







Languages
Pages
Legal

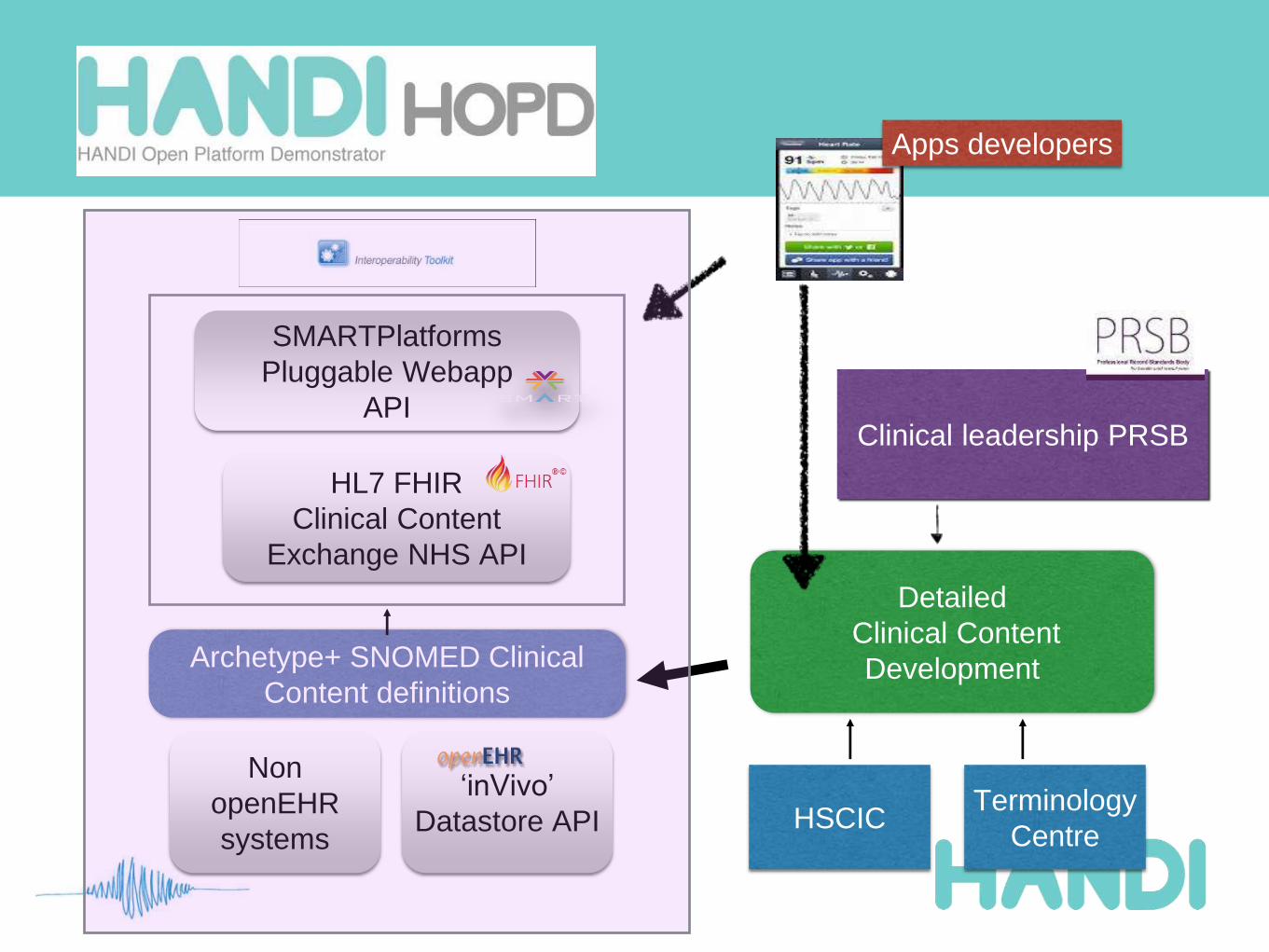
HANDI-HOPD:
What’s in the box?
Software apps to support health and care - Supporting the app paradigm –
Creating a community of interest - That's HANDI
www.handi-hopd.org
Dr Ian McNicoll
HANDIHealthopenEHR Foundation
freshEHR Clinical Informatics
HANDI-HOPD Planning meeting London Sept 2014
INTRODUCTION
2
Ian McNicoll
Clinician
Former Scottish GP
Health informaticsDirector openEHR Foundation
freshEHR Clinical Informatics
Ocean Informatics UK
HANDIHealth
NHS Scotland SCIMP
Commercial software developer‘GP Accounts’
3
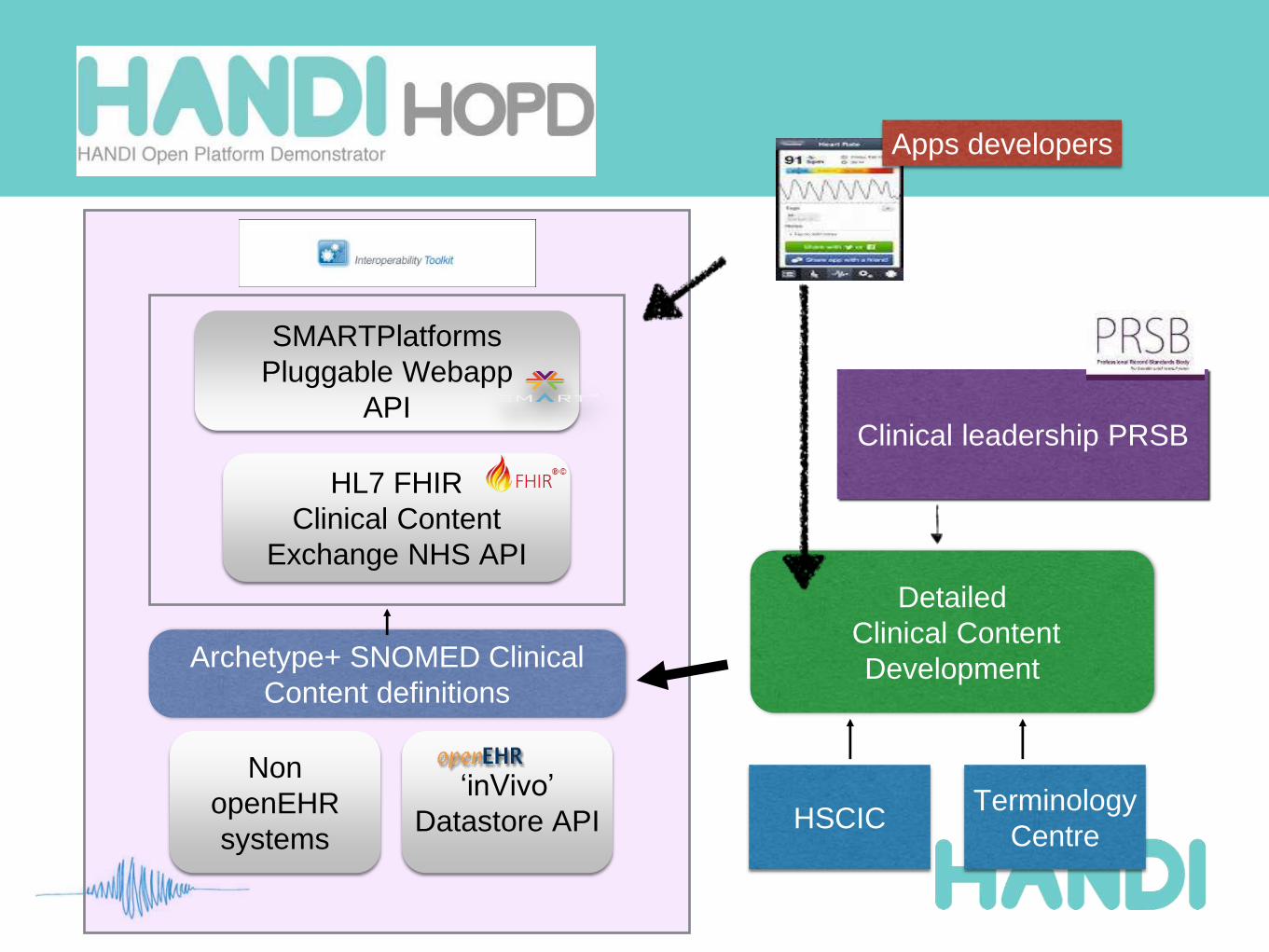
SMARTPlatforms
Pluggable Webapp
API
HL7 FHIR
Clinical Content
Exchange NHS API
‘inVivo’
Datastore API
Detailed
Clinical Content
Development
Clinical leadership PRSB
Terminology
CentreHSCIC
Non
openEHR
systems
Archetype+ SNOMED Clinical
Content definitions
Apps developers
What is an API?
• ‘Application Programming interface’
• allows one application to ‘talk’
directly to another.
• The app world runs on APIs
• how Gmail calendar talks to
Apple Calendar
• how my Train app knows “my
next train home”
4
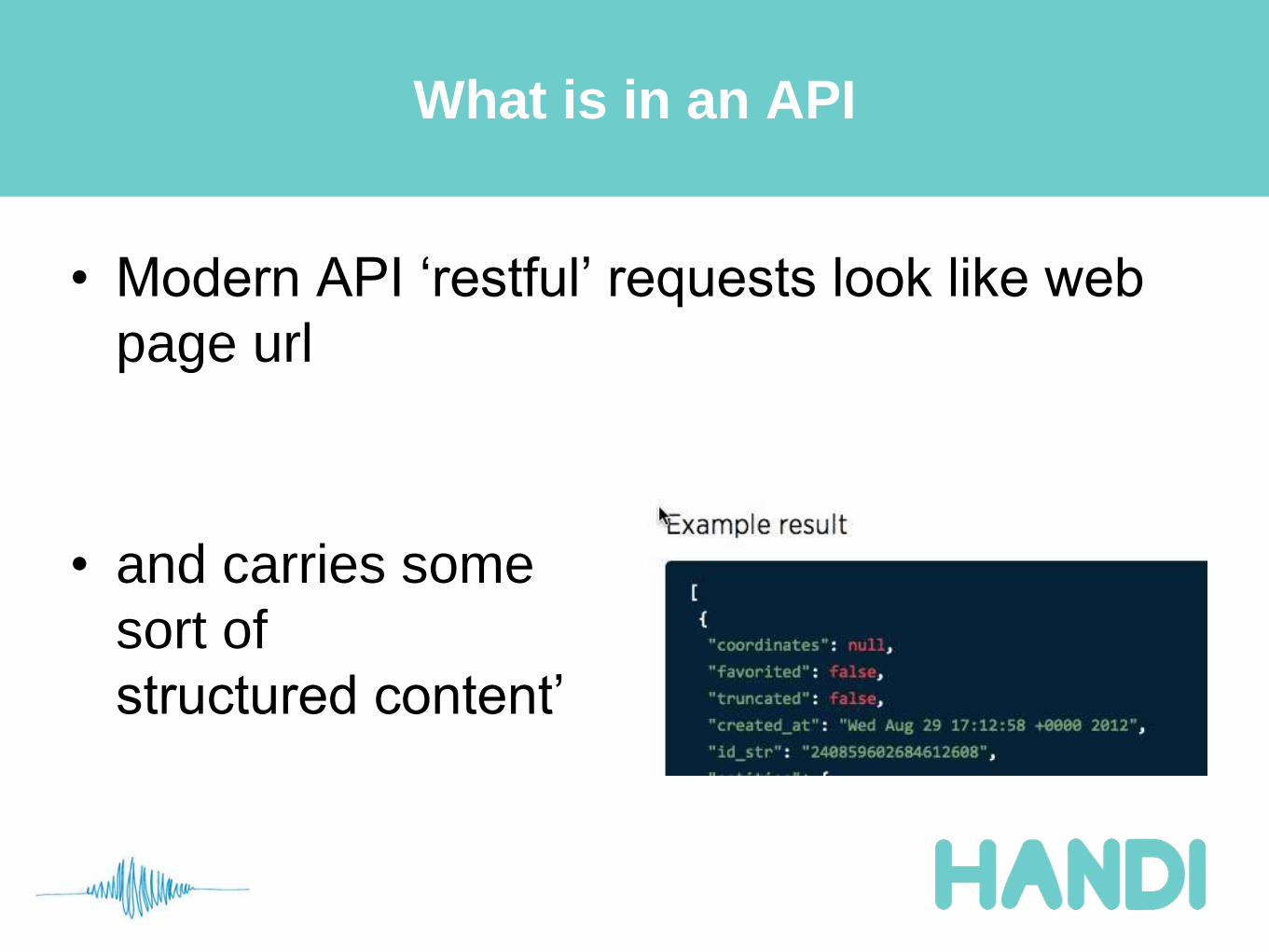
What is in an API
• Modern API ‘restful’ requests look like web
page urlhttps://api.twitter.com/1.1/statuses/user_timelin
e.json?screen_name=twitterapi&count=2
• and carries some
sort of
structured content’
5
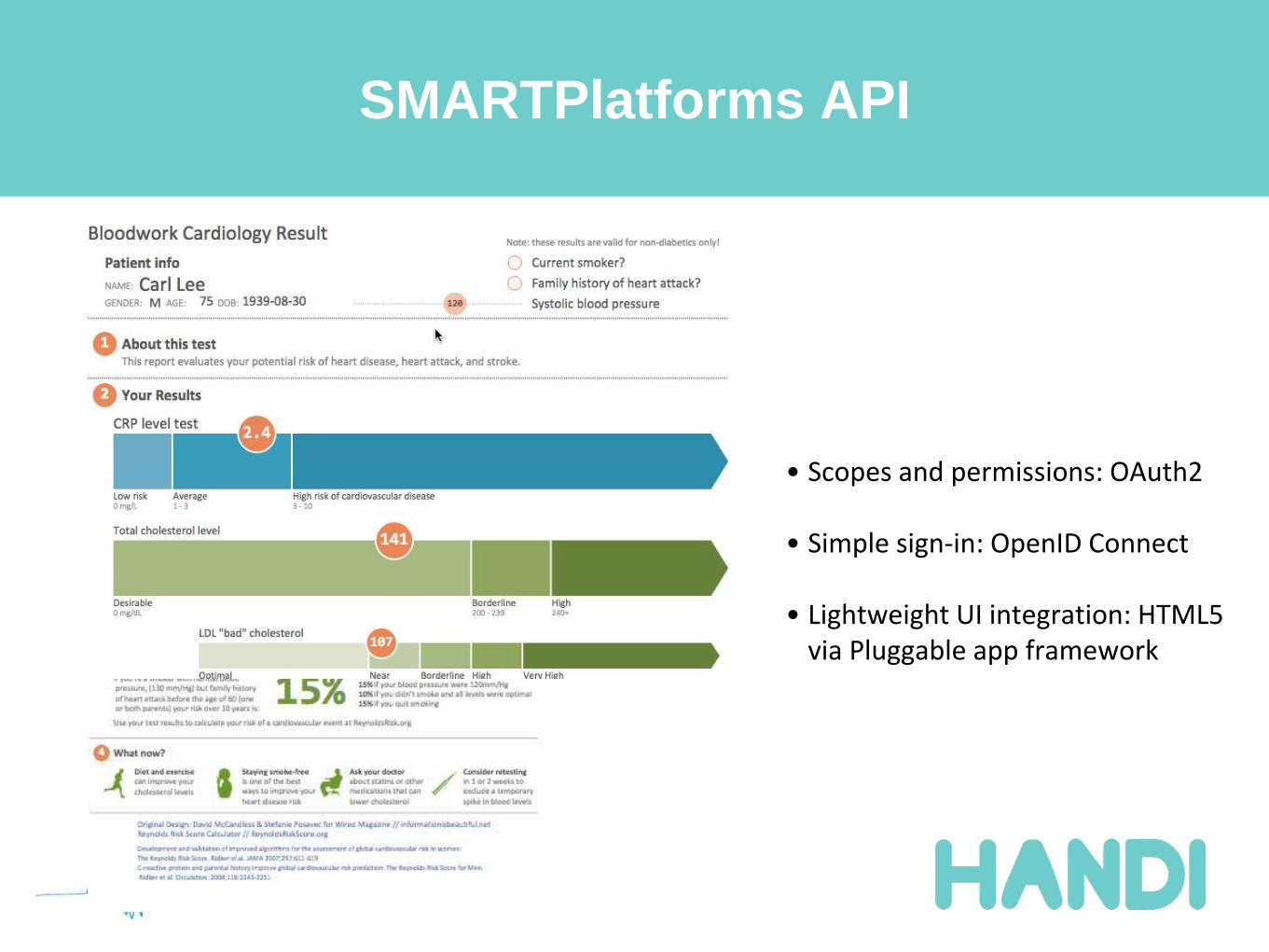
SMARTPlatforms API
6
• Scopes and permissions: OAuth2
• Simple sign-in: OpenID Connect
• Lightweight UI integration: HTML5 via Pluggable app framework
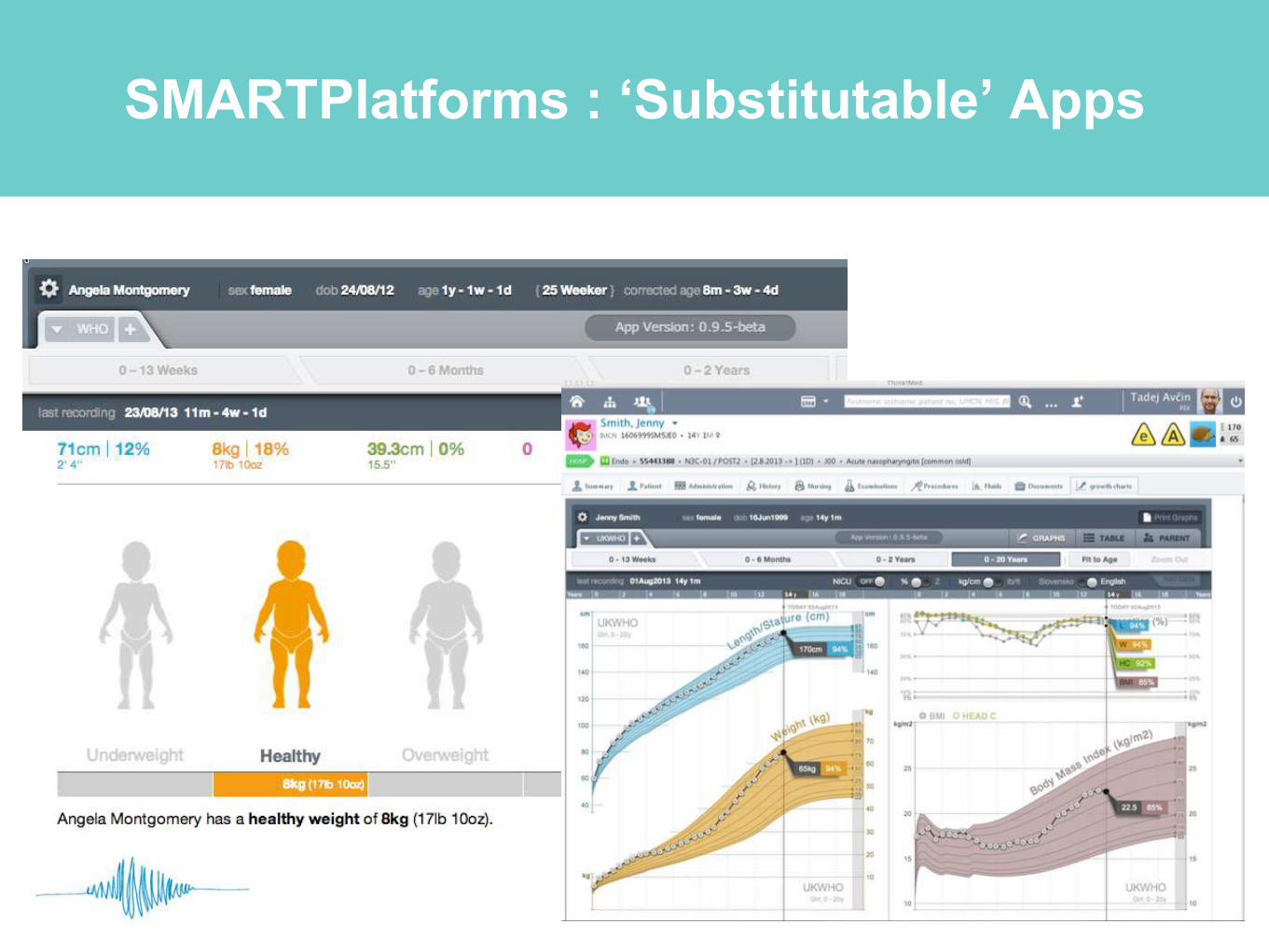
SMARTPlatforms : ‘Substitutable’ Apps
7
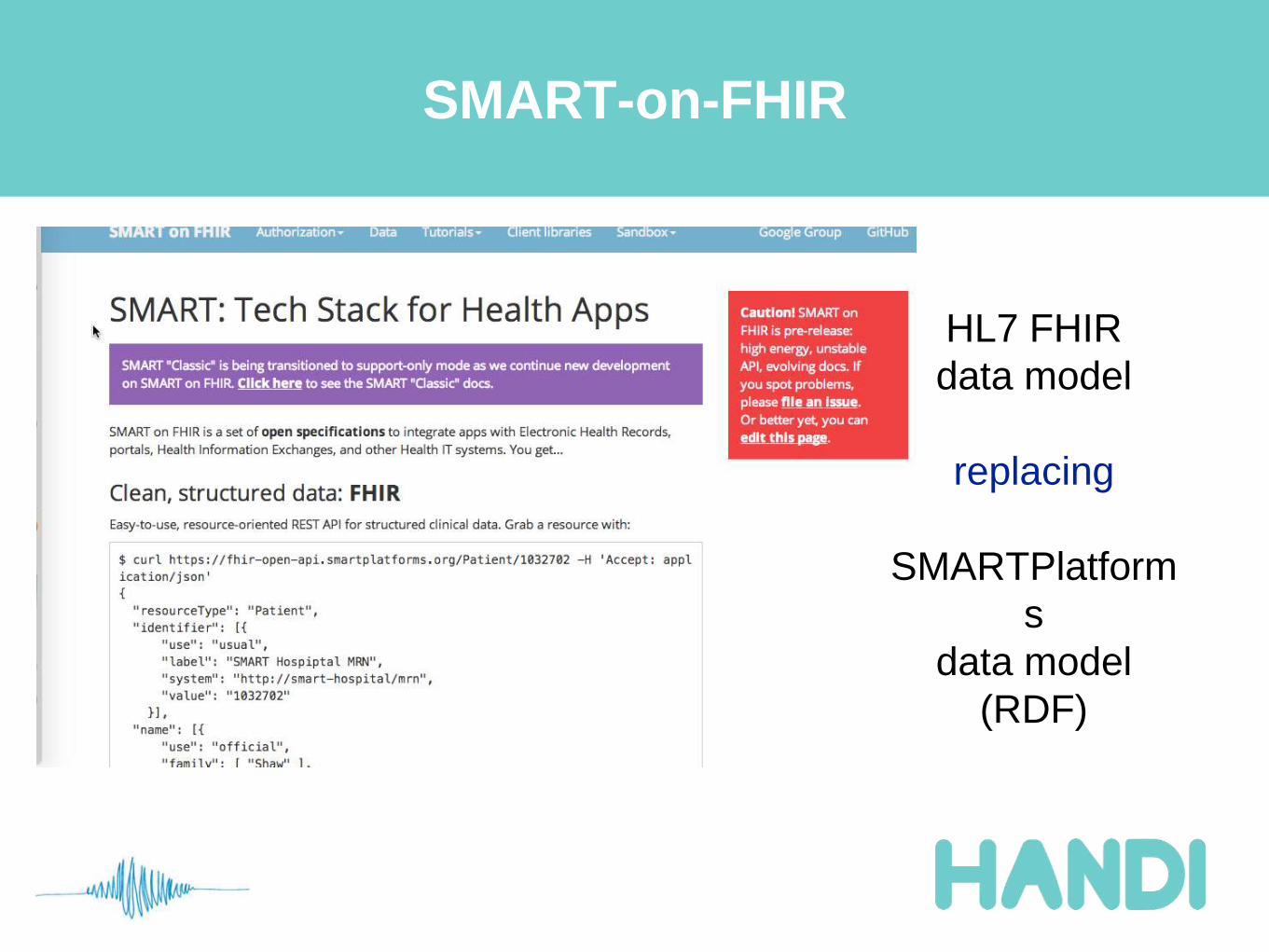
SMART-on-FHIR
8
HL7 FHIR
data model
replacing
SMARTPlatform
s
data model
(RDF)

HL7 FHIR API
9
What is FHIR good at?
• Communication of information between
systems with limited querying
• Strengths
• Developer friendly
• Lightweight approach
• Great documentation / community
10
Where might FHIR be weaker?
• Not designed for persistence
• can work but will it scale?
• partial querying only
• Resources will not work ‘out of the box’ in
the real world
• Need local extensions and profiles
• Version control / governance of the profiles
11
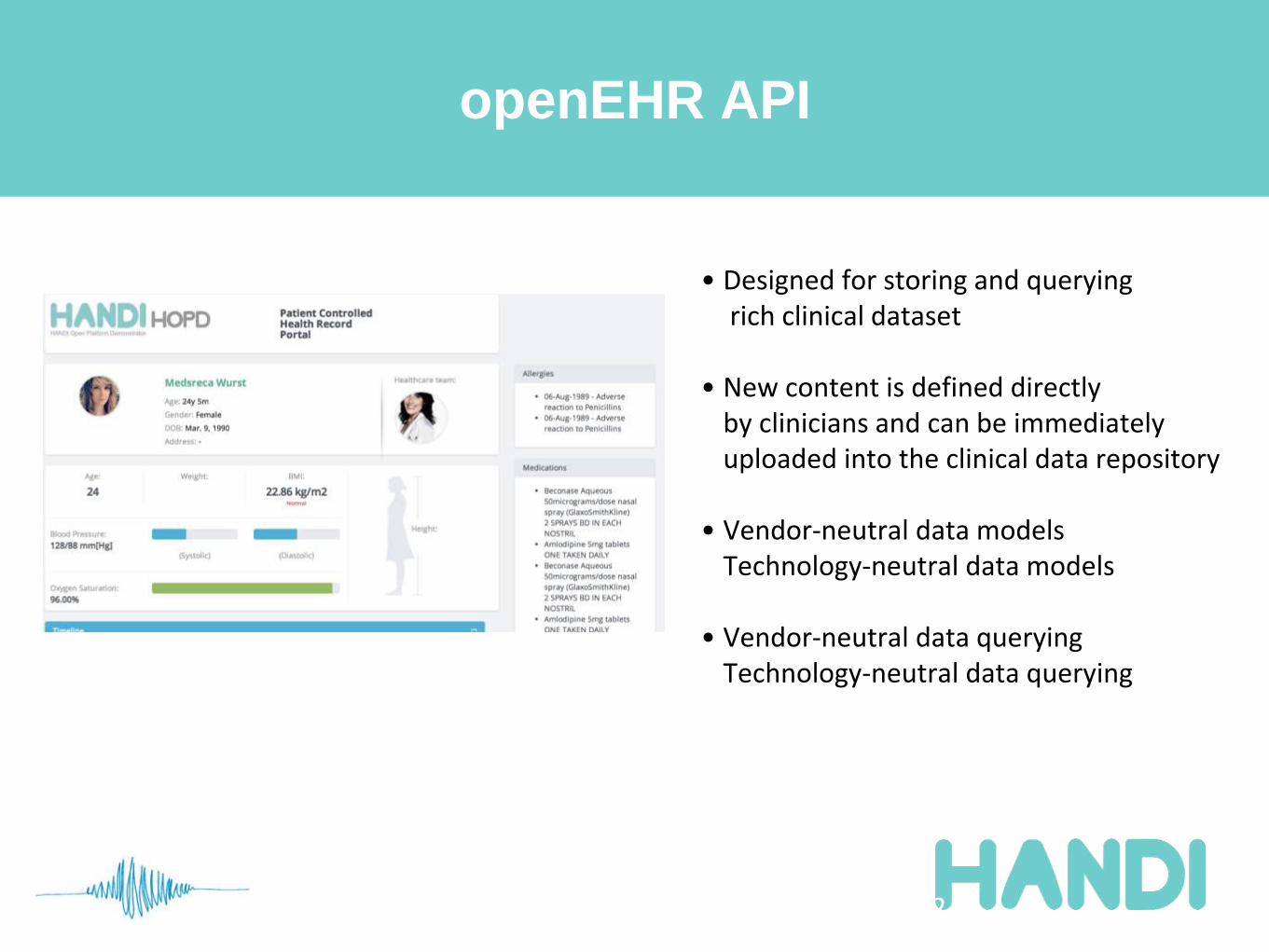
openEHR API
12
• Designed for storing and queryingrich clinical dataset
• New content is defined directlyby clinicians and can be immediately uploaded into the clinical data repository
• Vendor-neutral data modelsTechnology-neutral data models
• Vendor-neutral data queryingTechnology-neutral data querying
openEHR
• Weaknesses
• Complex technology
• but new simplifying APIs appearing
• Strengths
• clinically-led data modelling
• sharing archetypes = interoperability
• Enterprise strength performance
• Mature versioning/governance
13
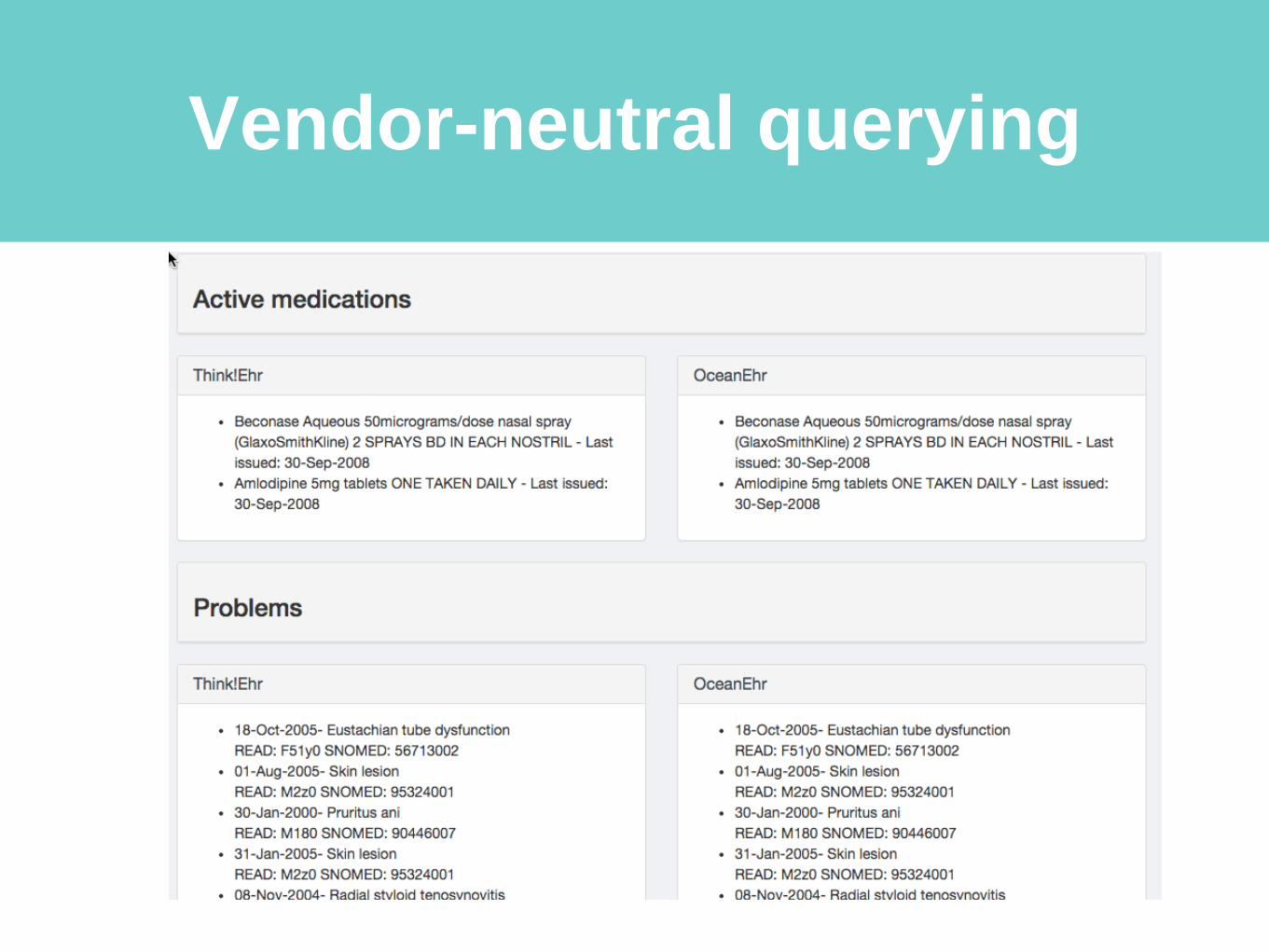
Vendor-neutral querying
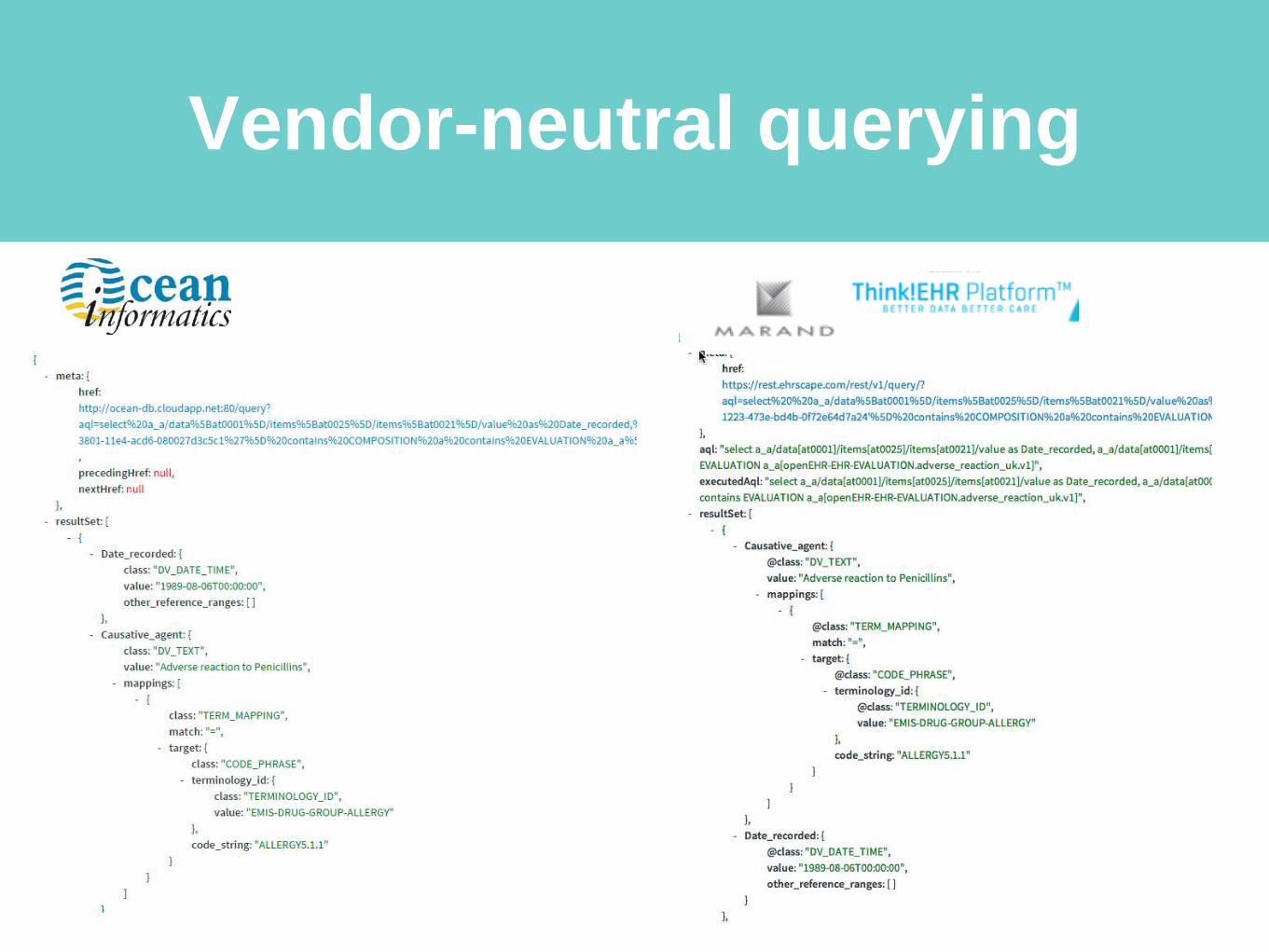
Vendor-neutral querying
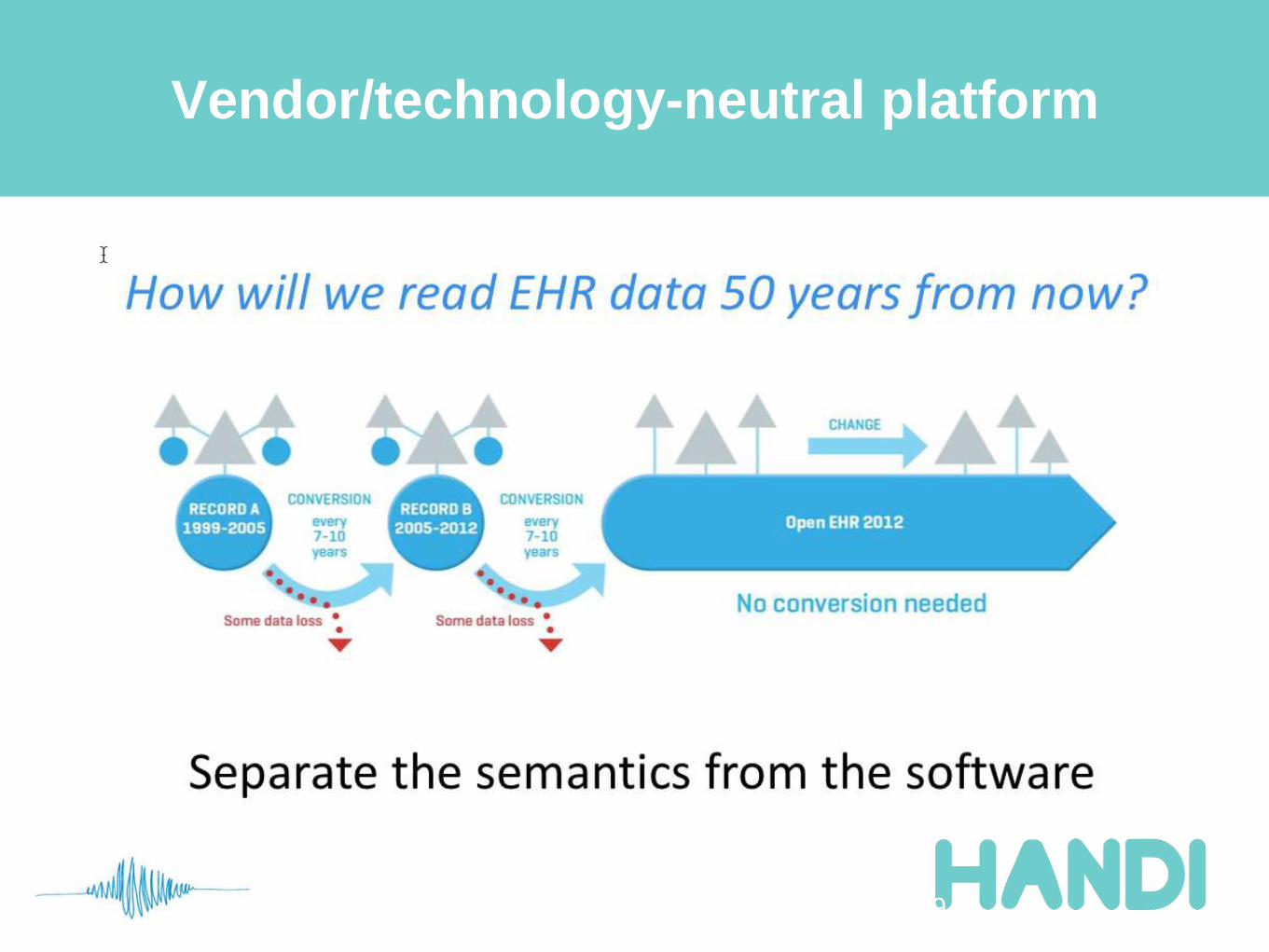
Vendor/technology-neutral platform
19
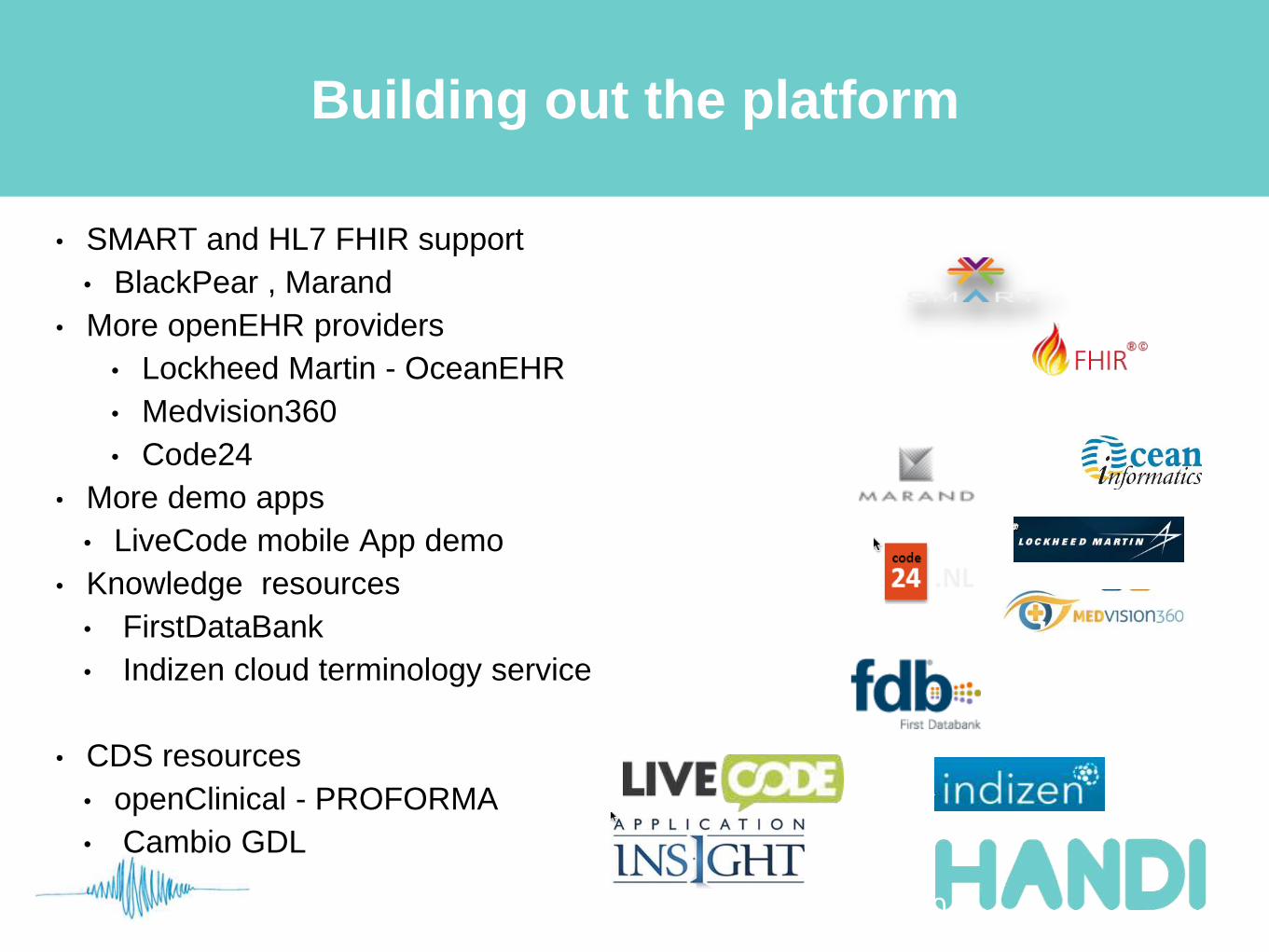
Building out the platform
• SMART and HL7 FHIR support
• BlackPear , Marand
• More openEHR providers
• Lockheed Martin - OceanEHR
• Medvision360
• Code24
• More demo apps
• LiveCode mobile App demo
• Knowledge resources
• FirstDataBank
• Indizen cloud terminology service
• CDS resources
• openClinical - PROFORMA
• Cambio GDL
20
SMARTPlatforms
Pluggable Webapp
API
HL7 FHIR
Clinical Content
Exchange NHS API
‘inVivo’
Datastore API
Detailed
Clinical Content
Development
Clinical leadership PRSB
Terminology
CentreHSCIC
Non
openEHR
systems
Archetype+ SNOMED Clinical
Content definitions
Apps developers
Interoperability is not a tech problem
“The real barriers to practical interoperability are
cultural and clinical”
–Diverse recording practice (sometimes arbitrary)
–Diverse recording requirements
–Complexity / contextual nature of health data
–Lack of clinical involvement in standards development
•Too technical, too philosophical
•Too time-consuming, too slow
23
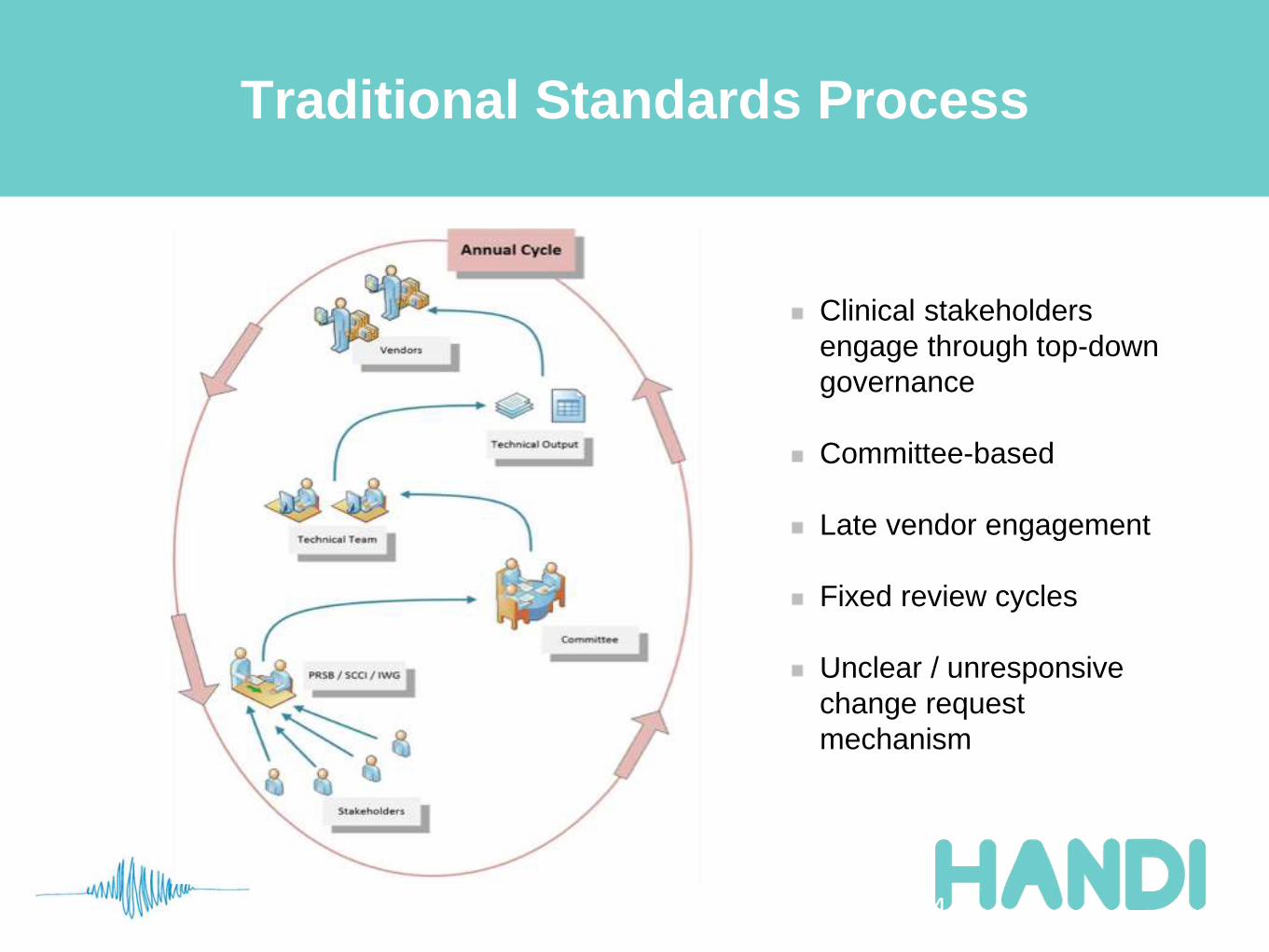
Traditional Standards Process
24
Clinical stakeholders
engage through top-down
governance
Committee-based
Late vendor engagement
Fixed review cycles
Unclear / unresponsive
change request
mechanism
Formal standards process is a barrier
• “Standards can be a barrier to progress”
– Ewan Davis, HANDI
– http://www.woodcote-consulting.com/farwell-to-ruthless-standardisation/
• Technical (ISO / SCCI)
– Still largely a paper and committee-bound process
• No clear problem report/change request mechanism
• Slow review cycles
• Professional (PRSB)
• Valuable clinical requirements input
• but distant from implementation
25
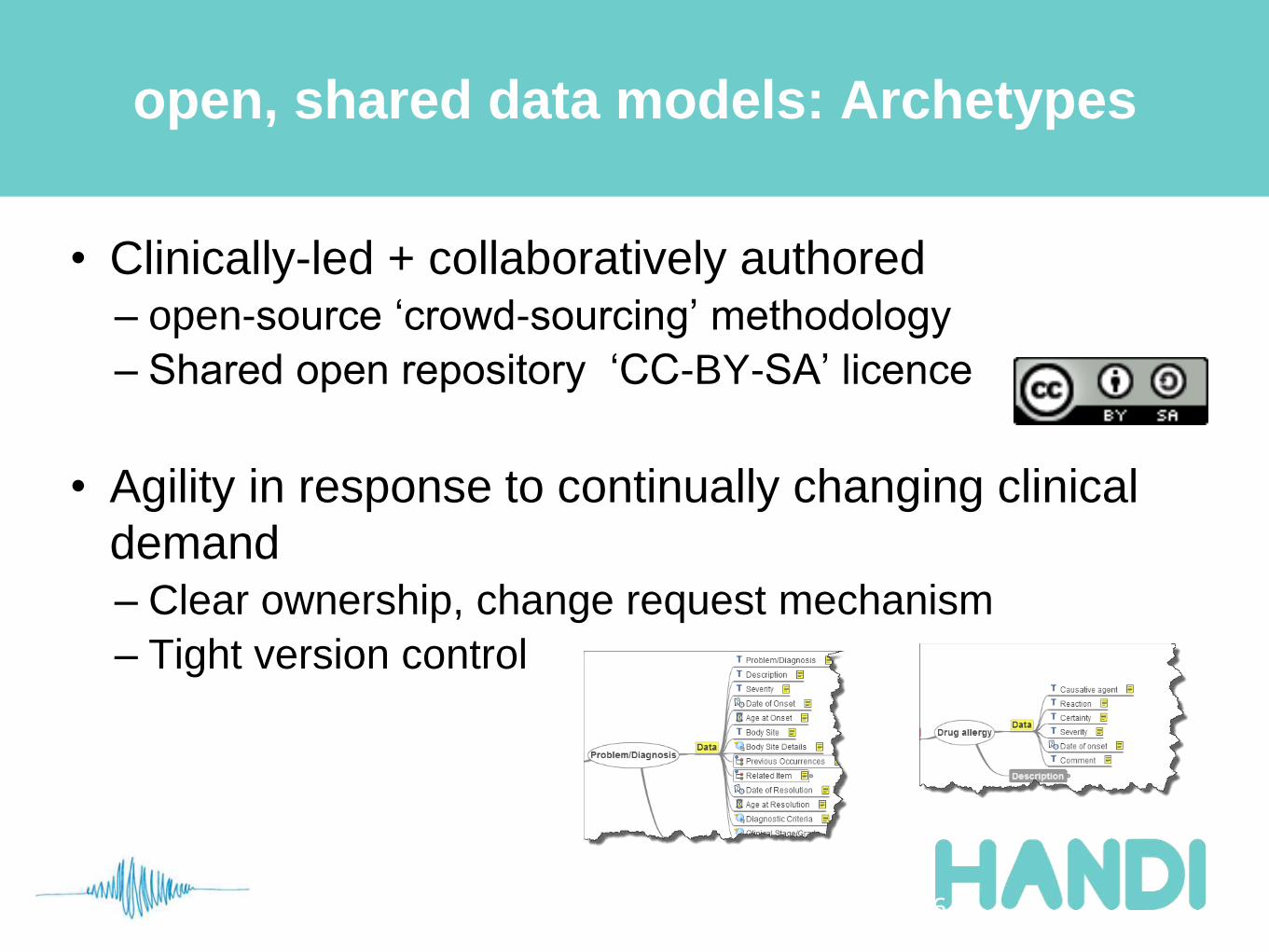
open, shared data models: Archetypes
• Clinically-led + collaboratively authored
– open-source ‘crowd-sourcing’ methodology
– Shared open repository ‘CC-BY-SA’ licence
• Agility in response to continually changing clinical
demand
– Clear ownership, change request mechanism
– Tight version control
26
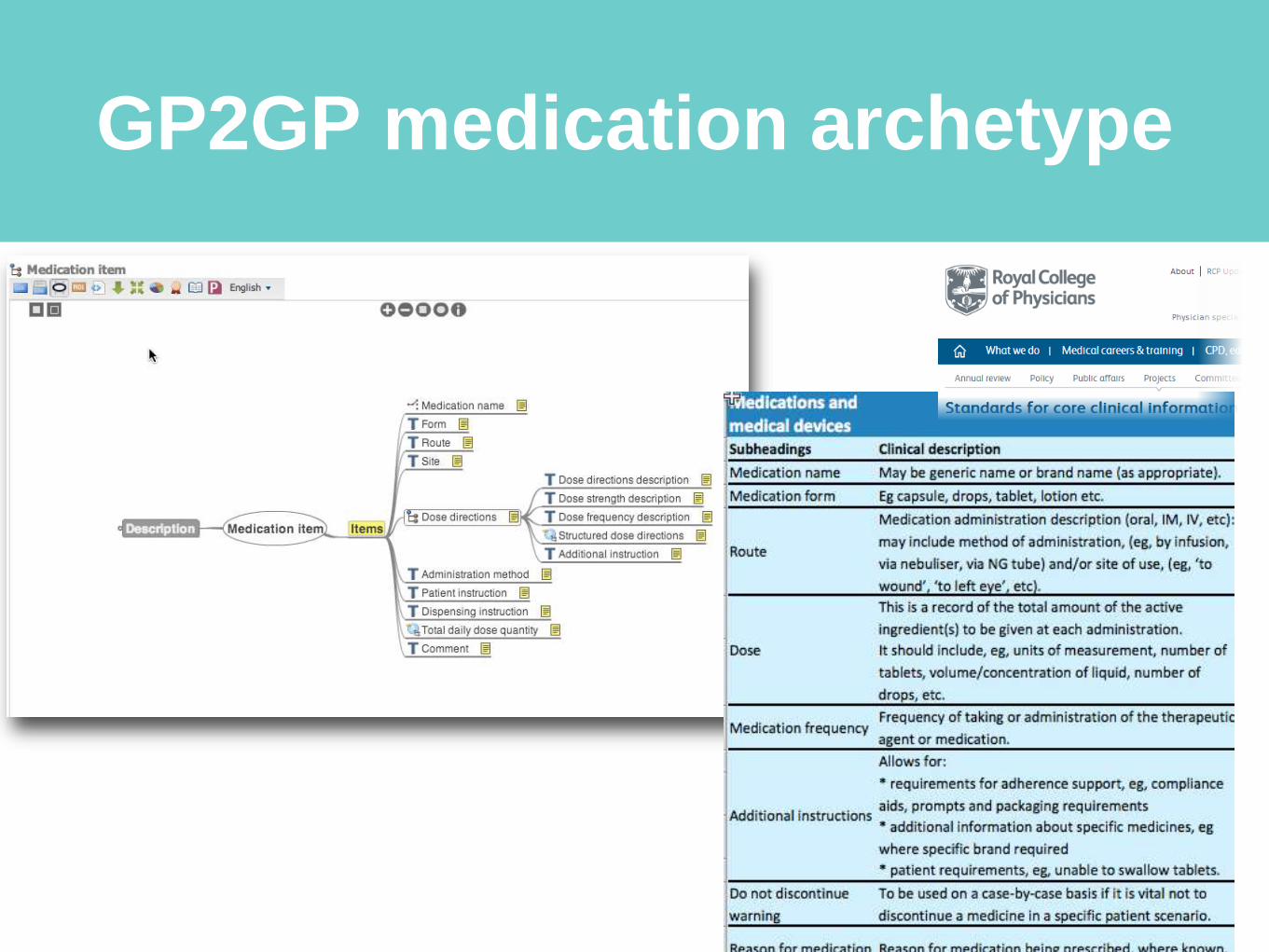
GP2GP medication archetype
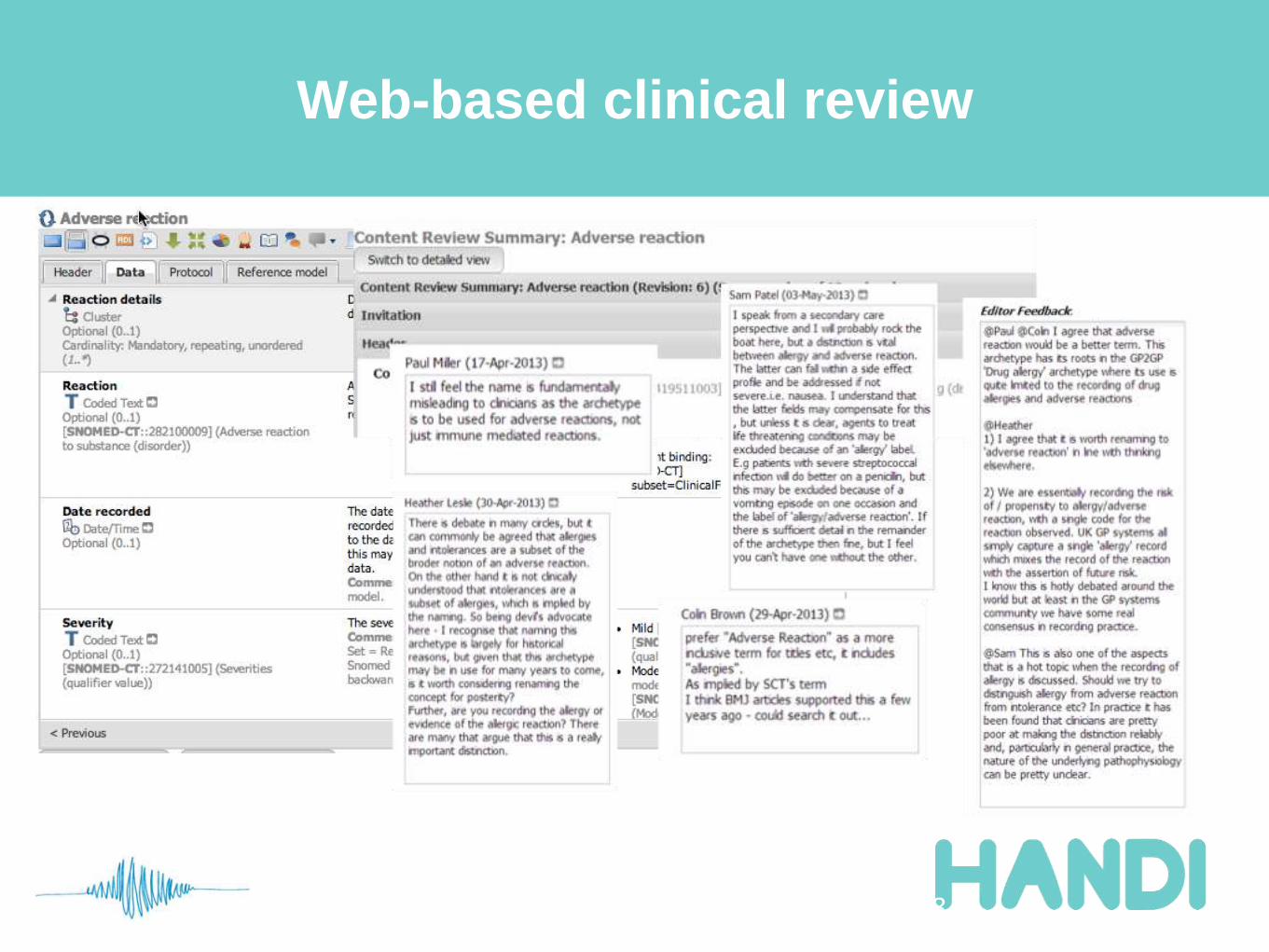
Web-based clinical review
28
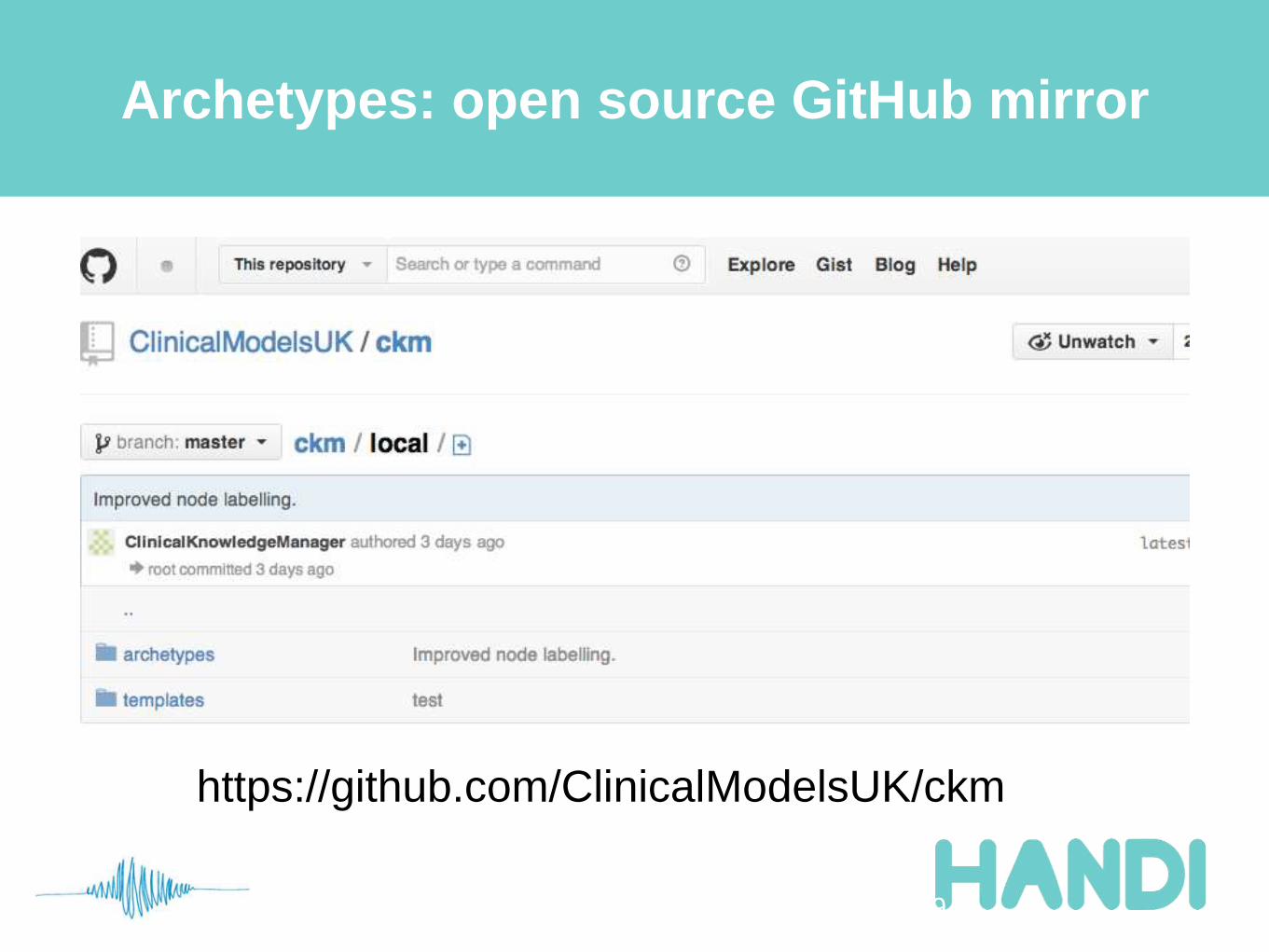
Archetypes: open source GitHub mirror
29
https://github.com/ClinicalModelsUK/ckm
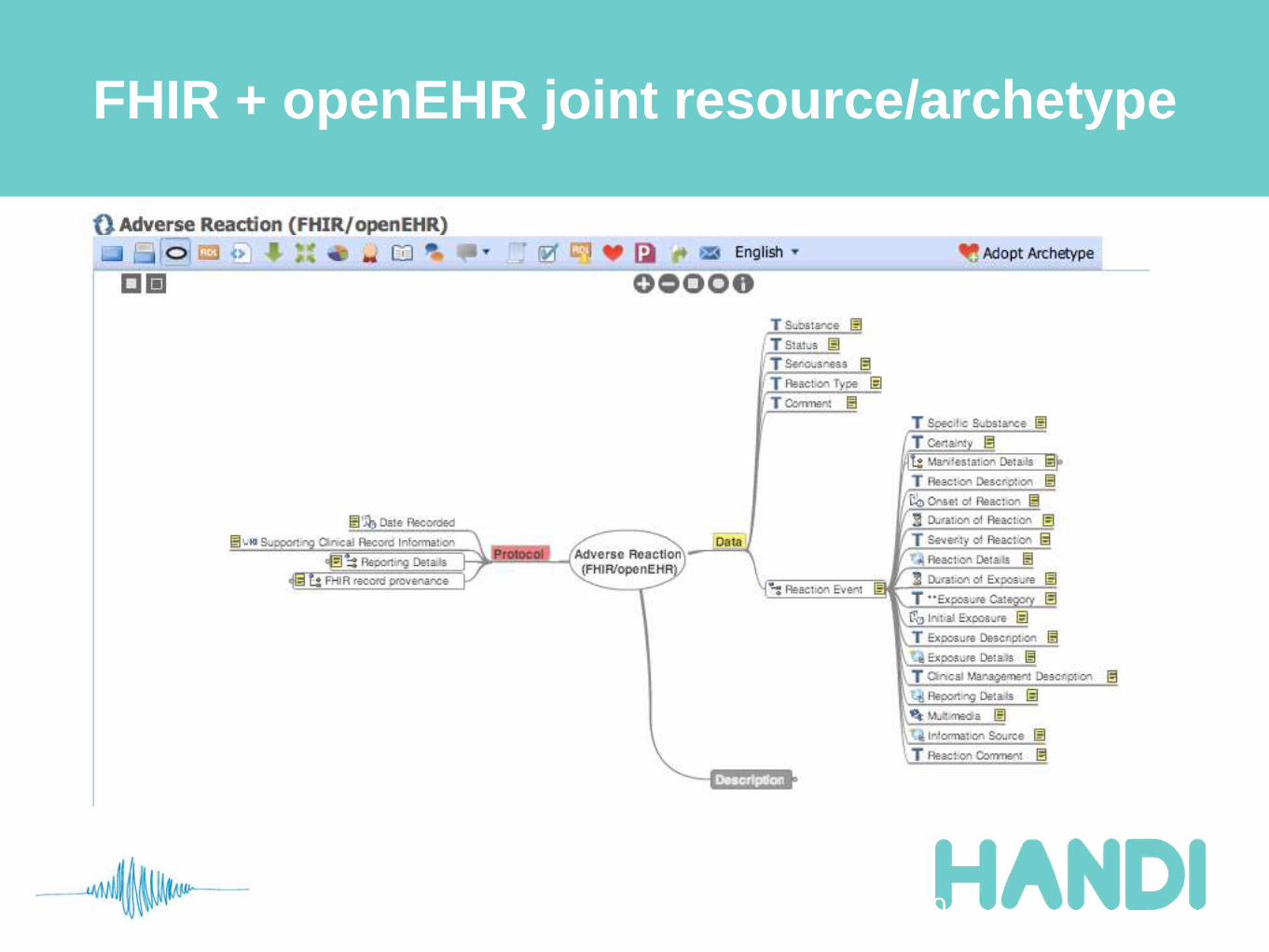
FHIR + openEHR joint resource/archetype
30
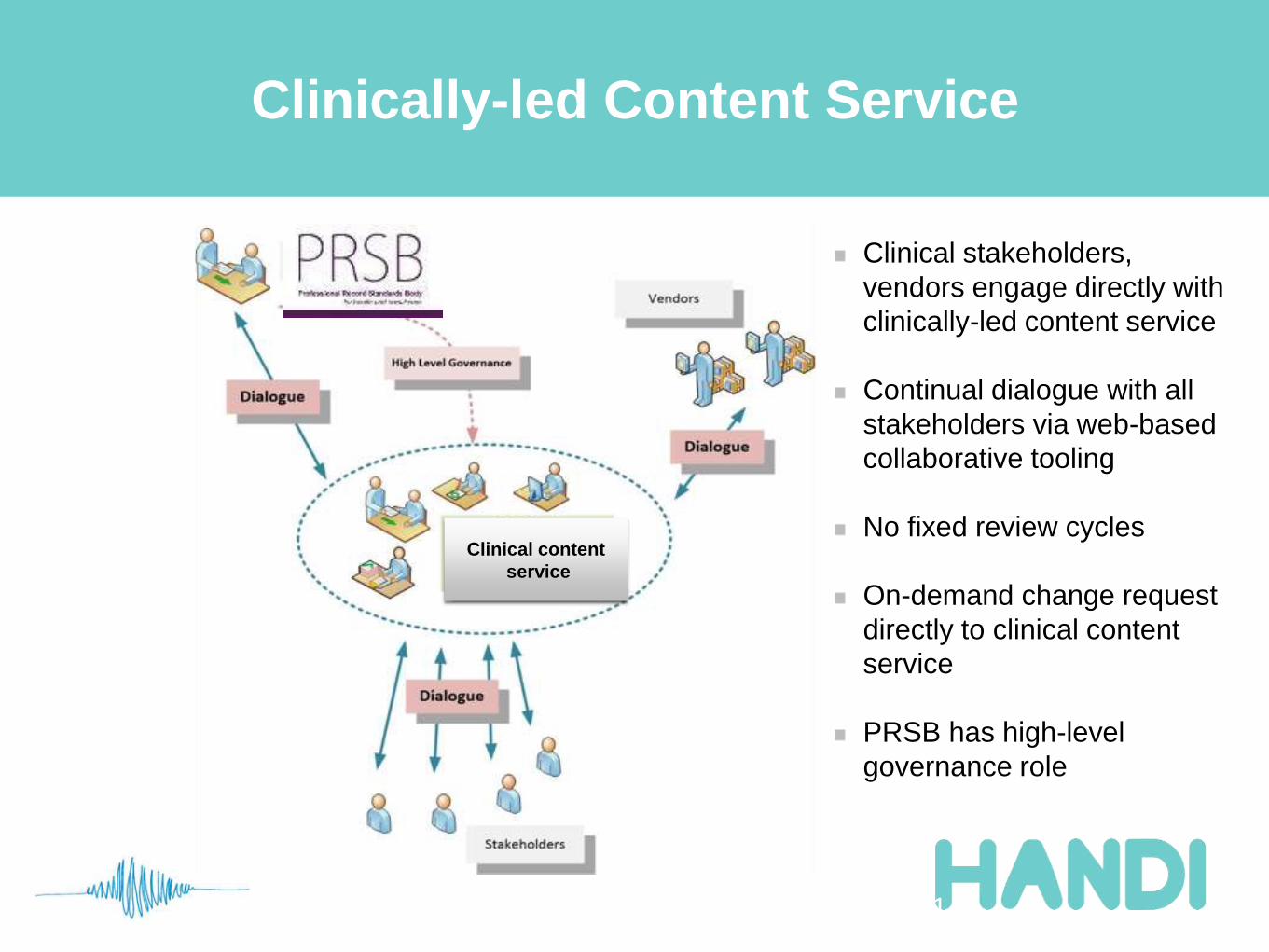
Clinically-led Content Service
31
Clinical content
service
Clinical stakeholders,
vendors engage directly with
clinically-led content service
Continual dialogue with all
stakeholders via web-based
collaborative tooling
No fixed review cycles
On-demand change request
directly to clinical content
service
PRSB has high-level
governance role
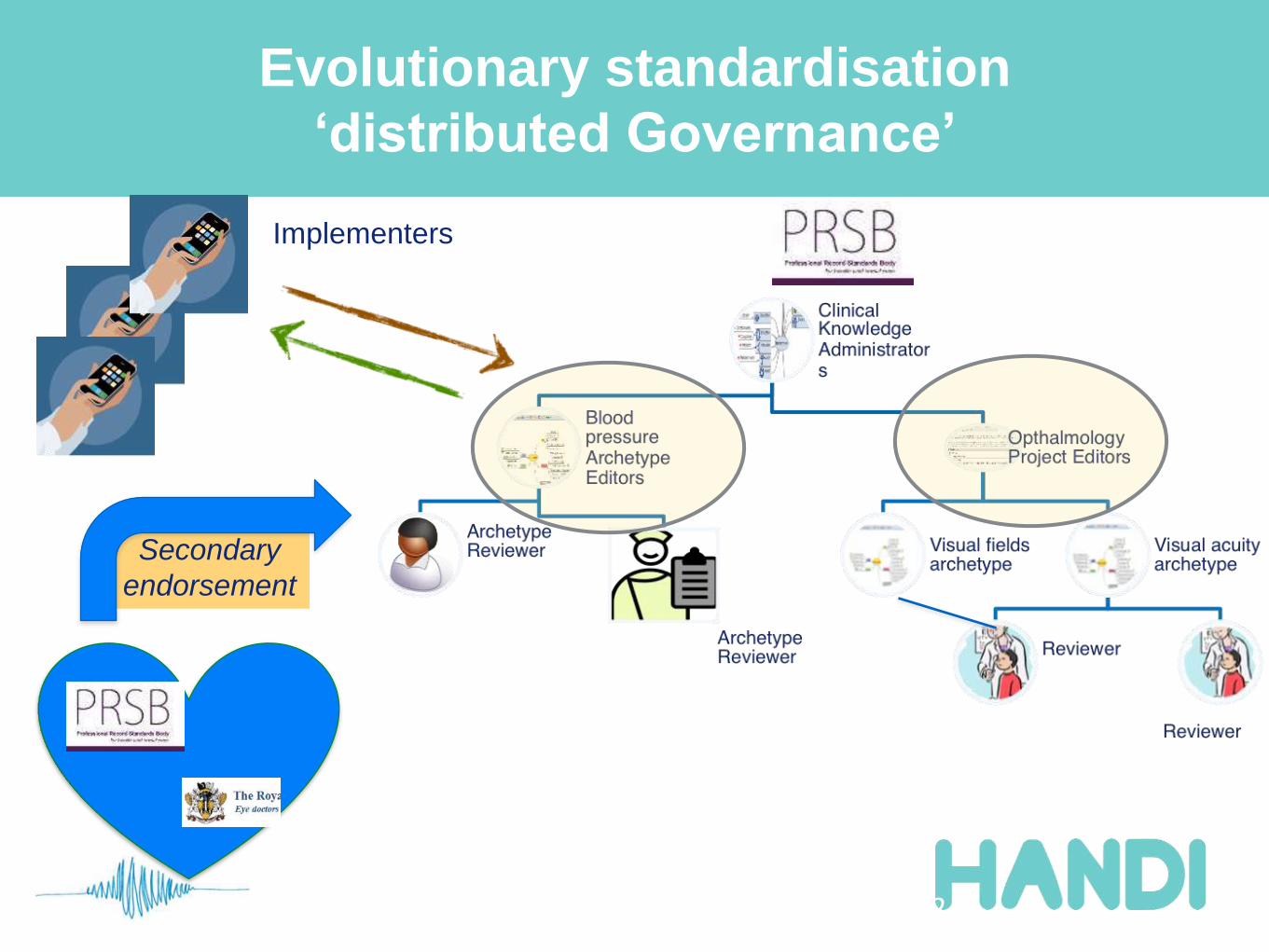
Evolutionary standardisation
‘distributed Governance’
32
Implementers
Secondary
endorsement
Publication and Secondary Endorsement
33
Project editors decide on
formal publication, acting as
“Benign Dictators”
Professional bodies, vendors
and PRSB may Endorse a
resource as a secondary
exercise
this does not restrain the
formal publication process
“By Royal Appointment”
PRSB hires and fires Editors
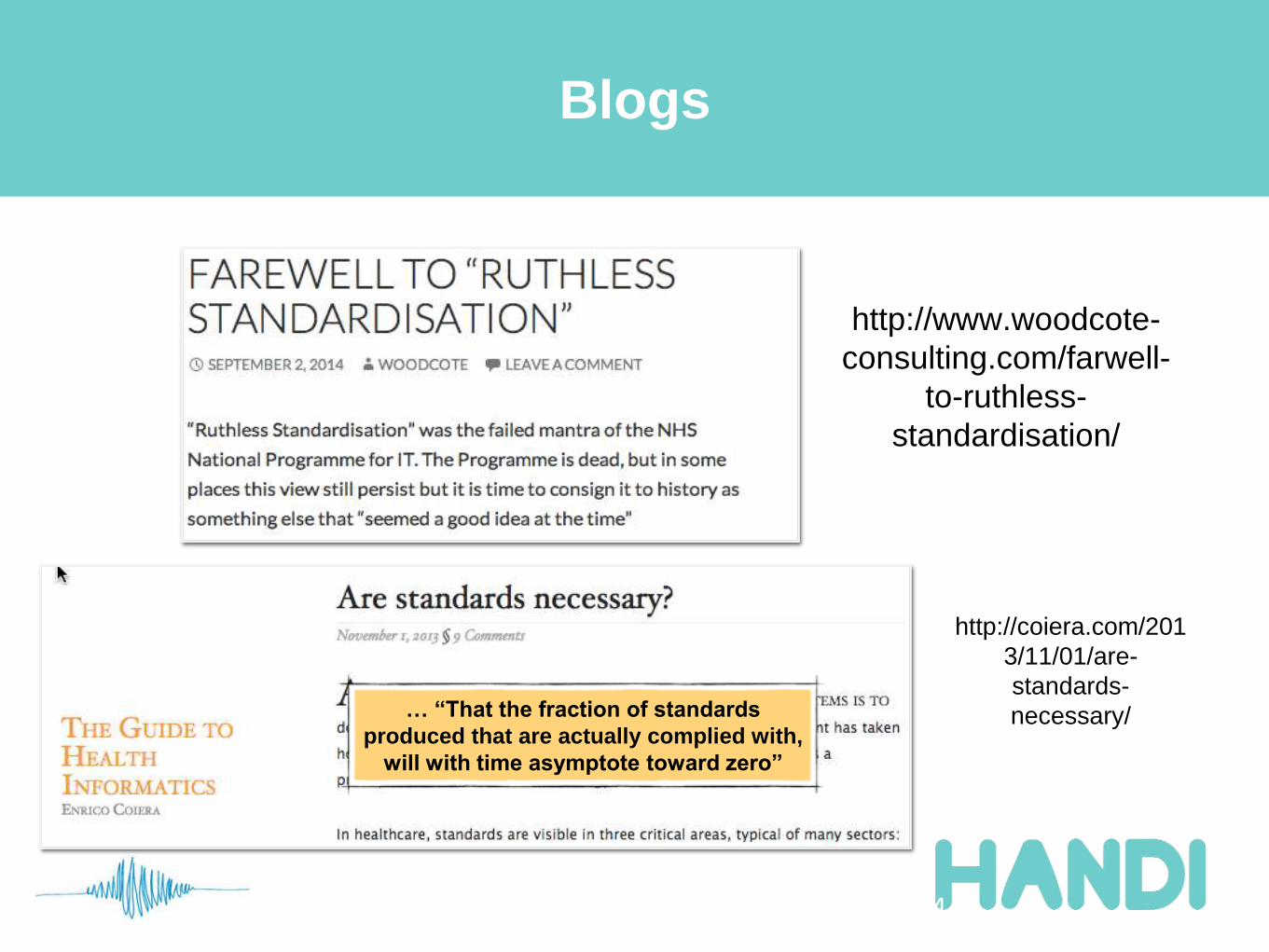
Blogs
34
http://www.woodcote-
consulting.com/farwell-
to-ruthless-
standardisation/
http://coiera.com/201
3/11/01/are-
standards-
necessary/… “That the fraction of standards
produced that are actually complied with,
will with time asymptote toward zero”
Links
• twitter: @ianmcnicoll
• HANDI-HOPD: handi-hopd.org
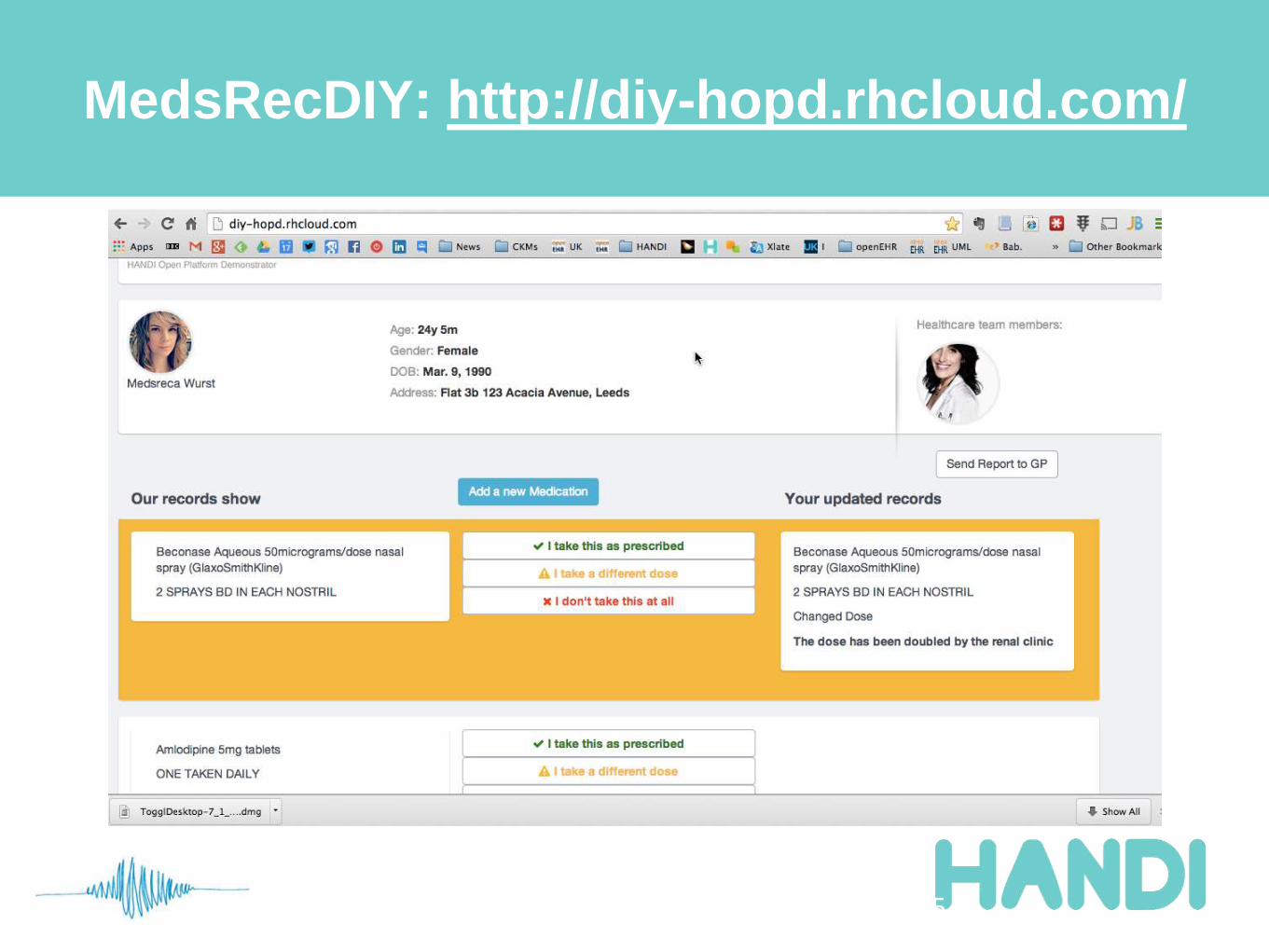
• http://diy-hopd.rhcloud.com/
• hopdscape-hopd.rhcloud.com
• minimal-hopd.rhcloud.com
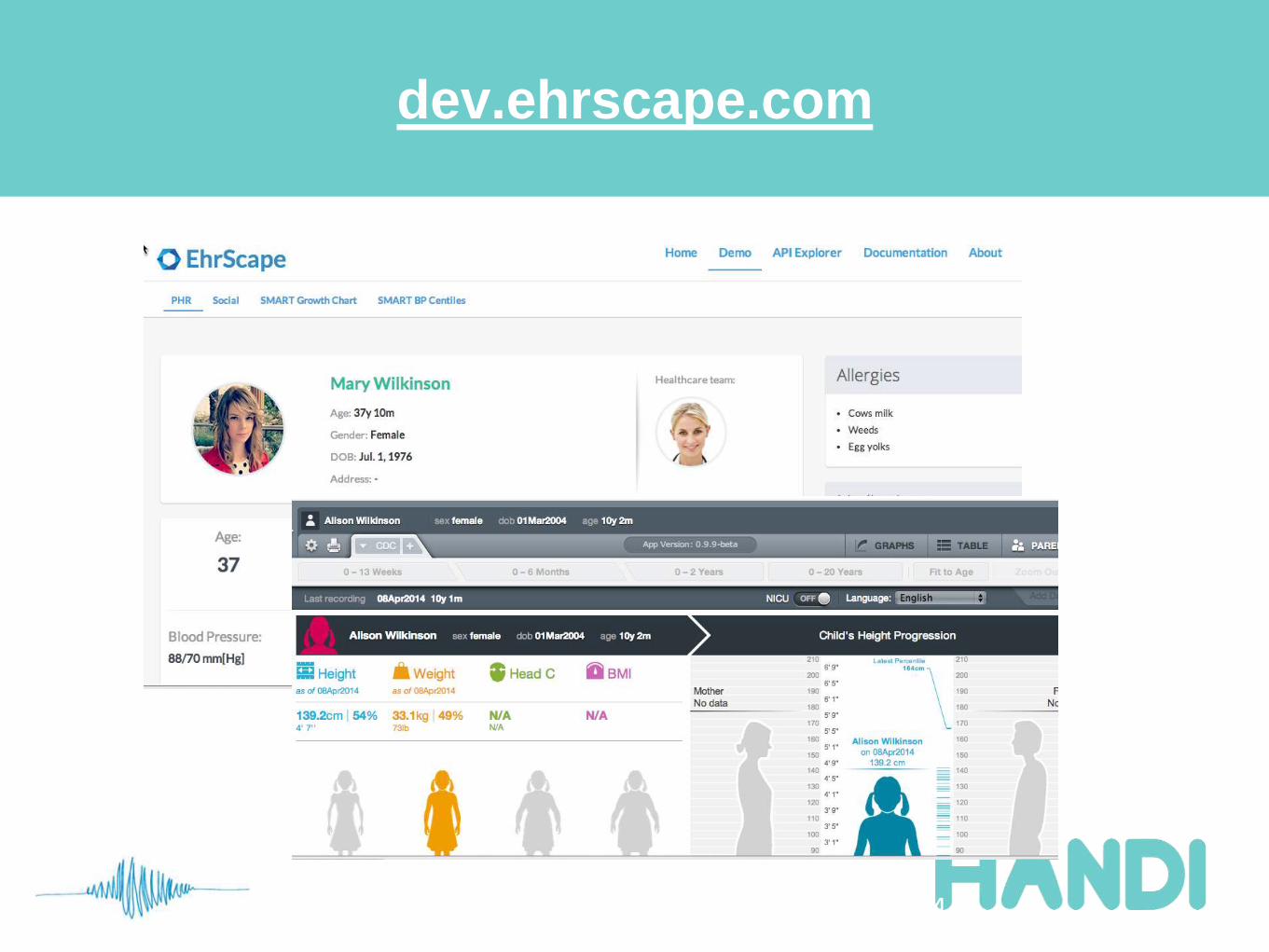
• Marand Ehrscape API: dev.ehrscape.com
• Leeds Innovation Lab Health Platform : http://leedslabplatform.com
• openEHR Foundation : www.openehr.org
• SMARTPlatforms: smartplatforms.org
• HL7 FHIR: hl7.org/implement/standards/fhir/
• International archetype repository: www.openehr.org/ckm
• UK archetype repository: www.clinicalmodels.org.uk
35
Top Related