







Languages
Pages
Legal


==
Fatigue in patients with Chronic
Obstructive Pulmonary Disease
Marileen Kouijzer
Master’s thesis
September 15, 2017
Marileen Kouijzer (S1454196)
Master: Health Psychology & Technology
Internal organization: University of Twente
External organization: Medical Spectrum Twente
Internal supervisors: 1st. Dr. Christina Bode
2nd
. Dr. Stans Drossaert
External supervisor: Dr. Marjolein Brusse-Keizer
Faculty of Behavioural, Management and Social sciences
A qualitative study on the perspective of the COPD
patient on the impact of fatigue on their daily life

Abstract
Background. Fatigue in patients with Chronic Obstructive Pulmonary Disease (COPD) is a problematic
symptom. Patients experience fatigue as a key factor that negatively influences their daily lives.
Currently, no effective treatment options are available for patients with COPD to tackle the burden of
fatigue. The aim of this study is to explore the impact of fatigue from a patients‟ perspective and address
treatment preferences, emphasizing the use of self-management and eHealth.
Methods. Semi-structured interviews were conducted with twenty COPD patients, varying in terms of
age, gender, and GOLD stage. The interview consisted of eighteen open-ended questions with sub
questions about the definitions of fatigue, vitality and sleepiness, fatigue as a symptom, and its impact
on the daily lives of patients. Furthermore, questions about treatment and communication preferences
were asked, including self-management and eHealth possibilities. The interviews lasted up to 70
minutes, were audio-recorded, transcribed verbatim and analysed by one coder using an iterative
process, which combined deductive and inductive coding.
Results. In this study, patients perceived severe impact of fatigue on their physical, psychological and
social functioning. They experienced severe limitations in their daily lives. These limitations caused a
high mental burden and make fatigue a challenging symptom to cope with. COPD patients mentioned
the need for effective treatment. Emphasizing the importance of increasing physical function, motivation
and social support. The opinion of patients on the use of self-management and eHealth to ease the
burden of fatigue differed among individuals. Multiple advantages and disadvantages were mentioned.
Overall, patients emphasized tailored treatment and blended care as effective options to tackle the
burden of fatigue.
Conclusion. These findings indicate that the COPD patients in this study found the impact of fatigue on
their daily functioning to be a key factor in decreasing their quality of life. This study gives insight in the
limitations they experience due to fatigue and the way they cope with this burden. Awareness needs to
be created in both healthcare professionals and patients about the impact of fatigue, and it being a
frequent symptom of COPD. In addition, a pro-active, multidisciplinary approach is needed to develop
tailored treatment which focuses on prevention of fatigue, rather than treating the severe burden of
fatigue when the disease progresses.
Keywords. COPD-related fatigue; Impact fatigue; Patients’ perspective; eHealth; self-management;
Chronic Obstructive Pulmonary Disease; multidisciplinary approach

1
Samenvatting
Achtergrond. Vermoeidheid bij patiënten met Chronic Obstructive Pulmonary Disease is een
problematisch symptoom. Patiënten ervaren vermoeidheid als een belangrijke factor die een negatieve
invloed heeft op hun dagelijks leven. Momenteel zijn er geen effectieve behandelmethoden beschikbaar
voor patiënten met COPD om de last die vermoeidheid met zich meebrengt aan te pakken. Het doel van
dit onderzoek is om de impact van vermoeidheid in kaart te brengen vanuit het perspectief van de
patiënt. Daarnaast wordt onderzocht wat de behandelvoorkeuren van de patiënt zijn, gefocust op het
gebruik van zelfmanagement en eHealth om vermoeidheid aan te pakken.
Methode. Semi-gestructureerde interviews zijn afgenomen bij twintig COPD patiënten, die varieerden in
leeftijd, geslacht en GOLD stadium. Het interview bestond uit achttien open vragen met sub vragen over
de definitie van vermoeidheid, vitaliteit en slaperigheid, vermoeidheid als een symptoom van COPD en
de impact die het heeft op het dagelijks leven van de patiënt. Daarnaast zijn er vragen gesteld over
behandeling en communicatie voorkeuren, inclusief zelfmanagement en eHealth mogelijkheden. De
interviews duurden maximaal 70 minuten, zijn opgenomen met audioapparatuur, verbatim
getranscribeerd en geanalyseerd door één onderzoeker in een iteratief proces. Inductieve codering werd
gecombineerd met deductieve codering.
Resultaten. Patiënten gaven in dit onderzoek aan dat vermoeidheid impact heeft op hun fysiek,
psychologisch en sociaal funcioneren. Ze voelen zich hierdoor beperkt in hun dagelijks leven. Deze
beperkingen zorgen voor een grote mentale last en dat maakt dat vermoeidheid een moeilijke klacht is
om mee om te gaan. COPD patiënten benoemen de behoefte aan een effectieve behandeling. Het
verbeteren van de fysieke conditie, motivatie en sociale ondersteuning werd benadrukt. De mening van
de patiënten over het gebruik van zelfmanagement en eHealth in een behandeling tegen vermoeidheid
verschilt. Meerdere voor- en nadelen werden benoemd. Over het algemeen benadrukken patiënten een
gepersonaliseerde behandeling en blended care als effectieve mogelijkheiden om vermoeidheid te
kunnen verminderen.
Conclusie. Deze resultaten geven aan dat de COPD patiënten uit dit onderzoek de impact van
vermoeidheid op hun dagelijks functioneren zien als een belangrijke factor die de kwaliteit van leven
aanzienlijk verminderd. Dit onderzoek biedt belangrijke informatie over de beperkingen die patiënten
ervaren in hun leven en de manier waarop ze daarmee omgaan. Bewustwording moet gecreëerd worden
in zorgprofessionals, maar ook in patiënten, over de impact die vermoeidheid kan hebben en het feit dat
vermoeidheid een frequent symptoom van COPD is. Bovendien, is er een pro-actieve, multidisciplinaire
aanpak nodig om gepersonaliseerde behandelopties te ontwikkelen die focussen op de preventie van
vermoeidheid, in plaats van het behandelen van vermoeidheid in een verder gevorderd stadium.
Trefwoorden. Vermoeidheid bij COPD; Impact vermoeidheid; Patiëntperspectief; eHealth;
zelfmanagement; Chronic Obstructive Pulmonary Disease; multidisciplinaire aanpak

2
Content
Introduction ........................................................................................................................................... 3
Chronic Obstructive Pulmonary Disease ............................................................................................. 3
Fatigue in Chronic Obstructive Pulmonary Disease ............................................................................ 5
Patient perspective on COPD-related fatigue ...................................................................................... 6
Self-management to address decreased vitality and fatigue ................................................................. 7
eHealth to address decreased vitality and fatigue ................................................................................ 8
Current study ...................................................................................................................................... 9
Methods ................................................................................................................................................. 9
Participants....................................................................................................................................... 10
Materials .......................................................................................................................................... 11
Procedure ......................................................................................................................................... 11
Analysis ........................................................................................................................................... 12
Results ................................................................................................................................................. 13
1. Definitions and differences between fatigue, decreased vitality and sleepiness.............................. 13
2. The start, causes and fluctuations of fatigue .................................................................................. 15
3. Impact of fatigue on the life of COPD patients.............................................................................. 18
4. Treatment options to tackle the burden of fatigue and improve vitality ......................................... 24
Discussion ........................................................................................................................................... 33
References ........................................................................................................................................... 39
Appendix ............................................................................................................................................. 44
Appendix A. Informatiebrief onderzoek „Van vermoeid naar vitaal!‟ ................................................ 44
Appendix B. Informed consent ......................................................................................................... 47
Appendix C. Medisch Ethische Toetsingscommissie (METC) .......................................................... 48
Appendix D. Interview schedule ....................................................................................................... 49
Appendix E. Codescheme ................................................................................................................. 53
3
Introduction
Fatigue in Chronic Disease
A chronic disease can have a major impact on the physical and psychological health of patients. Chronic
disease is defined as an inherently aversive, long-term condition with a relatively high degree of
uncontrollability and unpredictability (Evers, Kraaimaat, Van Lankveld, Jongen, Jacobs & Bijlsma,
2001). In 2014, 8.2 million inhabitants of the Netherlands had one or more chronic diseases. (RIVM,
2014). Living with a chronic disease has a major impact on the quality of life of patients and this
deteriorates with disease severity and age (Ståhl et al., 2005; Peruzza et al., 2003).
In addition to decreased quality of life, one of the most common complaints among patients with
a chronic disease is fatigue (Swain, 2000). Due to its subjective nature and differences in interpretation
and assessment, fatigue is difficult to define and to characterize (Lewko, Bidgood, Jewell & Garrod,
2012). It has been medically defined as „the state, following a period of mental or bodily activity,
characterized by a lessened capacity of work and reduced efficiency of accomplishment, usually
accompanied by a feeling of weariness, sleepiness or irritability‟ (Hensyl, 1989). It consists of complex
interactions between behavioural, psychosocial and biological processes (Swain, 2000). Patients with a
chronic disease rate fatigue often as one of the key factors leading to a decrease in quality of life (Swain,
2000). In addition, the lack of specific, evidence-based treatment options makes it a symptom that is
often ignored or overlooked by healthcare professionals (Swain, 2000; Spruit, Vercoulen, Sprangers &
Wouters, 2017).
Chronic Obstructive Pulmonary Disease
Fatigue is often described by patients as a lack of energy, as is the term subjective vitality. These terms
are in some cases difficult to distinguish, because of the overlapping vocabulary used in defining them.
In the current study, the term fatigue is used to describe the Chronic Obstructive Pulmonary Disease-
related fatigue (COPD-RF). The term subjective vitality is used to describe a positive feeling of
aliveness and of possessing personal energy (Ryan & Frederick, 1997). The patients‟ perspective on
these terms can provide input for adequate healthcare and may guide treatment priorities (Van Manen et
al., 2003).
Patients with COPD also suffer from fatigue. (Baltzan et al., 2011). According to the World
Health Organization (2016), COPD is a progressive lung disease characterized by chronic obstruction of
lung airflow that interferes with normal breathing and is not fully reversible. Physical symptoms of

4
COPD mainly consist of coughing, sputum production and dyspnoea (World Health Organization,
2016). The World Health Organization (2016) predicts that in 2020, COPD is the third cause of death
and rank fifth as a worldwide burden of disease (Pauwels, Buist, Calverley, Jenkins & Hurd, 2012). The
primary cause of COPD is tobacco smoke and the prevalence of COPD in smokers is 10-15% (Geijer et
al., 2005). The prevalence of COPD is increasing worldwide (Waatevik et al., 2013). According to the
RIVM (2016), in the Netherlands, about 607.300 people have COPD.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has constructed guidelines
for the assessment and management of patients with COPD. The most important practical aspect of these
guidelines was that COPD is classified by severity into four stages, which constitute the basis of
treatment recommendations. (Köhler, Fischer, Raschke & Schönhofer, 2003). However, recent
developments show that the airway obstruction is no longer the only central aspect in the standard of
care of COPD. This chronic disease is complex and heterogeneous, and the airflow limitation is poorly
related to many other clinically relevant aspects of COPD (Agusti et al., 2013). Therefore, new
guidelines were developed. The new guidelines consider the symptoms, the symptom burden, the
exacerbation risk, and the possible comorbidities. The refined assessment process according to these
new guidelines is shown in figure 1 (GOLD, 2017).
Figure 1. New GOLD ABCD Assessment Tool (GOLD, 2017)

5
Fatigue in Chronic Obstructive Pulmonary Disease
In the current study, the term fatigue is used to describe the Chronic Obstructive Pulmonary Disease-
related fatigue (COPD-RF). This fatigue is an increasing problem for COPD patients and this becomes
clear in a study of Tselebis et al. (2011). Fatigue was present in their whole research population,
consisting of 139 COPD outpatients from one of the largest respiratory diseases hospitals in Greece. In
addition, a study of Theander and Unosson (2004) showed that half of their research population,
consisting of COPD patients, reported fatigue every day during the preceding month, compared to
13.5% in the control group without COPD. Furthermore, 52.7% of the COPD patients reported that the
duration of fatigue was more than six hours a day and 44.4% reported that fatigue was the worst
symptom they had. At last, patients reported significantly greater impact of fatigue on physical,
cognitive and psychosocial functioning compared to the control group. The control group consisted of
individuals without COPD and with the same age and gender as the patients (Theander & Unosson,
2004).
Fatigue in COPD patients remains poorly understood as a distinct symptom, separate from other
psychological and physiological symptoms, which are frequently associated with COPD. These
psychological symptoms can be depression, anxiety, and emotional stress. Physiological symptoms can
be an increase in severity of pulmonary impairment and reduction in exercise tolerance (Breslin et al.,
1998). Fatigue may be sought in a combination of all these factors, reflecting the multidimensional
nature of the symptom (Spruit, Vercoulen, Sprangers & Wouters, 2017). Additionally, COPD is
associated with important chronic comorbid diseases, such as cardiovascular disease, diabetes and
hypertension, which could also contribute to fatigue (Mannino, Thorn, Swensen & Holguin, 2008).
The current study focuses on COPD-related fatigue. However, fatigue is often difficult to
distinguish from decreased subjective vitality. Patients who experience fatigue, also often suffer from
decreased vitality due to COPD. Decreased vitality in COPD patients, also described as a lack of energy
(Breslin et al., 1998), can have multiple causes. In COPD, respiratory symptoms, like dyspnoea, are
associated with an increase in energy consumption and exercise limitations (Aliverti & Macklem, 2008).
This results in peripheral muscle weakness which also contributes to a decrease in subjective vitality
(Breslin et al., 1998; Spruit, Gosselink, Troosters, De Paepe & Decramer, 2002). Furthermore, the
exacerbations most COPD patients experience have significant negative effect on subjective vitality
(Esteban, 2009). According to Wedzicha and Seemungal (2007), COPD exacerbations are triggered
mainly by respiratory bacteria and viruses. In addition, it can also be triggered by cold weather or over-

6
activity in COPD patients (Watz, Waschki, Meyer & Magnussen, 2009; Donaldson & Wedzicha, 2014).
In the current study, it is important to clearly describe the difference between fatigue and vitality to
develop effective treatment options to tackle the burden of fatigue. It is beneficial to research the
perspective of the patient on the definitions of fatigue and vitality based on their own experiences.
Patient perspective on COPD-related fatigue
In contrast to the poorly understood symptom that COPD-related fatigue is (Swain, 2000), the
percentages of patients who report this symptom are significant. However, there are still no evidence-
based treatment options for COPD patients to cope with this burden. To decrease fatigue in COPD
patients, treatment should not only be directed towards pulmonary function (Van Manen et al., 2003).
Rather, treatment should be focussed on addressing all of the patients‟ symptoms, including
psychological aspects (Van Manen et al., 2003; Theander & Unossen, 2011). The patients‟ perspective
on this burden can be of great value in developing effective treatment. The importance of healthcare
professionals listening to the perspective of the patient is often overlooked. According to Jagosh,
Boudreau, Steinert, MacDoland & Ingram (2011), patients explained that listening is an essential
component of clinical data gathering and diagnosis. However, listening to the patients‟ perspective can
also function as a healing and therapeutic agent. Lastly, focusing on the patients‟ perspective can
strengthen the patient-provider relationship. To communicate fatigue with the patient, knowledge should
be increased on the impact of fatigue on the daily life of the patient, on their social life, and on their
treatment preferences. Who better than the patients themselves to describe these aspects?
COPD-related fatigue has increasingly been recognised as an important area of research (Lewko,
Bidgood, Jewell and Garrod, 2012). A study from Kappella et al. (2006) reported that 70% of the COPD
patients that took part in their research stated that “current fatigue is different in quality and intensity
than the fatigue they experienced before developing this condition”. The impact of fatigue is clear in a
study from Ream and Richardson (1997), whereby COPD patients described fatigue as a feeling of
„exhaustion‟, which decreases their concentration and motivation to “get up and go”. The same study
stated that fatigue increases the feeling of depression, low self-esteem and constant low mood. Fatigue is
a multi-component symptom that reflects aspects of motivation, mood states, cognitions and physical
ability (Lewko, Bidgood, Jewell & Garred, 2012). To conclude, it is clear that fatigue has a negative
impact on patient outcomes. However, it remains unclear how fatigue exactly affects the daily life of
COPD patients and what physical, social, and emotional challenges this entails. In addition, treatment

7
preferences of patients should be explored to create input for effective treatments. Current research on
the patients‟ perspective is needed to explore this impact, and how it can be decreased to improve
quality of life and subjective vitality.
Self-management to address decreased vitality and fatigue
It is important to offer the best possible treatment available to COPD patients who suffer from fatigue
(Lorig, Sobel, Ritter, Laurent & Hobbs, 2000; Effing et al., 2007). The problem is that there are no
evidence-based treatments for treating fatigue of COPD patients. Furthermore, healthcare professionals
do not always know how to cope with fatigue as a symptom, how to communicate it with the patient and
what treatment should be offered (Swain, 2000). Self-management is of increasing importance in COPD
management. According to Effing et al. (2016), the definition of a COPD self-management intervention
is; “A COPD self-management intervention is structured but personalised and often multi-component,
with goals of motivating, engaging, and supporting the patients to positively adapt their health
behaviour(s) and develop skills to better manage their disease. The goals of self-management in COPD
are optimising and preserving physical health, reducing symptoms and functional impairments in daily
life and increasing emotional well-being, social well-being and quality of life. The process of self-
management requires iterative interactions between patients and healthcare professionals. These patient-
centered interactions focus on identifying needs, health beliefs and enhancing intrinsic motivations. Also
eliciting personalised goals, formulating appropriate strategies to achieve these goals, and evaluating and
re-adjusting strategies.” This definition is based on an international expert group consensus. An
increasing number of healthcare professionals agree that patients with COPD should receive support to
help them cope with their disease (Bourbeau & Van der Palen, 2009).
Additionally, self-management interventions exert positive effects in COPD patients on
respiratory-related and all-cause hospitalization. Modest improvements in health-related quality of life
are also stated in research of Jonkman et al. (2016). However, fatigue is not frequently integrated within
self-management interventions, because the current focus lies on exacerbations and dyspnoea as a
primary activity-limiting symptom (Effing et al., 2016; Breslin, 1998). Given the high levels of fatigue
in COPD patients and its relation to functional patient outcomes, the self-management of fatigue
requires serious consideration (Breslin, 1998). Patients have extensive experience in managing the
disease and possibly are able to verbalize the coping strategies (Fraser, Kee & Minick, 2006).
Incorporating these aspects in treatment can motivate patients to cope with their illness and change their

8
health behaviour. The study of Effing et al. (2016), states that the patients‟ perspective may not fit into
the professionals‟ perspective and may change during the different stages of COPD, and between
individual patients. This should be taken into account when developing self-management interventions.
In conclusion, self-management interventions could be of great value to patients with COPD to improve
their health-related quality of life (Zwerink et al., 2014). However, it is not clear which specific
components could be of value for different types of COPD patients (Bourbeau & Van der Palen, 2009)
and in which way fatigue should be addressed by self-management. Therefore, more insight into the
patients‟ perspective is needed on their treatment preferences and on which self-management
components could be most effective in tackling the burden of fatigue and increasing subjective vitality.
eHealth to address decreased vitality and fatigue
A possibility to address fatigue in self-management treatment is eHealth. It can be of great value to
patients to manage their symptoms. The definition of eHealth given by Eysenbach (2001) states:
“eHealth is an emerging field in the intersection of medical informatics, public health and business,
referring to health services and information delivered or enhanced through the Internet and related
technologies.” Additionally, eHealth is a dynamic environment and constantly moving. It should be
defined by how it is used (Eysenbach, 2001). An example of an existing eHealth programme for self-
management of COPD exacerbations and an active lifestyle is called the Condition Coach (CoCo). This
telehealth programme consists of a web-based exercise programme, an activity coach and a
teleconsultation module for asking questions to the patient‟s primary care physiotherapist, via a web
portal. The last component is a module for the self-treatment of COPD exacerbations. Patients have to
fill in an online diary, and then a decision-support system automatically forms an advice. For example,
in case of worsening of the condition of the patient, the advice can be to start medication (Tabak et al.,
2013). Before starting with Condition Coach, all patients had to participate in a training on how to use
CoCo. Although this programme does focus on COPD patients, it is not addressing fatigue as a distinct
symptom.
eHealth has the potential to improve health and deliver value in disease management, telehealth,
patient safety, and decision support (Silber, 2003). Other advantages focus on blended care, as eHealth
could provide an addition to face-to-face consultations and creating favourable circumstances for
strengthening patient participation (Townsend, Adam, McDonald & Backman, 2013). There are also
disadvantages of using eHealth. It may disturb the patient-provider relationship and it demands more
9
frequent and intense participation of the patient (Townsend, Adam, McDonald & Backman, 2013),
which can form a problem with patients that suffer from extreme fatigue. Additionally, all patients need
to have access to internet, via a computer, tablet or smartphone.
Self-management applications using eHealth to monitor chronic conditions have shown a
positive clinical effect in systematic reviews on patient management (Townsend, Adam, McDonald &
Backman, 2013). According to research from Thorndike et al. (2013), internet interventions can reduce
fatigue symptoms in patients with insomnia. According to Seiler, Klaas, Tröster and Fagundes (2017),
fatigue can also decrease as a consequence of eHealth interventions in cancer patients. However, there is
no record yet of decreasing fatigue as a consequence of eHealth interventions in COPD patients. In the
current study, COPD patients are invited to share their ideas on effective components in eHealth and
self-management interventions that can decrease the burden of fatigue and increase subjective vitality.
Current study
The current study investigates the patients‟ perspective on fatigue and subjective vitality and its impact
on daily life of COPD patients. Moreover, patients‟ treatment preferences to tackle the burden of fatigue
are researched. The following research questions are answered in this study:
1. What is the patients’ perspective on the definitions and differences between fatigue, decreased
vitality and sleepiness?
2. What is the patients’ perspective on the start, causes and fluctuations of fatigue?
3. How is the impact of fatigue on the life of COPD patients described from the patients’
perspective?
4. What is the patients’ perspective on the effectiveness of treatment options to tackle the burden of
fatigue and improve vitality, emphasizing eHealth and self-management interventions?
Methods
To answer these research questions, a qualitative study among COPD patients, both inpatients and
outpatients, using semi-structured interviews was conducted. The Medical Ethical Review committee of
Medical Spectrum Twente decided that the current study was not complying with the Dutch law on
Medical Research on Human subjects (Appendix C - File reference number: K16-58). Meaning that
there were no medical or ethical objections to perform this research.

10
Participants
The recruitment of patients was carried out by purposive sampling, to identify and select the most
information-rich cases. Patients were selected based on shared characteristics, which formed the
inclusion criteria. These criteria were: (1) COPD patients who were under supervision of a respiratory
physician at Medical Spectrum Twente (2) and suffered from fatigue. Furthermore, (3) inpatients were
admitted to the hospital for a severe COPD exacerbation. The exclusion criteria were (1) a diagnosis of
lung cancer, (2) sleep apnoea and (3) cognitive impairments. Since, lung cancer and sleep apnoea can
trigger fatigue. However, this fatigue is difficult to distinguish from COPD-related fatigue. Therefore,
these patients were not suitable for this study. Patients with cognitive impairments were excluded
because participants needed to be capable to understand and answer all interview questions. The
pulmonary research department selected outpatients and a physician assistant selected inpatients. A total
of 23 patients were approached to take part in the interview study, 20 patients agreed to participate
(Table 1). Reasons for non-participation were; no present fatigue symptoms or being too sick to
participate in an interview. The group consisted of 8 men and 12 women, with an average age of 67.7
years (SD 7.6). The participants had no personal relationship with the interviewer. Only the name, the
education, and the position of the interviewer within the organization were known to the patients.
Table 1
Patient characteristics
Respondent
number Gender Age In-/Outpatient GOLD stage Comorbidities
1 Male 57 Outpatient GOLD 4 Tinnitus
2 Female 52 Outpatient GOLD 4 Dystrophy
3 Female 59 Outpatient GOLD 4 Sjorgen’s
syndrome
4 Female 62 Outpatient GOLD 3 Osteoporosis,
Arthritis,
Fibromyalgia
5 Male 65 Outpatient GOLD 2 Cardiac
arrhythmia
6 Male 65 Outpatient GOLD 3
7 Male 64 Outpatient GOLD 3 Chronic back pain
8 Male 74 Outpatient GOLD 3 Balance disorder,
Cardiac arrhythmia
9 Male 71 Outpatient GOLD 3 Irritable Bowel
Syndrome

11
10 Female 64 Outpatient GOLD 3
11 Female 65 Inpatient GOLD 3 Diabetes
12 Male 72 Inpatient GOLD 2 Cardiac
arrhythmia
13 Female 85 Inpatient GOLD 3
14 Female 64 Inpatient GOLD 2
15 Female 72 Inpatient GOLD 2 Diabetes, Cardiac
arrhythmia
16 Male 67 Inpatient GOLD 3
17 Female 77 Inpatient GOLD 3 Rheumatoid arthritis
18 Female 71 Inpatient GOLD 3
19 Female 67 Inpatient GOLD 3
20 Female 80 Inpatient GOLD 2 Arthritis
Materials
A semi-structured interview schedule was developed (Appendix D). The schedule was checked and
approved by two experts. To improve the research instrument, three pilot interviews took place before
the official data collection started. The interview schedule consisted of 18 open-ended questions, with
multiple sub questions. Firstly, demographic questions were asked. Followed by questions about the
definitions and differences between fatigue, vitality and sleepiness, to see the patients‟ perspective on
these constructs. Fatigue was discussed, the symptom, its impact, and its characteristics. Subsequently,
current coping strategies of the patient on how to deal with fatigue were discussed. The interview closed
with questions about current communication about fatigue, treatment preferences, and advantages and
disadvantages of self-management and eHealth interventions in tackling the burden of fatigue. Patients
were shown the eHealth example of CoCo (condition coach) and encouraged to name improvements of
the design based on their own needs. The participants were often asked to elaborate on their answers and
to give examples, to further explore their opinion on the topic. The interviews were recorded with a
voice-recorder.
Procedure
In total, twenty interviews took place in a private environment, of which eleven interviews in the
GOLD 1 = Mild, GOLD 2 = Moderate, GOLD 3 = Severe, GOLD 4 = Very Severe

12
hospital (ten inpatients, one outpatient), and nine interviews at the patients‟ home. Before the start of the
interview, the participants had read the information letter (Appendix A), about the aim of the study and
how the results would be processed. The researcher answered any questions patients had and then asked
them to sign the informed consent form (Appendix B). Afterwards, the researcher clearly communicated
with the patient that the interview was about to begin and that the audio recorder started. During the
interviews, there were no non-participants present except the interviewer. This way, respondents could
talk openly and did not have to feel reserved in answering questions. The interview went on until all
questions were answered, to the point that there was no new information coming from the patient.
Participants were offered the option to get feedback on the results of the current study.
Analysis
The audio recordings were transcribed verbatim by the researcher. To guarantee anonymity of the
respondents, their names and any other personal information were removed. The researcher was the only
one that transcribed and coded all interviews. The data analysis was an iterative process, in which
deductive- and inductive coding were combined. First, the researcher read all transcripts thoroughly to
ensure familiarization with the data. The transcripts were coded using qualitative data analysis and
research software; ATLAS.ti 8.0. First, based on the suitability to answer the research questions,
relevant categories were deductively selected to build a preliminary organizing framework. The
following main categories were created: (1) Definitions and differences between fatigue, decreased
vitality, and sleepiness; (2) Characteristics of fatigue; the start, the causes, and its fluctuations; (3) The
impact of fatigue on the life of COPD patients; (4) Treatment options to tackle the burden of fatigue,
emphasizing eHealth, self-management, and blended care.
Furthermore, with inductive coding analysis, subdomains were selected using constant
comparison between interview transcripts. Initially, the researcher coded three interviews using a
concept coding scheme. This coding scheme was adjusted after a discussing with the research team. The
transcripts were coded and compared until the saturation point at which no new themes related to the
research question became apparent in the data. A coding tree was developed (Appendix E), in which the
code levels, codes, and remarks or discussion points were documented. The unit of analysis to which the
codes were applied were often multiple phrases to give information about the context and add meaning
to the coding. Subsequently, the analysed transcripts were divided into two groups to determine any
differences in answers between patients with GOLD 2 and patients with GOLD 3 or 4. In both groups,

13
the same coding scheme was utilized during analysis.
Results
In this section, the results of the interviews are presented. The duration of the interviews was between 14
and 70 minutes. The result section contains the following domains: (1) Definitions and differences
between fatigue, decreased vitality, and sleepiness. (2) Characteristics of fatigue; the start, the causes,
and its fluctuations; (3) The impact of fatigue on the life of COPD patients; (4) Treatment options to
tackle the burden of fatigue, emphasizing eHealth, self-management, and blended care.
1. Definitions and differences between fatigue, decreased vitality and sleepiness based on
experience of patients
To answer the first research question: “What is the patients’ perspective on the definitions and
differences between fatigue, decreased vitality and sleepiness?” the patients‟ viewpoints on the
definitions of fatigue, sleepiness, vitality, and on the connection between fatigue and vitality were
analysed.
1.1 Physical and mental fatigue
Physical fatigue was mainly associated with limitations in physical activities. Patients frequently
mentioned the lack of energy: “Dat je de fut niet meer hebt om dingen te doen die je wilt doen. Ja, dat is
het belangrijkste. Dat je geen energie hebt.” (P10, female, 64, GOLD 3). It was associated with
exertion: “Erg snel moe met inspanning” (P2, female, 52, GOLD 4), and with the excessive need for
rest and sleep: “Pff, veel slapen. Uhm, als je gaat zitten dan slaap je meteen. Veel stoppen tussendoor
om te rusten.” (P5, male, 65, GOLD 2). Although a majority of patients described fatigue with physical
aspects, one respondent gave a definition of COPD related fatigue focused on mental fatigue.
Associating mental fatigue with worrying, that increased when he was inactive: “Mentale vermoeidheid
komt iedere keer weer terug, zodra ik ga zitten begint het, het piekeren. Zolang ik in beweging blijf is er
niks aan de hand. (…) Als ik me moe voel en ga zitten dan blijf ik moe.” (P5, male, 65, GOLD 2).
Multiple patients associated mental fatigue with a gloomy, depressive state that demotivates patients:
“Dat heeft meer te maken met somberheid. Dat je dan, niet echt depressief, maar ja somber. Dan heb je
ook geen fut of energie om dingen te doen. Geen motivatie.” (P10, female, 64, GOLD 3). In addition, it
was mentioned that physical and mental fatigue were related: “Ik denk dat het in relatie tot elkaar staat.

14
Als je fysiek moe wordt, dan ben je daar ook met je hoofd mee bezig. Het is een proces van je hele
lichaam. Daarna ben ik net zo goed in mijn hoofd moe als in mijn lichaam.” (P7, male, 64, GOLD 2).
1.2 Differences between fatigue, decreased vitality and sleepiness
Table 2
Patients’ associations with fatigue, vitality and sleepiness
According to patients, fatigue is associated with the incapability of engaging in physical activities. Vice
versa, when asked to give a definition of physical vitality, patients gave similar answers (Table 2). For
example: “Als je vitaal bent, dan kun je alles aan. Dat je geen fysieke drempels hebt en dat alles veel
makkelijker gaat.” (P4, female, 62, GOLD 3). “Gewoon dat ze [vitale mensen] van alles en nog wat
kunnen doen. Ramen lappen, in de tuin bezig. Voor mij is dat gewoon zo veel moeite. Vooral praktisch.”
(P2, female, 52, GOLD 4). Mental vitality was only described by patients when specifically asked for
and patients found it more difficult to define. One patient tried by comparing her mental vitality to that
of healthy people: “Ze [vitale mensen] zitten ook wat lekkerder in hun vel dan ik.” (P2, female, 52,
GOLD 4). Other patients defined mental vitality as feeling energetic or motivated, in contrast to sad,
gloomy, or depressive feelings: “Dat ik energiek ben en zin heb om dingen te doen. Dat ik ook die
somberheid niet heb. Als je somber bent, al ben je nog zo fit, je hebt er gewoon geen zin in om iets te
doen.” (P10, female, 64, GOLD 3). Thus, while mental fatigue is associated with a gloomy and
depressive state, mental vitality is associated with opposite feelings (e.g., feeling energetic and
motivated). In addition, when defining physical vitality patients mentioned having no physical
limitations, opposite to defining physical fatigue, where patients mainly used physical limitations to
explain this symptom.
The overall opinion on the differences between fatigue and vitality was that they were closely
Concept Associated with Physical fatigue
Mental fatigue
- Feeling of exhaustion and extreme burden on daily life.
- Incapability of engaging in physical and social activities. - Not being capable to improve physical condition.
- Gloomy, depressive feelings.
- Decreasing motivation to improve physical condition.
Physical vitality
Mental vitality
Sleepiness
- Capability to engage in physical and social activities.
- Feeling energetic and motivated.
- Feeling after a sleepless night, heavy eyelids and having
no motivation to stay awake.

15
connected and fatigue had a negative influence on the vitality of patients: “Als dat [vermoeidheid] er
niet was geweest, dan was ik veel vitaler geweest om dingen te gaan doen.” (P3, female, 59, GOLD 4)
In addition, fatigue was perceived as decreasing the ability to improve vitality by exercising, and
decreasing the motivation to improve vitality: “Ik bouw daardoor ook geen conditie meer op door de
inactiviteit. Dan wordt de vitaliteit steeds slechter en gaat achteruit door de vermoeidheid. Ik ben moe,
beweeg niet, conditie gaat achteruit en voel me minder vitaal.” (P7, male, 64, GOLD). According to
other respondents, increased vitality can help decrease feelings of fatigue: “Als je vitaler bent, dan druk
je de vermoeidheid ook makkelijker weg. Dus ergens mee bezig zijn (…) en in beweging zijn.” (P5, male,
65, GOLD 2).
All patients agreed on the difference between fatigue and sleepiness. They clearly described
fatigue as different from being tired, or sleepy. Sleepiness was described as the feeling you get when
you have had a sleepless night, heavy eyelids and no motivation to stay awake. Sleepiness could be
resolved by getting a good night‟s sleep. However, fatigue was still present when they woke up. It
stayed with them day and night. Fatigue was described as a feeling of physical and mental exhaustion. A
heavy feeling and extreme burden in daily life of patients. To illustrate: “Als ik slaperig ben dan denk ik
nog niet van; Ik kan die dingen allemaal niet meer doen zeg maar. En als ik echt moe ben, dan kan ik
niks meer. Dat is fysiek en mentaal veel zwaarder.” (P4, female, 62, GOLD 3) “Vermoeidheid is echt
niet met het ene been voor het andere been uitkomen. En slaperigheid is gewoon dat je geen zin meer
hebt om wakker te blijven, omdat je wilt slapen of je ogen vallen dicht. Dat is een hele andere manier
van moeheid.” (P11, female, 65, GOLD 3). All associations with fatigue, decreased vitality and
sleepiness, according to patients, are listed in table 2.
2. The start, causes and fluctuations of fatigue
To answer the second research question: “What is the patients’ perspective on the start, causes and
fluctuations of fatigue?” the patients‟ viewpoints on these characteristics of fatigue were analysed.
2.1 Start of fatigue and its fluctuations
Regarding the start of fatigue symptoms, 15 out of 20 respondents answered with a general description
of the time period: “Een hele tijd terug, sinds mijn COPD eigenlijk al. Vanaf het begin. En misschien
wel langer, want toen ik gediagnosticeerd werd, toen zat ik al op GOLD 3, dus daarvoor had ik er ook
al last van.” (P4, female, 62, GOLD 3). “Dat sluipt erin, het gaat heel langzaam. Je zit steeds meer
omdat je pijn hebt, benauwd bent, je kan niks meer doen dus je bent steeds meer vermoeid.” (P7, male,

16
64, GOLD 2). Despite fatigue being described as gradually increasing by a majority of patients, five
respondents described the start of fatigue with a concrete time period: “Ik denk iets van 4 à 5 maanden
geleden.” (P1, male, 57, GOLD 4). “Eigenlijk zijn die begonnen sinds de laatste keer dat ik in het
ziekenhuis lag. In 2015, 2 jaar terug.” (P3, female, 59, GOLD 4). Patients who mentioned a concrete
starting point of symptoms, often described a triggering event, e.g., a severe COPD exacerbation causing
a hospital admission, or heavy physical activity as starting point for an increase in fatigue: “Toen in eind
2011 ging het niet meer [extreme vermoeidheid tijdens werk]. Toen zeiden ze [longarts] ook, je bent
binnen een half jaar naar 4 gedonderd [GOLD 4].” (P1, male, 57, GOLD 4). “Ja, nou toen ik met de
badkamer bezig was, daar twee weken aan gewerkt en na die twee weken was ik helemaal uitgeblust.
(…) Toen was het echt afgelopen.” (P12, male, 72, GOLD 2). Thus, according to these patients, fatigue
symptoms increased significantly when triggered by a specific event, not by the start of their COPD.
The burden of fatigue was perceived to be susceptible to change. Respondents pointed out that
they experienced positive, as well as negative fluctuations in the burden of fatigue. The main reason they
gave for an improvement in symptoms were pleasant weather conditions: “Ja als het mooi weer is dan is
het wat beter, dan ga je eerder naar buiten en beweeg je ook meer.” (P8, male, 74, GOLD 3). “In de
zomer had ik niet eens medicijnen nodig, niks aan de hand. Met mooi weer ben je ook niet moe en heb je
ook geen klachten.” (P1, male, 57, GOLD 4). However, in constract to positive effects, the weather also
caused negative fluctuations in fatigue: “Als het vochtig is, dan is het [vermoeidheid] veel erger. En in
de winterperiode. Ook als het heel warm is, dan heb ik er ook meer last van. Dus of te warm of te nat of
te koud, dan kan ik al niet meer naar buiten.” (P5, male, 65, GOLD 2). Fatigue symptoms were
perceived to increase directly when pulmonary function decreased due to bad weather conditions.
Furthermore, fatigue symptoms could fluctuate due to a bad night‟s rest: “Ik slaap ook vaak slecht, dus
daar word je ook moe van.” (P10, female, 64, GOLD 3). Additionally, patients perceived a decrease in
fatigue due to positive changes in their mental state: “Dan kan ik van die kleine dingen genieten, van het
huis, van alles. Dan is de vermoeidheid minder, dan ben ik weer blijer.” (P13, female, 85, GOLD 3).
“Kijk als het met je kinderen goed gaat, dan gaat het met jezelf ook goed. Als het minder met de
kinderen gaat, dan ben je zelf ook minder, meer zorgen. Dat heeft ook wel invloed hoor op de
gesteldheid.” (P9, male, 71, GOLD 3).

17
2.2. Causes of fatigue
Table 3
Causes of fatigue according to patients
2.2.1 COPD and over-activity
All respondents mentioned COPD as the main indirect cause of their daily fatigue (Table 3). The cause
of fatigue directly associated with COPD was dyspnoea: “Je wordt echt moe door die benauwdheid ook
natuurlijk.” (P6, male, 65, GOLD 3). In addition, over-activity while having COPD was mentioned as a
cause of fatigue by almost all patients. To illustrate: “Ik denk dat vermoeidheid hoort bij COPD. (…) Ik
denk dat de oorzaak is dat je meer doet dan dat je aan kan. Ja, want als ik moe wordt, dan weet ik dat ik
teveel gedaan heb.” (P4, female, 62, GOLD 3). Over-activity often causes oxygen deficiency and
according to patients, this increases the heavy feeling associated with fatigue: “Ik denk bij inspanning
dat de COPD wel van invloed is op het verergeren van die vermoeidheid. (…) Het ontstaat gewoon door
activiteit, teveel zuurstof gebruik. Te weinig zuurstof voor je spieren en daar word je zo moe van.” (P7,
male, 64, GOLD 2). However, inactivity and an incorrect breathing technique were also mentioned as
causes that increased fatigue: “De inactiviteit. De slechte ademhaling. Alles wordt onregelmatig en dan
kom ik op hetzelfde punt uit [erg vermoeid].” (P7, male, 64, GOLD 2). Thus, fatigue was caused by
multiple factors associated with COPD, including the use of medication: “Het zijn de medicijnen, veel
dingen doen, slecht slapen. Dat hele pakketje samen dat moet één lichaam aan. En dat lichaam is al heel
ziek, dat maakt het niet makkelijker.” (P5, male, 65, GOLD 2).
2.2.2 Comorbidities Besides COPD, respondents suffered from multiple comorbidities. Nine patients mentioned
comorbidities as an additional cause of fatigue. “Niet alleen de COPD, maar ook de spierziekte. (…)
Dat vergt heel veel energie. (…) Dan heb ik veel pijn, slaap ik slecht en word ik moe wakker.” (P2,
female, 52, GOLD 4). “De reuma misschien ook wel een beetje [oorzaak vermoeidheid].” (P17, female,
Causes COPD
- Dyspnoea
Over-activity
- Oxygen deficiency
Inactivity
- Worsening physical condition
Incorrect breathing technique
Medication use Comorbidities

18
77, GOLD 3). “Die andere aandoeningen ja, ik denk dat pijn [door artrose] ook wel te maken heeft met
vermoeidheid. Ik sta elke dag op met pijn en ik ga elke dag naar bed met pijn.” (P4, female, 62, GOLD
3). In addition to physical comorbidities, psychological stress also increased fatigue according to
multiple patients: “Ik ben heel vroeg wakker en dan gaat gelijk mijn hoofd malen. Ik ben een beetje
stress gevoelig, dus dan ga ik maar weer uit bed. Ik word nooit wakker door de COPD. Maar door het
piekeren, en dan slaap ik niet meer in.” (P10, female, 64, GOLD 3). “Ik heb de laatste tijd vrij veel
stress gehad, voor de opname en die stress moest ergens heen. Dus die heeft zich nou op de
vermoeidheid gefocust. (…). Maar de hele dag nadenken en piekeren, dan wordt het dus lichamelijk.
Dat is heel fout.” (P11, female, 65, GOLD 3).
Most respondents found it difficult to explain the difference between COPD and comorbidities as
causes of fatigue: “Dus dan zit er wel verschil in, ja. Waarschijnlijk. Het is moeilijk om dat te kunnen
onderscheiden ja, bij mij wel.” (P5, male, 65, GOLD 2).
3. Impact of fatigue on the life of COPD patients
To answer the third research question, “How is the impact of fatigue on the life of COPD patients
described from the patients’ perspective?” the limitations as a cause of fatigue and the level of impact
were analysed.
3.1 Limitations due to fatigue
Table 4
Limitations due to fatigue
3.1.1 Fatigue limits daily activities
According to all respondents, several daily activities are no longer possible to perform due to fatigue
(Table 4). All patients mentioned household tasks to be too physically demanding: “Ik kan niet
stofzuigen, stoffen gaat al niet. (…) Door die vermoeidheid, om te blijven staan, dat lukt me niet meer.
Activity Limitations
Daily activity
Physical health and activity
E.g., Not capable of household tasks, personal
hygiene, walking the stairs, a toilet visit.
E.g., Restrictions in walking and exercising, and having physical pain due to extreme inactivity.
Social activity
E.g., Not capable of participating in social
interactions with total social isolation as a
consequence.
19
(…) Naar de winkel lukt mij ook niet meer. En de apotheek, om medicijnen te halen. Ik dacht; jeetje,
moet het?” (P1, male, 57, GOLD 4). “Ik heb sinds vorig jaar al hulp in de huishouding genomen, ik vind
het vreselijk, maar ik krijg het zelf niet meer voor elkaar. De ramen lappen of de gordijnen wassen. Nou
ik deed er twee dagen over.” (P11, female, 65, GOLD 3). Even small, daily tasks, such as personal
hygiene, going to the bathroom or walking up the stairs are already challenging when suffering from
fatigue: “Wassen kan ik niet zelf. Van douchen moet ik eerst bijkomen. (…) Als ik naar de WC heen ga,
dan ben ik dood en dood moe. Dan ga ik maar weer in bed liggen en van eten word ik ook al dood moe.”
(P18, female, 71, GOLD 3). “Ik sleep me met moeite naar de wc. Dat is het. Thuis doe ik dat met een
stoel, ik ga met een stoel op wieltjes naar de wc, naar de keuken.” (P15, female, 72, GOLD 2).
Due to daily limitations, motivation to engage in activities decreased drastically in some
patients: “Nou, de goede voornemens worden tegengehouden door de vermoeidheid. Het is lastig te
omschrijven. Je zit zo vijf uur in de stoel, terwijl je eigenlijk had moeten eten. (…) Maar aardappels
schillen kost teveel energie.” (P16, male, 67, GOLD 3). “Ik heb nergens zin aan, echt niet. Door de
ziekte neemt de motivatie ook af.” (P18, female, 71, GOLD 3). In contrast, multiple respondents stated
that this motivation was still present. The association between daily limitations and mental states
became clear: “Ik ben in mijn hoofd heel positief. Ik wil van alles en nog wat. Ik wil voetballen met mijn
kleinkinderen. Maar lichamelijk [door de vermoeidheid] lukt dat gewoon niet. Ik wil geestelijk zoveel,
maar dat wil gewoon niet.” (P2, female, 52, GOLD 4). “Ik wil graag zoveel dingen doen, maar dat kan
niet, dat lukt me niet.” (P18, female, 71, GOLD 3).
3.1.2 Fatigue limits physical health and activity
Physical limitations, as mentioned by a majority of respondents, focused mainly on restrictions in
walking and exercising: “We lopen 5 meter en ik moest stilstaan. Ik kon niet met mijn eigen dochter
naar de stad lopen. En toch probeer je het, je probeert jezelf erover heen te zetten, maar het gaat niet.”
(P1, male, 57, GOLD 4). “Door de vermoeidheid kan ik niet alleen staan, ik heb geen kracht of energie
om mijn lichaam tegen te houden. Ik val zo om.” (P16, male, 67, GOLD 3). Furthermore, decreased
physical health can also be an indirect consequence of suffering from fatigue. Multiple respondents
mentioned that they were suffering from pain: “Ja je doet niks, dus alles gaat verzuren.” (P1, male, 57,
GOLD 4). “Benauwdheid en last van mijn heupen omdat ik zoveel zit en lig.” (P5, male, 65, GOLD 2).
“Zie je die trillende handen en spieren? Dat komt ook door de vermoeidheid. Ik heb gewoon geen
energie. (…) Ik kan ook niet te lang staan, of te lang zitten of liggen. Dan begint het me onderin de rug

20
zeer te doen of ik krijg kramp.” (P16, male, 67, GOLD 3).
3.1.3 Fatigue limits participation in social activities
Fatigue is reported to have an influence on multiple aspects of the social environment of patients. As
mentioned by respondents, they often cannot participate in social activities due to fatigue: “Het is meer
dat je niet mee kunt doen. (…) Familiefeestjes, even de stad in gaan. Dat zeg ik, je wilt heel fanatiek
meedoen en op een gegeven moment moet je afhaken.” (P2, female, 52, GOLD 4). “Kijk, als ik alleen
ben dan is het niet zo een heel groot probleem, maar vooral als mijn dochter er is of de kleinkinderen er
zijn of mijn vriend is er, ja dan wil je zoveel meer. Maar dan kost alles ook zoveel moeite.” (P2, female,
52, GOLD 4). “Maar als nu mijn kleinkinderen komen, dan denk ik wel eens; nou dat mag wel wat
minder. En dat is wel heel erg jammer.” (P6, male, 65, GOLD 3).
These limitations have led to social isolation and feelings of loneliness: “Ik denk wel dat je
langzaam isoleert van je omgeving. Je kan niet meer naar de markt, of naar familie. Helemaal niet
meer. (…) Ik kan nauwelijks meer naar buiten of met mensen afspreken. Totale isolatie.” (P7, male, 64,
GOLD 2). “Ik ben echt een mensen mens en dat mis ik. Hoe zieker dat je wordt, de kring wordt steeds
minder. Die wordt heel klein.” (P13, female, 85, GOLD 3). Despite their fatigue, some patients felt the
need, or the pressure, to participate in social activities “Vooral voor andere mensen doorzetten, daar doe
je het voor. Voor jezelf hoeft het niet meer.” (P1, male, 57, GOLD 4). “Ik kan het niet meer dragen ik
moet echt gaan liggen, maar dan toch blijf je door gaan omdat je naar de omgeving je verplicht voelt.
Best een belastend iets.” (P7, male 64, GOLD 2). Another aspect of the impact of fatigue on social
activities was the patients’ feeling of being misunderstood by their direct environment and even their
own family when it comes to dealing with the burden of fatigue:
“Ook kan je niet aan iemand zien dat hij COPD heeft, dus je wordt niet begrepen. Net
alsof je zit te zeuren, nou vreselijk! (…) Met slecht weer voel ik me heel moe. De
maatschappij snapt dat niet. Aan de buitenkant kun je niks aan mij zien, de ziekte zit
aan de binnenkant en ik voel me dan ook echt niet begrepen door iedereen.(…)
Anderen vinden dat je overdrijft met die vermoeidheid. (…) Heel frustrerend. Bij
kanker kan je zien dat iemand ziek is en andere mensen hebben medelijden, maar bij
COPD niet. Mensen geloven ook niet dat ik ziek ben, als ik geen zuurstof in mijn neus
heb.” (P3, female, 59, GOLD 4).

21
3.2 Mental burden due to fatigue
The daily limitations due to fatigue, brought along a heavy mental burden. A majority of patients
mentioned that they had, in some degree, lost the joy in life due to fatigue: “Ik merk wel dat ik steeds
moeier begin te worden en ook echt dat ik denk van; Pff, laat maar het interesseert me niet meer! Mijn
interesse valt weg door de vermoeidheid. (…) Niet dat ik dood wil, maar ik heb geen lust meer. Het is
weg. (…) Ik ken mezelf niet meer terug.” (P1, male, 57, GOLD 4). In addition, some patients mentioned
losing the will to live, due to the extreme mental burden: “Nou ik vind het leven natuurlijk niet meer
leuk. Er is niks aan. Je moet je tijd uitliggen. (…) Maar ik heb het opgegeven.” (P15, female, 72, GOLD
2). “Ik snap ook niet dat ik altijd zo moe moet zijn. (…) je stapt niet zomaar uit het leven omdat je moe
bent, maar soms denk ik er wel over, omdat het zoveel pijn doet dat je niks meer kunt ondernemen. (…)
Bah, wat een slecht leven toch.” (P3, female, 59, GOLD 4).
In addition, the fact that patients are limited in their daily activities and social interactions was
extremely confronting and frustrating for the majority of respondents: “Ik ga even in een hoekje staan en
begin te vloeken. Van waarom kan ik dat nou niet? Zo frustrerend. Je wordt er constant mee
geconfronteerd. (…) Ik vind het verschrikkelijk. Het is in woorden niet uit te leggen. Gewoon
waardeloos, echt waardeloos.” (P5, male, 65, GOLD 2). Furthermore, fatigue being constantly present
throughout the day was frustrating for patients: “Je bent vermoeid, je slaapt onrustig, dus je wordt ’s
ochtends weer vermoeid wakker. (…) Dus ik kom nooit door die vermoeidheid heen! Dat is zo
frustrerend.” (P1, male, 57, GOLD 4). In addition, patients mentioned the fear of losing all physical
capabilities and becoming dependent on others: “Maar ik ben er heel bang voor, wanneer ik helemaal
niks meer kan en afhankelijk word. Het gaat de verkeerde kant op.” (P15, female, 72, GOLD 2). “Ik ben
aan het piekeren en nadenken over hoe ik de dagelijkse dingen aan ga pakken, ondanks dat ik zo moe
ben. (…) Vreselijk. Je wordt er bang van, dat je steeds minder kan doen. Het is eng.” (P16, male, 67,
GOLD 3).
3.2 Rating of the impact fatigue has on the life of COPD patients and of their subjective vitality
Patients ranked the level of impact that fatigue had on their lives on a scale from 1 to 10. Scores ranged
from 3 to 10, with a median of 8 (SD 4.2). Six respondents ranked the impact of fatigue with a 9. Two
patients even ranked the impact of fatigue with a 10: “Oh, dan moet ik wel een 10 geven. (…) Ook wel
een dubbele 10. Ja dat is heel erg. Dat bepaald mijn hele leven.” (P13, female, 85, GOLD 3). Five
patients rated the impact with a 5. One of them stated that fatigue had major impact on her physical

22
abilities. However, emotionally she was very positive and had a lot of motivation: “Het weerhoudt mij er
niet van om dingen te doen. Ik wil het graag allemaal nog wel, maar mijn gevoel wil meer dan dat ik
aankan.” (P4, female, 62, GOLD 3). There was no difference found during analysis in severity of
fatigue between male or female patients (Figure 3), or between COPD patients with GOLD 2 and
patients with GOLD 3 or 4 (Figure 2). Perceived fatigue did not directly correlate with disease severity
based on pulmonary function. In addition, patients with GOLD 2 mentioned the same aspects during
interviews in describing the impact of fatigue as patients with GOLD 3 or 4 did.
Figure 2. Ranking by patients of the impact of fatigue on their daily lives on a scale of 1 to 10 (1 = no impact, 10 = Extreme impact on patients' lives) divided into GOLD stages
Figure 3. Ranking by patients of the impact of fatigue on their daily lives on a scale of 1 to 10 (1 = no impact, 10 = Extreme
impact on patients' lives) divided into gender
0
1
2
3
4
5
6
7
8
1 2 3 4 5 6 7 8 9 10
Fre
qu
ency
Rating impact fatigue
GOLD 3 / 4
GOLD 1 / 2
0
1
2
3
4
5
6
7
8
1 2 3 4 5 6 7 8 9 10
Fre
quen
cy
Rating impact fatigue
Female
Male
23
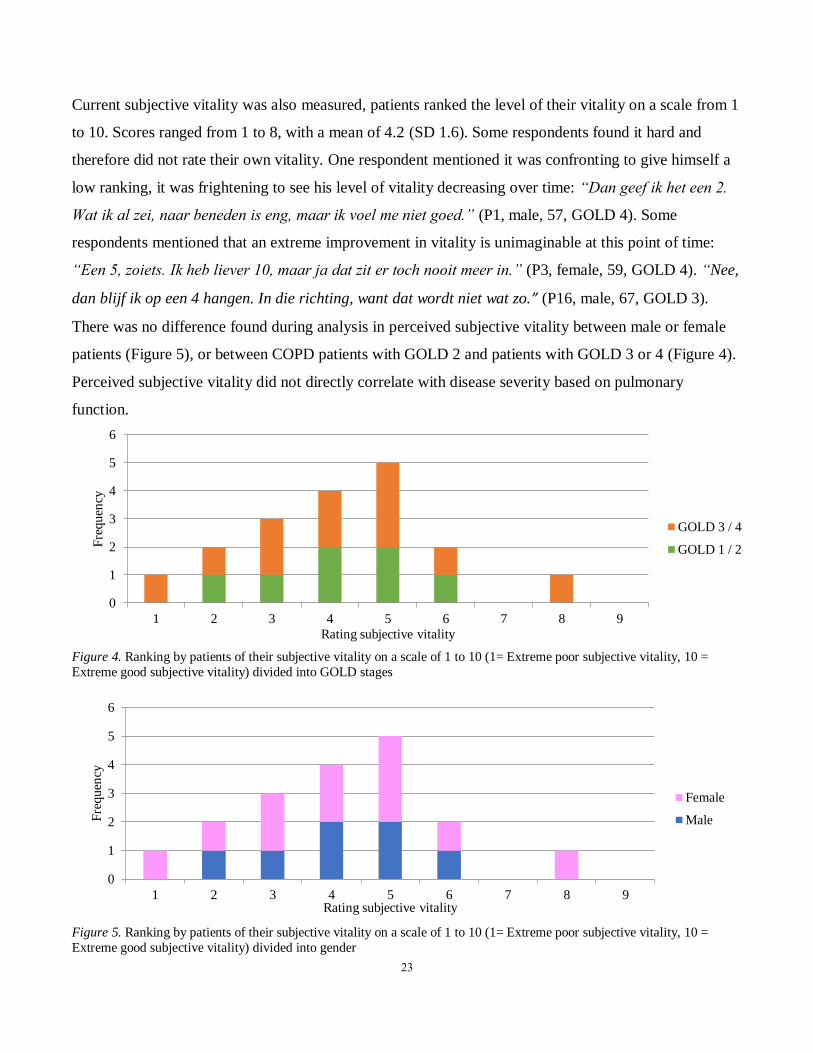
Current subjective vitality was also measured, patients ranked the level of their vitality on a scale from 1
to 10. Scores ranged from 1 to 8, with a mean of 4.2 (SD 1.6). Some respondents found it hard and
therefore did not rate their own vitality. One respondent mentioned it was confronting to give himself a
low ranking, it was frightening to see his level of vitality decreasing over time: “Dan geef ik het een 2.
Wat ik al zei, naar beneden is eng, maar ik voel me niet goed.” (P1, male, 57, GOLD 4). Some
respondents mentioned that an extreme improvement in vitality is unimaginable at this point of time:
“Een 5, zoiets. Ik heb liever 10, maar ja dat zit er toch nooit meer in.” (P3, female, 59, GOLD 4). “Nee,
dan blijf ik op een 4 hangen. In die richting, want dat wordt niet wat zo.” (P16, male, 67, GOLD 3).
There was no difference found during analysis in perceived subjective vitality between male or female
patients (Figure 5), or between COPD patients with GOLD 2 and patients with GOLD 3 or 4 (Figure 4).
Perceived subjective vitality did not directly correlate with disease severity based on pulmonary
function.
Figure 4. Ranking by patients of their subjective vitality on a scale of 1 to 10 (1= Extreme poor subjective vitality, 10 =
Extreme good subjective vitality) divided into GOLD stages
Figure 5. Ranking by patients of their subjective vitality on a scale of 1 to 10 (1= Extreme poor subjective vitality, 10 =
Extreme good subjective vitality) divided into gender
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9
Fre
qu
ency
Rating subjective vitality
GOLD 3 / 4
GOLD 1 / 2
0
1
2
3
4
5
6
1 2 3 4 5 6 7 8 9
Fre
quen
cy
Rating subjective vitality
Female
Male

24
3.3 Acceptance of fatigue
Accepting the burden of fatigue is not an easy task for the majority of respondents: “Het hoeft van mij
niet meer. (…) Ik merk nu dat ik heel snel achteruit ga. En dat kan ik niet accepteren, vooral ineens de
vermoeidheid. Ik kan het niet accepteren dat het niet meer lukt wat ik wil.” (P1, male, 57, GOLD 4).
One respondent mentioned that she did not want to accept her fatigue: “Het is alleen erg als ik heel moe
ben. Maar ik wil ook niet, ik wil niet toegeven. Nu nog niet, nee daar ben ik nog veel te jong voor.” (P4,
female, 62, GOLD 3). However, the overall opinion of respondents was that they had no other choice
than to accept their fatigue. When patients resist and try to fight the burden of fatigue, its impact
increases even more. “Kunnen of moeten? Er zit verschil in. Je zal het wel moeten accepteren. (…) Je er
tegen verzetten dat kan je niet.” (P4, female, 62, GOLD 3). “Ik accepteer het en denk het hoort bij de
ziekte. Ik kan er wel tegenin gaan, maar het helpt helemaal niks. Als ik er tegenin ga wordt het alleen
maar erger.” (P14, female, 64, GOLD 2). “Nu wel. Ik zal wel moeten. (…) Op een gegeven moment moet
je gewoon accepteren dat het zo is, anders beïnvloed het alles. Dat mag niet gebeuren, want dan kan ik
niks meer doen.” (P2, female, 52, GOLD 4). The majority of patients mentioned the difficulty of truly
accepting fatigue and the frustrations that this brings along as a consequence. Patients felt like they had
no other choice than to accept the physical, daily, and social limitations caused by fatigue.
4. Treatment options to tackle the burden of fatigue and improve vitality
To answer the last research question: “What is the patients’ perspective on the effectiveness of treatment
options to tackle the burden of fatigue and improve vitality, emphasizing eHealth and self-management
interventions?”, the patients‟ perspective on the current communication about fatigue, their
communication needs and their treatment preferences were analysed.
4.1 Communication about fatigue
4.1.1 Current communication about fatigue with social network
Respondents mentioned that they do not want their fatigue to be a burden on their family and friends.
Three respondents mentioned this specifically as the reason they do not speak with their partner or
family about their fatigue symptoms: “Je gaat niet met je klachten naar je partner of vrienden, dat is
veel te belastend.” (P1, male, 57, GOLD 4). “Mijn zoon komt elke dag langs een kop koffie drinken. (…)
Maar we hebben het er niet echt over verder. Ik wil hem er ook niet teveel mee belasten.” (P3, female,
59, GOLD 4). Another respondent mentioned that he did not speak about his fatigue with anyone, until

25
the moment he found out that other COPD patients also suffered from fatigue: “Nou toevallig dat we het
er van de week op de [fysio]therapie over gehad hebben. Daar zijn we met drie mannen. Nu blijkt
gewoon dat ze allemaal last hebben van vermoeidheid! Ik dacht echt dat ik daar een uitzondering in
was.” (P5, male, 65, GOLD 2). Despite these patients not liking to talk about their burden with close
family, communicating fatigue with fellow COPD patients had a comforting and supporting effect: “Ik
zit op COPD site [facebookgroep voor COPD patiënten]. Daar gaan we onderling elkaar steunen en
ook ideeën uitwisselen. (…) [Medepatiënten zeiden:] Wij zitten er [vermoeidheid] ook mee! Iemand zei;
weet je dat er 80% is die hier last van heeft? Waarom is er niet eerder een onderzoek opgezet!?” (P1,
male, 57, GOLD 4).
The fact that a few patients felt misunderstood or ignored by their social network, as described
earlier, could form another reason why patients no longer communicated on fatigue with close family or
friends: “Nee. Mensen luisteren niet naar je. Vooral niet als je 72 bent. Dan ben je toch geen mens meer,
dan ben je een oude vrouw.” (P15, female, 72, GOLD 2). “Het is moeilijk uitleggen aan andere mensen.
Als ik zo zit zie je niks aan me. Ik heb niet veel moeite met wat andere mensen van mij denken, maar toch
is het wel zo dat je je omgeving vaak onvoldoende ziet.” (P7, male, 64, GOLD 2).
In contrast, multiple patients did not have trouble communicating fatigue with their social
network. The main reason they spoke about their fatigue was to inform their social network about their
condition and limitations during social activities: “Ja zeker, allemaal. Bij de biljartclub en voetbal weten
ze het (…) Dan is het ook makkelijker om bepaalde dingen te zeggen he. (…) Dat begrijpen ze allemaal
wel.” (P6, male, 65, GOLD 3). “Jawel. Want als iemand iets van me wil en ik kan het niet, dan moet ik
het ook kunnen benoemen. Want mensen vragen; Waarom wil je dan niet? Dus ik praat er wel echt
over.” (P11, female, 65, GOLD 3).
4.1.2 Current communication about fatigue with healthcare professionals
Fatigue is often not mentioned during communication with pulmonologists. Neither patients, nor
pulmonologists mentioned the symptom during a consult: “Weinig. Nou ja, het consult is maar 10
minuten en dan is er vaak al heel veel wat er besproken moet worden. Dan wordt er niet over
vermoeidheid nagedacht. Zowel niet vanuit de arts, maar ook vanuit de patiënt niet. (…) daar wordt te
weinig over gesproken.” (P11, female, 65, GOLD 3). “Nee, dokters hebben toch geen tijd meer. (…) Ze
kunnen verder toch niks meer doen.” (P19, female, 67, GOLD 3). Furthermore, fatigue is not
specifically mentioned by the healthcare professional when informing patients about symptoms of

26
COPD. Multiple patients found this frustrating: “Dat [vermoeidheid] is mij ook niet verteld, maar dat
vind ik één van de ergste dingen.” (P1, male, 57, GOLD 4). “Dat de artsen er wat meer aandacht aan
geven, want patiënten zijn er niet altijd van op de hoogte van die vermoeidheid door de COPD.” (P3,
female, 59, GOLD 4). “Dan vraag ik hoe ik daar aan kom en wat het is, maar daar kunnen ze helemaal
geen antwoord op geven. (…) Ik weet ook niet waarom ik zo moe ben, niemand legt het uit.” (P15,
female, 72, GOLD 2). When fatigue is mentioned during a consultation with a pulmonologist, in most
cases patients themselves have to take the initiative: “Ik heb het hem wel gezegd. Ja, komt wel vanuit
mezelf. Dan zeg ik gewoon dat ik heel moe ben.” (P4, female, 62, GOLD 3). “Ze weten wel dat ik altijd
moe ben. Dan zeg ik eerlijk hoe ik me voel. Maar dat komt niet vanuit de zorgverlener. Het moet wel
echt vanuit mezelf komen, want de arts zegt er niks over verder hoor.” (P3, female, 59, GOLD 4).
However, in contrast to the pulmonologist, the physiotherapists, pulmonary nurses, and
psychologists do address fatigue and give advice on a more regular basis: “Nou met de fysiotherapie wel.
Die ziet dan ook aan mij dat ik vermoeid ben tijdens die oefeningen.” (P8, male, 74, GOLD 3). “Ik heb
wel bij een psycholoog gelopen op het ziekenhuis, daar heb ik wel heel veel van geleerd. Die gaf ook tips
dat je het rustig aan moet doen.” (P6, male, 65, GOLD 3). “Zij [longverpleegkundige] heeft ook meer
tijd denk ik. De longarts is veel drukker. Dat is gewoon zo, is ook wel begrijpelijk. Zij geeft wel tips over
wat je moet doen. Gewoon rustig aan doen, luisteren naar je lichaam.” (P8, male, 74, GOLD 3).
In contrast to the communication with physiotherapists, pulmonary nurses and psychologists, the
content of the communication about fatigue with pulmonologists is often superficial and no advice is
given to patients. To illustrate with multiple comments: “Al die klachten, het enige antwoord dat je
krijgt is; Het komt door de COPD. Ik krijg alleen nooit een advies over wat ik eraan moet doen! Dus,
dat schiet niet op.” (P3, female, 59, GOLD 4). “Ik praat erover en ik scheld erbij. Ik moet het iedere
keer opnieuw uitleggen en erover beginnen. Daar heb ik geen zin meer in, ik ben geen papagaai..” (P16,
male, 67, GOLD 3). In addition, when patients mentioned fatigue during previous consultations,
pulmonologists often ignored them: “Maar de longarts, ja. Die zegt weinig. Hij geeft nooit antwoord als
je zegt dat je heel erg vermoeid bent. Dan negeert hij het volledig.” (P8, male, 74, GOLD 3). “Ik heb zo
vaak geprobeerd te praten hierover. Hij negeert me gewoon. (…) Het boeit hem totaal niet. (…) Qua
communicatie en gewoon aandacht geven aan de patiënt, dat lukt de meesten niet.” (P15, female, 72,
GOLD 2). One patient even felt rejected by his pulmonologist in previous encounters when sharing
complaints. For this reason, he did not feel comfortable doing this again: “Ik heb het idee dat dat weinig

27
zin heeft. (…) Ik heb altijd het idee dat je op één of andere manier afgewezen wordt of dat ze geen
belang hebben bij jouw verhaal. Dus dan denk ik; Bekijk het maar, dan vertel ik het gewoon niet.” (P12,
male, 72, GOLD 2). Another respondent felt misunderstood by her healthcare professional and therefore
does not dare to share personal information again. She also mentioned the impatience of healthcare
professionals:
“Ik klap in het ziekenhuis veel dicht bij de dokters. Ik klap dicht, dan wil ik van alles
vertellen en ik heb het op een briefje staan, maar dan komt het er nog niet uit. Dan
durf ik het niet te vertellen. I: Waar komt dat door denkt u? R: Weet ik niet. Of hij mij
dan niet begrijpt, zo voel ik dat. Onbegrepen. Maar daar ben ik niet alleen in. (…) Ze
hebben er ook geen geduld voor. Sommigen luisteren wel hoor, maar de meesten niet.
Die laten je niet uitpraten. Maar dat is wel belangrijk.” (P13, female, 85, GOLD 3).
4.1.3 Patient needs for communication about fatigue
Multiple patients mentioned having the need to talk about their fatigue and possible coping
strategies with their healthcare professionals: “Je gaat niet met je klachten naar je partner of
vrienden, dat is veel te belastend. Dus dan heb je wel een uitlaatklep nodig bij een dokter.”
(P1, male, 57, GOLD 4). “In eerste instantie [behoefte aan] begrip en tips om daar mee om te
gaan.” (P10, female, 64, GOLD 3). “Dan denk ik dat het die vermoeidheid beperkt. Doordat
je weet hoe je ermee om moet gaan. Want dat is het nou juist, je weet niet hoe je ermee om
moet gaan, dus dan geef je er ook minder aandacht aan.” (P11, female, 65, GOLD 3).
Despite the majority of patients emphasizing their need to communicate about fatigue,
some respondents did not have this need. To illustrate: “Het schiet niet zoveel op als je er
over praat. Dan is die vermoeidheid er nog steeds wel” (P3, female, 59, GOLD 4). “Nee, niet
echt om te praten. Wel advies natuurlijk, dat zal ik nooit afslaan. Maar echt lang erover
praten, nee dat zit niet echt in mij. Ik ben niet zo een prater.” (P5, male, 65, GOLD 2).
However, as mentioned before, these patients do want to communicate about fatigue when
actions can be undertaken to decrease their symptoms: “Hij [longarts] zegt; Dat komt door de
COPD. En dat begrijp ik ook wel. Maar ik wil graag een ander antwoord, ik wil weten wat ik
eraan kan doen.” (P20, female, 80, GOLD 2).

28
4.2 Treatment preferences
Table 5
Treatment preferences to tackle the burden of fatigue, according to patients
4.2.1 Improving physical condition
Improving the physical condition of patients was specifically mentioned by multiple respondents as an
effective method to tackle fatigue: “Kijk mijn conditie is 0. Ik denk als je daarmee gaat beginnen. Om
die conditie weer op te bouwen. (…) Als daar nou eens wat voor was, denk ik ook dat er met de
vermoeidheid wat meer gedaan kan worden!” (P2, female, 52, GOLD 4). “Ik mis eigenlijk gewoon zelf
wat mogelijkheden tot revalidatie. (…) Bewegen onder begeleiding omdat je toch wat kwetsbaarder
bent. Bewegen onder deskundige begeleiding, gericht op die ademhaling. (…) Daarmee bouw je ook je
vermoeidheid wat af. Door meer te bewegen wordt je vermoeidheid minder.” (P7, male, 64, GOLD 2).
4.2.2 Social support
In addition to improving physical condition, a majority of patients mentioned combining treatment with
social activities and social support as important motivators: “Die sociale contacten en vergelijking is
belangrijk, zolang ze dezelfde symptomen hebben en iedereen zit met hetzelfde. Dat je van elkaar leert
wat handige, praktische tips zijn.” (P1, male, 57, GOLD 4). “Ja misschien wel goed in groepsverband
met meerderen. Je kunt elkaar dan ook steunen en helpen.” (P2, female, 52, GOLD 4). “Ik weet ook niet
dat ik niet de enige ben. En de longgroep, het mooie is dat die mensen dezelfde problemen hebben. Dus
je belt elkaar en je weet wat er aan de hand is.” (P4, female, 62, GOLD 3).
4.2.3 Focus on capabilities and feeling understood
Multiple patients wanted treatment to focus on their capabilities, instead of emphasizing their limitations
(Table 5): “Het is van belang om te kijken naar de dingen die wel goed gaan en naar de dingen die ik
Treatment preferences Treatment activities
Improving physical condition
Increasing social support
Focus on capabilities
Increasing feeling of understanding
- Exercising, rehabilitation possibilities, improving
breathing technique.
- Participating in social activities, increasing social
network, activating social support.
- Positive thinking and not focussing on limitations.
- Listening to patients and recognizing the severity of their symptoms.

29
nog wel kan. Daar word ik dan weer heel blij van zeg maar.” (P10, female, 64, GOLD 3). “Begeleiding
bij wat je nog wel kunt doen! Positief kijken. Langzamerhand beter worden. Dat hebben wij nodig.”
(P13, female, 85, GOLD 3). In addition to improving physical condition, social support and positive
thinking, multiple patients mentioned the need to feel understood and listened to by their healthcare
professional: “Ja, dat toch iemand begrip ervoor toont en misschien zou ik met iemand kunnen gaan
praten waardoor ik het beter accepteer of zo. Want als je erg vermoeid bent, dan gaat het nooit meer
over. Dan moet je daar wel mee leren dealen of mee leren leven.” (P10, female, 64, GOLD 3). “Ze
moeten goed naar me luisteren. En dan iemand, die je een beetje begeleid bij wat je nog kunt doen.”
(P13, female, 85, GOLD 3).
4.2.4 The role of healthcare professionals and patients in treatment of fatigue
When asked which healthcare professional could play a role in treatment of fatigue, multiple patients
mentioned a multidisciplinary approach between pulmonologists, pulmonary nurses, physical therapists,
general practitioners, occupational therapists, dieticians, psychologists, social workers, and homecare
workers. “Maar naast die fysiotherapie had ik ook veel gesprekken. Met een diëtist, ergotherapeut,
psycholoog. Daar heb ik wel heel veel aan gehad. Die heeft mij ook geholpen om open over die
vermoeidheid te spreken.” (P6, male, 65, GOLD 3).
“Je longarts weet hoe het met je longen is. Je huisarts weet de algemene dingen en
kan je advies geven en controleren. De psycholoog weet jou te motiveren en te
luisteren wat je niet met je partner en vrienden kan doen. (…) Een
longverpleegkundige sowieso, want die zie je altijd. En een diëtiste niet te vergeten!”
(P1, male, 57, GOLD 4).
The main conclusion of patients was that these healthcare professionals could set up an effective
treatment when they collaborate on a solution: “Misschien als ze samenwerken. (…) Dat ze de koppen bij
elkaar steken om een oplossing te vinden.” (P3, female, 59, GOLD 4). “Ik denk op zichzelf een
combinatie van fysiotherapie en een psycholoog. (…) Dat je een stukje bewustwording krijgt van de
fysieke en mentale processen en hoe dat zo goed mogelijk op elkaar af te stemmen.” (P7, male, 64,
GOLD 2).

30
A physiotherapist was mentioned most frequently as the healthcare professional that could help
decrease the burden of fatigue. Further treatment preferences focussed on the need for personal attention
and the healthcare professional as a motivator for treatment: “Ja op de mens zelf. Mensgericht. Concreet
op de persoon zelf en een stok achter de deur! Ik moest bijvoorbeeld fietsen, ik dacht; Ik trek het niet
meer dus ik doe het niet meer. Maar de arts zei; kom op, nog 10 minuten. Dat kan je wel. En toen kon ik
weer, want hij bleef naast me staan als motivatie!” (P1, male, 57, GOLD 4).
In addition, patients mentioned the difficulty to adhere to treatment because of their fatigue. The
feeling of fatigue could affect patients at random, unexpected times a day. Therefore, it was difficult to
adhere to a daily schedule of activities. According to patients, future treatment should take into account
this irregular occurrence of the symptom. Furthermore, when asked how patients can contribute to
treatment themselves, answers mainly included commitment to treatment, being motivated, listening to
the healthcare professional, and asking for help on time. “Het meedoen en de motivatie opbouwen. Ik
denk dat als je achter een behandeling staat, dat dat ook een positieve bijdrage geeft. Als je het in je
hoofd wilt, dat als een doel stelt voor een behandeling, dan kom je een eind verder.” (P6, male, 65,
GOLD 3).
4.3 eHealth and Self-management treatment to tackle the burden of fatigue and improve vitality
4.3.1 Experience and opinions about eHealth and self-management treatments
A few patients had experience in self-management treatment to cope with pain: “Ja, zoiets had ik ook
bij de pijnpoli, een dagboek invullen enzo.” (P7, male, 64, GOLD 2). “Ik heb bij het Roessingh wat
moeten invullen. In een boekje. Je was alleen maar bezig met schrijven en daar waar je mee bezig
moest zijn, dat kon niet.” (P2, female, 52, GOLD 4). In addition, experience with eHealth treatment
was mentioned by multiple patients: “Ik heb een keer in het Roessingh ook met een proef meegedaan,
met een laptop die je mee naar huis kreeg en dan stond je in verbinding met het Roessingh. En dan
moest je allemaal oefeningen doen, op een camera, ze keken mee. Je had rechtstreeks verbinding.”
(P5, male, 65, GOLD 2). “Ik heb wel een keer meegedaan aan een onderzoek waar je een tablet bij
kreeg. (…) Een tablet werkt makkelijker dan een computer, omdat ik die bij me kan houden en op elk
moment kan gebruiken.” (P8, male, 74, GOLD 3)
Patients had different views on the use of self-management and eHealth to tackle the burden of
fatigue. Advantages and disadvantages, as mentioned by patients, are listed in table 6. An advantage of
eHealth combined with self-management that was mentioned, was that it gives the patient structure

31
and insight in their own symptoms: “En het voordeel is natuurlijk, je kunt het altijd nakijken. Als het
op dat ding staat, op het internet. Het wordt helemaal bijgehouden.” (P2, female, 52, GOLD 4).
“Doordat je dit invult kan je jouw negatieve, maar ook pluspunten eruit halen. Je kunt zien of je je
energie goed gebruikt, of je het goed verdeeld. Wanneer je veel en weinig energie nodig hebt. Ik noem
maar een dwarsstaat. Het is heel overzichtelijk.” (P11, female, 65, GOLD 3). Furthermore, multiple
patients mentioned the time- and cost effectiveness and the motivational aspect of using eHealth: “Nou
ten eerste wordt de behandeling goedkoper. (…) Een ander voordeel is; Je kan het thuis doen. Je hebt
zelf controle. (…) Je moet, want dan verwachten ze dat je die [online] oefeningen of opdrachten doet,
dus die stok achter de deur is helemaal goed. Dat werkt.” (P5, male, 65, GOLD 2).
In addition to the advantages, multiple disadvantages were mentioned. Frequently named
disadvantages were aimed at privacy, internet connection, loss of personal contact, commitment of the
patient and this treatment being confrontational. To illustrate: “Nadelen zijn; heeft iedereen internet?
En is het veilig om het te doen? Kan er niet van buitenaf ingebroken worden?” (P1, male, 57, GOLD
4). “Je moet van alles invullen en ik kan niks meer, dus dan moet ik dat gaan invullen. Dat is heel
confronterend, ja dat doet wel pijn.” (P3, female, 59, GOLD 4).
Table 6
Advantages and disadvantages of using eHealth and self-management in tackling the burden of fatigue,
according to patients.
Advantages Disadvantages
Insight into own symptom frequency, history, and
energy levels
Privacy and security issues
Immediate insight for healthcare professionals in
symptoms
Need for working internet connection
Time and energy saving
- Patient can stay at home
Cost effective
Majority of patients does not use a computer or tablet
Less face-to-face contact with healthcare professional
Online personalized feedback Can increase fatigue by asking too much time and
commitment of the patient
Seeing a decrease in symptoms works motivating Confronting for patients to fill in all symptoms
Patient feels in control

32
4.3.2 Considerations in using blended care for treating the burden of fatigue
To illustrate the perspective of a patient on combining eHealth, self-management, and face-to-face
treatment in blended care to tackle the burden of fatigue:
“Misschien kunnen uit die online informatie die ik heb ingevuld dan grafieken ofzo
gemaakt worden, zodat er een duidelijker beeld ontstaat van mijn klachten. Dan heb
je meer tijd tijdens een afspraak om het echte onderwerp eruit te pakken. Nu praat je
over van alles en je tijd is al kostbaar. (…) Alle zorgverleners weten aan het einde
van de rit hoe jij je gedragen hebt en of je verbeterd hebt of bent gedaald in je
gezondheid. Ik denk dat mijn vermoeidheid dan veel eerder aan het licht was
gekomen.” (P1, male, 57, GOLD 4)
A majority of patients emphasized the need for face-to-face contact in treatment .They perceived face-
to-face contact as being more personal, more reliable, and forming better support for themselves than
eHealth options. “Maar het praat toch fijner en opener als je tegenover elkaar zit.” (P2, female, 52,
GOLD 4). “Dat is voor mij vertrouwder. Dan denk ik: Ja, die ken ik en die vertrouw ik wat die zegt.”
(P14, female, 64, GOLD 2). However, disadvantages of face-to-face treatment are mainly aimed at the
fact that the patient has to come to the hospital and this being very tiring: “Je ziet er namelijk echt
tegenop om het hele stuk naar het ziekenhuis te lopen en vooral ook in het ziekenhuis. (…) De trap op, en
als ik boven ben dan ben ik kapot. En dan moet de hele test of afspraak nog beginnen!” (P1, male, 57,
GOLD 4). All mentioned advantages and disadvantages of face-to-face treatment are listed in table 7.
Table 7
Advantages and disadvantages of using face-to-face treatment according to patients
Effective and efficient communication with
healthcare professionals
Advantages Disadvantages
Communication is perceived as more personal,
reliable and supportive
Patient has to come to the hospital

33
According to patients, it is important to use blended care when treating fatigue for the following reasons:
“Als je de vermoeidheid zo wilt bestrijden met ondersteuning van andere hulpverleners, dan zou dit in
combinatie best effectief kunnen zijn. (…) Maar je hebt daar wel iemand bij nodig waarmee je een
persoonlijke relatie en contact over hebt. Als je hier alleen aan moet beginnen denk ik dat het snel
verwatert en dat je betrokkenheid vermindert.” (P7, male, 64, GOLD 2). For blended care to work, one
respondent mentioned that it is important to keep things simple: “Als het maar niet te moeilijk gemaakt
wordt, gewoon simpel houden. Dan ben je al een heel eind.” (P11, female, 65, GOLD 3). “Als zoiets in
gebruik genomen wordt dan moet dus ook iemand uitleggen hoe het werkt en moet het zo simpel
mogelijk zijn.” (P20, female, 80, GOLD 2). An advantage of blended care to keep the disease in control
is that the healthcare professionals can see the progress the COPD patient is making. If the symptoms
increase in severity or frequency, treatment can be started immediately:
“Het beste is dat je dan één keer in de 14 dagen of één keer in de week een
verslagje wegstuurt naar de zorgverlener. Dat de arts alleen maar aan hoeft te
klikken wat hij wil zien. En de patiënt kan dan vertellen wat hij wel/niet gedaan heeft
en ook een duidelijke reden aangeven. Zo wordt het verhaal en de ziekte allemaal
wat duidelijker. En dan kan de longarts altijd zeggen van hé, ik moet hem even
bellen want hij gaat de berg af.” (P1, male, 57, GOLD 4).
Discussion
The purpose of this study was to examine the patients‟ perspective on COPD-related fatigue, its impact
on the daily life of patients, and patients‟ treatment preferences to tackle the burden of fatigue. In this
study patients perceived fatigue as a cause of extreme limitations on daily activities, physical
functioning and emotional well-being. This is in line with results from Theander and Unosson (2004),
Social aspect of treatment should not be forgotten
- Mental support
- Practical support
- Opportunity to ask questions/discuss
treatments
More time and energy consuming
Participating in a group of likeminded COPD
patients
Needs increased commitment of the patient
Patients feel like they can talk more openly about
symptoms

34
who stated that fatigue influences physical, cognitive, and psychological functioning. However, the
current study also showed perceived limitations in social functioning, in some cases resulting in total
social isolation due to fatigue. Patients emphasized that the ability and motivation to participate in
activities decreased. These findings are in line with results of Ream and Richardson (1997), who showed
that these limitations decreased concentration and motivation to „get up and go‟. In addition, current
participants mentioned even more intense feelings of low mood and depression due to a high mental
burden. Some patients even described losing the will to live due to this burden. This supports the
findings of Bjorner et al. (2007) and Van Dijken and Kort (2006), who showed that these limitations,
including social isolation, can lead to anxiety and depression. The current study showed that fatigue
negatively influenced multiple aspects of patients‟ lives, making it a multidimensional symptom which
is hard for patients to accept and difficult to tackle with the standard COPD treatment.
This multidimensional aspect of fatigue makes it harder to establish the difference between
fatigue, decreased vitality, and sleepiness. In the current study patients were clear that fatigue is closely
connected with decreased vitality. A decrease in physical functioning was mentioned as a consequence
of fatigue and decreased vitality. This is consistent with findings of Hensyl (1989), Swain (2000) and
Ryan and Frederick (1997), who state that there is coherence between fatigue and lower subjective
vitality. However, patients did mention a clear difference between fatigue and sleepiness. In contrast to
Hensyl (1989), who stated that sleepiness is a part of the definition of fatigue. In the current study,
fatigue is described by patients as different from sleepiness in quality, quantity and intensity. Whereas
sleepiness is described by patients as nonlimiting and a „normal‟ feeling. It can be resolved by taking
enough rest. COPD-related fatigue is physically and mentally far more demanding for patients than
sleepiness is and it increases negative impact on patients‟ daily lives.
Patients perceived that fatigue is mainly caused by symptoms of COPD. This is consistent with
findings from Breslin et al. (1998) and Esteban (2009). Interestingly, in the current study, unpleasant
weather conditions like the temperature being too cold or too hot were frequently mentioned as a cause
of fatigue. According to Donaldson and Wedzicha (2004) and Watz, Waschki, Meyers and Magnussen
(2009), negative weather conditions can also cause COPD exacerbations. Thus, fatigue is perceived to
be connected in intensity, and occurs simultaneously with other COPD symptoms. These experiences by
patients are in strong contrast with the relationship with the severity of COPD. Since, in the current
study, there was no difference found in the impact of fatigue between patients diagnosed with GOLD 2
and patients diagnosed with GOLD 3 or 4. Meaning that their fatigue was not directly correlated with

35
pulmonary function or disease severity. It indicates again that there are multiple aspects influencing the
severity of fatigue, instead of pulmonary function only. Although the burden of fatigue is often
gradually increasing and caused by COPD or even further increased by comorbidities (Mannino, Thom,
Swensen & Holguin, 2008), some patients mentioned a triggering event that started their severe fatigue
symptoms. Events mentioned that suddenly increased fatigue were a severe exacerbation, which is in
line with a study of Esteban (2009), but also heavy physical activity. This is in line with results from
Spruit et al. (2017), who mentioned that behavioural aspects influence fatigue. Thus, fatigue is often
associated with an increase of COPD symptoms. However, it is not directly correlated with pulmonary
function and influences multiple aspects of patients‟ daily lives. Therefore, it needs a multidisciplinary
treatment approach. This is in line with findings from Van Manen et al. (2011) and Theander and
Unossen (2011).
Patients mentioned that it was important to improve their physical condition, increase their
motivation, and increase their social support. In emphasizing their preferences, the pulmonologist was
often mentioned as having a key role in communication about fatigue. Currently, pulmonologists do not
address fatigue during consultations, do not inform patients about fatigue, and do not recognize its
impact on patients‟ lives. This supports findings from Swain (2000) and Spruit, Vercoulen, Sprangers
and Wouters (2017), who showed that pulmonologists often overlook or ignore fatigue during
consultations. Interestingly, patients expressed the need for pulmonologist to inform them about fatigue
symptoms and recognize the impact of fatigue that they are experiencing. This is in line with findings
from Jagosh, Boudreau, Steinert, MacDoland and Ingram (2011). However, when focussing on effective
treatment, other healthcare professionals like physiotherapists, psychologists, and pulmonary nurses
were mentioned as leading figures in treatment of fatigue. These professionals, in contrast to a
pulmonologist, can directly focus on increasing physical condition, increasing motivation, focus on the
needed social support and address fatigue during their consultations.
In addition to selecting healthcare professionals that could contribute to effective treatment, it
was also mentioned that treatment should be tailored to individual patients. In the current study,
participants emphasized that the degree of physical activity differs among individuals, depending on
their physical abilities and restrictions associated with their disease. Furthermore, some patients
mentioned the need for psycho-social treatment to cope with the heavy mental burden of fatigue, while
other patients did not feel this need. Therefore, treatment should be tailored to patients‟ needs and
capabilities. One way to support face-to-face treatment to tackle fatigue is the use of eHealth and self-

36
management interventions. Patients emphasized the potential of blended care. This is in line with
findings from Effing et al. (2016). Blended care in fatigue treatment can be of added value in tailoring
treatment. Patients can improve their physical condition in their own home environment, with exercises
especially selected for them by their physiotherapist. In addition, the face-to-face contact can ensure that
patients receive social support and psychological treatment when needed. Blended care could provide an
effective treatment option to tackle the burden of fatigue and decrease its impact on the daily lives of
COPD patients.
Strengths and limitations of the current study
The results of the current study need to be interpreted with caution. It is plausible that a number of
limitations might have influenced the results obtained. The first limitation of this study is based on the
interview setting. In total, 11 out of 20 patients were interviewed in a hospital setting, a private room at
the pulmonary department. A reserved attitude from the patient could arise due to the clinical setting and
the presence of the researcher. The latter being unavoidable in qualitative research. To minimize this
effect, the patients were encouraged to openly convey their viewpoints by asking for examples and to
further elaborate on their answers when needed. The patients who took part in the interview study were
very talkative, open, and willing to answer questions in great detail.
The second limitation is based on representativeness and generalizability. Current findings are
based on a limited number of respondents, recruited from a non-random sample. All outpatients had
participated in medical research before and were therefore more willing to participate. The third
limitation is the human element in this study, which can be a point of weakness because quality of
research depends solely on the researcher‟s skills and personal biases. These biases were controlled in
order to not let it influence the results. This is shown in multiple strengths of this research.
The first strength is based on the qualitative aspect of this research. The interviews were
conducted to clarify the patients‟ perspective. It gives detailed and in depth insights into the life of
patients with COPD suffering from fatigue. The data is based on direct human experience, this being
powerful information and can be very compelling. It reveals the real impact and importance of further
research on treatment options to tackle the burden of fatigue and increase vitality.
The second strength is based on the semi-structured interview scheme. During the interviews, the
researcher was not restricted to specific questions and the interview could be guided, or redirected by the
researcher in real time. This increased the chance to gain relevant information from patients. In addition,

37
because qualitative research depends on the researcher‟s skills, a semi-structured interview scheme can
also increase validity and create a handhold during interviews.
The last strong point of this study is focused on reducing possible biases. To reduce these, the
researcher considered how she was perceived by the respondents and the effect of features related to the
researcher, such as education and aims of current research. The researcher tried to have a neutral attitude
towards the patients. Making them aware that the researcher is not a doctor, to partially avoid socially
desirable responses. Collecting data in a qualitative setting is challenging. However, based on
consensus, research setup and execution were talked through with the research team and with an
extensive description of data collection and data analysis, the validity of this research increased.
Implications & Recommendations for future research
From the current findings, it can be concluded that the impact of fatigue on COPD patients is extensive
and present in all aspects of their lives. This study underlines the importance of a multidisciplinary
approach when developing effective, tailored treatment options. Fatigue needs to be addressed at an
early stage and treatment should be focussed on prevention and increasing vitality, rather than start
treatment when fatigue symptoms are already severely affecting the quality of life of patients. Therefore,
there lies a responsibility with the pulmonologists to take a pro-active approach and inform patients in
due time about the possible fatigue symptoms that they can experience as a consequence of their COPD.
In addition, they need to recognize the symptom and its impact on patients and refer them to suitable
healthcare professionals who have more time and tools to address fatigue (e.g., pulmonary nurse,
psychologist, or physiotherapist). Further treatment should incorporate personalized treatment
programmes, tailored to the physical capabilities of patients and their psychological needs. Not only
physical symptoms, but also the heavy psychological burden must be recognized within treatment. It is
recommended that awareness is created within pulmonary departments of the existing impact of fatigue
on the lives of patients and its multidimensional nature.
Future research should focus on validation by setting up quantitative research with a large group
of COPD patients. For example, developing a questionnaire about daily activities that are negatively
influenced by fatigue and checking if a larger population of patients (GOLD 1-4) agrees that these
aspects are influenced by their fatigue. By using a sequential research design, it can be checked whether
these qualitative findings can be generalized over a broader COPD population. This can help increase
awareness in healthcare professionals on the impact of fatigue and the need for effective treatment.

38
Furthermore, future research can focus on patient-provider communication, the way healthcare
professionals should inform patients about fatigue being a symptom of COPD and its impact, and which
healthcare professional has most added value in helping patients cope with fatigue and in what way this
should be established. To conclude, further research needs to be carried out to establish awareness on
fatigue and on the importance of developing an effective, tailored, multidimensional treatment.

39
References
Agusti, A., Hurd, S., Jones, P., Fabbri, L. M., Martinez, F., Vogelmeier, C. & Rodriguez-Roisin, R.
(2013). FAQs about the GOLD 2011 assessment proposal of COPD: a comparative analysis of
four different cohorts. European Respiratory Journal, 42(5), 1391-1401.
Aliverti, A., & Macklem, P. T. (2008). The major limitation to exercise performance in COPD is
inadequate energy supply to the respiratory and locomotor muscles. Journal of applied
physiology, 105(2), 749-751.
Baltzan, M. A., Scott, A. S., Wolkove, N., Bailes, S., Bernard, S., Bourbeau, J. & Canadian COPD
Pulmonary Rehabilitation Research Group. (2011). Fatigue in COPD: prevalence and effect on
outcomes in pulmonary rehabilitation. Chronic respiratory disease, 8(2), 119-128.
Bjorner, J. B., Wallenstein, G. V., Martin, M. C., Lin, P., Blaisdell-Gross, B., Tak Piech, C., & Mody, S.
H. (2007). Interpreting score differences in the SF-36 Vitality scale: using clinical conditions and
functional outcomes to define the minimally important difference. Current medical research and
opinion, 23(4), 731-739.
Bourbeau, J., & Van der Palen, J. (2009). Promoting effective self-management programmes to improve
COPD. European Respiratory Journal, 33(3), 461-463.
Breslin, E., Van Der Schans, C., Breukink, S., Meek, P., Mercer, K., Volz, W., & Louie, S. (1998).
Perception of fatigue and quality of life in patients with COPD. CHEST Journal, 114(4), 958-
964.
Donaldson, G. C., & Wedzicha, J. A. (2014). The causes and consequences of seasonal variation in
COPD exacerbations. International journal of chronic obstructive pulmonary disease, 9, 1101.
Effing, T., Monninkhof, E. M., Van der Valk, P. D., Van der Palen, J., Van Herwaarden, C. L., Partidge,
M. R., & Zielhuis, G. A. (2007). Self-management education for patients with chronic
obstructive pulmonary disease. Cochrane Database Syst Rev, 4.
Effing, T. W., Vercoulen, J. H., Bourbeau, J., Trappenburg, J., Lenferink, A., Cafarella, P., &
Bucknall, C. (2016). Definition of a COPD self-management intervention: International Expert
Group consensus. European respiratory journal, ERJ-00025
Esteban, C., Quintana, J. M., Moraza, J., Aburto, M., Egurrola, M., España, P. P., & Capelastegui, A.
(2009). Impact of hospitalisations for exacerbations of COPD on health-related quality of
life. Respiratory medicine, 103(8), 1201-1208
Evers, A. W., Kraaimaat, F. W., van Lankveld, W., Jongen, P. J., Jacobs, J. W., & Bijlsma, J. W. (2001).

40
Beyond unfavorable thinking: the illness cognition questionnaire for chronic diseases. Journal of
consulting and clinical psychology, 69(6), 1026.
Eysenbach, G. (2001). What is e-health?. Journal of medical Internet research, 3(2), e20.
Fraser, D. D., Kee, C. C., & Minick, P. (2006). Living with chronic obstructive pulmonary
disease: insiders' perspectives. Journal of advanced nursing, 55(5), 550-558.
Geijer, R. M., Sachs, A. P., Hoes, A. W., Salomé, P. L., Lammers, J. W. J., & Verheij, T. J. (2005).
Prevalence of undetected persistent airflow obstruction in male smokers 40–65 years old. Family
Practice, 22(5), 485- 489.
GOLD. (2017). GOLD 2017 Global Strategy for the Diagnosis, Management and Prevention of COPD.
Retrieved March 27, 2017, from http://goldcopd.org/gold-2017-global-strategy-diagnosis-
management-prevention-copd/
Hensyl, W. R. (1989). Stedman's medical dictionary. In Stedman's medical dictionary. Williams &
Wilkins.
Jagosh, J., Boudreau, J. D., Steinert, Y., MacDonald, M. E., & Ingram, L. (2011). The importance of
physician listening from the patients‟ perspective: Enhancing diagnosis, healing, and the
doctor–patient relationship. Patient education and counseling, 85(3), 369-374.
Jonkman, N. H., Westland, H., Trappenburg, J. C., Groenwold, R. H., Bischoff, E. W., Bourbeau, J., &
Gallefoss, F. (2016). Do self-management interventions in COPD patients work and which
patients benefit most? An individual patient data meta-analysis. International journal of chronic
obstructive pulmonary disease, 11, 2063.
Köhler, D., Fischer, J., Raschke, F., & Schönhofer, B. (2003). Usefulness of GOLD classification of
COPD severity. Thorax, 58(9), 825-825.
Lewko, A., Bidgood, P., Jewell, A., & Garrod, R. (2012). A comprehensive literature review of COPD-
related fatigue. Current Respiratory Medicine Reviews, 8(5), 370-382.
Lorig, K. R., Sobel, D. S., Ritter, P. L., Laurent, D., & Hobbs, M. (2000). Effect of a self-management
program on patients with chronic disease. Effective clinical practice: ECP, 4(6), 256-262.
Mannino, D. M., Thorn, D., Swensen, A., & Holguin, F. (2008). Prevalence and outcomes of diabetes,
hypertension and cardiovascular disease in COPD. European Respiratory Journal, 32(4), 962-
969.
Pauwels, R. A., Buist, A. S., Calverley, P. M., Jenkins, C. R., & Hurd, S. S. (2012). Global strategy for
the diagnosis, management, and prevention of chronic obstructive pulmonary disease. American
41
journal of respiratory and critical care medicine.
Peruzza, S., Sergi, G., Vianello, A., Pisent, C., Tiozzo, F., Manzan, A., ... & Enzi, G. (2003). Chronic
obstructive pulmonary disease (COPD) in elderly subjects: impact on functional status and
quality of life. Respiratory medicine, 97(6), 612-617.
Ream, E., & Richardson, A. (1997). Fatigue in patients with cancer and chronic obstructive airways
disease: a phenomenological enquiry. International journal of nursing studies, 34(1), 44-53.
Ryan, R. M., & Frederick, C. (1997). On energy, personality, and health: Subjective vitality as a
dynamic reflection of well‐being. Journal of personality, 65(3), 529-565.
RIVM. (2014) Chronische ziekten en multimorbiditeit. Retrieved March 27, 2017, from
https://www.volksgezondheidenzorg.info/onderwerp/chronische-ziekten-en-
multimorbiditeit/cijfers-context/prevalentie#node-prevalentie-chronische-ziekte-naar-leeftijd-en-
geslacht
RIVM. (2016). COPD - Prevalentie - Huidige cijfers. Retrieved March 27, 2017, from
https://www.volksgezondheidenzorg.info/onderwerp/copd/cijfers-context/huidige-situatie#node-
prevalentie-en-nieuwe-gevallen-copd
Seiler, A., Klaas, V., Tröster, G., & Fagundes, C. P. (2017). eHealth and mHealth Interventions in the
Treatment of Fatigued Cancer Survivors: A Systematic Review and Meta‐Analysis. Psycho‐
Oncology.
Silber, D. (2003). The case for eHealth. European Institute of Public Administration.
Spruit, M. A., Gosselink, R., Troosters, T., De Paepe, K., & Decramer, M. (2002). Resistance versus
endurance training in patients with COPD and peripheral muscle weakness. European
Respiratory Journal, 19(6), 1072-1078
Spruit, M. A., Vercoulen, J. H., Sprangers, M. A., & Wouters, E. F. (2017). Fatigue in COPD: an
important yet ignored symptom. The Lancet. Respiratory medicine.
Ståhl, E., Lindberg, A., Jansson, S. A., Rönmark, E., Svensson, K., Andersson, F., ... & Lundbäck, B.
(2005). Health-related quality of life is related to COPD disease severity. Health and quality of
life outcomes, 3(1), 1.
Swain, M. G. (2000). Fatigue in chronic disease. Clinical Science, 99(1), 1-8.
Tabak, M., Brusse-Keizer, M., van Ommeren, C., Kotte, H., Weltevreden, P., Hermens, H., &
Vollenbroek-Hutten, M. (2013). A telecare programme for self-management of COPD
exacerbations and promotion of an active lifestyle. European Respiratory Journal, 42 (Suppl

42
57), P4911.
Theander, K., & Unosson, M. (2004). Fatigue in patients with chronic obstructive pulmonary
disease. Journal of advanced nursing, 45(2), 172-177.
Theander, K., & Unosson, M. (2011). No gender differences in fatigue and functional limitations due to
fatigue among patients with COPD. Journal of clinical nursing, 20(9‐10), 1303-1310.
Thorndike, F. P., Ritterband, L. M., Gonder‐Frederick, L. A., Lord, H. R., Ingersoll, K. S., & Morin, C.
M. (2013). A randomized controlled trial of an internet intervention for adults with insomnia:
effects on comorbid psychological and fatigue symptoms. Journal of clinical psychology, 69(10),
1078-1093.
Townsend, A., Adam, P., Li, L. C., McDonald, M., & Backman, C. L. (2013). Exploring eHealth ethics
and multi-morbidity: protocol for an interview and focus group study of patient and healthcare
provider views and experiences of using digital media for health purposes. JMIR research
protocols, 2(2), e38.
Tselebis, A., Bratis, D., Kosmas, E., Harikiopoulou, M., Theodorakopoulou, E., Dumitru, S., ... &
Vgontzas, A. (2011). Psychological symptom patterns and vital exhaustion in outpatients with
chronic obstructive pulmonary disease. Annals of general psychiatry, 10(1), 1.
Van Dijken, F., & Kort, H. S. M. (2006). A vital living environment for people with COPD. In HB2006:
proceedings of the 8th international conference healthy buildings; Oliveira Fernandes, E. de;
Gameiro da Silva, M.; Rosada Pinto, J.(red). (pp. 141-144). ISIAQ.
Van Manen, J. G., Bindels, P. J., Dekker, F. W., Bottema, B. J., van der Zee, J. S., Ijzermans, C. J., &
Schadé, E. (2003). The influence of COPD on health-related quality of life independent of
the influence of comorbidity. Journal of clinical epidemiology, 56(12), 1177-1184.
Wedzicha, J. A., & Seemungal, T. A. (2007). COPD exacerbations: defining their cause and prevention.
The Lancet, 370(9589), 786-796.
Waatevik, M., Skorge, T. D., Omenaas, E., Bakke, P. S., Gulsvik, A., & Johannessen, A. (2013).
Increased prevalence of chronic obstructive pulmonary disease in a general population.
Respiratory medicine, 107(7), 1037-1045.
Watz, H., Waschki, B., Meyer, T., & Magnussen, H. (2009). Physical activity in patients with COPD.
European Respiratory Journal, 33(2), 262-272.
World Health Organization. (2016). COPD: Definition. Retrieved November 16, 2016, from
http://www.who.int/respiratory/copd/definition/en/

43
Zwerink, M., Brusse‐Keizer, M., van der Valk, P. D., Zielhuis, G. A., Monninkhof, E. M., van der Palen,
J. & Effing, T. (2014). Self-management for patients with chronic obstructive pulmonary
disease. The Cochrane Library.

44
Appendix
Appendix A. Informatiebrief onderzoek ‘Van vermoeid naar vitaal!’
Titel: Vermoeidheid bij COPD; Van vermoeid naar vitaal! Inleiding Geachte heer/mevrouw, Wij vragen u vriendelijk om mee te doen aan een medisch-wetenschappelijk onderzoek in Medisch Spectrum Twente. U beslist daarbij zelf of u mee wilt doen. Voordat u de beslissing neemt, is het belangrijk om meer te weten over het onderzoek. Lees deze informatiebrief dan ook rustig door. Bespreek het eventueel met uw partner, vrienden of familie. Wanneer u na het lezen nog vragen heeft kunt u terecht bij de onderzoeker. Onderaan bladzijde 2 vindt u de contactgegevens. Het onderzoek wordt uitgevoerd door een onderzoeker van de afdeling psychologie aan de Universiteit Twente, onder begeleiding van het Onderzoeksbureau Longgeneeskunde. 1. Wat is het doel van het onderzoek?
Graag zouden we meer inzicht krijgen in de impact die vermoeidheid heeft op het leven van patiënten met COPD. Tevens zijn wij geïnteresseerd in de mening van COPD patiënten over vermoeidheid. Met deze informatie hopen wij later adequaat hulp te kunnen bieden om vermoeidheid tegen te gaan. 2. Hoe wordt het onderzoek uitgevoerd?
Het onderzoek zal bestaan uit een interview. Er zullen vragen aan u worden gesteld over uw mening en ervaringen met vermoeidheid bij COPD. Het interview duurt maximaal een uur en kan plaatsvinden in MST, bijvoorbeeld voor of na een afspraak of tijdens een opname. Het interview kan ook bij u thuis plaatsvinden (op voorwaarde dat uw huis bereikbaar is via het openbaar vervoer). Het interview zal worden opgenomen met geluidsapparatuur. 3. Wat wordt er van u verwacht? Na ontvangst van deze formulieren heeft u één week de tijd om te beslissen of u mee wilt doen of niet. Wanneer u akkoord gaat met deelname kan u dit per e-mail of telefoon laten weten aan de onderzoeker. De onderzoeker zal contact met u opnemen voor het maken van een afspraak. Wanneer wij niets van u horen zullen wij na één week telefonisch contact met u opnemen om te vragen of u wilt deelnemen. De onderzoeker vraagt u om een uur tijd te reserveren voor het afnemen van het interview. Verder wordt er niets van u verwacht. Bij het plannen van een afspraak voor het interview kunt u aangeven wat voor uzelf het beste uitkomt qua tijdstip, dag en locatie. 4. Wat zijn mogelijke voor- en nadelen van deelname aan dit onderzoek?
Voor de toekomst kan het onderzoek nuttige gegevens opleveren, omdat we zo wellicht de vermoeidheid bij COPD beter in kaart te kunnen brengen. Uiteindelijk kan deze informatie bijdragen aan een effectieve aanpak tegen vermoeidheid bij COPD. U heeft zelf op de korte termijn geen voordeel van het meedoen aan dit onderzoek. Een nadeel van deelname is dat u een uur tijd moet vrijmaken om vragen te beantwoorden tijdens het interview.

45
5. Wat gebeurt er als u niet wenst deel te nemen aan dit onderzoek?
U beslist zelf of u mee wilt doen aan het onderzoek. Deelname is vrijwillig. Als u besluit om niet mee te doen, krijgt u gewoon de behandeling die u anders ook zou krijgen. U hoeft ook niet te zeggen waarom u niet mee wilt doen. Als u wel mee wilt doen, kunt u zich op ieder moment bedenken en toch stoppen. Ook tijdens het interview is het mogelijk om te stoppen. 6. Wat gebeurt er met uw gegevens?
Er zijn een aantal personen die uw gegevens kunnen inzien, dit zijn leden van het onderzoeksteam die meewerken aan dit onderzoek en leden van de Medisch Ethische Toetsingscommissie MST. Het interview zal worden opgenomen met geluidsapparatuur. Aan de hand van deze opnames zal het interview worden uitgeschreven en geanalyseerd. Uw persoonlijke gegevens blijven te allen tijde anoniem, geslacht en leeftijd zullen wel bekend zijn. Daarnaast kunt u eventueel, wanneer u dat wilt, de onderzoeker vragen om uw interview in te zien en eventueel stukken te verbeteren, aan te vullen, te verwijderen of af te schermen. Gegevens van het interview worden samengevat en mogelijk gebruikt voor wetenschappelijke publicaties met letterlijke citaten uit het interview. Deze citaten zullen anoniem blijven. Wij willen uw gegevens ook graag bewaren. Misschien kunnen we daar later een ander onderzoek mee uitvoeren of andere onderzoeken mee helpen. Als u dat niet wilt, respecteren wij dat. U kunt uw keuze op het toestemmingsformulier aangeven. Vindt u het goed dat wij uw gegevens bewaren? Als er een nieuw onderzoek gaat beginnen vragen wij u opnieuw toestemming hiervoor. U kunt ook dan nog beslissen of wij uw gegevens echt mogen gebruiken. 7. Welke medisch-ethische toetsingscommissie heeft dit onderzoek goedgekeurd? De Medisch Ethische Toetsingscommissie (METC) van Medisch Spectrum Twente heeft voor dit onderzoek een verklaring ‘niet WMO-plichtig onderzoek’ afgegeven. Dit betekent dat dit onderzoek is aangemeld bij deze METC en niet valt onder de wet medisch-wetenschappelijk onderzoek met mensen. 8. Zijn er extra kosten/is er een vergoeding wanneer u besluit aan dit onderzoek mee te doen? Voor uw deelname aan dit onderzoek wordt u niet betaald. U ontvangt geen reiskosten/onkostenvergoeding. Mocht u dit op prijs stellen, dan kan zoals eerder aangegeven het interview bij u thuis afgenomen worden (indien bereikbaar via openbaar vervoer) waardoor u geen reiskosten/onkosten hoeft te maken. 8. Wilt u verder nog iets weten? Voor het stellen van vragen, maken van afspraken, en het inwinnen van meer informatie voor, tijdens of na het onderzoek kunt u contact opnemen met de onderzoeker: Marileen Kouijzer Telefonisch contact op werkdagen via: *** E-mail: ***
Indien u na zorgvuldige overweging besluit om deel te nemen aan dit onderzoek, vragen wij u om samen met de onderzoeker het toestemmingsformulier te ondertekenen en dateren. Dit gebeurt voordat het interview wordt afgenomen. U zou ons erg helpen met uw deelname,

46
zodat het perspectief van de patiënt eindelijk belicht wordt en de zorg voor COPD patiënten verbeterd kan worden! Met vriendelijke groet, Het onderzoeksteam, Marileen Kouijzer, onderzoeker afdeling Longgeneeskunde en Health Psychology & Technology Paul van der Valk, longarts Medewerkers Onderzoeksbureau Longgeneeskunde

47
Appendix B. Informed consent
Toestemmingsformulier Titel van het onderzoek: Vermoeidheid bij COPD, van vermoeid naar vitaal! Ik heb de informatiebrief voor deelname gelezen. Ik kon aanvullende vragen stellen indien nodig. Mijn vragen zijn voldoende beantwoord. Ik had voldoende tijd om te beslissen of ik wil meedoen of niet. Ik weet dat meedoen geheel vrijwillig is en dat ik op elk moment kan besluiten om toch niet mee te doen of te stoppen. Daarvoor hoef ik geen reden te geven. Het is mij bekend dat bepaalde personen mijn gegevens in kunnen zien. Deze personen staan vermeld in de informatiebrief. Ik geef toestemming om mijn gegevens te gebruiken voor de doeleinden die in de informatiebrief genoemd zijn. Ik geef wel/geen* toestemming om gegevens maximaal 15 jaar na afloop van dit onderzoek te bewaren. *doorhalen wat niet van toepassing is
Ik neem deel aan dit onderzoek. Naam proefpersoon:___________________________ Handtekening: Datum: _______________________________ ___________________________
Ik verklaar hierbij dat ik deze proefpersoon volledig heb geïnformeerd over het genoemde onderzoek. Wanneer er tijdens het onderzoek informatie bekend wordt die de toestemming van de proefpersoon zou kunnen beïnvloeden, dan breng ik hem/haar daarvan tijdig op de hoogte. Naam onderzoeker/vertegenwoordiger: _____________________________ Handtekening: Datum: ________________________________ ___________________________

48
Appendix C. Medisch Ethische Toetsingscommissie (METC)

49
Appendix D. Interview schedule
Naam interviewer: Marileen Kouijzer
Nummer respondent: …
Leeftijd respondent: …
Geslacht respondent: ………
Datum: ……-……-……
Locatie: Medisch Spectrum Twente, Enschede / Thuis bij patiënt
Inleiding:
- Welkom & Bedanken
- Voorstellen: Marileen Kouijzer, Master student UT Afstudeeronderzoek Gezondheidspsychologie
bij MST
- Doel interview: Het doel van dit interview is om meer inzicht te krijgen in de impact die vermoeidheid
heeft op uw leven. Daarnaast zijn we geïnteresseerd in uw mening over vermoeidheid en vitaliteit bij
COPD. In het interview worden uw vitaliteit en vermoeidheid besproken en naar mogelijke oplossingen
gevraagd. Ik wil graag van te voren benadrukken dat er geen goede of foute antwoorden zijn, maar dat ik
alleen geïnteresseerd ben in uw eigen ervaring en mening.
- Duur: 30 tot 60 minuten
- Geluidsopname: Zoals u heeft kunnen lezen in de informatie die u gekregen heeft, wordt er een
geluidsopname gemaakt tijdens dit interview. Deze wordt veilig en anoniem bewaard en uw persoonlijke
gegevens worden geanonimiseerd.
Dan zal ik nu de geluidsopname starten en beginnen met het interview.
___________________________________________________________________________
0. Algemene vragen: a. Leeftijd?
b. Kunt u kort aangeven wat u in het dagelijks leven doet (of heeft gedaan)? (Werk, hobby)
c. Mag ik vragen hoelang u al COPD heeft?
d. Hoe lang bent u al onder behandeling hiervoor? (In MST?)
e. Mag ik vragen of u naast COPD, ook andere aandoeningen heeft; Zowel mentaal als fysiek?
De volgende vragen over de termen vermoeidheid en vitaliteit
1. Als u de term vermoeidheid zou moeten beschrijven; Welke definitie geeft u dan?
a. In hoeverre is er voor u een verschil tussen fysieke en mentale vermoeidheid? (Lichamelijk
/emotioneel vermoeid) Kan u dit verschil beschrijven?
b. Denkt u dat er een verschil is tussen vermoeidheid en slaperigheid? Waarom wel/niet? Kan u
dit verschil beschrijven?
2. Als u de term vitaliteit zou moeten beschrijven; Welke definitie geeft u dan?
a. In hoeverre is er voor u een verschil tussen fysieke en mentale vitaliteit? (Waarbij fysieke
vitaliteit slaat op uw lichamelijke energie en fitheid en mentale vitaliteit zou u kunnen zien als
een levendig gevoel of alertheid) Kan u dit verschil beschrijven?
De volgende vragen gaan over uw ervaring met vermoeidheidsklachten en vermindering in vitaliteit
3. Hoe ervaart u uw eigen vermoeidheidsklachten?
a. In hoeverre heeft u lichamelijke klachten door de vermoeidheid? Hoe en wanneer uit zich dat?

50
b. In hoeverre heeft u emotionele klachten door de vermoeidheid? Hoe en wanneer uit zich dat?
c. Wanneer zijn uw vermoeidheidsklachten begonnen?
d. In hoeverre heeft COPD een aandeel gehad in het verergeren van deze klachten?
e. In hoeverre verschillen de klachten per maand/dag/tijdstip? Waar hangt dit vanaf?
4. In hoeverre denkt u dat uw vermoeidheid samenhangt met uw vitaliteit?
a. Op wat voor manier? Kan u hiervan een voorbeeld geven?
5. Zou u uzelf nu beschrijven als vitaal?
a. In hoeverre vindt u uzelf vitaal als het gaat om uw emotionele gesteldheid?
b. In hoeverre vindt u uzelf vitaal als het gaat om uw lichamelijke gesteldheid?
c. Als u een cijfer zou moeten geven aan uw gevoel van vitaliteit (1= niet vitaal, 10= erg vitaal),
welk cijfer geeft u dan? Kan u dat uitleggen?
c. Wanneer voelt u zich (wel) vitaal/goed? In hoeverre verschilt dat per maand/dag/tijdstip?
Waar hangt dit vanaf?
De volgende vragen gaan over de mogelijke oorzaken van uw vermoeidheidsklachten
6. Wat denkt u dat de oorzaken van uw vermoeidheid zijn?
(a. In hoeverre denkt u dat uw andere aandoeningen bijdragen aan de vermoeidheid?)
(b. Hoe dragen deze aandoeningen bij aan de vermoeidheid?)
(c. In hoeverre kan u onderscheid maken tussen de oorzaken van de vermoeidheid?)
De volgende vragen gaan over de impact die deze klachten hebben op uw leven
7. In hoeverre heeft de vermoeidheid invloed op uw kwaliteit van leven?
a. Waarin uit zich dat? Kan u daar een voorbeeld van geven?
b. Als u een cijfer zou moeten geven aan de invloed die vermoeidheid op uw leven heeft (1=
geen invloed, 10= bepaald mijn hele leven), welk cijfer geeft u dan? Kan u dat toelichten?
8. In hoeverre is uw leven veranderd door uw vermoeidheidsklachten?
a. Kan u daar voorbeelden van geven?
b. Zijn er bepaalde activiteiten die u niet meer kunt uitvoeren door de vermoeidheid?
c. Welke activiteiten?
d. Wat vindt u daarvan?
De volgende vragen gaan over de manier waarop u omgaat met deze vermoeidheidsklachten (Nogmaals,
er zijn geen goede of foute antwoorden)
9. In hoeverre kunt u de vermoeidheidsklachten die u ervaart accepteren?
(a. Wel: Heeft het lang geduurd voordat u de klachten accepteerde? Waarom?)
(b. Niet: Ondanks dat u het niet geaccepteerd heeft; Heeft u een manier gevonden om met deze
klachten om te gaan? Hoe?)

51
10. In hoeverre heeft u aanpassingen moeten doen in uw leven vanwege uw vermoeidheid of
juist om extra vermoeidheid te voorkomen?
a. Welke aanpassingen? (Dagelijks leven, sociaal leven, werk of hobby etc.)
b. Wat vindt u daarvan?
c. Heeft u ook aanpassingen gedaan die achteraf niet bleken te werken?
De volgende vragen gaan over de communicatie tussen u en uw sociale omgeving over vermoeidheid
11. In hoeverre praat u met anderen over uw vermoeidheid? Met wie?
a. Praat u ook met uw zorgverleners (longarts, longverpleegkundige, fysiotherapeut etc.) over
deze klachten? Waarom wel/niet? Wie neemt het initiatief?
b. Wat wordt er besproken tussen u en uw zorgverlener over de vermoeidheid?
c. In hoeverre krijgt u momenteel behandelopties of advies aangereikt van uw zorgverlener?
Vraagt u hier zelf om?
d. Heeft u behoefte aan advies van uw zorgverlener? Kan u uitleggen waarom?
e. Heeft u het gevoel dat vermoeidheid en vitaliteit voldoende besproken worden tijdens een
consult? Kan u uitleggen waarom u dat denkt?
f. In hoeverre heeft u behoefte om hier uitgebreider over te praten met uw zorgverlener?
Waarom? Wat verwacht u dan van uw zorgverlener?
De volgende vragen gaan over mogelijke behandelopties tegen vermoeidheid en om vitaliteit te bevorderen
12. Wat zijn uw wensen als het gaat om een behandeling tegen vermoeidheid?
a. Wat zijn belangrijke aandachtspunten in uw leven waarop de behandeling zich moet richten?
b. In hoeverre zou uw vitaliteit verbeteren door een soortgelijke behandeling? Voorbeeld?
13. Wat zou uw eigen aandeel kunnen zijn in een behandeling tegen vermoeidheid?
a. Wat kan u zelf doen?
14. Welke zorgverleners zouden een rol kunnen spelen in de behandeling en op welke manier?
(Longarts, longverpleegkundige, fysiotherapeut, psycholoog/maatschappelijk werker, huisarts,
thuiszorg)
a. Wat is uw verwachting van zorgverleners als het gaat om het tegengaan van
vermoeidheidsklachten?
b. Waarom vindt u dit belangrijk?
De volgende vragen gaan over zelfmanagementbehandelingen en eHealth. Weet u wat deze termen
inhouden of zal ik een korte uitleg geven?
Zelfmanagement: Zelf verantwoordelijk voor de eigen gezondheid; op een goede manier omgaan met
klachten, behandeling, leefstijlveranderingen en lichamelijk/mentale gevolgen van COPD. CoCo als
voorbeeld. Website met ademhalingsoefeningen, monitoren van dagelijkse activiteiten en uw symptomen.
eHealth: is het gebruik van technologie ter ondersteuning of verbetering van de gezondheid. Zowel bij
eHealth als zelfmanagement: regie en verantwoordelijkheid over gezondheid/ziekte nemen (met
ondersteuning van arts).

52
15. In hoeverre heeft u ervaring met een zelfmanagement behandeling om uw vitaliteit te
bevorderen of vermoeidheid tegen te gaan?
a. Welke? / Geen ervaring: voorbeelden: CoCo, ConditionCoach; samenwerking met Roessingh:
Ademhalingsoefeningen, Activiteiten monitoren, Symptomen monitoren Dagboek, Actieplan
16. Wat zou u vinden van een zelfmanagement behandeling om uw klachten tegen te gaan?
a. Waarom positief of negatief?
b. Wat zou volgens u zeker terug moeten komen in deze behandeling?
17. In hoeverre heeft u ervaring met eHealth interventies in de gezondheidszorg?
a. Wel; voorbeeld?, Niet: voorbeeld van CoCo herhalen
Dan zijn we nu alweer aangekomen bij de laatste vraag van dit interview.
18. Wat is uw mening over het inzetten van eHealth tegen vermoeidheidsklachten en voor het
bevorderen van vitaliteit?
a. Waarom positief of negatief?
b. In hoeverre denkt u dat eHealth gecombineerd kan worden met een zelfmanagementbehandeling?
c. Wat zijn volgens u de mogelijke voor- en nadelen aan het inzetten van een soortgelijke
behandeling?
Dit was de laatste vraag. Zijn er van uw kant nog vragen aan mij of informatie die u graag zou willen
toevoegen? - Bedankt voor uw medewerking aan het interview!

53
Appendix E. Codescheme
Code level 1 Code level 2 Code level 3 Quotation examples Remarks, points
for discussion
Impact fatigue Limitations
due to fatigue
Physical “Douchen en scheren
is eigenlijk al teveel,
dan moet ik op de
wasbak hangen om te
kunnen blijven staan
(…) Al je energie
vloeit weg en dan wil
het gewoon niet
meer.”
Sommige fysieke
beperkingen
hebben ook
(in)direct invloed
op dagelijkse
activiteiten.
Daily activities “Huishouden,
familiefeestjes, even
de stad in gaan,
shoppen,
boodschappen, dat
soort dingen. Dat zeg
ik, je wilt heel
fanatiek meedoen en
op een gegeven
moment moet je
afhaken.”
Social
environment “Maar als nu mijn
kleinkinderen komen,
dan denk ik wel is;
nou dat mag wel wat
minder. Dat is wel
heel erg jammer.”
Mental burden due
to limitations “Ja je doet niks meer,
je hebt geen zin meer.
Het hoeft van mij niet
meer. Niet dat ik dood
wil, maar ik heb geen
lust meer. Het is weg.”
“Dat [vermoeidheid]
vind ik één van de
ergste dingen.
Benauwdheid hoort
erbij, zeker in de
wintermaanden, maar
die vermoeidheid is
echt slopend en zo

54
frustrerend (…) ook
echt dat ik denk van;
Pff, laat maar het
interesseert me niet
meer! Mijn interesse
valt weg door de
vermoeidheid.”
Level of
impact
fatigue
“8 of 9. Hoog ja.” Cijfer voor invloed
van vermoeidheid
op leven patiënt.
Start fatigue
symptoms
Concrete
time period
“Ik denk iets van 4 a 5
maanden geleden.”
General
description of
start fatigue
“Dat sluipt erin, het
gaat heel langzaam. Je
zit steeds meer omdat
je pijn hebt, benauwd
bent, je kan niks meer
doen dus je bent
steeds meer
vermoeid.”
Fluctuations in
burden fatigue
Positive “Nu is het goed weer,
dan ben ik in mijn
element, dat scheelt
een hele boei in de
vermoeidheid.”
Verbetering in
vermoeidheidsklac
hten.
Negative “Als het vochtig is,
dan is het veel erger.
En in de
winterperiode. Ook als
het heel warm is, dan
heb ik er ook meer last
van.”
Verslechtering in
vermoeidheidsklac
hten.
Causes fatigue COPD “Ik denk de COPD. En
ja, alleen de COPD
denk ik. De
benauwdheid die
iedere keer weer
terugkomt. Dat is wel
de voornaamste
oorzaak.”
Comorbiditie
s
“… en ook wel de pijn
door de reuma en zo.
Dat speelt ook wel een
rol.”
Differentiatio “Jawel met

55
n between
causes
lichamelijke dingen.
Dan merk ik gewoon
dat ik lucht te kort
kom. Dus dat is dan de
COPD. En als ik mijn
prothese omdoe, dan
gaan de spieren
tintelen en doen [door
spierziekte]. Dus dat is
wel verschil.”
Fatigue
acceptance
“…nou in het begin
heb je zoiets van; ach
joh, dat lukt me wel,
dat gaat wel. Dan ga je
meerdere malen op je
gezicht. En op een
gegeven moment moet
je gewoon accepteren
dat het zo is, anders
beïnvloed het alles.
Dat mag niet
gebeuren, want dan
kan ik niks meer
doen.”
Definitions
based on
experiences
patient
Fatigue Physical “…niet voldoende
energie hebben om de
dingen te doen die je
eigenlijk graag zou
willen doen. (…) Zoals
verder wandelen dan
300 meter.”
Deze code alleen
gebruiken wanneer
de patiënt de
algemene definitie
probeert te
beschrijven vanuit
eigen ervaring.
Anders coderen
met ‘Limitations
due to fatigue - …’.
Mental “Mentale
vermoeidheid komt
iedere keer weer terug,
zodra je ga zitten
begint het, het
piekeren.”
Differentiatio
n Fatigue +
Sleepiness
“Als ik slaperig ben
dan denk ik nog niet
van; Ik kan die dingen
allemaal niet meer
doen zeg maar. En als
ik echt moe ben, dan
kan ik niks meer. Dat
is fysiek en mentaal
veel zwaarder.”
56
Vitality Physical “Als je vitaal bent, dan
kun je alles aan. Dat je
geen fysieke drempels
hebt en dat alles veel
makkelijker gaat. (…)
Dan kon ik veel meer.
Dan kon ik ook
sporten en naar de
fitness.”
Mental “Ik heb heel veel
ideeën in mijn hoofd
zitten. Mentaal ben ik
heel actief.”
Connection
fatigue +
vitality
“Ik ben moe, beweeg
niet, conditie gaat
achteruit en voel me
minder vitaal.”
Verband tussen
vermoeidheid en
vitaliteit. De
invloed die ze op
elkaar kunnen
uitoefenen.
Vitality history “Als je vroeger altijd
druk bent geweest,
ook qua karakter en ja
ik heb 35 jaar hard
gewerkt dus en dan 3
kinderen. Dan komt er
nog wel iets op je af.
Dat kon ik altijd
fluitend.”
Gevoel van
vitaliteit voordat
vermoeidheidsklac
hten begonnen.
Fluctuations in
vitality
experience
Positive “Ja hoor! Als ik een
feestje heb. Ik ben een
gezelligheidsmens.
Dus als er een feestje
is dan ga ik er gewoon
naar toe en gezellig
doen. Ja hoor. Dan
kan ik het goed
volhouden. Alleen de
volgende dag moet je
het weer bezuren
natuurlijk.”
Verbetering in
vitaliteit (patiënten
beschrijven
vitaliteit standaard
als laag/slecht, met
soms een kleine
verbetering.
Daarom geen
negatieve
veranderingen in
vitaliteit).
Level of current
vitality
“Dan geef ik het een
2. Wat ik al zei, naar
beneden is eng, maar
ik voel me niet goed.”
Cijfer voor gevoel
van vitaliteit.
Communication Social “I: Praat u wel eens

57
about fatigue network met anderen over uw
vermoeidheid?
R: Hmhm. Ja met mijn
partner (…) en mijn
hulp.”
Health
professional
Initiative
“In eerste instantie
kwam het terloops ter
sprake vanuit de
patiënt [mede patiënt
in revalidatie]. En
gisteren was er een
maatschappelijk
werkster, die erover
begon.”
Advice “Die gaf ook het
advies om een hobby
op te pakken tegen de
vermoeidheid, maar
ook [om] de vitaliteit
[te verbeteren]. Als je
vitaler bent, dan druk
je de vermoeidheid
ook makkelijker weg.
Dus ergens mee bezig
zijn.”
Patient needs “Maar de
vermoeidheid, ja ik
weet wel waar het van
komt. Ik weet alleen
niet wat ik er aan moet
doen. Dat zou ik wel
graag willen weten.”
Treatment
options to
decrease (the
burden of)
fatigue
Treatment
Preferences
Improving
physical condition “Ik denk een beetje
conditie training op
een zeer laag niveau
wel belangrijk is om
basis oefeningen te
doen. Ook
ademhalingsoefeninge
n. Maar ik denk dat je
dat ook meer in
groepsverband zou
moeten doen, dat je
samen beweegt..”
Health
professional “Een combinatie van Verwachtingspatro
on met voorkeuren

58
fysiotherapie en een
psycholoog. Daar
moet ook de kracht uit
komen, om door te
gaan. Om het mentale
te ontdekken en het
fysieke met elkaar in
balans te brengen. Dat
je een stukje
bewustwording krijgt
van de fysieke en
mentale processen en
hoe dat zo goed
mogelijk op elkaar af
te stemmen”
patiënt van taken
zorgprofessional in
behandeling tegen
vermoeidheid.
Additional
treatment
preferences
“Ik denk dat er
misschien wel
medicijnen zijn die
zouden helpen. Dat is
ook gewoon zo. Maar
teveel medicijnen
werkt ook niet mee.”
Treatment
focus on
important
aspects of
patients’ life
“Ik denk op het op de
juiste manier de
dingen doen die je nog
kunt doen. Focussen
op wat nog wel lukt en
hoe je dat dan het
beste kan doen. Ik heb
ook geleerd om te
ontspannen, op de
juiste manier bewegen
en ademhalen. Dat is
heel belangrijk om je
vermoeidheid en je
rust te voelen, je te
ontspannen.”
Belangrijke
aspecten uit het
leven van de
patiënt waar een
behandeling tegen
vermoeidheid zich
op zou moeten
richten.
Active
contribution
in treatment
Patient “Het meedoen en de
motivatie opbouwen.
Ik denk dat als je
achter een
behandeling staat, dat
dat ook een positieve
bijdrage geeft. Als je
het in je hoofd wil, dat
als een doel stelt voor
Verantwoordelijkh
eid patiënt in een
behandeling tegen
vermoeidheid.

59
een behandeling, dan
kom je een eind
verder.”
Face-to-face
treatment
Experience “Ik moest
bijvoorbeeld fietsen,
ik dacht; ik trek het
niet meer dus ik doe
het niet meer. Maar de
arts zei; kom op, nog
10 minuten. Dat kan je
wel. En toen kon ik
weer, want hij bleef
naast me staan als
motivatie!”
Opinion Advantages
“Ja op de mens zelf.
Mensgericht. Concreet
op de persoon zelf. En
je hebt een stok achter
de deur. Je moet wel.”
Disadvantages “ Niks. [ik praat er]
met niemand [over].
Ook niet met mijn
arts. Ik wil niemand
belasten.
Ze kunnen er toch niks
aan doen.”
Self-
management &
eHealth
Experience “Ik heb een keer in het
Roessingh ook met
een proef meegedaan,
met een laptop die je
mee naar huis kreeg
en dan stond je in
verbinding met het
Roessingh. En dan
moest je allemaal
oefeningen doen, op
een camera, ze keken
mee”
Opinion Advantages “je kan het thuis doen.
Je hebt zelf controle”
Voor- en nadelen
van
zelfmanagement en
eHealth
behandelingen
hangen vaak samen
/ komen
grotendeels

60
overeen in mening
patiënt.
Disadvantages “Het is alleen, als ik
dit zo bekijken. Dat
dagboek en
oefeningen en zo. Dan
lijkt het alsof het
allemaal veel erger is
dan ik denk. Het is een
beetje confronterend.”
Blended care Consideratio
ns
Conditions Ja, als je de
vermoeidheid zo wil
bestrijden met
ondersteuning van
andere hulpverleners,
dan zou dit in
combinatie best
effectief kunnen zijn
(…) Maar je hebt daar
wel iemand bij nodig
waarmee je een
persoonlijke relatie en
contact over hebt.”
Patiënten vinden
online
zelfmanagement
tegen
vermoeidheid
alleen een optie
wanneer dat
gecombineerd
wordt met face-to-
face contact met
een
zorgprofessional.
Top Related