





Languages
Pages
Legal


GASTROESOPHAGEAL REFLUX
DISEASE (GERD)
IAGH Meeting
S Darvish Moghadam
KMU, Bahman 1393

Sources 1-Katz, et al. ACG Guidelines for the Diagnosis and
Management of GERD. Am J Gastroenterol 2013
2-Kahrilas, et al. AGA Medical Position Statement on
the Management of GERD, Gastroenterol 2008
3-Auyang, et al. Endoluminal Treatments for GERD.
Society of American Gastrointestinal and Endoscopic
Surgeons. Surgical Endoscopy. 2010, 2012
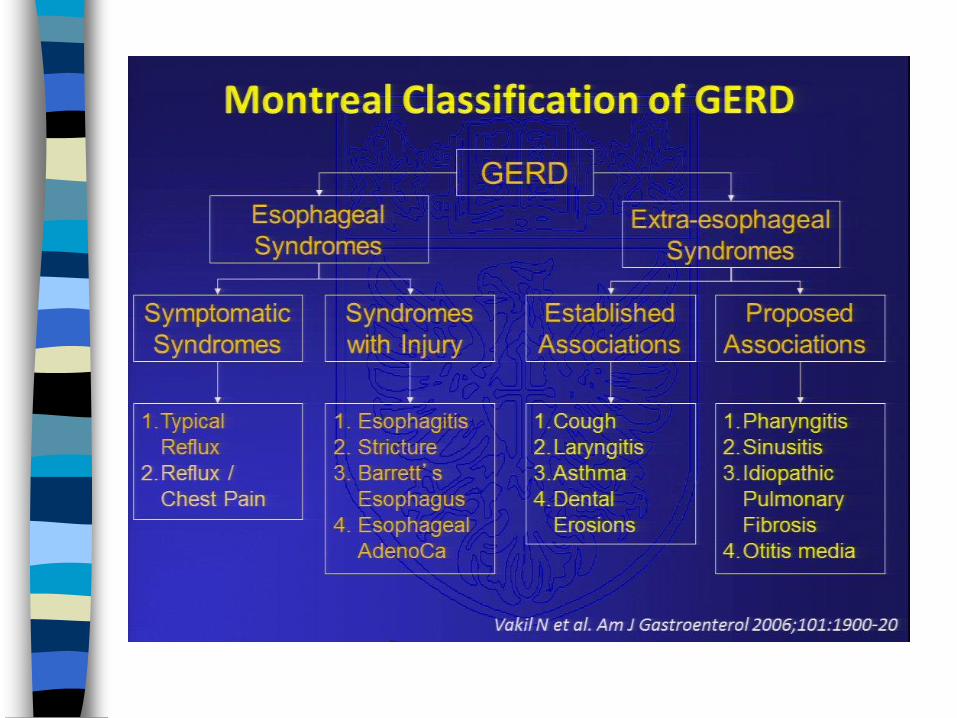
4-Vakil, et al. The Montreal definition and
classification of GERD: Am J Gastroenterol 2006
5-Richter, the management of heartburn in
pregnancy, APT 2005

Sources
6-Heidelbaugh,et al. atypical presentations of GERD.
Am Fam Physician. 2008
7-Kahrilas. GERD. N Engl J Med. 2008
Bloom.The modern investigation and management of
GERD. Clinical Medicine 2009
Kripke. Medical management vs. surgery for GERD. Am Fam Physician. 2010
UTD 2015
DDW 2014

GERD Definition:Montreal Classification
No standard criterion definition
Reflux of stomach & duodenal contents into
the esophagus with troublesome symptoms
and/or complications
Heartburn is the main symptom
occuring two or more days a week
Chronic recurrent disease
Impaired QOL
Am J Gastroenterol 2006, Gastroenterol 2008

Definitions of Reflux
Physiologic reflux
– occur postprandially, short-lived,
asymptomatic, rarely during sleep
Pathologic reflux
– symptomatic or mucosal injury, often
nocturnal episodes
Reflux esophagitis
– endoscopic or histopathologic
inflammation

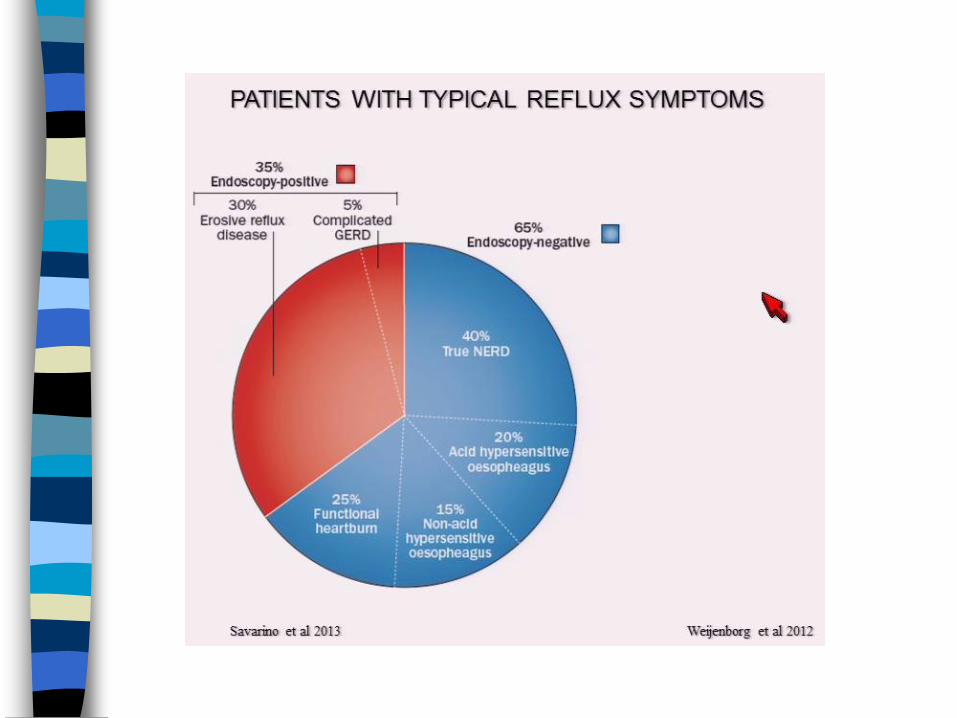
GERD: prevalence
Is based on heartburn &/or regurgitation
But
objective evidence of GERD
(esophagitis or Barrett's) always have
heartburn? No
Heartburn is always indicative of
GERD? No Gut 2008; 57:1354

GERD: prevalence
Prevalence: increasing trend in last 2
decade
weekly heartburn and/or regurgitation
Western world: 10 – 20% 48%
Asia: < 5 %
2.5%-4.8% before 2005 5.2%-8.5%
from 2005 to 2010 Gut 2005; 54:710
J Neurogastroenterol Motil 2011;17:14

GERD: prevalence in Iran
Ehsani:Tehran 39.7%;D: 7%, W: 8%, M: 21% Gastroenterol 2006
Mansour-Ghanaei: D: 2.4%, W: 9.1%, M:
11.3% Int J Mol Epidemiol Genet 2013
Somi: W: 26.8%, M: 34.1%, Iranian J Publ Health
2008
Kerman: 29.3%, 2012 IAGH congress abstract
Fazel: Sepahan Systematic Review, 22 study
1.9 - 52%. Int J Prevent Med, 2012
Delavari: Systematic Review, 15 study, W:
21.2%, MEJDD 2012

Frequency of Endoscopic GERD
Iranian Experience: 1994-1999
GERD
0%
20%
40%
60%
80%
100%
94 95 96 97 98 99
Retrospective study of 4500 UGIE reports (5y): 34.3% E-GERD
Malekzadeh,et al 2000

GERD- pathphysiology
Acid reflux
Non acid reflux- weak acid
Physiologic reflux
Pathologic reflux

non-acid reflux: estimated prevalence




GERD- Risk factors
Hiatal hernia
Obesity
Pregnancy
prolonged gastric emptying
Smoking
Alcohol
Anticholinergic, calcium channel
blockers, smooth muscle relaxants
2º GERD!!

Heartburn-
retrosternal burning
pain extend up into
the neck
GERD- manifestations

GERD- manifestations
Esophageal: heartburn- poor predictor
– regurgitation, dysphagia, odynophagia,
nausea
Extraesophageal
– bronchospasm, laryngitis, chronic cough,
chest pain, water brash, hoarseness, throat
clearing, globus?
Complications
– esophagitis, ulcer, stricture, Barrett’s, Ca



GERD- diagnosis
can be based on clinical symptoms
alone
Diagnostic evaluation neither necessary
nor practical to do for every patient with
heartburn
Response to Rx is not accurate enough

GERD- additional evaluation
Double contrast barium swallow
Low accuracy
Useful for * esophagitis * stricture
EGD, Bx
pH monitoring, Pepsin in refluxate
MII + pH
Manometry
ECG, exercise stress test in chest pain

GERD- esophagoscopy
intra & inter- operator variability
– Non-erosive, vs erosive
Los Angeles classification: A – D
– Based on mucosal breaks
Savary-Miller: Includes complications
– I: reddish spots
– II: erosions
– III: exudative circumferential erosions,
– IV: ulcers, stenosis, Barrett's V: metaplasia

GERD- EGD
Endoscopy indicated if:
Prolonged duration >5- 10 y, men > 50 y/o
not responsive to empiric Rx
troublesome dysphagia, GIB
systemic symptoms: weight loss, anemia
Repeat endoscopy in severe erosive esophagitis after a course of Rx
GERD guideline, AJG 2013
No sufficient data for screening endoscopy to diminish
the risk of death from Barrett’s or Ca Gastroenterol 2008

GERD- Bx
Normal endoscopy is not equal to Nl histology
Not indicated for diagnosis of GERD
Bx for suspected metaplasia, dysplasia
normal mucosa for eosinophilic esophagitis
Findings: non specific
– basal cell layer hyperplasia
– papillae elongation
– Neutrophils, eosinophils
– Vascular dilation, "balloon" squamous cells
Gastroenterol 2008

GERD- pH monitoring
Acid reflux: reflux of gastric contents
with a pH <4.0
withhold PPI Rx for 1 week before test
Recording devices
– transnasal catheter
– wireless capsule
combined multichannel intraluminal
impedance and pH (MII-pH) monitoring

GERD- pH monitoring indications
confirming Dx with persistent symptoms
& with normal endoscopy
failed twice daily PPI Rx
Monitoring adequacy of Rx in persistent
symptoms
supra-esophageal complications such
as reflux laryngitis or cough
Considering endoscopic or surgical Rx GERD guideline, AJG 2013, Gastroenterol 2008

GERD- Manometry
minimal role in diagnosis of GERD
ensuring correct place of pH probes
before antireflux surgery for peristaltic
function
to exclude motor disorders: achalasia /
scleroderma UTD 2015

GERD- Management, lifestyle
Recommended
Weight loss
Head elevation
avoidance of late-night meals
No meals 2 – 3 h before bedtime
Beneficial for nighttime heartburn or
regurgitation
GERD guideline, AJG 2013, Gastroenterol 2008
GERD- Management, lifestyle
Avoid
coffee, chocolate, fatty foods
acidic foods: citrus, carbonated drinks
spicy foods
alcohol, tobacco
GERD guideline, AJG 2013, Gastroenterol 2008

GERD- drug Rx
H2RA: mild symptoms, NERD
Also as maintenance in NERD
Duration: 8 w, D/C if asymptomatic
PPI: severe frequent symptoms, Erosive
As maintenance Rx in severe erosive
esophagitis, Barrett's

GERD Rx- role of PPI
PPIs inhibit gastric acid secretion
do not affect structural and motility
– HH, LES pressure, tLESR
PPIs do not decrease reflux

PPI concerns
no major difference in efficacy between PPIs
“step up” or “step down”?
titrate down to the lowest effective dose
Non-responders should refer for evaluation
no evidence to support adding nocturnal
H2RA to twice-daily PPI
Gastroenterol 2008

GERD-on-demand Rx
Reasonable strategy in esophageal GERD without
esophagitis
– Practically, many subjects often use intermittently
Not recommended in:
– Extra- esophageal
– Healed erosive esophagitis
Gastroenterol 2008



GERD- Rx, other drugs
Antacids
Sodium alginate
Metoclopramide
Domperidone
Cisapride
Baclofen

Am Fam Physician.
2008

DDW 2014

GERD Rx- in pregnancy
Antacids or sucralfate: first-line drug Rx
Then: H2RA
PPI roton for intractable symptoms or
complicated GERD
All but omeprazole are FDA category B
Of systemic agents, only the H2RA, except
nizatidine, are safe during lactation
APT 2005



GERD- preoperative evaluation
Upper endoscopy
esophageal manometry
assessment of esophageal length
degree of hiatal herniation

GERD- Fundoplication
Nissen, Troupet, Hill gastropexy

GERD- Endoluminal Treatments
Radiofrequency Rx
Endoscopic Plication System (EPS)
EsophyX: Endoluminal fundoplication
(ELF)
– Transoral Incisionless Fundoplication (TIF)
– “hybrid” technique: laparoscopic posterior
cruroplasty and standard TIF

GERD- radiofrequency Rx
unsatisfactory control of GERD with PPI
do not wish to be on long-term medical
Rx
considering fundoplication
Overall response , 55 – 83% in 12 - 33
months
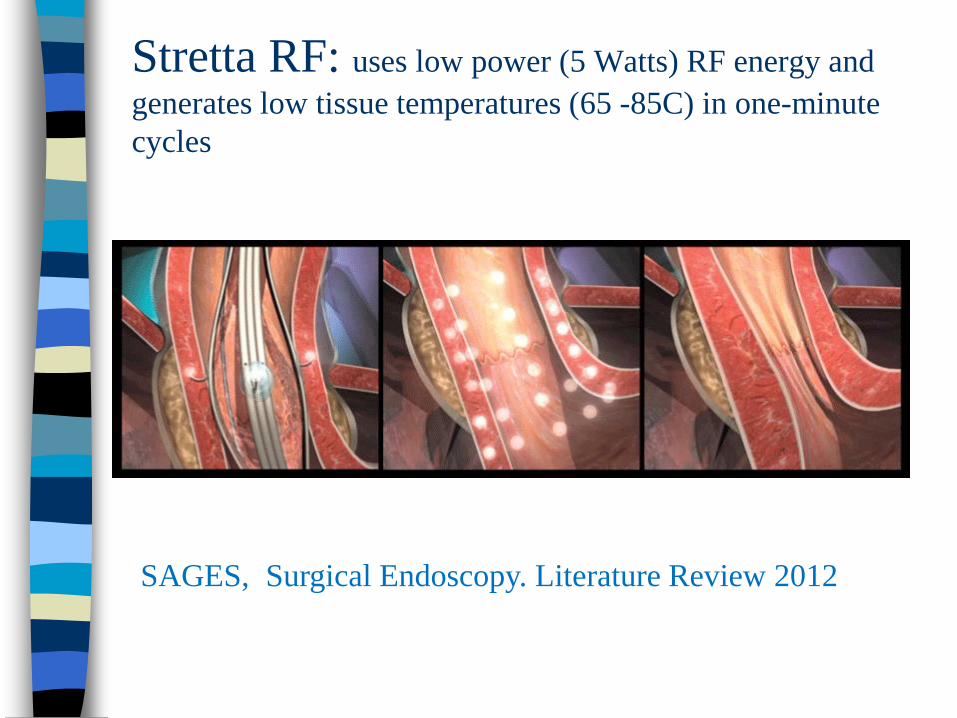
Stretta RF: uses low power (5 Watts) RF energy and
generates low tissue temperatures (65 -85C) in one-minute
cycles
SAGES, Surgical Endoscopy. Literature Review 2012

EsophyX: Transoral Incisionless Fundoplication
A-TIF 1 gastrogastric wrap fundoplication
B- TIF 2 esophagogastric fundoplication above Z line
Society of American Gastrointestinal and Endoscopic Surgeons
Surgical Endoscopy. 2010

GERD- challenges
Does GERD progress in Severity?
Does non-erosive progress to erosive,
metaplasia, Barrett’s?
Does it warrant endoscopic monitoring? No
Can we stop medications?
What about Hpylori?
Gastroenterol 2008
Does GERD progress?
first view: “spectrum of disease”
progressive disease: going from today’s
nonerosive to tomorrow’s erosive &, Barrett’s
contrasted view: “discreet categories”
nonerosive, erosive esophagitis, Barrett’s
conversion is unusual, subjects stay in their
initial category
Gastroenterol 2008

Does GERD progress?
Available limited data: GERD sometimes may
progress from non-erosive to erosive dis.
reported rates of progression are relatively
low over a 20-year period
Progression after a normal index endoscopy,
in 7-year follow-up:
stricture:1.9%, Barrett’s: 0.0%, adenoca:
0.1%,

GERD- endoscopy F/U
Most importantly, endoscopic
monitoring in chronic GERD without
alarm symptoms has not been shown to
diminish the risk of cancer, and this
practice is discouraged Gastroenterol 2008

GERD- stop medications?
Yes in: mild , non frequent symptoms and no
relapse after a course of Rx
No in: severe symptoms, severe esophagitis
(LA: C-D), Barrett's
UTD 2015

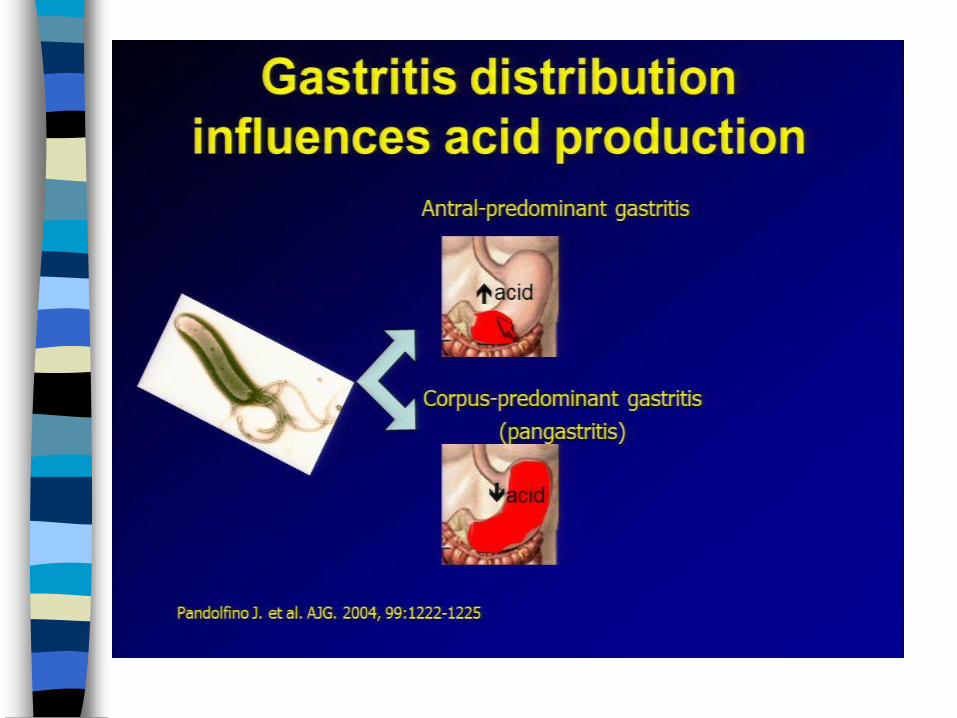
GERD & H. pylori
available data suggest that H. pylori,
particularly Cag A strains, may be protective
against the severe forms of GERD, Barrett's
metaplasia, esoph. adenocarcinoma
corpus-dominant or pangastritis
antrum-dominant gastritis
Long term PPI use
Screening & treatment for is not recommended
GERD guideline, AJG 2013

Jovārish-e Jālīnūs, the herbal treatment of GERD,
Shirzad, Res Hist Med 2013

GERD- overall recommendation
Don’t use many combined Dx procedures
Do not switch PPIs frequently
No routine use of calcium supplement, BDM,
H pylori screening due to PPI Rx
Give him/ her an opportunity for a simple life

I’m worried and concerned
GI symptoms bother me!
My whole life is affected
Heartburn disturbs my
sleep
I cannot eat and drink whatever
I like
I cannot bend over or exercise
Illustrator: Eric Werner
Top Related