







Languages
Pages
Legal

the risk of heart disease and stroke in alabama:
b u r d e n d o c u m e n t
findinG the Path toCardioVasCUlar health
2010
table of Contents
executive Summary ................................................................................................................. 1
demographic characteristics of Alabama ................................................................................. 2
Leading causes of death ......................................................................................................... 3
cardiovascular disease ........................................................................................................... 4
Heart disease ......................................................................................................................... 8
Stroke ................................................................................................................................... 11
cardiovascular risk Factors: High blood Pressure ................................................................. 14
cardiovascular risk Factors: High blood cholesterol .............................................................. 16
cardiovascular risk Factors: diabetes ................................................................................... 18
cardiovascular risk Factors: overweight and obesity ............................................................. 20
cardiovascular risk Factors: Smoking ................................................................................... 22
cardiovascular risk Factors: Physical Inactivity ..................................................................... 24
cardiovascular risk Factors: Fruit and Vegetable consumption .............................................. 26
economic cost of cardiovascular disease .............................................................................. 28
Access to care ...................................................................................................................... 29
Signs and Symptoms of Heart Attack or Stroke ...................................................................... 32
Sodium consumption ............................................................................................................ 33
references ........................................................................................................................... 34
exeCUtiVe sUmmary
cardiovascular disease (cVd), which includes heart disease and stroke, is the leading cause of death in the united States and in Alabama.
Heart disease, the most common form of cVd, is the single leading cause of death in Alabama. In 2006, heart disease accounted for 12,583 (26.7 percent) deaths in the state. men continue to have a higher age-adjusted heart disease mortality rate than women. coronary heart disease, the most common type of heart disease, can result in a heart attack. Heart attacks may be preventable by modifying risk factors.
brain attack, a cerebrovascular accident (cVA) also known as stroke, is the third leading cause of death in Alabama, following heart disease and cancer. In 2006, strokes accounted for 2,740 (5.83 percent) deaths in the state. men are about 50 percent more likely to die from stroke than women, and there are strong race/ethnic differences. blacks have significantly higher age-adjusted stroke mortality rates when compared to whites. As with heart disease, cerebrovascular accidents can be preventable by modifying risk factors.
modifiable risk factors for heart disease and stroke are as follows:
1. High blood pressure 2. High blood cholesterol 3. diabetes 4. overweight and obesity 5. Smoking 6. Physical inactivity 7. Inadequate fruit and vegetable consumption
compared to the nation, Alabama continues to have a high prevalence of these risk factors. the following Alabama statistical data compiled in 2009 revealed that all these factors contributed to an increase in cVd in the state.
• 27.2 percent of Alabama adults reported being affected by high blood pressure.
• 39.9 percent of Alabama adults were diagnosed with elevated blood cholesterol.
• Prevalence of diabetes in Alabamians is 12.2 percent—an increase of 74 percent since 1998.
• currently, 68.1 percent of obese and overweight individuals in Alabama have multiple risk factors that contribute to cVd.
• 22.5 percent of Alabama adults are smokers—doubling an individual’s risk for cVd.
• 31 percent of Alabama adults indicated they were physically inactive.
• only 20.6 percent of Alabama adults met recommended fruit and vegetable intake requirements.
Focusing on prevention can help reduce deaths from heart disease and stroke by:
1. reducing risk factors 2. Increasing public awareness of warning signs and symptoms of heart attack and stroke
3. decreasing the time between the appearance of warning signs and symptoms and the receipt of appropriate medical care
this report provides details about the burden of cVd by describing the mortality rates and risk factors associated with heart disease and stroke.
findinG the Path to CardioVasCUlar health 2010 • 1
2 • the risk of heart disease and stroke in alabama: bUrden doCUment
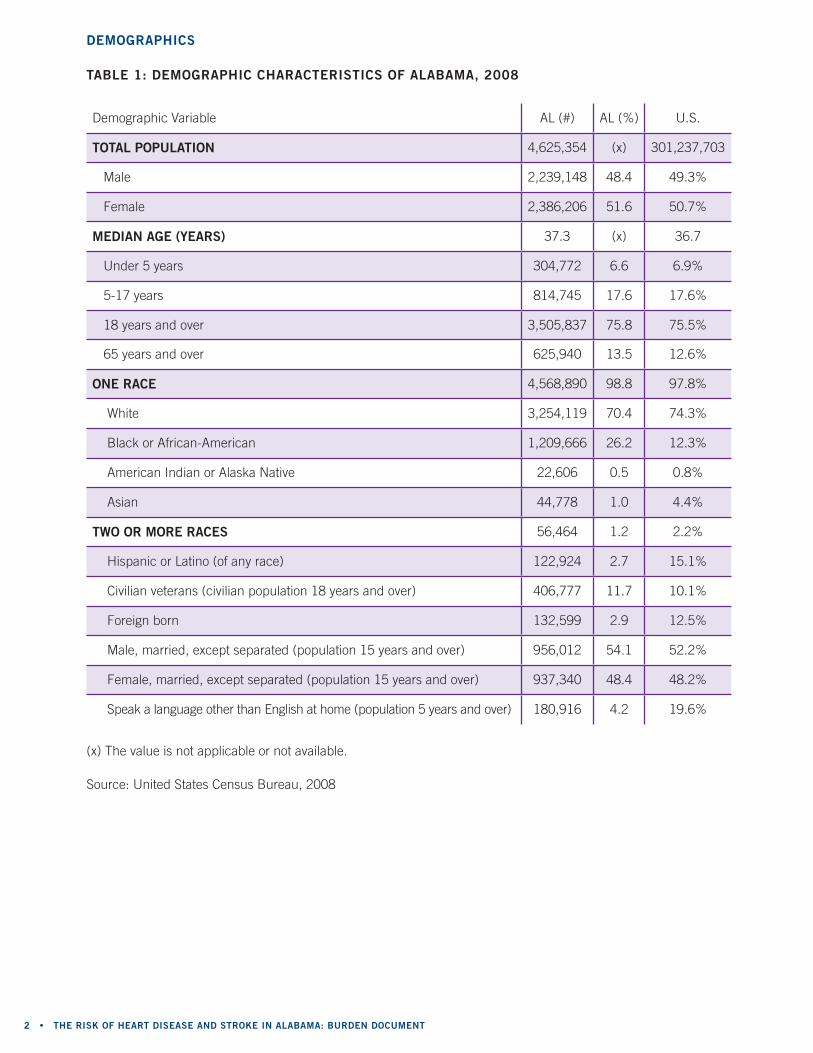
demoGraPhiCs
table 1: demoGraPhiC CharaCteristiCs of alabama, 2008
demographic Variable AL (#) AL (%) u.S.
total PoPUlation 4,625,354 (x) 301,237,703
male 2,239,148 48.4 49.3%
Female 2,386,206 51.6 50.7%
median aGe (years) 37.3 (x) 36.7
under 5 years 304,772 6.6 6.9%
5-17 years 814,745 17.6 17.6%
18 years and over 3,505,837 75.8 75.5%
65 years and over 625,940 13.5 12.6%
one raCe 4,568,890 98.8 97.8%
White 3,254,119 70.4 74.3%
black or African-American 1,209,666 26.2 12.3%
American Indian or Alaska native 22,606 0.5 0.8%
Asian 44,778 1.0 4.4%
two or more raCes 56,464 1.2 2.2%
Hispanic or Latino (of any race) 122,924 2.7 15.1%
civilian veterans (civilian population 18 years and over) 406,777 11.7 10.1%
Foreign born 132,599 2.9 12.5%
male, married, except separated (population 15 years and over) 956,012 54.1 52.2%
Female, married, except separated (population 15 years and over) 937,340 48.4 48.2%
Speak a language other than english at home (population 5 years and over) 180,916 4.2 19.6%
Source: united States census bureau, 2008
(x) the value is not applicable or not available.
findinG the Path to CardioVasCUlar health 2010 • 3
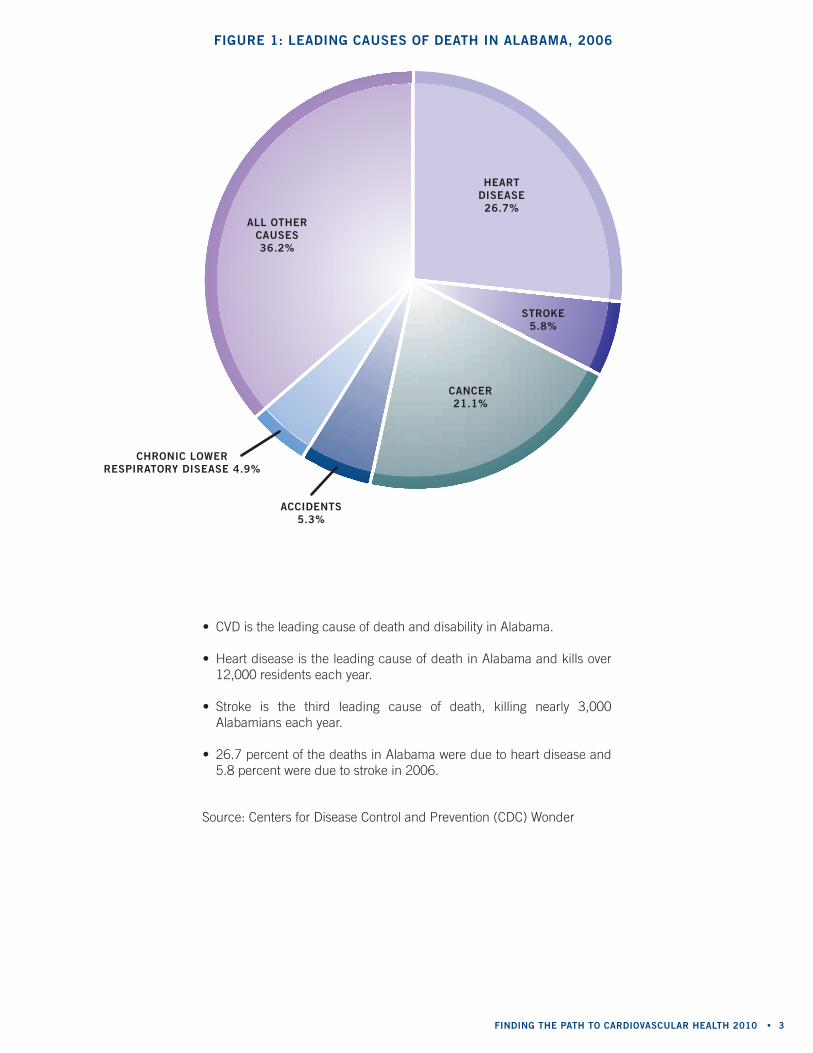
fiGUre 1: leadinG CaUses of death in alabama, 2006
• cVd is the leading cause of death and disability in Alabama.
• Heart disease is the leading cause of death in Alabama and kills over 12,000 residents each year.
• Stroke is the third leading cause of death, killing nearly 3,000 Alabamians each year.
• 26.7 percent of the deaths in Alabama were due to heart disease and 5.8 percent were due to stroke in 2006.
Source: centers for disease control and Prevention (cdc) Wonder
aCCidents 5.3%
CanCer21.1%
all other CaUses36.2%
ChroniC lower resPiratory disease 4.9%
heartdisease26.7%
stroke5.8%
4 • the risk of heart disease and stroke in alabama: bUrden doCUment
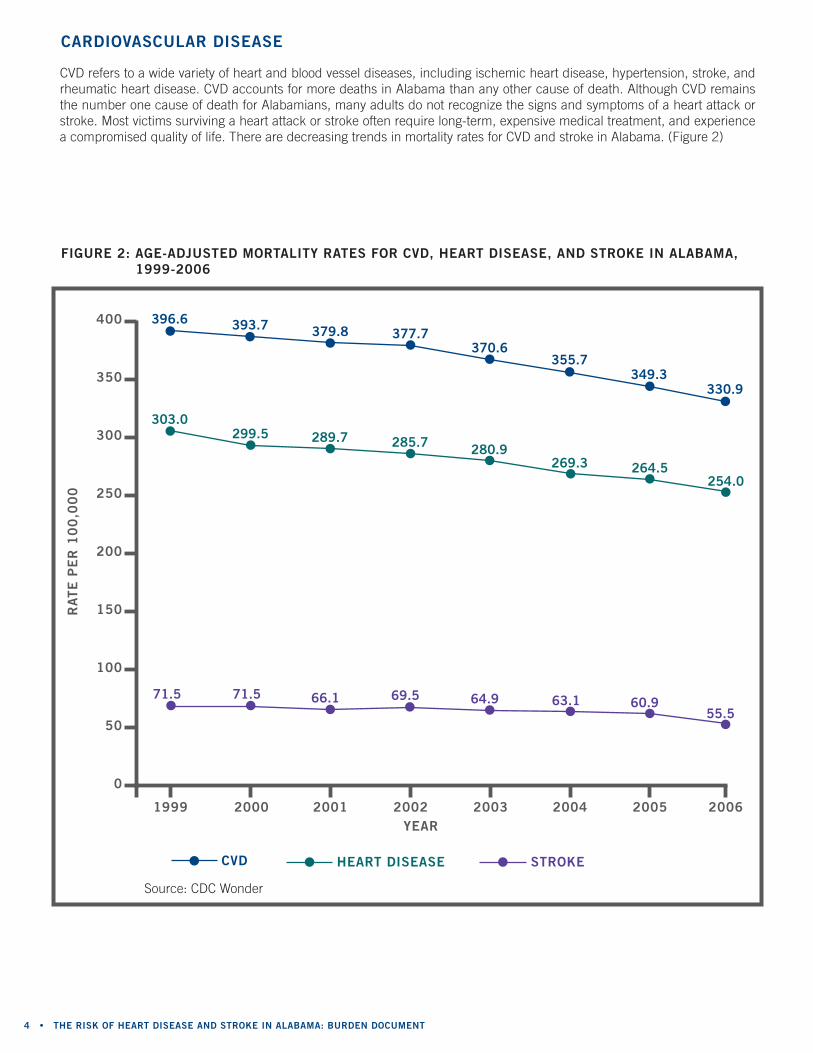
fiGUre 2: aGe-adjUsted mortality rates for CVd, heart disease, and stroke in alabama, 1999-2006
400
350
300
250
200
150
100
50
0
rate
Pe
r 1
00
,00
0
year
60.955.5
349.3330.9
2005 20061999 2000 2001 2002 2003 2004
396.6
71.5 71.5 66.1 69.5 64.9 63.1
264.5254.0
303.0299.5 289.7 285.7 280.9
269.3
393.7 379.8 377.7370.6
355.7
strokeCVd heart disease
Source: cdc Wonder
cVd refers to a wide variety of heart and blood vessel diseases, including ischemic heart disease, hypertension, stroke, and rheumatic heart disease. cVd accounts for more deaths in Alabama than any other cause of death. Although cVd remains the number one cause of death for Alabamians, many adults do not recognize the signs and symptoms of a heart attack or stroke. most victims surviving a heart attack or stroke often require long-term, expensive medical treatment, and experience a compromised quality of life. there are decreasing trends in mortality rates for cVd and stroke in Alabama. (Figure 2)
CardioVasCUlar disease
findinG the Path to CardioVasCUlar health 2010 • 5
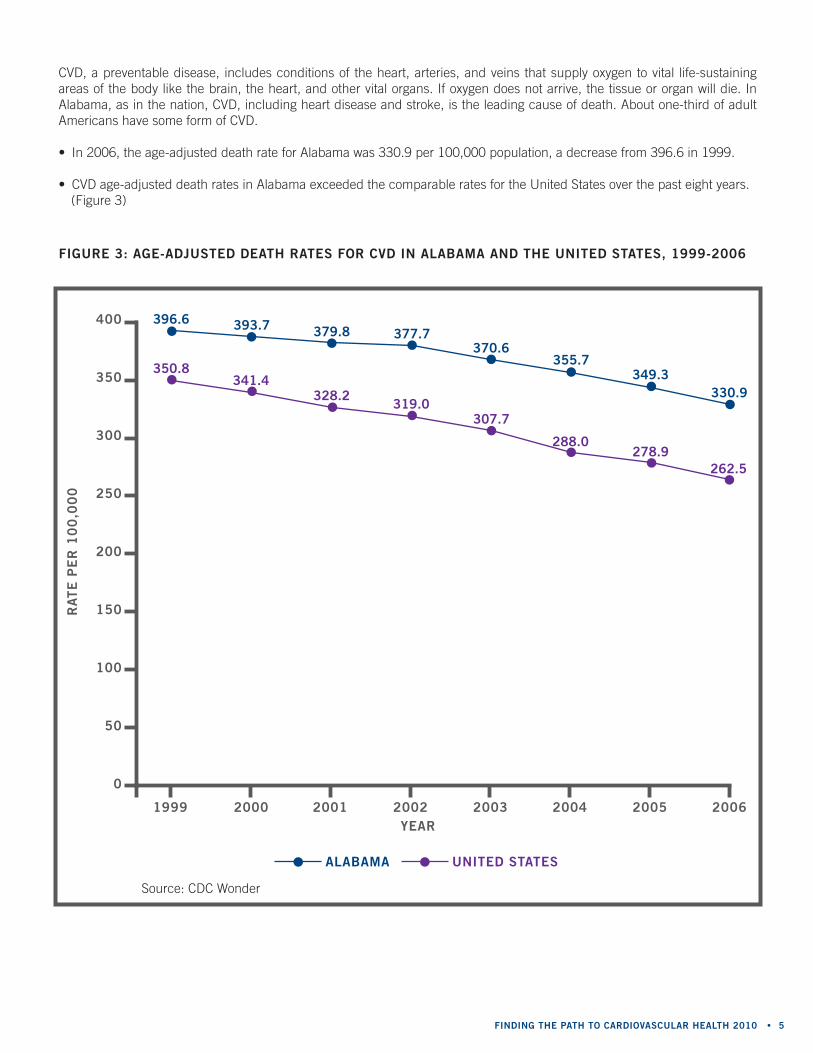
fiGUre 3: aGe-adjUsted death rates for CVd in alabama and the United states, 1999-2006
year
400
350
300
250
200
150
100
50
0
rate
Pe
r 1
00
,00
0
1999 2000 2001 2002 2003 2004 2005 2006
396.6
350.8341.4
328.2319.0
307.7
288.0278.9
262.5
393.7 379.8 377.7370.6
355.7349.3
330.9
Source: cdc Wonder
alabama United states
cVd, a preventable disease, includes conditions of the heart, arteries, and veins that supply oxygen to vital life-sustaining areas of the body like the brain, the heart, and other vital organs. If oxygen does not arrive, the tissue or organ will die. In Alabama, as in the nation, cVd, including heart disease and stroke, is the leading cause of death. About one-third of adult Americans have some form of cVd.
• In 2006, the age-adjusted death rate for Alabama was 330.9 per 100,000 population, a decrease from 396.6 in 1999.
• cVd age-adjusted death rates in Alabama exceeded the comparable rates for the united States over the past eight years.(Figure 3)
6 • the risk of heart disease and stroke in alabama: bUrden doCUment
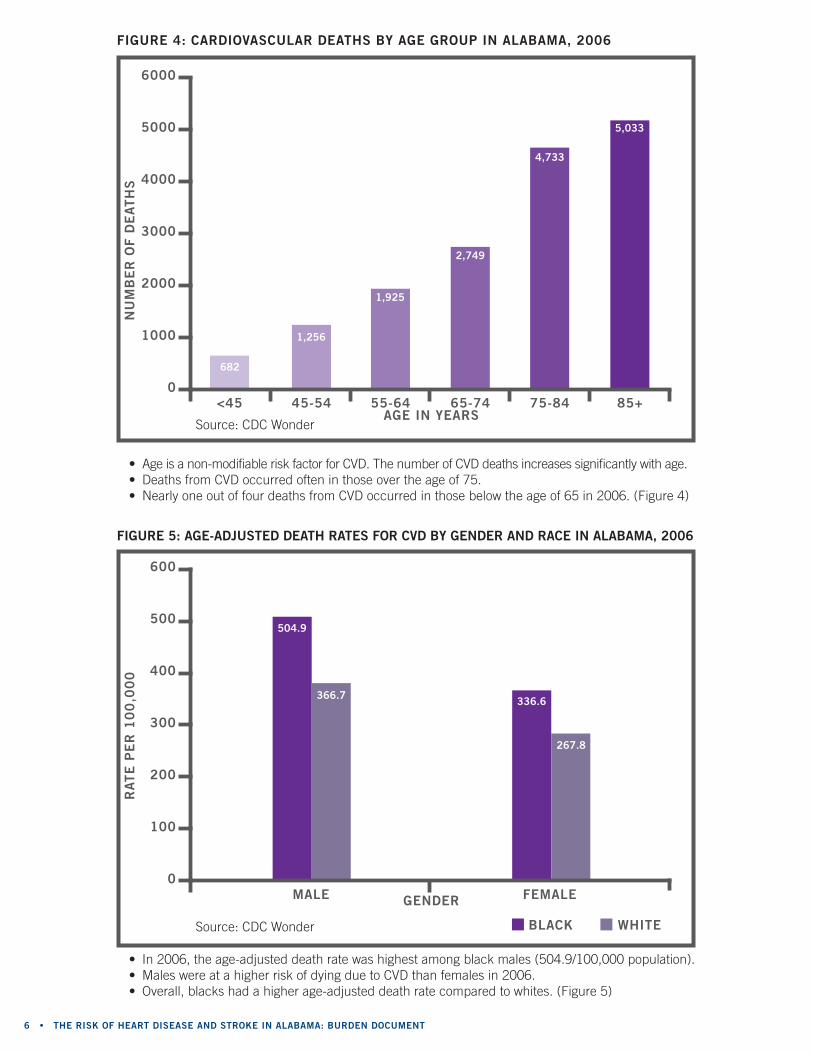
fiGUre 4: CardioVasCUlar deaths by aGe GroUP in alabama, 2006
• Age is a non-modifiable risk factor for cVd. the number of cVd deaths increases significantly with age.• deaths from cVd occurred often in those over the age of 75.• nearly one out of four deaths from cVd occurred in those below the age of 65 in 2006. (Figure 4)
Source: cdc Wonder
6000
5000
4000
3000
2000
1000
0<45 45-54 55-64 65-74 75-84 85+
682
1,256
1,925
2,749
4,733
5,033
aGe in years
nU
mb
er
of d
eath
s
fiGUre 5: aGe-adjUsted death rates for CVd by Gender and raCe in alabama, 2006
• In 2006, the age-adjusted death rate was highest among black males (504.9/100,000 population).• males were at a higher risk of dying due to cVd than females in 2006.• overall, blacks had a higher age-adjusted death rate compared to whites. (Figure 5)
Source: cdc Wonder
600
500
400
300
200
100
0male female
504.9
366.7 336.6
267.8
whiteblaCk
Gender
rate
Pe
r 1
00
,00
0
findinG the Path to CardioVasCUlar health 2010 • 7
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
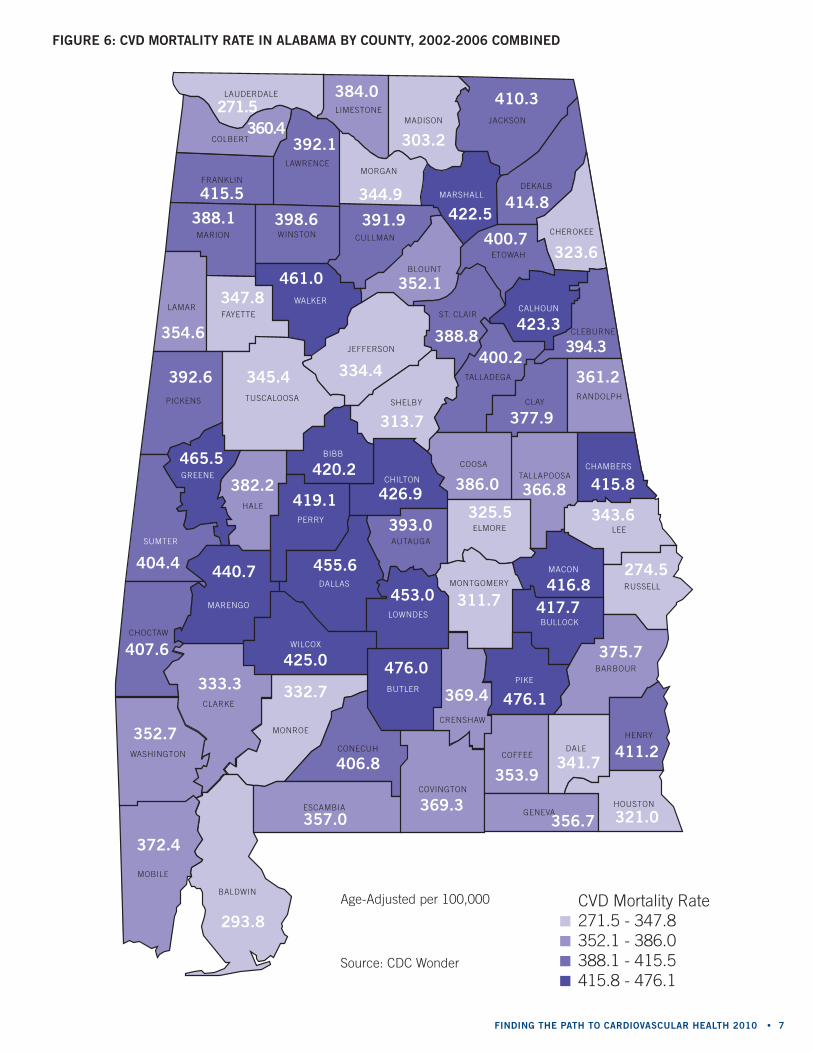
Age-Adjusted per 100,000
Source: cdc Wonder
fiGUre 6: CVd mortality rate in alabama by CoUnty, 2002-2006 Combined
344.9
271.5360.4
392.1
384.0
303.2
410.3
414.8422.5391.9398.6
415.5
388.1
461.0347.8
354.6
345.4392.6
404.4
465.5
382.2420.2
419.1 426.9 386.0 366.8 415.8
343.6
416.8
325.5
311.7
393.0
453.0
425.0
332.7
293.8
372.4
357.0
406.8
476.0
369.4
353.9
476.1
341.7411.2
321.0369.3
356.7
440.7
333.3
407.6
352.7
455.6 274.5
375.7
417.7
334.4
352.1
388.8423.3
400.7323.6
394.3
361.2
377.9
400.2
313.7
cVd mortality rate271.5 - 347.8352.1 - 386.0388.1 - 415.5415.8 - 476.1

8 • the risk of heart disease and stroke in alabama: bUrden doCUment
Heart disease is a grouping of various conditions of the heart including coronary heart disease, congestive heart failure, heart attack, hypertension, and others. It is the leading cause of death for both men and women. more than 600,000 deaths occur each year in the united States. It is the most common form of cVd and can cause angina (chest pain), myocardial infarction (heart attacks), and cardiac arrest. many times, a heart attack is the first sign of heart disease.
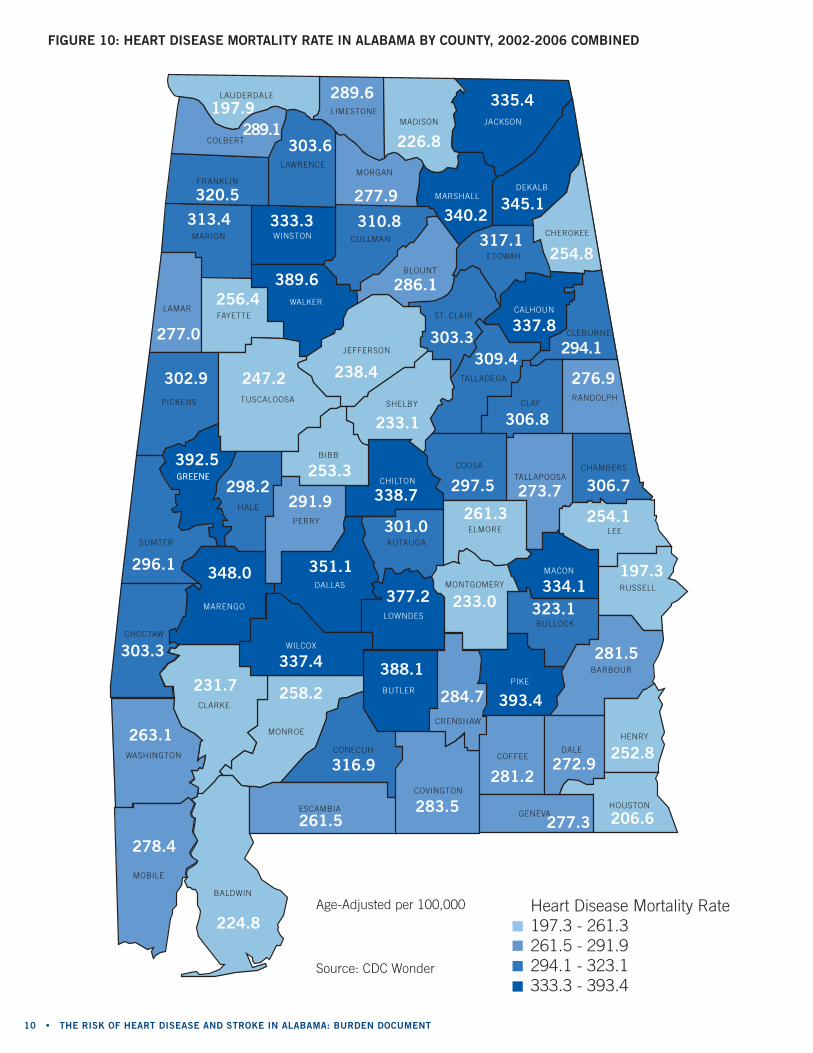
• In 2006, the age-adjusted mortality rate for heart disease was 254.0 per 100,000 population in Alabama and 200.2 per 100,000 population in the united States.
• Heart disease death rates in Alabama have shown to be consistently higher than the united States heart disease death rates since 1999. (Figure 7)
heart disease
fiGUre 7: aGe-adjUsted death rates for heart disease in alabama and the United states, 1999-2006
Source: cdc Wonder
300
250
200
150
100
50
0
266.4257.6
247.8 240.8232.3
217.0 211.1200.2
303.0 299.5 289.7 285.7 280.9269.3
264.5254
United statesalabama
2005 20061999 2000 2001 2002 2003 2004
year
rate
Pe
r 1
00
,00
0
findinG the Path to CardioVasCUlar health 2010 • 9
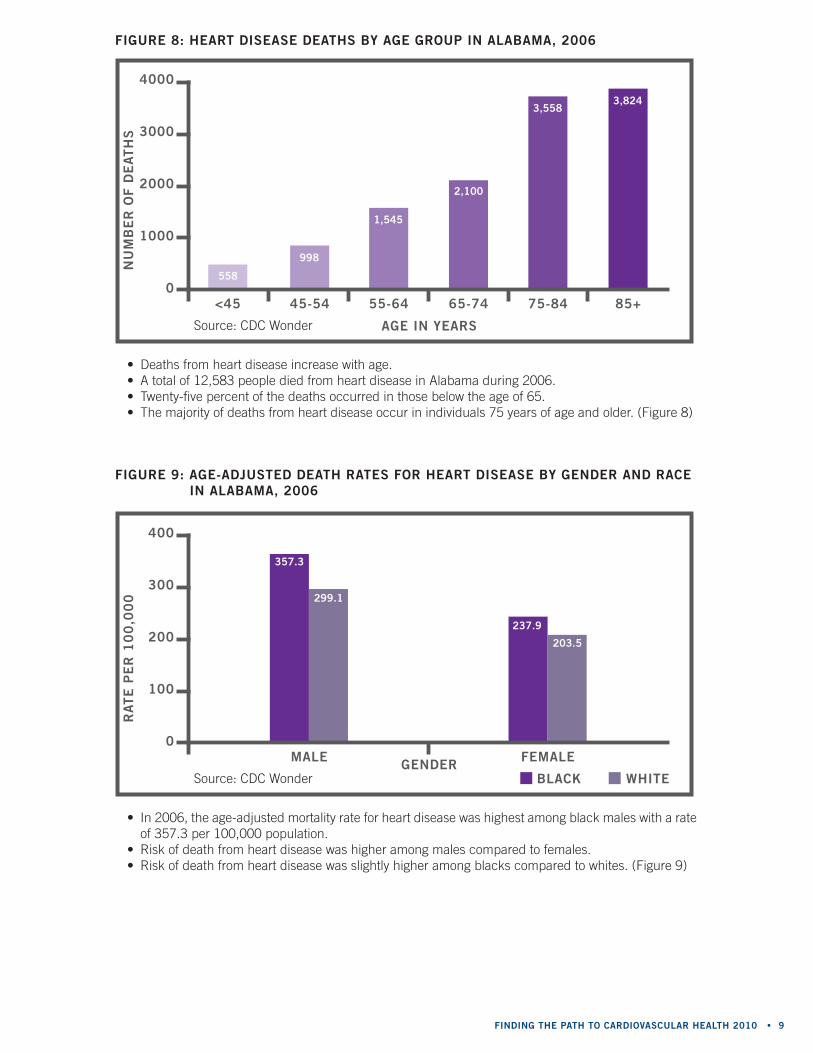
fiGUre 8: heart disease deaths by aGe GroUP in alabama, 2006
• deaths from heart disease increase with age.• A total of 12,583 people died from heart disease in Alabama during 2006.• twenty-five percent of the deaths occurred in those below the age of 65.• the majority of deaths from heart disease occur in individuals 75 years of age and older. (Figure 8)
Source: cdc Wonder
4000
3000
2000
1000
0<45 45-54 55-64 65-74 75-84 85+
558
998
1,545
2,100
3,5583,824
fiGUre 9: aGe-adjUsted death rates for heart disease by Gender and raCe in alabama, 2006
• In 2006, the age-adjusted mortality rate for heart disease was highest among black males with a rate of 357.3 per 100,000 population.
• risk of death from heart disease was higher among males compared to females.• risk of death from heart disease was slightly higher among blacks compared to whites. (Figure 9)
Source: cdc Wonder
400
300
200
100
0male female
357.3
299.1
237.9
203.5
whiteblaCk
aGe in years
Gender
nU
mb
er
of d
eath
sr
ate
Pe
r 1
00
,00
0
10 • the risk of heart disease and stroke in alabama: bUrden doCUment
fiGUre 10: heart disease mortality rate in alabama by CoUnty, 2002-2006 Combined
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENEGREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
277.9
197.9289.1
303.6
289.6
226.8
335.4
345.1340.2310.8333.3
320.5
313.4
389.6256.4
277.0
247.2302.9
296.1
392.5
298.2253.3
291.9 338.7 297.5 273.7 306.7
254.1
334.1
261.3
233.0
301.0
377.2
337.4
258.2
224.8
278.4
261.5
316.9
388.1
284.7
281.2
393.4
272.9252.8
206.6283.5
277.3
348.0
231.7
303.3
263.1
351.1 197.3
281.5
323.1
238.4
286.1
303.3337.8
317.1254.8
294.1
276.9
306.8
309.4
233.1
Heart disease mortality rate197.3 - 261.3261.5 - 291.9294.1 - 323.1333.3 - 393.4
Age-Adjusted per 100,000
Source: cdc Wonder
findinG the Path to CardioVasCUlar health 2010 • 11
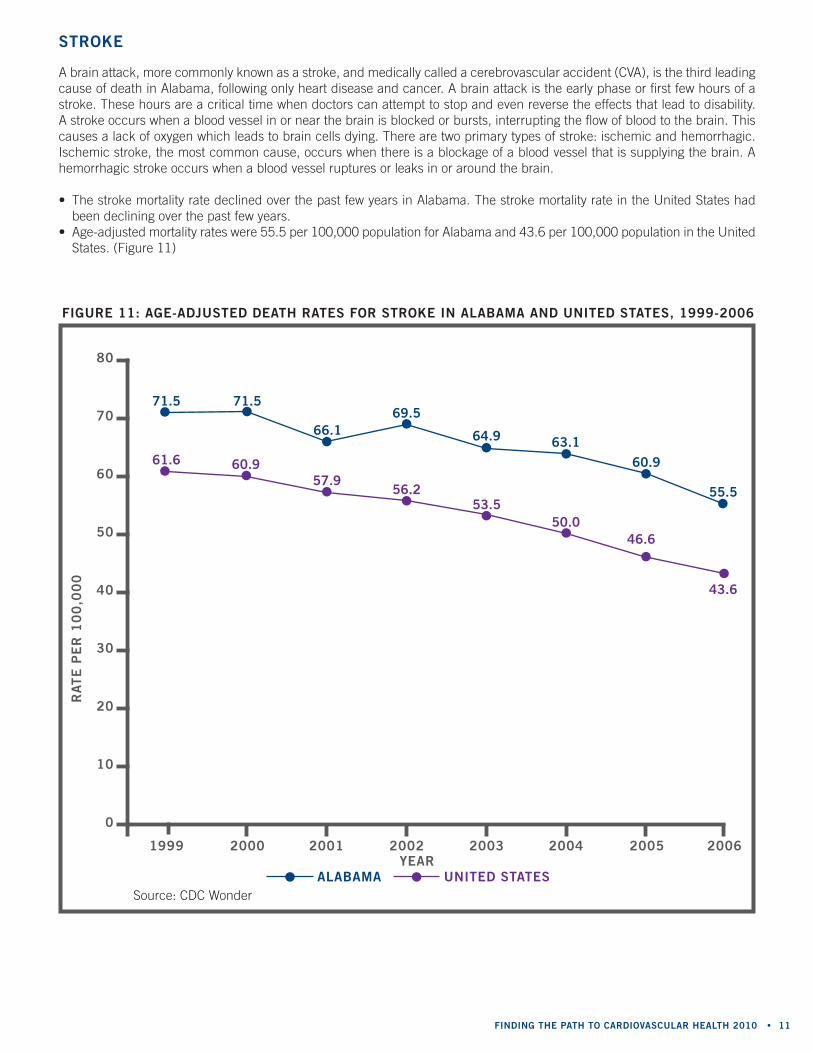
A brain attack, more commonly known as a stroke, and medically called a cerebrovascular accident (cVA), is the third leading cause of death in Alabama, following only heart disease and cancer. A brain attack is the early phase or first few hours of a stroke. these hours are a critical time when doctors can attempt to stop and even reverse the effects that lead to disability. A stroke occurs when a blood vessel in or near the brain is blocked or bursts, interrupting the flow of blood to the brain. this causes a lack of oxygen which leads to brain cells dying. there are two primary types of stroke: ischemic and hemorrhagic. Ischemic stroke, the most common cause, occurs when there is a blockage of a blood vessel that is supplying the brain. A hemorrhagic stroke occurs when a blood vessel ruptures or leaks in or around the brain.
• the stroke mortality rate declined over the past few years in Alabama. the stroke mortality rate in the united States had been declining over the past few years.
• Age-adjusted mortality rates were 55.5 per 100,000 population for Alabama and 43.6 per 100,000 population in the united States. (Figure 11)
stroke
fiGUre 11: aGe-adjUsted death rates for stroke in alabama and United states, 1999-2006
Source: cdc Wonder
1999 2000 2001 2002 2003 2004 2005 2006
80
70
60
50
40
30
20
10
0
71.5 71.5
66.169.5
64.9 63.160.9
55.5
61.6 60.957.9
56.253.5
43.6
50.046.6
alabama United statesyear
rate
Pe
r 1
00
,00
0
12 • the risk of heart disease and stroke in alabama: bUrden doCUment12
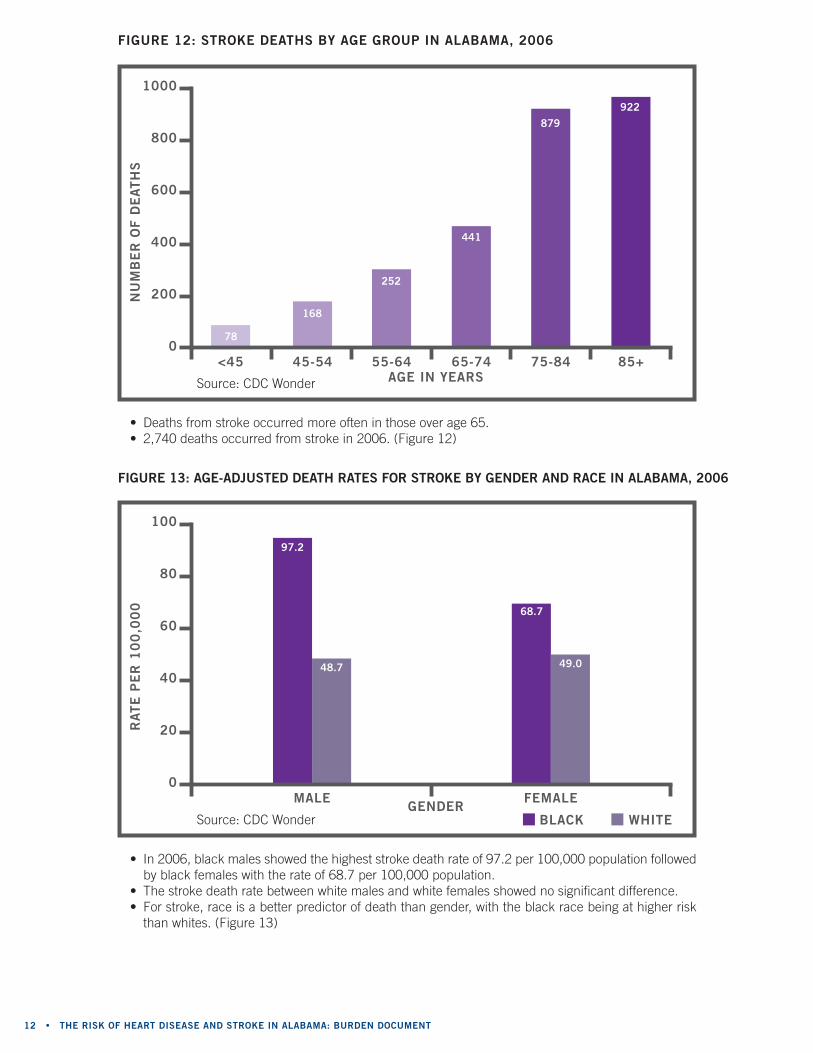
fiGUre 12: stroke deaths by aGe GroUP in alabama, 2006
• deaths from stroke occurred more often in those over age 65.• 2,740 deaths occurred from stroke in 2006. (Figure 12)
fiGUre 13: aGe-adjUsted death rates for stroke by Gender and raCe in alabama, 2006
• In 2006, black males showed the highest stroke death rate of 97.2 per 100,000 population followed by black females with the rate of 68.7 per 100,000 population.
• the stroke death rate between white males and white females showed no significant difference.• For stroke, race is a better predictor of death than gender, with the black race being at higher risk
than whites. (Figure 13)
Source: cdc Wonder
100
80
60
40
20
0male female
97.2
48.7
68.7
49.0
whiteblaCk
Source: cdc Wonder
1000
800
600
400
200
0<45 45-54 55-64 65-74 75-84 85+
78
168
252
441
879
922
aGe in years
Gender
nU
mb
er
of d
eath
sr
ate
Pe
r 1
00
,00
0

findinG the Path to CardioVasCUlar health 2010 • 13
fiGUre 14: stroke mortality rate in alabama by CoUnty, 2002-2006 Combined
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
51.0
60.352.9
71.5
66.4
54.9
60.0
51.167.565.346.6
79.3
58.6
54.269.1
63.5
67.962.7
76.7
54.0
60.4141.7
104.2 64.9 60.5 59.6 92.5
69.3
55.6
47.3
56.0
67.0
57.8
70.1
58.5
48.0
61.2
58.7
78.4
69.3
68.1
51.9
58.6
46.297.1
47.070.2
58.5
70.9
77.6
87.3
57.9
77.2 58.3
72.5
64.4
72.1
48.5
66.563.7
66.959.0
59.0
62.1
55.4
74.3
60.8
Age-Adjusted per 100,000
Source: cdc Wonder
Stroke mortality rate46.2 - 57.857.9 - 62.162.7 - 70.170.2 - 141.7
14 • the risk of heart disease and stroke in alabama: bUrden doCUment
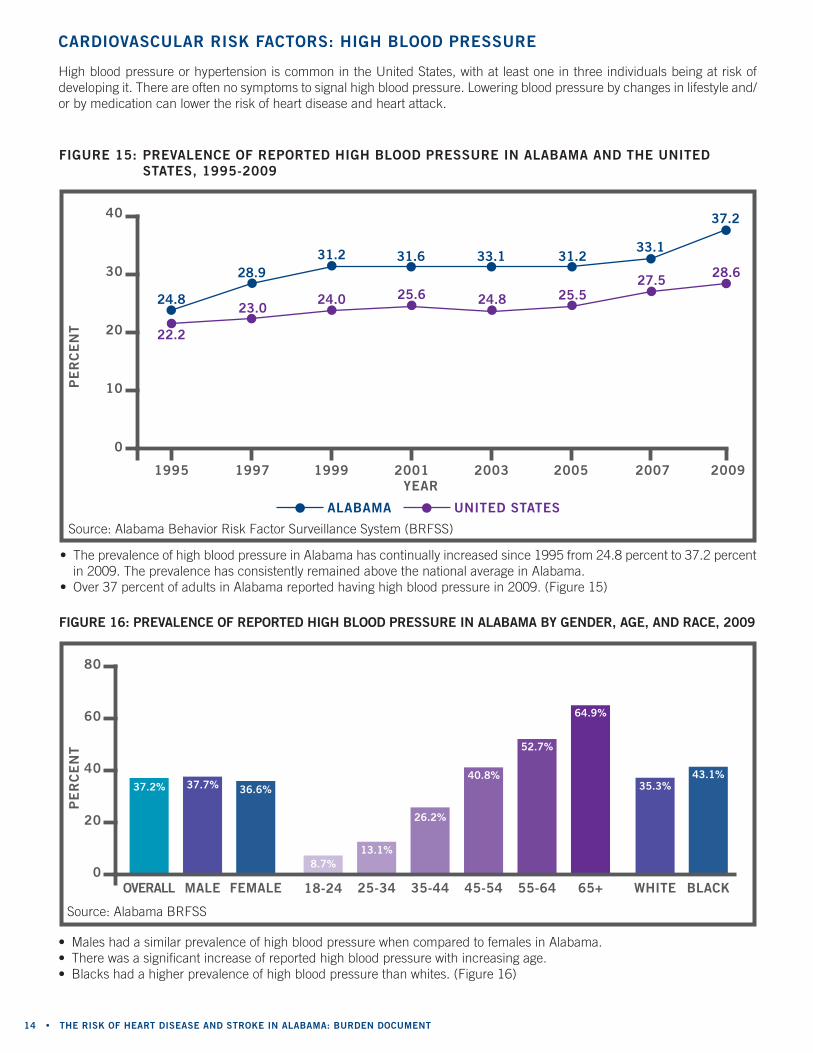
• the prevalence of high blood pressure in Alabama has continually increased since 1995 from 24.8 percent to 37.2 percent in 2009. the prevalence has consistently remained above the national average in Alabama.
• over 37 percent of adults in Alabama reported having high blood pressure in 2009. (Figure 15)
fiGUre 15: PreValenCe of rePorted hiGh blood PressUre in alabama and the United states, 1995-2009
40
30
20
10
0
2007 2009
33.1
37.2
27.5 28.6
1995 1997 1999 2001 2003 2005
24.8
28.931.2 31.6 33.1 31.2
22.2
23.024.0 25.6 24.8 25.5
alabama United states
• males had a similar prevalence of high blood pressure when compared to females in Alabama.• there was a significant increase of reported high blood pressure with increasing age.• blacks had a higher prevalence of high blood pressure than whites. (Figure 16)
fiGUre 16: PreValenCe of rePorted hiGh blood PressUre in alabama by Gender, aGe, and raCe, 2009
blaCk
43.1%35.3%
80
60
40
20
0maleoVerall female
37.7%37.2% 36.6%
white18-24
8.7%
25-34
13.1%
35-44
26.2%
45-54
40.8%
55-64
52.7%
65+
64.9%
High blood pressure or hypertension is common in the united States, with at least one in three individuals being at risk of developing it. there are often no symptoms to signal high blood pressure. Lowering blood pressure by changes in lifestyle and/or by medication can lower the risk of heart disease and heart attack.
CardioVasCUlar risk faCtors: hiGh blood PressUre
year
Pe
rC
en
tP
er
Ce
nt
Source: Alabama behavior risk Factor Surveillance System (brFSS)
Source: Alabama brFSS
findinG the Path to CardioVasCUlar health 2010 • 1515
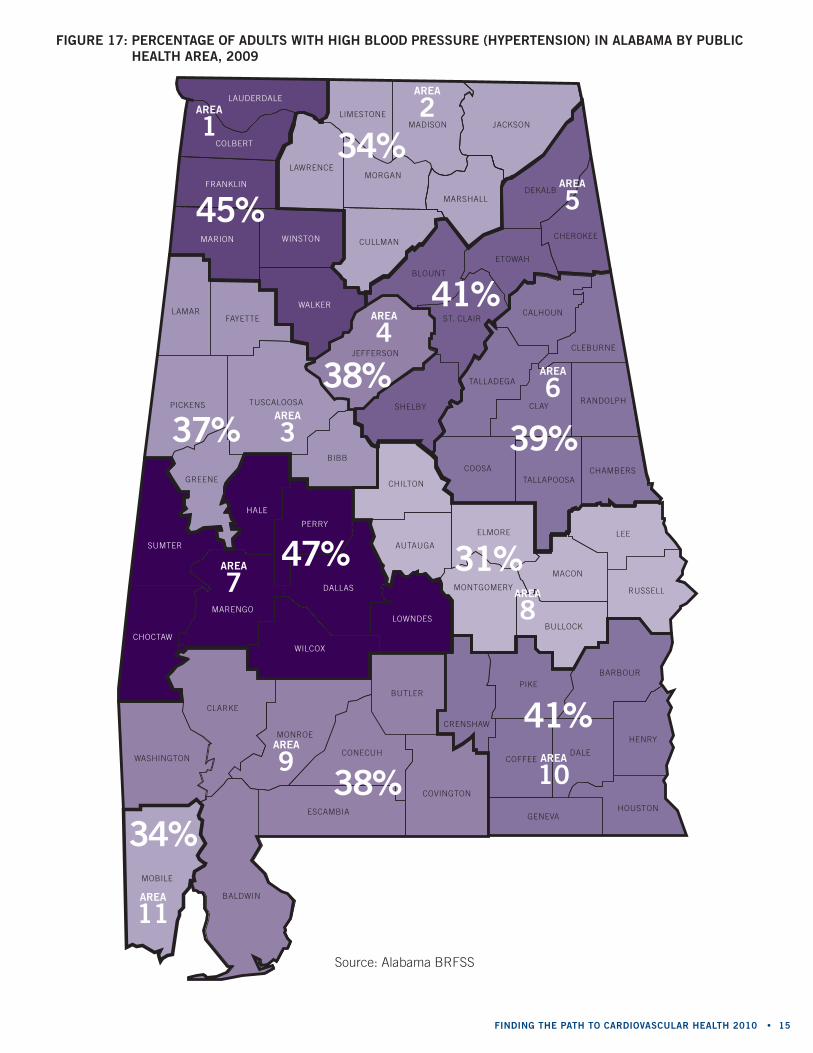
fiGUre 17: PerCentaGe of adUlts with hiGh blood PressUre (hyPertension) in alabama by PUbliC health area, 2009
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8
area
7
area
3
area
4area
6
area
5
area
2area
1
34%38%
41%
31%47%
37%
38%
39%
41%
34%
45%
Source: Alabama brFSS
16 • the risk of heart disease and stroke in alabama: bUrden doCUment16
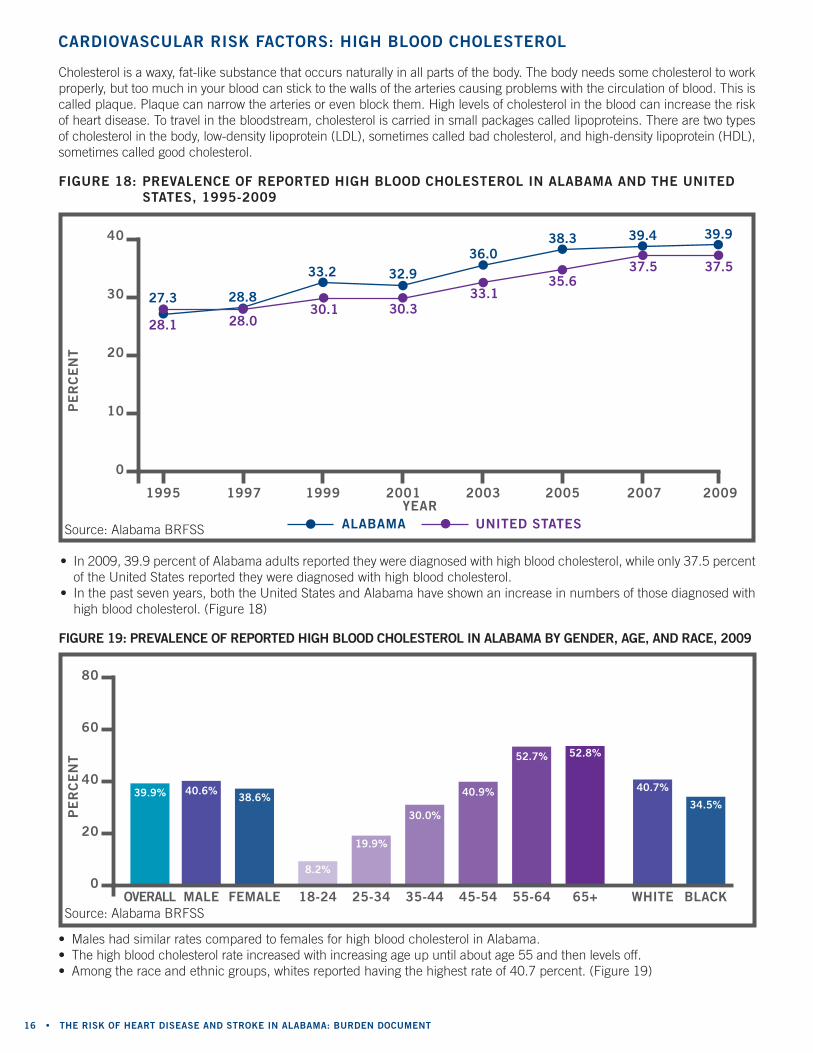
• males had similar rates compared to females for high blood cholesterol in Alabama.• the high blood cholesterol rate increased with increasing age up until about age 55 and then levels off.• Among the race and ethnic groups, whites reported having the highest rate of 40.7 percent. (Figure 19)
fiGUre 19: PreValenCe of rePorted hiGh blood Cholesterol in alabama by Gender, aGe, and raCe, 2009
blaCk
34.5%
40.7%
80
60
40
20
0male female
40.6%38.6%
white18-24
8.2%
25-34
19.9%
35-44
30.0%
45-54
40.9%
55-64
52.7%
65+
52.8%
• In 2009, 39.9 percent of Alabama adults reported they were diagnosed with high blood cholesterol, while only 37.5 percent of the united States reported they were diagnosed with high blood cholesterol.
• In the past seven years, both the united States and Alabama have shown an increase in numbers of those diagnosed with high blood cholesterol. (Figure 18)
fiGUre 18: PreValenCe of rePorted hiGh blood Cholesterol in alabama and the United states, 1995-2009
40
30
20
10
0
alabama United states
38.3 39.4 39.9
27.3 28.8
33.2 32.9
36.0
2007 20092005
35.637.5 37.5
1995 1997 1999 2001 2003
28.1 28.030.1 30.3
33.1
cholesterol is a waxy, fat-like substance that occurs naturally in all parts of the body. the body needs some cholesterol to work properly, but too much in your blood can stick to the walls of the arteries causing problems with the circulation of blood. this is called plaque. Plaque can narrow the arteries or even block them. High levels of cholesterol in the blood can increase the risk of heart disease. to travel in the bloodstream, cholesterol is carried in small packages called lipoproteins. there are two types of cholesterol in the body, low-density lipoprotein (LdL), sometimes called bad cholesterol, and high-density lipoprotein (HdL), sometimes called good cholesterol.
CardioVasCUlar risk faCtors: hiGh blood Cholesterol
year
Pe
rC
en
tP
er
Ce
nt
Source: Alabama brFSS
Source: Alabama brFSSoVerall
39.9%
findinG the Path to CardioVasCUlar health 2010 • 17
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8
area
7
area
3
area
4area
6
area
5
area
2area
1
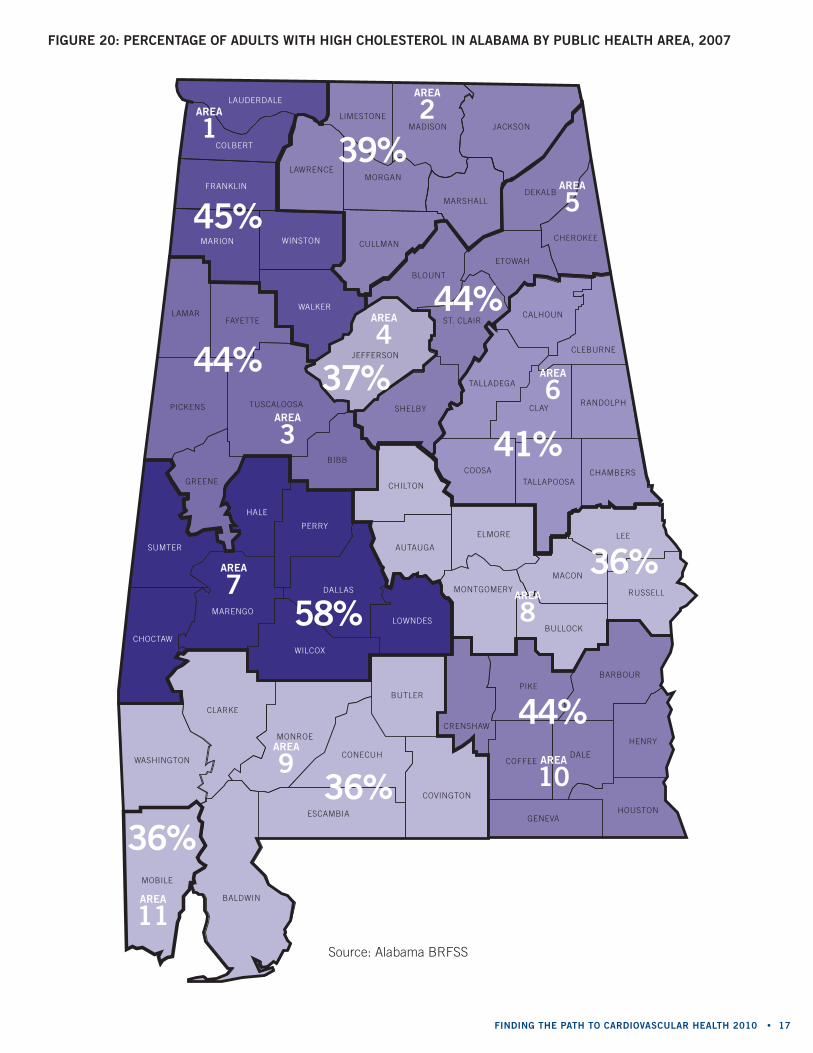
36%36%
44%
36%58%
44% 37%
41%
44%
39%
45%
fiGUre 20: PerCentaGe of adUlts with hiGh Cholesterol in alabama by PUbliC health area, 2007
Source: Alabama brFSS
18 • the risk of heart disease and stroke in alabama: bUrden doCUment
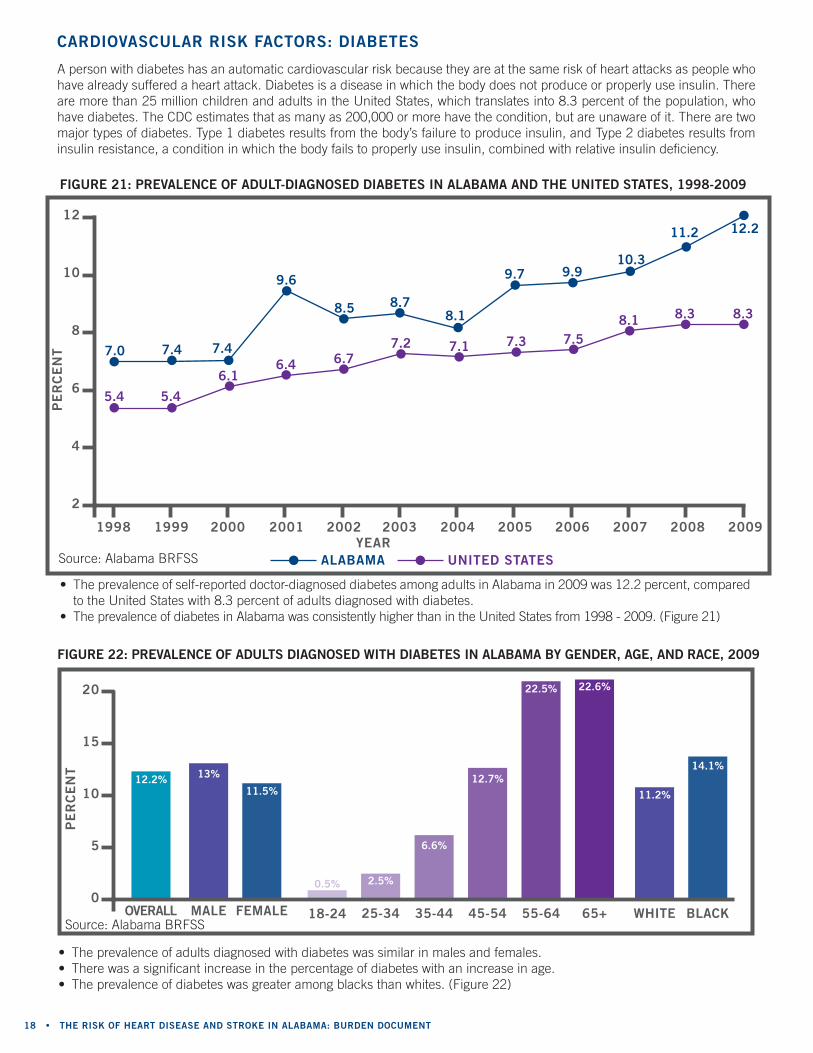
• the prevalence of self-reported doctor-diagnosed diabetes among adults in Alabama in 2009 was 12.2 percent, compared to the united States with 8.3 percent of adults diagnosed with diabetes.
• the prevalence of diabetes in Alabama was consistently higher than in the united States from 1998 - 2009. (Figure 21)
fiGUre 21: PreValenCe of adUlt-diaGnosed diabetes in alabama and the United states, 1998-2009
12
10
8
6
4
2
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
7.0 7.4 7.4
9.6
8.5 8.78.1
9.7 9.910.3
11.2 12.2
5.4 5.4
6.16.4 6.7
7.2 7.1 7.3 7.58.1 8.3 8.3
alabama United states
A person with diabetes has an automatic cardiovascular risk because they are at the same risk of heart attacks as people who have already suffered a heart attack. diabetes is a disease in which the body does not produce or properly use insulin. there are more than 25 million children and adults in the united States, which translates into 8.3 percent of the population, who have diabetes. the cdc estimates that as many as 200,000 or more have the condition, but are unaware of it. there are two major types of diabetes. type 1 diabetes results from the body’s failure to produce insulin, and type 2 diabetes results from insulin resistance, a condition in which the body fails to properly use insulin, combined with relative insulin deficiency.
CardioVasCUlar risk faCtors: diabetes
year
Pe
rC
en
t
Source: Alabama brFSS
• the prevalence of adults diagnosed with diabetes was similar in males and females.• there was a significant increase in the percentage of diabetes with an increase in age.• the prevalence of diabetes was greater among blacks than whites. (Figure 22)
fiGUre 22: PreValenCe of adUlts diaGnosed with diabetes in alabama by Gender, aGe, and raCe, 2009
blaCk
14.1%
11.2%
20
15
10
5
0male female
13%
11.5%
white18-24
0.5%
25-34
2.5%
35-44
6.6%
45-54
12.7%
55-64
22.5%
65+
22.6%
Pe
rC
en
t
Source: Alabama brFSSoVerall
12.2%
findinG the Path to CardioVasCUlar health 2010 • 19
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8
area
7
area
3
area
4area
6
area
5
area
2area
1
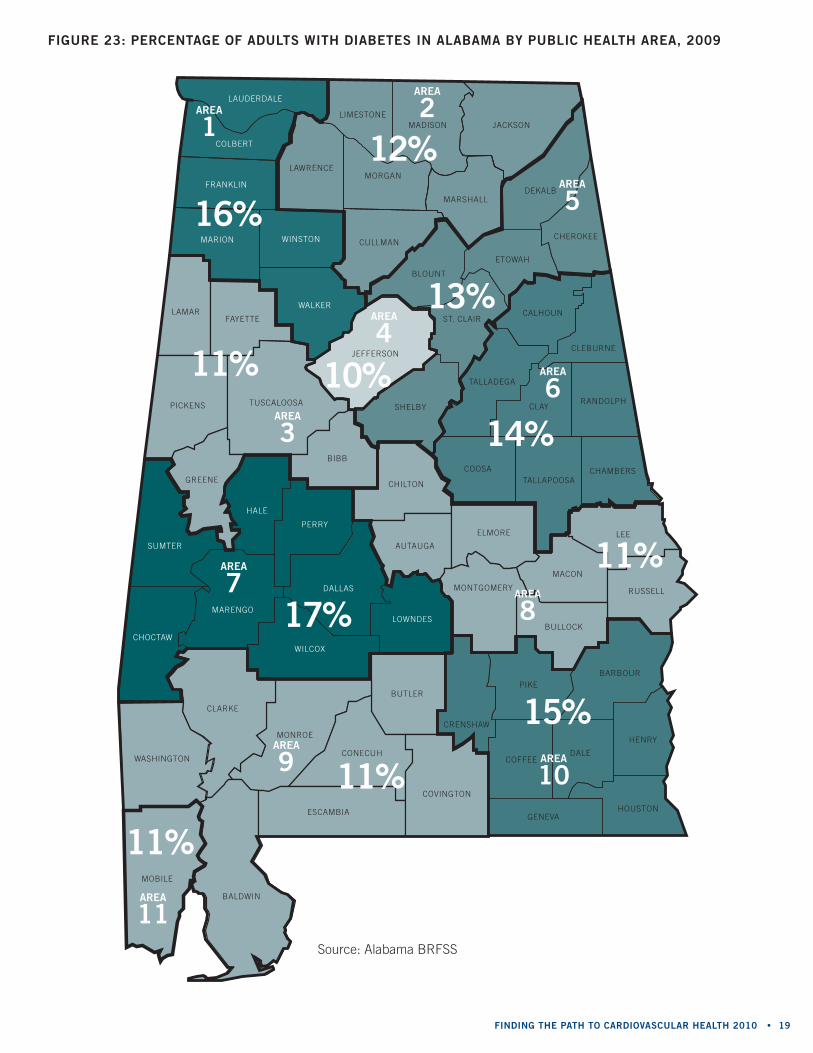
11%
11%
15%
11%
17%
11% 10%
14%
13%
12%
16%
fiGUre 23: PerCentaGe of adUlts with diabetes in alabama by PUbliC health area, 2009
Source: Alabama brFSS
20 • the risk of heart disease and stroke in alabama: bUrden doCUment
blaCk
74.2%
66.1%
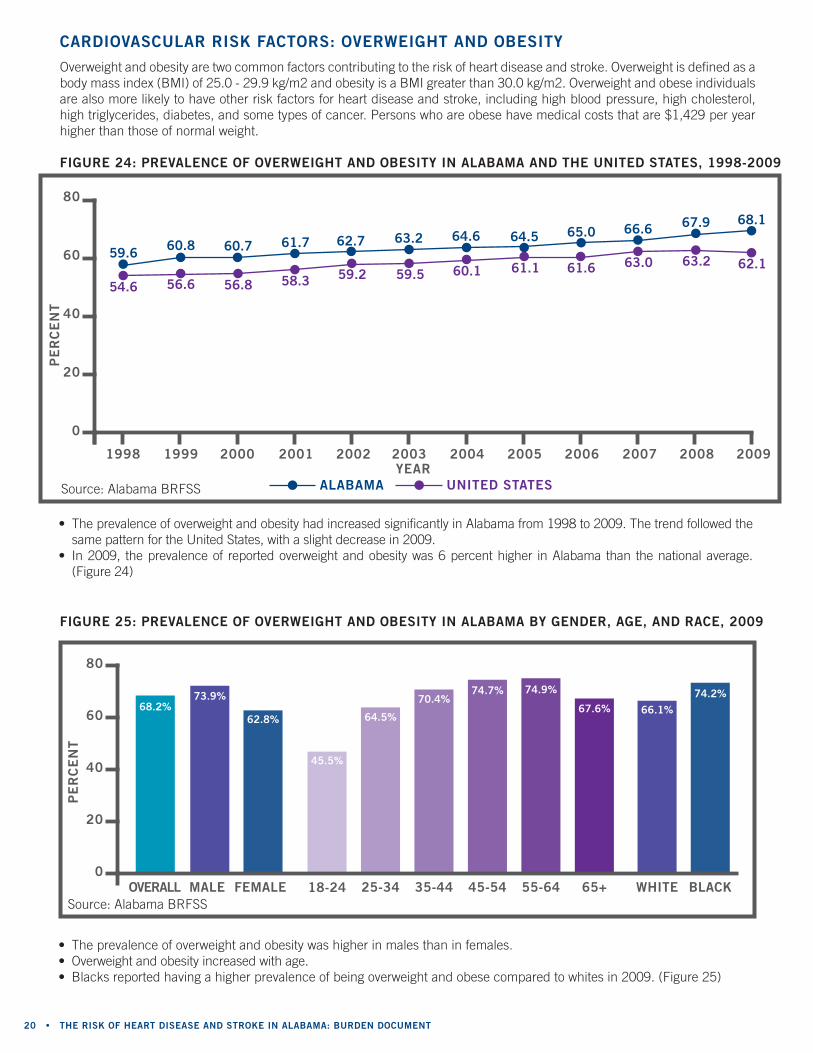
fiGUre 25: PreValenCe of oVerweiGht and obesity in alabama by Gender, aGe, and raCe, 2009
• the prevalence of overweight and obesity was higher in males than in females.• overweight and obesity increased with age.• blacks reported having a higher prevalence of being overweight and obese compared to whites in 2009. (Figure 25)
80
60
40
20
0male female
73.9%68.2%
62.8%
white18-24
45.5%
25-34
64.5%
35-44
70.4%
45-54
74.7%
55-64
74.9%
65+
67.6%
• the prevalence of overweight and obesity had increased significantly in Alabama from 1998 to 2009. the trend followed the same pattern for the united States, with a slight decrease in 2009.
• In 2009, the prevalence of reported overweight and obesity was 6 percent higher in Alabama than the national average. (Figure 24)
fiGUre 24: PreValenCe of oVerweiGht and obesity in alabama and the United states, 1998-2009
59.6 60.8 60.7 61.7 62.7 63.2 64.6 64.5 65.0 66.6 67.9 68.1
54.6 56.6 56.8 58.3 59.2 59.5 60.1 61.1 61.6 63.0 63.2 62.1
alabama United states
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
80
60
40
20
0
overweight and obesity are two common factors contributing to the risk of heart disease and stroke. overweight is defined as a body mass index (bmI) of 25.0 - 29.9 kg/m2 and obesity is a bmI greater than 30.0 kg/m2. overweight and obese individuals are also more likely to have other risk factors for heart disease and stroke, including high blood pressure, high cholesterol, high triglycerides, diabetes, and some types of cancer. Persons who are obese have medical costs that are $1,429 per year higher than those of normal weight.
CardioVasCUlar risk faCtors: oVerweiGht and obesity
year
Pe
rC
en
tP
er
Ce
nt
Source: Alabama brFSS
Source: Alabama brFSSoVerall
findinG the Path to CardioVasCUlar health 2010 • 21
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8area
7
area
3
area
4area
6
area
5
area
2area
1
66%
69%
73%
69%78%
71% 66%
72%
69%
62%
74%
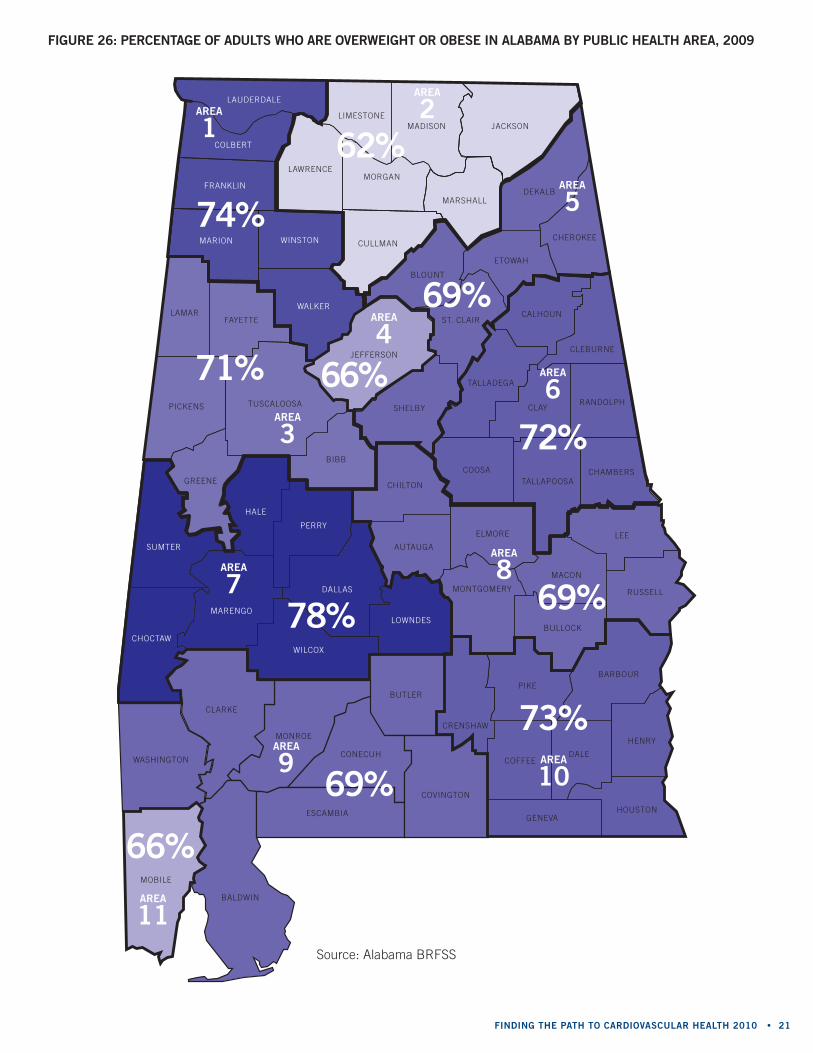
fiGUre 26: PerCentaGe of adUlts who are oVerweiGht or obese in alabama by PUbliC health area, 2009
Source: Alabama brFSS
22 • the risk of heart disease and stroke in alabama: bUrden doCUment
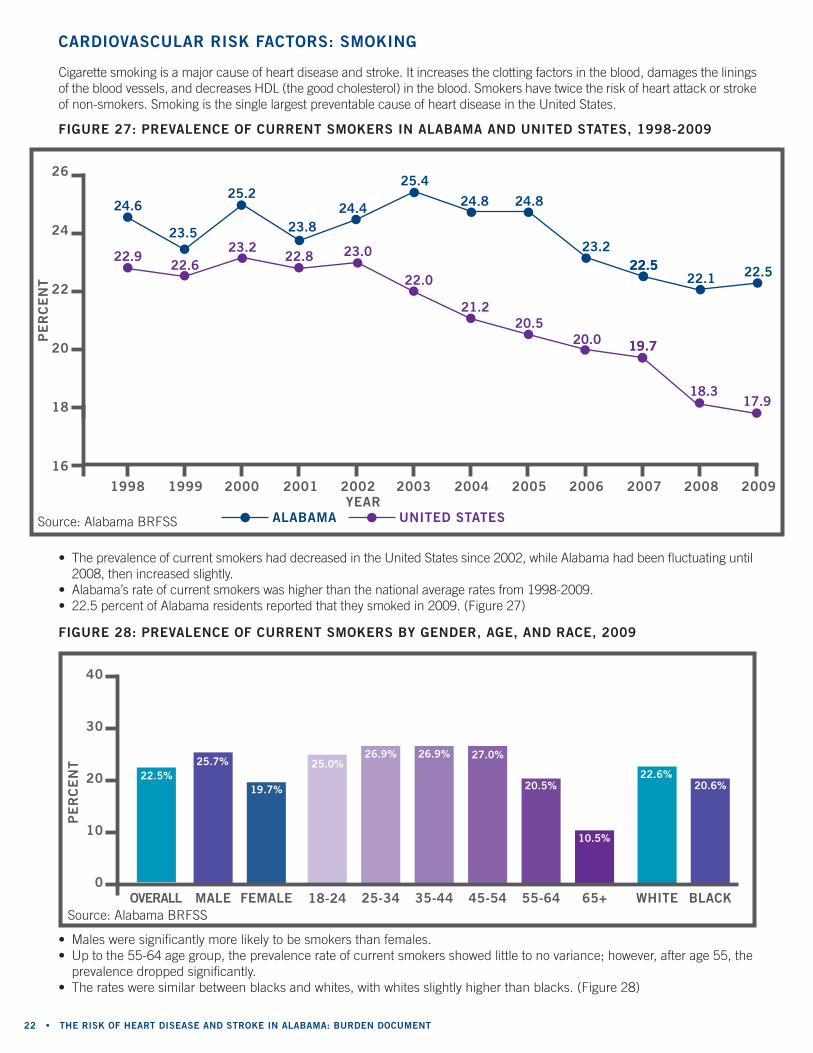
fiGUre 28: PreValenCe of CUrrent smokers by Gender, aGe, and raCe, 2009
• males were significantly more likely to be smokers than females.• up to the 55-64 age group, the prevalence rate of current smokers showed little to no variance; however, after age 55, the
prevalence dropped significantly.• the rates were similar between blacks and whites, with whites slightly higher than blacks. (Figure 28)
blaCk
20.6%22.6%
40
30
20
10
0male female
25.7%
19.7%
white18-24
25.0%
25-34
26.9%
35-44
26.9%
45-54
27.0%
55-64
20.5%
65+
10.5%
• the prevalence of current smokers had decreased in the united States since 2002, while Alabama had been fluctuating until 2008, then increased slightly.
• Alabama’s rate of current smokers was higher than the national average rates from 1998-2009.• 22.5 percent of Alabama residents reported that they smoked in 2009. (Figure 27)
cigarette smoking is a major cause of heart disease and stroke. It increases the clotting factors in the blood, damages the linings of the blood vessels, and decreases HdL (the good cholesterol) in the blood. Smokers have twice the risk of heart attack or stroke of non-smokers. Smoking is the single largest preventable cause of heart disease in the united States.
CardioVasCUlar risk faCtors: smokinG
Pe
rC
en
t
fiGUre 27: PreValenCe of CUrrent smokers in alabama and United states, 1998-2009
24.6
23.5
25.2
23.824.4
25.4
24.8 24.8
23.222.522.5
22.1 22.522.9
22.623.2
22.8 23.0
22.0
21.220.5
20.0 19.719.7
18.317.9
26
24
22
20
18
16
Pe
rC
en
t
alabama United states
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009year
Source: Alabama brFSS
Source: Alabama brFSS
22.5%
oVerall
findinG the Path to CardioVasCUlar health 2010 • 23
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8area
7
area
3
area
4area
6
area
5
area
2area
1
27%22%
20%
20%22%
22%
21%
27%
21%
24%
24%
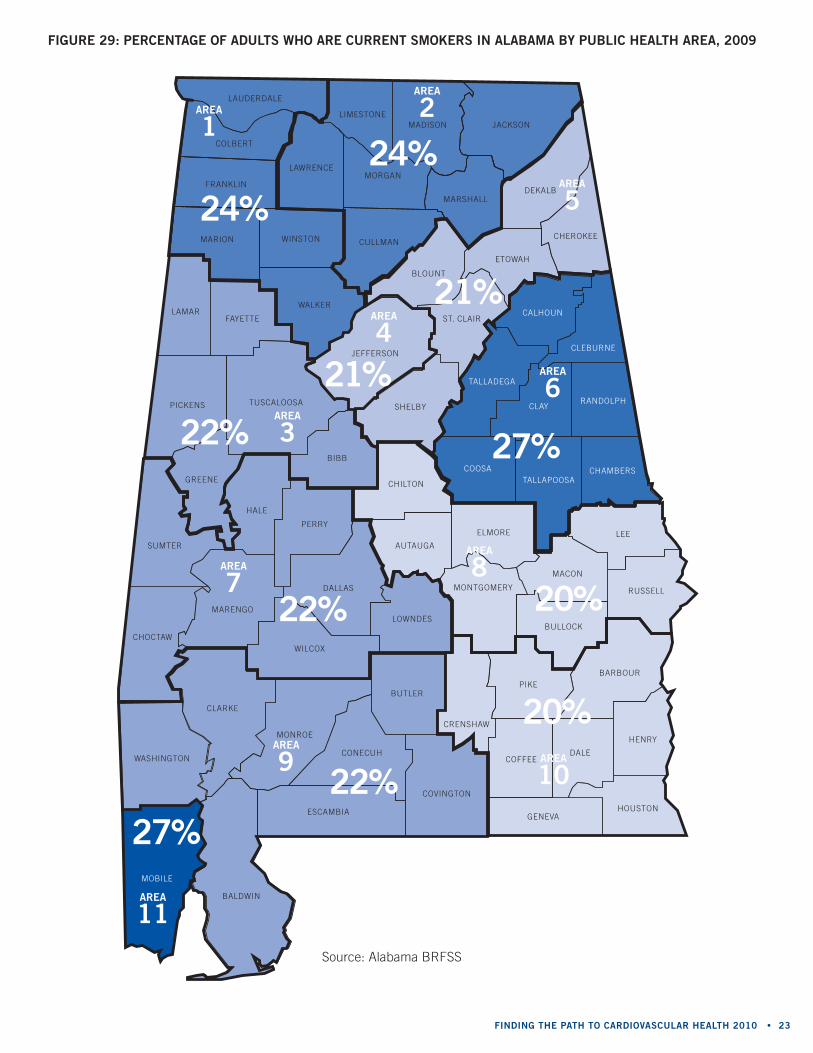
fiGUre 29: PerCentaGe of adUlts who are CUrrent smokers in alabama by PUbliC health area, 2009
Source: Alabama brFSS
24 • the risk of heart disease and stroke in alabama: bUrden doCUment
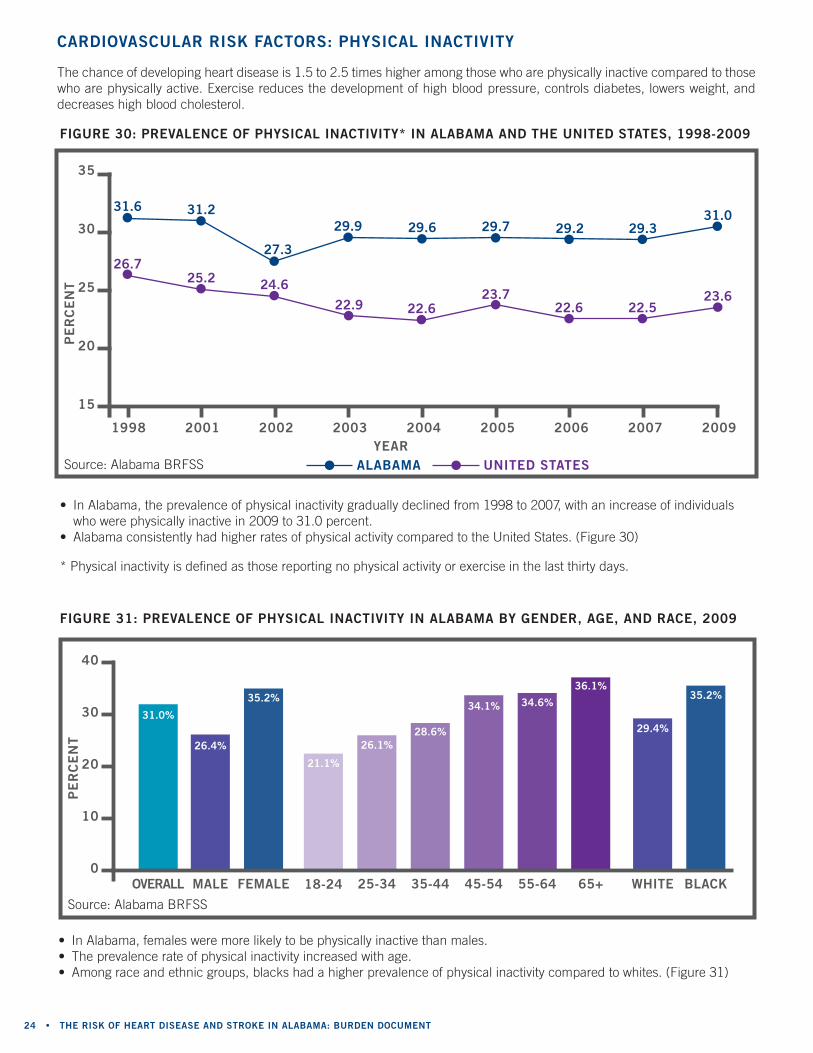
fiGUre 31: PreValenCe of PhysiCal inaCtiVity in alabama by Gender, aGe, and raCe, 2009
• In Alabama, females were more likely to be physically inactive than males.• the prevalence rate of physical inactivity increased with age.• Among race and ethnic groups, blacks had a higher prevalence of physical inactivity compared to whites. (Figure 31)
blaCk
35.2%
29.4%
40
30
20
10
0maleoVerall female
26.4%
31.0%
35.2%
white18-24
21.1%
25-34
26.1%
35-44
28.6%
45-54
34.1%
55-64
34.6%
65+
36.1%
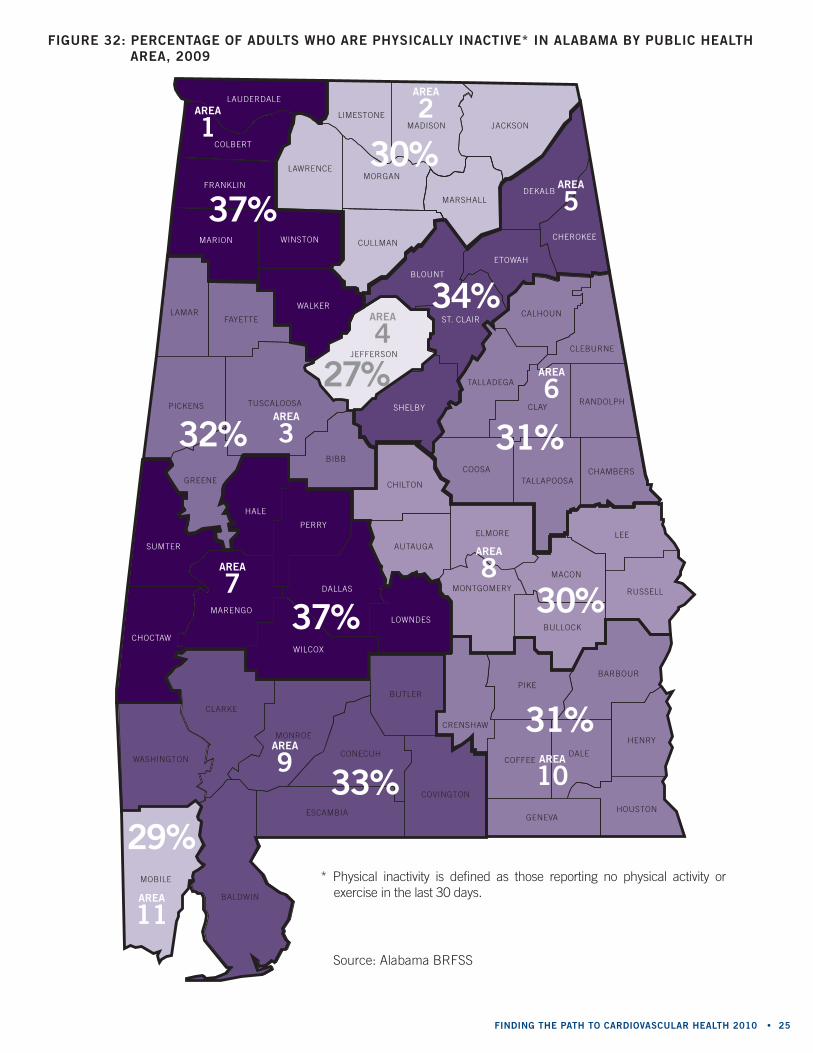
• In Alabama, the prevalence of physical inactivity gradually declined from 1998 to 2007, with an increase of individuals who were physically inactive in 2009 to 31.0 percent.
• Alabama consistently had higher rates of physical activity compared to the united States. (Figure 30)
* Physical inactivity is defined as those reporting no physical activity or exercise in the last thirty days.
fiGUre 30: PreValenCe of PhysiCal inaCtiVity* in alabama and the United states, 1998-2009
the chance of developing heart disease is 1.5 to 2.5 times higher among those who are physically inactive compared to those who are physically active. exercise reduces the development of high blood pressure, controls diabetes, lowers weight, and decreases high blood cholesterol.
CardioVasCUlar risk faCtors: PhysiCal inaCtiVity
Pe
rC
en
t
Source: Alabama brFSS
31.0
23.6
1998 2001 2002 2003 2004 2005 2006 2007 2009
35
30
25
20
15
31.6 31.2
27.3
29.9 29.6 29.7 29.2 29.3
26.725.2 24.6
22.9 22.623.7
22.6 22.5
year
Pe
rC
en
t
Source: Alabama brFSS alabama United states
findinG the Path to CardioVasCUlar health 2010 • 25
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8area
7
area
3
area
4area
6
area
5
area
2area
1
29%
33%
31%
30%37%
32%
27%
31%
34%
30%
37%
fiGUre 32: PerCentaGe of adUlts who are PhysiCally inaCtiVe* in alabama by PUbliC health area, 2009
Source: Alabama brFSS
* Physical inactivity is defined as those reporting no physical activity or exercise in the last 30 days.
26 • the risk of heart disease and stroke in alabama: bUrden doCUment
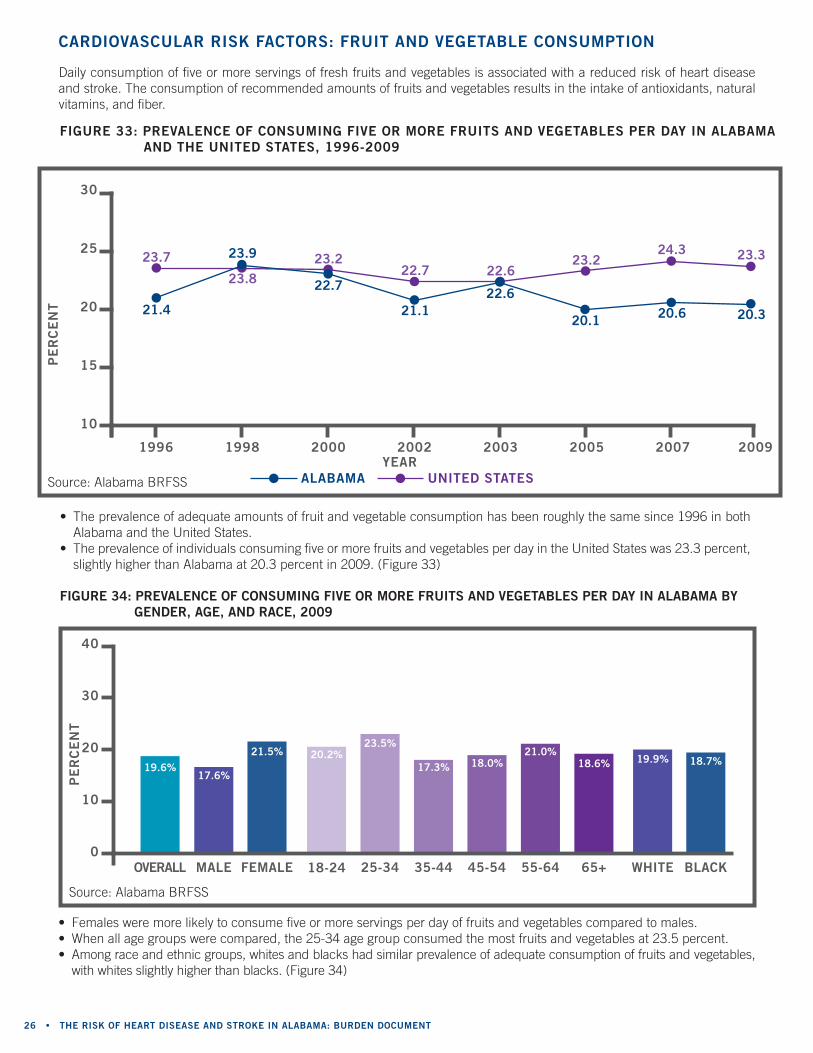
fiGUre 34: PreValenCe of ConsUminG fiVe or more frUits and VeGetables Per day in alabama by Gender, aGe, and raCe, 2009
• Females were more likely to consume five or more servings per day of fruits and vegetables compared to males.• When all age groups were compared, the 25-34 age group consumed the most fruits and vegetables at 23.5 percent.• Among race and ethnic groups, whites and blacks had similar prevalence of adequate consumption of fruits and vegetables,
with whites slightly higher than blacks. (Figure 34)
blaCk
18.7%19.9%
40
30
20
10
0maleoVerall female
17.6%19.6%
21.5%
white18-24
20.2%
25-34
23.5%
35-44
17.3%
45-54
18.0%
55-64
21.0%
65+
18.6%
daily consumption of five or more servings of fresh fruits and vegetables is associated with a reduced risk of heart disease and stroke. the consumption of recommended amounts of fruits and vegetables results in the intake of antioxidants, natural vitamins, and fiber.
CardioVasCUlar risk faCtors: frUit and VeGetable ConsUmPtion
• the prevalence of adequate amounts of fruit and vegetable consumption has been roughly the same since 1996 in both Alabama and the united States.
• the prevalence of individuals consuming five or more fruits and vegetables per day in the united States was 23.3 percent, slightly higher than Alabama at 20.3 percent in 2009. (Figure 33)
fiGUre 33: PreValenCe of ConsUminG fiVe or more frUits and VeGetables Per day in alabama and the United states, 1996-2009
alabama United states
1996 1998 2000 2002 2003 2005 2007 2009
30
25
20
15
10
21.4
23.9
22.7
21.122.6
20.1 20.6 20.3
23.7
23.823.2
22.7 22.623.2
24.3 23.3
year
Pe
rC
en
t
Pe
rC
en
t
Source: Alabama brFSS
Source: Alabama brFSS

findinG the Path to CardioVasCUlar health 2010 • 27
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEELEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
area
11
area
9 area
10
area
8area
7
area
3
area
4area
6
area
5
area
2area
1
17%
18%
15%
26%20%
16% 21%
17%
17%
23%
17%
fiGUre 35: PerCentaGe of adUlts ConsUminG fiVe serVinGs of frUit and VeGetables in alabama by PUbliC health area, 2009
Source: Alabama brFSS
28 • the risk of heart disease and stroke in alabama: bUrden doCUment
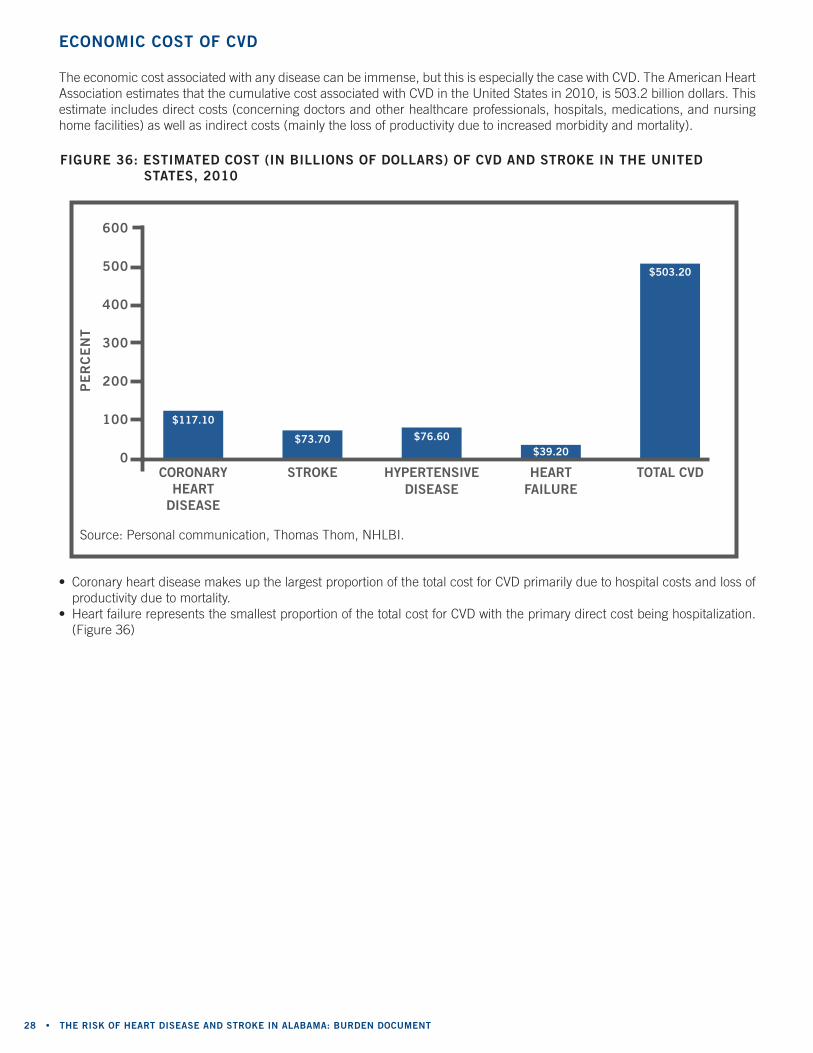
the economic cost associated with any disease can be immense, but this is especially the case with cVd. the American Heart Association estimates that the cumulative cost associated with cVd in the united States in 2010, is 503.2 billion dollars. this estimate includes direct costs (concerning doctors and other healthcare professionals, hospitals, medications, and nursing home facilities) as well as indirect costs (mainly the loss of productivity due to increased morbidity and mortality).
eConomiC Cost of CVd
fiGUre 36: estimated Cost (in billions of dollars) of CVd and stroke in the United states, 2010
• coronary heart disease makes up the largest proportion of the total cost for cVd primarily due to hospital costs and loss of productivity due to mortality.
• Heart failure represents the smallest proportion of the total cost for cVd with the primary direct cost being hospitalization. (Figure 36)
600
500
400
300
200
100
0Coronary
heart disease
$117.10
stroke
$73.70
hyPertensiVe disease
$76.60
heart failUre
$39.20
total CVd
$503.20
Pe
rC
en
t
Source: Personal communication, thomas thom, nHLbI.
findinG the Path to CardioVasCUlar health 2010 • 29
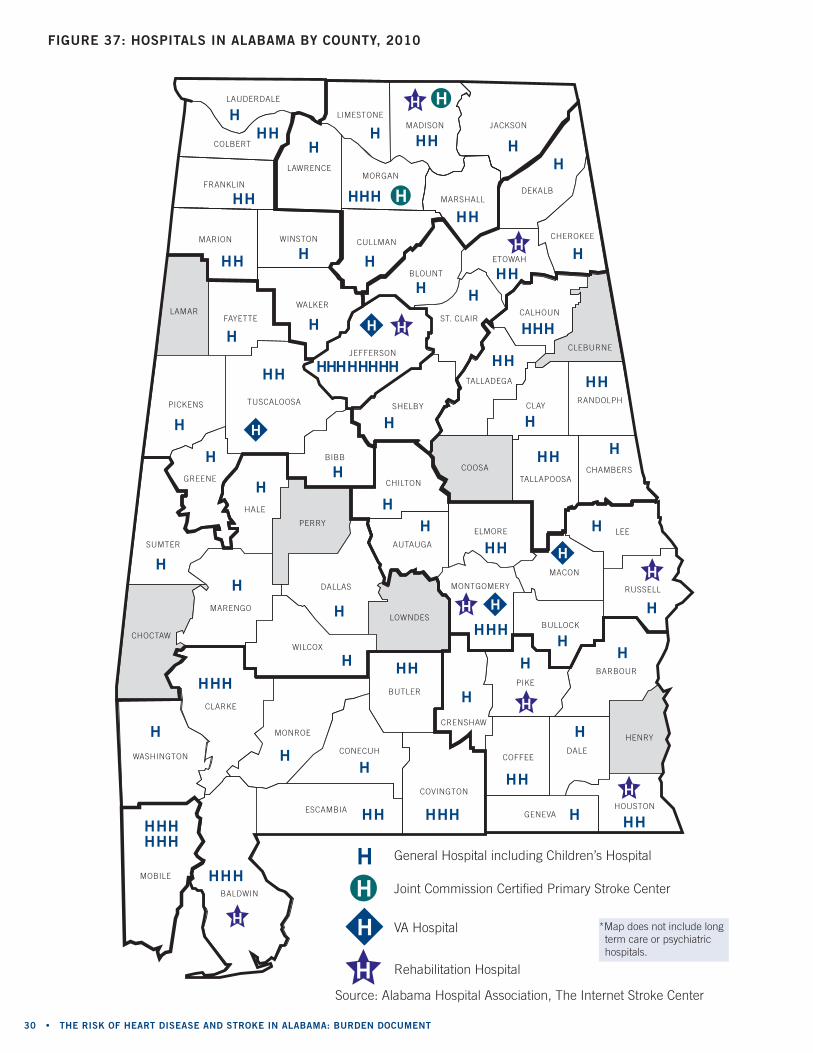
Access to all types of health care has been and continues to be a serious problem in Alabama. In situations where literally every second counts, such as during a heart attack or stroke, being able to receive prompt medical care is critical to the survival of the patient. this can be quite a daunting task in some areas of the state where the nearest hospital can be several hours drive. Hospitals in Alabama are categorized as follows: General hospitals (including the children’s Hospital), rehabilitation Long term care, Psychiatric, and the Veterans Administration (VA) hospitals. For the purpose of this report, General, rehabilitation, and VA hospitals will be highlighted.
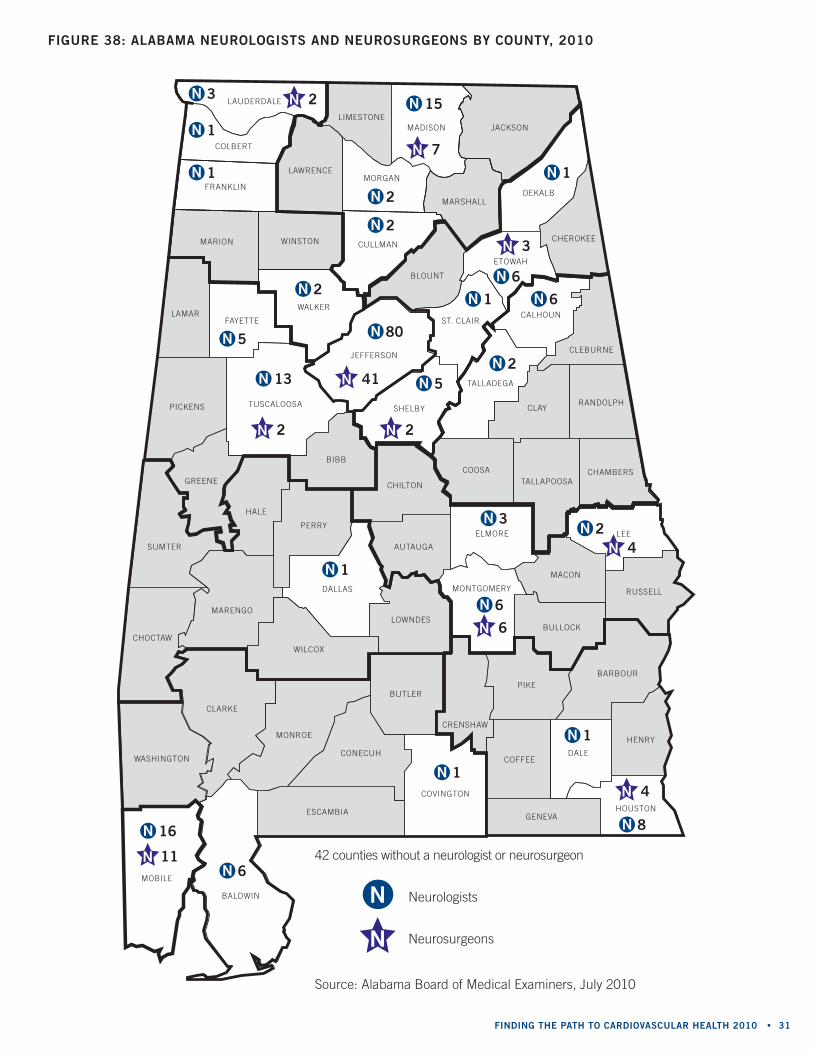
When preparing the state to care for patients having a stroke or rehabilitating from a stroke, access to a neurologist is a vital part of any plan of care. In the united States there are approximately 4.0 neurologists per 100,000 people caring for more than 700,000 acute strokes per year. In Alabama, there are 44 out of 67 counties without a neurologist. Some stroke victims have to travel across three counties to access a neurologist for care. Figure 37 and 38 shows obvious gaps in access to care involving hospitals and neurologists which also correlate to the stroke mortality rate maps included in this document.
once diagnosed with an ischemic stroke the neurosurgeon may be asked to evaluate the patient and determine whether they are a candidate for surgical intervention. the only university in Alabama training neurosurgeons and is limited to six per year is the university of Alabama at birmingham (uAb). this past year only one of six neurosurgeons stayed in Alabama to practice. Please refer to Figure 38 for a comparison of the availability of neurologists and neurosurgeons.
recovering from a stroke can be a long process, financially tasking, and overwhelming to a patient and their family. A rehabilitation hospital has a team of highly focused professionals that include physicians, nurses, occupational therapists, physical therapists, and speech therapists. these professionals will custom design programs specific to individual patient’s needs with therapy and treatment programs that have a goal to ultimately get the patient back to living life to the fullest. When needing the specialty care of a cardiovascular rehabilitation facility the urban areas have better access than rural. many counties in the rural southern portions of the state do not have a facility leaving those residents at risk of not receiving proper rehabilitation. Forty-three counties in the state do not have rehabilitation hospitals or centers of any kind for patients to access.
• In Alabama, hospitals tend to be concentrated in highly populated, urban regions of the counties. Several counties in the state do not have a hospital: cleburne, choctaw, coosa, Henry, Lamar, Lowndes, and Perry counties.
• only two hospitals in Alabama are Joint commission certified Primary Stroke centers: decatur General in morgan county, and Huntsville Hospital in madison county. (Figure 37)
aCCess to Care
30 • the risk of heart disease and stroke in alabama: bUrden doCUment
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
fiGUre 37: hosPitals in alabama by CoUnty, 2010
Source: Alabama Hospital Association, the Internet Stroke center
h General Hospital including children’s Hospital
Joint commission certified Primary Stroke center
VA Hospital
rehabilitation Hospital
h
h
h
h
h
h
h
h
h
h
h
h
h
h
h
h
h
h hh h hh h h
h
hhh
h
h
h
h
h
h
h
h
h
hh
h
h
h
h
h
hhhh
hh h
hh h
h
h
hh
hh
h
h
h
h
hh
h
h
h
hh
h
h
h
hh
h
hh
h
h
h
h
h
h
h
h
h h
h
h
h
h
h
h
h
h
h
h
h
h
h h
h
h
h
h
h
h
h
h
h
h h
*map does not include long term care or psychiatric hospitals.
findinG the Path to CardioVasCUlar health 2010 • 31
LAUDERDALE
LAWRENCE
LIMESTONE
MORGAN
CULLMAN
MARSHALLDEKALB
CHEROKEE
CALHOUN
CLEBURNE
RANDOLPHCLAY
TALLADEGA
COOSATALLAPOOSA
CHAMBERS
ETOWAH
BLOUNT
ST. CLAIR
SHELBY
JEFFERSON
LAMARFAYETTE
TUSCALOOSA
BIBB
GREENE
SUMTER
CHOCTAW
MARENGO
HALE
PERRY
DALLAS
WILCOX
LOWNDES
AUTAUGA
CHILTON
ELMORE
MONTGOMERY
MACON
BULLOCK
PIKE
CRENSHAW
BUTLER
CONECUH
MONROE
CLARKE
WASHINGTON
BALDWIN
COVINGTON
ESCAMBIA
MOBILE
COFFEEDALE
BARBOUR
HENRY
HOUSTONGENEVA
RUSSELL
LEE
PICKENS
JACKSONMADISON
COLBERT
FRANKLIN
MARION WINSTON
WALKER
fiGUre 38: alabama neUroloGists and neUrosUrGeons by CoUnty, 2010
Source: Alabama board of medical examiners, July 2010
42 counties without a neurologist or neurosurgeon
neurologists
neurosurgeonsn
n
n 3
n 3
n 2
n 2
n 2
n 2
n 5
n 5 n 80
n 2
n 1
n 1
n 1
n 6
n 6
n 6
n 6
n 1
n 1
n 1
n 1
n 8
n 15
n 13
n 2
n 2 n 2
n 4
n 4
n 3
n 41
n 7
n 6
n 16
n 11
32 • the risk of heart disease and stroke in alabama: bUrden doCUment
one of the Healthy People 2010 objectives is to increase the proportion of people who are aware of the early warning signs and symptoms of stroke. the time variance between the onset of symptoms and actually receiving treatment can adversely affect the outcome of an acute heart attack or stroke event. there are three stages at which time delays can occur: • the onset of symptoms and the 911 call for help; • during pre-hospital care; and • during transportation.
Stroke: The FAST test
the fast test is an easy way to recognize and remember the signs of stroke or a transient ischemic attack (tIA). using the fast test involves asking three simple questions.
fast stands for: F = Facial weakness - can the person smile; has his or her mouth or eyes drooped? A = Arm weakness - can the person raise both arms; is one arm slightly lower? S = Speech/sight difficulty - can the person speak or see clearly and understand what you say? T = time to act - time loss is brain lost. call 911.
If you suddenly experience any of these symptoms, go to a hospital immediately. remember, stroke is a life-threatening emergency.
Heart Attack: Signs and Symptoms: • Pain or discomfort in jaw, neck, or back • Feeling weak, lightheaded, faint • chest pain or discomfort • Shortness of breath • Pain or discomfort in arms or shoulders
A risk factor that can cause heart attack and stroke is high blood pressure or hypertension. the national guidelines for defining hypertension are the following:
siGns and symPtoms of a heart attaCk or stroke
ClassifiCation of blood PressUre (bP)
cAteGorySbP mm Hg
SystolicdbP mm Hg
diastolic
normal <120 and <80
Pre-hypertension 120-139 or 80-89
Hypertension, Stage 1 140-159 or 90-99
Hypertension, Stage 2 >160 or >100
Seventh report of the Joint national committee on Prevention, detection, evaluation, and treatment of High blood Pressure (Jnc7) Guidelines.
Help For Smoking ceSSATionAnother risk factor that can lead to heart attack and stroke is smoking. Imagine yourself tobacco free! call the AdPH tobacco Quitline at 1-800-QuIt-noW, or go online at www.alabamaquitnow.org.

findinG the Path to CardioVasCUlar health 2010 • 33
Americans consume too much sodium. High sodium consumption raises blood pressure, and high blood pressure is a major risk factor for heart disease and stroke. Heart disease and stroke are the nation’s first and third leading causes of death.
salt and high blood pressure• research strongly shows a dose-dependent relationship between consuming too much salt and
raised levels of blood pressure. • When salt intake is reduced, blood pressure begins decreasing within weeks on average.• Populations who consume diets low in salt do not experience the increase in blood pressure with age
that is seen in most Western countries.
is it salt or is it sodium?• Sodium chloride is the chemical name for salt.• the words salt and sodium are not exactly the same, yet these words are often used in place of each
other. For example, the nutrition Facts Panel uses “sodium,” whereas the front of the package may say “low salt.”
• ninety percent of the sodium we consume is in the form of salt.
sodium consumption and sodium in our food supply• We all need a small amount of sodium to keep our bodies working properly. • the 2005 dietary Guidelines for Americans recommend limiting sodium to less than 2,300 milligrams
(mg) per day (about one teaspoon of table salt). Individuals with hypertension, blacks, and middle-aged and older adults should limit intake to 1,500 mg of sodium per day. these specific populations account for about 70 percent of adults.
• the average daily sodium intake for Americans age two years and older is more than 3,400 mg. • the majority of the sodium consumed is from processed and restaurant foods; only a small portion is
used in cooking or added at the table. • nutrition labeling and package messaging are easily misunderstood by consumers. • Sodium information is not readily available for restaurant foods and can be hard for the consumer
to estimate. For example, consumers might be surprised to find that the restaurant salad they are consuming may contain more than 900 mg of sodium—and could only find this information on the company’s website.
reducing sodium, reducing CVd burden • In general, even if a person does not have high blood pressure, the lower one’s blood pressure, the
lower the risk of heart disease and stroke. • Sodium intake from processed and restaurant foods contributes to high rates of high blood pressure,
heart attack, and stroke. because nearly 400,000 deaths each year are attributed to high blood pressure, decreasing sodium intake could prevent thousands of deaths annually.
the abCs of heart disease and stroke
heart disease and stroke are Preventable!A = Aspirin use. Ask your provider about taking:
• one baby aspirin (81 mg) every day, or • one regular aspirin (325 mg) every other day.
B = blood pressure treatment and control. bP <120/80• consume only 2300 mg sodium daily.
c = cholesterol. Ask your provider about how often to check your cholesterol.• total cholesterol < 200• LdL (bad cholesterol) < 100
S = Smoking cessation. research shows using a quitline with medication increases abstinence rates.• call 1-800-QuItnoW for more details or ask your provider.
sodiUm: the faCts
Source: cdc Salt

34 • the risk of heart disease and stroke in alabama: bUrden doCUment
Alabama department of Public Health ......................donald e. Williamson, m.d., State Health officerAlabama department of Public Health ......................thomas m. miller, m.d., m.P.H., Assistant State Health officerbureau of Health Promotion and chronic disease .....Jim mcVay, dr.P.A., bureau directorchronic disease Prevention office ............................bob Hinds, directorchronic disease epidemiology branch ......................Sondra reese, m.P.H., directorbrFSS unit .............................................................Jesse Pevear, III, m.S.P.H., coordinatorcardiovascular Health branch ..................................melanie rightmyer, r.n., m.S.n., Program manager
aCknowledGements
American Heart Association. Heart disease and Stroke Statistics – 2008 update. retrieved from: http://www.americanheart.org
centers for disease control and Prevention (cdc). behavioral risk Factor Surveillance System (brFSS): overview and a brief History. retrieved from: http://www.cdc.gov/brfss/about.htm centers for disease control and Prevention (cdc). behavioral risk Factor Surveillance System (brFSS). retrieved from: http://www.cdc.gov/brfss centers for disease control and Prevention. cdc Wonder. retrieved from: http://wonder.cdc.gov
united States census bureau. American Fact Finder. (2007). retrieved from: http://www.census.gov
Alabama board of medical examiners. (2010). Systems network.
referenCes
this publication was supported by Grant/cooperative Agreement number 5u50dP000732-04 from the cdc. Its contents are solely the responsibility of its authors and do not necessarily represent the official views of the cdc.
Top Related