







Languages
Pages
Legal



‘secondary’ headaches:
with a defined pathophysiological basis
Primary headache syndromes:
of uncertain pathogenesis

Increased intracranial pressure
Idiopathic intracranial hypertension
Meningeal irritation
Giant cell arteritis (cranial arteritis, temporal arteritis)
stroke, haemorrhage, intracranial venous sinus thrombosis or arterial dissection ,, Metabolic disturbances, e.g. hypoxia, hypercapnia and hypoglycaemia, vasoactive drugs, alcohol, monosodium glutamate, nitrites and nitrates


Due to raised ICP either tumor “ usually has a short history days to weeks the pain start suddenly and persist, daily, nausea and vomiting, “Effortless vomiting” or SOL.
Other focal neurological signs are more definitive of raised ICP than headache
Wake the patient from sleep or at morning with headache
Exacerbated by coughing, sneezing, bending and lying down.

Headaches of low ICP characterized by
relieving on lying down.
Usually follow LP
“Spontaneous low pressure headache”

Young and obese women
Raised ICP with no mass, pathophysiology is incompletely known but may due to “impaired CSF absorbtion”
Patients present with morning headache, vomiting and sometimes visual disturbance –typically diplopia and visual obscurations, + tinnitus
O/E Bilateral papilloedema
6th nerve palsy. No othe FNS.
Ventricles are small
High ICP with normal CSF content

Resolve by weight reduction or LP.
TRT.
- Acetazolamaide CA inhibitor
- Chlorothalidone
- Corticosteroid
- Surgical:*Lumboperitoneal shunt*Optic nerve fenestration

intracranial venous sinus thrombosis
hypervitaminosis A,
disturbances of calcium metabolism,
systemic lupus erythematosus,
drugs, including tetracyclines and
corticosteroids

Meningism or irritation of the meninges due to inflammation or blood accumulation
characteristically produces severe global or occipitalheadache with vomiting, exacerbation of symptoms by bright lights (photophobia) and neck stiffness (nuchal rigidity).
In SA haemorrhage, the pain is very sudden (within seconds) and severe, and the patient may lose consciousness
In bacterial meningitis, the headache is also acute in onset, but usually worsening over minutes or hours.
Kernig’s signch.

Over 50
Granulomatous inflammatory changes (with giant cells) are present in branches of the external carotid artery.
narrowing of the lumen, then thrombotic occlusion
Viral infection ,, autoimmunity ??
Scalp tenderness on coping hair.
intermittent claudication of the jaw, difficulty of chewing
The temporal arteries may become swollen and non-pulsatile
Amaurosis fugax
low-grade fever, night sweats, shoulder
and/or pelvic girdle pains, malaise,
anorexia and weight loss.
Important investigations:
-ESR > 100, CRP high
-CBC normocytic normochromic anemia
- LFT abnormal
-temporal artery biopsy. skip lesions

IV hydrocortisone. 40–60 mg daily of
prednisolone become better in 24-48 hrs
treatment may be needed for 18 months- 2
yrs
polymyalgia rheumatica
7.5–15 mg daily of prednisolone


Migraine is a periodic disorder
characterized by unilateral (or
sometimes bilateral) headache, which
may be associated with vomiting and
visual disturbance.

-common, 10% of the general population
experience at least one attach
-any age ,typically teens and twenties
-Female >male
-family history in the majority
-travel sickness and cyclical vomiting in
childhood
-relate to hypertension and head injury

-obscure
-Neurologic symptoms ,aura
(intercerebral vasoconstriction
-Headache phase ,subsequent
vasodilation of extracerebral vessel in
scalp and dura
-Serotoninergic pathway
-Genetic >> calcium channels


● stress, particularly after the stress is over, e.g. at weekends and holidays;
● physical exercise;
● diet – alcohol; occasionally specific dietary triggers can be identified, e.g. cheese, chocolate, red wine;
● hormones – the onset of migraine may follow
the menarche, and symptoms may also increase
in severity around the menopause. Attacks may be
related to menstruation.

-Migraine with aura(classical migraine)
-Migraine without aura(common migraine)
-Basilar migraine (Bickerstaff variant)
-Hemiplegic and ophthalmoplegic
migraine

-experience vague prodromal symptoms for hours preceding an attack, including drowsiness, mood changes, hunger or anorexia
-classical attack begins with the aura- Visual symptoms
-Expanding scotoma ,teichopsia,fortificationspectra
-homonymous hemianopia,or complete blindness- Sensory symptoms- Dysphasia and limb weakness
The aura generally resolves after 15–20 minutes (it may last as long as an hour ).


The headache of migraine is typically
unilateral and periorbital,. Pain is throbbing
in quality and may be exacerbated by
coughing, straining or bending (jolt
phenomenon). It lasts several hours
(generally between 4 and 72 hours).
Patients prefer to lie in a darkened room
and may gain relief from sleep. Associated
symptoms include photophobia, nausea,
vomiting, pallor and diuresis.

Migraine without aura (common migraine)
In this case, the aura is absent but patients
may experience vague prodromal
symptoms. Headache may be present
on waking but is otherwise similar to that
of classical migraine.

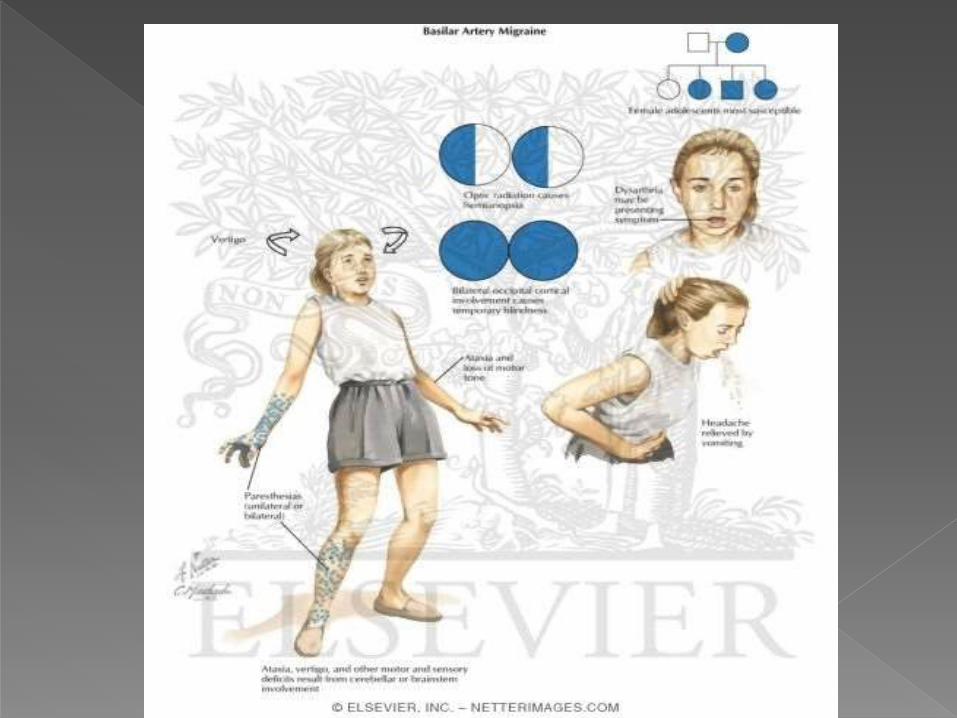
Basilar migraine (Bickerstaff variant)
This syndrome, which particularly affects
teenage female patients, is
characterized by prominent features
suggestive of vertebrobasilar ischaemia
during the aura, including vertigo,
diplopia, dysarthria, ataxia and syncope

Hemiplegic and ophthalmoplegic
migraine
These rare syndromes, in which migrainous
headaches are accompanied by
hemiplegia or ophthalmoplegia, with
focal neurological signs persisting for
days or weeks, should be diagnosed only
after structural causes, e.g. aneurysm,
have been excluded.

- History (periodicity)
- Status migrainosus
- neurological examination is normal
(except during an attack of hemiplegic
or ophthalmoplegic migraine, or unless
migrainous cerebral infarction has
occurred)
- a cranial bruit >vascular malformation

the differential diagnosis of transient focal
neurological symptoms is:
● migraine,
● transient cerebral ischaemia,
● epilepsy.

Acute attach -dark room and sleep-analgesic and antiemetic-ergotamine(vasoconstrictor) OR triptans( sumatriptan,5-HT1 receptor agonist)
Prophylaxis-avoid dietary triggers-oestrogen containing preparation;OC,hormone replacement therapy-drugs (frequent attachs) propranolol and other beta blockers,pizotifen,sodiumvalproate,verapamil,topiramate,methysergide

Despite also being characterized by
unilateral headache, this syndrome is
distinct from migraine, though the two
conditions may coexist. Histaminergic
and other humoral mechanisms are
thought to underlie the autonomic
accompaniments of the headache.

-Male>female
-age onset 20-60
- Severe attacks of pain around one eye (always the same side) characteristically last 20–120 minutes and may recur several times a day, often waking the patient more than once at night. Alcohol may precipitate an attack. This pattern continues for days, weeks or months, and the patient may then be symptom-free for many weeks, months or even years, hence the disorder’s name.
Unlike migraine, patients with cluster headache are often restless during an attack and may appear red rather than pale. More pronounced autonomic accompaniments of the pain include conjunctivalinjection, lacrimation and nasal discharge or congestion


-high flow 100% O2
-ergotamine ( bedtime ,best with caffine)
-Sumatriptan
-corticosteroid
*long term treatment
(methysergide,verapamil,pizotifen)
*chronic cluster headache (Lithium)
*trigeminal autonomic
syndromes>>indometacin

The most common headache of unknown
cause though abnormal contraction of
muscles of the head and neck has been
invoked as one putative mechanism.
Muscle contraction may be triggered by
-psychogenic factors, i.e. anxiety or
depression, -local disease of the head
and neck, e.g. cervical spondylosis or
dental malocclusion.

- headache vary from dull pain at various
sites, to a global pressure sensation, to
the feeling of a tight band around the
head
- are no associated symptoms
- neurological examination is normal
* Migraine and tension-type headache
frequently coexist.

Treatment :
- no sinister underlying cause
- 3–6-month course of a tricyclic or
related compound, e.g. amitriptyline or
dosulepin, may be helpful if tension-type
headache is frequent or persistent
-physiotherapist ( relaxation exercise)
-psychotherapy( stress management)


>15 days/month
causes:
-secondary headache syndrome
-chronic tension type headache
-transformed migraine
-medication overuse

Trigeminal neuralgia
Post-herpetic neuralgia
Atypical facial pain

->50 years
-compression of the trigeminal sensory root
-idiopathic and symptomatic(tumor of the
cerebellopontine angle ,younger MS)
-unilateral facial pain within the distribution
of one or more divisions of the trigeminal
nerve(mandibular and maxillary are
most common )

-The pain is lancinating in quality-brief,severe,sharp,stabbing,electric shock-like jolts of pain.
-trigger areas (fear of provoking an attach by washing face or shaving)
-speaking, cold breeze , chewing produce pain
-Glossopharyngeal neuralgia>pain in throat or deep inside the ear
-normal trigeminal nerve examination ,abnormal neurologic signs indicate tumor (MRI)
-Tic douloureux:anxiety about trigger areas may lead to involuntary facial spasm
-analgesic unuseful,Carbamazepine ,other drugs,surgically.

Patients who have suffered shingles in one of the
branches of the trigeminal nerve (often the first –zoster ophthalmicus) may experience persistent facial pain after the rash has healed. The pain may be very severe and intractable, lasting 2–3years after the eruption, but sometimes responds
to tricyclic antidepressants, carbamazepine or topical application of capsaicin
Atypical facial neuralgiaSome patients present with constant facial pain in
a non-anatomical distribution, and for which no
local cause is found. Treatment is unsatisfactory
but coexistent anxiety and/or depression may indicatepotential benefit from tricyclic and related
drugs, e.g. dosulepin.

-local causes of pain :eyes,ears,nose,paranasal sinuses,throator teeth
- cough,exertion,and sexual intercourse headache (benign ) *exclude cerebellar ectopia
- Coital headache (benign)*exclude subarachnoid hemorrhage
- Ice-pick headache (benign) :sharp jabs felt anywhere in head
Top Related