





Languages
Pages
Legal


EoHaCGA
ah
h
p
mbTs
esopmh
cmmn©
Ta
v
pI
3
stimate of Body Water Compartments andf Body Composition in Maintenanceemodialysis Patients: Comparison of Singlend Multifrequency Bioimpedance Analysisarlo Donadio, MD, Cristina Consani, BSci, Michela Ardini, MD,iada Bernabini, MD, Francesca Caprio, MD, Giulia Grassi, MD,nnalisa Lucchesi, MD, and Barbara Nerucci, MD
Objective: The goal of this study was to compare the adequacy of single and multifrequency bioimpedancenalysis (BIA) to evaluate body water compartments, body composition, and nutritional status in maintenanceemodialysis patients.Design: Cross-sectional study.Setting: University-based hemodialysis unit.Patients: Nineteen patients (12 male, 7 female), ages 28 to 82 years (mean, 58.9), treated with maintenance
emodialysis (MHD) for 0.5 to 15 years (mean, 7.3).Intervention: This was a noninterventional study. Patients gave their informed consent to the diagnostic
rocedures performed.Main outcome measures: Total body water (TBW), extracellular water (ECW), fat-free mass (FFM), and body cellass (BCM) volumes were estimated with single-frequency (sf BIA) and multifrequency (mf BIA) plethysmographsefore and after a midweek dialytic session. Predialysis TBW also was estimated from anthropometric data (eBW). Serum albumin, prealbumin and myoglobin, and creatinine index were determined as indicators of nutritionaltatus and muscle mass.Results: Sf BIA and mf BIA gave very similar results for TBW volumes. A high linear correlation was also found betweenTBW values and both sf TBW and mf TBW; however, a statistically significant difference was found between e TBW and
f and mf TBW. Sf BIA and mf BIA gave quite different results for ECW, particularly when measured predialysis. The resultsbtained for FFM indicate a poor agreement between sf and mf BIA. The agreement was better when FFM was measuredostdialysis. The values of BCM, either measured predialysis or postdialysis, indicate a significant difference between sf andf BIA. FFM and BCM estimated with mf BIA had a closer correlation with creatinine index than sf BIA. mf BCM had also a
igher correlation with serum myoglobin, which is produced by muscle cells.Conclusions: TBW can be estimated with enough confidence from either sf or mf BIA at any time. On the
ontrary, the results of ECW are significantly different with sf and mf BIA when measured predialysis. Thus, it seemsore convenient to perform BIA after dialysis, in particular when assessing the “ideal” body weight. Theeasurements of FFM and BCM, obtained with either sf or mf BIA, are correlated with different indicators of
utritional status. In particular, mf BCM seems more appropriate than sf BCM for estimating muscle mass.2005 by the National Kidney Foundation, Inc.
rftc(td
ic
HE ASSESSMENT OF the nutritional sta-tus of chronic kidney disease patients plays
central role in nephrologic practice. In fact,
Department of Internal Medicine, Division of Nephrology, Uni-ersity of Pisa, Pisa, Italy.
Address reprint requests to Carlo Donadio, MD, Unit of Ne-hrology, Department of Internal Medicine, University of Pisa,-56100 Pisa, Italy. E-mail: [email protected]
© 2005 by the National Kidney Foundation, Inc.1051-2276/05/1503-1507$30.00/0
mdoi:10.1016/j.jrn.2005.04.001
Jou32
enal insufficiency is probably an important riskactor for malnutrition in older adults, and nutri-ional status is a major determinant of the out-ome of maintenance hemodialysis patientsMHD). In particular, in these patients malnutri-ion is closely related to morbidity and is a pre-ictor of mortality.In MHD patients, protein-energy malnutrition
s frequent and is related to dialysis vintage, andan be caused by a decreased intake of nutrients,
ainly proteins and calories; scarce appetite; orrnal of Renal Nutrition, Vol 15, No 3 ( July), 2005: pp 332-344

iaavatia
mapQpmttscmamlas(dcribccmmmd
stihtaehtem
(m
sietflbtocssmmf
tflmnnp
P
mef2hwbpttthr
ttc
S
mBwotm
ESTIMATE OF BODY WATER COMPARTMENTS 333
ncreased protein catabolism due to metaboliccidosis, hyperparathyroidism, insulin resistance,nd inflammation. In any case, moderate to se-ere malnutrition induces a body weight loss andlterations in body composition, mainly a reduc-ion in fat mass and in muscle mass and anncrease in total body fluids (TBW), with a prev-lent increase in extracellular water (ECW).
One essential point, still debated, is whichethodology to choose for early identification
nd accurate evaluation of malnutrition in MHDatients. The Kidney Disease Outcomes anduality Initiative (K/DOQI) guidelines 2000 re-
orted that studies are needed to determine theost effective combination of measures of nutri-
ional status for evaluating protein-energy malnu-rition.1 On the basis of a recent European con-ensus, nutritional status should be evaluated fromlinical data, such as history of weight loss, bodyass index, muscle mass, subcutaneous fat mass,
nd biochemical parameters, such as plasma albu-in, and creatinine, bicarbonate, and cholesterol
evels. Subjective global assessment is consideredwell-validated tool for evaluating nutritional
tatus, and dual-energy X-ray absorptiometryDEXA) is a useful method for attaining a moreetailed assessment of lean body mass. In any case,omorbid conditions should be assessed and C-eactive protein (CRP) measured as a marker ofnflammation, because there is a close relationshipetween malnutrition on one side and comorbidonditions and inflammation on the other.2 Theurrent opinion is that the assessment of uremicalnutrition requires using multiple measure-ents concomitantly, with no definitive singleethod that can be considered as a gold stan-
ard.3
In addition to nutritional evaluation, the mea-urement of body fluid compartments is necessaryo accomplish the maintenance of the equilibriumn body fluids, which is one of the major tasks ofemodialysis. Furthermore, the achievement ofhe “ideal” or “dry” body weight is crucial for andequate control of arterial blood pressure. How-ver, the assessment of ideal body weight inemodialysis patients is still controversial. In par-icular, different methods have been proposed tovaluate TBW, ECW, and hence the achieve-ent of ideal body weight.The analysis of electrical body impedance
BIA) is a simple, objective, and inexpensive
ethod of analyzing body composition and mea- puring body fluid volumes in normal subjects andn patients affected by different chronic diseas-s.4–6 Thus, BIA should allow evaluating nutri-ional status and the equilibrium between bodyuids compartments in MHD patients. BIA cane performed using single-frequency (sf) or mul-ifrequency (mf) plethysmographs. The adequacyf sf BIA and mf BIA for the evaluation of bodyomposition and of body fluids compartments istill debated. Finally, the usefulness of the mea-urements of fat-free mass (FFM) and of body cellass (BCM) obtained by BIA as indicators ofuscle mass in MHD patients still needs to be
ully validated.The primary goal of this study was to compare
he adequacy of sf and mf BIA to evaluate bodyuids compartments (TBW and ECW) and bodyass composition (FFM and BCM). The useful-ess of sf BIA and mf BIA for the evaluation ofutritional status in MHD patients will be com-ared.
Patients and MethodsatientsNineteen end-stage renal disease patients (12ale, 7 female), clinically stable, without signs of
dema, treated with maintenance hemodialysisor 6 months to 15 years (mean, 7.3 years), ages8 to 82 years (mean, 58.9 years), with a bodyeight of 143 to 179 cm (mean, 165 cm), bodyeight of 48.9 to 99.3 kg (mean, 68.2 kg), and aody mass index of 17.9 of 35.6 (mean, 25.0)articipated in this study. Seven patients werereated with bicarbonate hemodialysis; 12 werereated with hemodiafiltration. Patients werereated with a 3 dialysis/week schedule, 3 to 4ours long for each session. All patients had nullesidual renal function and were totally anuric.
The study was conducted in accordance withhe ethical guidelines proposed by the Declara-ion of Helsinki. All patients gave their informedonsent.
tudy ProtocolPatients were examined on the occasion of aidweek dialytic session and at the next session.ody weight, serum urea, and serum creatinineere measured immediately before the beginningf the two dialysis sessions and 30 minutes afterhe end of the first session. Serum proteins, albu-in, prealbumin, myoglobin, and C-reactive
rotein were measured immediately before the

maa
MW
cmn
MI
aawpfuas
S
viIsaotcftdea
M
c(aBiatpio
T
TgsdoT
EptE
F
B(mtaBBop
C
iHpmDcasrBm(Iss
CM
e
DONADIO ET AL334
idweek session. BIA was performed immedi-tely before both dialytic sessions and 30 minutesfter the end of the midweek dialysis session.
easurement of Body Height andeightBody height was measured at the nearest 0.5
m using a standard stadiometer; weight waseasured with an electronic bed scale at theearest 0.1 kg.
easurement of Electrical Bodympedance
Four electrodes were placed on the right handnd foot,4 or on the side contralateral to therteriovenous fistula, of supine patients, andhole-body BIA was measured with sf and mflethysmographs. The measurements were per-ormed immediately before the start and 30 min-tes after the end of a midweek dialytic session,nd immediately before the start of the nextession, 2 days later.
ingle-Frequency Impedance AnalyzerResistance and reactance, which are the two
ectors of impedance, were measured with an sfmpedance analyzer (STA-BIA, Akern, Florence,taly), using a low-amplitude alternate current atingle frequency (0.8 mA, 50 KHz). It is generallycknowledged that resistance depends positivelyn fat content of the body and negatively fromotal body fluids. Reactance, which expresses theapacitance of the body, is positively dependentrom the number of cell membranes. In additiono resistance and reactance values, this apparatusisplays a value of BCM, estimated from theselectrical data, without knowledge of the heightnd weight of the patients.
ultifrequency Impedance AnalyzerTotal body electrical impedance to an alternate
urrent (0.2 mA) with four different frequencies5, 50, 100, and 200 KHertz) was measured using
multifrequency analyzer (Quadscan 4000,odystat, UK). It is generally acknowledged that
mpedance is low in the presence of a highmount of body fluids. In particular, impedanceo the passage of a high-frequency current de-ends on total body fluids, whereas impedance tontroduction of a low-frequency current depends
nly from extracellular fluids. sotal and Extracellular Body WaterPredialysis volume of TBW was estimated (e
BW) according to Chertow et al7 from age,ender, height, predialysis weight, and diabetestatus. In the same patients, predialysis and post-ialysis values of TBW were obtained by meansf the sf BIA (sf TBW) and by the mf BIA (mfBW).Because no formula is available for predicting
CW from anthropometric data, predialysis andostdialysis values of ECW volume were ob-ained only by means of BIA: sf ECW and mfCW.
at-Free Mass and Body Cell MassPredialysis and postdialysis values of FFM and
CM volume were obtained by means of sf BIAsf FFM and sf BCM) and mf BIA (mf FFM andf BCM), using the different manufacturer equa-
ions that combine electric data with body weightnd height of patients. An additional value ofCM (sf1 BCM) was directly obtained with sfIA apparatus from electric measurements, with-ut knowledge of the body weight and height ofatients.
linical Chemistry DeterminationsSerum creatinine and urea were measured us-
ng a standard autoanalyzer method (Crea Roche,itachi 917; Urea Roche, Hitachi 917). Serum
realbumin was measured with a nephelometricethod (N Antiserum to human prealbumin,ade Behring, Italy). Serum total protein con-
entration was measured by the biuret method,nd albumin percentage was determined by den-itometry, after electrophoretic separation on aga-ose gel of plasma proteins (Hydragel, Sebia,enelux). Plasma myoglobin was determined byeans of a sandwich immune enzymatic method
Access Myoglobin; Beckman Coulter, Milan,taly). Serum C-reactive protein level was mea-ured with a nephelometric method (N Highensitivity CRP, Dade Behring, Italy).
reatinine Generation, Creatinineetabolism, and Creatinine Index
Creatinine is produced by muscles and isxcreted almost exclusively via the kidneys. In
teady-state conditions, 24-hour urinary creat-
itaMbdupntmda
lcetvTnmtbfi
C
md
nttd
lt
D
vr
P
cbb
ts
S
a
stvsiv
opttsitqaarppniwt
T
TTitT((m9TL
T
ESTIMATE OF BODY WATER COMPARTMENTS 335
nine excretion equals creatinine production,hus it is commonly measured to assess themount of muscle mass.8,9 Similarly, in anuricHD patients, creatinine appearance in the
lood in the interdialytic period or in theialysate during the dialytic session may besed to assess creatinine generation. In theseatients, creatinine also undergoes an extrare-al degradation. Creatinine generation plus ex-rarenal degradation of creatinine (or creatinineetabolism) gives the value of creatinine pro-
uction, which can be used to assess themount of muscle mass in MHD patients.10
Creatinine generation (mg/24 h) was calcu-ated in MHD from the increase in serumreatinine, in the interdialytic period from thend of the midweek dialysis to the beginning ofhe next dialysis session, assuming a distributionolume of creatinine equal to the volume ofBW, because it has been shown that creati-ine distribution space is very close to TBWeasured by BIA.11 Serum creatinine concen-
ration at the end of dialysis was adjusted on theasis of the decrease in TBW caused by ultra-ltration during dialysis.
reatinine generation (mg ⁄ 24h)
� � Serum creatinine � TBW � 24 h � t (h)
� t (h): time interval between the end of theidweek dialysis and the beginning of the next
ialysis session.Creatinine metabolism (mg/24 h), or extrare-
al degradation rate, was estimated from an ex-rarenal clearance of 0.038 L/kg BW/ 24 h12 andhe average creatinine concentration in the inter-ialytic period.11
Finally, creatinine index (mg 24/h) was calcu-ated as creatinine generation plus creatinine me-abolism.
ialytic EfficiencyDialytic efficiency was calculated as single-pool
ariable volume Kt/V and as a urea reductionatio with the standard formulas.
rotein Catabolic RateNormalized protein catabolic rate (nPCR) was
alculated from the interdialytic increase in ureaetween the end of the midweek session and the
eginning of the next dialysis session, and the fime interval between the two samples with thetandard formula.
tatistical AnalysisThe linear correlation and the agreement13
mong the different measurements were tested.The Student’s t-test was used to evaluate the
tatistical significance of the differences betweenhe mean values of different groups of data. A Palue lower than .05 was considered statisticallyignificant. Statistical analysis was performed us-ng MedCalc Software, Mariakerke, Belgium,ersion 6.00.016, 2000.
ResultsThe results (median, mean, and range values)
f sf BIA and mf BIA and of the biochemicalarameters commonly measured in MHD pa-ients to assess the adequacy of renal replacementherapy, to evaluate inflammatory and nutritionaltatus, and the protein catabolic rate are reportedn Table 1. The values of Kt/V and urea reduc-ion ratios indicate that patients received an ade-uate dose of dialysis. Serum levels of CRP, oftenbove the upper level of reference range, suggestn inflammatory status in most patients. The wideanges found for serum creatinine, urea, albumin,realbumin, and nPCR indicate that this group ofatients comprises either malnourished or well-ourished subjects. The wide ranges of creatininendex and of serum myoglobin values suggestide differences in the amount of muscle mass in
he examined patients.
otal Body Water VolumesA high linear correlation was found between e
BW values and both sf TBW (r � 0.967) and mfBW (r � 0.971). However, the agreement plots
ndicated a statistically significant difference be-ween anthropometrically estimated values ofBW and those measured with either sf BIA
mean difference, �1.72 L, P � .01) or mf BIAmean difference, �1.67 L, P � .01). Further-ore, the ranges of agreement (which encompass
5% of patients) between e TBW and either sfBW or mf TBW were very wide (10.7 and 8.27, respectively).Sf BIA and mf BIA gave very similar results for
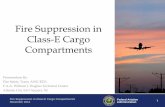
BW volumes measured predialysis (Fig 1). In
act, a very high linear correlation was found
brwTfcsL
E
fetacmF
ESsmem
ibo
F
tpi0
TS
s
DONADIO ET AL336
etween sf TBW and mf TBW, the slope of theirelationship was near 1, and the intercept valueas near 0. Thus, mean values of sf TBW and mfBW were not significantly different (mean dif-
erence, 0.04 L). Very high correlation and goodoncordance were also found between postdialy-is measurements, with a mean difference of 0.45
(Fig 1).
xtracellular Body Water VolumesPredialysis sf BIA and mf BIA gave quite dif-
erent results for ECW volumes (Fig 1). In fact,ven if a high linear correlation was found be-ween these two measurements, the analysis ofgreement plots indicates a relevant and statisti-ally significant difference between sf ECW andf ECW (mean difference, �1.22 L, P � .01).
able 1. Clinical Chemistry Determinations, Body Wingle-Frequency and Multifrequency Analysis at M
Pre-dialysisSerum creatinine, mg/dLSerum urea, mg dLSerum prealbumin, mg/dLSerum albumin, g/LSerum C-reactive protein, mg/dLSerum myoglobin, ng/mLBody weight, kgsf TBW, Lmf TBW, Lsf ECW, Lmf ECW, Lsf FFM, kgmf FFM, kgsf BCM, kgmf BCM, kg
PostdialysisBody weight, kgsf TBW, Lmf TBW, Lsf ECW, Lmf ECW, Lsf FFM, kgmf FFM, kgsf BCM, kgmf BCM, kgKt/VUrea reduction ratio, %n Protein catabolic rate, g/kg
BW/dayCreatinine index, mg/24 hCreatinine index, mg/kg BW
Abbreviations: TBW, total body water; ECW, extraceinglefrequency BIA; mf, multifrequency BIA.
urthermore, the range of agreement between sf M
CW and mf ECW was also very wide (6.9 L).lightly better results were found after the dialy-is. In fact, at this time the values of sf ECW andf ECW were not statistically different. How-
ver, the range of agreement between the twoeasures was 6.0 L.Lower values of TBW and ECW were found
n female patients. In any case, the relationshipetween sf BIA and mf BIA seems similar to thatf male patients.
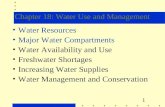
at-Free MassA very high linear correlation was found be-
ween sf FFM and mf FFM, measured eitherredialysis or postdialysis (Fig 2). However, thentercept values were significantly different from
(�5.64 kg predialysis, �8.08 kg postdialysis).
t, and Body Impedance Analysis Performed withek Dialytic Session
n Mean Range
10.4 4.8–15.8157.3 57–24230.4 20.2–3839.4 34.0–45.01.6 0.3–7.3
248.4 82–67968.2 48.9–99.337.5 20.8–52.537.6 22.8–51.317.9 12.2–26.016.7 11.5–21.849.1 28.5–71.847.7 24.9–70.923.3 7.7–41.628.9 17.1–42.1
64.9 45.9–95.033.6 20.7–45.334.0 21.4–45.014.9 10.1–23.815.0 10.8–19.343.9 26.9–61.943.4 22.3–64.522.3 10.0–37.127.1 15.9–38.4
7 1.51 1.19–2.2070.8 63.9–83.9
6 1.06 0.70–1.44
1251 535–206619.0 10.2–29.6
water; FFM, fat-free mass; BCM, body cell mass; sf,
eighidwe
Media
10.916632.2391.1
24664.839.938.818.016.750.148.322.730.9
61.535.836.715.315.645.645.423.429.71.4
69.91.0
136020.0
llular
ean values of predialysis sf FFM and mf FFM

Fewca
ESTIMATE OF BODY WATER COMPARTMENTS 337
igure 1. TBW and ECW volumes (L) measured before a midweek dialysis session and 30 minutes after thend of dialysis with BIA. sf TBW and sf ECW are measured with sf BIA; mf TBW and mf ECW are measuredith mf BIA (Œ, female patients; ●, male patients). The equations for linear correlations and the correlationoefficients are reported on the correlation plots (left side). The mean differences and the ranges of
greement (mean difference � 1.96 SD) are reported on the agreement plots (right side).
Fa●ca
DONADIO ET AL338
igure 2. FFM and BCM volumes (kg) measured before and after a midweek dialysis session with BIA. sf FFMnd sf BCM are measured with sf BIA; mf FFM and mf BCM are measured with mf BIA (Œ, female patients;, male patients). The equations for linear correlations and the correlation coefficients are reported on theorrelation plots (left side). The mean differences and the ranges of agreement (mean difference � 1.96 SD)
re reported on the agreement plots (right side).
wdtFpimbs
B
fwatvctaoBrmr
tfplwts.akaw
rpanoptlABtw
taaltms.hrmiFs.tPTmtop
bpd0r�cf0OdPc
wucwiBmoepa
ESTIMATE OF BODY WATER COMPARTMENTS 339
ere slightly but significantly different (meanifference, mf-sf FFM � 0.45 kg, P � .05), andhe range of agreement between sf FFM and mfFM was quite wide (7.94 kg). Mean values ofostdialysis sf FFM and mf FFM were not signif-cantly different; however, the range of agree-ent between sf FFM and mf FFM continued to
e quite wide (11.27 kg), and the agreementeems different in female and male subjects.
ody Cell MassPredialysis sf BIA and mf BIA gave quite dif-
erent results for BCM volumes; mf BCM valuesere higher than sf BCM values. In fact, even ifhigh and statistically significant linear correla-
ion was found between mf BCM and sf BCMalues (Fig 2), the analysis of agreement plots andorresponding data indicate a relevant and statis-ically significant difference between mf BCMnd sf BCM (P � .001). Furthermore, the rangef agreement of mf BCM with sf BCM and sf1CM was also very wide (17.58 and 18.55 kg,
espectively). Postdialysis measurement of sf andf BCM gave no particular improvement with
espect to predialysis measures.A very high linear correlation was found be-
ween sf BCM and sf1 BCM (obtained directlyrom electrical data of sf BIA), either measuredredialysis or postdialysis. The slope of their re-ationship was close to 1, and. the intercept valueas not significantly different from 0. However,
he mean values of sf BCM and sf1 BCM werelightly but significantly different (�1.82 kg, P �001 predialysis; �1.21 kg, P � .001 postdialysis)nd the ranges of agreement were 2.81 and 2.32g, respectively. The results of BCM show a poorgreement between the measurements obtainedith sf and mf BIA.Attempting to establish the kind of BIA appa-
atus, the time of BIA measurement, and thearameters of body composition that are moredequate for evaluating the muscle mass and theutritional status of MHD patients and the resultsf FFM and BCM obtained with sf and mf BIA,redialysis and postdialysis, were compared withhe values of creatinine index and with serumevels of myoglobin, prealbumin, and albumin.ll of the different measurements of FFM andCM had statistically significant linear correla-
ions with the values of creatinine index (Fig 3),
hich is a marker of the amount of muscle mass Ehat a patient has. In particular, the results of FFMnd BCM obtained with mf BIA, both predialysisnd postdialysis, had higher values of the corre-ation coefficient r with the creatinine index thanhe results of sf BIA. Furthermore, the values off BCM, either predialysis or postdialysis, had a
ignificant correlation (predialysis, r � 0.696, P �001; postdialysis, r � 0.688, P � .005), slightlyigher than that of sf BCM (r � 0.689, P � .005;� 0.617, P � .005) with the serum levels ofyoglobin, a low-molecular-weight protein that
s produced by muscle cells. The values of mfFM, either predialysis or postdialysis, also had aignificant correlation (predialysis, r � 0.666, P �005; postdialysis, r � 0.663, P � .005), similar tohat of sf BCM (r � 0.651, P � .005; r � 0.656,
� .005) with the serum levels of myoglobin.hese data indicate that mf BCM is the measure-ent of body composition best correlated with
he amount of muscle mass, and the significancef the correlation is similar for predialysis andostdialysis measurements.Statistically significant correlations were found
etween serum levels of prealbumin and eitherredialysis or postdialysis values of sf FFM (pre-ialysis, r � 0.5784, P � .01; postdialysis, r �.5806, P � .01), mf FFM (r � 0.5927, P � .01;� 0.5665, P � .05) and mf BCM (r � 0.560, P
.05; r � 0.5566, P � .05). A significantorrelation with serum levels of prealbumin wasound for postdialysis values of sf BCM (r �.5265, P � .05, but not predialysis sf BCM.nly sf BCM values, both predialysis and post-
ialysis, were significantly correlated (r � 0.514,� .05; r � 0.5477, P � .05) with serum
oncentrations of albumin.
DiscussionBody mass index (BMI), which relates bodyeight to squared height, is the most commonlysed parameter to evaluate nutritional status. BMIan give useful information in population studies,hereas it is less useful in the evaluation of
ndividual subjects. In fact, in overweight patientsMI cannot discriminate among increase of fat,uscle mass, or body water volumes. On thether hand, in malnourished patients BMI under-stimates the severity of malnutrition, because inrotein-energy malnutrition the decrease of fatnd muscle mass is accompanied by an increase in
CW volume. Therefore, an accurate evaluation
Fmmc
DONADIO ET AL340
igure 3. Creatinine index (mg/24 h) versus FFM and BCM volumes (kg), measured before and after aidweek dialysis session with BIA. sf FFM and sf BCM are measured with sf BIA; mf FFM and mf BCM areeasured with mf BIA (Œ, female patients; ●, male patients). The equations for linear correlations and the
orrelation coefficients are reported on the correlation plots.

oatDpfbctfltmfit
tnrfllaccfltoBsrwammsBigggfDaelrngbatT
BE
sotdpttwHftaeeai(ttBasttawme
ccBdw
tpfMaaagpdpds
ESTIMATE OF BODY WATER COMPARTMENTS 341
f nutritional status needs a precise quantitativessessment of the constituents of body mass andhe evaluation of the distribution of body fluids.EXA is a recommended method for body com-osition analysis in adult dialysis patients.1–2 Inact, DEXA allows measurement of fat mass, leanody mass, and bone mass. However, DEXAannot give an exhaustive evaluation of nutri-ional status because it does not measure bodyuids compartments and body cell mass, which ishe edema-free lean body mass. Thus, DEXAeasurements are commonly used to assess body
at. It is worthy of notice that not all malnour-shed patients present a decrease in body fat con-ent.
BIA is a simple and nonexpensive techniquehat should allow a thorough evaluation of theutritional status because it estimates the mostelevant components of body mass and the bodyuids compartments. However, data from pub-
ished papers aimed at assessing the adequacy of sfnd mf BIA for the evaluation of body fluidsompartments (TBW and ECW) and of bodyomposition (FFM and BCM) seem quite con-icting. In fact, results in healthy subjects indicatehat TBW can be adequately estimated by meansf sf BIA, and ECW by means of dual-frequencyIA.14 Furthermore, bioimpedance spectroscopy
eems to improve the prediction of ECW.15 Inenal transplantation patients mf BIA, comparedith isotope dilution techniques, resulted in suit-
ble measurement of TBW, whereas the agree-ent between the isotope dilution method andf BIA for the measurement of ECW was not
atisfactory.16 In renal transplantation patients, sfIA was found adequate for highlighting changes
n body compartments not only in patients withraft dysfunction, but even in those with goodraft function.17,18 In hemodialysis patients, aood correlation and excellent agreement wereound between TBW measured by sf BIA and
2O dilution.5 Mf BIA seemed very useful inssessing both TBW and body composition innd-stage renal disease patients.6 In patients onong-term dialysis therapy, using DEXA as aeference method, the method of skinfold thick-ess was preferable over BIA, which showedender-specific variability in the assessment ofody fat.19 Other articles report that in hemodi-lysis patients the agreement between mf BIA andracer dilution techniques in the assessment of
BW and ECW is unsatisfactory; in any case, mf dIA adequately predicted acute changes inCW.20
In addition to the conventional whole-bodyf BIA, a new approach for routine monitoringf the body fluid variation in the single pa-ients, based on the analysis of the bivariateistribution of the impedance vector, has beenroposed21 and applied in hemodialysis pa-ients.22 This method avoids potential difficul-ies caused by the use of prediction equations,hich are necessary for classic BIA analysis.owever, in a large population study per-
ormed on normal subjects and on dialysis pa-ients, the results obtained by means of phasengle analysis, bivariate analysis, and predictionquation method, using sf BIA, corroborateach other.23 On the other hand, the phasengle and bivariate analysis do not give numer-cal values for the different body compartmentsFFM, BCM, TBW, ECW, etc), thus the in-erpretation of results and of the variations inhe time is less intuitive than with conventionalIA. Furthermore, the measurement of phasengle and the bivariate analysis need the mea-urement of both resistance and reactance vec-ors of impedance, which are measurable withhe sf BIA apparatus but not with the mf BIApparatus that we used. For all of these reasons,e decided to analyze all of our BIA measure-ents with the classic method of prediction
quations.The ideal time to perform the analysis of body
omposition by means of BIA has not beenlearly established. It has been reported that theIA can be appropriately performed in the post-ialysis period of 2 hours in patients treated onlyith a standard diffusive technique.24
Our data indicate a similar relationship be-ween sf and mf TBW, both predialysis andostdialysis. In fact, the present study was per-ormed in a small group of nonhomogeneous
HD patients, differing in age, dialysis vintagend technique, nutritional status, and possibly inchievement of “ideal” body weight. In spite ofll of these difference, sf BIA and mf BIA clearlyave very similar values for TBW, measuredredialysis and postdialysis at a midweek hemo-ialysis session. To the contrary, in our patients,redialysis TBW, estimated from anthropometricata, gave significantly different results from bothf TBW and mf TBW. For practical reasons, we
id not measure, as a gold standard, the TBW by
trtsomftiFsuetstaBvFE
immmnhrvdmwt
tpecimawFtwscnlmc
sn
wraotdtolswmaicepcttcmswptB
abtw
w(oagcmncdiwsiw
DONADIO ET AL342
he D2O dilution method. However, it seemseasonable to assume that sf and mf TBW valueshat were very similar to each other, being mea-ured by means of sf BIA and mf BIA, which relyn very different physical principles, are probablyore accurate than TBW volumes estimated
rom anthropometric data. These results confirmhat BIA provides more consistent and reproduc-ble results than standard anthropometry alone.25
urthermore, our results agree with the reportedignificant overestimation of modeled urea vol-me in MHD patients by anthropometricallystimated TBW.26 In any case, BIA is consideredhe most accurate surrogate marker for the mea-urement of TBW in end-stage renal failure pa-ients.6 To the contrary, BIA seems not fullydequate for measuring ECW. In fact, sf and mfIA gave significantly different results for ECWolumes, particularly when measured predialysis.urther studies should address the assessment ofCW volumes in hemodialysis patients.Body cell mass, or edema-free lean body mass,
s the constituent of body mass with the highestetabolic activity. Muscle mass represents theajor constituent of BCM. Thus, the measure-ent of BCM can give important information onutritional status of MHD patients, who are atigh risk of protein-energy malnutrition witheduction of muscle mass and increase in ECWolumes. Because the value of BCM is indepen-ent from the amount of ECW, it should beore adequate than the measurement of FFM,hich is influenced by ECW, to assess malnutri-
ion in MHD patients.In normal healthy subjects and in patients with
he human immunodeficiency virus, body com-osition (TBW, FFM, and BCM) was accuratelystimated with sf BIA, and such estimates areonsidered sufficiently precise for use in clinicalnvestigation and practice.27 Similarly, using anf BIA–derived equation, it was possible to
ccurately estimate FFM and total body nitrogen,hich is a reference marker of nutritional status.6
urthermore, the measurements of BCM, ob-ained with sf BIA, were in excellent agreementith those obtained with deuterium oxide and
odium bromide isotope dilution methods, indi-ating that BIA is a valid and reliable method ofutritional assessment in MHD patients.5 Pub-
ished data seem to indicate that both sf BIA andf BIA can be used for the analysis of body
omposition. However, there are no exhaustive B
tudies addressed to compare these two tech-iques.In the present study, body composition analysisith sf BIA was compared with mf BIA. The
esults of FFM and mainly those of BCM showedpoor agreement between the measurements
btained with sf and mf BIA. However, all ofhese measurements significantly correlated withifferent biochemical indicators of nutritional sta-us. FFM and BCM values, particularly thosebtained with mf BIA, were more strictly corre-
ated with biochemical markers of muscle mass,uch as creatinine index and myoglobin, thanith indicators of visceral proteins, such as albu-in and prealbumin. These results, which prob-
bly depend on the fact that muscle mass is anmportant constituent of FFM and the majoronstituent of BCM, are in agreement with thextensive study by Chertow et al in hemodialysisatients.28 These investigators found that BCMorrelated more closely with serum creatininehan with albumin and prealbumin concentra-ions, suggesting that bioimpedance and bio-hemical markers capture somewhat different di-ensions of nutritional status. Our previous data
howed that in chronic kidney disease patientsith different degrees of renal function, it isossible to estimate the daily creatinine produc-ion and excretion from the values of FFM andCM obtained with sf-BIA.29–30
Preliminary data in healthy volunteers, using asreference method the measurement of total
ody potassium, suggest that it should be possibleo measure accurately BCM with sf or mf BIA,ith device-specific equations.31
The measurement of BCM obtained directlyith sf plethysmograph soft tissue analyzer
STA)-BIA, without the need for measurementf height and weight, could greatly simplify thenalysis of body composition in particularroups of patients, such as those in intensiveare units. Our results indicate that this esti-ate of BCM was strictly correlated with butot identical to the standard BCM obtained byombining body weight and height to electricalata of sf BIA. The few other data availablendicate that this estimate of BCM is correlatedith BCM measured from total body potas-
ium, although differing significantly from thedentity, whereas the BCM values obtainedith standard sf BIA were more similar to
CM measured by total body potassium; thus
tc
cBebbBwapm
ctorbbmpBdtam
fD
sT
u
tc
tt
mK
aw
m4
l
hr4
mnp
l
ac
cpt
ab
Bat1
as1
ip
CamN
bp2
mR
sJ
eCs
ed
t
ESTIMATE OF BODY WATER COMPARTMENTS 343
his simplified method cannot be used withonfidence.32
As far as body composition analysis is con-erned, the results of this study suggest that mfIA is more adequate than sf BIA for thevaluation of muscle mass in MHD patientsecause the highest correlations were foundetween data derived from mf BIA, namelyCM, and the creatinine index, which is aell-documented parameter of muscle mass,
nd serum myoglobin levels, which can beroposed as a simple tool for estimating muscleass in MHD patients.
ConclusionsTBW volume can be estimated with enough
onfidence from both sf and mf BIA in main-enance hemodialysis patients. On the contrary,ne should be very prudent in evaluating theesults of body water compartments analysisecause the measurement of ECW volume maye significantly different depending on theethod used. Both sf and mf BIA estimate
arameters of body composition, FFM, andCM, which are significantly correlated withifferent indicators of muscle mass and nutri-ional status. However, mf BIA seems moredequate than sf BIA for estimating muscleass in dialysis patients.
References1. Clinical practice guidelines for nutrition in chronic renal
ailure. K/DOQI, National Kidney Foundation. Am J Kidneyis 35(suppl 2):s1-s140, 20002. Locatelli F, Fouque D, Heimburger O, et al: Nutritional
tatus in dialysis patients: A European consensus. Nephrol Dialransplant 17:563-572, 20023. Pupim LB, Ikizler TA: Assessment and monitoring of
remic malnutrition. J Ren Nutr 14:6-19, 20044. Lukaski HC, Bolonchuk WW, Hall CB, et al: Validation of
etrapolar bioelectrical impedance method to assess human bodyomposition. J Appl Physiol 60:1327-1332, 1986
5. Chertow GM, Lowrie EG, Wilmore DW, et al: Nutri-ional assessment with bioelectrical impedance analysis in main-enance hemodialysis patients. J Am Soc Nephrol 6:75-81, 1995
6. Cooper BA, Aslani A, Ryan M, et al: Comparing differentethods of assessing body composition in end-stage renal failure.idney Int 58:408-416, 20007. Chertow GM, Lazarus JM, Lew NL, et al: Development ofpopulation-specific regression equation to estimate total bodyater in hemodialysis patients. Kidney Int 51:1578-1582, 1997
8. Keshaviah PR, Nolph KD, Moore HL, et al: Lean body tass estimation by creatinine kinetics. J Am Soc Nephrol:1475-1485, 19949. Forbes GB, Bruining GJ: Urinary creatinine excretion and
ean body mass. Am J Clin Nutr 29:1359-1366, 197610. Kaizu Y, Ohkawa S, Kumagai H: Muscle mass index in
aemodialysis patients: A comparison of indices obtained byoutine clinical examinations. Nephrol Dial Transplant 17:442-48, 200211. Canaud B, Garred LJ, Argles A, et al: Creatinine kineticodeling: A simple and reliable tool for the assessment of proteinutritional status in haemodialysis patients. Nephrol Dial Trans-lant 10:1405-1410, 199512. Mitch WE, Collier VU, Walser M: Creatinine metabo-
ism in chronic renal failure. Clin Sci 58:327-335, 198013. Bland JM, Altman DG: Statistical methods for assessing
greement between two methods of clinical measurement. Lan-et i:307-310, 1986
14. Simpson JA, Lobo DN, Anderson JA, et al: Body waterompartment measurements: A comparison of bioelectrical im-edance analysis with tritium and sodium bromide dilutionechniques. Clin Nutr 20:339-343, 2001
15. Matthie J, Zarowitz B, De Lorenzo A, et al: Analyticssessment of the various bioimpedance methods used to estimateody water. J Appl Physiol 84:1801-1816, 199816. van den Ham ECH, Kooman JP, Christiaans MHL, et al:
ody composition in renal transplant patients: Bioimpedancenalysis compared to isotope dilution, dual energy X-ray absorp-iometry, and anthropometry. J Am Soc Nephrol 10:1067-1079,99917. Coroas A, de Oliveira JGG, Sampaio S, et al: Bioimped-
nce analysis highlights changes in body composition at the earlytages of impairment of kidney transplant function. J Ren Nutr4:157-163, 200418. Lucchesi A, Ardini M, Donadio E, et al: Nutritional status
n renal transplant recipients, evaluated by means of body com-osition analysis. Transplant Proc 33:3398-3399, 200119. Kamimura MA, Avesani CM, Cendoroglo M, et al:omparison of skinfold thickness and bioelectrical impedance
nalysis with dual-energy X-ray absorptiometry for the assess-ent of body fat in patients on long-term haemodialysis therapy.ephrol Dial Transplant 18:101-105, 200320. Cox-Reijven PL, Kooman JP, Soeters PB, et al: Role of
ioimpedance spectroscopy in assessment of body water com-artments in hemodialysis patients. Am J Kidney Dis 38:832-838,00121. Piccoli A, Rossi B, Pillon L, et al: A new method foronitoring body fluid variation by bioimpedance analysis: TheXc graph. Kidney Int 46:534-539, 199422. Mancini A, Grandaliano G, Magarelli P, et al: Nutritional
tatus in hemodialysis patients and bioimpedance vector analysis.Ren Nutr 13:199-204, 200323. Dumler F, Kilates C: Body composition analysis by bio-
lectrical impedance in chronic maintenance dialysis patients:omparison to the national health and nutrition examination
urvey III. J Ren Nutr 13:166-172, 200324. Di Iorio BR, Scalfi L, Terracciano V, et al: A systematic
valuation of bioelectrical impedance measurement after hemo-ialysis session. Kidney Int 63:2435-2440, 200425. Dumler F, Kilates C: Use of bioelectrical impedance
echniques for monitoring nutritional status in patients on main-
enance hemodialysis. J Ren Nutr 10:116-124, 2000
mma
ciN
n1
cr
cc
ai1
t
DONADIO ET AL344
26. Daugirdas JT, Green T, Depner TA, et al: Anthropo-etrically estimated total body water volumes are larger thanodeled urea volume in chronic hemodialysis patients: Effects of
ge, race, and gender. Kidney Int 64:1108-1119, 200327. Kotler DP, Burastero S, Wang J, et al: Prediction of body
ell mass, fat-free mass, and total body water with bioelectricalmpedance analysis: Effects of race, sex, and disease. Am J Clinutr 64(suppl):489s-497s, 199628. Chertow GM, Lazarus MJ, Lew NL, et al: Bioimpedance
orms for the hemodialysis population. Kidney Int 52:1617-621, 1997
29. Donadio C, Lucchesi A, Tramonti G, et al: Creatinine mlearance predicted from body cell mass is a good indicator ofenal function. Kidney Int 52:S166-S168, 1997
30. Donadio C, Lucchesi A, Tramonti G, et al: Prediction ofreatinine clearance from body composition analysis and plasmareatinine. Ren Fail 20:285-293, 1998
31. Dittmar M, Reber H: Validation of different bioimped-nce analyzers for predicting cell mass against whole-body count-ng of potassium (40K) as a reference method. Am J Hum Biol6:697-703, 2004
32. Ward LC, Heitmann BL: Assessment of body composi-ion by bioelectrical impedance analysis without the need for
easurement of height. Clin Nutr 20:21-26, 2001Top Related