







Languages
Pages
Legal


8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 1/40
A GUIDE TO
BREAST SURGERY

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 2/40

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 3/40
1
Introduction
Faulkner Hospital’s Breast Centre
and Sago Imaging and Diagnostic
Centre are nationally recognized
or their eorts in the detection and
treatment o breast disease. Our
mission is to provide our patientswith the best possible care with
dignity and compassion. Toward
this end, a team o Faulkner
physicians, nurses, sta educators
and administrative sta developed
this guide on breast surgery.
This guide is designed with patients
and amily in mind and should be
used as a reerence guide beore,
during and ater breast surgery.
You may not need the inormationcontained in every section. For
easy reerence we have divided
the book into several sections.
The index will help you identiy the
pages o the sections you will need
to review as outlined in your care
plan. Please read those sections
careully and direct questions or
concerns to your doctor or nurse
practitioner.
The rst section, Faulkner HealthCare Team, identies the various
providers that will be caring or
you. The second section, Breast
Health, explains the anatomy o
the breast as well as a guide or
completing sel-breast exams. All
patients should review both these
sections.
The third section, Types o Breast
Surgery and their Risk and
Complications, explains the
various breast surgeries (in order)
rom basic to complex. In addition,
it includes a description o the
possible risks and complications
associated with each procedure.
As you review the inormation it is
important or you to ocus only
on the procedure(s) (use the index
to identiy the proper pages) which
you and your physician(s) have
agreed upon in your care plan. This
will help avoid conusion among the
dierent procedures and may also
help prevent unnecessary anxiety
over procedures or tests that you
may not require.
The ourth section, Preparing or
Surgery, outlines the necessarysteps all patients must ollow to
be prepared or surgery. The th
section, Same Day Surgery,
should be reviewed by patients
who will not stay overnight in
the hospital and the next section,
Hospital Stay, should be reviewed
by patients who are admitted to
the hospital.
The seventh section, Arm
Exercises ater Axillary Lymph
Node Dissection, Sentinel
Lymph Node Biopsy and/
or Mastectomy, provides
important arm exercise instructions
or patients who have had an
axillary node dissection and/or a
mastectomy.
The nal three sections include
inormation on requently asked
questions, a glossary o terms
and a list o local and national
resources. We hope this
inormation will be useul to you
and your amily. Please keep this
book to use as a guide during your
treatment and recovery period rom
breast surgery.
The printing o this guide was made possible through the generosity o Carol Rabinovitz.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 4/40
2
Table o Contents
A. Faulkner Health Care Team . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
B. Breast Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Anatomy o the Breast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Sel Breast Exams . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
C. Types o Breast Surgery and their Risks and Complications . . . . . . . . . . . 6
Breast Biopsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Duct excision (including surgical ductogram) . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Partial Mastectomy (lumpectomy or wide excision or re-excision) . . . . . . . . . . . . . . . . 8
Wire Localization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Sentinel Lymph Node Biopsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Axillary Lymph Node Dissection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Total Mastectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Mastectomy with Axillary Node Dissection (or Modied Radical Mastectomy) . . . . . . . . 13
Mastectomy with Sentinel Lymph Node Biopsy . . . . . . . . . . . . . . . . . . . . . . . . 14
Breast Reconstruction (includes explanation o the various reconstruction procedures) . . . 15D. Preparing or Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Additional Support or Coping with Breast Cancer . . . . . . . . . . . . . . . . . . . . . . 17
Pre Admission Testing (PAT) clinic appointment . . . . . . . . . . . . . . . . . . . . . . . . 19
Pre-Operative (Pre-op) physical examination appointment . . . . . . . . . . . . . . . . . . 19
Two weeks prior to surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Seven (7) to ten (10) days beore surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
One week beore surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
The day beore surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
The day o surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
Immediately ollowing surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
E. Day Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Recovery process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Dressing Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Signs and symptoms o inection: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Pathology Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
Post-operative exam . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
F. Hospital Stay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
Patient Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Pain Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Prevention o post-operative pneumonia . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Dressing Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Drains and Drain management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Pathology Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
Recovery Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
Additional Post-op instructions: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
G. Arm exercises ater an Axillary Lymph Node Dissection and/or a Mastectomy 27
Beginning Exercises . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Advanced Exercises . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
H. Frequently Asked Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30
I Glossary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32
J. Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .35

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 5/40
3
•Breast Surgeon - The doctorwho perorms the surgery and
who is responsible or your
overall care. I you have breast
reconstruction your plastic
surgeon is also involved in your
care. Since some surgeons
operate at other hospitals as
well as maintain oces outside
o the Faulkner Hospital, they
may not always be available at
a given moment. However, the
surgeon always has coverage
available in his/her absence
and has reviewed your care
with the Physician Assistant
and Residents.
• Anesthesiologist - The doctor
who is responsible or your well
being during the operation.
The anesthesiologist works
with a Nurse Anesthetist who
will be present during the entire
procedure.
•Radiologist - The doctor who
reviews mammograms and
other diagnostic images. The
radiologist also perorms core
biopsies and wire-localizations.
•Pathologist - The doctor
who dissects and examines
the tissue in order to make a
diagnosis.
•Physician Assistant (PA) - Alicensed health care practitioner
who works with your surgeon
and the rest o the health care
team to ensure that your care
is the best possible we can
provide. I you are admitted to
the hospital, the PA will check
on your progress and may
perorm a physical examination.
•Resident - A licensed medical
doctor who works with yoursurgeon. Oten, the residents
have assisted in your surgery
as well. The residents are
available to address any
medical issues you may have
while in the hospital.
•Nurse - A licensed practitioner
who coordinates your care with
the members o the health care
team. The nurse acts as your
advocate to assure the plannedtreatments are progressing.
The nurse also works closely
with the nursing assistants to
provide physical care.
•Nursing Assistant - The
nursing assistant works under
the direction o the nurse in
providing physical care.
•Case Manager - A RegisteredNurse with knowledge o
health insurance, benets,
rehabilitation, skilled nursing
acilities, and certied home
care agencies. He/she will
meet with you and your amily
to discuss your discharge
plan. Your plan is based on
your treatment and health care
needs. Insurance benets and
your liestyle will determine your
individual discharge plan. With
your consent, the nurse case
manager will coordinate the
necessary arrangements.
•Clinical Social Worker - A
licensed proessional trained
to help with emotional issues
acing you and your amily.
The social worker helps you
cope during your recovery
period and assists with amily
concerns.
•Nurse Practitioner - A
licensed advance practice
nurse who works with the
surgeons in providing pre-
opertive education, post-
operative care and ollow up.
A. Faulkner Health Care Team
While a patient at Faulkner Hospital, you will have multidisciplinary team o providers monitor your care beore, during
and ater your surgery.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 6/40
4
B. Breast Health
Anatomy o the Breast
Pectoral Muscle The chest
muscle extends rom yourbreastbone to your shoulder and
collarbone. It is located under your
breast and contracts and expands
to help move your arm.
Lymph Nodes Help deend your
body against inections. They are
located under your arm and lter
fuid rom your breast and arm.
Fat and Connective Tissue
Supports and encases your entire
breast. The more brous tissue, the
rmer the breast.
Fatty Tissue Located throughout
the breast. The more you have thesoter the breast.
Lobules Enlarge during pregnancy
and produce milk or nursing. The
mammary lobules are clustered
throughout your breast and empty
into the ducts.
Ducts Carry milk rom your
mammary glands to your nipples
during breasteeding. The ducts
are tube-shaped structures lined by
a single layer o cells.
Nipple Located in the center o
each breast. It is the outlet orducts carrying milk.
Areola Pigmented (or colored)
circle o skin that surrounds each
nipple.
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 7/40
5
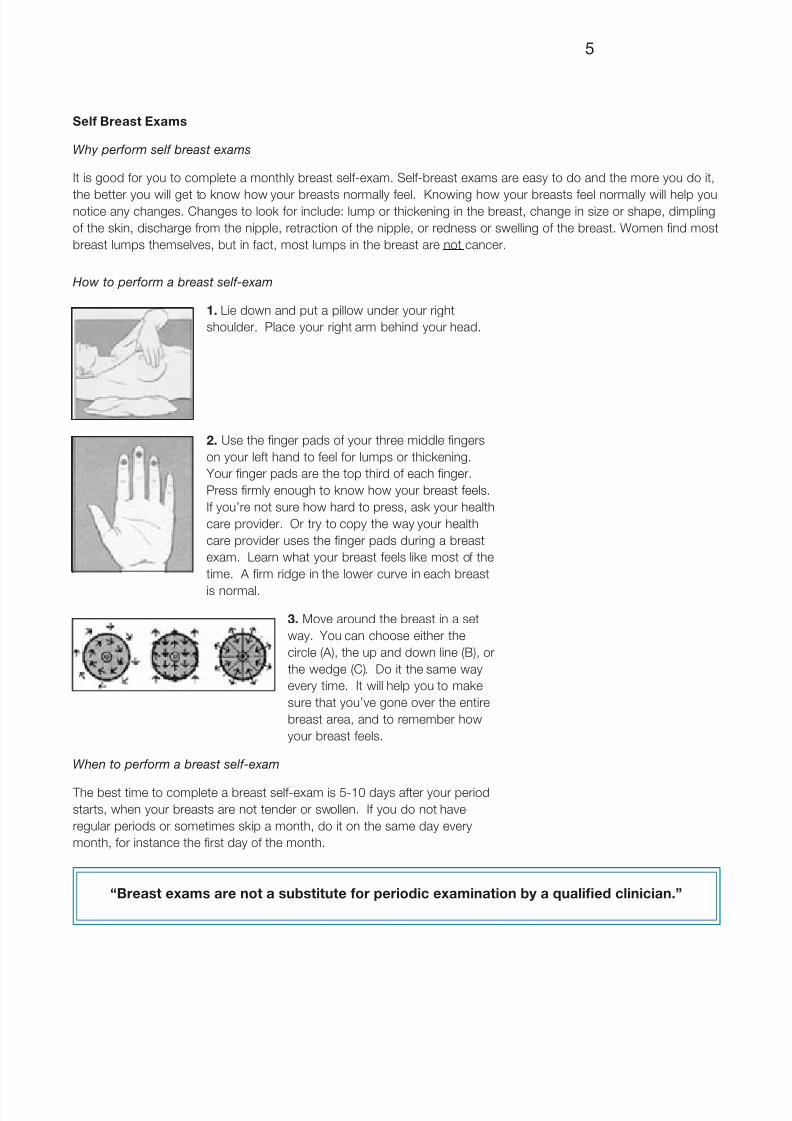
How to perform a breast self-exam
1. Lie down and put a pillow under your right
shoulder. Place your right arm behind your head.
2. Use the nger pads o your three middle ngers
on your let hand to eel or lumps or thickening.
Your nger pads are the top third o each nger.
Press rmly enough to know how your breast eels.
I you’re not sure how hard to press, ask your health
care provider. Or try to copy the way your health
care provider uses the nger pads during a breast
exam. Learn what your breast eels like most o the
time. A rm ridge in the lower curve in each breast
is normal.
3. Move around the breast in a set
way. You can choose either the
circle (A), the up and down line (B), or
the wedge (C). Do it the same way
every time. It will help you to make
sure that you’ve gone over the entire
breast area, and to remember how
your breast eels.
When to perform a breast self-exam
The best time to complete a breast sel-exam is 5-10 days ater your period
starts, when your breasts are not tender or swollen. I you do not have
regular periods or sometimes skip a month, do it on the same day every
month, or instance the rst day o the month.
Sel Breast Exams
Why perform self breast exams
It is good or you to complete a monthly breast sel-exam. Sel-breast exams are easy to do and the more you do it,
the better you will get to know how your breasts normally eel. Knowing how your breasts eel normally will help younotice any changes. Changes to look or include: lump or thickening in the breast, change in size or shape, dimpling
o the skin, discharge rom the nipple, retraction o the nipple, or redness or swelling o the breast. Women nd most
breast lumps themselves, but in act, most lumps in the breast are not cancer.
“Breast exams are not a substitute or periodic examination by a qualied clinician.”

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 8/40
6
C. Types o Breast Surgery and their Risks and Complications
There are three basic types o breast surgeries: biopsy, partial mastectomy and mastectomy. These surgeries may
involve additional procedures such as a duct excision, wire localization, axillary lymph node dissection, sentinel
lymph node biopsy and/or breast reconstruction. In reviewing this section please note that your surgery may include
one or more o the additional procedures.
Most breast surgeries and recovery are uncomplicated, however occasionally complications may occur. The risks
and complications that are associated with the various breast surgery procedures ollow the description o the
procedure. Please review and do not hesitate to ask your surgeon or clarication.
Breast Biopsy
A breast biopsy is perormed to
remove an area o breast tissue
or the purpose o diagnosis. The
biopsy procedure usually takes
about 45 minutes to one hour.
Once the surgeon removes the
tissue, the surgeon sends it to the
pathology department or their
review and diagnosis.
Sometimes this procedure is
done in conjunction with a wire
localization (see page 9) to indicate
the area to be removed or with a
duct excision (see page 7).
This surgery is considered sameday surgery and there is no need
to stay overnight in the hospital.
This means that ater the surgery,
you will go to the Post Anesthesia
Care Unit (PACU) until you are
eeling well enough to go home.
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
Please review the inormation on
“Day Surgery” on page 21.
Risks and complications include
inection, local bleeding, scarring,bruising, hematoma (blood clot in
the area o the surgery) and ailure
to remove the entire abnormal
area. There may also be a change
in the appearance o the breast.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 9/40
7
Duct excision (including
surgical ductogram)
A duct excision is a type o breast
biopsy. Your surgeon will remove a
portion o the milk duct to diagnosethe cause o discharge rom the
duct onto the nipple. The radiologist
will perorm a ductogam at the
Sago Centre (4th foor in Belkin
House) beore you come to the
operating room, the day o the
surgery.
To perorm the ductogram, the
radiologist will insert a small, very
narrow cannula (tube) into the
duct (in the nipple) rom which thedischarge can be expressed. X-ray
contrast material containing blue
dye is injected through the cannula
into the milk duct. A mammogram
is then taken. The dye helps the
surgeon identiy the discharging
duct during surgery. Sago sta
will bring you to the Day Surgery
department ater the ductogram
procedure is completed.
In the operating room, the surgeon
will make a skin incision to remove
tissue. The wound is usuallyclosed with sel-absorbing sutures
(stitches). The tissue is sent to
the pathology department or
processing, review and diagnosis
by the pathologist. The duct
excision surgery usually takes I to 2
hours.
I the radiologist cannot express
discharge the day o the procedure,
that is, you have no nipple
discharge, a ductogram usuallycannot be perormed. I this
happens, the radiologist will coner
with your surgeon and with you to
discuss whether we will proeeed
with surgery; i the surgery should
be rescheduled; or i an oce
appointment should be scheduled
with the surgeon.
The surgery is considered “same
day” surgery and there is no need
to be admitted to the hospital. Thismeans that ater the surgery, you
will go to the Post Anesthesia Care
Unit (PACU) until you are eeling well
enough to go home. Please review
the section on “Day Surgery” on
page 21.
Risks and potential complications
include but are not limited to:
inability to breast eed; a change
in the appearance o the breast
and nipple; change in sensationin the nipple and/or surgical site;
insucient blood supply to the
nipple; inection; local bleeding;
scarring; bruising; hematoma (blood
clot in the area o the surgery) and
ailure to remove or completely
remove the abnormal area.
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 10/40
8
Partial Mastectomy
(lumpectomy or wide excision
or re-excision)
A partial mastectomy is perormed
to remove the abnormal tissueor lump and a margin o normal
tissue surrounding the abnormal
area. This may be reerred to as
breast conserving surgery. Once
the surgeon removes the tissue, the
surgeon sends it to the pathology
department or their review and
diagnosis. The surgery usually
takes about one (1) to two (2) hours
and there will be a 2-3 inch scar on
your breast. The incision is closed
with sutures that disolve.
Sometimes this procedure is
perormed using a wire localization
to indicate the area to be removed.
I you are having a wire localizationplease see the explanation o the
procedure on page 9.
Sometimes this procedure also
includes perorming an axillary
lymph node dissection or sentinel
lymph node biopsy to remove
lymph nodes rom under the arm.
Please see the explanation or these
procedures on pages 9 or 11.
This surgery is considered sameday surgery and there is no need
to be admitted to the hospital. This
means that ater the surgery, you
will go to the Post Anesthesia Care
Unit (PACU) until you are eeling wellenough to go home. Please review
the section on “Day Surgery” on
page 21.
Risks and complications include
inection, local bleeding, scarring,
bruising, hematoma (a collection o
blood in the area o the surgery),
seroma (fuid collection in the
area o the surgery) and ailure to
remove the entire abnormal area.
There may also be a change inthe appearance o the breast as a
result o the procedure.
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 11/40
9
Wire Localization
This procedure is perormed
immediately prior to a biopsy (page
9) or partial mastectomy (page 8)
in help guide the surgeon to themammographic abnormality that
he/she cannot eel.
Wire localization is a technique
used to locate an abnormal area in
the breast when the area cannot be
palpated and/or when calcications
are seen on mammogram. The
wire localization procedure makes
it more likely that the area seen on
the mammogram and the tissue
removed in surgery correspond.In addition, this relatively painless
procedure makes it possible or
the surgeon to remove less breast
tissue during surgery without
increasing the risk o missing the
mammographic abnormality.
The wire localization is perormed
by a radiologist at the Sago
Centre in the Belkin House on
the ourth (4th ) foor. To localize a
mammographic abnormal area, theradiologist will position your breast
in the mammography machine.
The compression plate or this
procedure is a special plate with
an opening and a grid to mark your
mammogram. The radiologist uses
the grid markings to determine
exactly where the area (tissue) to be
removed is located.
Sometimes the wire localization
can be perormed using ultrasoundinstead o mammography. For this,
you will lie down on the ultrasound
table and the radiologist will use
the ultrasound sensor to nd the
area where the wire needs to be
inserted.
Beore starting the localization
procedure the radiologist numbs
your breast with a local anesthetic.
Then he or she will insert a
needle into the area where the
abnormality is located. A ew more
mammographic pictures may be
taken beore a thin, fexible wire
is passed through the needle
and than the needle is removed.
The nal X-rays are taken to
demonstrate that the wire is located
in the correct area and to act as a
guide or the surgeon.
A bandage is taped over the sot
wire and you can get dressed
leaving your bra o. Once you are
dressed you are accompanied back
to the surgical area in the hospital
or the surgery.
Sentinel Lymph Node Biopsy
This procedure is oten perormed
in conjunction with a partial
mastectomy or mastectomy. It may
also be perormed in conjunction
with an axillary node dissection.
The procedure identies andremoves sentinel lymph node(s)
rom under the arm. These are
the rst lymph nodes to receive
drainage rom the area o the tumor.
There is oten more than one
sentinel lymph node.
Your surgeon will use a blue dye, a
radionuclide dye, or a combination
o both to identiy the sentinel
lymph node. Once the surgeon has
identied and removed the sentinellymph node(s), he/she sends it to
the pathologist or their review and
diagnosis. The results will be given
to you when you awaken
This procedure does require
that you perorm post-operative
exercises, please see “ Arm
Exercises” on page 27.
I a radionuclide dye is used, it will
be injected into the breast in the
area where the tumor is located ornear the areola. This injection is
done by a radiologist at the Sago
Centre in Belkin House on the
ourth (4th) foor. The radiologist
uses either mammography or
ultrasound to guide the injection,
with a technique that is very
similar to the technique described
or “wire localization”. The
injection o radionuclide is usually
done at least 2 hours prior to your
scheduled surgery. The amount
o radiation exposure is less than a
routine chest x-ray. Ater injection,
you can get dressed leaving your
bra o. Once you are dressed
you will either be accompanied to
the surgical area or your surgery
or to Nuclear Medicine, where a
scan is done to check the location
o the sentinel lymph node. Once
your scan is completed, you are
escorted back to the surgical areaor the surgery.
I blue dye is used, it will be injected
into your breast by your surgeon in
the operating room. This is done
immediately prior to the surgery.
Risks and complications o sentinel
lymph node biopsy include all the
risks described or Axillary Node
Dissection on page 11 and the
instructions on page 27. In addition,
i blue dye is used, you may notice
a blue discoloration o your breast
ater surgery. This will ade in time.
You may also notice a blue-green
discoloration or your urine or other
bodily fuids immediately ater
surgery.
An axillary node dissection may be

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 12/40
10
required at the time o surgery or at
a later date. At the time o surgery,
an axillary node dissection would
be perormed i the sentinel node(s)
could not be identied or i the
surgeon nds cancer in the axilla.
It might also be required once the
nal pathology results are known i
those results are positive or cancer
in the sentinel node(s).
Care o your arm
It is important to always watch out or and prevent inections on the aected
arm. Avoid cuts, scratches, irritations and burns as much as possible by
doing the ollowing:
· use insect repellent and protective sunscreen
· wear gloves or washing dishes and using cleaners· wear gloves or gardening
· wear padded gloves or reaching into a hot oven
· use an electric razor or underarm shaving
· and do not cut your cuticles
In addition, avoid tight jewelry or clothing on the aected arm, carry your
purse on the opposite shoulder, avoid blood draws, injections, IV’s and
blood pressures on the aected side.
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 13/40
11
Axillary Lymph Node Dissection
This procedure is oten perormed in conjunction with a partial mastectomy (page 8) or total mastectomy (page 12)
in order to remove some o the lymph nodes rom under the arm. The atty tissue that is removed usually contains
about six to twenty lymph nodes.
This procedure usually takes an additional hour. Once the surgeon has removed the breast tissue and lymph nodes,
he/she sends it to the pathologist or their review and diagnosis. I the axillary node dissection is perormed in
conjunction with a mastectomy you will be admitted to the Hospital, see page 23, otherwise you will go home the
same day, see page 21.
This procedure does require that you perorm post-operative exercises, please see “Arm Exercises” on page 27.
Risks and complications include:
• Injury to the intercostal
brachial nerves: These
nerves run through the middle
o the lymph nodes and give
sensation to a small area in the
back o the armpit. Every eort
is made to save these nerves.
However, should they be cut or
stretched during the procedure,
the result would be an area o
numbness along the armpit and
the back portion o the upper
arm. This may be temporary or
permanent and will in no way
aect unction or use o thearm or hand. Please be careul
when shaving your armpit.
• Collection o lymph fuid
(Seroma): The fuid that
traveled through the lymph
nodes may accumulate in the
space where the lymph nodes
were removed until your body
absorbs it. This is usually not
signicant and results in a small
amount o swelling. I there
is a larger amount o swelling
and it is painul, aspiration o
the fuid may make you more
comortable. Please contact
your doctor’s oce to make
arrangements or you to havethe fuid aspirated.
•Swollen arm (Lymphedema):
This may occur because the
lymph fuids rom the arm must
reroute and lter through the
remaining axillary lymph nodes.
Because only the lower lymph
nodes are removed with this
procedure, this complication
happens much less oten
than it did with more radical
types o surgery done in the
past. Lymphedema occurs
in a small number o patients,
and symptoms can range rom
hand swelling alone to total armswelling. Should you note any
swelling o your hand or arm,
please contact your surgeon’s
oce who will instruct you in
the appropriate exercises and
ollow-up care. Intervention
includes physical therpy,
manual lymph drainage and
garments. Early intervention is
important, please review “care
o your arm” page 10.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 14/40
12
Total Mastectomy
A total mastectomy is the removal
o the entire breast. The surgery
usually takes 1-1/2 to three hours
and there will be a 4-8 inch scar.Once the surgeon removes the
tissue, he or she sends it to the
pathology department or their
review and diagnosis. Drains will be
placed under the skin at the bottom
o the incision to collect fuid during
the rst ew post-operative days.
See drain inormation page 25.
Ater the procedure, you will go the
Post Anesthesia Care Units (PACU)
or observation until you eel well
enough to be transported to your
room. Patients are admitted to the
hospital overnight. Please see page
23 or inormation on “Hospital
Stay”
Risks and complications include
inection, local bleeding, scarring,
bruising, hematoma (a blood clot
in the area o the surgery), seroma
(fuid collection in the area o the
surgery). Delayed healing o the
scar may occasionally occur due
to decreased blood supply. This
is more common in women who
smoke or who have diabetes. I this
happens a large “scab” will orm
and will gradually all o as healing
occurs. The incision will still heal
normally.
The mastectomy procedure does
require that you perorm post-
operative exercises. Please see
“Arm Exercises” on page 27.
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 15/40
13
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
Mastectomy with Axillary
Lymph Node Dissection (or
Modied Radical Mastectomy)
The surgery will take 2 to 4 hours
including removing both the breasttissue and axillary lymph nodes.
There will be a 4-8 inch scar. Once
the surgeon removes the tissue, the
surgeon sends it to the pathology
department or their review and
diagnosis. Drains will be placed
under the skin at the bottom o the
incision to collect fuid during the
rst ew post-operative days.
Ater the procedure, you will go the
Post Anesthesia Care Units (PACU)or observation until you eel well
enough to be transported to your
room. Patients are admitted to thehospital overnight. Please see the
inormation on “Hospital Stay” on
page 23.
Risks and complications include
inection, local bleeding, scarring,
bruising, hematoma (a blood clot
in the area o the surgery), seroma
(fuid collection in the area o the
surgery). Delayed healing o the
scar may occasionally occur due
to decreased blood supply. Thisis more common in women who
smoke or are diabetic. I this
happens a large “scab” will ormand will gradually all o as healing
occurs. The incision will still heal
normally.
To understand the risks and
complications o an axillary lymph
node dissection, please review the
description on page 11.
This procedure does require
that you perorm post-operative
exercises. Please see “ArmExercises” on page 27.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 16/40
14
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
Mastectomy with Sentinel
Lymph Node Biopsy
This procedure removes the
entire breast and the sentinel
lymph node(s). The surgery willtake two to our hours and there
will be a 4-8 inch scar. Once the
surgeon removes the tissue, the
surgeon sends it to the pathology
department or their review and
diagnosis. Drains will be placed
under the skin at the bottom o the
incision to collect fuid during the
rst ew post-operative days.
Ater the procedure, you will go
to the Post Anesthesia Care Units(PACU) or observation until you eel
well enough to be transported to
your room. Patients admitted to the
hospital overnight. Please see page
23 or inormation on “HospitalStay.”
Risks and complications include
inection, local bleeding, scarring,
bruising, hematoma (a blood clot
in the area o the surgery), seroma
(fuid collection in the area o the
surgery). Delayed healing o the
scar may occasionally occur due
to decreased blood supply. This
is more common in women who
smoke or who have diabetes. I thishappens a large “scab” will orm
and will gradually all o as healing
occurs. The incision will still heal
normally.
To understand the risks and
complications o the Sentinel
Lymph Node Biopsy, please review
the inormation on page 9.
The mastectomy procedure
does require that you perorm
post-operative exercises.
Please see “Arm Exercises” on
page 27.
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 17/40
15
Breast Reconstruction
(includes explanation o
the various reconstruction
procedures)
Breast reconstruction is intendedto restore your breast shape.
Reconstruction can be done at
the same time as a mastectomy
(immediate reconstruction) or
months or years later (delayed
reconstruction). There are several
techniques a plastic surgeon can
use or breast reconstruction.
One is using articial materials
(expanders and implants), the
second uses your own tissue, and
the third uses a combination o
both. Patients who have breast
reconstruction are admitted to
the hospital or approximately 3-5
days. Please see the section on
“Hospital Stay” on page 23.
Each type o reconstruction
technique has risks and
complications that are unique to
that procedure. However, as or
all surgeries the usual risks and
complication include inection,
local bleeding, scarring, bruising,
hematoma (a blood clot in the
area o the surgery) and seroma
(fuid collection in the area o the
surgery).
Risks o smoking: Smoking
causes the blood vessels to
narrow. This lowers the supply o
nutriebts and oxygen to the body.
Smoking can slow down healing
ater surgery, making recovery time
longer.
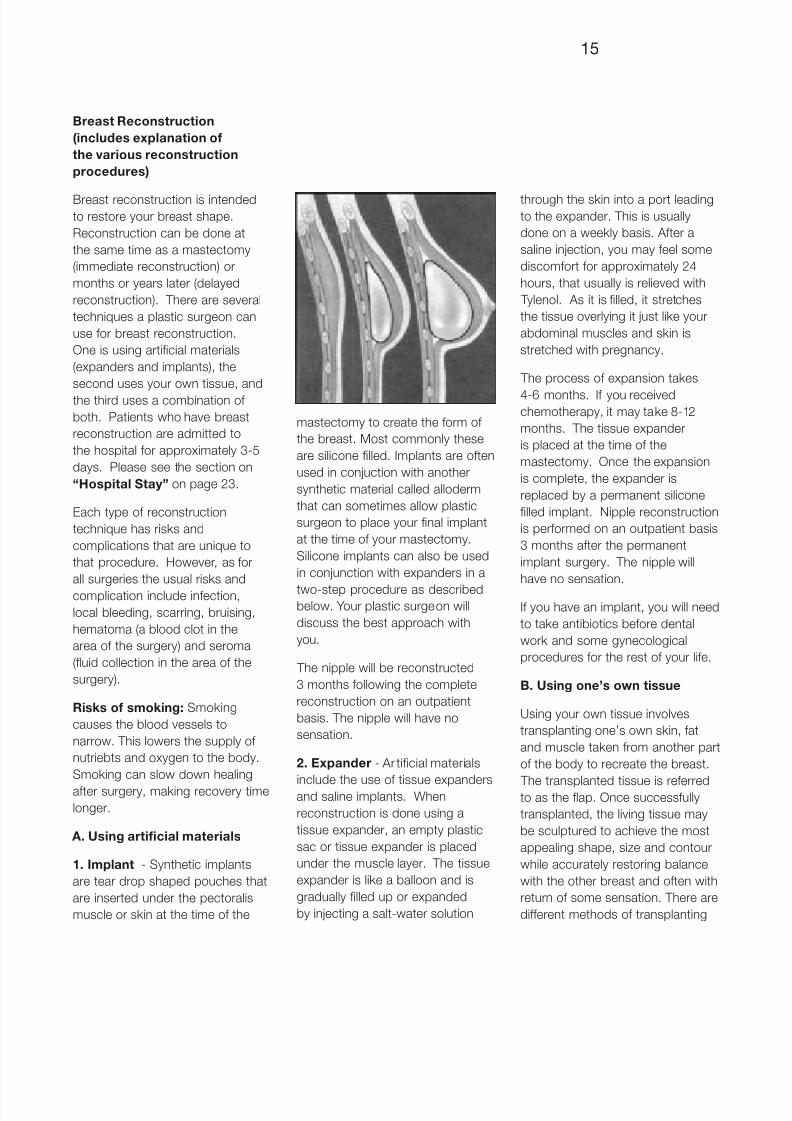
A. Using articial materials
1. Implant - Synthetic implants
are tear drop shaped pouches that
are inserted under the pectoralis
muscle or skin at the time o the
mastectomy to create the orm o
the breast. Most commonly these
are silicone lled. Implants are oten
used in conjuction with another
synthetic material called alloderm
that can sometimes allow plastic
surgeon to place your nal implant
at the time o your mastectomy.
Silicone implants can also be used
in conjunction with expanders in a
two-step procedure as describedbelow. Your plastic surgeon will
discuss the best approach with
you.
The nipple will be reconstructed
3 months ollowing the complete
reconstruction on an outpatient
basis. The nipple will have no
sensation.
2. Expander - Ar ticial materials
include the use o tissue expandersand saline implants. When
reconstruction is done using a
tissue expander, an empty plastic
sac or tissue expander is placed
under the muscle layer. The tissue
expander is like a balloon and is
gradually lled up or expanded
by injecting a salt-water solution
through the skin into a port leadingto the expander. This is usually
done on a weekly basis. Ater a
saline injection, you may eel some
discomort or approximately 24
hours, that usually is relieved with
Tylenol. As it is lled, it stretches
the tissue overlying it just like your
abdominal muscles and skin is
stretched with pregnancy.
The process o expansion takes
4-6 months. I you receivedchemotherapy, it may take 8-12
months. The tissue expander
is placed at the time o the
mastectomy. Once the expansion
is complete, the expander is
replaced by a permanent silicone
lled implant. Nipple reconstruction
is perormed on an outpatient basis
3 months ater the permanent
implant surgery. The nipple will
have no sensation.
I you have an implant, you will need
to take antibiotics beore dental
work and some gynecological
procedures or the rest o your lie.
B. Using one’s own tissue
Using your own tissue involves
transplanting one’s own skin, at
and muscle taken rom another part
o the body to recreate the breast.
The transplanted tissue is reerredto as the fap. Once successully
transplanted, the living tissue may
be sculptured to achieve the most
appealing shape, size and contour
while accurately restoring balance
with the other breast and oten with
return o some sensation. There are
dierent methods o transplanting
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 18/40
16
your own tissue and your body’s size
and medical history help determine
which method is best or you.
1. TRAM Flap -
The TRAM fap tissue is harvested
rom the abdomen using a similar
incision to that used or a “tummy
tuck” procedure. The muscle
can be detached rom its normal
position and brought up to the
chest area to reconstruct a new
breast. There will be a straight-
line incision across your lower
abdomen. The chest will have an
oval shaped incision where the skin
and muscle rom the abdomen are
attached to the skin o the chest.
The TRAM fap is not suitable or
patients who have too much or too
little abdominal at.
Your plastc surgen will urther
explain this procedure to you aswell as determine whether you are
an appropriate candidate.
Please see page 23 or discussion
on pain control and patient
controlled analgesia.
Please see page 21 or discussion
on pain control o constipation.
This surgery can take an additional
3-4 hours ater the mastectomy.
Drains are placed to collect
fuid post-operatively. Nipplereconstruction is perormed on an
outpatient basis 3 months ater the
surgery. The nipple will have no
sensation.
Risks and complications include
poor blood fow to the TRAM
fap and thereore tissue may
partially or entirely die. Patients
who are smokers, have diabetes,
prior abdominal surgery or are
obese may be at a higher risk orcomplications.I this happens,
the dead tissue may need to be
removed surgically. The incision will
still heal normally. This technique
may also cause abdominal wall
weakness that can lead to an
abdominal bulge or hernia. You
may experience unusual sensations
in the abdomen or breast areas,
including numbness. This may
last rom several weeks to several
months or may be permanent.
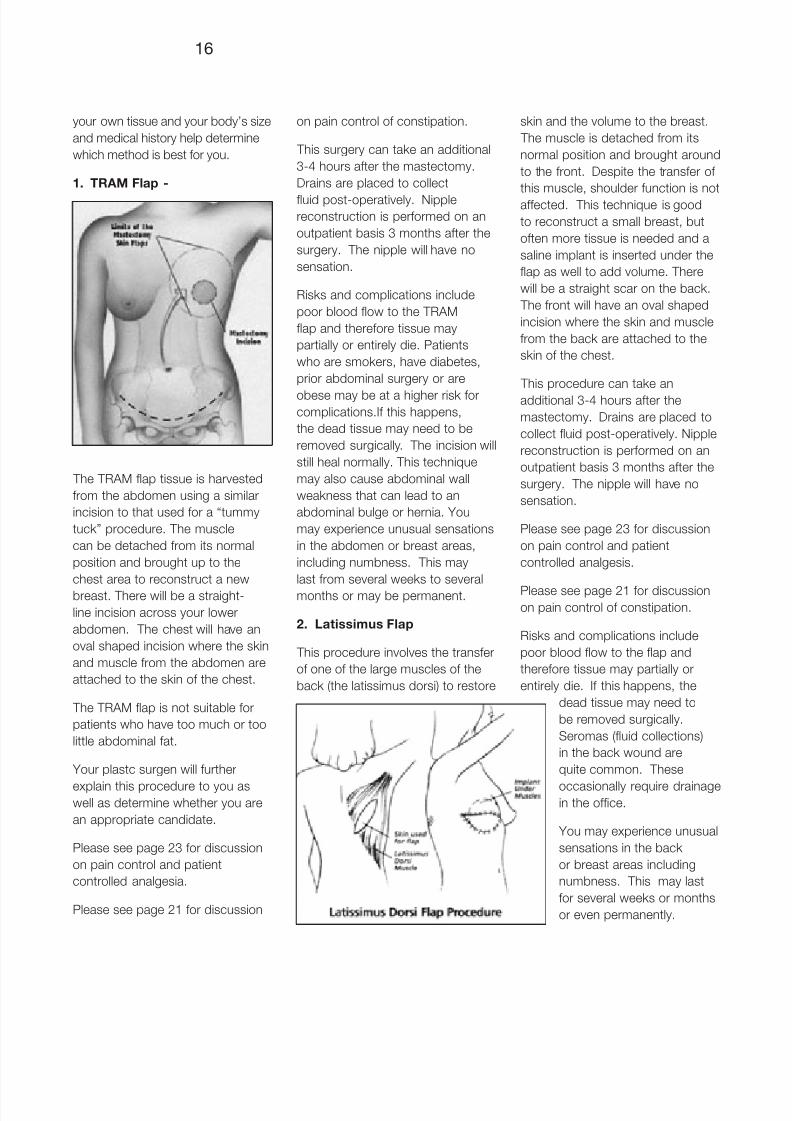
2. Latissimus Flap
This procedure involves the transer
o one o the large muscles o the
back (the latissimus dorsi) to restore
skin and the volume to the breast.
The muscle is detached rom its
normal position and brought around
to the ront. Despite the transer o
this muscle, shoulder unction is not
aected. This technique is good
to reconstruct a small breast, but
oten more tissue is needed and a
saline implant is inserted under the
fap as well to add volume. There
will be a straight scar on the back.
The ront will have an oval shaped
incision where the skin and muscle
rom the back are attached to the
skin o the chest.
This procedure can take an
additional 3-4 hours ater the
mastectomy. Drains are placed to
collect fuid post-operatively. Nipple
reconstruction is perormed on an
outpatient basis 3 months ater the
surgery. The nipple will have no
sensation.
Please see page 23 or discussion
on pain control and patient
controlled analgesis.
Please see page 21 or discussionon pain control o constipation.
Risks and complications include
poor blood fow to the fap and
thereore tissue may partially or
entirely die. I this happens, the
dead tissue may need to
be removed surgically.
Seromas (fuid collections)
in the back wound are
quite common. These
occasionally require drainagein the oce.
You may experience unusual
sensations in the back
or breast areas including
numbness. This may last
or several weeks or months
or even permanently.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 19/40
17
D. Preparing or Surgery
It is important to have all your
questions answered beore surgery
in order to eel condent about
the choices and plan you have
made with your surgeon. Women
are anxious prior to surgery. In
the days beore the surgery, be
sure to do some nice things or
yoursel, eat well, and do whatever
you can to eel as relaxed as
possible. Make sure your work
responsibilities are covered in your
absence, so you can concentrate
ully on your recovery. Women living
alone nd it helpul to have some
meals prepared ahead o time at
home and groceries bought, so that
they won’t have to prepare much
when they get home. I riends
ask how they can be helpul, have
someone suggest to them that they
send over some prepared meals.
Additional Support or Coping
with Breast Cancer
The ollowing will explain the steps
you may need to take in order toprepare or surgery.
Social Work Services
One o the most stressul times in
the breast cancer experience is at
the point o diagnosis. For most
women the diagnosis o breast
cancer comes as a surprise without
advance notice or warning. Most
women do not have a amily history
o breast cancer and do not havea ready-made team o clinicians to
treat their breast cancer. Women
typically eel physically well, which
makes it hard to believe that
anything is actually wrong. In the
absence o complete medical
inormation it’s common to have
one’s mind wander toward worst
case scenarios. During this time o
enormous anxiety, women need
to integrate inormation about a
complicated disease, and make
complex decisions about their own
care. Family and riends mean well,
but are oten themselves distraught
by news o the diagnosis and don’t
always know the right thing to say.
Breast cancer causes distress in
many areas o one’s lie. Women
worry about how they will be able
to continue working, or caring or
their children. Women worry about
side eects rom breast cancer
treatment. Women worry about
their mortality. At the Faulkner
Breast Centre, we are concerned
not only with your physical recovery
rom breast cancer, but also with
your emotional health during breast
cancer treatment. We have, as
part o our proessional team, a
clinical social worker specializing
in counseling women with breast
cancer. The counseling is designed
to provide you with additional
support or coping with the myriad
o stresses caused by the diagnosis
as well as reduce your risk or
anxiety or depression. Some o the
topics covered in counseling can
include:
•decidingbetweentreatment
options
•helpingone’schildrencope
with the diagnosis and
treatment
•managingworkresponsibilities
during breast cancer treatment
•maximizingone’ssupport
system
•interactionofbreastcancer
treatment with other personal
or amily stressors
•psychologicalimpactof
stopping hormone replacement
therapy
• referralstocommunity
resources and supports
•makingconnectionstoother
women who have completed
breast cancer treatment
•howbreastcancertreatment
will interact with a history o
depression or anxiety
• “whydidthishappentome;
what does this diagnosis mean
in my lie?”
Most women begin to eel less
anxiety once some o their
particular issues o concern have
been addressed, and once the ull
details o their diagnosis are known
and a treatment plan is underway.
For more inormation, or to
schedule an individual or amily
appointment please call Janet
Rustow, LICSW at (617)983-7967.
Helping Your Children Cope
with Your Breast Cancer
Diagnosis and Treatment
When diagnosed with breast
cancer, a mother’s most immediate
concern is oten how to help her
children cope with the experience.
While parents generally want
to protect their children rom
dicult and painul situations, theirchildren may actually be imagining
something ar worse than the reality
o the breast cancer diagnosis.
Children rely on their parents
or inormation and or ways o
coping with dicult situations. The
ollowing suggestions are designed

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 20/40
18
to give parents a basic guideline to
begin thinking about how best to
help their children.
Tell Your Children Early on
About Your Breast Cancer
Many children have already picked
up that something is wrong by the
increase o telephone calls and the
anxiety that is present in the home.
Children’s antasies are oten worse
than the reality. Set the example
with them, early on, that you will
give them honest inormation,
answer their questions, and listen to
their concerns. We recommend that
children hear the inormation romtheir parents and that you use the
word cancer. Wait until a time when
you are able to ocus on your child’s
needs. It is ne to take a ew days
to allow yoursel to begin to digest
the news, beore you share it with
your children.
Assure Your Child That You are
Taking Active Steps to Treat
Your Breast Cancer
Children oten eel helpless in their
ability to help in a time o crisis and
need reassurance that you are
working with doctors who have
helpul treatments or your breast
cancer. Let them know what needs
to happen. Children should be told
about the treatments you will be
having, how it will impact the amily
routine, and who will be available to
them when you are busy with your
treatments. Encourage them to askquestions. Answer them truthully. I
you don’t know the answer, assure
them you will nd out and get back
to them. All mothers ear their child
asking whether they are going to
die rom the cancer. Assure them
that the doctors are hopeul about
the treatments they are oering.
The doctors will let you know i
the treatments are not working, in
which case, you will let your childknow.
How Children React
Children will typically react to their
mothers’ breast cancer with ear,
curiosity, sadness and anger. Young
children will be most concerned
with how the illness will eect them.
Even though they cannot ully
comprehend the meaning o the
illness, they should be told aboutit, with age-appropriate language.
Young children are very dependent
upon their parents or their
emotional wellbeing. Try to arrange
or their dad, or avorite baby
sitter inormation or grandparent
to spend extra time with them.
Try to keep routines as normal as
possible. Since children o this
age engage in magical thinking, it
is important to assure them that
they did not cause your cancer,and that cancer is not contagious.
I your child wants to help you, let
them, in age-appropriate ways.
Drawing pictures or you is a great
way or young children to express
emotions.
Older children are typically
concerned about themselves and
their own world. Discuss with them
in more detail how your illness and
treatments will impact their lie. Arrange or avorite other people
to accompany them to activities
in your absence. Adolescents
are keenly worried about body
image and may be embarrassed
or worried about various side
eects o your treatment. Seek
out their specic concerns and
address them. For example, you
may need to assure them that you
won’t arrive at their school without
a wig or scar in place while on
chemotherapy
Notiy Key People in Your
Child’s Lie About Your Breast
Cancer
It is wise to let your child’s
babysitter, teacher or guidance
counselor know about your illness.
They can watch or signs o anxiety
or depression in your child. Let your
child know that you have discussed
your illness with the babysitter,
teacher or counselor. This willprovide your child with someone
during the day that they can talk
to about what is happening in the
amily.
Most children who were coping
well beore their mother was
diagnosed with breast cancer do
not require proessional help to
cope with their mother’s illness.
Do watch or the ollowing signs
and seek proessional help i younotice any o them lasting or more
than a couple o weeks: sleep
or eating disturbance, inability to
concentrate, sudden changes in
school perormance or attendance.
We hope these guidelines are
helpul. They are meant only as
general suggestions. You know
your child best, and are in the best
position to convey the inormation in
a way most helpul to your child.
For more specic inormation, or to
discuss your particular concerns,
please call our clinical social worker,
Janet Rustow, LICSW at (617)
983-7967.
Pre Admission Testing (PAT)

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 21/40
19
clinic appointment /
At the same time your surgeon’s
oce sta schedules the surgery,
a vist to PAT (Pre Admission
Testing) will be scheduled. Thisis a separate appointment rom
your pre operative physical by your
primary care physican. During this
time, you will meet with a member
o the anesthesiology sta who
will evaluate you and answer any
questions you have concerning
anesthesia. You will also meet
with a day surgery registered nurse
who will explain specically what to
expect during your hospital stay.
Pre-Operative (Pre-op) physical
examination appointment
A pre-op physical exam must be
completed beore surgery to ensure
that you have no health --problems
that may put you at risk or surgery
and anesthesia. Should you have
health problems, both your Primary
Care Physician (PCP) and surgeon
will coordinate a treatment plan
to minimize your surgical risk.
The pre-op physical exam can be
completed by your PCP or at the
Faulkner Hospital. The oce sta
at your surgeon’s oce who books
the surgery will help you plan or the
pre-op.
Two weeks prior to surgery
Be sure to inorm the anesthesiology sta o any medication you are taking and whether you
smoke and your previous anesthesia experience.
I you have any questions about your medications and surgery, you may call anesthesia
at Faulkner Hospital at 617-983-7179.
•PleasediscontinueVitaminE
and any herbal supplements.
•Pleasediscontinueanydiet
drugs (notiy your physician)
•Pleasedonottakeaspirinfor
10 to 14 days prior to your
scheduled surgery. I you take
aspirin daily, please notiy us
and check with your doctor
beore stopping.
Seven (7) to ten (10) days beore
surgery
Do not take any non-steroidal
anti-infammatory drugs such as
ibuproen (Motrin, Advil, Aleve,
Naprosyn, Relaen, etc) or 7 to10 days prior to surgery. Tylenol is
okay to take.
One week beore surgery
•PleasediscontinuePlavixafter
checking with your physician.
The day beore surgery
On the last business day beore
your surgery you must contact the
Day Surgery Unit at (617) 983-7179
between 9 a.m. - 3 p.m. to conrm
your time o arrival.
•Do not eat or drink
(including water, ice,
vitamins, hard candy, gum,
etc.) ater midnight on the
night beore your operation.
•Removenailpolish
•Removeall jewelry including
rings
•Removecontactlenses
•Leavevaluables(checkbook,
credit cards, etc.) at home
•Arrangetohavesomeonedrive
you home once your are ready
to be discharged.
•Arrangeforsomeonetobeat
home with you during the rst
24 hours ater surgery
•Youmaybrushyourteeththe
morning o surgery
• Ifyouareinstructedtotakesome o your medication on the
morning o your surgery, pleasetake with just a sip o water
•Bringyourasthmainhalerswith
you
• Ifyouhavediabetes,donot
take insulin or diabetic pills
The hospital sta will make
every eort to saeguard your
possessions while you are a patient.
Our ocus is on the important
essentials or daily living such as
eyeglasses, dentures, and hearingaids.
Please consult with your doctor to determine the best plan or you.
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 22/40
20
The day o surgery
On the day o surgery, go directly
to the Day Surgery PreOp unit on
the rst foor. Plan to arrive at the
designated time.
Ater checking in at Day Surgery,
you will remain in the waiting room
where your amily and riends can
join you. I you are scheduled or a
wire-localization or sentinel lymph
node biopsy, the nurse will direct
you to the Sago Centre in the
Belkin House on the ourth (4th)
foor. Once the radiologist has
placed the wire, you will return to
the day surgery unit.
The nurse will ask you to change
your clothes and she/he will meet
with you to prepare you or surgery.
At this time, the nurse will answer
any questions or address any
concerns you may have.
Next, the nurse will escort you to
the anesthesia holding area where
a member o the anesthesia team
will place an intravenous (I.V.) linein your arm. Your surgeon will also
visit you briefy. You may bring
along a book or portable cassette/
cd player with headphones to help
pass the time.
A nurse anesthetist will then take
you by stretcher to the Operating
Room. During your operation, anurse anesthetist continuously
monitors your heart rhythm, blood
pressure, breathing and oxygen
saturation (eectiveness o oxygen
delivery to the tissues o the body).
Immediately ollowing surgery
Ater surgery, the sta will transport
you to the Post Anesthesia Care
Unit (PACU or Recovery Room),
where you will remain until youare ully awake. Your vital signs
(blood pressure and heart rate) will
be monitored and the ollowing
medical devices may be used:
• Oxygen mask
• Heart Monitor
• Automatic blood pressure
cu
• Small device on your nger
to monitor blood oxygen
levels
Recovery time varies by individual,
but the average stay in the PACU is
typically between 1 and 2 hours.
With a breast biopsy or partial
mastectomy, you may have a
bandage on your chest, which you
can remove 24 hours ater surgery,
or you may have a clear dressing
which will wear o in a couple
weeks. Do not try to remove
it. Under the bandage there are
multiple steri-strips (narrow, one
inch long adhesive strips) across
the incision. These strips will all o
on their own about 7-10 days ater
surgery. The nursing sta will give
you instructions on how to care or
the incision at home. It may help to
place a pillow under seat belt or
the ride home.
Only patients who had a
mastectomy, with or without breast
reconstruction, will be admitted
to the hospital. Please see the
inormation on “Hospital Stay”,
on page 23. All other patients go
home as soon as they eel ready
to go. Please see “Day Surgery”
section on page 21.
This section will explain what you
can expect once you are home.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 23/40
21
E. Day Surgery
This section will explain what you
can expect once you are home.
Recovery process
You will receive pain medication
in the PACU. Your surgeon will
give you a prescription or pain
medication or at home, especially
the rst night. You may experience
pain or discomort in the area o
the incision as well as tiredness
rom the general anesthesia. The
tiredness may last a ew days.
Constipation can occur rom
anesthesea or pain medicinecontaining a narcotic. Do not avoid
pain medication because o risk o
constipation. Constipation can be
prevented / minimized by:
•adequateuidintake
•earlyambulationastolerated
•useofstoolsoftnerorlaxative
while taking pain medication
containing narcotics.
Recovering rom surgery is an
emotional process as well as a
physical one. Not only will you be
tired rom the anesthesia, you will
need time to catch up emotionally
with all that has happened
physically. Don’t rush yoursel.
You may wish to begin preparing
yoursel or the next phase o
treatment by reading or by talking
to other women who have been
through the experience.
Dressing Care
The surgeon will cover your incision
with a dressing, or a clear liquidbandaid sometimes with an elastic
(ace) bandage wrapped around
it. You will be discharged with the
dressing in place, please note the
ollowing (the nurse will review all o
this with you beore you go home):
•Removethedressing24hours
ater surgery, you may then
shower
•Gentlywashtheincisionarea
and pat dry•Iftheincisioniscoveredwith
strips o tape (steri strips) they
should remain in place until
they loosen on their own (may
take as long as 7 to 10 days.) or
are removed by your surgeon
Signs and symptoms o
inection:
Please contact your doctor’s oce
i you note the ollowing:
•Elevatedtemperature
•Increasedrednessaroundthe
incision
•Foulsmellingdrainagefrom
incision
For patients who also had an
axillary node dissection or sentinel
lymph node biopsy, have a
simliar bandage as your breast
incision. Please ollow the same
guidelines or incision care and
inection monitoring as or the
breast incision. It is not unusual
to have decreased sensation or
numbness in the armpit and along
the back portion o your upper
arm. This may last or weeks or
months and in some instances
may be permanent. You may also
experience a eeling o “pulling”
under your arm and have some
restriction in the use o your arm
initially ater surgery.
Pathology Results
The pathology report outlines the
results o the examination o the
breast tissue and/or lymph nodes.
Your surgeon will ollow up with
you by phone to inorm you o
the pathology results as soon as
they are available. At that time the
surgeon will review the results with
you as well as discuss any urther
consults you may need.
Important components o the
pathology report include:
•whetherthemarginsoredges
o the tissue are “clean” (ree
o cancer cells) or “dirty” (have
cancer cells present) - dirty
margins usually indicate the
need or a re-excision to
remove the remaining cancer
cells
•whetherestrogen-receptors
DO wear a bra at all times or support ater a partial mastectomy (or re-excision) or 48 hours
or more and then while you are awake or at least three weeks
You may use an ice pack or relie o moderate pain or swelling. Apply to incision intermittently
(Twenty minutes on / twenty minutes o.)

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 24/40
22
are present - i estrogen
receptors are present itindicates that the breast cancer
is sensitive to hormones and
may respond to hormonal
treatment.
•ifyouhadanaxillarynode
dissection, whether there
are any breast cancer cells
in the lymph nodes - i the
lymph nodes contain tumor
cells urther treatment
may be indicated, such as
chemotherapy or hormonetherapy
Post-operative exam
You will need to make a post-
operative appointment with your
surgeon or a post-operative check.
Your surgeon will inorm you about
scheduling this appointment.
Please review the inormation on “ Arm Exercises” on page 27.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 25/40
23
F. Hospital Stay
This section is or patients who
are admitted to the hospital and
explains the services and care
patients receive while in the
hospital. The rooms are located
on the 7th foor and all are private.
Visiting hours are rom 12 pm to 8
pm daily. Family may visit but rest
is important and it is wise not to
overexert onesel.
Patients who had a mastectomy
stay overnight in the hospital.
Patients who also had breast
reconstruction will stay in the
hospital or 3-5 days.
I you had a TRAM Flap
reconstruction you will have an
abdominal incision as well as the
breast incision. With a Latissimus
Flap reconstruction you will have an
incision on your back to the side o
the scapula as well as the breast
incision.
Patient Care
Your surgeon will stop by and
check on you daily. I you had
breast reconstruction your plastic
surgeon will also come in to check
on you. In addition to the surgeon
monitoring your care, a team o
residents, physician assistants and
foor nurses will do the same. We
encourage you to ask questions
you may have or the health care
team.
You will eel drowsy or a ew hours
ater arriving in your room. Your
incision will be bandaged and
you will have one or more drains
in place as well as oxygen and
Venodyne Boots. Venodyne Boots
are special compression wraps
which are applied to your legs to
help maintain good circulation to
avoid blood clots rom orming in
your legs. These gently squeeze
and release your legs in the cal,
knee and thigh areas. They will be
removed once you are out o bed
and walking. You may also have a
Foley catheter in place and an IV or
fuids.
A nurse or nursing assistant will
help you get out o bed or the
rst time and activity is increased
gradually. Once the Foley catheter
is removed, a nurse or assistant
will help you go to the bathroom.Moving helps to increase your
strength and is good or your
circulation.
Once your bowel unctions have
returned you are ready to eat.
You will start with clear liquids
and advance to regular ood, as
you are able to tolerate this. This
usually occurs over one to two days
ollowing surgery. For patients who
had TRAM Flap reconstruction, bowel unction takes longer to
return.
For patients who had breast
reconstruction the nurse will visit
requently to check the skin fap or
adequate blood fow by checking
the skin’s color and temperature.
Your room temperature will be kept
warm to acilitate optimal blood
fow.
For patients who did not have
breast reconstruction, your doctor
will order a consult or you to be
tted or a prosthesis and special
bra. In the initial post-op period,
you will receive a temporary orm.
When your incision has healed,
you can then be tted with the
permanent prosthesis and surgical
bras.
Pain Control
When you rst awaken, you may
have some discomort over your
chest and under your arm i you
also had lymph node surgery.
Many women describe the pain
as moderate although you may
eel more or less discomort
depending on your procedure and
your individual sensitivity to pain
(everyone is dierent.)
Various methods o pain control
are available. You may receive
injections o pain medicine or a
Patient Controlled Analgesia
(PCA) pump. The pump
administers intravenous medication
that you control. The nurse will
instruct you on how to use the
pump to administer a dose by
pushing a button. Use o this
device allows a steady level o
pain medication to remain in thebloodstream.
• You cannot overdose! The
pump has been preset to
deliver only certain amounts o
medication; you cannot receive
more than is programmed.
• Do not feel the need to
tolerate pain! You must
have adequate pain control,
particularly early in the post-
operative period, in order
to actively participate in the
recuperative process.
See constipation inormation page
21.
Eventually, your pain medication will
be changed to the oral orm (pills) in
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 26/40
24
anticipation o your discharge rom
the hospital.
Prevention o post-operative
pneumonia
Pain control ater surgery is
important not only or your comort
but also to ensure you maintain
adequate breathing and to allow
you to actively participate in your
physical therapy. As is the case
ater any type o surgery, deep
breathing, coughing and using an
incentive spirometer are important
or preventing post-operative
pneumonia. Being out o bed
and walking, as you are able,are also preventive measures or
pneumonia.
The nurse will show you how to
use an incentive spirometer and
help you practice the breathing
exercises. The spirometer is a
clear plastic tube with a ball inside
and the tube is attached to a
mouthpiece. As you take a deep
breath IN, the plastic ball should
rise to the top. This ensures youare taking deep breaths to prevent
respiratory congestion and ever.
Dressing Care
The surgeon will cover your incision
with a dressing, or liquid bandaid,
or with an elastic (ace) bandage
wrapped around it. The surgeon or
physician assistant will remove the
dressing on the rst or second day
ater surgery. Your incision may be
covered with strips o tape (steri-
strips) or xeroorm gauze. The steri
strips should remain in place until
they are removed by your surgeon
or until they loosen on their own.
(May take as long as 7 to 10 days.)
Drains and Drain management
You will have one or more drains
(also called Jackson-Pratt or
JP drain ) placed during surgery
to help drain fuid and blood rom
around the surgical site. Drainage
and/or bleeding into the drain is
normal and expected or the rstseveral days ater surgery. The
nurses will check your drains and
empty them. Each shit the nurse
will document the amount o fuid
in the drain(s). I the drain(s) is/are
ready to come out beore you are
discharged rom the hospital, the
surgeon or physician assistant will
remove them.
Should you go home with drains
in place please ollow theseinstructions (the nurse will review
them with you beore you leave the
hospital):
•Keeptheincisiondryuntilyour
drain is removed.
•Pinthetabonthebulbtoyour
clothing to prevent pulling or
put drain bulb in camisole
pocket.
•“Strip”or“milk”theJ.P.tube
to release any clotty threads
that may accumulate along theinside o the JP drains. This
will help keep the tube rom
clogging.
•Keeptrackoftheamountof
fuid in the drain. Once the
fuid is less than 30 cc’s over
24 hrs per drain, call your
surgeon’s oce to schedule an
appointment to have the drain
removed. It is advisable to take
a pain pill one hour beore thedrain is removed.
•Toemptythedrain:
- wash your hands, wear
gloves
- open the top o the bulb and
empty contents into reuse
container
- compress sides o bulb and
close top
- measure fuid and record
under appropriate drainnumber
•Donotputanythingintodrain
bulb - only empty it. Empty
twice daily.
In order to make the monitoring
process easier; the nurse will give
you a orm to take home, so you
can write down the fuid measures.
See example.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 27/40
25
I your drain loses suction open the top, compress the sides o the bulb and replace the top.
Call your doctors oce to schedule appointment or drain removal when amount is less
than 3Occ or ml’s in 24 hours per drain. You need to empty your drains twice a day.
How to record your output:
– EXAMPLE –
Date Time Drain #1 Drain #2 Drain #3
Drain #4
1/1 8 AM 10 15 20 30
1/1 2 PM 15 8 16 7
1/1 10 PM 8 5 6 10
1/1 24 HR TOTAL____________________________________________________________
33 28 42 47
DATE TIME DRAIN #1 DRAIN #2 DRAIN #3 DRAIN #4
•Forpatientswhohadbreast
reconstruction, please call your
plastic surgeon to have the
drain removed.
•Ifyouhaveadressingover
the drain site, it will need to
be changed daily. Wash your
hands ater careully removing
the existing dressing. Place
the new dressing over the drain
site. I you have someone to
help you, have him or her apply
the tape while you hold the
dressing in place. Use only a
small strip o paper tape. Avoid
placing the tape on the incision.I you are doing this alone, tear
the piece o tape rst, then hold
the dressing with one hand
over your drain site and apply
the tape with your other hand.
•Onceyourdrainhasbeen
removed you will only need a
dressing over the site or one
day in case o any drainage
rom the drain site. Shower
24 hours ater last drain is
removed.
Signs and symptoms o
inection:
Please contact your doctor’s oce
i you note the ollowing:
•Elevatedtemperature
•Increasedrednessaroundthe
incision or drain site
•Foulsmellingdrainagefrom
incision or drain site
Pathology Results
A pathology report is a report on
the examination o the breast tissue
and/or lymph nodes. The surgeon
will ollow up with you to inorm you
o the pathology results as soon
as they are available. This may be
while you are still in the hospital
or by telephone. At that time the
surgeon will review the results with
DO NOT shower, shave underarms, use deodorant, or powder on this area until the drain is removed,
unless otherwise instructed by your surgeon.
DO resume the above activities ater the drain is removed as instructed by your surgeon.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 28/40
26
you as well as discuss any urther
consults you may need. You will
then schedule a ollow up vist with
the breast surgeon.
Important components o thepathology report include:
•whetherthemarginsoredges
o the tissue removed are ree
o cancer cells or have cancer
cells present.
•whetherestrogen-receptorsare
present - i estrogen receptors
are present it indicates that the
breast cancer is sensitive to
hormones and may respond to
hormonal treatment•ifyoualsohadanaxillarylymph
node dissection or sentinel
lymph node biopsy, whether
there are any breast cancer
cells in the lymph nodes
Recovery Process
It is important to take requent rests
during the day and not to “overdo”
it. It can take several weeks to
get back to your previous level o activity. Recovering rom surgery is
an emotional process as well as a
physical one. Not only will you be
tired rom the anesthesia, you will
need time to catch up emotionally
with all that has happened
physically. Don’t rush yoursel.
You might wish to begin preparing
yoursel or the next phase o
treatment by reading or talking
to other women who have been
through the experience.
For lumpectomies or lymph node
surgery, there is a chance o blood
or fuid collecting under the skin
(seroma) that can cause swelling
and discomort. To ease the
discomort, apply ice to the area.
Call the surgeon’s oce i the area
continues to swell and cause pain.
It may need to be aspirated (remove
fuid with a needle and syringe)
at the doctor’s oce. This is not
painul since the area is usually still
numb. I the fuid re-accumulates,
the aspiration may be repeated.
Vigorous movement or activity o
the aected arm may increase the
chance o developing a seroma or
worsen an existing one.
Additional Post Operative
Instructions:
Mastectomy withreconstruction:
•Youwillneedapostoperative
appointment with your plastic
surgeon and your breast
surgeon.
•Donotsleeponyourstomach
or on the operative side.
•Yourplasticsurgeonwillinstruct
you about wearing a bra.
•DoNotliftanythingheavier
than 5-10 lbs or 6-8 weeks.
Mastectomy without
reconstruction:
•Youwillneedapostoperative
appointment with your surgeon.
•Prosthesis-youmayweara
camisole with insert ollowing
your surgery. Ater your drains
are removed you may wear
a sot bra with insert. In one
month you may be tted ora permanent prosthesis. A
representative rom a supply
company may visit you in the
hospital and provide you with
a camisole. A list o prosthesis
providers is also on page 43,
these products are covered by
your insurance.
•Yoursticheswilldissolve.
•DoNotliftanythingheavier
than 5-10 lbs or 4 weeks.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 29/40
27
G. Arm exercises ater an Axillary Lymph Node Dissection and/or a Mastectomy
The ollowing are general Range o Motion exercises to help you increase your arm motion. Please check with
your doctor beore attempting. Do the exercises slowly. Aim or gentle stretching. Remember not to hold your
breath while exercising. You might want to exercise ater your muscles are relaxed rom a warm shower, or 45
minutes ater pain medication. Try to do each exercise 5-10 times, 2-3 times per day
Beginning Exercises
A series - WEEK 1
I you had an axillary node dissection, start 2 days ater surgery. I you had a mastectomy , start 1 day ater the
drains are removed. I you had breast reconstruction, check with the plastic surgeon.
B Series - Week 2
Advanced Exercises
Add these exercises as follows:
For axillary node dissection,
1 week ater surgery. For
mastectomy 1 week ater
drains are removed.
Standing rmly
with eet slightly
apart, rotate trunk
while swinging arm
behind.
Elbow bent at right
angle and held
against trunk, slide
arm on table surace
in an inward arc.
Seated with elbow
bent and held against
side, slide arm in an
arc, outward with table
surace or support.
Holding arms with
hands under elbows,
move side to side as
i rocking a baby.
Lit arm out to side, elbow
straight, palm downward.
Do not shrug shoulders or
hit trunk.
With elbow straight use
ngers to “crawl” up a
wall or door rame as
ar as possible
Graphics source: Visual Health
Inormation

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 30/40
28
Advanced Exercises
Do the exerises slowly. Aim or gentle stretching. Remember not to hold your breathe while exercising. Try to do
each exercise 5-10 times, 2-3 times a day. Call your surgeon’s oce i you have any questions or concerns about
the exercises, or your progress.
For axillary node dissection, start 2 days ater surgery and you have mastered the beginning exercises. For
mastectomy , start 2 weeks ater the drains are removed and you mastered the beginning exercises.
WEEK 3
Bring arm across
ront to opposite
side.
Gently pull on elbow
with opposite hand
until a stretch is elt in
the shoulder.
Maintaining erect
posture, draw
shoulders back while
bringing elbows back
and inward. Return to
starting position.
Raise arm to point
to ceiling, keeping
elbows straight
With ngers clasped
relaxed at sides. Roll
shoulders continuously in
backward direction. This
exercise can also be done
one shoulder at a time.
With elbow straight use
behind head, pull elbows
back while pinching
shoulder blades together.
Stand straight with arms
ngers to “crawl” up a
wall or door rame as
ar as possible

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 31/40
29
Important Do’s and Don’ts
or patients who had an
axillary lymph node surgery.
Inormation ollowing axillary lymph
node surgery:
1. Start exercises as instructed;
do not exceed exercise times
and amounts. Your surgeon
will instruct you on weight
limitations.
2. You may use an electric razor
on the aected side one week
ater surgery.
3. Do not use powder or
deodorant or one week
ollowing surgery. When
showering, use soap and water.
Dry gently.
4. Maintain arm precaution (see
page 10) indenitely.
5. Use moisturizer on hands.
6. Call your surgeon/NP with any
questions or concerns you mayhave.
7. Call immediately i you notice
swelling or redness on the
aected arm.
Note that you may experience
swelling o the hand or arm (please
see risk and complications or
“axillary lymph node dissection”
on page 11). This may occur
immediately ater surgery, or yearslater. I you note any swelling o your
hand or arm, contact your surgeon
and you will receive appropriate
instructions.
It is important to watch out or and
prevent inections on the aected
arm. You should avoid cuts,
scratches, irritations and burns
as much as possible by doingthe ollowing; use insect repellent
and protective sunscreen, wear
gloves or washing dishes and
using cleaners, wear gloves or
gardening, wear padded gloves or
reaching into a hot oven, use an
electric razor or underarm shaving,
and do not cut your cuticles. Keep
your skin sot and ree o cracks
with a moisturizing lotion.
In addition, avoid tight jewelryor clothing on the aected arm,
carry your purse on the opposite
shoulder, avoid blood draws,
injections, IV’s and blood pressures
on the aected side.
8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 32/40
30
F. Frequently Asked
Questions
1. How long is the recovery
period ater surgery?
Approximately 2 days or a
biopsy or duct excision, 2
weeks or partial mastectomy
and sentinel lymph node
biopsy, 2-3 weeks or partial
mastectomy and axillary node
dissection and 3-4 weeks or
mastectomy. Mastectomy with
breast reconstruction can have
a 4-6 week recovery period. I
complications occur, recovery
may be longer.
2. Do you have a drain in ater
a partial mastectomy? I
you have a drain, how long
does it stay in?
Usually a drain is not placed
or a partial mastectomy .
Some surgeons place drains
ater axillary dissections.
Mastectomy with or without
breast reconstruction will
always have drains. Over the
course o several postoperative
days, the amount o drainage
will decrease and the drains
can be removed. I the drain is
not ready to be removed, you
will go home with the drain.
You will be taught how to take
care o the drain and measure
the drainage. A visiting nurse
will visit you daily to check on
you. The drain will be removed
at the surgeon’s oce.
3. Are there stitches to be
removed?
Most surgeons use absorbable
stitches on the inside and these
do not need to be removed.
On the outside you will see
liquid bandaid or steri-strips
across the incision. Steri-
strips are small pieces o white
adhesive tape which stay in
place or 7-10 days, when they
usually all o. Your surgeon
may remove them at your post-
op visit.
4. Will I experience pain ater
the surgery?
You may experience
postoperative pain at the
incision area (breast, chest,
abdomen or back) and/or
your upper arm or under the
arm. I you are in the hospital,
you will receive pain medicine
intravenously or by injection
initially, and then orally with
pain pills, once you are able to
tolerate a diet. I you have day
surgery, your surgeon will give
you a prescription or a pain pill.
5. Is the surgery “ day
surgery” or do I stay in
the hospital? I I stay in
the hospital, how long do I
stay?
Biopsy, duct excision, partial
mastectomy and axillary
lymph node dissections or
sentinel lymph node biopsy are
day surgery and you will be
discharged rom the recovery
room once you are ully awake
and recovered rom the eects
o anesthesia. I you have a
mastectomy , you will be in
the hospital approximately 1
day. I you also have breast
reconstruction, you will be in
the hospital or 3-5 days.
6. Where will the incision(s)
be?
Incisions will be made on your
breast or a partial mastectomy,
under your arm or an axillary
lymph node dissection, on
your chest or mastectomy and
additional incisions on your
abdomen or back or breast
reconstruction.
7. When can I take a shower?
Following a partial mastectomy
and/or axillary lymph node
dissection or sentinel lymph
node biopsy , you can shower
approximately 24 hours ater
the surgery when the bandage
is removed. I you have had
a mastectomy with or without
breast reconstruction, you
cannot shower until ater
the last J.P. drain has been
removed.
8. Can you travel by plane i
you have an implant?
Yes, it is sae to fy with an
implant.
9. When can I resume sexual
activity?
The general rule is that you may
resume sex when you eel able
and your wound has healed. I you have had reconstruction,
avoid activities that will make
you sweaty, red in the ace
or out o breath or the rst
ew weeks ater surgery. It is

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 33/40
31
important or you to remember
that your sensation in the
reconstructed breast will be
decreased or absent. Check
with your individual surgeon or
urther inormation.
10. How soon can I start
driving again?
For same day surgery patients
you can drive again 24 hours
ater the procedure i you are
not taking prescription pain
medication and are able to
move your arm easily.
For mastectomy patients youcan drive again 24 hours ater
discharge rom the hospital i
you are not taking prescription pain
medication and are able to move
your arm easily.
It is best to drive only short distances
at rst and gradually increase your
driving time over a ew days.
I you had breast reconstruction,
please check with the plasticsurgeon beore driving.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 34/40
32
I. Glossary
Adjuvant therapy (AD-ju-vant):
Treatment given in addition to
the primary treatment.
Areola (a-REE-oe-la)): The
area o dark-colored skin that
surrounds the nipple.
Aspiration (asp-er-AY-shun):
Removal o fuid rom a lump,
oten a cyst or post operative
fuid (a seroma), with a needle.
Atypical hyperplasia (hy-
per-PLAY-zha): A benign
(non-cancerous) condition
in which breast tissue has
certain abnormal eatures. This
condition increases the risk o
breast cancer.
Axilla (ak-SIL-a): The underarm
(armpit).
Benign (bee-NINE): Not
cancerous; does not invade
nearby tissue or spread to other
parts o the body.
Biopsy (BY-op-see): The removal
o a sample o tissue, which
is then examined under a
microscope to check or cancer
cells. Excisional biopsy is
surgery to remove an entire
lump. Incisional biopsy, is
when the surgeon removes part
o the tumor. Removal o tissue
with a needle is called a needle
biopsy.
Bone Scan: A nuclear medicine
scan to assess whether the
breast cancer has spread
(metastasized) to the bones
Cancer: A term or more
than 100 diseases in which
abnormal cells divide without
control.
Carcinoma (kar-sin-OE-ma):
Cancer that begins in the lining
or covering o an organ.
Carcinoma in situ (kar-sin-
OE-ma in SY-too): Cancer that
involves only the tissue in which
it began; it has not invaded
other tissues.
Chemotherapy (kee-moe-
THER-a-pee): Sometimes
chemotherapy is used in
addition to surgery and
radiation therapy. Chemo
therapy involves using drugs
to destroy cancer cells by
stopping them rom growing
or multiplying at one or more
points in the cell’s lie cycle.
Chemotherapy may oten
consist o more than one drug.
How oten and or how long
you will get chemotherapy
depends on the kind o cancer
you have. Depending on
the type o cancer you have
the chemotherapy may be
administered intravenously,
by mouth or into the muscle.
I you are a candidate or
chemotherapy, your surgeon
will reer you to a medical
oncologist or a discussion
o the dierent types o chemotherapy.
Clinical trials: Research studies
that involve patients. Each
study is designed to answer
scientic questions and to nd
better ways to prevent or treat
cancer. Your decision about
participating in a clinical trialdoes not aect your care.
Core Biopsy: Removal o a
portion o the breast lump
or abnormality seen on
mammogram or ultrasound
using local anesthesia and a
special core biopsy instrument
Cyst (sist): A closed sac or
capsule lled with fuid.
Duct: A tube in the breast
through which milk passes
rom the lobules to the nipple.
Cancer that begins in a duct is
called ductal carcinoma.
Ductal carcinoma in situ:
involves only the ducts and has
not spread to other tissue.
Estrogen (ES-troe-jin): A emale
hormone.
Estrogen Receptor: A binding
site on tumor cells or estrogen.
This can be measured in breast
cancer cells
Estrogen receptor test: A
test to measure the amount
o certain proteins, called
hormone receptors, in breast
cancer tissue. Hormones can
attach to these proteins.
Hematoma (hem-a-to-ma):
collection o bloody fuid which
may accumulate in areas where
tissue was removed.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 35/40
33
Her-2: A tumor marker that can
be measured in breast cancer
cells.
Hormones: Chemicals produced
by glands in the body.Hormones control the actions
o certain cells or organs.
Hormone therapy: Treatment o
cancer by removing, blocking,
or adding hormones.
Jackson-Pratt (J.P.) Drain :
A device which drains and
collects fuid rom the incisional
area.
Lobe: A part o the breast; each
breast contains 15-20 lobes.
Lobular carcinoma in situ:
involves only the lobules o the
breast and has not spread to
other tissues.
Lobule (LOB-yool): A subdivision
o the lobes o the breast.
Cancer that begins in a lobule
is called lobular carcinoma.
Local therapy: Treatment that
aects cells in the tumor and
the area close to it. (i.e. the
breast and adjoining lymph
nodes)
Lumpectomy (lump-EK-toe-
mee): Surgery to remove only
the cancerous breast lump;
and margin o normal tissue ,
usually ollowed by radiation
therapy. Also reerred to aspartial mastectomy.
Lymph (lim): The almost
colorless fuid that travels
through the lymphatic system
and carries cells that help ght
inection and disease.
Lymph nodes: Small, bean-
shaped organs located along
the channels o the lymphatic
system. Bacteria pr cancer cells
that enter the lymphatic system
may be ound in the nodes.
Also called lymph glands.
Lymphatic system (lim-FAT-
ik): The tissue and organs
(including the bone marrow,
spleen, thymus, and lymph
nodes) that produce and store
cells that ght inection and
disease. The channels that
carry lymph also are part o this
system.
Lymphedema (lim-a-DEE-ma):
Swelling o the hand and arm
caused by extra fuid that may
collect in tissue when underarm
lymph nodes are removed or
blocked.
Malignant (ma-LIG-nant):
Cancerous; can spread to other
parts o the body.
Mammogram (MAM-o-gram): An x-ray o the breast.
Mammography (mam-OG-ra-
ee): The use o x-rays to create
a picture o the breast.
Mastectomy (mas-TEK-to-
mee): Surgery to remove the
breast. Modied Radical
(MRM) Mastectomy includes
removal o lymph nodes. Total
Mastectomy does not include
removal o lymph nodes.
Menopause: The time o a
woman's lie when menstrual
periods stop; also called
"changing o lie."
Metastasis (meh-TAS-ta-
sis): The spread o cancer
rom one part o the body to
another. Cells in the metastatic
(secondary) tumor are like
those in the original (primary)
tumor.
Microcalcications (MY-
krow-kal-si--KA-shunz):
Tiny deposits o calcium in
the breast that cannot be
elt but can be detected on
a mammogram. A cluster o
these very small slecks o
calcium may indicate that
cancer is present.
Milking & Stripping: technique
or releasing clotty threadsthat may accumulate along the
inside o the J.P. Drain.
MRI: A type o breast imaging
that is done with the use o a
large magnet. No radiation is
used.
PACU: Past Anesthesia
Care Unit, the unit you are
transported to right ater your
surgery.
Palpation (pal-PAY-shun): A
simple technique in which a
doctor presses on the surace
o the body to eel the organs
or tissues underneath.
Partial Mastectomy: Partial
mastectomy is surgery to
remove the abnormal tissue
or lump and a margin o
normal tissue surrounding the
abnormal area; is also reerred
to as lumpectomy.
Pathologist (path-OL-o-jist): A
doctor who identies disease
by studying cells and tissues
under a microscope.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 36/40
34
Progesterone (proe-JES-ter-
own): A emale hormone.
Prognosis (prog-NOE-sis): The
probable outcome or course
o a disease; the chance o recovery.
Prosthesis (pros-THEE-sis):
An articial replacement o
a part o the body. A breast
prosthesis is a breast orm
worn under clothing.
Radiation therapy (ray-dee-
AY-shun): Sometimes radiation
therapy is used in addition to
surgery. Radiation therapyconsists o X-ray treatments to
the tumor containing area in
the breast. The X-rays can kill
the tumor cells or keep them
rom growing and dividing.
The treatments involve
positioning you in a radiation
therapy machine to receive the
treatments. Small tattoos are
placed on your skin to allow
exact positioning o the X-rays.
The treatments are given on anoutpatient basis 5 times a week
or 6.5 weeks, 5 weeks are or
total breast irradiation and 1.5
weeks o a boost (extra dose)
to the tumor area.
Remission: Disappearance o
the signs and symptoms o
cancer. When this happens,
the disease is said to be “in
remission.” A remission can be
temporary or permanent.
Risk actor: Something that
increases a person’s chance o
developing a disease.
Sentinel Lymph Node: First
lymph node or nodes to receive
drainage rom the area o the
tumor
Seroma: collection o bodily
fuid which may accumulate
postoperatively in area where
tissue was removed.
Stage: The extent o the cancer.
The stage o breast cancer
depends on the size o the
cancer and whether it has
spread rom its original site to
lymph nodes and/or distant
sites.
Staging: Staging is a term
used to describe those tests
we do on all patients with
a new diagnosis o breast
cancer to determine i there
are any obvious signs o
spread (metastasis). The tests
commonly used include a chest
x-ray, liver unction tests and
tumor makers (a blood test),
and a bone scan. (You may
eat and drink as you usually
do beore and ater these
tests.)
Systemic therapy (sis-TEM-ik):
Treatment that reaches and
aects cells all over the body.
Tissue (TISH-oo): A group or
layer o cells that perorms aspecic unction.
Tumor: An abnormal mass o
tissue.
Ultrasonography (ul-tra-son-
OG-ra-ee): A test in which
sound waves are bounced
o tissues and the echoes
are converted into a picture
(sonogram). These pictures
are shown on a monitor like a TV screen. Tissues o dierent
densities look dierent in the
picture because they refect
sound waves dierently. A
sonogram can show whether a
breast lump is a fuid-lled cyst
or a solid mass.
Wire-Localization: A technique
to localize a breast abnormality
that cannot be elt. The
procedure involves placing awire into the breast under local
anesthesia beore the surgical
procedure. The localization
can be done under guidance
o either mammography or
ultrasound.
X-ray: Radiation is used in low
doses to diagnose diseases
and in high doses to treat
cancer.

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 37/40
35
J. Resources
Service Category Local Resources National Resources
Counselling Faulkner Breast Centre Cancer Care Inc. 1-800-813-Hope
social worker Janet Rustow, LICSW www.youngsurviva l.org www.cancercare.org1153 Centre Street, Boston, MA 02130 www.lotsahelpinghands.com617-983-7967
Look Good, Feel Better Peer support Zakim Center for Integrative Therapies 1-800-395-LOOK
617-632-3322 National Coalition for Cancer Survivors
1-877-NCLS-YWSwww.cansearch.org
Genetic Counseling Dana Farber Cancer Institute
High Risk Clinic617-632-2170
New England Medical CenterDivision of Genetics617-636-5461
Lymphedema Support Greater Boston Lymphedema Network National Lymphedema Network
Meetings on 3rd Wednesday of the month 1-800-541-3259781-894-2309 www.lymphnet.org
Breast Prosthesis New England Medical Fitting988 Middle StreetWeymouth, MA 021881-800-341-1512
Friends Boutique - DFCI44 Binney StreetBoston, MA 02115617-632-6178
Internet Sources
Internet Massachusetts Breast Cancer Coalition www.breastcancer.org1-800-649-MBCC
American Cancer Society – MA American Cancer Society (ACS)www.ma.cancer.org 1-800-227-2345 www.cancer.org
Breast Cancer Network of Strength National Alliance of Breast Cancer 312-986-8338 www.networkofstrength.org Organizations (NABCO)
1-888-806-2266 www.nabco.org Young Survival Coalition 646-257-3000 www.youngsurvival.org National Breast Cancer Coalition
1-202-296-7477 www.natlbcc.org
National Cancer Institute1-800-4-CANCERwww.cancernet.nci.nih.govwww.nci.nih.gov
Center for Cancer Suppport and Education
781-648-0312 www.centerforcancer.org
Susan G Komen Breast Cancer Foundation1-800-462-9273 www.komen.org
Oncology Nursing Societywww.ons.org
Onco.Linkwww.onco.link.upenn.edu
Lance Armstrong Foundationwww.livestrong.com
Lotsa Helping Handswww.lotsahelpinghands.com
CaringBridge651-452-7940 www.caringbridge.org

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 38/40
36
NOTES:
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 39/40

8/3/2019 Guide to Breast Surgery 2 EVANS
http://slidepdf.com/reader/full/guide-to-breast-surgery-2-evans 40/40
www.FaulknerHospital.org
Faulkner Hospital
1153 Centre Street
Boston, MA 02130
Top Related