






Languages
Pages
Legal

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
COPD and PFTs
Tereza Martinu, MD
Anna Person, MD
Nathan Shores, MD
Jeff Vandeusen, MD

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Case
• A 60 year-old white, female smoker presents with increasing dyspnea on exertion and shortness of breath for 1 year.
• She has a 50 pack-year history. Her exam shows a prolonged expiratory time and distant heart sounds.
• You Suspect COPD

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
PFT Indications
• Evaluation of symptoms (chronic cough, wheezing, dyspnea)• Assessment of risk before surgery • Evaluation of possible exposure in the workplace (reactive
airway disease or occupational asthma)• Objective measurement of impairment or disability• Surveillance of patients after lung transplantation for early
rejection• Note: Only do PFTs on patients who can follow directions and
don’t have an acute pulmonary problem. Cannot do PFTs on intubated patients and should not do them on hospitalized COPD patients in an acute exacerbation.
• Prolonged smoking history

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
What is It?
• Spirometry: Measurement of airflow rate and expired volume over time. This can actually be done in outpatient setting, and does not require massive machinery. Small clinics can do their own spirometry. We even have bedside spirometry that can be used if necessary at the VA and all lung transplant patients have their own spirometry to track FEV1 at home (every morning).
• Lung volumes & DLCO: need sophisticated equipment and an accredited PFT lab – make sure that this is done at a place that you trust.
• At Duke, when you order PFTs, you actually only get spirometry. If you want the lung volumes and DLCO along with it, you have to order PFDs (stands for “pulmonary function studies with diffusion capacity”).

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Results
• Quality – Will be addressed in report– Affected by effort,
musculoskeletal disease– Can be assessed by
assessing the graph and taking repeated measurements
• Standards – Age, Sex, Race, Height, and
Weight all dictate reference standards, influencing “percent predicted”

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Abnormal Tests
• If results are abnormal, what is the disease process?– First look at FEV1/FVC: if ratio is < 70% of predicted, there
is obstruction– If no obstruction, look at FVC: if < 80% of predicted, there
may be restriction

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Interpretation
• If there is obstruction, look at FEV1 to determine severity of obstruction.– >70% mild
– 60-70% moderate
– 50-60% moderately severe
– 35-50% severe
– <35% very severe
• If FVC < 80%, think restriction and consider getting lung volume studies:– TLC < 80% indicates
restrictive process. FRC, RV, & VC are usually markedly low as well.

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Flow Loops
Obstructive
Normal
Restrictive

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Interpretation Algorithm
Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
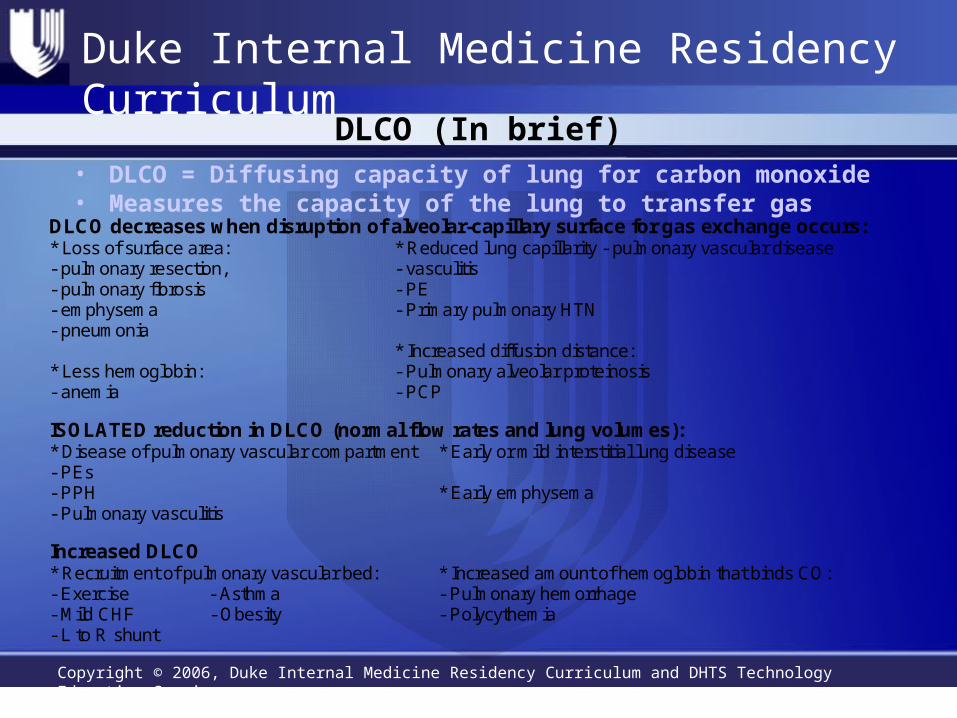
DLCO (In brief)• DLCO = Diffusing capacity of lung for carbon monoxide• Measures the capacity of the lung to transfer gas
DLCO decreases when disruption of alveolar-capillary surface for gas exchange occurs: * Loss of surface area: - pulmonary resection, - pulmonary fibrosis - emphysema - pneumonia
* Reduced lung capillarity - pulmonary vascular disease - vasculitis - PE - Primary pulmonary HTN
* Less hemoglobin: - anemia
* Increased diffusion distance: - Pulmonary alveolar proteinosis - PCP
ISOLATED reduction in DLCO (normal flow rates and lung volumes): * Early or mild interstitial lung disease * Disease of pulmonary vascular compartment
- PEs - PPH - Pulmonary vasculitis
* Early emphysema
Increased DLCO * Recruitment of pulmonary vascular bed: - Exercise - Asthma - Mild CHF - Obesity - L to R shunt
* Increased amount of hemoglobin that binds CO: - Pulmonary hemorrhage - Polycythemia

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Chronic Obstructive Pulmonary Disease

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
COPD
• As defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines:
• “A disease state characterized by airflow limitation that is not fully reversible. Airflow limitation is usually both progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases.”

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Which is the best predictor of survival in COPD?
• pO2• FEV1 as a percent of predicted• Diffusing capacity• Presence of emphysema on CT scan• Composite score of BMI, airflow obstruction, dyspnea level and
exercise tolerance
Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
• Index based on:• Body mass• Obstruction of airflow Better than FEV1 in predicting
survival• Dyspnea level• Exercise

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
BODE score• Quartile 1: 0-2• Quartile 2: 3-4• Quartile 3: 5-6• Quartile 4: 7-10
FEV1 % predictedStage 1: >50%Stage 2: 36-50%Stage 3: <35%

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
COPD: Assessment and Monitoring
• The diagnosis of COPD is made based on risk factors and spirometry
• Spirometry is the GOLD standard for diagnosis of COPD– FEV1/FVC <70%– More severe stage with decreasing FEV1
• Perform ABG’s if FEV1 is <40% of predicted• Test of alpha-1 antitrypsin deficiency if patients are <45 or have
a strong family history
• *NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD)
• Workshop summary. Am J Respir Crit Care Med. 2001 Apr;163(5):1256-76.

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
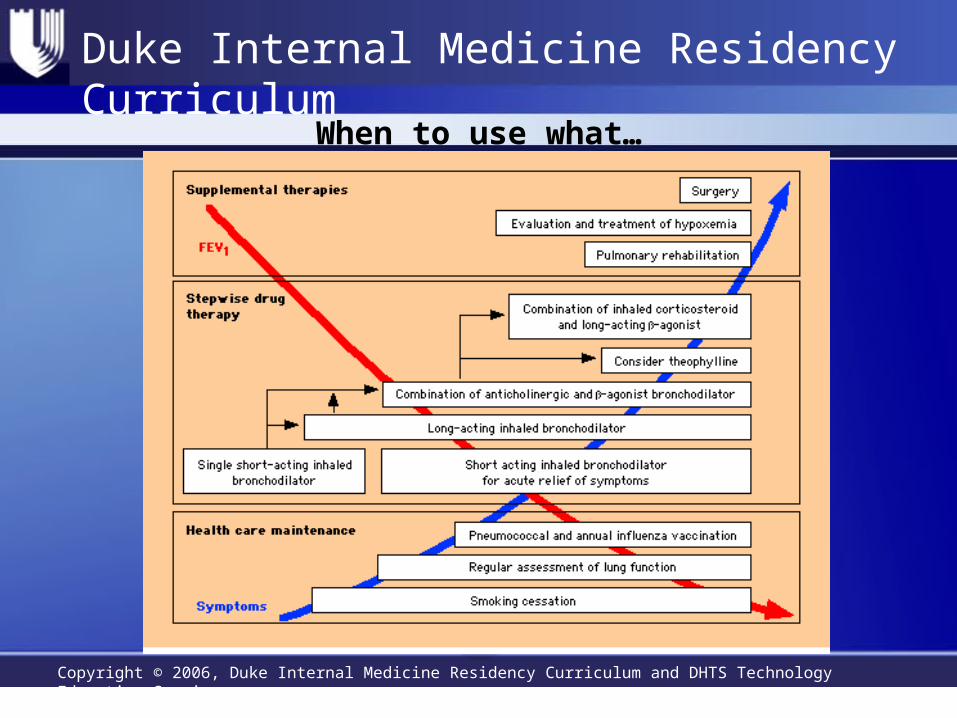
Management of Stable COPD
• Stepwise, symptom based approach• There are no medications that affect mortality or attenuate
decline in lung function• Bronchodilator treatment central to symptomatic management• Consider inhaled steroids for patients with documented
response to steroids or in those with FEV1 < 50% predicted and a history of repeated exacerbations
Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
When to use what…

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
COPD Exacerbations
• 1.5 million ED visits, 726,000 visits in 2000• Acute exacerbation with PaC02 of 50mmHg or more is
associated with 6 month mortality rate of 33%, 12 month of 43%• Exacerbations caused by infection, environmental pollutants,
ambient temperature, aspiration, unknown factors

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
COPD Exacerbations: When to Admit
Indications for Admission:
-Marked increase in intensity of sx
-Severe background COPD
-New physical signs
-Failure to respond to initial management
-Many comorbities
-New arrhythmias
-Older age
-Poor home environment or social support
(from the Global Initiative for Chronic Obstructive Pulmonary Disease (4/1998)

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Treatment of Acute Exacerbations
• Inhaled beta-2 adrenergic agonists (albuterol, etc)• Anticholinergic bronchodilators (ipratropium bromide)• Systemic corticosteroids• Antibiotics• Oxygen (target Pa02 of 60-65 mmHg)• Noninvasive positive pressure ventilation

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Corticosteroids
• Role in COPD exacerbations had been unclear• Trial in N Engl J Med in 1999 of corticosteroids vs. placebo showed
length of hospitalization was 8.5 days vs. 9.7 days (p=0.03)• FEV1 improved faster in pts who received steroids (but no difference
from placebo group at 2 weeks)• Steroids reduced rate of treatment failure at 30 and 90 days, but not 6
months• 2 week course as effective as 8 week course• Hyperglycemia, possible increased rate of infections were
complications

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
NPPV- CPAP and BiPAP
• Benefit in hypercapnic COPD exacerbations• Decrease mortality, intubation rates, treatment
failure, length of hospital stay• American Association for Respiratory Care criteria for
use when 2 or more of the following are present:– respiratory distress w/ mod to severe dyspnea– Arterial pH <7.35 w/ PaC02>45 mmHg– RR of >25– absence of contraindications (inability to protect airway,
facial trauma, etc)

Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Summary
• PFT’s can distinguish between obstructive and restrictive lung disease
• Make sure you know what you’re ordering• Staging COPD can help determine tx regimens and prognosis• Beware of exacerbations- mortality may be high. • Know when to admit.
Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
References
• Pauwels, RA, et al. Global Strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med 2001; 163:1256.
• Niewoehner, D, et al. N Engl J Med 1999;340:1941-7. • Mannino, DM, et al. Chronic obstructive pulmonary disease surveillance– United
States, 1971-2000. MMWR Surveill Summ 2002; 51:1. • Connors, AF et al. Outcomes following acute exacerbation of severe chronic
obstructive lung disease: The SUPPORT investigators. Am J Respir Crit Care med 1996; 154:959.
• Miravitlles, M et al. Factors associated with increased risk of exacerbation and hospital admission in a chorot of ambulatory COPD patients: A multiple logistic regression analysis. Respiration 2000; 67:495.
• Ram, FS et al. Non-invasive positive pressure ventilation for treatment of respiratory failure due to exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2004; :CD004104
• Bach, JR et al. Consensus conference: Noninvasive positive pressure ventilation. Respir Care 1997: 42:261.
Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
Please click here to complete the course evaluation.
Click Next arrow to continue to Reference pages.
Duke Internal Medicine Residency Curriculum
Copyright © 2006, Duke Internal Medicine Residency Curriculum and DHTS Technology Education Services
• Crapo RO. Pulmonary-Function Testing. NEJM 1994;331:25.• Evaluation of impairment / disability secondary to respiratory disorders. American
Thoracic Society. Am Rev Respir Dis. 1986;133:1205-9.• Standardization of Spirometry, 1994 Update. American Thoracic Society. Am J Respir
Crit Care Med. 1995;152:1107.• Lung function testing: selection of reference values and interpretative strategies.
American Thoracic Society. Am Rev Respir Dis. 1991;144:1202.• MKSAP-13, Pulmonary Function Testing• Pulmonary Board Review 2000-2001, American College of Chest Physicians.• Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS; GOLD Scientific
Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001 Apr;163(5):1256-76.
• Celli BR, Cote CG, Marin JM, Casanova C, Montes de Oca M, Mendez RA, Pinto Plata V, Cabral HJ. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004 Mar 4;350(10):1005-12.
References
Top Related