








Languages
Pages
Legal

Emory University School of Medicine Department of Medicine
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Presents
EMORY CONFERENCE CENTER
ATLANTA

MICAH FISHER, MD Assistant Professor, Pulmonary and Critical Care
Emory University School of Medicine Section Chief, Emory University Hospital
JENNY HAN, MD, MSc Assistant Professor, Pulmonary and Critical Care
Emory University School of Medicine
GREG MARTIN, MD, MSc, FCCM Professor, Pulmonary and Critical Care
Associate Division Director for Critical Care Emory University School of Medicine
Director of Research, Emory Critical Care Center Section Chief, Grady Memorial Hospital
ASHISH MEHTA, MD, MSc Assistant Professor, Pulmonary and Critical Care
Emory University School of Medicine Medical Director, MICU, Atlanta VA Medical Center
GABRIEL NAJARRO, MMSc, PA-C Adjunct Assistant Professor, Family and Preventative Medicine
Emory University School of Medicine Lead Affiliate Provider, Cardiac Critical Care Unit
Emory Healthcare
MARINA RABINOVICH, PharmD, BCPS Critical Care Clinical Pharmacist Specialist, Grady Health System
PGY-1 Pharmacy Residency Coordinator President, SCCM Southeast Chapter
MARY D. STILL, MSN, APRN, FCCM Clinical Nurse Specialist Critical Care
Emory University Hospital
ADAM WEBB, MD Assistant Professor of Neurology and Neurosurgery
Emory University Hospital Medical Director, Neuroscience ICU, Grady Memorial Hospital
PLENARY LECTURERS
Kyle Gunnerson, MD
Dr. Kyle Gunnerson is Associate Professor in the Departments of Emergency Medicine, Anesthesiology, and Internal Medicine at the University of Michigan. He received his B.S. degree in Chemistry and Biology from Kansas Wesleyan University and his medical degree from the University of Kansas. Dr. Gunnerson trained in the combined Emergency Medicine/Internal Medicine program at Henry Ford Health System, after which he completed his critical care training at the University of Pittsburgh. He was a faculty member at Virginia Commonwealth University and served as the Division Chief of Critical Care in the Department of Anesthesiology, Associate Director of the Center for Adult Critical Care, Medical Director of the
Cardiac Surgery ICU, and the Medical Director for the ECMO program. Dr. Gunnerson’s research is funded by both industry and the federal government, focusing on early identification and resuscitation of patients in shock or at risk of organ dysfunction, including discovery and development of novel biomarkers, treatment of septic shock, utilization of ECMO, and the development of non-invasive therapeutic technologies. In 2013 Dr. Gunnerson moved to Michigan to work both in the CVICU as an intensivist and lead an ED-based Critical Care program. Dr. Gunnerson’s role as the Chief of the newly formed Division of Critical Care in the Department of Emergency Medicine at the University of Michigan spans the tripartite mission of high quality clinical care, education, and innovative and collaborative research. Uniquely, Dr. Gunnerson has helped guide the creation of a dedicated Emergency Department Critical Care Unit in cooperation with the adult inpatient ICU’s. This partnership has led to incorporate a formal multi-disciplinary critical care fellowship in both Anesthesiology and Internal Medicine. Dr. Gunnerson is a past member of the American Board of Internal Medicine Critical Care Subspecialty Committee and currently serves on the Council of the Society of Critical Care Medicine.
Kay Guntupalli, MD
Dr. Kalpalatha (Kay) Guntupalli is an endowed Professor in Pulmonary, Critical Care and Sleep at the Baylor College of Medicine in Houston, Texas. After obtaining her medical degree from Osmania Medical College in Hyderabad, India, she immigrated to the United States and completed her medical and subspecialty training in Washington D.C. and the University of Pittsburgh. She served on the faculty at Pittsburgh and at Emory University before joining Baylor and rising to the role of Division Chief for Pulmonary, Critical Care and Sleep Medicine while also serving as Fellowship Program Director. Her research interests are in
medical education and acute respiratory distress syndrome (ARDS) and she has published 150 articles in prestigious journals including the New England Journal of Medicine, Critical Care Medicine, CHEST and Annals of Internal Medicine. She has held many leadership positions including serving as President of the American College of Chest Physicians and as the first woman President of the American Association of Physicians of Indian Origin. Dr. Guntupalli has been recognized as a Master of the American College of Physicians and the American College of Chest Physicians, Master Clinician at Baylor, World Lung Health award from the American Thoracic Society and a Lifetime Achievement Award from the Indian Society of Critical Care Medicine. She is internationally recognized for her expertise and dedication to medical education and she continues her global work including at a hospital and medical school in India that she helped to found.
WILLIAM S. BENDER, MD Assistant Professor, Pulmonary and Critical Care Medicine Emory University School of Medicine BRUCE BRAY, RRT, RCP, FAARC Division Director, Respiratory Care, Emory ECMO Center, EKG, Pulmonary & ABG Laboratories, Emory University Hospital LAURENCE BUSSE, MD, MBA Assistant Professor, Pulmonary and Critical Care Medicine, Emory University School of Medicine, Medical Director, MSICU, Emory Saint Joseph’s Hospital MARK CARIDI-SCHEIBLE, MD Assistant Professor, Cardiothoracic Anesthesiology and Critical Care Medicine Emory University School of Medicine Program Director, Anesthesiology Critical Care Fellowship DAVID CARPENTER, MPAS, FCCM, DFAAPA, PA-C, CPC-A Physician Assistant - 5T South Surgical/Transplant ICU, Emory University Hospital MICHAEL CONNOR, JR., MD Divisions of Nephrology and Pulmonary and Critical Care Emory University School of Medicine LISA DANIELS, MD Assistant Professor, Pulmonary and Critical Care Medicine Emory University School of Medicine OMAR K. DANNER, MD, FACS Associate Professor of Surgery, Morehouse School of Medicine Chief, Department of Surgery at Grady Memorial Hospital ASHLEY DEPRIEST, MS, RD, LD, CNSC Department of Pharmacy, Northside Hospital NEAL DICKERT, MD, PHD Assistant Professor, Cardiology, Emory University School of Medicine ANNETTE ESPER, MD, MSC Associate Professor of Medicine, Pulmonary and Critical Care Medicine Emory University School of Medicine LEON EYDELMAN, MD Medical House Staff, Emory University School of Medicine DAVID GREEN, MD Assistant Professor, Pulmonary and Critical Care Medicine Atlanta VA Medical Center, Emory University School of Medicine WENDY GREENE, MD Associate Professor, Surgery, Emory University School of Medicine CASEY HALL, MD, MAT Neuroscience Critical Care, Neurology, Emory University School of Medicine ANTHONY HAWKINS, PHARMD, BCCCP Clinical Assistant Professor, Department of Clinical and Administrative Pharmacy University of Georgia College of Pharmacy
KILEY HODGE, BS, RRT-ACCS Education Coordinator, Respiratory Care, Emory University Hospital WILLIAM R. HUNT, MD Assistant Professor, Pulmonary and Critical Care Medicine Emory University School of Medicine ALLEY KILLIAN, PHARMD, BCPS Clinical Pharmacy Specialist, Surgical Intensive Care Unit, Emory University Hospital GERALD LEE, MD Assistant Professor, Pulmonary and Critical Care Medicine Emory University School of Medicine KIMBERLY D. MANNING, MD, FACP, FAAP Associate Professor of Medicine, Director, Distinction in Teaching and Leadership Program, Emory University School of Medicine ANEESH K. MEHTA, MD, FIDSA, FAST Associate Professor of Medicine, Associate Professor of Surgery Assistant Director Transplant Infectious Diseases, Emory University School of Medicine OMER MIRZA, MD Cardiology Fellow, Emory University School of Medicine DAVID J. MURPHY, MD, PHD Assistant Professor, Pulmonary and Critical Care Medicine Emory University School of Medicine KELLY OUELLETTE, PHARMD, BCPS Clinical Coordinator, Cardiology Clinical Pharmacy Specialist Emory Saint Joseph’s Hospital CEDERIC PIMENTEL, MD Assistant Professor, Neurology, Emory University School of Medicine TAMMIE E. QUEST, MD, FAAHPM Professor, Department of Emergency Medicine, Montgomery Chair in Palliative Medicine Emory University School of Medicine PRIYANKA RAJARAM, MD Assistant Professor, Pulmonary and Critical Care Medicine Emory University School of Medicine SAM SHARTAR, MSN, RN, CEN, CEM Senior Administrator, Office of Critical Event Preparedness and Response CEPAR, Emory University MICHAEL J. STENTZ, MD, MS Assistant Professor, Anesthesiology, Associate Director, Emory ECMO Program Emory University School of Medicine, Emory University RAM SUBRAMANIAN, MD Associate Professor of Medicine and Surgery, Medical Director, Liver Transplantation Emory University School of Medicine

2018 Southeastern Critical Care Summit
May 10‐11, 2018 in Atlanta, Georgia
Disclosure statement
It is the intent of Emory University School of Medicine to assure that its educational mission, and continuing medical education activities in particular, not be influenced by the special interest of individuals associated with its programs. All faculty members participating in a sponsored activity are expected to disclose to the audience two important points:
Any significant financial interest of other relationship with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in an educational presentation; any significant financial interest with any commercial supporters of the activity. (Significant financial interest or other relationships can include such things as grants or research support, employee, consultant, major stock holder, member of speaker’s bureau, etc.).
All disclosed financial relationships were reviewed for potential conflicts of interest. Actions were taken to resolve any identified conflicts. The following committee members and/or speakers have disclosed potential conflicts of interest.
The Ochsner Clinic Foundation relies upon invited speakers at all sponsored continuing medical education activities to provide information objectively and free from bias of conflict of interest. In accordance with ACCME and institutional guidelines pertaining to potential conflicts of interest, the faculty for this continuing medical education activity has been asked to complete faculty disclosure forms. In the event that some invited speakers indicate that they have a relationship which, in the context of the subject of their invited presentation, could be perceived as a potential conflict of interest, their materials have been peer reviewed in order to ensure that their presentations are free of commercial bias.
Speaker / Committee Member Role / Type Name of Company
Adam Webb, MD Consultant Bard Medical

The following sponsors have provided generous support for the
2018 Southeastern Critical Care Summit
Exhibitors:
GOLD SPONSORS
ACell, Inc
Allergan Pharmaceuticals
bioMérieux / Astute Medical
Boehringer - Ingelheim
Cheetah Medical Inc.
Edwards Lifesciences
GE Healthcare
Gilead Sciences
Hamilton Medical
Janssen Pharmaceuticals
La Jolla Pharmaceuticals
Masimo
Medtronic Medical Equipment
NxStage
Portola Pharmaceuticals
Southeastern Chapter of SCCM
DAY 1 – THURSDAY MAY 10, 2018
7:30 – 8:00 CONTINENTAL BREAKFAST 8:00 – 8:10 WELCOME AND INTRODUCTION FROM CO‐CHAIRS
8:10 – 9:20 FIRST MORNING SESSION
Alphabet soup of ICU scoring systems – D. Murphy
To bleed or not to bleed: ICU coagulopathy in the era of DOACs – K. Oullette
Antibiotic utilization: does this bug you? – A. Killian
9:20 – 9:30 MORNING BREAK AND POSTER EXHIBIT
9:30 – 10:40 SECOND MORNING SESSION
Beyond low tidal volume ventilation in ARDS – G. Martin
New vasopressor options in sepsis – L. Busse
Why is my patient swelling? Solving the mystery of angioedema – G. Lee
10:40 – 11:00 SECOND BREAK AND POSTER VIEWING
11:00 – 12:00 PLENARY LECTURE True ED‐ICU integration: The Michigan Experience Dr. Kyle Gunnerson, University of Michigan
12:00 – 1:00 LUNCH
1:00 – 2:10 FIRST AFTERNOON SESSION
Management of the organ donor: searching for the evidence – R. Subramanian
Beyond AKI: early renal replacement – PRO! – M. Connor
Beyond AKI: early renal replacement – CON! – M. Connor
2:10 – 2:20 AFTERNOON BREAK
2:20 – 3:30 SECOND AFTERNOON SESSION
Ethics in mass casualty and disaster triage – S. Shartar
Novel clinical diagnostics for infectious diseases – A. Mehta
Fancy footsteps: The palliative care dance – T. Quest
3:30 – 3:40 SECOND AFTERNOON BREAK
3:40 – 4:40 CHALLENGING ICU CASES
Diagnostic dilemma – J. Han
Management dilemma – M. Caridi‐Scheible Ethical dilemma – N. Dickert
4:40 – 5:00 WRAP‐UP AND RAFFLE DRAWING
Page 7
emoryhealthcare.org
Alphabet Soup of ICU Scoring Systems
David J. Murphy, M.D., Ph.D.Patient Safety Officer, Emory HealthcareMedical Director, EUHM Medical ICUAssistant ProfessorEmory University School of MedicineAtlanta, [email protected] conflicts to disclose
Southeast Critical Care SummitAtlanta, GA
May 10, 2018
emoryhealthcare.org
OBJECTIVES
• To understand the different uses for ICU scoring systems• To describe different data and assumptions underlying current ICU scoring
systems
• NOT a comprehensive discussion of– Statistical modeling– Disease specific scoring systems– Every general ICU scoring system ever created
2
MPM II
MPM III
emoryhealthcare.org
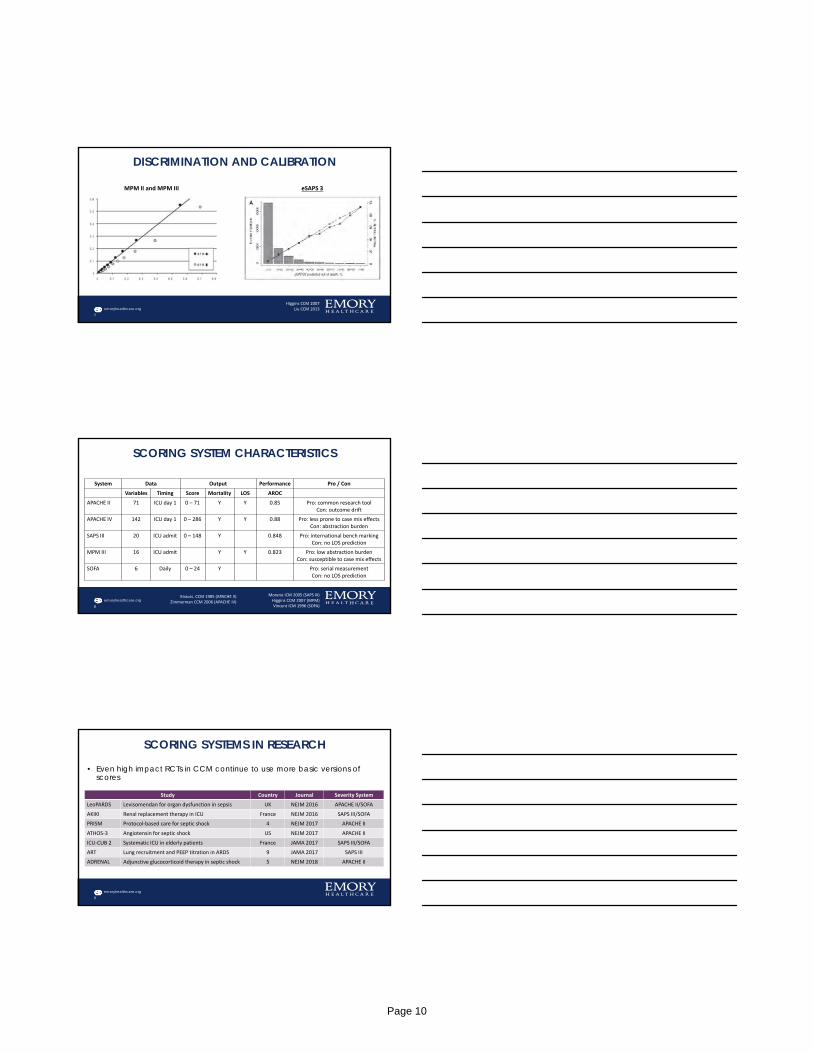
SEVERITY SCORING SYSTEM OVERVIEW
3
• Purpose– Evaluate the delivery of care and predict outcomes of groups of critically ill patients
admitted to ICUs• Use:
– Research: risk adjustment when evaluating efficacy of an intervention– Quality: comparing health care delivery effectiveness– Bedside: informing clinical actions when integrated with Early Warning Systems (EWS)
Data• Demographics• Acute physiology• Diagnostic data• Chronic health • Hospital course
Output• Severity score• Predicted outcomes
Scoring System EWSClinical Action
‐ Adjust monitoring‐ Trigger assessment
Page 8
emoryhealthcare.org
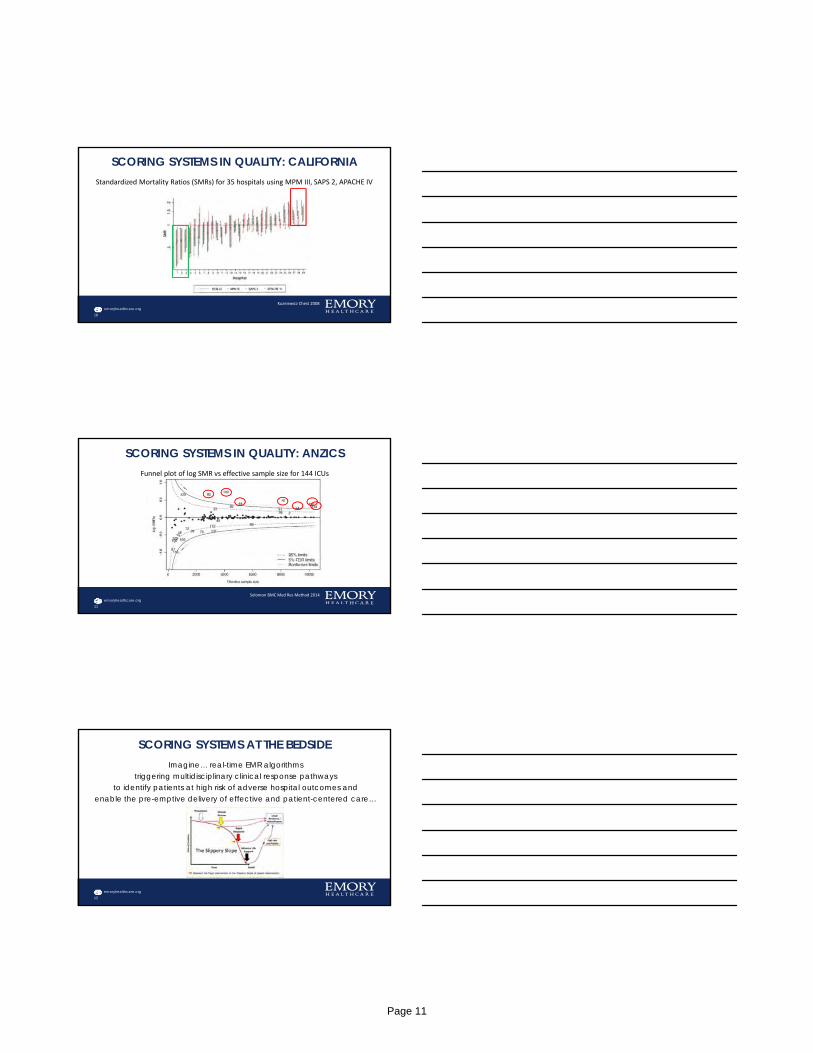
A BRIEF HISTORY OF SEVERITY SCORES
4
1980 1985 1990 1995 2000
• APACHE• SAPS• APACHE II
• SAPS II• MPM
• APACHE III• MODS• MPM II• ODIN
• SOFA• CIS
• SAPS III• APACHE IV• MPM III
emoryhealthcare.org
IDEAL SEVERITY SCORE ATTRIBUTES
• Motivated employer seeking an algorithm that – predicts everything that matters when it matters– applies to all patient population– uses easily / routinely recorded data– accurately predicts outcomes across a wide range of predictions– is easily available / free
Position still open
5
emoryhealthcare.org
DISCRIMINATION AND CALIBRATION
6
APACHE IVDiscrimination the ability of a model to separate individuals who develop outcome from those who do not.
Calibrationagreement between observed and predicted risk over the range of predicted risk
Zimmerman CCM 2006
Page 9
emoryhealthcare.org
DISCRIMINATION AND CALIBRATION
7
MPM II and MPM III eSAPS 3
Higgins CCM 2007Liu CCM 2013
emoryhealthcare.org
SCORING SYSTEM CHARACTERISTICS
System Data Output Performance Pro / Con
Variables Timing Score Mortality LOS AROC
APACHE II 71 ICU day 1 0 – 71 Y Y 0.85 Pro: common research toolCon: outcome drift
APACHE IV 142 ICU day 1 0 – 286 Y Y 0.88 Pro: less prone to case mix effectsCon: abstraction burden
SAPS III 20 ICU admit 0 – 148 Y 0.848 Pro: international bench markingCon: no LOS prediction
MPM III 16 ICU admit Y Y 0.823 Pro: low abstraction burdenCon: susceptible to case mix effects
SOFA 6 Daily 0 – 24 Y Pro: serial measurementCon: no LOS prediction
8
Moreno ICM 2005 (SAPS III)Higgins CCM 2007 (MPM)Vincent ICM 1996 (SOFA)
Knauss. CCM 1985 (APACHE II)Zimmerman CCM 2006 (APACHE IV)
emoryhealthcare.org
SCORING SYSTEMS IN RESEARCH
• Even high impact RCTs in CCM continue to use more basic versions of scores
9
Study Country Journal Severity System
LeoPARDS Levisomendan for organ dysfunction in sepsis UK NEJM 2016 APACHE II/SOFA
AKIKI Renal replacement therapy in ICU France NEJM 2016 SAPS III/SOFA
PRISM Protocol‐based care for septic shock 4 NEJM 2017 APACHE II
ATHOS‐3 Angiotensin for septic shock US NEJM 2017 APACHE II
ICU‐CUB 2 Systematic ICU in elderly patients France JAMA 2017 SAPS III/SOFA
ART Lung recruitment and PEEP titration in ARDS 9 JAMA 2017 SAPS III
ADRENAL Adjunctive glucocorticoid therapy in septic shock 5 NEJM 2018 APACHE II
Page 10
emoryhealthcare.org
SCORING SYSTEMS IN QUALITY: CALIFORNIA
10
Kuzniewicz Chest 2008
Standardized Mortality Ratios (SMRs) for 35 hospitals using MPM III, SAPS 2, APACHE IV
emoryhealthcare.org
SCORING SYSTEMS IN QUALITY: ANZICS
11
Solomon BMC Med Res Method 2014
Funnel plot of log SMR vs effective sample size for 144 ICUs
emoryhealthcare.org
SCORING SYSTEMS AT THE BEDSIDEImagine… real-time EMR algorithms
triggering multidisciplinary clinical response pathwaysto identify patients at high risk of adverse hospital outcomes and
enable the pre-emptive delivery of effective and patient-centered care…
12
Page 11

emoryhealthcare.org
SCORING SYSTEMS AT THE BEDSIDE• Multiple existing tools including:
– Modified Early Warning Score (MEWS)– National Early Warning Score (NEWS)– Between the Flags (BTF)
• Scores can be used to inform:– Frequency of vital sign monitoring– Transferring to higher levels of care– Rapid response system activation– Palliative care consults
13
emoryhealthcare.org
SCORING SYSTEMS AT THE BEDSIDE
14
Additional Saves Compared to BTF Additional False Positives Compared to BTF
Green Resuscitation 2018
emoryhealthcare.org
SCORING SYSTEMS AT THE BEDSIDE: MIXED RESULTS
Retrospective pre-post cohort in adultsHospital mortality decreased by 1.5%
15
Cluster randomized RCT in pediatric hospitalsNo change in hospital mortality
Schmidt BMJ Qual Saf 2015Parshuram JAMA 2018
Page 12
emoryhealthcare.org
EWS CONSIDERATIONS: NOT JUST THE ALGORITHM• Data source
– How in line with clinical care (EMR vs external system) will the EWS be?
• Analysis/Algorithm– What is the model performance of the selected EWS?– What is the optimal alert threshold selected? SN, SP, workup, detection– What type of quality control system is needed for ongoing scoring systems?
• Response– How mature or effective is the afferent arm (e.g. RRT) of the clinical response?– What is the training plan for end-users of the scoring system?– What are the response pathways? What is the follow up mechanism?– What is the communication plan for patients and families?
16
emoryhealthcare.org
ICU SEVERITY SCORING SYSTEMS…… can provide useful information to predict risk ICU patient populations.
… typically need calibration (updating) for local and contemporary use
… require careful consideration of data availability, model performance, and predicted outcomes prior to implementation.
… can be integrated into Early Warning Systems, but further investigation is required to evaluate usability and effectiveness.
17
Page 13
emoryhealthcare.org
To Bleed or Not to Bleed: ICU Coagulopathy in the era of DOACs
Kelly Ouellette, PharmD, BCPSClinical Coordinator
Cardiology Specialist (previously)Emory Saint Joseph’s Hospital
emoryhealthcare.org
DISCLOSURES
Disclosure statement:
I have nothing to disclose concerning possible financial or personal relationships with commercial entities (or their competitors) that may be referenced in this presentation.
2
emoryhealthcare.org
OBJECTIVES
• Discuss currently available Direct Oral Anticoagulants (DOACs) and bleeding rates
• Discuss appropriate monitoring parameters for DOACs
• Evaluate non-urgent and emergency reversal options for DOACs
• Review reversal options that will be available in the future
3
Page 14
emoryhealthcare.org
CURRENTLY AVAILABLE DOACS AND BLEEDING RATES
emoryhealthcare.org
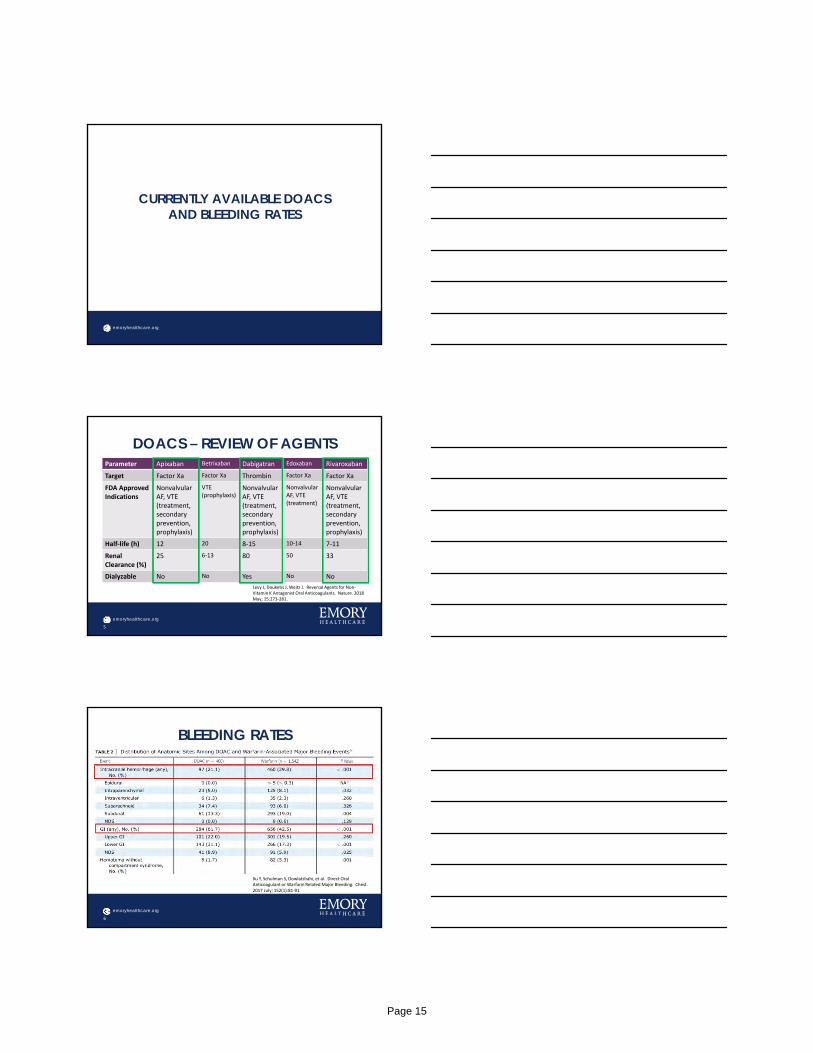
DOACS – REVIEW OF AGENTSParameter Apixaban Betrixaban Dabigatran Edoxaban Rivaroxaban
Target Factor Xa Factor Xa Thrombin Factor Xa Factor Xa
FDA ApprovedIndications
NonvalvularAF, VTE (treatment, secondary prevention,prophylaxis)
VTE (prophylaxis)
NonvalvularAF, VTE (treatment, secondary prevention,prophylaxis)
NonvalvularAF, VTE (treatment)
NonvalvularAF, VTE (treatment, secondary prevention,prophylaxis)
Half‐life (h) 12 20 8‐15 10‐14 7‐11
Renal Clearance (%)
25 6‐13 80 50 33
Dialyzable No No Yes No No
5
Levy J, Douketis J, Weitz J. Reversal Agents for Non‐Vitamin K Antagonist Oral Anticoagulants. Nature. 2018 May; 15:273‐281.
emoryhealthcare.org
BLEEDING RATES
6
Xu Y, Schulman S, Dowlatshahi, et al. Direct Oral Anticoagulant or Warfarin Related Major Bleeding. Chest. 2017 July; 152(1):81‐91
Page 15
emoryhealthcare.org
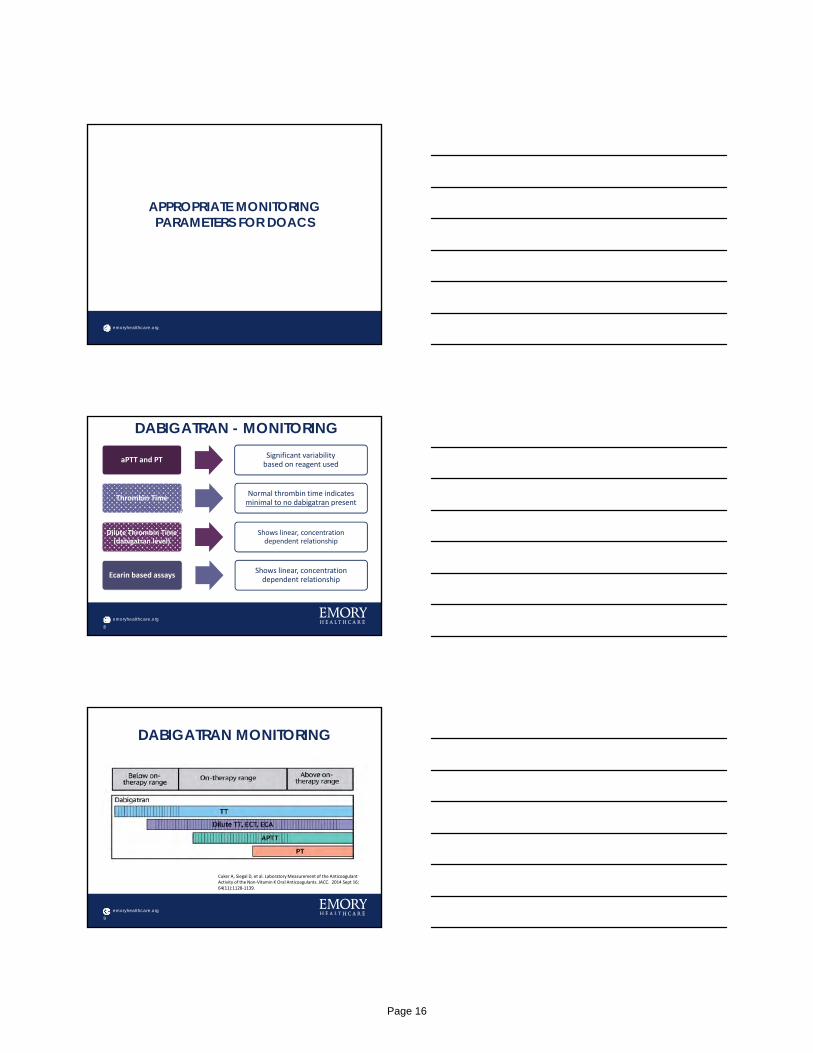
APPROPRIATE MONITORING PARAMETERS FOR DOACS
emoryhealthcare.org
DABIGATRAN - MONITORING
8
aPTT and PTSignificant variabilitybased on reagent used
Thrombin TimeNormal thrombin time indicates minimal to no dabigatran present
Dilute Thrombin Time(dabigatran level)
Shows linear, concentrationdependent relationship
Ecarin based assaysShows linear, concentration dependent relationship
emoryhealthcare.org
DABIGATRAN MONITORING
9
Cuker A, Siegal D, et al. Laboratory Measurement of the Anticoagulant Activity of the Non‐Vitamin K Oral Anticoagulants. JACC. 2014 Sept 16; 64(11):1128‐1139.
Page 16

emoryhealthcare.org
APIXABAN/RIVAROXABAN -MONITORING
10
aPTT and PT
‐ Effects vary depending on reagent/drug
‐ Poorly reflects the intensity of anticoagulation
‐ Can’t quantify drug plasma concentration
Anti‐factor Xa level (apixaban/
rivaroxaban level)
‐ Need drug specific calibrators
‐ Linear, concentration dependent relationship
emoryhealthcare.org
APIXABAN/RIVAROXABAN -MONITORING
11
Cuker A, Siegal D, et al. Laboratory Measurement of the Anticoagulant Activity of the Non‐Vitamin K Oral Anticoagulants. JACC. 2014 Sept 16; 64(11):1128‐1139.
emoryhealthcare.org
REVERSAL OPTIONSFOR DOACS
Page 17
emoryhealthcare.org
TO REVERSE OR NOT….Indications for reversal
• Life threatening bleeding
• Bleeding in a closed space/critical organ
• Persistent major bleeding despite local hemostatic measures
• Need for urgent intervention
• Emergency surgery
Avoid reversal
• Elective surgery
• GI bleeds responding to supportive measures
• High drug levels without associated bleeding
• Need for intervention that can be delayed enough to permit drug clearance
13
Levy JH, Ageno W, Chan NC, et al. When and how to use antidotes for the reversal of direct oral anticoagulants: guidance from the SSC of the ISTH. J Thromb Haemost 2016;14: 623–7.
emoryhealthcare.org
NON-URGENT REVERSAL
Supportive Care
• Fluid administration
Blood Products
• Packed red blood cells
• Fresh frozen plasma
14
Interruption of anticoagulation
• Assess timing of last dose of DOAC
Others
• Tranexamic acid
emoryhealthcare.org
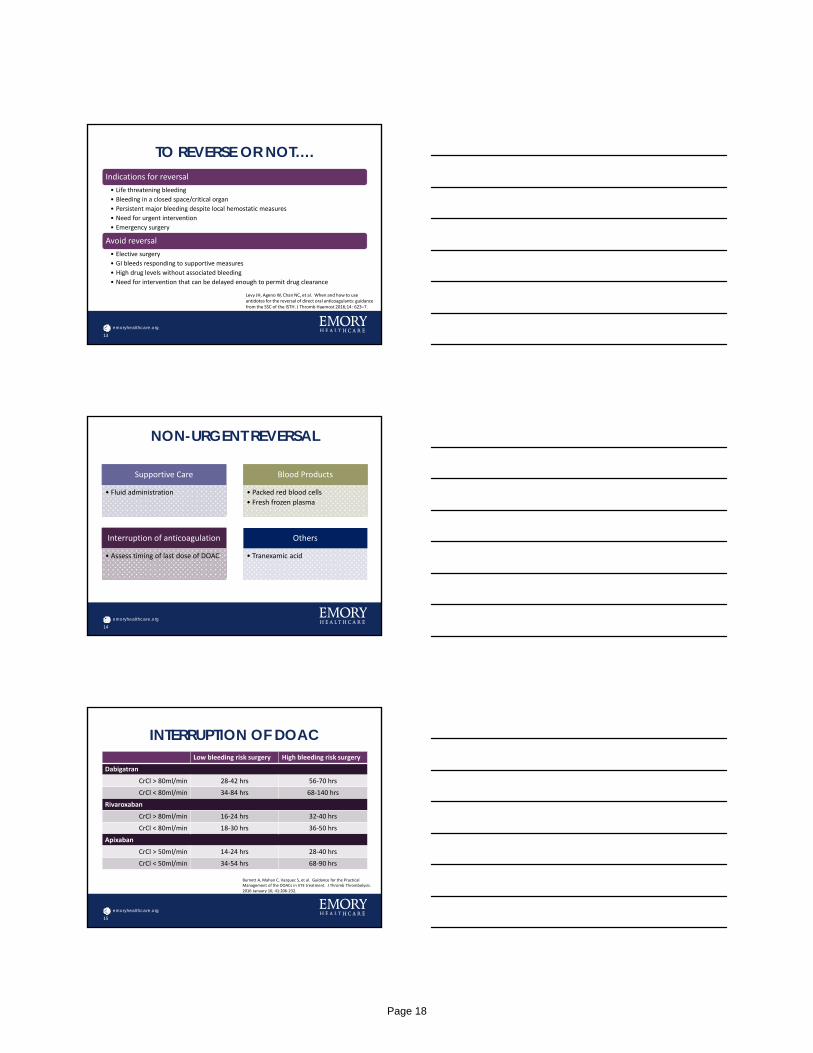
INTERRUPTION OF DOACLow bleeding risk surgery High bleeding risk surgery
Dabigatran
CrCl > 80ml/min 28‐42 hrs 56‐70 hrs
CrCl < 80ml/min 34‐84 hrs 68‐140 hrs
Rivaroxaban
CrCl > 80ml/min 16‐24 hrs 32‐40 hrs
CrCl < 80ml/min 18‐30 hrs 36‐50 hrs
Apixaban
CrCl > 50ml/min 14‐24 hrs 28‐40 hrs
CrCl < 50ml/min 34‐54 hrs 68‐90 hrs
15
Burnett A, Mahan C, Vazquez S, et al. Guidance for the Practical Management of the DOACs in VTE treatment. J Thromb Thrombolysis. 2016 January 16; 41:206‐232.
Page 18
emoryhealthcare.org
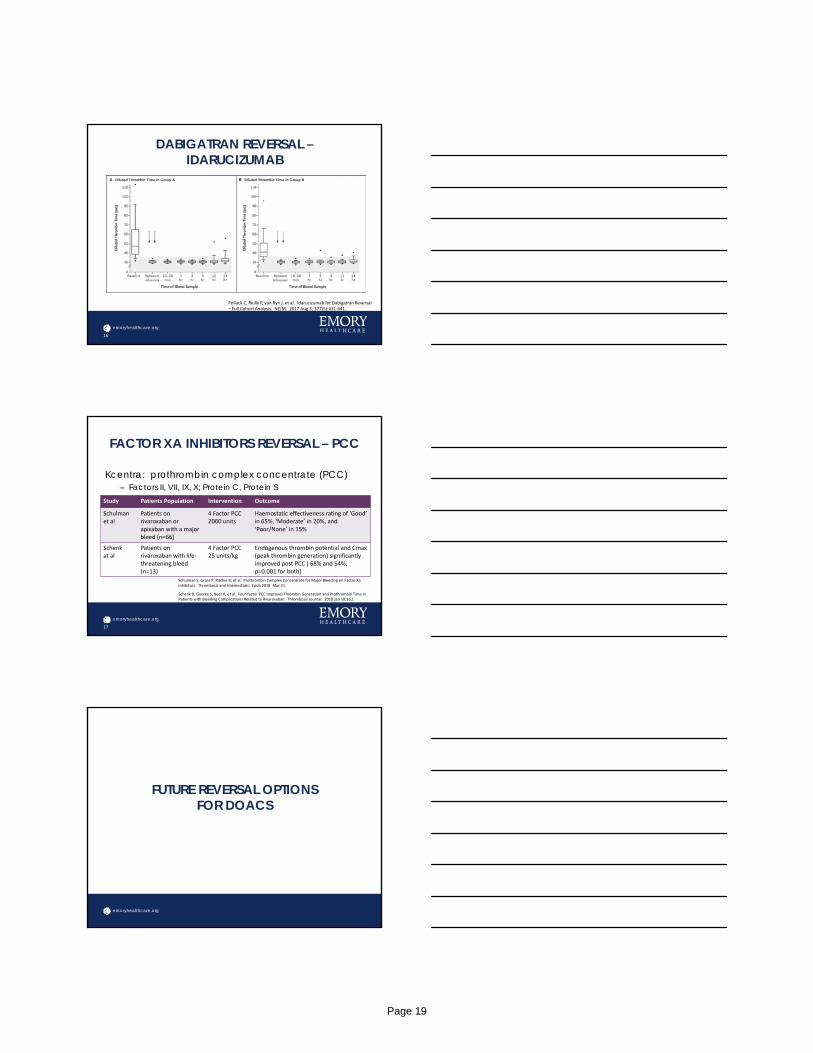
DABIGATRAN REVERSAL –IDARUCIZUMAB
16
Pollack C, Reilly P, van Ryn J, et al. Idarucizumab for Dabigatran Reversal – Full Cohort Analysis. NEJM. 2017 Aug 3; 377(5):431‐441.
emoryhealthcare.org
FACTOR XA INHIBITORS REVERSAL – PCC
Kcentra: prothrombin complex concentrate (PCC)– Factors II, VII, IX, X; Protein C, Protein S
17
Schulman S, Gross P, Ritchie B, et al. Prothrombin Complex Concentrate for Major Bleeding on Factor XaInhibitors. Thrombosis and Haemostasis. Epub 2018 Mar 21.
Schenk B, Goerke S, Beer R, et al. Four‐factor PCC Improves Thrombin Generation and Prothrombin Time in Patients with Bleeding Complications Related to Rivaroxaban. Thrombosis Journal. 2018 Jan 10;16;1
Study Patients Population Intervention Outcome
Schulman et al
Patients on rivaroxaban or apixaban with a major bleed (n=66)
4 Factor PCC2000 units
Haemostatic effectiveness rating of ‘Good’ in 65%, ‘Moderate’ in 20%, and ‘Poor/None’ in 15%
Schenk at al
Patients on rivaroxaban with life‐threatening bleed (n=13)
4 Factor PCC 25 units/kg
Endogenous thrombin potential and Cmax(peak thrombin generation) significantly improved post PCC ( 68% and 54%, p=0.001 for both)
emoryhealthcare.org
FUTURE REVERSAL OPTIONSFOR DOACS
Page 19
emoryhealthcare.org
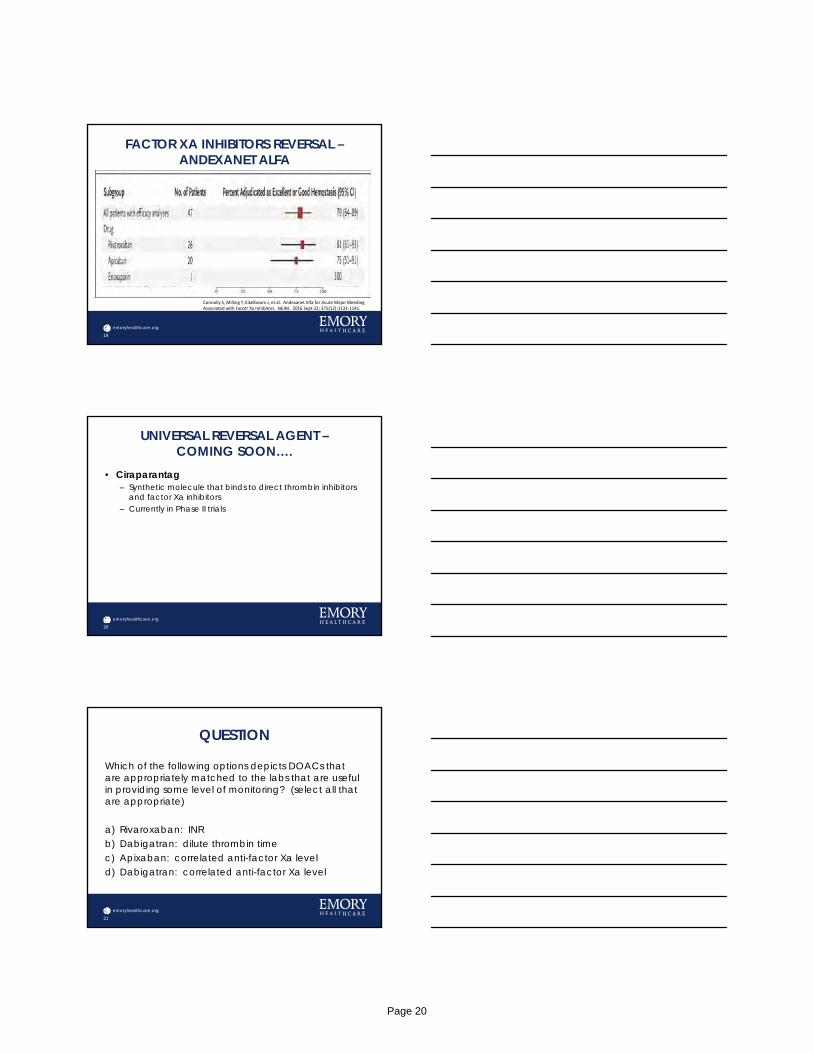
FACTOR XA INHIBITORS REVERSAL –ANDEXANET ALFA
19
Connolly S, Milling T, Eikelboom J, et al. Andexanet Alfa for Acute Major Bleeding Associated with Facotr Xa Inhibitors. NEJM. 2016 Sept 22; 375(12):1131‐1141.
emoryhealthcare.org
UNIVERSAL REVERSAL AGENT –COMING SOON….
• Ciraparantag– Synthetic molecule that binds to direct thrombin inhibitors
and factor Xa inhibitors– Currently in Phase II trials
20
emoryhealthcare.org
QUESTION
Which of the following options depicts DOACs that are appropriately matched to the labs that are useful in providing some level of monitoring? (select all that are appropriate)
a) Rivaroxaban: INRb) Dabigatran: dilute thrombin timec) Apixaban: correlated anti-factor Xa leveld) Dabigatran: correlated anti-factor Xa level
21
Page 20
emoryhealthcare.org
QUESTION
Which of the following agents would be appropriate to emergently reverse the effects of apixaban or rivaroxaban? (select all that are appropriate).
a) Kcentrab) Idarucizumabc) Andexanet alfad) Ciraparantag
22
emoryhealthcare.org
QUESTIONS???
23
Page 21
Antibiotic Utilization: Does This Bug You?ALLEY KILLIAN, PHARMD, BCPS ([email protected]) CLINICAL PHARMACY SPECIALIST, SURGICAL-TRANSPLANT ICUEMORY UNIVERSITY HOSPITALNO CONFLICTS TO DISCLOSE
Objectives
Discuss available literature and strategies for antibiotic stewardship in the ICU setting
Describe the literature regarding double-coverage of suspected and confirmed gram-negative infections
Review current recommendations regarding duration of treatment for common infections in the ICU
Antibiotic Stewardship
Infectious Diseases Society of American (IDSA) / Society for Healthcare Epidemiology of America (SHEA) Definition “Coordinated interventions designed to improve and measure the appropriate
use of antibiotic agents by promoting the selection of the optimal antibiotic drug regimen including dosing, duration of therapy, and route of administration”
Improved outcomes, reduced adverse events (including Clostridium difficile infection), improved susceptibilities to targeted antibiotics, optimization of resource utilization
Barlam TF, et al. Clin Infect Dis 2016; 62:e51-e77.
Page 22
Antibiotic Stewardship in the ICU
Study evaluating prospective interaction between infectious disease and critical care providers Decreased use of extended-spectrum penicillins, carbapenems, vancomycin,
and metronidazole
Lower rate of treatments not corresponding to guidelines
Fewer days of mechanical ventilation
Shorter ICU length of stay
Lower in-hospital mortality
~$90,000 savings from antibiotic discontinuation alone
Rimawa RH, et al. Crit Care Med 2013;41:2099-2107.
Components of ICU Stewardship
Rapid identification of patients Time to appropriate antibiotics
Role of serum biomarkers
Appropriate selection of empiric agents Local antibiograms
Consider recent regimens and patient-specific microbiology data
Empiric multidrug therapy
Kumar A. Virulence 2014;5:80-97. Kumar A, et al. Crit Car Med 2006;34:1589-1596. Luyt CE, et al. Crit Care 2014;18:480-491.
Utilization of pharmacokinetic (PK) / pharmacodynamic (PD) parameters
Increased volume of distribution Reduced elimination Organ support devices
Renal replacement therapy
Liver assist devices
Extracorporeal membrane oxygenation
Specific Strategies Loading Doses
Bactericidal agents
Extended infusions
Kumar A. Virulence 2014;5:80-97. Luyt CE, et al. Crit Care 2014;18:480-491.
Page 23
Multidrug Therapy: Sepsis Guidelines
Definitions: multidrug vs combination therapy
Suggest empiric combination therapy in septic shock
Suggest empiric combination therapy not be routinely used for sepsis without shock
Recommend against combination therapy for routine treatment of neutropenic sepsis
Recommend de-escalation to monotherapy within first few days based on clinical improvement for both targeted and empiric therapy
Rhodes A, et al. Crit Care Med 2016;45:486-552.
Multidrug Therapy: Pneumonia Guidelines
Empiric therapy Ventilator associated pneumonia (VAP)
Suggest combination therapy only in patients with a risk factor for MDR, patients in an ICU where >10% gram negative isolates are resistant to agent being considered for monotherapy, or patients in an ICU where local susceptibility rates are not available
Hospital-acquired pneumonia (HAP) Suggest combination therapy only in patients with factors increasing likelihood of
Pseudomonas aeruginosa or other gram-negative infection or high risk for mortality High risk for mortality: need for ventilator support or septic shock
Targeted therapy (P. aeruginosa) Recommend monotherapy in patients without shock or high risk of death Suggest combination therapy in patients who remain in shock or at high risk of death
Kalil AC, et al. Clin Infect Dis 2016;63:1-51.
Antibiotic De-escalation
De-escalation widely recommended in various guidelines but no standard definition Systematic review 2016: N=1688
Factors positively associated with de-escalation Initially appropriate empiric therapy
Broad-spectrum empiric therapy
Compliance with guidelines
Treatment with multiple and “companion” antimicrobials
Positive cultures
Factors negatively associated with de-escalation Multidrug resistant pathogen
Polymicrobial infections
Intra-abdominal infections
. Tabah A, et al. Clin Infect Dis 2016;62:1009-1017.
Page 24
Antibiotic De-escalation
Systematic review 2016: N=1688 Mortality: protective effect of de-escalation
No effect on antibiotic days
Two studies reported no effect regarding emergence of multidrug resistant (MDR) organisms
Two studies reported lower costs associated with de-escalation
Reassess daily or as microbiology data results
Tabah A, et al. Clin Infect Dis 2016;62:1009-1017.
Antibiotic De-escalation
Recommended by all major guidelines Sepsis guidelines: “thoughtful de-escalation of antimicrobials based on
adequate clinical improvement even if cultures are negative”
Pneumonia guidelines: patients without sputum cultures, decreased reliability of cultures, or high risk for MDR infections may not be candidates
Switch to monotherapy Sepsis guidelines: within the first few days but continue if remain in shock
Pneumonia guidelines Pseudomonas aeruginosa: continue combination therapy if remain in septic shock or
high risk of death
Kalil AC, et al. Clin Infect Dis 2016;63:1-51.Rhodes A, et al. Crit Care Med 2016;45:486-552.
Components of ICU Stewardship
Minimize duration Role of serum biomarkers
Reduce numbers of unnecessarily treated patients
Luyt CE, et al. Crit Care 2014;18:480-491.
Page 25
Duration of Therapy
Sepsis guidelines Suggest 7-10 days for most serious infections Suggest longer courses for slow clinical response, undrainable foci of infection,
bacteremia with S. aureus, some fungal and viral infections, or immunologic deficiencies
Pneumonia guidelines Recommend 7 days regardless of type or organism
Intra-abdominal infections Current IDSA guidelines: 4-7 days unless difficult to achieve source control STOP-IT trial: 4 days
Kalil AC, et al. Clin Infect Dis 2016;63:1-51. Rhodes A, et al. Crit Care Med 2016;45:486-552.Sawyer RG, et al. New Engl J Med 2015;273:1996-2005. Solomkin JS, et al. Clin Infect dis 2010;50:133-164.
Duration of Therapy
Catheter-associated urinary tract infection (CAUTI) Prompt resolution: 7 days
Delayed response: 10-14 days
Catheter-related bloodstream infection (CRBSI) Uncomplicated
Organism-dependent but generally 7-14 days
Complicated 4-6 weeks (6-8 weeks for osteomyelitis)
Day 1 = first day on which negative blood culture results are obtained
Hooton TM, et al. Clin Infect Dis 2010;50:625-663.Mermal LA, et al. Clin Infect Dis 2009; 49:1-45.
Antibiotic Stewardship in the ICU
Strategies Bundle into small (5-8) groups of interventions that are practical and measurable
Multidisciplinary approach
Utilize technology
Education and feedback
Barriers Severity of illness
Complex decision-making process for empiric selection
Frequent lack of causative organism
Difficult to ensure continuity of care
Lawrence KL. Am J Respir Crit Car Med 2009;179:434-438.Luyt CE, et al. Crit Care 2014;18:480-491.
Page 26
ARDS:Beyond Low Tidal Volume Ventilation!
Greg S. Martin, M.D., M.Sc.Associate Director for Critical Care, Pulmonary, Allergy and Critical Care
Director of Research, Emory Critical Care Center
Section Chief and MICU/CCU Co-Director, Grady Memorial Hospital
Contact me: [email protected]
12th Annual Southeastern Critical Care SummitEmory Conference Center Hotel – Atlanta, GA – May 10, 2018
Conflict disclosure: much of my research involves sepsis and ARDS and Emory University receives funds on my behalf from NIH, FDA and for-profit companies
Interventions That MayDecrease ARDS Mortality
Validated: • Low tidal volume ventilation (ARMA trial, NEJM 2000)
– 25% RRR, 11% ARR in mortality at day 28– Meta-analyses confirmed reductions in 28-day and hospital mortality
Unvalidated:• Higher PEEP for patients with moderate-severe ARDS (P/F <200 mmHg)• Prone positioning
– RCT in France, 28-day mortality reduction 51% RRR, 16.8% ARR (Guerin NEJM 2013)– Meta analyses show improved mortality only in patients with ARDS and P/F <100
• Early paralysis– French RCT, 28-day mortality reduction 29% RRR, 9.6% ARR (Papazian NEJM 2010)– Being replicated by PETAL network, study terminated, results to be released next week at ATS
Interventions That Benefit the PatientPatient but Don’t Decrease MortalityValidated: • Fluid conservative fluid management (FACTT, NEJM 2006)
– 2.5 more days alive and free of mechanical ventilation (VFD, p<0.001)– 2.2 more days alive and free of the ICU (ICU-FD, p<0.001)– Fewer patients needing dialysis at day 60 (10% vs 14%, p=0.06)– More cardiovascular organ dysfunction (p=0.04), less CNS organ dysfunction
(p=0.02)– 10% RRR, 2.9% ARR in 28-day mortality (p=0.30)
Unvalidated:• Acute “rehabilitation” (ICU mobility)
– Shorter duration of mechanical ventilation– Shorter duration of ICU & hospital length of stay, with reduced costs– Fewer hospital re-admissions
Page 27
Nutrition in ARDS• Antioxidant vs. standard enteral nutrition
– Twice daily supplements of n-3 fatty acids, γ-linolenic acid and antioxidants (OMEGA study)
– ARDS-Net terminated the trial for “futility” after enrolling 272 ALI & ARDS patients
• Supplement patients had:– 8-fold increase in plasma eicosapentaenoic acid – More days with diarrhea (29% vs. 21%; p = 0.001)
– Fewer ventilator-free days (14.0 vs. 17.2; p = 0.02)
– Fewer ICU-free days (14.0 vs. 16.7; p = 0.04)
– Fewer non-pulmonary organ failure-free days (12.3 vs. 15.5; p = 0.02)
– Higher 60-day hospital mortality (26.6% vs. 16.3%; p = 0.054)
• EDEN study of early vs. late enteral nutrition in 1000 ALI & ARDS patients– Nutrition at ICU
admission vs. day 6• No difference in
mortality or other relevant clinical outcomes
• Less feeding intolerance in the late nutrition group
* Rice TW, et al. JAMA 2011; 306(14): 1574-1581.† Rice TW, et al. JAMA 2012; 307(8): 795-803.
In patients with documented ARDS, iNO at 1.25, 5, 20, 40, or 80 ppm:• Is associated with a significant improvement in oxygenation compared with placebo
over the first four hours of treatment. An improvement in oxygenation index was observed over the first four days.
• Acutely increased the PaO2 in 60% of the patients
• The percentage of patients having an acute increase in PaO2 and the magnitude of the change were similar in each of the inhaled NO dose groups.
• Appears to be well tolerated in doses between 1.25 to 40 ppm.
• Although these concentrations appear to be safe, it is prudent to closely monitor NO2
concentrations and methemoglobin levels.
• There are trends in decreasing the intensity of mechanical ventilation needed to maintain adequate oxygenation and improved patient benefit at 5 ppm inhaled NO.
Dellinger RP, et al. Crit Care Med 1998; 26(1): 15-23.
Inhaled Nitric Oxide in ARDS
Inhaled Nitric Oxide in ARDS• In patients with severe acute lung injury (PaO2/FiO2 250) but without
sepsis or other organ system failure, iNO at 5 ppm:– Induces short-term improvements in oxygenation with a 20% increase in PaO2
that were maintained only during 24 - 48 hours.– Does not improve clinical outcomes or mortality *
• iNO should not be routinely used in ARDS patients but may be considered (Grade C recommendation) as a salvage therapy in patients with life-threatening hypoxemia despite optimization of conventional mechanical ventilator support.
• Optimal iNO dosing should be determined each day because iNOsensitivity increases over time (no tachyphylaxis) and higher than necessary doses decrease oxygenation (dose-response) †
* Taylor RW, et al. JAMA 2004; 291(13) 1603-1609.† Gerlach H, et al. Am J Respir Crit Care Med 2003; 167(7): 1008-15.
Page 28
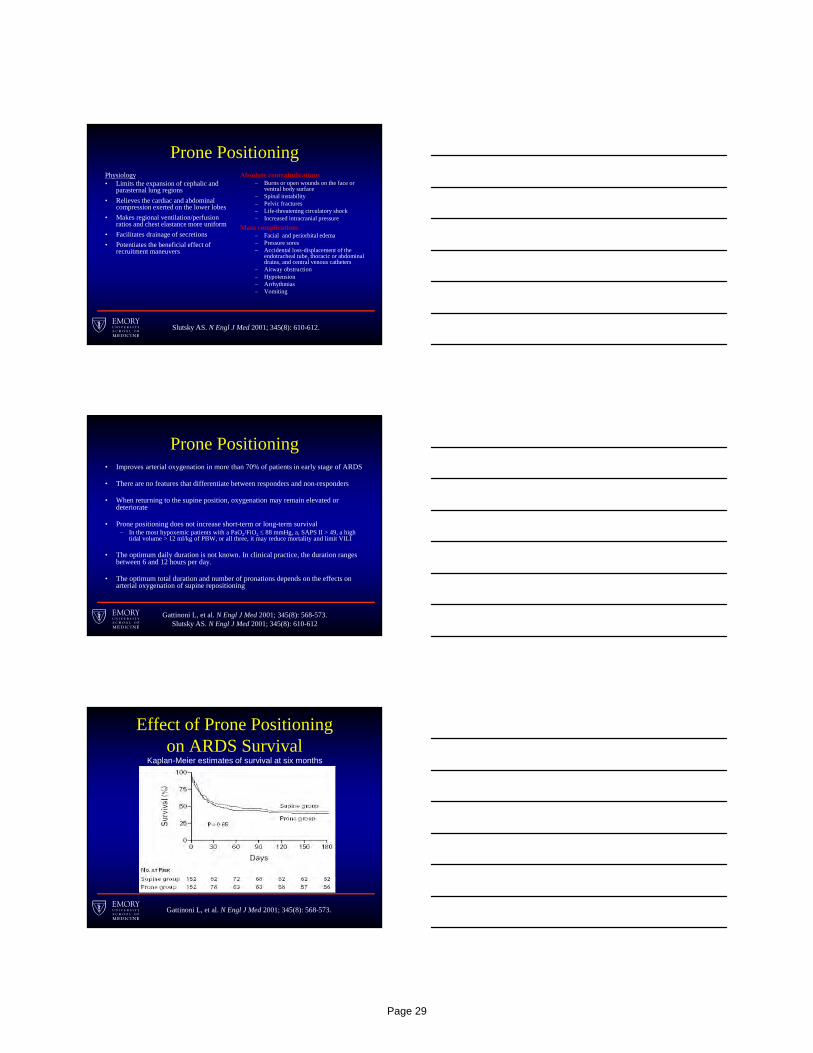
Prone PositioningPhysiology• Limits the expansion of cephalic and
parasternal lung regions
• Relieves the cardiac and abdominal compression exerted on the lower lobes
• Makes regional ventilation/perfusion ratios and chest elastance more uniform
• Facilitates drainage of secretions
• Potentiates the beneficial effect of recruitment maneuvers
Absolute contraindications– Burns or open wounds on the face or
ventral body surface– Spinal instability– Pelvic fractures– Life-threatening circulatory shock– Increased intracranial pressure
Main complications– Facial and periorbital edema– Pressure sores– Accidental loss-displacement of the
endotracheal tube, thoracic or abdominal drains, and central venous catheters
– Airway obstruction– Hypotension– Arrhythmias– Vomiting
Slutsky AS. N Engl J Med 2001; 345(8): 610-612.
Prone Positioning• Improves arterial oxygenation in more than 70% of patients in early stage of ARDS
• There are no features that differentiate between responders and non-responders
• When returning to the supine position, oxygenation may remain elevated or deteriorate
• Prone positioning does not increase short-term or long-term survival– In the most hypoxemic patients with a PaO2/FiO2 88 mmHg, a, SAPS II > 49, a high
tidal volume > 12 ml/kg of PBW, or all three, it may reduce mortality and limit VILI
• The optimum daily duration is not known. In clinical practice, the duration ranges between 6 and 12 hours per day.
• The optimum total duration and number of pronations depends on the effects on arterial oxygenation of supine repositioning
Gattinoni L, et al. N Engl J Med 2001; 345(8): 568-573.Slutsky AS. N Engl J Med 2001; 345(8): 610-612
Gattinoni L, et al. N Engl J Med 2001; 345(8): 568-573.
Kaplan-Meier estimates of survival at six months
Effect of Prone Positioning on ARDS Survival
Page 29
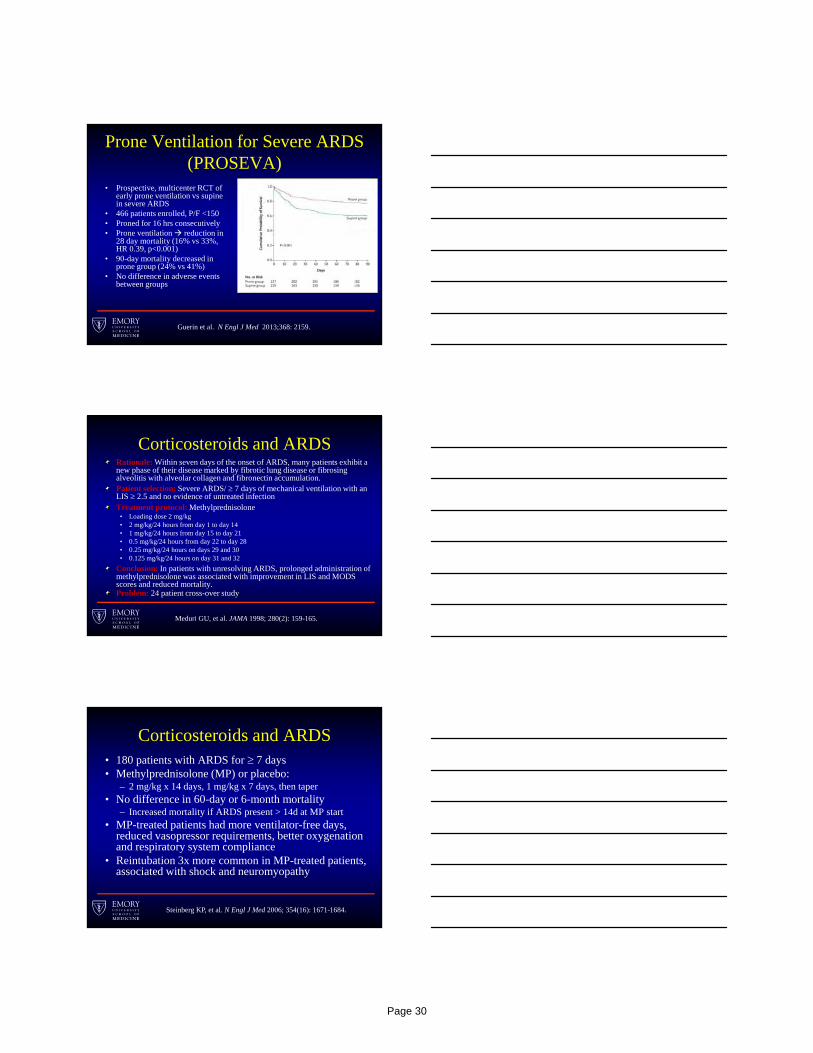
Prone Ventilation for Severe ARDS (PROSEVA)
• Prospective, multicenter RCT of early prone ventilation vs supine in severe ARDS
• 466 patients enrolled, P/F <150• Proned for 16 hrs consecutively• Prone ventilation reduction in
28 day mortality (16% vs 33%, HR 0.39, p<0.001)
• 90-day mortality decreased in prone group (24% vs 41%)
• No difference in adverse events between groups
Guerin et al. N Engl J Med 2013;368: 2159.
Rationale: Within seven days of the onset of ARDS, many patients exhibit a new phase of their disease marked by fibrotic lung disease or fibrosing alveolitis with alveolar collagen and fibronectin accumulation.Patient selection: Severe ARDS/ 7 days of mechanical ventilation with an LIS 2.5 and no evidence of untreated infectionTreatment protocol: Methylprednisolone
• Loading dose 2 mg/kg • 2 mg/kg/24 hours from day 1 to day 14• 1 mg/kg/24 hours from day 15 to day 21• 0.5 mg/kg/24 hours from day 22 to day 28• 0.25 mg/kg/24 hours on days 29 and 30• 0.125 mg/kg/24 hours on day 31 and 32
Conclusion: In patients with unresolving ARDS, prolonged administration of methylprednisolone was associated with improvement in LIS and MODS scores and reduced mortality.Problem: 24 patient cross-over study
Meduri GU, et al. JAMA 1998; 280(2): 159-165.
Corticosteroids and ARDS
Corticosteroids and ARDS• 180 patients with ARDS for 7 days• Methylprednisolone (MP) or placebo:
– 2 mg/kg x 14 days, 1 mg/kg x 7 days, then taper• No difference in 60-day or 6-month mortality
– Increased mortality if ARDS present > 14d at MP start• MP-treated patients had more ventilator-free days,
reduced vasopressor requirements, better oxygenation and respiratory system compliance
• Reintubation 3x more common in MP-treated patients, associated with shock and neuromyopathy
Steinberg KP, et al. N Engl J Med 2006; 354(16): 1671-1684.
Page 30
Corticosteroids and ARDS• 92 patients with ARDS 72 hours
• Methylprednisolone (MP) or placebo (2:1)– 1 mg/kg/day for 14 days, 0.5 mg/kg x 7d, 0.25 mg/kg x 7d
• MP-treated patients had greater reduction in LIS by day 7 (primary outcome) and MODS
• MP-treated patients had shortened duration of mechanical ventilation (5.0 vs. 9.5 days) and ICU stay (7.0 vs. 14.5 days), lower rates of infection and decreased mortality (20.6% vs. 42.9%)
Meduri GU, et al. Chest 2007; 131(4) 954-963.
Beta-Agonists in ALI/ARDS• 40 ALI / ARDS patients were randomized to
blindly receive either intravenous salbutamol (15 mcg/kg/hr) or placebo for 7 days (BALTI trial)
• Lung water (pulmonary edema) and airway plateau pressure decreased with salbutamol– Salbutamol use resulted in more supraventricular
arrhythmias and lower serum potassium
• No difference in duration of mechanical ventilation or survival
Perkins G, et al. Am J Respir Crit Care Med 2006; 173: 281-287.
Beta-Agonists in ALI/ARDS• Multi-center study of 282 ALI / ARDS patients
randomized to blindly receive aerosolized albuterol (5 mg) or saline q4 hours for 10 days
• Trial terminated early for “futility”– Ventilator-free days was less with albuterol (p=0.095)– Number of ICU days higher with albuterol (p=0.018)– Death before hospital discharge not different
(23.0% vs. 17.7%, p=0.30)– Modest increases in heart rate with albuterol (4 bpm)
• No measurements of lung water or edema
ARDS Network. Am J Respir Crit Care Med 2011; 184: 561-568.
Page 31

• Multi-centre UK study of 326 ARDS patients randomized to blindly receive intravenous salbutamol (15 mcg/kg IBW/hr) or placebo for 7 days (BALTI-2)
• Trial terminated early for safety concerns:– Increased 28-day mortality: 34% vs. 23%, p=0.03; risk
ratio of 1.47 (95% CI 1.03–2.08)• Tachycardia requiring drug suspension, 14% vs. 1%, p<0.001• New arrhythmias 9% vs. 2%, p=0.006• New lactic acidosis, 6% vs. 1%, p=0.005
Beta-Agonists in ARDS
Smith FG, et al. Lancet 2011; DOI:10.1016/S0140-6736(11)61623-1.
• Multi-centre UK study of 326 ARDS patients randomized to blindly receive intravenous salbutamol (15 mcg/kg IBW/hr) or placebo for 7 days (BALTI-2)
• Trial terminated early for safety concerns:– Increased 28-day mortality: 34% vs. 23%, p=0.03; risk
ratio of 1.47 (95% CI 1.03–2.08)• Tachycardia requiring drug suspension, 14% vs. 1%, p<0.001• New arrhythmias 9% vs. 2%, p=0.006• New lactic acidosis, 6% vs. 1%, p=0.005
Beta-Agonists in ARDS
Smith FG, et al. Lancet 2011; DOI:10.1016/S0140-6736(11)61623-1.
Neuromuscular Blocking Agents in ARDS
• Multicenter, double blind trial in patients with severe ARDS– Severe ARDS defined as PaO2/FiO2 ratio < 150
• Cis-atracurium vs. placebo for 48 hours
• Primary outcome: 90 day in-hospital mortality
• 340 ARDS patients randomized and treated
– HR for death at 90 days in treatment group 0.68 (p=0.04)
– 28 day mortality 23.7% vs. 33.3% (p=0.05)
– 90 day mortality 31.6% vs. 40.7% (p=0.08)
– No difference in ICU-acquired paresis
Papazian L, et al. N Engl J Med 2010; 33: 1107-16.
Page 32

Neuromuscular Blocking Agents in ARDS
• Multicenter, double blind trial in patients with severe ARDS– Severe ARDS defined as PaO2/FiO2 ratio < 150
• Cis-atracurium vs. placebo for 48 hours
• Primary outcome: 90 day in-hospital mortality
• 340 ARDS patients randomized and treated
– HR for death at 90 days in treatment group 0.68 (p=0.04)
– 28 day mortality 23.7% vs. 33.3% (p=0.05)
– 90 day mortality 31.6% vs. 40.7% (p=0.08)
– No difference in ICU-acquired paresis
Papazian L, et al. N Engl J Med 2010; 33: 1107-16.
ECMO in ARDS
Abrams and Brodie. CHEST 2017; 152(3):639-649.
ECMO in ARDS• CESAR trial
– Only RCT evaluating ECMO in ARDS
– 180 patients randomized– Only 75% of those in ECMO arm
actually received ECMO– 30% of patients in control arm did
not receive LTVV– improved survival at 6 months
• Indications: Severe ARDS (LIS >3, pH<7.20)
• Contraindications: high risk for anticoagulation, ICH, refusal of blood products … (high-pressure or high FiO2, mechanical ventilation >7 days)
• Role of ECMO remains uncertain; variably used, most often as salvage
* Peek GJ, et al. Lancet 2009; 374(9698): 1351-63.
Page 33
Other Drug Therapy
Prostaglandin E1 (PGE1) (pulmonary vasodilatation and anti-inflammatory effects on neutrophils/macrophages)
Aerosolized prostacyclin (PGI2) (selective pulmonary vasodilatation of ventilated lung areas)
Almitrine (selective pulmonary vasoconstrictor of non-ventilated lung areas)
Surfactant (prevents alveolar collapse and protects against intrapulmonary injury and infection)
Antioxidants (protect the lung from free oxygen radical production)
Partial liquid ventilation (recruitment of collapsed areas and anti-inflammatory effect)
Anti-inflammatory drugs (ibuprofen, ketoconazole, lisofylline)
No recommendation can be made for their use - Rescue modality in the patient with refractory hypoxemia?
Combination Therapy in ARDS?• Combination of iNO and prone position
– Papazian L, et al. Crit Care Med. 1998.
• Combination of iNO and almitrine – Gallart L, et al. Am J Respir Crit Care Med. 1998.
• Combination of prone position, iNO, and almitrine– Jolliet P, et al. Crit Care Med. 1997. – Gillart T, et al. Can J Anaesth. 1998.
• Combination of iNO and iv prostacyclin– Kuhlen R, et al. Intensive Care Med. 1999.
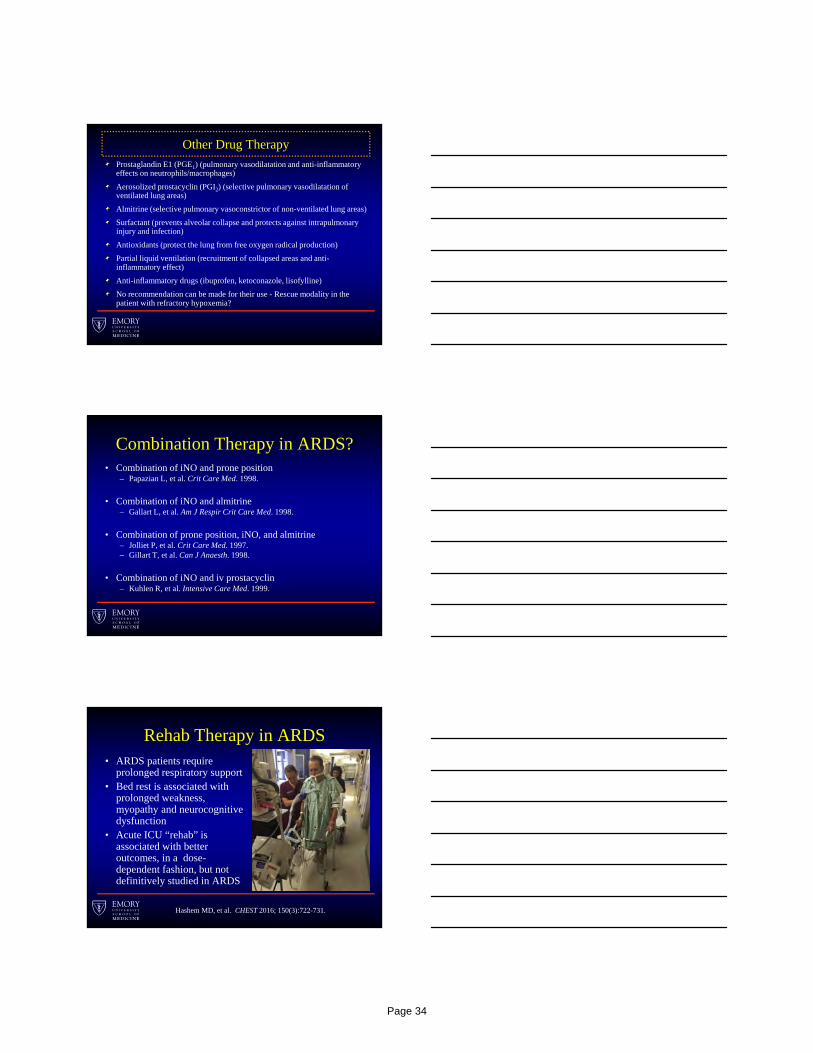
Rehab Therapy in ARDS• ARDS patients require
prolonged respiratory support• Bed rest is associated with
prolonged weakness, myopathy and neurocognitive dysfunction
• Acute ICU “rehab” is associated with better outcomes, in a dose-dependent fashion, but not definitively studied in ARDS
Hashem MD, et al. CHEST 2016; 150(3):722-731.
Page 34
Treating ARDSWhat has NOT worked:• Rosuvastatin (NEJM 2014)• Nebulized or IV β-agonists (AJRCCM 2009 & Lancet 2012)• Surfactant (NEJM 2004)• Ketoconazole (JAMA 2000), lisofylline (CCM 2002)• High frequency oscillatory ventilation (NEJM 2013)• Inhaled nitric oxide (JAMA 2004)• Supplementation of n-3 fatty acids, γ-linolenic acid, and
antioxidants (OMEGA study, JAMA 2011)• Pulmonary artery catheter instead of CVC (NEJM 2006)
Conclusions• Lung protective, low tidal volume, ventilation is the major proven strategy for
saving lives with ARDS• Beneficial non-ventilatory strategies include:
– Conservative fluid management• Potentially beneficial non-ventilatory strategies include:
– Early pharmacologic paralysis (pending ROSE study)– Prone position (awaiting validation)– Corticosteroids in ARDS (uncertain timing, dose, duration, patient selection)– ECMO (uncertain patient selection to balance risk and benefit)– ICU mobility and rehabilitation– ABCDEF bundle (e.g. minimizing delirium)
• Non-beneficial or potentially harmful non-ventilatory strategies include:– Inhaled or intravenous beta-agonists– Immune-modulating enteral nutrition (and early initiation of parenteral nutrition)– Pulmonary artery catheterization
Page 35
New Vasopressor Options in Sepsis
Laurence Busse, M.D.
Assistant Professor, Division of Pulmonary, Critical Care, Allergy and Sleep Medicine
Emory University, Atlanta, GA
Potential Conflicts of Interest
• La Jolla Pharmaceutical Company
• Portola Pharmaceutical Company
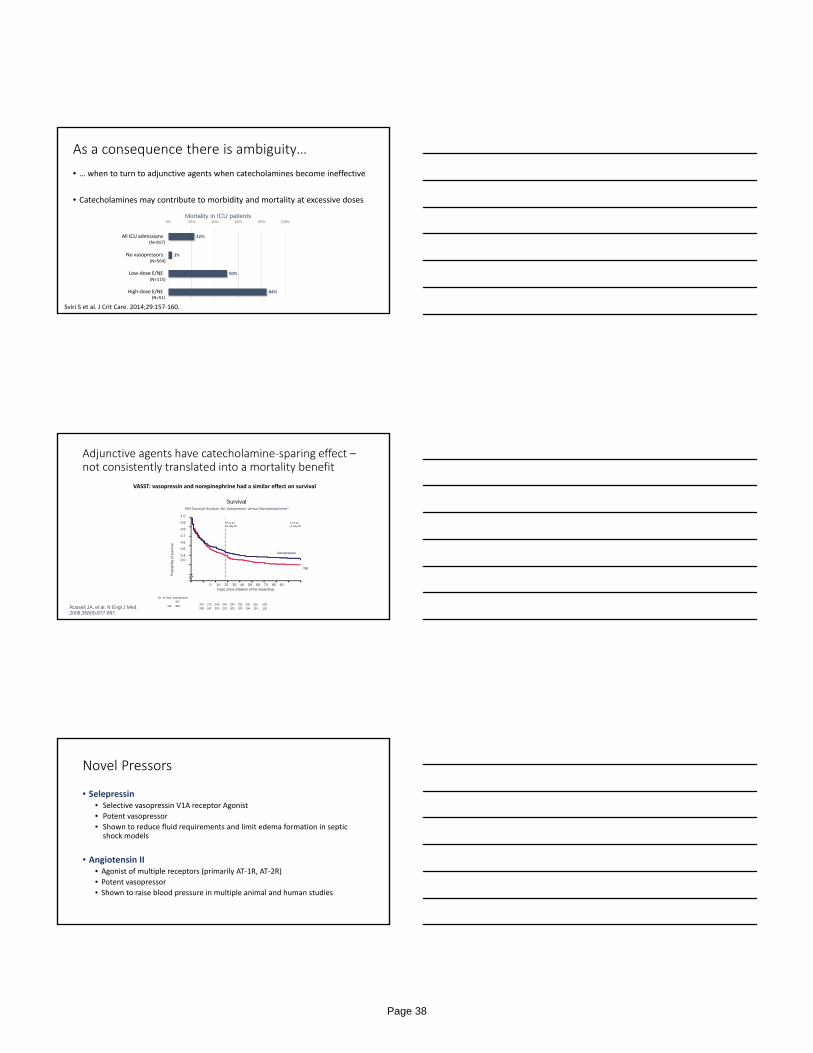
AKI and MI by Lowest MAP
Shock is bad for organs…
Page 36
Cox regression model for ICU survival based on mean 24‐hour values of lactate and MAP1
0.8
0 500 2,000 2,5001,000 1,500
Length of ICU stay (hrs)
Sur
viva
l(p
rop
otio
n)
0.0
0.2
0.4
0.6
1.0
Lactate <2 mmol/l; MAP >65 mmHg
Lactate <2 mmol/l; MAP <65 mmHg
Lactate >2 mmol/l; MAP >65 mmHg
Lactate >2 mmol/l; MAP <65 mmHg
MAP < 65 mmHg an independent predictor of
mortality on >800 septic shock patients1
MAP < 65 mmHg an independent predictor of
mortality on >800 septic shock patients1
Houwink, AP, et al., Crit Care 2016;20:56
Shock is associated with increase in mortality
Our management of septic shock is guided by consensus guidelines…
NE is the recommended initial choice of pressor but guidelines
for second‐ and third‐line vasoactive agents is lacking
a
Conclusions• Choice of specific vasopressor is individualized and may be left to discretion of
physician• Patient-specific variables should be taken into consideration
• 28 RCTs (3497 participants) with 1773 mortality outcomes• 6 different vasopressors, given alone or in combination, studied in 12 different
comparisons
Findings• No differences in total mortality in any comparisons of vasopressors or combinations
in any of the predefined analyses• Most available data involve norepinephrine
aBest exemplified by the recent Cochrane Review…
No vasopressor or combination is better than any other
Page 37
As a consequence there is ambiguity…
• … when to turn to adjunctive agents when catecholamines become ineffective
• Catecholamines may contribute to morbidity and mortality at excessive doses
22%
3%
50%
84%
0% 20% 40% 60% 80% 100%
All ICU admissions
No vasopressors
Low‐dose E/NE
High‐dose E/NE
Mortality in ICU patients
(N=917)
(N=564)
(N=115)
(N=51)
Sviri S et al. J Crit Care. 2014;29:157‐160.
Adjunctive agents have catecholamine‐sparing effect –not consistently translated into a mortality benefit
Russell JA, et al. N Engl J Med. 2008;358(9):877-887.
SurvivalKM‐Survival Analysis for Vasopressin versus Noreprinephrine1
Pro
bab
ility
of s
urvi
val
1.0
0.9
0.8
0.7
0.6
0.5
0.40.0
Vasopressin
NE
0 10 20 30 40 50 60 70 80 90Days since initiation of the study drug
No. at Risk Vasopressin
397
NE 382301 272 249 240 234 232 230 226 220
289 247 230 212 205 200 194 193 191
P=0.27at day 28
P=0.10at day 90
VASST: vasopressin and norepinephrine had a similar effect on survival
Novel Pressors
• Selepressin• Selective vasopressin V1A receptor Agonist
• Potent vasopressor
• Shown to reduce fluid requirements and limit edema formation in septic shock models
• Angiotensin II• Agonist of multiple receptors (primarily AT‐1R, AT‐2R)
• Potent vasopressor
• Shown to raise blood pressure in multiple animal and human studies
Page 38

Blood pressure effect
Antidiuretic effect,
vasodilation
Vasopressin Selepressin
Slide courtesy of Pierre Francois Laterre, Cliniques universitaires Saint‐Luc, presented @ ISICEM, Brussels, 2018
• Phase IIa study• 53 patients• Multiple doses of selepressin
and placebo (1.25 ng/kg/min, 2.5 ng/kg/min, 3.75 ng/kg/min)
Proportion of pts maintaining MAP w/o NE (Catecholamine sparing)
Fluid sparing
Page 39
• Phase 2b/3 Adaptive Clinical Trial• 1800 patients• Multiple doses of selepressin and placebo• Endpoints:
• P&VFDs up to Day 30
STOPPED!
…result of the final interim analysis of Part 1/Phase 2b of SEPSIS‐ACT.
…the result does not meet the pre‐specified criteria on predictive probability of success for the trial
required to continue
Page 40
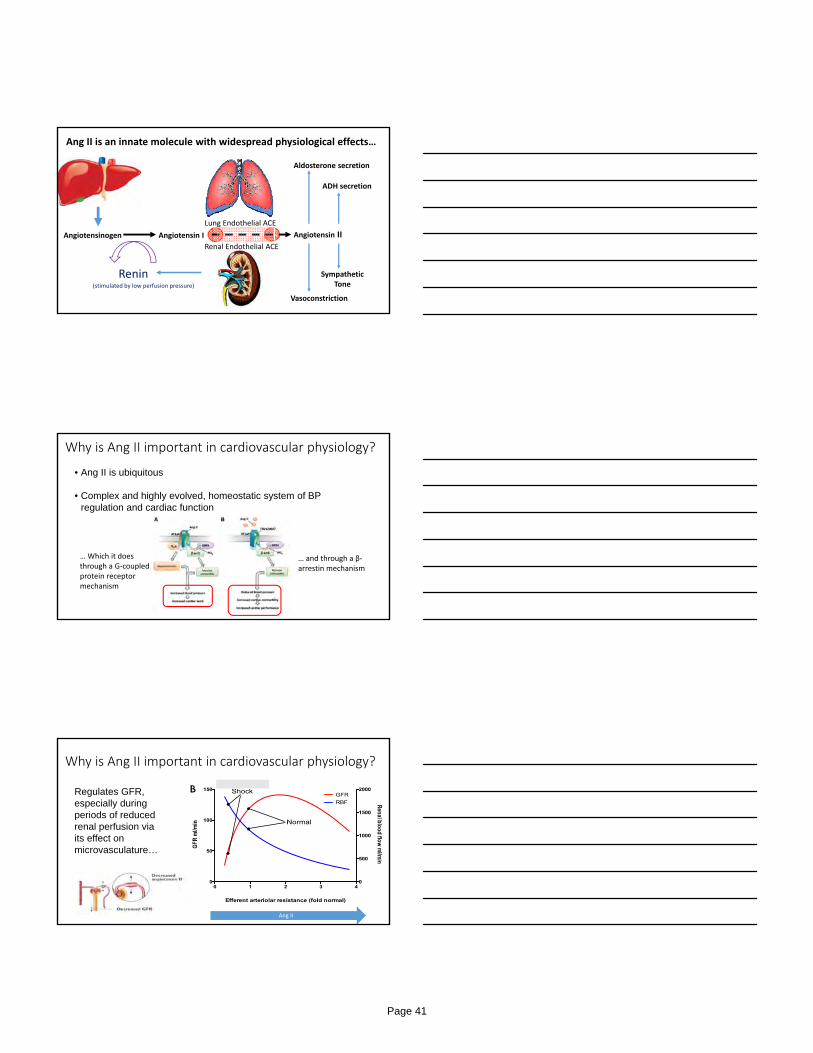
Angiotensinogen
Renin
Angiotensin I
(stimulated by low perfusion pressure)
Renal Endothelial ACE
Lung Endothelial ACE
Angiotensin II
Aldosterone secretion
ADH secretion
Vasoconstriction
Sympathetic Tone
Ang II is an innate molecule with widespread physiological effects…
Why is Ang II important in cardiovascular physiology?
• Ang II is ubiquitous
• Complex and highly evolved, homeostatic system of BP regulation and cardiac function
… Which it does through a G‐coupled protein receptor mechanism
… and through a β‐arrestin mechanism
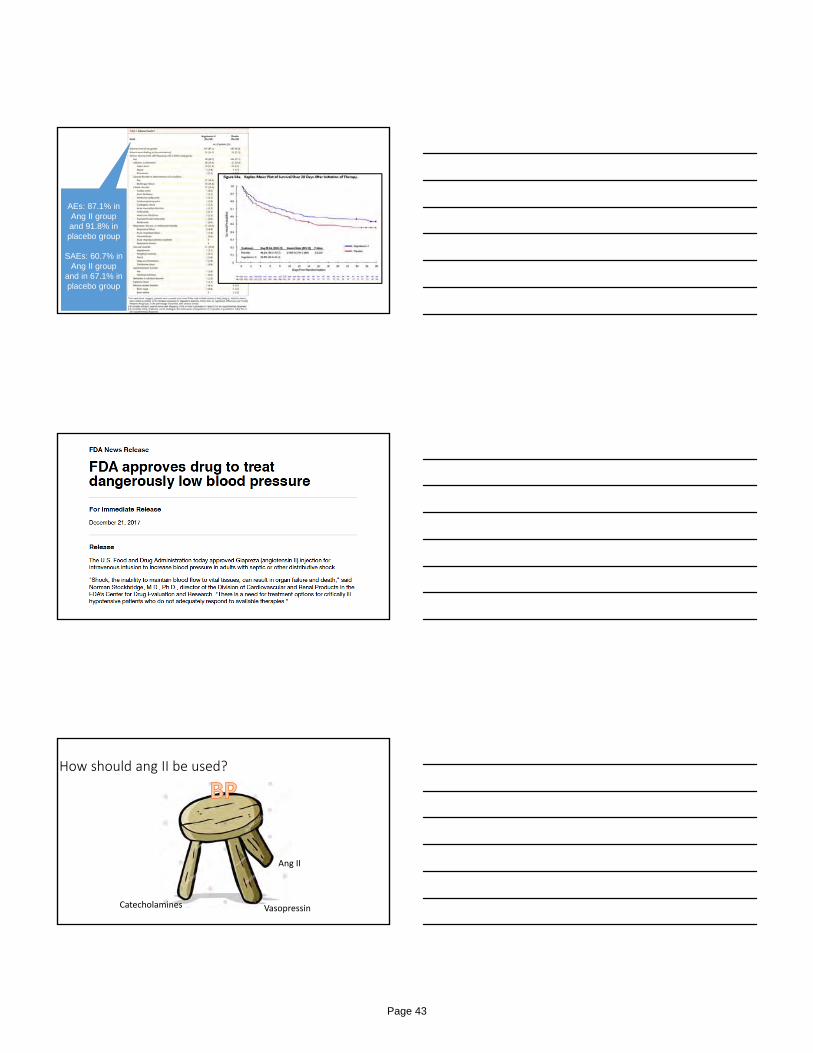
Why is Ang II important in cardiovascular physiology?
Regulates GFR, especially during periods of reduced renal perfusion via its effect on microvasculature…
Ang II
Page 41
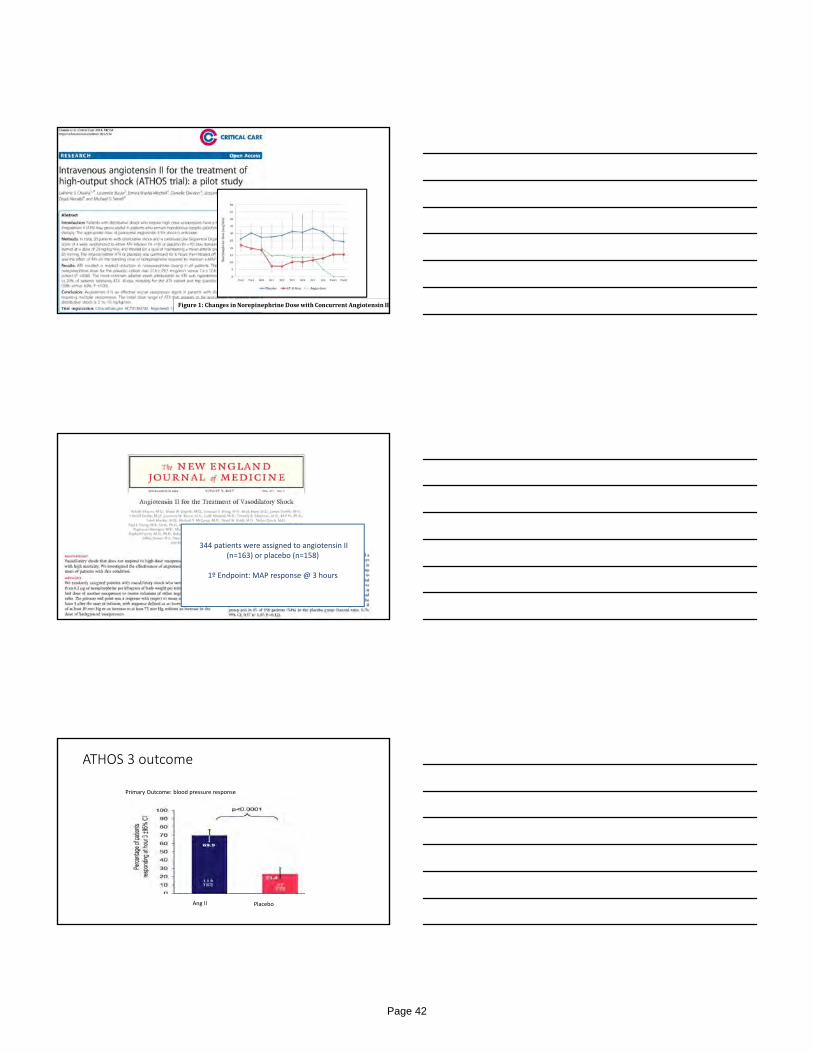
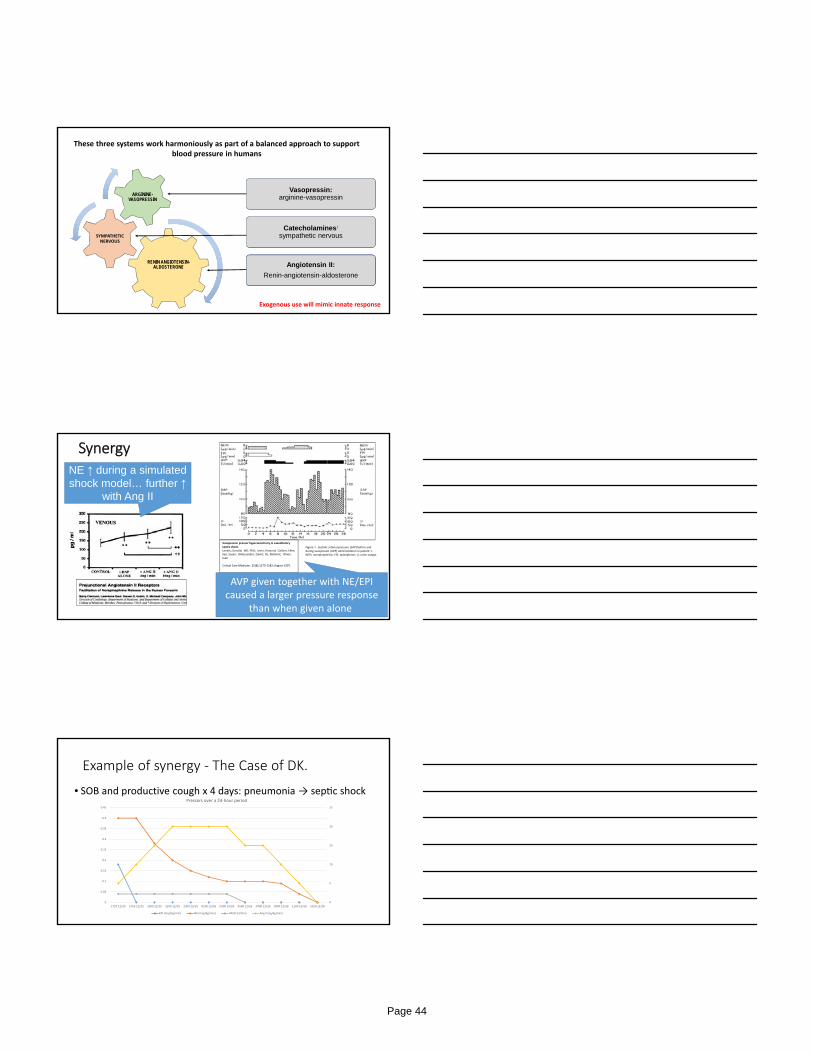
Figure1:ChangesinNorepinephrineDosewithConcurrentAngiotensinII
344 patients were assigned to angiotensin II (n=163) or placebo (n=158)
1º Endpoint: MAP response @ 3 hours
ATHOS 3 outcome
Primary Outcome: blood pressure response
Ang II Placebo
Page 42
AEs: 87.1% in Ang II group and 91.8% in placebo group
SAEs: 60.7% in Ang II group
and in 67.1% in placebo group
How should ang II be used?
Ang II
VasopressinCatecholamines
Page 43
RENIN ANGIOTENSIN-ALDOSTERONE
SYMPATHETIC NERVOUS
ARGININE-VASOPRESSIN
Catecholamines:
sympathetic nervous
Vasopressin: arginine-vasopressin
Angiotensin II:
Renin-angiotensin-aldosterone
These three systems work harmoniously as part of a balanced approach to support blood pressure in humans
Exogenous use will mimic innate response
SynergyNE ↑ during a simulated shock model… further ↑
with Ang II
Vasopressin pressor hypersensitivity in vasodilatory septic shock.Landry, Donald; MD, PhD; Levin, Howard; Gallant, Ellen; Seo, Susan; DAlessandro, David; Oz, Mehmet; Oliver, Juan
Critical Care Medicine. 25(8):1279‐1282, August 1997.
Figure 1 . Systolic arterial pressure (SAP) before and during vasopressin (AVP) administration in patient 1. NEPI, norepinephrine; EPI, epinephrine; U, urine output.
AVP given together with NE/EPI caused a larger pressure response
than when given alone
Example of synergy ‐ The Case of DK.
• SOB and productive cough x 4 days: pneumonia → sep c shock
0
5
10
15
20
25
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
1727 12/25 1755 12/25 1900 12/25 2100 12/25 2300 12/25 0100 12/26 0300 12/26 0500 12/26 0700 12/26 0900 12/26 1100 12/26 1024 12/28
Pressors over a 24‐hour period
EPI (mcg/kg/min) NE (mcg/kg/min) VASO (U/min) Ang II (ng/kg/min)
Page 44

Example of synergy ‐ The case of a 45F w/ flu
• Tx for consideration of extracorporeal membrane oxygena on → sep c shock, fulminant liver failure, kidney failure requiring CRRT
The Emory Protocol
Table 3: Vasopressor Titration – Titration of pressors NE Equivalenta (mcg/kg/min)
Vasopressin (U/min)
Angiotensin II (ng/kg/min)
b 0.25 0.03 40 0.24 0.03 30 0.23 0.03 30 0.22 0.03 30 0.21 0.03 30 0.2 0.03 20 0.19 0.03 20 0.18 0.03 20 0.17 0.03 20 0.16 0.03 15
0.15 0.03 15 0.14 0.03 15 0.13 0.03 10 0.12 0.03 10 0.11 0.03 10 0.1 0.03 0.1 0.03 5c 0.09 0.03 5c 0.08 0.03 5c 0.07 0.03 5c 0.06 0.03 5c 0.05 0.03 2.5c 0.05 0.04 0 2.5c 0.03 0 2.5c 0.02 0 0 0.01 0 0 0 0 0
Titration driven by NE dosing, based on MAP goals. aNE equivalent doses represented in Table 4. bAng II maximum dose is 80 ng/kg/min if needed, within the first 3 hours. Thereafter, max dose is 40 ng/kg/min. cAng II doses of 2.5‐5 ng/kg/min should be used when titrating down, or when MAP response necessitates.
START ANG II HERE
UP‐TITRATION
DOWN‐TIT
RATIO
N
Table 1: Angiotensin II Initiation Threshold
Drug Dose Ang II Starting Dose
Norepinephrine Equivalent
a + Vasopressin
0.1 g/kg/min 0.03 U/min
10 ng/kg/min aNorepinephrine equivalence adopted from Khanna, NEJM, 2017. See Table 4 for Norepinephrine Equivalent conversions.
START VASO HERE
Table 2: Vasopressin Initiation Threshold
Drug Dose Vasopressin Dose
Norepinephrine Equivalenta
0.05 g/kg/min
0.03 U/min
aNorepinephrine equivalence adopted from Khanna, NEJM, 2017. See Table 4 for Norepinephrine Equivalent conversions.
Table 4: Conversion to Norepinephrine Equivalenta
Drug Dose Norepinephrine Equivalent
Epinephrine 0.1 g/kg/min 0.1 g/kg/min Norepinephrine 0.1 g/kg/min 0.1 g/kg/min Dopamine 15 g/kg/min 0.1 g/kg/min Phenylephrine 1.0 g/kg/min 0.1 g/kg/min aNorepinephrine equivalence adopted from Khanna, NEJM, 2017.
1. Ang II should NOT be first‐line treatment
2. Ang II should not be used as a rescue therapy for moribund patients
3. Patient must have clinical features of distributive shock
4. Norepinephrine should be considered as first‐line therapy
5. With worsening shock and increasing vasopressor requirements (NE ≥ 0.05 mcg/kg/min), a balanced approach of vasopressors is recommended
Calcium
High-volume isovolemic hemofiltration
Methylene blue
Sodium bicarbonateSodium bicarbonate
Vitamin B12Vitamin B12
Steroids
Catecholamines Vasopressin
Vitamin C
Angiotensin IIAngiotensin II
?
?
?
??
?
Personalized approach
Page 45

Plasma vasopressin levels (AVP) of patients in septic shock and cardiogenic shock.
Donald W. Landry et al. Circulation. 1997;95:1122-1125
Copyright © American Heart Association, Inc. All rights reserved.
“Vasopressin plasma levels are inappropriately low in vasodilatory
shock”
Russell suggests that the dose of norepinephrine at baseline (5 μg per
kilogram per minute) in VASST identified patients who had profound
vasopressin deficiency, but...
Vasopressin levels in a convenience sample
Page 46
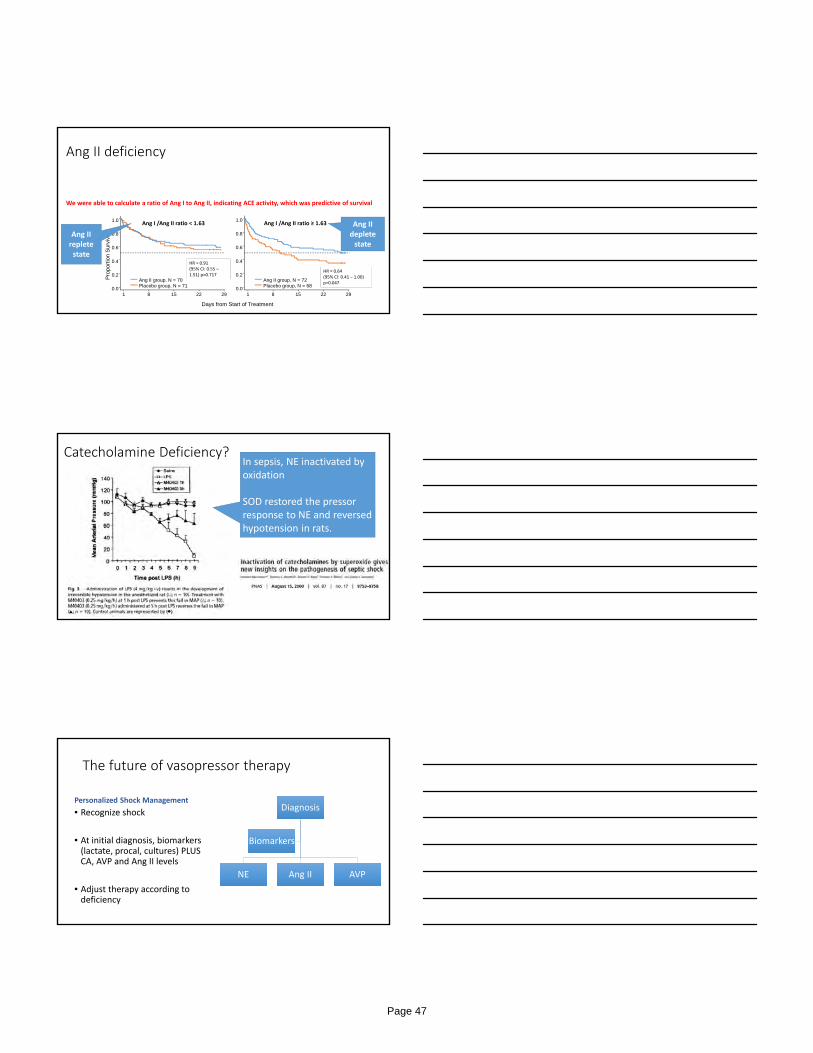
Ang II deficiency
We were able to calculate a ratio of Ang I to Ang II, indicating ACE activity, which was predictive of survival
Days from Start of Treatment
Pro
port
ion
Sur
vivi
ng
1 8 15 22 290.0
0.2
0.4
0.6
0.8
1.0
Ang II group, N = 70Placebo group, N = 71
1 8 15 22 290.0
0.2
0.4
0.6
0.8
1.0
Ang II group, N = 72Placebo group, N = 68
Ang I /Ang II ratio < 1.63 Ang I /Ang II ratio ≥ 1.63
HR = 0.91 (95% CI: 0.55 –1.51) p=0.717
Ang II replete state
Ang II deplete state
HR = 0.64 (95% CI: 0.41 – 1.00) p=0.047
Catecholamine Deficiency?In sepsis, NE inactivated by oxidation
SOD restored the pressor response to NE and reversed hypotension in rats.
The future of vasopressor therapy
Personalized Shock Management
• Recognize shock
• At initial diagnosis, biomarkers (lactate, procal, cultures) PLUS CA, AVP and Ang II levels
• Adjust therapy according to deficiency
Diagnosis
NE Ang II AVP
Biomarkers
Page 47
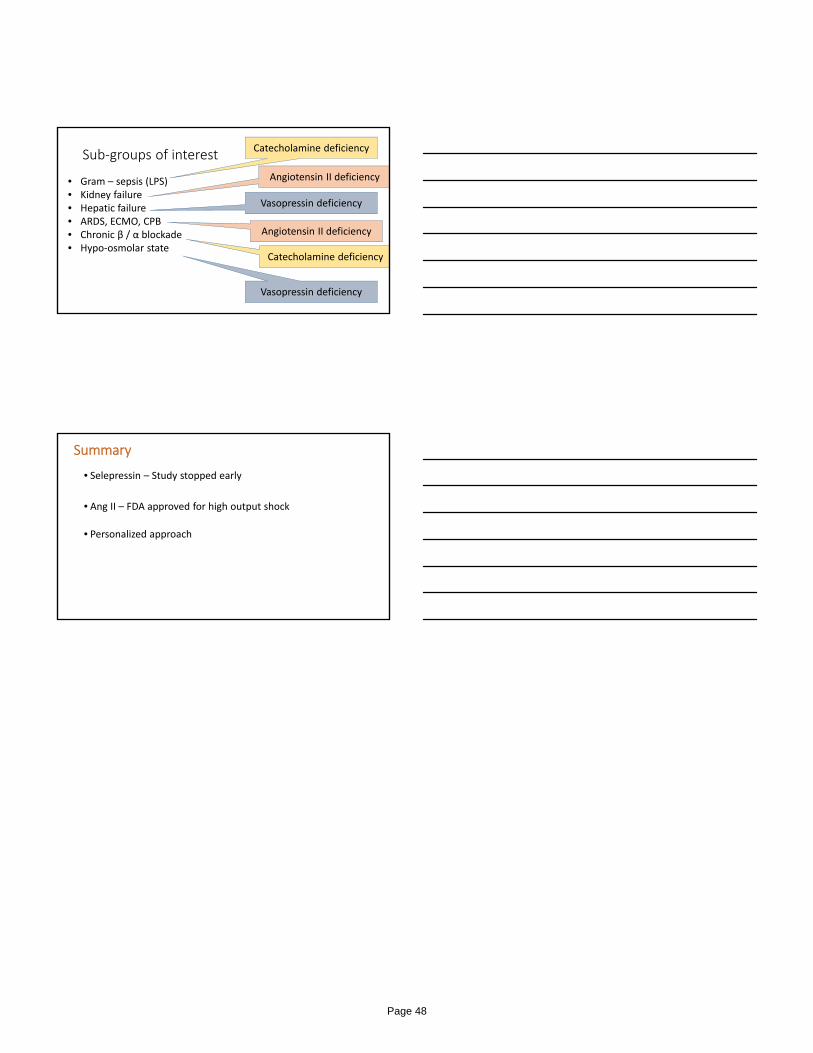
Sub‐groups of interest
• Gram – sepsis (LPS)• Kidney failure• Hepatic failure• ARDS, ECMO, CPB• Chronic β / α blockade• Hypo‐osmolar state
Catecholamine deficiency
Catecholamine deficiency
Vasopressin deficiency
Angiotensin II deficiency
Vasopressin deficiency
Angiotensin II deficiency
Summary
• Selepressin – Study stopped early
• Ang II – FDA approved for high output shock
• Personalized approach
Page 48
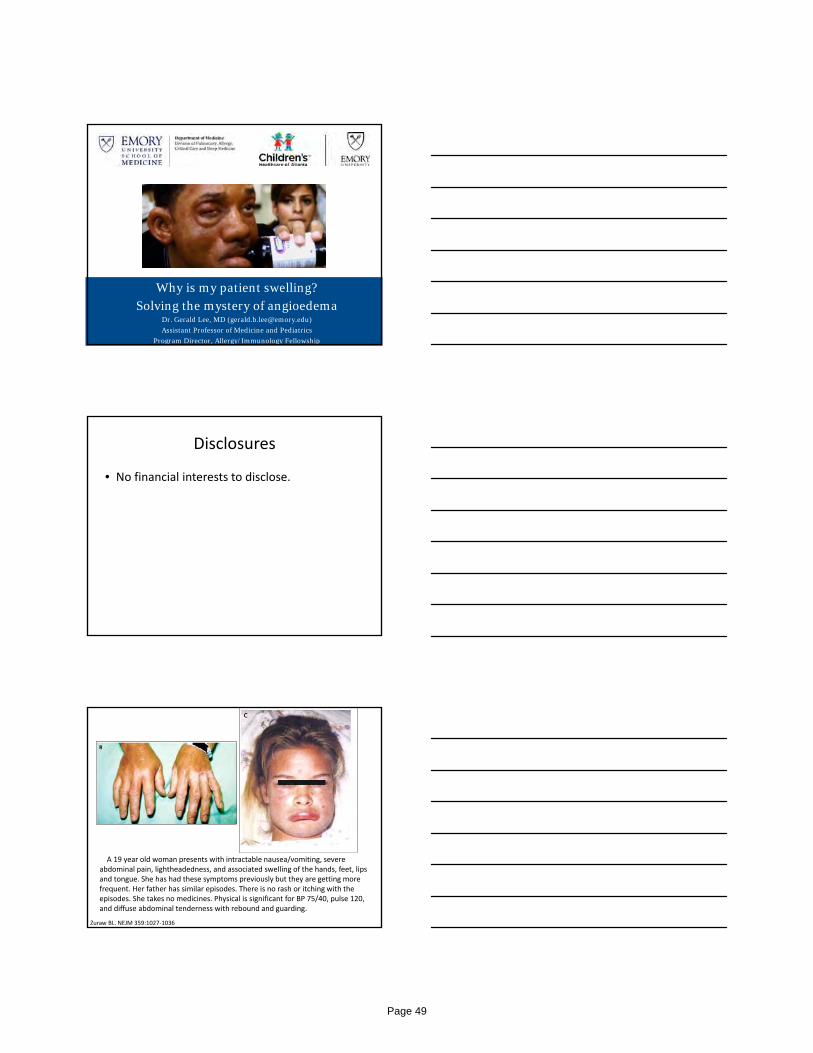
Why is my patient swelling?Solving the mystery of angioedema
Dr. Gerald Lee, MD ([email protected])
Assistant Professor of Medicine and Pediatrics
Program Director, Allergy/Immunology Fellowship
Disclosures
• No financial interests to disclose.
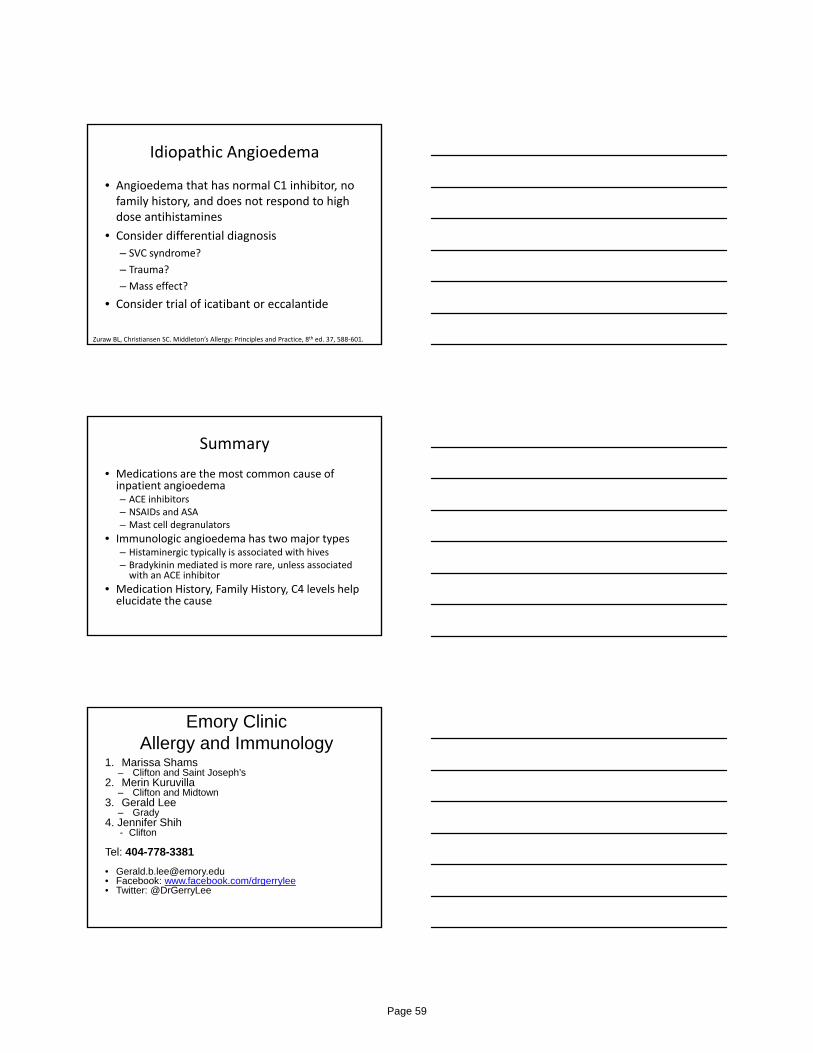
A 19 year old woman presents with intractable nausea/vomiting, severe abdominal pain, lightheadedness, and associated swelling of the hands, feet, lips and tongue. She has had these symptoms previously but they are getting more frequent. Her father has similar episodes. There is no rash or itching with the episodes. She takes no medicines. Physical is significant for BP 75/40, pulse 120, and diffuse abdominal tenderness with rebound and guarding.
Zuraw BL. NEJM 359:1027‐1036
Page 49
Learning Objectives
1. Describe the most common causes of angioedema in the ICU setting
2. Develop a diagnosis and treatment plan for angioedema
What is the most common causes of angioedema in the inpatient setting?
10 year experience at Mass General:
69 patients requiring treatment for angioedema• 20 requiring intubation• 93% secondary to medications
– ACE inhibitors– NSAIDS/ASA– Direct mast cell degranulators– Other: (antibiotics, chemotherapy, anesthesia, progesterone)
• 1 ‐ hereditary angioedema• 3 ‐ idiopathic
Banerji A et al. Allergy Asthma Proc 29:88–92, 2008
Nonspecific Mast Cell Degranulators
• Opiates• Radiocontrast Media• Vancomycin• Amphotericin B• Dextromethorphan• Ethanol• Polymyxin B• Quinine• Muscle relaxants (pancuronium, vercuronium better
tolerated)• Local anesthetics (lidocaine, prilocaine, bupivacaine better
tolerated)
Banerji A et al. Allergy Asthma Proc 29:88–92, 2008https://tmsforacure.org/wp‐content/uploads/2016‐TMS‐ER‐Protocol‐Pages‐2.pdf
Page 50
Banerji A et al. Allergy Asthma Proc 29:88–92, 2008
Majority of inpatient moderate to severe angioedema is due to combinations of medications
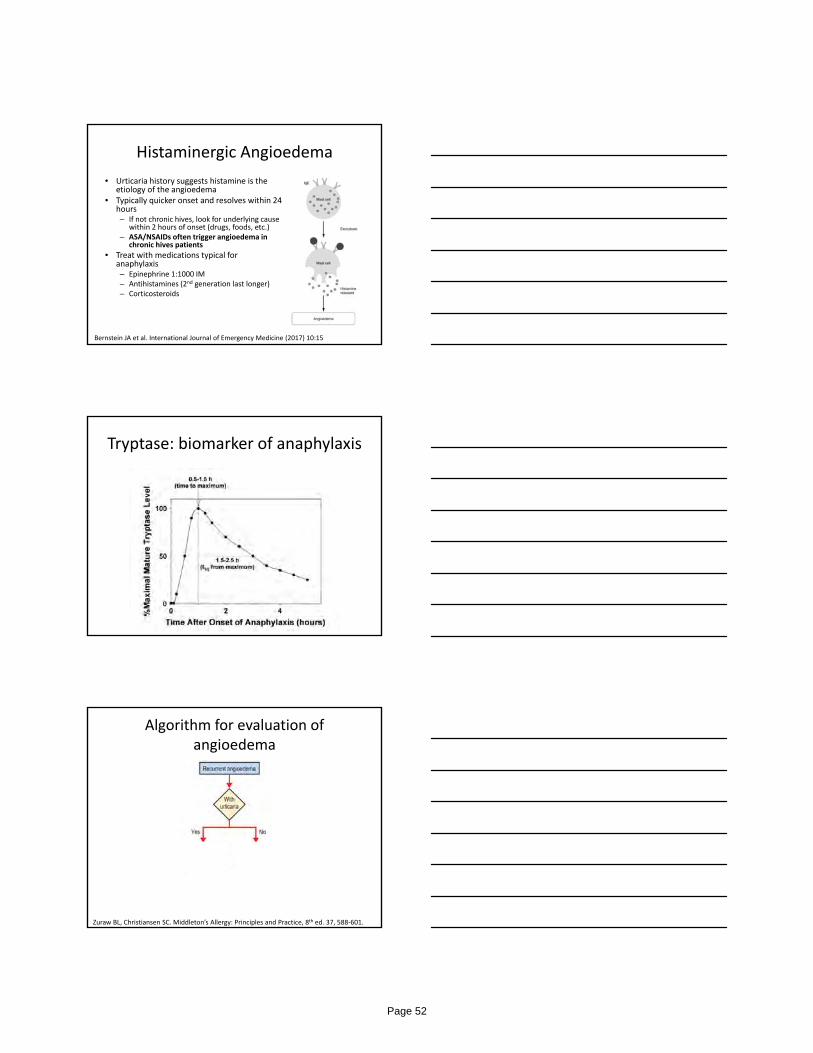
A 19 year old woman presents with intractable nausea/vomiting, severe abdominal pain, lightheadedness, and associated swelling of the hands, feet, lips and tongue. She has had these symptoms previously but they are getting more frequent. Her father has similar episodes. There is no rash or itching with the episodes. She takes no medicines. Physical is significant for BP 75/40, pulse 120, and diffuse abdominal tenderness with rebound and guarding.
Zuraw BL. NEJM 359:1027‐1036
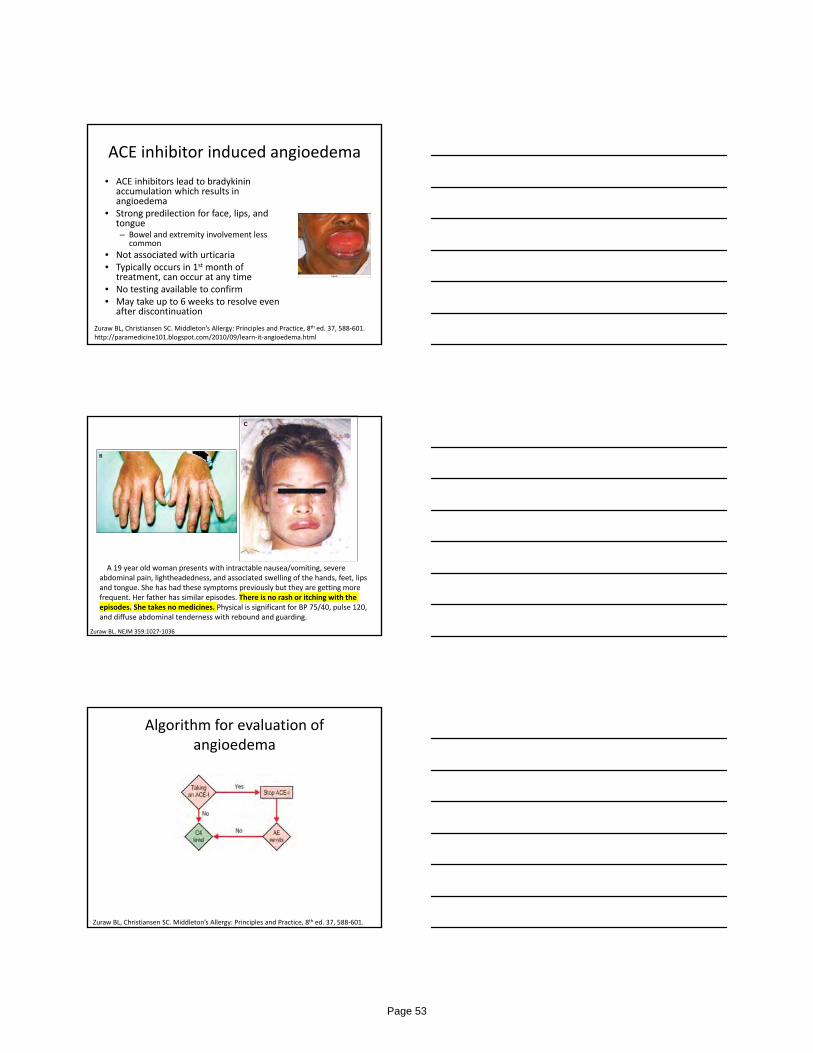
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 51
Histaminergic Angioedema
• Urticaria history suggests histamine is the etiology of the angioedema
• Typically quicker onset and resolves within 24 hours– If not chronic hives, look for underlying cause
within 2 hours of onset (drugs, foods, etc.)– ASA/NSAIDs often trigger angioedema in
chronic hives patients
• Treat with medications typical for anaphylaxis– Epinephrine 1:1000 IM– Antihistamines (2nd generation last longer)– Corticosteroids
Bernstein JA et al. International Journal of Emergency Medicine (2017) 10:15
Tryptase: biomarker of anaphylaxis
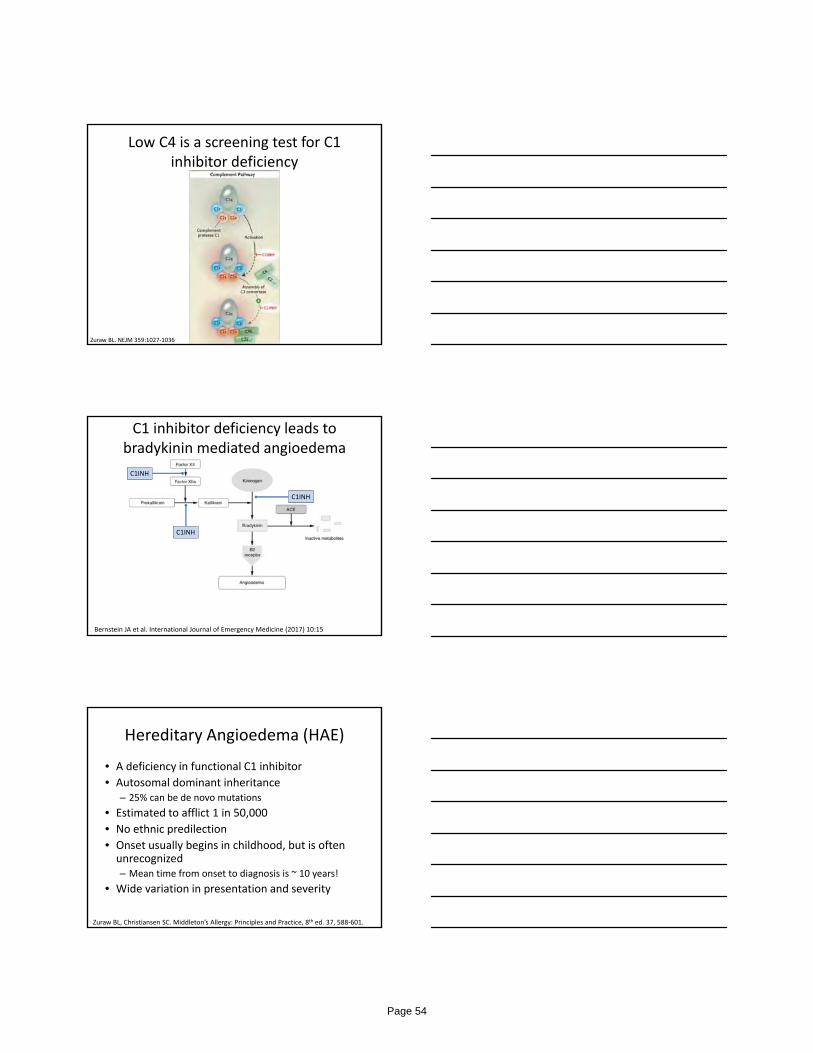
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 52
ACE inhibitor induced angioedema
• ACE inhibitors lead to bradykinin accumulation which results in angioedema
• Strong predilection for face, lips, and tongue– Bowel and extremity involvement less
common
• Not associated with urticaria• Typically occurs in 1st month of
treatment, can occur at any time• No testing available to confirm• May take up to 6 weeks to resolve even
after discontinuation
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601. http://paramedicine101.blogspot.com/2010/09/learn‐it‐angioedema.html
A 19 year old woman presents with intractable nausea/vomiting, severe abdominal pain, lightheadedness, and associated swelling of the hands, feet, lips and tongue. She has had these symptoms previously but they are getting more frequent. Her father has similar episodes. There is no rash or itching with the episodes. She takes no medicines. Physical is significant for BP 75/40, pulse 120, and diffuse abdominal tenderness with rebound and guarding.
Zuraw BL. NEJM 359:1027‐1036
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 53
Low C4 is a screening test for C1 inhibitor deficiency
Zuraw BL. NEJM 359:1027‐1036
Bernstein JA et al. International Journal of Emergency Medicine (2017) 10:15
C1INH
C1INH
C1INH
C1 inhibitor deficiency leads to bradykinin mediated angioedema
Hereditary Angioedema (HAE)
• A deficiency in functional C1 inhibitor
• Autosomal dominant inheritance– 25% can be de novo mutations
• Estimated to afflict 1 in 50,000
• No ethnic predilection
• Onset usually begins in childhood, but is often unrecognized– Mean time from onset to diagnosis is ~ 10 years!
• Wide variation in presentation and severity
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 54
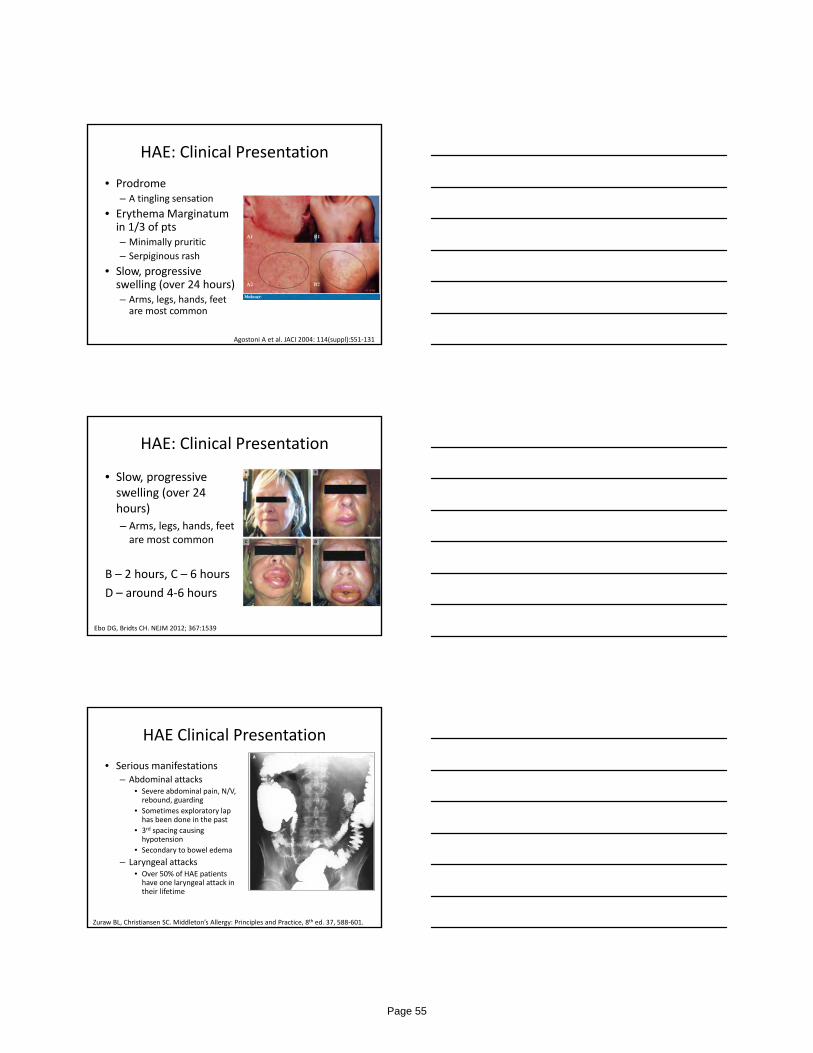
HAE: Clinical Presentation
• Prodrome– A tingling sensation
• Erythema Marginatumin 1/3 of pts– Minimally pruritic
– Serpiginous rash
• Slow, progressive swelling (over 24 hours)– Arms, legs, hands, feet are most common
Agostoni A et al. JACI 2004: 114(suppl):S51‐131
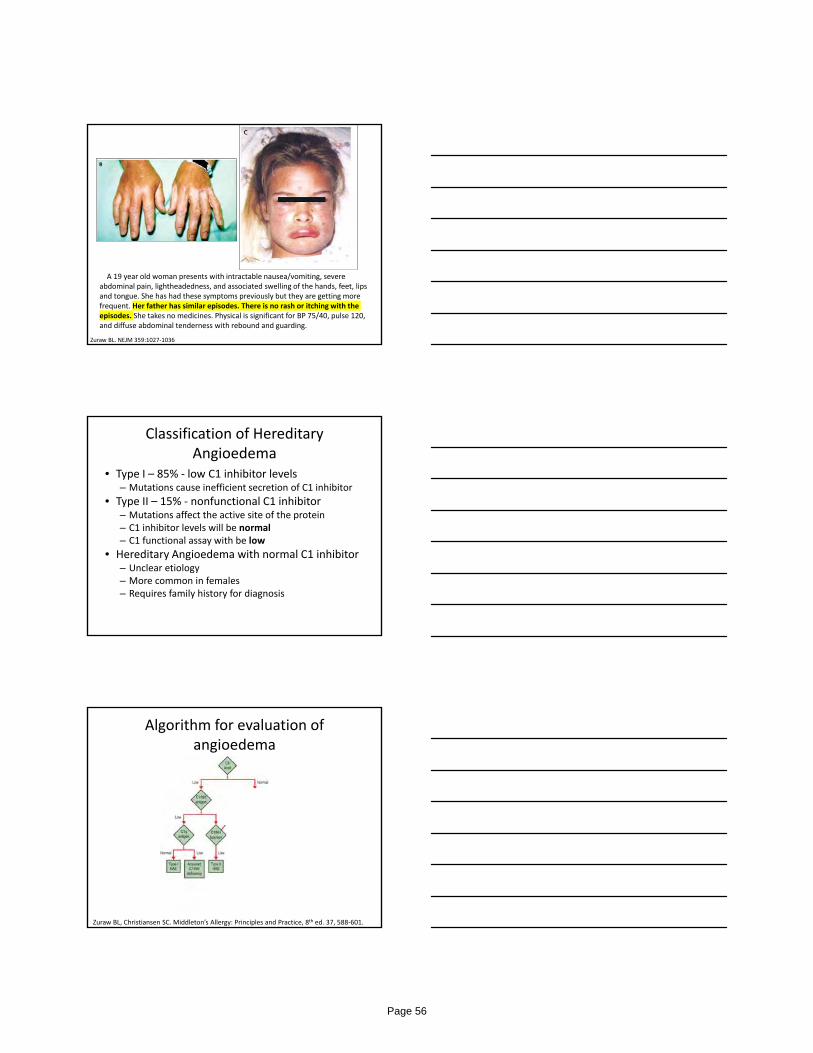
HAE: Clinical Presentation
• Slow, progressive swelling (over 24 hours)
– Arms, legs, hands, feet are most common
B – 2 hours, C – 6 hours
D – around 4‐6 hours
Ebo DG, Bridts CH. NEJM 2012; 367:1539
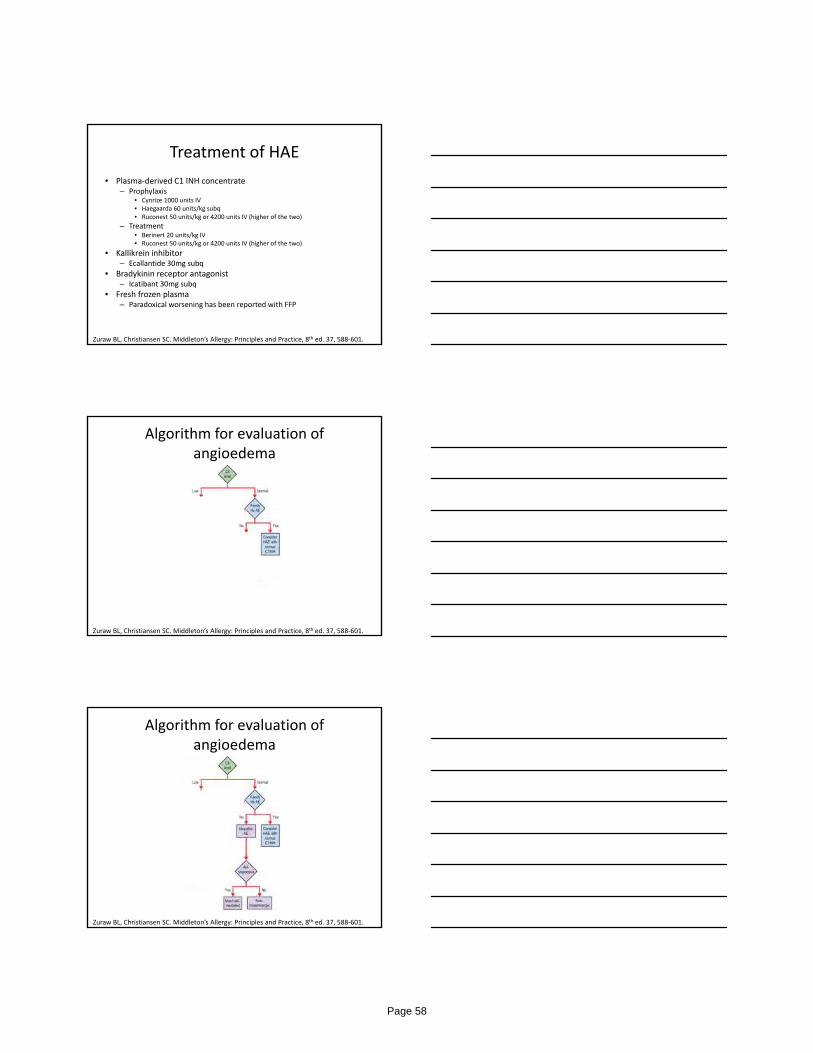
HAE Clinical Presentation
• Serious manifestations– Abdominal attacks
• Severe abdominal pain, N/V, rebound, guarding
• Sometimes exploratory lap has been done in the past
• 3rd spacing causing hypotension
• Secondary to bowel edema
– Laryngeal attacks• Over 50% of HAE patients have one laryngeal attack in their lifetime
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 55
A 19 year old woman presents with intractable nausea/vomiting, severe abdominal pain, lightheadedness, and associated swelling of the hands, feet, lips and tongue. She has had these symptoms previously but they are getting more frequent. Her father has similar episodes. There is no rash or itching with the episodes. She takes no medicines. Physical is significant for BP 75/40, pulse 120, and diffuse abdominal tenderness with rebound and guarding.
Zuraw BL. NEJM 359:1027‐1036
Classification of Hereditary Angioedema
• Type I – 85% ‐ low C1 inhibitor levels– Mutations cause inefficient secretion of C1 inhibitor
• Type II – 15% ‐ nonfunctional C1 inhibitor– Mutations affect the active site of the protein– C1 inhibitor levels will be normal– C1 functional assay with be low
• Hereditary Angioedema with normal C1 inhibitor– Unclear etiology– More common in females– Requires family history for diagnosis
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 56

Acquired Angioedema
• Associated with malignancy (lymphoproliferative) or autoimmune disease
• Onset at 4th decade of life or later (not hereditary)
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Laboratory evaluation
Diagnosis C4 C1 INH level
C1 INH function
C1q
HAEType I
nl
HAE Type II nl nl
Acquired C1 INH deficiency
nl or nl
HAE with normal C1INH
nl nl nl nl
ACEI induced AE
nl nl nl nl
Page 57
Treatment of HAE
• Plasma‐derived C1 INH concentrate– Prophylaxis
• Cynrize 1000 units IV• Haegaarda 60 units/kg subq• Ruconest 50 units/kg or 4200 units IV (higher of the two)
– Treatment• Berinert 20 units/kg IV• Ruconest 50 units/kg or 4200 units IV (higher of the two)
• Kallikrein inhibitor– Ecallantide 30mg subq
• Bradykinin receptor antagonist– Icatibant 30mg subq
• Fresh frozen plasma– Paradoxical worsening has been reported with FFP
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Algorithm for evaluation of angioedema
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Page 58
Idiopathic Angioedema
• Angioedema that has normal C1 inhibitor, no family history, and does not respond to high dose antihistamines
• Consider differential diagnosis
– SVC syndrome?
– Trauma?
– Mass effect?
• Consider trial of icatibant or eccalantide
Zuraw BL, Christiansen SC. Middleton’s Allergy: Principles and Practice, 8th ed. 37, 588‐601.
Summary
• Medications are the most common cause of inpatient angioedema– ACE inhibitors– NSAIDs and ASA– Mast cell degranulators
• Immunologic angioedema has two major types– Histaminergic typically is associated with hives– Bradykinin mediated is more rare, unless associated with an ACE inhibitor
• Medication History, Family History, C4 levels help elucidate the cause
Emory ClinicAllergy and Immunology
1. Marissa Shams– Clifton and Saint Joseph’s
2. Merin Kuruvilla– Clifton and Midtown
3. Gerald Lee– Grady
4. Jennifer Shih- Clifton
Tel: 404-778-3381
• [email protected]• Facebook: www.facebook.com/drgerrylee• Twitter: @DrGerryLee
Page 59
Kyle Gunnerson, MD, FCCMChief, Division of Emergency Critical CareAssociate Professor, Departments of Emergency Medicine, Internal Medicine, and AnesthesiologyUniversity of Michigan Health System
Federal Grant Funding A Multimodal Integrative Platform for Continuous Monitoring and Decision Support during Postoperative
Care in Cardiac Patients. BA150235 Army‐DoD‐US‐ 16‐PAF04693: Co‐I with effort
Strategies to Innovate EmeRgENcy Care Clinical Trials Network (SIREN)‐Michigan Collaborative. NINDS/NHLBI 1 U24 NS100680‐01: Site‐PI (Spoke)
Clinical Centers (CC) for the NHLBI Prevention and Early Treatment of Acute Lung Injury(PETAL) Clinical Trials Network. 5 U01 HL123031‐07: Co‐I with effort
Extracorporeal CPR for Refractory Out‐of‐Hospital Cardiac Arrest (EROCA) Trial Planning Grant. NHLBI 1R34HL130738‐01A1: Co‐I with effort
Committees American Board of Internal Medicine ‐ Critical Care Subspecialty (2010‐2016) Society of Critical Care Medicine – Council Member (2016‐current)
Institutional Funding University of Michigan Health System ‐ Peking University Health Science Center Joint Institute –
Development of ED‐ICU severity scoring system ED‐ECMO team simulation – University of Michigan Simulation Center Grant
Current perspective of Critical Care in the ED
University of Michigan approach (ED based ICU)
How we did it (process)
Operations, Clinical, Educational, Research
Year to date results
Page 60
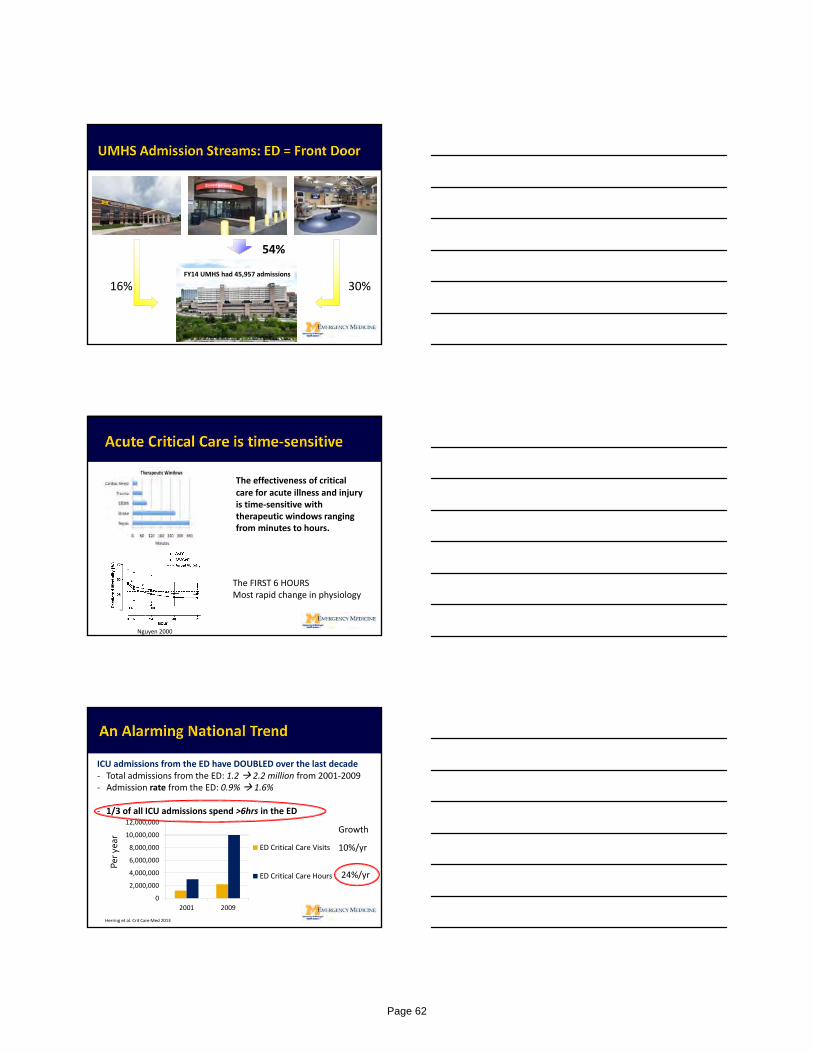
One of the largest single center health systems in the world. 2017 ranked 6th in USNWR
> 6.3 M square feet of clinical space 1000 beds 180 ICU beds
> 2.3 M patient clinic visits/yr> 48,700 inpatient stays > 54,300 surgical cases
> 104,000 Emergency Department Visits $512M/yr research grants (10th NIH)
Adult ED ED patient population – complex tertiary/quaternary care
Current volume – 70,000 ‐ 75,000 adults/year
Admit rate – 35%
ICU admit rate – 10% of admissions
Transfer call volume – 350 ‐ 400/month
Transfer call decline – 750/year (25% ICU level)
LBE Rate – 3%
Volume projection – 2 ‐ 3% annual increase overall, 10% critical care
Why is this important…NOW?
Page 61
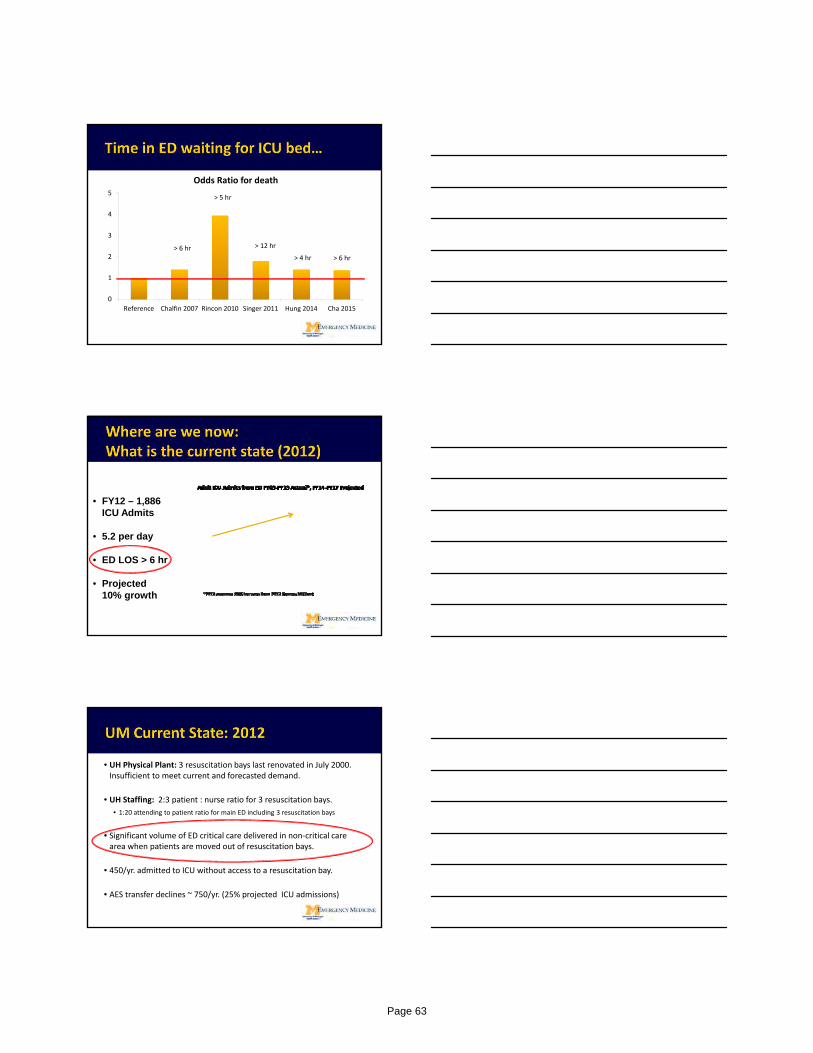
16% 30%
54%
FY14 UMHS had 45,957 admissions
The effectiveness of critical care for acute illness and injury is time‐sensitive with therapeutic windows ranging from minutes to hours.
The FIRST 6 HOURSMost rapid change in physiology
Nguyen 2000
ICU admissions from the ED have DOUBLED over the last decade‐ Total admissions from the ED: 1.2 2.2 million from 2001‐2009‐ Admission rate from the ED: 0.9% 1.6%
‐ 1/3 of all ICU admissions spend >6hrs in the ED
0
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
12,000,000
2001 2009
ED Critical Care Visits
ED Critical Care Hours
Herring et al. Crit Care Med 2013
Per yea
r
10%/yr
24%/yr
Growth
Page 62
0
1
2
3
4
5
Reference Chalfin 2007 Rincon 2010 Singer 2011 Hung 2014 Cha 2015
Odds Ratio for death
> 6 hr
> 5 hr
> 12 hr
> 4 hr > 6 hr
• FY12 – 1,886 ICU Admits
• 5.2 per day
• ED LOS > 6 hr
• Projected 10% growth
• UH Physical Plant: 3 resuscitation bays last renovated in July 2000. Insufficient to meet current and forecasted demand.
• UH Staffing: 2:3 patient : nurse ratio for 3 resuscitation bays. • 1:20 attending to patient ratio for main ED including 3 resuscitation bays
• Significant volume of ED critical care delivered in non‐critical care area when patients are moved out of resuscitation bays.
• 450/yr. admitted to ICU without access to a resuscitation bay.
• AES transfer declines ~ 750/yr. (25% projected ICU admissions)
Page 63

• Execution of the UMHS Strategic Plan to double adult high complexity market share (from 6%‐ to 12%) will amplify the demand for emergency critical care in our system
•The emergency care system, in it's current structure, is not prepared to respond to these challenges.
Increasing ED visits
Increasing ICU demand (ED and transfers)
Increasing ED LOS for our ICU patients
Outcomes?
Page 64
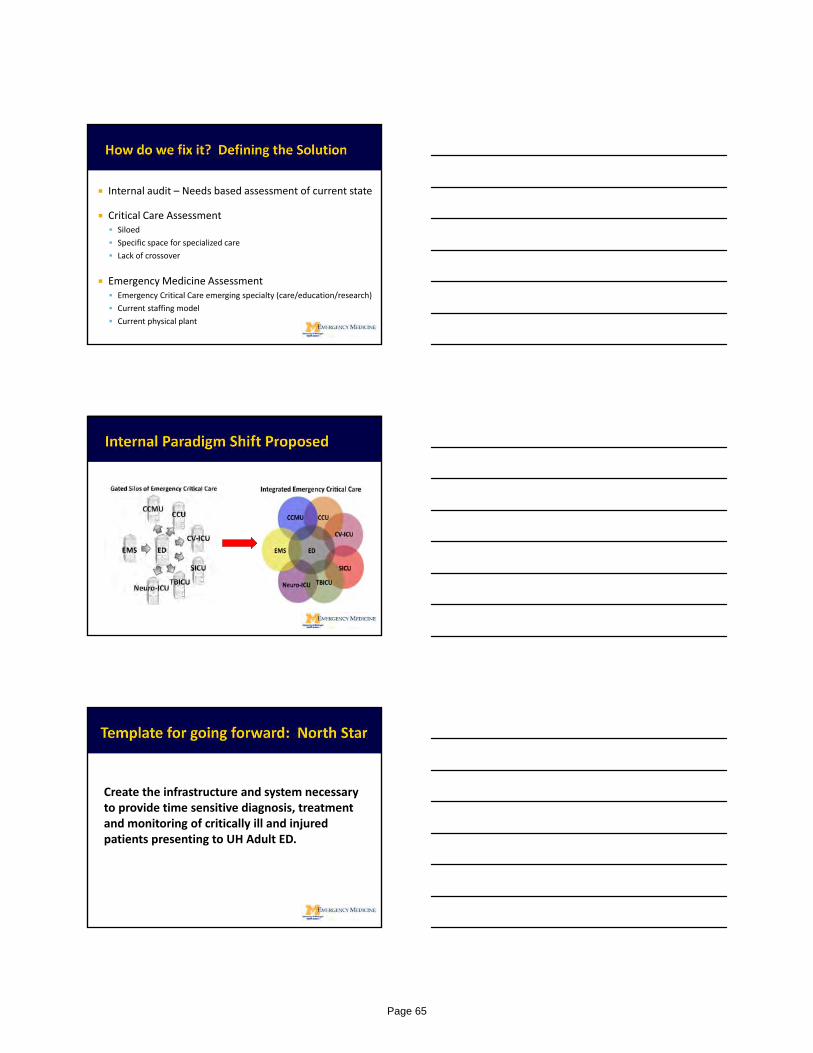
Internal audit – Needs based assessment of current state
Critical Care Assessment Siloed
Specific space for specialized care
Lack of crossover
Emergency Medicine Assessment Emergency Critical Care emerging specialty (care/education/research)
Current staffing model
Current physical plant
Create the infrastructure and system necessary to provide time sensitive diagnosis, treatment and monitoring of critically ill and injured patients presenting to UH Adult ED.
Page 65

Page 66
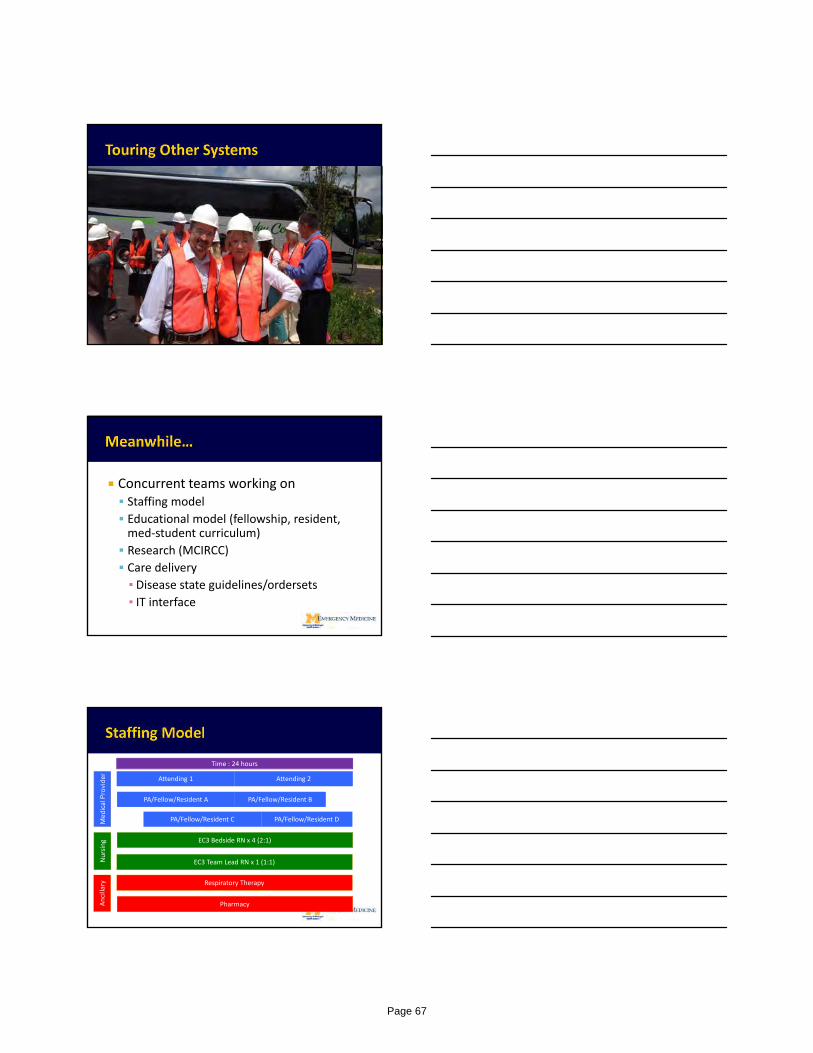
Concurrent teams working on Staffing model
Educational model (fellowship, resident, med‐student curriculum)
Research (MCIRCC)
Care delivery
▪ Disease state guidelines/ordersets▪ IT interface
Attending 1 Attending 2
PA/Fellow/Resident A PA/Fellow/Resident B
PA/Fellow/Resident C PA/Fellow/Resident D
EC3 Bedside RN x 4 (2:1)
EC3 Team Lead RN x 1 (1:1)
Respiratory Therapy
Pharmacy
MedicalProvider
Nursing
Ancillary
Time : 24 hours
Page 67
EM Attendings
Core – 4 EM/Intensivist (2018 there are 6)
Not fellowship trained:
▪ 2 Day FCCS course hosted locally and taught by EM intensivists as well as other inpatient intensivists (also PAs participation)
▪ Monthly chart review
▪ Monthly divisional meeting requirement
▪ Monthly CCM CME requirement
Nurses
CCRN‐ Director of Critical Care Nursing Education
Essentials of Critical Care Orientation from AACN
▪ Initially ‐ 8 week ICU orientation
▪ PDCA cycle performed with many tweaks to orientation
▪ Sweet spot – 4 weeks in CCMU, 4 weeks in EC3 (2‐3 as staff nurse, 1‐2 as EC3 TL)
Didactic education and equipment overview – 8 hours
Dedicated CC curriculum Frequent “hands on” workshops (airway, CC boot camp) Medical Students 4 senior “sub‐internship” month for MS4
Residents 1st and 2nd years spend 2‐4 weeks Integrative for 3rd and 4th year EM residents Rotators:
▪ IM residents▪ Ob/Gyn residents▪ Interest from outside residents
Fellowship Rotations Anesth CC – mandatory Neuro CC – mandatory Pulm/CC and Surg CC ‐ elective
Page 68
2 ACGME pathways (Anesth CC and IM CC) 1 fellow EACH pathway per year (4 total) Training primarily in each respective program EC3 rotations at least 6 total in 2 years (more?)
Included in EM‐CC divisional meetings EM CC Division – Education committee EC3 specific journal club and other educational opportunities
Teach MS/residents
Expand clinical research infrastructure in critical care in synergy with the newly established M‐CIRCC
EC3 functions similar as traditional ICU – only earlier in course of treatment
Three NIH funded (PETAL, SIREN, EROCA)
Recently awarded NIH K12 Career Development in Emergency Critical Care
Goal – 24/7 ‐ Early subject identification and enrollment to facilitate time sensitive diagnostics, monitoring, and research protocols
Page 69

Critical Care Translational ScienceBest in Class
Together, we will change the face of Critical Care Medicine
CC Advisory group met once a month – now quarterly
Order sets created in MiChart (EPIC)
Discuss operational and care issues – Address in PDCA format
RT, Pharmacy, Nursing, Social Work
Page 70
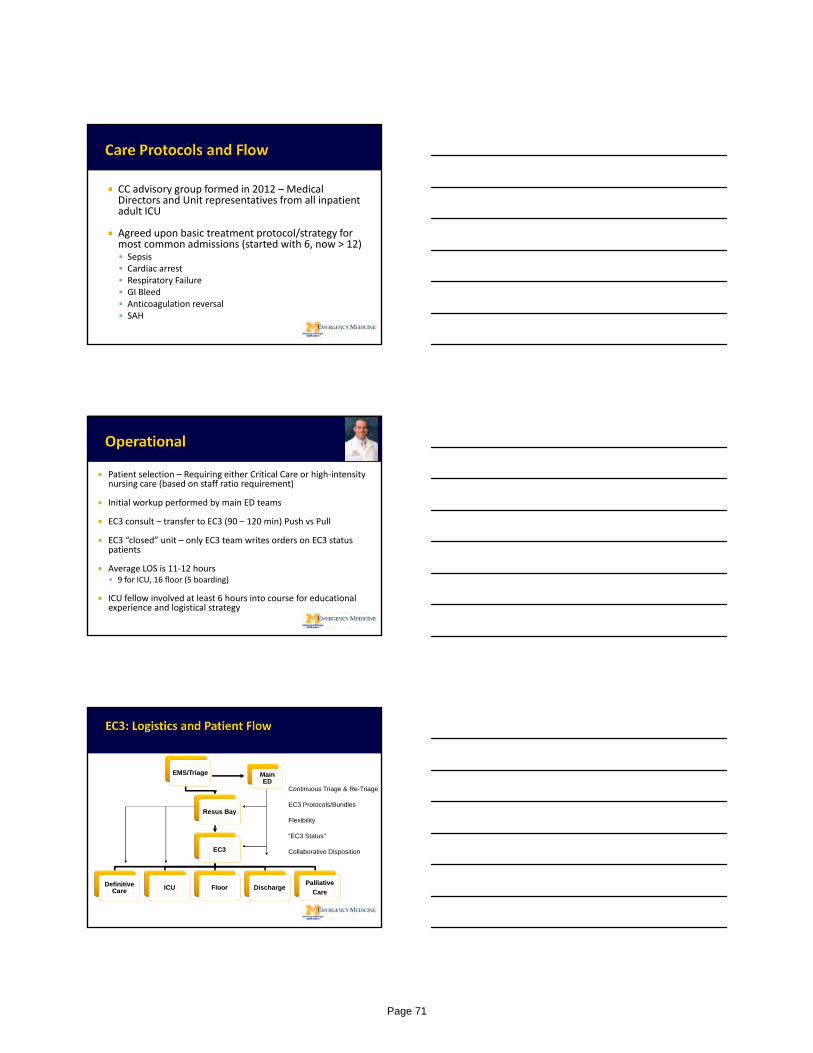
CC advisory group formed in 2012 – Medical Directors and Unit representatives from all inpatient adult ICU
Agreed upon basic treatment protocol/strategy for most common admissions (started with 6, now > 12) Sepsis Cardiac arrest Respiratory Failure GI Bleed Anticoagulation reversal SAH
Patient selection – Requiring either Critical Care or high‐intensity nursing care (based on staff ratio requirement)
Initial workup performed by main ED teams
EC3 consult – transfer to EC3 (90 – 120 min) Push vs Pull
EC3 “closed” unit – only EC3 team writes orders on EC3 status patients
Average LOS is 11‐12 hours 9 for ICU, 16 floor (5 boarding)
ICU fellow involved at least 6 hours into course for educational experience and logistical strategy
EMS/TriageEMS/Triage
Resus BayResus Bay
EC3EC3
Definitive Care
Definitive Care ICUICU FloorFloor DischargeDischarge
Palliative
Care
Palliative
Care
Main ED
Main ED
Continuous Triage & Re-Triage
EC3 Protocols/Bundles
Flexibility
“EC3 Status”
Collaborative Disposition
Page 71
Engage frontline workers to create optimal workflows and eliminate waste
Architects and designers transform process maps into a design
Focus on removing physical barriers from the workflows
Paradigm shift of architects from project leads to team member and facilitators
Existing space vacated when pediatric ED relocated
Page 72

Multidisciplinary groups all walked through mockup with valuable input and ideas over the course of 2 weeks.
UM with lead architect, division director, director of operations, project manager, facilities manager.
Feedback from physicians, nurses, RT, Pharmacist, Medics, In‐patient teams
Page 73
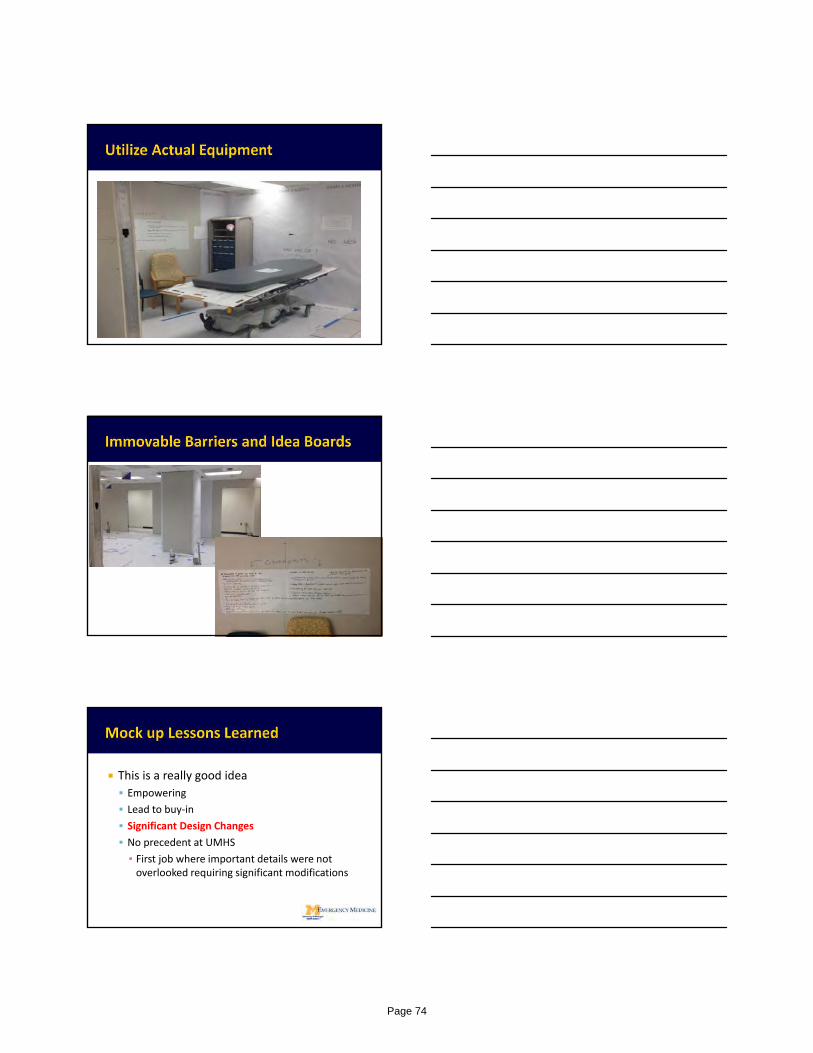
This is a really good idea
Empowering
Lead to buy‐in
Significant Design Changes
No precedent at UMHS
▪ First job where important details were not overlooked requiring significant modifications
Page 74
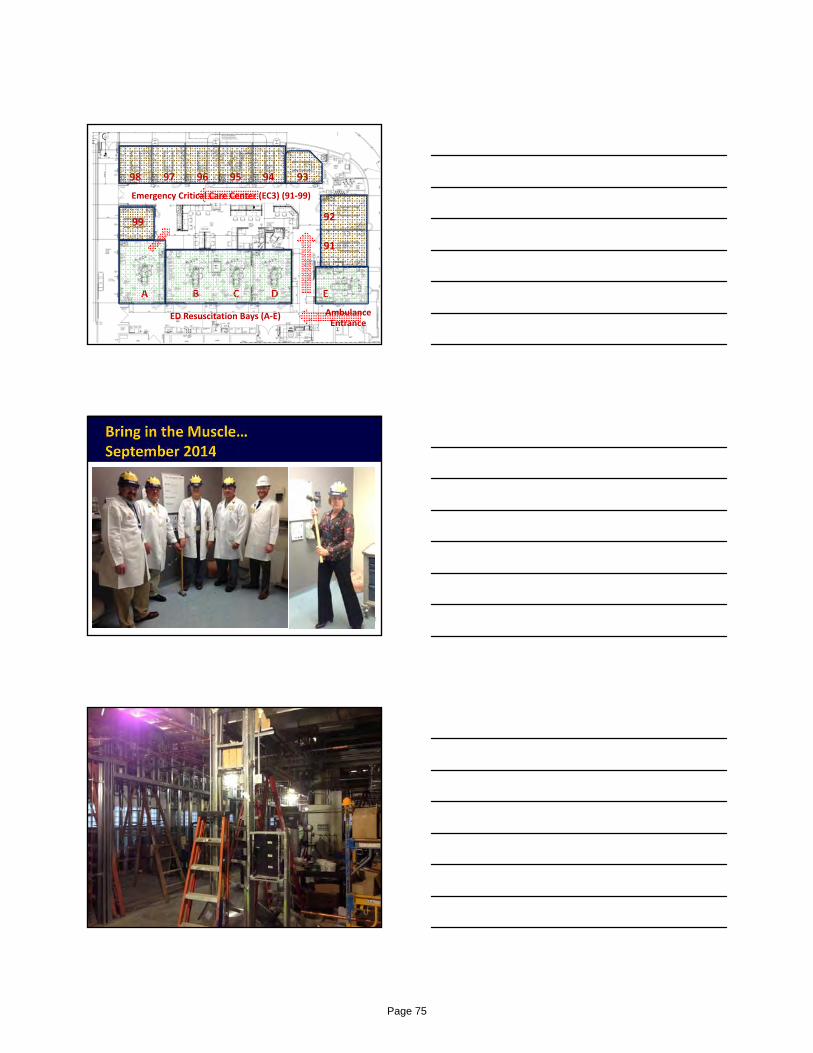
Emergency Critical Care Center
99
98 97 96 95
92
9394
EDCBA
91
Emergency Critical Care Center (EC3) (91‐99)
ED Resuscitation Bays (A‐E) Ambulance Entrance
Page 75
Joyce and Don Massey Family Foundation Emergency Critical Care Center
Cold, CAT scan in zone
No crowd control
Patients and families not in ideal environment at their greatest time of need.
Page 76

Cluttered, old, poorly designed boom systems.
ER flea market with tons of equipment pushed to the back. Can’t find anything quickly
Direct Access to EC3
Multiple Video Displays
Cameras for QA and Teaching
Page 77
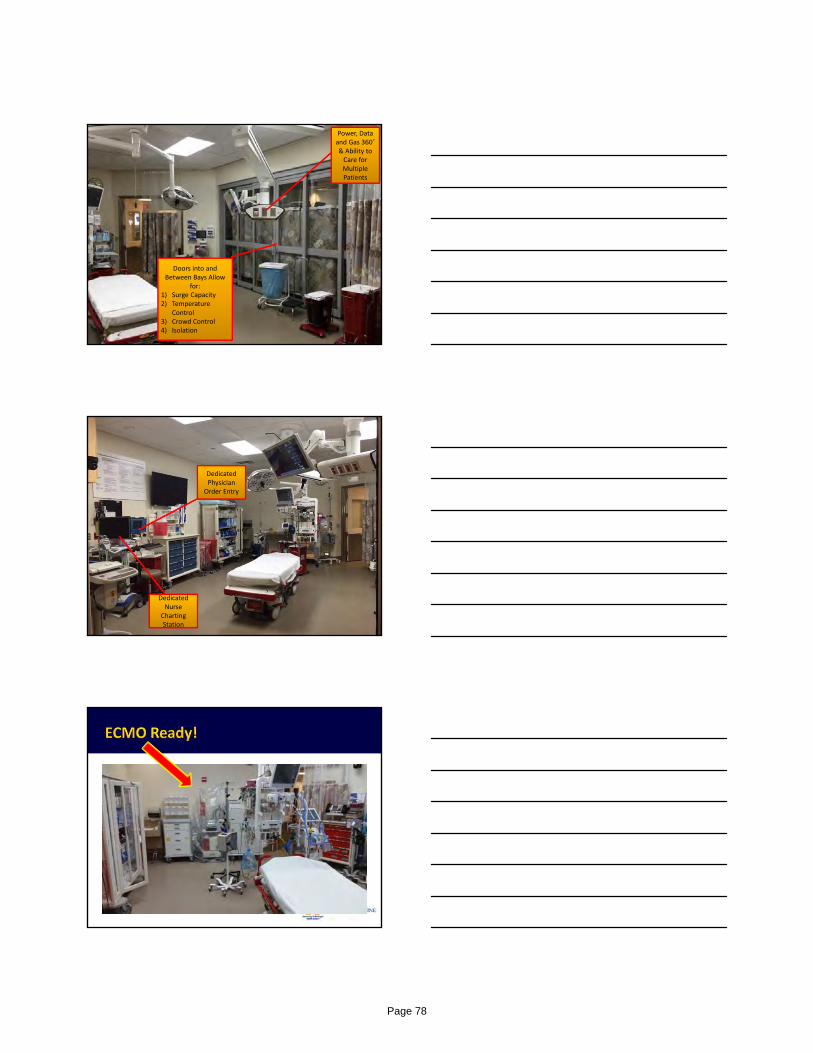
Doors into and Between Bays Allow
for:1) Surge Capacity2) Temperature
Control3) Crowd Control4) Isolation
Power, Data and Gas 360˚ & Ability to Care for Multiple Patients
Dedicated Nurse
Charting Station
Dedicated Physician
Order Entry
Page 78
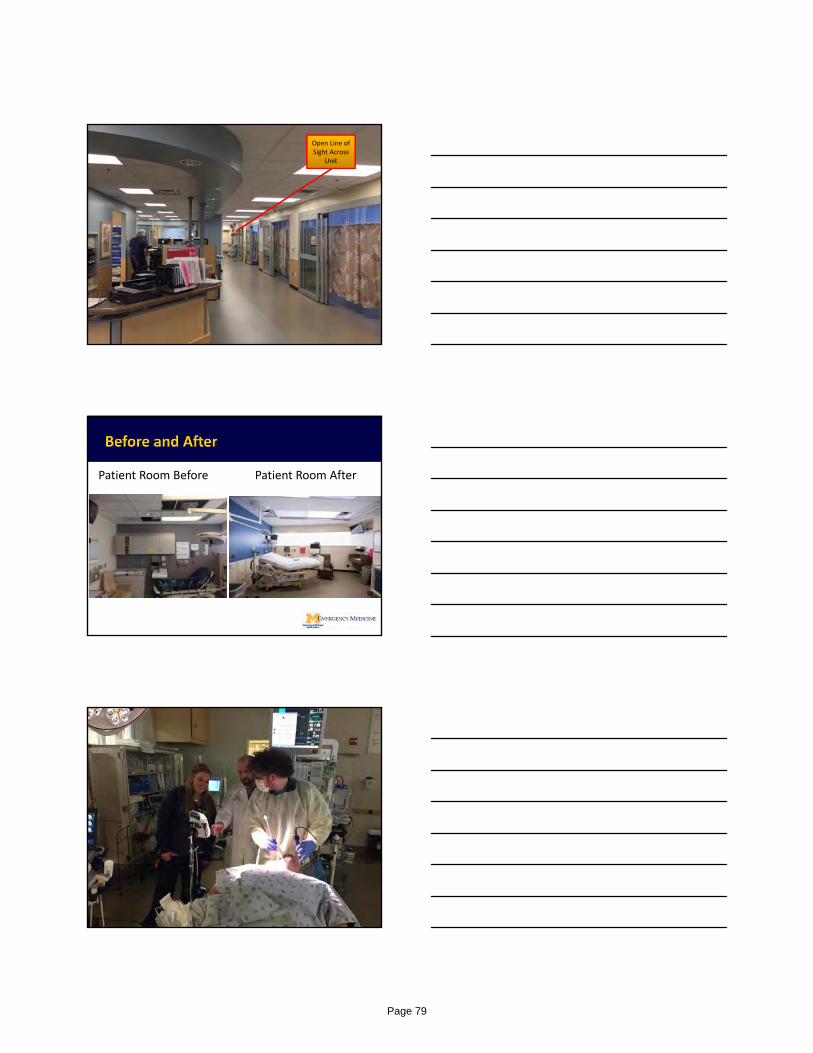
Open Line of Sight Across
Unit
Patient Room Before Patient Room After
file:///.file/id=6571367.12173219
Page 79

Fiberoptic video image can be displayed on multiple HD screens around RESUS bay
Multiple image display options
Page 80
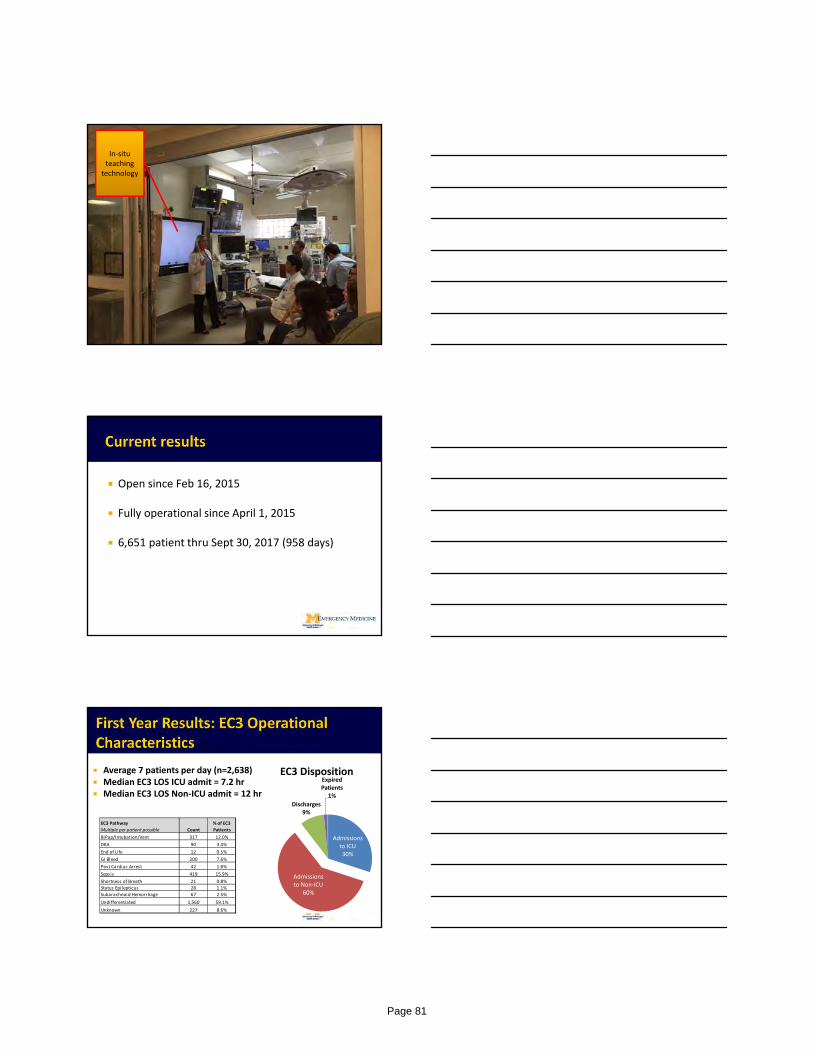
In‐situ teaching
technology
Open since Feb 16, 2015
Fully operational since April 1, 2015
6,651 patient thru Sept 30, 2017 (958 days)
Admissions to ICU 30%
Admissions to Non‐ICU
60%
Discharges9%
Expired Patients
1%
EC3 Disposition Average 7 patients per day (n=2,638) Median EC3 LOS ICU admit = 7.2 hr Median EC3 LOS Non‐ICU admit = 12 hr
BiPap/Intubation/Vent 317 12.0%
DKA 90 3.4%
End of Life 12 0.5%
GI Bleed 200 7.6%
Post Cardiac Arrest 42 1.6%
Sepsis 419 15.9%
Shortness of Breath 21 0.8%
Status Epilepticus 28 1.1%
Subarachnoid Hemorrhage 67 2.5%
Undifferentiated 1,560 59.1%
Unknown 227 8.6%
% of EC3
PatientsCount
EC3 Pathway
Multiple per patient possible
Page 81
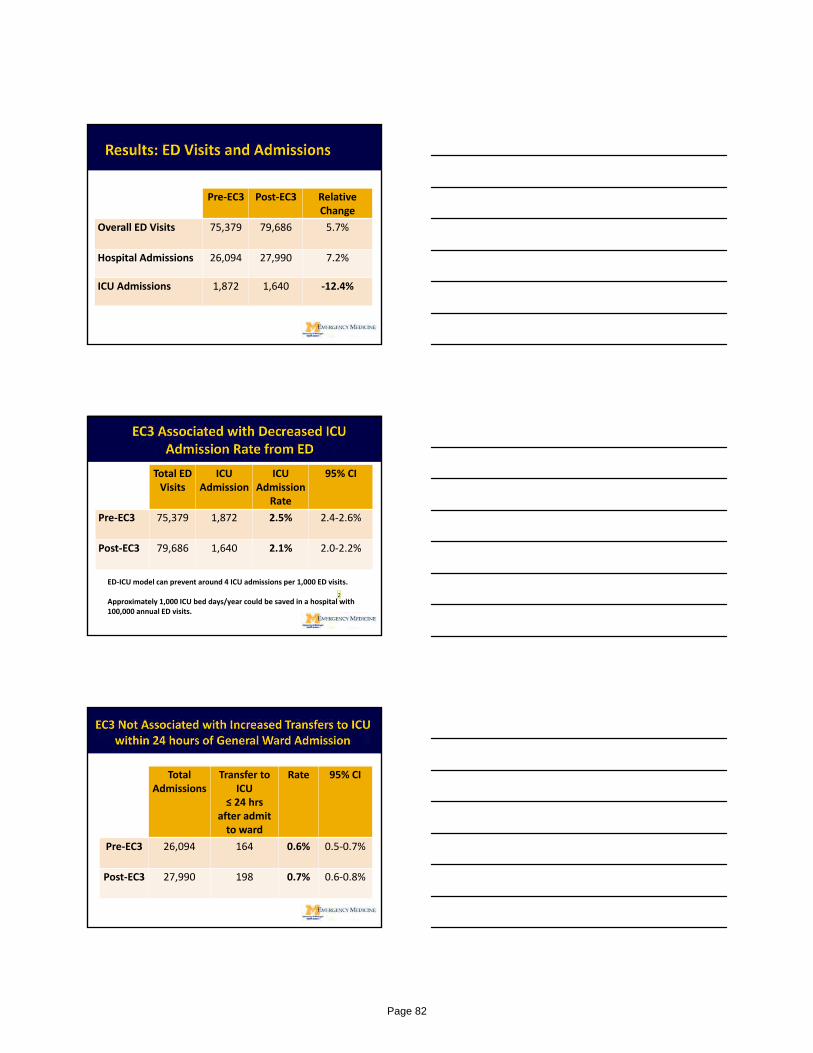
Pre‐EC3 Post‐EC3 Relative Change
Overall ED Visits 75,379 79,686 5.7%
Hospital Admissions 26,094 27,990 7.2%
ICU Admissions 1,872 1,640 ‐12.4%
Total ED Visits
ICU Admission
ICU Admission
Rate
95% CI
Pre‐EC3 75,379 1,872 2.5% 2.4‐2.6%
Post‐EC3 79,686 1,640 2.1% 2.0‐2.2%
ED‐ICU model can prevent around 4 ICU admissions per 1,000 ED visits.
Approximately 1,000 ICU bed days/year could be saved in a hospital with 100,000 annual ED visits.
2
Total Admissions
Transfer to ICU
≤ 24 hrsafter admit to ward
Rate 95% CI
Pre‐EC3 26,094 164 0.6% 0.5‐0.7%
Post‐EC3 27,990 198 0.7% 0.6‐0.8%
Page 82
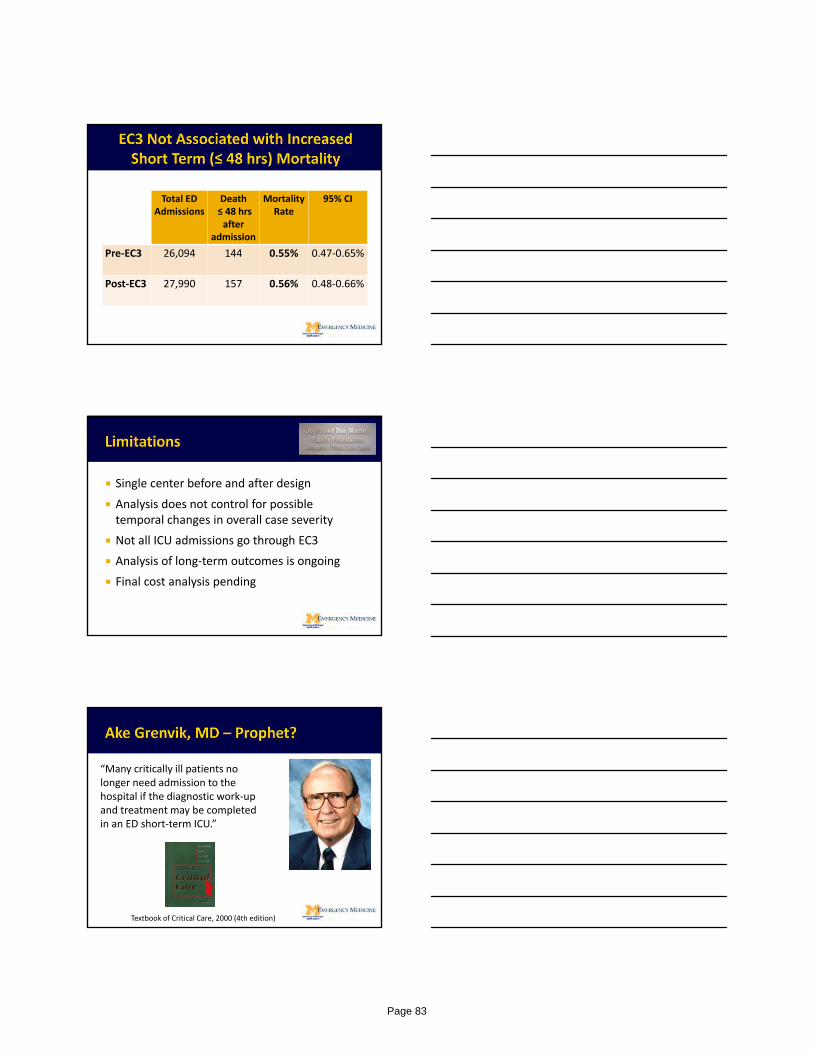
Total ED Admissions
Death≤ 48 hrsafter
admission
MortalityRate
95% CI
Pre‐EC3 26,094 144 0.55% 0.47‐0.65%
Post‐EC3 27,990 157 0.56% 0.48‐0.66%
Single center before and after design
Analysis does not control for possible temporal changes in overall case severity
Not all ICU admissions go through EC3
Analysis of long‐term outcomes is ongoing
Final cost analysis pending
“Many critically ill patients no longer need admission to the hospital if the diagnostic work‐up and treatment may be completed in an ED short‐term ICU.”
Textbook of Critical Care, 2000 (4th edition)
Page 83
Emergency based ICU is a safe and effective approach towards addressing current increases in demand of high acuity, traditional ICU patient, especially the < 24hr ICU admit
Takes a large multidisciplinary team approach
Cannot do this alone in the ED
Using a formal “LEAN” based approach was very effective in identifying and addressing obstacles and incorporating “best” practice strategies.
Continued data‐driven outcomes is essential to ongoing success
Page 84
MANAGEMENT OF THE ORGAN DONOR: Searching for the Evidence
Ram Subramanian, MD Medical Director, Liver Transplant
Hepatology and Critical Care
Emory Transplant Center
Disclosures: None
OUTLINE• Review pathophysiology of systemic derangements
related to brain death, and compare to physiology of septic shock
• Discuss management issues in specific systems:
– Cardiovascular
– Pulmonary
– Endocrine
• Describe research advances in donor management
• Review recent advances in the utilization of HIV and HCV positive donors
Pathophysiology of Critical Illness in Brain Death (1)
• Cardiovascular:– Progressive brain herniation results in an initial
catecholamine storm with associated hypertension, with subsequent spinal shock associated distributive shock(similar to septic shock physiology?)
• Pulmonary: – Risk for cardiogenic and non-cardiogenic pulmonary
edema associated hypoxemia, due to catecholamine storm associated hypertension and systemic cytokine mediated inflammatory response (similarity to extrathoracic/septic ARDS?)
Page 85
Pathophysiology (2)
• Endocrine: – Loss of posterior pituitary function, resulting in diabetes
insipidus associated hypotension and hypernatremia.– Possible derangements in ACTH and TRH, resulting in
adrenal insufficiency (similar to septic shock?) and thyroid hormone dysfunction
• Inflammatory:– Systemic pro-inflammatory cytokine mediated
inflammatory response possibly resulting from injured neural tissue and end organ ischemia-reperfusion injury (similarities to SIRS response in sepsis?)
Management of Organ System Derangements
CV Management (1):Fluid Management
• Target volume status? : Euvolemia vs Hypervolemia– Restrictive fluid strategy (CVP <6 mm Hg) shown not to adversely
affect renal graft survival or increase DGF (Minambres et al. Nephrol Dial Transplant 2010)
• Optimal hemodynamic monitoring?– In general critical care, fluid management guided increasingly by:
• dynamic indices of preload ( PPV, SVV) instead of static indices (CVP, PCWP)
• Echocardiography and Central Venous Saturation (ScVO2)
• MONITOR RCT ( Al-Khafaji et al. Intensive Care Med 2015)
– N= 556, comparing ‘protocolized’ vs ‘usual’ fluid therapy in DBD donors.
– Primary endpoint: OTPD
– Results: No difference in OTPD ( 3.39 P vs 3.29 U, P =0.56); no specific data on lung donor rates
Page 86
CV Management (1):Choice of Fluid
• Crystalloid vs Colloid ?– No studies comparing these options in organ donors, with
crystalloids being the conventional choice
– In general critical care, comparisons of albumin vs NS showed no difference in ICU mortality ( e.g. SAFE study, Finfer et al. NEJM 2004)
• RCT, n=6997; Primary endpoint: 28 day mortality
• RR for albumin: 0.99 (0.91- 1.09)
– Potential role for albumin in improving oxygenation in ARDS when combined with furosemide ( Martin et al. Crit Care Med 2002)
• Blood Transfusion Target?– No studies related to organ donor management
– Based on current CCM guidelines, restrictive transfusion strategy to maintain Hgb > 7g/ dl ( TRICC trial. Hebert et al. NEJM 1999; of note, fewer cases of pulmonary edema in ‘restrictive strategy’ group)
CV Management (2):Vasoactive Drug Therapy-a
• Dopamine:
– Traditionally first-line agent due to potential immunomodulatory and anti IR properties
– Beneficial effects of low dose (4ug/kg/min) on renal graft function
( Schuelle et al. JAMA 2009)
• RCT, n= 487. Primary endpoint: Dialysis requirement during 1st
week post txt
• Results: reduction in dialysis requirement ( D 24.7% vs C 35.4%, P=0.01)
– De-emphasized increasingly in septic shock management
• Vasopressin:
– Attractive option in DBD given vasoactive and antidiuretic properties
– Increasing use as 1st or 2nd line agent in donor management
– Associated with increased rate of organ recovery in observational study of OPTN DBD data (Plurad et al. Am J Surg 2012)
CV Management (2):Vasoactive Drug Therapy-b
• Norepinephrine:
– Traditionally 2nd or 3rd line option for pressor choice
– Theoretical concern of more potent α-receptor stimulation, with associated coronary, mesenteric and pulmonary vasocontriction
– Increasing prominence in general critical care ( 1st line agent for septic shock)
• Thyroxine (T4):
– Conflicting evidence regarding its efficacy
– Retrospective studies suggest beneficial effect in patients with hemodynamic instability and depressed EF, with associated improved OTPD ( e.g. Salim et al. Clin Transplant 2007)
– Current expert recommendations suggest thyroid replacement therapy for hemodynamically unstable donors, or for potential cardiac donors with abnormal EF ( < 45%)
Page 87

Pulmonary Issues
• Minimal acceptable P/F ratio?– Standard criteria: PO2 > 300 mm Hg on 100% FIO2 and PEEP 5
– However, studies have demonstrated acceptable graft and patient survival with lower PO2 ( e.g. Reyes et al. Ann Thorac Surg 2010)
• Analysis of UNOS lung donor database (n=10,0000) found 18% of cases (n=1751) with P/F < 300, with lowest value of 230 mm Hg.
• Graft and patient survival similar in P/F groups < & > 300
• Fluid strategy to optimize lung donation?– Restrictive fluid strategy (CVP <6 mm Hg) shown to increase lung
donation without adversely affecting renal graft survival or increasing risk of DGF (Minambres et al. Nephrol Dial Transplant 2010)
– Potential role for albumin in improving oxygenation when combined with furosemide? ( Martin et al. Crit Care Med 2002)
Pulmonary Issues:Ventilator Strategies
• Optimal ventilator settings?– As in general critical care, benefits of ‘lung protective ventilation’
using lower tidal volumes (6-8 ml/kg PBW) being increasingly used to minimize ventilator associated lung injury
– European RCT demonstrates benefit of low tidal volume ventilation on lung recovery: (Mascia et al. JAMA 2010)
• N= 118
• Conventional Vent Strategy (n=59); TV 10-12 ml/kg PBW, PEEP 5
• Protective Vent Strategy (n=59); TV 6-8 ml/ kg PBW, PEEP 8-10
• Lung Recovery rates: P 54% vs C 27% (P < 0.05)
• Recruitment Strategies:– Increasing use of initial high PEEP (8-10)
– Protocolized recruitment maneuvers (e.g. San Antonio protocol- PC 25 PEEP 15 for 2 hrs)
Lung Donation and Intensivist Involvement
Singbartl et al. AJT 2011; 11: 1517
Page 88
Endocrine Issues• Evidence for Corticosteroid benefit?
– Rationale: Mitigate the proinflammatory cytokine storm related to brain death that can adversely affect graft function
– RCT related to donor livers(n=100): ( Kotsch et al. Ann Surg 2008)
• decreased proinflammatory serum cytokine levels, IR injury and ACR in steroid treated hepatic grafts
– Retrospective study related to donor lungs ( Follette et al. J Heart Lung Transplant 1998)
• Improved oxygenation and lung donation in steroid group
– RCT in donor kidneys (Kainz et al. Ann Intern Med 2010) and retrospective study in heart donors did not demonstrate steroid benefit with respect to graft function
– No documented benefit of steroid on MAP; role for hydrocortisone?
Research Advances• Ex-vivo Lung Perfusion (EVLP) (Cypel et al. NEJM 2011):
– Rationale: Perfusion of lungs with hyperoncotic acellular perfusate to extract extravascular lung fluid, and thereby improve oxygenation.
– EVLP successfully used to convert 20 high risk donor lungs ( P/F < 300) to acceptable donor criteria median P/F increase from 335 mm Hg to 443 mm Hg
• Post transplant graft function similar to ‘standard criteria donor’control group
• Hypothermia and Renal graft function (Niemann et al. NEJM 2015):– Rationale: Mild hypothermia may confer a renal-protective effect in the
setting of IR injury related to brain death.
– RCT,n=370. Hypothermia: 34 to 35° C, Normothermia: 36.5 to 37.5°C
– Primary endpoint: DGF
– Results: DGF Rates ( adjusted for multiple donor co-variates)
Overall: 28% H vs 39% N (OR 0.62, CI 0.43 to 0.92)
ECD: 31% H vs 56% N (OR 0.31, CI 0.15 to 0.68)
No adverse effects of hypothermia noted.
Utilization of HIV and HCV Positive Donors
• HIV Positive Donors:– HOPE (HIV Organ Policy Equity) Act (2013) authorizes
clinical research related to transplanting organs from HIV positive donors to HIV positive recipients.
– Current multi-center study under way in kidney and liver transplantation, with potential implications regarding increased use of HIV positive organs.
• HCV Positive Donors:– New highly effective PO antiviral therapy for HCV with high
rates of eradication
– Therefore, renewed interest in utilizing HCV positive donors for HCV positive recipients ( and potentially HCV negative recipients)
Page 89

Summary• Paucity of evidence based practices in critical care related to donor
management
• Best practices from general critical care may provide useful insights into donor management (e.g. lung protective ventilation)
• The unique physiology of brain death lends itself to specific novel research questions that need further inquiry ( e.g. role of thyroid hormone in hemodynamic management)
• The success of EVLP may further stimulate interest in other perfusion systems to enhance donor organ function (e.g. normothermic liver perfusion)
• The success of mild hypothermia in renal donors may stimulate hypothermia research in other donor organs
• Increased use of HIV and HCV positive donors will expand the donor pool
Page 90

TIMING OF DIALYSIS FOR AKI IN ICU
DEBATE:CONVENTIONAL VS EARLY RRT
Michael J. Connor, Jr., MD Michael J. Connor, Jr., MDEmory – Nephrology Emory – Critical Care Medicine
[email protected]@criticalbeansmd
Disclosures
Prior Member: ASN AKI Advisory Group
Prior Advisory Board: CR Bard, Inc Baxter, Inc - Acute Kidney Injury + CRRT (non-compensated)
Current Consulting: GE Healthcare, Inc – Clinical Events Adjudication Committee
Current research collaboration: Potrero, Inc
Wife (Emory faculty): no conflicts of interest
Goals & Outline
Describe studies on timing of acute RRT
Understand when “early” RRT may be indicated
Describe factors that may influence RRT decisions
Case & Background
Debate
Nephrology
VS
Critical Care Medicine
GOALS OUTLINE
Page 91
Case
37 yo M presents with acute onset of severe abdominal pain with SOB. In ED, noted to have profound epigastrictenderness, firm abdomen. HR 128, BP 85/45, temp 38.1
Initial labs: Calcium 8.4 Lipase 1100 AST 40, ALT 52
CT Abd/pelvis: marked inflammation of pancreas with no evidence of pancreatic necrosis
138
4.3
106
20104
24
1.2
Case - Continued
Admitted to ICU. Aggressive volume resuscitation with 10L NS over the next 24 hrs BP improved to 105/58 but dependent low dose norepi @ 0.05
mcg/kg/min UOP only 120cc since admission
Labs:
pH 7.22/48/88 with lactic acid 3.5 on 50% ventimask
Progressive resp distress secondary to worsening pulmonary infiltrates (ARDS), abd pain and distention requiring intubation
145
5.2
116
14180
60
3.4
Case - Questions
Does AKI impact pt’s outcomes?
Does patient need RRT now?
Page 92
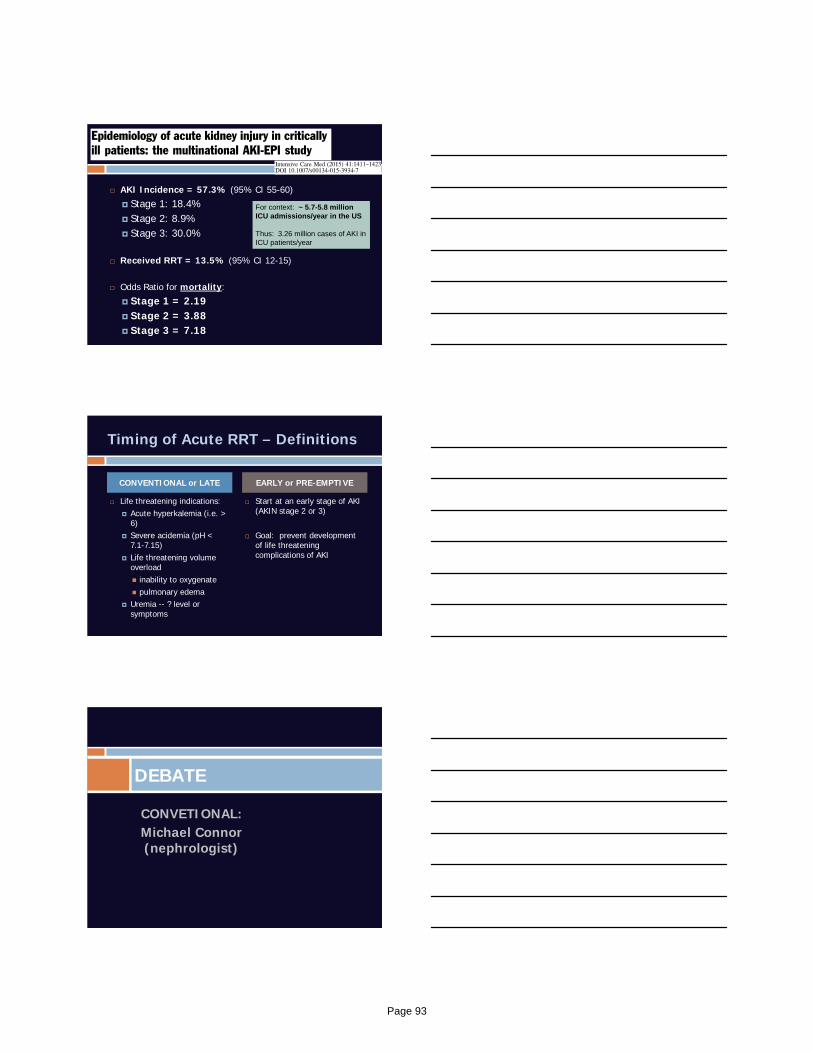
AKI Incidence = 57.3% (95% CI 55-60)
Stage 1: 18.4% Stage 2: 8.9% Stage 3: 30.0%
Received RRT = 13.5% (95% CI 12-15)
Odds Ratio for mortality:
Stage 1 = 2.19 Stage 2 = 3.88 Stage 3 = 7.18
For context: ~ 5.7-5.8 million ICU admissions/year in the US
Thus: 3.26 million cases of AKI in ICU patients/year
Timing of Acute RRT – Definitions
CONVENTIONAL or LATE
Life threatening indications: Acute hyperkalemia (i.e. >
6) Severe acidemia (pH <
7.1-7.15) Life threatening volume
overload inability to oxygenate pulmonary edema
Uremia -- ? level or symptoms
EARLY or PRE-EMPTIVE
Start at an early stage of AKI (AKIN stage 2 or 3)
Goal: prevent development of life threatening complications of AKI
CONVETIONAL:Michael Connor (nephrologist)
DEBATE
Page 93
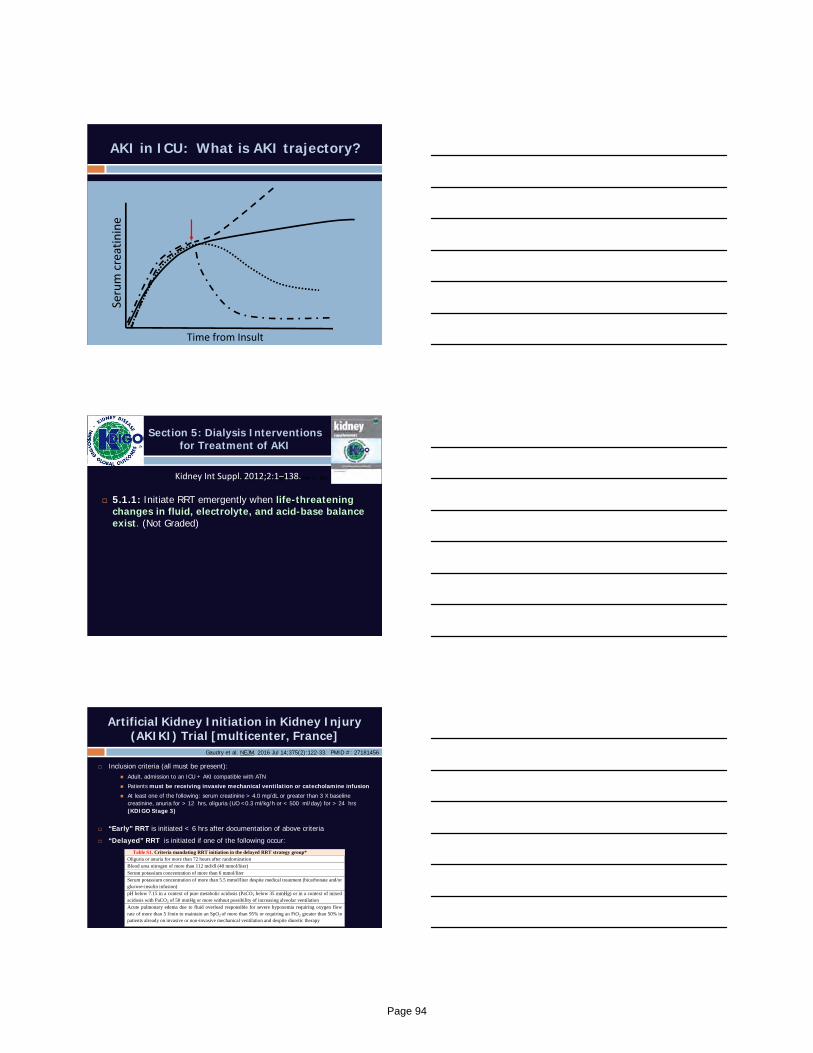
AKI in ICU: What is AKI trajectory?
Serum creatinine
Time from Insult
Section 5: Dialysis Interventions for Treatment of AKI
5.1.1: Initiate RRT emergently when life-threatening changes in fluid, electrolyte, and acid-base balance exist. (Not Graded)
Kidney Int. Suppl. Volume 2, No 1 (March 2012) Kidney Int Suppl. 2012;2:1–138.
Artificial Kidney Initiation in Kidney Injury (AKIKI) Trial [multicenter, France]
Inclusion criteria (all must be present): Adult, admission to an ICU + AKI compatible with ATN
Patients must be receiving invasive mechanical ventilation or catecholamine infusion
At least one of the following: serum creatinine > 4.0 mg/dL or greater than 3 X baseline creatinine, anuria for > 12 hrs, oliguria (UO <0.3 ml/kg/h or < 500 ml/day) for > 24 hrs(KDIGO Stage 3)
“Early” RRT is initiated < 6 hrs after documentation of above criteria
“Delayed” RRT is initiated if one of the following occur:
Table S1. Criteria mandating RRT initiation in the delayed RRT strategy group* Oliguria or anuria for more than 72 hours after randomization
Blood urea nitrogen of more than 112 md/dl (40 mmol/liter)
Serum potassium concentration of more than 6 mmol/liter
Serum potassium concentration of more than 5.5 mmol/liter despite medical treatment (bicarbonate and/or glucose-insulin infusion)
pH below 7.15 in a context of pure metabolic acidosis (PaCO2 below 35 mmHg) or in a context of mixed acidosis with PaCO2 of 50 mmHg or more without possibility of increasing alveolar ventilation
Acute pulmonary edema due to fluid overload responsible for severe hypoxemia requiring oxygen flow rate of more than 5 l/min to maintain an SpO2 of more than 95% or requiring an FiO2 greater than 50% in patients already on invasive or non-invasive mechanical ventilation and despite diuretic therapy
Gaudry et al. NEJM. 2016 Jul 14;375(2):122-33. PMID #: 27181456
Page 94
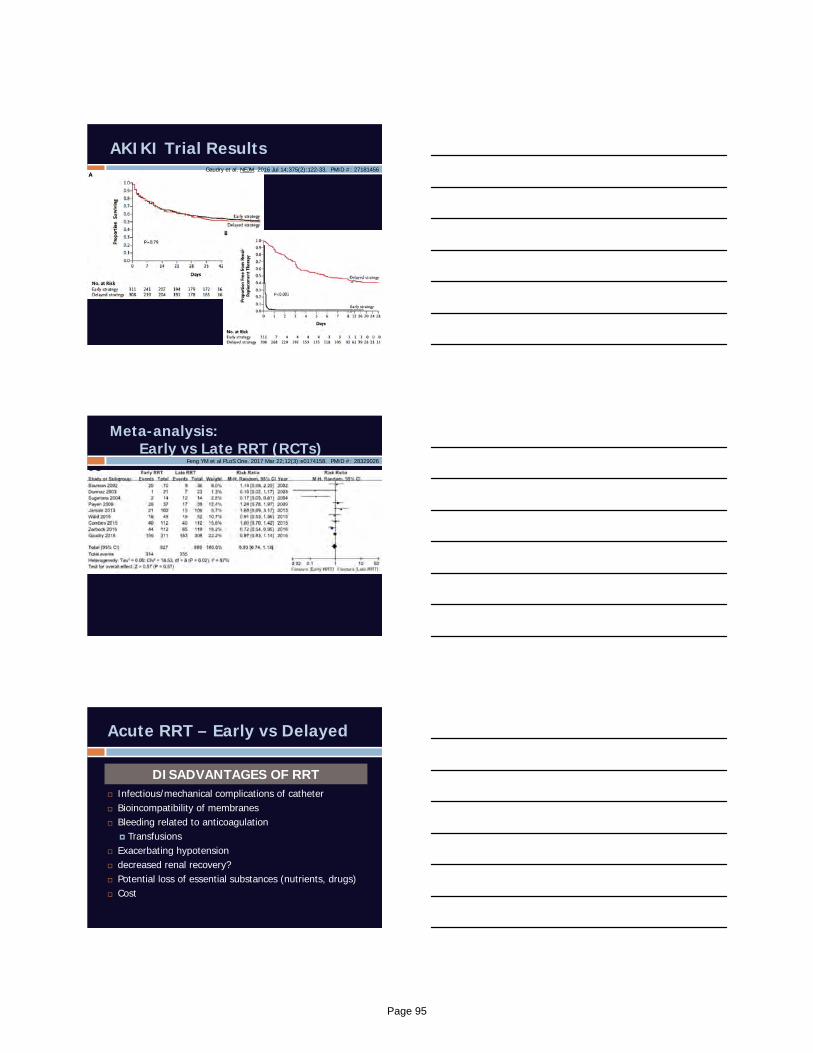
AKIKI Trial ResultsGaudry et al. NEJM. 2016 Jul 14;375(2):122-33. PMID #: 27181456
Meta-analysis: Early vs Late RRT (RCTs)
Feng YM et al PLoS One. 2017 Mar 22;12(3):e0174158. PMID #: 28329026
Acute RRT – Early vs Delayed
DISADVANTAGES OF RRT Infectious/mechanical complications of catheter Bioincompatibility of membranes Bleeding related to anticoagulation
Transfusions Exacerbating hypotension decreased renal recovery? Potential loss of essential substances (nutrients, drugs) Cost
Page 95
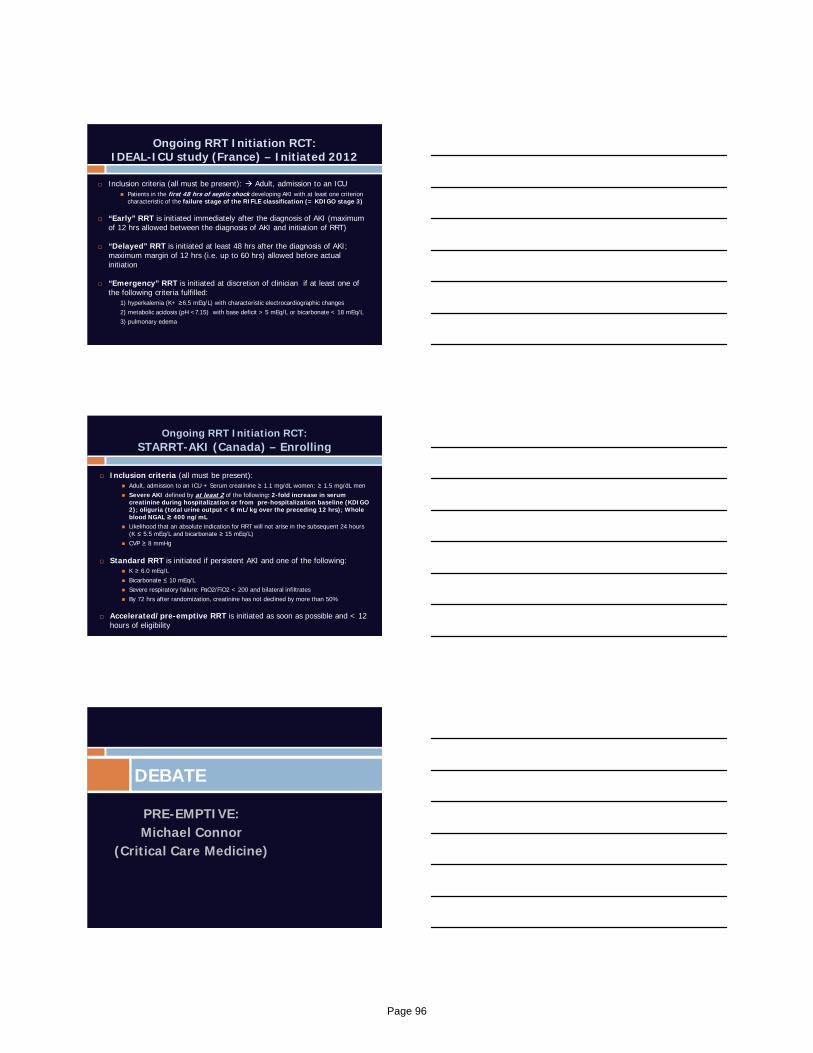
Ongoing RRT Initiation RCT:IDEAL-ICU study (France) – Initiated 2012
Inclusion criteria (all must be present): Adult, admission to an ICU Patients in the first 48 hrs of septic shock developing AKI with at least one criterion
characteristic of the failure stage of the RIFLE classification (= KDIGO stage 3)
“Early” RRT is initiated immediately after the diagnosis of AKI (maximum of 12 hrs allowed between the diagnosis of AKI and initiation of RRT)
“Delayed” RRT is initiated at least 48 hrs after the diagnosis of AKI; maximum margin of 12 hrs (i.e. up to 60 hrs) allowed before actual initiation
“Emergency” RRT is initiated at discretion of clinician if at least one of the following criteria fulfilled:
1) hyperkalemia (K+ ≥6.5 mEq/L) with characteristic electrocardiographic changes2) metabolic acidosis (pH <7.15) with base deficit > 5 mEq/L or bicarbonate < 18 mEq/L3) pulmonary edema
Ongoing RRT Initiation RCT:STARRT-AKI (Canada) – Enrolling
Inclusion criteria (all must be present): Adult, admission to an ICU + Serum creatinine ≥ 1.1 mg/dL women; ≥ 1.5 mg/dL men Severe AKI defined by at least 2 of the following: 2-fold increase in serum
creatinine during hospitalization or from pre-hospitalization baseline (KDIGO 2); oliguria (total urine output < 6 mL/kg over the preceding 12 hrs); Whole blood NGAL ≥ 400 ng/mL
Likelihood that an absolute indication for RRT will not arise in the subsequent 24 hours (K ≤ 5.5 mEq/L and bicarbonate ≥ 15 mEq/L)
CVP ≥ 8 mmHg
Standard RRT is initiated if persistent AKI and one of the following: K ≥ 6.0 mEq/L Bicarbonate ≤ 10 mEq/L Severe respiratory failure: PaO2/FiO2 < 200 and bilateral infiltrates By 72 hrs after randomization, creatinine has not declined by more than 50%
Accelerated/pre-emptive RRT is initiated as soon as possible and < 12 hours of eligibility
PRE-EMPTIVE:Michael Connor
(Critical Care Medicine)
DEBATE
Page 96

Acute RRT – Early vs Delayed
THEORETICAL ADVANTAGES Uremic/metabolic control Improved fluid management & prevention of fluid
overload Acid-base homeostasis Non-renal organ function “Unloading” or “resting” stressed and damaged kidneys Improved clinical outcomes (i.e. survival)?
Death from AKI is from Complications of AKI
Excess hospital mortality was driven by: Fluid overload >
5%
Hyperkalemia
Metabolic acidosis
RRT improved survival in AKI patients with: Hyperkalemia
Metaboic acidosis
Fluid overload
Azotemia
Liborio et al. CJASN. 2015.
Hypervolemia in AKI in ICU:Re-analysis of PICARD database
Bouchard, J., Mehta, R., et al. KI. 2009;76:422‐27. PMID: 19436332
Fluid Overload = > 10% increase in weight from baseline
OR for death if fluid overload present at RRT initiation = 2.07(95% CI 1.27-3.37)
Fluid Status
30 day mortality
60 day mortality
Death at hospital
discharge
Overload 37% 46% 48%
No fluid overload
25% 32% 35%
P value 0.02 0.006 0.01
Page 97

Improving Critical Care Outcomes
1. ADQI 12th Consensus Conference. 2013. Available at: www.adqi.org2. Hoste EA., et al. Br J Anaesth. 2014 Nov;113(5):740‐7. PMID: 25204700
Improving Critical Care Outcomes
Page 98
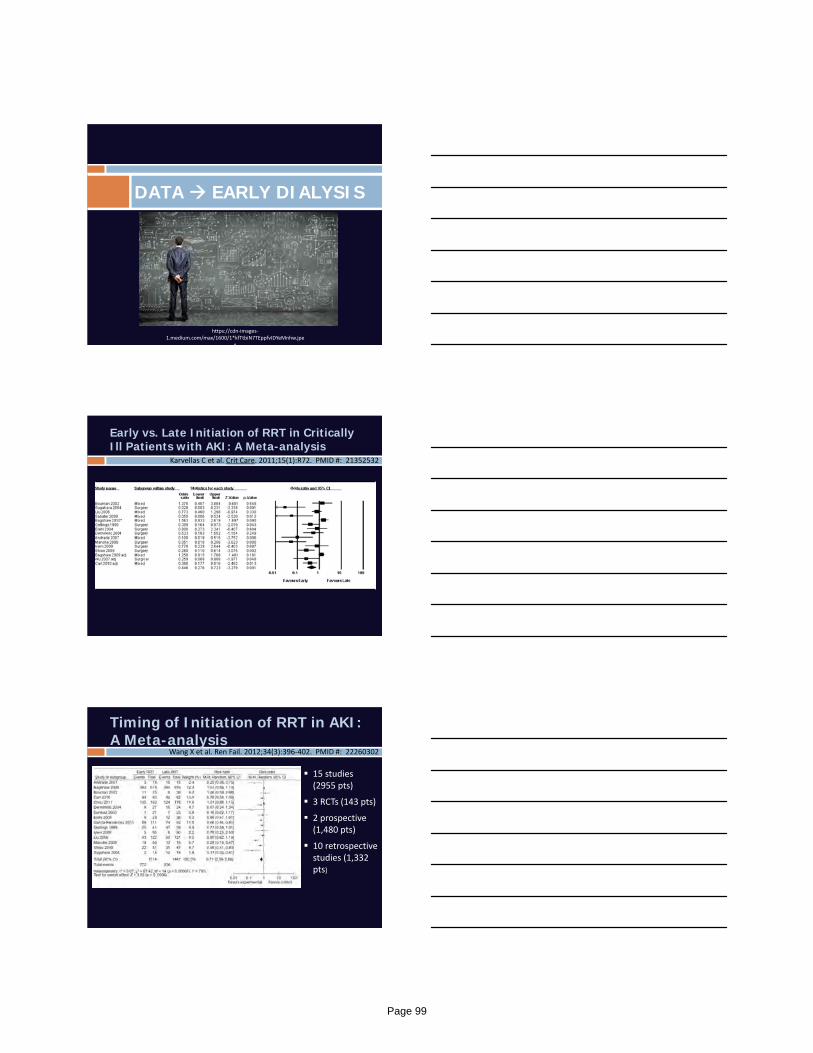
DATA EARLY DIALYSIS
https://cdn‐images‐1.medium.com/max/1600/1*kfTtbiN7TEppfvIDYeMnhw.jpe
g
Karvellas C et al. Crit Care. 2011;15(1):R72. PMID #: 21352532
Early vs. Late Initiation of RRT in Critically Ill Patients with AKI: A Meta-analysis
15 studies (2955 pts)
3 RCTs (143 pts)
2 prospective (1,480 pts)
10 retrospective studies (1,332 pts)
Timing of Initiation of RRT in AKI: A Meta-analysis
Wang X et al. Ren Fail. 2012;34(3):396‐402. PMID #: 22260302
Page 99
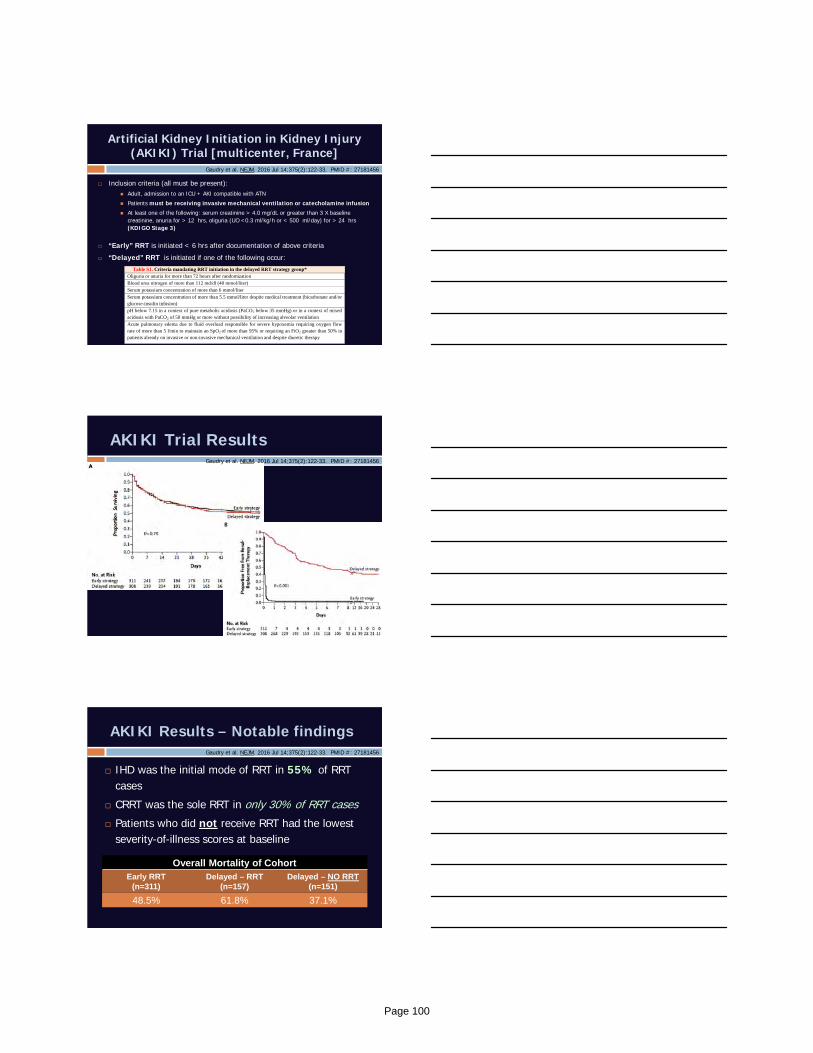
Artificial Kidney Initiation in Kidney Injury (AKIKI) Trial [multicenter, France]
Inclusion criteria (all must be present): Adult, admission to an ICU + AKI compatible with ATN
Patients must be receiving invasive mechanical ventilation or catecholamine infusion
At least one of the following: serum creatinine > 4.0 mg/dL or greater than 3 X baseline creatinine, anuria for > 12 hrs, oliguria (UO <0.3 ml/kg/h or < 500 ml/day) for > 24 hrs(KDIGO Stage 3)
“Early” RRT is initiated < 6 hrs after documentation of above criteria
“Delayed” RRT is initiated if one of the following occur:
Table S1. Criteria mandating RRT initiation in the delayed RRT strategy group* Oliguria or anuria for more than 72 hours after randomization
Blood urea nitrogen of more than 112 md/dl (40 mmol/liter)
Serum potassium concentration of more than 6 mmol/liter
Serum potassium concentration of more than 5.5 mmol/liter despite medical treatment (bicarbonate and/or glucose-insulin infusion)
pH below 7.15 in a context of pure metabolic acidosis (PaCO2 below 35 mmHg) or in a context of mixed acidosis with PaCO2 of 50 mmHg or more without possibility of increasing alveolar ventilation
Acute pulmonary edema due to fluid overload responsible for severe hypoxemia requiring oxygen flow rate of more than 5 l/min to maintain an SpO2 of more than 95% or requiring an FiO2 greater than 50% in patients already on invasive or non-invasive mechanical ventilation and despite diuretic therapy
Gaudry et al. NEJM. 2016 Jul 14;375(2):122-33. PMID #: 27181456
AKIKI Trial ResultsGaudry et al. NEJM. 2016 Jul 14;375(2):122-33. PMID #: 27181456
AKIKI Results – Notable findings
IHD was the initial mode of RRT in 55% of RRT cases
CRRT was the sole RRT in only 30% of RRT cases
Patients who did not receive RRT had the lowest severity-of-illness scores at baseline
Overall Mortality of CohortEarly RRT
(n=311)Delayed – RRT
(n=157)Delayed – NO RRT
(n=151)
48.5% 61.8% 37.1%
Gaudry et al. NEJM. 2016 Jul 14;375(2):122-33. PMID #: 27181456
Page 100
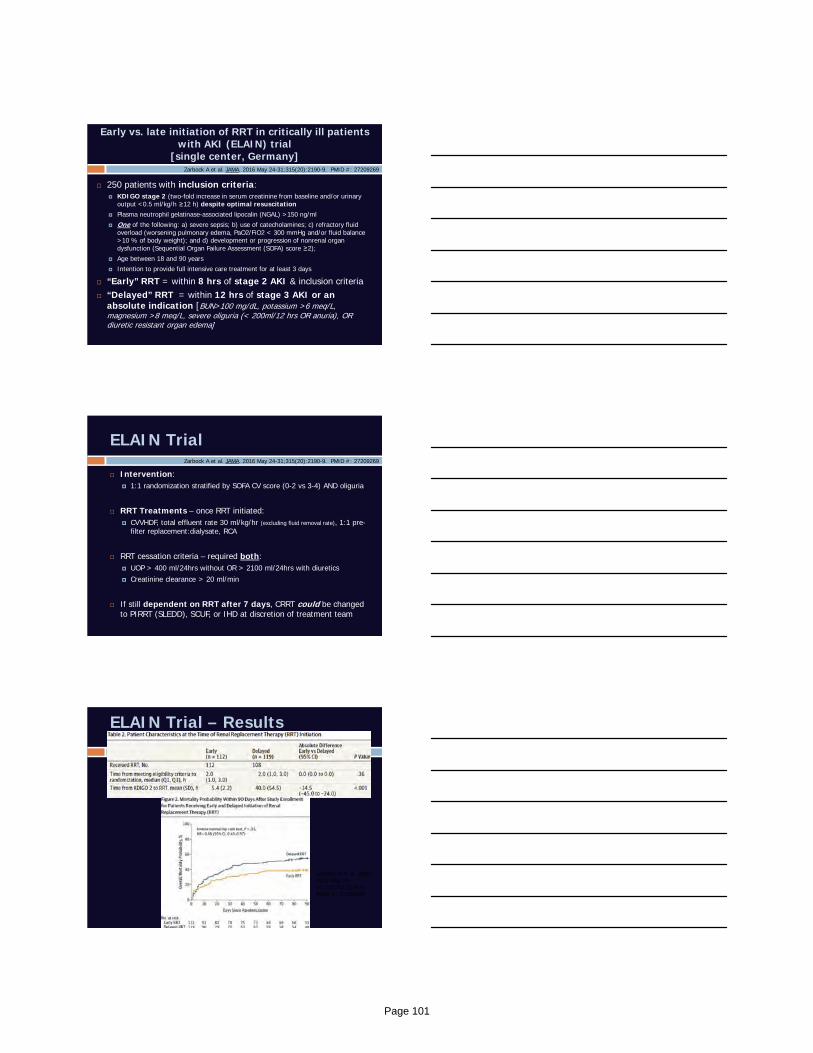
Early vs. late initiation of RRT in critically ill patients with AKI (ELAIN) trial
[single center, Germany]
250 patients with inclusion criteria: KDIGO stage 2 (two-fold increase in serum creatinine from baseline and/or urinary
output <0.5 ml/kg/h ≥12 h) despite optimal resuscitation Plasma neutrophil gelatinase-associated lipocalin (NGAL) >150 ng/ml
One of the following: a) severe sepsis; b) use of catecholamines; c) refractory fluid overload (worsening pulmonary edema, PaO2/FiO2 < 300 mmHg and/or fluid balance >10 % of body weight); and d) development or progression of nonrenal organ dysfunction (Sequential Organ Failure Assessment (SOFA) score ≥2);
Age between 18 and 90 years
Intention to provide full intensive care treatment for at least 3 days
“Early” RRT = within 8 hrs of stage 2 AKI & inclusion criteria “Delayed” RRT = within 12 hrs of stage 3 AKI or an
absolute indication [BUN>100 mg/dL, potassium >6 meq/L, magnesium >8 meq/L, severe oliguria (< 200ml/12 hrs OR anuria), OR diuretic resistant organ edema]
Zarbock A et al. JAMA. 2016 May 24-31;315(20):2190-9. PMID #: 27209269
ELAIN Trial
Intervention: 1:1 randomization stratified by SOFA CV score (0-2 vs 3-4) AND oliguria
RRT Treatments – once RRT initiated: CVVHDF, total effluent rate 30 ml/kg/hr (excluding fluid removal rate), 1:1 pre-
filter replacement:dialysate, RCA
RRT cessation criteria – required both: UOP > 400 ml/24hrs without OR > 2100 ml/24hrs with diuretics Creatinine clearance > 20 ml/min
If still dependent on RRT after 7 days, CRRT could be changed to PIRRT (SLEDD), SCUF, or IHD at discretion of treatment team
Zarbock A et al. JAMA. 2016 May 24-31;315(20):2190-9. PMID #: 27209269
ELAIN Trial – Results
Zarbock A et al. JAMA. 2016 May 24-31;315(20):2190-9.PMID #: 27209269
Page 101
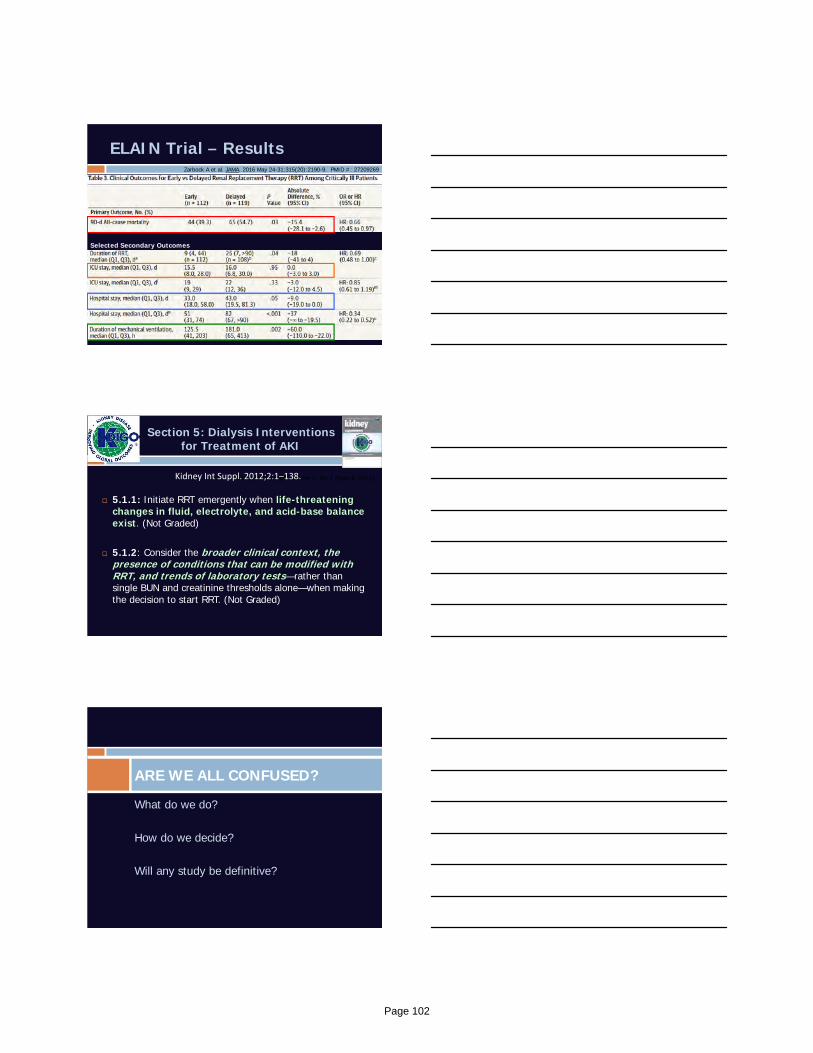
ELAIN Trial – ResultsZarbock A et al. JAMA. 2016 May 24-31;315(20):2190-9. PMID #: 27209269
Selected Secondary Outcomes
Section 5: Dialysis Interventions for Treatment of AKI
5.1.1: Initiate RRT emergently when life-threatening changes in fluid, electrolyte, and acid-base balance exist. (Not Graded)
5.1.2: Consider the broader clinical context, the presence of conditions that can be modified with RRT, and trends of laboratory tests—rather than single BUN and creatinine thresholds alone—when making the decision to start RRT. (Not Graded)
Kidney Int. Suppl. Volume 2, No 1 (March 2012) Kidney Int Suppl. 2012;2:1–138.
What do we do?
How do we decide?
Will any study be definitive?
ARE WE ALL CONFUSED?
Page 102
Case – Review
Admitted to ICU. Aggressive volume resuscitation with 10L NS over the next 24 hrs BP improved to 105/58 but dependent low dose norepi @ 0.05 mcg/kg/min
UOP only 120cc since admission
Labs:
pH 7.22/48/88 with lactic acid 3.5 on 50% ventimask
Progressive resp distress secondary to worsening pulmonary infiltrates (ARDS), abd pain and distention requiring intubation
145
5.2
116
14180
60
3.4
Problem Solving
https://static.wixstatic.com/media/e2d94c_a1d462119a83474a93574d1f3caf4a39~mv2.jpg
AKI & oliguriaVolume overloadAcute Resp FailureAcidemiaCritically ill
Start acute RRTWait to start RRT
?
Severity of AKI
• Creatinine & urea and trajectories
• Urine output / fluid status• Electrolyte derangement• Acid base status• Complications of uremia
Severity of Critical Illness
• Inciting event leading to AKI• Non‐renal organ dysfunction• Degree of fluid overload• Pre‐existing comorbidities• Trajectory
Potential Risks of RRT
• Line insertion• Hypotension during RRT• Clearance of nutrients/drugs
Other Factors
•Availability of machines•Availability of staff •Patient’s / relatives’ wishes•Futility / long‐term prognosis
Factors to Consider for RRT Initiation
Page 103
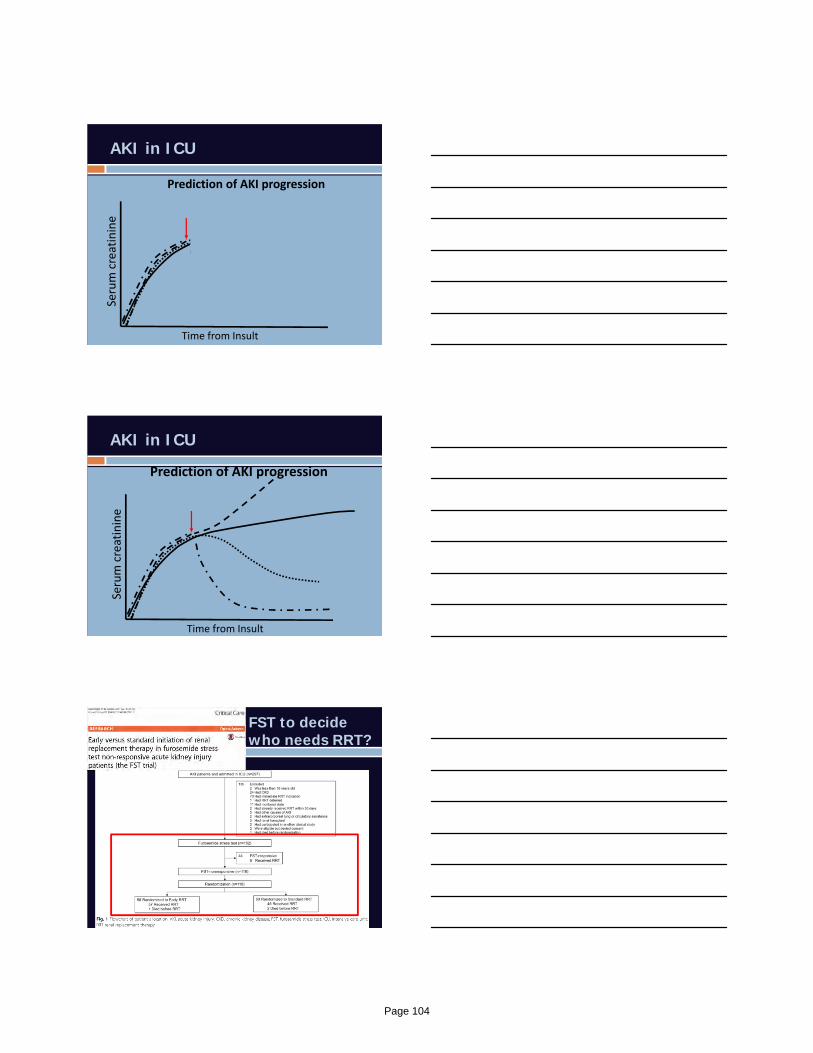
AKI in ICU
Serum creatinine
Time from Insult
Prediction of AKI progression
AKI in ICU
Serum creatinine
Time from Insult
Prediction of AKI progression
FST to decide who needs RRT?
Page 104

RRT Initiation: Individualized Approach
Key principles:
1. Kidneys have limited capacity.
2. The degree and impact of fluid & metabolic derangement vary between patients.
harm
time of initiation of RRT
“early RRT” for one patient may be “too late” for a different patient
benefit
Renal Demand vs Capacity
Consensus statement Acute RRT should be considered when metabolic
and fluid demands exceed total kidney capacity
Not based solely on renal function or AKI stage
RRT Initiation based on ability of kidney to meet demands
Results of ADQI 17th Conference on CRRT. Blood Purif 2016; 42
Renal Demand vs CapacityResults of ADQI 17th Conference on CRRT. Blood Purif 2016; 42
Page 105

Case – Review
Admitted to ICU. Aggressive volume resuscitation with 10L NS over the next 24 hrs BP improved to 105/58 but dependent low dose norepi @ 0.05 mcg/kg/min
UOP only 120cc since admission
Labs:
pH 7.22/48/88 with lactic acid 3.5 on 50% ventimask
Progressive resp distress secondary to worsening pulmonary infiltrates (ARDS), abd pain and distention requiring intubation
145
5.2
116
14180
60
3.4
Problem Solving
https://static.wixstatic.com/media/e2d94c_a1d462119a83474a93574d1f3caf4a39~mv2.jpg
AKI & oliguriaVolume overloadAcute Resp FailureAcidemiaCritically ill
Start acute RRTWait to start RRT
Start CRRT
6 Steps For Successful CRRT
1. Close collaboration between CCM & nephrology
2. Goals of therapy Daily discussion for volume removal & CRRT goals
3. Keep CRRT running – make ICU nurse happy Establish & maintain a great vascular access Anticoagulation options – use whenever possible
4. Address medication dosing daily5. Ensure appropriate nutrition support6. Avoid complications
Hypophosphatemia (avoid < 2.0)
Page 106
Ethics in Mass Casualty and Disaster
Triage
Samuel Shartar, MSN, RN, CEN, GA-PCEM
Senior Administrator
Emory University
Office of Critical Event
Preparedness and Response
No conflicts of interest to disclose
Ethics of Disaster Response
• Triage
• Crisis Standards of Care
• Ethical Framework for provision of care
• Four principles apply– Beneficence
– Nonmalfeicence
– Autonomy
– Justice
“Greatest Good for
the Greatest Number”
Prevention‐Preparedness
Well‐founded
Respect for Persons/ Autonomy
Proportionality
Distributive Justice/Fairness
Stewardship
BeneficenceNon‐
maleficence
Duty to Provide Care
Reciprocity
Balancing Individual and Community Interests
Solidarity
Transparency
Crisis Standards of Care in an Environment of Scarce Resources: Ethical Values & Processes
Page 107
Beneficence and Nonmaleficence
• Beneficence is action that is done for the benefit of others.
• Nonmaleficence means to do no harm.
• One of the most common ethical dilemmas and plays a role in all medical decision making.
• Intervention must outweigh the risks to be ethical
Crisis Standards of Care• Crisis Standards of Care (CSC) is
defined as a substantial change in usual healthcare operations & care delivery, which is made necessary by a pervasive or catastrophic disaster. Institute of Medicine (IOM)
• Shifting to Crisis Standards of Care is justified by specific circumstances and is formally declared by state government, thus enabling specific legal and regulatory powers and protections for healthcare providers in the necessary tasks of allocating and using scarce medical resources and implementing alternate care facility operations.
Crisis Standards of Care• Duty to care
– Moral obligations
– “Duty to provide the best care possible”
• Necessity of Rationing.– Not whether, but how to implement
– Altered scopes of practice
– Modified staffing ratios
– Scare resource allocation
• IOM Report
– Guidance for establishing crisis standards of care for use in disaster situations: A letter report
Page 108
Mass Casualty Triage• Triage: The assignment of degrees of
urgency to wounds or illnesses to decide the order of treatment for a large number of patients or casualties.
• Multiple methods, Start, Jump-Start, SALT
• The Model Uniform Core Criteria (MUCC) for Mass Casualty Triage is a science and consensus based national guideline that recommends 24 core criteria for all mass casualty triage systems.
Challenges with Mass Casualty Triage
• Requires efficiency and coordination among multiple response agencies.
• Doing the greatest good for the greatest amount of people, is counter to day-to-day operations.
• Plans are complex, field personnel may not know the details of the plans.
• Lack of standardized processes
• Provider experience
Page 109
Triage Tags
Background• There have been multiple mass casualty
events in the past twelve years. Madrid, London, Mumbai, Boston, Paris, San Bernardino, Brussels, Orlando, Nice, Las Vegas.
• 2008 Congressional study showed that the United States was ill prepared to handle an incident like Madrid.
• Boston response handled well, but atypical because of extenuating circumstances.
• Hospitals must focus on the concept of Immediate Bed Availability in the emergency department.
• Multiple surges present in waves as the incident evolves.
Background• Mortality numbers blurred by “walking
wounded”.
• 60% of victims self transport to closest hospital(s).
• Percentage of critical injuries remains constant at 7-10%.
• EMS must coordinate with hospitals and focus efforts on these critically injured patients.
• Focusing on this subset of patients, and leveraging damage control surgery, has the most impact on mitigating mortality.
Page 110
Background• Systems become overwhelmed and are
temporarily unable to provide care to all.
• Ethical principles must be applied.
• Need for pre-established crisis standards of care
Madrid• March 11, 2004 ten bombs detonated on
four commuter trains during the morning rush hour. 191 deaths.
• Over 1,800 injured.
London• July 7, 2005, four suicide bombers
detonated portable devices on three underground trains and a commuter bus in London between 8:50 am and 9:47 am.
• Largest MCI since World War 2.
• 52 dead.
• ~ 700 injuries.
• Sites cleared of casualties within four hours.
Page 111

Paris• November 13, 2015, 3 explosions and
four shootings in the heart of Paris.
• Ironically the SAMU had conducted a FSE that morning for the same type of event.
• 131 deaths.
• ~300 injuries.
Brussels• March 22, 2016, two coordinated attacks,
using an active shooter and bombs.
• Brussels-Zaventem International Airport.
• Maalbeek Metro Station.
• 35 dead.
• ~300 injuries.
• 60 critically injured.
Orlando• June 12, 2016, active shooter attack.
• Pulse Nightclub.
• 50 dead.
• 52 injuries.– 44 to ORMC ~ 1 block away
– 8 to Florida Hospital Orlando.
Page 112
Nice• July 14, 2016, 19 ton cargo truck driven
into a crowd.
• Bastille Day Celebration in Nice, France.
• 86 dead.
• 434 injuries.
Las Vegas• Route 91 Harvest Music festival
• 59 dead, 527 injured
• ~21,500 self evacuated
• High velocity rifle/sniper attack
• Less than 20% transported by EMS
Lessons Learned• Controlling and Securing Incident Sites
– Incident Command
– Clear roles and procedures
– Processing victims
• Use of Emergency Resources
– Onsite triage and clinical prioritization of hospital bound patients
– Keeping personnel in reserve to manage additional incidents
– Plans to quickly create bed space in emergency departments
– Need to move EMS triage to ambulance ramp
• Communications
– Information control
– Coping with telecommunications outages
– Open and frequent communications between responders and victims
Page 113
Current State• Multiple hospitals and emergency
departments at capacity.
• EDs boarding multiple admissions.
• Multiple EDs on diversion
• Limited capacity for patient surges.
• EMS capabilities are strained..
• RCHs and MOUs with hospitals
• Engagement
Assumptions
• Personnel will step up to do the best they can to manage the event.
• Medical infrastructure has to absorb casualties.
• The numbers of critically ill victims remains constant at 7-10 percent, and are the patients who we can most impact.
– Damage control surgical strategies work.
• Patient volumes in ED and the numbers of EMS calls will remain at baseline, or may increase.
• “Walking wounded” patients, self-transport.
• Trauma will have to be managed at “Non-Trauma” hospitals.
References
• Ashkenazi, I., Turegano-Fuentes, F., Einav, S., Alfici, R., & Olsha, O. (2014). Pitfalls to avoid in the medical management of mass casualty incidents following terrorist bombings: the hospital perspective. European Journal of Trauma and Emergency Surgery, 40, 445-450. doi:10.1007/s00068-014-0403x
• Aylwin, C., Konig, T., Brennan, N., Shirley, P., Davies, G., Walsh, M., & Brohi, K. (2006). Reduction in critical mortality in urban mass casualty incidents: analysis of triage, surge, and resource use after the London bombings on July 7, 2005. Lancet, 9554(368), 2219-2225. doi:10.1016/S0140-6736(06)69896-6
• Bhalla, M., Frey, J., Rider, C., Nord, M., & Hegerhorst, M. (2015). Simple triage algorithm and rapid treatment and sort, assess, lifesaving, interventions, treatment, and transportation mass casualty triage methods for sensitivity, specificity, and predictive values. American Journal of Emergency Medicine, 33, 1687-1691. doi:10.1016/j.ajem.2015.08.021
• Boykins, A. (2014). Core communication competencies in patient-centered care. ABNF Journal, 25, 40-45. Retrieved from http://eds.b.ebscohost.com.vlib.excelsior.edu/eds/pdfviewer/pdfviewer?sid=d1aad459-f58f-4fe7-b17e-002348ecaa34%40sessionmgr120&vid=2&hid=117
• Clancy, C. (2007). Emergency departments in crisis: Opportunities for research. Health Services Research, 42, 13-20. doi:10.1111/j.1475-6773.2006.00692.x
• Dawson, D. (2013). National implementation of the model uniform core criteria for mass casualty incident triage. A Report of the FICEMS, 1-25. Retrieved from http://www.ems.gov/nemsac/dec2013/FICEMS-MUCC-Implementation-Plan.pdf
• http://www.ems.gov/nemsac/dec2013/FICEMS-MUCC-Implementation-Plan.pdf
• Evans, D., Shartar, S., & Gordan, J. (2012). The role of the nurse. In Local planning for terror and disaster: From bioterrorism to earthquakes (pp. 61-70). New York, NY: John Wiley and Sons, Inc.
• Final Report of the Joint Comprehensive State Trauma Services Study Committee (2008) The State Senate Senate Research Office, State of Georgia
• Fratta, A. (2010). Post-9/11 responses to mass casualty bombings in Europe: Lessons, trends and implications for the United States. Studies in Conflict & Terrorism, 33, 364-385. doi:10.1080/10576101003587192
• Institute of Medicine Guidance for establishing crisis standards of care for use in disaster situations: A letter Report (2009)
• Lozano, K., Ogbu, U., Amin, A., Chakravarathy, B., & Lotfipor, S. (2015). Administration of emergency medicine: Patient motivators for emergency department utilization: A pilot cross-sectional survey of uninsured admitted patients at a university teaching hospital. Journal of Emergency Medicine, 49, 203-210. doi:10.1016/j.jemermed.2015.03.019
• Nesbitt, I. (2015). Mass casualties and major incidents. Surgery, 33, 410-412. doi:10.1016/j.mpsur.2015.07.003
• Shartar, S., Moore, B, Wood, L. (2017) Developing a Mass Casualty Surge Capacity Protocol for Emergency Medical Services to Use for Patient Distribution, 0038-43/2017/110-12. DOI: 10.14423/SMJ.0000000000000740
• Schenk, E., Wijetunge, G., Mann, C., Lerner, B., Longthorne, A., & Dawson, D. (2014). Epidemiology of mass casualty incidents in the United States. Prehospital Emergency Care, 18, 408-416. doi:10.3109/10903127.2014.882999
Page 114

Novel Diagnostics in Infectious Diseases
Aneesh K. Mehta, MDDivision of Infectious Diseases
Emory University School of [email protected]
May 10, 2018
2018 Southeastern Critical Care Summit
Atlanta, Georgia
Case
• 19 y/o healthy male college student who just finished exams and spent the weekend moving out of his dorm room
• Found by his parents on delirious and tachypneic
• EMS was called and transported him to a local hospital
• Found to have significant hypoxia, bilateral pulmonary infiltrates
• Started on vancomycin and piperacillin/tazobactam
• Emergently intubated difficult to ventilate diagnosed with ARDS transferred to a larger hospital cannulated for VA ECMO with plans to transfer to Emory for ECMO management
Case
• No known sick contacts• Roommate, girlfriend, and parents are without recent illnesses
• By the time of transfer to Emory University Hospital• Blood cultures were no growth to date (~48 hours)
• Monospot negative
• HIV‐1/2 antibody negative
• Rapid influenza negative
• Mini BAL Gram stain: Rare WBCs, rare squamous epithelial cells, no organisms
• WBC count, platelet count, creatinine, other labs were normal
• Transferring hospital did a test that made the diagnosis
Page 115
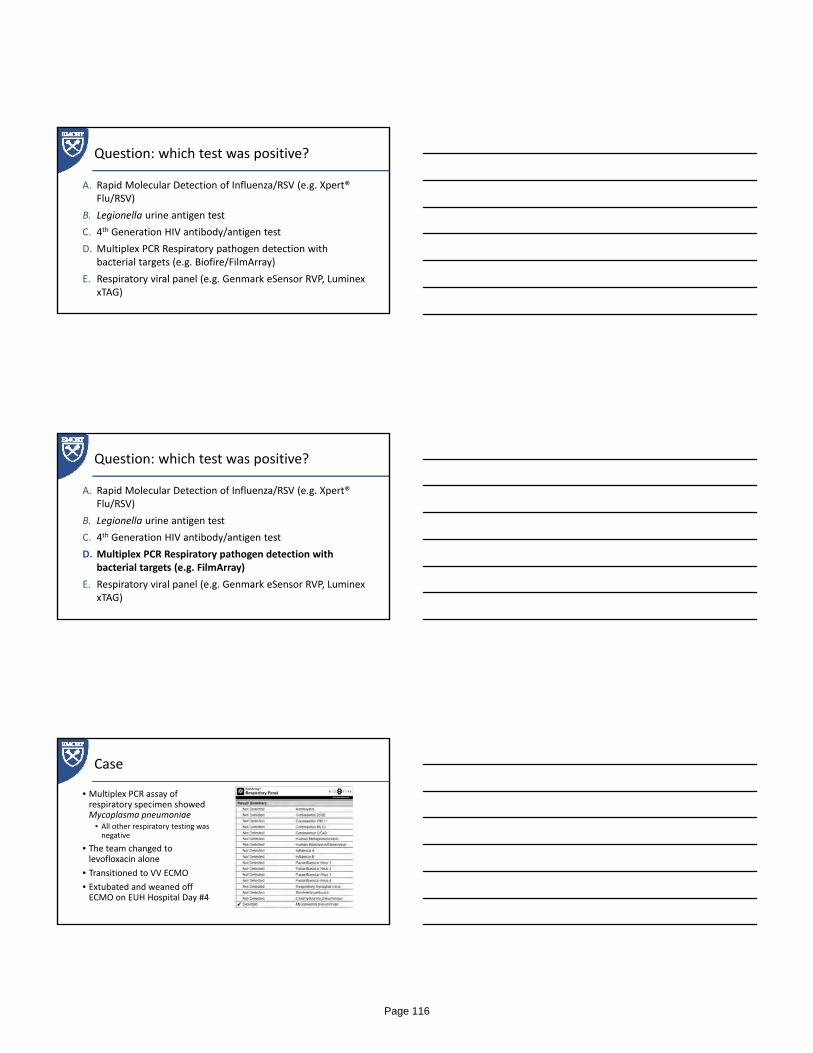
Question: which test was positive?
A. Rapid Molecular Detection of Influenza/RSV (e.g. Xpert® Flu/RSV)
B. Legionella urine antigen test
C. 4th Generation HIV antibody/antigen test
D. Multiplex PCR Respiratory pathogen detection with bacterial targets (e.g. Biofire/FilmArray)
E. Respiratory viral panel (e.g. Genmark eSensor RVP, Luminex xTAG)
Question: which test was positive?
A. Rapid Molecular Detection of Influenza/RSV (e.g. Xpert® Flu/RSV)
B. Legionella urine antigen test
C. 4th Generation HIV antibody/antigen test
D. Multiplex PCR Respiratory pathogen detection with bacterial targets (e.g. FilmArray)
E. Respiratory viral panel (e.g. Genmark eSensor RVP, Luminex xTAG)
Case
• Multiplex PCR assay of respiratory specimen showed Mycoplasma pneumoniae
• All other respiratory testing was negative
• The team changed to levofloxacin alone
• Transitioned to VV ECMO
• Extubated and weaned off ECMO on EUH Hospital Day #4
Page 116
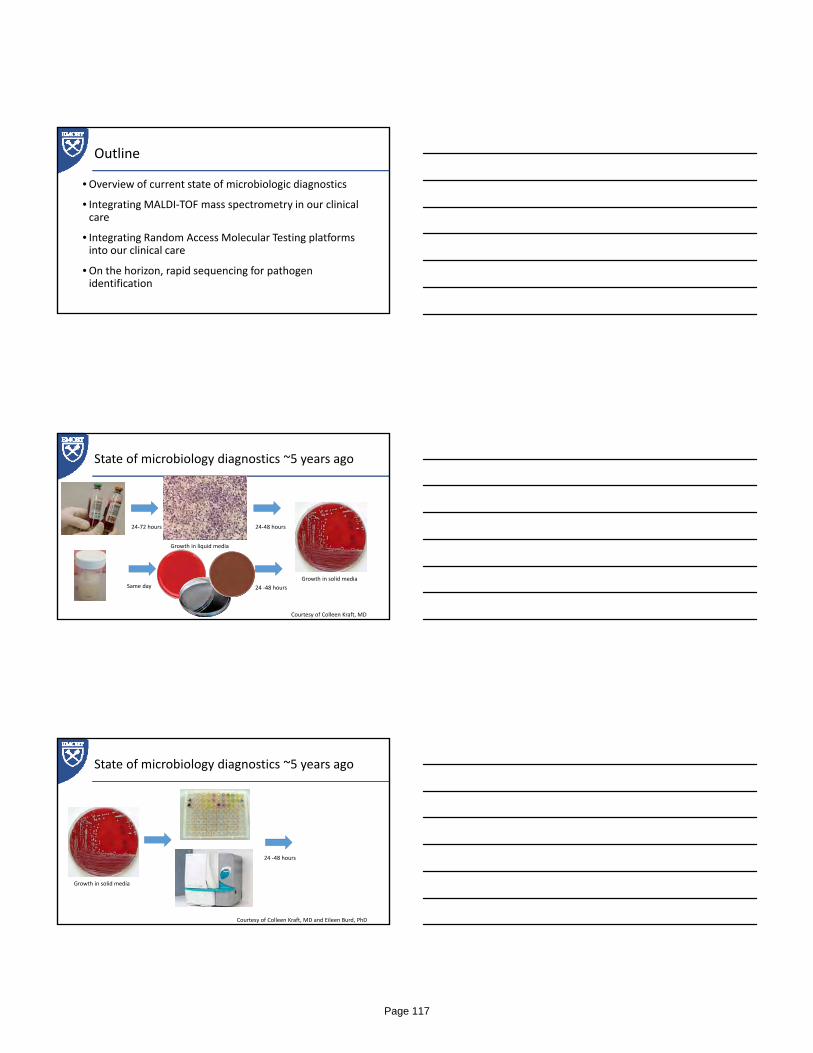
Outline
•Overview of current state of microbiologic diagnostics
• Integrating MALDI‐TOF mass spectrometry in our clinical care
• Integrating Random Access Molecular Testing platforms into our clinical care
•On the horizon, rapid sequencing for pathogen identification
State of microbiology diagnostics ~5 years ago
24‐72 hours
Same day 24 ‐48 hours
24‐48 hours
Growth in liquid media
Growth in solid media
Courtesy of Colleen Kraft, MD
State of microbiology diagnostics ~5 years ago
24 ‐48 hours
Growth in solid media
Courtesy of Colleen Kraft, MD and Eileen Burd, PhD
Page 117
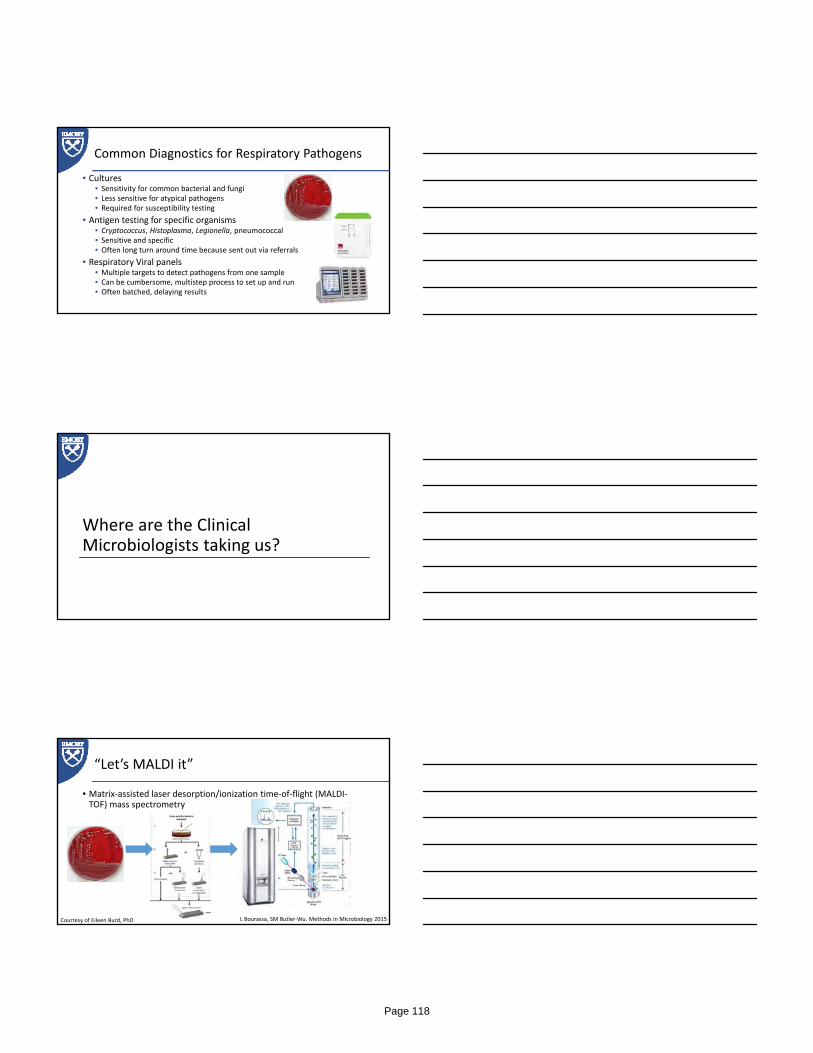
Common Diagnostics for Respiratory Pathogens
• Cultures• Sensitivity for common bacterial and fungi• Less sensitive for atypical pathogens• Required for susceptibility testing
• Antigen testing for specific organisms• Cryptococcus, Histoplasma, Legionella, pneumococcal• Sensitive and specific• Often long turn around time because sent out via referrals
• Respiratory Viral panels• Multiple targets to detect pathogens from one sample• Can be cumbersome, multistep process to set up and run• Often batched, delaying results
Where are the Clinical Microbiologists taking us?
“Let’s MALDI it”
• Matrix‐assisted laser desorption/ionization time‐of‐flight (MALDI‐TOF) mass spectrometry
L Bourassa, SM Butler‐Wu. Methods in Microbiology 2015Courtesy of Eileen Burd, PhD
Page 118

Advantages of MALDI‐TOF
• Rapid identification of the organism species• Within an hour from detectable culture growth vs 24‐48 hours by traditional methods
• An even greater difference more fastidious bacteria
• Requires only a small amount of microorganism (a single colony)
• Does not require a predefined target as compared to molecular techniques
• Does not need pre‐differentiation (e.g. gram‐positive bacteria vs gram‐negative bacteria)
American Proficiency Institute – 2014
Limitations to MALDI TOF
• Culture of the microorganism is currently still necessary
• Reference spectra databases are limited for many genera• They can be amended by company’s updates or by internal laboratory personnel
• Closely related species or genera are sometimes confused
• Capital equipment costs are high• However long‐term cost saving to both the laboratory and the clinical enterprise should offset this with time
American Proficiency Institute – 2014
• 12‐month retrospective cost savings analysis of potential at the University of North Carolina hospitals after implementation of MALDI‐TOF MS for routine identification of bacteria and yeasts
• Examined reagent costs and a total cost analysis (technologist time + reagent expenses + maintenance service agreement)
• Reagent cost savings of $69,108.61, or 87.8%, in over 12 months
• Total cost savings of $73,646.18, or 51.7%
• Return on investment at ~3 years
Page 119

Key Pearls for Clinicians with MALDI‐TOF
• You will see genus and species of bacteria and fungi identified earlier• Use your local antibiogram to focus antimicrobial
• You will see species that you do not recognize• They previously identified as groups (eg viridans Streptococci, Mycobacteria abscessus), but now you are given the exact species
• You will not see the susceptibility testing at the same time as the species identification
• Susceptibility testing usually still needs another 24‐48 hours of incubation
• Use the local antibiogram
• If you see something that does not make sense, call you Microbiology lab or your friendly neighborhood ID doc
Random access molecular testing
Random access molecular testing
• Many companies out there• FilmArray (previously Biofire), Cepheid, Verigene, Prodesse, BD MAX
• Some are single pathogen• C diff, Influenza
• Some are Multiplex• Respiratory viral panels
• Gastrointestinal panels
• CNS infection panels
• Blood culture identification
Page 120
I can test for everything at once? Awesome!
Children’s Healthcare of Atlanta
Time to Optimal Therapy Improved by BCID and ASP
20
Courtesy of Craig Shapiro, MDEnterprise Director of Antimicrobial StewardshipNemours Children’s Health System, Wilmington, DE
But these tests are not magic bullets
• False‐positive result for Herpes Simplex by multiplex assay
• Received 7 days of antivirals, but worsened
• Finally diagnosed with TB meningitis after repeat LP
CA Gomez, et al. OFID, 4 (1), 2017, ofw245
Page 121
And also false‐negatives
EB Popowitch, et al. J Clin Microbiol. 2013; 51(5)
Limitations to the random access multiplex tests
• Usually only approved from certain sample types• e.g. Biofire Respiratory panel approved nasopharyngeal swabs, not on lower respiratory samples
• Different sensitivities and specificities for different pathogens in the assays
• False positive and false negative results are more common than we would like
• If the result does not make sense or if the patient does not get better, question the result
• Cost• $700 ‐ $1500 a test!
On the horizon:
Next Gen Sequencing for Pathogen Identification
Page 122
Future state of microbiology diagnostics?
Same Day Identification
and susceptibility by
genomic sequencing
Courtesy of Colleen Kraft, MD
Molecular Microbiology: Diagnostic Principles and Practice, 3rd Edition
Page 123

Question: if you get a result on one of these tests that does not make sense, you will…?
A. Go with it, because the technology is cool, and how could it be wrong?
B. Order it again to see if you get the same result
C. Add Micafungin
D. Question the validity of the test result
E. Never order this test again
Acknowledgements
• Colleen S Kraft, MD, MSc• Medical Director, Microbiology Laboratory, Emory University Hospital
• Eileen M Burd, PhD• Director, Clinical Microbiology, Emory University Hospital
• Craig Shapiro, MD• Enterprise Director of Antimicrobial Stewardship, Nemours Children’s Health System, Wilmington, DE
Page 124
emoryhealthcare.org
Fancy Footsteps: The Palliative Care Dance
Tammie E. Quest, MD FAAHPMProfessor
Director, Emory Palliative Care CenterPresident, American Academy of Hospice and Palliative Medicine
[email protected] conflicts of interest to disclose
emoryhealthcare.org
Objectives
• Identify concerns of ICU providers when consultation of palliative care teams are considered
• Discuss strategies for successful integration of primary and subspecialty palliative care
emoryhealthcare.org
The Critical Care Team
The Patient/Family
The Critical Care Experience
Page 125

emoryhealthcare.org
When the “Dance” is Going Well….
• Sense of accomplishment
• Sense of progress
• Collaborative discussion
• Attainment of mutual goals
emoryhealthcare.org
When the “Dance” is NOT going Well
• Lack of clinical progress• Patient/Family vs. Team in
conflict• Identified unresolved
distress– Physical, spiritual,
psychological or social
• OFTEN revolve around END OF LIFE ISSUES
emoryhealthcare.org
Page 126
emoryhealthcare.org
Team Decision Tree
Patient Likely to Die
Add more consultants?
Yes No
Should we call Palliative Care? Why? Why Not?
emoryhealthcare.org
“We would like for you to come and support the family.”
8
emoryhealthcare.org
Key Interventions of a Palliative Care Team
• Assessment of Goals of Care
• Symptom management
– Pain & Non‐Pain (Dyspnea, depression, anxiety)
• Advance care planning (NOT JUST DNR)
• Spiritual Support
• Caregiver Support
9
Which elements were you thinking? Is there anything that we SHOULD
NOT be DOING?Why should PC NOT be DOING
THAT?
Page 127
emoryhealthcare.org
ICU – PC Integration
emoryhealthcare.org
Key Challenges to PC‐ICU Integration• Timing
• Consult Boundaries
• Level of Response
– Palliative care team – who is needed?
• Concern about duplicity
– PC Social Worker/Chaplain vs. ICU Social Worker/Chaplain
• Concern about “added value”
– Do more cooks in the kitchen deliver a better outcome?
• Don’t need another group of “Monday Morning Quarter backers”
emoryhealthcare.org
Possible Benefits• Another set of eyes and ears to assess:– Perception of effectiveness?
• What have you heard the ICU say about what’s happening with you?
– Are key needs met?• Symptoms• Spiritual• Social
– Communication gaps• What was missed? Who else needs to be communicated with?
Page 128

emoryhealthcare.org
What’s Needed to Dance together Well?
• Mutual Respect
• Clear Communication
• Willingness to allow missteps and try it again
emoryhealthcare.org
Questions?
Page 129
Challenging ICU Cases Gabriel Najarro, PA‐C, MMSc Emory Critical Care Center
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 130

Clinical Dilemma Jenny Han, MD, MSc
Assistant Professor, Emory University ___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 131
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Clinical Dilemma
Jenny Han, MD,[email protected]
No Disclosures
May 10, 2018
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
29 y/o male presents to ED in law enforcement custody after being arrested for stuffing items resembling crack cocaine into his mouth 20-30 min prior to arrival.
PMH: h/o small ventricular septal defect from childbirth w/ normal cardiac function.
Diagnostic Dilemma
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Presentation
On arrival, patient was non-verbal, extremely agitated and violently thrashing.
• Haldol 20mg IM and Ativan 10mg IM
• Questionable tonic clonic seizure, he is intubated w/ serosanguinous frothy secretions and no obvious trauma.
• On exam, patient is sedated on Fentanyl and Versed with RASS -5, normotensive and HR 110s.
• EKG performed.
Page 132
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
EKG was notable for wide-complex tachycardia, peaked T-waves, and prolonged QTc.
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Clinical Course
• Treated with Sodium Bicarb IV 75mEq and NS x 3 L IV, EKG converts to NSR.
• 7.29 / 40 / 184
• Bicarb 20
• Bun 21, Creatinine 2.3
• WBC 12.5
• Hb 16.7
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Page 133
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Clinical course
• CPK > 50,000
• POCT ABG: pH 6.6, pCO2 120, PaO2 200
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
180
20
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Page 134

Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
What vent changes would you make?
• 6.93 / 142 / 259
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
High Peak and High Plateau
• Peak & plateau elevated= decrease compliance
Differential:
-Right main stem
-Asynchrony
-Auto-peep
-Chf/pneumonia
-Pneumothorax
High Peak and Normal Plateau
• Peak>35, Plt<35= High resistance
Differential:
-Mucus plug
-Biting
-Tracheal obstruction
-Bronchospasm
Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
180
20
Page 135

Critical Care SummitEmory Division of Pulmonary, Allergy, Critical Care and Sleep Medicine
Take home points
• Exam your patient
• Consider what is going on physiologically with the patient
Page 136
A Management Dilemma Mark Caridi‐Scheible, MD
Assistant Professor CT‐Anesthesiology Emory University School of Medicine
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 137
Ethical Dilemma Neal Dickert, MD, PhD
Assistant Professor, Emory University ___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 138
Patient A
• 35 yo male with no relevant PMH
• Admitted with hypoxemic respiratory failure and intubated 2 days ago
• Influenza A
• Worsening oxygenation
– 100% FiO2, 18 PEEP, P/F 55, on NM blockade
• Hemodynamically stable and other organs intact
Patient B
• 74 yo male with h/o CABG x 4, ischemic cardiomyopathy (EF 40%), and CKD 2
• Admitted with hypoxemic respiratory failure 10 days ago in context of influenza A
• V‐V ECMO for past week
• CRRT and high‐dose vasopressors
• Family aware of severity of illness, son arriving from out of state tomorrow and plan to de‐escalate
The Problem
Patient A needs ECMO, but no machines are available. This patient is not stable for transport to another facility.
Page 139
Potential Solutions
1. Treat Patient A the best you can, cannulate for ECMO as soon as Patient B’s family decides to de‐escalate.
2. Tell Patient B’s family that you cannot keep Patient B on ECMO any longer because he cannot be saved and there is someone who needs the therapy.
3. Tell Patient B’s family that you cannot keep Patient B on ECMO any longer because he cannot be saved but do not say anything about other patients.
4. Tell Patient B’s family that you need to use the ECMO machine for another patient, but ultimately it is their choice when/whether to de‐escalate therapy.
Key Challenges
• These issues receive attention in public health emergencies, but we face them regularly in individual cases
• Much more challenging to address in individual cases because no policy guidance
• Optimal strategies are not defined for communication with families
Suggested References
Truog RD, et al. “Rationing in the Intensive Care Unit.” Critical Care Medicine. 2006; 34(4): 958‐963.
White DB, et al. “Who Should Receive Life Support During a Public Health Emergency? Using Ethical Principles to Improve Allocation Decisions.” Annals of Internal Medicine. 2009; 150(2): 132‐138.
Sprung CL, et al. “Triage of Intensive Care Patients: Identifying Agreement and Controversy.” Intensive Care Medicine. 2013; 39(11):1916‐24
Page 140

DAY 2 – FRIDAY MAY 11, 2018
7:30 – 8:00 CONTINENTAL BREAKFAST AND VISIT TO THE EXHIBIT HALL 8:00 – 8:10 WELCOME AND INTRODUCTION FROM CO‐CHAIRS
8:10 – 9:10 FIRST MORNING SESSION: BITE‐SIZED TEACHING (BST MODE) – K. MANNING
Intra‐abdominal hypertension – W. Greene
Chest tube fundamentals – P. Rajaram
I/O access, the new CODE line – D. Carpenter
Stress ulcer prophylaxis – A. Hawkins
Nutritional support – A. DePriest
High flow oxygen therapy – K. Hodge
Atrial fibrillation in the ICU – O. Mirza
9:10 – 9:30 MORNING BREAK AND EXHIBIT HALL
9:30 – 10:30 SECOND MORNING SESSION
Year‐in‐review: Medical Critical Care – W. Bender
Year‐in‐review: Neurological Critical Care – C. Pimentel
Year‐in‐review: Surgical and Burn Critical Care – O. Danner
10:30 – 11:00 SECOND BREAK AND EXHIBIT HALL
11:00 – 12:00 PLENARY LECTURE Nature’s Fury & Man’s Flurry: How Prepared are We for Disasters? Dr. Kay Guntupalli, Baylor College of Medicine
12:00 – 1:00 LUNCH
1:00 – 2:00 BREAKOUT SESSION #1
Basic / Advanced Mechanical Ventilation – A. Esper, B. Bray
ICU Ultrasonography – A. Mehta, D. Green, R. Hunt
ECMO Pearls and Pitfalls – M. Stentz
Hemodynamic Monitoring – M. Fisher, M. Still
Vascular Access and Simulation – L. Daniels, L. Eydelman
Targeted Temperature Management – A. Webb, C. Hall
2:00 – 2:20 AFTERNOON BREAK AND EXHIBIT HALL
2:20 – 3:20 BREAKOUT SESSION #2
3:20 – 3:30 LAST AFTERNOON BREAK
3:30 – 4:30 BREAKOUT SESSION #3
4:30 – 4:45 WRAP‐UP AND RAFFLE DRAWING
Page 141
Bite‐Sized Teaching (BST) Kimberly Manning, MD
Assoc Professor of Medicine, Emory University
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 142

Intra‐Abdominal Hypertension and the Abdominal Compartment
SyndromeWENDY GREENE, MD FACS FCCM
Southeastern Critical Care Summit
MAY 11, 2018
No conflicts of interest to disclose
Objectives
• Presentation
• Given a hypotensive and anuric patient
who has undergone massive fluid
resuscitation after exploratory laparotomy
for intra‐abdominal sepsis, the participant
can independently recognize intra‐
abdominal hypertension and abdominal
compartment syndrome.
Objectives
• Diagnosis
• In a patient with suspected abdominal compartment syndrome, the participant can describe the technique of intravesicularmeasurement.
• Operative Treatment (General Concepts)
o Given a patient with suspected abdominal compartment syndrome, the participant can identify when to call for surgical consultation.
Page 143

Objectives
• Non‐Operative Management, including Alternative and Adjuvant Treatments
– Given a patient with intra‐abdominal hypertension, the participant can describe non‐operative management.
– Given a patient with abdominal compartment syndrome the participant can describe when alternatives to operative management are appropriate.
Background
• Definition
• Intra‐Abdominal Pressure (IAP): pressure in abdominal cavity
• How ensure accurate IAP measurements
– End of expiration
– Supine
– No abdominal muscle contraction
– Transducer zeroed at midaxillary line
Intra‐Abdominal Pressure (IAP)
• Grade I, IAP 12‐15 mmHg
• Grade II, IAP 16‐20 mmHg
• Grade III, IAP 21‐25 mmHg
• Grade IV, IAP > 25 mmHg
1Malbrain ML et al., Results from the International Conference of Experts on Intra‐Abdominal hypertension and Abdominal Compartment Syndrome. I. Definitions ,Intensive Care Medicine 2006;32:1722 ‐1732
Page 144
Intraabdominal Hypertension
• Definition: Sustained intraabdominal pressure (IAP) ≥12 mmHg (nml 5‐7mmHg)
• Categories of IAH and timing of symptoms
– Hyperacute: seconds (laugh)
– Acute: hours (trauma)
– Subacute: days (medical patient)
– Chronic: months/years (pregnancy obesity)
Definition
• Abdominal Compartment Syndrome (ACS)
• Organ dysfunction caused by intra‐abdominal pressure >20 (+/‐ Abdominal Perfusion Pressure “APP” <60 mmHg) that is associated with new organ dysfunction / failure
Abdominal Compartment Syndrome
• Classification ACS
• Primary ACS: if the intra‐abdominal hypertension is due to intra‐abdominal injury
• Secondary ACS: if the splanchnic reperfusion occurs after massive resuscitation.
Page 145

Etiology
Primary ACS:
• Injury/disease to abdominal pelvic region
• Abdominal trauma
• Hemoperitoneum
• Pancreatitis
• Abdominal surgery
Secondary ACS:
• Injury/disease outside of abdominal/pelvic region
• fluid resuscitation, sepsis, burns; due to edema and ascites after shock and aggressive resuscitation
Etiology
Recurrent ACS:
redevelopment of the abdominal compartment syndrome following treatment of a primary or secondary type.
Etiology
Abdominal:
• Massive ascites,
• bowel distension,
• abdominal surgery
• intraperitoneal bleeding
• Retroperitoneal:
• ruptured abdominal aortic aneurysm
• pelvic fracture with bleeding
• pancreatitis
Page 146
Evidence Based Risk Factors
• Abdominal Surgery
• Acidemia
• Acute Pancreatitis
• Age
• Gastroparesis/ileus
• Hemo‐/pneumoperitoneum
• Increased head of bed angle
• Intra‐abdominal infection
(WSACS 2013 Guidelines)
• Liver dysfunction
• Major trauma
• Massive fluid resuscitation
• Mechanical Ventilation
• Obesity
• PEEP > 10
• Polytransfusion
• Prone positioning
• Sepsis
• Shock
Morbidity and Mortality
• Mortality for patients who have progressed to ACS: 10.6‐100%
• Most deaths are due to sepsis or multiple organ failure
• Majority of deaths within first 24 hours of injury
• Mortality is directly affected by decompression
– Evidence supports use of selective mesh closure after laparotomy for prevention
Pathophysiology
–Affects ALL systems of the body:
–Cardiovascular: Decreased CO; Markedly increased SVR
–Pulmonary: Reduced chest wall compliance and tidal volume; resulting in hypoxemia and hypercarbia
Page 147
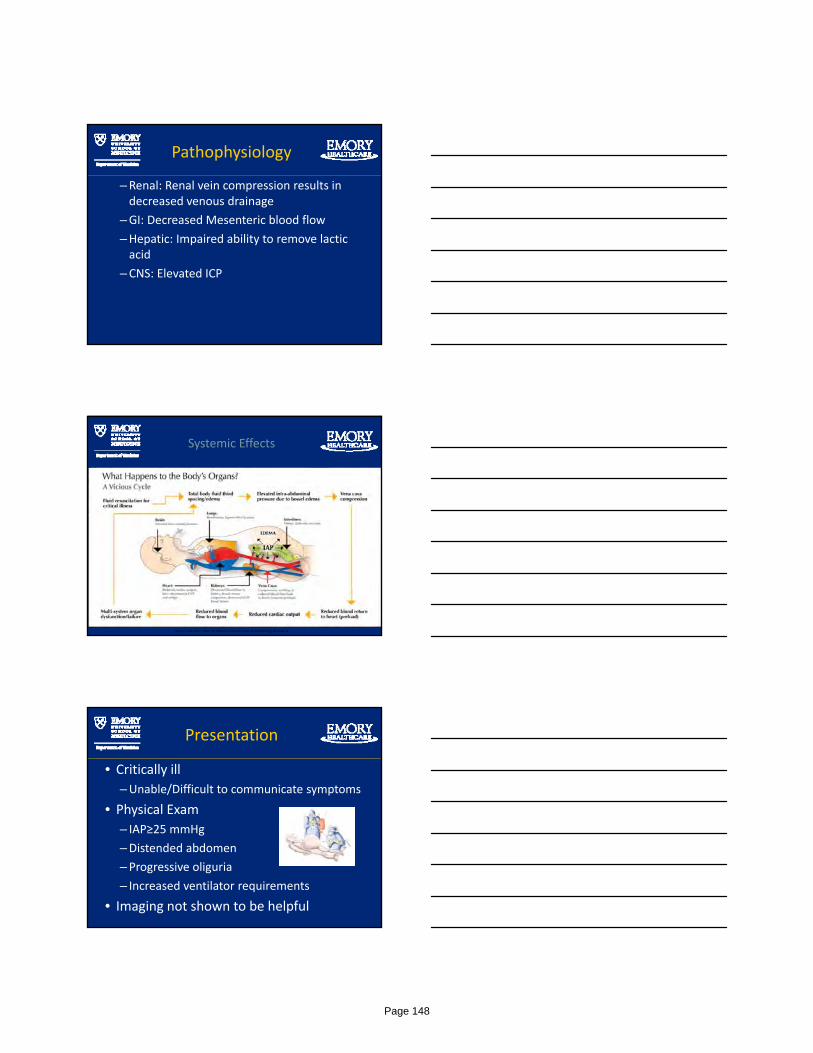
Pathophysiology
–Renal: Renal vein compression results in decreased venous drainage
–GI: Decreased Mesenteric blood flow
–Hepatic: Impaired ability to remove lactic acid
–CNS: Elevated ICP
Systemic Effects
http://abviser.com/products/abviser-iap-monitoring-device/a
Presentation
• Critically ill
–Unable/Difficult to communicate symptoms
• Physical Exam
– IAP≥25 mmHg
–Distended abdomen
–Progressive oliguria
– Increased ventilator requirements
• Imaging not shown to be helpful
Page 148
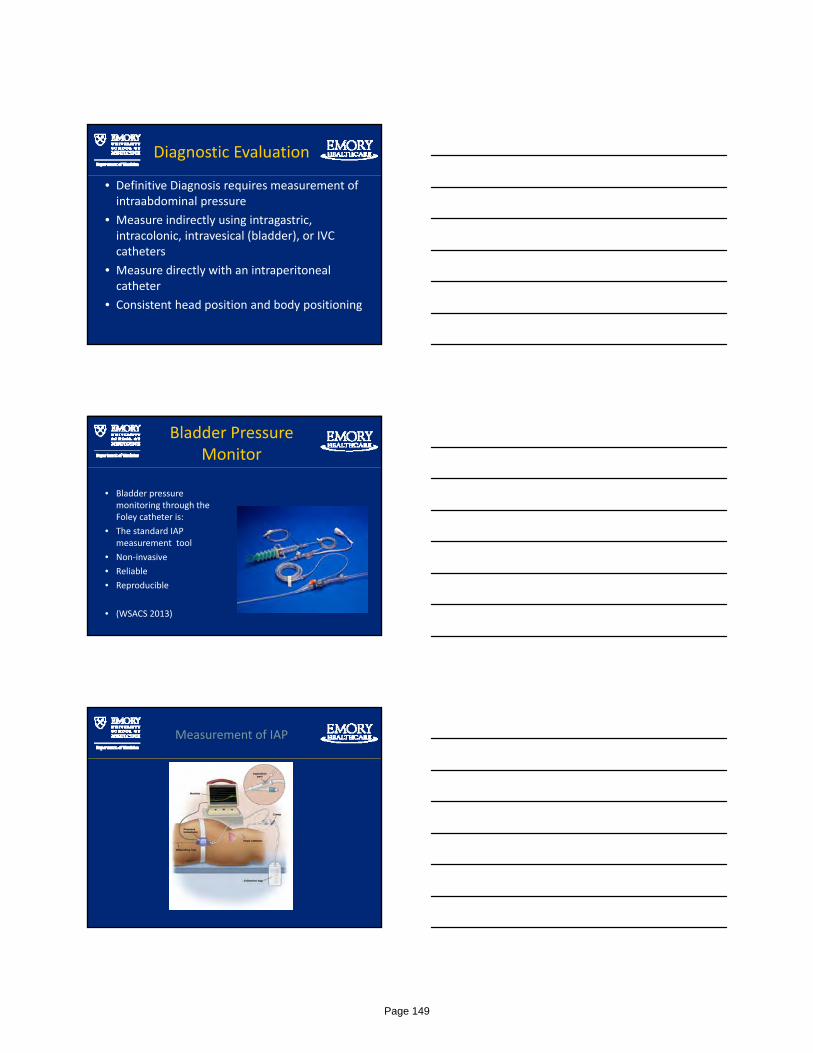
Diagnostic Evaluation
• Definitive Diagnosis requires measurement of intraabdominal pressure
• Measure indirectly using intragastric, intracolonic, intravesical (bladder), or IVC catheters
• Measure directly with an intraperitoneal catheter
• Consistent head position and body positioning
Bladder Pressure Monitor
• Bladder pressure monitoring through the Foley catheter is:
• The standard IAP measurement tool
• Non‐invasive
• Reliable
• Reproducible
• (WSACS 2013)
Measurement of IAP
Page 149
Management
• Supportive Care: neuromuscular blockade
• Ventilator Support
• Hemodynamic Support
• Surgical Decompression
–Percutaneous drain to remove fluid
–Decompressive Celiotomy
–Bedside laparotomy
• We could make no recommendation regardinguse of diuretics to mobilize fluids in hemodynamically stable patients with IAH after the acute resuscitation has been completed and the inciting issues/source control have been addressed
• We could make no recommendation regardingthe use of renal replacement therapies to mobilize fluid in hemodynamically stable patients with IAH after the acute resuscitation has been completed and the incitingissues/source control have been addressed
Page 150

• We could make n o recommendation regardingthe administration of albumin versus not, tomobilize fluid in hemodynamically stable patients with IAH after the acute resuscitation has been completed and the incitingissues/source control have been addressed
Page 151
WSACS Medical Management Algorithm
Intensive Care Med (2013) 39:1190–1206 DOI 10.1007/s00134-013-2906-z
Intensive Care Med (2013) 39:1190–1206 DOI 10.1007/s00134-013-2906-z
Temporary Abdominal Closure
• Goal: Control fluid losses and minimize loss of domain
• Techniques:
– Patch
– Negative Pressure Wound Systems
• Towel based
• Sponge Based
– Skin only
Page 152
Case: Dyspnea in ER
67 y.o. female presenting to ER with pleurisy, dyspnea• Hypotensive, agitated, H&P suggest liver disease• IVF resuscitation, intubation, sedation• Worsened over next 4‐6 hours ‐ Difficult to ventilate, hypoxic/hypercarbic, hypotension, no UOP.
• IAP = 45 mm Hg, abdominal ultrasound showed tense ascites paracentesis of 4500 cc fluid (IAP = 14)
• Immediate resolution of renal, pulmonary and hemodynamic compromise.
• Pathology shows malignant effusion – pancreatic CA.• Care withdrawn at later time and allowed to expire.
Etzion, Am J EM 2004
Case: Aspiration patient
77 y.o. male aspirated on general medicine floor. Transferred to MICU & intubated; hypotensive.
• 10 liters IVF overnight, Levophed 40 mcg/min. • Anuric (35 ml urine in 8 hours). • IAP = 31 mm Hg. KUB – massively distended small and large bowel. U/S shows no free ascitic fluid.
• Surgeon consulted for possible decompressive surgery• Rx: NGT, Rectal Tube, oral cathartics• 1 hour later: IAP 12 mm Hg, UOP 210 ml, norepinephrine discontinued.
Cheatham, WSACS 2006
Pearls
• Trauma is not required for ACS to develop:
• Intra‐abdominal hypertension and ACS occur in many settings (PICU, MICU, SICU, CVICU, NCC, OR, ER).
• IAP measurements are clinically useful: Help to determine if IAH is contributing to organ dysfunction (i.e. useful if normal or abnormal)
Page 153
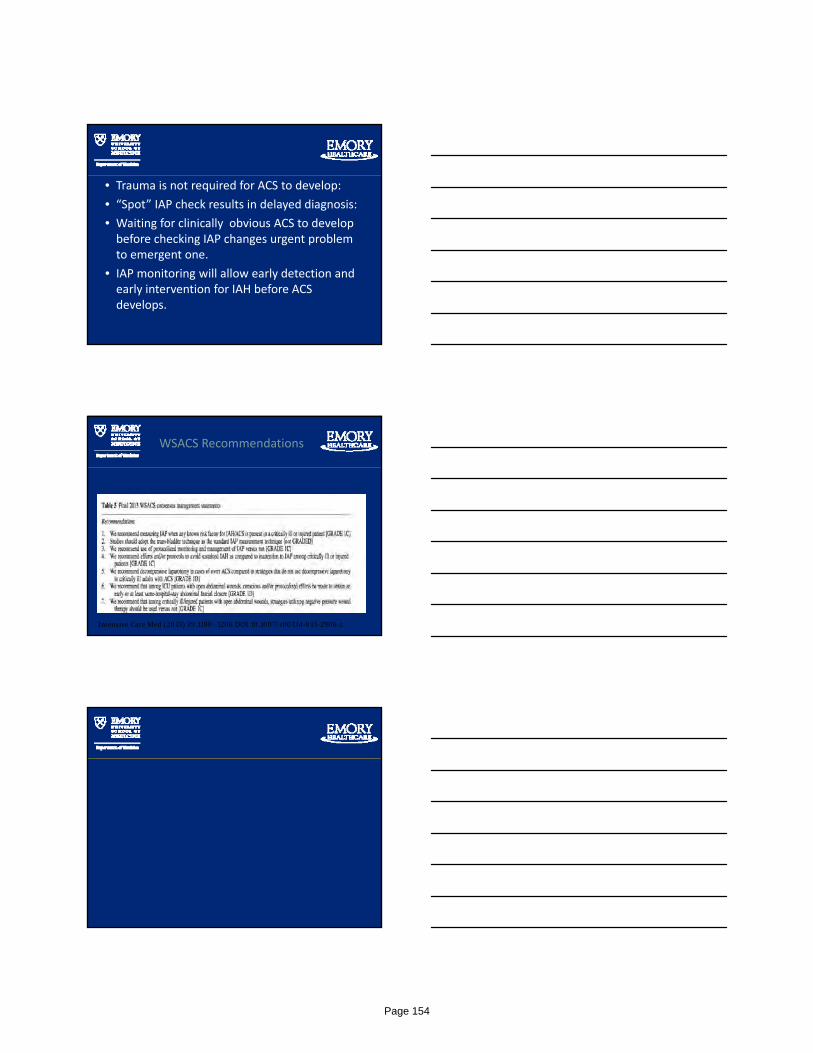
• Trauma is not required for ACS to develop:
• “Spot” IAP check results in delayed diagnosis:
• Waiting for clinically obvious ACS to develop before checking IAP changes urgent problem to emergent one.
• IAP monitoring will allow early detection and early intervention for IAH before ACS develops.
WSACS Recommendations
Intensive Care Med (2013) 39:1190–1206 DOI 10.1007/s00134-013-2906-z
Page 154

Thank You
?
References
• Kirkpatrick, Andrew W., Derek J. Roberts, Jan De Waele, Roman Jaeschke, Manu LNG Malbrain, Bart De Keulenaer, Juan Duchesne et al. "Intra‐abdominal hypertension and the abdominal compartment syndrome: updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome." Intensive care medicine 39, no. 7 (2013): 1190‐1206.
References
• Bailey J, Shapiro ML. Abdominal compartment syndrome. Crit Care. 2000;4(1):23–9
• Fabian TC, Bee TK. Chapter 29. Liver and Biliary Tract. In: Mattox KL, Moore EE, Feliciano DV. eds. Trauma, 7e. New York, NY: McGraw‐Hill; 2013. http://accesssurgery.mhmedical.com/content.aspx?bookid=529&Sectionid=41077269. Accessed September 22, 2014.
Page 155

References
• Wyrzykowski AD, Feliciano DV. Chapter 38. Trauma Damage Control. In: Mattox KL, Moore EE, Feliciano DV. eds. Trauma, 7e. New York, NY: McGraw‐Hill; 2013.
• Cothren C, Biffl WL, Moore EE. Chapter 7. Trauma. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Hunter JG, Matthews JB, Pollock RE. eds. Schwartz's Principles of Surgery, 9e. New York, NY: McGraw‐Hill; 2010.
References
• Balogh, Zsolt J., William Lumsdaine, Ernest E. Moore, and Frederick A. Moore. "Postinjuryabdominal compartment syndrome: from recognition to prevention." The Lancet 384, no. 9952 (2014): 1466‐1475.
References
• Björck, Martin, and Anders Wanhainen. "Management of abdominal compartment syndrome and the open abdomen." European Journal of Vascular and Endovascular Surgery47, no. 3 (2014): 279‐287.
Page 156
References
• Hunt, Leanne, Steve A. Frost, Ken Hillman, Phillip J. Newton, and Patricia M. Davidson. "Management of intra‐abdominal hypertension and abdominal compartment syndrome: a review." Journal of trauma management & outcomes 8, no. 1 (2014): 2.
• Hong JJ, Cohn SM, Perez JM, et al. Prospective study of the incidence and outcome of intra‐abdominal hypertension and the abdominal compartment syndrome. Br J Surg 2002; 89:591.
• Balogh Z, McKinley BA, Holcomb JB, et al. Both primary and secondary abdominal compartment syndrome can be predicted early and are harbingers of multiple organ failure. J Trauma 2003; 54:848.
• Balogh Z, McKinley BA, Cocanour CS, et al. Secondary abdominal compartment syndrome is an elusive early complication of traumatic shock resuscitation. Am J Surg 2002; 184:538.
Page 157

• Sugrue M. Abdominal compartment syndrome. Curr Opin Crit Care 2005; 11:333.
• Malbrain ML, Chiumello D, Pelosi P, et al. Incidence and prognosis of intraabdominal hypertension in a mixed population of critically ill patients: a multiple‐center epidemiological study. Crit Care Med 2005; 33:315.
• An G, West MA. Abdominal compartment syndrome: a concise clinical review. Crit Care Med 2008; 36:1304.
• Kron IL, Harman PK, Nolan SP. The measurement of intra‐abdominal pressure as a criterion for abdominal re‐exploration. Ann Surg 1984; 199:28.
• Cheatham ML, Safcsak K. Is the evolving management of intra‐abdominal hypertension and abdominal compartment syndrome improving survival? Crit Care Med 2010; 38:402.
Page 158
PRIYANKA RAJARAM, MDASS I STANT PROFESSOR OF MED IC INE
EMORY PULMONARY HYPERTENS ION PROGRAM
D IV I S I ON OF PULMONARY, AL LERGY, CR IT I CAL CARE AND SLEEP MED IC INE
MAY 1 1 TH , 2 0 1 8
PR IYANKA .RA JARAM@EMORY. EDU
Disclosure Summary
As a provider accredited by ACCME, Emory Clinic must ensure balance, independence, objectivity and scientific rigor in its educational activities. Course Director(s), Planning Committee Members, Faculty, and all others who are in a position to control the content of this educational activity are required to disclose all relevant financial relationships with any commercial interest related to the subject matter of the educational activity. Safeguards against commercial bias have been put in place. Faculty also will disclose any off label and/or investigational use of pharmaceuticals or instruments discussed in their presentation. Disclosure of this information will be published in course materials so those participants in the activity may formulate their own judgments regarding the presentation.
Nothing to disclose
Disclosure Summary
• Understand the fundamentals of a chest tube drainage system
• Understand the basics of troubleshooting a chest tube
Page 159

Chest Wall RecoilLung Elastic Recoil
Maron. Relating basic concepts of pulmonarymechanics to clinical situations. Advances in Physiology Education.
Maron. Relating basic concepts of pulmonarymechanics to clinical situations. Advances in Physiology Education.
Lung Elastic Recoil Chest Wall Recoil
Page 160
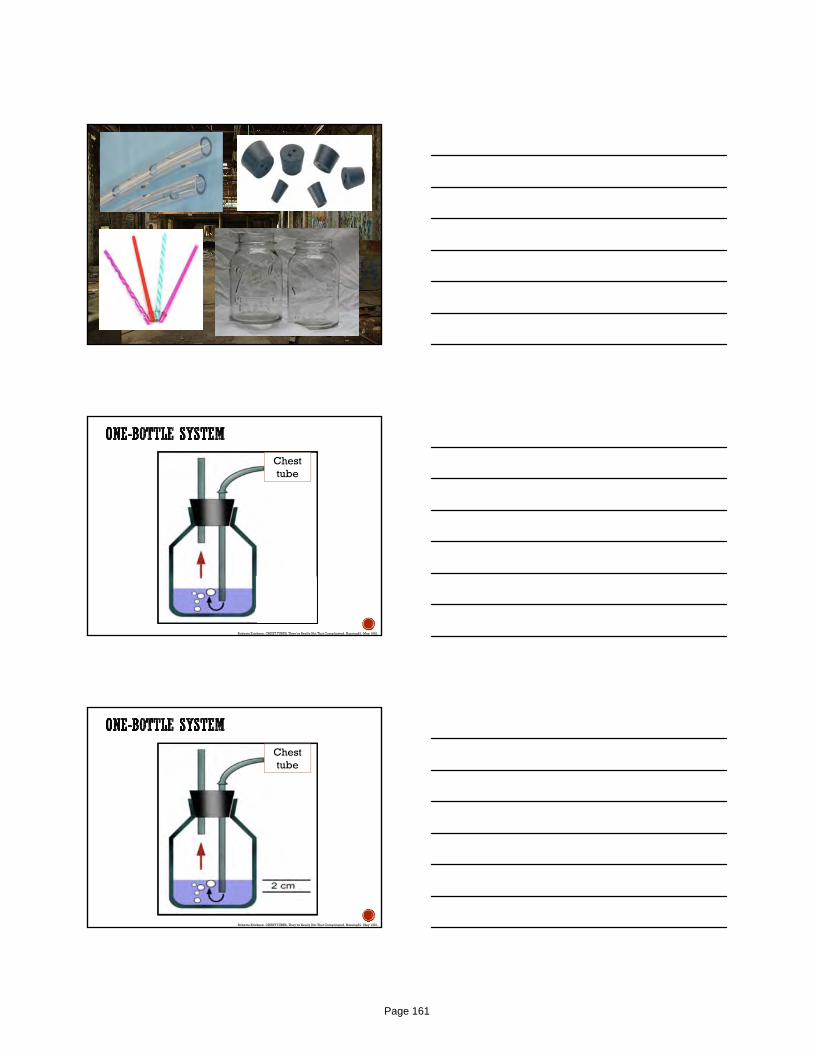
Chest tube
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Chest tube
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Page 161
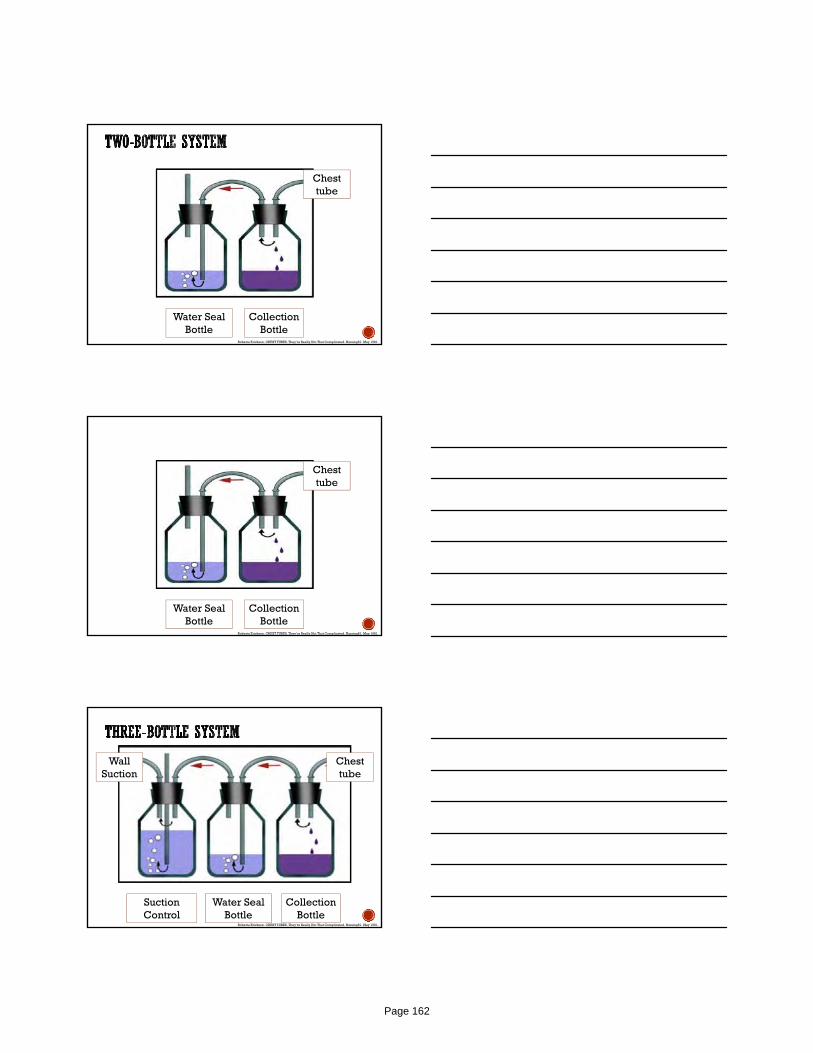
Chest tube
Water Seal Bottle
CollectionBottle
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Chest tube
Water Seal Bottle
CollectionBottle
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
12
Chest tube
Wall Suction
Water Seal Bottle
CollectionBottle
Suction Control
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Page 162

13
Chest tube
Wall Suction
Water Seal Bottle
CollectionBottle
Suction Control
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Page 163
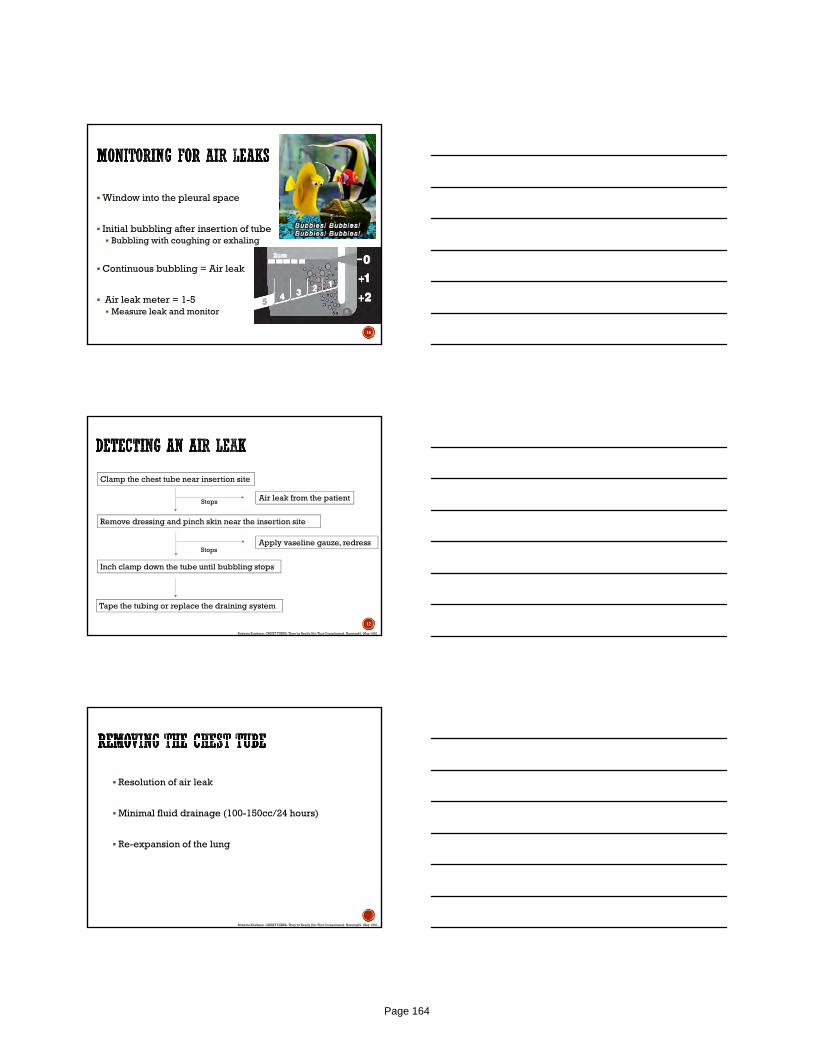
Window into the pleural space
Initial bubbling after insertion of tube Bubbling with coughing or exhaling
Continuous bubbling = Air leak
Air leak meter = 1-5 Measure leak and monitor
16
17
Clamp the chest tube near insertion site
Stops Air leak from the patient
Remove dressing and pinch skin near the insertion site
Stops Apply vaseline gauze, redress
Inch clamp down the tube until bubbling stops
Tape the tubing or replace the draining system
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Resolution of air leak
Minimal fluid drainage (100-150cc/24 hours)
Re-expansion of the lung
Roberta Erickson. CHEST TUBES. They’re Really Not That Complicated. Nursing81. May 1981.
Page 164
One-piece disposable box = Three bottle system
Depth of water is important for water seal
Continuous bubbling = Air leak
Too much suction can prolong air leaks
19
Page 165
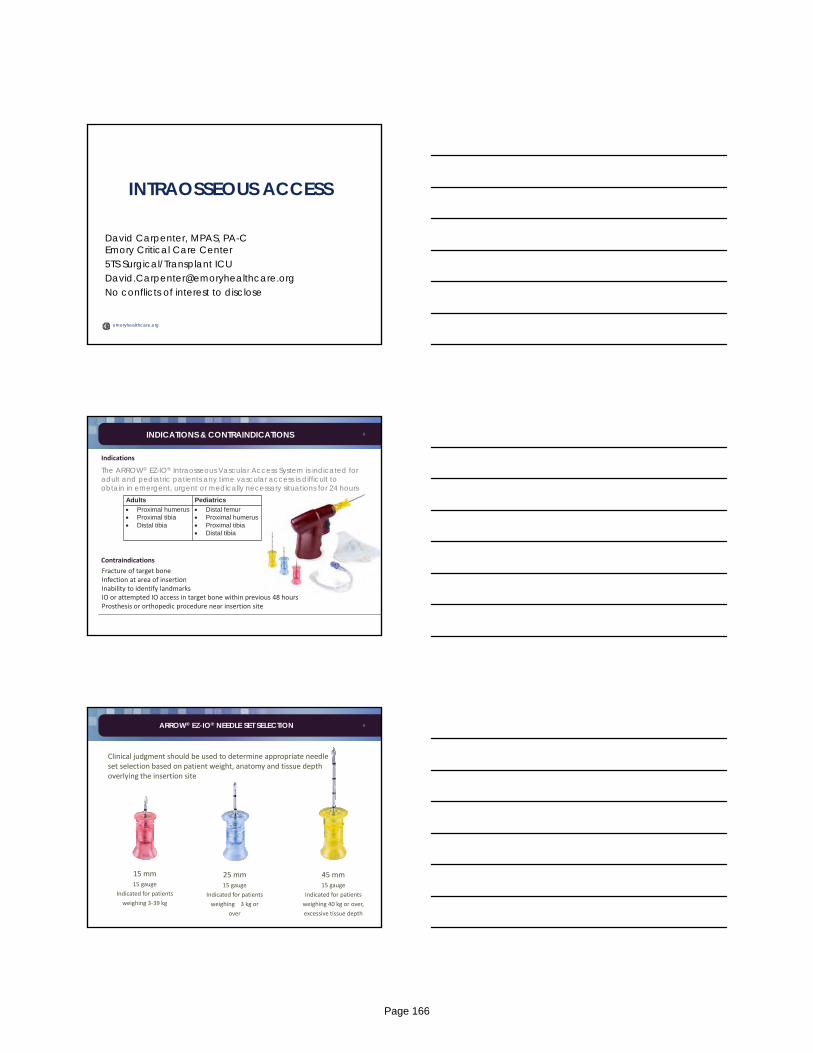
emoryhealthcare.org
INTRAOSSEOUS ACCESS
David Carpenter, MPAS, PA-CEmory Critical Care Center5TS Surgical/Transplant [email protected] conflicts of interest to disclose
2
The ARROW® EZ-IO® Intraosseous Vascular Access System is indicated for adult and pediatric patients any time vascular access is difficult to obtain in emergent, urgent or medically necessary situations for 24 hours
Contraindications
Fracture of target bone Infection at area of insertionInability to identify landmarksIO or attempted IO access in target bone within previous 48 hoursProsthesis or orthopedic procedure near insertion site
Adults Pediatrics
Proximal humerus Proximal tibia Distal tibia
Distal femur Proximal humerus Proximal tibia Distal tibia
Indications
INDICATIONS & CONTRAINDICATIONS
3ARROW® EZ-IO® NEEDLE SET SELECTION
15 mm15 gauge
Indicated for patients
weighing 3‐39 kg
25 mm15 gauge
Indicated for patients
weighing 3 kg or
over
45 mm15 gauge
Indicated for patients
weighing 40 kg or over,
excessive tissue depth
Clinical judgment should be used to determine appropriate needle set selection based on patient weight, anatomy and tissue depth overlying the insertion site
Page 166
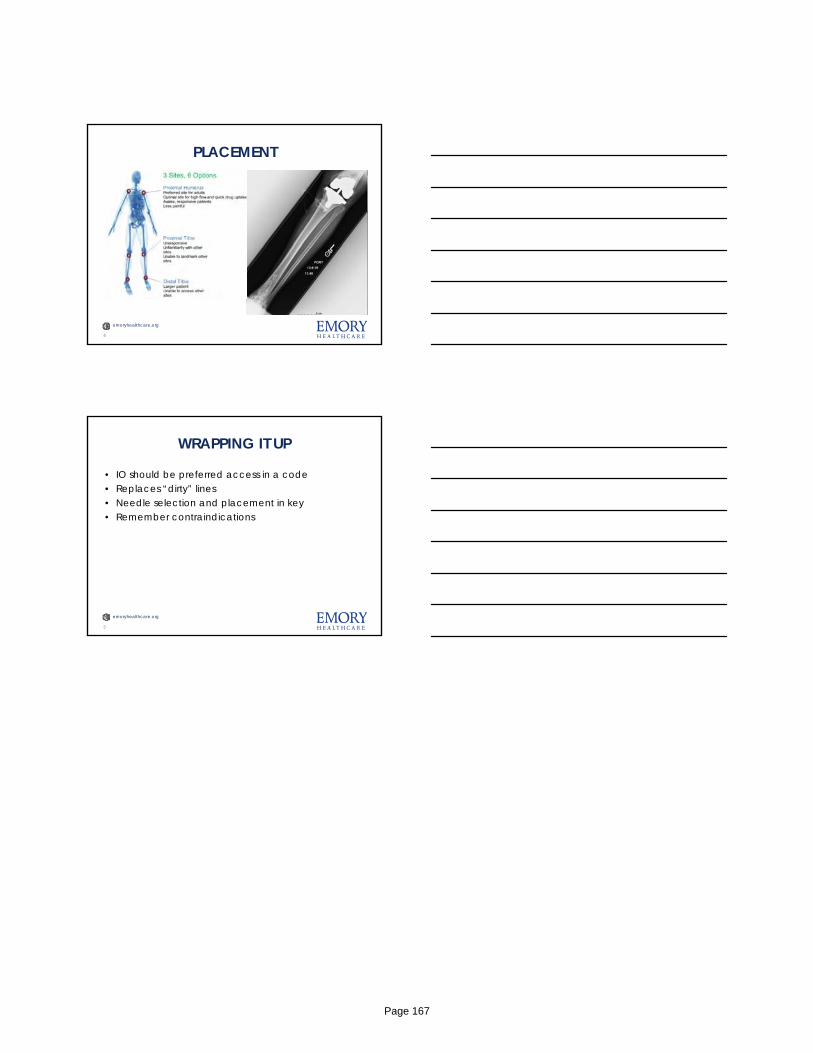
emoryhealthcare.org
PLACEMENT
4
emoryhealthcare.org
WRAPPING IT UP
• IO should be preferred access in a code• Replaces “dirty” lines• Needle selection and placement in key• Remember contraindications
5
Page 167
Stress Ulcer Prophylaxis
Anthony Hawkins, PharmD, BCCCPClinical Assistant Professor
University of Georgia College of PharmacyMedical College of Georgia at Augusta University
Clinical Specialist, Medical ICU, Phoebe Putney Memorial HospitalNo conflicts of interest to disclose
Objective
1994
Cook DJ. N Engl J Med 1994;330:377‐81
Page 168

1999
AJHP 1999;56:347‐79.
October 2017
Page 169
PROTO
N PUMP
INHIBITORS
H‐2 RECEPTO
R
BLO
CKER
S
Preferred Agent?
• EAST (2008)
– No difference between H2RAs and PPIs (level 1)
• Danish Society of ICM (2014)
– We suggest using PPIs when SUP is indicated in the ICU (2C)
• Surviving Sepsis Campaign
– 2008: We recommend SUP using H2RA (1A) or PPI (1B)
– 2012: We suggest the use of PPIs rather than H2RAs (2C)
– 2016: We suggest using either PPIs or H2RAs (weak recommendation, low quality of evidence)
Dellinger RP. Intensive Care Med 2008;34:17‐60. Dellinger RP. Crit Care Med 2013;41:580‐637. Rhodes A. Intensive Care Med 2017;43:304‐77. www.East.org. Madsen KR. Dan Med J 2014;61:C4811.
Incidence of clinically‐significant bleeding
0
2
4
6
8
10
12
14
16
1979‐1985 1995‐2001 After 2001
15%
< 3%
< 1.5%
No prophylaxisEN practice?
ProphylaxisEN practice?
Better ProphylaxisEN practice?
Percentage
Cook DJ. N Engl J Med 1994;330:377‐81.Schuman RB. Ann Intern Med 1987;106:562‐7. Ben‐Menachem T. Ann Intern Med 1994;121:568‐75. MacLaren R. J Pharm Practice 2002;15:147‐57.
Page 170
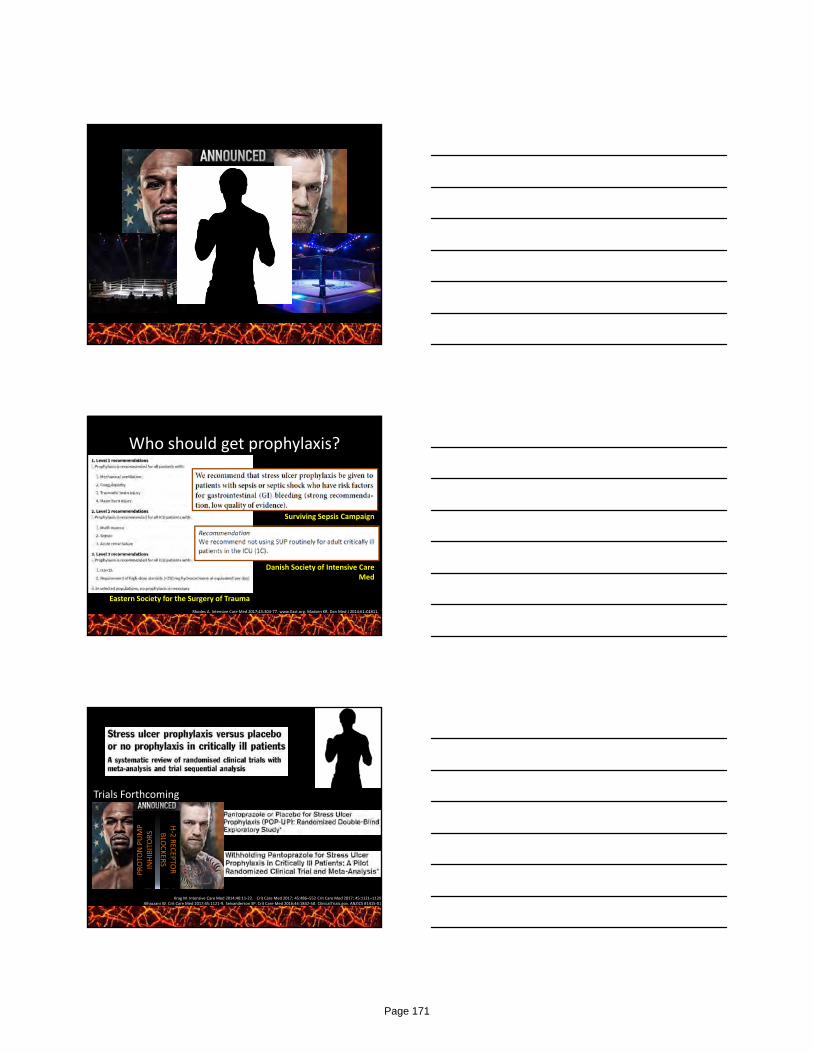
PROTO
N PUMP
INHIBITORS
H‐2 RECEPTO
R
BLO
CKER
S
Who should get prophylaxis?
Rhodes A. Intensive Care Med 2017;43:304‐77. www.East.org. Madsen KR. Dan Med J 2014;61:C4811.
Eastern Society for the Surgery of Trauma
Surviving Sepsis Campaign
Danish Society of Intensive Care Med
Krag M. Intensive Care Med 2014;40:11‐22. Crit Care Med 2017; 45:486–552 Crit Care Med 2017; 45:1121–1129 Alhazzani W. Crit Care Med 2017;45:1121‐9. Selvanderson SP. Crit Care Med 2016;44:1842‐50. ClinicalTrials.gov. ANZICS #1415‐01
Trials Forthcoming
– PEPTIC (ANZICS)
– SUP‐ICU (Denmark)
– PPI‐EN (USA)
PROTO
N PUMP
INHIBITORS
H‐2 RECEPTO
R
BLO
CKER
S
Page 171

Conclusions
• Confident that not all ICU patients need SUP
• Not real sure which patients do
– Less than we think
• Controversy of PPI vs H2RAs lives on
• Feed when you can
• Potential for cost savings
Page 172
Choosing the Right Enteral Nutrition Formula for the Critically Ill PatientChoosing the Right Enteral Nutrition Formula for the Critically Ill Patient
Ashley DePriest, MS, RD, LD, CNSCNutrition Support Dietitian | Northside Hospital AtlantaPresident- Elect | Southeast Chapter Society of Critical Care Medicine
Ashley DePriest, MS, RD, LD, CNSCNutrition Support Dietitian | Northside Hospital AtlantaPresident- Elect | Southeast Chapter Society of Critical Care Medicine
Types of FormulasTypes of Formulas
Standard Elemental/Semi Elemental
Immune Modulating
Disease Specific
StandardStandard
Polymeric, intact nutrients +/-soluble and/or insoluble fiber
Non fiber containing appropriate for most ICU patients Best to start this ASAP and wait for Dietitian
assessment for specialized formulas
Examples: Isosource HN, Osmolite 1.5
Polymeric, intact nutrients +/-soluble and/or insoluble fiber
Non fiber containing appropriate for most ICU patients Best to start this ASAP and wait for Dietitian
assessment for specialized formulas
Examples: Isosource HN, Osmolite 1.5
Page 173
Elemental/Semi ElementalElemental/Semi Elemental
Hydrolyzed formula
Contains partially (semi) or completely hydrolyzed, or “pre digested” nutrients
Diarrhea (NOT related to medication); digestive enzyme deficiencies
Peptamen, Vital (semi), Vivonex(elemental)
Hydrolyzed formula
Contains partially (semi) or completely hydrolyzed, or “pre digested” nutrients
Diarrhea (NOT related to medication); digestive enzyme deficiencies
Peptamen, Vital (semi), Vivonex(elemental)
Immune ModulatingImmune Modulating
Contain supplemental nutrients to support metabolically stressed patients Arginine, glutamine, nucleic acids, omega 3 FAs
Not recommended for routine use in MICU Best data in surgical, trauma, burn or head/neck cancer patients
Also appropriate for large wounds such as stage III, IV pressure ulcers
Must provide at least 60-80% of total caloric and protein needs in order to gain benefits of immune enhancing nutrients (i.e. do not use for tickle feeds, too expensive!)
Can come in standard or semi-elemental formulations
Impact, Impact Peptide, Pivot
Contain supplemental nutrients to support metabolically stressed patients Arginine, glutamine, nucleic acids, omega 3 FAs
Not recommended for routine use in MICU Best data in surgical, trauma, burn or head/neck cancer patients
Also appropriate for large wounds such as stage III, IV pressure ulcers
Must provide at least 60-80% of total caloric and protein needs in order to gain benefits of immune enhancing nutrients (i.e. do not use for tickle feeds, too expensive!)
Can come in standard or semi-elemental formulations
Impact, Impact Peptide, Pivot
Other Disease Specific FormulasOther Disease Specific Formulas
Renal – NOT an automatic use for renal failure; NOT therapeutic, only treats “symptoms” i.eelevated electrolytes; NOT recommended for use in ICU patients
Hepatic – Branch Chain amino acids, lower protein; NOT recommended for use in ICU patients unless as last ditch effort
Lung/Respiratory – Newer data suggests that older studies had better outcomes because of more adequate PROTEIN rather than the therapeutic effects of the formulation
Renal – NOT an automatic use for renal failure; NOT therapeutic, only treats “symptoms” i.eelevated electrolytes; NOT recommended for use in ICU patients
Hepatic – Branch Chain amino acids, lower protein; NOT recommended for use in ICU patients unless as last ditch effort
Lung/Respiratory – Newer data suggests that older studies had better outcomes because of more adequate PROTEIN rather than the therapeutic effects of the formulation
Page 174
Other ConsiderationsOther Considerations
Concentration
• Hypertonic feedings may cause osmotic diarrhea
• Concentration also affects caloric density
• Consider fluid balance/needs
Osmolality by Caloric ConcentrationOsmolality by Caloric Concentration
Caloric Density Osmolality mOsm/kg H20
1 kcal/mL 300-3301.2 kcal/mL 400-5101.5 kcal/mL 525-550
2 kcal/mL 780-800
~300 mOsm
Other ConsiderationsOther Considerations
Concentration
• Hypertonic feedings may cause osmotic diarrhea
• Concentration also affects caloric density
• Consider fluid balance/needs
Fiber
• Insoluble not recommended• Soluble OK as needed but
not routinely• Some formulas have
inherent fiber, sometimes need supplemental
• Do not use in patients at risk for gut ischemia or severe dysmotility
• Remember fiber’s affect on gastric emptying!
Modulars
• Protein• HMB
Page 175
SCCM/ASPEN Guidelines for the Provision & Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient
SCCM/ASPEN Guidelines for the Provision & Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient
Section E1.Section E1.
Based on expert consensus, we suggest using a standard polymeric formula when initiating EN in the ICU setting. We suggest avoiding the routine use of all specialty formulas in critically ill patients in a MICU and disease-specific formulas in the SICU.
Based on expert consensus, we suggest using a standard polymeric formula when initiating EN in the ICU setting. We suggest avoiding the routine use of all specialty formulas in critically ill patients in a MICU and disease-specific formulas in the SICU.
Consult your Registered Dietitian! Consult your Registered Dietitian!
Page 176
HIGH FLOW OXYGEN THERAPY
Kiley Hodge, BS, RRT-ACCS
No conflicts of interest to disclose
Objectives
❏ Review of oxygen therapy
❏ Explain high flow oxygen therapy
❏ Management of high flow oxygen therapy
Oxygen Therapy
First-line treatment in hypoxemic patients
Low Flow
Up to 15 lpm
FiO2 varies
Insufficient humidification
Page 177

Oxygen Therapy
Low Flow High Flow
This is High Flow
FLOW
Page 178
HFNC Devices
High Flow Indications
Hypoxemic ARF
Research is ongoing in other settings
● Pre intubation
● Post extubation
● Obese patients
● Bronchoscopy
High Flow
Page 179
Temperature31, 34, 37
Patient comfort
Mucociliary clearance
Prevent airway desiccation
Sophisticated circuits prevent rainout
Flow20 - 60 L/min
60 L/min
Why?
Quiet, restful breathing
15 - 30 L/min
Respiratory distress
60 - 180 L/min
FIO2
.21 - 1.0
Oxygen dilution
Flow-dependent FIO2
Wean for SpO2 90 - 92%
Page 180
Weaning
FIO2 for SpO2 90 - 92%
Assess respiratory rate, pattern, SpO2
Improvement continue to wean
Decrease to FIO2 .4, Decrease Flow
40/40
30/30
Low flow HFNC
Increased work of breathing continues
Escalate care to NIV or Intubation
Beware of 60/100
Patient Selection
No Nose
COPDNIV
Pulmonary Edema
NIV
Benefits
Page 181

PEEP
Low PAP not CPAP
Mouth breathers (most ARF)
Increased lung volumes and FRC
Prone Position
1 cmH2O per 10 L/min flow
Page 182
CO2 Removal
Decrease in CO2 rebreathing
Clears airway dead space
Increases alveolar ventilation
Prediction of Success
ROX Index
SpO2/FiO2
RR> 4.88
88/1 = 3.1428
90/.6 = 625
JCC 2016
Prediction of FailurePattern
Respiratory rate
Oxygen
60/100
Page 183
There’s an App!
THANK YOU!Hernández, G., Roca, O., & Colinas, L. (2017). High-flow nasal cannula support therapy: new insights and improving performance. Critical Care,21(1). doi:10.1186/s13054-017-1640-2
Nielsen, K. R., Ellington, L. E., Gray, A. J., Stanberry, L. I., Smith, L. S., & Diblasi, R. M. (2017). Effect of High-Flow Nasal Cannula on Expiratory Pressure and Ventilation in Infant, Pediatric, and Adult Models. Respiratory Care,63(2), 147-157. doi:10.4187/respcare.05728
Papazian, L., Corley, A., Hess, D., Fraser, J. F., Frat, J., Guitton, C., . . . Azoulay, E. (2016). Use of high-flow nasal cannula oxygenation in ICU adults: a narrative review. Intensive Care Medicine,42(9), 1336-1349. doi:10.1007/s00134-016-4277-8
Page 184
Atrial fibrillation
in the ICU ::Something rapid this
way comes
Omer Mirza, MD
Cardiology Fellow (PGY6)
Southeastern Critical Care Summit
No conflicts of interest to disclose
Objectives :: Upcoming Attractions
1. Differentiate atrial fibrillation from other atrial tachyarrhythmias
2. Identify key etiologies that would change medical management
3. Implement appropriate pharmacotherapy for various common scenarios
No financial disclosures
Diagnosis :: Insert Tachy Joke Here
Sinus tach
O'Keefe, et al. Complete Guide to ECGs, 2017.
Page 185
O'Keefe, et al. Complete Guide to ECGs, 2017.
Diagnosis :: Insert Tachy Joke Here
Sinus tach
Atrial tach
Diagnosis :: Bombarding Beats
Sinus tach
Atrial tach
Multifocal atrial tach
O'Keefe, et al. Complete Guide to ECGs, 2017.
Diagnosis :: Bombarding Beats
Sinus tach
Atrial tach
Multifocal atrial tach
Atrial flutter
O'Keefe, et al. Complete Guide to ECGs, 2017.
Page 186
Diagnosis :: Full of Sound and Foci
Sinus tach
Atrial tach
Multifocal atrial tach
Atrial flutter
Atrial Fibrillation
Kibose, et al. Cardiac Arrhythmias,, 2016, pp. 401–412.Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Walkey, et al. “New‐Onset Atrial Fibrillation During Hospitalization.” JACC, 2014
Risk Factors :: Prickly Predisposition
Alteration in adrenergic tone
Increased atrial stretch
Fibrotic remodeling
Inflammatory disruption of electrical
channels
• Thyrotoxicosis• Sepsis• Acute
pulmonary pathology
• HTN• Valvular
pathology• CHF
• Age > 65• Myocardial
ischemia
• Pericarditis, myocarditis
• Post cardiac surgery
Block Shock
UnstableStable
Key Decision :: Unstable or Under‐caffeinated
Page 187

Cardioversion :: Shockingly Simple
– Hemodynamic instability
– Poor peripheral perfusion
– Cardiogenic shock / low output
– Altered mental status.
S
H
O
C
K
ynchronized
igh voltage
Anti C agulate
all if stable
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Cardioversion :: Phone a Friendly Cardiologist
– If stable, the decision to cardiovert includes:
• Risk for current intra‐atrial thrombus if atrial
fibrillation has occurred for > 48H
• Necessity for anticoagulation for subsequent thirty
days regardless of CHA2DS2VASc
• Is underlying trigger adequately treated; how
effective will this cardioversion be
S
H
O
C
K
ynchronized
igh voltage
Anti C agulate
all if stable
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Rate Control :: AFFIRMative
Drug of Choice Bolus Drip Indication
Esmolol 0.5mcg/kg over 1min
50mcg/kg/min up to 200mcg/kg/min
First line therapy, adrenergically driven afib.
Diltiazem 0.25mg/kg over 2 min
5‐15mg/hr Alternative therapy if significant bronchospasm.
Amiodarone 150mg over 10 min
1mg/min x 6 hrs then 0.5mg/min x 18 hrs
Second line therapy if evidence of ADHF.
Digoxin 500mcg IV 125‐250mcg q6H for total 10‐12mcg/kg
Third line therapy if contraindications to above
B
L
O
C
K
eta blocker
Di tiazem
Ami darone
aveat
ids
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Page 188
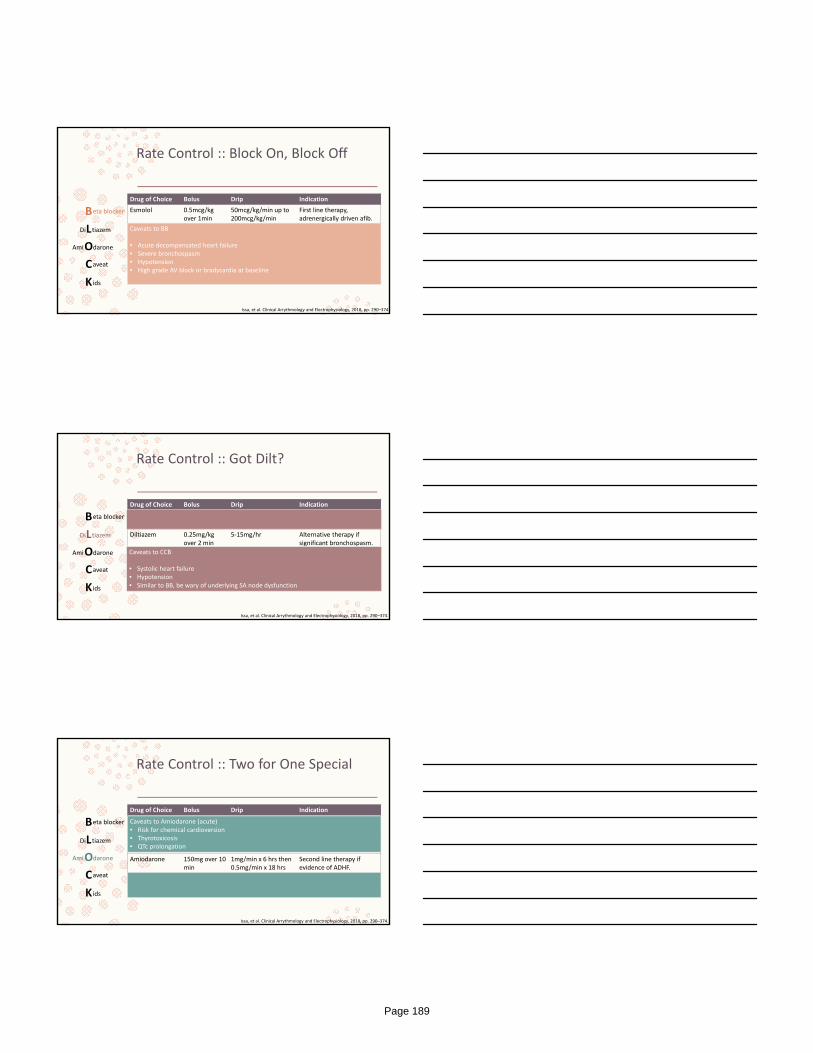
Rate Control :: Block On, Block Off
Drug of Choice Bolus Drip Indication
Esmolol 0.5mcg/kg over 1min
50mcg/kg/min up to 200mcg/kg/min
First line therapy, adrenergically driven afib.
Diltiazem 0.25mg/kg over 2 min
5‐15mg/hr Alternative therapy if significant bronchospasm.
Amiodarone 150mg over 10 min
1mg/min x 6 hrs then 0.5mg/min x 18 hrs
Second line therapy if evidence of ADHF.
Digoxin 500mcg IV 125‐250mcg q6H for total 10‐12mcg/kg
Third line therapy if contraindications to above
B
L
O
C
K
eta blocker
Di tiazem
Ami darone
aveat
ids
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374
Caveats to BB
• Acute decompensated heart failure• Severe bronchospasm• Hypotension• High grade AV block or bradycardia at baseline
Rate Control :: Got Dilt?
Drug of Choice Bolus Drip Indication
Esmolol 0.5mcg/kg over 1min
50mcg/kg/min up to 200mcg/kg/min
First line therapy, adrenergically driven afib.
Diltiazem 0.25mg/kg over 2 min
5‐15mg/hr Alternative therapy if significant bronchospasm.
Amiodarone 150mg over 10 min
1mg/min x 6 hrs then 0.5mg/min x 18 hrs
Second line therapy if evidence of ADHF.
Digoxin 500mcg IV 125‐250mcg q6H for total 10‐12mcg/kg
Third line therapy if contraindications to above
B
L
O
C
K
eta blocker
Di tiazem
Ami darone
aveat
ids
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Caveats to CCB
• Systolic heart failure• Hypotension• Similar to BB, be wary of underlying SA node dysfunction
Rate Control :: Two for One Special
Drug of Choice Bolus Drip Indication
Esmolol 0.5mcg/kg over 1min
50mcg/kg/min up to 200mcg/kg/min
First line therapy, adrenergically driven afib.
Diltiazem 0.25mg/kg over 2 min
5‐15mg/hr Alternative therapy if significant bronchospasm.
Amiodarone 150mg over 10 min
1mg/min x 6 hrs then 0.5mg/min x 18 hrs
Second line therapy if evidence of ADHF.
Digoxin 500mcg IV 125‐250mcg q6H for total 10‐12mcg/kg
Third line therapy if contraindications to above
B
L
O
C
K
eta blocker
Di tiazem
Ami darone
aveat
ids
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Caveats to Amiodarone (acute)• Risk for chemical cardioversion• Thyrotoxicosis• QTc prolongation
Page 189
Rate Control :: Pharmacologic Kitchen Sink
Drug of Choice Bolus Drip Indication
Esmolol 0.5mcg/kg over 1min
50mcg/kg/min up to 200mcg/kg/min
First line therapy, adrenergically driven afib.
Diltiazem 0.25mg/kg over 2 min
5‐15mg/hr Alternative therapy if significant bronchospasm.
Amiodarone 150mg over 10 min
1mg/min x 6 hrs then 0.5mg/min x 18 hrs
Second line therapy if evidence of ADHF.
Digoxin 500mcg IV 125‐250mcg q6H for total 10‐12mcg/kg
Third line therapy if contraindications to above
B
L
O
C
K
eta blocker
Di tiazem
Ami darone
aveat
ids
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Caveats to Digoxin (acute)
• Note that Digoxin is vagally mediated.• Ineffective for adrenergically driven atrial fibrillation • Renal Impairment
B
L
O
C
K
eta blocker
Di tiazem
Ami darone
aveat
ids
Important Caveat :: Dangerous Detour
– In a young patient with a wide complex, aberrantly conducted rhythm, consider
pre‐excited afib through an accessory pathway (e.g. WPW)
– If hemodynamically stable, avoid agents that would preferentially block the AVN
Issa, et al. Clinical Arrythmology and Electrophysiology, 2018, pp. 290–374.
Summary :: Remember ‐ Shock Or Block… or Amio … or dig … or procainamide … … just call cards at this point
Irregularly Irregular Tachyarrhythmia without P waves
Hemodynamically Stable?
No > Synchronized Cardioversion
Yes > Decompensated Heart Failure?
No > Bronchospasm
No (or borderline BP) > Esmolol
Yes > Diltiazem
Yes > Thyrotoxicosis?
No > Amiodarone Yes > Digoxin
Page 190

Questions?
– Feel free to email:
– Thanks for listening!
Aidan Azhera.k.a. Chunkey Monkey
Page 191

Year In ReviewMedical Critical Care
William Bender MD, MPHAssistant Professor
Division of Pulmonary, Allergy, Critical Care and Sleep MedicineEmory University School of Medicine
May 11, 2018
I have no financial disclosures
Objectives
• Review relevant critical care literature published over the last year
• Assess the quality of the literature
• Evaluate the applicability of the literature to current bedside practice
Page 192
Methodology and Selection
• Reviewed core clinical journals for articles published over the past year
• Solicited input from faculty and fellows
• Perused the FOAM critical care landscape on the world wide web
Study 1
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Clinical Question– Is there an association between the timing of treatment and risk‐adjusted mortality for patients with severe sepsis and septic shock?
• Design– Retrospective observational study using the NYSDOH database
• April 2014 through June 2016• 185 hospitals
– Primary exposure was the time to completion of the 3‐hour bundle
– Primary outcome was in hospital mortality
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Page 193
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Inclusion– Greater than 17 years of age– Severe sepsis/septic shock as defined by Sepsis‐2– Sepsis protocol initiated in the ED within 6 hours after arrival at
the hospital
• Exclusion– Completion of the 3 hour bundle more than 12 hours after
initiation of the protocol– Bundle contraindicated– Patient declined intervention or with advance directives limiting
treatment– Enrollment in a clinical trial– 36 hospitals were excluded due to limited numbers
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Results– 111,816 patients screened 49,337 eligible
– 82.5% completed 3‐hour bundle within 3 hours• Median time – 1.30 hours (0.65 – 2.35)
• Median time to antibiotics – 0.95 hours (0.35 – 1.95)
• Median time to fluids – 2.56 hours (1.33 – 4.20)
– Characteristics of the patients who had the 3‐hour bundle completed within 3 hours were similar to those who had it completed between hours 3 through 12
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Results
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Page 194
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Results
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Results
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Results
– Additional analyses
• Delaying collection of blood cultures and lactates was associated with mortality
– OR 1.04 per hour (1.02 – 1.06)
• Hospitals that had a higher rate of bundle completion within 3 hours were somewhat smaller and less likely to be teaching hospitals
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Page 195

Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Strengths– Important clinical question
– Large data set
– Multiple centers
– Real world “pragmatic” data
– Multiple statistical analyses performed to minimize confounders
• Weaknesses– Observational data describe associations
– Better functioning hospitals >> bundle
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
• Discussion
– IV fluids
• Timing NOT amount
• Why no effect?– Confounding – sicker patients get fluid sooner
– Volume and rate administered led to adverse effects
• Fluid responsive heterogenity
– Teaching hospitals and adherence
• Anti‐standardized care bias
Seymour CW, Gesten F, Prescott H, Friedrich M, Iwashyna T, Phillips G et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. New Engl J Med 2017;376:2235‐44
Study 2
Page 196
ART Trial
• Clinical Question
– Does a lung recruitment maneuver associated with PEEP titration according to respiratory system compliance decrease 28 day mortality when compared with a conventional low‐PEEP strategy?
• Design
– Randomized control trial
– 120 ICUs from 9 countries (Europe/S. America)
– Primary outcome was 28 day mortalityWriting Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
ART Trial
• Inclusion– Moderate to severe ARDS of less than 72 hours duration
– Persistent hypoxemia after three hours of LTV with a PEEP of at least 10
• Exclusion– Age less than 18– Unstable shock– Contraindications to hypercapnia– Pneumothorax/Subcutaneous emphysema/ACS– Palliative care focus
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
ART Trial
• Intervention– Paralyze and use PCV (PI of 15)
– Recruitment• To PEEP of 25 for 1 min, 35 for 1 min then 45 for 2 min
• PEEP to 23, VCV initiated and static compliance checked
• PEEP down titrated by 3cm H2O every 4 min and static compliance checked
• Optimal PEEP taken to be when best compliance achieved + 2cm H2O
• VCV with optimal PEEP
• Control
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
Page 197
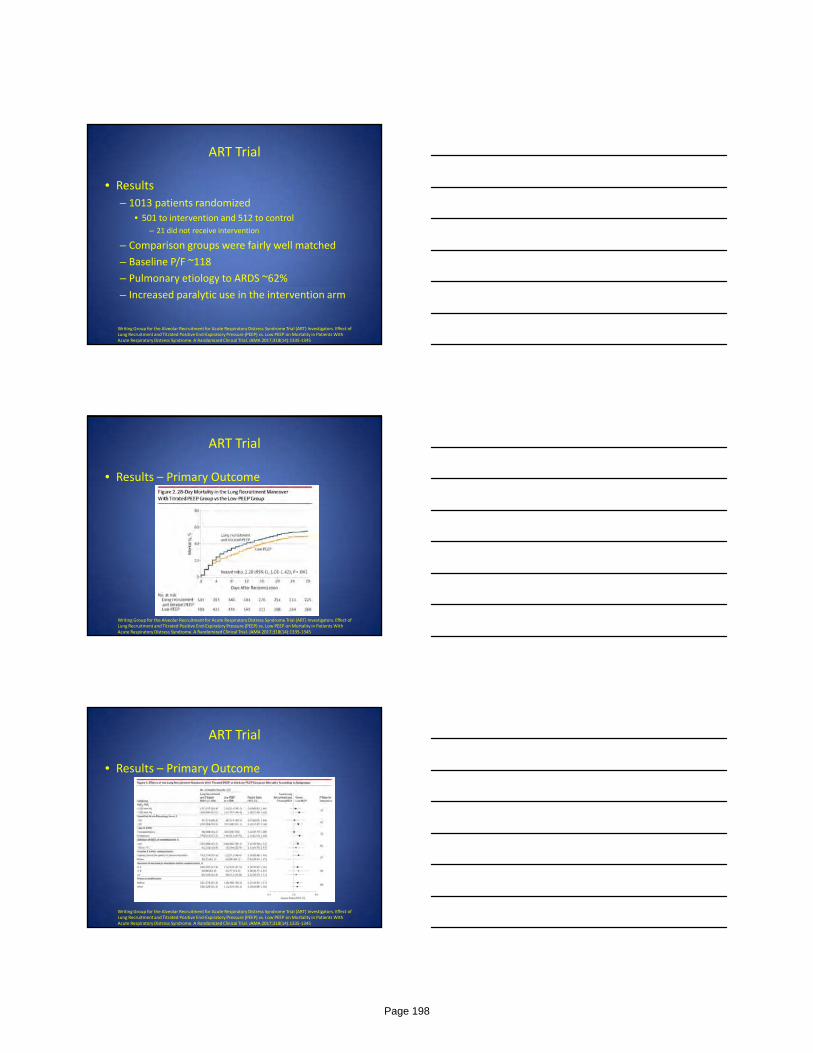
ART Trial
• Results
– 1013 patients randomized
• 501 to intervention and 512 to control– 21 did not receive intervention
– Comparison groups were fairly well matched
– Baseline P/F ~118
– Pulmonary etiology to ARDS ~62%
– Increased paralytic use in the intervention arm
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
ART Trial
• Results – Primary Outcome
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
ART Trial
• Results – Primary Outcome
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
Page 198
ART Trial
• Strengths– Multicenter randomized design
– Minimal loss to follow up
– Protocol adherence
• Weaknesses– Lack of blinding
– Length of ICU stay was not included in the original study protocol but was then added in the statistical analysis plan
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
ART Trial
• Discussion
– Applicability to our ICUs
• Local differences in care delivery and practices
• Higher mortality seen in both arms compared to similar ARDS studies
– Heterogeneity of ARDS
• Still possible that some ARDS subgroups are more likely to benefit with recruitment maneuver
Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of Lung Recruitment and Titrated Positive End‐Expiratory Pressure (PEEP) vs. Low PEEP on Mortality in Patients With Acute Respiratory Distress Syndrome. A Randomized Clinical Trial. JAMA 2017;318(14):1335‐1345
Study 3
Page 199
ADRENAL Trial
• Clinical question– In critically ill patients with septic shock, does hydrocortisone result in a lower mortality?
• Design– Randomized double blinded placebo controlled trial– Intervention was an infusion of 200mg hydrocortisone per day
– Primary outcome was death from any cause at 90 days after randomization
– 69 medical surgical ICUs across Australia, UK, New Zealand, Saudi Arabia and Denmark
– March 2013 – April 2017
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
ADRENAL Trial
• Inclusion– Adults with septic shock requiring vasopressors and mechanical ventilation
• Exclusion– Likely to receive systemic glucocorticoiods for another indication
– Had received Etomidate or Amphotericin B
– Likely to die from a preexisting disease within 90 days after randomization
– Met all inclusion criteria for more than 24 hours
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
ADRENAL Trial
• Results
– 21,818 patients screened
– 3658 were included in 90 day analysis
• 1832 to hydrocortisone and 1826 to placebo
– Baseline characteristics were evenly matched
• Approximately one third of patients in each group were surgical admissions
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
Page 200
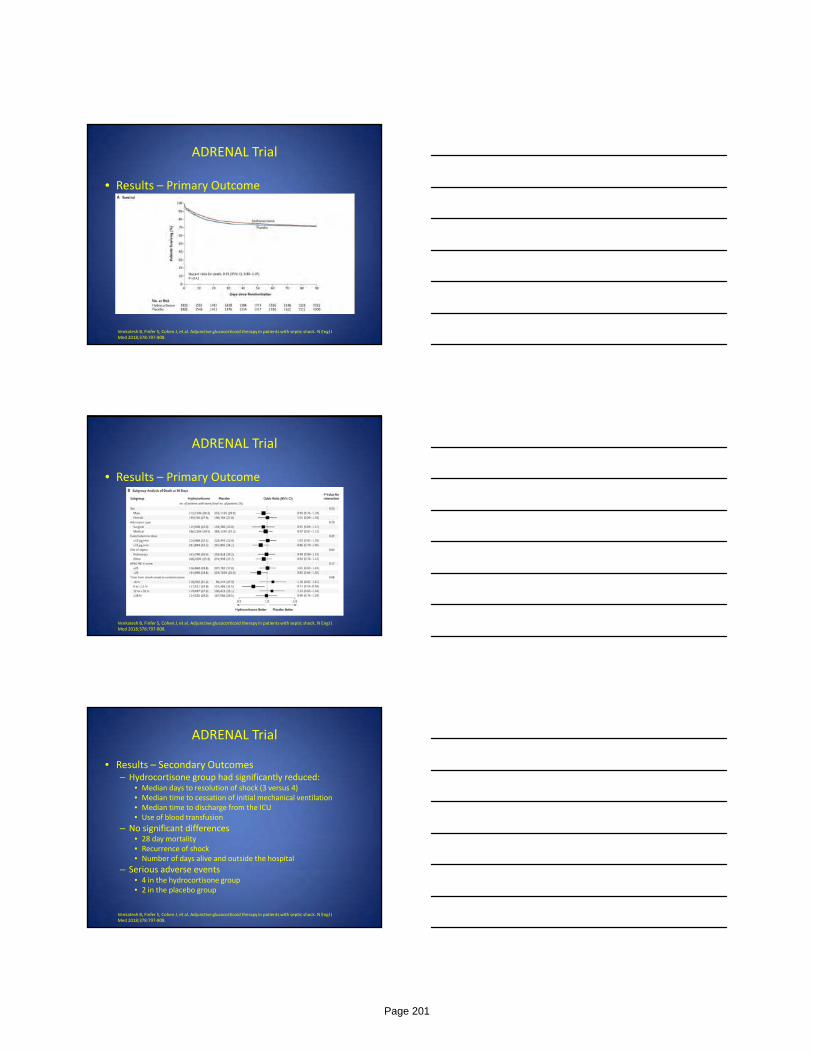
ADRENAL Trial
• Results – Primary Outcome
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
ADRENAL Trial
• Results – Primary Outcome
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
ADRENAL Trial
• Results – Secondary Outcomes– Hydrocortisone group had significantly reduced:
• Median days to resolution of shock (3 versus 4)• Median time to cessation of initial mechanical ventilation• Median time to discharge from the ICU• Use of blood transfusion
– No significant differences• 28 day mortality• Recurrence of shock• Number of days alive and outside the hospital
– Serious adverse events• 4 in the hydrocortisone group• 2 in the placebo group
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
Page 201
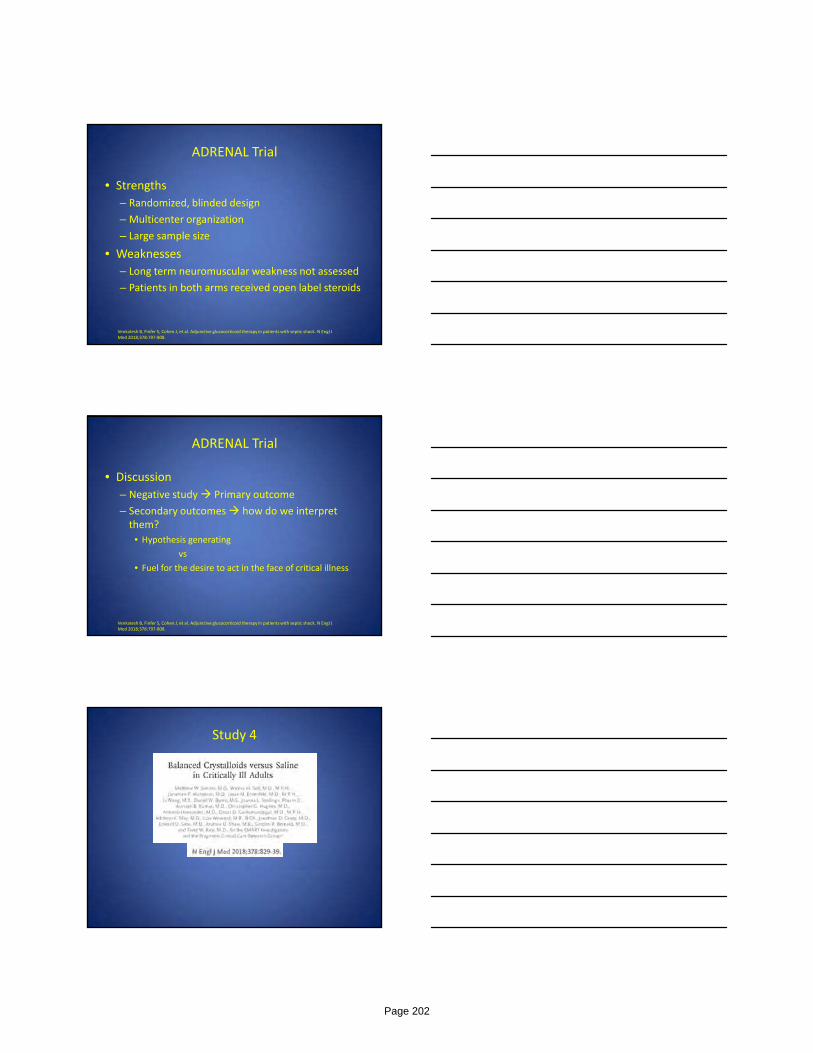
ADRENAL Trial
• Strengths
– Randomized, blinded design
– Multicenter organization
– Large sample size
• Weaknesses
– Long term neuromuscular weakness not assessed
– Patients in both arms received open label steroids
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
ADRENAL Trial
• Discussion
– Negative study Primary outcome
– Secondary outcomes how do we interpret them?
• Hypothesis generating
vs
• Fuel for the desire to act in the face of critical illness
Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med 2018;378:797‐808.
Study 4
Page 202
SMART Trial
• Clinical Question
– In critically ill patients, does the use of balanced crystalloids compared with saline reduce a 30 day composite outcome of death, new renal replacement therapy or persistent renal dysfunction?
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
SMART Trial
• Design– Unblinded, cluster randomized– Five ICUs at Vanderbilt University Medical Center– 0.9% sodium chloride vs lactated Ringer’s or Plasma‐Lyte A– Primary outcome was the proportion of patients who met one or more criteria for a major adverse kidney event within 30 days or at hospital discharge
• Death, new receipt of RRT, persistent renal dysfunction
• Inclusion criteria– All adult patients admitted to the ICU
• Exclusion criteria– Age less than 18
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
SMART Trial
• Results
– 15,802 patients enrolled
• 7942 to balanced crystalloid and 7860 to saline
– Median age was 58
– Mechanical ventilation ~34%
– Vasopressors ~26%
– Sepsis or septic shock ~15%
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
Page 203

SMART Trial
• Results – Primary Outcome
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
SMART Trial
• Results – Primary Outcome
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
SMART Trial
• Results – Secondary Outcomes– Death before discharge or at day 30
• 10.3% vs 11.1% (p=0.06)
– Receipt of new RRT• 2.5% vs 2.9% (p=0.08)
– Persistent renal dysfunction• 6.4% vs 6.6%
– No difference in ICU free days, ventilator free days, vasopressor free days, Stage 2 (or higher) AKI developing after enrollment
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
Page 204
SMART Trial
• Strengths
– Large sample size
– Mixed patient population
– Successful allocation of fluids
• Weaknesses
– Single center
– Lack of blinding
– Patients remaining in the ICU at the end of 30 days may have been exposed to both types of crystalloids
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
SMART Trial
• Discussion
– Saline for hyperkalemia – diminished observed difference in primary outcome?
– Composite outcome – applicability to other trials and understanding the definitions used to guide outcomes
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med 2018; 378:829‐39.
Thank You
Page 205
Neurocritical care year review CEDERIC PIMENTEL, MD
ASSISTANT PROFESSOR NEUROLOGY & NEUROSURGERY
EMORY NEUROCRITICAL CARE
Disclosures
No conflicts to disclose
Objectives
• Ischemic stroke• Quick overview
• 2018 guidelines (new recommendations)
• PFO closure vs medical management
• Hemorrhagic stroke• Quick review in management
Page 206

Acute ischemic stroke (AIS)
1 every 40 secs 780,000 strokes/year 3rd leading cause of death Leading cause of long term disability Stroke
Ischemic 80% Hemorrhagic 10-15% “Mimics” 3%
hypoglycemia, migraine, sz, tumor/abscess, WNV, Wernicke’s, trauma/contusion
Rosamond W. et Al. Heart disease and stroke statistics—2008 update. Circulation.2008;117(4):e25-e46
Jauch EC, et al. Stroke 2013;44:870-946
Diagnosis
Clinical Key history : LKN, trauma/surgeries, Meds: AC, anti HTN, anti convulsant, DM rx
Physical : NIHSS, cardiac exam/pulses, signs of liver disease, coagulopathy
NIH Stroke Scale Score Total range
Level of consciousness
0-3 0-42
Orientation 0-2Follows commands 0-2Gaze 0-2Visual Fields 0-3Facial Movement 0-3Motor Function (arm) 0-4Motor Function (leg) 0-4Limb Ataxia 0-2Sensory 0-2Language 0-3Articulation 0-2Extinction/Inattention 0-2
• Reliability + sensitivity• Anterior circulation
Jauch EC, et al. Stroke 2013; 44: 870-947Kasner SE. Clinical interpretation and use of stroke scales. Lancet Neurol.2005;5(7):603-612
Page 207
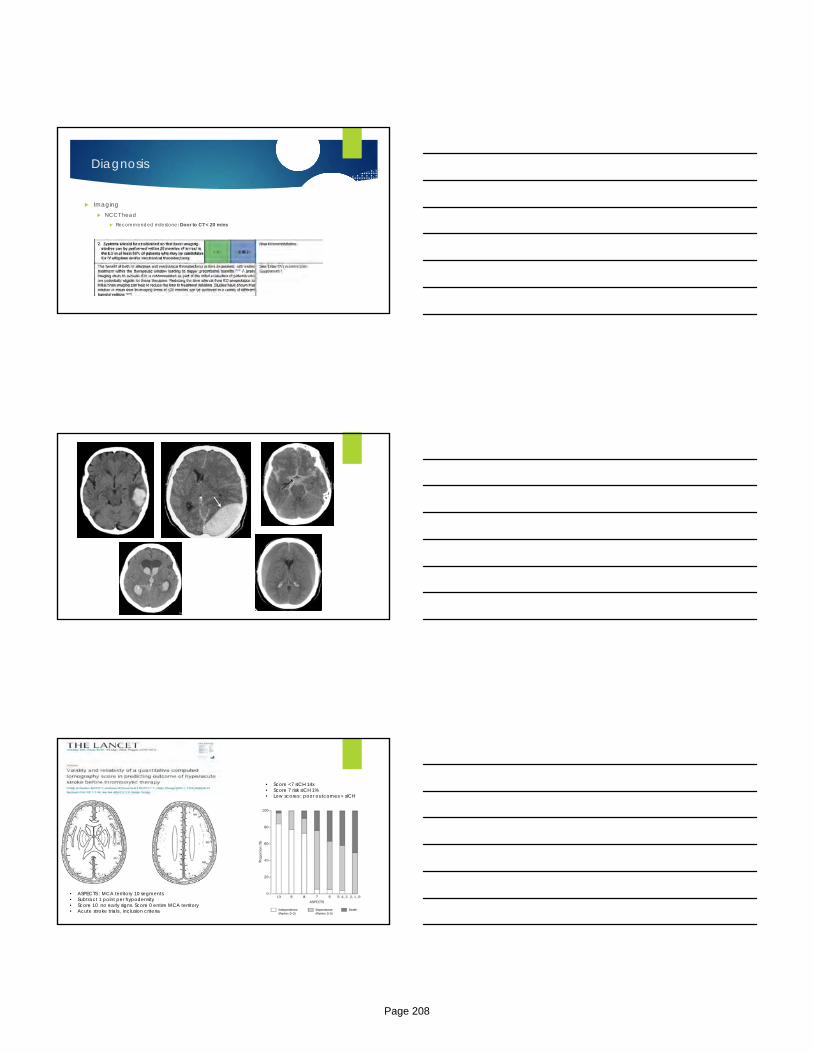
Diagnosis
Imaging NCCT head
Recommended milestone: Door to CT < 20 mins
• ASPECTS : MCA territory 10 segments• Subtract 1 point per hypodensity• Score 10 no early signs. Score 0 entire MCA territory• Acute stroke trials , inclusion criteria
• Score <7 sICH 14x • Score 7 risk sICH 1%• Low scores : poor outcomes + sICH
Page 208

Hyperdense sign• Indicator thromboembolism• Early sign : HCT elevation• Sp 90-100%• Assoc/ poor clinical outcome
Gacs G, et al. Stroke.1983;14:756-762Abdul-Kasim K, Acta Neurol Scand. 2010; 122:132-139Aries MJ.J Neurol Sci 2009;285:114-117
Diagnosis
Imaging CTA/CT perfusion
LVO = large hemispheric infarct
Tissue at risk (ischemia)
3 parameters : CBV, CBF, MTT
Penumbra: Early HD failure. CBV elevated, CBF normal
Infarct (Core) : very low CBV
MTT adjunct ( caution : asymmetry w/o penumbra or symmetry w/ penumbra)
Page 209
Treatment
Treatment
• Updates to 2013 guidelines• “early window” and “extended window” Tx• 6 RCT early and 2 RCT extended window
Page 210
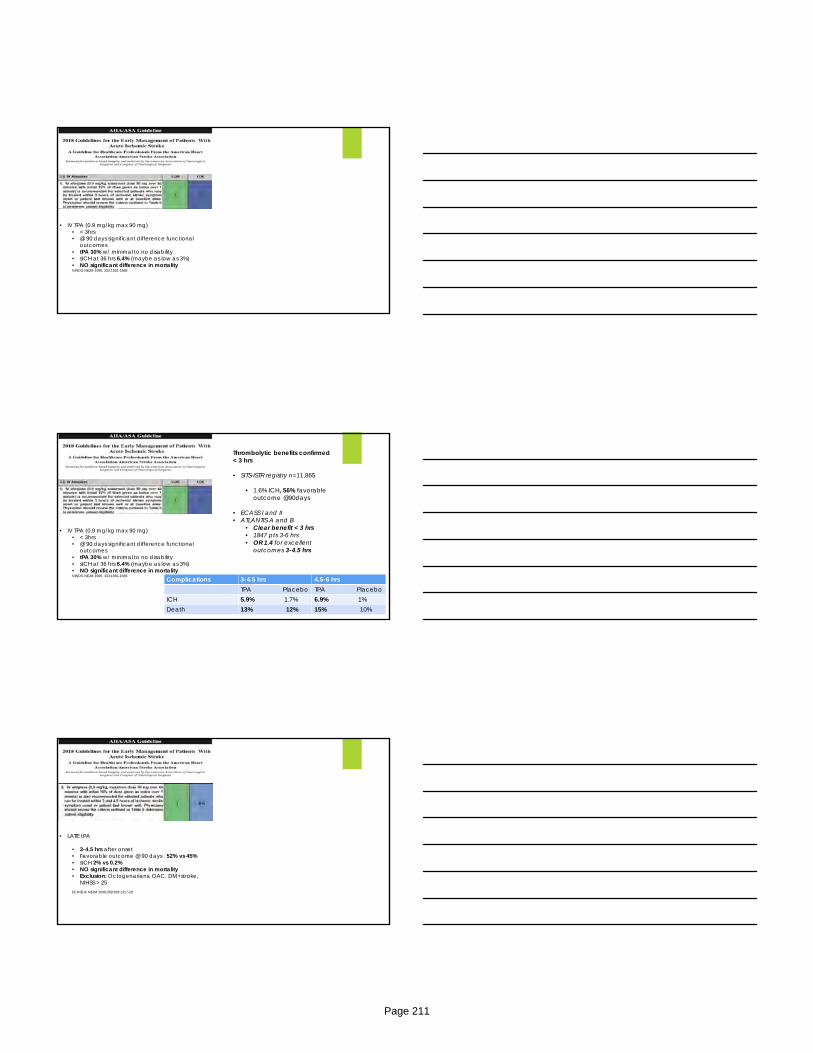
• IV TPA (0.9 mg/kg max 90 mg)• < 3hrs• @ 90 days significant difference functional
outcomes• tPA 30% w/ minimal to no disability• sICH at 36 hrs 6.4% (maybe as low as 3%)• NO significant difference in mortalityNINDS. NEJM 1995; 333:1581-1588
• IV TPA (0.9 mg/kg max 90 mg)• < 3hrs• @ 90 days significant difference functional
outcomes• tPA 30% w/ minimal to no disability• sICH at 36 hrs 6.4% (maybe as low as 3%)• NO significant difference in mortalityNINDS. NEJM 1995; 333:1581-1588
Thrombolytic benefits confirmed< 3 hrs
• SITS-ISTR registry n=11,865
• 1.6% ICH, 56% favorable outcome @90days
• ECASS I and II• ATLANTIS A and B
• Clear benefit < 3 hrs• 1847 pts 3-6 hrs• OR 1.4 for excellent
outcomes 3-4.5 hrs
Complications 3-4.5 hrs 4.5-6 hrsTPA Placebo TPA Placebo
ICH 5.9% 1.7% 6.9% 1%Death 13% 12% 15% 10%
• LATE tPA
• 3-4.5 hrs after onset• Favorable outcome @ 90 days : 52% vs 45%• sICH 2% vs 0.2%• NO significant difference in mortality• Exclusion: Octogenarians, OAC, DM+stroke,
NIHSS > 25ECASS III. NEJM 2008;359;359:1317-29
Page 211
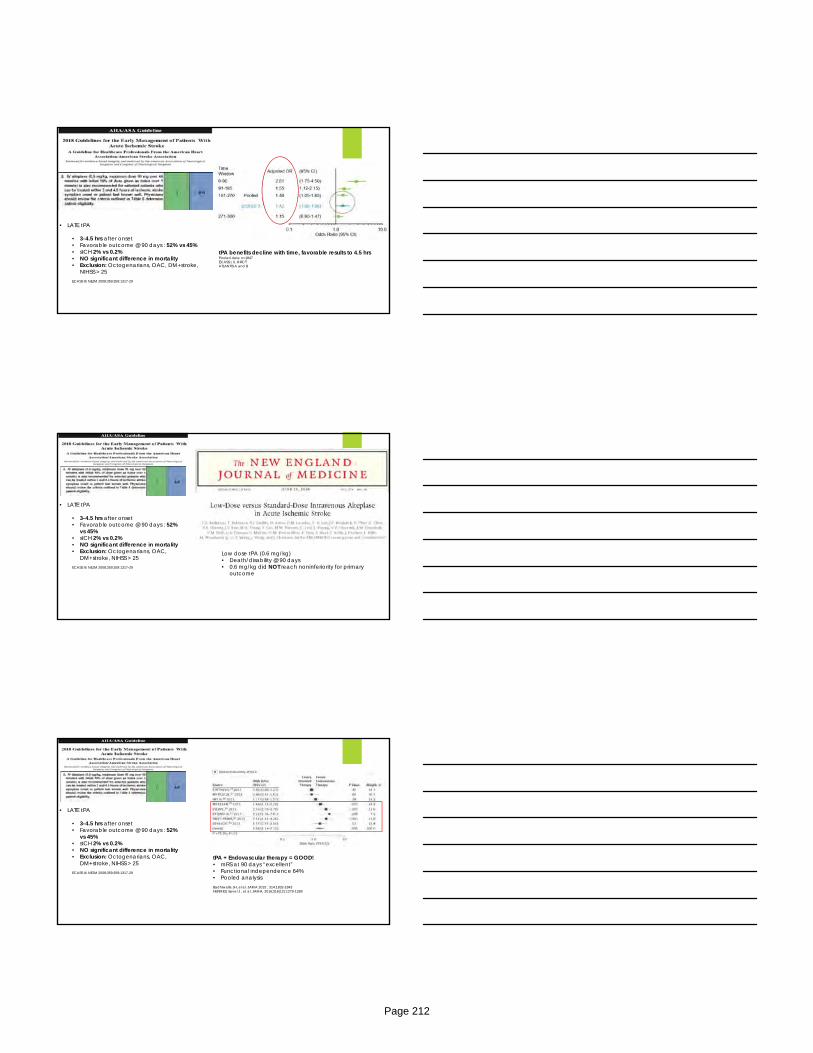
• LATE tPA
• 3-4.5 hrs after onset• Favorable outcome @ 90 days : 52% vs 45%• sICH 2% vs 0.2%• NO significant difference in mortality• Exclusion: Octogenarians, OAC, DM+stroke,
NIHSS > 25ECASS III. NEJM 2008;359;359:1317-29
tPA benefits decline with time, favorable results to 4.5 hrsPooled date n=1847ECASS I, II, III RCTATLANTIS A and B
• LATE tPA
• 3-4.5 hrs after onset• Favorable outcome @ 90 days : 52%
vs 45%• sICH 2% vs 0.2%• NO significant difference in mortality• Exclusion: Octogenarians, OAC,
DM+stroke, NIHSS > 25ECASS III. NEJM 2008;359;359:1317-29
Low dose tPA (0.6 mg/kg)• Death/disability @ 90 days• 0.6 mg/kg did NOT reach noninferiority for primary
outcome
• LATE tPA
• 3-4.5 hrs after onset• Favorable outcome @ 90 days : 52%
vs 45%• sICH 2% vs 0.2%• NO significant difference in mortality• Exclusion: Octogenarians, OAC,
DM+stroke, NIHSS > 25ECASS III. NEJM 2008;359;359:1317-29
tPA + Endovascular therapy = GOOD!• mRS at 90 days “excellent”• Functional independence 64%• Pooled analysisBadhiwalla JH, el al. JAMA 2015 ; 314:1832-1843HERMES. Saver J , et al. JAMA. 2016;316(12):1279-1289
Page 212
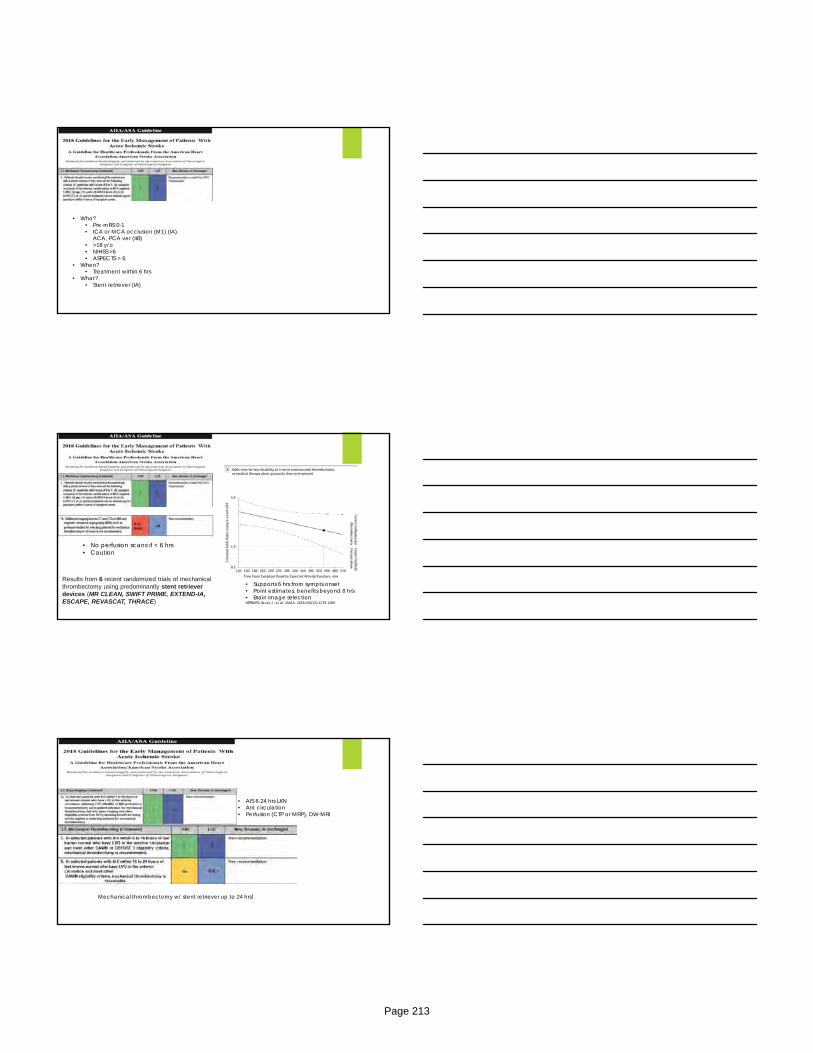
• Who?• Pre-mRS 0-1• ICA or MCA occlusion (M1) (IA).
ACA, PCA ver (IIB)• >18 y/o• NIHSS >6• ASPECTS > 6
• When?• Treatment within 6 hrs
• What?• Stent retriever (IA)
• Supports 6 hrs from sympts onset• Point estimates, benefits beyond 8 hrs• Brain image selectionHERMES. Saver J , et al. JAMA. 2016;316(12):1279-1289
Results from 6 recent randomized trials of mechanical thrombectomy using predominantly stent retriever devices (MR CLEAN, SWIFT PRIME, EXTEND-IA, ESCAPE, REVASCAT, THRACE)
• No perfusion scans if < 6 hrs• Caution
• AIS 6-24 hrs LKN• Ant circulation• Perfusion (CTP or MRP), DW-MRI
Mechanical thrombectomy w/ stent retriever up to 24 hrs!
Page 213

N Engl J Med 2018; 378:11-21DOI: 10.1056/NEJMoa1706442
• Thrombectomy vs standard• N=206• ICA/ Prox MCA, LKN 6-24 hrs• Clinico-radiographic mismatch• mRS 0-2 49% vs 13%• NNT 2• NO diff in sICH and mortality
• Thrombectomy vs standard• N=182• ICA/ Prox MCA, LKN 6-16 hrs• Perfusion/volumetric
• Infarct volume < 70 ml• Ratio ischemia:infarct >1.8• Reversible ischemia 15 ml
• mRS 0-2 45% vs 17%• 90 day mortality 14% vs 25%• NO diff in sICH
N Engl J Med 2018; 378:708-718DOI: 10.1056/NEJMoa1713973
Recommended treatments
ASA w/o tPA -> w/in 24-48 hrs W/ tPA -> After 24 hrs
BP Leave alone unless:
Before tPA < 185/110 mmHg After tPA < 180/105 mmHg EVT SBP < 140 (DAWN) Comorbidities (e.g HF, ACS, Aortic dissection, pre/eclampsia) : 15 % reduction safe
Avoid hypotension/hypovolemia Avoid fever
Page 214
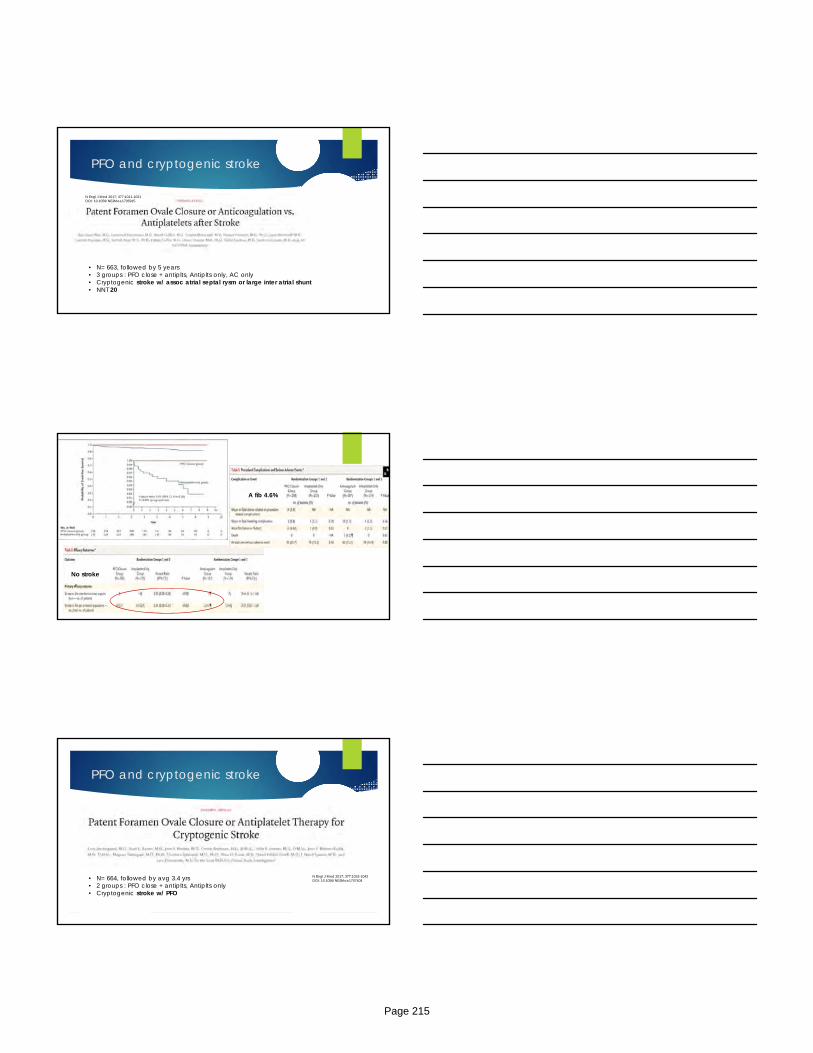
PFO and cryptogenic stroke
N Engl J Med 2017; 377:1011-1021DOI: 10.1056/NEJMoa1705915
• N= 663, followed by 5 years• 3 groups : PFO close + antiplts, Antiplts only, AC only• Cryptogenic stroke w/ assoc atrial septal rysm or large inter atrial shunt• NNT 20
A fib 4.6%
No stroke
PFO and cryptogenic stroke
N Engl J Med 2017; 377:1033-1042DOI: 10.1056/NEJMoa1707404• N= 664, followed by avg 3.4 yrs
• 2 groups : PFO close + antiplts, Antiplts only• Cryptogenic stroke w/ PFO
Page 215
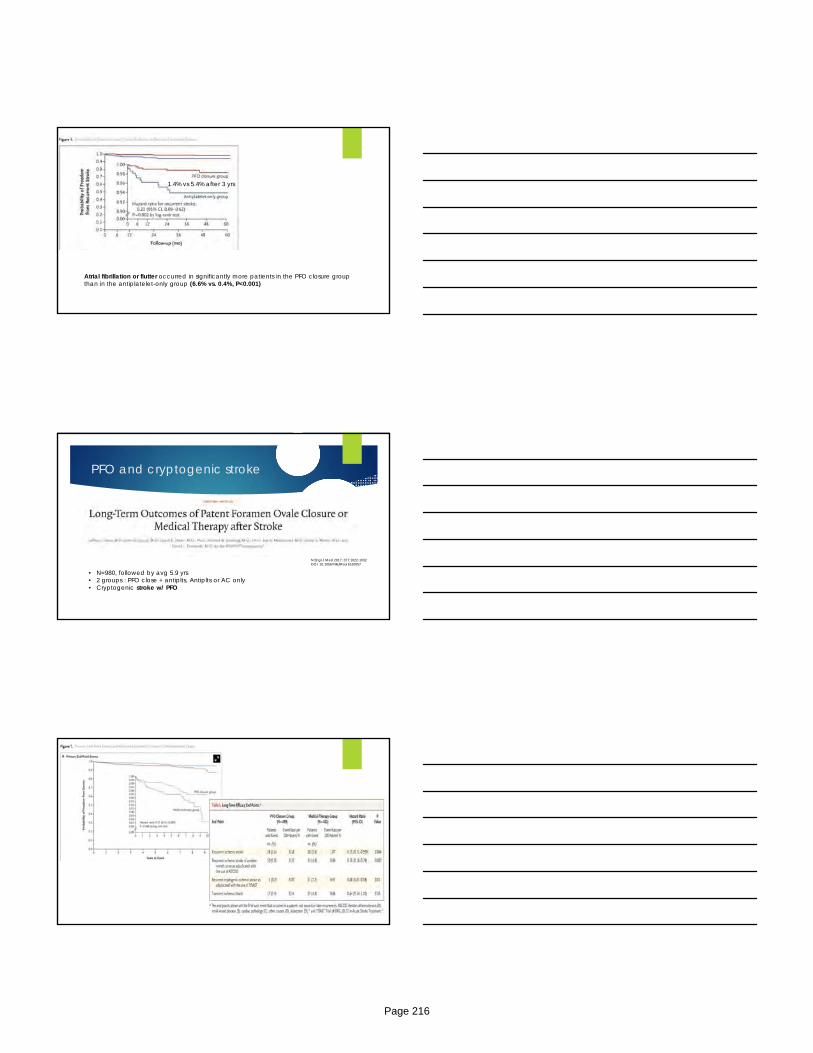
1.4% vs 5.4% after 3 yrs
Atrial fibrillation or flutter occurred in significantly more patients in the PFO closure group than in the antiplatelet-only group (6.6% vs. 0.4%, P<0.001)
PFO and cryptogenic stroke
• N=980, followed by avg 5.9 yrs• 2 groups : PFO close + antiplts, Antiplts or AC only• Cryptogenic stroke w/ PFO
N Engl J Med 2017; 377:1022-1032DOI: 10.1056/NEJMoa1610057
Page 216

PFO AHA/ASA 2014 guidelines
Hemorrhagic stroke
Risk factors HTN : important + prevalent. (Lipohyalinosis)
Non modifiable risks : Age, Males, Race
CAA : 1ary ICH elderly (B amyloid small and medium size vessels)
Other: OAC, drugs (cocaine, alcohol abuse), low cholesterol
Xiang W, et. al. Cholesterol and risk of hemorrhagic stroke. Stroke.2013;44:1833-1839Golstein LB, et al. Neurology2008;70:2364-2370
Hemorrhagic stroke
Initial treatment NICU admission
ICP monitoring : GCS < 8 , HCP, IVH, clinical herniation . Keep CPP 50-70 mmHg
Control BP, BG, Sz . Avoid fever
Correct coagulopathy 4 factor PCC faster with lower volume compared to VKA+FFP (Chest : 2C suggestion
PCC)
No diff in outcomes!
Hemphill JC, et al. Stroke 2015;46:2032-2060Holbrook A, et al. Chest 2012:141:e152s-84s
Page 217
Hemorrhagic stroke
1. Anderson CS, Stroke 2010;41:307-3122. Anderson CS, NEJM 2013;368:2355-23653. Qureshi Al, Arch Neuro l 2010:67:570-5764. Qureshi Al, NEJM 2016:1033-1043
Trial n Intervention Outcomes
INTERACT (1) 404 SBP <140 vs <180 • Safe• Less hematoma
expansion
INTERACT II (2) 2839 SBP < 140 vs <180 • No difference mortality/disability
• 2ary analysis “mild ICH”
ATACH (3) 60
ATACH II (4) 1000
Hemorrhagic stroke
1. Anderson CS, Stroke 2010;41:307-3122. Anderson CS, NEJM 2013;368:2355-23653. Qureshi Al, Arch Neuro l 2010:67:570-5764. Qureshi Al, NEJM 2016:1033-1043
Trial n Intervention Outcomes
INTERACT (1) 404 SBP <140 vs <180 • Safe• Less hematoma expansion
INTERACT II (2) 2839 SBP < 140 vs <180 • No diff mortality/disability• 2ary analysis “mild ICH”
ATACH (3) 60 SBP <140 vs <170 vs <200
• SAE and Neuro deterioration
• Below safety threshold
• Mortality decreased
ATACH II (4) 1000
Hemorrhagic stroke
1. Anderson CS, Stroke 2010;41:307-3122. Anderson CS, NEJM 2013;368:2355-23653. Qureshi Al, Arch Neuro l 2010:67:570-5764. Qureshi Al, NEJM 2016:1033-1043
Trial n Intervention Outcomes
INTERACT (1) 404 SBP <140 vs <180 • Safe• Less hematoma expansion
INTERACT II (2) 2839 SBP < 140 vs <180 • No diff mortality/disability• 2ary analysis “mild ICH”
ATACH (3) 60 SBP <140 vs <170 vs <200 • SAE and Neuro deterioration• Below safety threshold• Mortality decreased
ATACH II (4) 1000 SBP <140 vs <180 • No diff mortality/disability
• Less hematoma expansion19% vs 24% (p=0.09)
• Renal SAE (9 vs 4%)
Page 218
Hemorrhagic stroke
SBP to 140 mmHg is safe and improve functional outcome (IIa-B)
Hemorrhagic stroke
Please DO VTE ppx
Safe and effective after 48 hrs
Avoid Hypo/hyperglycemia
Please DON’T Hypothermia Anticonvulsants
10-30% seizure risk = worse outcomes Prophylactic AED’S = no benefits
Steroids Platelet transfusion for ASA reversal
Increased mortality/SAE PATCH Baharoglu MI, et al. Lancet 2016; 387:2605-2016Hemphill JC, et al. Stroke 2015; 46:2032-2060
Hemorrhagic stroke
Hematoma expansion Early neurologic deterioration (1,2)
Volume predictor of outcome (1,2)
CTA after ICH Active extravasation leading hematoma expansion (3)
Increased mortality (4)
1. Mayer SA. Ultraeraly hemostatic therapy for ICH. Stroke.2003;34(1):224-2292. Gebel JM Jr et Al. Relative edema volume is a predictor of outcome in patients with hyper acute spontaneous ICH. Stroke.2002;33(11):2636-
26413. Murai Y, Takagi R. et Al. 3-D CTA in patients with hyperacute ICH. J Neurosurg 1994;91(3):424-4314. Becker KJ, Baxter AB. Extravasation of radiographic contrast is an independent predictor of death in primary ICH. Stroke. 1999;30(10):2025-2032
Page 219
Sensitivity 91%NPV 96%
Hemorrhagic stroke
High risk patients (spot sign) STOP-IT/SPOTLIGHT (Flaherty ML, et al. ISC 2017)
“spot sign” predicts hematoma expansion
No benefits rFVII
VKA related ICH 4F –PCC vs FFP (Steiner T. INCH trial. Lancet 2016 May;15(6):566-73)
Dabigatran
N Engl J Med 2017; 377:431-441
Page 220
Surgical and Burn Critical Care Year in Review
2018 Southeastern Critical Care Summit
Atlanta, GA
May 11, 2018
Omar K. Danner, MD, FACS
Chief of Surgery
MSM Department of Surgery
Rib fracture fixation for flail chest: what is the benefit?J Am Coll Surg. 2012 Aug;215(2):201‐5. doi: 10.1016/j.jamcollsurg.2012.02.023.
Epub 2012 May 4.Bhatnagar A1, Mayberry J, Nirula R.
BACKGROUND:
Recently, rib fracture fixation for flail chest has been used increasingly at both academic and nonacademic trauma centers. Although a few small non‐US studies have demonstrated a clinical benefit, it was unclear whether this benefit outweighed the added expense and potential perioperative complications related to the procedure. Therefore, a study was performed to determine if open reduction and internal fixation of ribs for flail chest (ORIF‐FC) provided a cost‐effective means for managing these patients.
STUDY DESIGN:
Medicare 2010 reimbursement costs were used for diagnoses and procedures. A quality of life improvement factor ranging from 0 to 15% improvement was used to estimate the improvement in pain and functional outcomes related to ORIF‐FC. The most cost‐effective treatment was then determined, ranging the incidences of ventilator‐associated pneumonia and quality of life improvement factor.
RESULTS:
Cost effectiveness was $15,269 for ORIF‐FC compared with $16,810 for standard of care. Even when the quality of life improvement factor was set to 0%, rib fixation remained the most cost‐effective strategy. Similarly, rib fixation was the most cost‐effective strategy by $8,400 even though the incidence of ventilator‐associated pneumonia after the procedure was as high as 22%.
CONCLUSIONS:
Despite the additional cost of surgery, rib fracture fixation was deemed the standard of care, particularly in the management of appropriate flail chest patients based on these study findings.
Operative management versus non‐operative management of rib fracturesin flail chest injuries: a systematic review.
Eur J Trauma Emerg Surg. 2017 Apr;43(2):163‐168. doi: 10.1007/s00068‐016‐0721‐2. Epub 2016 Aug 29.Schuurmans J1, Goslings JC2, Schepers T2.
PURPOSE:
Flail chest is a life‐threatening complication of severe chest trauma with a mortality rate of up to 15%. Standard non‐operative management has high comorbidities with pneumonia and often leads to extended ICU stay, due to insufficient respiratory function and complications.
METHODS:
Randomized‐controlled trials comparing operative management versus non‐operative management of flail chest were evaluated in this systematic review and meta‐analysis. PubMed, Trip Database, and Google Scholar were used for the study . Mean difference and risk ratio for mortality, pneumonia rate, duration of mechanical ventilation, duration of ICU stay, duration of hospital stay, tracheostomy rate, and treatment costs were calculated by pooling these publication results.
RESULTS:
Three randomized‐controlled trials were included in this systematic review. In total, 61 patients received operative management compared to 62 patients in the non‐operative group. A positive effect of surgical rib fracture fixation was observed for pneumonia rate [ES 0.5, 95 % CI (0.3, 0.7)], days of mechanical ventilation (DMV) [ES ‐6.5 days 95 % CI (‐11.9, ‐1.2)], ICU LOS [ES ‐5.2 days 95 % CI (‐6.2, ‐4.2)], hospital LOS [ES ‐11.4 days 95 % CI (‐12.4, ‐10.4)], tracheostomy rate (TRCH) [ES 0.4, 95 % CI (0.2, 0.7)], and treatment costs (saving $9.968,00‐14.443,00 per patient). There was no significant difference was noted in mortality rate [ES 0.6, 95 % CI (0.1, 2.4)] between the two groups.
CONCLUSIONS:
Despite the relatively small number of patients included, different methodologies and differences in presentation of outcomes, operative management of flail chest using rib fixation still appears to be a promising treatment strategy that improves patients' outcomes in various ways. However, a clear mortality reduction benefit remains inconclusive.
Page 222
Resuscitative endovascular balloon occlusion of the aorta for control of non‐compressible truncal hemorrhage in the abdomen and pelvis.
Am J Surg. 2016 Dec;212(6):1222‐1230. doi: 10.1016/j.amjsurg.2016.09.027. Epub 2016 Sep 30.Moore LJ1, Martin CD2, Harvin JA3, Wade CE3, Holcomb JB3.
BACKGROUND:
Non-compressible truncal hemorrhage is a leading cause of potentially preventable death in trauma and acute care surgery patients. These patients are at high risk of exsanguination before potentially life-saving surgical intervention may be performed. Temporary aortic occlusion is an effective means of augmenting systolic blood pressure and perfusion of the heart and brain in these patients. The traditional method for temporary aortic occlusion is via resuscitative thoracotomy with cross clamping of the descending aorta. Resuscitative endovascular balloon occlusion of the aorta (REBOA) has been used to achieve temporary aortic occlusion. The purpose of this study was to describe the experience with the implementation of REBOA at our Level 1 trauma center.
METHODS:
A retrospective case series describing all cases of REBOA performed at a prominent level 1 trauma center between October 2011 and September 2015. The study inclusion criteria were any patient that received a REBOA procedure in the acute phases after injury. There were no exclusion criteria. Data were collected from electronic medical records and the hospital's trauma registry.
RESULTS:
A total of 31 patients underwent REBOA during the study period. The majority (87%) of patients had sustained blunt trauma. The median injury severity score was 34 (IQR = 22 to 42). The overall survival rate was 32% but varied greatly between subgroups. Balloon inflation resulted in a median increase in systolic blood pressure of 55-mm Hg (IQR 33 to 60), in cases where the data were available (n = 20). A return to spontaneous circulation was noted in 60% of patients who had arrested before REBOA (n = 10). Overall, early death by hemorrhage was 28% with only 2 deaths in the emergency department before reaching the operating room.
CONCLUSIONS:
REBOA was found to be an effective method for achieving temporary aortic occlusion in trauma patients with non-compressible truncal hemorrhage with increased blood pressure and temporary hemorrhage control in the majority of patients.
The AAST prospective Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry: Data on contemporary utilization and outcomes of aortic occlusion and
resuscitative balloon occlusion of the aorta (REBOA).J Trauma Acute Care Surg. 2016 Sep;81(3):409‐19. doi: 10.1097/TA.0000000000001079.
DuBose JJ1, Scalea TM, Brenner M, Skiada D, Inaba K, Cannon J, Moore L, Holcomb J, Turay D, ArbabiCN, Kirkpatrick A, Xiao J, Skarupa D, Poulin N; AAST AORTA Study Group.
INTRODUCTION:
Aortic occlusion (AO) for resuscitation in traumatic shock remains controversial. Resuscitative endovascular balloon occlusion of the aorta (REBOA) offers an emerging alternative.
METHODS:
The American Association for the Surgery of Trauma Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery working group prospectively looked at trauma patients requiring AO from eight ACS Level 1 centers from November 2013 to February 2015.
RESULTS:
They reviewed 114 AO patients (REBOA, 46; open AO, 68); 80.7% were male, and 62.3% were blunt injured. Aortic occlusion occurred in the emergency department (73.7%) or the operating room (26.3%). Hemodynamic improvement after AO was observed in 62.3% [REBOA, 67.4% versus open OA, 61.8%); 36.0% achieving stability (systolic blood pressure consistently >90 mm Hg, >5 minutes); REBOA, (47.8%) versus open OA, (27.9%); p =0.014]. Deployment was achieved in Zones I (78.6%) and III (19.0%). Overall survival was 21.1% (24 of 114), with no significant difference between REBOA and open AO with regard to mortality [REBOA, 28.2% (13 of 46); open OA, 16.1% (11 of 68); p = 0.120].
CONCLUSION:
Resuscitative endovascular balloon occlusion of the aorta has emerged as a viable alternative to open AO in centers that have developed this capability.
A meta‐analysis of resuscitative endovascular balloon occlusion of the aorta (REBOA) or open aortic cross‐clamping by resuscitative thoracotomy in non‐compressible torso hemorrhage patients.World J Emerg Surg. 2017 Jul 14;12:30. doi: 10.1186/s13017‐017‐0142‐5. eCollection 2017.
Manzano Nunez R1, Naranjo MP1, Foianini E2, Ferrada P3, Rincon E1, García‐Perdomo HA4, BurbanoP5, Herrera JP6, García AF4,7, Ordoñez CA4,7.
BACKGROUND:
A systematic review and meta‐analysis was performed to determine the effect of resuscitative endovascular balloon occlusion of the aorta (REBOA), compared to resuscitative thoracotomy, on mortality among non‐compressible torso hemorrhage trauma patients.
METHODS:
Relevant articles were identified by a literature search in MEDLINE and EMBASE. We included studies involving trauma patients suffering non‐compressible torso hemorrhage. Studies were eligible if they evaluated REBOA and compared it to resuscitative thoracotomy. Two investigators independently assessed articles for inclusion and exclusion criteria and selected studies for final analysis. Random effect models was used to conduct the meta‐analysis.
RESULTS:
Three studies were included in the systematic review. There was a total of 1276 patients. Initial analysis found that the odds of mortality did not differ between the compared groups (OR 0.42; 95% CI 0.17‐1.03), although lower in REBOA‐treated patients. Sensitivity analysis showed that the risk of mortality was significantly lower among patients who underwent REBOA, compared to resuscitative thoracotomy (RT) (RR 0.81; 95% CI 0.68‐0.97).
CONCLUSION:
This meta‐analysis suggests a positive effect of REBOA on mortality among non‐compressible torso hemorrhage patients.
Page 223
Resuscitative Endovascular Balloon Occlusion of the Aorta and Resuscitative Thoracotomy in Select Patients with Hemorrhagic Shock: Early Results from the American Association for the Surgery of
Trauma Aortic Occlusion in Resuscitation for Trauma and Acute Care Surgery Registry.J Am Coll Surg. 2018 Feb 6. pii: S1072‐7515(18)30098‐X. doi: 10.1016/j.jamcollsurg.2018.01.044
Brenner M1, Inaba K2, Aiolfi A2, DuBose J3, Fabian T4, Bee T4, Holcomb JB5, Moore L5, Skarupa D6, Scalea TM3; AAST AORTA Study Group.
BACKGROUND:
Aortic occlusion is a potentially valuable tool for early resuscitation in patients nearing extremis or in arrest from severe hemorrhage.
STUDY DESIGN:
The American Association for the Surgery of Trauma and Aortic Occlusion in Resuscitation for Trauma and Acute Care Surgery registry identified trauma patients without penetrating thoracic injury undergoing aortic occlusion at the level of the descending thoracic aorta (resuscitative thoracotomy [RT] or zone 1 resuscitative endovascular balloon occlusion of the aorta [REBOA]) in the emergency department (ED). Survival outcomes relative to the timing of CPR need and admission hemodynamic status were examined.
RESULTS:
Two hundred and eighty-five patients were included: 81.8% were males, with injury due to penetrating mechanisms in 41.4%; median age was 35.0 years (interquartile range 29 years) and median Injury Severity Score was 34.0 (interquartile range 18). Resuscitative thoracotomy was used in 71%, and zone 1 REBOA in 29%. Overall survival beyond the ED was 50% (RT 44%, REBOA 63%; p = 0.004) and survival to discharge was 5% (RT 2.5%, REBOA 9.6%; p = 0.023). Discharge Glasgow Coma Scale score was 15 in 85% of survivors. Patients who did not require any CPR before had a survival beyond the ED of 70% (RT 48%, REBOA 93%; p < 0.001) and survival to discharge of 13% (RT 3.4%, REBOA 22.2%, p = 0.048). If aortic occlusion patients did not require CPR but presented with hypotension (systolic blood pressure <90 mmHg; 9% [65% RT; 35% REBOA]), they achieved survival beyond the ED in 65% (p = 0.009) and survival to discharge of 15% (RT 0%, REBOA 44%; p = 0.008).
CONCLUSIONS:
Overall, REBOA can confer a survival benefit over RT, particularly in patients not requiring CPR.
Expanding the field of acute care surgery: a systematic review of the use of resuscitative endovascular balloon occlusion of the aorta (REBOA) in cases of morbidly adherent placenta.
Eur J Trauma Emerg Surg. 2017 Sep 19. doi: 10.1007/s00068‐017‐0840‐4.Manzano‐Nunez R1,2, Escobar‐VidarteMF3, Naranjo MP4,5, Rodriguez F5, Ferrada P6, Casallas JD4,3, Ordoñez CA5,7.
PURPOSE:
Prophylactic placement of endovascular balloon occlusion catheters has grown to be part of the surgical plans to control intraoperative hemorrhage in cases of abnormal placentation. A systematic literature review was performed to investigate the safety and effectiveness of the use of REBOA during cesarean delivery in pregnant woman with morbidly adherent placenta.
METHODS:
The authors included studies involving pregnant women with diagnosis of abnormal placentation who underwent cesarean delivery with REBOA placed for hemorrhage control. MINORS' criteria were used to evaluate the risk of bias of included studies. A formal meta-analysis was not performed.
RESULTS:
Eight studies were included in cumulative results. These studies included a total of 392 patients. Overall, REBOA was deployed in 336 patients. Six studies reported the use of REBOA as an adjunct for prophylactic hemorrhage control in pregnant woman with diagnosis of morbidly adherent placenta undergoing elective cesarean delivery. In two studies, REBOA was deployed in patients already in established hemorrhagic shock at the moment of cesarean delivery. REBOA was deployed primarily by interventional radiologists; however, one study reported a surgeon as the REBOA provider. The results from our qualitative synthesis indicate that the use of REBOA during cesarean delivery resulted in less blood loss with a low rate complications occurrence.
CONCLUSION:
REBOA was found to be feasible, safe, and effective as a means of prophylactic and remedial hemorrhage control in pregnant women with abnormal placental bleeding undergoing cesarean delivery.
Validation of the Emergency General Surgery Frailty Index in Patients with Burn InjuriesD W Maxwell, DO P Rhee, MDM D Drake, DO J S Hodge, MDW L Ingram, MDR Y Williams, MD
Journal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages S47, https://doi.org/10.1093/jbcr/iry006.087
Published: 09 April 2018
Introduction
As demonstrated in trauma and critical care literature, a diagnosis of frailty, as opposed to chronologic age, is a more significant predictor of morbidity and mortality. There are a variety of frailty scores, some of which have over 50 criteria requiring lengthy calculations. Recently, a 15‐question validated Emergency General Surgery Frailty Index (EGSFI) has been published. Since there is no burn injury specific frailty score, the authors sought to validate the EGSFI in the burn patient population.
Methods
This was a two part study. First, a retrospective review was conducted on 100 patients, ≥65 years old, admitted to the burn unit between 2013 to 2017. They calculated frailty scores based on EGSFI criteria and collected demographics and survival data. Subsequently, they conducted a prospective validation of 20 patients, ≥65 years. Univariate and multivariate analysis were performed.
Results
In the retrospective population, n=34/100 were determined to be frail. There were no significant differences in demographics between frail and non‐frail patients. Thirteen of the 15 EGSFI factors were significantly different between frail and non‐frail patients (Table 1). Patients classified as frail had more statistically significant (p<0.05) complications (61.8% vs 10.6%), non‐home discharges (67.6% vs 13.6%), ICU admissions (52.9% vs 10.6%), longer ICU stays (17 ± 23.0 vs 1 ± 7.0 days), and in hospital mortalities (11.8% vs 1.5%). Frail patients also had statistically significant lower GCS on presentation, increased presence of inhalation injury, and increased need for intubation on arrival.
Conclusions
The abbreviated EGSFI accurately predicted morbidity and mortality in burn patients and aided in both the planning of needed resources and as counseling adjunct for family members.
Page 224
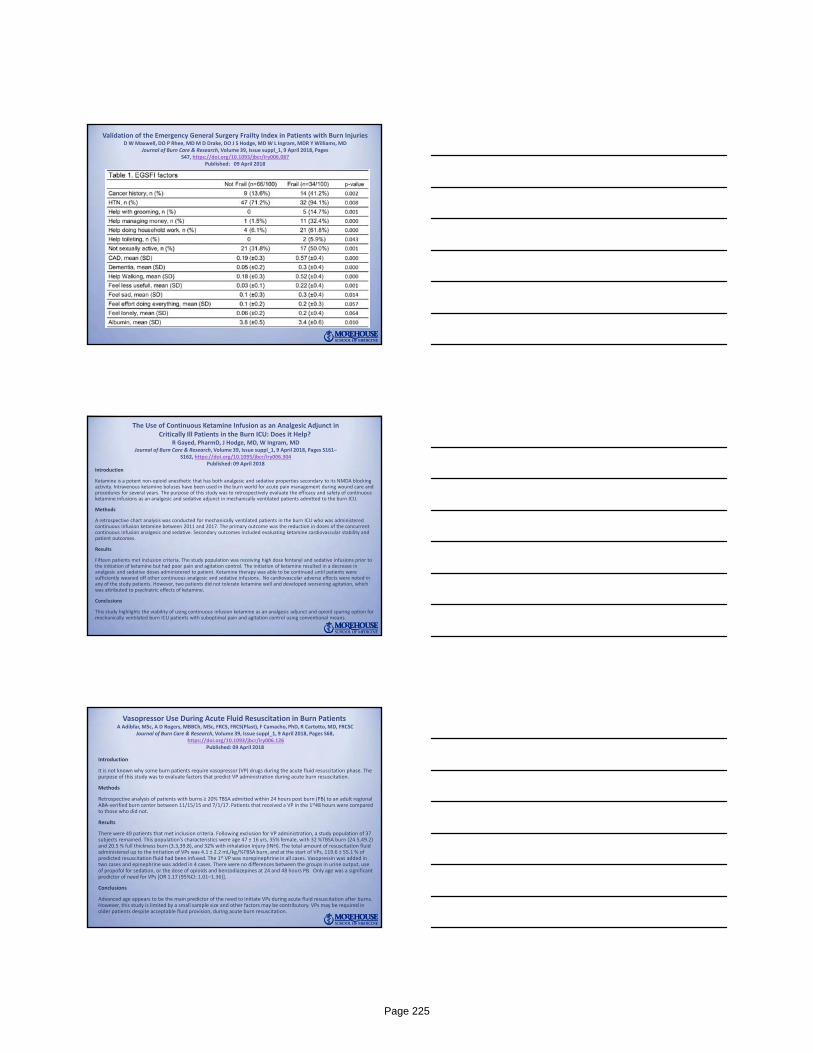
Validation of the Emergency General Surgery Frailty Index in Patients with Burn InjuriesD W Maxwell, DO P Rhee, MDM D Drake, DO J S Hodge, MDW L Ingram, MDR Y Williams, MD
Journal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages S47, https://doi.org/10.1093/jbcr/iry006.087
Published: 09 April 2018
The Use of Continuous Ketamine Infusion as an Analgesic Adjunct in Critically Ill Patients in the Burn ICU: Does it Help?
R Gayed, PharmD, J Hodge, MD, W Ingram, MDJournal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages S161–
S162, https://doi.org/10.1093/jbcr/iry006.304Published: 09 April 2018
Introduction
Ketamine is a potent non‐opioid anesthetic that has both analgesic and sedative properties secondary to its NMDA blocking activity. Intravenous ketamine boluses have been used in the burn world for acute pain management during wound care and procedures for several years. The purpose of this study was to retrospectively evaluate the efficacy and safety of continuous ketamine infusions as an analgesic and sedative adjunct in mechanically ventilated patients admitted to the burn ICU.
Methods
A retrospective chart analysis was conducted for mechanically ventilated patients in the burn ICU who was administered continuous infusion ketamine between 2011 and 2017. The primary outcome was the reduction in doses of the concurrent continuous infusion analgesic and sedative. Secondary outcomes included evaluating ketamine cardiovascular stability and patient outcomes.
Results
Fifteen patients met inclusion criteria. The study population was receiving high dose fentanyl and sedative infusions prior to the initiation of ketamine but had poor pain and agitation control. The initiation of ketamine resulted in a decrease in analgesic and sedative doses administered to patient. Ketamine therapy was able to be continued until patients were sufficiently weaned off other continuous analgesic and sedative infusions. No cardiovascular adverse effects were noted in any of the study patients. However, two patients did not tolerate ketamine well and developed worsening agitation, which was attributed to psychiatric effects of ketamine.
Conclusions
This study highlights the viability of using continuous infusion ketamine as an analgesic adjunct and opioid sparing option for mechanically ventilated burn ICU patients with suboptimal pain and agitation control using conventional means.
Vasopressor Use During Acute Fluid Resuscitation in Burn PatientsA Adibfar, MSc, A D Rogers, MBBCh, MSc, FRCS, FRCS(Plast), F Camacho, PhD, R Cartotto, MD, FRCSC
Journal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages S68, https://doi.org/10.1093/jbcr/iry006.126
Published: 09 April 2018
Introduction
It is not known why some burn patients require vasopressor (VP) drugs during the acute fluid resuscitation phase. The purpose of this study was to evaluate factors that predict VP administration during acute burn resuscitation.
Methods
Retrospective analysis of patients with burns ≥ 20% TBSA admitted within 24 hours post burn (PB) to an adult regional ABA‐verified burn center between 11/15/15 and 7/1/17. Patients that received a VP in the 1st48 hours were compared to those who did not.
Results
There were 49 patients that met inclusion criteria. Following exclusion for VP administration, a study population of 37 subjects remained. This population’s characteristics were age 47 ± 16 yrs, 35% female, with 32 %TBSA burn (24.5,49.2) and 20.5 % full thickness burn (3.3,39.8), and 32% with inhalation injury (INH). The total amount of resuscitation fluid administered up to the initiation of VPs was 4.1 ± 2.2 mL/kg/%TBSA burn, and at the start of VPs, 119.6 ± 55.1 % of predicted resuscitation fluid had been infused. The 1st VP was norepinephrine in all cases. Vasopressin was added in two cases and epinephrine was added in 4 cases. There were no differences between the groups in urine output, use of propofol for sedation, or the dose of opioids and benzodiazepines at 24 and 48 hours PB. Only age was a significant predictor of need for VPs [OR 1.17 (95%CI: 1.01–1.36)].
Conclusions
Advanced age appears to be the main predictor of the need to initiate VPs during acute fluid resuscitation after burns. However, this study is limited by a small sample size and other factors may be contributory. VPs may be required in older patients despite acceptable fluid provision, during acute burn resuscitation.
Page 225
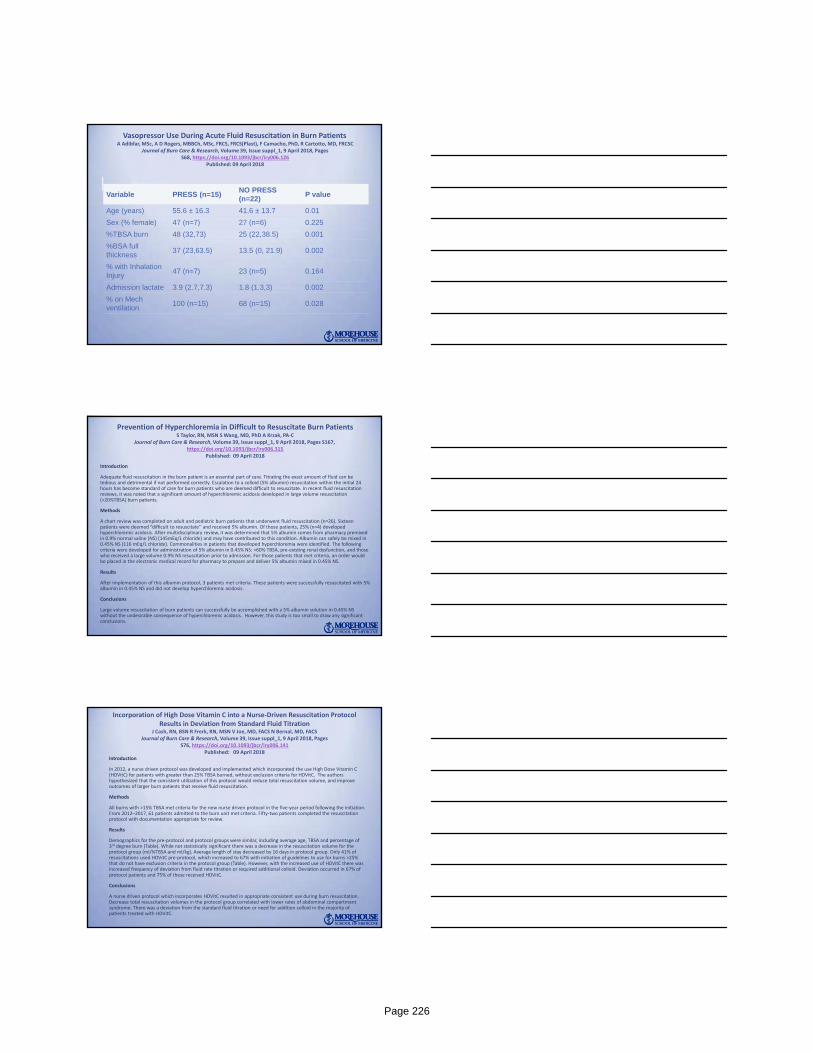
Vasopressor Use During Acute Fluid Resuscitation in Burn PatientsA Adibfar, MSc, A D Rogers, MBBCh, MSc, FRCS, FRCS(Plast), F Camacho, PhD, R Cartotto, MD, FRCSC
Journal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages S68, https://doi.org/10.1093/jbcr/iry006.126
Published: 09 April 2018
Variable PRESS (n=15)NO PRESS (n=22)
P value
Age (years) 55.6 ± 16.3 41.6 ± 13.7 0.01
Sex (% female) 47 (n=7) 27 (n=6) 0.225
%TBSA burn 48 (32,73) 25 (22,38.5) 0.001
%BSA full thickness
37 (23,63.5) 13.5 (0, 21.9) 0.002
% with Inhalation Injury
47 (n=7) 23 (n=5) 0.164
Admission lactate 3.9 (2.7,7.3) 1.8 (1.3,3) 0.002
% on Mechventilation
100 (n=15) 68 (n=15) 0.028
Prevention of Hyperchloremia in Difficult to Resuscitate Burn PatientsS Taylor, RN, MSN S Wang, MD, PhD A Krzak, PA‐C
Journal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages S167,https://doi.org/10.1093/jbcr/iry006.315
Published: 09 April 2018
Introduction
Adequate fluid resuscitation in the burn patient is an essential part of care. Titrating the exact amount of fluid can be tedious and detrimental if not performed correctly. Escalation to a colloid (5% albumin) resuscitation within the initial 24 hours has become standard of care for burn patients who are deemed difficult to resuscitate. In recent fluid resuscitation reviews, it was noted that a significant amount of hyperchloremic acidosis developed in large volume resuscitation (>20%TBSA) burn patients.
Methods
A chart review was completed on adult and pediatric burn patients that underwent fluid resuscitation (n=26). Sixteen patients were deemed “difficult to resuscitate” and received 5% albumin. Of those patients, 25% (n=4) developed hyperchloremic acidosis. After multidisciplinary review, it was determined that 5% albumin comes from pharmacy premixed in 0.9% normal saline (NS) (145mEq/L chloride) and may have contributed to this condition. Albumin can safely be mixed in 0.45% NS (116 mEq/L chloride). Commonalities in patients that developed hyperchloremia were identified. The following criteria were developed for administration of 5% albumin in 0.45% NS: >60% TBSA, pre‐existing renal dysfunction, and those who received a large volume 0.9% NS resuscitation prior to admission. For those patients that met criteria, an order would be placed in the electronic medical record for pharmacy to prepare and deliver 5% albumin mixed in 0.45% NS.
Results
After implementation of this albumin protocol, 3 patients met criteria. These patients were successfully resuscitated with 5%albumin in 0.45% NS and did not develop hyperchloremic acidosis.
Conclusions
Large volume resuscitation of burn patients can successfully be accomplished with a 5% albumin solution in 0.45% NS without the undesirable consequence of hyperchloremic acidosis. However, this study is too small to draw any significant conclusions.
Incorporation of High Dose Vitamin C into a Nurse‐Driven Resuscitation Protocol Results in Deviation from Standard Fluid Titration
J Cash, RN, BSN R Frerk, RN, MSN V Joe, MD, FACS N Bernal, MD, FACSJournal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages
S76, https://doi.org/10.1093/jbcr/iry006.141Published: 09 April 2018
Introduction
In 2012, a nurse driven protocol was developed and implemented which incorporated the use High Dose Vitamin C (HDVitC) for patients with greater than 25% TBSA burned, without exclusion criteria for HDVitC. The authors hypothesized that the consistent utilization of this protocol would reduce total resuscitation volume, and improve outcomes of larger burn patients that receive fluid resuscitation.
Methods
All burns with >15% TBSA met criteria for the new nurse driven protocol in the five‐year period following the initiation. From 2012–2017, 61 patients admitted to the burn unit met criteria. Fifty‐two patients completed the resuscitation protocol with documentation appropriate for review.
Results
Demographics for the pre‐protocol and protocol groups were similar, including average age, TBSA and percentage of 3rd degree burn (Table). While not statistically significant there was a decrease in the resuscitation volume for the protocol group (ml/%TBSA and ml/kg). Average length of stay decreased by 16 days in protocol group. Only 41% of resuscitations used HDVitC pre‐protocol, which increased to 67% with initiation of guidelines to use for burns >25% that do not have exclusion criteria in the protocol group (Table). However, with the increased use of HDVitC there was increased frequency of deviation from fluid rate titration or required additional colloid. Deviation occurred in 67% of protocol patients and 75% of these received HDVitC.
Conclusions
A nurse driven protocol which incorporates HDVitC resulted in appropriate consistent use during burn resuscitation. Decrease total resuscitation volumes in the protocol group correlated with lower rates of abdominal compartment syndrome. There was a deviation from the standard fluid titration or need for addition colloid in the majority of patients treated with HDVitC.
Page 226
Incorporation of High Dose Vitamin C into a Nurse‐Driven Resuscitation Protocol Results in Deviation from Standard Fluid Titration
J Cash, RN, BSN R Frerk, RN, MSN V Joe, MD, FACS N Bernal, MD, FACSJournal of Burn Care & Research, Volume 39, Issue suppl_1, 9 April 2018, Pages
S76, https://doi.org/10.1093/jbcr/iry006.141Published: 09 April 2018
Surgical and Burn Critical Care Year in Review
Questions?
Surgical and Burn Critical Care Year in Review
The end!
Thank you!
Page 227
Nature’s FuryMan’s Flurry
Emory Critical Care Conference May 9th 2018
K. Guntupalli, M.D., FCCM, Master FCCP, MACPFrances K. Friedman and Oscar Friedman, MD '36 Endowed Professor for Pulmonary Disorders
Chief, Pulmonary, Critical Care and Sleep Medicine, Ben Taub General HospitalProgram Director, Critical Care Fellowship
Baylor College of Medicine, Houston, Tx
Outline:Experiences from the Hurricane Harvery
1. Houston ‘s vulnerability to Tropical storms and Hurricanes 2. Defining infrastructure priorities 3. Hurricane Harvey – its magnitude and impact 4. City of Houston, Texas Medical Center and Ben Taub General
Hospital 5. Bracing for “Harvey” – Preparation 6. Facing “Harvey” – Happenings during the Hurricane: Facing the
unexpected 7. Governance, Personnel, Medical issues – Organization and
implementation 8. Post Harvey – Houston faces major recovery challenges 9. Lessons learned
My Experience in Texas in Hurricanes/Tropical Storms
Tropical Storm Allison• 2001• 40 Inches of Rain• 23 deaths• 2 Billion in damages• Hermann Hospital
Evacuated 600 patients
Hurricane Katrina • 2005• 250,000 refugees
45,000 in Astrodome• 40 bed clinic
complex• > 1000 people killed
between LA and Tx
Hurricane Rita • 2005
Hurricane Ike • 2008• 21 people Killed
Page 228
Defining,Describing,andCategorizingPublicHealthInfrastructurePrioritiesforTropicalCyclone,Flood,Storm,Tornado,andTsunami‐RelatedDisasters.
RyanBJ,etal.DisasterMedPublicHealthPrep. 2016;10(4):598‐610.
1. Workforce 2. Water 3. Sanitation 4. Equipment 5. Communication 6. Physical structure 7. Power
8. Governance 9. Prevention 10. Supplies 11. Service 12. Transport 13. Surveillance
Infrastructure Governance Workforce Supplies/Service SurveilancePre,DuringPost
Water SETREC Needs assessment Equipment Prevention
Sanitation Set up Command and Control center
Ride out teamsRescue teams
Food Medical and psychological impact
Physical structure Keeping up the personal and team spirit
Structural and other damage
IT, Electricity Morale Transport
LegalPreparedness:CareoftheCriticallyIllandInjuredDuringPandemicsandDisasters:CHESTConsensusStatement
CourtneyB,etal.Chest. 2014;146(4Suppl):e134S‐44S.
1. 35 key questions
2.Developed expert opinion‐based suggestions
3. Seven final suggestions
Page 229
Hurricane Harvey Hits Houston! Made landfall on the Texas coast at 130 MPH Rain registered at > 50” breaking all records in
continental USA 20 trillion gallons of water 1 in 1000 yr flood – an exceptionally rare event 300,000 without power Houston experiencing its 3rd 500 yr flood in 3
years Hurricane with 1, 2 punch – came twice 75 deaths
Texas Medical CenterHouston is the fourth largest city in USA 6.5 million population in greater
Houston area
Largest medical complex in the world 1600 acres 22 institutions 2 Medical schools 14 hospitals 105,000 employees Underground utility facilities as compact as Manhattan 4500 hospital beds 3 of top 5 hospitals in the country are in TMC If a city, 18th in USA
Prevention: Texas Medical CenterAfter 2001 Allison; remedial measures around TMC
1. Submarine type walls isolating hospitals connected by tunnels
2. Flood gates constructed after Allison around Baylor College offices/labs
3. Contain Bio hazard4. Construct underground vivarium.5. Develop disaster plans - review from time to time6. Back up generators previously located in
basements placed high and protected
Page 230
Hurricane Harvey - The State of the City of Houston
Downtown Houston, Highway 45
Aug 27th 2017
Page 231

The State of the Texas Medical Center
Harris Health System: Ben Taub General Hospital
1. One of two Level 1 Trauma centers 2. 560 bed safety net hospital2. 60% of teaching for BCM done at BTGH4. Police and prisoners both get admitted 5. Part of Harris Health system, 2 hospitals, 22 clinics around
Houston city.6. BTGH staffed by Baylor College of Medicine, LBJ hospital by
University of Texas Medical School.
Page 232
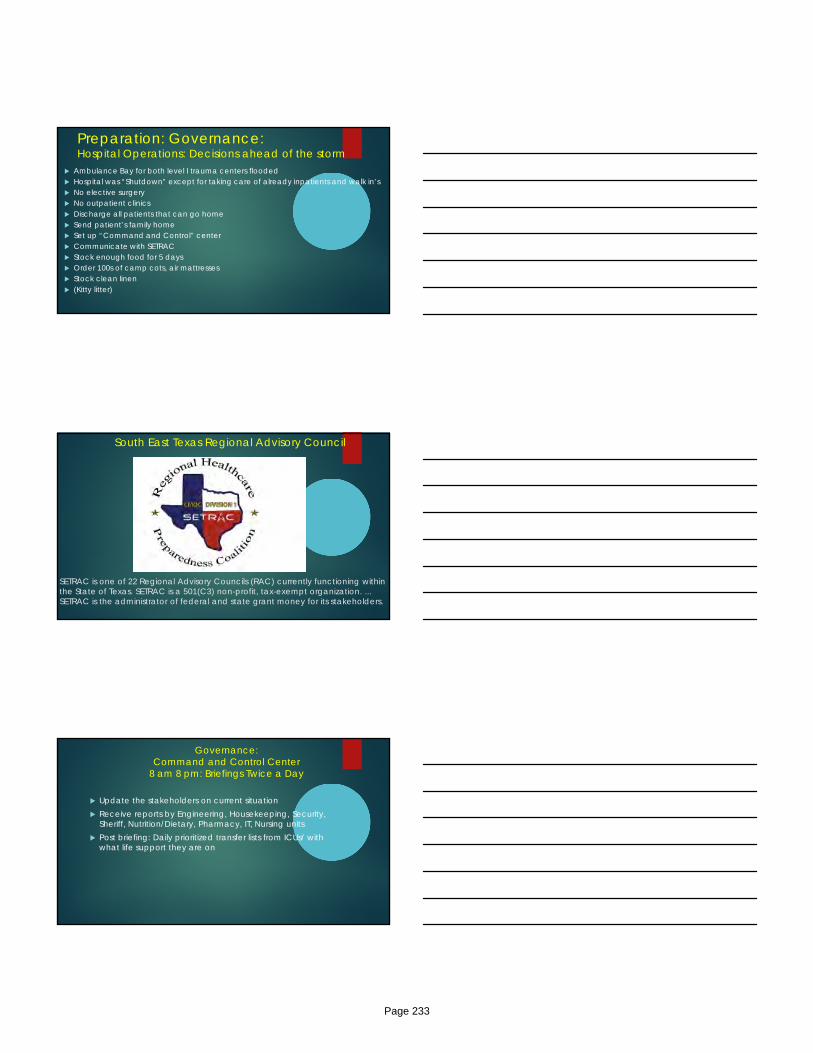
Preparation: Governance:Hospital Operations: Decisions ahead of the storm
Ambulance Bay for both level I trauma centers flooded Hospital was “Shutdown” except for taking care of already inpatients and walk in’s No elective surgery No outpatient clinics Discharge all patients that can go home Send patient’s family home Set up “Command and Control” center Communicate with SETRAC Stock enough food for 5 days Order 100s of camp cots, air mattresses Stock clean linen (Kitty litter)
SETRAC is one of 22 Regional Advisory Councils (RAC) currently functioning within the State of Texas. SETRAC is a 501(C3) non-profit, tax-exempt organization. ... SETRAC is the administrator of federal and state grant money for its stakeholders.
South East Texas Regional Advisory Council
Governance: Command and Control Center
8 am 8 pm: Briefings Twice a Day
Update the stakeholders on current situation Receive reports by Engineering, Housekeeping, Security,
Sheriff, Nutrition/Dietary, Pharmacy, IT, Nursing units Post briefing: Daily prioritized transfer lists from ICUs/ with
what life support they are on
Page 233
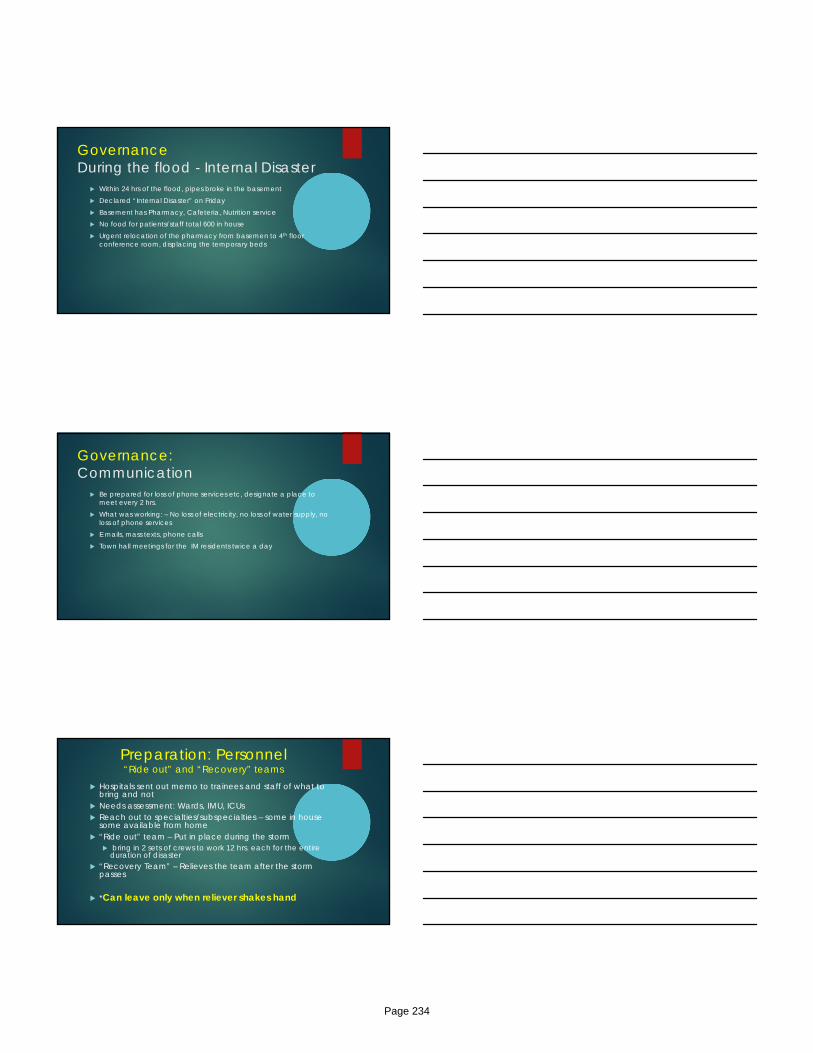
GovernanceDuring the flood - Internal Disaster
Within 24 hrs of the flood, pipes broke in the basement Declared “Internal Disaster” on Friday Basement has Pharmacy, Cafeteria, Nutrition service No food for patients/staff total 600 in house Urgent relocation of the pharmacy from basemen to 4th floor
conference room, displacing the temporary beds
Governance:Communication
Be prepared for loss of phone services etc, designate a place to meet every 2 hrs.
What was working: – No loss of electricity, no loss of water supply, no loss of phone services
E mails, mass texts, phone calls Town hall meetings for the IM residents twice a day
Preparation: Personnel“Ride out” and “Recovery” teams
Hospitals sent out memo to trainees and staff of what to bring and not
Needs assessment: Wards, IMU, ICUs Reach out to specialties/subspecialties – some in house
some available from home “Ride out” team – Put in place during the storm
bring in 2 sets of crews to work 12 hrs. each for the entire duration of disaster
“Recovery Team” – Relieves the team after the storm passes
*Can leave only when reliever shakes hand
Page 234
Personnel : Issues During the Hurricane
Prioritize and revise transfer list everyday for evacuation Some nurses worked from Friday to Tuesday Shower water was “salty” Food shortage – basement flooded Food for family members - a problem Pharmacy emergency evacuation from basement “Curfew” several days – to avoid robberies All family members sent to Reliant stadium/GRB evacuees
camp
Personnel: Keep up the MoraleRest and Relaxation
Off teams : Must sleep and not make this a class “picnic” Games Videos Movies Food Jeopardy style quizzes Check if people reached home or able to reach work Walk and exercise on the parking lot roof when rain eased up
Murphy’s Law – ”Anything that can go wrong will go wrong”
5 SICU and 1 medical floor patient was able to be transferred out. 3 came back could not reach destination.
Inpatients and ICU patients crashed requiring emergent interventions
Page 235
Ben Taub General Hospital Critical Care “Ride out” Team
PersonnelSome rules for Family: in disasters extended over a long period
Self and family welfare first Do not challenge the nature! This is August; many new trainees on board Check on – water supply, power supply even at work Many of our faculty/fellows got flooded, some were mandatorily
evacuated on third day due to controlled release of two water reservoirs At least half lost power, some lost water supply – filled bath tubs pool water Many friends lost their cars – garages flooded, stuck on roads, hydroplaning,
drive carefully Do not hesitate to ask for help
Personnel: Some rules for work ……
It’s a marathon NOT a Sprint! Its all about endurance not a point performance Sleep is important - A 16 hr. continuous working = legally
drunk levels of alcohol Keep head straight, body healthy Sleep deprivation – Errors of omission and commission Work needs to be coordinated, not in silos Evacuating patients may be more dangerous than caring in
your place
Page 236
Mass Casualty Evacuation Ambulance
Debriefing
Meet after the situation settled down to evaluate what worked, what didn’t
Unprecedented feeling of camaraderie, team spirit Poor planning = Fatigued, demoralized work force Forum to share their experiences , thank and appreciate each other Free psychiatric counseling Arrange coverage for those affected by the storm; takes weeks to
clean up, file insurance claims, etc
Page 237

When people around you get affected ….
Biked 8 miles to get to work At least 15 faculty in the section lost cars due to garage flooding Our research coordinator, secretary, fellows, Chair of Medicine Escape from drowned cars – (Cafeteria selling hammers) day
before) Chief of Medicine fell in the park in 3 feet of water almost drowned Chief of staff house lost! Hospitalist delivered, no home to take the baby to Neighborhoods devastated PTSD …..
The Houston Community in Trouble !
Our Experience During Hurricane Katrina: Refugee Evacuees from New Orleans - 2005
Main difference – The Houston Community was not affected
They were hosts unaffected by the flood we had intact infrastructure – water, electricity, communication and healthcare
Large space available close to the largest medical center complex
25,000 in Astrodome/Reliant stadium, 10,000 in GRB convention center
Tulane med school shifted to Baylor for 9 months Took in a fellow for training for months
Page 238
Astrodome/Reliant stadium - KatrinaMedical complex – 2 miles from Texas Medical Center
Built on 100,000 sq foot space in the astrodome/reliant arena complex
Within 12 hrs medical service area with 68 examining rooms –triage/intake, Gen Medicine/FP, Surgery, Ob/Gyn, Psychiatry Pediatrics, Radiology, Orthopedics, Ophthalmology, ENT clinics were set up.
Volunteered after our regular working hours
Hurricane Katrina – 2005Houston Medical Camp
Page 239

> 1000 patients in 11 days
Hurricane Harvey - George R. Brown Convention CenterShelter > 17,000 Evacuees
Harvey GRB : 10,000People
Sheltered
NRG: 9000
Page 240
Hurricane Harvey may have totaled 500,000 cars – motor trend
The “Aftermath”
The aftermath: Repairs to infrastructure
Page 241
The aftermath
The Reliant/GRB evacuee center medical camp open for weeks
Many volunteers from outside came to help Many Baylor alumni plus others
Those who fall thru the cracks…..
AfterFlooding:MedicalProblems
Traumaticinjuries
Communicablediseases
Chemicalexposures
Malnutrition
Decreasedaccesstocare
Mentalhealthdisorders
Page 242
FloodAssociatedInfections
Vibrio
NTM
Aeromonas
Meloidosis
Leptospirosis
Chromobacterium
Blastomycosis
Mucormycosis
Chromoblastomycosis
Environment‐DermatologicalConsequences
Miliaria
ImmersionFootSyndromes
ContactDermatitis
Traumaticwounds
Animalbites
Insectbites
Psychodermatological disorders Bandino JP,etal.AmJClin Dermatol.2015;16(5):399‐424
Major Health Risks When Working on Water-Damaged Homes? – Baylor released a brochure
Mold Lead Dust (homes before 1978)Cuts and PuncturesCarbon Monoxide Electric Shocks Snakes /Insects/Animals/Gators InfectionsPTSD
Page 243
Electric Shocks Electric shocks can kill. Danger of electrical shock from any electrical device
that has been flooded. Rubber boots and gloves do not always protect from
electric shock. Turn off the electricity at the breaker before starting work
if you do not know the condition of the wiring behind walls
Health effects associated with exposure to mold?
People most often are exposed to mold by breathing in mold spores that float in the air.
These mold spores are too small to be seen with the naked eye. When people with mold allergies breathe air that has high mold levels, they can have allergy symptoms such as stuffy nose, sinus problems and shortness of breath.
Even worse, they may have a life-threatening asthma attack.
Symptoms of mold exposure?
Breathing difficulties Shortness of breath Wheezing Sore throat Flu-like aches and pains Fatigue
Page 244
Carbon Monoxide
Carbon monoxide (CO) is an odorless, colorless gas that can cause sudden illness and death. Burning fuels, such as gas, oil, kerosene, wood or charcoal, produce CO. No fuel burning equipment, including portable generators, should be used inside flood damaged homes.
Cuts and Punctures
Broken glass, boards, exposed nails and other hazards are common in flood and storm damaged homes. Floodwaters may contain germs or viruses that can enter the skin through cuts and scrapes. Wear protective equipment to prevent serious injuries. Take
special care to protect hands and feet. Check that you and your workers have current tetanus shots
(within the last 10 years) before working in flooded areas. If a cut or puncture occurs, wash the cut immediately and treat
with an antiseptic ointment such as Betadine or Povidine Iodine Cream.
Posttraumaticstresssymptoms,co‐morbidpsychiatricsymptomsanddistortedcognitionsamongflood
victimsofdifferentages.ChungMC,etal.
JMent Health. 2017;26(3):204‐211.
AdolescentsandyoungadultsreportedsignificantlyfewerPTSD,psychiatriccomorbidityanddistortedcognition
symptomsthanpeoplewhowereolder.Preoccupationwithdangerandhopelessnesswereassociatedwithbothoutcomesforadolescents,peopleintheirthirtiesand
middle‐aged/olderpeople.
Page 245
Page 246

The “Key” to keeping the patients and personnel safe
Flexibility Frequency of communication Adequate staff Adequate resources
Page 247
“Learning Beyond Books” My 4 “A” s
Anticipate Adopt
Adept
Adapt
Anticipate and prepare for problems from prior experience of your area and others
Meet several times to assess operations and accommodate the fluid situation
Know issues unique to your area - Many issues are local Expect the unexpected; think on your feet Earn respect from leading from the front You can inspire others to go beyond expectations
Life Lessons: “Learning Beyond Books”
What it means to be a part of a multi departmental successful team Cooperation beyond patient care For learners – “Learning beyond books” Administration during emergency situation Help arrives from unexpected corners - Community pulls together Think out of the Box! -– medical voyeurism, credentialing, trainee
relocation, communicate with ACGME, Board certification dates etc
Each situation is similar but also very different. --
After all the trauma the Houstonians went thru….
We needed this …….
Page 248

Thank You!
Acute epidemic of diarrhoeal outbreak after floods and hurricanes is due to
A. Leptospirosis B. Shigella C. Noro virus D. Influenza virus E. Amoebiasis
Page 249
Breakout Session Notes Mechanical Ventilation ICU Ultrasonography
ECMO Pearls and Pitfalls Hemodynamic Monitoring Vascular Access Simulation
Targeted Temperature Management ___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 250
2018 Critical Care Summit
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 251
2018 Critical Care Summit
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________ ___________________________________________________________________
Page 252
Top Related