






Languages
Pages
Legal

Deiaa El-Din M. TamerP.I.C.U. Specialist
A.U.C.H

How to do rapid and accurate evaluation of cases in ED to determine critically ill cases.
Know the three components of the Pediatric Assessment Triangle
Have systematic approach to sick child in ED
Know the ED management of Common Pediatric Emergencies

Children are not young adults
Adults are big children but with chest pain
Different age group
Age specific norms
Remember important differences between adult and kids
RR : upper limit
< 2 mo 60 c/min
2-12 mo 50 c/min
1-5 years 40 c/min

BP
0 to 28 days 60 mm Hg in term neonates
1 -12 mo 70 mm Hg in infants
1 to 10 years 70 mm Hg + (2 x age in years)
>10 years 90 mm Hg in children

HR
Newborn to 3 mo: 85: 205
3 months to 2yrs: 100—190
2yrs to 10 yrs: 60—140
> 10yrs: 60—100
Wt crude Estimation:
<1year: [Age]+9/2
< 8 years:2x[Age]+8
> 8 years:3x[Age]

BreathingAppearance
Circulation

It is a rapid, accurate and easily-learned model for theinitial assessment of any child.
It allows the clinician, using only visual clues, torapidly assess the severity of the child’s illness or injuryand urgency for treatment, regardless of theunderlying diagnosis.

Tone
Interactiveness
Consolability
Look/Gaze
Speech/Cry
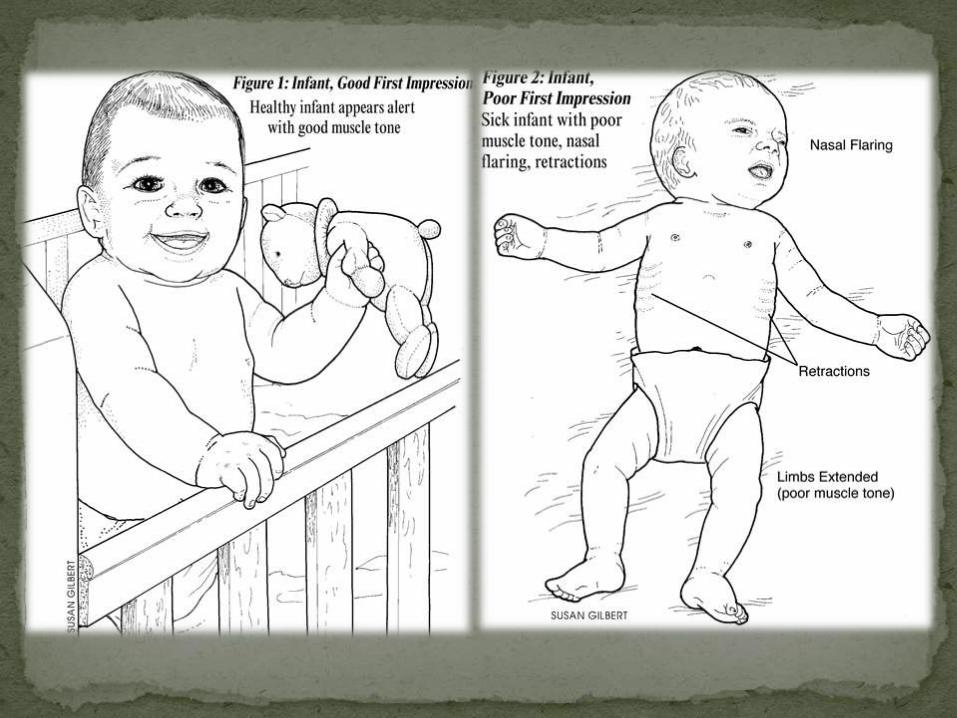

Abnormal airway sounds
Abnormal positioning
Retractions
Nasal flaring
Head bobbing

Work of breathing is a more accurate immediateindicator of oxygenation and ventilation thanconventional measures, such as counting RR or chestauscultation.
Work of breathing reflects the child’s physiologiccompensatory response to cardiopulmonary stress.
Assessing work of breathing entails careful listeningfor abnormal airway sounds and observing for specificvisual information about breathing effort.characteristics of work of breathing.

Combining assessment of appearance and work ofbreathing can establish severity.
A child with normal appearance and increased work ofbreathing is in respiratory distress.
Abnormal appearance and increased work ofbreathing means early respiratory failure.
Abnormal appearance and abnormally decreased workof breathing is late respiratory failure.

Pallor
Mottling
Cyanosis
An important indicator of core perfusion iscirculation to skin.
When cardiac output is inadequate, the body shutsdown circulation to non-essential anatomic areassuch as the skin in order to preserve blood supplyto vital end organs (e.g. brain, heart and kidney).
Therefore, circulation to skin reflects the overallstatus of circulation to the body’s important endorgans. Pallor, mottling and cyanosis are key visualindicators of reduced circulation to skin

The three elements of the PAT are interdependent andtogether allow rapid assessment of the child’s overallphysiologic stability. For example:
If a child is alert and interactive, pink, but has mildretractions, one can take time to approach the child in adevelopmentally appropriate manner to complete thephysical assessment.
On the other hand, if the child is poorly responsive, withunlabored rapid respirations, and has pale or mottledskin, one should move rapidly through the pediatricprimary survey, and initiate resuscitation.
Abnormal appearance and decreased circulation to skinmeans shock.

History
It is important to recognize those infants who are atrisk of becoming critically ill. For example:
1) Children with severe acute intoxications, such asacetaminophen, iron, or cyclic antidepressants maybe asymptomatic early in their presentation. Despitetheir benign appearance, they have potential todevelop lethal complications in the ensuing minutesor hours.
2) A child with blunt trauma may be able to maintainadequate core perfusion despite internal bleeding byincreasing cardiac output and systemic vascularresistance. When these compensatory mechanismsfail, she may acutely “crash”, with rapid progressionto clinical shock.

Anticipating Cardiopulmonary Arrest

ShockResp. Failure
1) Hypoxia.
2) Hypotension.
3) Hypothermia.
4) Hypoglycemia.
5) Acidosis (H+).
6) Hypokalemia(electrolyte disturbance).
1) Cardiac Tamponade.
2) Tension pneumothorax.
3) Thromboembolism(pulmonary, coronary).
4) Toxicity (eg. digoxin, local
anesthetics, TCA, insecticides).

Respiratory
Shock
Cardiac
10%10%
80%

The commonest cause ofcardiopulmonary arrest in pediatricis respiratory

Difficult compared to adults.
Significant portion of kids respond to AW management alone!
Time spent securing a vascular access at the expense of adequate AW management is a common mistake.
Drugs can be given through ETT.
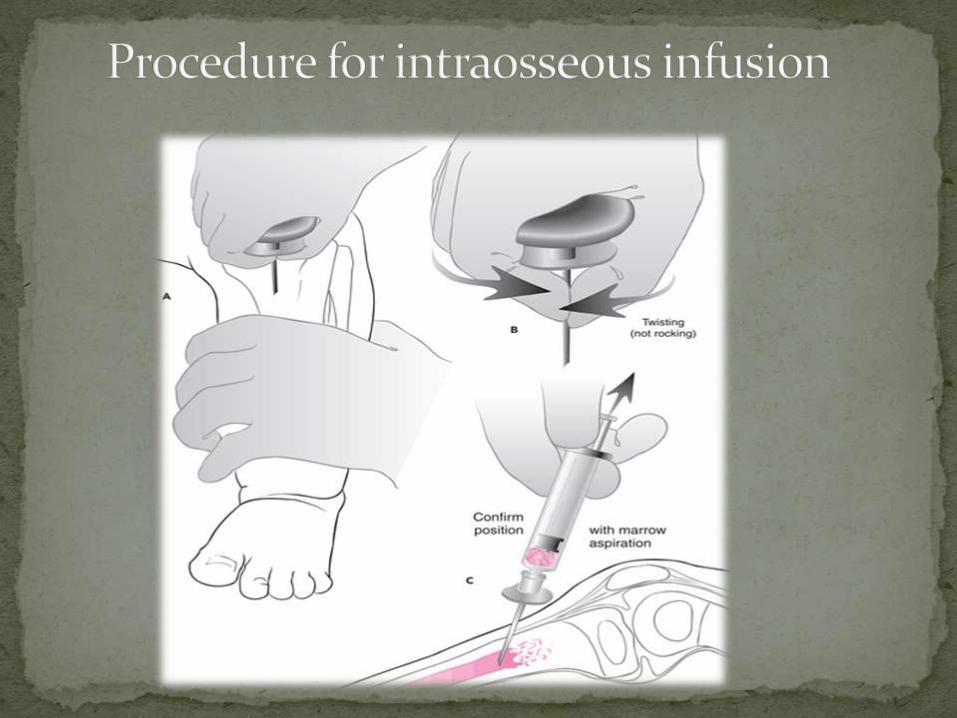
General order of attempts should be: antecubital, hand, or foot and then intraosseous.



Indication
Vascular access required
Peripheral site cannot be obtained
In three attempts, or
After 90 seconds

SiteChildren 0 to 6 years of age:
A. Medially to tibial tuberosity
B. Above medial malleolus
Children 6 to 12 years of age:
A. Medially to tibial tuberosity
B. Above medial malleolus
C. Femoral head

Contraindications
Fractures
Failed attempt on same bone
What can be put thru an IO?
Anything that can be put through an IV!

4-year-old previously well child is admitted to our hospital with fever, bloody diarrhea x 1 day. He lose his Interactiveness, had no urine x 24 hrs.
On exam : HR is 160, BP 70/30, temp 39 C. His skin is motteled with capillary refill <1 second.
What is your assessment?What is the stage of shock?What is the classification of shock?What is your differential for the etiology?What is your initial management?


Thank You
Top Related