







Languages
Pages
Legal

Formulary
2015
List of Covered Drugs
premera.com
Version 6
Premera Blue Cross Medicare Advantage (HMO)Premera Blue Cross Medicare Advantage Plus (HMO)Premera Blue Cross Medicare Advantage (HMO-POS)Premera Blue Cross Medicare Advantage Plus (HMO-POS)
Customer Service:
PLEASE READ: This document contains information about the drugs we cover in this plan.
Premera Blue Cross Medicare AdvantagePO Box 4196, Portland, OR 97208-4196Call toll free 888-850-8526 (TTY: 711). Representatives are available between 8 a.m. and 8 p.m., seven days a week.

H7245_2015PBCRX11_Errata 031902 (10-2014)
Correction
Please note:
On pages 50 and 87, the following drug was included in the printed formulary document in error:
omeprazole magnesium
This drug is not covered for Medicare members by the Centers for Medicare and Medicaid Services (CMS).
Your Premera Blue Cross Medicare Advantage plan does cover omeprazole (10mg, 40mg, 20mg).
Please insert this document in your current Premera Blue Cross Medicare Advantage formulary booklet for future reference.
If you have any questions regarding this notice, please contact the Premera Blue Cross Medicare Advantage Customer Service Team at 1-888-850-8526 (TTY 711), between 8 a.m. and 8 p.m., seven days a week.
The benefit information provided is a brief summary, not a complete description of benefits. For more information, contact the plan. Limitations, copayments, and restrictions may apply. Beneficiaries must use network pharmacies to access their prescription drug benefit. Benefits, formulary, pharmacy network, provider network, premium and/or copayments/coinsurance may change on January 1 of each year.
Premera Blue Cross is an HMO and HMO-POS plan with a Medicare contract. Enrollment in Premera Blue Cross depends on contract renewal.
i
Premera Blue Cross Medicare Advantage (HMO),
Premera Blue Cross Medicare Advantage Plus (HMO),
Premera Blue Cross Medicare Advantage (HMO-POS) and
Premera Blue Cross Medicare Advantage Plus (HMO-POS)
2015 Formulary
(List of Covered Drugs)
PLEASE READ: THIS DOCUMENT CONTAINS INFORMATION ABOUT SOME OF THE DRUGS WE COVER IN THIS PLAN
Formulary ID: 00015063, Version: 6 This formulary was updated on 08/01/2014. For more recent information or other questions, please contact Premera Blue Cross Medicare Advantage Plans Customer Service at 1-888-850-8526 or, for TTY users, 711, seven days a week between 8 a.m. and 8 p.m., or visit www.premera.com.
Note to existing members: This formulary has changed since last year. Please review this document to make sure that it still contains the drugs you take.
When this drug list (formulary) refers to “we,” “us,” or “our,” it means Premera Blue Cross Medicare Advantage Plans. When it refers to “plan” or “our plan,” it means Premera Blue Cross Medicare Advantage Plans.
This document includes a list of the drugs (formulary) for our plan, which is current as of 01/2015. For an updated formulary, please contact us. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages.
You must generally use network pharmacies to use your prescription drug benefit. Benefits, formulary, pharmacy network, provider network and/or copayments/coinsurance may change on January 1, 2016, and from time to time during the year.
ii
What is the Premera Blue Cross Medicare Advantage (HMO), Premera Blue Cross Medicare Advantage Plus (HMO), Premera Blue Cross Medicare Advantage (HMO-POS) and Premera Blue Cross Medicare Advantage Plus (HMO-POS) Formulary?
A formulary is a list of covered drugs selected by Premera Blue Cross Medicare Advantage Plans in consultation with a team of health care providers, which represents the prescription therapies believed to be a necessary part of a quality treatment program. Premera Blue Cross Medicare Advantage Plans will generally cover the drugs listed in our formulary as long as the drug is medically necessary, the prescription is filled at a Premera Blue Cross Medicare Advantage Plans network pharmacy, and other plan rules are followed. For more information on how to fill your prescriptions, please review your Evidence of Coverage.
Can the Formulary (drug list) change?
Generally, if you are taking a drug on our 2015 formulary that was covered at the beginning of the year, we will not discontinue or reduce coverage of the drug during the 2015 coverage year except when a new, less expensive generic drug becomes available or when new adverse information about the safety or effectiveness of a drug is released. Other types of formulary changes, such as removing a drug from our formulary, will not affect members who are currently taking the drug. It will remain available at the same cost-sharing for those members taking it for the remainder of the coverage year. We feel it is important that you have continued access for the remainder of the coverage year to the formulary drugs that were available when you chose our plan, except for cases in which you can save additional money or we can ensure your safety.
If we remove drugs from our formulary, add prior authorization, quantity limits and/or step therapy restrictions on a drug or move a drug to a higher cost-sharing tier, we must notify affected members of the change at least 60 days before the change becomes effective, or at the time the member requests a refill of the drug, at which time the member will receive a 60-day supply of the drug. If the Food and Drug Administration deems a drug on our formulary to be unsafe or the drug’s manufacturer removes the drug from the market, we will immediately remove the drug from our formulary and provide notice to members who take the drug. The enclosed formulary is current as of 01/01/2015. To get updated information about the drugs covered by Premera Blue Cross Medicare Advantage Plans, please contact us. Our contact information appears on the front and back cover pages. If we make any mid-year non-maintenance changes to the Premera Blue Cross Medicare Advantage Plans formulary, we will mail you a copy of the formulary changes via errata sheets to ensure that you have a complete and updated formulary.
How do I use the Formulary?
There are two ways to find your drug within the formulary:
Medical Condition
The formulary begins on page 1. The drugs in this formulary are grouped into categories depending on the type of medical conditions that they are used to treat. For example, drugs
iii
used to treat a heart condition are listed under the category, “Cardiovascular Agents.” If you know what your drug is used for, look for the category name in the list that begins on page 94. Then look under the category name for your drug.
Alphabetical Listing
If you are not sure what category to look under, you should look for your drug in the Index that begins on page 76. The Index provides an alphabetical list of all of the drugs included in this document. Both brand name drugs and generic drugs are listed in the Index. Look in the Index and find your drug. Next to your drug, you will see the page number where you can find coverage information. Turn to the page listed in the Index and find the name of your drug in the first column of the list.
What are generic drugs?
Premera Blue Cross Medicare Advantage Plans covers both brand name drugs and generic drugs. A generic drug is approved by the FDA as having the same active ingredient as the brand name drug. Generally, generic drugs cost less than brand name drugs.
Are there any restrictions on my coverage?
Some covered drugs may have additional requirements or limits on coverage. These requirements and limits may include:
• Prior Authorization: Premera Blue Cross Medicare Advantage Plans requires you or your physician to get prior authorization for certain drugs. This means that you will need to get approval from Premera Blue Cross Medicare Advantage Plans before you fill your prescriptions. If you don’t get approval, Premera Blue Cross Medicare Advantage Plans may not cover the drug.
• Quantity Limits: For certain drugs, Premera Blue Cross Medicare Advantage Plans limits the amount of the drug that Premera Blue Cross Medicare Advantage Plans will cover. For example, Premera Blue Cross Medicare Advantage Plans provides 30 tablets per prescription for Zolpidem. This may be in addition to a standard one-month or three-month supply.
• Step Therapy: In some cases, Premera Blue Cross Medicare Advantage Plans requires you to first try certain drugs to treat your medical condition before we will cover another drug for that condition. For example, if Drug A and Drug B both treat your medical condition, Premera Blue Cross Medicare Advantage Plans may not cover Drug B unless you try Drug A first. If Drug A does not work for you, Premera Blue Cross Medicare Advantage Plans will then cover Drug B.
You can find out if your drug has any additional requirements or limits by looking in the formulary that begins on page 1. You can also get more information about the restrictions applied to specific covered drugs by visiting our website. We have posted on line documents that explain our prior authorization and step therapy restrictions. You may also ask us to send you a copy. Our contact
iv
information, along with the date we last updated the formulary, appears on the front and back cover pages.
You can ask Premera Blue Cross Medicare Advantage Plans to make an exception to these restrictions or limits or for a list of other, similar drugs that may treat your health condition. See the section, “How do I request an exception to the Premera Blue Cross Medicare Advantage Plans’ formulary?” on page iv for information about how to request an exception.
What if my drug is not on the Formulary?
If your drug is not included in this formulary (list of covered drugs), you should first contact Customer Service and ask if your drug is covered.
If you learn that Premera Blue Cross Medicare Advantage Plans does not cover your drug, you have two options:
• You can ask Customer Service for a list of similar drugs that are covered by Premera Blue Cross Medicare Advantage Plans. When you receive the list, show it to your doctor and ask him or her to prescribe a similar drug that is covered by Premera Blue Cross Medicare Advantage Plans.
• You can ask Premera Blue Cross Medicare Advantage Plans to make an exception and cover your drug. See below for information about how to request an exception.
How do I request an exception to Premera Blue Cross Medicare Advantage (HMO), Premera Blue Cross Medicare Advantage Plus (HMO), Premera Blue Cross Medicare Advantage (HMO-POS) and Premera Blue Cross Medicare Advantage Plus (HMO-POS)’s Formulary?
You can ask Premera Blue Cross Medicare Advantage Plans to make an exception to our coverage rules. There are several types of exceptions that you can ask us to make.
• You can ask us to cover a drug even if it is not on our formulary. If approved, this drug will be covered at a pre-determined cost-sharing level, and you would not be able to ask us to provide the drug at a lower cost-sharing level.
• You can ask us to cover a formulary drug at a lower cost-sharing level if this drug is not on the specialty tier. If approved this would lower the amount you must pay for your drug.
• You can ask us to waive coverage restrictions or limits on your drug. For example, for certain drugs, Premera Blue Cross Medicare Advantage Plans limits the amount of the drug that we will cover. If your drug has a quantity limit, you can ask us to waive the limit and cover a greater amount.
Generally, Premera Blue Cross Medicare Advantage Plans will only approve your request for an exception if the alternative drugs included on the plan’s formulary, the lower cost-sharing drug or additional utilization restrictions would not be as effective in treating your condition and/or would cause you to have adverse medical effects.
v
You should contact us to ask us for an initial coverage decision for a formulary, tiering or utilization restriction exception. When you request a formulary, tiering or utilization restriction exception you should submit a statement from your prescriber or physician supporting your request. Generally, we must make our decision within 72 hours of getting your prescriber’s supporting statement. You can request an expedited (fast) exception if you or your doctor believe that your health could be seriously harmed by waiting up to 72 hours for a decision. If your request to expedite is granted, we must give you a decision no later than 24 hours after we get a supporting statement from your doctor or other prescriber.
What do I do before I can talk to my doctor about changing my drugs or requesting an exception?
As a new or continuing member in our plan you may be taking drugs that are not on our formulary. Or, you may be taking a drug that is on our formulary but your ability to get it is limited. For example, you may need a prior authorization from us before you can fill your prescription. You should talk to your doctor to decide if you should switch to an appropriate drug that we cover or request a formulary exception so that we will cover the drug you take. While you talk to your doctor to determine the right course of action for you, we may cover your drug in certain cases during the first 90 days you are a member of our plan. For each of your drugs that is not on our formulary or if your ability to get your drugs is limited, we will cover a temporary 90-day supply (unless you have a prescription written for fewer days) when you go to a network pharmacy. After your first 90-day supply, we will not pay for these drugs, even if you have been a member of the plan less than 90 days. If you are a resident of a long-term care facility, we will allow you to refill your prescription until we have provided you with a 98-day transition supply, consistent with dispensing increment, (unless you have a prescription written for fewer days). We will cover more than one refill of these drugs for the first 90 days you are a member of our plan. If you need a drug that is not on our formulary or if your ability to get your drugs is limited, but you are past the first 90 days of membership in our plan, we will cover a 34-day emergency supply of that drug (unless you have a prescription for fewer days) while you pursue a formulary exception.
Level of care change: Day Supply For members transitioning from a SNF to LTC: 34 day supply SNF to Home (Retail): 30 day supply LTC LTC: -‐ 34 day supply Hospital to Home (Retail): 30 day supply
vi
For more information
For more detailed information about your Premera Blue Cross Medicare Advantage Plans prescription drug coverage, please review your Evidence of Coverage and other plan materials.
If you have questions about Premera Blue Cross Medicare Advantage Plans, please contact us. Our contact information, along with the date we last updated the formulary, appears on the front and back cover pages.
If you have general questions about Medicare prescription drug coverage, please call Medicare at 1-800-MEDICARE (1-800-633-4227) 24 hours a day/7 days a week. TTY users should call 1-877-486-2048. Or, visit http://www.medicare.gov.
Premera Blue Cross Medicare Advantage Plans’ Formulary
The formulary that begins on page 1 provides coverage information about some of the drugs covered by Premera Blue Cross Medicare Advantage Plans. If you have trouble finding your drug in the list, turn to the Index that begins on page 76.
The first column of the chart lists the drug name. Brand name drugs are capitalized (e.g., CELEBREX®) and generic drugs are listed in lower-case italics (e.g., simvastatin).
The second column of the chart lists the Drug Tier. The Drug Tier name lets you know the amount you will pay at the pharmacy.
The information in the Requirements/Limits column tells you if Premera Blue Cross Medicare Advantage Plans has any special requirements for coverage of your drug.
vii
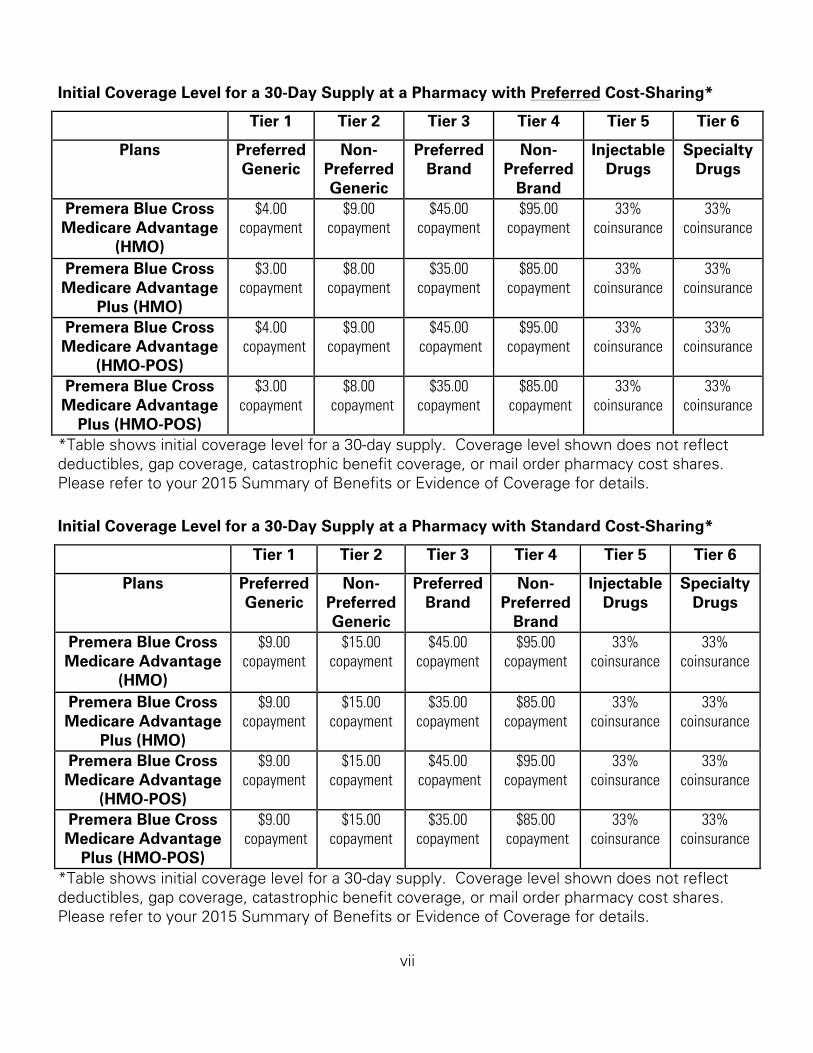
Initial Coverage Level for a 30-Day Supply at a Pharmacy with Preferred Cost-Sharing*
Tier 1 Tier 2 Tier 3 Tier 4 Tier 5 Tier 6
Plans Preferred Generic
Non-Preferred Generic
Preferred Brand
Non- Preferred
Brand
Injectable Drugs
Specialty Drugs
Premera Blue Cross $4.00 $9.00 $45.00 $95.00 33% 33% Medicare Advantage
(HMO) copayment copayment copayment copayment coinsurance coinsurance
Premera Blue Cross $3.00 $8.00 $35.00 $85.00 33% 33% Medicare Advantage
Plus (HMO) copayment copayment copayment copayment coinsurance coinsurance
Premera Blue Cross $4.00 $9.00 $45.00 $95.00 33% 33% Medicare Advantage
(HMO-POS) copayment copayment copayment copayment coinsurance coinsurance
Premera Blue Cross $3.00 $8.00 $35.00 $85.00 33% 33% Medicare Advantage
Plus (HMO-POS) copayment copayment copayment copayment coinsurance coinsurance
*Table shows initial coverage level for a 30-day supply. Coverage level shown does not reflect deductibles, gap coverage, catastrophic benefit coverage, or mail order pharmacy cost shares. Please refer to your 2015 Summary of Benefits or Evidence of Coverage for details.
Initial Coverage Level for a 30-Day Supply at a Pharmacy with Standard Cost-Sharing*
Tier 1 Tier 2 Tier 3 Tier 4 Tier 5 Tier 6
Plans Preferred Generic
Non- Preferred Generic
Preferred Brand
Non- Preferred
Brand
Injectable Drugs
Specialty Drugs
Premera Blue Cross $9.00 $15.00 $45.00 $95.00 33% 33% Medicare Advantage
(HMO) copayment copayment copayment copayment coinsurance coinsurance
Premera Blue Cross $9.00 $15.00 $35.00 $85.00 33% 33% Medicare Advantage
Plus (HMO) copayment copayment copayment copayment coinsurance coinsurance
Premera Blue Cross $9.00 $15.00 $45.00 $95.00 33% 33% Medicare Advantage
(HMO-POS) copayment copayment copayment copayment coinsurance coinsurance
Premera Blue Cross $9.00 $15.00 $35.00 $85.00 33% 33% Medicare Advantage
Plus (HMO-POS) copayment copayment copayment copayment coinsurance coinsurance
*Table shows initial coverage level for a 30-day supply. Coverage level shown does not reflect deductibles, gap coverage, catastrophic benefit coverage, or mail order pharmacy cost shares. Please refer to your 2015 Summary of Benefits or Evidence of Coverage for details.
viii
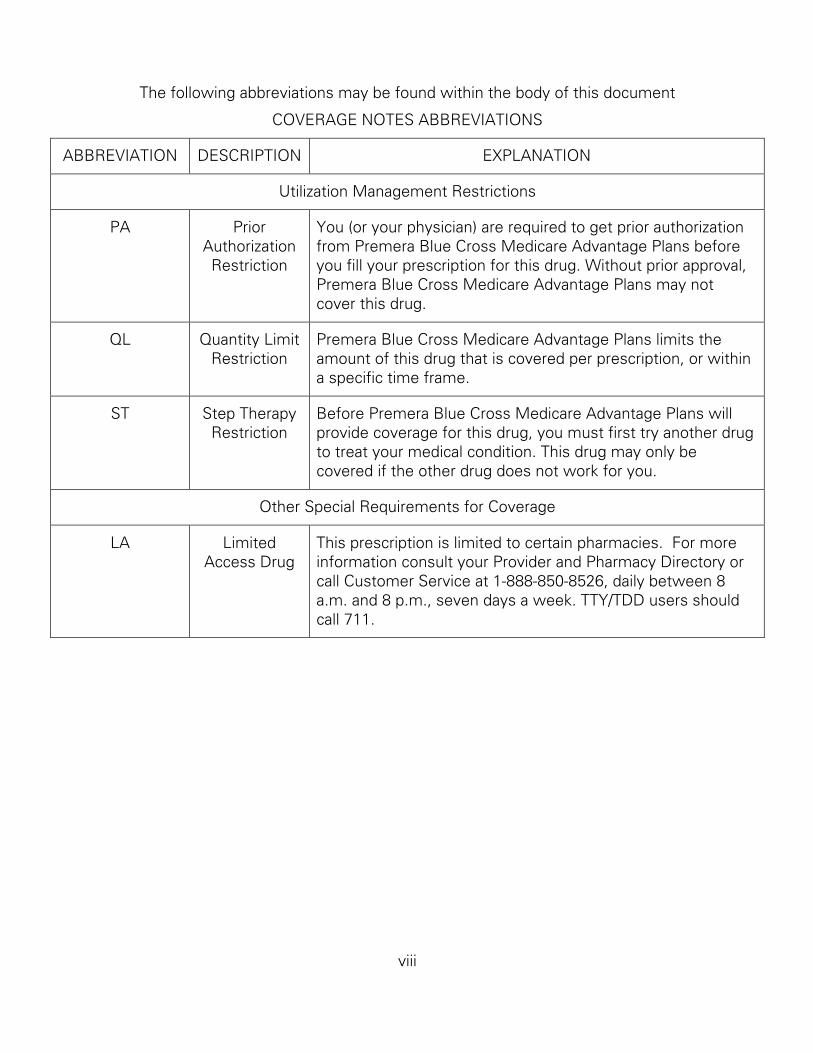
The following abbreviations may be found within the body of this document
COVERAGE NOTES ABBREVIATIONS
ABBREVIATION DESCRIPTION EXPLANATION
Utilization Management Restrictions
PA Prior Authorization Restriction
You (or your physician) are required to get prior authorization from Premera Blue Cross Medicare Advantage Plans before you fill your prescription for this drug. Without prior approval, Premera Blue Cross Medicare Advantage Plans may not cover this drug.
QL Quantity Limit Restriction
Premera Blue Cross Medicare Advantage Plans limits the amount of this drug that is covered per prescription, or within a specific time frame.
ST Step Therapy Restriction
Before Premera Blue Cross Medicare Advantage Plans will provide coverage for this drug, you must first try another drug to treat your medical condition. This drug may only be covered if the other drug does not work for you.
Other Special Requirements for Coverage
LA Limited Access Drug
This prescription is limited to certain pharmacies. For more information consult your Provider and Pharmacy Directory or call Customer Service at 1-888-850-8526, daily between 8 a.m. and 8 p.m., seven days a week. TTY/TDD users should call 711.
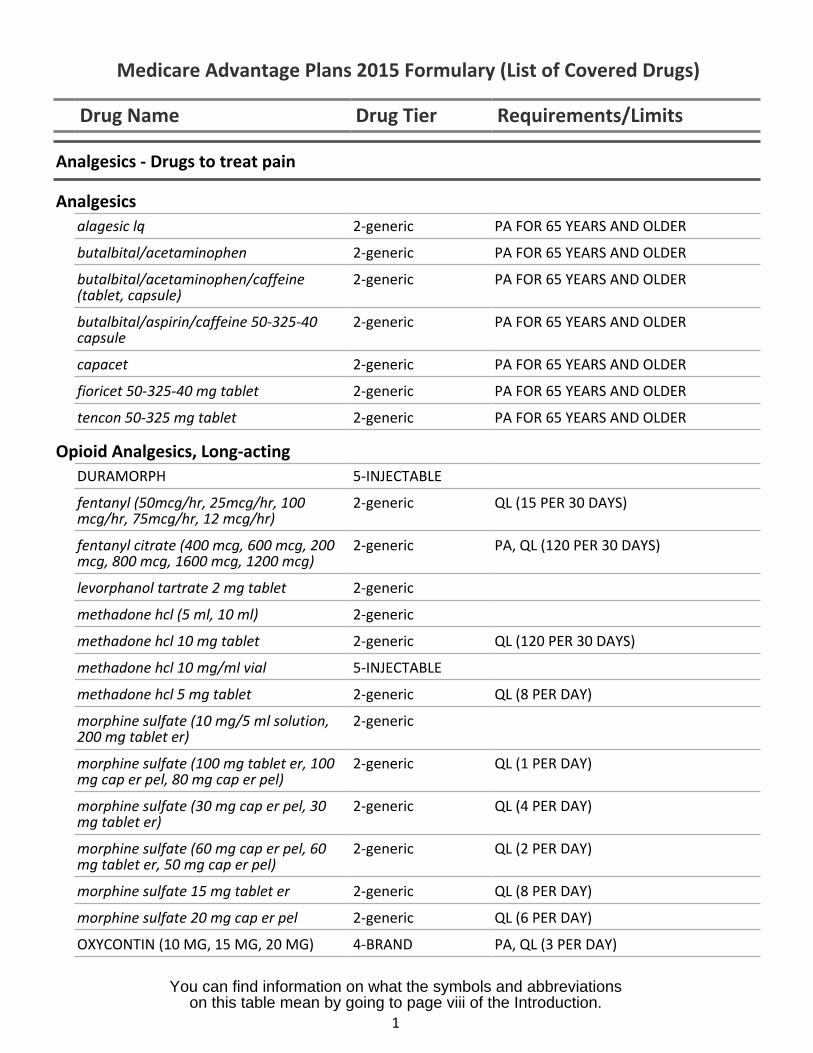
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Analgesics - Drugs to treat pain
Analgesicsalagesic lq 2-generic PA FOR 65 YEARS AND OLDER
butalbital/acetaminophen 2-generic PA FOR 65 YEARS AND OLDER
butalbital/acetaminophen/caffeine(tablet, capsule)
2-generic PA FOR 65 YEARS AND OLDER
butalbital/aspirin/caffeine 50-325-40capsule
2-generic PA FOR 65 YEARS AND OLDER
capacet 2-generic PA FOR 65 YEARS AND OLDER
fioricet 50-325-40 mg tablet 2-generic PA FOR 65 YEARS AND OLDER
tencon 50-325 mg tablet 2-generic PA FOR 65 YEARS AND OLDER
Opioid Analgesics, Long-actingDURAMORPH 5-INJECTABLE
fentanyl (50mcg/hr, 25mcg/hr, 100mcg/hr, 75mcg/hr, 12 mcg/hr)
2-generic QL (15 PER 30 DAYS)
fentanyl citrate (400 mcg, 600 mcg, 200mcg, 800 mcg, 1600 mcg, 1200 mcg)
2-generic PA, QL (120 PER 30 DAYS)
levorphanol tartrate 2 mg tablet 2-generic
methadone hcl (5 ml, 10 ml) 2-generic
methadone hcl 10 mg tablet 2-generic QL (120 PER 30 DAYS)
methadone hcl 10 mg/ml vial 5-INJECTABLE
methadone hcl 5 mg tablet 2-generic QL (8 PER DAY)
morphine sulfate (10 mg/5 ml solution,200 mg tablet er)
2-generic
morphine sulfate (100 mg tablet er, 100mg cap er pel, 80 mg cap er pel)
2-generic QL (1 PER DAY)
morphine sulfate (30 mg cap er pel, 30mg tablet er)
2-generic QL (4 PER DAY)
morphine sulfate (60 mg cap er pel, 60mg tablet er, 50 mg cap er pel)
2-generic QL (2 PER DAY)
morphine sulfate 15 mg tablet er 2-generic QL (8 PER DAY)
morphine sulfate 20 mg cap er pel 2-generic QL (6 PER DAY)
OXYCONTIN (10 MG, 15 MG, 20 MG) 4-BRAND PA, QL (3 PER DAY)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
1
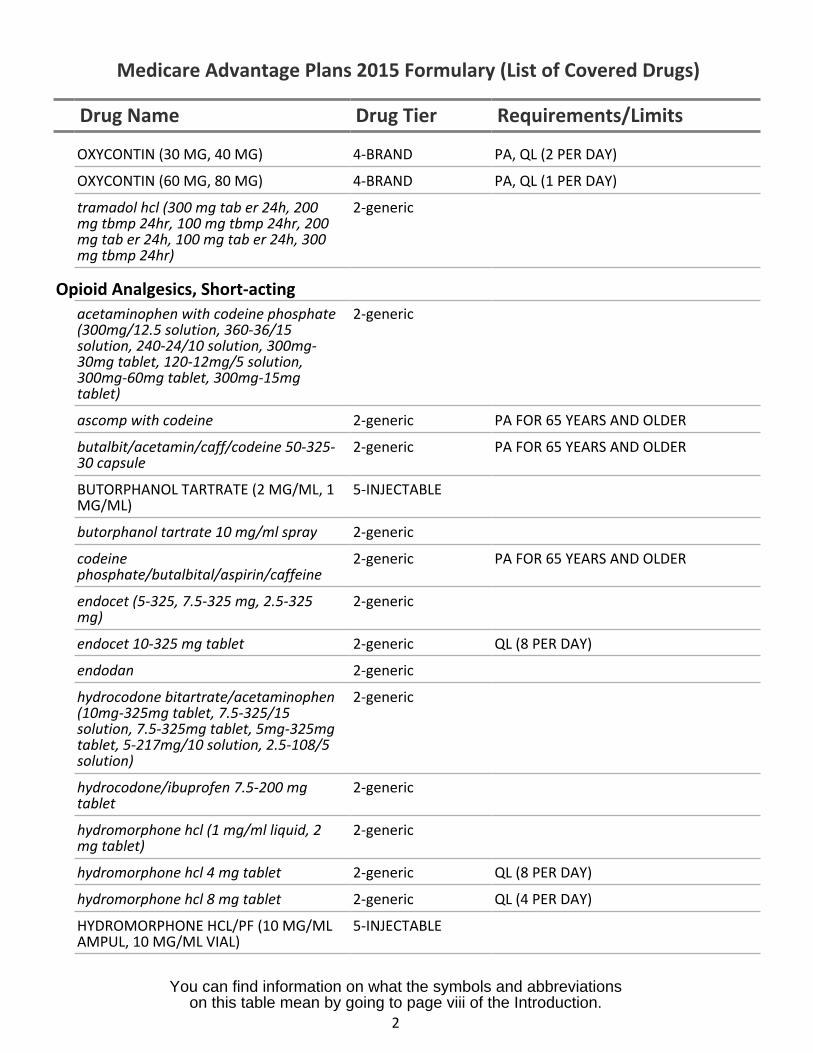
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
OXYCONTIN (30 MG, 40 MG) 4-BRAND PA, QL (2 PER DAY)
OXYCONTIN (60 MG, 80 MG) 4-BRAND PA, QL (1 PER DAY)
tramadol hcl (300 mg tab er 24h, 200 2-genericmg tbmp 24hr, 100 mg tbmp 24hr, 200mg tab er 24h, 100 mg tab er 24h, 300mg tbmp 24hr)
Opioid Analgesics, Short-actingacetaminophen with codeine phosphate 2-generic(300mg/12.5 solution, 360-36/15solution, 240-24/10 solution, 300mg-30mg tablet, 120-12mg/5 solution,300mg-60mg tablet, 300mg-15mgtablet)
ascomp with codeine 2-generic PA FOR 65 YEARS AND OLDER
butalbit/acetamin/caff/codeine 50-325- 2-generic PA FOR 65 YEARS AND OLDER30 capsule
BUTORPHANOL TARTRATE (2 MG/ML, 1 5-INJECTABLEMG/ML)
butorphanol tartrate 10 mg/ml spray 2-generic
codeine 2-generic PA FOR 65 YEARS AND OLDERphosphate/butalbital/aspirin/caffeine
endocet (5-325, 7.5-325 mg, 2.5-325 2-genericmg)
endocet 10-325 mg tablet 2-generic QL (8 PER DAY)
endodan 2-generic
hydrocodone bitartrate/acetaminophen 2-generic(10mg-325mg tablet, 7.5-325/15solution, 7.5-325mg tablet, 5mg-325mgtablet, 5-217mg/10 solution, 2.5-108/5solution)
hydrocodone/ibuprofen 7.5-200 mg 2-generictablet
hydromorphone hcl (1 mg/ml liquid, 2 2-genericmg tablet)
hydromorphone hcl 4 mg tablet 2-generic QL (8 PER DAY)
hydromorphone hcl 8 mg tablet 2-generic QL (4 PER DAY)
HYDROMORPHONE HCL/PF (10 MG/ML 5-INJECTABLEAMPUL, 10 MG/ML VIAL)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
2
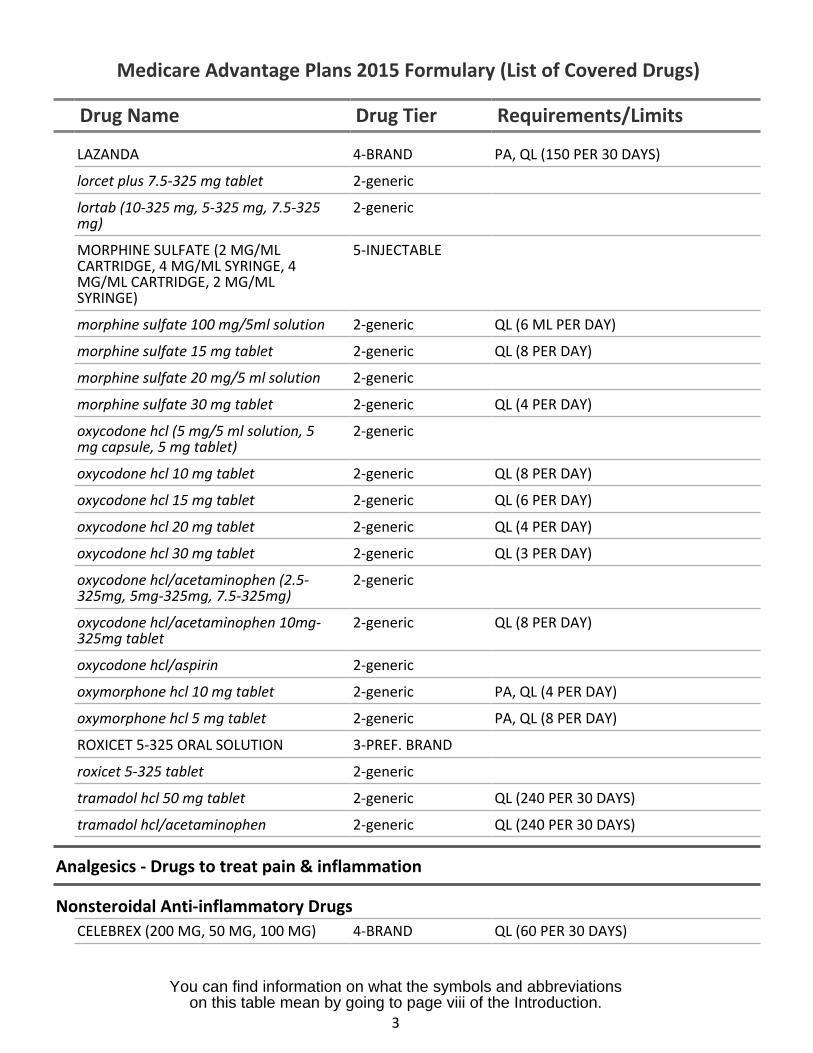
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
LAZANDA 4-BRAND PA, QL (150 PER 30 DAYS)
lorcet plus 7.5-325 mg tablet 2-generic
lortab (10-325 mg, 5-325 mg, 7.5-325mg)
2-generic
MORPHINE SULFATE (2 MG/MLCARTRIDGE, 4 MG/ML SYRINGE, 4MG/ML CARTRIDGE, 2 MG/MLSYRINGE)
5-INJECTABLE
morphine sulfate 100 mg/5ml solution 2-generic QL (6 ML PER DAY)
morphine sulfate 15 mg tablet 2-generic QL (8 PER DAY)
morphine sulfate 20 mg/5 ml solution 2-generic
morphine sulfate 30 mg tablet 2-generic QL (4 PER DAY)
oxycodone hcl (5 mg/5 ml solution, 5mg capsule, 5 mg tablet)
2-generic
oxycodone hcl 10 mg tablet 2-generic QL (8 PER DAY)
oxycodone hcl 15 mg tablet 2-generic QL (6 PER DAY)
oxycodone hcl 20 mg tablet 2-generic QL (4 PER DAY)
oxycodone hcl 30 mg tablet 2-generic QL (3 PER DAY)
oxycodone hcl/acetaminophen (2.5-325mg, 5mg-325mg, 7.5-325mg)
2-generic
oxycodone hcl/acetaminophen 10mg-325mg tablet
2-generic QL (8 PER DAY)
oxycodone hcl/aspirin 2-generic
oxymorphone hcl 10 mg tablet 2-generic PA, QL (4 PER DAY)
oxymorphone hcl 5 mg tablet 2-generic PA, QL (8 PER DAY)
ROXICET 5-325 ORAL SOLUTION 3-PREF. BRAND
roxicet 5-325 tablet 2-generic
tramadol hcl 50 mg tablet 2-generic QL (240 PER 30 DAYS)
tramadol hcl/acetaminophen 2-generic QL (240 PER 30 DAYS)
Analgesics - Drugs to treat pain & inflammation
Nonsteroidal Anti-inflammatory DrugsCELEBREX (200 MG, 50 MG, 100 MG) 4-BRAND QL (60 PER 30 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
3
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
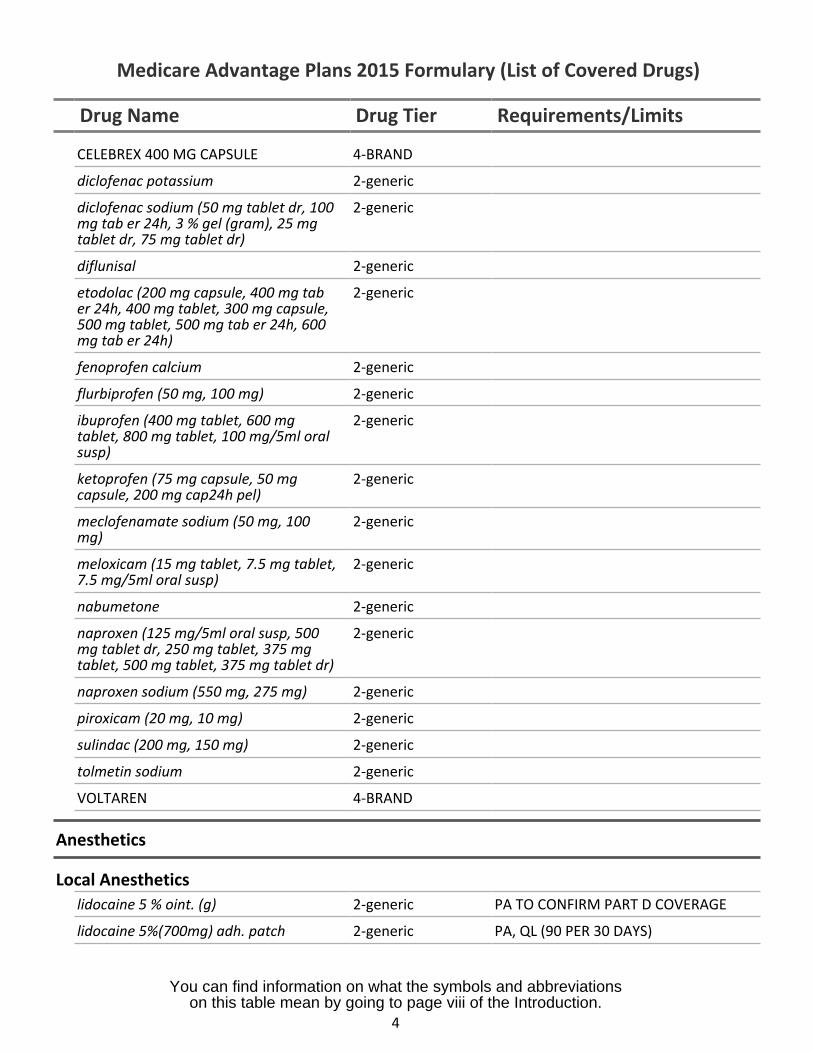
CELEBREX 400 MG CAPSULE 4-BRAND
diclofenac potassium 2-generic
diclofenac sodium (50 mg tablet dr, 100mg tab er 24h, 3 % gel (gram), 25 mgtablet dr, 75 mg tablet dr)
2-generic
diflunisal 2-generic
etodolac (200 mg capsule, 400 mg taber 24h, 400 mg tablet, 300 mg capsule,500 mg tablet, 500 mg tab er 24h, 600mg tab er 24h)
2-generic
fenoprofen calcium 2-generic
flurbiprofen (50 mg, 100 mg) 2-generic
ibuprofen (400 mg tablet, 600 mgtablet, 800 mg tablet, 100 mg/5ml oralsusp)
2-generic
ketoprofen (75 mg capsule, 50 mgcapsule, 200 mg cap24h pel)
2-generic
meclofenamate sodium (50 mg, 100mg)
2-generic
meloxicam (15 mg tablet, 7.5 mg tablet,7.5 mg/5ml oral susp)
2-generic
nabumetone 2-generic
naproxen (125 mg/5ml oral susp, 500mg tablet dr, 250 mg tablet, 375 mgtablet, 500 mg tablet, 375 mg tablet dr)
2-generic
naproxen sodium (550 mg, 275 mg) 2-generic
piroxicam (20 mg, 10 mg) 2-generic
sulindac (200 mg, 150 mg) 2-generic
tolmetin sodium 2-generic
VOLTAREN 4-BRAND
Anesthetics
Local Anestheticslidocaine 5 % oint. (g) 2-generic PA TO CONFIRM PART D COVERAGE
lidocaine 5%(700mg) adh. patch 2-generic PA, QL (90 PER 30 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
4

Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
lidocaine hcl (40 mg/ml solution, 2 %solution, 2 % jel (ml))
2-generic
lidocaine hcl 5 mg/ml vial 5-INJECTABLE
lidocaine hcl/pf 5 mg/ml vial 5-INJECTABLE
lidocaine/prilocaine (2.5 cream (g), 2.5kit)
2-generic PA TO CONFIRM PART D COVERAGE
Anti-Addiction/Substance Abuse Treatment Agents
Alcohol Deterrents/Anti-cravingacamprosate calcium 2-generic PA
disulfiram (500 mg, 250 mg) 2-generic
Opioid Dependence TreatmentsBUPRENORPHINE HCL (0.3 MG/MLVIAL, 0.3 MG/ML SYRINGE)
5-INJECTABLE
buprenorphine hcl (2 mg, 8 mg) 2-generic QL (90 PER 30 DAYS)
buprenorphine hcl/naloxone hcl 2-generic PA, QL (90 PER 30 DAYS)
depade 2-generic
naltrexone hcl 50 mg tablet 2-generic
revia 2-generic
Opioid Reversal Agentsnaloxone hcl 1 mg/ml syringe 5-INJECTABLE
Smoking Cessation AgentsCHANTIX 3-PREF. BRAND
NICOTROL 4-BRAND
NICOTROL NS 4-BRAND
Antibacterials - Drugs to treat bacterial infections
Aminoglycosidesgaramycin 0.3% eye drops 2-generic
gentak (0.3 % ointment, 3 mg/ml drops) 2-generic
gentamicin sulfate (0.3 oint. (g), 0.1 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
5
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
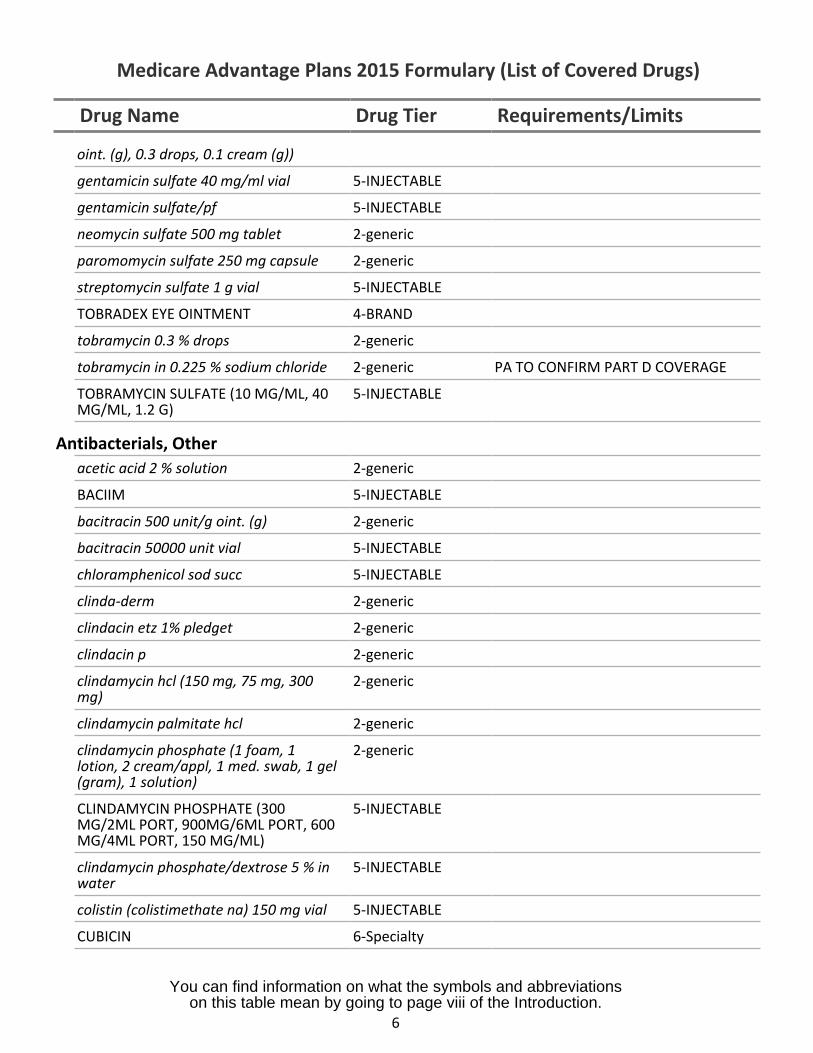
oint. (g), 0.3 drops, 0.1 cream (g))
gentamicin sulfate 40 mg/ml vial 5-INJECTABLE
gentamicin sulfate/pf 5-INJECTABLE
neomycin sulfate 500 mg tablet 2-generic
paromomycin sulfate 250 mg capsule 2-generic
streptomycin sulfate 1 g vial 5-INJECTABLE
TOBRADEX EYE OINTMENT 4-BRAND
tobramycin 0.3 % drops 2-generic
tobramycin in 0.225 % sodium chloride 2-generic PA TO CONFIRM PART D COVERAGE
TOBRAMYCIN SULFATE (10 MG/ML, 40MG/ML, 1.2 G)
5-INJECTABLE
Antibacterials, Otheracetic acid 2 % solution 2-generic
BACIIM 5-INJECTABLE
bacitracin 500 unit/g oint. (g) 2-generic
bacitracin 50000 unit vial 5-INJECTABLE
chloramphenicol sod succ 5-INJECTABLE
clinda-derm 2-generic
clindacin etz 1% pledget 2-generic
clindacin p 2-generic
clindamycin hcl (150 mg, 75 mg, 300mg)
2-generic
clindamycin palmitate hcl 2-generic
clindamycin phosphate (1 foam, 1lotion, 2 cream/appl, 1 med. swab, 1 gel(gram), 1 solution)
2-generic
CLINDAMYCIN PHOSPHATE (300MG/2ML PORT, 900MG/6ML PORT, 600MG/4ML PORT, 150 MG/ML)
5-INJECTABLE
clindamycin phosphate/dextrose 5 % inwater
5-INJECTABLE
colistin (colistimethate na) 150 mg vial 5-INJECTABLE
CUBICIN 6-Specialty
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
6
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
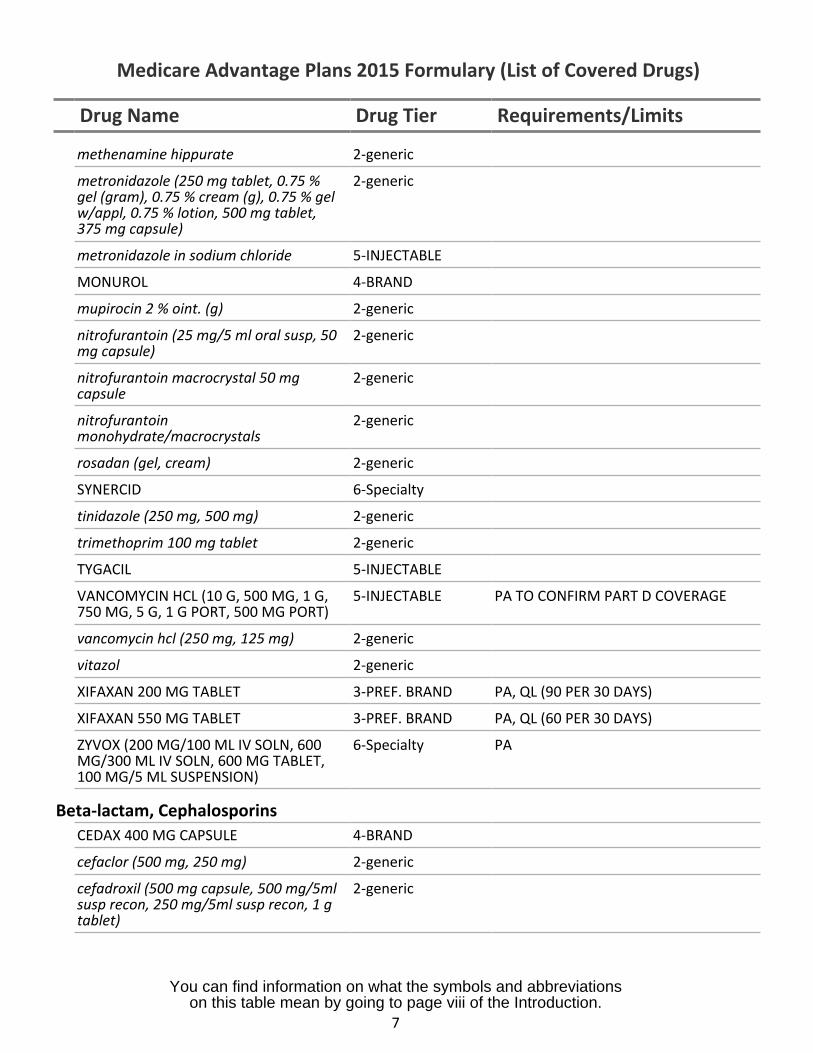
methenamine hippurate 2-generic
metronidazole (250 mg tablet, 0.75 %gel (gram), 0.75 % cream (g), 0.75 % gelw/appl, 0.75 % lotion, 500 mg tablet,375 mg capsule)
2-generic
metronidazole in sodium chloride 5-INJECTABLE
MONUROL 4-BRAND
mupirocin 2 % oint. (g) 2-generic
nitrofurantoin (25 mg/5 ml oral susp, 50mg capsule)
2-generic
nitrofurantoin macrocrystal 50 mgcapsule
2-generic
nitrofurantoinmonohydrate/macrocrystals
2-generic
rosadan (gel, cream) 2-generic
SYNERCID 6-Specialty
tinidazole (250 mg, 500 mg) 2-generic
trimethoprim 100 mg tablet 2-generic
TYGACIL 5-INJECTABLE
VANCOMYCIN HCL (10 G, 500 MG, 1 G,750 MG, 5 G, 1 G PORT, 500 MG PORT)
5-INJECTABLE PA TO CONFIRM PART D COVERAGE
vancomycin hcl (250 mg, 125 mg) 2-generic
vitazol 2-generic
XIFAXAN 200 MG TABLET 3-PREF. BRAND PA, QL (90 PER 30 DAYS)
XIFAXAN 550 MG TABLET 3-PREF. BRAND PA, QL (60 PER 30 DAYS)
ZYVOX (200 MG/100 ML IV SOLN, 600MG/300 ML IV SOLN, 600 MG TABLET,100 MG/5 ML SUSPENSION)
6-Specialty PA
Beta-lactam, CephalosporinsCEDAX 400 MG CAPSULE 4-BRAND
cefaclor (500 mg, 250 mg) 2-generic
cefadroxil (500 mg capsule, 500 mg/5mlsusp recon, 250 mg/5ml susp recon, 1 gtablet)
2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
7
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
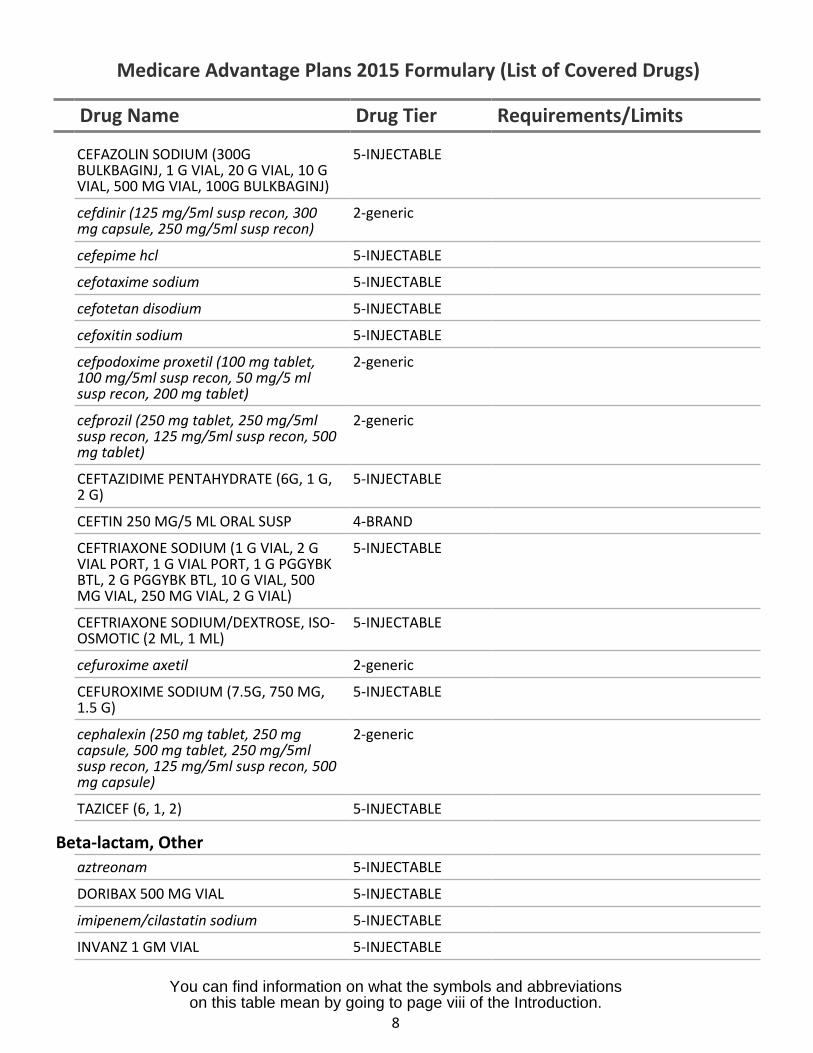
CEFAZOLIN SODIUM (300GBULKBAGINJ, 1 G VIAL, 20 G VIAL, 10 GVIAL, 500 MG VIAL, 100G BULKBAGINJ)
5-INJECTABLE
cefdinir (125 mg/5ml susp recon, 300mg capsule, 250 mg/5ml susp recon)
2-generic
cefepime hcl 5-INJECTABLE
cefotaxime sodium 5-INJECTABLE
cefotetan disodium 5-INJECTABLE
cefoxitin sodium 5-INJECTABLE
cefpodoxime proxetil (100 mg tablet,100 mg/5ml susp recon, 50 mg/5 mlsusp recon, 200 mg tablet)
2-generic
cefprozil (250 mg tablet, 250 mg/5mlsusp recon, 125 mg/5ml susp recon, 500mg tablet)
2-generic
CEFTAZIDIME PENTAHYDRATE (6G, 1 G,2 G)
5-INJECTABLE
CEFTIN 250 MG/5 ML ORAL SUSP 4-BRAND
CEFTRIAXONE SODIUM (1 G VIAL, 2 GVIAL PORT, 1 G VIAL PORT, 1 G PGGYBKBTL, 2 G PGGYBK BTL, 10 G VIAL, 500MG VIAL, 250 MG VIAL, 2 G VIAL)
5-INJECTABLE
CEFTRIAXONE SODIUM/DEXTROSE, ISO-OSMOTIC (2 ML, 1 ML)
5-INJECTABLE
cefuroxime axetil 2-generic
CEFUROXIME SODIUM (7.5G, 750 MG,1.5 G)
5-INJECTABLE
cephalexin (250 mg tablet, 250 mgcapsule, 500 mg tablet, 250 mg/5mlsusp recon, 125 mg/5ml susp recon, 500mg capsule)
2-generic
TAZICEF (6, 1, 2) 5-INJECTABLE
Beta-lactam, Otheraztreonam 5-INJECTABLE
DORIBAX 500 MG VIAL 5-INJECTABLE
imipenem/cilastatin sodium 5-INJECTABLE
INVANZ 1 GM VIAL 5-INJECTABLE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
8
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
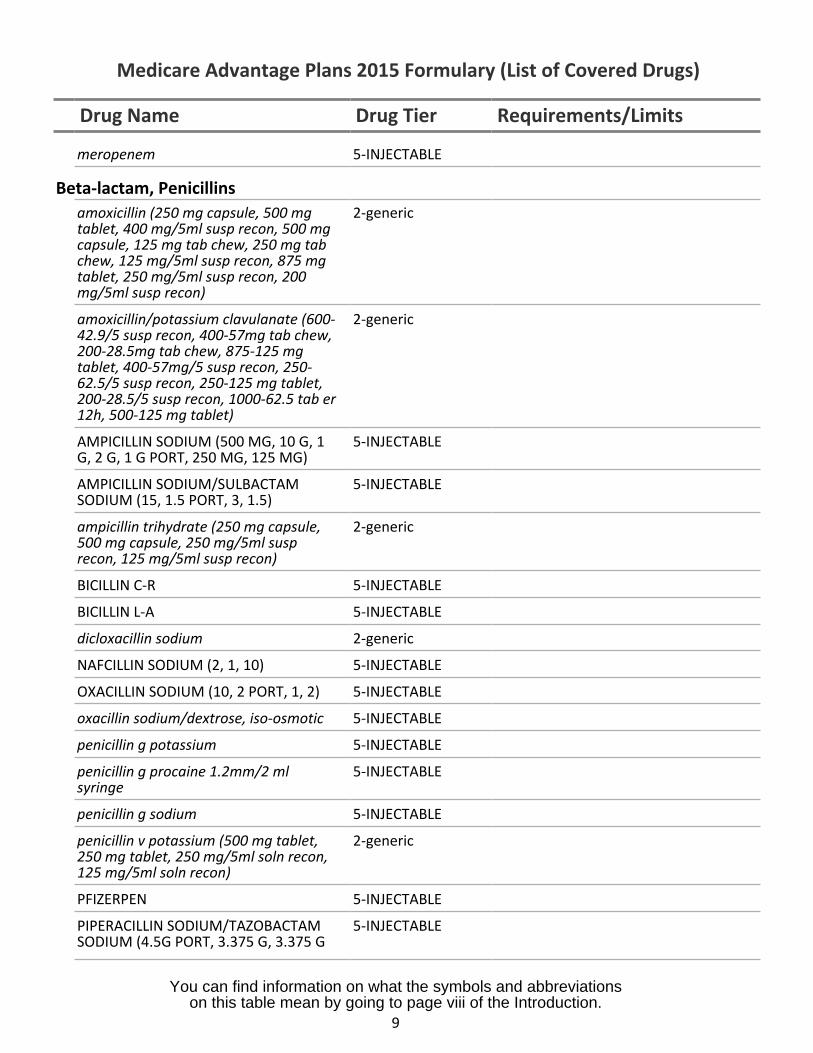
meropenem 5-INJECTABLE
Beta-lactam, Penicillinsamoxicillin (250 mg capsule, 500 mgtablet, 400 mg/5ml susp recon, 500 mgcapsule, 125 mg tab chew, 250 mg tabchew, 125 mg/5ml susp recon, 875 mgtablet, 250 mg/5ml susp recon, 200mg/5ml susp recon)
2-generic
amoxicillin/potassium clavulanate (600-42.9/5 susp recon, 400-57mg tab chew,200-28.5mg tab chew, 875-125 mgtablet, 400-57mg/5 susp recon, 250-62.5/5 susp recon, 250-125 mg tablet,200-28.5/5 susp recon, 1000-62.5 tab er12h, 500-125 mg tablet)
2-generic
AMPICILLIN SODIUM (500 MG, 10 G, 1G, 2 G, 1 G PORT, 250 MG, 125 MG)
5-INJECTABLE
AMPICILLIN SODIUM/SULBACTAMSODIUM (15, 1.5 PORT, 3, 1.5)
5-INJECTABLE
ampicillin trihydrate (250 mg capsule,500 mg capsule, 250 mg/5ml susprecon, 125 mg/5ml susp recon)
2-generic
BICILLIN C-R 5-INJECTABLE
BICILLIN L-A 5-INJECTABLE
dicloxacillin sodium 2-generic
NAFCILLIN SODIUM (2, 1, 10) 5-INJECTABLE
OXACILLIN SODIUM (10, 2 PORT, 1, 2) 5-INJECTABLE
oxacillin sodium/dextrose, iso-osmotic 5-INJECTABLE
penicillin g potassium 5-INJECTABLE
penicillin g procaine 1.2mm/2 mlsyringe
5-INJECTABLE
penicillin g sodium 5-INJECTABLE
penicillin v potassium (500 mg tablet,250 mg tablet, 250 mg/5ml soln recon,125 mg/5ml soln recon)
2-generic
PFIZERPEN 5-INJECTABLE
PIPERACILLIN SODIUM/TAZOBACTAMSODIUM (4.5G PORT, 3.375 G, 3.375 G
5-INJECTABLE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
9
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
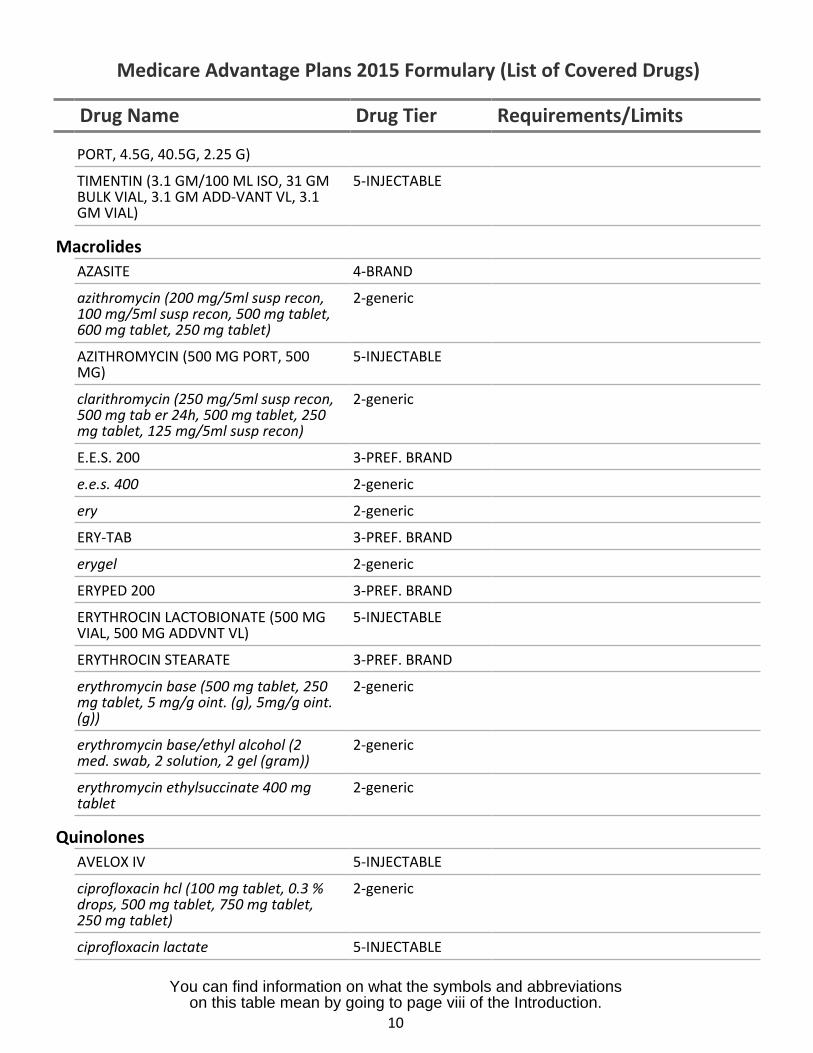
PORT, 4.5G, 40.5G, 2.25 G)
TIMENTIN (3.1 GM/100 ML ISO, 31 GMBULK VIAL, 3.1 GM ADD-VANT VL, 3.1GM VIAL)
5-INJECTABLE
MacrolidesAZASITE 4-BRAND
azithromycin (200 mg/5ml susp recon,100 mg/5ml susp recon, 500 mg tablet,600 mg tablet, 250 mg tablet)
2-generic
AZITHROMYCIN (500 MG PORT, 500MG)
5-INJECTABLE
clarithromycin (250 mg/5ml susp recon,500 mg tab er 24h, 500 mg tablet, 250mg tablet, 125 mg/5ml susp recon)
2-generic
E.E.S. 200 3-PREF. BRAND
e.e.s. 400 2-generic
ery 2-generic
ERY-TAB 3-PREF. BRAND
erygel 2-generic
ERYPED 200 3-PREF. BRAND
ERYTHROCIN LACTOBIONATE (500 MGVIAL, 500 MG ADDVNT VL)
5-INJECTABLE
ERYTHROCIN STEARATE 3-PREF. BRAND
erythromycin base (500 mg tablet, 250mg tablet, 5 mg/g oint. (g), 5mg/g oint.(g))
2-generic
erythromycin base/ethyl alcohol (2med. swab, 2 solution, 2 gel (gram))
2-generic
erythromycin ethylsuccinate 400 mgtablet
2-generic
QuinolonesAVELOX IV 5-INJECTABLE
ciprofloxacin hcl (100 mg tablet, 0.3 %drops, 500 mg tablet, 750 mg tablet,250 mg tablet)
2-generic
ciprofloxacin lactate 5-INJECTABLE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
10
Drug Name Drug Tier Requirements/Limits
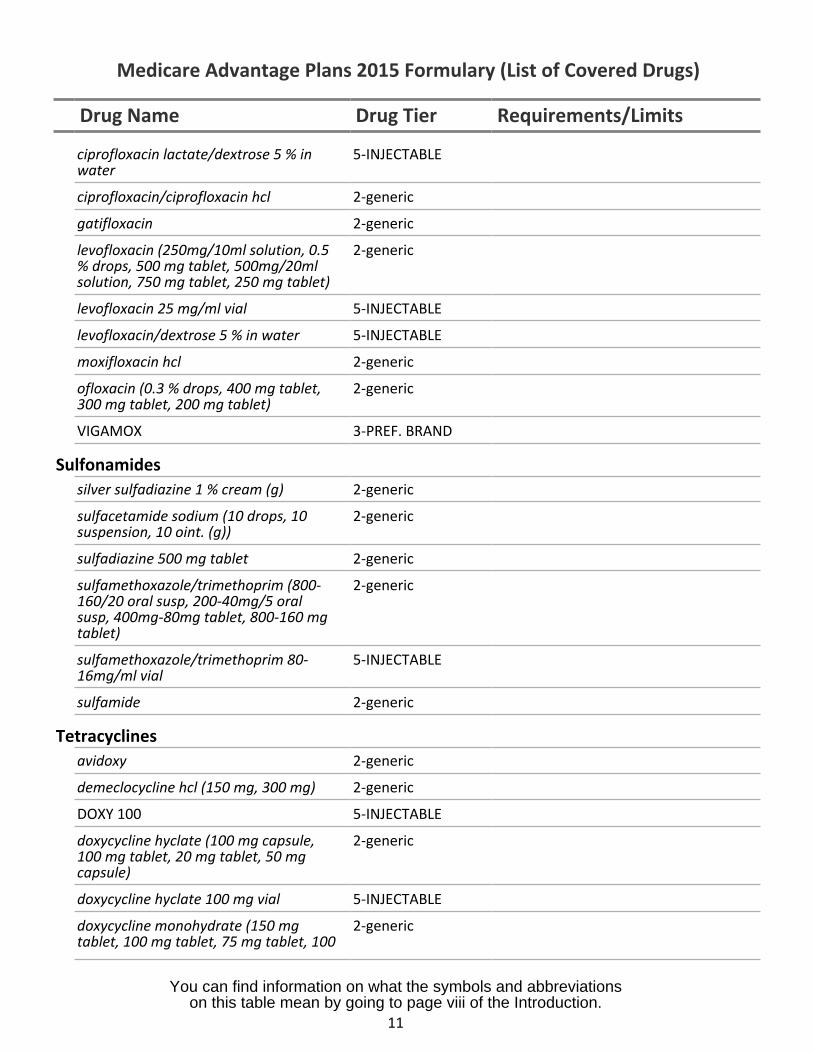
ciprofloxacin lactate/dextrose 5 % inwater
5-INJECTABLE
ciprofloxacin/ciprofloxacin hcl 2-generic
gatifloxacin 2-generic
levofloxacin (250mg/10ml solution, 0.5% drops, 500 mg tablet, 500mg/20mlsolution, 750 mg tablet, 250 mg tablet)
2-generic
levofloxacin 25 mg/ml vial 5-INJECTABLE
levofloxacin/dextrose 5 % in water 5-INJECTABLE
moxifloxacin hcl 2-generic
ofloxacin (0.3 % drops, 400 mg tablet,300 mg tablet, 200 mg tablet)
2-generic
VIGAMOX 3-PREF. BRAND
Sulfonamidessilver sulfadiazine 1 % cream (g) 2-generic
sulfacetamide sodium (10 drops, 10suspension, 10 oint. (g))
2-generic
sulfadiazine 500 mg tablet 2-generic
sulfamethoxazole/trimethoprim (800-160/20 oral susp, 200-40mg/5 oralsusp, 400mg-80mg tablet, 800-160 mgtablet)
2-generic
sulfamethoxazole/trimethoprim 80-16mg/ml vial
5-INJECTABLE
sulfamide 2-generic
Tetracyclinesavidoxy 2-generic
demeclocycline hcl (150 mg, 300 mg) 2-generic
DOXY 100 5-INJECTABLE
doxycycline hyclate (100 mg capsule,100 mg tablet, 20 mg tablet, 50 mgcapsule)
2-generic
doxycycline hyclate 100 mg vial 5-INJECTABLE
doxycycline monohydrate (150 mgtablet, 100 mg tablet, 75 mg tablet, 100
2-generic
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
11
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
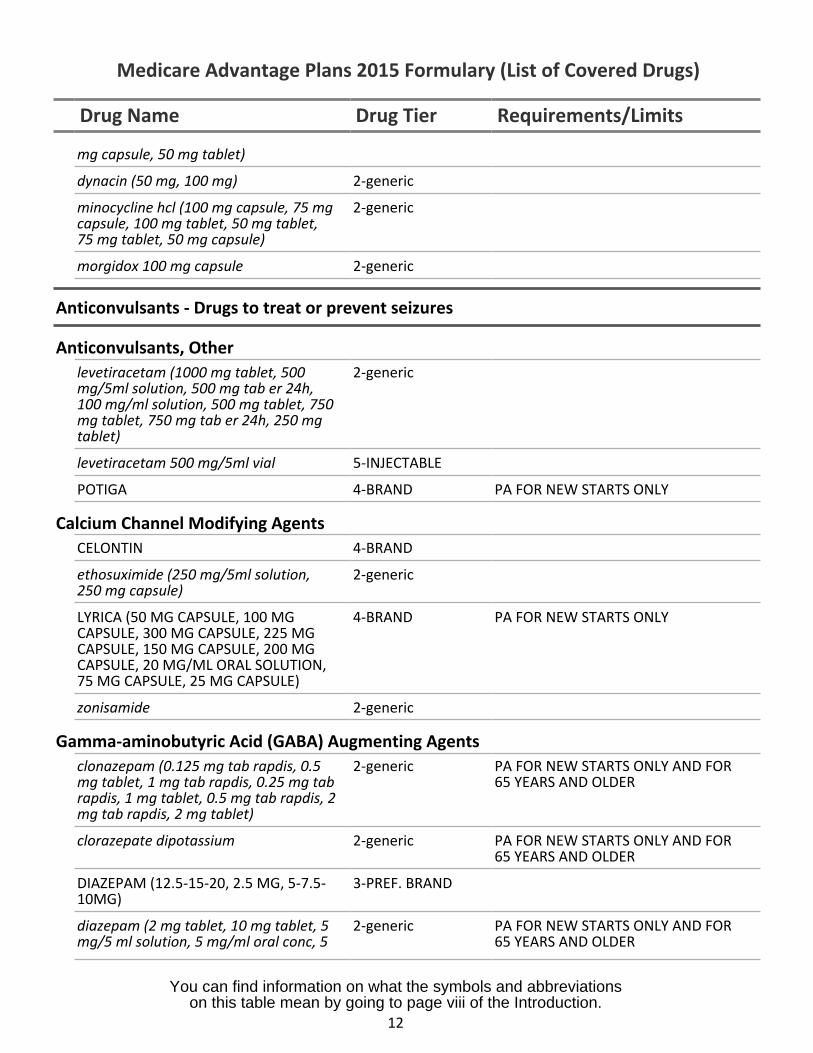
mg capsule, 50 mg tablet)
dynacin (50 mg, 100 mg) 2-generic
minocycline hcl (100 mg capsule, 75 mg 2-genericcapsule, 100 mg tablet, 50 mg tablet,75 mg tablet, 50 mg capsule)
morgidox 100 mg capsule 2-generic
Anticonvulsants - Drugs to treat or prevent seizures
Anticonvulsants, Otherlevetiracetam (1000 mg tablet, 500 2-genericmg/5ml solution, 500 mg tab er 24h,100 mg/ml solution, 500 mg tablet, 750mg tablet, 750 mg tab er 24h, 250 mgtablet)
levetiracetam 500 mg/5ml vial 5-INJECTABLE
POTIGA 4-BRAND PA FOR NEW STARTS ONLY
Calcium Channel Modifying AgentsCELONTIN 4-BRAND
ethosuximide (250 mg/5ml solution, 2-generic250 mg capsule)
LYRICA (50 MG CAPSULE, 100 MG 4-BRAND PA FOR NEW STARTS ONLYCAPSULE, 300 MG CAPSULE, 225 MGCAPSULE, 150 MG CAPSULE, 200 MGCAPSULE, 20 MG/ML ORAL SOLUTION,75 MG CAPSULE, 25 MG CAPSULE)
zonisamide 2-generic
Gamma-aminobutyric Acid (GABA) Augmenting Agentsclonazepam (0.125 mg tab rapdis, 0.5 2-generic PA FOR NEW STARTS ONLY AND FORmg tablet, 1 mg tab rapdis, 0.25 mg tab 65 YEARS AND OLDERrapdis, 1 mg tablet, 0.5 mg tab rapdis, 2mg tab rapdis, 2 mg tablet)
clorazepate dipotassium 2-generic PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER
DIAZEPAM (12.5-15-20, 2.5 MG, 5-7.5- 3-PREF. BRAND10MG)
diazepam (2 mg tablet, 10 mg tablet, 5 2-generic PA FOR NEW STARTS ONLY AND FORmg/5 ml solution, 5 mg/ml oral conc, 5 65 YEARS AND OLDER
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
12
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
mg tablet)
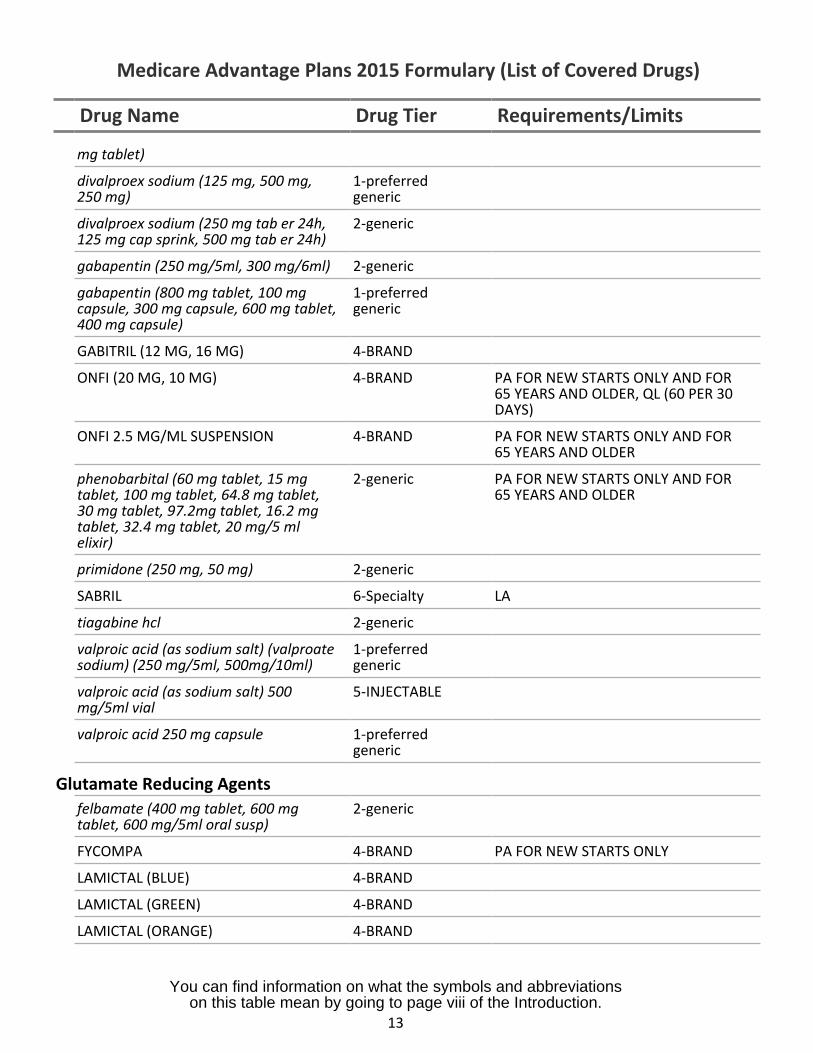
divalproex sodium (125 mg, 500 mg,250 mg)
1-preferredgeneric
divalproex sodium (250 mg tab er 24h,125 mg cap sprink, 500 mg tab er 24h)
2-generic
gabapentin (250 mg/5ml, 300 mg/6ml) 2-generic
gabapentin (800 mg tablet, 100 mgcapsule, 300 mg capsule, 600 mg tablet,400 mg capsule)
1-preferredgeneric
GABITRIL (12 MG, 16 MG) 4-BRAND
ONFI (20 MG, 10 MG) 4-BRAND PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER, QL (60 PER 30DAYS)
ONFI 2.5 MG/ML SUSPENSION 4-BRAND PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER
phenobarbital (60 mg tablet, 15 mgtablet, 100 mg tablet, 64.8 mg tablet,30 mg tablet, 97.2mg tablet, 16.2 mgtablet, 32.4 mg tablet, 20 mg/5 mlelixir)
2-generic PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER
primidone (250 mg, 50 mg) 2-generic
SABRIL 6-Specialty LA
tiagabine hcl 2-generic
valproic acid (as sodium salt) (valproatesodium) (250 mg/5ml, 500mg/10ml)
1-preferredgeneric
valproic acid (as sodium salt) 500mg/5ml vial
5-INJECTABLE
valproic acid 250 mg capsule 1-preferredgeneric
Glutamate Reducing Agentsfelbamate (400 mg tablet, 600 mgtablet, 600 mg/5ml oral susp)
2-generic
FYCOMPA 4-BRAND PA FOR NEW STARTS ONLY
LAMICTAL (BLUE) 4-BRAND
LAMICTAL (GREEN) 4-BRAND
LAMICTAL (ORANGE) 4-BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
13
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
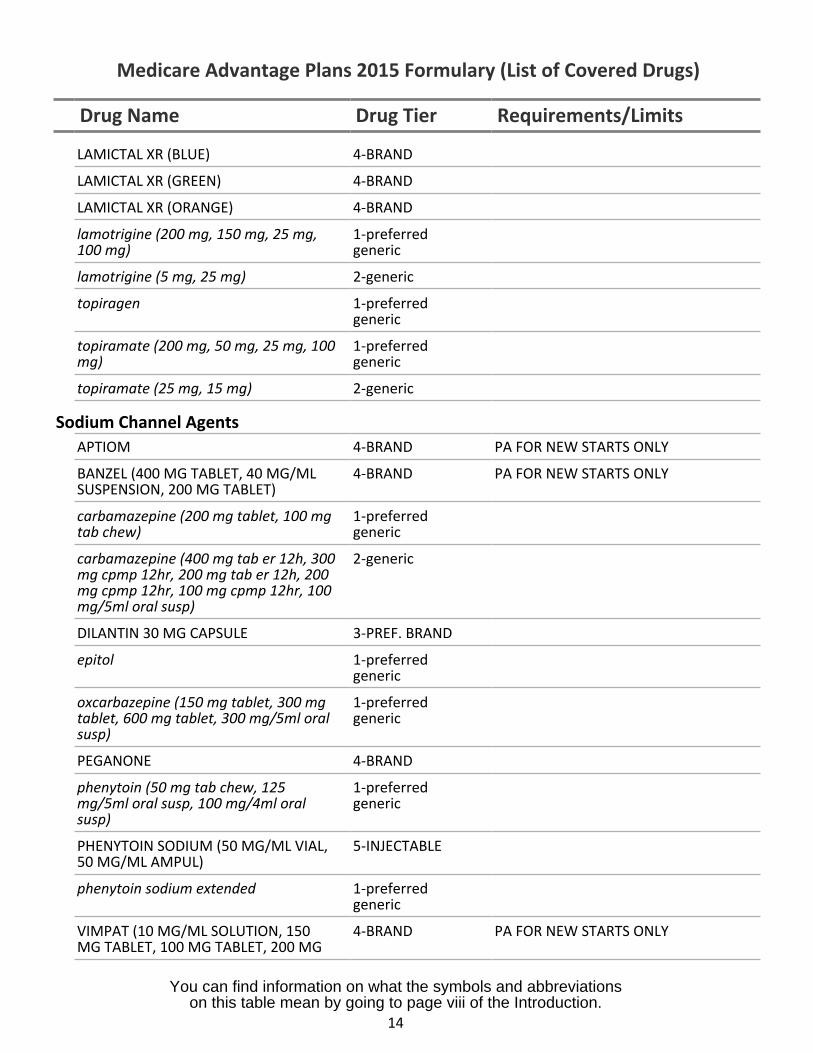
LAMICTAL XR (BLUE) 4-BRAND
LAMICTAL XR (GREEN) 4-BRAND
LAMICTAL XR (ORANGE) 4-BRAND
lamotrigine (200 mg, 150 mg, 25 mg,100 mg)
1-preferredgeneric
lamotrigine (5 mg, 25 mg) 2-generic
topiragen 1-preferredgeneric
topiramate (200 mg, 50 mg, 25 mg, 100mg)
1-preferredgeneric
topiramate (25 mg, 15 mg) 2-generic
Sodium Channel AgentsAPTIOM 4-BRAND PA FOR NEW STARTS ONLY
BANZEL (400 MG TABLET, 40 MG/MLSUSPENSION, 200 MG TABLET)
4-BRAND PA FOR NEW STARTS ONLY
carbamazepine (200 mg tablet, 100 mgtab chew)
1-preferredgeneric
carbamazepine (400 mg tab er 12h, 300mg cpmp 12hr, 200 mg tab er 12h, 200mg cpmp 12hr, 100 mg cpmp 12hr, 100mg/5ml oral susp)
2-generic
DILANTIN 30 MG CAPSULE 3-PREF. BRAND
epitol 1-preferredgeneric
oxcarbazepine (150 mg tablet, 300 mgtablet, 600 mg tablet, 300 mg/5ml oralsusp)
1-preferredgeneric
PEGANONE 4-BRAND
phenytoin (50 mg tab chew, 125mg/5ml oral susp, 100 mg/4ml oralsusp)
1-preferredgeneric
PHENYTOIN SODIUM (50 MG/ML VIAL,50 MG/ML AMPUL)
5-INJECTABLE
phenytoin sodium extended 1-preferredgeneric
VIMPAT (10 MG/ML SOLUTION, 150MG TABLET, 100 MG TABLET, 200 MG
4-BRAND PA FOR NEW STARTS ONLY
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
14
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
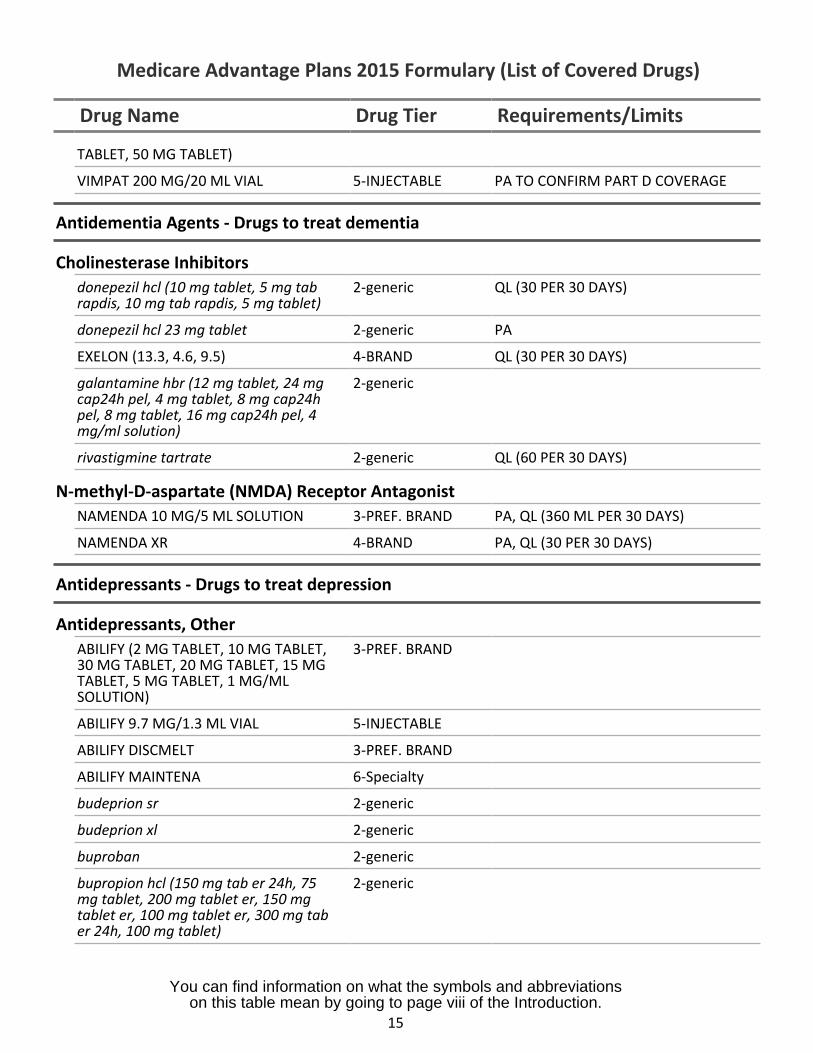
TABLET, 50 MG TABLET)
VIMPAT 200 MG/20 ML VIAL 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
Antidementia Agents - Drugs to treat dementia
Cholinesterase Inhibitorsdonepezil hcl (10 mg tablet, 5 mg tab 2-genericrapdis, 10 mg tab rapdis, 5 mg tablet)
QL (30 PER 30 DAYS)
donepezil hcl 23 mg tablet 2-generic PA
EXELON (13.3, 4.6, 9.5) 4-BRAND QL (30 PER 30 DAYS)
galantamine hbr (12 mg tablet, 24 mg 2-genericcap24h pel, 4 mg tablet, 8 mg cap24hpel, 8 mg tablet, 16 mg cap24h pel, 4mg/ml solution)
rivastigmine tartrate 2-generic QL (60 PER 30 DAYS)
N-methyl-D-aspartate (NMDA) Receptor AntagonistNAMENDA 10 MG/5 ML SOLUTION 3-PREF. BRAND PA, QL (360 ML PER 30 DAYS)
NAMENDA XR 4-BRAND PA, QL (30 PER 30 DAYS)
Antidepressants - Drugs to treat depression
Antidepressants, OtherABILIFY (2 MG TABLET, 10 MG TABLET,30 MG TABLET, 20 MG TABLET, 15 MGTABLET, 5 MG TABLET, 1 MG/MLSOLUTION)
3-PREF. BRAND
ABILIFY 9.7 MG/1.3 ML VIAL 5-INJECTABLE
ABILIFY DISCMELT 3-PREF. BRAND
ABILIFY MAINTENA 6-Specialty
budeprion sr 2-generic
budeprion xl 2-generic
buproban 2-generic
bupropion hcl (150 mg tab er 24h, 75mg tablet, 200 mg tablet er, 150 mgtablet er, 100 mg tablet er, 300 mg taber 24h, 100 mg tablet)
2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
15
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier
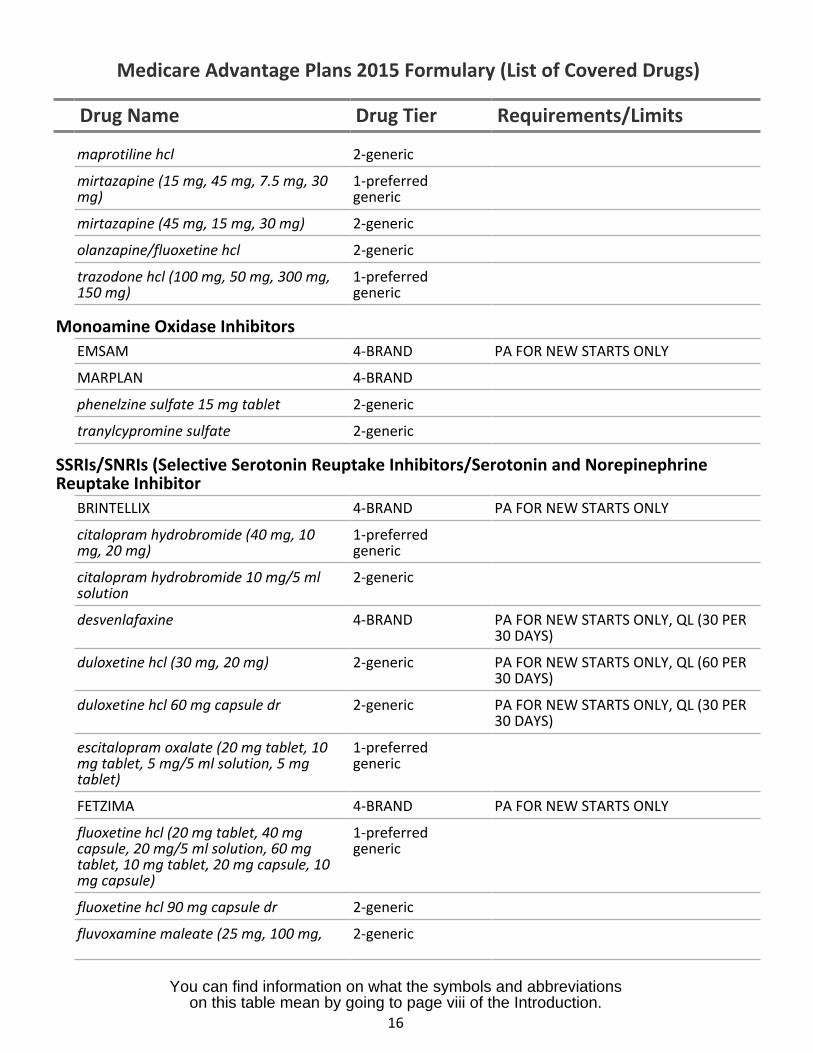
maprotiline hcl 2-generic
mirtazapine (15 mg, 45 mg, 7.5 mg, 30 1-preferred
Requirements/Limits
mg) generic
mirtazapine (45 mg, 15 mg, 30 mg) 2-generic
olanzapine/fluoxetine hcl 2-generic
trazodone hcl (100 mg, 50 mg, 300 mg, 1-preferred150 mg) generic
Monoamine Oxidase InhibitorsEMSAM 4-BRAND
MARPLAN 4-BRAND
phenelzine sulfate 15 mg tablet 2-generic
tranylcypromine sulfate 2-generic
SSRIs/SNRIs (Selective Serotonin Reuptake Inhibitors
PA FOR NEW STARTS ONLY
/Serotonin and NorepinephrineReuptake Inhibitor
BRINTELLIX 4-BRAND PA FOR NEW STARTS ONLY
citalopram hydrobromide (40 mg, 10 1-preferredmg, 20 mg) generic
citalopram hydrobromide 10 mg/5 ml 2-genericsolution
desvenlafaxine 4-BRAND PA FOR NEW STARTS ONLY, QL (30 PER30 DAYS)
duloxetine hcl (30 mg, 20 mg) 2-generic PA FOR NEW STARTS ONLY, QL (60 PER30 DAYS)
duloxetine hcl 60 mg capsule dr 2-generic PA FOR NEW STARTS ONLY, QL (30 PER30 DAYS)
escitalopram oxalate (20 mg tablet, 10 1-preferredmg tablet, 5 mg/5 ml solution, 5 mg generictablet)
FETZIMA 4-BRAND PA FOR NEW STARTS ONLY
fluoxetine hcl (20 mg tablet, 40 mg 1-preferredcapsule, 20 mg/5 ml solution, 60 mg generictablet, 10 mg tablet, 20 mg capsule, 10mg capsule)
fluoxetine hcl 90 mg capsule dr 2-generic
fluvoxamine maleate (25 mg, 100 mg, 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
16
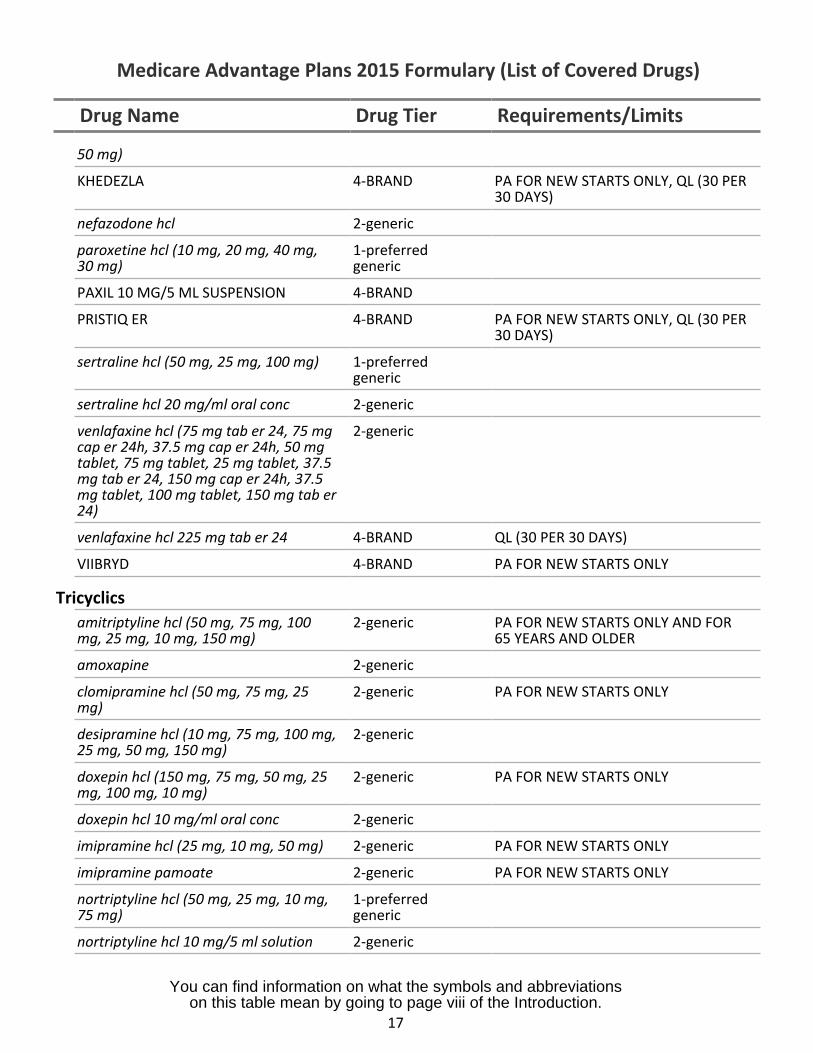
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
50 mg)
KHEDEZLA 4-BRAND PA FOR NEW STARTS ONLY, QL (30 PER30 DAYS)
nefazodone hcl 2-generic
paroxetine hcl (10 mg, 20 mg, 40 mg, 1-preferred30 mg) generic
PAXIL 10 MG/5 ML SUSPENSION 4-BRAND
PRISTIQ ER 4-BRAND PA FOR NEW STARTS ONLY, QL (30 PER30 DAYS)
sertraline hcl (50 mg, 25 mg, 100 mg) 1-preferredgeneric
sertraline hcl 20 mg/ml oral conc 2-generic
venlafaxine hcl (75 mg tab er 24, 75 mg 2-genericcap er 24h, 37.5 mg cap er 24h, 50 mgtablet, 75 mg tablet, 25 mg tablet, 37.5mg tab er 24, 150 mg cap er 24h, 37.5mg tablet, 100 mg tablet, 150 mg tab er24)
venlafaxine hcl 225 mg tab er 24 4-BRAND QL (30 PER 30 DAYS)
VIIBRYD 4-BRAND PA FOR NEW STARTS ONLY
Tricyclicsamitriptyline hcl (50 mg, 75 mg, 100 2-generic PA FOR NEW STARTS ONLY AND FORmg, 25 mg, 10 mg, 150 mg) 65 YEARS AND OLDER
amoxapine 2-generic
clomipramine hcl (50 mg, 75 mg, 25 2-generic PA FOR NEW STARTS ONLYmg)
desipramine hcl (10 mg, 75 mg, 100 mg, 2-generic25 mg, 50 mg, 150 mg)
doxepin hcl (150 mg, 75 mg, 50 mg, 25 2-generic PA FOR NEW STARTS ONLYmg, 100 mg, 10 mg)
doxepin hcl 10 mg/ml oral conc 2-generic
imipramine hcl (25 mg, 10 mg, 50 mg) 2-generic PA FOR NEW STARTS ONLY
imipramine pamoate 2-generic PA FOR NEW STARTS ONLY
nortriptyline hcl (50 mg, 25 mg, 10 mg, 1-preferred75 mg) generic
nortriptyline hcl 10 mg/5 ml solution 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
17
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
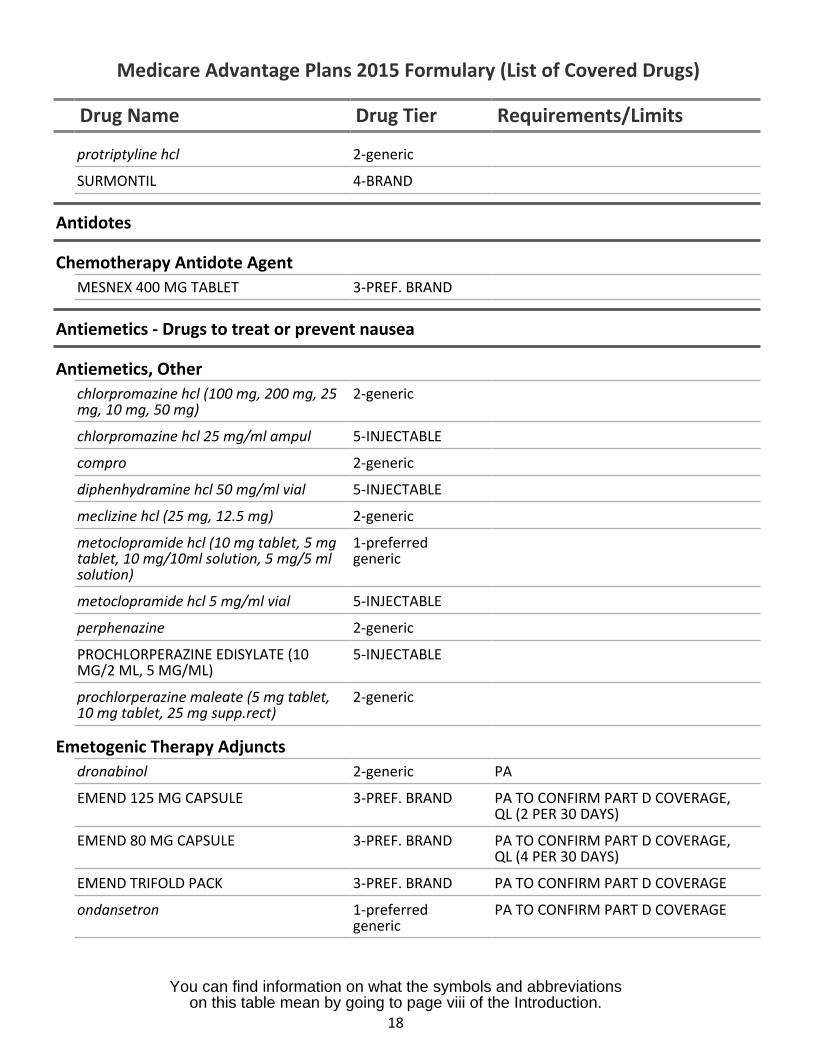
protriptyline hcl 2-generic
SURMONTIL 4-BRAND
Antidotes
Chemotherapy Antidote AgentMESNEX 400 MG TABLET 3-PREF. BRAND
Antiemetics - Drugs to treat or prevent nausea
Antiemetics, Otherchlorpromazine hcl (100 mg, 200 mg, 25mg, 10 mg, 50 mg)
2-generic
chlorpromazine hcl 25 mg/ml ampul 5-INJECTABLE
compro 2-generic
diphenhydramine hcl 50 mg/ml vial 5-INJECTABLE
meclizine hcl (25 mg, 12.5 mg) 2-generic
metoclopramide hcl (10 mg tablet, 5 mgtablet, 10 mg/10ml solution, 5 mg/5 mlsolution)
1-preferredgeneric
metoclopramide hcl 5 mg/ml vial 5-INJECTABLE
perphenazine 2-generic
PROCHLORPERAZINE EDISYLATE (10MG/2 ML, 5 MG/ML)
5-INJECTABLE
prochlorperazine maleate (5 mg tablet,10 mg tablet, 25 mg supp.rect)
2-generic
Emetogenic Therapy Adjunctsdronabinol 2-generic PA
EMEND 125 MG CAPSULE 3-PREF. BRAND PA TO CONFIRM PART D COVERAGE,QL (2 PER 30 DAYS)
EMEND 80 MG CAPSULE 3-PREF. BRAND PA TO CONFIRM PART D COVERAGE,QL (4 PER 30 DAYS)
EMEND TRIFOLD PACK 3-PREF. BRAND PA TO CONFIRM PART D COVERAGE
ondansetron 1-preferredgeneric
PA TO CONFIRM PART D COVERAGE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
18
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
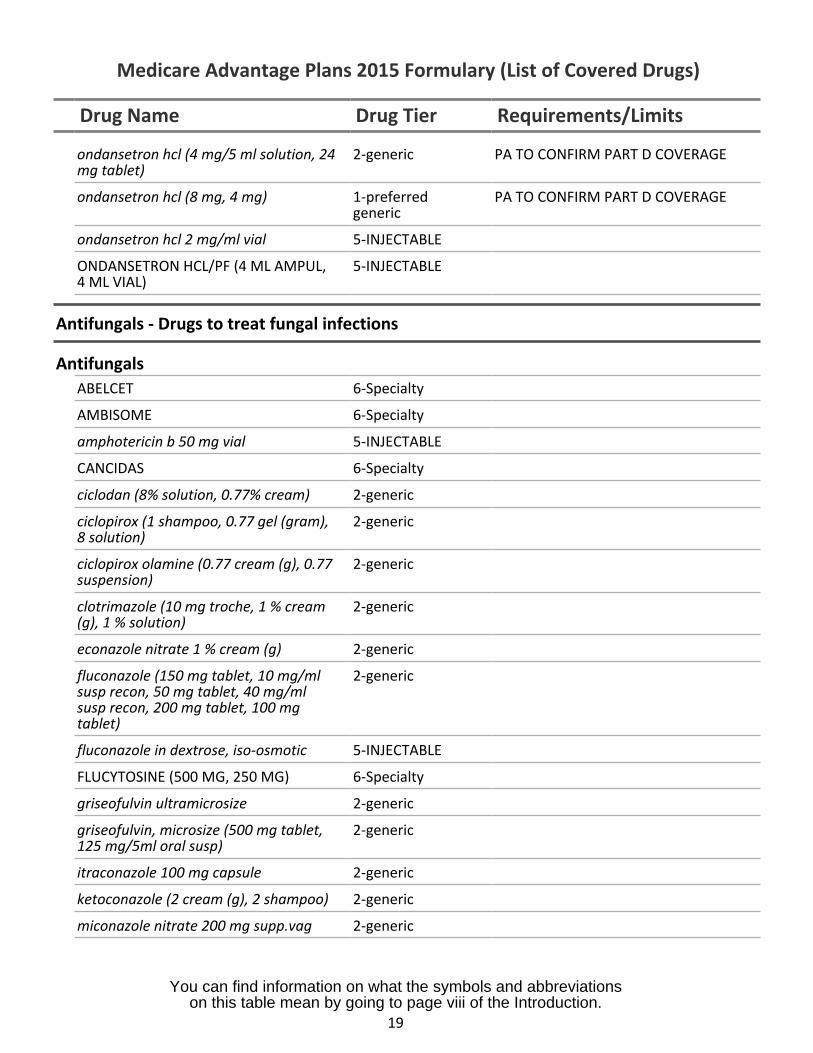
ondansetron hcl (4 mg/5 ml solution, 24mg tablet)
2-generic PA TO CONFIRM PART D COVERAGE
ondansetron hcl (8 mg, 4 mg) 1-preferredgeneric
PA TO CONFIRM PART D COVERAGE
ondansetron hcl 2 mg/ml vial 5-INJECTABLE
ONDANSETRON HCL/PF (4 ML AMPUL,4 ML VIAL)
5-INJECTABLE
Antifungals - Drugs to treat fungal infections
AntifungalsABELCET 6-Specialty
AMBISOME 6-Specialty
amphotericin b 50 mg vial 5-INJECTABLE
CANCIDAS 6-Specialty
ciclodan (8% solution, 0.77% cream) 2-generic
ciclopirox (1 shampoo, 0.77 gel (gram),8 solution)
2-generic
ciclopirox olamine (0.77 cream (g), 0.77suspension)
2-generic
clotrimazole (10 mg troche, 1 % cream(g), 1 % solution)
2-generic
econazole nitrate 1 % cream (g) 2-generic
fluconazole (150 mg tablet, 10 mg/mlsusp recon, 50 mg tablet, 40 mg/mlsusp recon, 200 mg tablet, 100 mgtablet)
2-generic
fluconazole in dextrose, iso-osmotic 5-INJECTABLE
FLUCYTOSINE (500 MG, 250 MG) 6-Specialty
griseofulvin ultramicrosize 2-generic
griseofulvin, microsize (500 mg tablet,125 mg/5ml oral susp)
2-generic
itraconazole 100 mg capsule 2-generic
ketoconazole (2 cream (g), 2 shampoo) 2-generic
miconazole nitrate 200 mg supp.vag 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
19
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
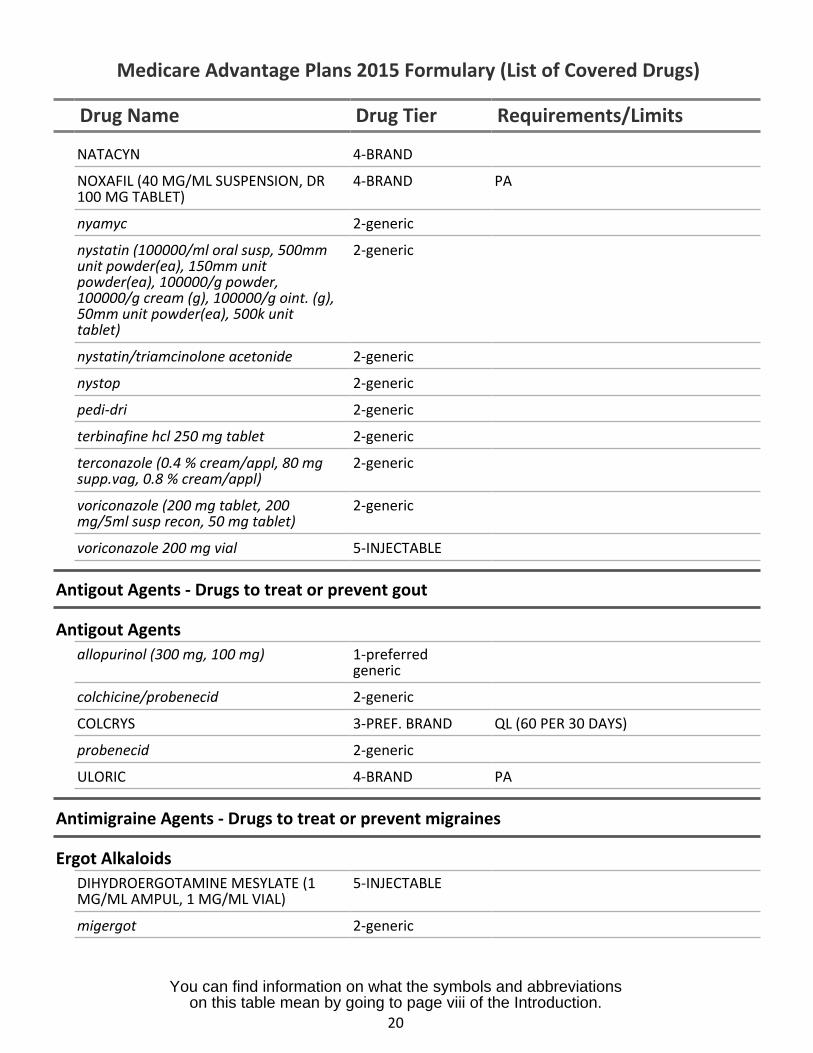
NATACYN 4-BRAND
NOXAFIL (40 MG/ML SUSPENSION, DR100 MG TABLET)
4-BRAND PA
nyamyc 2-generic
nystatin (100000/ml oral susp, 500mmunit powder(ea), 150mm unitpowder(ea), 100000/g powder,100000/g cream (g), 100000/g oint. (g),50mm unit powder(ea), 500k unittablet)
2-generic
nystatin/triamcinolone acetonide 2-generic
nystop 2-generic
pedi-dri 2-generic
terbinafine hcl 250 mg tablet 2-generic
terconazole (0.4 % cream/appl, 80 mgsupp.vag, 0.8 % cream/appl)
2-generic
voriconazole (200 mg tablet, 200mg/5ml susp recon, 50 mg tablet)
2-generic
voriconazole 200 mg vial 5-INJECTABLE
Antigout Agents - Drugs to treat or prevent gout
Antigout Agentsallopurinol (300 mg, 100 mg) 1-preferred
generic
colchicine/probenecid 2-generic
COLCRYS 3-PREF. BRAND QL (60 PER 30 DAYS)
probenecid 2-generic
ULORIC 4-BRAND PA
Antimigraine Agents - Drugs to treat or prevent migraines
Ergot AlkaloidsDIHYDROERGOTAMINE MESYLATE (1MG/ML AMPUL, 1 MG/ML VIAL)
5-INJECTABLE
migergot 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
20
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
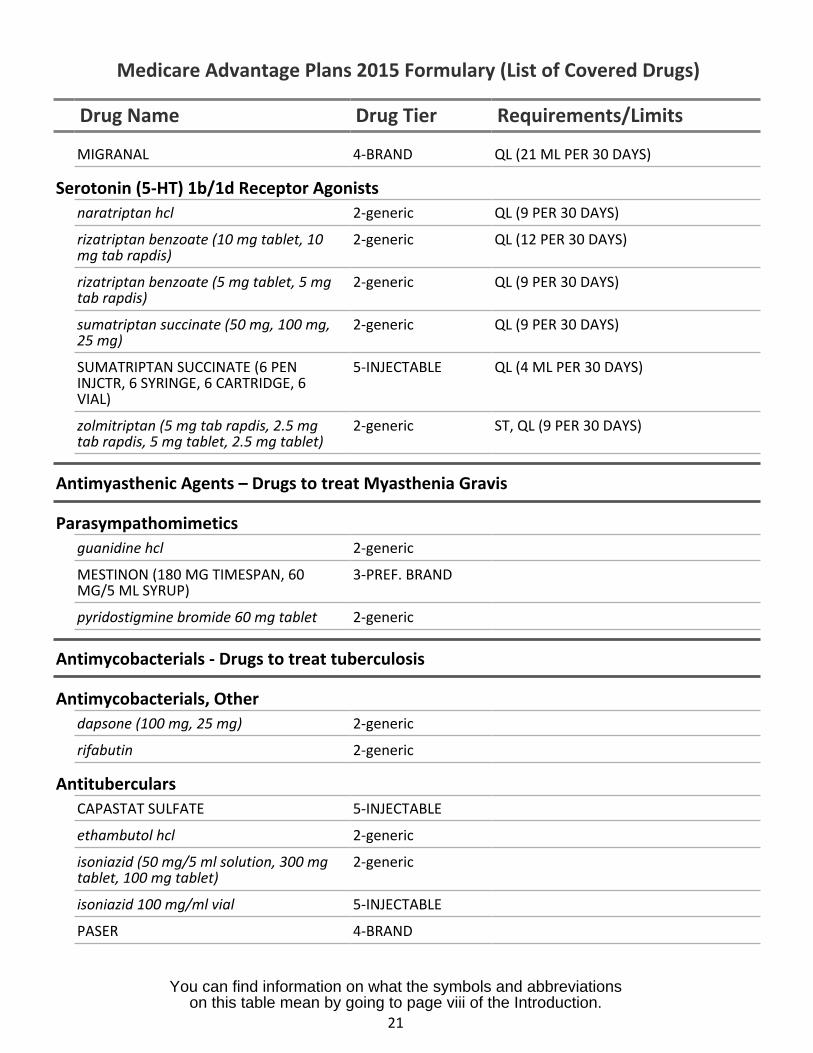
MIGRANAL 4-BRAND QL (21 ML PER 30 DAYS)
Serotonin (5-HT) 1b/1d Receptor Agonistsnaratriptan hcl 2-generic QL (9 PER 30 DAYS)
rizatriptan benzoate (10 mg tablet, 10 2-generic QL (12 PER 30 DAYS)mg tab rapdis)
rizatriptan benzoate (5 mg tablet, 5 mg 2-generic QL (9 PER 30 DAYS)tab rapdis)
sumatriptan succinate (50 mg, 100 mg, 2-generic QL (9 PER 30 DAYS)25 mg)
SUMATRIPTAN SUCCINATE (6 PEN 5-INJECTABLE QL (4 ML PER 30 DAYS)INJCTR, 6 SYRINGE, 6 CARTRIDGE, 6VIAL)
zolmitriptan (5 mg tab rapdis, 2.5 mg 2-generic ST, QL (9 PER 30 DAYS)tab rapdis, 5 mg tablet, 2.5 mg tablet)
Antimyasthenic Agents – Drugs to treat Myasthenia Gravis
Parasympathomimeticsguanidine hcl 2-generic
MESTINON (180 MG TIMESPAN, 60 3-PREF. BRANDMG/5 ML SYRUP)
pyridostigmine bromide 60 mg tablet 2-generic
Antimycobacterials - Drugs to treat tuberculosis
Antimycobacterials, Otherdapsone (100 mg, 25 mg) 2-generic
rifabutin 2-generic
AntitubercularsCAPASTAT SULFATE 5-INJECTABLE
ethambutol hcl 2-generic
isoniazid (50 mg/5 ml solution, 300 mg 2-generictablet, 100 mg tablet)
isoniazid 100 mg/ml vial 5-INJECTABLE
PASER 4-BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
21
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
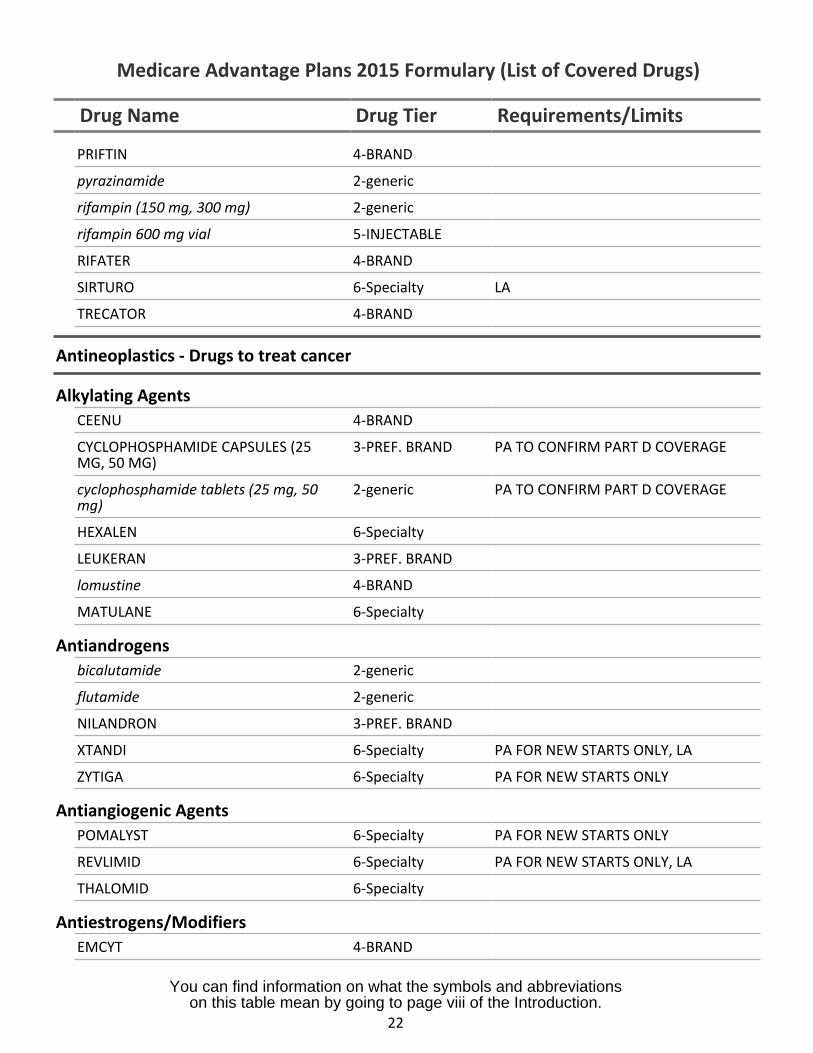
PRIFTIN 4-BRAND
pyrazinamide 2-generic
rifampin (150 mg, 300 mg) 2-generic
rifampin 600 mg vial 5-INJECTABLE
RIFATER 4-BRAND
SIRTURO 6-Specialty LA
TRECATOR 4-BRAND
Antineoplastics - Drugs to treat cancer
Alkylating AgentsCEENU 4-BRAND
CYCLOPHOSPHAMIDE CAPSULES (25MG, 50 MG)
3-PREF. BRAND PA TO CONFIRM PART D COVERAGE
cyclophosphamide tablets (25 mg, 50mg)
2-generic PA TO CONFIRM PART D COVERAGE
HEXALEN 6-Specialty
LEUKERAN 3-PREF. BRAND
lomustine 4-BRAND
MATULANE 6-Specialty
Antiandrogensbicalutamide 2-generic
flutamide 2-generic
NILANDRON 3-PREF. BRAND
XTANDI 6-Specialty PA FOR NEW STARTS ONLY, LA
ZYTIGA 6-Specialty PA FOR NEW STARTS ONLY
Antiangiogenic AgentsPOMALYST 6-Specialty PA FOR NEW STARTS ONLY
REVLIMID 6-Specialty PA FOR NEW STARTS ONLY, LA
THALOMID 6-Specialty
Antiestrogens/ModifiersEMCYT 4-BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
22
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
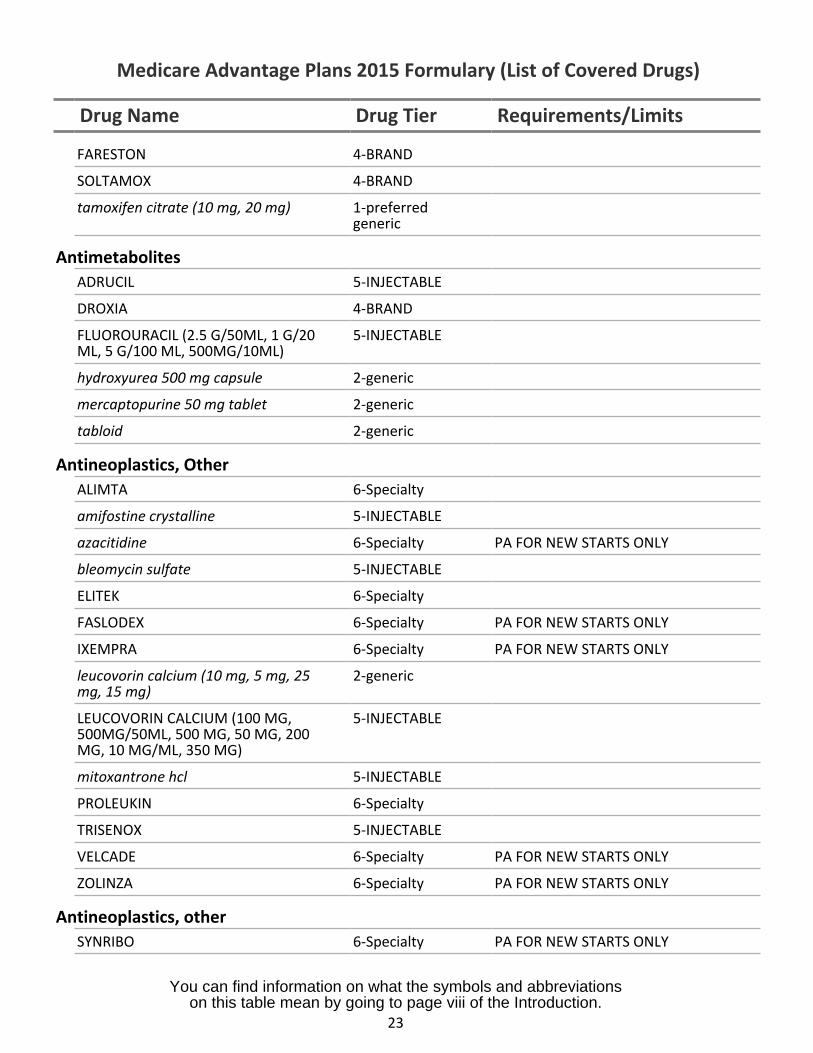
FARESTON 4-BRAND
SOLTAMOX 4-BRAND
tamoxifen citrate (10 mg, 20 mg) 1-preferredgeneric
AntimetabolitesADRUCIL 5-INJECTABLE
DROXIA 4-BRAND
FLUOROURACIL (2.5 G/50ML, 1 G/20ML, 5 G/100 ML, 500MG/10ML)
5-INJECTABLE
hydroxyurea 500 mg capsule 2-generic
mercaptopurine 50 mg tablet 2-generic
tabloid 2-generic
Antineoplastics, OtherALIMTA 6-Specialty
amifostine crystalline 5-INJECTABLE
azacitidine 6-Specialty PA FOR NEW STARTS ONLY
bleomycin sulfate 5-INJECTABLE
ELITEK 6-Specialty
FASLODEX 6-Specialty PA FOR NEW STARTS ONLY
IXEMPRA 6-Specialty PA FOR NEW STARTS ONLY
leucovorin calcium (10 mg, 5 mg, 25mg, 15 mg)
2-generic
LEUCOVORIN CALCIUM (100 MG,500MG/50ML, 500 MG, 50 MG, 200MG, 10 MG/ML, 350 MG)
5-INJECTABLE
mitoxantrone hcl 5-INJECTABLE
PROLEUKIN 6-Specialty
TRISENOX 5-INJECTABLE
VELCADE 6-Specialty PA FOR NEW STARTS ONLY
ZOLINZA 6-Specialty PA FOR NEW STARTS ONLY
Antineoplastics, otherSYNRIBO 6-Specialty PA FOR NEW STARTS ONLY
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
23
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
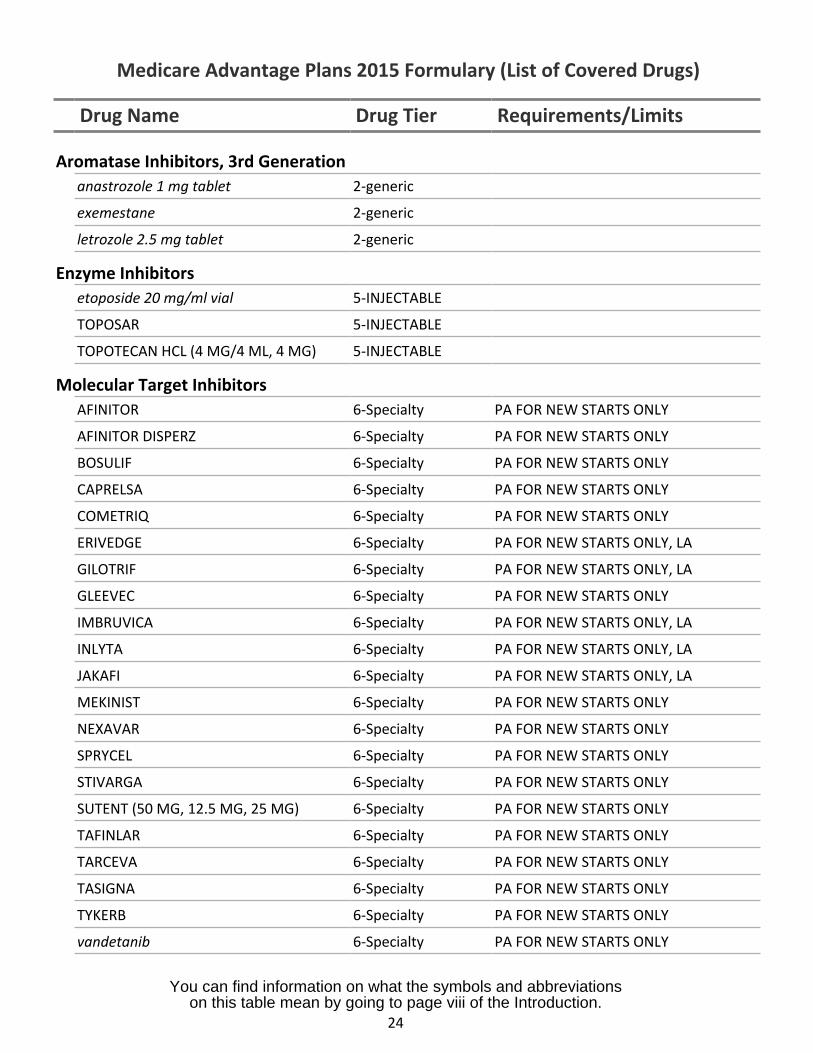
Aromatase Inhibitors, 3rd Generationanastrozole 1 mg tablet 2-generic
exemestane 2-generic
letrozole 2.5 mg tablet 2-generic
Enzyme Inhibitorsetoposide 20 mg/ml vial 5-INJECTABLE
TOPOSAR 5-INJECTABLE
TOPOTECAN HCL (4 MG/4 ML, 4 MG) 5-INJECTABLE
Molecular Target InhibitorsAFINITOR 6-Specialty PA FOR NEW STARTS ONLY
AFINITOR DISPERZ 6-Specialty PA FOR NEW STARTS ONLY
BOSULIF 6-Specialty PA FOR NEW STARTS ONLY
CAPRELSA 6-Specialty PA FOR NEW STARTS ONLY
COMETRIQ 6-Specialty PA FOR NEW STARTS ONLY
ERIVEDGE 6-Specialty PA FOR NEW STARTS ONLY, LA
GILOTRIF 6-Specialty PA FOR NEW STARTS ONLY, LA
GLEEVEC 6-Specialty PA FOR NEW STARTS ONLY
IMBRUVICA 6-Specialty PA FOR NEW STARTS ONLY, LA
INLYTA 6-Specialty PA FOR NEW STARTS ONLY, LA
JAKAFI 6-Specialty PA FOR NEW STARTS ONLY, LA
MEKINIST 6-Specialty PA FOR NEW STARTS ONLY
NEXAVAR 6-Specialty PA FOR NEW STARTS ONLY
SPRYCEL 6-Specialty PA FOR NEW STARTS ONLY
STIVARGA 6-Specialty PA FOR NEW STARTS ONLY
SUTENT (50 MG, 12.5 MG, 25 MG) 6-Specialty PA FOR NEW STARTS ONLY
TAFINLAR 6-Specialty PA FOR NEW STARTS ONLY
TARCEVA 6-Specialty PA FOR NEW STARTS ONLY
TASIGNA 6-Specialty PA FOR NEW STARTS ONLY
TYKERB 6-Specialty PA FOR NEW STARTS ONLY
vandetanib 6-Specialty PA FOR NEW STARTS ONLY
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
24
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
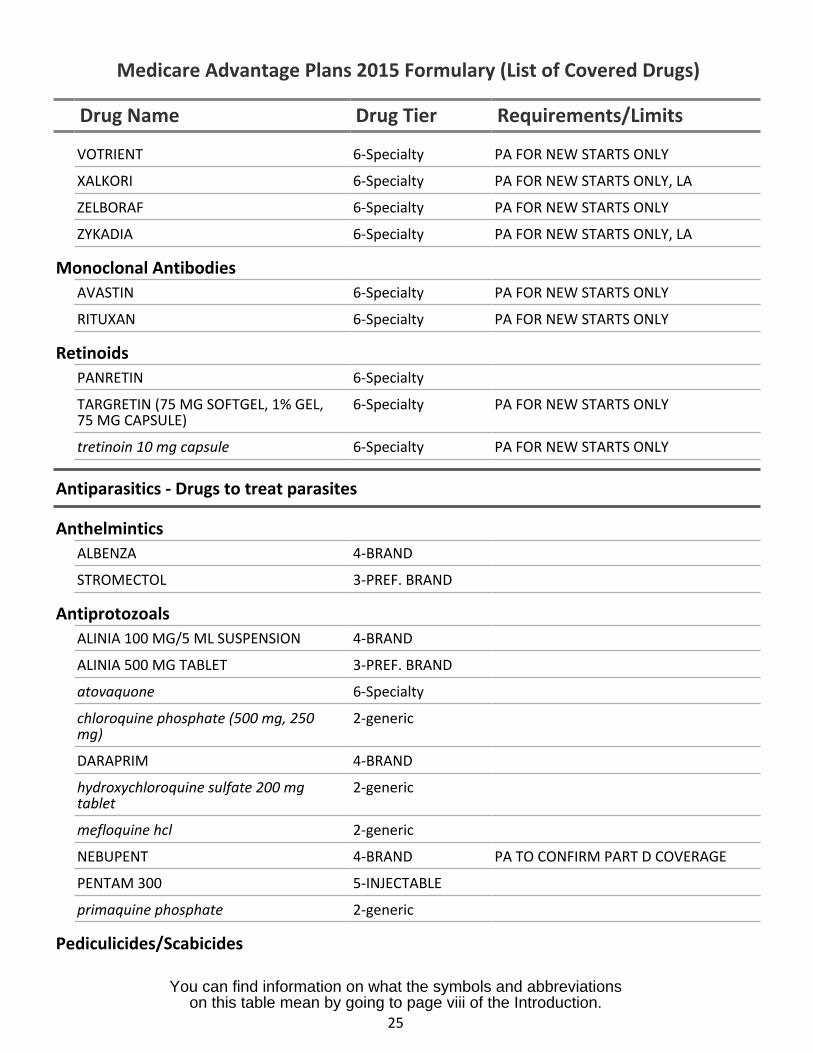
VOTRIENT 6-Specialty PA FOR NEW STARTS ONLY
XALKORI 6-Specialty PA FOR NEW STARTS ONLY, LA
ZELBORAF 6-Specialty PA FOR NEW STARTS ONLY
ZYKADIA 6-Specialty PA FOR NEW STARTS ONLY, LA
Monoclonal AntibodiesAVASTIN 6-Specialty PA FOR NEW STARTS ONLY
RITUXAN 6-Specialty PA FOR NEW STARTS ONLY
RetinoidsPANRETIN 6-Specialty
TARGRETIN (75 MG SOFTGEL, 1% GEL,75 MG CAPSULE)
6-Specialty PA FOR NEW STARTS ONLY
tretinoin 10 mg capsule 6-Specialty PA FOR NEW STARTS ONLY
Antiparasitics - Drugs to treat parasites
AnthelminticsALBENZA 4-BRAND
STROMECTOL 3-PREF. BRAND
AntiprotozoalsALINIA 100 MG/5 ML SUSPENSION 4-BRAND
ALINIA 500 MG TABLET 3-PREF. BRAND
atovaquone 6-Specialty
chloroquine phosphate (500 mg, 250mg)
2-generic
DARAPRIM 4-BRAND
hydroxychloroquine sulfate 200 mgtablet
2-generic
mefloquine hcl 2-generic
NEBUPENT 4-BRAND PA TO CONFIRM PART D COVERAGE
PENTAM 300 5-INJECTABLE
primaquine phosphate 2-generic
Pediculicides/Scabicides
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
25
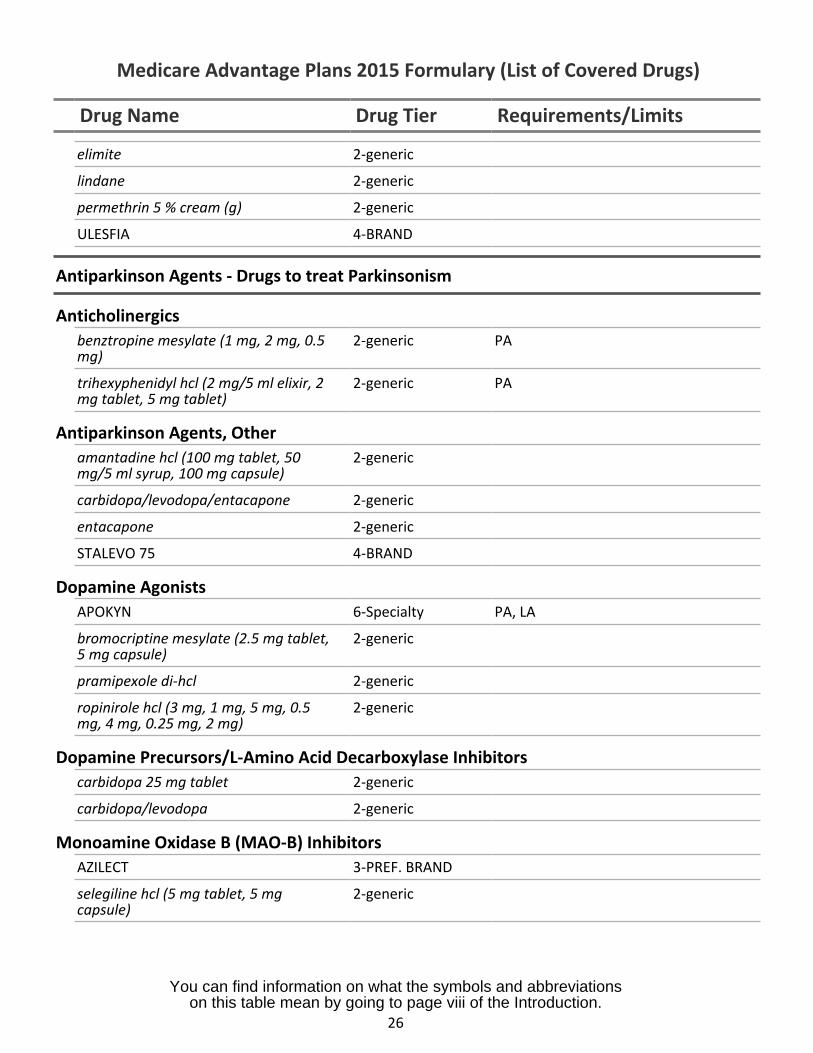
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
elimite 2-generic
lindane 2-generic
permethrin 5 % cream (g) 2-generic
ULESFIA 4-BRAND
Antiparkinson Agents - Drugs to treat Parkinsonism
Anticholinergicsbenztropine mesylate (1 mg, 2 mg, 0.5 2-genericmg)
PA
trihexyphenidyl hcl (2 mg/5 ml elixir, 2 2-genericmg tablet, 5 mg tablet)
PA
Antiparkinson Agents, Otheramantadine hcl (100 mg tablet, 50 2-genericmg/5 ml syrup, 100 mg capsule)
carbidopa/levodopa/entacapone 2-generic
entacapone 2-generic
STALEVO 75 4-BRAND
Dopamine AgonistsAPOKYN 6-Specialty PA, LA
bromocriptine mesylate (2.5 mg tablet, 2-generic5 mg capsule)
pramipexole di-hcl 2-generic
ropinirole hcl (3 mg, 1 mg, 5 mg, 0.5 2-genericmg, 4 mg, 0.25 mg, 2 mg)
Dopamine Precursors/L-Amino Acid Decarboxylase Inhibitorscarbidopa 25 mg tablet 2-generic
carbidopa/levodopa 2-generic
Monoamine Oxidase B (MAO-B) InhibitorsAZILECT 3-PREF. BRAND
selegiline hcl (5 mg tablet, 5 mg 2-genericcapsule)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
26
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
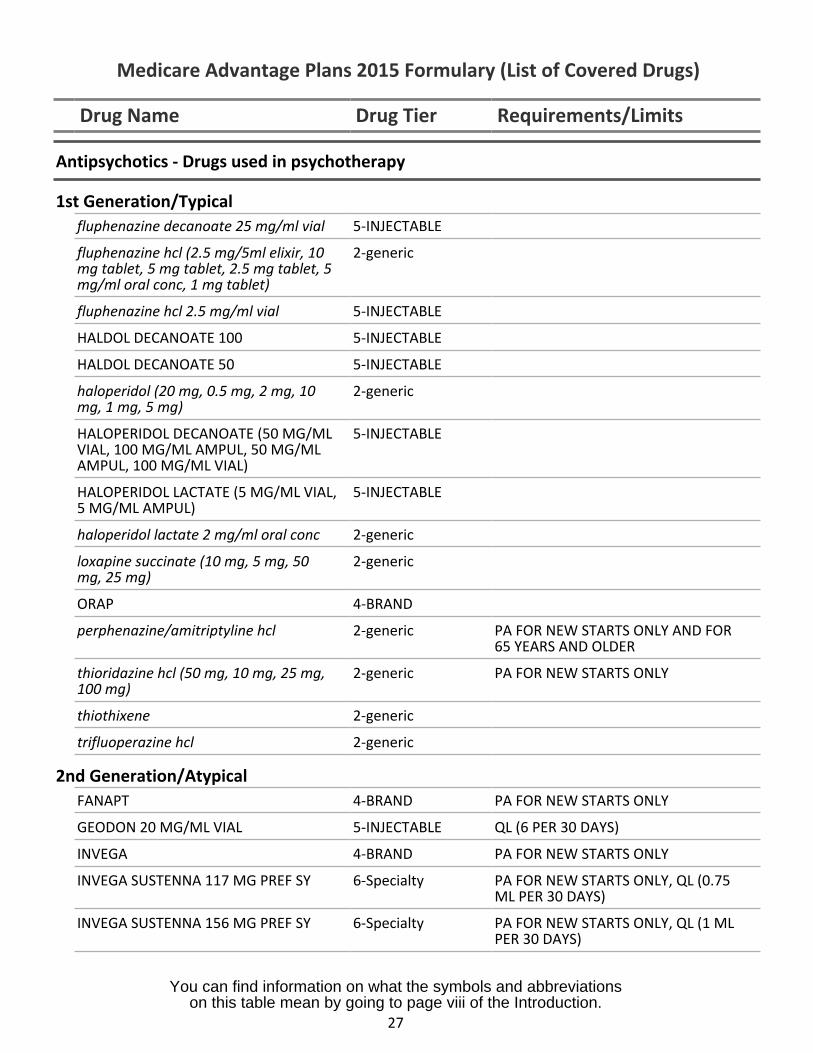
Antipsychotics - Drugs used in psychotherapy
1st Generation/Typicalfluphenazine decanoate 25 mg/ml vial 5-INJECTABLE
fluphenazine hcl (2.5 mg/5ml elixir, 10mg tablet, 5 mg tablet, 2.5 mg tablet, 5mg/ml oral conc, 1 mg tablet)
2-generic
fluphenazine hcl 2.5 mg/ml vial 5-INJECTABLE
HALDOL DECANOATE 100 5-INJECTABLE
HALDOL DECANOATE 50 5-INJECTABLE
haloperidol (20 mg, 0.5 mg, 2 mg, 10mg, 1 mg, 5 mg)
2-generic
HALOPERIDOL DECANOATE (50 MG/MLVIAL, 100 MG/ML AMPUL, 50 MG/MLAMPUL, 100 MG/ML VIAL)
5-INJECTABLE
HALOPERIDOL LACTATE (5 MG/ML VIAL,5 MG/ML AMPUL)
5-INJECTABLE
haloperidol lactate 2 mg/ml oral conc 2-generic
loxapine succinate (10 mg, 5 mg, 50mg, 25 mg)
2-generic
ORAP 4-BRAND
perphenazine/amitriptyline hcl 2-generic PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER
thioridazine hcl (50 mg, 10 mg, 25 mg,100 mg)
2-generic PA FOR NEW STARTS ONLY
thiothixene 2-generic
trifluoperazine hcl 2-generic
2nd Generation/AtypicalFANAPT 4-BRAND PA FOR NEW STARTS ONLY
GEODON 20 MG/ML VIAL 5-INJECTABLE QL (6 PER 30 DAYS)
INVEGA 4-BRAND PA FOR NEW STARTS ONLY
INVEGA SUSTENNA 117 MG PREF SY 6-Specialty PA FOR NEW STARTS ONLY, QL (0.75ML PER 30 DAYS)
INVEGA SUSTENNA 156 MG PREF SY 6-Specialty PA FOR NEW STARTS ONLY, QL (1 MLPER 30 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
27
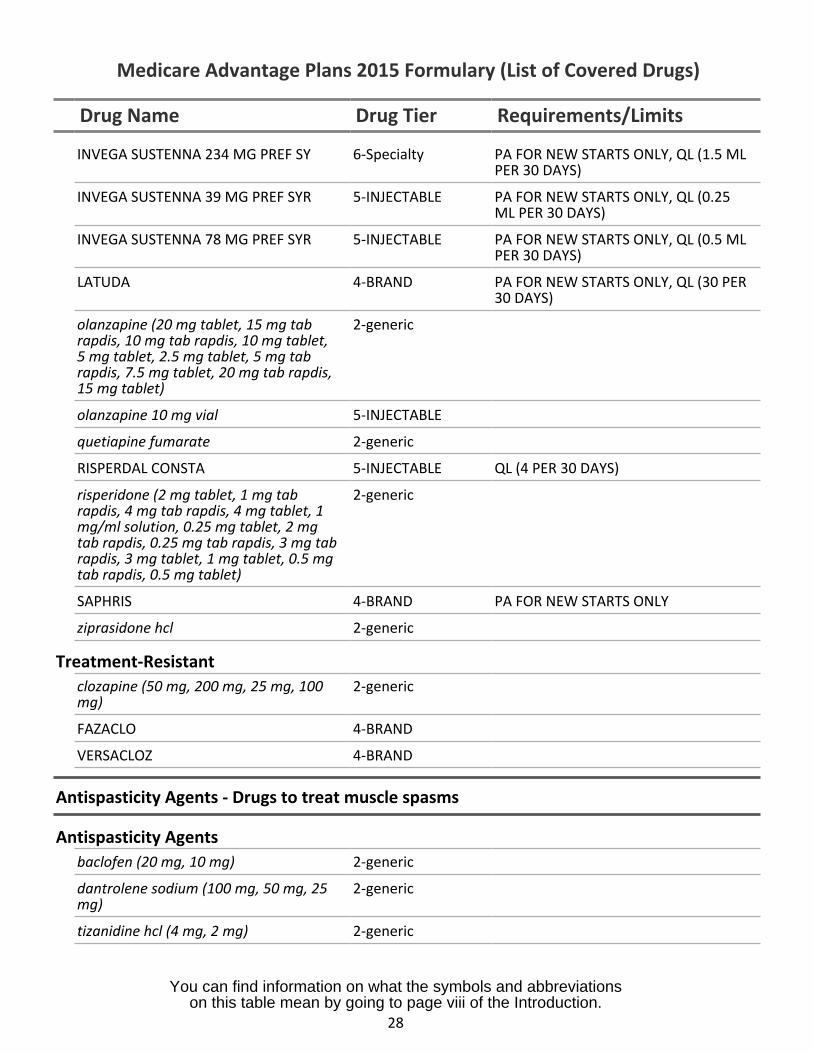
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
INVEGA SUSTENNA 234 MG PREF SY 6-Specialty PA FOR NEW STARTS ONLY, QL (1.5 MLPER 30 DAYS)
INVEGA SUSTENNA 39 MG PREF SYR 5-INJECTABLE PA FOR NEW STARTS ONLY, QL (0.25ML PER 30 DAYS)
INVEGA SUSTENNA 78 MG PREF SYR 5-INJECTABLE PA FOR NEW STARTS ONLY, QL (0.5 MLPER 30 DAYS)
LATUDA 4-BRAND PA FOR NEW STARTS ONLY, QL (30 PER30 DAYS)
olanzapine (20 mg tablet, 15 mg tabrapdis, 10 mg tab rapdis, 10 mg tablet,5 mg tablet, 2.5 mg tablet, 5 mg tabrapdis, 7.5 mg tablet, 20 mg tab rapdis,15 mg tablet)
2-generic
olanzapine 10 mg vial 5-INJECTABLE
quetiapine fumarate 2-generic
RISPERDAL CONSTA 5-INJECTABLE QL (4 PER 30 DAYS)
risperidone (2 mg tablet, 1 mg tabrapdis, 4 mg tab rapdis, 4 mg tablet, 1mg/ml solution, 0.25 mg tablet, 2 mgtab rapdis, 0.25 mg tab rapdis, 3 mg tabrapdis, 3 mg tablet, 1 mg tablet, 0.5 mgtab rapdis, 0.5 mg tablet)
2-generic
SAPHRIS 4-BRAND PA FOR NEW STARTS ONLY
ziprasidone hcl 2-generic
Treatment-Resistantclozapine (50 mg, 200 mg, 25 mg, 100mg)
2-generic
FAZACLO 4-BRAND
VERSACLOZ 4-BRAND
Antispasticity Agents - Drugs to treat muscle spasms
Antispasticity Agentsbaclofen (20 mg, 10 mg) 2-generic
dantrolene sodium (100 mg, 50 mg, 25mg)
2-generic
tizanidine hcl (4 mg, 2 mg) 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
28
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
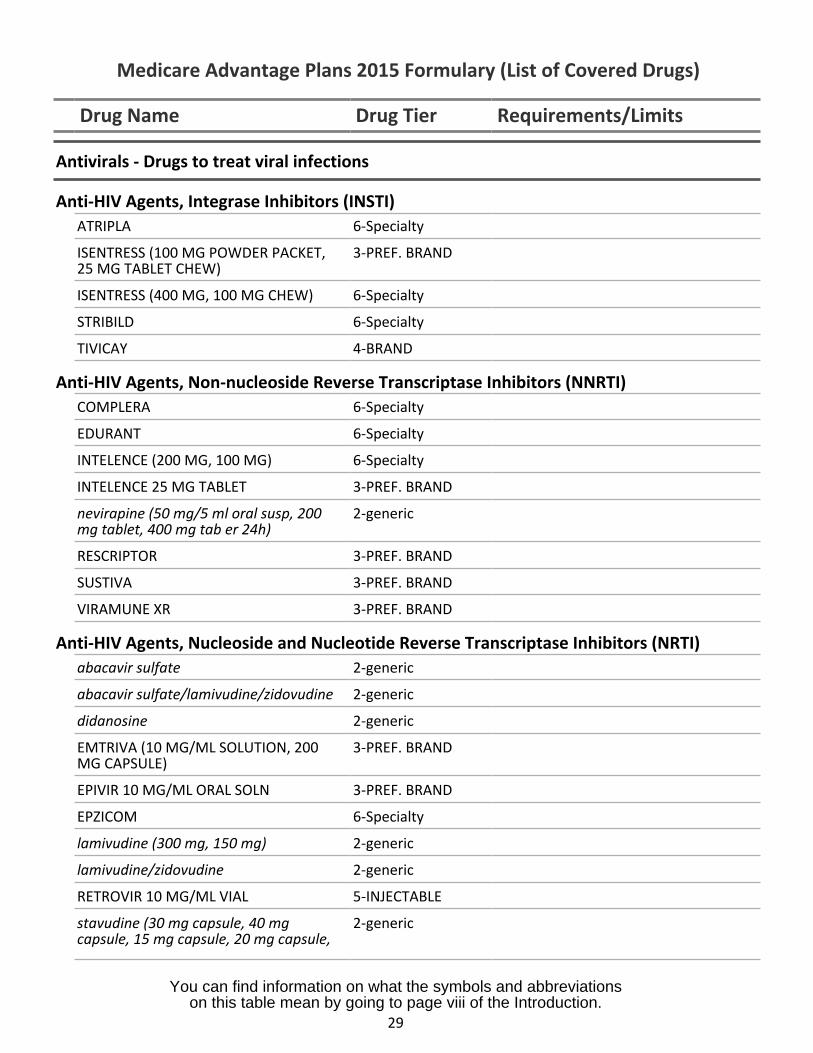
Antivirals - Drugs to treat viral infections
Anti-HIV Agents, Integrase Inhibitors (INSTI)ATRIPLA 6-Specialty
ISENTRESS (100 MG POWDER PACKET, 3-PREF. BRAND25 MG TABLET CHEW)
ISENTRESS (400 MG, 100 MG CHEW) 6-Specialty
STRIBILD 6-Specialty
TIVICAY 4-BRAND
Anti-HIV Agents, Non-nucleoside Reverse Transcriptase Inhibitors (NNRTI)COMPLERA 6-Specialty
EDURANT 6-Specialty
INTELENCE (200 MG, 100 MG) 6-Specialty
INTELENCE 25 MG TABLET 3-PREF. BRAND
nevirapine (50 mg/5 ml oral susp, 200 2-genericmg tablet, 400 mg tab er 24h)
RESCRIPTOR 3-PREF. BRAND
SUSTIVA 3-PREF. BRAND
VIRAMUNE XR 3-PREF. BRAND
Anti-HIV Agents, Nucleoside and Nucleotide Reverse Transcriptase Inhibitors (NRTI)abacavir sulfate 2-generic
abacavir sulfate/lamivudine/zidovudine 2-generic
didanosine 2-generic
EMTRIVA (10 MG/ML SOLUTION, 200 3-PREF. BRANDMG CAPSULE)
EPIVIR 10 MG/ML ORAL SOLN 3-PREF. BRAND
EPZICOM 6-Specialty
lamivudine (300 mg, 150 mg) 2-generic
lamivudine/zidovudine 2-generic
RETROVIR 10 MG/ML VIAL 5-INJECTABLE
stavudine (30 mg capsule, 40 mg 2-genericcapsule, 15 mg capsule, 20 mg capsule,
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
29
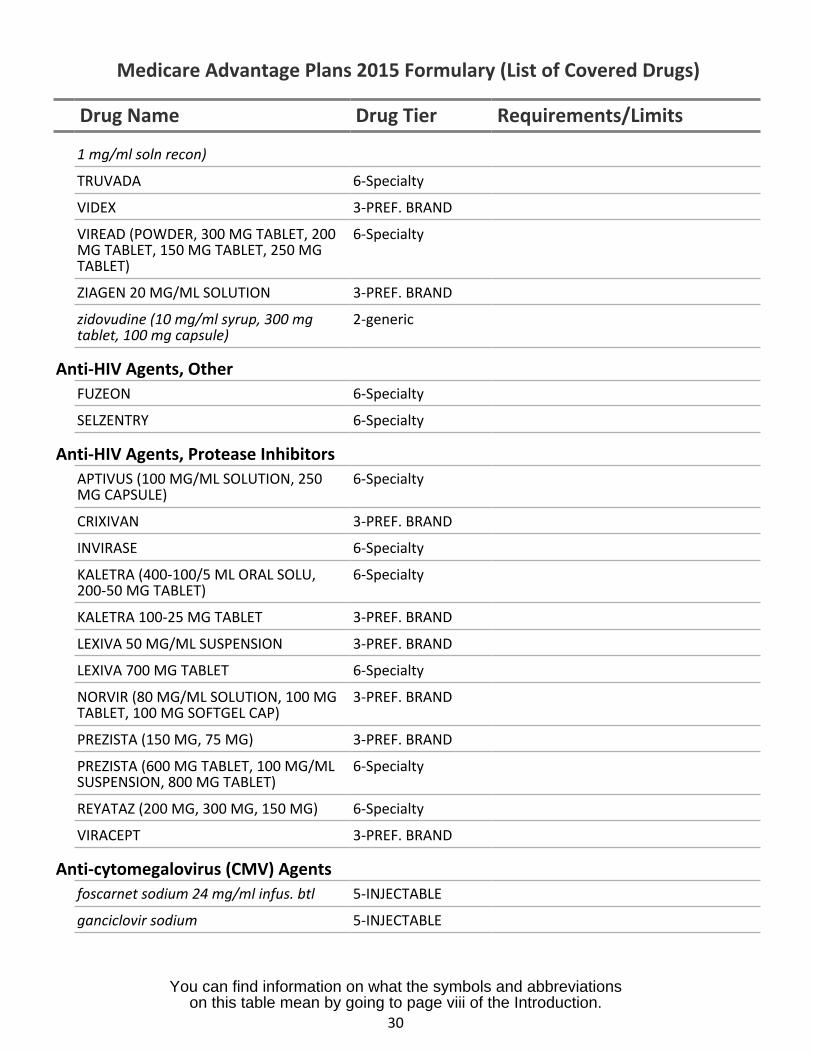
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
1 mg/ml soln recon)
TRUVADA 6-Specialty
VIDEX 3-PREF. BRAND
VIREAD (POWDER, 300 MG TABLET, 200MG TABLET, 150 MG TABLET, 250 MGTABLET)
6-Specialty
ZIAGEN 20 MG/ML SOLUTION 3-PREF. BRAND
zidovudine (10 mg/ml syrup, 300 mgtablet, 100 mg capsule)
2-generic
Anti-HIV Agents, OtherFUZEON 6-Specialty
SELZENTRY 6-Specialty
Anti-HIV Agents, Protease InhibitorsAPTIVUS (100 MG/ML SOLUTION, 250MG CAPSULE)
6-Specialty
CRIXIVAN 3-PREF. BRAND
INVIRASE 6-Specialty
KALETRA (400-100/5 ML ORAL SOLU,200-50 MG TABLET)
6-Specialty
KALETRA 100-25 MG TABLET 3-PREF. BRAND
LEXIVA 50 MG/ML SUSPENSION 3-PREF. BRAND
LEXIVA 700 MG TABLET 6-Specialty
NORVIR (80 MG/ML SOLUTION, 100 MGTABLET, 100 MG SOFTGEL CAP)
3-PREF. BRAND
PREZISTA (150 MG, 75 MG) 3-PREF. BRAND
PREZISTA (600 MG TABLET, 100 MG/MLSUSPENSION, 800 MG TABLET)
6-Specialty
REYATAZ (200 MG, 300 MG, 150 MG) 6-Specialty
VIRACEPT 3-PREF. BRAND
Anti-cytomegalovirus (CMV) Agentsfoscarnet sodium 24 mg/ml infus. btl 5-INJECTABLE
ganciclovir sodium 5-INJECTABLE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
30
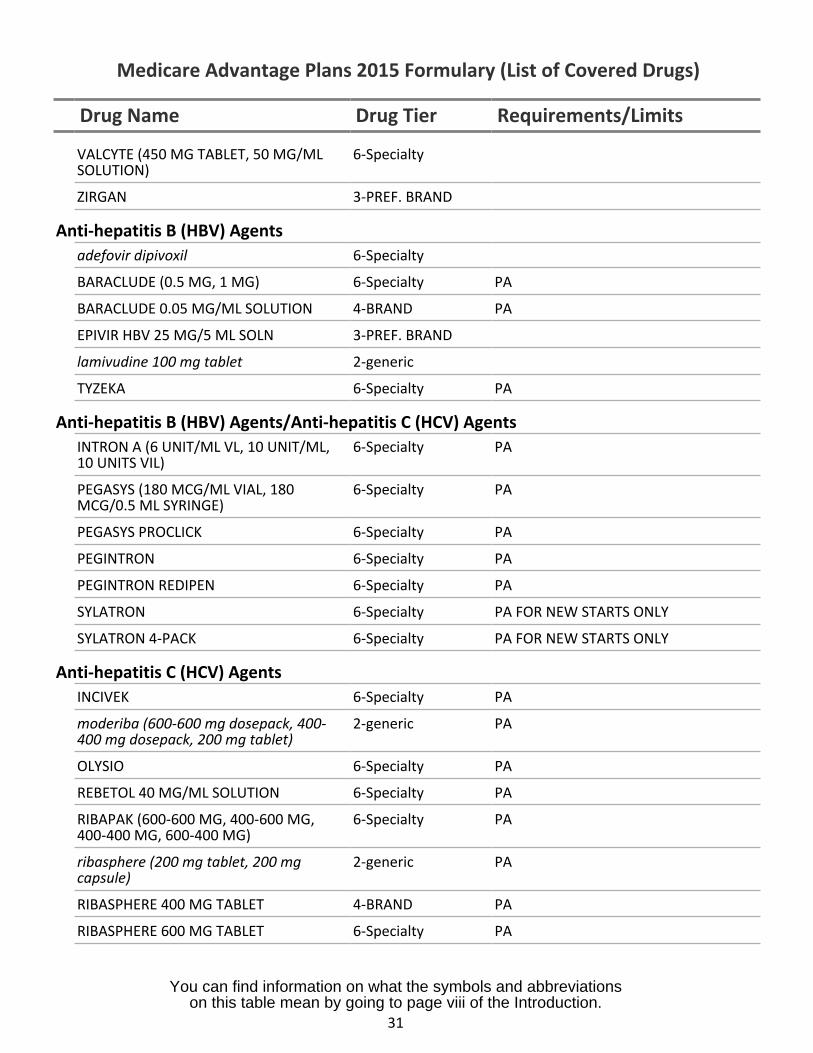
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
VALCYTE (450 MG TABLET, 50 MG/ML 6-SpecialtySOLUTION)
ZIRGAN 3-PREF. BRAND
Anti-hepatitis B (HBV) Agentsadefovir dipivoxil 6-Specialty
BARACLUDE (0.5 MG, 1 MG) 6-Specialty PA
BARACLUDE 0.05 MG/ML SOLUTION 4-BRAND PA
EPIVIR HBV 25 MG/5 ML SOLN 3-PREF. BRAND
lamivudine 100 mg tablet 2-generic
TYZEKA 6-Specialty PA
Anti-hepatitis B (HBV) Agents/Anti-hepatitis C (HCV) AgentsINTRON A (6 UNIT/ML VL, 10 UNIT/ML, 6-Specialty PA10 UNITS VIL)
PEGASYS (180 MCG/ML VIAL, 180 6-Specialty PAMCG/0.5 ML SYRINGE)
PEGASYS PROCLICK 6-Specialty PA
PEGINTRON 6-Specialty PA
PEGINTRON REDIPEN 6-Specialty PA
SYLATRON 6-Specialty PA FOR NEW STARTS ONLY
SYLATRON 4-PACK 6-Specialty PA FOR NEW STARTS ONLY
Anti-hepatitis C (HCV) AgentsINCIVEK 6-Specialty PA
moderiba (600-600 mg dosepack, 400- 2-generic PA400 mg dosepack, 200 mg tablet)
OLYSIO 6-Specialty PA
REBETOL 40 MG/ML SOLUTION 6-Specialty PA
RIBAPAK (600-600 MG, 400-600 MG, 6-Specialty PA400-400 MG, 600-400 MG)
ribasphere (200 mg tablet, 200 mg 2-generic PAcapsule)
RIBASPHERE 400 MG TABLET 4-BRAND PA
RIBASPHERE 600 MG TABLET 6-Specialty PA
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
31
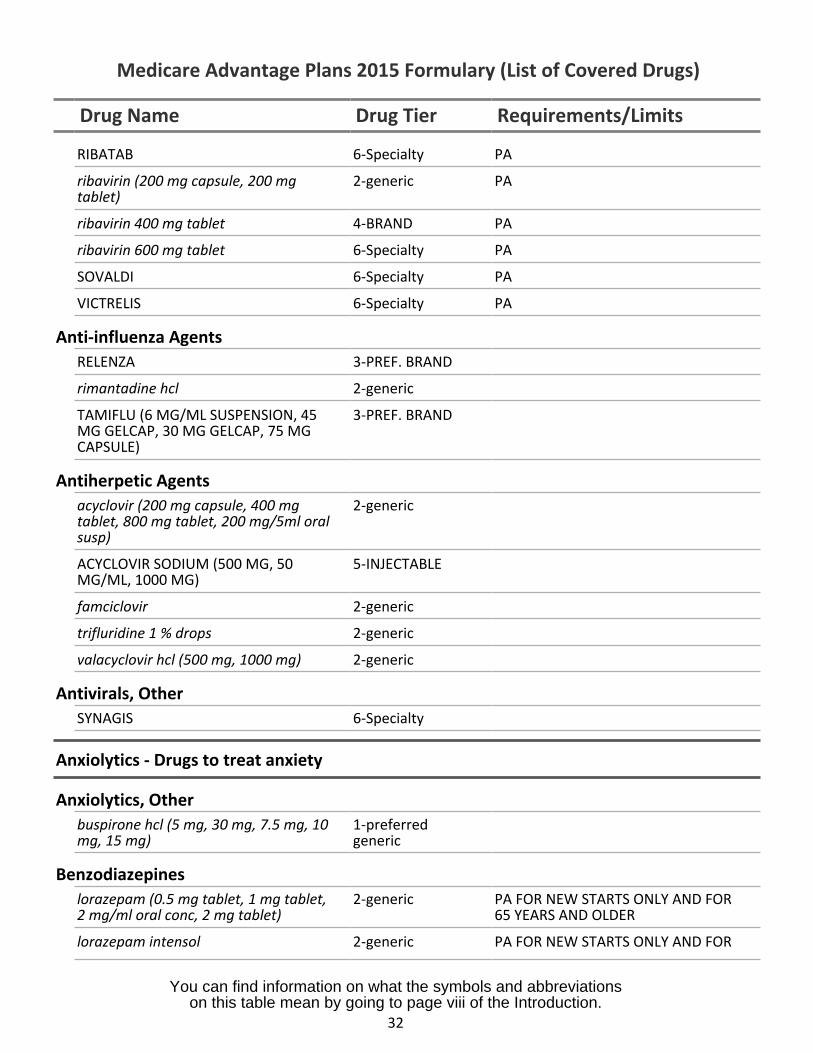
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
RIBATAB 6-Specialty PA
ribavirin (200 mg capsule, 200 mgtablet)
2-generic PA
ribavirin 400 mg tablet 4-BRAND PA
ribavirin 600 mg tablet 6-Specialty PA
SOVALDI 6-Specialty PA
VICTRELIS 6-Specialty PA
Anti-influenza AgentsRELENZA 3-PREF. BRAND
rimantadine hcl 2-generic
TAMIFLU (6 MG/ML SUSPENSION, 45MG GELCAP, 30 MG GELCAP, 75 MGCAPSULE)
3-PREF. BRAND
Antiherpetic Agentsacyclovir (200 mg capsule, 400 mgtablet, 800 mg tablet, 200 mg/5ml oralsusp)
2-generic
ACYCLOVIR SODIUM (500 MG, 50MG/ML, 1000 MG)
5-INJECTABLE
famciclovir 2-generic
trifluridine 1 % drops 2-generic
valacyclovir hcl (500 mg, 1000 mg) 2-generic
Antivirals, OtherSYNAGIS 6-Specialty
Anxiolytics - Drugs to treat anxiety
Anxiolytics, Otherbuspirone hcl (5 mg, 30 mg, 7.5 mg, 10mg, 15 mg)
1-preferredgeneric
Benzodiazepineslorazepam (0.5 mg tablet, 1 mg tablet,2 mg/ml oral conc, 2 mg tablet)
2-generic PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER
lorazepam intensol 2-generic PA FOR NEW STARTS ONLY AND FOR
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
32
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
65 YEARS AND OLDER
oxazepam 2-generic PA FOR NEW STARTS ONLY AND FOR65 YEARS AND OLDER
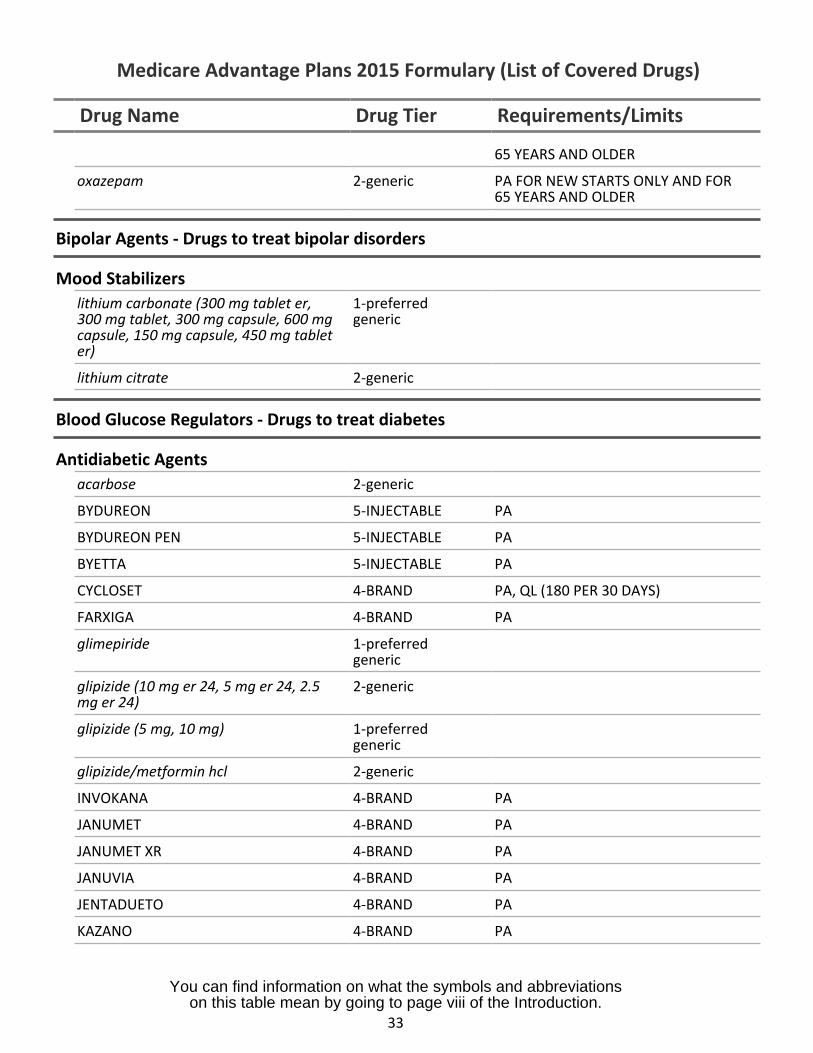
Bipolar Agents - Drugs to treat bipolar disorders
Mood Stabilizerslithium carbonate (300 mg tablet er,300 mg tablet, 300 mg capsule, 600 mgcapsule, 150 mg capsule, 450 mg tableter)
1-preferredgeneric
lithium citrate 2-generic
Blood Glucose Regulators - Drugs to treat diabetes
Antidiabetic Agentsacarbose 2-generic
BYDUREON 5-INJECTABLE PA
BYDUREON PEN 5-INJECTABLE PA
BYETTA 5-INJECTABLE PA
CYCLOSET 4-BRAND PA, QL (180 PER 30 DAYS)
FARXIGA 4-BRAND PA
glimepiride 1-preferredgeneric
glipizide (10 mg er 24, 5 mg er 24, 2.5mg er 24)
2-generic
glipizide (5 mg, 10 mg) 1-preferredgeneric
glipizide/metformin hcl 2-generic
INVOKANA 4-BRAND PA
JANUMET 4-BRAND PA
JANUMET XR 4-BRAND PA
JANUVIA 4-BRAND PA
JENTADUETO 4-BRAND PA
KAZANO 4-BRAND PA
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
33
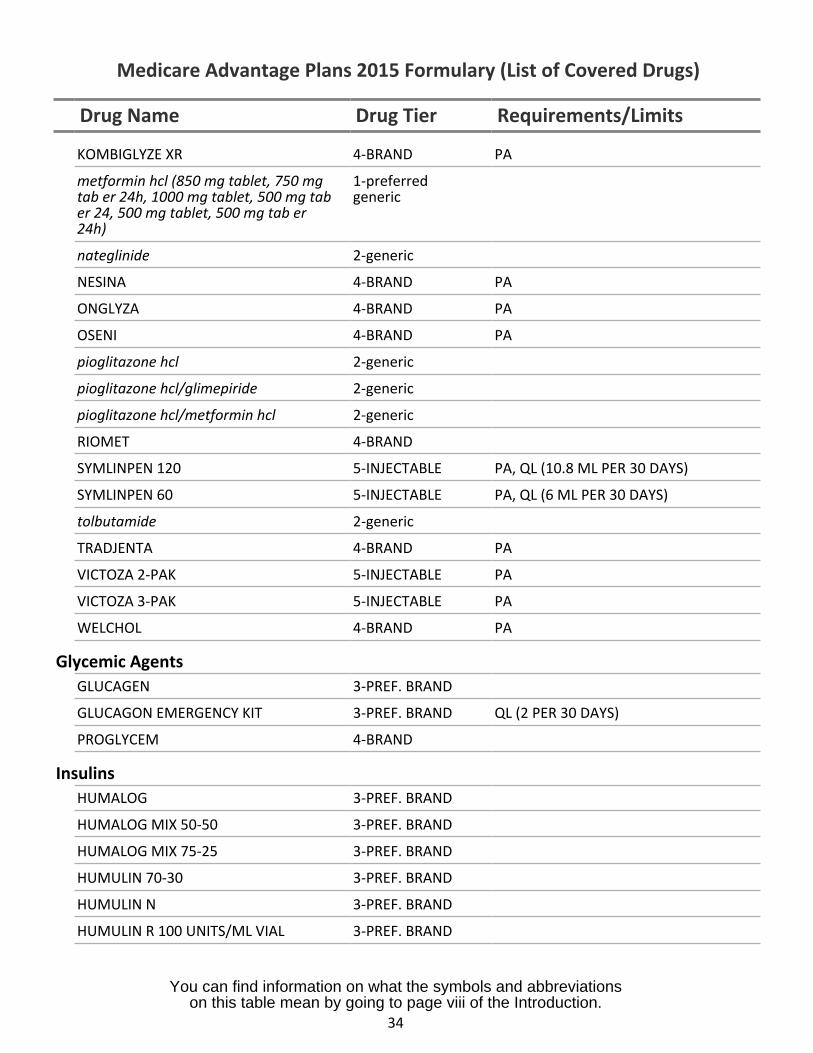
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
KOMBIGLYZE XR 4-BRAND PA
metformin hcl (850 mg tablet, 750 mgtab er 24h, 1000 mg tablet, 500 mg taber 24, 500 mg tablet, 500 mg tab er24h)
1-preferredgeneric
nateglinide 2-generic
NESINA 4-BRAND PA
ONGLYZA 4-BRAND PA
OSENI 4-BRAND PA
pioglitazone hcl 2-generic
pioglitazone hcl/glimepiride 2-generic
pioglitazone hcl/metformin hcl 2-generic
RIOMET 4-BRAND
SYMLINPEN 120 5-INJECTABLE PA, QL (10.8 ML PER 30 DAYS)
SYMLINPEN 60 5-INJECTABLE PA, QL (6 ML PER 30 DAYS)
tolbutamide 2-generic
TRADJENTA 4-BRAND PA
VICTOZA 2-PAK 5-INJECTABLE PA
VICTOZA 3-PAK 5-INJECTABLE PA
WELCHOL 4-BRAND PA
Glycemic AgentsGLUCAGEN 3-PREF. BRAND
GLUCAGON EMERGENCY KIT 3-PREF. BRAND QL (2 PER 30 DAYS)
PROGLYCEM 4-BRAND
InsulinsHUMALOG 3-PREF. BRAND
HUMALOG MIX 50-50 3-PREF. BRAND
HUMALOG MIX 75-25 3-PREF. BRAND
HUMULIN 70-30 3-PREF. BRAND
HUMULIN N 3-PREF. BRAND
HUMULIN R 100 UNITS/ML VIAL 3-PREF. BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
34
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
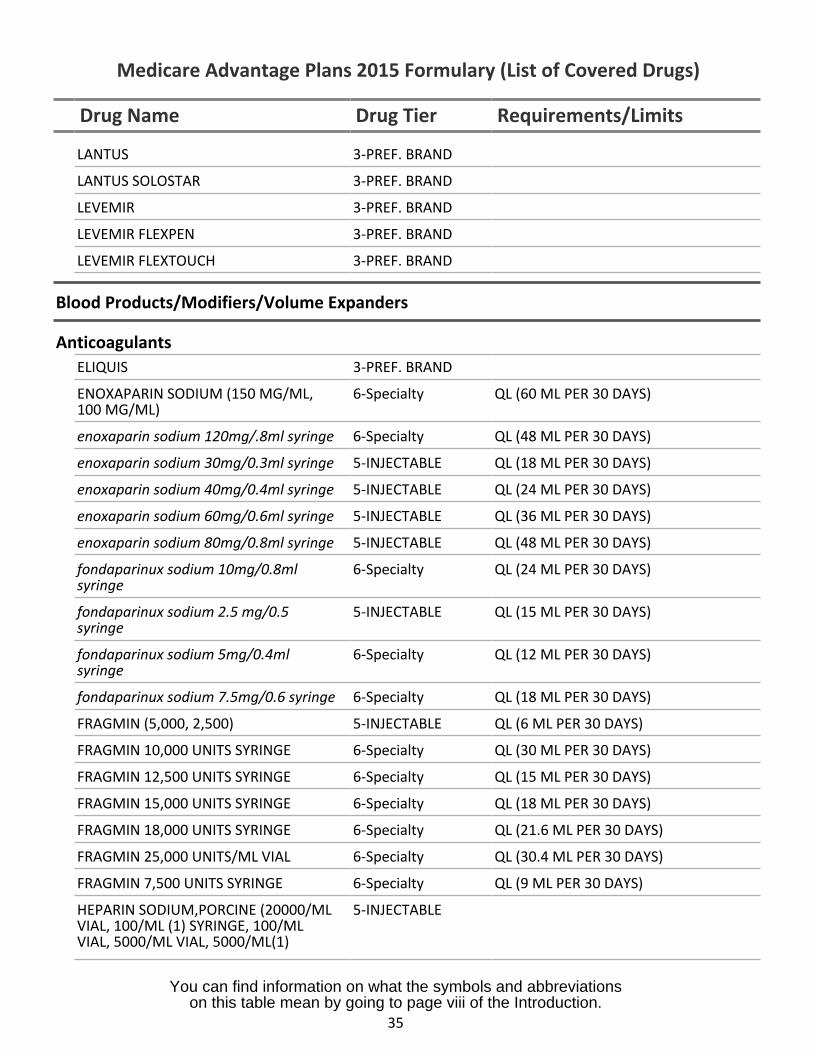
LANTUS 3-PREF. BRAND
LANTUS SOLOSTAR 3-PREF. BRAND
LEVEMIR 3-PREF. BRAND
LEVEMIR FLEXPEN 3-PREF. BRAND
LEVEMIR FLEXTOUCH 3-PREF. BRAND
Blood Products/Modifiers/Volume Expanders
AnticoagulantsELIQUIS 3-PREF. BRAND
ENOXAPARIN SODIUM (150 MG/ML,100 MG/ML)
6-Specialty QL (60 ML PER 30 DAYS)
enoxaparin sodium 120mg/.8ml syringe 6-Specialty QL (48 ML PER 30 DAYS)
enoxaparin sodium 30mg/0.3ml syringe 5-INJECTABLE QL (18 ML PER 30 DAYS)
enoxaparin sodium 40mg/0.4ml syringe 5-INJECTABLE QL (24 ML PER 30 DAYS)
enoxaparin sodium 60mg/0.6ml syringe 5-INJECTABLE QL (36 ML PER 30 DAYS)
enoxaparin sodium 80mg/0.8ml syringe 5-INJECTABLE QL (48 ML PER 30 DAYS)
fondaparinux sodium 10mg/0.8mlsyringe
6-Specialty QL (24 ML PER 30 DAYS)
fondaparinux sodium 2.5 mg/0.5syringe
5-INJECTABLE QL (15 ML PER 30 DAYS)
fondaparinux sodium 5mg/0.4mlsyringe
6-Specialty QL (12 ML PER 30 DAYS)
fondaparinux sodium 7.5mg/0.6 syringe 6-Specialty QL (18 ML PER 30 DAYS)
FRAGMIN (5,000, 2,500) 5-INJECTABLE QL (6 ML PER 30 DAYS)
FRAGMIN 10,000 UNITS SYRINGE 6-Specialty QL (30 ML PER 30 DAYS)
FRAGMIN 12,500 UNITS SYRINGE 6-Specialty QL (15 ML PER 30 DAYS)
FRAGMIN 15,000 UNITS SYRINGE 6-Specialty QL (18 ML PER 30 DAYS)
FRAGMIN 18,000 UNITS SYRINGE 6-Specialty QL (21.6 ML PER 30 DAYS)
FRAGMIN 25,000 UNITS/ML VIAL 6-Specialty QL (30.4 ML PER 30 DAYS)
FRAGMIN 7,500 UNITS SYRINGE 6-Specialty QL (9 ML PER 30 DAYS)
HEPARIN SODIUM,PORCINE (20000/MLVIAL, 100/ML (1) SYRINGE, 100/MLVIAL, 5000/ML VIAL, 5000/ML(1)
5-INJECTABLE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
35
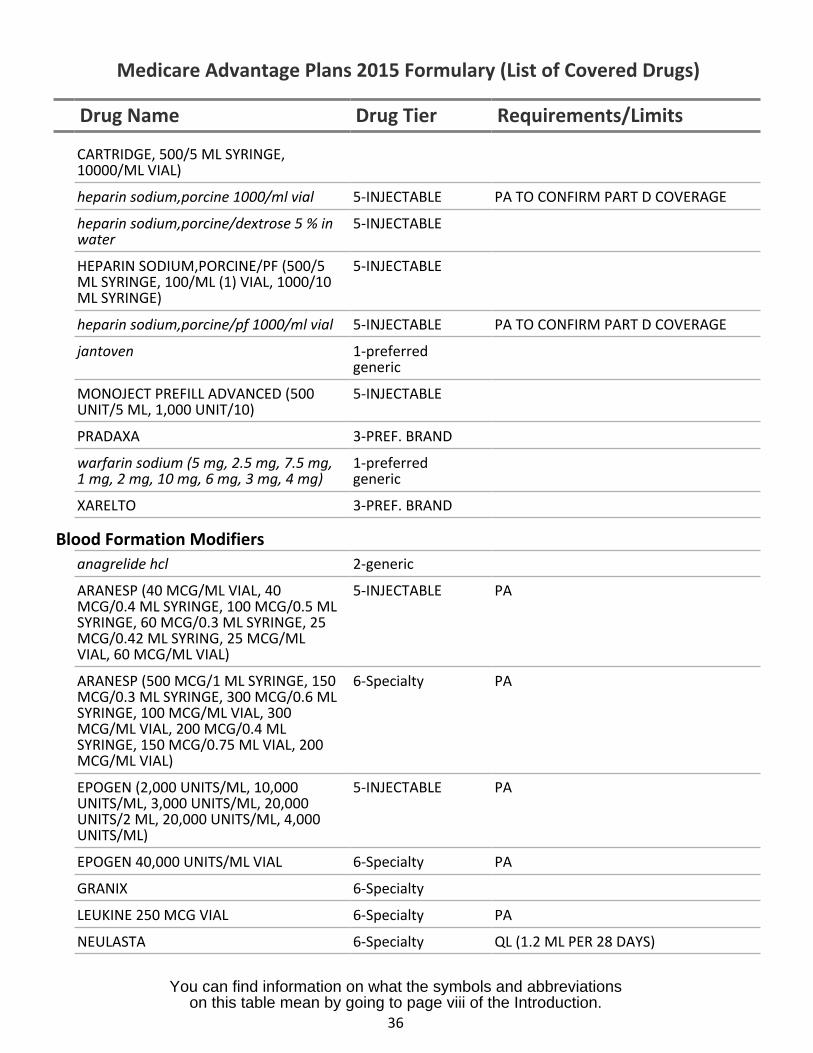
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
CARTRIDGE, 500/5 ML SYRINGE,10000/ML VIAL)
heparin sodium,porcine 1000/ml vial 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
heparin sodium,porcine/dextrose 5 % in 5-INJECTABLEwater
HEPARIN SODIUM,PORCINE/PF (500/5 5-INJECTABLEML SYRINGE, 100/ML (1) VIAL, 1000/10ML SYRINGE)
heparin sodium,porcine/pf 1000/ml vial 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
jantoven 1-preferredgeneric
MONOJECT PREFILL ADVANCED (500 5-INJECTABLEUNIT/5 ML, 1,000 UNIT/10)
PRADAXA 3-PREF. BRAND
warfarin sodium (5 mg, 2.5 mg, 7.5 mg, 1-preferred1 mg, 2 mg, 10 mg, 6 mg, 3 mg, 4 mg) generic
XARELTO 3-PREF. BRAND
Blood Formation Modifiersanagrelide hcl 2-generic
ARANESP (40 MCG/ML VIAL, 40 5-INJECTABLE PAMCG/0.4 ML SYRINGE, 100 MCG/0.5 MLSYRINGE, 60 MCG/0.3 ML SYRINGE, 25MCG/0.42 ML SYRING, 25 MCG/MLVIAL, 60 MCG/ML VIAL)
ARANESP (500 MCG/1 ML SYRINGE, 150 6-Specialty PAMCG/0.3 ML SYRINGE, 300 MCG/0.6 MLSYRINGE, 100 MCG/ML VIAL, 300MCG/ML VIAL, 200 MCG/0.4 MLSYRINGE, 150 MCG/0.75 ML VIAL, 200MCG/ML VIAL)
EPOGEN (2,000 UNITS/ML, 10,000 5-INJECTABLE PAUNITS/ML, 3,000 UNITS/ML, 20,000UNITS/2 ML, 20,000 UNITS/ML, 4,000UNITS/ML)
EPOGEN 40,000 UNITS/ML VIAL 6-Specialty PA
GRANIX 6-Specialty
LEUKINE 250 MCG VIAL 6-Specialty PA
NEULASTA 6-Specialty QL (1.2 ML PER 28 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
36
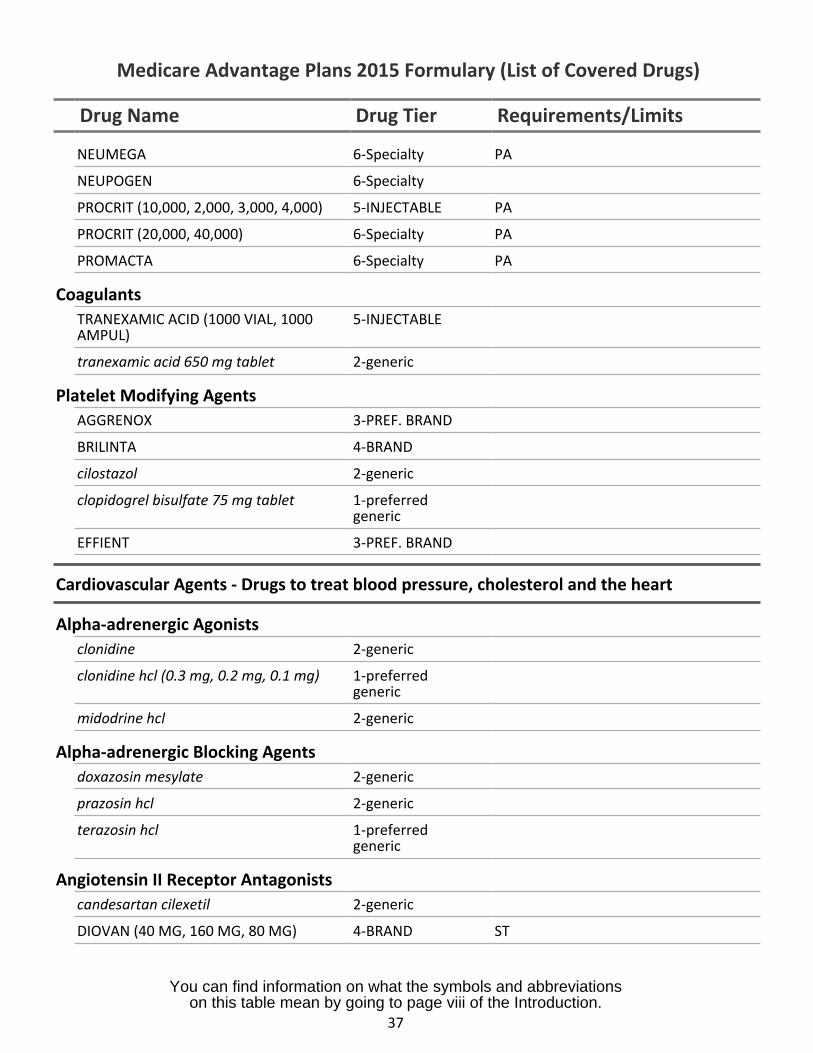
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
NEUMEGA 6-Specialty PA
NEUPOGEN 6-Specialty
PROCRIT (10,000, 2,000, 3,000, 4,000) 5-INJECTABLE PA
PROCRIT (20,000, 40,000) 6-Specialty PA
PROMACTA 6-Specialty PA
CoagulantsTRANEXAMIC ACID (1000 VIAL, 1000AMPUL)
5-INJECTABLE
tranexamic acid 650 mg tablet 2-generic
Platelet Modifying AgentsAGGRENOX 3-PREF. BRAND
BRILINTA 4-BRAND
cilostazol 2-generic
clopidogrel bisulfate 75 mg tablet 1-preferredgeneric
EFFIENT 3-PREF. BRAND
Cardiovascular Agents - Drugs to treat blood pressure, cholesterol and the heart
Alpha-adrenergic Agonistsclonidine 2-generic
clonidine hcl (0.3 mg, 0.2 mg, 0.1 mg) 1-preferredgeneric
midodrine hcl 2-generic
Alpha-adrenergic Blocking Agentsdoxazosin mesylate 2-generic
prazosin hcl 2-generic
terazosin hcl 1-preferredgeneric
Angiotensin II Receptor Antagonistscandesartan cilexetil 2-generic
DIOVAN (40 MG, 160 MG, 80 MG) 4-BRAND ST
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
37
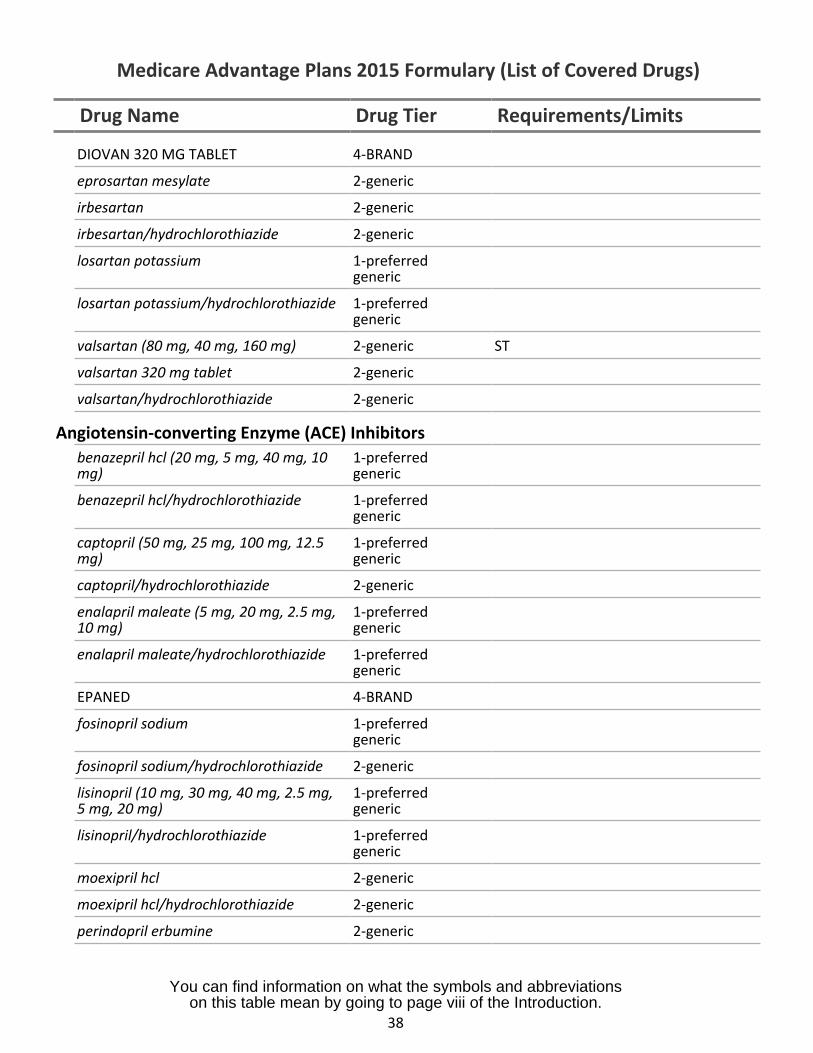
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
DIOVAN 320 MG TABLET 4-BRAND
eprosartan mesylate 2-generic
irbesartan 2-generic
irbesartan/hydrochlorothiazide 2-generic
losartan potassium 1-preferredgeneric
losartan potassium/hydrochlorothiazide 1-preferredgeneric
valsartan (80 mg, 40 mg, 160 mg) 2-generic ST
valsartan 320 mg tablet 2-generic
valsartan/hydrochlorothiazide 2-generic
Angiotensin-converting Enzyme (ACE) Inhibitorsbenazepril hcl (20 mg, 5 mg, 40 mg, 10 1-preferredmg) generic
benazepril hcl/hydrochlorothiazide 1-preferredgeneric
captopril (50 mg, 25 mg, 100 mg, 12.5 1-preferredmg) generic
captopril/hydrochlorothiazide 2-generic
enalapril maleate (5 mg, 20 mg, 2.5 mg, 1-preferred10 mg) generic
enalapril maleate/hydrochlorothiazide 1-preferredgeneric
EPANED 4-BRAND
fosinopril sodium 1-preferredgeneric
fosinopril sodium/hydrochlorothiazide 2-generic
lisinopril (10 mg, 30 mg, 40 mg, 2.5 mg, 1-preferred5 mg, 20 mg) generic
lisinopril/hydrochlorothiazide 1-preferredgeneric
moexipril hcl 2-generic
moexipril hcl/hydrochlorothiazide 2-generic
perindopril erbumine 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
38
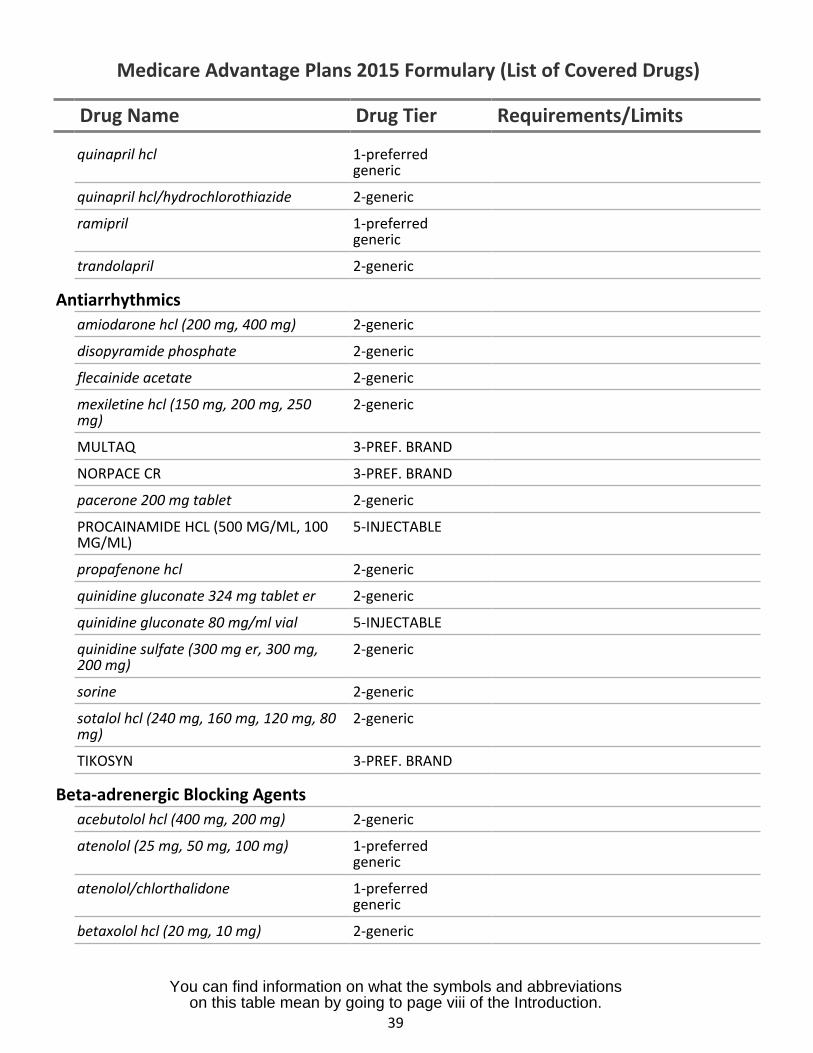
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
quinapril hcl 1-preferredgeneric
quinapril hcl/hydrochlorothiazide 2-generic
ramipril 1-preferredgeneric
trandolapril 2-generic
Antiarrhythmicsamiodarone hcl (200 mg, 400 mg) 2-generic
disopyramide phosphate 2-generic
flecainide acetate 2-generic
mexiletine hcl (150 mg, 200 mg, 250 2-genericmg)
MULTAQ 3-PREF. BRAND
NORPACE CR 3-PREF. BRAND
pacerone 200 mg tablet 2-generic
PROCAINAMIDE HCL (500 MG/ML, 100 5-INJECTABLEMG/ML)
propafenone hcl 2-generic
quinidine gluconate 324 mg tablet er 2-generic
quinidine gluconate 80 mg/ml vial 5-INJECTABLE
quinidine sulfate (300 mg er, 300 mg, 2-generic200 mg)
sorine 2-generic
sotalol hcl (240 mg, 160 mg, 120 mg, 80 2-genericmg)
TIKOSYN 3-PREF. BRAND
Beta-adrenergic Blocking Agentsacebutolol hcl (400 mg, 200 mg) 2-generic
atenolol (25 mg, 50 mg, 100 mg) 1-preferredgeneric
atenolol/chlorthalidone 1-preferredgeneric
betaxolol hcl (20 mg, 10 mg) 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
39
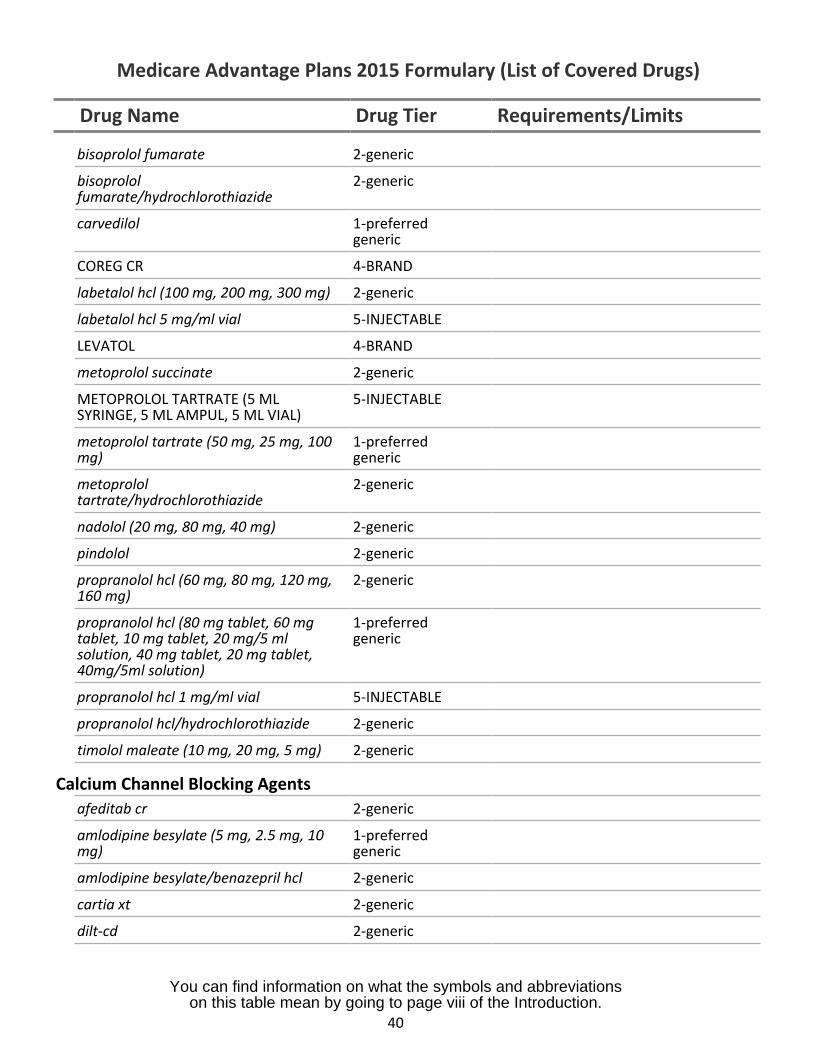
Drug Name Drug Tier Requirements/Limits
bisoprolol fumarate 2-generic
bisoprolol 2-genericfumarate/hydrochlorothiazide
carvedilol 1-preferredgeneric
COREG CR 4-BRAND
labetalol hcl (100 mg, 200 mg, 300 mg) 2-generic
labetalol hcl 5 mg/ml vial 5-INJECTABLE
LEVATOL 4-BRAND
metoprolol succinate 2-generic
METOPROLOL TARTRATE (5 ML 5-INJECTABLESYRINGE, 5 ML AMPUL, 5 ML VIAL)
metoprolol tartrate (50 mg, 25 mg, 100 1-preferredmg) generic
metoprolol 2-generictartrate/hydrochlorothiazide
nadolol (20 mg, 80 mg, 40 mg) 2-generic
pindolol 2-generic
propranolol hcl (60 mg, 80 mg, 120 mg, 2-generic160 mg)
propranolol hcl (80 mg tablet, 60 mg 1-preferredtablet, 10 mg tablet, 20 mg/5 ml genericsolution, 40 mg tablet, 20 mg tablet,40mg/5ml solution)
propranolol hcl 1 mg/ml vial 5-INJECTABLE
propranolol hcl/hydrochlorothiazide 2-generic
timolol maleate (10 mg, 20 mg, 5 mg) 2-generic
Calcium Channel Blocking Agentsafeditab cr 2-generic
amlodipine besylate (5 mg, 2.5 mg, 10 1-preferredmg) generic
amlodipine besylate/benazepril hcl 2-generic
cartia xt 2-generic
dilt-cd 2-generic
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
40
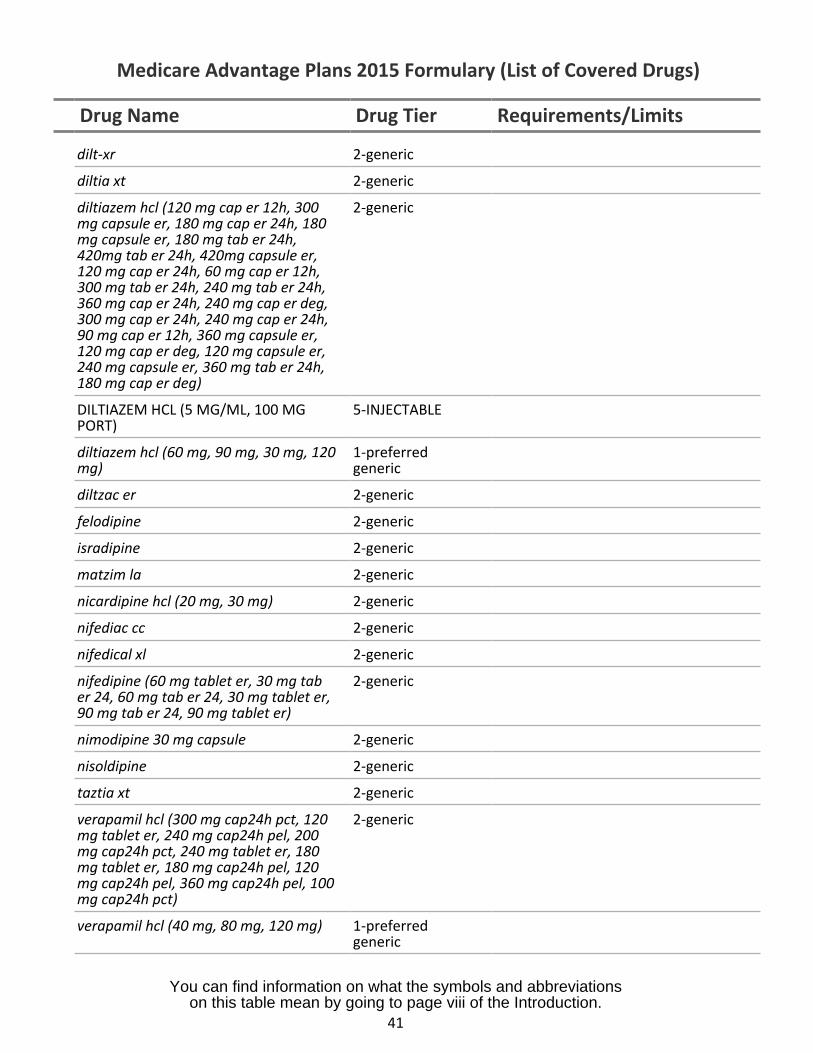
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
dilt-xr 2-generic
diltia xt 2-generic
diltiazem hcl (120 mg cap er 12h, 300 2-genericmg capsule er, 180 mg cap er 24h, 180mg capsule er, 180 mg tab er 24h,420mg tab er 24h, 420mg capsule er,120 mg cap er 24h, 60 mg cap er 12h,300 mg tab er 24h, 240 mg tab er 24h,360 mg cap er 24h, 240 mg cap er deg,300 mg cap er 24h, 240 mg cap er 24h,90 mg cap er 12h, 360 mg capsule er,120 mg cap er deg, 120 mg capsule er,240 mg capsule er, 360 mg tab er 24h,180 mg cap er deg)
DILTIAZEM HCL (5 MG/ML, 100 MG 5-INJECTABLEPORT)
diltiazem hcl (60 mg, 90 mg, 30 mg, 120 1-preferredmg) generic
diltzac er 2-generic
felodipine 2-generic
isradipine 2-generic
matzim la 2-generic
nicardipine hcl (20 mg, 30 mg) 2-generic
nifediac cc 2-generic
nifedical xl 2-generic
nifedipine (60 mg tablet er, 30 mg tab 2-genericer 24, 60 mg tab er 24, 30 mg tablet er,90 mg tab er 24, 90 mg tablet er)
nimodipine 30 mg capsule 2-generic
nisoldipine 2-generic
taztia xt 2-generic
verapamil hcl (300 mg cap24h pct, 120 2-genericmg tablet er, 240 mg cap24h pel, 200mg cap24h pct, 240 mg tablet er, 180mg tablet er, 180 mg cap24h pel, 120mg cap24h pel, 360 mg cap24h pel, 100mg cap24h pct)
verapamil hcl (40 mg, 80 mg, 120 mg) 1-preferredgeneric
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
41
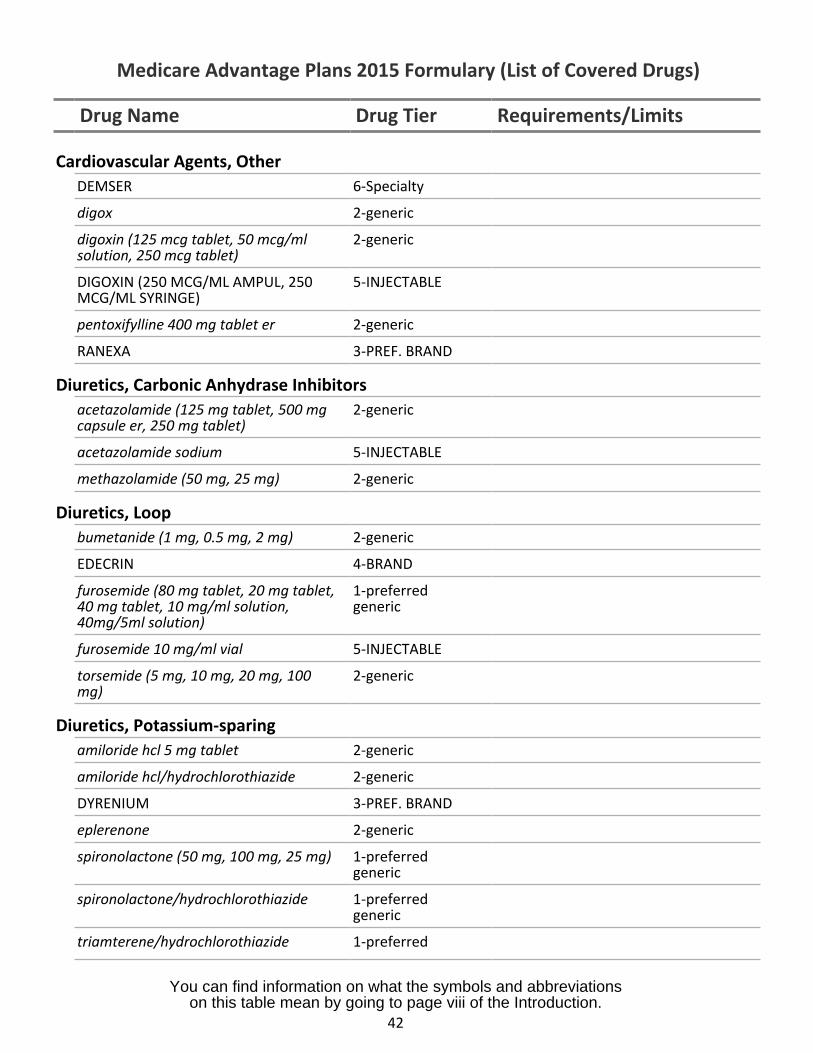
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Cardiovascular Agents, OtherDEMSER 6-Specialty
digox 2-generic
digoxin (125 mcg tablet, 50 mcg/ml 2-genericsolution, 250 mcg tablet)
DIGOXIN (250 MCG/ML AMPUL, 250 5-INJECTABLEMCG/ML SYRINGE)
pentoxifylline 400 mg tablet er 2-generic
RANEXA 3-PREF. BRAND
Diuretics, Carbonic Anhydrase Inhibitorsacetazolamide (125 mg tablet, 500 mg 2-genericcapsule er, 250 mg tablet)
acetazolamide sodium 5-INJECTABLE
methazolamide (50 mg, 25 mg) 2-generic
Diuretics, Loopbumetanide (1 mg, 0.5 mg, 2 mg) 2-generic
EDECRIN 4-BRAND
furosemide (80 mg tablet, 20 mg tablet, 1-preferred40 mg tablet, 10 mg/ml solution, generic40mg/5ml solution)
furosemide 10 mg/ml vial 5-INJECTABLE
torsemide (5 mg, 10 mg, 20 mg, 100 2-genericmg)
Diuretics, Potassium-sparingamiloride hcl 5 mg tablet 2-generic
amiloride hcl/hydrochlorothiazide 2-generic
DYRENIUM 3-PREF. BRAND
eplerenone 2-generic
spironolactone (50 mg, 100 mg, 25 mg) 1-preferredgeneric
spironolactone/hydrochlorothiazide 1-preferredgeneric
triamterene/hydrochlorothiazide 1-preferred
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
42
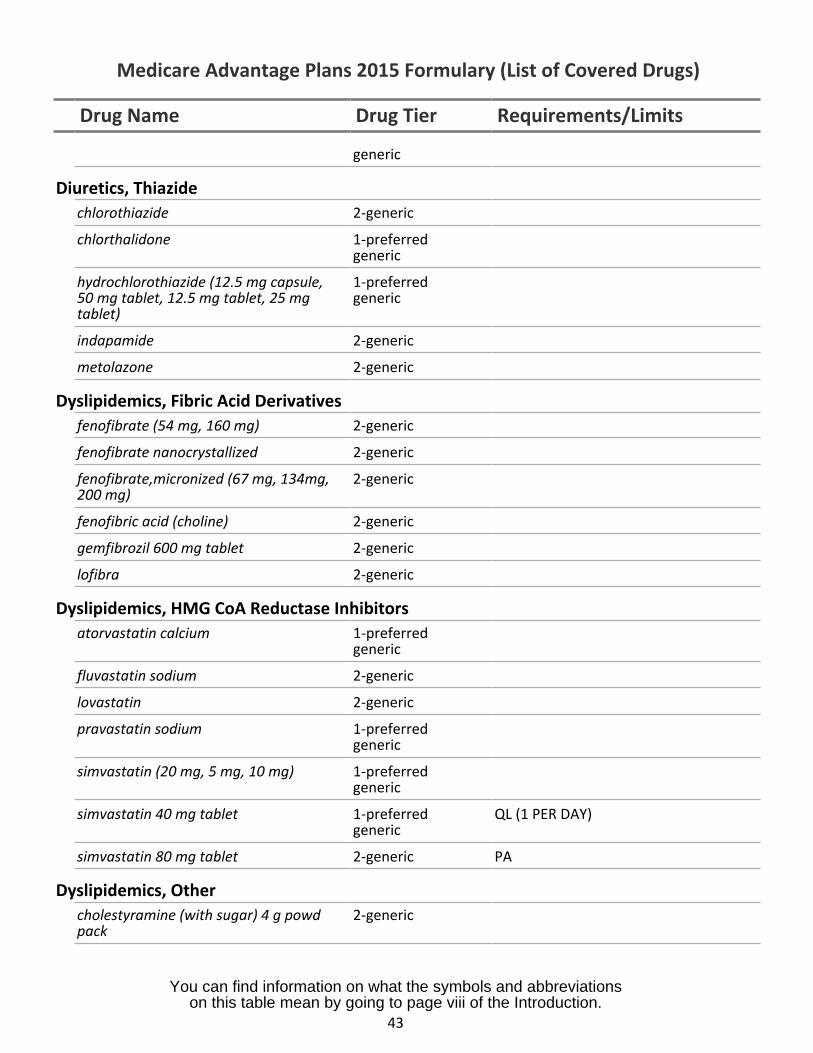
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
generic
Diuretics, Thiazidechlorothiazide 2-generic
chlorthalidone 1-preferredgeneric
hydrochlorothiazide (12.5 mg capsule, 1-preferred50 mg tablet, 12.5 mg tablet, 25 mg generictablet)
indapamide 2-generic
metolazone 2-generic
Dyslipidemics, Fibric Acid Derivativesfenofibrate (54 mg, 160 mg) 2-generic
fenofibrate nanocrystallized 2-generic
fenofibrate,micronized (67 mg, 134mg, 2-generic200 mg)
fenofibric acid (choline) 2-generic
gemfibrozil 600 mg tablet 2-generic
lofibra 2-generic
Dyslipidemics, HMG CoA Reductase Inhibitorsatorvastatin calcium 1-preferred
generic
fluvastatin sodium 2-generic
lovastatin 2-generic
pravastatin sodium 1-preferredgeneric
simvastatin (20 mg, 5 mg, 10 mg) 1-preferredgeneric
simvastatin 40 mg tablet 1-preferred QL (1 PER DAY)generic
simvastatin 80 mg tablet 2-generic PA
Dyslipidemics, Othercholestyramine (with sugar) 4 g powd 2-genericpack
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
43
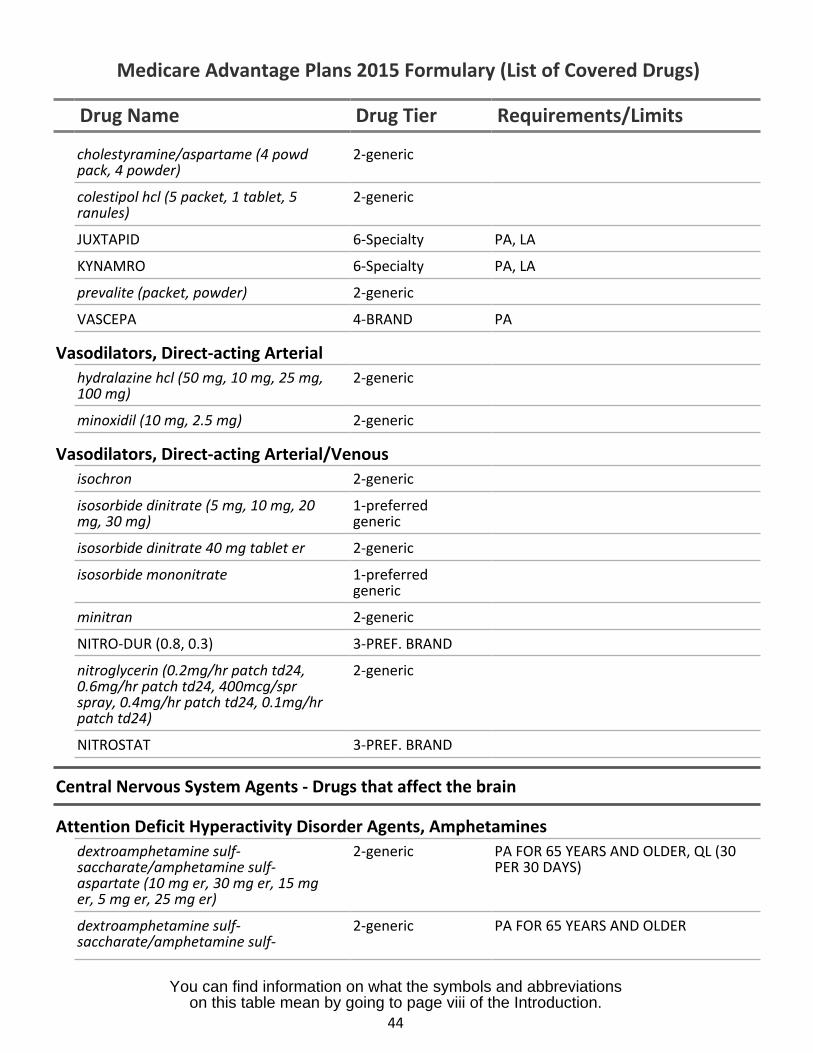
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
cholestyramine/aspartame (4 powd 2-genericpack, 4 powder)
colestipol hcl (5 packet, 1 tablet, 5 2-genericranules)
JUXTAPID 6-Specialty PA, LA
KYNAMRO 6-Specialty PA, LA
prevalite (packet, powder) 2-generic
VASCEPA 4-BRAND PA
Vasodilators, Direct-acting Arterialhydralazine hcl (50 mg, 10 mg, 25 mg, 2-generic100 mg)
minoxidil (10 mg, 2.5 mg) 2-generic
Vasodilators, Direct-acting Arterial/Venousisochron 2-generic
isosorbide dinitrate (5 mg, 10 mg, 20 1-preferredmg, 30 mg) generic
isosorbide dinitrate 40 mg tablet er 2-generic
isosorbide mononitrate 1-preferredgeneric
minitran 2-generic
NITRO-DUR (0.8, 0.3) 3-PREF. BRAND
nitroglycerin (0.2mg/hr patch td24, 2-generic0.6mg/hr patch td24, 400mcg/sprspray, 0.4mg/hr patch td24, 0.1mg/hrpatch td24)
NITROSTAT 3-PREF. BRAND
Central Nervous System Agents - Drugs that affect the brain
Attention Deficit Hyperactivity Disorder Agents, Amphetaminesdextroamphetamine sulf- 2-generic PA FOR 65 YEARS AND OLDER, QL (30saccharate/amphetamine sulf- PER 30 DAYS)aspartate (10 mg er, 30 mg er, 15 mger, 5 mg er, 25 mg er)
dextroamphetamine sulf- 2-generic PA FOR 65 YEARS AND OLDERsaccharate/amphetamine sulf-
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
44
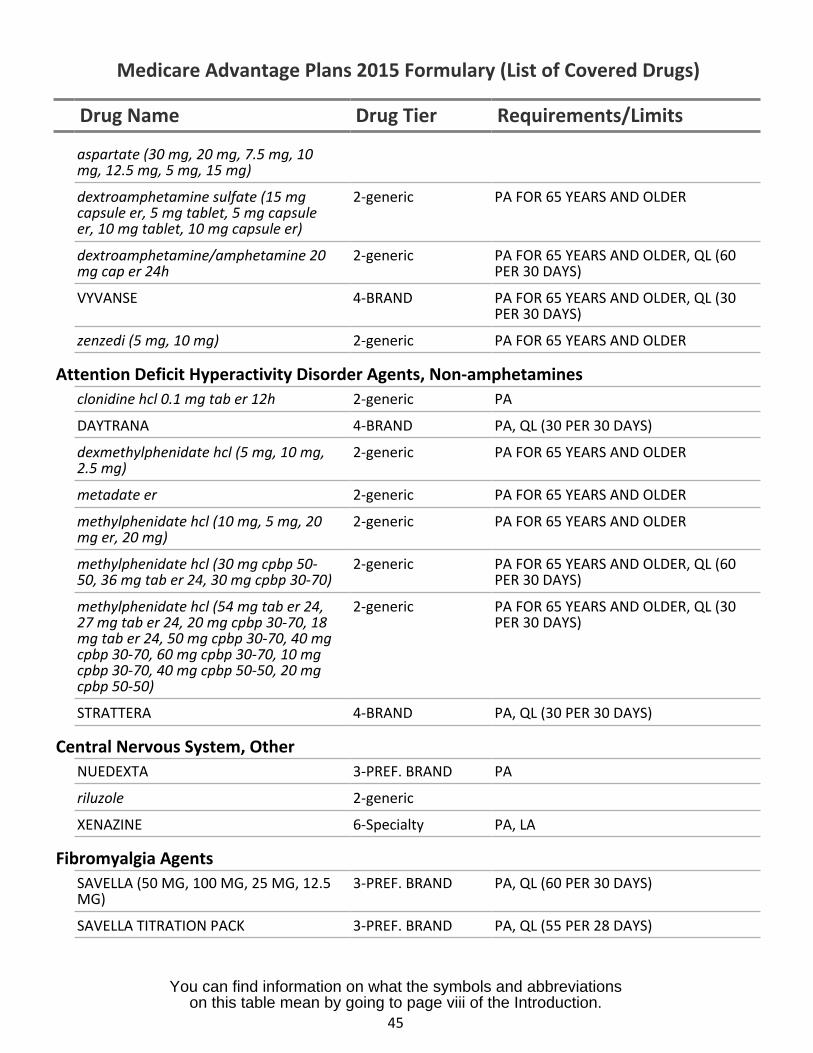
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
aspartate (30 mg, 20 mg, 7.5 mg, 10mg, 12.5 mg, 5 mg, 15 mg)
dextroamphetamine sulfate (15 mg 2-generic PA FOR 65 YEARS AND OLDERcapsule er, 5 mg tablet, 5 mg capsuleer, 10 mg tablet, 10 mg capsule er)
dextroamphetamine/amphetamine 20 2-generic PA FOR 65 YEARS AND OLDER, QL (60mg cap er 24h PER 30 DAYS)
VYVANSE 4-BRAND PA FOR 65 YEARS AND OLDER, QL (30PER 30 DAYS)
zenzedi (5 mg, 10 mg) 2-generic PA FOR 65 YEARS AND OLDER
Attention Deficit Hyperactivity Disorder Agents, Non-amphetaminesclonidine hcl 0.1 mg tab er 12h 2-generic PA
DAYTRANA 4-BRAND PA, QL (30 PER 30 DAYS)
dexmethylphenidate hcl (5 mg, 10 mg, 2-generic PA FOR 65 YEARS AND OLDER2.5 mg)
metadate er 2-generic PA FOR 65 YEARS AND OLDER
methylphenidate hcl (10 mg, 5 mg, 20 2-generic PA FOR 65 YEARS AND OLDERmg er, 20 mg)
methylphenidate hcl (30 mg cpbp 50- 2-generic PA FOR 65 YEARS AND OLDER, QL (6050, 36 mg tab er 24, 30 mg cpbp 30-70) PER 30 DAYS)
methylphenidate hcl (54 mg tab er 24, 2-generic PA FOR 65 YEARS AND OLDER, QL (3027 mg tab er 24, 20 mg cpbp 30-70, 18 PER 30 DAYS)mg tab er 24, 50 mg cpbp 30-70, 40 mgcpbp 30-70, 60 mg cpbp 30-70, 10 mgcpbp 30-70, 40 mg cpbp 50-50, 20 mgcpbp 50-50)
STRATTERA 4-BRAND PA, QL (30 PER 30 DAYS)
Central Nervous System, OtherNUEDEXTA 3-PREF. BRAND PA
riluzole 2-generic
XENAZINE 6-Specialty PA, LA
Fibromyalgia AgentsSAVELLA (50 MG, 100 MG, 25 MG, 12.5 3-PREF. BRAND PA, QL (60 PER 30 DAYS)MG)
SAVELLA TITRATION PACK 3-PREF. BRAND PA, QL (55 PER 28 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
45
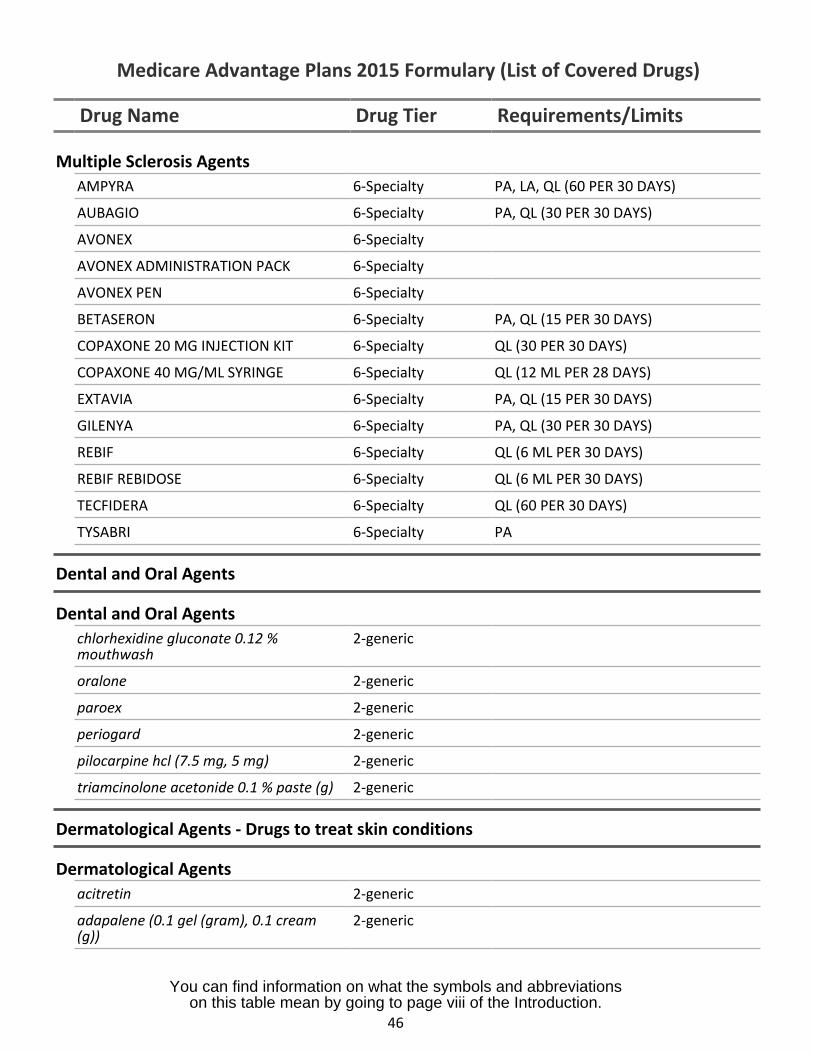
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Multiple Sclerosis AgentsAMPYRA 6-Specialty PA, LA, QL (60 PER 30 DAYS)
AUBAGIO 6-Specialty PA, QL (30 PER 30 DAYS)
AVONEX 6-Specialty
AVONEX ADMINISTRATION PACK 6-Specialty
AVONEX PEN 6-Specialty
BETASERON 6-Specialty PA, QL (15 PER 30 DAYS)
COPAXONE 20 MG INJECTION KIT 6-Specialty QL (30 PER 30 DAYS)
COPAXONE 40 MG/ML SYRINGE 6-Specialty QL (12 ML PER 28 DAYS)
EXTAVIA 6-Specialty PA, QL (15 PER 30 DAYS)
GILENYA 6-Specialty PA, QL (30 PER 30 DAYS)
REBIF 6-Specialty QL (6 ML PER 30 DAYS)
REBIF REBIDOSE 6-Specialty QL (6 ML PER 30 DAYS)
TECFIDERA 6-Specialty QL (60 PER 30 DAYS)
TYSABRI 6-Specialty PA
Dental and Oral Agents
Dental and Oral Agentschlorhexidine gluconate 0.12 %mouthwash
2-generic
oralone 2-generic
paroex 2-generic
periogard 2-generic
pilocarpine hcl (7.5 mg, 5 mg) 2-generic
triamcinolone acetonide 0.1 % paste (g) 2-generic
Dermatological Agents - Drugs to treat skin conditions
Dermatological Agentsacitretin 2-generic
adapalene (0.1 gel (gram), 0.1 cream(g))
2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
46
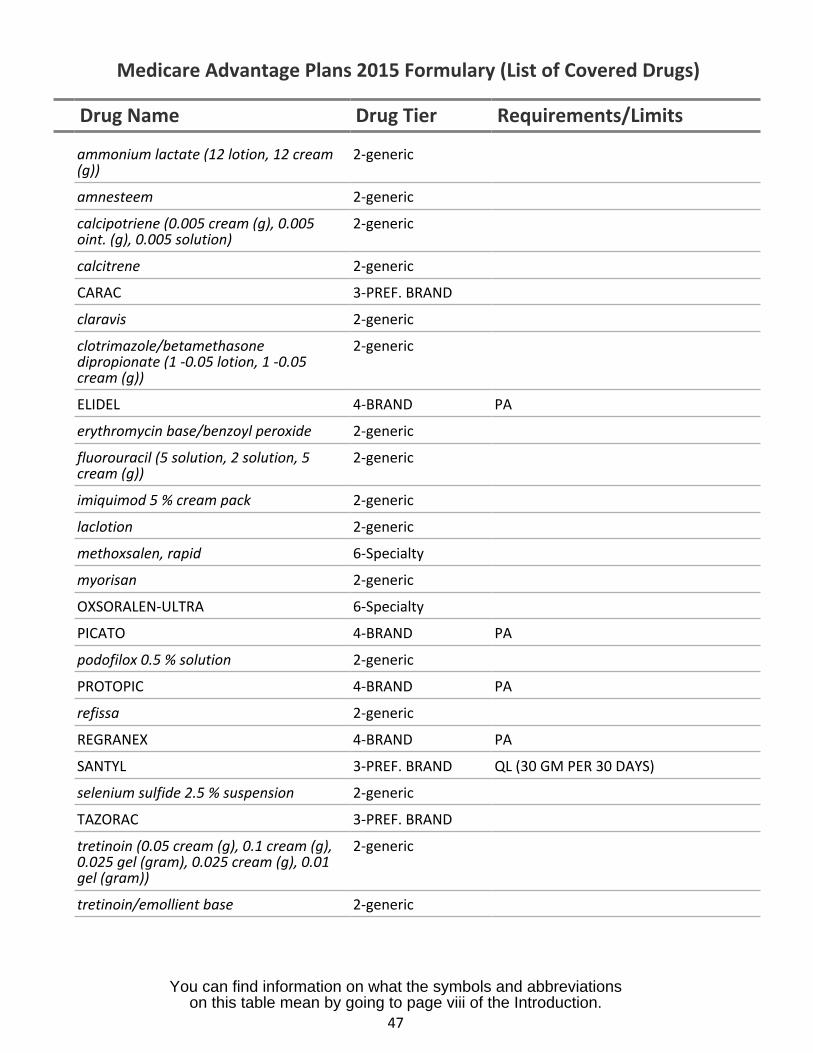
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
ammonium lactate (12 lotion, 12 cream(g))
2-generic
amnesteem 2-generic
calcipotriene (0.005 cream (g), 0.005oint. (g), 0.005 solution)
2-generic
calcitrene 2-generic
CARAC 3-PREF. BRAND
claravis 2-generic
clotrimazole/betamethasonedipropionate (1 -0.05 lotion, 1 -0.05cream (g))
2-generic
ELIDEL 4-BRAND PA
erythromycin base/benzoyl peroxide 2-generic
fluorouracil (5 solution, 2 solution, 5cream (g))
2-generic
imiquimod 5 % cream pack 2-generic
laclotion 2-generic
methoxsalen, rapid 6-Specialty
myorisan 2-generic
OXSORALEN-ULTRA 6-Specialty
PICATO 4-BRAND PA
podofilox 0.5 % solution 2-generic
PROTOPIC 4-BRAND PA
refissa 2-generic
REGRANEX 4-BRAND PA
SANTYL 3-PREF. BRAND QL (30 GM PER 30 DAYS)
selenium sulfide 2.5 % suspension 2-generic
TAZORAC 3-PREF. BRAND
tretinoin (0.05 cream (g), 0.1 cream (g),0.025 gel (gram), 0.025 cream (g), 0.01gel (gram))
2-generic
tretinoin/emollient base 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
47
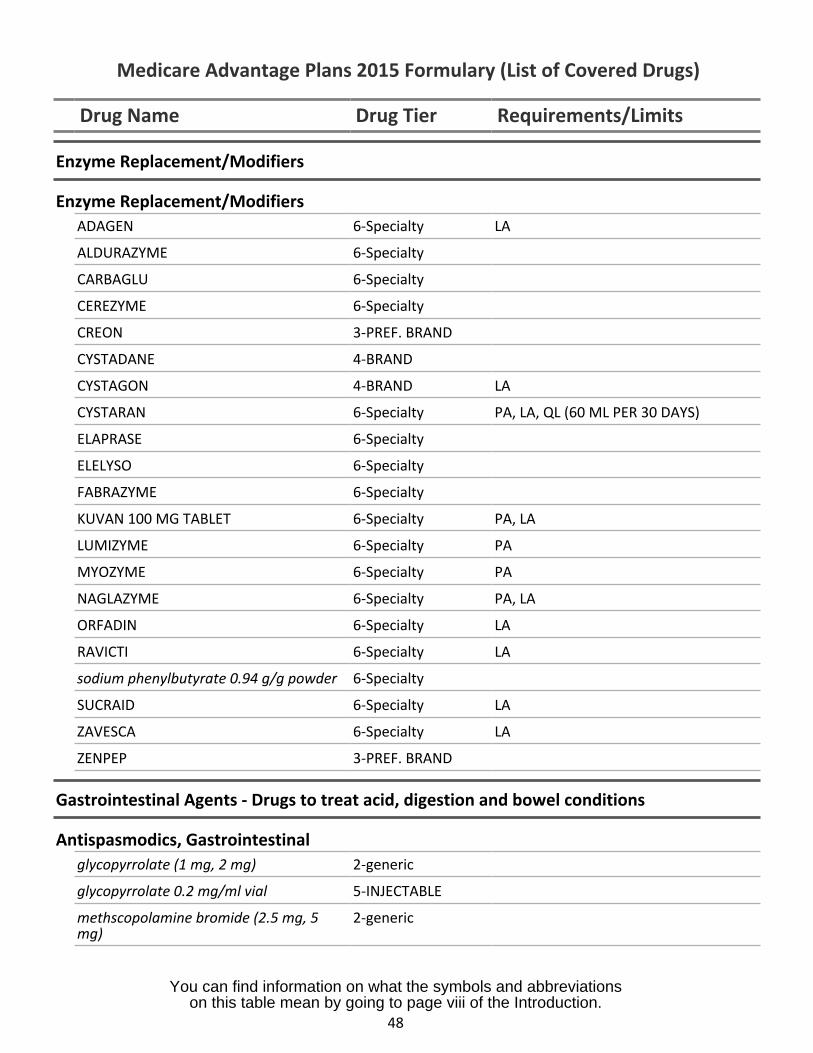
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Enzyme Replacement/Modifiers
Enzyme Replacement/ModifiersADAGEN 6-Specialty LA
ALDURAZYME 6-Specialty
CARBAGLU 6-Specialty
CEREZYME 6-Specialty
CREON 3-PREF. BRAND
CYSTADANE 4-BRAND
CYSTAGON 4-BRAND LA
CYSTARAN 6-Specialty PA, LA, QL (60 ML PER 30 DAYS)
ELAPRASE 6-Specialty
ELELYSO 6-Specialty
FABRAZYME 6-Specialty
KUVAN 100 MG TABLET 6-Specialty PA, LA
LUMIZYME 6-Specialty PA
MYOZYME 6-Specialty PA
NAGLAZYME 6-Specialty PA, LA
ORFADIN 6-Specialty LA
RAVICTI 6-Specialty LA
sodium phenylbutyrate 0.94 g/g powder 6-Specialty
SUCRAID 6-Specialty LA
ZAVESCA 6-Specialty LA
ZENPEP 3-PREF. BRAND
Gastrointestinal Agents - Drugs to treat acid, digestion and bowel conditions
Antispasmodics, Gastrointestinalglycopyrrolate (1 mg, 2 mg) 2-generic
glycopyrrolate 0.2 mg/ml vial 5-INJECTABLE
methscopolamine bromide (2.5 mg, 5mg)
2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
48
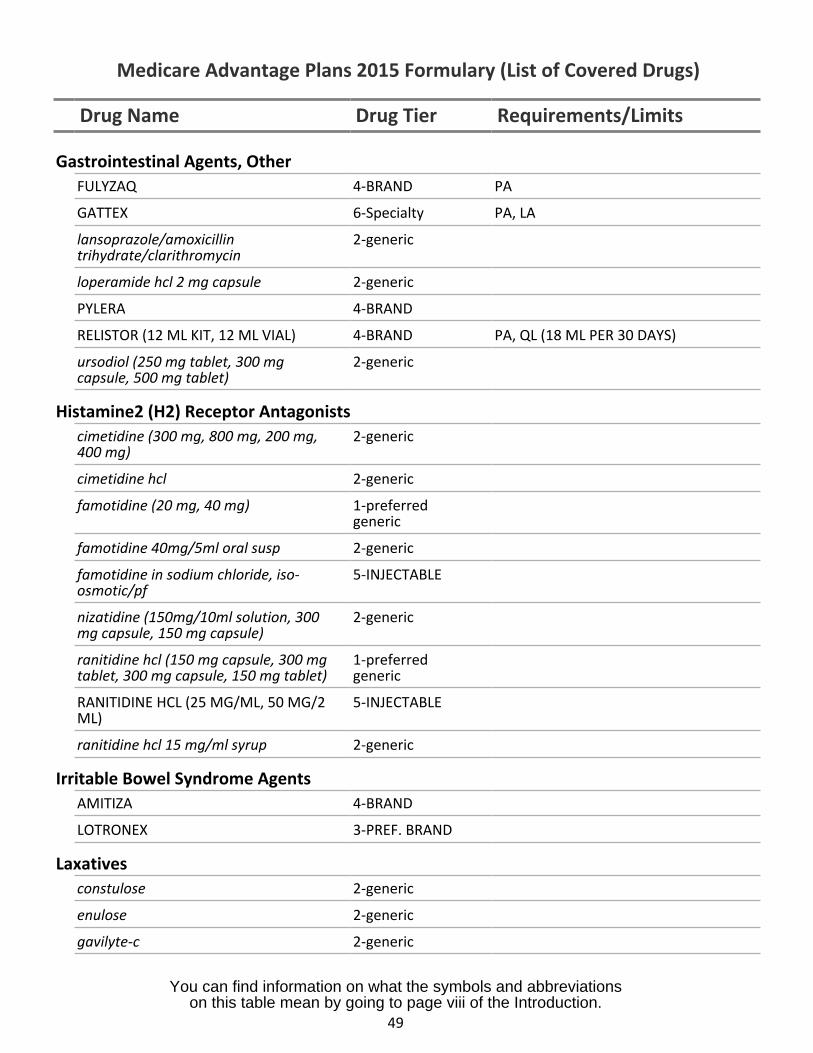
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Gastrointestinal Agents, OtherFULYZAQ 4-BRAND PA
GATTEX 6-Specialty PA, LA
lansoprazole/amoxicillin 2-generictrihydrate/clarithromycin
loperamide hcl 2 mg capsule 2-generic
PYLERA 4-BRAND
RELISTOR (12 ML KIT, 12 ML VIAL) 4-BRAND PA, QL (18 ML PER 30 DAYS)
ursodiol (250 mg tablet, 300 mg 2-genericcapsule, 500 mg tablet)
Histamine2 (H2) Receptor Antagonistscimetidine (300 mg, 800 mg, 200 mg, 2-generic400 mg)
cimetidine hcl 2-generic
famotidine (20 mg, 40 mg) 1-preferredgeneric
famotidine 40mg/5ml oral susp 2-generic
famotidine in sodium chloride, iso- 5-INJECTABLEosmotic/pf
nizatidine (150mg/10ml solution, 300 2-genericmg capsule, 150 mg capsule)
ranitidine hcl (150 mg capsule, 300 mg 1-preferredtablet, 300 mg capsule, 150 mg tablet) generic
RANITIDINE HCL (25 MG/ML, 50 MG/2 5-INJECTABLEML)
ranitidine hcl 15 mg/ml syrup 2-generic
Irritable Bowel Syndrome AgentsAMITIZA 4-BRAND
LOTRONEX 3-PREF. BRAND
Laxativesconstulose 2-generic
enulose 2-generic
gavilyte-c 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
49
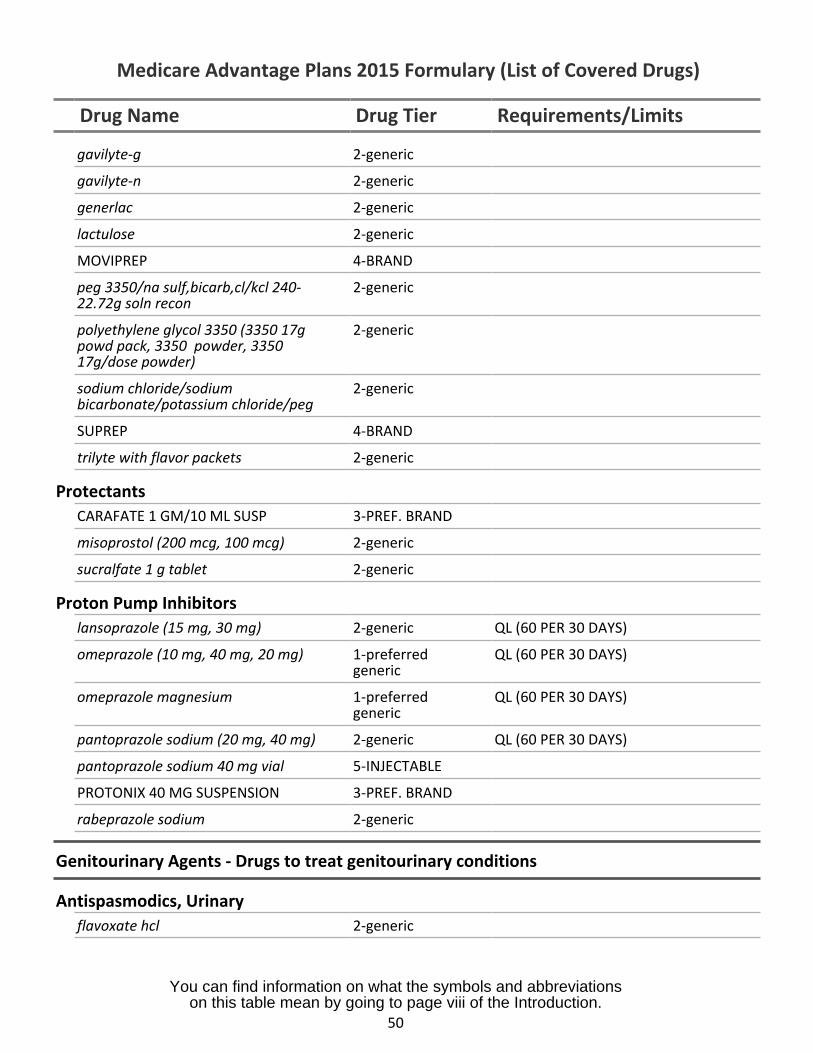
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
gavilyte-g 2-generic
gavilyte-n 2-generic
generlac 2-generic
lactulose 2-generic
MOVIPREP 4-BRAND
peg 3350/na sulf,bicarb,cl/kcl 240-22.72g soln recon
2-generic
polyethylene glycol 3350 (3350 17gpowd pack, 3350 powder, 335017g/dose powder)
2-generic
sodium chloride/sodiumbicarbonate/potassium chloride/peg
2-generic
SUPREP 4-BRAND
trilyte with flavor packets 2-generic
ProtectantsCARAFATE 1 GM/10 ML SUSP 3-PREF. BRAND
misoprostol (200 mcg, 100 mcg) 2-generic
sucralfate 1 g tablet 2-generic
Proton Pump Inhibitorslansoprazole (15 mg, 30 mg) 2-generic QL (60 PER 30 DAYS)
omeprazole (10 mg, 40 mg, 20 mg) 1-preferredgeneric
QL (60 PER 30 DAYS)
omeprazole magnesium 1-preferredgeneric
QL (60 PER 30 DAYS)
pantoprazole sodium (20 mg, 40 mg) 2-generic QL (60 PER 30 DAYS)
pantoprazole sodium 40 mg vial 5-INJECTABLE
PROTONIX 40 MG SUSPENSION 3-PREF. BRAND
rabeprazole sodium 2-generic
Genitourinary Agents - Drugs to treat genitourinary conditions
Antispasmodics, Urinaryflavoxate hcl 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
50
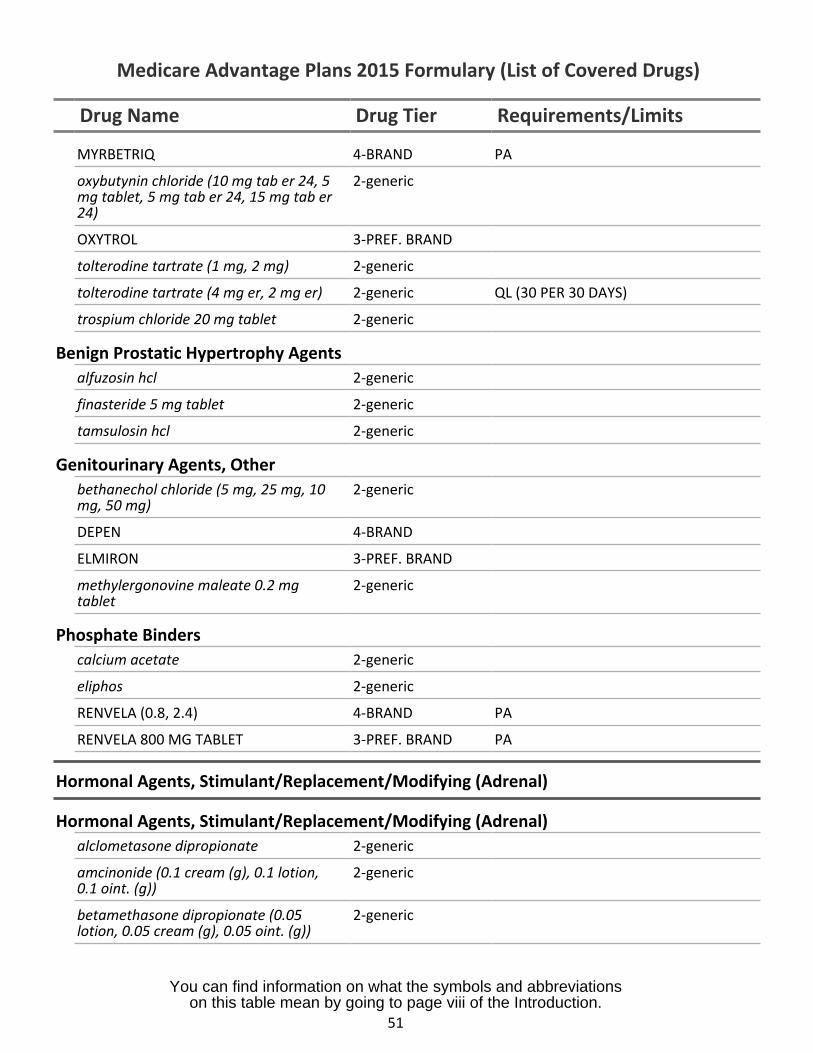
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
MYRBETRIQ 4-BRAND PA
oxybutynin chloride (10 mg tab er 24, 5mg tablet, 5 mg tab er 24, 15 mg tab er24)
2-generic
OXYTROL 3-PREF. BRAND
tolterodine tartrate (1 mg, 2 mg) 2-generic
tolterodine tartrate (4 mg er, 2 mg er) 2-generic QL (30 PER 30 DAYS)
trospium chloride 20 mg tablet 2-generic
Benign Prostatic Hypertrophy Agentsalfuzosin hcl 2-generic
finasteride 5 mg tablet 2-generic
tamsulosin hcl 2-generic
Genitourinary Agents, Otherbethanechol chloride (5 mg, 25 mg, 10mg, 50 mg)
2-generic
DEPEN 4-BRAND
ELMIRON 3-PREF. BRAND
methylergonovine maleate 0.2 mgtablet
2-generic
Phosphate Binderscalcium acetate 2-generic
eliphos 2-generic
RENVELA (0.8, 2.4) 4-BRAND PA
RENVELA 800 MG TABLET 3-PREF. BRAND PA
Hormonal Agents, Stimulant/Replacement/Modifying (Adrenal)
Hormonal Agents, Stimulant/Replacement/Modifying (Adrenal)alclometasone dipropionate 2-generic
amcinonide (0.1 cream (g), 0.1 lotion, 2-generic0.1 oint. (g))
betamethasone dipropionate (0.05 2-genericlotion, 0.05 cream (g), 0.05 oint. (g))
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
51
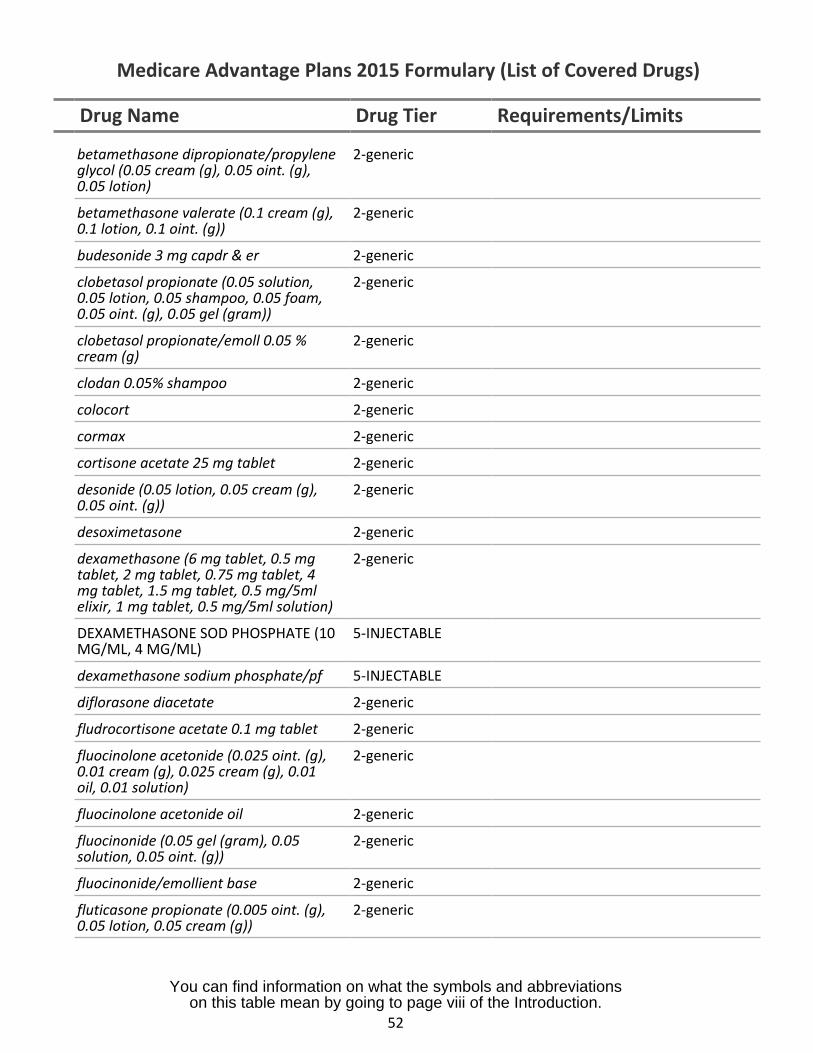
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
betamethasone dipropionate/propylene 2-genericglycol (0.05 cream (g), 0.05 oint. (g),0.05 lotion)
betamethasone valerate (0.1 cream (g), 2-generic0.1 lotion, 0.1 oint. (g))
budesonide 3 mg capdr & er 2-generic
clobetasol propionate (0.05 solution, 2-generic0.05 lotion, 0.05 shampoo, 0.05 foam,0.05 oint. (g), 0.05 gel (gram))
clobetasol propionate/emoll 0.05 % 2-genericcream (g)
clodan 0.05% shampoo 2-generic
colocort 2-generic
cormax 2-generic
cortisone acetate 25 mg tablet 2-generic
desonide (0.05 lotion, 0.05 cream (g), 2-generic0.05 oint. (g))
desoximetasone 2-generic
dexamethasone (6 mg tablet, 0.5 mg 2-generictablet, 2 mg tablet, 0.75 mg tablet, 4mg tablet, 1.5 mg tablet, 0.5 mg/5mlelixir, 1 mg tablet, 0.5 mg/5ml solution)
DEXAMETHASONE SOD PHOSPHATE (10 5-INJECTABLEMG/ML, 4 MG/ML)
dexamethasone sodium phosphate/pf 5-INJECTABLE
diflorasone diacetate 2-generic
fludrocortisone acetate 0.1 mg tablet 2-generic
fluocinolone acetonide (0.025 oint. (g), 2-generic0.01 cream (g), 0.025 cream (g), 0.01oil, 0.01 solution)
fluocinolone acetonide oil 2-generic
fluocinonide (0.05 gel (gram), 0.05 2-genericsolution, 0.05 oint. (g))
fluocinonide/emollient base 2-generic
fluticasone propionate (0.005 oint. (g), 2-generic0.05 lotion, 0.05 cream (g))
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
52
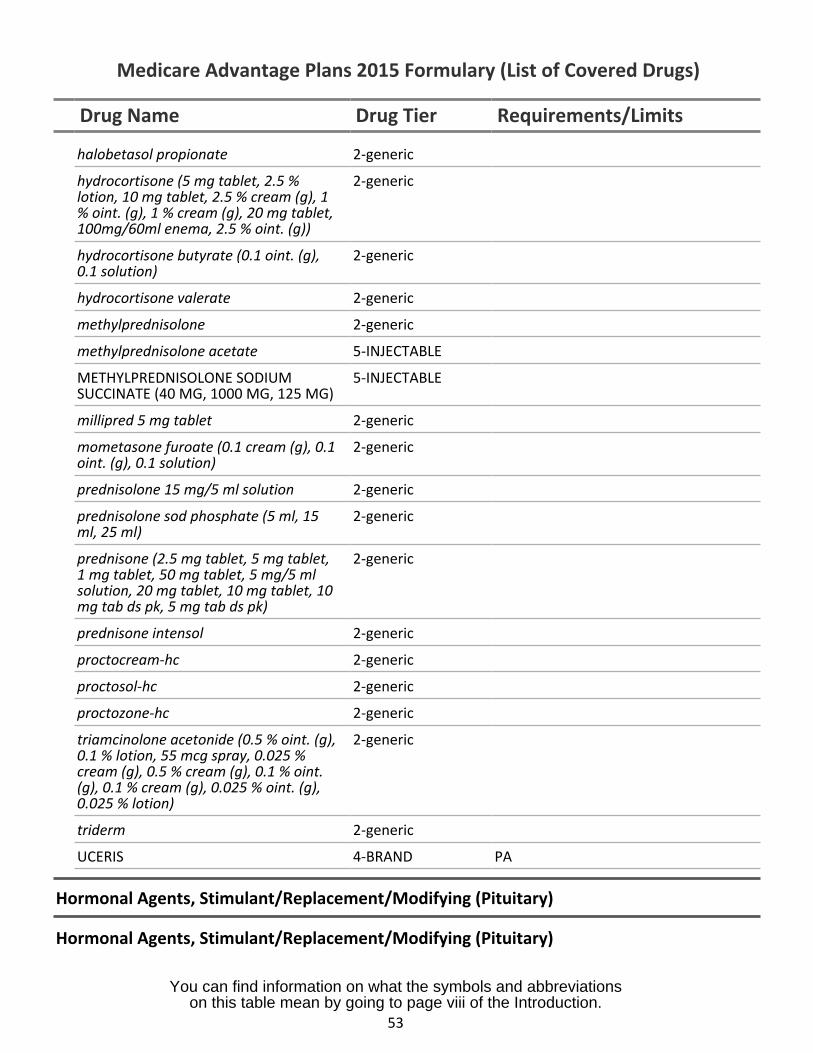
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
halobetasol propionate 2-generic
hydrocortisone (5 mg tablet, 2.5 %lotion, 10 mg tablet, 2.5 % cream (g), 1% oint. (g), 1 % cream (g), 20 mg tablet,100mg/60ml enema, 2.5 % oint. (g))
2-generic
hydrocortisone butyrate (0.1 oint. (g),0.1 solution)
2-generic
hydrocortisone valerate 2-generic
methylprednisolone 2-generic
methylprednisolone acetate 5-INJECTABLE
METHYLPREDNISOLONE SODIUMSUCCINATE (40 MG, 1000 MG, 125 MG)
5-INJECTABLE
millipred 5 mg tablet 2-generic
mometasone furoate (0.1 cream (g), 0.1oint. (g), 0.1 solution)
2-generic
prednisolone 15 mg/5 ml solution 2-generic
prednisolone sod phosphate (5 ml, 15ml, 25 ml)
2-generic
prednisone (2.5 mg tablet, 5 mg tablet,1 mg tablet, 50 mg tablet, 5 mg/5 mlsolution, 20 mg tablet, 10 mg tablet, 10mg tab ds pk, 5 mg tab ds pk)
2-generic
prednisone intensol 2-generic
proctocream-hc 2-generic
proctosol-hc 2-generic
proctozone-hc 2-generic
triamcinolone acetonide (0.5 % oint. (g),0.1 % lotion, 55 mcg spray, 0.025 %cream (g), 0.5 % cream (g), 0.1 % oint.(g), 0.1 % cream (g), 0.025 % oint. (g),0.025 % lotion)
2-generic
triderm 2-generic
UCERIS 4-BRAND PA
Hormonal Agents, Stimulant/Replacement/Modifying (Pituitary)
Hormonal Agents, Stimulant/Replacement/Modifying (Pituitary)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
53
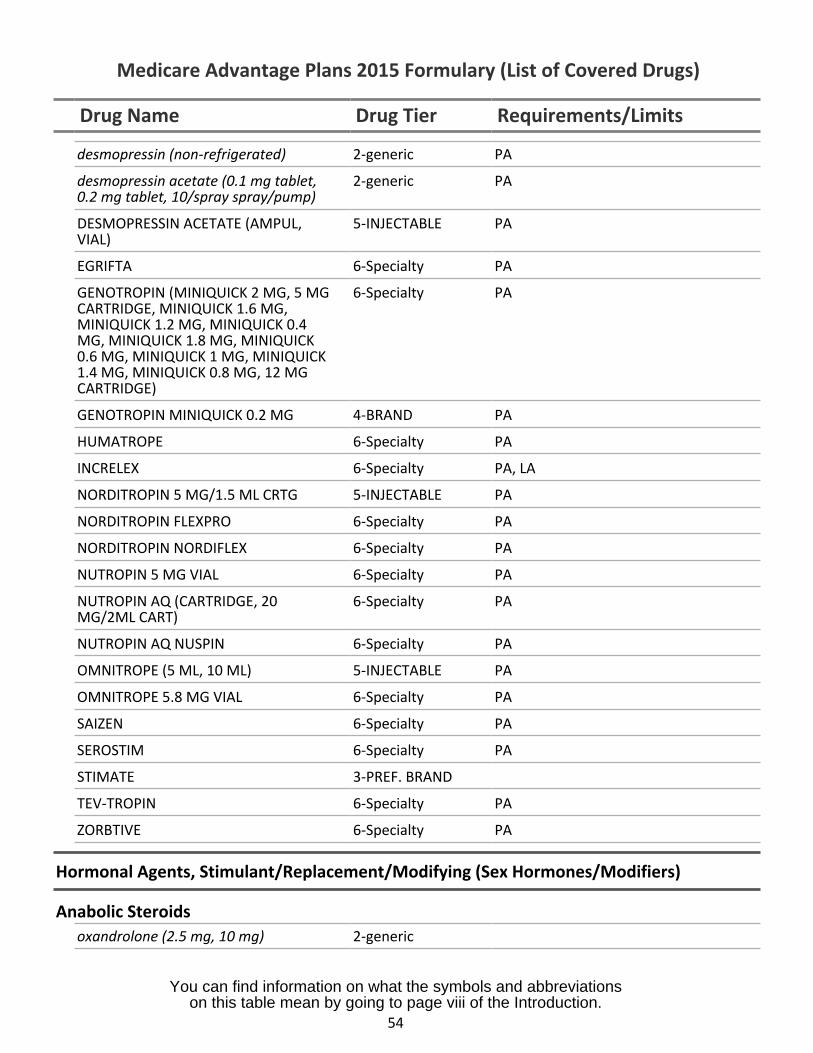
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
desmopressin (non-refrigerated) 2-generic PA
desmopressin acetate (0.1 mg tablet,0.2 mg tablet, 10/spray spray/pump)
2-generic PA
DESMOPRESSIN ACETATE (AMPUL,VIAL)
5-INJECTABLE PA
EGRIFTA 6-Specialty PA
GENOTROPIN (MINIQUICK 2 MG, 5 MGCARTRIDGE, MINIQUICK 1.6 MG,MINIQUICK 1.2 MG, MINIQUICK 0.4MG, MINIQUICK 1.8 MG, MINIQUICK0.6 MG, MINIQUICK 1 MG, MINIQUICK1.4 MG, MINIQUICK 0.8 MG, 12 MGCARTRIDGE)
6-Specialty PA
GENOTROPIN MINIQUICK 0.2 MG 4-BRAND PA
HUMATROPE 6-Specialty PA
INCRELEX 6-Specialty PA, LA
NORDITROPIN 5 MG/1.5 ML CRTG 5-INJECTABLE PA
NORDITROPIN FLEXPRO 6-Specialty PA
NORDITROPIN NORDIFLEX 6-Specialty PA
NUTROPIN 5 MG VIAL 6-Specialty PA
NUTROPIN AQ (CARTRIDGE, 20MG/2ML CART)
6-Specialty PA
NUTROPIN AQ NUSPIN 6-Specialty PA
OMNITROPE (5 ML, 10 ML) 5-INJECTABLE PA
OMNITROPE 5.8 MG VIAL 6-Specialty PA
SAIZEN 6-Specialty PA
SEROSTIM 6-Specialty PA
STIMATE 3-PREF. BRAND
TEV-TROPIN 6-Specialty PA
ZORBTIVE 6-Specialty PA
Hormonal Agents, Stimulant/Replacement/Modifying (Sex Hormones/Modifiers)
Anabolic Steroidsoxandrolone (2.5 mg, 10 mg) 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
54
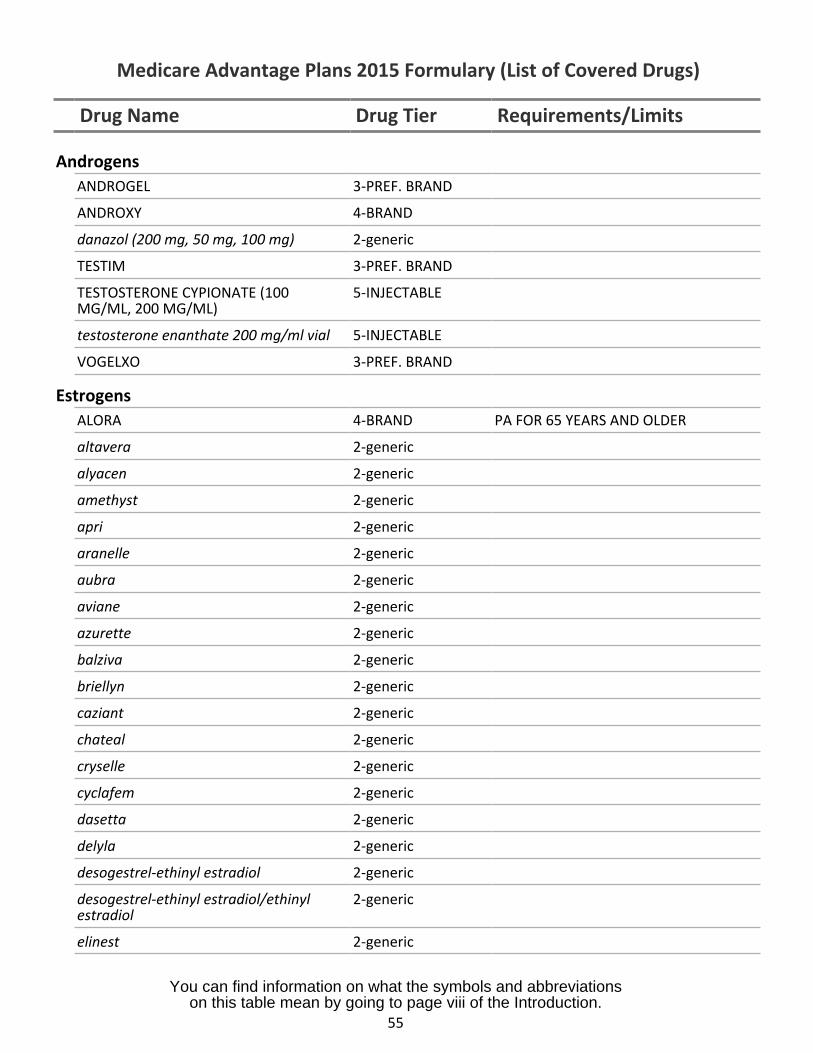
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
AndrogensANDROGEL 3-PREF. BRAND
ANDROXY 4-BRAND
danazol (200 mg, 50 mg, 100 mg) 2-generic
TESTIM 3-PREF. BRAND
TESTOSTERONE CYPIONATE (100MG/ML, 200 MG/ML)
5-INJECTABLE
testosterone enanthate 200 mg/ml vial 5-INJECTABLE
VOGELXO 3-PREF. BRAND
EstrogensALORA 4-BRAND PA FOR 65 YEARS AND OLDER
altavera 2-generic
alyacen 2-generic
amethyst 2-generic
apri 2-generic
aranelle 2-generic
aubra 2-generic
aviane 2-generic
azurette 2-generic
balziva 2-generic
briellyn 2-generic
caziant 2-generic
chateal 2-generic
cryselle 2-generic
cyclafem 2-generic
dasetta 2-generic
delyla 2-generic
desogestrel-ethinyl estradiol 2-generic
desogestrel-ethinyl estradiol/ethinylestradiol
2-generic
elinest 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
55
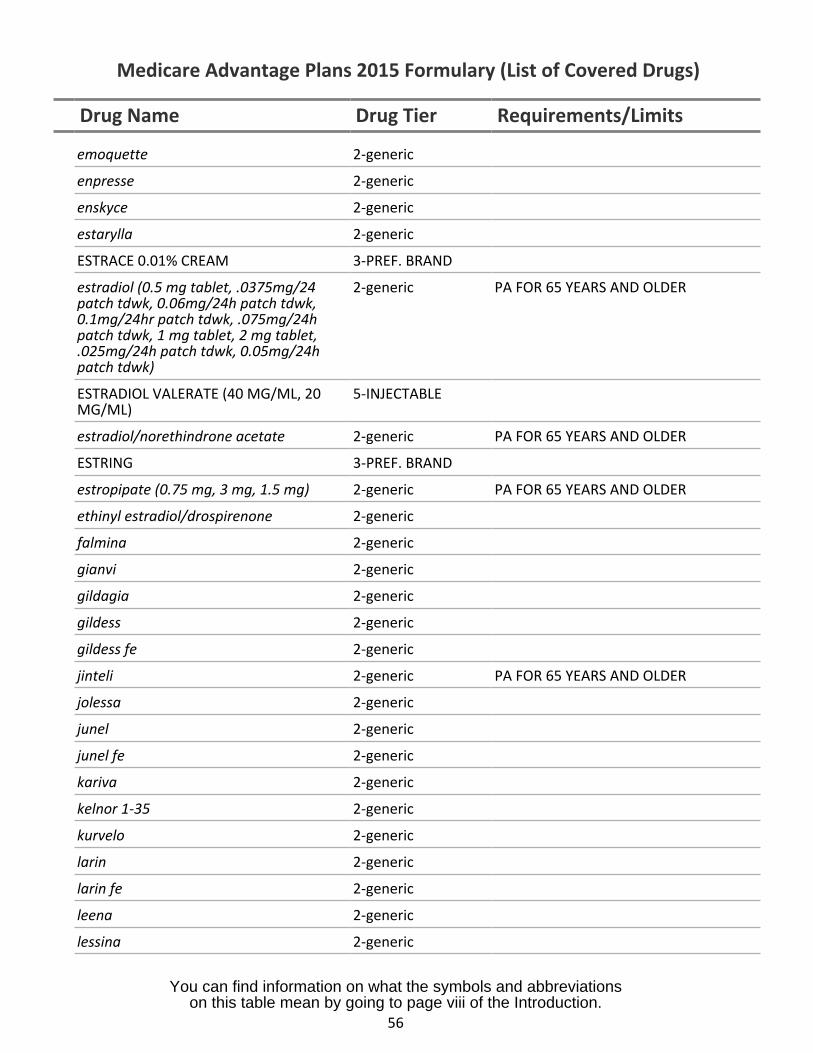
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
emoquette 2-generic
enpresse 2-generic
enskyce 2-generic
estarylla 2-generic
ESTRACE 0.01% CREAM 3-PREF. BRAND
estradiol (0.5 mg tablet, .0375mg/24 2-generic PA FOR 65 YEARS AND OLDERpatch tdwk, 0.06mg/24h patch tdwk,0.1mg/24hr patch tdwk, .075mg/24hpatch tdwk, 1 mg tablet, 2 mg tablet,.025mg/24h patch tdwk, 0.05mg/24hpatch tdwk)
ESTRADIOL VALERATE (40 MG/ML, 20 5-INJECTABLEMG/ML)
estradiol/norethindrone acetate 2-generic PA FOR 65 YEARS AND OLDER
ESTRING 3-PREF. BRAND
estropipate (0.75 mg, 3 mg, 1.5 mg) 2-generic PA FOR 65 YEARS AND OLDER
ethinyl estradiol/drospirenone 2-generic
falmina 2-generic
gianvi 2-generic
gildagia 2-generic
gildess 2-generic
gildess fe 2-generic
jinteli 2-generic PA FOR 65 YEARS AND OLDER
jolessa 2-generic
junel 2-generic
junel fe 2-generic
kariva 2-generic
kelnor 1-35 2-generic
kurvelo 2-generic
larin 2-generic
larin fe 2-generic
leena 2-generic
lessina 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
56
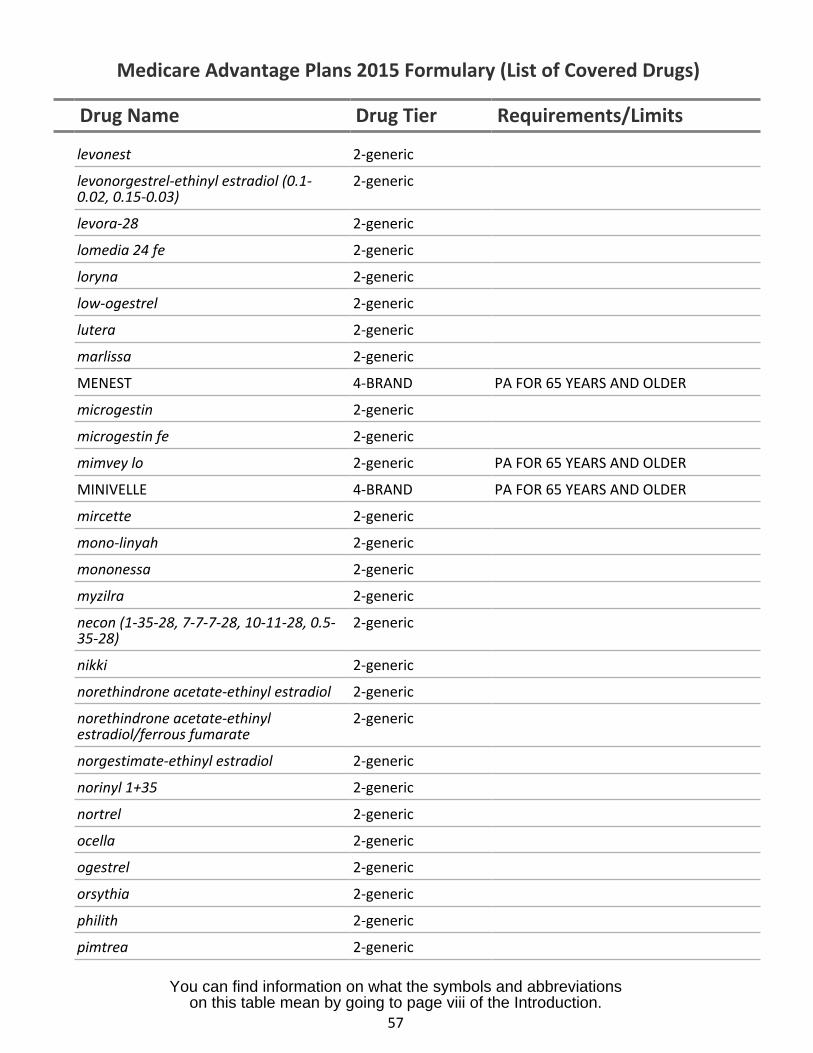
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
levonest 2-generic
levonorgestrel-ethinyl estradiol (0.1-0.02, 0.15-0.03)
2-generic
levora-28 2-generic
lomedia 24 fe 2-generic
loryna 2-generic
low-ogestrel 2-generic
lutera 2-generic
marlissa 2-generic
MENEST 4-BRAND PA FOR 65 YEARS AND OLDER
microgestin 2-generic
microgestin fe 2-generic
mimvey lo 2-generic PA FOR 65 YEARS AND OLDER
MINIVELLE 4-BRAND PA FOR 65 YEARS AND OLDER
mircette 2-generic
mono-linyah 2-generic
mononessa 2-generic
myzilra 2-generic
necon (1-35-28, 7-7-7-28, 10-11-28, 0.5-35-28)
2-generic
nikki 2-generic
norethindrone acetate-ethinyl estradiol 2-generic
norethindrone acetate-ethinylestradiol/ferrous fumarate
2-generic
norgestimate-ethinyl estradiol 2-generic
norinyl 1+35 2-generic
nortrel 2-generic
ocella 2-generic
ogestrel 2-generic
orsythia 2-generic
philith 2-generic
pimtrea 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
57
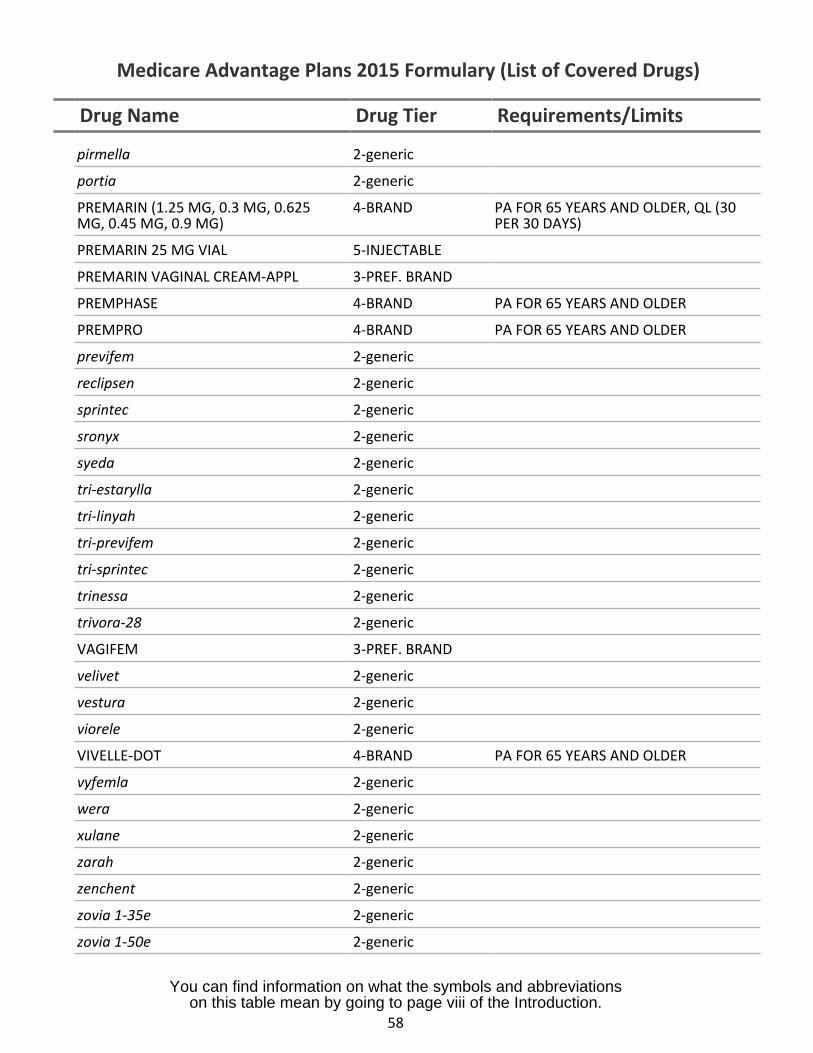
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
pirmella 2-generic
portia 2-generic
PREMARIN (1.25 MG, 0.3 MG, 0.625MG, 0.45 MG, 0.9 MG)
4-BRAND PA FOR 65 YEARS AND OLDER, QL (30PER 30 DAYS)
PREMARIN 25 MG VIAL 5-INJECTABLE
PREMARIN VAGINAL CREAM-APPL 3-PREF. BRAND
PREMPHASE 4-BRAND PA FOR 65 YEARS AND OLDER
PREMPRO 4-BRAND PA FOR 65 YEARS AND OLDER
previfem 2-generic
reclipsen 2-generic
sprintec 2-generic
sronyx 2-generic
syeda 2-generic
tri-estarylla 2-generic
tri-linyah 2-generic
tri-previfem 2-generic
tri-sprintec 2-generic
trinessa 2-generic
trivora-28 2-generic
VAGIFEM 3-PREF. BRAND
velivet 2-generic
vestura 2-generic
viorele 2-generic
VIVELLE-DOT 4-BRAND PA FOR 65 YEARS AND OLDER
vyfemla 2-generic
wera 2-generic
xulane 2-generic
zarah 2-generic
zenchent 2-generic
zovia 1-35e 2-generic
zovia 1-50e 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
58
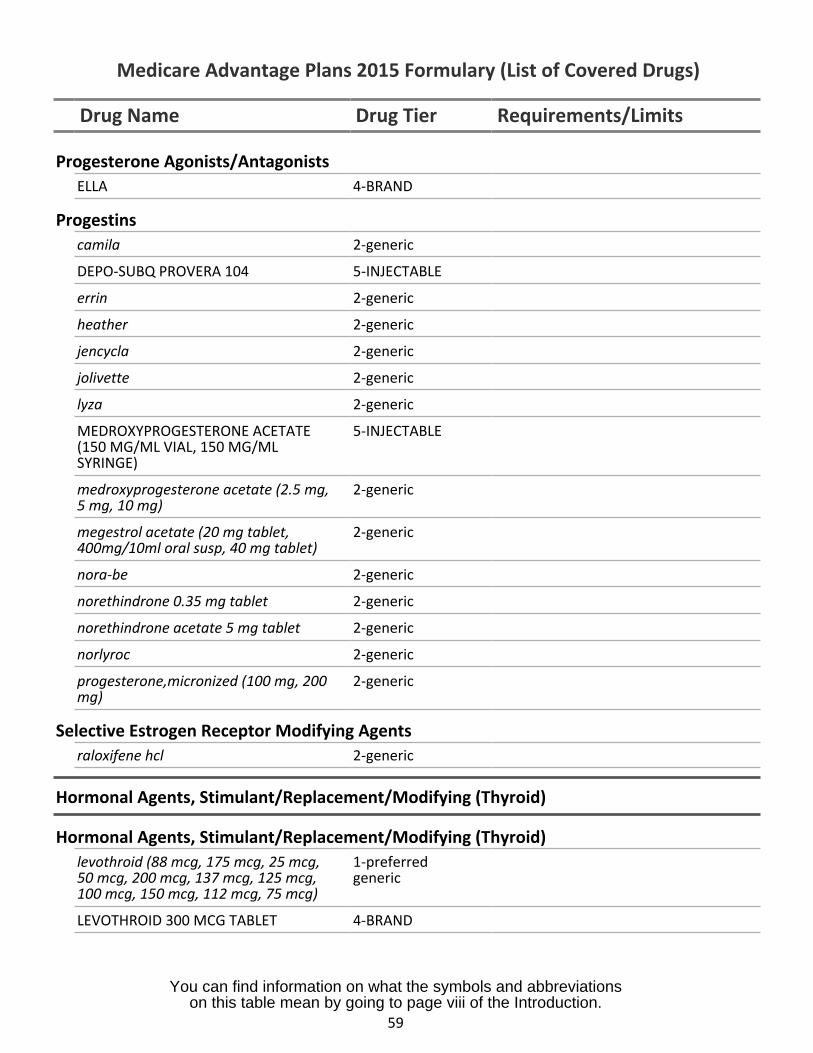
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Progesterone Agonists/AntagonistsELLA 4-BRAND
Progestinscamila 2-generic
DEPO-SUBQ PROVERA 104 5-INJECTABLE
errin 2-generic
heather 2-generic
jencycla 2-generic
jolivette 2-generic
lyza 2-generic
MEDROXYPROGESTERONE ACETATE 5-INJECTABLE(150 MG/ML VIAL, 150 MG/MLSYRINGE)
medroxyprogesterone acetate (2.5 mg, 2-generic5 mg, 10 mg)
megestrol acetate (20 mg tablet, 2-generic400mg/10ml oral susp, 40 mg tablet)
nora-be 2-generic
norethindrone 0.35 mg tablet 2-generic
norethindrone acetate 5 mg tablet 2-generic
norlyroc 2-generic
progesterone,micronized (100 mg, 200 2-genericmg)
Selective Estrogen Receptor Modifying Agentsraloxifene hcl 2-generic
Hormonal Agents, Stimulant/Replacement/Modifying (Thyroid)
Hormonal Agents, Stimulant/Replacement/Modifying (Thyroid)levothroid (88 mcg, 175 mcg, 25 mcg, 1-preferred50 mcg, 200 mcg, 137 mcg, 125 mcg, generic100 mcg, 150 mcg, 112 mcg, 75 mcg)
LEVOTHROID 300 MCG TABLET 4-BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
59
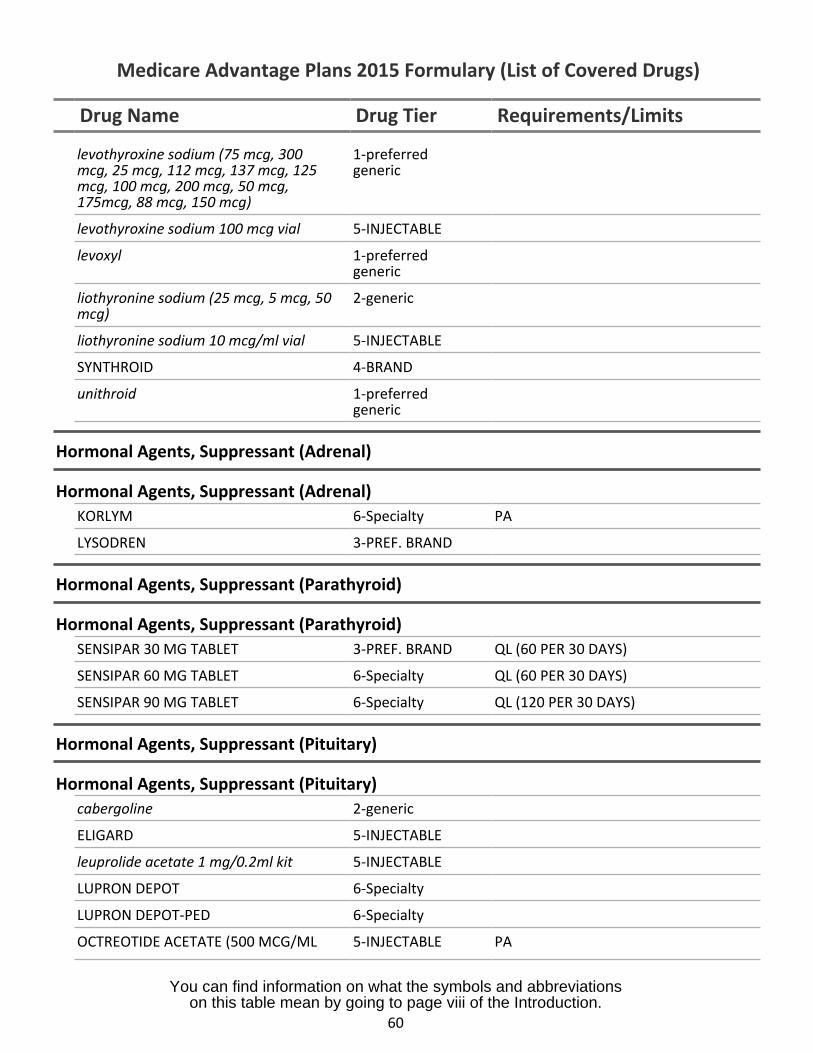
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
levothyroxine sodium (75 mcg, 300mcg, 25 mcg, 112 mcg, 137 mcg, 125mcg, 100 mcg, 200 mcg, 50 mcg,175mcg, 88 mcg, 150 mcg)
1-preferredgeneric
levothyroxine sodium 100 mcg vial 5-INJECTABLE
levoxyl 1-preferredgeneric
liothyronine sodium (25 mcg, 5 mcg, 50mcg)
2-generic
liothyronine sodium 10 mcg/ml vial 5-INJECTABLE
SYNTHROID 4-BRAND
unithroid 1-preferredgeneric
Hormonal Agents, Suppressant (Adrenal)
Hormonal Agents, Suppressant (Adrenal)KORLYM 6-Specialty PA
LYSODREN 3-PREF. BRAND
Hormonal Agents, Suppressant (Parathyroid)
Hormonal Agents, Suppressant (Parathyroid)SENSIPAR 30 MG TABLET 3-PREF. BRAND QL (60 PER 30 DAYS)
SENSIPAR 60 MG TABLET 6-Specialty QL (60 PER 30 DAYS)
SENSIPAR 90 MG TABLET 6-Specialty QL (120 PER 30 DAYS)
Hormonal Agents, Suppressant (Pituitary)
Hormonal Agents, Suppressant (Pituitary)cabergoline 2-generic
ELIGARD 5-INJECTABLE
leuprolide acetate 1 mg/0.2ml kit 5-INJECTABLE
LUPRON DEPOT 6-Specialty
LUPRON DEPOT-PED 6-Specialty
OCTREOTIDE ACETATE (500 MCG/ML 5-INJECTABLE PA
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
60
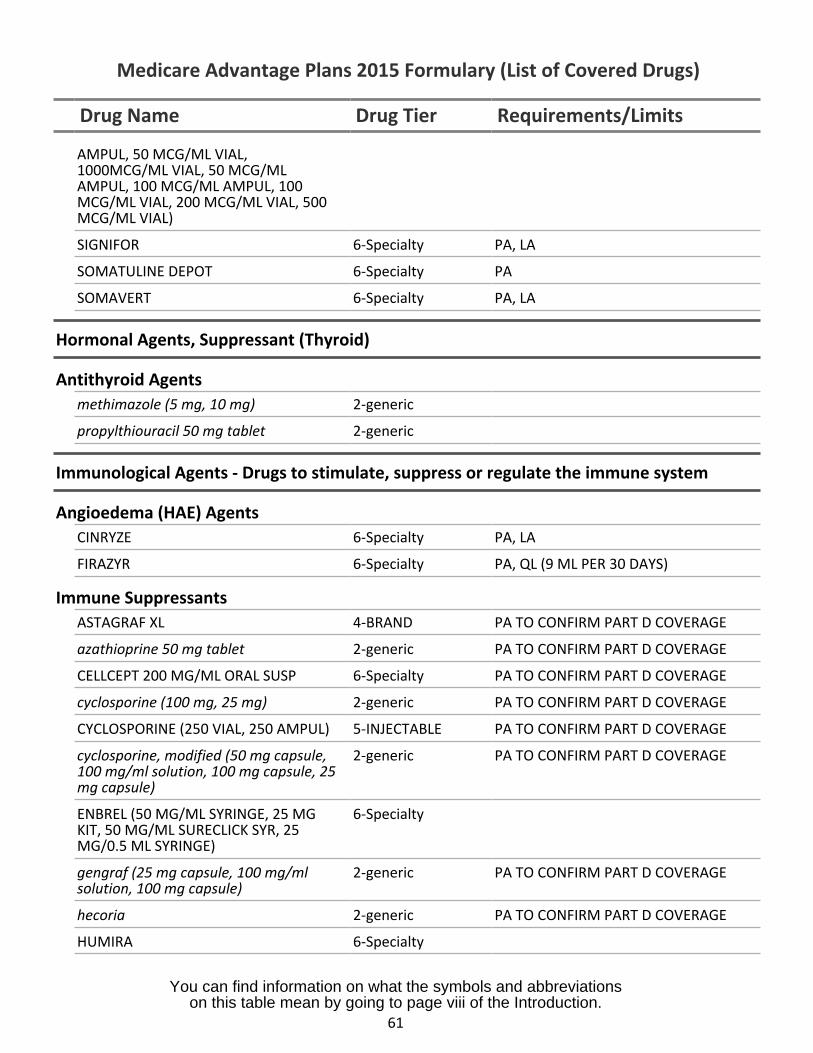
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
AMPUL, 50 MCG/ML VIAL,1000MCG/ML VIAL, 50 MCG/MLAMPUL, 100 MCG/ML AMPUL, 100MCG/ML VIAL, 200 MCG/ML VIAL, 500MCG/ML VIAL)
SIGNIFOR 6-Specialty PA, LA
SOMATULINE DEPOT 6-Specialty PA
SOMAVERT 6-Specialty PA, LA
Hormonal Agents, Suppressant (Thyroid)
Antithyroid Agentsmethimazole (5 mg, 10 mg) 2-generic
propylthiouracil 50 mg tablet 2-generic
Immunological Agents - Drugs to stimulate, suppress or regulate the immune system
Angioedema (HAE) AgentsCINRYZE 6-Specialty PA, LA
FIRAZYR 6-Specialty PA, QL (9 ML PER 30 DAYS)
Immune SuppressantsASTAGRAF XL 4-BRAND PA TO CONFIRM PART D COVERAGE
azathioprine 50 mg tablet 2-generic PA TO CONFIRM PART D COVERAGE
CELLCEPT 200 MG/ML ORAL SUSP 6-Specialty PA TO CONFIRM PART D COVERAGE
cyclosporine (100 mg, 25 mg) 2-generic PA TO CONFIRM PART D COVERAGE
CYCLOSPORINE (250 VIAL, 250 AMPUL) 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
cyclosporine, modified (50 mg capsule,100 mg/ml solution, 100 mg capsule, 25mg capsule)
2-generic PA TO CONFIRM PART D COVERAGE
ENBREL (50 MG/ML SYRINGE, 25 MGKIT, 50 MG/ML SURECLICK SYR, 25MG/0.5 ML SYRINGE)
6-Specialty
gengraf (25 mg capsule, 100 mg/mlsolution, 100 mg capsule)
2-generic PA TO CONFIRM PART D COVERAGE
hecoria 2-generic PA TO CONFIRM PART D COVERAGE
HUMIRA 6-Specialty
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
61
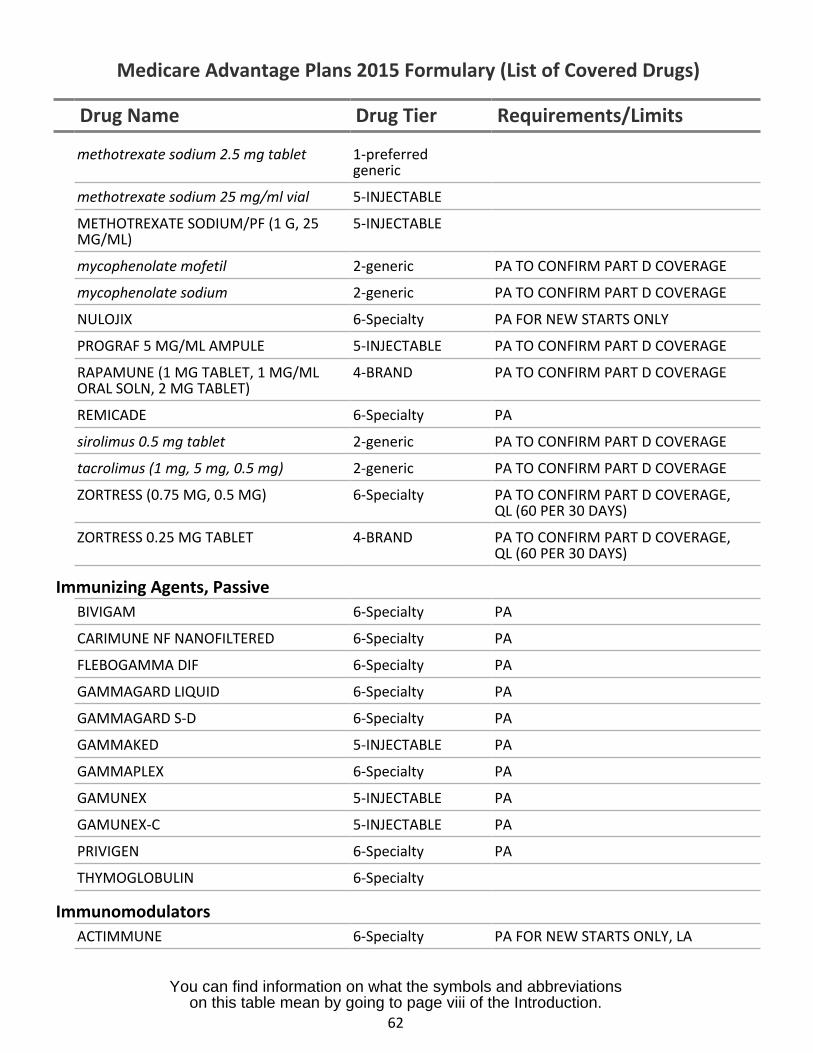
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
methotrexate sodium 2.5 mg tablet 1-preferredgeneric
methotrexate sodium 25 mg/ml vial 5-INJECTABLE
METHOTREXATE SODIUM/PF (1 G, 25MG/ML)
5-INJECTABLE
mycophenolate mofetil 2-generic PA TO CONFIRM PART D COVERAGE
mycophenolate sodium 2-generic PA TO CONFIRM PART D COVERAGE
NULOJIX 6-Specialty PA FOR NEW STARTS ONLY
PROGRAF 5 MG/ML AMPULE 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
RAPAMUNE (1 MG TABLET, 1 MG/MLORAL SOLN, 2 MG TABLET)
4-BRAND PA TO CONFIRM PART D COVERAGE
REMICADE 6-Specialty PA
sirolimus 0.5 mg tablet 2-generic PA TO CONFIRM PART D COVERAGE
tacrolimus (1 mg, 5 mg, 0.5 mg) 2-generic PA TO CONFIRM PART D COVERAGE
ZORTRESS (0.75 MG, 0.5 MG) 6-Specialty PA TO CONFIRM PART D COVERAGE,QL (60 PER 30 DAYS)
ZORTRESS 0.25 MG TABLET 4-BRAND PA TO CONFIRM PART D COVERAGE,QL (60 PER 30 DAYS)
Immunizing Agents, PassiveBIVIGAM 6-Specialty PA
CARIMUNE NF NANOFILTERED 6-Specialty PA
FLEBOGAMMA DIF 6-Specialty PA
GAMMAGARD LIQUID 6-Specialty PA
GAMMAGARD S-D 6-Specialty PA
GAMMAKED 5-INJECTABLE PA
GAMMAPLEX 6-Specialty PA
GAMUNEX 5-INJECTABLE PA
GAMUNEX-C 5-INJECTABLE PA
PRIVIGEN 6-Specialty PA
THYMOGLOBULIN 6-Specialty
ImmunomodulatorsACTIMMUNE 6-Specialty PA FOR NEW STARTS ONLY, LA
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
62
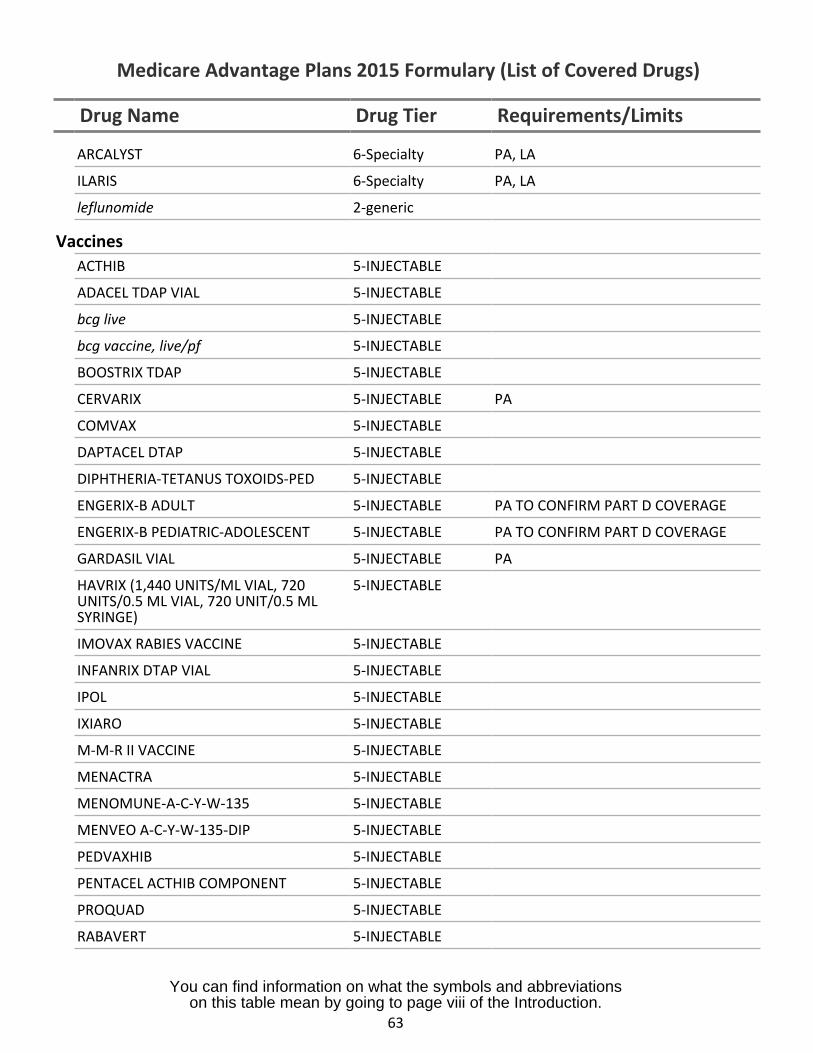
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
ARCALYST 6-Specialty PA, LA
ILARIS 6-Specialty PA, LA
leflunomide 2-generic
VaccinesACTHIB 5-INJECTABLE
ADACEL TDAP VIAL 5-INJECTABLE
bcg live 5-INJECTABLE
bcg vaccine, live/pf 5-INJECTABLE
BOOSTRIX TDAP 5-INJECTABLE
CERVARIX 5-INJECTABLE PA
COMVAX 5-INJECTABLE
DAPTACEL DTAP 5-INJECTABLE
DIPHTHERIA-TETANUS TOXOIDS-PED 5-INJECTABLE
ENGERIX-B ADULT 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
ENGERIX-B PEDIATRIC-ADOLESCENT 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
GARDASIL VIAL 5-INJECTABLE PA
HAVRIX (1,440 UNITS/ML VIAL, 720UNITS/0.5 ML VIAL, 720 UNIT/0.5 MLSYRINGE)
5-INJECTABLE
IMOVAX RABIES VACCINE 5-INJECTABLE
INFANRIX DTAP VIAL 5-INJECTABLE
IPOL 5-INJECTABLE
IXIARO 5-INJECTABLE
M-M-R II VACCINE 5-INJECTABLE
MENACTRA 5-INJECTABLE
MENOMUNE-A-C-Y-W-135 5-INJECTABLE
MENVEO A-C-Y-W-135-DIP 5-INJECTABLE
PEDVAXHIB 5-INJECTABLE
PENTACEL ACTHIB COMPONENT 5-INJECTABLE
PROQUAD 5-INJECTABLE
RABAVERT 5-INJECTABLE
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
63
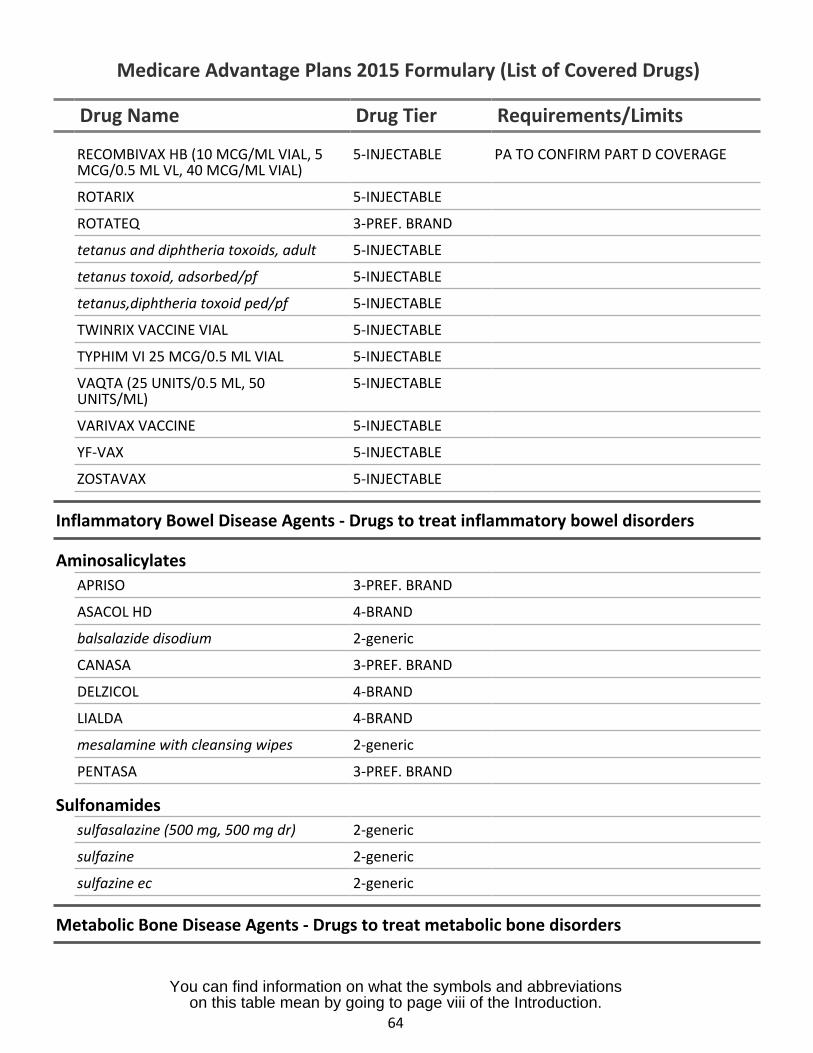
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
RECOMBIVAX HB (10 MCG/ML VIAL, 5MCG/0.5 ML VL, 40 MCG/ML VIAL)
5-INJECTABLE PA TO CONFIRM PART D COVERAGE
ROTARIX 5-INJECTABLE
ROTATEQ 3-PREF. BRAND
tetanus and diphtheria toxoids, adult 5-INJECTABLE
tetanus toxoid, adsorbed/pf 5-INJECTABLE
tetanus,diphtheria toxoid ped/pf 5-INJECTABLE
TWINRIX VACCINE VIAL 5-INJECTABLE
TYPHIM VI 25 MCG/0.5 ML VIAL 5-INJECTABLE
VAQTA (25 UNITS/0.5 ML, 50UNITS/ML)
5-INJECTABLE
VARIVAX VACCINE 5-INJECTABLE
YF-VAX 5-INJECTABLE
ZOSTAVAX 5-INJECTABLE
Inflammatory Bowel Disease Agents - Drugs to treat inflammatory bowel disorders
AminosalicylatesAPRISO 3-PREF. BRAND
ASACOL HD 4-BRAND
balsalazide disodium 2-generic
CANASA 3-PREF. BRAND
DELZICOL 4-BRAND
LIALDA 4-BRAND
mesalamine with cleansing wipes 2-generic
PENTASA 3-PREF. BRAND
Sulfonamidessulfasalazine (500 mg, 500 mg dr) 2-generic
sulfazine 2-generic
sulfazine ec 2-generic
Metabolic Bone Disease Agents - Drugs to treat metabolic bone disorders
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
64
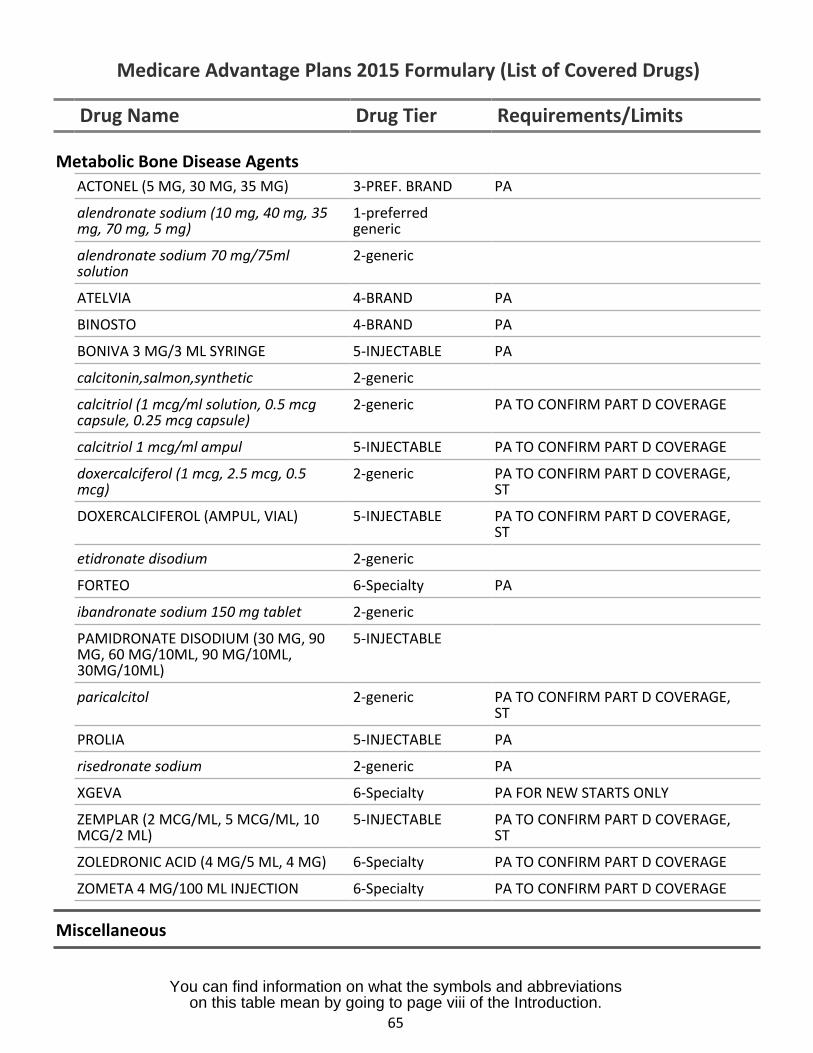
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Metabolic Bone Disease AgentsACTONEL (5 MG, 30 MG, 35 MG) 3-PREF. BRAND PA
alendronate sodium (10 mg, 40 mg, 35mg, 70 mg, 5 mg)
1-preferredgeneric
alendronate sodium 70 mg/75mlsolution
2-generic
ATELVIA 4-BRAND PA
BINOSTO 4-BRAND PA
BONIVA 3 MG/3 ML SYRINGE 5-INJECTABLE PA
calcitonin,salmon,synthetic 2-generic
calcitriol (1 mcg/ml solution, 0.5 mcgcapsule, 0.25 mcg capsule)
2-generic PA TO CONFIRM PART D COVERAGE
calcitriol 1 mcg/ml ampul 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
doxercalciferol (1 mcg, 2.5 mcg, 0.5mcg)
2-generic PA TO CONFIRM PART D COVERAGE,ST
DOXERCALCIFEROL (AMPUL, VIAL) 5-INJECTABLE PA TO CONFIRM PART D COVERAGE,ST
etidronate disodium 2-generic
FORTEO 6-Specialty PA
ibandronate sodium 150 mg tablet 2-generic
PAMIDRONATE DISODIUM (30 MG, 90MG, 60 MG/10ML, 90 MG/10ML,30MG/10ML)
5-INJECTABLE
paricalcitol 2-generic PA TO CONFIRM PART D COVERAGE,ST
PROLIA 5-INJECTABLE PA
risedronate sodium 2-generic PA
XGEVA 6-Specialty PA FOR NEW STARTS ONLY
ZEMPLAR (2 MCG/ML, 5 MCG/ML, 10MCG/2 ML)
5-INJECTABLE PA TO CONFIRM PART D COVERAGE,ST
ZOLEDRONIC ACID (4 MG/5 ML, 4 MG) 6-Specialty PA TO CONFIRM PART D COVERAGE
ZOMETA 4 MG/100 ML INJECTION 6-Specialty PA TO CONFIRM PART D COVERAGE
Miscellaneous
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
65
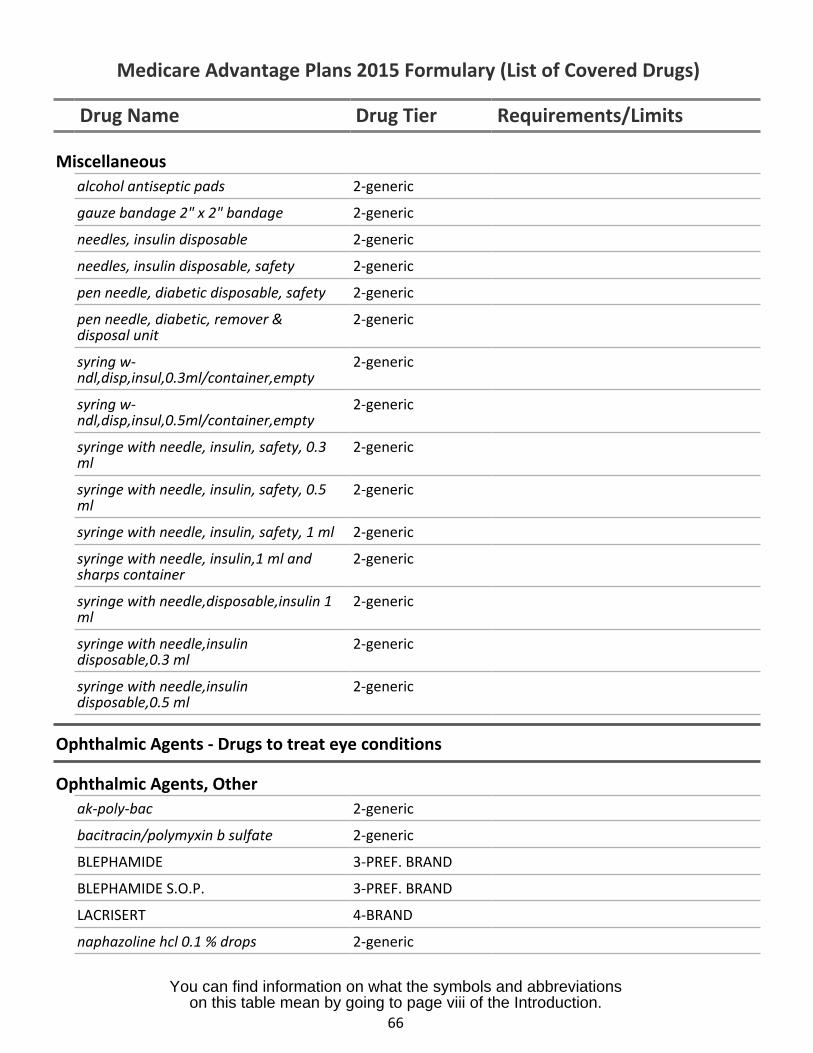
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Miscellaneousalcohol antiseptic pads 2-generic
gauze bandage 2" x 2" bandage 2-generic
needles, insulin disposable 2-generic
needles, insulin disposable, safety 2-generic
pen needle, diabetic disposable, safety 2-generic
pen needle, diabetic, remover &disposal unit
2-generic
syring w-ndl,disp,insul,0.3ml/container,empty
2-generic
syring w-ndl,disp,insul,0.5ml/container,empty
2-generic
syringe with needle, insulin, safety, 0.3ml
2-generic
syringe with needle, insulin, safety, 0.5ml
2-generic
syringe with needle, insulin, safety, 1 ml 2-generic
syringe with needle, insulin,1 ml andsharps container
2-generic
syringe with needle,disposable,insulin 1ml
2-generic
syringe with needle,insulindisposable,0.3 ml
2-generic
syringe with needle,insulindisposable,0.5 ml
2-generic
Ophthalmic Agents - Drugs to treat eye conditions
Ophthalmic Agents, Otherak-poly-bac 2-generic
bacitracin/polymyxin b sulfate 2-generic
BLEPHAMIDE 3-PREF. BRAND
BLEPHAMIDE S.O.P. 3-PREF. BRAND
LACRISERT 4-BRAND
naphazoline hcl 0.1 % drops 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
66
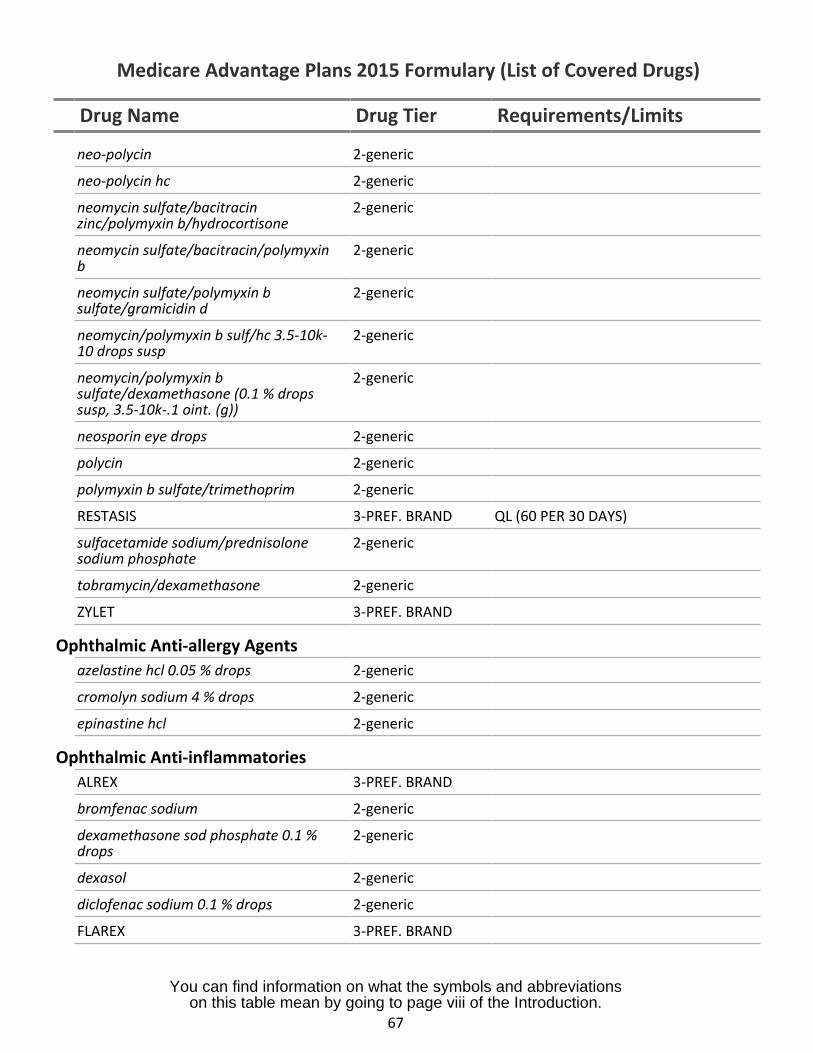
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
neo-polycin 2-generic
neo-polycin hc 2-generic
neomycin sulfate/bacitracinzinc/polymyxin b/hydrocortisone
2-generic
neomycin sulfate/bacitracin/polymyxinb
2-generic
neomycin sulfate/polymyxin bsulfate/gramicidin d
2-generic
neomycin/polymyxin b sulf/hc 3.5-10k-10 drops susp
2-generic
neomycin/polymyxin bsulfate/dexamethasone (0.1 % dropssusp, 3.5-10k-.1 oint. (g))
2-generic
neosporin eye drops 2-generic
polycin 2-generic
polymyxin b sulfate/trimethoprim 2-generic
RESTASIS 3-PREF. BRAND QL (60 PER 30 DAYS)
sulfacetamide sodium/prednisolonesodium phosphate
2-generic
tobramycin/dexamethasone 2-generic
ZYLET 3-PREF. BRAND
Ophthalmic Anti-allergy Agentsazelastine hcl 0.05 % drops 2-generic
cromolyn sodium 4 % drops 2-generic
epinastine hcl 2-generic
Ophthalmic Anti-inflammatoriesALREX 3-PREF. BRAND
bromfenac sodium 2-generic
dexamethasone sod phosphate 0.1 %drops
2-generic
dexasol 2-generic
diclofenac sodium 0.1 % drops 2-generic
FLAREX 3-PREF. BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
67
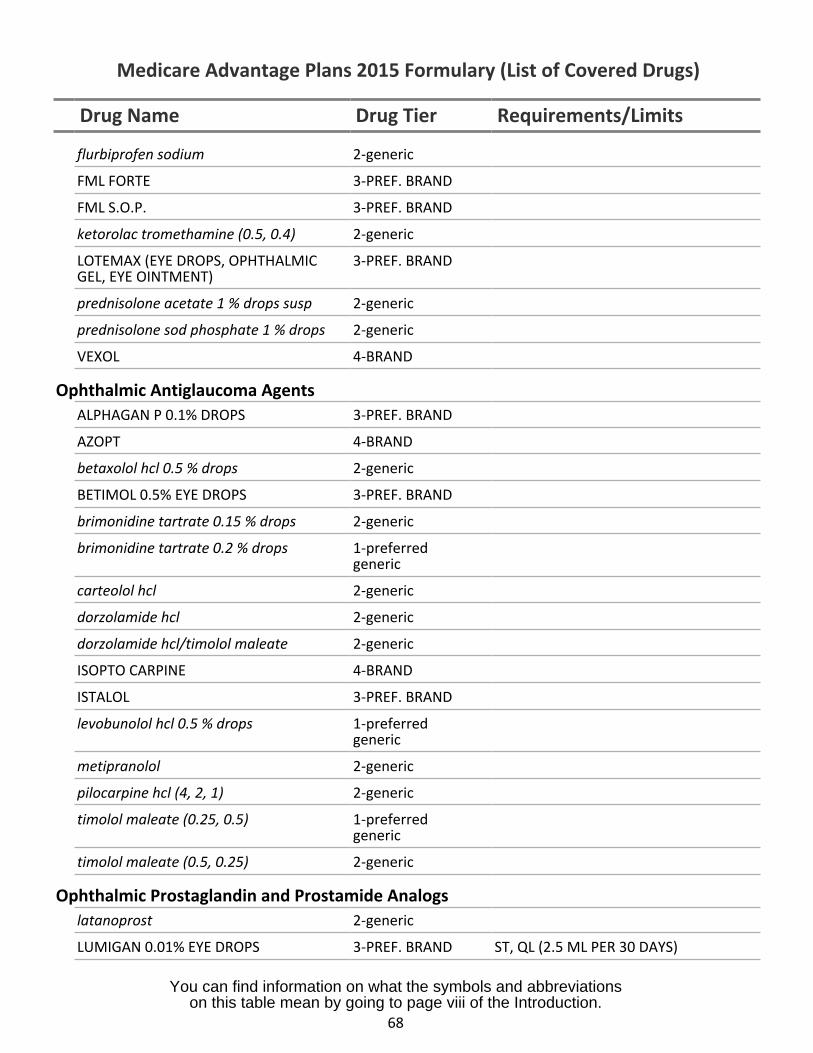
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
flurbiprofen sodium 2-generic
FML FORTE 3-PREF. BRAND
FML S.O.P. 3-PREF. BRAND
ketorolac tromethamine (0.5, 0.4) 2-generic
LOTEMAX (EYE DROPS, OPHTHALMIC 3-PREF. BRANDGEL, EYE OINTMENT)
prednisolone acetate 1 % drops susp 2-generic
prednisolone sod phosphate 1 % drops 2-generic
VEXOL 4-BRAND
Ophthalmic Antiglaucoma AgentsALPHAGAN P 0.1% DROPS 3-PREF. BRAND
AZOPT 4-BRAND
betaxolol hcl 0.5 % drops 2-generic
BETIMOL 0.5% EYE DROPS 3-PREF. BRAND
brimonidine tartrate 0.15 % drops 2-generic
brimonidine tartrate 0.2 % drops 1-preferredgeneric
carteolol hcl 2-generic
dorzolamide hcl 2-generic
dorzolamide hcl/timolol maleate 2-generic
ISOPTO CARPINE 4-BRAND
ISTALOL 3-PREF. BRAND
levobunolol hcl 0.5 % drops 1-preferredgeneric
metipranolol 2-generic
pilocarpine hcl (4, 2, 1) 2-generic
timolol maleate (0.25, 0.5) 1-preferredgeneric
timolol maleate (0.5, 0.25) 2-generic
Ophthalmic Prostaglandin and Prostamide Analogslatanoprost 2-generic
LUMIGAN 0.01% EYE DROPS 3-PREF. BRAND ST, QL (2.5 ML PER 30 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
68
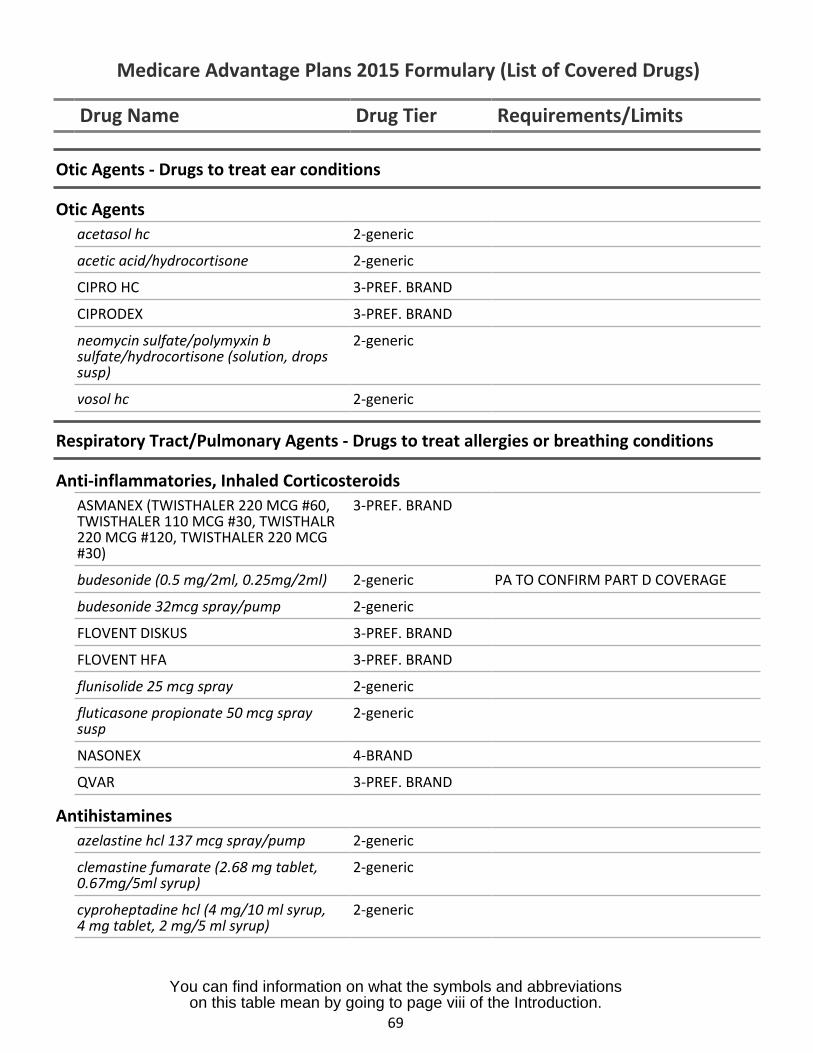
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Otic Agents - Drugs to treat ear conditions
Otic Agentsacetasol hc 2-generic
acetic acid/hydrocortisone 2-generic
CIPRO HC 3-PREF. BRAND
CIPRODEX 3-PREF. BRAND
neomycin sulfate/polymyxin bsulfate/hydrocortisone (solution, dropssusp)
2-generic
vosol hc 2-generic
Respiratory Tract/Pulmonary Agents - Drugs to treat allergies or breathing conditions
Anti-inflammatories, Inhaled CorticosteroidsASMANEX (TWISTHALER 220 MCG #60, 3-PREF. BRANDTWISTHALER 110 MCG #30, TWISTHALR220 MCG #120, TWISTHALER 220 MCG#30)
budesonide (0.5 mg/2ml, 0.25mg/2ml) 2-generic PA TO CONFIRM PART D COVERAGE
budesonide 32mcg spray/pump 2-generic
FLOVENT DISKUS 3-PREF. BRAND
FLOVENT HFA 3-PREF. BRAND
flunisolide 25 mcg spray 2-generic
fluticasone propionate 50 mcg spray 2-genericsusp
NASONEX 4-BRAND
QVAR 3-PREF. BRAND
Antihistaminesazelastine hcl 137 mcg spray/pump 2-generic
clemastine fumarate (2.68 mg tablet, 2-generic0.67mg/5ml syrup)
cyproheptadine hcl (4 mg/10 ml syrup, 2-generic4 mg tablet, 2 mg/5 ml syrup)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
69
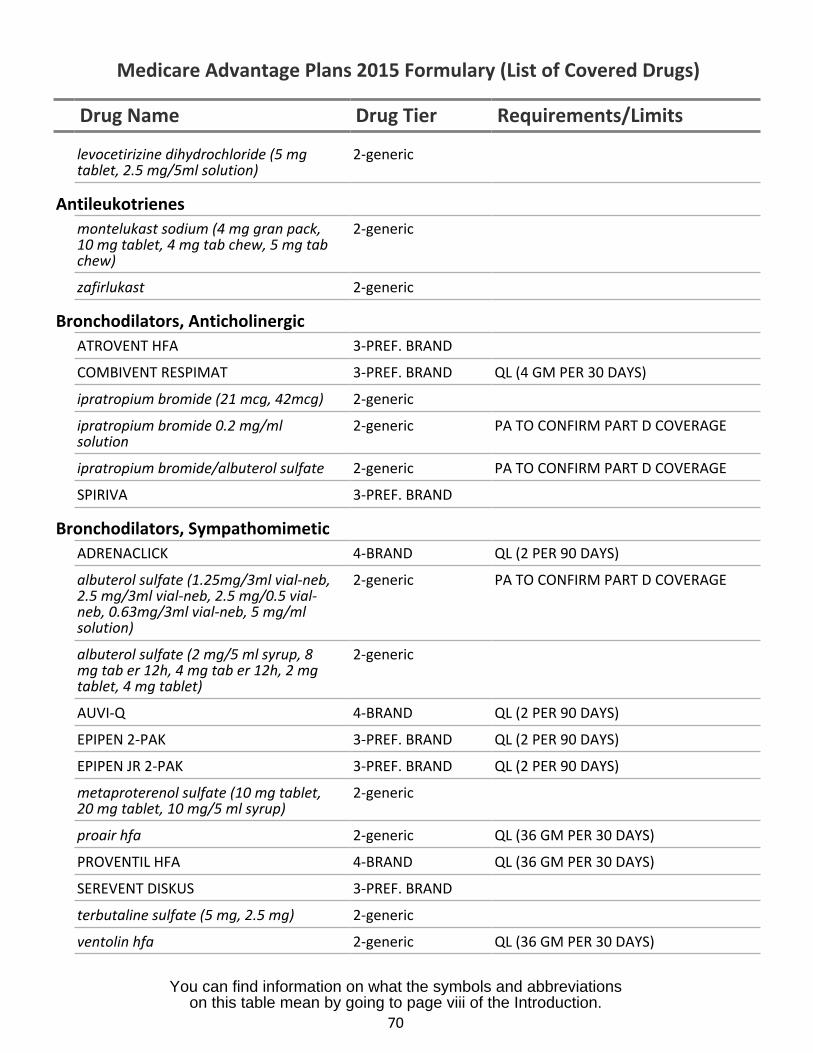
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
levocetirizine dihydrochloride (5 mgtablet, 2.5 mg/5ml solution)
2-generic
Antileukotrienesmontelukast sodium (4 mg gran pack,10 mg tablet, 4 mg tab chew, 5 mg tabchew)
2-generic
zafirlukast 2-generic
Bronchodilators, AnticholinergicATROVENT HFA 3-PREF. BRAND
COMBIVENT RESPIMAT 3-PREF. BRAND QL (4 GM PER 30 DAYS)
ipratropium bromide (21 mcg, 42mcg) 2-generic
ipratropium bromide 0.2 mg/mlsolution
2-generic PA TO CONFIRM PART D COVERAGE
ipratropium bromide/albuterol sulfate 2-generic PA TO CONFIRM PART D COVERAGE
SPIRIVA 3-PREF. BRAND
Bronchodilators, SympathomimeticADRENACLICK 4-BRAND QL (2 PER 90 DAYS)
albuterol sulfate (1.25mg/3ml vial-neb,2.5 mg/3ml vial-neb, 2.5 mg/0.5 vial-neb, 0.63mg/3ml vial-neb, 5 mg/mlsolution)
2-generic PA TO CONFIRM PART D COVERAGE
albuterol sulfate (2 mg/5 ml syrup, 8mg tab er 12h, 4 mg tab er 12h, 2 mgtablet, 4 mg tablet)
2-generic
AUVI-Q 4-BRAND QL (2 PER 90 DAYS)
EPIPEN 2-PAK 3-PREF. BRAND QL (2 PER 90 DAYS)
EPIPEN JR 2-PAK 3-PREF. BRAND QL (2 PER 90 DAYS)
metaproterenol sulfate (10 mg tablet,20 mg tablet, 10 mg/5 ml syrup)
2-generic
proair hfa 2-generic QL (36 GM PER 30 DAYS)
PROVENTIL HFA 4-BRAND QL (36 GM PER 30 DAYS)
SEREVENT DISKUS 3-PREF. BRAND
terbutaline sulfate (5 mg, 2.5 mg) 2-generic
ventolin hfa 2-generic QL (36 GM PER 30 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
70
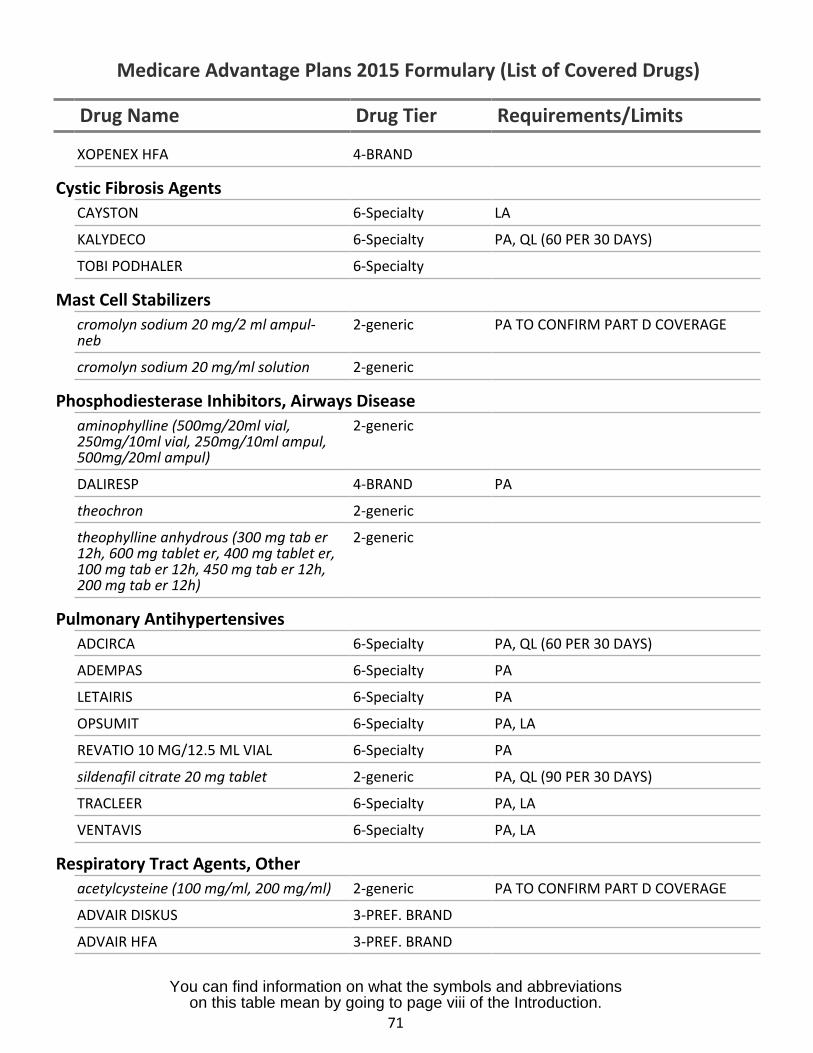
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
XOPENEX HFA 4-BRAND
Cystic Fibrosis AgentsCAYSTON 6-Specialty LA
KALYDECO 6-Specialty PA, QL (60 PER 30 DAYS)
TOBI PODHALER 6-Specialty
Mast Cell Stabilizerscromolyn sodium 20 mg/2 ml ampul- 2-genericneb
PA TO CONFIRM PART D COVERAGE
cromolyn sodium 20 mg/ml solution 2-generic
Phosphodiesterase Inhibitors, Airways Diseaseaminophylline (500mg/20ml vial, 2-generic250mg/10ml vial, 250mg/10ml ampul,500mg/20ml ampul)
DALIRESP 4-BRAND PA
theochron 2-generic
theophylline anhydrous (300 mg tab er 2-generic12h, 600 mg tablet er, 400 mg tablet er,100 mg tab er 12h, 450 mg tab er 12h,200 mg tab er 12h)
Pulmonary AntihypertensivesADCIRCA 6-Specialty PA, QL (60 PER 30 DAYS)
ADEMPAS 6-Specialty PA
LETAIRIS 6-Specialty PA
OPSUMIT 6-Specialty PA, LA
REVATIO 10 MG/12.5 ML VIAL 6-Specialty PA
sildenafil citrate 20 mg tablet 2-generic PA, QL (90 PER 30 DAYS)
TRACLEER 6-Specialty PA, LA
VENTAVIS 6-Specialty PA, LA
Respiratory Tract Agents, Otheracetylcysteine (100 mg/ml, 200 mg/ml) 2-generic PA TO CONFIRM PART D COVERAGE
ADVAIR DISKUS 3-PREF. BRAND
ADVAIR HFA 3-PREF. BRAND
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
71
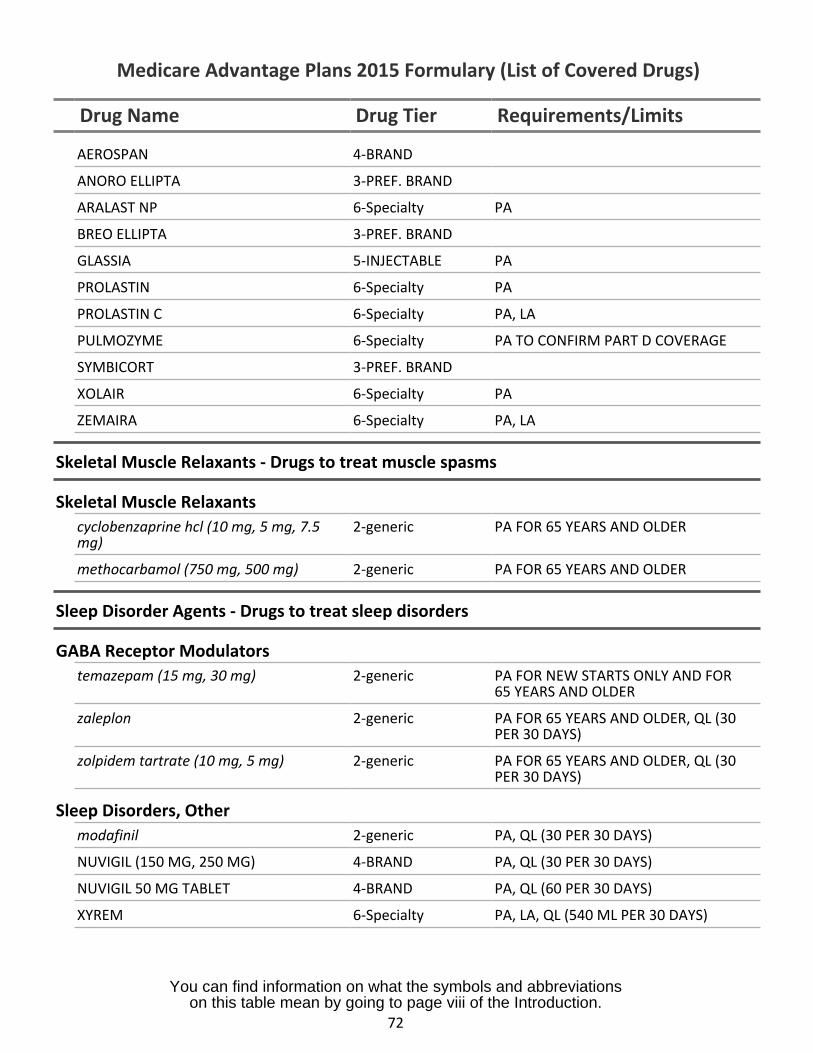
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
AEROSPAN 4-BRAND
ANORO ELLIPTA 3-PREF. BRAND
ARALAST NP 6-Specialty PA
BREO ELLIPTA 3-PREF. BRAND
GLASSIA 5-INJECTABLE PA
PROLASTIN 6-Specialty PA
PROLASTIN C 6-Specialty PA, LA
PULMOZYME 6-Specialty PA TO CONFIRM PART D COVERAGE
SYMBICORT 3-PREF. BRAND
XOLAIR 6-Specialty PA
ZEMAIRA 6-Specialty PA, LA
Skeletal Muscle Relaxants - Drugs to treat muscle spasms
Skeletal Muscle Relaxantscyclobenzaprine hcl (10 mg, 5 mg, 7.5mg)
2-generic PA FOR 65 YEARS AND OLDER
methocarbamol (750 mg, 500 mg) 2-generic PA FOR 65 YEARS AND OLDER
Sleep Disorder Agents - Drugs to treat sleep disorders
GABA Receptor Modulatorstemazepam (15 mg, 30 mg) 2-generic PA FOR NEW STARTS ONLY AND FOR
65 YEARS AND OLDER
zaleplon 2-generic PA FOR 65 YEARS AND OLDER, QL (30PER 30 DAYS)
zolpidem tartrate (10 mg, 5 mg) 2-generic PA FOR 65 YEARS AND OLDER, QL (30PER 30 DAYS)
Sleep Disorders, Othermodafinil 2-generic PA, QL (30 PER 30 DAYS)
NUVIGIL (150 MG, 250 MG) 4-BRAND PA, QL (30 PER 30 DAYS)
NUVIGIL 50 MG TABLET 4-BRAND PA, QL (60 PER 30 DAYS)
XYREM 6-Specialty PA, LA, QL (540 ML PER 30 DAYS)
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
72
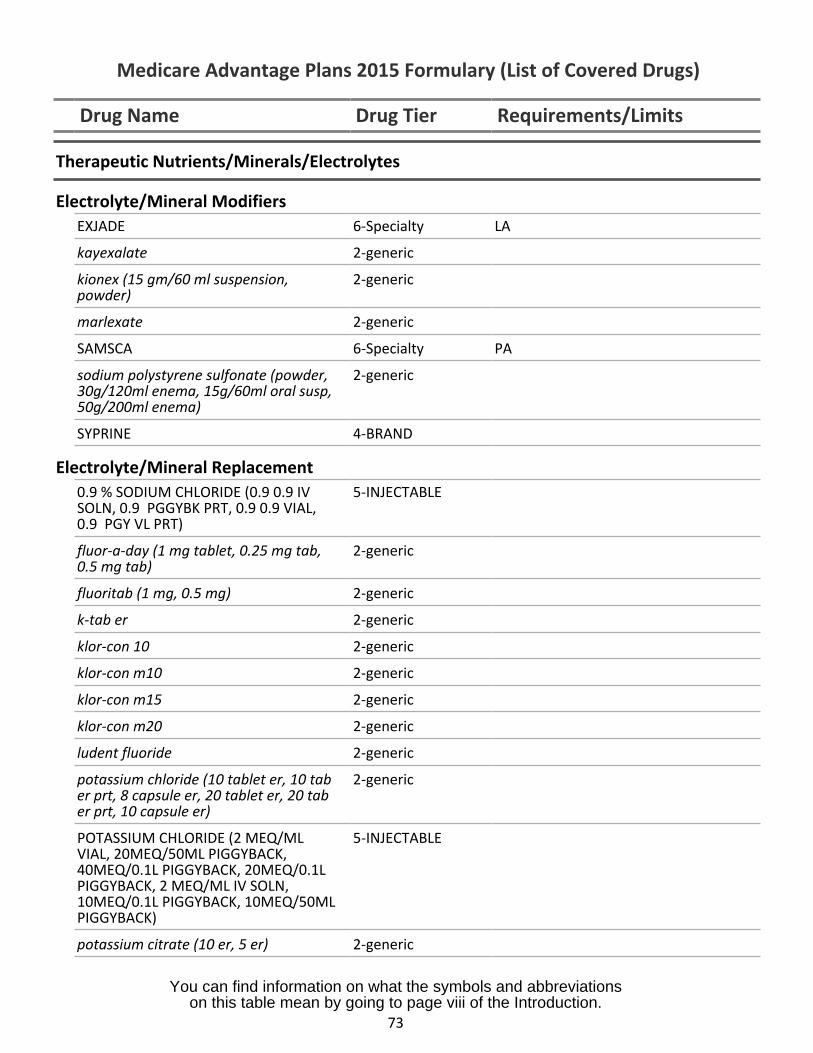
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
Therapeutic Nutrients/Minerals/Electrolytes
Electrolyte/Mineral ModifiersEXJADE 6-Specialty LA
kayexalate 2-generic
kionex (15 gm/60 ml suspension,powder)
2-generic
marlexate 2-generic
SAMSCA 6-Specialty PA
sodium polystyrene sulfonate (powder,30g/120ml enema, 15g/60ml oral susp,50g/200ml enema)
2-generic
SYPRINE 4-BRAND
Electrolyte/Mineral Replacement0.9 % SODIUM CHLORIDE (0.9 0.9 IVSOLN, 0.9 PGGYBK PRT, 0.9 0.9 VIAL,0.9 PGY VL PRT)
5-INJECTABLE
fluor-a-day (1 mg tablet, 0.25 mg tab,0.5 mg tab)
2-generic
fluoritab (1 mg, 0.5 mg) 2-generic
k-tab er 2-generic
klor-con 10 2-generic
klor-con m10 2-generic
klor-con m15 2-generic
klor-con m20 2-generic
ludent fluoride 2-generic
potassium chloride (10 tablet er, 10 taber prt, 8 capsule er, 20 tablet er, 20 taber prt, 10 capsule er)
2-generic
POTASSIUM CHLORIDE (2 MEQ/MLVIAL, 20MEQ/50ML PIGGYBACK,40MEQ/0.1L PIGGYBACK, 20MEQ/0.1LPIGGYBACK, 2 MEQ/ML IV SOLN,10MEQ/0.1L PIGGYBACK, 10MEQ/50MLPIGGYBACK)
5-INJECTABLE
potassium citrate (10 er, 5 er) 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
73
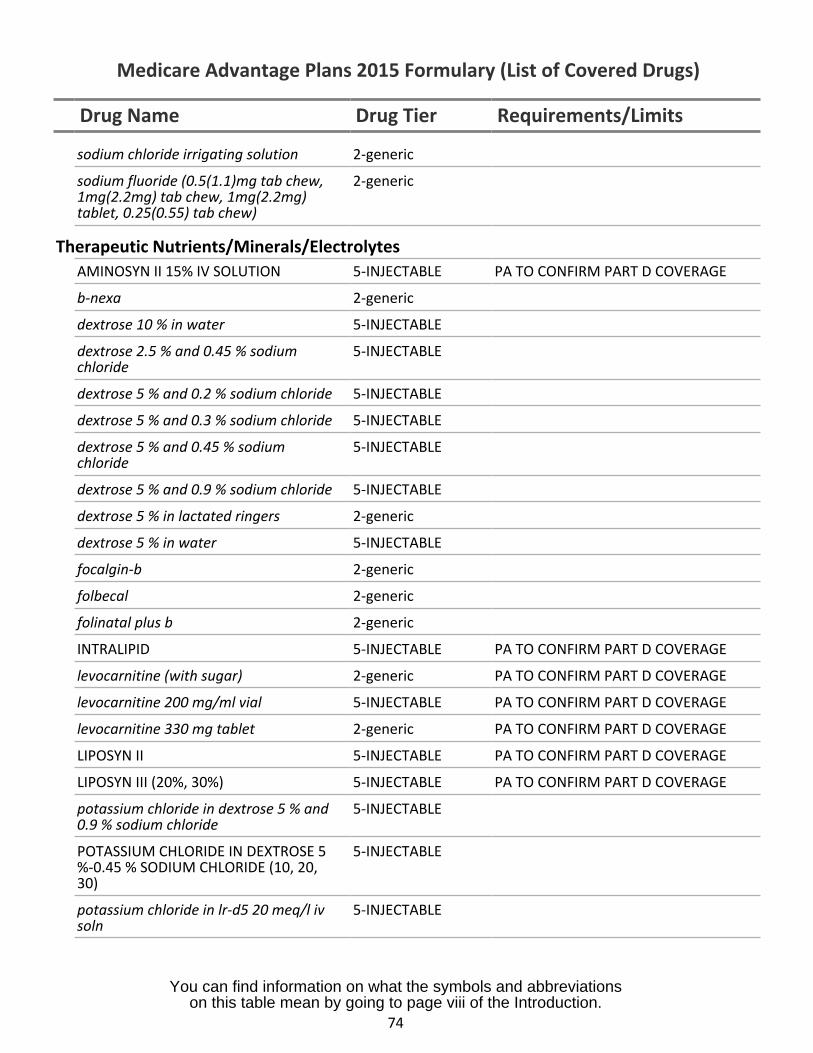
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
sodium chloride irrigating solution 2-generic
sodium fluoride (0.5(1.1)mg tab chew, 2-generic1mg(2.2mg) tab chew, 1mg(2.2mg)tablet, 0.25(0.55) tab chew)
Therapeutic Nutrients/Minerals/ElectrolytesAMINOSYN II 15% IV SOLUTION 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
b-nexa 2-generic
dextrose 10 % in water 5-INJECTABLE
dextrose 2.5 % and 0.45 % sodium 5-INJECTABLEchloride
dextrose 5 % and 0.2 % sodium chloride 5-INJECTABLE
dextrose 5 % and 0.3 % sodium chloride 5-INJECTABLE
dextrose 5 % and 0.45 % sodium 5-INJECTABLEchloride
dextrose 5 % and 0.9 % sodium chloride 5-INJECTABLE
dextrose 5 % in lactated ringers 2-generic
dextrose 5 % in water 5-INJECTABLE
focalgin-b 2-generic
folbecal 2-generic
folinatal plus b 2-generic
INTRALIPID 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
levocarnitine (with sugar) 2-generic PA TO CONFIRM PART D COVERAGE
levocarnitine 200 mg/ml vial 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
levocarnitine 330 mg tablet 2-generic PA TO CONFIRM PART D COVERAGE
LIPOSYN II 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
LIPOSYN III (20%, 30%) 5-INJECTABLE PA TO CONFIRM PART D COVERAGE
potassium chloride in dextrose 5 % and 5-INJECTABLE0.9 % sodium chloride
POTASSIUM CHLORIDE IN DEXTROSE 5 5-INJECTABLE%-0.45 % SODIUM CHLORIDE (10, 20,30)
potassium chloride in lr-d5 20 meq/l iv 5-INJECTABLEsoln
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
74
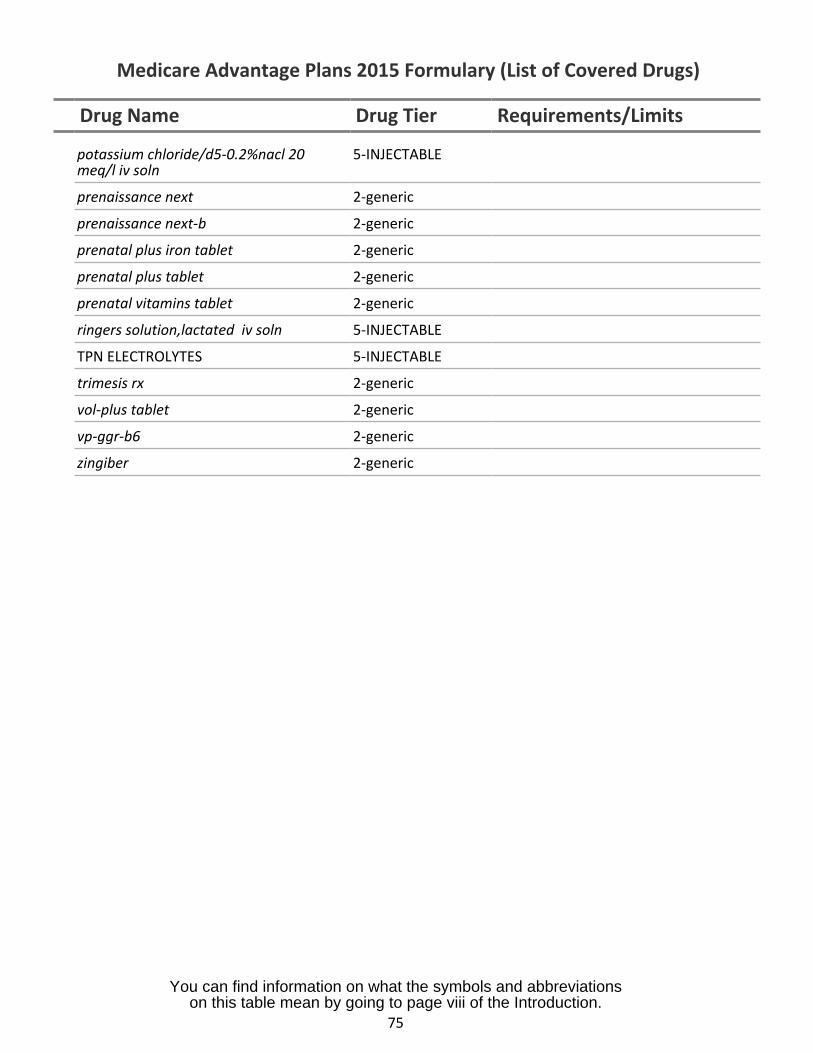
Medicare Advantage Plans 2015 Formulary (List of Covered Drugs)
Drug Name Drug Tier Requirements/Limits
potassium chloride/d5-0.2%nacl 20 5-INJECTABLEmeq/l iv soln
prenaissance next 2-generic
prenaissance next-b 2-generic
prenatal plus iron tablet 2-generic
prenatal plus tablet 2-generic
prenatal vitamins tablet 2-generic
ringers solution,lactated iv soln 5-INJECTABLE
TPN ELECTROLYTES 5-INJECTABLE
trimesis rx 2-generic
vol-plus tablet 2-generic
vp-ggr-b6 2-generic
zingiber 2-generic
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
75
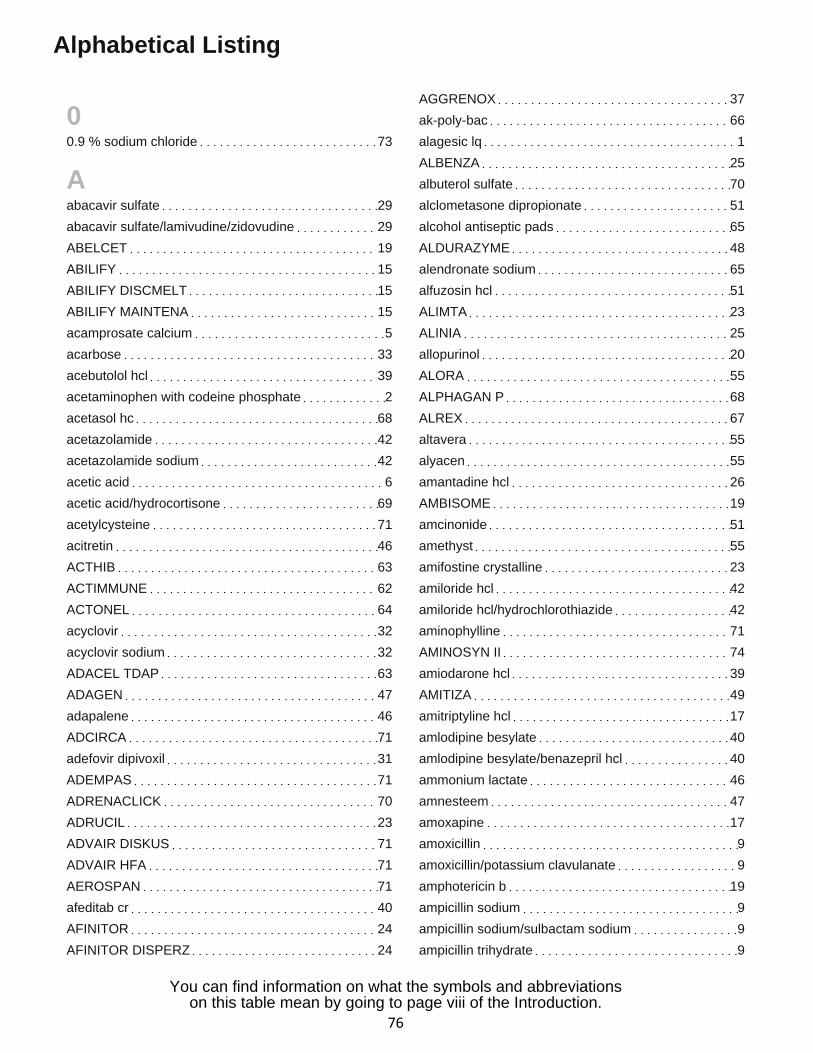
Alphabetical Listing
00.9 % sodium chloride 73
Aabacavir sulfate 29
abacavir sulfate/lamivudine/zidovudine 29
ABELCET 19
ABILIFY 15
ABILIFY DISCMELT 15
ABILIFY MAINTENA 15
acamprosate calcium 5
acarbose 33
acebutolol hcl 39
acetaminophen with codeine phosphate 2
acetasol hc 68
acetazolamide 42
acetazolamide sodium 42
acetic acid 6
acetic acid/hydrocortisone 69
acetylcysteine 71
acitretin 46
ACTHIB 63
ACTIMMUNE 62
ACTONEL 64
acyclovir 32
acyclovir sodium 32
ADACEL TDAP 63
ADAGEN 47
adapalene 46
ADCIRCA 71
adefovir dipivoxil 31
ADEMPAS 71
ADRENACLICK 70
ADRUCIL 23
ADVAIR DISKUS 71
ADVAIR HFA 71
AEROSPAN 71
afeditab cr 40
AFINITOR 24
AFINITOR DISPERZ 24
AGGRENOX 37
ak-poly-bac 66
alagesic lq 1
ALBENZA 25
albuterol sulfate 70
alclometasone dipropionate 51
alcohol antiseptic pads 65
ALDURAZYME 48
alendronate sodium 65
alfuzosin hcl 51
ALIMTA 23
ALINIA 25
allopurinol 20
ALORA 55
ALPHAGAN P 68
ALREX 67
altavera 55
alyacen 55
amantadine hcl 26
AMBISOME 19
amcinonide 51
amethyst 55
amifostine crystalline 23
amiloride hcl 42
amiloride hcl/hydrochlorothiazide 42
aminophylline 71
AMINOSYN II 74
amiodarone hcl 39
AMITIZA 49
amitriptyline hcl 17
amlodipine besylate 40
amlodipine besylate/benazepril hcl 40
ammonium lactate 46
amnesteem 47
amoxapine 17
amoxicillin 9
amoxicillin/potassium clavulanate 9
amphotericin b 19
ampicillin sodium 9
ampicillin sodium/sulbactam sodium 9
ampicillin trihydrate 9
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
76
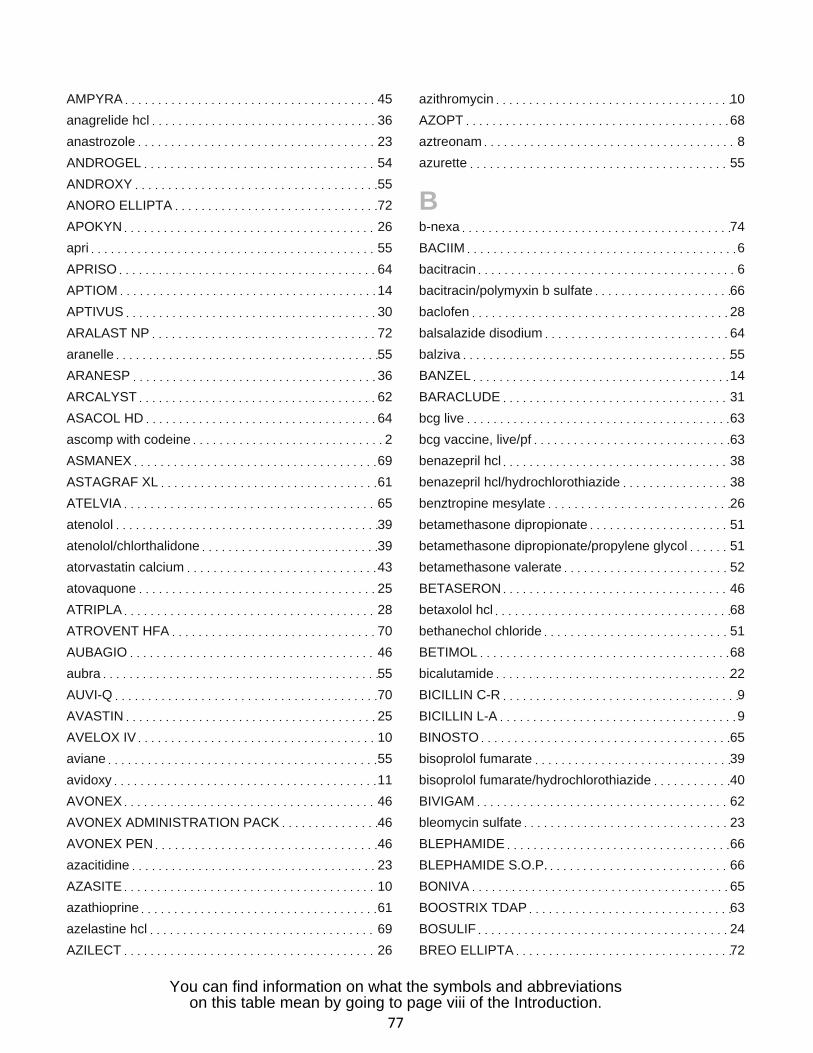
AMPYRA 45
anagrelide hcl 36
anastrozole 23
ANDROGEL 54
ANDROXY 55
ANORO ELLIPTA 72
APOKYN 26
apri 55
APRISO 64
APTIOM 14
APTIVUS 30
ARALAST NP 72
aranelle 55
ARANESP 36
ARCALYST 62
ASACOL HD 64
ascomp with codeine 2
ASMANEX 69
ASTAGRAF XL 61
ATELVIA 65
atenolol 39
atenolol/chlorthalidone 39
atorvastatin calcium 43
atovaquone 25
ATRIPLA 28
ATROVENT HFA 70
AUBAGIO 46
aubra 55
AUVI-Q 70
AVASTIN 25
AVELOX IV 10
aviane 55
avidoxy 11
AVONEX 46
AVONEX ADMINISTRATION PACK 46
AVONEX PEN 46
azacitidine 23
AZASITE 10
azathioprine 61
azelastine hcl 69
AZILECT 26
azithromycin 10
AZOPT 68
aztreonam 8
azurette 55
Bb-nexa 74
BACIIM 6
bacitracin 6
bacitracin/polymyxin b sulfate 66
baclofen 28
balsalazide disodium 64
balziva 55
BANZEL 14
BARACLUDE 31
bcg live 63
bcg vaccine, live/pf 63
benazepril hcl 38
benazepril hcl/hydrochlorothiazide 38
benztropine mesylate 26
betamethasone dipropionate 51
betamethasone dipropionate/propylene glycol 51
betamethasone valerate 52
BETASERON 46
betaxolol hcl 68
bethanechol chloride 51
BETIMOL 68
bicalutamide 22
BICILLIN C-R 9
BICILLIN L-A 9
BINOSTO 65
bisoprolol fumarate 39
bisoprolol fumarate/hydrochlorothiazide 40
BIVIGAM 62
bleomycin sulfate 23
BLEPHAMIDE 66
BLEPHAMIDE S.O.P. 66
BONIVA 65
BOOSTRIX TDAP 63
BOSULIF 24
BREO ELLIPTA 72
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
77
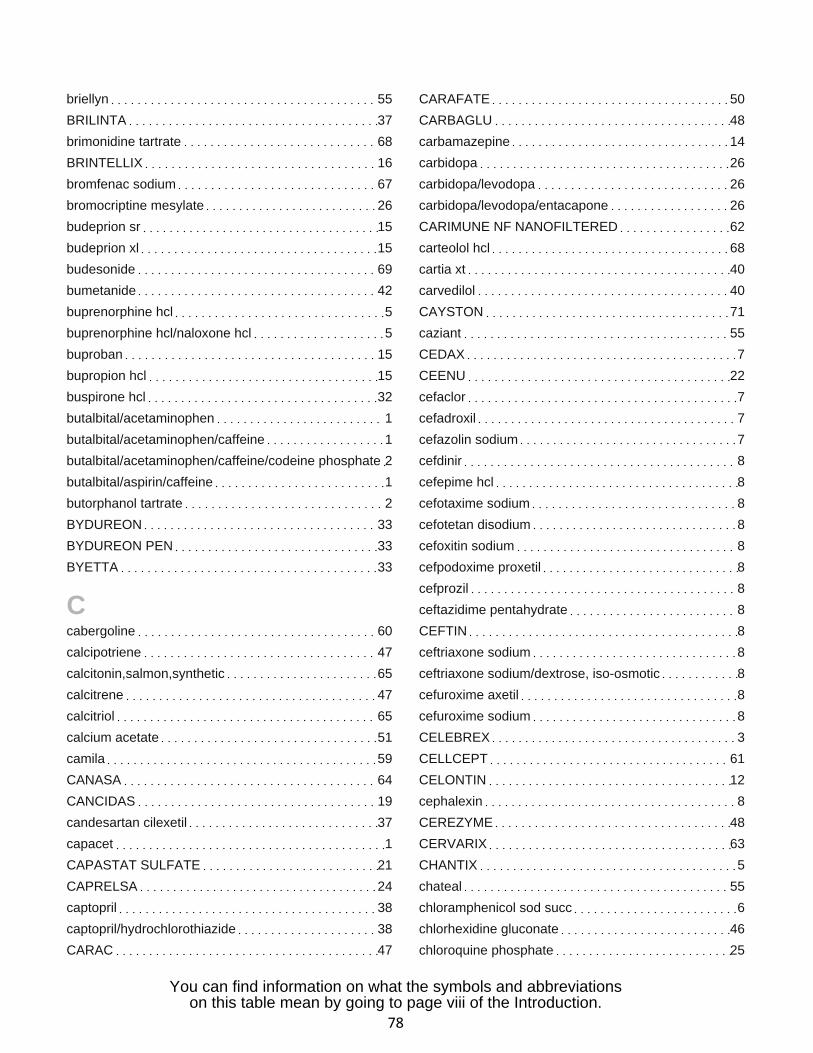
briellyn 55
BRILINTA 37
brimonidine tartrate 68
BRINTELLIX 16
bromfenac sodium 67
bromocriptine mesylate 26
budeprion sr 15
budeprion xl 15
budesonide 69
bumetanide 42
buprenorphine hcl 5
buprenorphine hcl/naloxone hcl 5
buproban 15
bupropion hcl 15
buspirone hcl 32
butalbital/acetaminophen 1
butalbital/acetaminophen/caffeine 1
butalbital/acetaminophen/caffeine/codeine phosphate 2
butalbital/aspirin/caffeine 1
butorphanol tartrate 2
BYDUREON 33
BYDUREON PEN 33
BYETTA 33
Ccabergoline 60
calcipotriene 47
calcitonin,salmon,synthetic 65
calcitrene 47
calcitriol 65
calcium acetate 51
camila 59
CANASA 64
CANCIDAS 19
candesartan cilexetil 37
capacet 1
CAPASTAT SULFATE 21
CAPRELSA 24
captopril 38
captopril/hydrochlorothiazide 38
CARAC 47
CARAFATE 50
CARBAGLU 48
carbamazepine 14
carbidopa 26
carbidopa/levodopa 26
carbidopa/levodopa/entacapone 26
CARIMUNE NF NANOFILTERED 62
carteolol hcl 68
cartia xt 40
carvedilol 40
CAYSTON 71
caziant 55
CEDAX 7
CEENU 22
cefaclor 7
cefadroxil 7
cefazolin sodium 7
cefdinir 8
cefepime hcl 8
cefotaxime sodium 8
cefotetan disodium 8
cefoxitin sodium 8
cefpodoxime proxetil 8
cefprozil 8
ceftazidime pentahydrate 8
CEFTIN 8
ceftriaxone sodium 8
ceftriaxone sodium/dextrose, iso-osmotic 8
cefuroxime axetil 8
cefuroxime sodium 8
CELEBREX 3
CELLCEPT 61
CELONTIN 12
cephalexin 8
CEREZYME 48
CERVARIX 63
CHANTIX 5
chateal 55
chloramphenicol sod succ 6
chlorhexidine gluconate 46
chloroquine phosphate 25
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
78

chlorothiazide 43
chlorpromazine hcl 18
chlorthalidone 43
cholestyramine (with sugar) 43
cholestyramine/aspartame 43
ciclodan 19
ciclopirox 19
ciclopirox olamine 19
cilostazol 37
cimetidine 49
cimetidine hcl 49
CINRYZE 61
CIPRO HC 69
CIPRODEX 69
ciprofloxacin hcl 10
ciprofloxacin lactate 10
ciprofloxacin lactate/dextrose 5 % in water 10
ciprofloxacin/ciprofloxacin hcl 11
citalopram hydrobromide 16
claravis 47
clarithromycin 10
clemastine fumarate 69
clinda-derm 6
clindacin etz 6
clindacin p 6
clindamycin hcl 6
clindamycin palmitate hcl 6
clindamycin phosphate 6
clindamycin phosphate/dextrose 5 % in water 6
clobetasol propionate 52
clobetasol propionate/emollient base 52
clodan 52
clomipramine hcl 17
clonazepam 12
clonidine 37
clonidine hcl 45
clopidogrel bisulfate 37
clorazepate dipotassium 12
clotrimazole 19
clotrimazole/betamethasone dipropionate 47
clozapine 28
codeine phosphate/butalbital/aspirin/caffeine 2
colchicine/probenecid 20
COLCRYS 20
colestipol hcl 44
colistin (as colistimethate sodium) 6
colocort 52
COMBIVENT RESPIMAT 70
COMETRIQ 24
COMPLERA 29
compro 18
COMVAX 63
constulose 49
COPAXONE 46
COREG CR 40
cormax 52
cortisone acetate 52
CREON 48
CRIXIVAN 30
cromolyn sodium 71
cryselle 55
CUBICIN 6
cyclafem 55
cyclobenzaprine hcl 72
CYCLOPHOSPHAMIDE CAPSULES (25 MG, 50
MG) 22
cyclophosphamide tablets (25 mg, 50 mg) 22
CYCLOSET 33
cyclosporine 61
cyclosporine, modified 61
cyproheptadine hcl 69
CYSTADANE 48
CYSTAGON 48
CYSTARAN 48
DDALIRESP 71
danazol 55
dantrolene sodium 28
dapsone 21
DAPTACEL DTAP 63
DARAPRIM 25
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
79
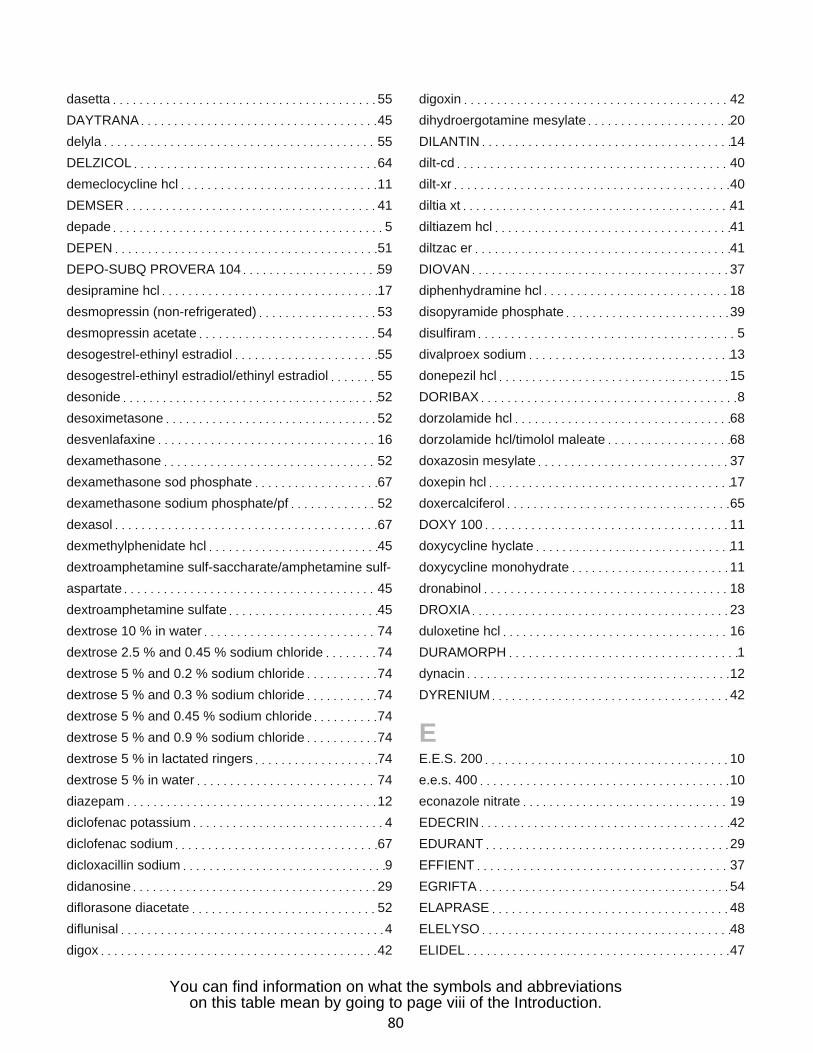
dasetta 55
DAYTRANA 45
delyla 55
DELZICOL 64
demeclocycline hcl 11
DEMSER 41
depade 5
DEPEN 51
DEPO-SUBQ PROVERA 104 59
desipramine hcl 17
desmopressin (non-refrigerated) 53
desmopressin acetate 54
desogestrel-ethinyl estradiol 55
desogestrel-ethinyl estradiol/ethinyl estradiol 55
desonide 52
desoximetasone 52
desvenlafaxine 16
dexamethasone 52
dexamethasone sod phosphate 67
dexamethasone sodium phosphate/pf 52
dexasol 67
dexmethylphenidate hcl 45
dextroamphetamine sulf-saccharate/amphetamine sulf-
aspartate 45
dextroamphetamine sulfate 45
dextrose 10 % in water 74
dextrose 2.5 % and 0.45 % sodium chloride 74
dextrose 5 % and 0.2 % sodium chloride 74
dextrose 5 % and 0.3 % sodium chloride 74
dextrose 5 % and 0.45 % sodium chloride 74
dextrose 5 % and 0.9 % sodium chloride 74
dextrose 5 % in lactated ringers 74
dextrose 5 % in water 74
diazepam 12
diclofenac potassium 4
diclofenac sodium 67
dicloxacillin sodium 9
didanosine 29
diflorasone diacetate 52
diflunisal 4
digox 42
digoxin 42
dihydroergotamine mesylate 20
DILANTIN 14
dilt-cd 40
dilt-xr 40
diltia xt 41
diltiazem hcl 41
diltzac er 41
DIOVAN 37
diphenhydramine hcl 18
disopyramide phosphate 39
disulfiram 5
divalproex sodium 13
donepezil hcl 15
DORIBAX 8
dorzolamide hcl 68
dorzolamide hcl/timolol maleate 68
doxazosin mesylate 37
doxepin hcl 17
doxercalciferol 65
DOXY 100 11
doxycycline hyclate 11
doxycycline monohydrate 11
dronabinol 18
DROXIA 23
duloxetine hcl 16
DURAMORPH 1
dynacin 12
DYRENIUM 42
EE.E.S. 200 10
e.e.s. 400 10
econazole nitrate 19
EDECRIN 42
EDURANT 29
EFFIENT 37
EGRIFTA 54
ELAPRASE 48
ELELYSO 48
ELIDEL 47
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
80
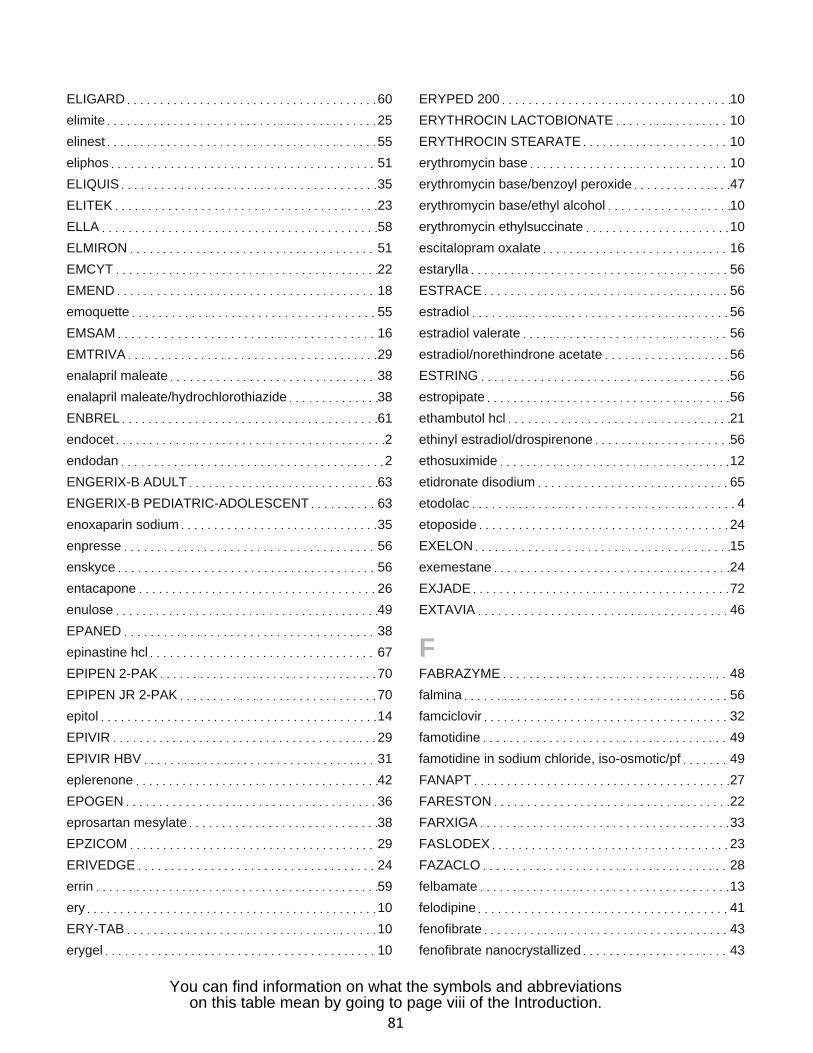
ELIGARD 60
elimite 25
elinest 55
eliphos 51
ELIQUIS 35
ELITEK 23
ELLA 58
ELMIRON 51
EMCYT 22
EMEND 18
emoquette 55
EMSAM 16
EMTRIVA 29
enalapril maleate 38
enalapril maleate/hydrochlorothiazide 38
ENBREL 61
endocet 2
endodan 2
ENGERIX-B ADULT 63
ENGERIX-B PEDIATRIC-ADOLESCENT 63
enoxaparin sodium 35
enpresse 56
enskyce 56
entacapone 26
enulose 49
EPANED 38
epinastine hcl 67
EPIPEN 2-PAK 70
EPIPEN JR 2-PAK 70
epitol 14
EPIVIR 29
EPIVIR HBV 31
eplerenone 42
EPOGEN 36
eprosartan mesylate 38
EPZICOM 29
ERIVEDGE 24
errin 59
ery 10
ERY-TAB 10
erygel 10
ERYPED 200 10
ERYTHROCIN LACTOBIONATE 10
ERYTHROCIN STEARATE 10
erythromycin base 10
erythromycin base/benzoyl peroxide 47
erythromycin base/ethyl alcohol 10
erythromycin ethylsuccinate 10
escitalopram oxalate 16
estarylla 56
ESTRACE 56
estradiol 56
estradiol valerate 56
estradiol/norethindrone acetate 56
ESTRING 56
estropipate 56
ethambutol hcl 21
ethinyl estradiol/drospirenone 56
ethosuximide 12
etidronate disodium 65
etodolac 4
etoposide 24
EXELON 15
exemestane 24
EXJADE 72
EXTAVIA 46
FFABRAZYME 48
falmina 56
famciclovir 32
famotidine 49
famotidine in sodium chloride, iso-osmotic/pf 49
FANAPT 27
FARESTON 22
FARXIGA 33
FASLODEX 23
FAZACLO 28
felbamate 13
felodipine 41
fenofibrate 43
fenofibrate nanocrystallized 43
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
81
fenofibrate,micronized 43
fenofibric acid (choline) 43
fenoprofen calcium 4
fentanyl 1
fentanyl citrate 1
FETZIMA 16
finasteride 51
fioricet 1
FIRAZYR 61
FLAREX 67
flavoxate hcl 50
FLEBOGAMMA DIF 62
flecainide acetate 39
FLOVENT DISKUS 69
FLOVENT HFA 69
fluconazole 19
fluconazole in dextrose, iso-osmotic 19
flucytosine 19
fludrocortisone acetate 52
flunisolide 69
fluocinolone acetonide 52
fluocinolone acetonide oil 52
fluocinonide 52
fluocinonide/emollient base 52
fluor-a-day 73
fluoritab 73
fluorouracil 47
fluoxetine hcl 16
fluphenazine decanoate 26
fluphenazine hcl 27
flurbiprofen 4
flurbiprofen sodium 67
flutamide 22
fluticasone propionate 69
fluvastatin sodium 43
fluvoxamine maleate 16
FML FORTE 68
FML S.O.P. 68
focalgin-b 74
folbecal 74
folinatal plus b 74
fondaparinux sodium 35
FORTEO 65
foscarnet sodium 30
fosinopril sodium 38
fosinopril sodium/hydrochlorothiazide 38
FRAGMIN 35
FULYZAQ 48
furosemide 42
FUZEON 30
FYCOMPA 13
Ggabapentin 13
GABITRIL 13
galantamine hbr 15
GAMMAGARD LIQUID 62
GAMMAGARD S-D 62
GAMMAKED 62
GAMMAPLEX 62
GAMUNEX 62
GAMUNEX-C 62
ganciclovir sodium 30
garamycin 5
GARDASIL 63
gatifloxacin 11
GATTEX 49
gauze bandage 66
gavilyte-c 49
gavilyte-g 49
gavilyte-n 50
gemfibrozil 43
generlac 50
gengraf 61
GENOTROPIN 54
gentak 5
gentamicin sulfate 6
gentamicin sulfate/pf 6
GEODON 27
gianvi 56
gildagia 56
gildess 56
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
82
gildess fe 56
GILENYA 46
GILOTRIF 24
GLASSIA 72
GLEEVEC 24
glimepiride 33
glipizide 33
glipizide/metformin hcl 33
GLUCAGEN 34
GLUCAGON EMERGENCY KIT 34
glycopyrrolate 48
GRANIX 36
griseofulvin ultramicrosize 19
griseofulvin, microsize 19
guanidine hcl 21
HHALDOL DECANOATE 100 27
HALDOL DECANOATE 50 27
halobetasol propionate 52
haloperidol 27
haloperidol decanoate 27
haloperidol lactate 27
HAVRIX 63
heather 59
hecoria 61
heparin sodium,porcine 36
heparin sodium,porcine/dextrose 5 % in water 36
heparin sodium,porcine/pf 36
HEXALEN 22
HUMALOG 34
HUMALOG MIX 50-50 34
HUMALOG MIX 75-25 34
HUMATROPE 54
HUMIRA 61
HUMULIN 70-30 34
HUMULIN N 34
HUMULIN R 34
hydralazine hcl 44
hydrochlorothiazide 43
hydrocodone bitartrate/acetaminophen 2
hydrocodone/ibuprofen 2
hydrocortisone 53
hydrocortisone butyrate 53
hydrocortisone valerate 53
hydromorphone hcl 2
hydromorphone hcl/pf 2
hydroxychloroquine sulfate 25
hydroxyurea 23
Iibandronate sodium 65
ibuprofen 4
ILARIS 63
IMBRUVICA 24
imipenem/cilastatin sodium 8
imipramine hcl 17
imipramine pamoate 17
imiquimod 47
IMOVAX RABIES VACCINE 63
INCIVEK 31
INCRELEX 54
indapamide 43
INFANRIX DTAP 63
INLYTA 24
INTELENCE 29
INTRALIPID 74
INTRON A 31
INVANZ 8
INVEGA 27
INVEGA SUSTENNA 28
INVIRASE 30
INVOKANA 33
IPOL 63
ipratropium bromide 70
ipratropium bromide/albuterol sulfate 70
irbesartan 38
irbesartan/hydrochlorothiazide 38
ISENTRESS 29
isochron 44
isoniazid 21
ISOPTO CARPINE 68
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
83
isosorbide dinitrate 44
isosorbide mononitrate 44
isradipine 41
ISTALOL 68
itraconazole 19
IXEMPRA 23
IXIARO 63
JJAKAFI 24
jantoven 36
JANUMET 33
JANUMET XR 33
JANUVIA 33
jencycla 59
JENTADUETO 33
jinteli 56
jolessa 56
jolivette 59
junel 56
junel fe 56
JUXTAPID 44
Kk-tab er 73
KALETRA 30
KALYDECO 71
kariva 56
kayexalate 73
KAZANO 33
kelnor 1-35 56
ketoconazole 19
ketoprofen 4
ketorolac tromethamine 68
KHEDEZLA 17
kionex 73
klor-con 10 73
klor-con m10 73
klor-con m15 73
klor-con m20 73
KOMBIGLYZE XR 33
KORLYM 60
kurvelo 56
KUVAN 48
KYNAMRO 44
Llabetalol hcl 40
laclotion 47
LACRISERT 66
lactulose 50
LAMICTAL (BLUE) 13
LAMICTAL (GREEN) 13
LAMICTAL (ORANGE) 13
LAMICTAL XR (BLUE) 13
LAMICTAL XR (GREEN) 14
LAMICTAL XR (ORANGE) 14
lamivudine 31
lamivudine/zidovudine 29
lamotrigine 14
lansoprazole 50
lansoprazole/amoxicillin trihydrate/clarithromycin 49
LANTUS 34
LANTUS SOLOSTAR 35
larin 56
larin fe 56
latanoprost 68
LATUDA 28
LAZANDA 2
leena 56
leflunomide 63
lessina 56
LETAIRIS 71
letrozole 24
leucovorin calcium 23
LEUKERAN 22
LEUKINE 36
leuprolide acetate 60
LEVATOL 40
LEVEMIR 35
LEVEMIR FLEXPEN 35
LEVEMIR FLEXTOUCH 35
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
84
levetiracetam 12
levobunolol hcl 68
levocarnitine 74
levocarnitine (with sugar) 74
levocetirizine dihydrochloride 69
levofloxacin 11
levofloxacin/dextrose 5 % in water 11
levonest 56
levonorgestrel-ethinyl estradiol 57
levora-28 57
levorphanol tartrate 1
levothroid 59
LEVOTHROID 59
levothyroxine sodium 60
levoxyl 60
LEXIVA 30
LIALDA 64
lidocaine 4
lidocaine hcl 5
lidocaine hcl/pf 5
lidocaine/prilocaine 5
lindane 26
liothyronine sodium 60
LIPOSYN II 74
LIPOSYN III 74
lisinopril 38
lisinopril/hydrochlorothiazide 38
lithium carbonate 33
lithium citrate 33
lofibra 43
lomedia 24 fe 57
lomustine 22
loperamide hcl 49
lorazepam 32
lorazepam intensol 32
lorcet plus 3
lortab 3
loryna 57
losartan potassium 38
losartan potassium/hydrochlorothiazide 38
LOTEMAX 68
LOTRONEX 49
lovastatin 43
low-ogestrel 57
loxapine succinate 27
ludent fluoride 73
LUMIGAN 68
LUMIZYME 48
LUPRON DEPOT 60
LUPRON DEPOT-PED 60
lutera 57
LYRICA 12
LYSODREN 60
lyza 59
MM-M-R II VACCINE 63
maprotiline hcl 15
marlexate 73
marlissa 57
MARPLAN 16
MATULANE 22
matzim la 41
meclizine hcl 18
meclofenamate sodium 4
medroxyprogesterone acetate 59
mefloquine hcl 25
megestrol acetate 59
MEKINIST 24
meloxicam 4
MENACTRA 63
MENEST 57
MENOMUNE-A-C-Y-W-135 63
MENVEO A-C-Y-W-135-DIP 63
mercaptopurine 23
meropenem 8
mesalamine with cleansing wipes 64
MESNEX 18
MESTINON 21
metadate er 45
metaproterenol sulfate 70
metformin hcl 34
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
85
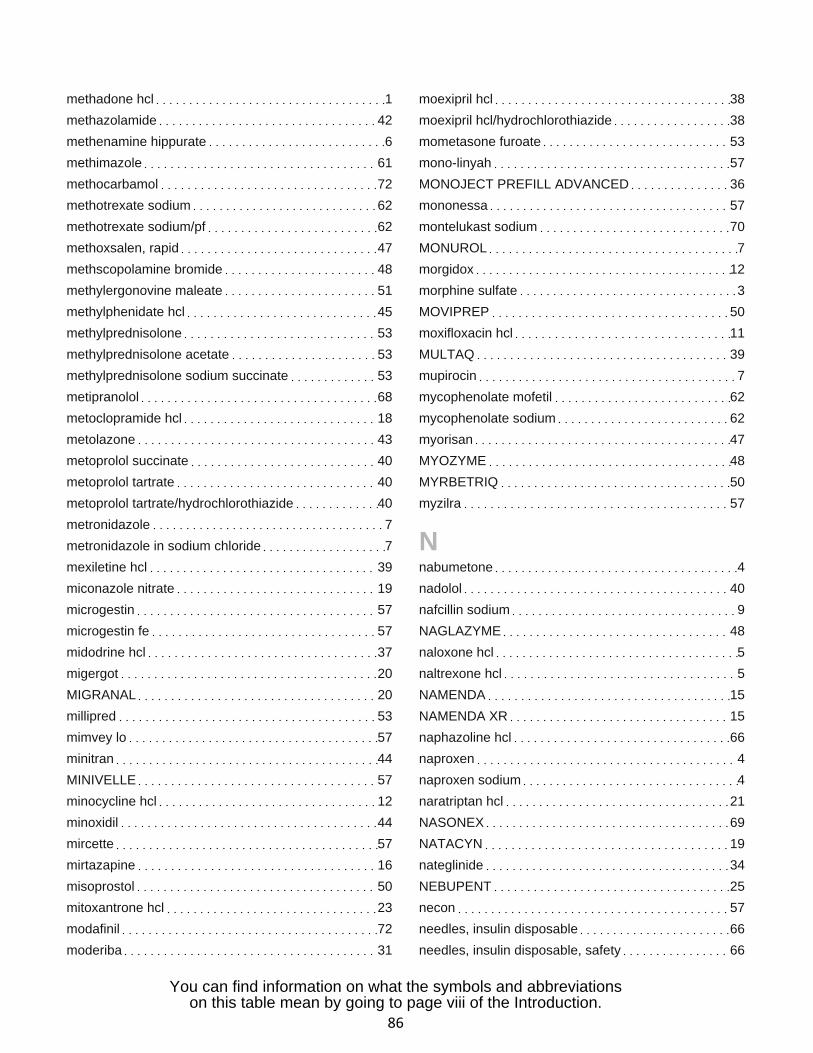
methadone hcl 1
methazolamide 42
methenamine hippurate 6
methimazole 61
methocarbamol 72
methotrexate sodium 62
methotrexate sodium/pf 62
methoxsalen, rapid 47
methscopolamine bromide 48
methylergonovine maleate 51
methylphenidate hcl 45
methylprednisolone 53
methylprednisolone acetate 53
methylprednisolone sodium succinate 53
metipranolol 68
metoclopramide hcl 18
metolazone 43
metoprolol succinate 40
metoprolol tartrate 40
metoprolol tartrate/hydrochlorothiazide 40
metronidazole 7
metronidazole in sodium chloride 7
mexiletine hcl 39
miconazole nitrate 19
microgestin 57
microgestin fe 57
midodrine hcl 37
migergot 20
MIGRANAL 20
millipred 53
mimvey lo 57
minitran 44
MINIVELLE 57
minocycline hcl 12
minoxidil 44
mircette 57
mirtazapine 16
misoprostol 50
mitoxantrone hcl 23
modafinil 72
moderiba 31
moexipril hcl 38
moexipril hcl/hydrochlorothiazide 38
mometasone furoate 53
mono-linyah 57
MONOJECT PREFILL ADVANCED 36
mononessa 57
montelukast sodium 70
MONUROL 7
morgidox 12
morphine sulfate 3
MOVIPREP 50
moxifloxacin hcl 11
MULTAQ 39
mupirocin 7
mycophenolate mofetil 62
mycophenolate sodium 62
myorisan 47
MYOZYME 48
MYRBETRIQ 50
myzilra 57
Nnabumetone 4
nadolol 40
nafcillin sodium 9
NAGLAZYME 48
naloxone hcl 5
naltrexone hcl 5
NAMENDA 15
NAMENDA XR 15
naphazoline hcl 66
naproxen 4
naproxen sodium 4
naratriptan hcl 21
NASONEX 69
NATACYN 19
nateglinide 34
NEBUPENT 25
necon 57
needles, insulin disposable 66
needles, insulin disposable, safety 66
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
86
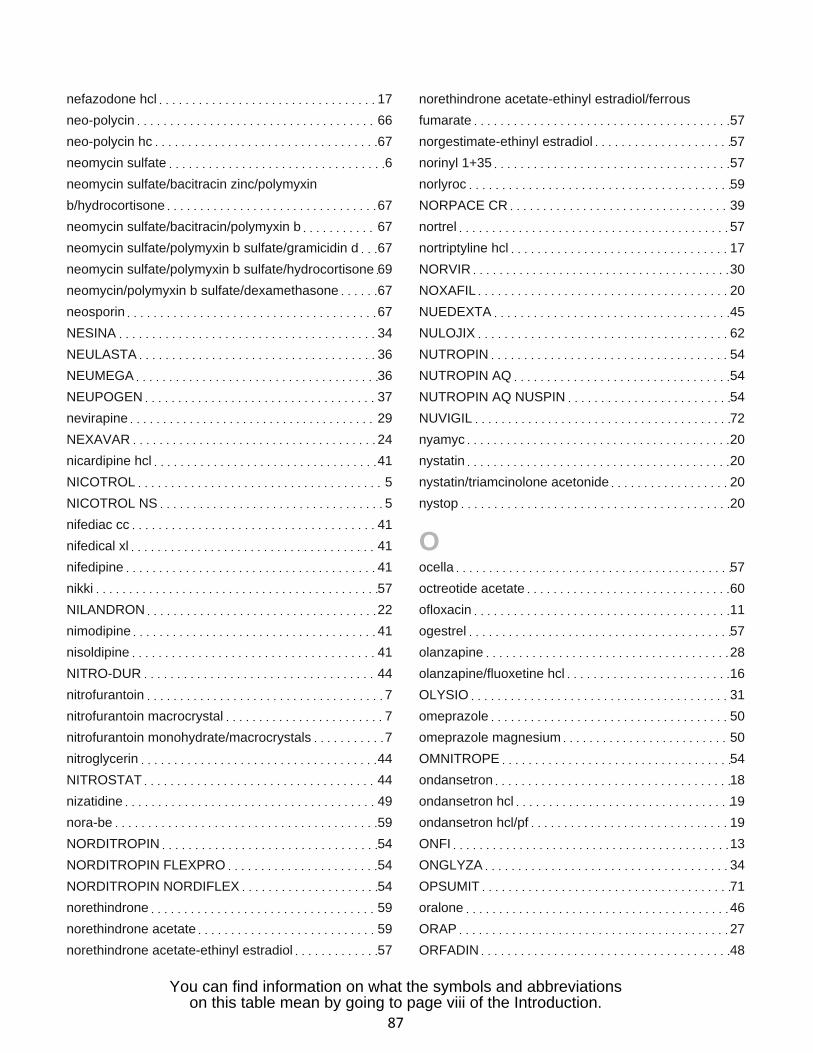
nefazodone hcl 17
neo-polycin 66
neo-polycin hc 67
neomycin sulfate 6
neomycin sulfate/bacitracin zinc/polymyxin
b/hydrocortisone 67
neomycin sulfate/bacitracin/polymyxin b 67
neomycin sulfate/polymyxin b sulfate/gramicidin d 67
neomycin sulfate/polymyxin b sulfate/hydrocortisone 69
neomycin/polymyxin b sulfate/dexamethasone 67
neosporin 67
NESINA 34
NEULASTA 36
NEUMEGA 36
NEUPOGEN 37
nevirapine 29
NEXAVAR 24
nicardipine hcl 41
NICOTROL 5
NICOTROL NS 5
nifediac cc 41
nifedical xl 41
nifedipine 41
nikki 57
NILANDRON 22
nimodipine 41
nisoldipine 41
NITRO-DUR 44
nitrofurantoin 7
nitrofurantoin macrocrystal 7
nitrofurantoin monohydrate/macrocrystals 7
nitroglycerin 44
NITROSTAT 44
nizatidine 49
nora-be 59
NORDITROPIN 54
NORDITROPIN FLEXPRO 54
NORDITROPIN NORDIFLEX 54
norethindrone 59
norethindrone acetate 59
norethindrone acetate-ethinyl estradiol 57
norethindrone acetate-ethinyl estradiol/ferrous
fumarate 57
norgestimate-ethinyl estradiol 57
norinyl 1+35 57
norlyroc 59
NORPACE CR 39
nortrel 57
nortriptyline hcl 17
NORVIR 30
NOXAFIL 20
NUEDEXTA 45
NULOJIX 62
NUTROPIN 54
NUTROPIN AQ 54
NUTROPIN AQ NUSPIN 54
NUVIGIL 72
nyamyc 20
nystatin 20
nystatin/triamcinolone acetonide 20
nystop 20
Oocella 57
octreotide acetate 60
ofloxacin 11
ogestrel 57
olanzapine 28
olanzapine/fluoxetine hcl 16
OLYSIO 31
omeprazole 50
omeprazole magnesium 50
OMNITROPE 54
ondansetron 18
ondansetron hcl 19
ondansetron hcl/pf 19
ONFI 13
ONGLYZA 34
OPSUMIT 71
oralone 46
ORAP 27
ORFADIN 48
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
87

orsythia 57
OSENI 34
oxacillin sodium 9
oxacillin sodium/dextrose, iso-osmotic 9
oxandrolone 54
oxazepam 33
oxcarbazepine 14
OXSORALEN-ULTRA 47
oxybutynin chloride 51
oxycodone hcl 3
oxycodone hcl/acetaminophen 3
oxycodone hcl/aspirin 3
OXYCONTIN 2
oxymorphone hcl 3
OXYTROL 51
Ppacerone 39
pamidronate disodium 65
PANRETIN 25
pantoprazole sodium 50
paricalcitol 65
paroex 46
paromomycin sulfate 6
paroxetine hcl 17
PASER 21
PAXIL 17
pedi-dri 20
PEDVAXHIB 63
peg 3350/sod sulf/sod bicarbonate/sod
chloride/potassium chl 50
PEGANONE 14
PEGASYS 31
PEGASYS PROCLICK 31
PEGINTRON 31
PEGINTRON REDIPEN 31
pen needle, diabetic disposable, safety 66
pen needle, diabetic, remover & disposal unit 66
penicillin g potassium 9
penicillin g procaine 9
penicillin g sodium 9
penicillin v potassium 9
PENTACEL ACTHIB COMPONENT 63
PENTAM 300 25
PENTASA 64
pentoxifylline 42
perindopril erbumine 38
periogard 46
permethrin 26
perphenazine 18
perphenazine/amitriptyline hcl 27
PFIZERPEN 9
phenelzine sulfate 16
phenobarbital 13
phenytoin 14
phenytoin sodium 14
phenytoin sodium extended 14
philith 57
PICATO 47
pilocarpine hcl 68
pimtrea 57
pindolol 40
pioglitazone hcl 34
pioglitazone hcl/glimepiride 34
pioglitazone hcl/metformin hcl 34
piperacillin sodium/tazobactam sodium 9
pirmella 57
piroxicam 4
podofilox 47
polycin 67
polyethylene glycol 3350 50
polymyxin b sulfate/trimethoprim 67
POMALYST 22
portia 58
potassium chloride 73
potassium chloride in dextrose 5 % and 0.9 % sodium
chloride 74
potassium chloride in dextrose 5 %-0.2 % sodium
chloride 74
potassium chloride in dextrose 5 %-0.45 % sodium
chloride 74
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
88
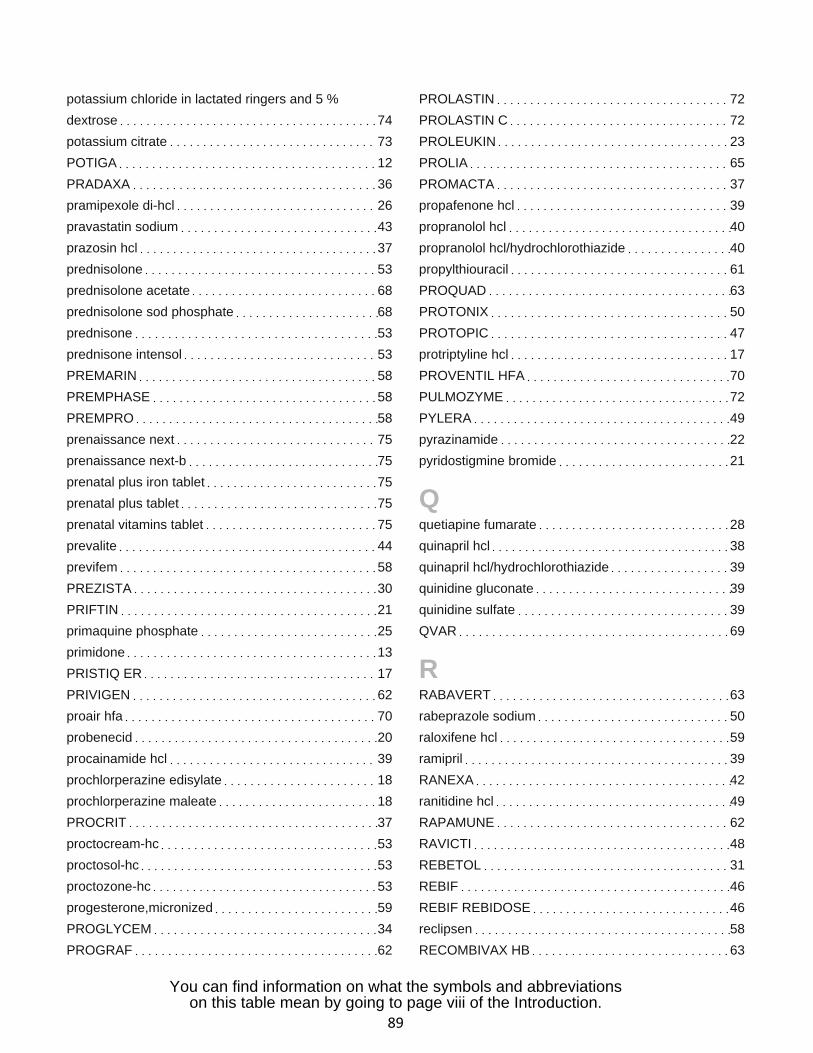
potassium chloride in lactated ringers and 5 %
dextrose 74
potassium citrate 73
POTIGA 12
PRADAXA 36
pramipexole di-hcl 26
pravastatin sodium 43
prazosin hcl 37
prednisolone 53
prednisolone acetate 68
prednisolone sod phosphate 68
prednisone 53
prednisone intensol 53
PREMARIN 58
PREMPHASE 58
PREMPRO 58
prenaissance next 75
prenaissance next-b 75
prenatal plus iron tablet 75
prenatal plus tablet 75
prenatal vitamins tablet 75
prevalite 44
previfem 58
PREZISTA 30
PRIFTIN 21
primaquine phosphate 25
primidone 13
PRISTIQ ER 17
PRIVIGEN 62
proair hfa 70
probenecid 20
procainamide hcl 39
prochlorperazine edisylate 18
prochlorperazine maleate 18
PROCRIT 37
proctocream-hc 53
proctosol-hc 53
proctozone-hc 53
progesterone,micronized 59
PROGLYCEM 34
PROGRAF 62
PROLASTIN 72
PROLASTIN C 72
PROLEUKIN 23
PROLIA 65
PROMACTA 37
propafenone hcl 39
propranolol hcl 40
propranolol hcl/hydrochlorothiazide 40
propylthiouracil 61
PROQUAD 63
PROTONIX 50
PROTOPIC 47
protriptyline hcl 17
PROVENTIL HFA 70
PULMOZYME 72
PYLERA 49
pyrazinamide 22
pyridostigmine bromide 21
Qquetiapine fumarate 28
quinapril hcl 38
quinapril hcl/hydrochlorothiazide 39
quinidine gluconate 39
quinidine sulfate 39
QVAR 69
RRABAVERT 63
rabeprazole sodium 50
raloxifene hcl 59
ramipril 39
RANEXA 42
ranitidine hcl 49
RAPAMUNE 62
RAVICTI 48
REBETOL 31
REBIF 46
REBIF REBIDOSE 46
reclipsen 58
RECOMBIVAX HB 63
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
89
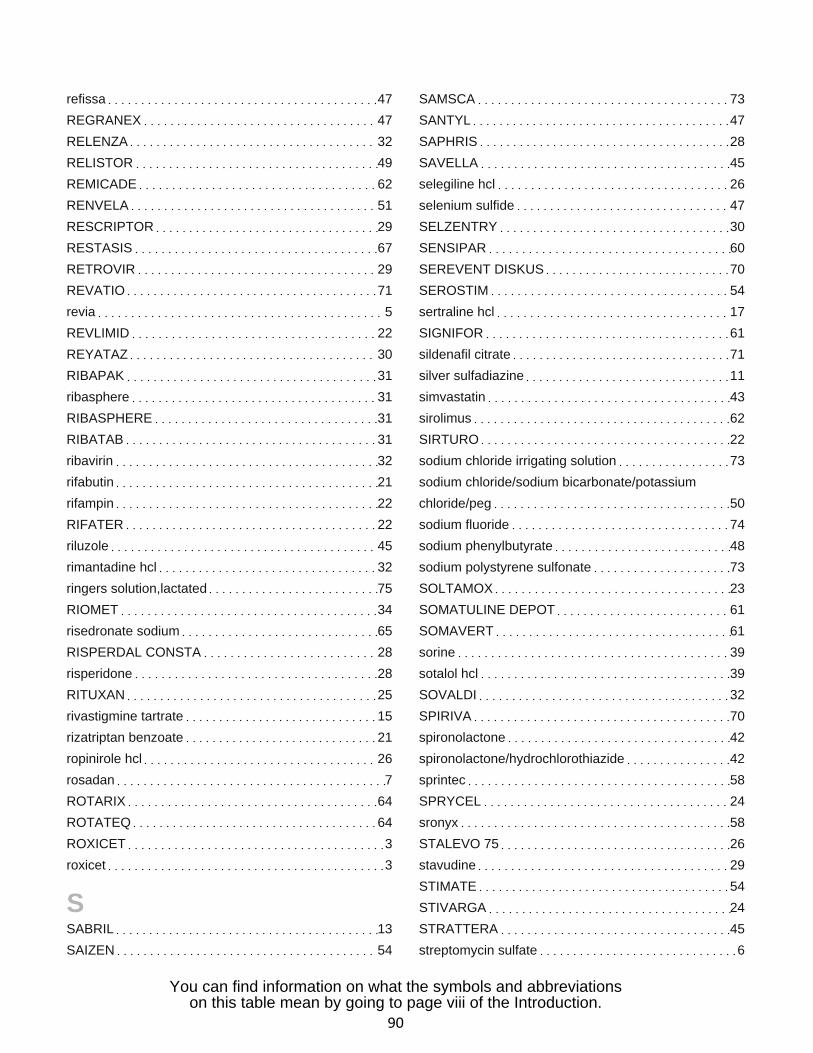
refissa 47
REGRANEX 47
RELENZA 32
RELISTOR 49
REMICADE 62
RENVELA 51
RESCRIPTOR 29
RESTASIS 67
RETROVIR 29
REVATIO 71
revia 5
REVLIMID 22
REYATAZ 30
RIBAPAK 31
ribasphere 31
RIBASPHERE 31
RIBATAB 31
ribavirin 32
rifabutin 21
rifampin 22
RIFATER 22
riluzole 45
rimantadine hcl 32
ringers solution,lactated 75
RIOMET 34
risedronate sodium 65
RISPERDAL CONSTA 28
risperidone 28
RITUXAN 25
rivastigmine tartrate 15
rizatriptan benzoate 21
ropinirole hcl 26
rosadan 7
ROTARIX 64
ROTATEQ 64
ROXICET 3
roxicet 3
SSABRIL 13
SAIZEN 54
SAMSCA 73
SANTYL 47
SAPHRIS 28
SAVELLA 45
selegiline hcl 26
selenium sulfide 47
SELZENTRY 30
SENSIPAR 60
SEREVENT DISKUS 70
SEROSTIM 54
sertraline hcl 17
SIGNIFOR 61
sildenafil citrate 71
silver sulfadiazine 11
simvastatin 43
sirolimus 62
SIRTURO 22
sodium chloride irrigating solution 73
sodium chloride/sodium bicarbonate/potassium
chloride/peg 50
sodium fluoride 74
sodium phenylbutyrate 48
sodium polystyrene sulfonate 73
SOLTAMOX 23
SOMATULINE DEPOT 61
SOMAVERT 61
sorine 39
sotalol hcl 39
SOVALDI 32
SPIRIVA 70
spironolactone 42
spironolactone/hydrochlorothiazide 42
sprintec 58
SPRYCEL 24
sronyx 58
STALEVO 75 26
stavudine 29
STIMATE 54
STIVARGA 24
STRATTERA 45
streptomycin sulfate 6
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
90
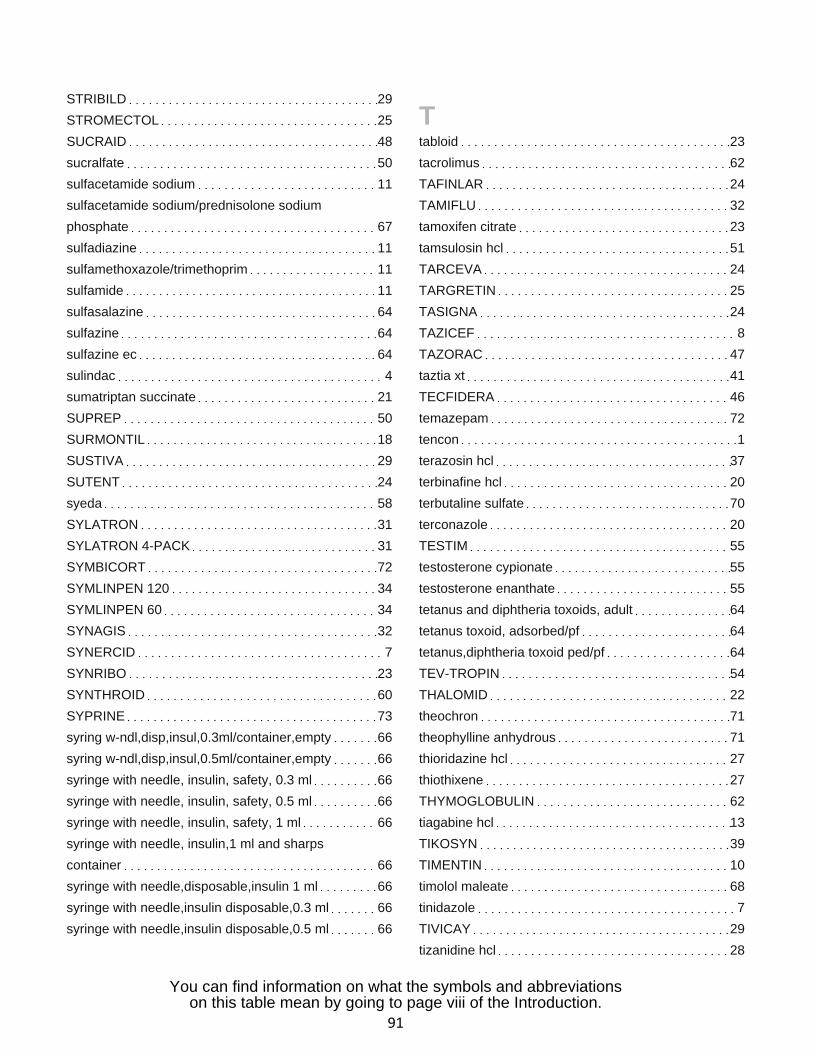
STRIBILD 29
STROMECTOL 25
SUCRAID 48
sucralfate 50
sulfacetamide sodium 11
sulfacetamide sodium/prednisolone sodium
phosphate 67
sulfadiazine 11
sulfamethoxazole/trimethoprim 11
sulfamide 11
sulfasalazine 64
sulfazine 64
sulfazine ec 64
sulindac 4
sumatriptan succinate 21
SUPREP 50
SURMONTIL 18
SUSTIVA 29
SUTENT 24
syeda 58
SYLATRON 31
SYLATRON 4-PACK 31
SYMBICORT 72
SYMLINPEN 120 34
SYMLINPEN 60 34
SYNAGIS 32
SYNERCID 7
SYNRIBO 23
SYNTHROID 60
SYPRINE 73
syring w-ndl,disp,insul,0.3ml/container,empty 66
syring w-ndl,disp,insul,0.5ml/container,empty 66
syringe with needle, insulin, safety, 0.3 ml 66
syringe with needle, insulin, safety, 0.5 ml 66
syringe with needle, insulin, safety, 1 ml 66
syringe with needle, insulin,1 ml and sharps
container 66
syringe with needle,disposable,insulin 1 ml 66
syringe with needle,insulin disposable,0.3 ml 66
syringe with needle,insulin disposable,0.5 ml 66
Ttabloid 23
tacrolimus 62
TAFINLAR 24
TAMIFLU 32
tamoxifen citrate 23
tamsulosin hcl 51
TARCEVA 24
TARGRETIN 25
TASIGNA 24
TAZICEF 8
TAZORAC 47
taztia xt 41
TECFIDERA 46
temazepam 72
tencon 1
terazosin hcl 37
terbinafine hcl 20
terbutaline sulfate 70
terconazole 20
TESTIM 55
testosterone cypionate 55
testosterone enanthate 55
tetanus and diphtheria toxoids, adult 64
tetanus toxoid, adsorbed/pf 64
tetanus,diphtheria toxoid ped/pf 64
TEV-TROPIN 54
THALOMID 22
theochron 71
theophylline anhydrous 71
thioridazine hcl 27
thiothixene 27
THYMOGLOBULIN 62
tiagabine hcl 13
TIKOSYN 39
TIMENTIN 10
timolol maleate 68
tinidazole 7
TIVICAY 29
tizanidine hcl 28
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
91
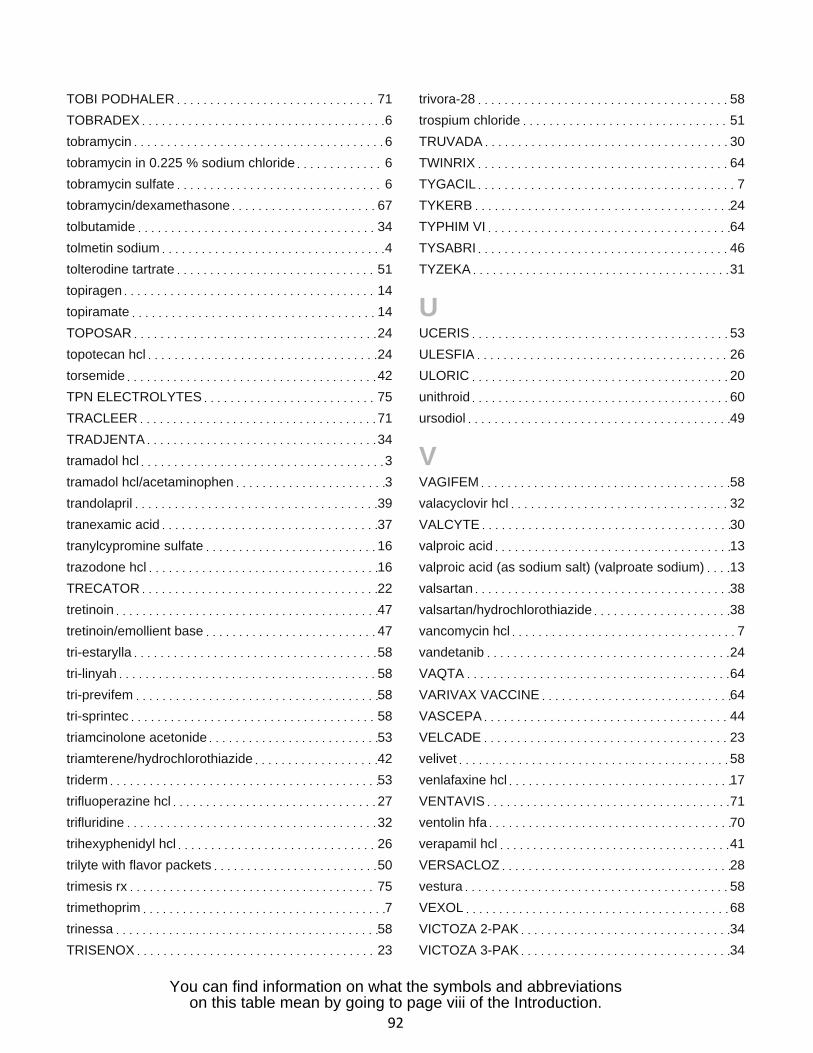
TOBI PODHALER 71
TOBRADEX 6
tobramycin 6
tobramycin in 0.225 % sodium chloride 6
tobramycin sulfate 6
tobramycin/dexamethasone 67
tolbutamide 34
tolmetin sodium 4
tolterodine tartrate 51
topiragen 14
topiramate 14
TOPOSAR 24
topotecan hcl 24
torsemide 42
TPN ELECTROLYTES 75
TRACLEER 71
TRADJENTA 34
tramadol hcl 3
tramadol hcl/acetaminophen 3
trandolapril 39
tranexamic acid 37
tranylcypromine sulfate 16
trazodone hcl 16
TRECATOR 22
tretinoin 47
tretinoin/emollient base 47
tri-estarylla 58
tri-linyah 58
tri-previfem 58
tri-sprintec 58
triamcinolone acetonide 53
triamterene/hydrochlorothiazide 42
triderm 53
trifluoperazine hcl 27
trifluridine 32
trihexyphenidyl hcl 26
trilyte with flavor packets 50
trimesis rx 75
trimethoprim 7
trinessa 58
TRISENOX 23
trivora-28 58
trospium chloride 51
TRUVADA 30
TWINRIX 64
TYGACIL 7
TYKERB 24
TYPHIM VI 64
TYSABRI 46
TYZEKA 31
UUCERIS 53
ULESFIA 26
ULORIC 20
unithroid 60
ursodiol 49
VVAGIFEM 58
valacyclovir hcl 32
VALCYTE 30
valproic acid 13
valproic acid (as sodium salt) (valproate sodium) 13
valsartan 38
valsartan/hydrochlorothiazide 38
vancomycin hcl 7
vandetanib 24
VAQTA 64
VARIVAX VACCINE 64
VASCEPA 44
VELCADE 23
velivet 58
venlafaxine hcl 17
VENTAVIS 71
ventolin hfa 70
verapamil hcl 41
VERSACLOZ 28
vestura 58
VEXOL 68
VICTOZA 2-PAK 34
VICTOZA 3-PAK 34
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
92
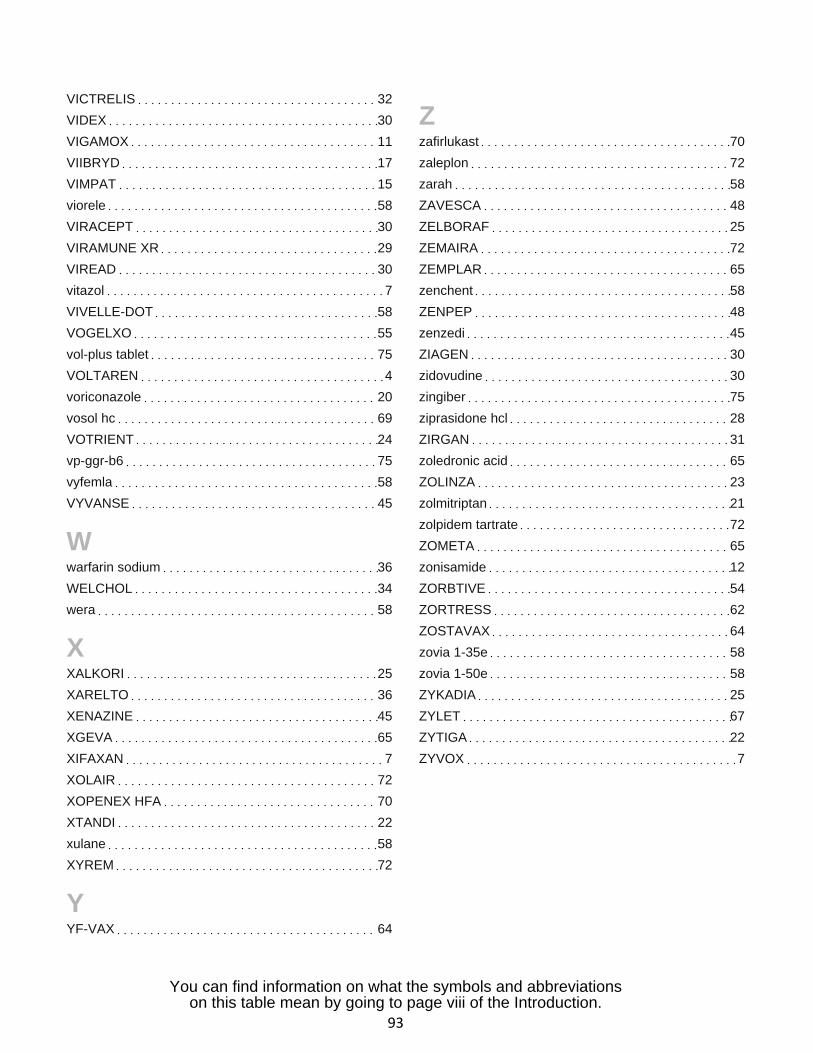
VICTRELIS 32
VIDEX 30
VIGAMOX 11
VIIBRYD 17
VIMPAT 15
viorele 58
VIRACEPT 30
VIRAMUNE XR 29
VIREAD 30
vitazol 7
VIVELLE-DOT 58
VOGELXO 55
vol-plus tablet 75
VOLTAREN 4
voriconazole 20
vosol hc 69
VOTRIENT 24
vp-ggr-b6 75
vyfemla 58
VYVANSE 45
Wwarfarin sodium 36
WELCHOL 34
wera 58
XXALKORI 25
XARELTO 36
XENAZINE 45
XGEVA 65
XIFAXAN 7
XOLAIR 72
XOPENEX HFA 70
XTANDI 22
xulane 58
XYREM 72
YYF-VAX 64
Zzafirlukast 70
zaleplon 72
zarah 58
ZAVESCA 48
ZELBORAF 25
ZEMAIRA 72
ZEMPLAR 65
zenchent 58
ZENPEP 48
zenzedi 45
ZIAGEN 30
zidovudine 30
zingiber 75
ziprasidone hcl 28
ZIRGAN 31
zoledronic acid 65
ZOLINZA 23
zolmitriptan 21
zolpidem tartrate 72
ZOMETA 65
zonisamide 12
ZORBTIVE 54
ZORTRESS 62
ZOSTAVAX 64
zovia 1-35e 58
zovia 1-50e 58
ZYKADIA 25
ZYLET 67
ZYTIGA 22
ZYVOX 7
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
93
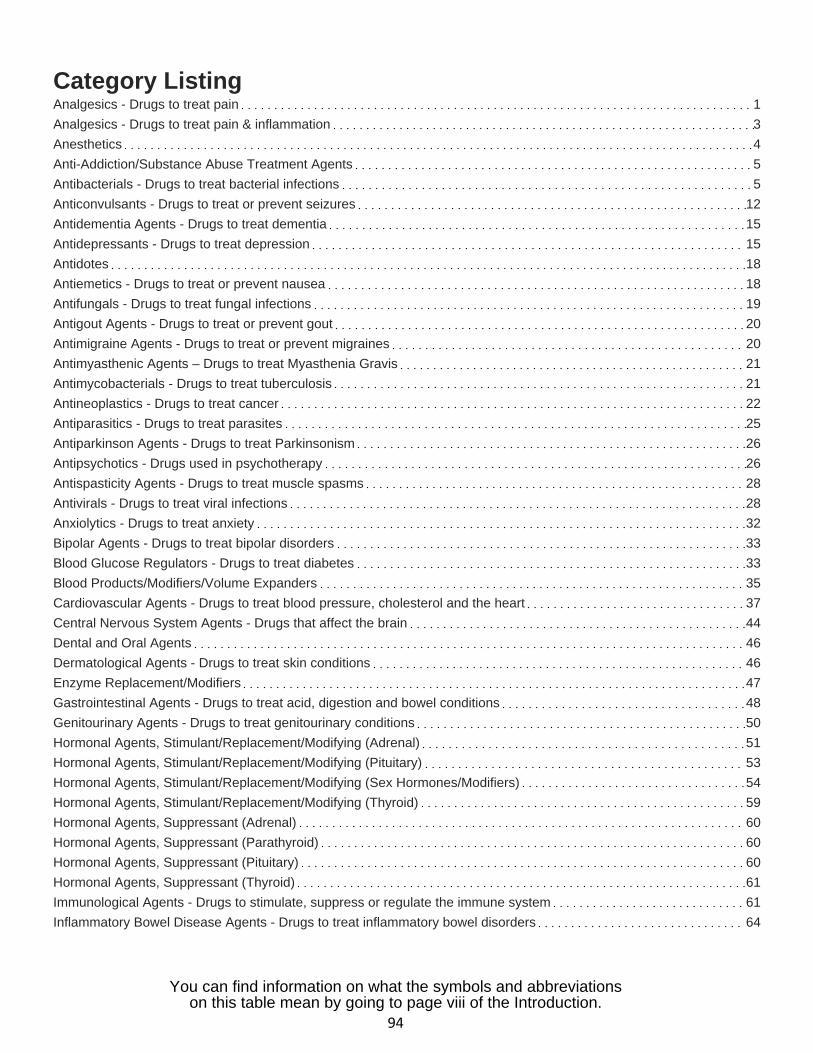
Category ListingAnalgesics - Drugs to treat pain 1
Analgesics - Drugs to treat pain & inflammation 3
Anesthetics 4
Anti-Addiction/Substance Abuse Treatment Agents 5
Antibacterials - Drugs to treat bacterial infections 5
Anticonvulsants - Drugs to treat or prevent seizures 12
Antidementia Agents - Drugs to treat dementia 15
Antidepressants - Drugs to treat depression 15
Antidotes 18
Antiemetics - Drugs to treat or prevent nausea 18
Antifungals - Drugs to treat fungal infections 19
Antigout Agents - Drugs to treat or prevent gout 20
Antimigraine Agents - Drugs to treat or prevent migraines 20
Antimyasthenic Agents – Drugs to treat Myasthenia Gravis 21
Antimycobacterials - Drugs to treat tuberculosis 21
Antineoplastics - Drugs to treat cancer 22
Antiparasitics - Drugs to treat parasites 25
Antiparkinson Agents - Drugs to treat Parkinsonism 26
Antipsychotics - Drugs used in psychotherapy 26
Antispasticity Agents - Drugs to treat muscle spasms 28
Antivirals - Drugs to treat viral infections 28
Anxiolytics - Drugs to treat anxiety 32
Bipolar Agents - Drugs to treat bipolar disorders 33
Blood Glucose Regulators - Drugs to treat diabetes 33
Blood Products/Modifiers/Volume Expanders 35
Cardiovascular Agents - Drugs to treat blood pressure, cholesterol and the heart 37
Central Nervous System Agents - Drugs that affect the brain 44
Dental and Oral Agents 46
Dermatological Agents - Drugs to treat skin conditions 46
Enzyme Replacement/Modifiers 47
Gastrointestinal Agents - Drugs to treat acid, digestion and bowel conditions 48
Genitourinary Agents - Drugs to treat genitourinary conditions 50
Hormonal Agents, Stimulant/Replacement/Modifying (Adrenal) 51
Hormonal Agents, Stimulant/Replacement/Modifying (Pituitary) 53
Hormonal Agents, Stimulant/Replacement/Modifying (Sex Hormones/Modifiers) 54
Hormonal Agents, Stimulant/Replacement/Modifying (Thyroid) 59
Hormonal Agents, Suppressant (Adrenal) 60
Hormonal Agents, Suppressant (Parathyroid) 60
Hormonal Agents, Suppressant (Pituitary) 60
Hormonal Agents, Suppressant (Thyroid) 61
Immunological Agents - Drugs to stimulate, suppress or regulate the immune system 61
Inflammatory Bowel Disease Agents - Drugs to treat inflammatory bowel disorders 64
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
94
Metabolic Bone Disease Agents - Drugs to treat metabolic bone disorders 64Miscellaneous 65Ophthalmic Agents - Drugs to treat eye conditions 66Otic Agents - Drugs to treat ear conditions 68Respiratory Tract/Pulmonary Agents - Drugs to treat allergies or breathing conditions 69Skeletal Muscle Relaxants - Drugs to treat muscle spasms 72Sleep Disorder Agents - Drugs to treat sleep disorders 72Therapeutic Nutrients/Minerals/Electrolytes 72
You can find information on what the symbols and abbreviationson this table mean by going to page viii of the Introduction.
95
Premera Blue Cross is an HMO and HMO-POS plan with a Medicare contract. Enrollment in Premera Blue Cross depends on contract renewal.
Customer Service:
Premera Blue Cross Medicare AdvantagePO Box 4196Portland, OR 97208-4196
Call toll free 888-850-8526 (TTY: 711)Representatives are available between8 a.m. and 8 p.m., seven days a week.
premera.com
027877 (10-2014)H7245_2015Rx_Accepted
Version 6
Top Related