that they provided after hours services. There was no difference between IMCI, IMCI ++, or non-IMCI facilities. Across all facilities (IMCI and non-IMCI), an average of 150 children under five were seen per month (roughly 5 per day). Of these just under half were in the first year of life, but very few were newborns. These data concur with the age distribution of children seen during survey visits.
Figure 3: Average days child health services are provided, Cambodia HFS, May 2010
010
20
30
num
ber
0 12 24 36 48 60age in months
Age of children
0
1
2
3
4
5
6
7
child health services provided immuninzation services provided
days
per
wee
k
IMCI IMCI ++ Non IMCI
Cambodia Health Facility Survey 2010
18
Figure 4: Number of child consultations in the previous month, Cambodia HFS, May 2010
Availability of essential drugs and supplies
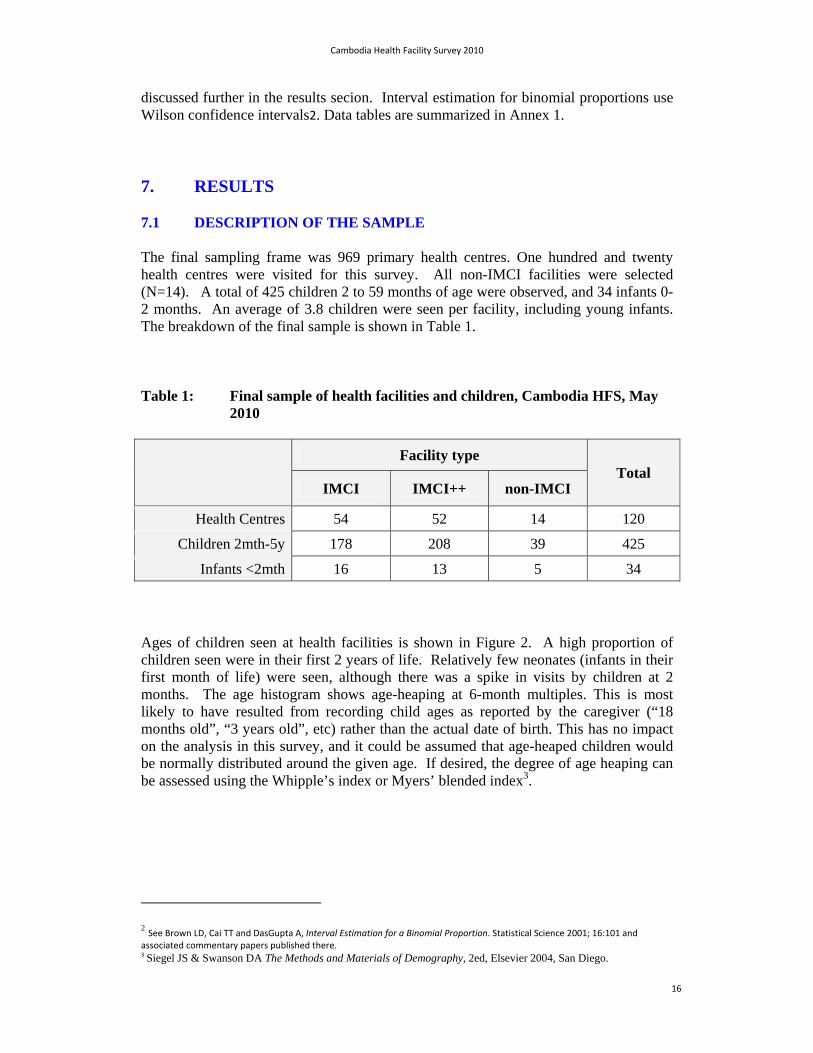
Findings on the availability of essential drugs and vaccines are shown in Figures 5 and 6. Most facilities had ORS and oral antibiotics available. A lower proportion of facilities (42%-75%) had pre-referral antibiotics available (injectible ampicillin and gentamicin). Ciprofloxacin was introduced as first-line treatment for dysentery in 2008, but was available in 42% - 69% of facilities. Very few facilities had quinolone ear drops - which reflects a problem with procurement at the national level. Zinc was available in 35% to 62% of facilities, although it is now part of the first line treatment for watery diarrhea. Availability of injectible antibiotics, ciprofloxacin, and zinc was higher in IMCI++ facilities. Magnesium sulfate (for the management of eclampsia) was present in a low proportion of facilities; oxytocin was available in over 90%.
Figure 5: Availability of essential drugs, Cambodia HFS, May 2010
Drug availability
0
10
20
30
40
50
60
70
80
90
100
Parac
etam
ol
ORS
Cotrim
oxaz
ole
Amox
ycilli
n
Ciproflo
xacin
Vitamin A
Zinc
Quino
lone
Ear D
rops
Antim
alar
ial d
rugs
Ampicil
lin in
j
Gen
tamicin in
j
Diaze
pam in
j
Oxy
tocin
Mag
nesiu
m S
ulph
ate
perc
ent
IMCI IMCI ++ Non IMCI
0
20
40
60
80
100
120
140
160
Under 5 years Newborn (<1 month)
1-3 months Infants (<12 months)
Immunization
num
ber
of c
onsu
ltatio
ns
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
19
The 7 essential oral drugs for IMCI are ORS, antibiotics for pneumonia and dysentery, mebendazole, vitamin A, iron and paracetamol. Their availability is not statistically different for the three survey groups. The index of availability of essential oral drugs is a measure of the proportion of the 7 expected drugs, multiplied by ten. On average, facilities had about .65 of essential oral drugs available on the day of the survey. The 6 required vaccines include BCG, DPT (including DPT-HepB or pentavalent vaccine), OPV, measles, HepB, and TT.
Figure 6: Availability of 7 essential oral drugs and 6 vaccines, Cambodia HFS, May 2010
Table 2: Availability of 7 essential drugs by IMCI status, Cambodia HFS, May 2010
Survey group Proportion of facilities with 7
essential drugs available Index of availability of 7 drugs
IMCI 55.6% (41.9-69.2) 6.50 (6.3-6.7)
IMCI++ 63.5% (49.9-77.0) 6.50 (6.3-6.7)
Non-IMCI 42.9% (13.2-72.5) 6.43 (6.1-6.7)
Availability of essential equipment is shown in Figure 7. Diagnostic tests for malaria were available in 62 – 79% of health centres, though only 7 facilities are located in malaria endemic areas. The national policy for malaria is for all health centres in endemic areas to have diagnostic tests available (rapid tests or microscopy). In addition, health centres that were former district hospitals in any area should be able to diagnose malaria through microscopy. Intravenous fluids and related equipment are generally available present, but nasogastric tubes are mostly lacking in IMCI facilities,
0
10
20
30
40
50
60
70
80
90
100
All 7 essential oral treatments available All 6 vaccines available
perc
ent
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
20
and were not available in non-IMCI facilities. Nasogastric tubes are particularly important for the provision of ORS to children with dehydration for whom intravenous access might be difficult or to have failed.
Figure 7: Availability of essential equipment, Cambodia HFS, May 2010
Availablity of hand-washing facilities and medical waste disposal is summarized in Figure 8. Although water was universally available in health centres, it was often not accessible in the room in which children were seen. Health workers generally did not wash their hands before seeing cases – handwashing was done by 4% of health workers in IMCI facilities, 6% of health workers in IMCI ++ facilities and by no health workers at non-IMCI facilities. This is a significant problem that should urgently be addressed. Incineration of medical waste occurs in about two thirds of IMCI health centres, but only in one third of non-IMCI facilities. Further details regarding the methods of waste disposal may be found in the data tables in the annex.
Figure 8: Availability of hand-washing facilities and medical waste disposal, Cambodia HFS, May 2010
0
10
20
30
40
50
60
70
80
90
100
functioning source of water
water tank on roof handwashing facilities inside
the HC
soap next to handwashing
area
Burnt medical waste in
incinerator
perc
ent
IMCI IMCI ++ Non IMCI
0
10
20
30
40
50
60
70
80
90
100
Dipstick for malaria Nasogastric tube IV fluids IV giving sets
per
cent
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
21
IMCI training status of health workers
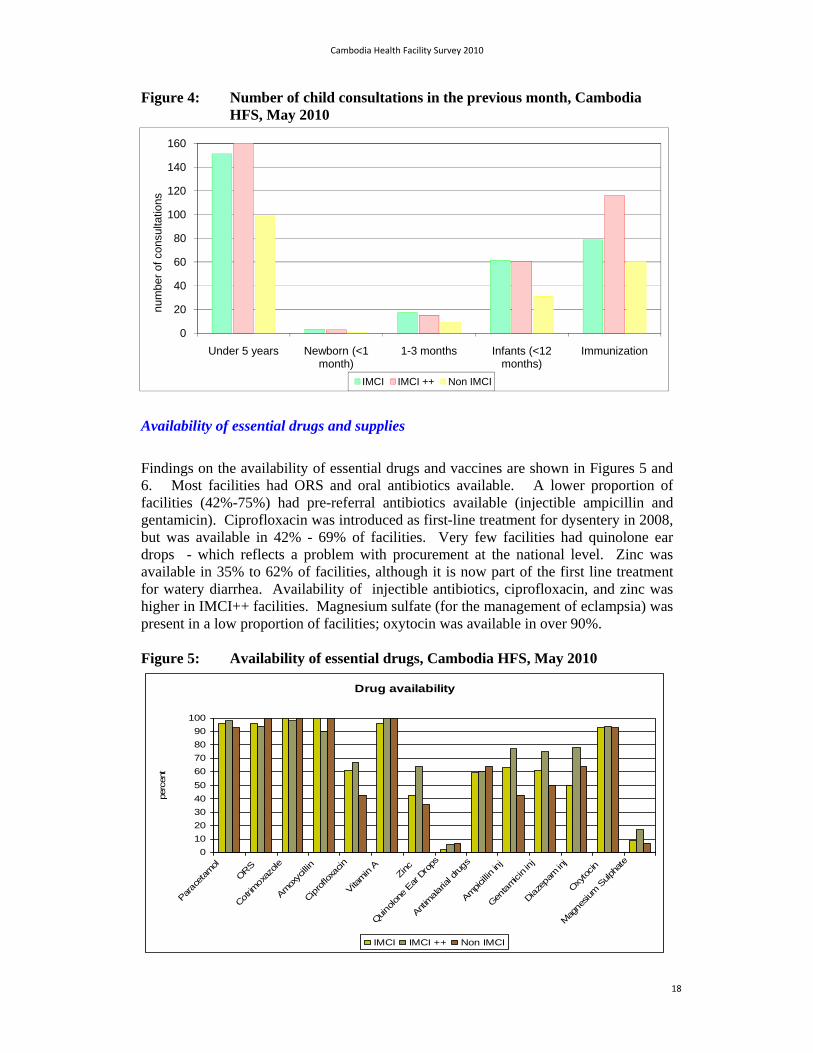
IMCI training status of health workers seeing sick children is summarized in Figures 9, 10 and 11 and table 3. Training status for nutrition, newborn resuscitation and other trainings are shown in the data annex. Children attending health centres are usually seen by nurses or midwives. In Cambodia a secondary midwife has had 4 years of training and a primary midwife has 1 year. Likewise, secondary nurses train for 3 years, and primary nurses for 1 year. Medical assistants’ training is 5years. Of the nurses and midwives who usually saw children at the surveyed facilities, the proportion that had been trained in IMCI is shown in Figure 10. Eighty-eight percent of IMCI facilities had at least 2 HW trained in IMCI compared with 36% in non-IMCI facilities.
Table 3: IMCI training status of health workers at sampled facilities, Cambodia HFS, May 2010
Survey group Mean number of HW
trained in IMCI
Proportion of facilities that have 2 or more health workers trained in
IMCI
IMCI 2.5 (95%CI: 2.2 – 2.9) 81% (95%CI: 71 – 92)
IMCI++ 3.4 (95%CI: 3.0 – 3.8) 94% (95%CI: 88 – 100)
Non-IMCI 1.1 (95%CI: 0.3 – 1.8) 36% (95%CI: 7 – 64)
Figure 9: Health workers seeing sick children at health centres, Cambodia HFS, May 2010
0
10
20
30
40
50
Doctor Medical Assistant
Secondary Midwife
Secondary Nurse
Primary Midwife
Primary Nurse Other
perc
ent
Cambodia Health Facility Survey 2010
22
Figure 10: Proportion of nurses and midwives with IMCI training, Cambodia HFS, May 2010
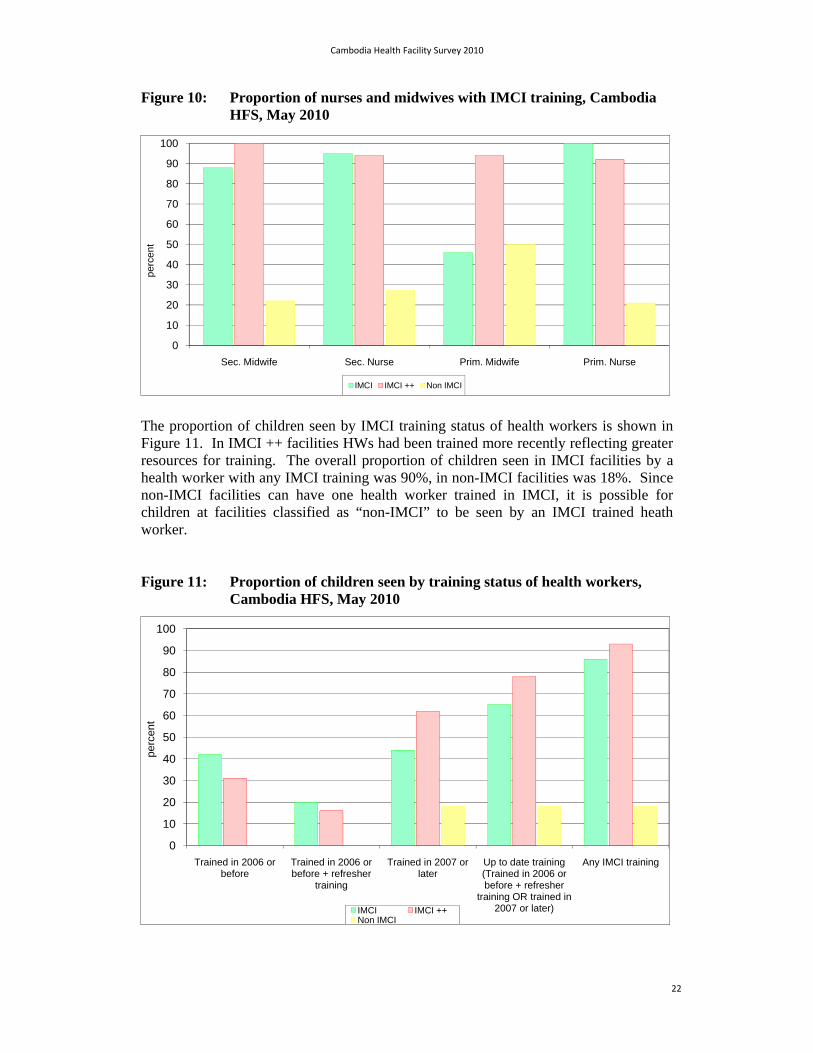
The proportion of children seen by IMCI training status of health workers is shown in Figure 11. In IMCI ++ facilities HWs had been trained more recently reflecting greater resources for training. The overall proportion of children seen in IMCI facilities by a health worker with any IMCI training was 90%, in non-IMCI facilities was 18%. Since non-IMCI facilities can have one health worker trained in IMCI, it is possible for children at facilities classified as “non-IMCI” to be seen by an IMCI trained heath worker.
Figure 11: Proportion of children seen by training status of health workers, Cambodia HFS, May 2010
0
10
20
30
40
50
60
70
80
90
100
Sec. Midwife Sec. Nurse Prim. Midwife Prim. Nurse
per
cen
t
IMCI IMCI ++ Non IMCI
0
10
20
30
40
50
60
70
80
90
100
Trained in 2006 or before
Trained in 2006 or before + refresher
training
Trained in 2007 or later
Up to date training (Trained in 2006 or before + refresher
training OR trained in 2007 or later)
Any IMCI training
perc
ent
IMCI IMCI ++Non IMCI
Cambodia Health Facility Survey 2010
23
Supervision
Supervisory visits received by facilities, and the proportion of visits that included an observation of practice are summarized in Tables 4 and 5. Supervisory visits were more likely to occur in IMCI ++ facilities, and more likely to include an observation of clinical practice. Supervisory visits occur at similar rates in standard IMCI facilities as in non-IMCI facilities, and in both groups the observation of case management is uncommon. This is an area that needs strengthening. Supportive supervision that includes an observation of case management practices with immediate feedback and problem solving is important to reinforce and sustain effective practices.
Table 4: Mean number of supervisory visits by IMCI status, Cambodia HFS, May 2010
Survey group Mean number of supervisory visits
in past 6 months
IMCI(any) vs non-IMCI
t-test
IMCI vs IMCI++
t-test
IMCI 4.73 (95%CI: 3.93-5.53)
p=0.6014 p=0.0238 IMCI++ 6.36 (95%CI: 5.17-7.55)
Non-IMCI 5.0 (95%CI: 3.55-6.45)
Table 5: Proportion of supervisory visits that included observation of practice, Cambodia HFS, May 2010
Survey group Proportion of facilities that had supervisory visits that included
observation of case management
IMCI(any) vs non-IMCI
2
IMCI vs IMCI++
2
IMCI 29.6% (95%CI: 17.0-42.2)
p=0.090 p=0.001 IMCI++ 61.50% (95%CI: 47.9-75.2)
Non-IMCI 21.4% (95%CI: -3.2-46.0)
Referral practices
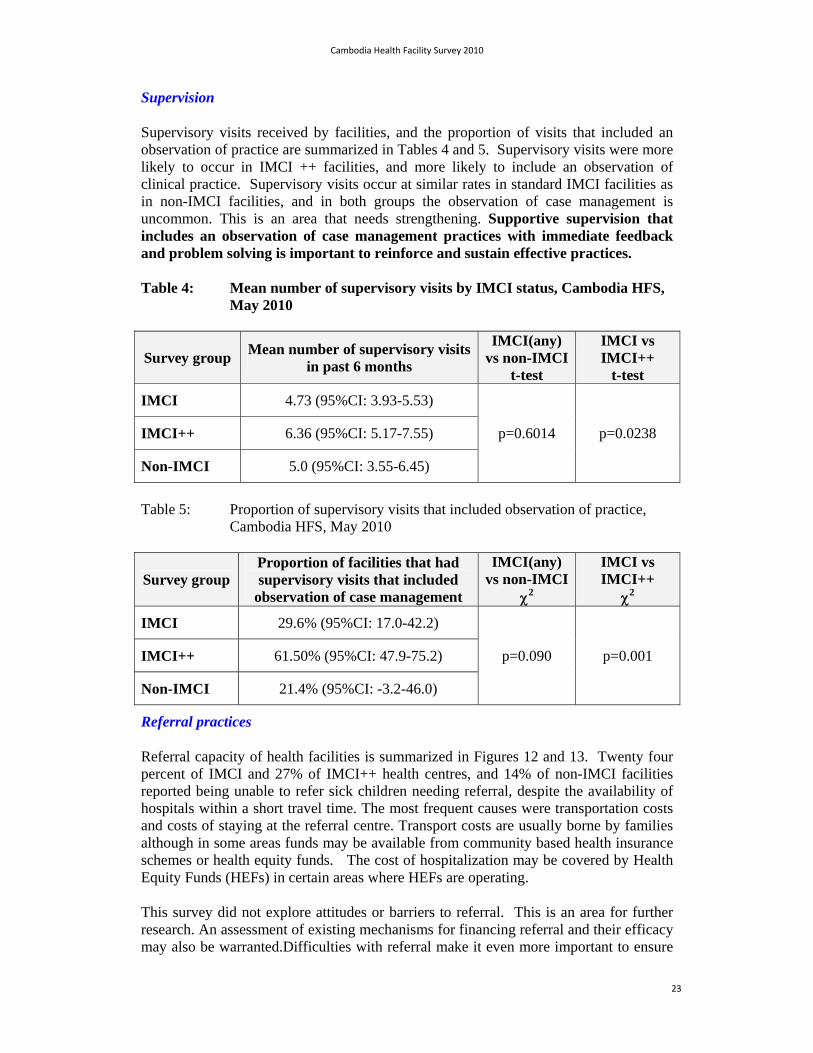
Referral capacity of health facilities is summarized in Figures 12 and 13. Twenty four percent of IMCI and 27% of IMCI++ health centres, and 14% of non-IMCI facilities reported being unable to refer sick children needing referral, despite the availability of hospitals within a short travel time. The most frequent causes were transportation costs and costs of staying at the referral centre. Transport costs are usually borne by families although in some areas funds may be available from community based health insurance schemes or health equity funds. The cost of hospitalization may be covered by Health Equity Funds (HEFs) in certain areas where HEFs are operating.
This survey did not explore attitudes or barriers to referral. This is an area for further research. An assessment of existing mechanisms for financing referral and their efficacy may also be warranted.Difficulties with referral make it even more important to ensure
Cambodia Health Facility Survey 2010
24
that health centres have life-saving drugs such as injectable antibiotics and drugs used for management of eclampsia and the third stage of labor.
Figure 12: Health worker perception of difficulties with referral, Cambodia HFS, May 2010
Figure 13: Median time to reach referral hospital, Cambodia HFS, May 2010
Administration
Figure 14 shows the availability of Health Centre Management Committees. HCMCs are local groups that oversee the management of Health Centres. The data show these committees exist for the majority of health centres, and that they meet regularly in most cases. HCMC at non-IMCI facilities are less likely to meet.
0
10
20
30
40
50
60
70
80
90
100
HWs report difficulties referring sick children needing referral in the past
HW perception of the proporiton of children needing referral who reach referral hospitals
per
cen
t
IMCI IMCI ++ Non IMCI
0
10
20
30
40
50
60
Median time to each RH from HC
min
utes
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
25
Figure 14: Availability of Health Centre Management Committees, Cambodia HFS, May 2010
0
10
20
30
40
50
60
70
80
90
100
HC has a HCMC HC with HCMC that met at least once in previous 6 mo
per
cen
t
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
26
Summary of findings: Availability of Facility Supports
IMCI-trained health workers are widely available. Essential drugs and supplies are available in the majority of facilities.
Gaps were noted in the availability of injectible antibiotics, ciprofloxacin, zinc and magnesium sulphate. Nasogastric tubes were not available in many facilities. Since injectible antibiotics are often life-saving pre-referral treatments, supplies of these drugs need to be urgently improved.
Despite availability of water, hand washing often cannot be conducted in the areas where sick children are seen, and hand-washing is not regularly performed by health workers before seeing sick children.
Supervisory visits are generally being made to health facilities. Supportive supervision which focuses observation of clinical practice, feedback and solving problems is still not a regular part of supervision. The performance of IMCI facilities is not much different from non-IMCI facilities.
Problems referring sick children needing referral are reported by many
health workers. Costs of transportation and of staying at referral hospitals were reported as barriers. More data are needed on barriers to referral, including financial barriers and perceptions of quality of care at referral facilities. Reviews should include an equity analysis, and explore the use and efficacy of fiscal mechanisms to minimize financial barriers.

Cambodia Health Facility Survey 2010
27
7.3 MANAGEMENT OF THE YOUNG INFANT 0-2 MONTHS OF AGE
A total of 34 infants aged 0-2 months were seen. Of these only 5 were seen in non-IMCI facilities. Since the sample size was small there was inadequate power to detect differences between IMCI and non-IMCI facilities for most outcomes. The results are presented for all infants combined, except where otherwise noted.
Age at presentation
Ages at presence of young infants are shown in Figure 15. The majority of them presented at around 6 weeks of age. As discussed in the previous section, this may reflect age heaping, since mothers were not asked to provide birth-dates for their children. The majority of children presenting at 6 weeks of age were brought for sick child visits, and not for immunization. Data from a verbal autopsy study conducted in Svey Rieng Operational district, Svay Rieng province in 2009 showed that many neonates who died were not brought for care at health facilities; in some cases, when they were recognized as very sick, they were taken directly to hospital4. These findings support reports from health workers that there is a strong cultural reluctance for both mother s and newborns to seek care outside of the home in the first 4 weeks of life. For this reason, sick newborns are often not seen at health centres.
Figure 15: Age of presentation for young infants, Cambodia HFS, May 2010
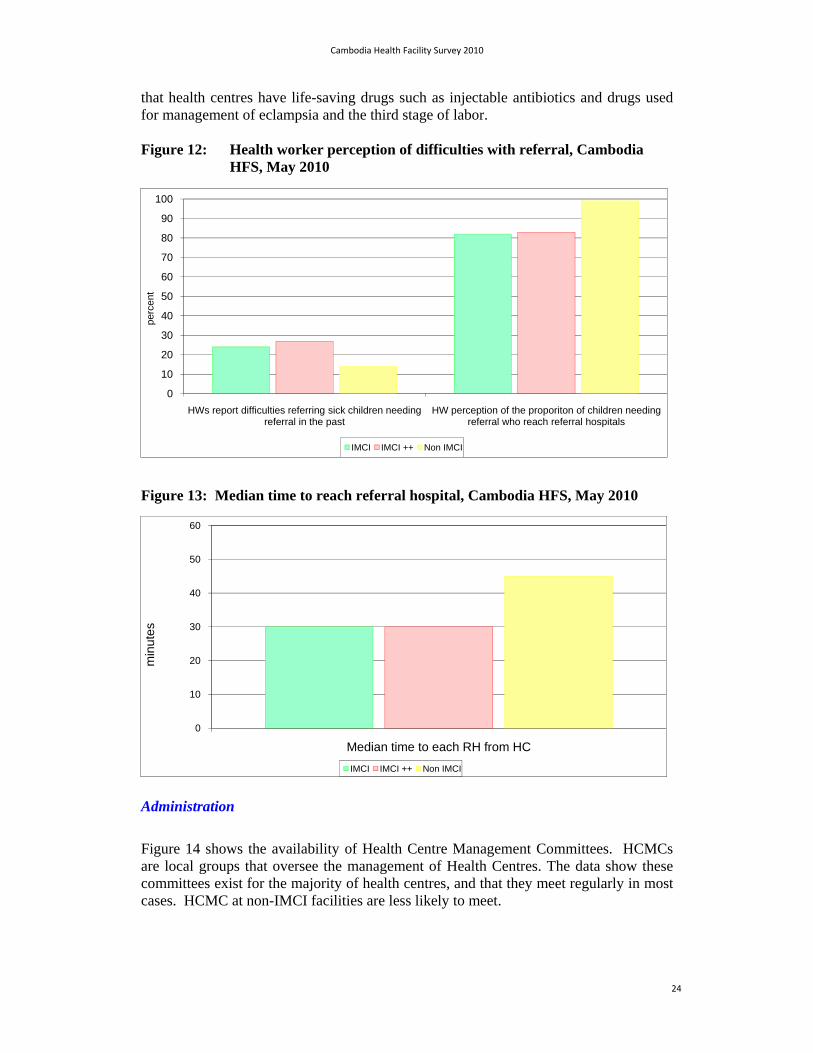
Reason for presentation
Presenting complaints are presented in Figure 16. Of 34 young infants seen in the survey, half presented with fever or cough, and about a third with diarrhoea. No infants were dehydrated. Other complaints included skin conditions, nappy rash, eye problems, and abdominal pain. Half the infants had more than one problem, and a third had 3 or more problems.
4 WHO Cambodia. Svat Rieng Verbal Autopsy Study. Preliminary Report. August 2010.
05
10
15
20
Fre
que
ncy
0 2 4 6 8A g e i n w e e k s
y o u n g in f a n t s
A g e a t p r e s e n t a t i o n
Cambodia Health Facility Survey 2010
28
Figure 16: Presenting complaints for young infants, Cambodia HFS, May 2010
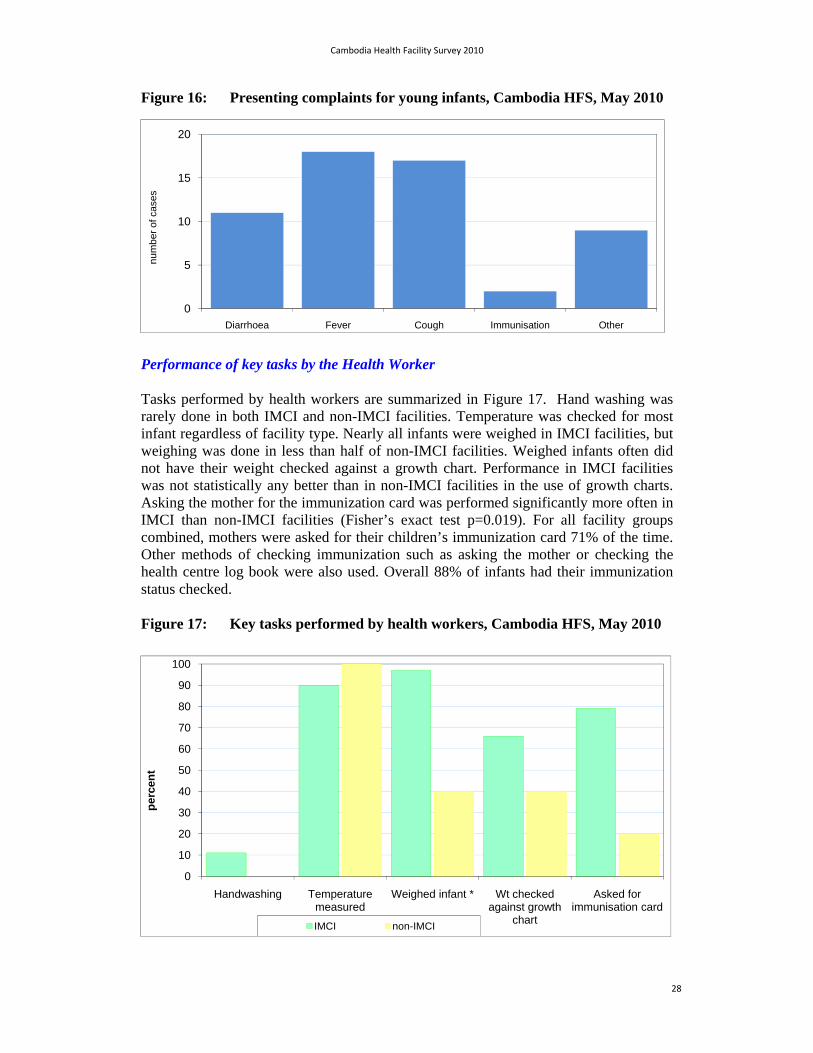
Performance of key tasks by the Health Worker
Tasks performed by health workers are summarized in Figure 17. Hand washing was rarely done in both IMCI and non-IMCI facilities. Temperature was checked for most infant regardless of facility type. Nearly all infants were weighed in IMCI facilities, but weighing was done in less than half of non-IMCI facilities. Weighed infants often did not have their weight checked against a growth chart. Performance in IMCI facilities was not statistically any better than in non-IMCI facilities in the use of growth charts. Asking the mother for the immunization card was performed significantly more often in IMCI than non-IMCI facilities (Fisher’s exact test p=0.019). For all facility groups combined, mothers were asked for their children’s immunization card 71% of the time. Other methods of checking immunization such as asking the mother or checking the health centre log book were also used. Overall 88% of infants had their immunization status checked.
Figure 17: Key tasks performed by health workers, Cambodia HFS, May 2010
0
5
10
15
20
Diarrhoea Fever Cough Immunisation Other
nu
mb
er o
f ca
ses
0
10
20
30
40
50
60
70
80
90
100
Handwashing Temperature measured
Weighed infant * Wt checked against growth
chart
Asked for immunisation card
per
cen
t
IMCI non-IMCI
Cambodia Health Facility Survey 2010
29
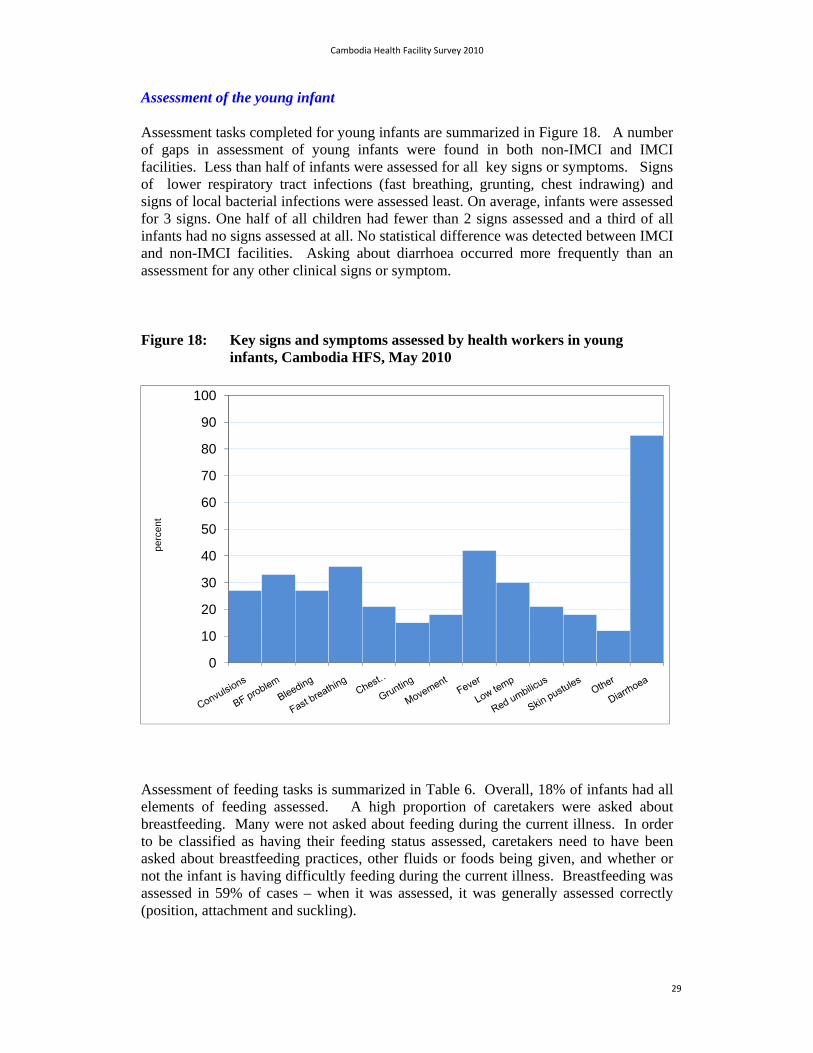
Assessment of the young infant
Assessment tasks completed for young infants are summarized in Figure 18. A number of gaps in assessment of young infants were found in both non-IMCI and IMCI facilities. Less than half of infants were assessed for all key signs or symptoms. Signs of lower respiratory tract infections (fast breathing, grunting, chest indrawing) and signs of local bacterial infections were assessed least. On average, infants were assessed for 3 signs. One half of all children had fewer than 2 signs assessed and a third of all infants had no signs assessed at all. No statistical difference was detected between IMCI and non-IMCI facilities. Asking about diarrhoea occurred more frequently than an assessment for any other clinical signs or symptom.
Figure 18: Key signs and symptoms assessed by health workers in young infants, Cambodia HFS, May 2010
Assessment of feeding tasks is summarized in Table 6. Overall, 18% of infants had all elements of feeding assessed. A high proportion of caretakers were asked about breastfeeding. Many were not asked about feeding during the current illness. In order to be classified as having their feeding status assessed, caretakers need to have been asked about breastfeeding practices, other fluids or foods being given, and whether or not the infant is having difficultly feeding during the current illness. Breastfeeding was assessed in 59% of cases – when it was assessed, it was generally assessed correctly (position, attachment and suckling).
0
10
20
30
40
50
60
70
80
90
100
per
cen
t
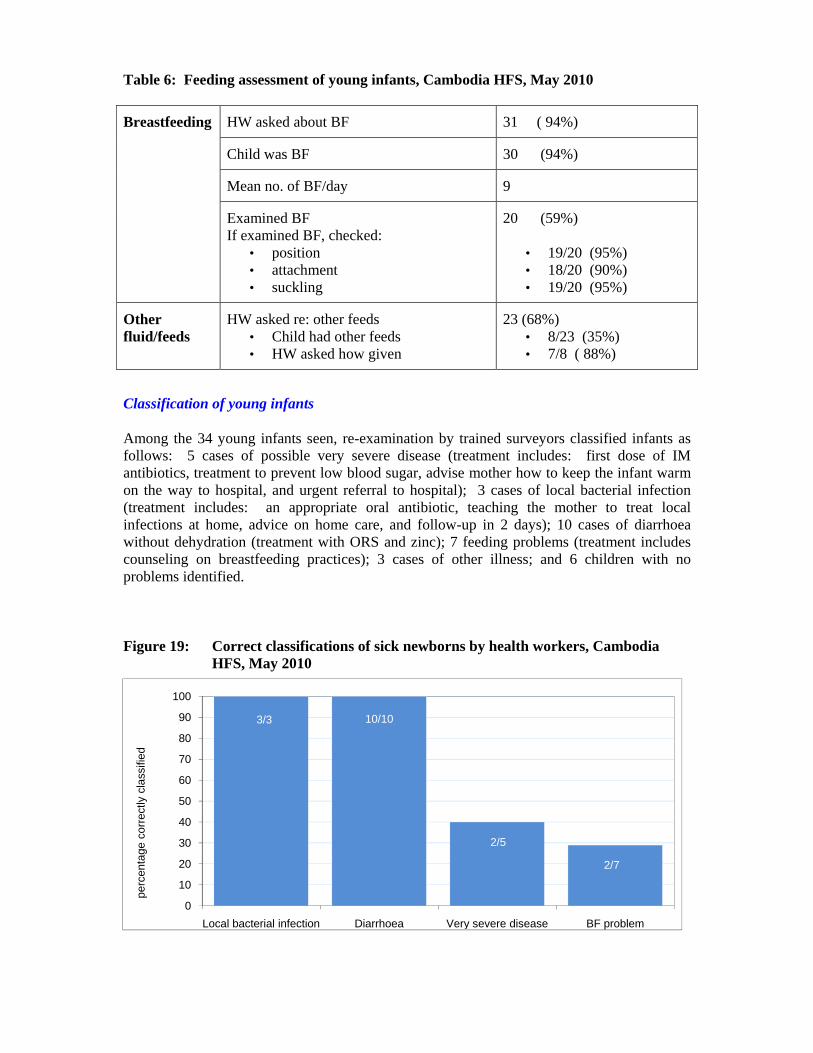
Table 6: Feeding assessment of young infants, Cambodia HFS, May 2010
Breastfeeding HW asked about BF 31 ( 94%)
Child was BF 30 (94%)
Mean no. of BF/day 9
Examined BF If examined BF, checked:
• position • attachment • suckling
20 (59%)
• 19/20 (95%) • 18/20 (90%) • 19/20 (95%)
Other fluid/feeds
HW asked re: other feeds • Child had other feeds • HW asked how given
23 (68%) • 8/23 (35%) • 7/8 ( 88%)
Classification of young infants
Among the 34 young infants seen, re-examination by trained surveyors classified infants as follows: 5 cases of possible very severe disease (treatment includes: first dose of IM antibiotics, treatment to prevent low blood sugar, advise mother how to keep the infant warm on the way to hospital, and urgent referral to hospital); 3 cases of local bacterial infection (treatment includes: an appropriate oral antibiotic, teaching the mother to treat local infections at home, advice on home care, and follow-up in 2 days); 10 cases of diarrhoea without dehydration (treatment with ORS and zinc); 7 feeding problems (treatment includes counseling on breastfeeding practices); 3 cases of other illness; and 6 children with no problems identified.
Figure 19: Correct classifications of sick newborns by health workers, Cambodia HFS, May 2010
3/3 10/10
2/5
2/7
0
10
20
30
40
50
60
70
80
90
100
Local bacterial infection Diarrhoea Very severe disease BF problem
perc
enta
ge c
orr
ectly
cla
ssifi
ed

Cambodia Health Facility Survey 2010
31
Classification of sick young infants by health workers is shown in Figure 19. Health workers classified all cases of local bacterial infection and diarrhoea correctly. Fewer cases of very severe disease and feeding problems were classified correctly – this is likely to reflect relatively limited assessments done of young infants –signs that are important for classifying severe disease or feeding probems were often not assessed.
Treatment of young infants
Treatment of young infants is summarized in Figure 20. No children who did not need antibiotics received them (26/26). ORS was given to infants with diarrhoea and no dehydration in 90% of cases. Zinc was given to 4/10 infants (40%). Of those infants needing antibiotics, 4/8 (50%) had them prescribed correctly. Of the 5 children with possible very severe disease needing immediate referral, 2/5 (40%) were referred. Both of these infants received oral antibiotics before referral. Overall, 70% of caretakers of infants were advised to increase fluids and food during the illness.
Figure 20: Correct treatment of sick newborns by health workers, Cambodia HFS, May 2010
Counseling of the mother
Counseling messages given to caretakers of young infants are presented in Figure 21. More than half of mothers were advised to increase feeds during illness. Information on key danger signs for when to return - including becoming unable to feed, fast or difficult breathing and fever – was often not given.
26/269/10
4/8
2/5
0
10
20
30
40
50
60
70
80
90
100
No antibitoics if not needed
ORS for diarrhoea Antibiotics precribed correctly
Needing referral referred
perc
enta
ge c
orre
ctly
tre
ated

Cambodia Health Facility Survey 2010
32
Figure 21: Counseling messages given to caretakers of young infants, Cambodia HFS, May 2010
0
10
20
30
40
50
60
70
80
90
100pe
rcen
t

Cambodia Health Facility Survey 2010
33
Summary of findings: Management of the young infant 0-2 months
Given the small number of young infants seen, the findings in this section should be interpreted with greater caution. Overall findings include:
The assessment of signs of illness in young infants needs improvement. Young
infants were often not assessed for all key signs needed in order to determine whether or not the infant was severely ill.
Diarrhoea and local bacterial infections were correctly classified by health
workers. Possible very severe disease, and feeding problems were not recognized by health workers in several cases. This may reflect limited assessment skills. Classification of these two areas needs improvement.
Treatment of diarrhoea was done well. Several cases of possible severe disease
were not treated with antibiotics or referred. Poor treatment of this classification probably reflects the fact that these cases were not assessed and classified correctly.
Counseling of the mother generally needs improvement. Caretakers were often not given advice on danger signs for when to return with their young infant – including signs of lower respiratory tract infections.
A high proportion of young infants had their breastfeeding status assessed and were given advice on breastfeeding – even though feeding problems were often not recognized.
Hand-washing is rarely performed despite availability of soap and water in the
facility. Making some water and soap available in the area where young infants are assessed may be required.

Cambodia Health Facility Survey 2010
34
7.4. MANAGEMENT OF CHILDREN AGED 2 TO 59 MONTHS
A total of 425 children aged 2 to 59 months were seen. Reasons for presentation are presented in Figure 22. More frequent presenting complaints were fever, cough, and diarrhoea. A number of children presented with skin problems. The average number of problems at presentation was 2. Most children presented with more than one problem. This supports the rationale of the integrated approach of IMCI.
Figure 22: Presenting complaints for sick children, Cambodia HFS, May 2010
Assessment of sick children
Assessment tasks conducted are summarized in Figure 23. In facilities practicing IMCI, nearly all children are weighed but only a half to two-thirds have their weight checked against a growth chart. Vaccination status is generally checked. A feeding assessment is counted as having been performed if the health worker asks the mother if they breastfeed the child, asks about any other fluids or foods and checks if the child is feeding less during illness. Among children younger than 2 attending with illness, the full feeding assessment was conducted less than half the time.
Comparisons between non-IMCI, IMCI and IMCI++ areas are shown in Table 6. For all assessment tasks, IMCI facilities perform better than non-IMCI facilities. IMCI ++ facilities perform better than IMCI facilities on some tasks, but not all. Use of growth charts, checking of vaccination status and full feeding assessment of children under 2 are all performed more frequently in IMCI++ facilities.
0
10
20
30
40
50
60
70
80
90
100
Diarrhoea Fever Cough or difficulty breathing
Ear problem Well child/Immunization
Other (skin diseases,
abscesses, injuries)
perc
ent
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
35
Figure 23: Assessment tasks conducted for sick children, Cambodia HFS, May 2010
Table 6: Assessment tasks performed by IMCI implementation status, Cambodia HFS, May 2010
Indicator
IMCI
IMCI++ Non-IMCI
IMCI(any) vs non-IMCI
2
IMCI vs IMCI++
2
Child weighed 89.3% (84.7-93.9)
(158/177)
92.8% (89.2-96.3)
(193/208)
53.8% (37.5-70.2)
(21/39)
p<0.001 p=0.226
Weight checked against growth chart
50.3% (42.8-57.7)
(89/177)
65.4% (58.9-71.9)
(136/208)
25.6% (11.3-40.0)
(10/39)
p<0.001 p=0.003
Vaccination status checked
86.0% (80.8-91.1)
(153/178)
94.2% (91.0-97.4)
(196/208)
41.0% (24.9-57.2)
(16/39)
p<0.001 p=0.006
Full feeding assessment in child <2yo
38.9% (30.5 – 47.4)
(51/131)
51.1% (42.7 – 59.5)
(71/139)
4.2% (-4.5-12.8)
(1/24)
p<0.001 p=0.045
Assessment of key signs and symptoms is shown in Figure 24 and Table 7. A high proportion of children are screened for cough, diarrhoea and fever. Checking for danger signs is done relatively poorly by all facility groups. Recognition of the severely ill children is crucial to reducing child deaths. Checking for danger signs of severe illness should be routinely performed in all children. IMCI facilities generally check danger signs more often than non-IMCI facilities, but over half of children attending IMCI facilities still do not have 3 danger signs assessed. No differences were seen between IMCI and IMCI++ facilities.
0
10
20
30
40
50
60
70
80
90
100
Weighed Weight checked against growth chart
Vaccination status checked
Children <2yo: feeding assessment performed
perc
ent
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
36
Figure 24: Assessment of key signs and symptoms in sick children, Cambodia HFS, May 2010
Table 7: Danger signs checked by IMCI implementation status, Cambodia HFS, May 2010
Indicator
IMCI % (95% CI) (proportion)
IMCI++ Non-IMCI
IMCI(any) vs non-IMCI 2
IMCI vs IMCI++
2
Proportion of children checked for all 3 danger signs
46.1% (38.6 – 53.7)
(82/178)
44.2% (37.4 – 51.3)
(92/208)
7.7% (-1.1 – 16.4)
(3/39)
p<0.001 p=0.718
Proportion of children checked for the presence of cough, diarrhoea, fever
83.1% (76.8-88.3) (148/178)
88.5% (83.3 – 92.5)
(184/208)
66.7% (49.8 – 80.9)
(26/39)
p=0.002 p= 0.133
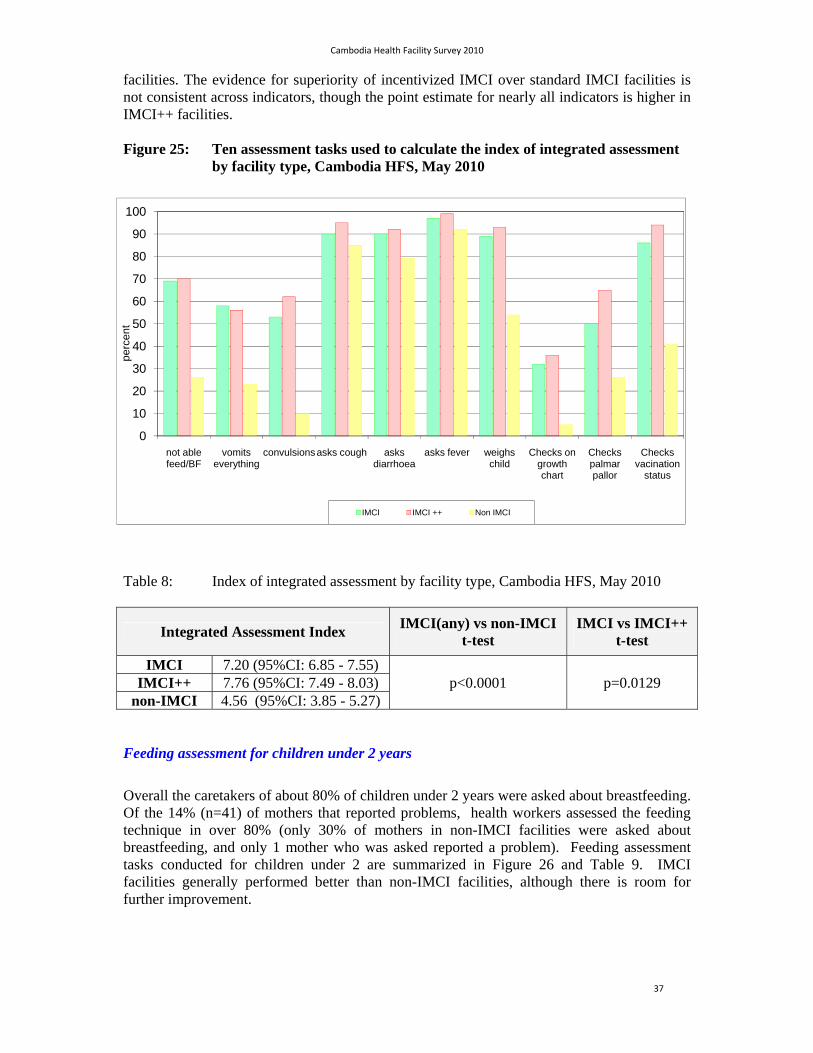
Index of integrated assessment
Assessment tasks required to screen sick children according to the IMCI case-management approach are presented in Figure 25. The index of integrated assessment is a summary measure which averages the total proportion of assessment tasks completed across all facilities, is presented in Table 8.
IMCI facilities generally perform better than non-IMCI facilities for all assessment tasks, and this is reflected by the difference in the Integrated Assessment Index. There is also evidence that IMCI++ facilities perform better than standard IMCI facilities. Assessment tasks need improvement in all facility types, however. Caution should be exercised in interpreting the p-values presented in Table 8. Undertaking multiple comparisons markedly raises the likelihood of finding falsely significant results (type-1 error). The crucial point that there is strong evidence suggesting that IMCI facilities of either group perform better than non-IMCI
0
10
20
30
40
50
60
70
80
90
100
Danger Sign: Is child able to drink/BF
Danger Sign: Vomits everything
Danger Sign: Convulsions
Check all 3 Danger Signs
Checked for cough, diarrhoea & fever
perc
ent
IMCI IMCI ++ Non IMCI
Cambodia Health Facility Survey 2010
37
facilities. The evidence for superiority of incentivized IMCI over standard IMCI facilities is not consistent across indicators, though the point estimate for nearly all indicators is higher in IMCI++ facilities.
Figure 25: Ten assessment tasks used to calculate the index of integrated assessment by facility type, Cambodia HFS, May 2010
Table 8: Index of integrated assessment by facility type, Cambodia HFS, May 2010
Integrated Assessment Index IMCI(any) vs non-IMCI
t-test IMCI vs IMCI++
t-test
IMCI 7.20 (95%CI: 6.85 - 7.55) p<0.0001 p=0.0129 IMCI++ 7.76 (95%CI: 7.49 - 8.03)
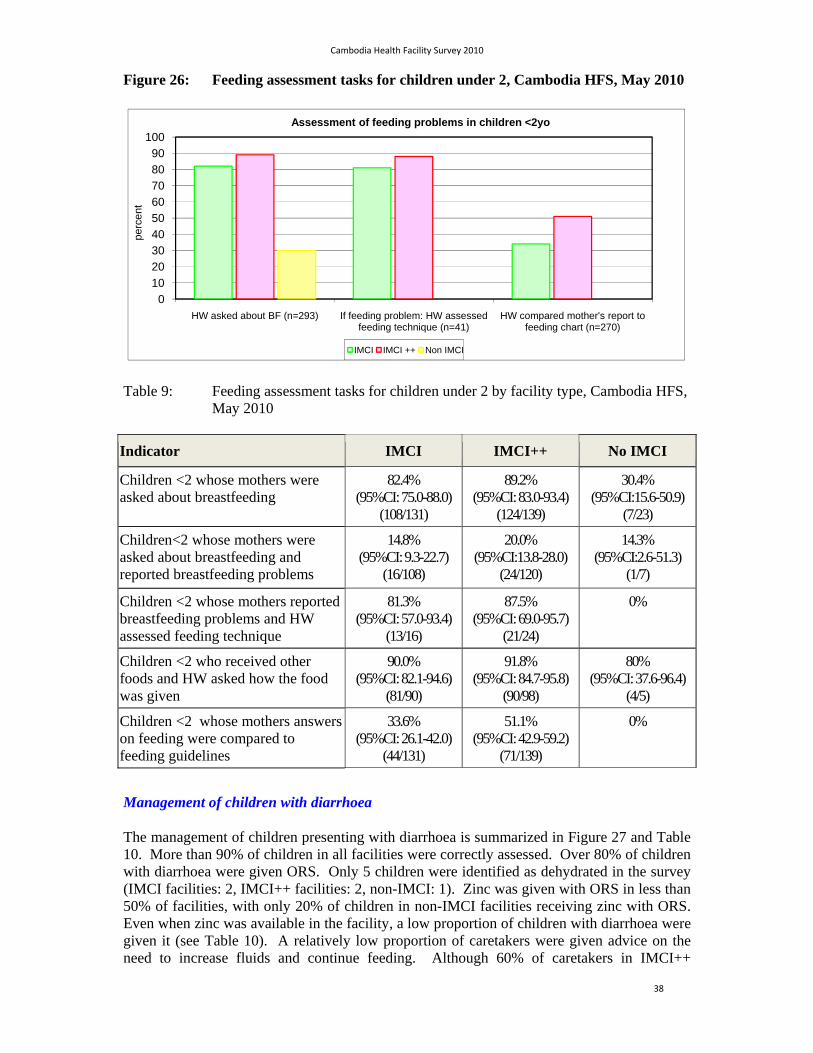
non-IMCI 4.56 (95%CI: 3.85 - 5.27) Feeding assessment for children under 2 years
Overall the caretakers of about 80% of children under 2 years were asked about breastfeeding. Of the 14% (n=41) of mothers that reported problems, health workers assessed the feeding technique in over 80% (only 30% of mothers in non-IMCI facilities were asked about breastfeeding, and only 1 mother who was asked reported a problem). Feeding assessment tasks conducted for children under 2 are summarized in Figure 26 and Table 9. IMCI facilities generally performed better than non-IMCI facilities, although there is room for further improvement.
0
10
20
30
40
50
60
70
80
90
100
not able feed/BF
vomits everything
convulsionsasks cough asks diarrhoea
asks fever weighs child
Checks on growth chart
Checks palmar pallor
Checks vacination
status
perc
ent
IMCI IMCI ++ Non IMCI
Cambodia Health Facility Survey 2010
38
Figure 26: Feeding assessment tasks for children under 2, Cambodia HFS, May 2010
Table 9: Feeding assessment tasks for children under 2 by facility type, Cambodia HFS, May 2010
Indicator IMCI IMCI++ No IMCI
Children <2 whose mothers were asked about breastfeeding
82.4% (95%CI: 75.0-88.0)
(108/131)
89.2% (95%CI: 83.0-93.4)
(124/139)
30.4% (95%CI:15.6-50.9)
(7/23)
Children<2 whose mothers were asked about breastfeeding and reported breastfeeding problems
14.8% (95%CI: 9.3-22.7)
(16/108)
20.0% (95%CI:13.8-28.0)
(24/120)
14.3% (95%CI:2.6-51.3)
(1/7)
Children <2 whose mothers reported breastfeeding problems and HW assessed feeding technique
81.3% (95%CI: 57.0-93.4)
(13/16)
87.5% (95%CI: 69.0-95.7)
(21/24)
0%
Children <2 who received other foods and HW asked how the food was given
90.0% (95%CI: 82.1-94.6)
(81/90)
91.8% (95%CI: 84.7-95.8)
(90/98)
80% (95%CI: 37.6-96.4)
(4/5)
Children <2 whose mothers answers on feeding were compared to feeding guidelines
33.6% (95%CI: 26.1-42.0)
(44/131)
51.1% (95%CI: 42.9-59.2)
(71/139)
0%
Management of children with diarrhoea
The management of children presenting with diarrhoea is summarized in Figure 27 and Table 10. More than 90% of children in all facilities were correctly assessed. Over 80% of children with diarrhoea were given ORS. Only 5 children were identified as dehydrated in the survey (IMCI facilities: 2, IMCI++ facilities: 2, non-IMCI: 1). Zinc was given with ORS in less than 50% of facilities, with only 20% of children in non-IMCI facilities receiving zinc with ORS. Even when zinc was available in the facility, a low proportion of children with diarrhoea were given it (see Table 10). A relatively low proportion of caretakers were given advice on the need to increase fluids and continue feeding. Although 60% of caretakers in IMCI++
0
10
20
30
40
50
60
70
80
90
100
HW asked about BF (n=293) If feeding problem: HW assessed feeding technique (n=41)
HW compared mother's report to feeding chart (n=270)
perc
ent
Assessment of feeding problems in children <2yo
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
39
facilities could report correctly how to give ORS, less than 50% of caretakers from other facilities could do so. Overall, counseling practices need improvement.
Figure 27: Management of children with diarrhoea, Cambodia HFS, May 2010
Table 10: Availability and use of zinc for the management of watery diarrhea, Cambodia HFS, May 2010
Survey group
Proportion of facilities with zinc available
Proportion of children with diarrhea prescribed ORS & zinc – when zinc was
available IMCI
42.6% (23/54) (95%CI: 29.0-56.2%)
57.6% (19/36) (95%CI: 39.8-75.4%)
IMCI++
63.5% (33/52) (95%CI: 50.0-77.0%)
44.9% (31/69) (95%CI: 32.9-57.0%)
Non-IMCI
35.7% (5/14) (95%CI: 7.0-64.4%)
25.0% (1/4) (95%CI is wider than 0-100%)
Management of children with pneumonia
Management of pneumonia is summarized in Figure 28. Pneumonia was generally recognized by health workers (>80% in facilities of any group). Although over 96% of children classified with pneumonia were treated with antibiotics, a lower proportion were treated correctly. In order to be considered to have used antibiotics correctly, health workers have to use the correct first line antibiotic, and to prescribe it for the recommended dose, and
0
10
20
30
40
50
60
70
80
90
100
Children with diarrhoea correctly
assessed
Children without dehydration
prescribed ORS
Children without dehydration
prescribed ORS + Zinc
Children with diarrhoea advised to
increase fluids & continue feeding
Children prescribed ORS whose
caretakers knew how to give it
perc
ent
Children presenting with diarrhoea
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
40
number of days. Pneumonia was correctly treated with antibiotics in 60-78% of cases in IMCI facilities, and in only 20% of cases in non-IMCI facilities. Caretakers left the facility knowing how to give antibiotics in most cases (72% of cases in IMCI and 85% in IMCI++ facilities), but a low proportion were advised on signs of illness that require immediate return to the health centre (20% in IMCI, 35% in IMCI++). Counseling is therefore done relatively poorly. Despite good recognition of pneumonia in non-IMCI facilities, treatment and counseling practices need improvement.
Figure 28: Management of pneumonia, Cambodia HFS, May 2010
General tasks
General tasks completed are shown in Figure 29.
Figure 29: General tasks completed for sick children, Cambodia HFS, May 2010
0
10
20
30
40
50
60
70
80
90
100
Correctly diagnosed Correctly treated with AB Child with pneumonia + given ab's and caretaker
knew how to give
Child with pneumonia + caretaker advised on when
to return immediately
perc
ent
IMCI IMCI ++ Non IMCI
0
10
20
30
40
50
60
70
80
90
100
AB correctly prescribed if needed
no AB if did not need them
Advised extra fluids & continue feeding
Child needs vaccination and is
vaccinated
Health worker used mothers card
perc
ent
IMCI IMCI ++ Non IMCI
Cambodia Health Facility Survey 2010
41
Overall 60-70% of children who needed antibiotics had these correctly prescribed. Almost half of children who did not need antibiotics were given them, indicating that inappropriate use of antibiotics is common. General advice on the need to give increased fluids and feeding to sick children was given in a relatively low proportion of cases. Only about a third of children who needed vaccination received a vaccination at the time of the sick child visit. This represents a missed opportunity to vaccine children. The IMCI mothers card was rarely used for counseling, since it was often not available. It is currently out of print in Cambodia. The mothers card is a useful counseling aid, that should be made available.
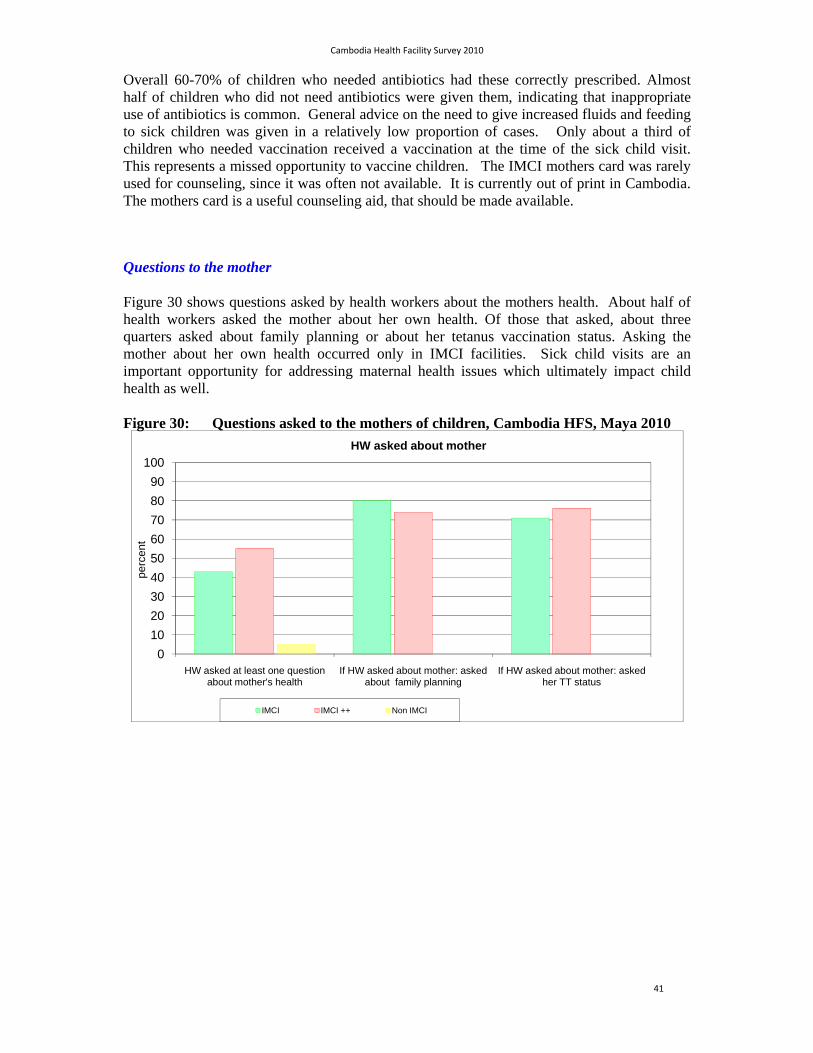
Questions to the mother
Figure 30 shows questions asked by health workers about the mothers health. About half of health workers asked the mother about her own health. Of those that asked, about three quarters asked about family planning or about her tetanus vaccination status. Asking the mother about her own health occurred only in IMCI facilities. Sick child visits are an important opportunity for addressing maternal health issues which ultimately impact child health as well.
Figure 30: Questions asked to the mothers of children, Cambodia HFS, Maya 2010
0
10
20
30
40
50
60
70
80
90
100
HW asked at least one question about mother's health
If HW asked about mother: asked about family planning
If HW asked about mother: asked her TT status
perc
ent
HW asked about mother
IMCI IMCI ++ Non IMCI
Cambodia Health Facility Survey 2010
42
Summary of findings: case management of children 2 – 59 months
The quality of care for children is better in IMCI facilities than in non-IMCI facilities, but important gaps in IMCI facilities remain. IMCI ++ facilities did better that IMCI facilities on some assessment tasks, on the management of diarrhoea and pneumonia and on a several counseling tasks.
Children are generally asked about their presenting complaint, weighed and
have their vaccination status checked. Health workers generally take an integrated approach to assessing children. Children are not always assessed for danger signs for severe illness, however. In addition, weights are often not plotted on growth charts, and children needing vaccines are often not vaccinated on the day of the visit.
Full feeding assessments are not done frequently enough, including asking
about difficulty feeding during the presenting illness and the using standardized feeding charts. Breastfeeding assessments are generally done well.
Children with diarrhoea are generally assessed correctly and treated with ORS. Zinc is still not used in most cases. Health workers in IMCI++ facilities used zinc and ORS more often that health workers in other facilities.
Children with pneumonia are generally correctly classified, but antibiotics are often not prescribed correctly.
Counseling practices need improvement in a number of areas, including on the need to continue feeds and increase fluids during illness, recognition of danger signs for when to return for care, and explaining properly how to take prescribed treatments.
Cambodia Health Facility Survey 2010
43
8. COMPARISON OF IMCI AND IMCI ++ FACILITIES
Facilities that had implemented IMCI through the routine health system, and those that had implemented IMCI with incentives (IMCI++) were compared on a number of measures. Findings are summarized below.
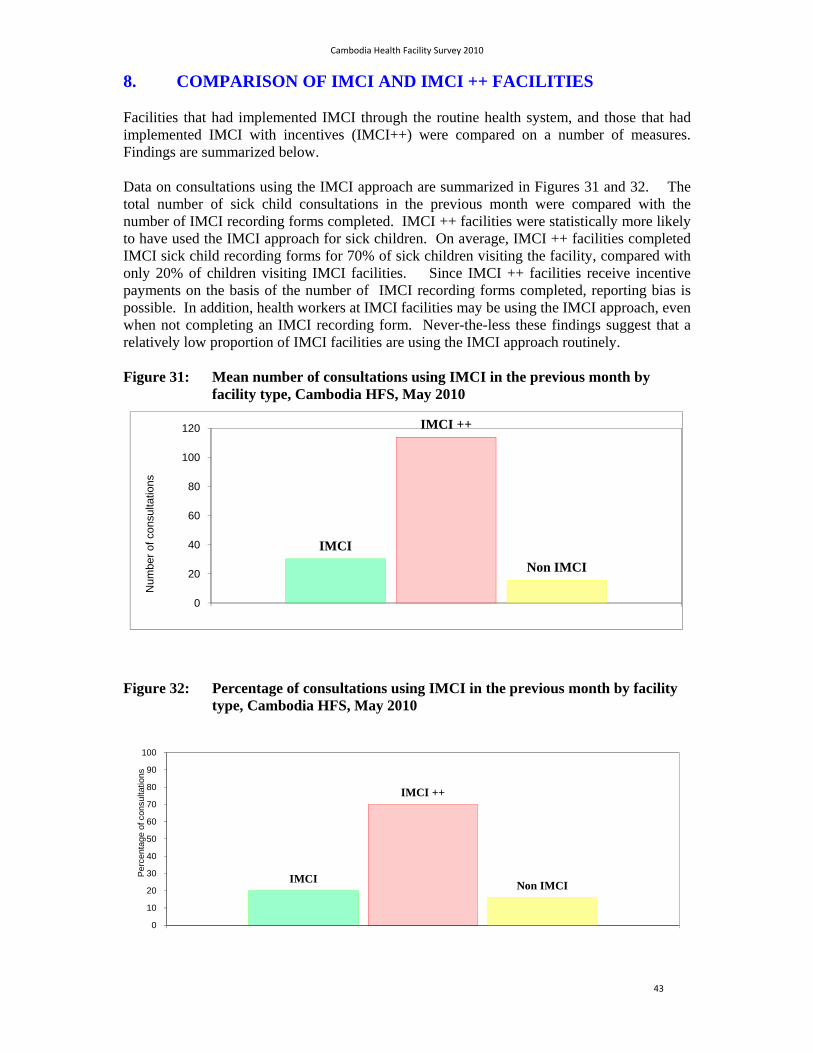
Data on consultations using the IMCI approach are summarized in Figures 31 and 32. The total number of sick child consultations in the previous month were compared with the number of IMCI recording forms completed. IMCI ++ facilities were statistically more likely to have used the IMCI approach for sick children. On average, IMCI ++ facilities completed IMCI sick child recording forms for 70% of sick children visiting the facility, compared with only 20% of children visiting IMCI facilities. Since IMCI ++ facilities receive incentive payments on the basis of the number of IMCI recording forms completed, reporting bias is possible. In addition, health workers at IMCI facilities may be using the IMCI approach, even when not completing an IMCI recording form. Never-the-less these findings suggest that a relatively low proportion of IMCI facilities are using the IMCI approach routinely.
Figure 31: Mean number of consultations using IMCI in the previous month by facility type, Cambodia HFS, May 2010
Figure 32: Percentage of consultations using IMCI in the previous month by facility type, Cambodia HFS, May 2010
IMCI
IMCI ++
Non IMCI
0
20
40
60
80
100
120
Num
ber
of c
ons
ulta
tion
s
IMCI
IMCI ++
Non IMCI
0
10
20
30
40
50
60
70
80
90
100
Pe
rcen
tage
of c
onsu
ltatio
ns
Cambodia Health Facility Survey 2010
44
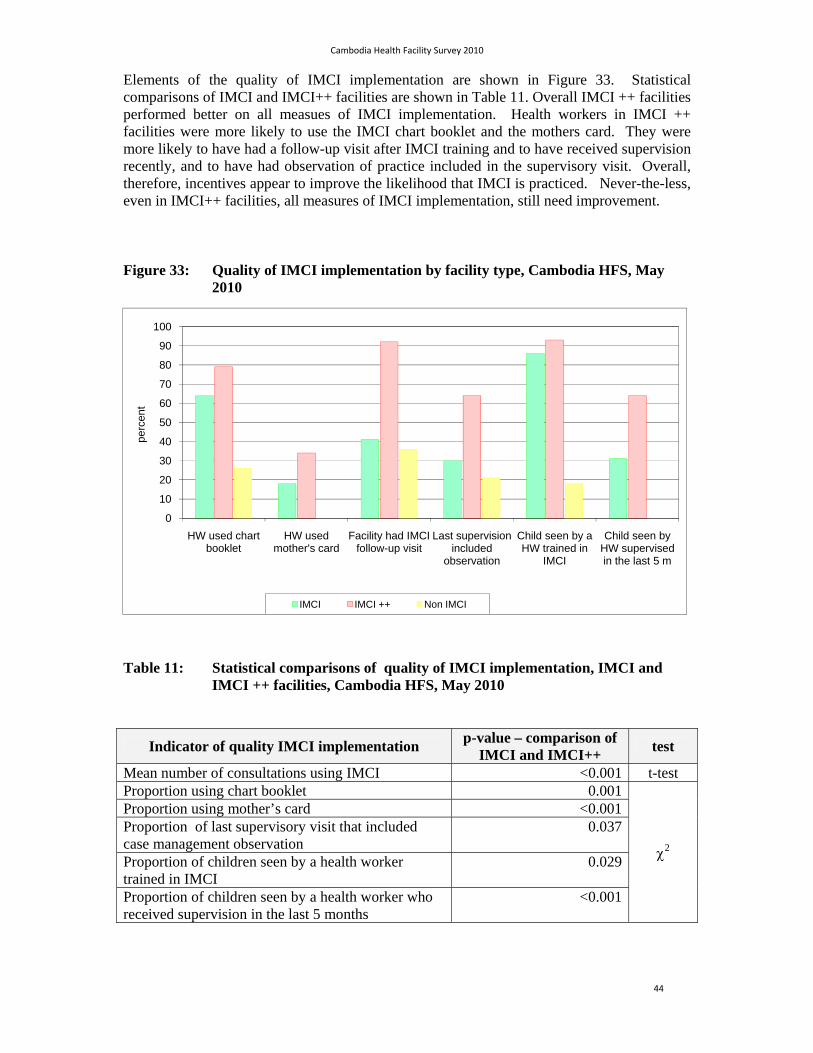
Elements of the quality of IMCI implementation are shown in Figure 33. Statistical comparisons of IMCI and IMCI++ facilities are shown in Table 11. Overall IMCI ++ facilities performed better on all measues of IMCI implementation. Health workers in IMCI ++ facilities were more likely to use the IMCI chart booklet and the mothers card. They were more likely to have had a follow-up visit after IMCI training and to have received supervision recently, and to have had observation of practice included in the supervisory visit. Overall, therefore, incentives appear to improve the likelihood that IMCI is practiced. Never-the-less, even in IMCI++ facilities, all measures of IMCI implementation, still need improvement.
Figure 33: Quality of IMCI implementation by facility type, Cambodia HFS, May 2010
Table 11: Statistical comparisons of quality of IMCI implementation, IMCI and IMCI ++ facilities, Cambodia HFS, May 2010
Indicator of quality IMCI implementation p-value – comparison of
IMCI and IMCI++ test
Mean number of consultations using IMCI <0.001 t-test Proportion using chart booklet 0.001
2
Proportion using mother’s card <0.001 Proportion of last supervisory visit that included case management observation
0.037
Proportion of children seen by a health worker trained in IMCI
0.029
Proportion of children seen by a health worker who received supervision in the last 5 months
<0.001
0
10
20
30
40
50
60
70
80
90
100
HW used chart booklet
HW used mother's card
Facility had IMCI follow-up visit
Last supervision included
observation
Child seen by a HW trained in
IMCI
Child seen by HW supervised in the last 5 m
perc
ent
IMCI IMCI ++ Non IMCI

Cambodia Health Facility Survey 2010
45
The management of diarrhoea and of pneumonia in IMCI and IMCI++ facilities was compared. There were 170 cases of diarrhoea and 56 cases of pneumonia in the survey. Diarrhea was diagnosed in 83 children in IMCI centres, 71 in IMCI++, and 16 in non-IMCI centres. Pneumonia was diagnosed in 25 children in IMCI centres, 26 in IMCI++, and 5 in non-IMCI centres. The non-IMCI centres were not included in the statistical comparison, but are shown in the graphs.
Indicators for management of diarrhoea and pneumonia are shown in Figures 34 and 35. Statistical comparisons between indicators for IMCI and IMCI++ facilities are shown in Table 12.
Figure 34: Case management of children with diarrhoea by facility type, Cambodia HFS, May 2010
Figure 35: Case management of children with pneumonia by facility type, Cambodia HFS, May 2010
0
10
20
30
40
50
60
Children with watery diarrhoea presecribed ORS and zinc
Children with watery diarrhoea advised to increase fluids and continue feeding
Children prescribed ORS whose caretakers knew how to give
perc
ent
IMCI IMCI ++ Non IMCI
0
10
20
30
40
50
60
70
80
90
100
Pneumonia correctly diagnosed
Pneumonia correctly treated
Child with pneumonia + given ab's and caretaker
knew how to give
Child with pneumonia + caretaker advised on when
to return immediately
perc
ent
IMCI IMCI ++ Non IMCI
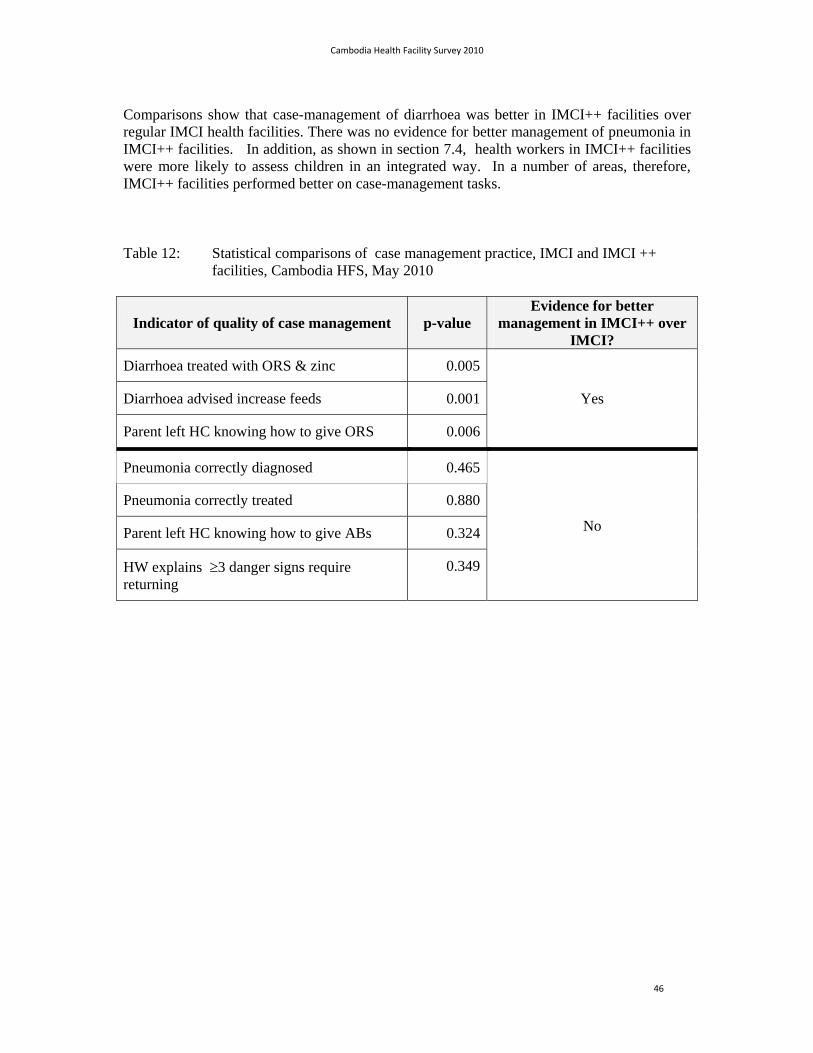
Cambodia Health Facility Survey 2010
46
Comparisons show that case-management of diarrhoea was better in IMCI++ facilities over regular IMCI health facilities. There was no evidence for better management of pneumonia in IMCI++ facilities. In addition, as shown in section 7.4, health workers in IMCI++ facilities were more likely to assess children in an integrated way. In a number of areas, therefore, IMCI++ facilities performed better on case-management tasks.
Table 12: Statistical comparisons of case management practice, IMCI and IMCI ++ facilities, Cambodia HFS, May 2010
Indicator of quality of case management p-value Evidence for better
management in IMCI++ over IMCI?
Diarrhoea treated with ORS & zinc 0.005
Yes Diarrhoea advised increase feeds 0.001
Parent left HC knowing how to give ORS 0.006
Pneumonia correctly diagnosed 0.465
No
Pneumonia correctly treated 0.880
Parent left HC knowing how to give ABs 0.324
HW explains 3 danger signs require returning
0.349

Summary of findings - comparison of IMCI and IMCI ++ facilities
There is evidence that IMCI++ facilities performed better in several areas of IMCI implementation, including:
More regular use of the IMCI approach
Better quality of supervision
More integrated approach to assessing sick children including checking vaccination status and plotting weights on growth charts
More frequent feeding assessments of sick children
More frequent use of ORS and zinc for diarrhoea
Better quality of counseling of caretakers on danger signs of when to return and how to give medications

Cambodia Health Facility Survey 2010
48
9. COMPARISON OF 2010 HFS AND 2006 HFS
The survey instruments and indicators used in both the 2006 and 2010 HFS were the same for children 2 to 59 months. The 2006 survey did not include the sick young infant 0-2 months of age, so these indicators cannot be compared. Indicator comparisons are shown in Table 13.
The data show that IMCI training coverage is much higher in 2010 than 2006. IMCI has been scaled up successfully to most areas of the country. This has been achieved at the same time as decentralization of planning and budgeting to district and provincial levels. During this time, the quality of care provided by health centres has not changed for most measures. Upward trends are noted in the following areas:
Proportion of sick children having their vaccination status checked
The index of integrated assessment of sick children
The proportion of sick children under 2 years receiving feeding assessments
The proportion of sick children needing an antibiotic who receive it, and
The proportion of caretakers who leave facilities with correct knowledge of how to give oral treatments.
These trends are positive. It should be noted, however, that many measures of quality of care have not changed, despite the fact that a much higher proportion of health facilities now have two or more IMCI trained health workers available. Many of these workers will have received refresher training since 2006. This finding confirms findings from the 2010 survey – that in many cases the IMCI approach is not used even when staff have been trained – and that ongoing supportive supervision is important for sustaining practices over time.

Cambodia Health Facility Survey 2010
49
Table 13: Comparisons of key indicators, HFS 2006 and HFS 2010
Indicator Total across all groups % or mean, (95%CI)
HFS 2006 HFS 2010
Proportion of children checked for all 3 danger signs 41.9% (37.3-46.6) 41.6% (36.9-46.3)
Proportion of children checked for the presence of cough, diarrhoea, fever
78.9% (74.9-82.5) 84.2% (80.8-87.7)
Child weighed and weight checked against a growth chart
53.5% (48.8-58.1) 54.4% (49.6-59.1)
Child <2yo assessed for feeding practices 30.4% (25.5-35.6) 41.8% (36.2-47.5)
Index of Integrated Assessment (mean number tasks done out of 10)
6.5 (6.4-6.6) 7.23 (7.0-7.5)
Child needing an antibiotic is correctly prescribed it 45.5% (36.4-54.8) 62.2% (53.7-70.8)
Child not needing antibiotic leaves without antibiotics
73.4% (68.5-77.9) 58.1% (53.4-62.8)
Caretakers know how to give oral treatment prescribed
24.9% (19.8-30.6) 60.2% (54.1-66.2)
Caretaker advised to continue feeds and give extra fluids
49.8% (45.0-54.5) 49.0% (44.2-53.8)
Vaccination status checked 57.5% (52.8-62.0) 85.9% (82.6-89.2)
Child needing a vaccine received all needed vaccinations
32.4% (23.4-42.3) 30.6% (19.7-41.5)
Index of oral drugs available 7.05 (7.02-7.08) of 8 of 7
Index of injectable drugs available 2.5 (2.37-2.64) of 4 of 3
Facility received supervisory visit including case obs. in past 6 Months
44.2% (35.1-53.5) 42.5% (33.5-51.5)
Proportion of HW trained in IMCI 62.9% (58.6-67.1) 83.0% (79.4-86.6)

Cambodia Health Facility Survey 2010
50
Summary of findings – comparison of 2010 and 2006 HFS
IMCI coverage has increased dramatically since 2006 Upward trends are noted for several indicators of quality of care since
2006, although overall there has been little significant change
Improving quality of care further will require investments in supportive supervision and other supports to ensure that the IMCI approach is used consistently
There is an urgent need to develop approaches to improving quality of care at first level facilities as well as at the referral level.

10. CONCLUSIONS
Main conclusions from the health facility survey are:
1. IMCI coverage in Cambodia is high.
2. IMCI facilities generally perform better than non-IMCI facilities on all measures of quality of care.
3. IMCI ++ health facilities tend to perform better than IMCI facilities without incentives in a number of areas, including more regular use of the IMCI approach, better quality of supervision, more integrated assessments, more frequent use of zinc for the treatment of diarrhoea and better quality counseling.
4. Key supports for IMCI are generally available, including:
Trained HWs
Essential medicines, vaccines and supplies
Functional cold chain
Regular supervisory visits
Health centre management committees
Soap and water
5. Health workers generally have an integrated approach to the sick child.
They perform on average 7 out of 10 key assessment tasks
Assessment and counseling of breastfeeding is generally done well
Mothers are asked about their health and family planning
6. Diarrhoea is generally managed well in both young infants and older children, with widespread use of ORS and increasing use of zinc
7. System supports that need improvement are:
Quality of supervision. Supervision often does not include an observation of case-management practice, feedback and problem solving.
Availability of some essential medicines and supplies - injectable ampicillin and gentamicin, oral ciprofloxacin, magnesium sulfate, and nasogastric tubes were often not available.
Referral. Although referral facilities are geographically close to most caretakers, health workers report that children needing referral are not taken in at least 20% of cases. More information on barriers to referral is needed.

Cambodia Health Facility Survey 2010
52
8. Case-management practices that need improvement are:
More widespread use of the IMCI approach
Currently used for 70% of cases in IMCI ++ facilities
Currently used for 20% of cases in IMCI facilities
Assessment and treatment of sick children
Checking for 3 danger signs is poor, occurring in <50% of cases
Children are weighed, but often not checked against a growth chart
A full assessment of feeding practices is often not done
Children with pneumonia are often not prescribed antibiotics correctly
Zinc still not used frequently enough for the treatment of diarrhoea
Assessment and treatment of young infants
Young infants are poorly assessed for all key signs
Very severe disease is often not classified correctly
Infants needing antibiotics are often not given them correctly
Infants with very severe disease needing referral are often not referred
Breastfeeding problems often not classified correctly
Caretakers often not counseled on danger signs
Counseling of mothers
Advice to mothers on danger signs or when to urgently return for care is not done often enough
Mothers leave the health centre not knowing important information
o <50% of HW explain how to give an oral medication
o 70% (95%CI: 68 – 73) of mothers know how to give AB
o 40% (95%CI: 42 – 62) of mothers know how to give ORS
o Only half of mothers are told to increase feeding during illness

Cambodia Health Facility Survey 2010
53
Missed opportunities to vaccinate
Children needing vaccines are often not given them
o IMCI facilities: <40%
o Non-IMCI facilities: 15%
Hand washing
Handwashing is rarely practices before, during or after a consultation, despite wide availability of soap and water.
Cambodia Health Facility Survey 2010
54
11. DRAFT RECOMMENDATIONS FROM FINDINGS OF THE HEALTH FACILITY SURVEY 2010
Improvements in the quality IMCI require a focus on:
1. Supportive supervision
2. Care of the young infant
3. Assessment of danger signs
4. Appropriate use of antibiotics
5. Counseling of the mother or caretaker
11.1. SPECIFIC RECOMMENDATIONS:
IMCI Training
Standard 11 day course
Emphasize care of the young infant in IMCI training. The Care of the Young Infant module should be taught early in the training rather than at the end, and re-visited during the training to emphasize its importance.
Emphasize the need to conduct assessment tasks correctly and to classify sick child based on this assessment. Review guidelines for treatment with antibiotics.
Reinforce the need to screen the vaccination status of sick children and to vaccinate the same day.
Emphasize counseling of the mother or caretaker on danger signs for seeking care with their child, and how to give treatment correctly at home. Consider:
o Increased use of counseling role-plays.
o Making a pass mark in counseling practices a requirement for passing IMCI training.
Care for the Young Infant should not be appended on to the end of the existing IMCI training block, but should be introduced early, and constantly revisited during training.
Refresher Training (5 day course)
Review and revise the refresher course curriculum to focus on the main areas of weakness
o Assessment of ARI (counting respiratory rate and looking for in-drawing).
o Correct antibiotic treatment.
o Assessment of newborn (recognizing that newborns often do not present with clear clinical signs but may still be severely ill).

Cambodia Health Facility Survey 2010
55
o Counseling the mother (antibiotic treatment, danger signs and when to return immediately, feeding).
o Assessment of growth using the growth chart.
o Opportunistic catch up for vaccinations.
o Treatment of diarrhoea using ORS and Zinc.
Pre-service IMCI
Complete the ICATT (IMCI Computerized Adaptation & Training Tool) adaption, field test and begin at University of Health Sciences for training Year 7 & 8 medical students on their paediatric rotation.
Roll out IMCI training by ICATT to TSMC for nursing and midwifery students and then to all Regional Training Centres over the next 3 years.
IMCI Implementation
Health Centre
All sick children should be assessed using IMCI.
Regularly audit the availability of injectable antibiotics and drugs used in obstetric emergencies. These should be made available in stock through regular ordering and ensuring a budget line is available for these items.
Audit the availability of mother’s card and order these from the Ministry of Health.
Water and soap should be made available in the room in which children are seen.
Regular promotion of handwashing.
PHD/OD
IMCI focal points to be appointed with an orientation on terms of reference and roles and responsibilities.
Ensure availability of injectable drugs and obstetric drugs for all HCs
Ensure follow up after training and supervision is included in AOP
Supervisory visits should:
1. Include case observation and review of case management.
Focus on assessment of danger signs of illness
Focus on the appropriate use of antibiotics, and encourage their use where indicated.
2. Include review of counseling of the mother and provide supportive feedback
Cambodia Health Facility Survey 2010
56
Focus on explaining to the mother the use of oral medication
Focus on recognizing danger signs of illness for which the mother should return to the health centre.
3. Focus specifically on the young infant: If no young infants are available during the supervisory visits, consideration should be given to using case scenarios as reminders for key areas of assessment and management of the young infant.
4. Remind health workers about hand washing.
Central Ministry of Health
Review of PHD/OD supervision and supervisory check list for IMCI and monitoring mechanisms
Discuss with DPHI about adding IMCI consultation data to HC1 form for better monitoring of IMCI implementation
Discuss with DPHI about collection of age disaggregated data through HIS (neonates, infants and under 5 years) from HC level (HC1) in order to be able to use the HIS data for monitoring of child survival interventions
Consideration and debate regarding the benefits and opportunity costs of investment in incentivized IMCI should be undertaken.
Discuss the possibilities of specific IMCI indicators being part of business plans for Service Delivery Grants (Special Operating Agencies)
IMCI Mother’s Card should be reviewed, revised (with new feeding recommendations in pictorial format from the National Nutrition Programme), printed and disseminated.
11.2. FURTHER SUGGESTED OPERATIONS RESEARCH
Barriers to referral (HC to RH) should be explored, including an evaluation of financial barriers and mechanisms for their alleviation
The low attendance of infants in the first few months of life should be further explored through qualitative and quantitative research. Possible explanations such as cultural attitudes may be amenable to parental advice or mass marketing campaigns about attendance to healthcare if their child shows any danger signs
Cambodia Health Facility Survey 2010
57
11.3. ACKNOWLEDGMENTS
Many thanks to the support and direction provided by His Excellency Professor Eng Hout, Secretary of State for Health and by Professor Sann Chan Soeung, Deputy Director General for Health, Ministry of Health, Cambodia.
Thanks are due to parents and children observed in the survey and to participating health centre staff.
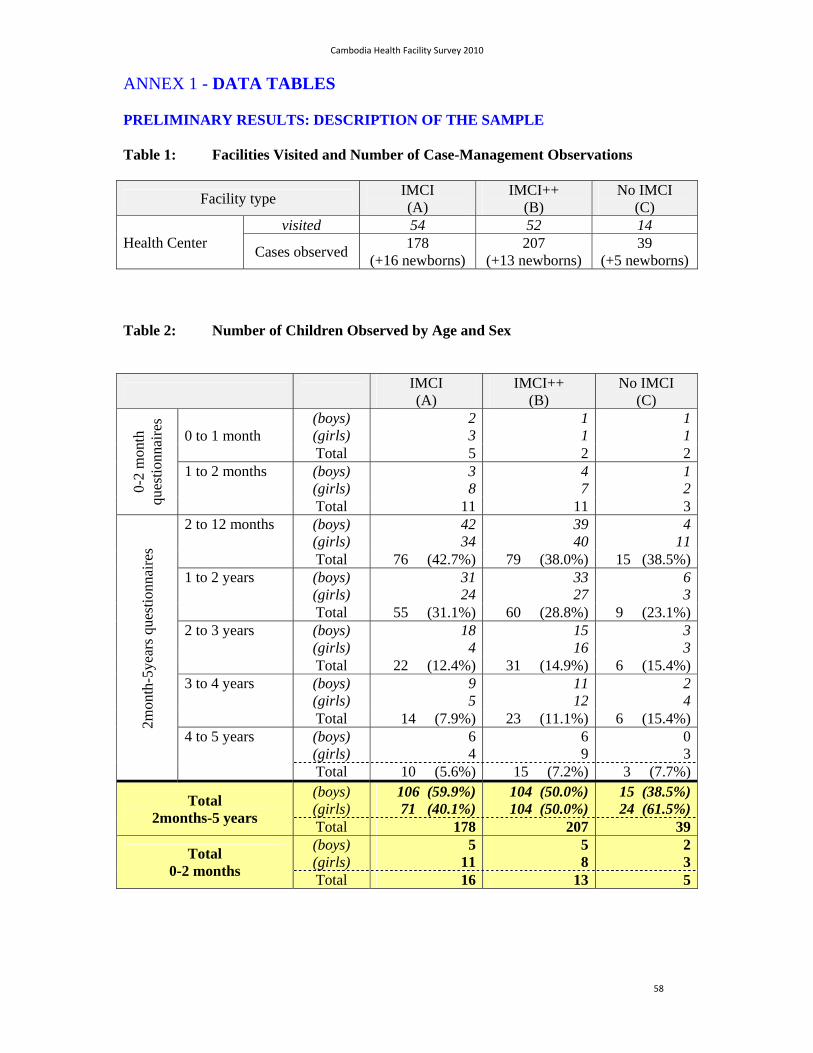
Cambodia Health Facility Survey 2010
58
ANNEX 1 - DATA TABLES
PRELIMINARY RESULTS: DESCRIPTION OF THE SAMPLE
Table 1: Facilities Visited and Number of Case-Management Observations
Facility type IMCI (A)
IMCI++ (B)
No IMCI (C)
Health Center visited 54 52 14
Cases observed 178
(+16 newborns) 207
(+13 newborns) 39
(+5 newborns)
Table 2: Number of Children Observed by Age and Sex
IMCI (A)
IMCI++ (B)
No IMCI (C)
0-2
mon
th
ques
tionn
aire
s
0 to 1 month (boys) (girls)
23
1 1
11
Total 5 2 21 to 2 months (boys)
(girls) 38
4 7
12
Total 11 11 3
2mon
th-5
year
s qu
estio
nnai
res
2 to 12 months (boys) (girls)
4234
39 40
411
Total 76 (42.7%) 79 (38.0%) 15 (38.5%)1 to 2 years (boys)
(girls) 3124
33 27
63
Total 55 (31.1%) 60 (28.8%) 9 (23.1%)2 to 3 years (boys)
(girls) 184
15 16
33
Total 22 (12.4%) 31 (14.9%) 6 (15.4%)3 to 4 years (boys)
(girls) 95
11 12
24
Total 14 (7.9%) 23 (11.1%) 6 (15.4%)4 to 5 years (boys)
(girls) 64
6 9
03
Total 10 (5.6%) 15 (7.2%) 3 (7.7%)
Total 2months-5 years
(boys) (girls)
106 (59.9%)71 (40.1%)
104 (50.0%) 104 (50.0%)
15 (38.5%)24 (61.5%)
Total 178 207 39
Total 0-2 months
(boys) (girls)
511
5 8
23
Total 16 13 5
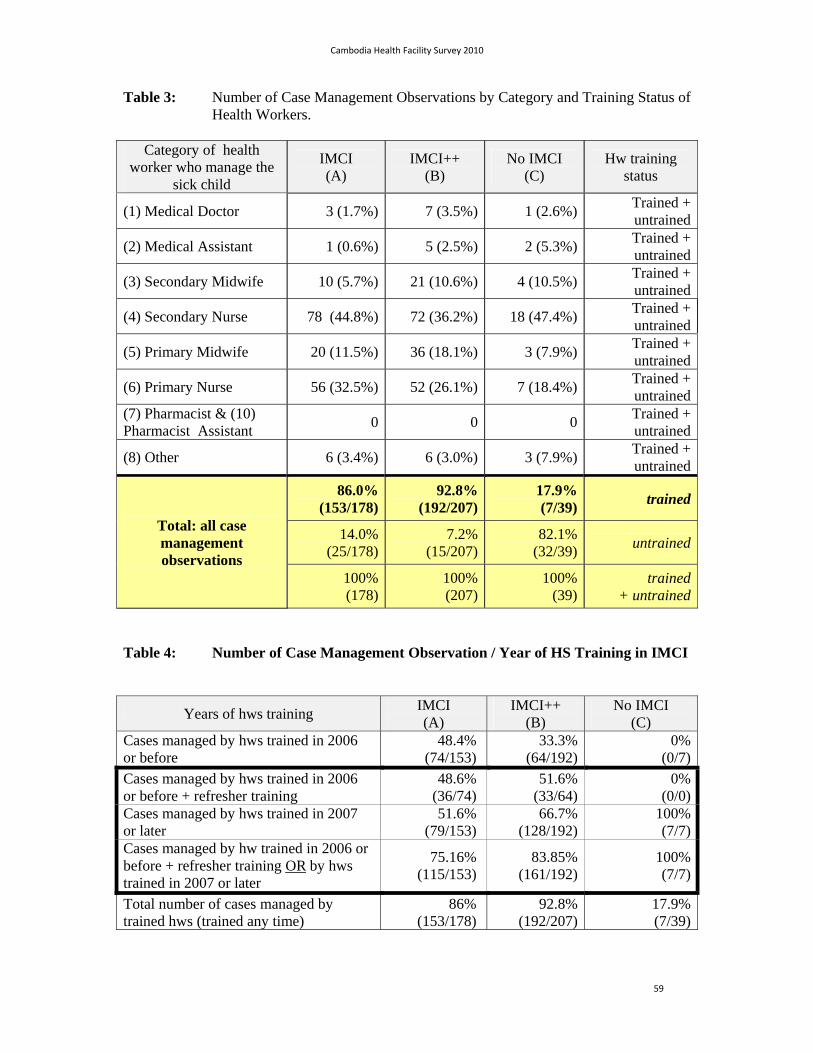
Cambodia Health Facility Survey 2010
59
Table 3: Number of Case Management Observations by Category and Training Status of Health Workers.
Category of health worker who manage the
sick child
IMCI (A)
IMCI++ (B)
No IMCI (C)
Hw training status
(1) Medical Doctor 3 (1.7%) 7 (3.5%) 1 (2.6%) Trained + untrained
(2) Medical Assistant 1 (0.6%) 5 (2.5%) 2 (5.3%) Trained + untrained
(3) Secondary Midwife 10 (5.7%) 21 (10.6%) 4 (10.5%) Trained + untrained
(4) Secondary Nurse 78 (44.8%) 72 (36.2%) 18 (47.4%) Trained + untrained
(5) Primary Midwife 20 (11.5%) 36 (18.1%) 3 (7.9%) Trained + untrained
(6) Primary Nurse 56 (32.5%) 52 (26.1%) 7 (18.4%) Trained + untrained
(7) Pharmacist & (10) Pharmacist Assistant
0 0 0 Trained + untrained
(8) Other 6 (3.4%) 6 (3.0%) 3 (7.9%) Trained + untrained
Total: all case management observations
86.0%(153/178)
92.8%(192/207)
17.9% (7/39)
trained
14.0%(25/178)
7.2%(15/207)
82.1% (32/39)
untrained
100%(178)
100%(207)
100% (39)
trained+ untrained
Table 4: Number of Case Management Observation / Year of HS Training in IMCI
Years of hws training IMCI (A)
IMCI++ (B)
No IMCI (C)
Cases managed by hws trained in 2006 or before
48.4% (74/153)
33.3% (64/192)
0%(0/7)
Cases managed by hws trained in 2006 or before + refresher training
48.6% (36/74)
51.6% (33/64)
0%(0/0)
Cases managed by hws trained in 2007 or later
51.6% (79/153)
66.7% (128/192)
100%(7/7)
Cases managed by hw trained in 2006 or before + refresher training OR by hws trained in 2007 or later
75.16% (115/153)
83.85% (161/192)
100%(7/7)
Total number of cases managed by trained hws (trained any time)
86% (153/178)
92.8% (192/207)
17.9%(7/39)

Cambodia Health Facility Survey 2010
60
Table 5: Number of Case Managed by IMCI trained health workers who received at least one visit of supervision during the last 6 months or during the last 18 months
IMCI (A)
IMCI++ (B)
No IMCI (C)
Cases managed by hws trained in IMCI and supervised at least once in 2010 (= during previous 5 months)
30.72% (47/153)
of the children managed by trained
hws
[or 26.4% of the total number of children]
64.1% (123/192)
of the children managed by trained
hws
[or 59.4% of the total number of children]
0.0% (0/7)
of the children managed by trained
hws
[or 0.0% of the total number of
children] Cases managed by hws trained in IMCI and who were not supervised in 2010 but had at least one supervision in 2009 (between 5 to 17 months prior to the survey)
16.3% (25/153)
of the children managed by trained
hws
[or 14.0% of the total number of children]
18.3% (28/153)
of the children managed by trained
hws
[or 13.5% of the total number of children]
14.3% (1/7)
of the children managed by trained
hws
[or 2.56% of the total number of
children]
Table 6: Caretaker reasons for bringing the child to the health facility on the day of the survey (and reasons from bringing children aged 0 to 2 months to the facility)
Reported complaints IMCI (A)
IMCI++ (B)
No IMCI (C)
Diarrhea 42.7%
(76/178) 42.8%
(89/208) 30.8%
(12/39)
Fever 77.0%
(137/178) 84.1%
(175/208) 82.1%
(32/39)
Difficult breathing/ cough 60.1%
(107/178) 63.9%
(133/208) 56.4%
(22/39)
Ear problem 6.2%
(11/178) 15.9%
(33/208) 0 0
Well child/ immunization 1.7%
(3/178) 2.4%
(5/208) 0 0
Others (most frequent: skin diseases; abscesses; and injuries)
15.2% (27/178)
21.2% (44/208)
10.3% (4/39)
Average reported problems per child (for 5 IMCI conditions):
1.88 2.09 1.69
Average reported problems per child including problems not included in IMCI ("others")
2.03 2.30 1.79
(x) children aged 0 to 2 months
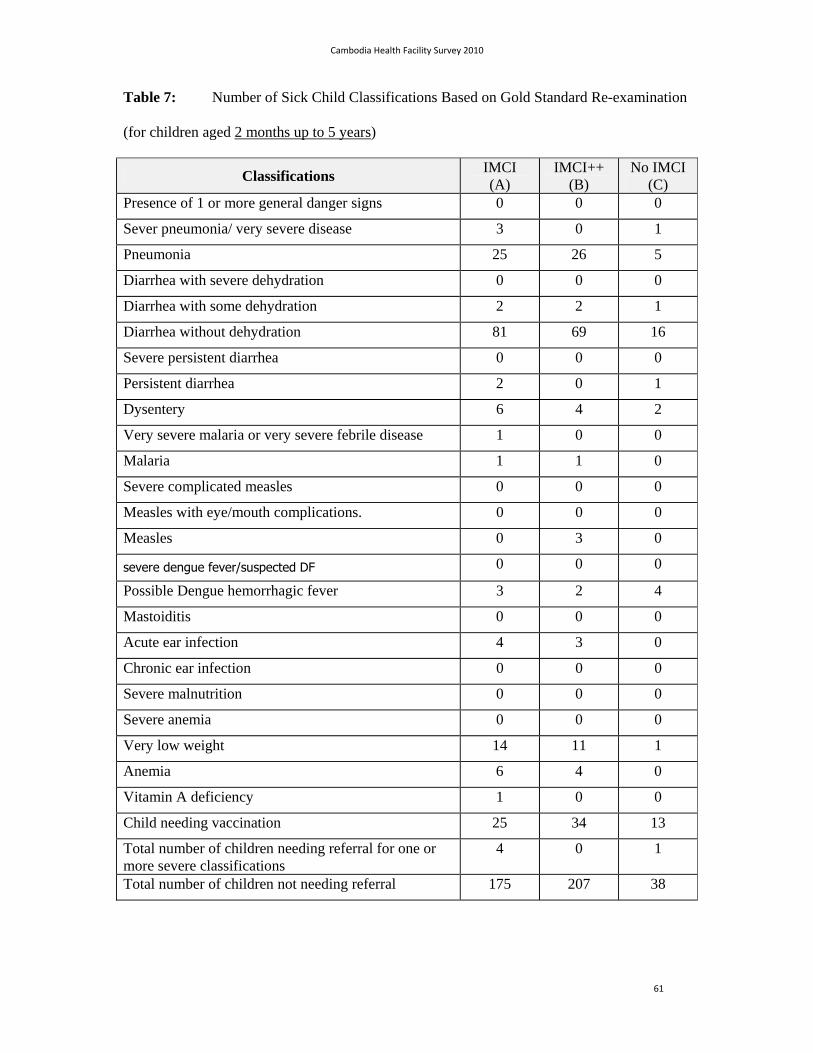
Cambodia Health Facility Survey 2010
61
Table 7: Number of Sick Child Classifications Based on Gold Standard Re-examination
(for children aged 2 months up to 5 years)
Classifications IMCI (A)
IMCI++ (B)
No IMCI (C)
Presence of 1 or more general danger signs 0 0 0
Sever pneumonia/ very severe disease 3 0 1
Pneumonia 25 26 5
Diarrhea with severe dehydration 0 0 0
Diarrhea with some dehydration 2 2 1
Diarrhea without dehydration 81 69 16
Severe persistent diarrhea 0 0 0
Persistent diarrhea 2 0 1
Dysentery 6 4 2
Very severe malaria or very severe febrile disease 1 0 0
Malaria 1 1 0
Severe complicated measles 0 0 0
Measles with eye/mouth complications. 0 0 0
Measles 0 3 0
severe dengue fever/suspected DF 0 0 0
Possible Dengue hemorrhagic fever 3 2 4
Mastoiditis 0 0 0
Acute ear infection 4 3 0
Chronic ear infection 0 0 0
Severe malnutrition 0 0 0
Severe anemia 0 0 0
Very low weight 14 11 1
Anemia 6 4 0
Vitamin A deficiency 1 0 0
Child needing vaccination 25 34 13
Total number of children needing referral for one or more severe classifications
4 0 1
Total number of children not needing referral 175 207 38
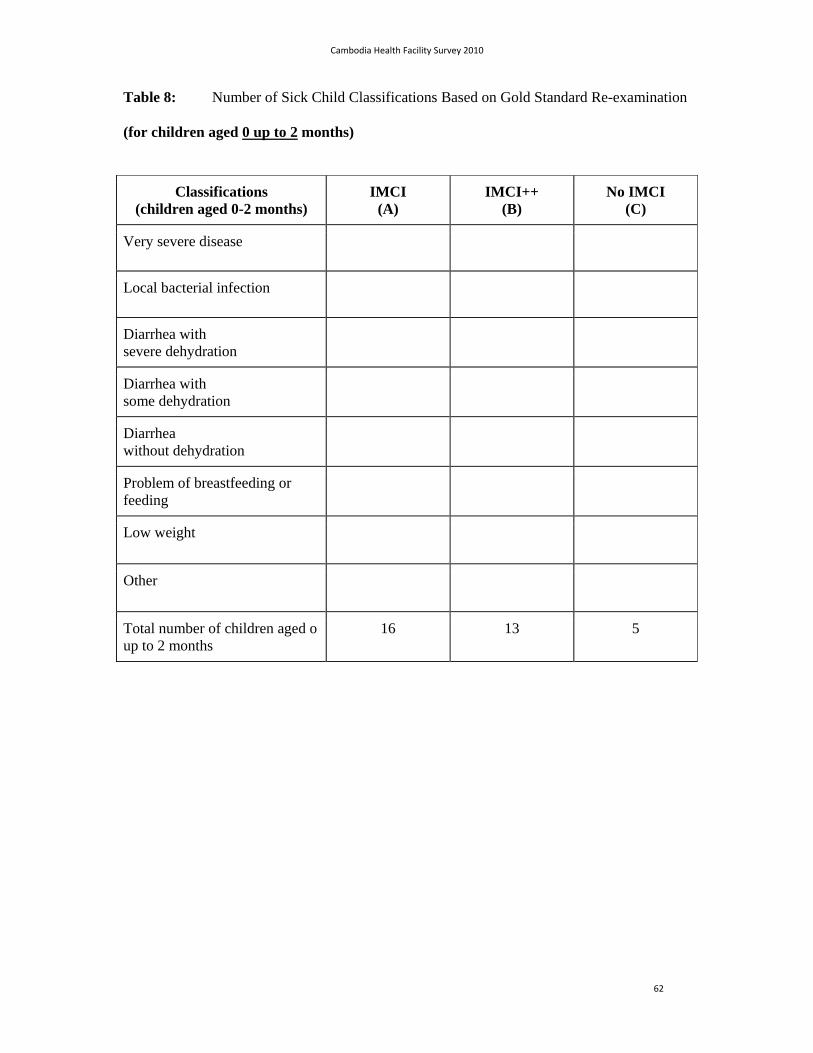
Cambodia Health Facility Survey 2010
62
Table 8: Number of Sick Child Classifications Based on Gold Standard Re-examination
(for children aged 0 up to 2 months)
Classifications (children aged 0-2 months)
IMCI (A)
IMCI++ (B)
No IMCI (C)
Very severe disease
Local bacterial infection
Diarrhea with severe dehydration
Diarrhea with some dehydration
Diarrhea without dehydration
Problem of breastfeeding or feeding
Low weight
Other
Total number of children aged o up to 2 months
16 13 5

Cambodia Health Facility Survey 2010
63
Table 9: Priority Indicators (Children aged 2 months up to 5 years)
Priority Indicators IMCI (A)
IMCI++ (B)
No IMCI (C)
1. Proportion of children checked for three general danger signs
46.1% (82/178)
44.2% (92/208)
7.7% (3/39)
ability to drink or breastfeed 68.6% (120/175)
69.8% (139/199)
25.6% (10/39)
Vomits everything 58.4% (104/178)
56.3% (116/206)
23.1% (9/39)
Convulsions 52.8% (94/178)
61.5% (128/208)
10.3% (4/39)
2 Proportion of children checked for the presence of cough, diarrhoea, and fever
83.1% (148/178)
88.5% (184/208)
66.7% (26/39)
3. Proportion of children who have been weighed the same day and have their weight checked against a recommended growth chart
49.4% (88/178)
64.9% (135/208)
20.5 (8/39)
Children weighed 89.3% (158/177)
92.8% (193/208)
53.8% (21/39)
Weight checked against growth chart 50.3% (89/177)
65.4% (136/208)
25.6% (10/39)
4. Proportion of children who have their vaccination status checked
86.0% (153/178)
94.2% (196/208)
41.0% (16/39)
5: Index of integrated assessment (mean of 10 tasks performed)
7.18 7.68 4.40
6. Proportion of children under two years of age whose caretakers are asked about breastfeeding, complementary foods, and feeding practices during this episode of illness
38.9% (51/131)
51.1% (71/139)
4.2% (1/24)
7a. Proportion of children who do not need urgent referral, who need an oral antibiotic who are prescribed the antibiotic correctly
58.2% (32/55)
73.3% (44/60)
21.4% (3/14)
7b. Proportion of children who do not need urgent referral, who need an antimalarial
who are prescribed the antimalarial correctly0/2 0/2 0/1
8. Proportion of children, who do not need urgent referral and who do not need antibiotic for one or more IMCI classifications, who leave the facility without having received or been prescribed antibiotics
58.9% (103/175)
60.4% (125/207)
42.1% (16/38)
9. Proportion of sick children whose caretakers are advised to give extra fluid and continue feeding
43.4% (76/175)
59.9% (124/207)
15.8% (6/38)
10: Child needing vaccinations leaves the facility with all needed vaccinations (based on vaccination card or history)
40.0% (10/25)
29.4% (10/34)
15.4% (2/13)
11. Proportion of children prescribed ORS, and/or oral antibiotic and/or an oral antimalarial whose caretaker can describe correctly how to give the treatment
59.3% (64/108)
67.5% (81/120)
32.1% (9/28)
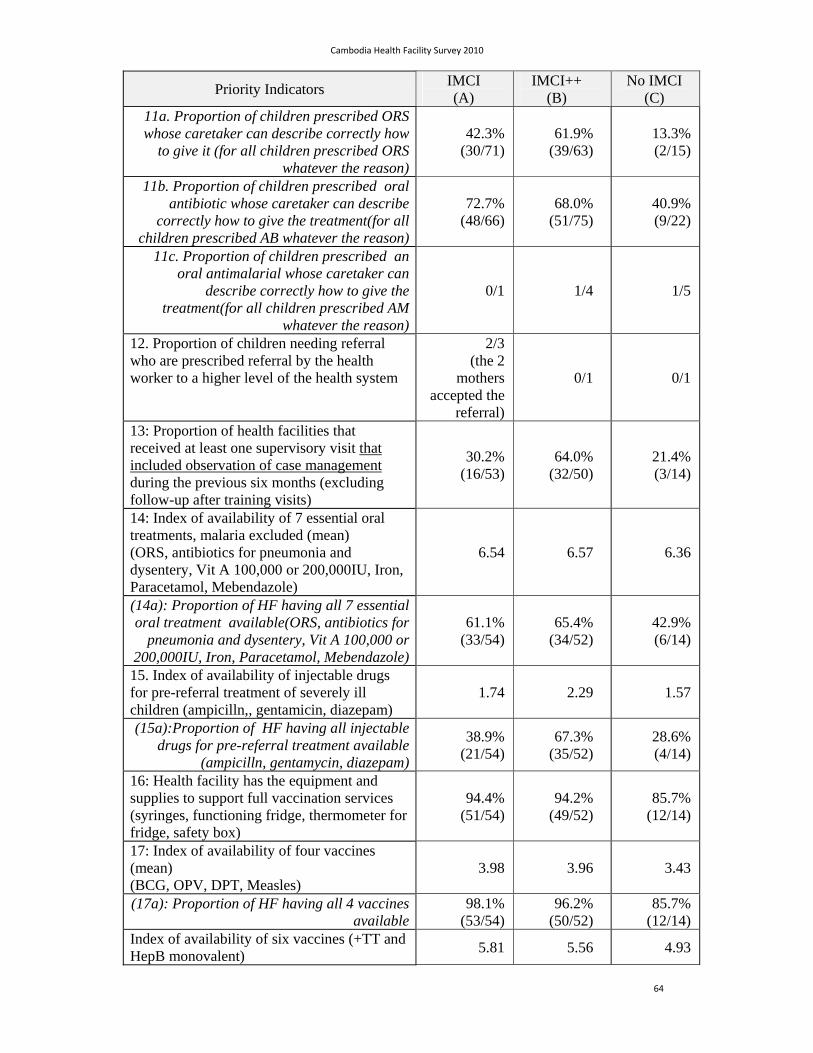
Cambodia Health Facility Survey 2010
64
Priority Indicators IMCI (A)
IMCI++ (B)
No IMCI (C)
11a. Proportion of children prescribed ORS whose caretaker can describe correctly how
to give it (for all children prescribed ORS whatever the reason)
42.3% (30/71)
61.9% (39/63)
13.3% (2/15)
11b. Proportion of children prescribed oral antibiotic whose caretaker can describe
correctly how to give the treatment(for all children prescribed AB whatever the reason)
72.7% (48/66)
68.0% (51/75)
40.9% (9/22)
11c. Proportion of children prescribed an oral antimalarial whose caretaker can
describe correctly how to give the treatment(for all children prescribed AM
whatever the reason)
0/1 1/4 1/5
12. Proportion of children needing referral who are prescribed referral by the health worker to a higher level of the health system
2/3 (the 2
mothers accepted the
referral)
0/1 0/1
13: Proportion of health facilities that received at least one supervisory visit that included observation of case management during the previous six months (excluding follow-up after training visits)
30.2% (16/53)
64.0% (32/50)
21.4% (3/14)
14: Index of availability of 7 essential oral treatments, malaria excluded (mean) (ORS, antibiotics for pneumonia and dysentery, Vit A 100,000 or 200,000IU, Iron, Paracetamol, Mebendazole)
6.54 6.57 6.36
(14a): Proportion of HF having all 7 essential oral treatment available(ORS, antibiotics for
pneumonia and dysentery, Vit A 100,000 or 200,000IU, Iron, Paracetamol, Mebendazole)
61.1% (33/54)
65.4% (34/52)
42.9% (6/14)
15. Index of availability of injectable drugs for pre-referral treatment of severely ill children (ampicilln,, gentamicin, diazepam)
1.74 2.29 1.57
(15a):Proportion of HF having all injectable drugs for pre-referral treatment available
(ampicilln, gentamycin, diazepam)
38.9% (21/54)
67.3% (35/52)
28.6% (4/14)
16: Health facility has the equipment and supplies to support full vaccination services (syringes, functioning fridge, thermometer for fridge, safety box)
94.4% (51/54)
94.2% (49/52)
85.7% (12/14)
17: Index of availability of four vaccines (mean) (BCG, OPV, DPT, Measles)
3.98 3.96 3.43
(17a): Proportion of HF having all 4 vaccines available
98.1% (53/54)
96.2% (50/52)
85.7% (12/14)
Index of availability of six vaccines (+TT and HepB monovalent)
5.81 5.56 4.93

Cambodia Health Facility Survey 2010
65
Priority Indicators IMCI (A)
IMCI++ (B)
No IMCI (C)
Proportion of HF having all 6 vaccines (BCG, Polio, DTP-Hep or Pentavalent,
Measles, TT, HepB)
81.1% (43/53)
62.0% (31/50)
64.3% (9/14)
18: Proportion of health facilities with at least 60% of workers managing children trained in IMCI
72.2% (39/54)
90.4% (47/52)
21.4% (3/14)
(18a): Health facilities with at least 60% of the health workers present the day of visit and
managing children trained in IMCI
64.8% (35/54)
73.1% (38/52)
21.4% (3/14)
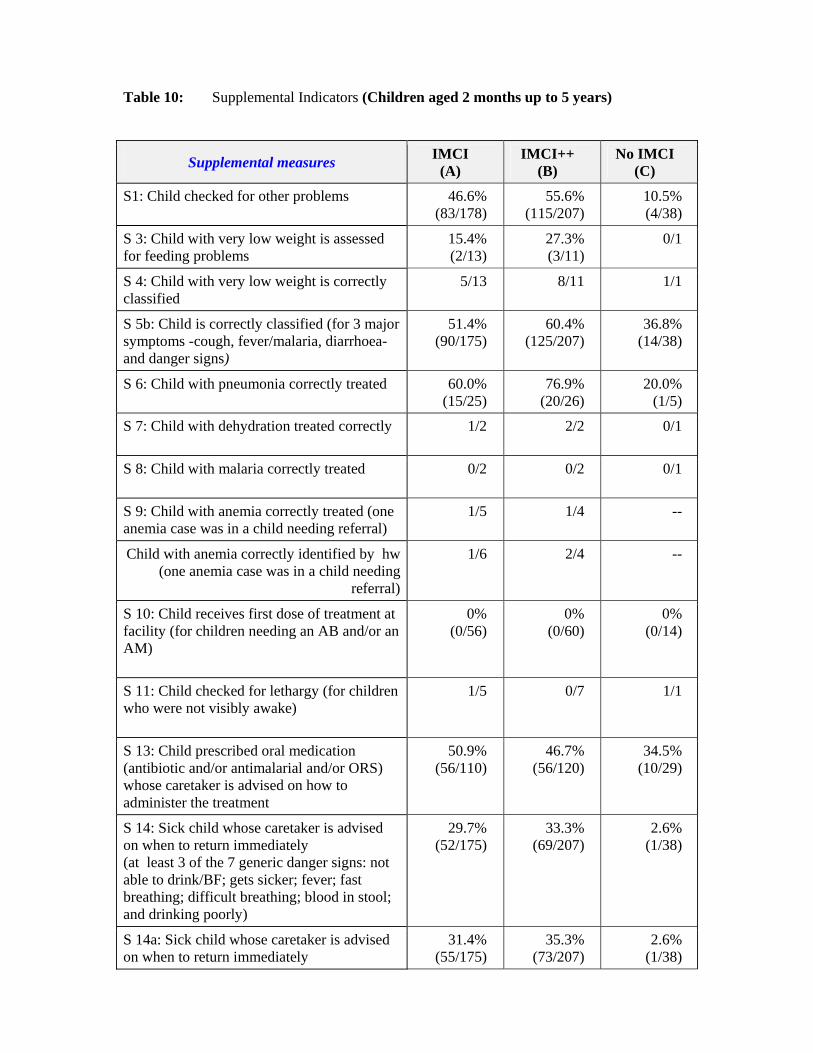
Table 10: Supplemental Indicators (Children aged 2 months up to 5 years)
Supplemental measures IMCI
(A) IMCI++
(B) No IMCI
(C)
S1: Child checked for other problems 46.6% (83/178)
55.6% (115/207)
10.5% (4/38)
S 3: Child with very low weight is assessed for feeding problems
15.4% (2/13)
27.3% (3/11)
0/1
S 4: Child with very low weight is correctly classified
5/13 8/11 1/1
S 5b: Child is correctly classified (for 3 major symptoms -cough, fever/malaria, diarrhoea- and danger signs)
51.4% (90/175)
60.4% (125/207)
36.8% (14/38)
S 6: Child with pneumonia correctly treated
60.0% (15/25)
76.9% (20/26)
20.0% (1/5)
S 7: Child with dehydration treated correctly
1/2 2/2 0/1
S 8: Child with malaria correctly treated
0/2 0/2 0/1
S 9: Child with anemia correctly treated (one anemia case was in a child needing referral)
1/5 1/4 --
Child with anemia correctly identified by hw (one anemia case was in a child needing
referral)
1/6 2/4 --
S 10: Child receives first dose of treatment at facility (for children needing an AB and/or an AM)
0% (0/56)
0% (0/60)
0% (0/14)
S 11: Child checked for lethargy (for children who were not visibly awake)
1/5 0/7 1/1
S 13: Child prescribed oral medication (antibiotic and/or antimalarial and/or ORS) whose caretaker is advised on how to administer the treatment
50.9% (56/110)
46.7% (56/120)
34.5% (10/29)
S 14: Sick child whose caretaker is advised on when to return immediately (at least 3 of the 7 generic danger signs: not able to drink/BF; gets sicker; fever; fast breathing; difficult breathing; blood in stool; and drinking poorly)
29.7% (52/175)
33.3% (69/207)
2.6% (1/38)
S 14a: Sick child whose caretaker is advised on when to return immediately
31.4% (55/175)
35.3% (73/207)
2.6% (1/38)
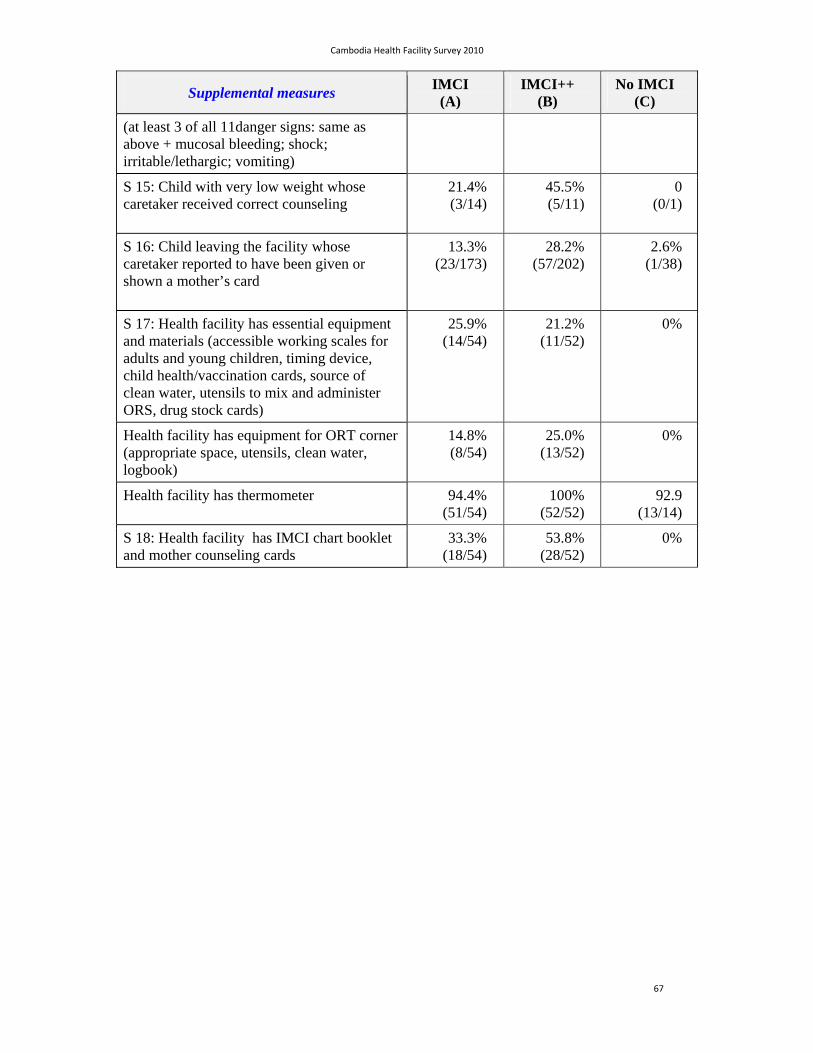
Cambodia Health Facility Survey 2010
67
Supplemental measures IMCI
(A) IMCI++
(B) No IMCI
(C)
(at least 3 of all 11danger signs: same as above + mucosal bleeding; shock; irritable/lethargic; vomiting)
S 15: Child with very low weight whose caretaker received correct counseling
21.4% (3/14)
45.5% (5/11)
0 (0/1)
S 16: Child leaving the facility whose caretaker reported to have been given or shown a mother’s card
13.3% (23/173)
28.2% (57/202)
2.6% (1/38)
S 17: Health facility has essential equipment and materials (accessible working scales for adults and young children, timing device, child health/vaccination cards, source of clean water, utensils to mix and administer ORS, drug stock cards)
25.9% (14/54)
21.2% (11/52)
0%
Health facility has equipment for ORT corner (appropriate space, utensils, clean water, logbook)
14.8% (8/54)
25.0% (13/52)
0%
Health facility has thermometer 94.4% (51/54)
100% (52/52)
92.9 (13/14)
S 18: Health facility has IMCI chart booklet and mother counseling cards
33.3% (18/54)
53.8% (28/52)
0%
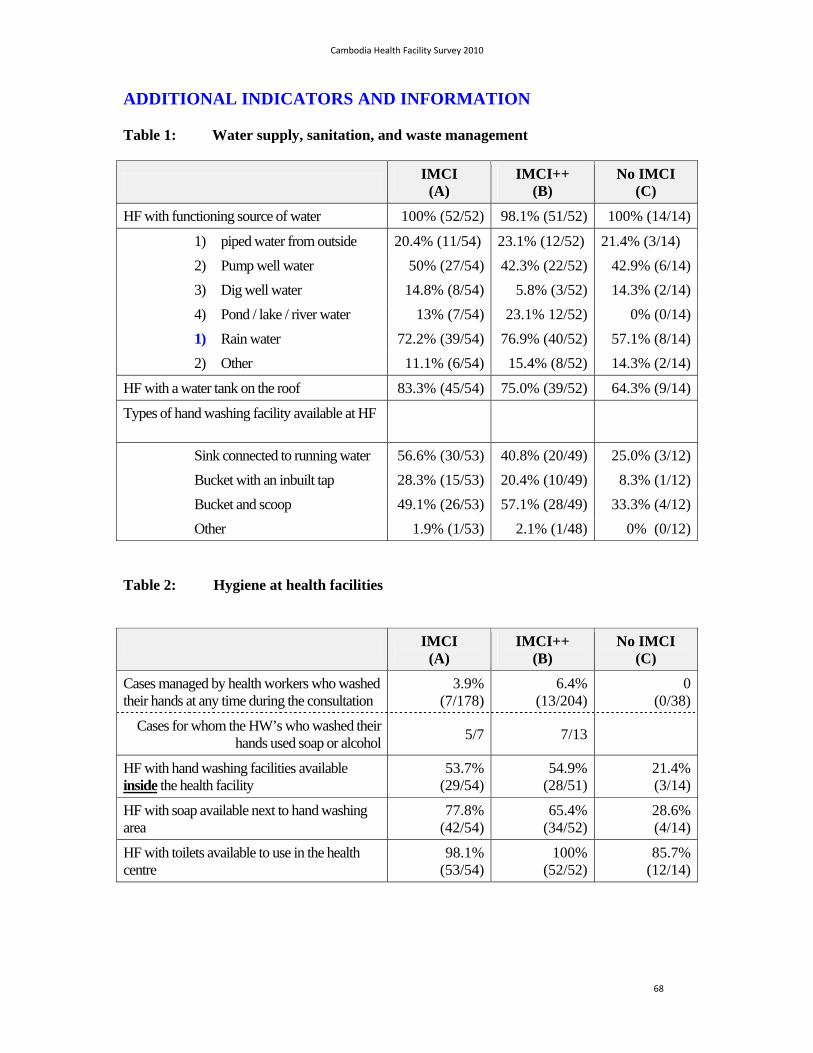
Cambodia Health Facility Survey 2010
68
ADDITIONAL INDICATORS AND INFORMATION
Table 1: Water supply, sanitation, and waste management
IMCI
(A) IMCI++
(B) No IMCI
(C)
HF with functioning source of water 100% (52/52) 98.1% (51/52) 100% (14/14)
1) piped water from outside 20.4% (11/54) 23.1% (12/52) 21.4% (3/14)
2) Pump well water 50% (27/54) 42.3% (22/52) 42.9% (6/14)
3) Dig well water 14.8% (8/54) 5.8% (3/52) 14.3% (2/14)
4) Pond / lake / river water 13% (7/54) 23.1% 12/52) 0% (0/14)
1) Rain water 72.2% (39/54) 76.9% (40/52) 57.1% (8/14)
2) Other 11.1% (6/54) 15.4% (8/52) 14.3% (2/14)
HF with a water tank on the roof 83.3% (45/54) 75.0% (39/52) 64.3% (9/14)
Types of hand washing facility available at HF
Sink connected to running water 56.6% (30/53) 40.8% (20/49) 25.0% (3/12)
Bucket with an inbuilt tap 28.3% (15/53) 20.4% (10/49) 8.3% (1/12)
Bucket and scoop 49.1% (26/53) 57.1% (28/49) 33.3% (4/12)
Other 1.9% (1/53) 2.1% (1/48) 0% (0/12)
Table 2: Hygiene at health facilities
IMCI
(A) IMCI++
(B) No IMCI
(C)
Cases managed by health workers who washed their hands at any time during the consultation
3.9%(7/178)
6.4% (13/204)
0(0/38)
Cases for whom the HW’s who washed their hands used soap or alcohol
5/7 7/13
HF with hand washing facilities available inside the health facility
53.7% (29/54)
54.9% (28/51)
21.4% (3/14)
HF with soap available next to hand washing area
77.8%(42/54)
65.4% (34/52)
28.6%(4/14)
HF with toilets available to use in the health centre
98.1%(53/54)
100% (52/52)
85.7%(12/14)

Cambodia Health Facility Survey 2010
69
Table 3: Disposal of medical wastes
IMCI
(A) IMCI++
(B) No IMCI
(C)
HF disposing their medical waste:
1. Mixed with general waste and thrown away
1.9% (1/54) 1.9% (1/52) 0% (0/14)
2. Separated from general waste and thrown
37% (20/54) 36.5% (19/52) 57.1% (8/14)
3. Mixed with general waste but buried 0% (0/54) (1/52) 0% (0/14)
4. Separated from general waste but buried
30.2% (16/53) 26.9% (14/52) 50.0% (7/14)
5. Mixed with general waste but burnt 3.8% (2/53) 17.3% (9/52) 21.4% (3/14)
6. Separated from general waste but burnt
54.7% (29/53) 63.5% (33/52) 57.1% (8/14)
7. Burnt medical waste in incinerator 71.7% (38/53) 63.5% (33/52) 35.7% (5/14)
8. Other 22.6% (12/53) 25.4% (13/51) 42.9% (6/14)
Table 4: Health Center Management Committee
IMCI
(A) IMCI++
(B) No IMCI
(C)
HF has a Health Center Management Committee
100% (54/54)
88.5% (46/52)
78.6% (11/14)
Form4, S12
For HF with a HCMC, average number of meetings per year (mean and range)
5.4 (range 0-12)
6.5 (range 0-24)
5.8 (range 4-12)
Form4, S13
HF with a HCMC, that met at least once during previous 6 months
78.8% (41/52)
91.1% (41/45)
63.6% (7/11)
Form4, S14

Cambodia Health Facility Survey 2010
70
5. Availability of services
IMCI
(A) IMCI++
(B) No IMCI
(C)
Proportion of HF open:
– 7 days a week 22.2%(12/54)
30.6% (16/52)
14.3%(2/14)
– 6 days a week 5.6%(3/54)
5.8% (3/52)
0%(0/14)
Health centre open both morning and afternoon 53.7%(29/54)
82.7% (43/52)
64.3%(9/14)
Average number of days/week when child health services are provided
5.33(5-7)
5.61 (5-7)
5.14(5-7)
Average number of days/week when immunization services are provided
5.16(2-7)
5.31 (5-7)
4.78(0-7)
Health centre with off-work services (on duty) 90.7%(49/54)
98.1% (51/52)
100%(14/14)
Health centre with appropriate means of transportation that can refer on time
90.7%(49/54)
98.1% (51/52)
78.6%(11/14)
Health centre with appropriate (quality) referral hospital 98.1%(53/54)
92.3% (48/52)
85.7%(12/14)
Issues with referral reported by health staff
Indicator IMCI
(A) IMCI++
(B) No IMCI
(C) Notes
Average time (in minutes) reported by health facilities to reach the referral center
30 min (5 – 95)
30 min (1 – 120)
45 min (5 – 150)
Form4, S9
Health Facilities reporting difficulties referring severely ill children in the past
24.1% (13/54)
26.9% (14/52)
14.3% (2/14)
Form4, S10
Most frequent reasons reported by health facilities that were unable to refer severely ill children
1-Financial issue, 2-no transportation
1-Financial issue, 2-Preference for private clinic
1-Financial issue
Perception of health facility staff regarding proportion of children prescribed referral who would actually go (from 10 referred children from a HF how many are estimated to actually go)
8.18 8.31 9.86 Form4, S11

Cambodia Health Facility Survey 2010
71
Table 7: Attendance data
Indicator IMCI (A) IMCI++ (B) No IMCI (C) Variable
Average number of consultations per HF by children under five during previous month (April 2010)
151.15 162.23 98.93 Form4, R1
Average number of consultations per HF by newborns (aged 0 to 1 month) during previous month
3.19 2.85 0.77 Form4, R1a
Average number of consultations per HF by infants aged 1 to 3 months during previous month
17.24 15.12 9.0 Form4,
Average number of consultations per HF by children under one year during previous month
61.26 60.60 31.15 Form4, R1b
Average number of consultations for immunization visits
78.61 116.15 60.5 Form4, R2
Table 8: Availability of diagnostic tests and IV materials
IMCI (A) IMCI++ (B) No IMCI (C)
Dipstick for malaria (optimal and/or paracheck)
63%(34/54)
61.5% (32/52)
78.6%(11/14)
Naso-gastric tube 11.1%(6/54)
9.6% (5/52)
0
Recommended IV fluids 87%(47/54)
96.2% (50/52)
92.9%(13/14)
IV sets for IV fluid infusion 74.1%(40/54)
96.2% (50/52)
64.3%(9/14)
Table 9: Availability of injectable drugs (pre-referral treatment)
IMCI (A) IMCI++ (B) No IMCI (C)
Ampicillin (inj) F4d3j 63%(34/54)
76.9% (40/52)
42.9%(6/14)
Gentamycin (inj) F4d3k 61.1%(33/54)
75% (39/52)
50%(7/14)
Diazepam (inj) F4d3l 50%(27/54)
78.4% (40/51)
64.3%(9/14)
Table 10: Availability of drugs for deliveries
IMCI (A) IMCI++ (B) No IMCI (C) Oxytocin 92.6%
(50/54)94.2%
(49/52) 92.9%
(13/14)Magnesium Sulphate 9.3%
(5/54)17.3% (9/52)
7.1%(1/14)

Cambodia Health Facility Survey 2010
72
Table 11: Availability of drugs
IMCI (A)
IMCI++ (B)
No IMCI (C)
ORS package (*1) F4d3a 96.3(52/54)
94.2% (49/52)
100%(14/14)
Cotrimoxazole (*2 or) F4d3b 100% 98.1% (51/52)
100%(14/14)
Amoxicillin (*2 or) F4d3c 100%(54/54)
90.4% (47/52)
100%(14/14)
Ciprofloxacin (*3) F4d3d 61.1%(33/54)
67.3% (35/52)
42.9%(6/14)
Erythromycine 79.6%(43/54)
84.6% (44/52)
78.6%(11/14)
Artesunate 1.9%(1/54)
9.6% (5/52)
7.1%(1/14)
Mefloquine 7.4%(4/54)
9.6% (5/52)
0
Chloroquine 31.5%(17/54)
50% (26/52)
42.9%(6/14)
Cotrimixazole , Amoxycillin pediatric formulation 96.3%(52/54)
96.1% (49/51)
85.7%(12/14)
Antimalarial drugs (A+M3 or A+M5) 59.3%(32/54)
59.6% (31/52)
64.3%(9/14)
Antimalarial pediatric formulation A+M1 or A+M2) 48.1%(26/54)
50% (26/52)
64.3%(9/14)
Duo Cotecxin 3.7%(2/54)
5.8% (3/52)
7.1%(1/14)
Paracetamol (*6) F4d3q
96.3%(52/54)
98% (50/51)
92.9%(13/14)
Vitamin A capsule 200,000 UI (*4 or) F4d3r 96.3%(52/54)
100% 100%
Vitamin A capsule 100,000 UI (*4 or) F4d3s 96.3%(52/54)
98.1% (51/52)
100%
Iron/folate (*5) F4d3t 100% 100% 100%Mebendazole / Albendazole (*7) F4d3u 100% 100% 100%Tetracycline eye ointment 94.4%
(51/54)88.5%
(46/52) 92.9%
(13/14)Gentian violet 96.3%
(52/54)96.2%
(50/52) 78.6%
(11/14)Zinc tablets 42.6%
(23/54)63.5%
(33/52) 35.7%(5/14)
Quinolone (eardrop) 1.9%(1/54)
5.8% (3/52)
7.1%(1/14)
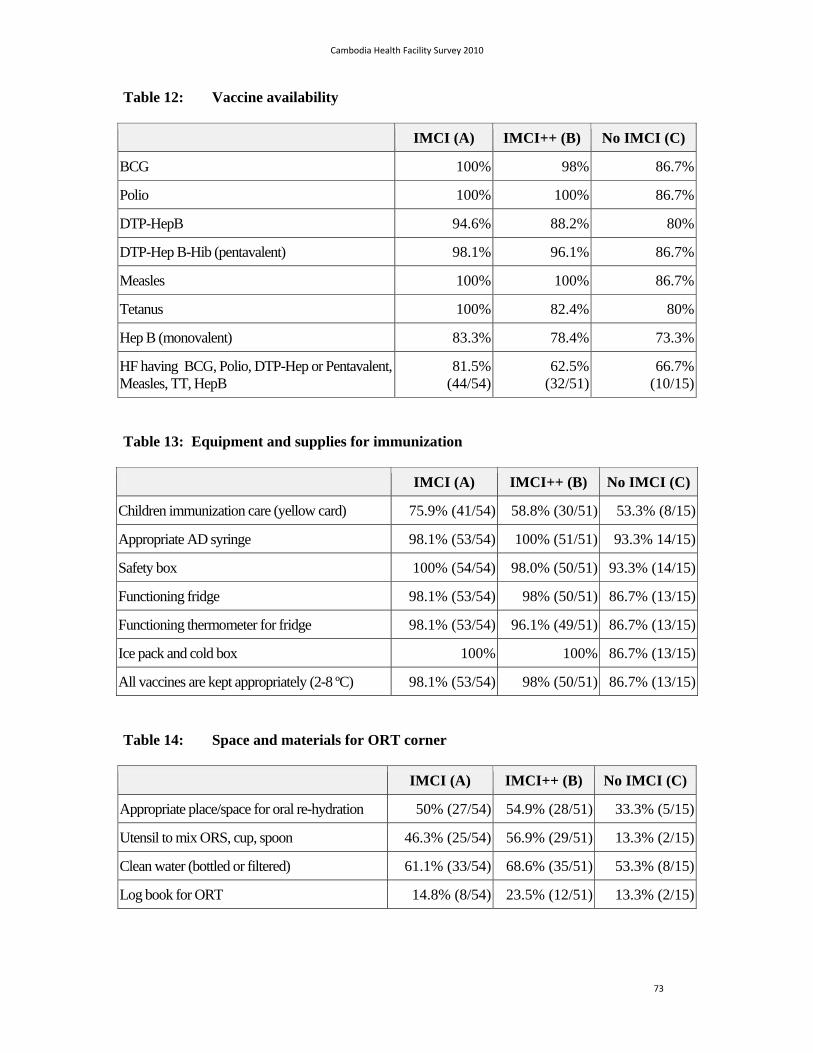
Cambodia Health Facility Survey 2010
73
Table 12: Vaccine availability
IMCI (A) IMCI++ (B) No IMCI (C)
BCG 100% 98% 86.7%
Polio 100% 100% 86.7%
DTP-HepB 94.6% 88.2% 80%
DTP-Hep B-Hib (pentavalent) 98.1% 96.1% 86.7%
Measles 100% 100% 86.7%
Tetanus 100% 82.4% 80%
Hep B (monovalent) 83.3% 78.4% 73.3%
HF having BCG, Polio, DTP-Hep or Pentavalent, Measles, TT, HepB
81.5%(44/54)
62.5% (32/51)
66.7%(10/15)
Table 13: Equipment and supplies for immunization
IMCI (A) IMCI++ (B) No IMCI (C)
Children immunization care (yellow card) 75.9% (41/54) 58.8% (30/51) 53.3% (8/15)
Appropriate AD syringe 98.1% (53/54) 100% (51/51) 93.3% 14/15)
Safety box 100% (54/54) 98.0% (50/51) 93.3% (14/15)
Functioning fridge 98.1% (53/54) 98% (50/51) 86.7% (13/15)
Functioning thermometer for fridge 98.1% (53/54) 96.1% (49/51) 86.7% (13/15)
Ice pack and cold box 100% 100% 86.7% (13/15)
All vaccines are kept appropriately (2-8 ºC) 98.1% (53/54) 98% (50/51) 86.7% (13/15)
Table 14: Space and materials for ORT corner
IMCI (A) IMCI++ (B) No IMCI (C)
Appropriate place/space for oral re-hydration 50% (27/54) 54.9% (28/51) 33.3% (5/15)
Utensil to mix ORS, cup, spoon 46.3% (25/54) 56.9% (29/51) 13.3% (2/15)
Clean water (bottled or filtered) 61.1% (33/54) 68.6% (35/51) 53.3% (8/15)
Log book for ORT 14.8% (8/54) 23.5% (12/51) 13.3% (2/15)
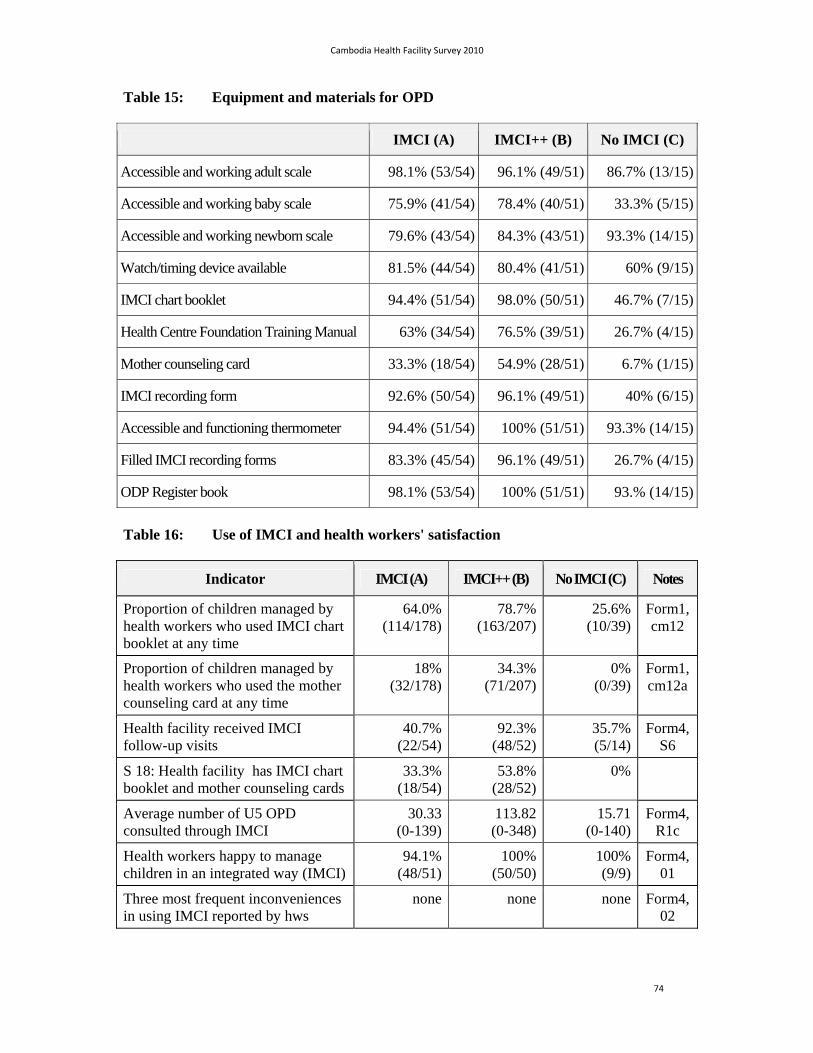
Cambodia Health Facility Survey 2010
74
Table 15: Equipment and materials for OPD
IMCI (A) IMCI++ (B) No IMCI (C)
Accessible and working adult scale 98.1% (53/54) 96.1% (49/51) 86.7% (13/15)
Accessible and working baby scale 75.9% (41/54) 78.4% (40/51) 33.3% (5/15)
Accessible and working newborn scale 79.6% (43/54) 84.3% (43/51) 93.3% (14/15)
Watch/timing device available 81.5% (44/54) 80.4% (41/51) 60% (9/15)
IMCI chart booklet 94.4% (51/54) 98.0% (50/51) 46.7% (7/15)
Health Centre Foundation Training Manual 63% (34/54) 76.5% (39/51) 26.7% (4/15)
Mother counseling card 33.3% (18/54) 54.9% (28/51) 6.7% (1/15)
IMCI recording form 92.6% (50/54) 96.1% (49/51) 40% (6/15)
Accessible and functioning thermometer 94.4% (51/54) 100% (51/51) 93.3% (14/15)
Filled IMCI recording forms 83.3% (45/54) 96.1% (49/51) 26.7% (4/15)
ODP Register book 98.1% (53/54) 100% (51/51) 93.% (14/15)
Table 16: Use of IMCI and health workers' satisfaction
Indicator IMCI (A) IMCI++ (B) No IMCI (C) Notes
Proportion of children managed by health workers who used IMCI chart booklet at any time
64.0%(114/178)
78.7%(163/207)
25.6% (10/39)
Form1, cm12
Proportion of children managed by health workers who used the mother counseling card at any time
18%(32/178)
34.3%(71/207)
0% (0/39)
Form1, cm12a
Health facility received IMCI follow-up visits
40.7%(22/54)
92.3%(48/52)
35.7% (5/14)
Form4, S6
S 18: Health facility has IMCI chart booklet and mother counseling cards
33.3%(18/54)
53.8%(28/52)
0%
Average number of U5 OPD consulted through IMCI
30.33(0-139)
113.82(0-348)
15.71 (0-140)
Form4, R1c
Health workers happy to manage children in an integrated way (IMCI)
94.1%(48/51)
100%(50/50)
100% (9/9)
Form4, 01
Three most frequent inconveniences in using IMCI reported by hws
none none none Form4, 02
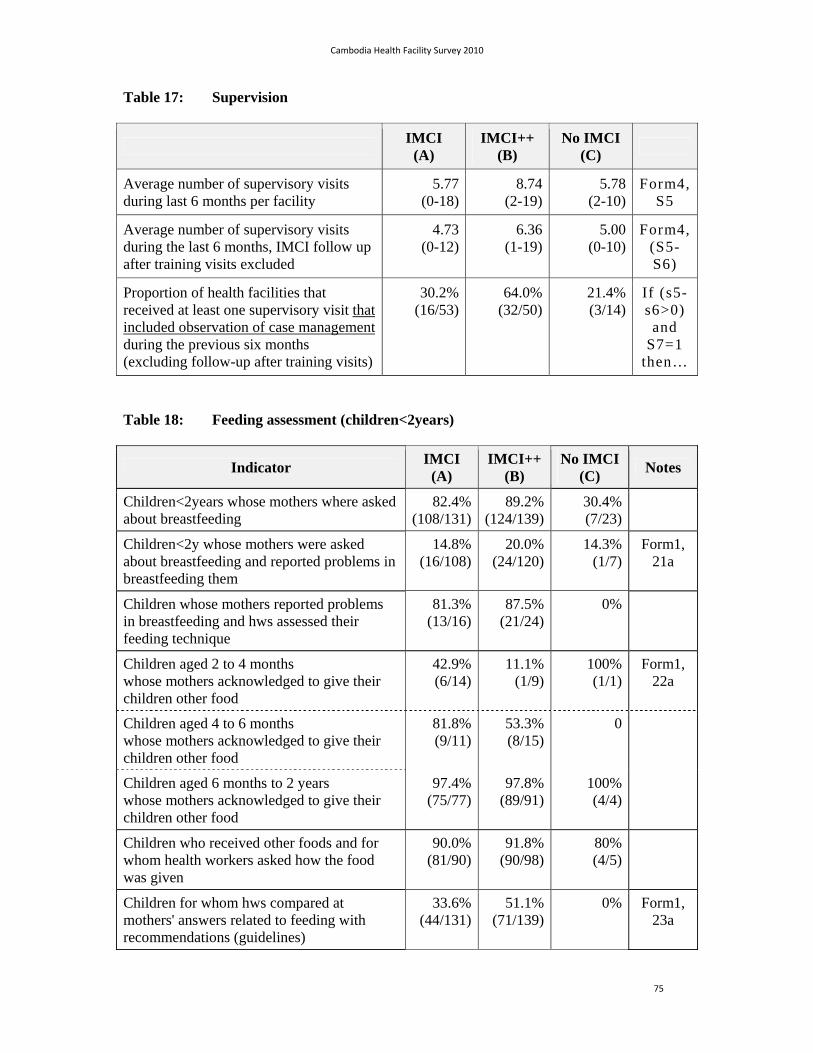
Cambodia Health Facility Survey 2010
75
Table 17: Supervision
IMCI
(A) IMCI++
(B) No IMCI
(C)
Average number of supervisory visits during last 6 months per facility
5.77(0-18)
8.74(2-19)
5.78 (2-10)
Form4, S5
Average number of supervisory visits during the last 6 months, IMCI follow up after training visits excluded
4.73(0-12)
6.36(1-19)
5.00 (0-10)
Form4, (S5-S6)
Proportion of health facilities that received at least one supervisory visit that included observation of case management during the previous six months (excluding follow-up after training visits)
30.2%(16/53)
64.0%(32/50)
21.4% (3/14)
If (s5-s6>0)
and S7=1
then…
Table 18: Feeding assessment (children<2years)
Indicator IMCI
(A) IMCI++
(B) No IMCI
(C) Notes
Children<2years whose mothers where asked about breastfeeding
82.4%(108/131)
89.2%(124/139)
30.4% (7/23)
Children<2y whose mothers were asked about breastfeeding and reported problems in breastfeeding them
14.8%(16/108)
20.0%(24/120)
14.3% (1/7)
Form1, 21a
Children whose mothers reported problems in breastfeeding and hws assessed their feeding technique
81.3%(13/16)
87.5%(21/24)
0%
Children aged 2 to 4 months whose mothers acknowledged to give their children other food
42.9%(6/14)
11.1%(1/9)
100% (1/1)
Form1, 22a
Children aged 4 to 6 months whose mothers acknowledged to give their children other food
81.8%(9/11)
53.3%(8/15)
0
Children aged 6 months to 2 years whose mothers acknowledged to give their children other food
97.4%(75/77)
97.8%(89/91)
100% (4/4)
Children who received other foods and for whom health workers asked how the food was given
90.0%(81/90)
91.8%(90/98)
80% (4/5)
Children for whom hws compared at mothers' answers related to feeding with recommendations (guidelines)
33.6%(44/131)
51.1%(71/139)
0% Form1, 23a
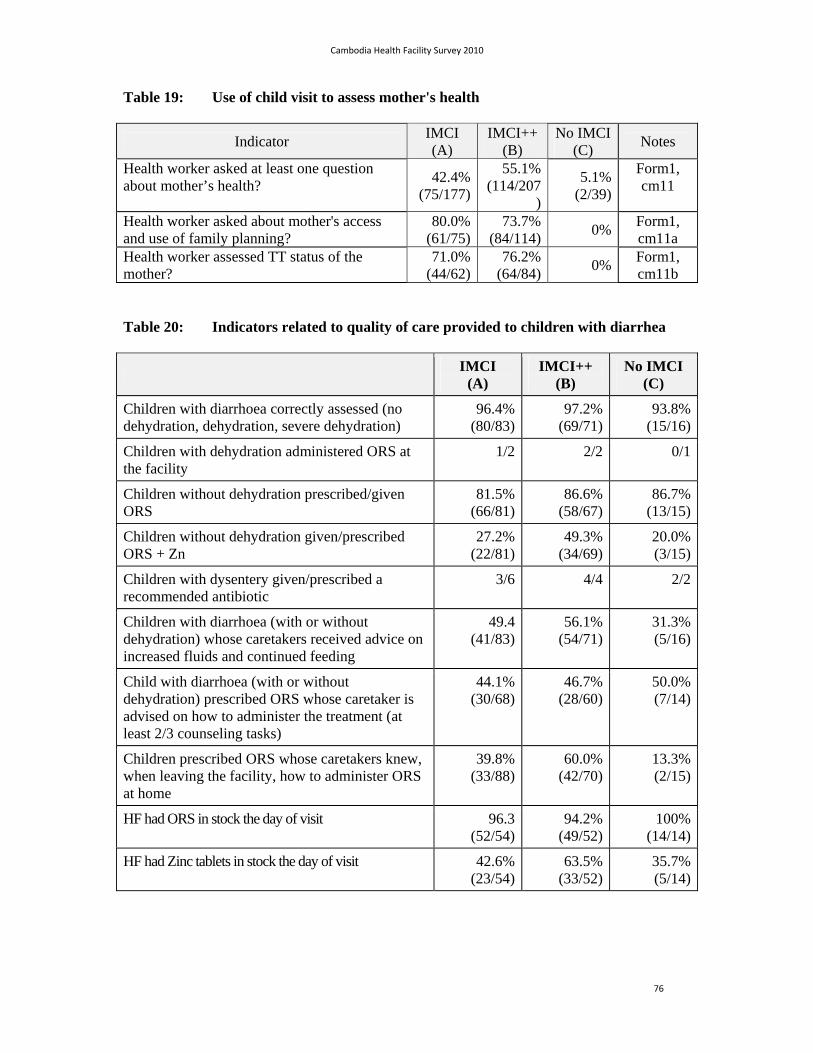
Cambodia Health Facility Survey 2010
76
Table 19: Use of child visit to assess mother's health
Indicator IMCI (A)
IMCI++ (B)
No IMCI (C)
Notes
Health worker asked at least one question about mother’s health?
42.4%(75/177)
55.1%(114/207
)
5.1% (2/39)
Form1, cm11
Health worker asked about mother's access and use of family planning?
80.0%(61/75)
73.7%(84/114)
0% Form1, cm11a
Health worker assessed TT status of the mother?
71.0%(44/62)
76.2%(64/84)
0% Form1, cm11b
Table 20: Indicators related to quality of care provided to children with diarrhea
IMCI
(A) IMCI++
(B) No IMCI
(C)
Children with diarrhoea correctly assessed (no dehydration, dehydration, severe dehydration)
96.4%(80/83)
97.2% (69/71)
93.8%(15/16)
Children with dehydration administered ORS at the facility
1/2 2/2 0/1
Children without dehydration prescribed/given ORS
81.5%(66/81)
86.6% (58/67)
86.7%(13/15)
Children without dehydration given/prescribed ORS + Zn
27.2%(22/81)
49.3% (34/69)
20.0%(3/15)
Children with dysentery given/prescribed a recommended antibiotic
3/6 4/4 2/2
Children with diarrhoea (with or without dehydration) whose caretakers received advice on increased fluids and continued feeding
49.4(41/83)
56.1% (54/71)
31.3%(5/16)
Child with diarrhoea (with or without dehydration) prescribed ORS whose caretaker is advised on how to administer the treatment (at least 2/3 counseling tasks)
44.1%(30/68)
46.7% (28/60)
50.0%(7/14)
Children prescribed ORS whose caretakers knew, when leaving the facility, how to administer ORS at home
39.8%(33/88)
60.0% (42/70)
13.3%(2/15)
HF had ORS in stock the day of visit 96.3(52/54)
94.2% (49/52)
100%(14/14)
HF had Zinc tablets in stock the day of visit 42.6%(23/54)
63.5% (33/52)
35.7%(5/14)

Cambodia Health Facility Survey 2010
77
Table 21: Indicators related to quality of care provided to children with pneumonia
IMCI
(A) IMCI++
(B) No IMCI
(C)
Children with pneumonia correctly identified by hws
80.0%(20/25)
88.5% (23/26)
80.0%(4/5)
S 6: Child with pneumonia correctly treated
60.0%(15/25)
76.9% (20/26)
20.0%(1/5)
Child with pneumonia and prescribed antibiotics whose whose caretakers are advised on how to administer the treatment at home (at least 2/3 counseling tasks)
62.5%(15/24)
56% (14/25)
40.0%(2/5)
Children with pneumonia and prescribed antibiotics whose caretakers knew, when leaving the facility, how to administer the antibiotics at home
72%(18/25)
84.6% (22/26)
40.0%(2/5)
Children with pneumonia whose caretakers are advised on when to return immediately (at least 3 out of the 7 generic danger signs)
20.0%(5/25)
34.6% (9/26)
0%(0/5)
HF had Cotrimoxazol in stock the day of visit 100%
98.1% (51/52)
100%(14/14)
HF had Amoxicillin in stock the day of visit 100%(54/54)
90.4% (47/52)
100%(14/14)
Table 22: Health facilities with at least 2 health workers trained in IMCI
IMCI (A)
IMCI++ (B)
No IMCI (C)
Health facilities with at least two health workers in charge of managing children trained in IMCI
81.48% (44/54)
94.2% (49/52)
35.7% (5/14)
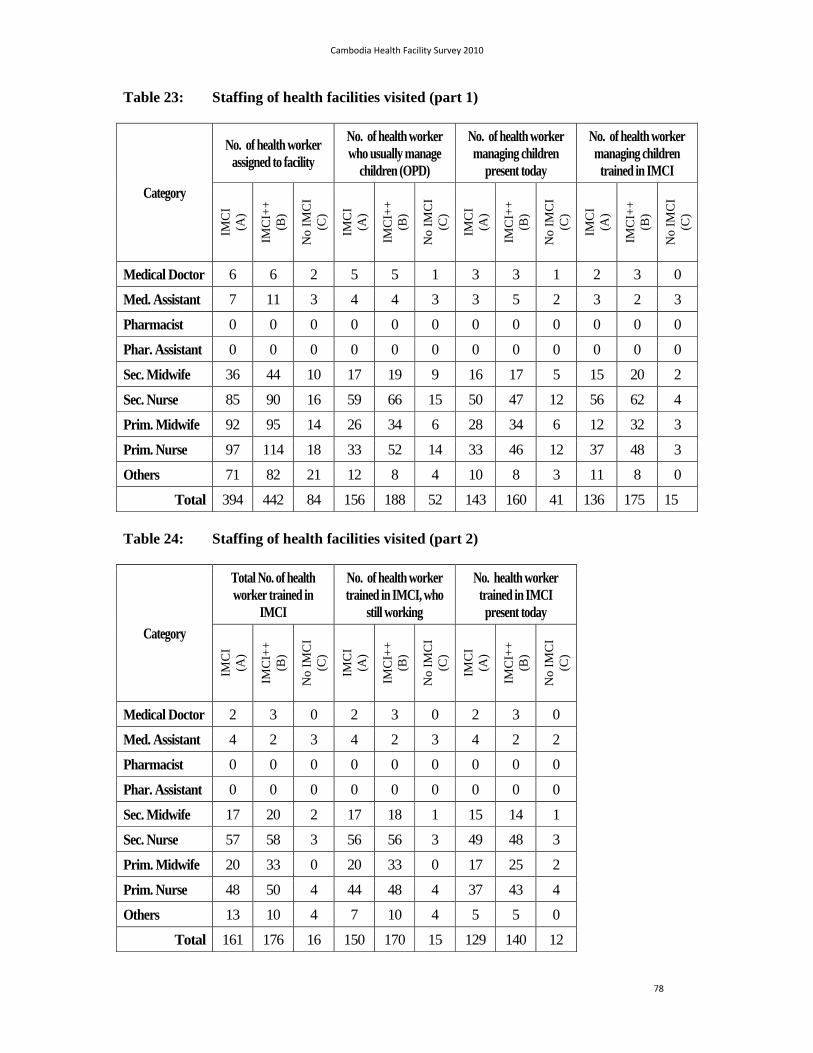
Cambodia Health Facility Survey 2010
78
Table 23: Staffing of health facilities visited (part 1)
Category
No. of health worker assigned to facility
No. of health worker who usually manage
children (OPD)
No. of health worker managing children
present today
No. of health worker managing children
trained in IMCI
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
Medical Doctor 6 6 2 5 5 1 3 3 1 2 3 0
Med. Assistant 7 11 3 4 4 3 3 5 2 3 2 3
Pharmacist 0 0 0 0 0 0 0 0 0 0 0 0
Phar. Assistant 0 0 0 0 0 0 0 0 0 0 0 0
Sec. Midwife 36 44 10 17 19 9 16 17 5 15 20 2
Sec. Nurse 85 90 16 59 66 15 50 47 12 56 62 4
Prim. Midwife 92 95 14 26 34 6 28 34 6 12 32 3
Prim. Nurse 97 114 18 33 52 14 33 46 12 37 48 3
Others 71 82 21 12 8 4 10 8 3 11 8 0
Total 394 442 84 156 188 52 143 160 41 136 175 15
Table 24: Staffing of health facilities visited (part 2)
Category
Total No. of health worker trained in
IMCI
No. of health worker trained in IMCI, who
still working
No. health worker trained in IMCI present today
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
Medical Doctor 2 3 0 2 3 0 2 3 0
Med. Assistant 4 2 3 4 2 3 4 2 2
Pharmacist 0 0 0 0 0 0 0 0 0
Phar. Assistant 0 0 0 0 0 0 0 0 0
Sec. Midwife 17 20 2 17 18 1 15 14 1
Sec. Nurse 57 58 3 56 56 3 49 48 3
Prim. Midwife 20 33 0 20 33 0 17 25 2
Prim. Nurse 48 50 4 44 48 4 37 43 4
Others 13 10 4 7 10 4 5 5 0
Total 161 176 16 150 170 15 129 140 12
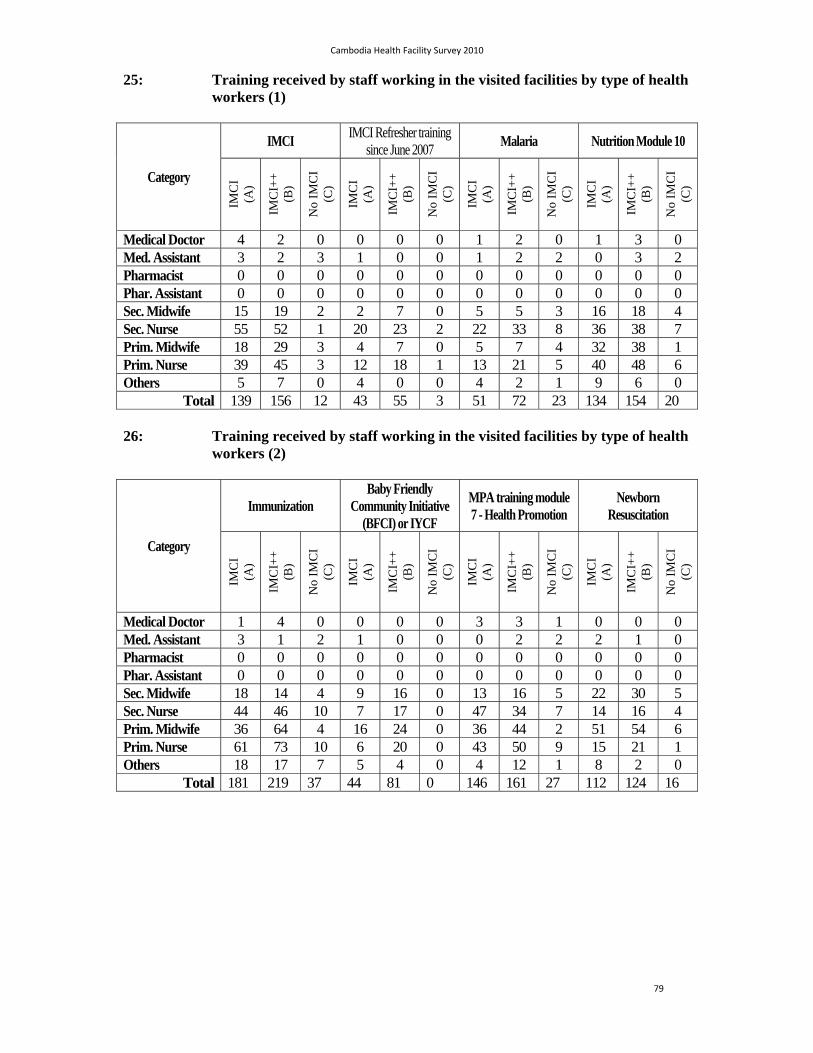
Cambodia Health Facility Survey 2010
79
25: Training received by staff working in the visited facilities by type of health workers (1)
Category
IMCI IMCI Refresher training
since June 2007 Malaria Nutrition Module 10
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
Medical Doctor 4 2 0 0 0 0 1 2 0 1 3 0 Med. Assistant 3 2 3 1 0 0 1 2 2 0 3 2 Pharmacist 0 0 0 0 0 0 0 0 0 0 0 0 Phar. Assistant 0 0 0 0 0 0 0 0 0 0 0 0 Sec. Midwife 15 19 2 2 7 0 5 5 3 16 18 4 Sec. Nurse 55 52 1 20 23 2 22 33 8 36 38 7 Prim. Midwife 18 29 3 4 7 0 5 7 4 32 38 1 Prim. Nurse 39 45 3 12 18 1 13 21 5 40 48 6 Others 5 7 0 4 0 0 4 2 1 9 6 0
Total 139 156 12 43 55 3 51 72 23 134 154 20
26: Training received by staff working in the visited facilities by type of health workers (2)
Category
Immunization Baby Friendly
Community Initiative (BFCI) or IYCF
MPA training module 7 - Health Promotion
Newborn Resuscitation
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
IMC
I (A
)
IMC
I++
(B
)
No
IMC
I (C
)
Medical Doctor 1 4 0 0 0 0 3 3 1 0 0 0 Med. Assistant 3 1 2 1 0 0 0 2 2 2 1 0 Pharmacist 0 0 0 0 0 0 0 0 0 0 0 0 Phar. Assistant 0 0 0 0 0 0 0 0 0 0 0 0 Sec. Midwife 18 14 4 9 16 0 13 16 5 22 30 5 Sec. Nurse 44 46 10 7 17 0 47 34 7 14 16 4 Prim. Midwife 36 64 4 16 24 0 36 44 2 51 54 6 Prim. Nurse 61 73 10 6 20 0 43 50 9 15 21 1 Others 18 17 7 5 4 0 4 12 1 8 2 0
Total 181 219 37 44 81 0 146 161 27 112 124 16
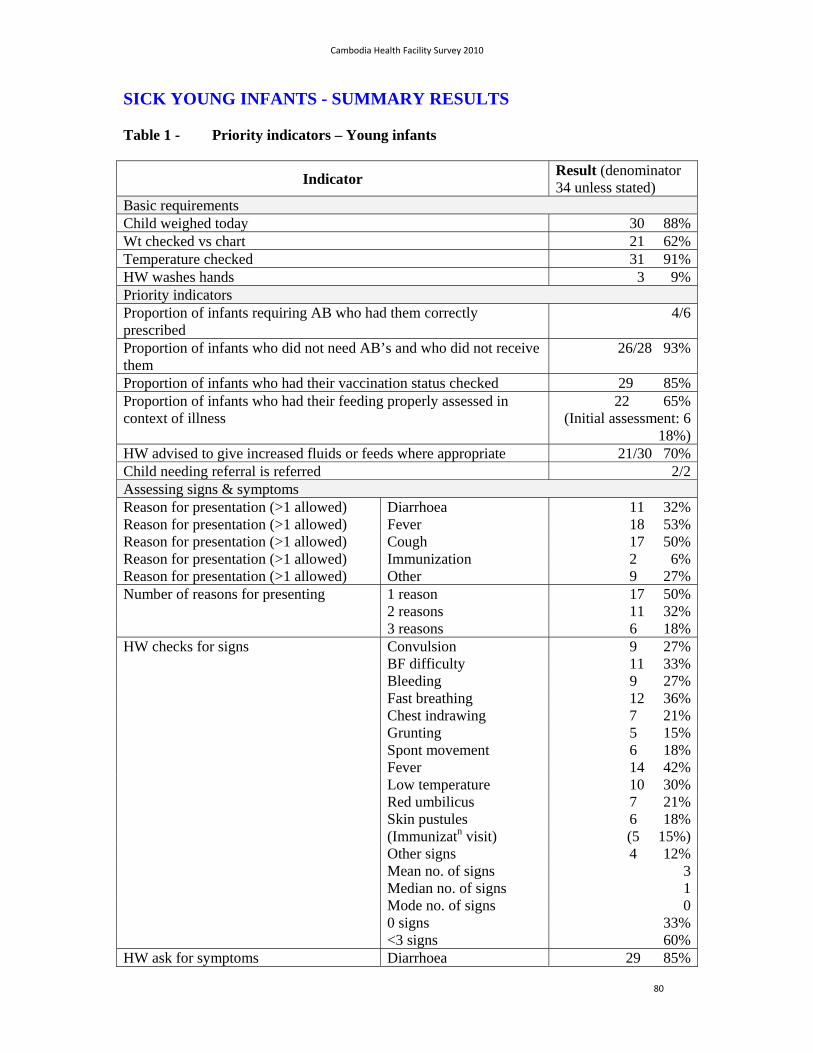
Cambodia Health Facility Survey 2010
80
SICK YOUNG INFANTS - SUMMARY RESULTS
Table 1 - Priority indicators – Young infants
Indicator Result (denominator 34 unless stated)
Basic requirements Child weighed today 30 88%Wt checked vs chart 21 62%Temperature checked 31 91%HW washes hands 3 9% Priority indicators Proportion of infants requiring AB who had them correctly prescribed
4/6
Proportion of infants who did not need AB’s and who did not receive them
26/28 93%
Proportion of infants who had their vaccination status checked 29 85%Proportion of infants who had their feeding properly assessed in context of illness
22 65%(Initial assessment: 6
18%)HW advised to give increased fluids or feeds where appropriate 21/30 70%Child needing referral is referred 2/2Assessing signs & symptoms Reason for presentation (>1 allowed) Diarrhoea 11 32%Reason for presentation (>1 allowed) Fever 18 53%Reason for presentation (>1 allowed) Cough 17 50%Reason for presentation (>1 allowed) Immunization 2 6%Reason for presentation (>1 allowed) Other 9 27%Number of reasons for presenting 1 reason 17 50% 2 reasons 11 32% 3 reasons 6 18%HW checks for signs Convulsion 9 27% BF difficulty 11 33% Bleeding 9 27% Fast breathing 12 36% Chest indrawing 7 21% Grunting 5 15% Spont movement 6 18% Fever 14 42% Low temperature 10 30% Red umbilicus 7 21% Skin pustules 6 18% (Immunizatn visit) (5 15%) Other signs 4 12% Mean no. of signs 3 Median no. of signs 1 Mode no. of signs 0 0 signs 33% <3 signs 60%HW ask for symptoms Diarrhoea 29 85%
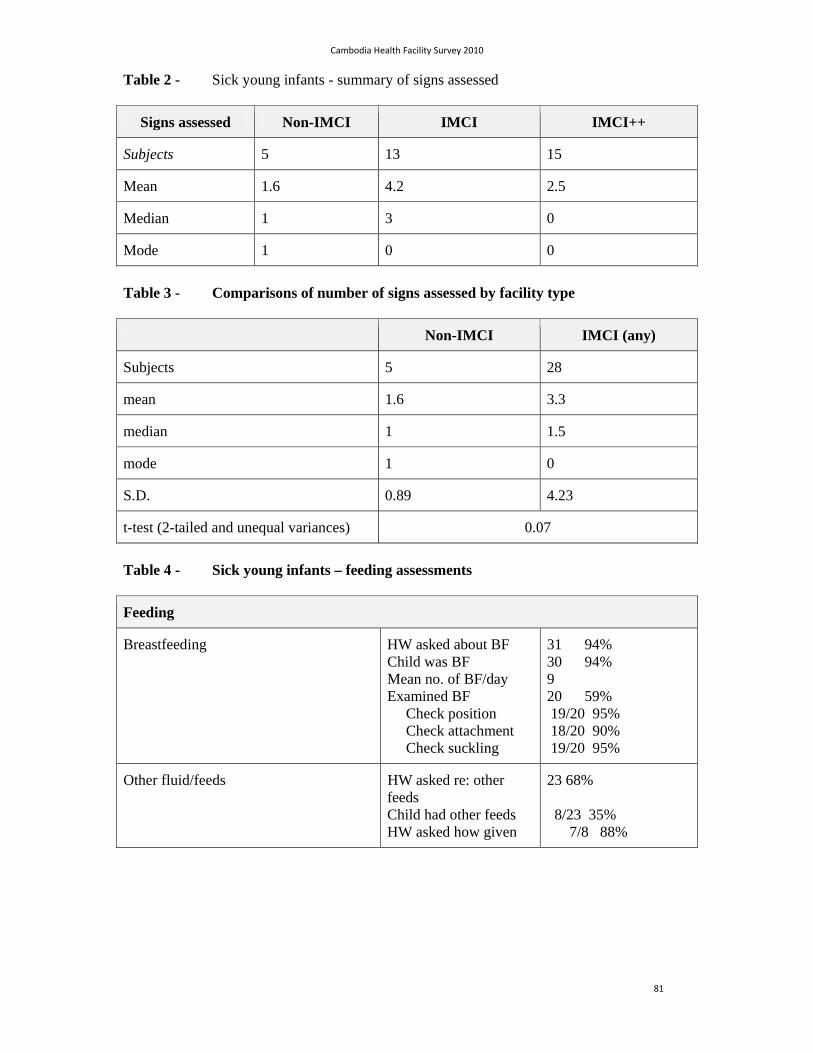
Cambodia Health Facility Survey 2010
81
Table 2 - Sick young infants - summary of signs assessed
Signs assessed Non-IMCI IMCI IMCI++
Subjects 5 13 15
Mean 1.6 4.2 2.5
Median 1 3 0
Mode 1 0 0
Table 3 - Comparisons of number of signs assessed by facility type
Non-IMCI IMCI (any)
Subjects 5 28
mean 1.6 3.3
median 1 1.5
mode 1 0
S.D. 0.89 4.23
t-test (2-tailed and unequal variances) 0.07
Table 4 - Sick young infants – feeding assessments
Feeding
Breastfeeding HW asked about BF Child was BF Mean no. of BF/day Examined BF Check position Check attachment Check suckling
31 94% 30 94% 9 20 59% 19/20 95% 18/20 90% 19/20 95%
Other fluid/feeds HW asked re: other feeds Child had other feeds HW asked how given
23 68% 8/23 35% 7/8 88%
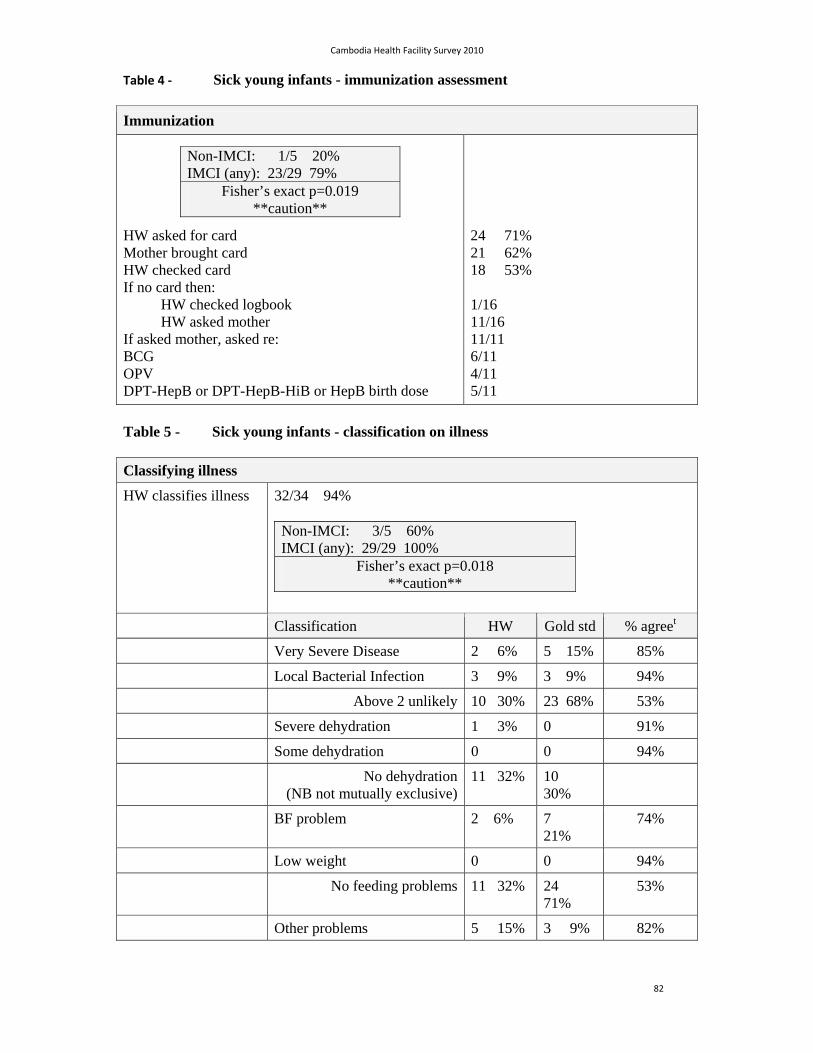
Cambodia Health Facility Survey 2010
82
Table 4 ‐ Sick young infants - immunization assessment
Immunization
HW asked for card Mother brought card HW checked card If no card then: HW checked logbook HW asked mother If asked mother, asked re: BCG OPV DPT-HepB or DPT-HepB-HiB or HepB birth dose
Non-IMCI: 1/5 20% IMCI (any): 23/29 79%
Fisher’s exact p=0.019 **caution**
24 71% 21 62% 18 53% 1/16 11/16 11/11 6/11 4/11 5/11
Table 5 - Sick young infants - classification on illness
Classifying illness
HW classifies illness 32/34 94% Non-IMCI: 3/5 60% IMCI (any): 29/29 100%
Fisher’s exact p=0.018 **caution**
Classification HW Gold std % agreet
Very Severe Disease 2 6% 5 15% 85%
Local Bacterial Infection 3 9% 3 9% 94%
Above 2 unlikely 10 30% 23 68% 53%
Severe dehydration 1 3% 0 91%
Some dehydration 0 0 94%
No dehydration(NB not mutually exclusive)
11 32% 10 30%
BF problem 2 6% 7 21%
74%
Low weight 0 0 94%
No feeding problems 11 32% 24 71%
53%
Other problems 5 15% 3 9% 82%

Cambodia Health Facility Survey 2010
83
Table 6 - Sick young infants – treatment of illness
Treatment
IM injection ORS prescribed Of these,
ORS given at HC zinc also given
PO/PR Rx prescribed Of these:
Antimotility agentRecommended AB
AB correctly prescribed in Paracetamol
ZincOther
Immediate referral Of these:
urgent Rx givenAB given
other drug givenHW advise warmth
0 9 27% ---9/11 0/9 4/9 44% 18 53% 0/18 6/18 33% 4/6 15/18 83% 4/18 22% 4/18 22% 2 6% 2/2 2/2 (oral amoxycillin in both) 0/2 ½

Cambodia Health Facility Survey 2010
84
Table 7 - Sick young infants – counseling
Communication
HW explains ABORSZinc
7 21% 8 24% 3 9%
HW demonstrates ABORSZinc
6 18% 4 12% 2 6%
HW checks mother’s understanding
ABORSZinc
5 15% 3 9% 2 6%
HW asks to observe mother give 1st dose AB
0/4 infants prescribed AB, 2/2 infants pre-referral urgent Rx
HW advises mother : to increase BF on frequency of feeds when to return urgently of these, HW specifies:
unable to feedcannot wake child
becomes sickerfever
low tempfast breathing
difficulty breathingbleeding
other
22 65% 22 65% 21/22 advise 8feeds/day 24 71% 12/24 % with denom 34: 35% 6/24 18% 15/24 44% 12/24 35% 2/24 6% 3/24 9% 3/24 9% 7/24 21% 2/24 8%
HW asks about mother Asks re mother’s health Asks re family planning
15 44% 12 35%
HW uses IMCI tools IMCI chart booklet IMCI mother’s card
25 74% Non-IMCI: 2/5 40% IMCI (any): 23/29 79%
Fisher’s exact p=0.10 NS 9 27% Non-IMCI: 0/5 0% IMCI (any): 9/29 31%
Fisher’s exact p=0.30 NS
Cambodia Health Facility Survey 2010
85
ANNEX 2: LIST OF SURVEYORS. CAMBODIA HFS, MAY 2010
Surveyors
1. Dr Teng Srey
2. Dr Nao Kornsophal
3. Dr Yi Sophoanrith
4. Dr Thai Savuth
5. Dr Mom Phalkun
6. Dr Bun Chanthan
7. Dr Chhorn Veasna
8. Dr Im Vansary
9. Dr Chou Sotharith
10. Dr Kry Soknov
11. Mr Chan Sokhomkanha
12. Ms Pech Seima
13. Dr Lek Sambath
14. Dr Chhim Soputhea
15. Ms Heng Ryvann
16. Mr Yos Pov
17. Dr Tat Veyvath
18. Mr Bin Samreth
19. Dr Ou Chandaramony
20. Dr Hok Kry
21. Dr Sok Samnam
22. Dr Ny Sam Ouen
23. Mr Pan Samkol
24. Ms Saing Dany
25. Ms Penh Sokunthy
26. Dr Yim Navy
27. Dr Bun Channa
28. Dr Thong Ramy
29. Dr Mou Phkakol
30. Dr Thong Puthy
31. Dr Iv Ngorn
32. Dr Som Sophal
33. Ms Saing Savath
34. Ms Chea Sophoan
35. Mr Nou Sorn
Facilitators
1. Dr Hong Rathmony
2. Dr Bun Sreng
3. Dr Ly Khunbunnarann
4. Dr Nam Sieng
5. Dr Krang Sidonn
WHO representatives
1. Dr Susan Jack
2. Dr Thierry Lambrechts
UNICEF representatives
1. Dr Viorica Berdaga
2. Dr Rasoka Thor
3. Dr Asheena Khalakdina
Resource person
1. Dr Naor Bar-Zeev
Top Related