







Languages
Pages
Legal


DRUGS USED IN ENDODONTICS
By
Dr.Anoop.V.Nair
PG
Dept of Cons. Dentistry & Endodontics
KVG Dental College, Sullia

CONTENTS
• Introduction and classifications
• PART I
Pain and analgesics
• PART II
Corticosteroids
• PART III
Antibiotics and its usage
• PART IV
Local anaesthetics
• PART V
Antimicrobial agents
• PART VI
Drugs and pregnant patients
• PART VII
Anxiety and fear
• PART VIII
The medically complex endodontic patient
References
• A medicine or other substance which has a physiological effectwhen ingested or otherwise introduced into the body
-Oxford dictionary
• A pharmaceutical drug, also referred to as a medicine or (loosely)medication, officially called medicinal product, can be looselydefined as any chemical substance — or product comprising such —intended for use in the medical diagnosis, cure, treatment, orprevention of disease.
• The word pharmaceutical comes from the Greek word Pharmakeia.
• According to the Food, Drug, and Cosmetic Act,
(1) : a substance recognized in an official pharmacopoeia or formulary
(2) : a substance intended for use in the diagnosis, cure, mitigation,treatment, or prevention of disease
(3) : a substance other than food intended to affect the structure orfunction of the body
(4) : a substance intended for use as a component of a medicine butnot a device or a component, part, or accessory of a device
Definitions
CLASSIFICATIONSBased on when the drug is administered-
• Pre treatment- analgesics, antibiotics, anti-anxiety
• Treatment- corticosteroids, antibiotics, anti-microbials, local anaesthesia
• Post treatment- antibiotics, corticosteroids, analgesics
Based on route of administration-
• Local- topical antibiotics, anti-microbials, topical anaesthetics
• Systemic- oral- antibiotics, analgesics, anti anxiety
- injectable- im/iv- antibiotics, analgesics, sedatives
• Inhalation- sedatives, anaesthesia

PART IPAIN AND ANALGESICS
IN ENDODONTICS
• The skill of the clinician is often judged primarily by their success or failure of pain control.
-Cohen, Pathways of the Pulp

The
Trigeminal
Pain
System
ANALGESICS-NONNARCOTIC
Management of endodontic pain is multifactorial anddirected at reducing the peripheral and centralcomponents of hyperalgesia through combinedendodontic procedures and pharmacotherapy.
2 classes mainly-
NSAIDS
Acetaminophen

NSAIDS
• Very effective in managing pain of inflammatory origin- binds toplasma proteins- exhibit increased delivery to inflamed tissue viaextravasation of plasma proteins.
• Less studies done comparing NSAIDS on endodontic pain inparticular
• Ibuprofen- considered the prototype of contemporary NSAIDs andhas a well-documented efficacy and safety profile.
• Etodolac (i.e., Lodine) has minimal gastrointestinal (GI) irritation.
• Ketoprofen (i.e., Orudis) has been shown in some studies to besomewhat more analgesic than ibuprofen
• They act primarily through the inhibition of cyclooxygenase (COX)enzymes 1 and2.
• COX-1 is expressed throughout the body and has a role in protection ofstomach mucosa, kidney function and platelet action.
• COX-2 is induced by various endogenous compounds such ascytokines, mitogens and endotoxins in inflammatory cells and isresponsible for the elevated production of prostaglandins duringinflammation.
• Nakanishi et al demonstrated high levels of expression of COX-2 in samples of human dental pulps with a diagnosis of irreversible pulpitis.
• These two proteins share a 60% homology and catalyze the conversion of arachidonic acid into prostaglandin E2.
• PGE2 is subsequently metabolized by a variety of syntheses into PGH2, PFI2, PGD2, PGF2 and thromboxane A2.
• Inhibiting COX-2 blocks prostaglandin formation and ultimately prevents inflammation and sensitization of the peripheral nociceptors.
Pharmacological Strategies to Control Post-operative Endodontic PainZahed Mohammad, Alireza Farhad, Meisam KhalesiDent Res J 2007; 4(2): 61-68
• NSAIDS combined with other drugs (e.g., flurbiprofen with tramadol) or pretreatment and posttreatment application of NSAIDs provides effective pain control.
• The introduction of selective inhibitors of COX-2 offered thepotential for both analgesic and antiinflammatory benefits andreduced GI irritation.
• Oral surgery pain studies evaluating COX-2 inhibitors haveindicated that Rofecoxib (i.e.,Vioxx) has significant analgesicefficacy.
• COX-2 levels are increased in inflamed human dental pulp, anda COX-2 inhibitor (rofecoxib) is analgesic in patients withendodontic pain.
• Concern has been raised that the COX-2 inhibitors may alsodisplay at least some GI irritation in patients with preexisting GIdisease

• Increased risk for prothrombic events following long-term administration
of rofecoxib (VIOXX), which led to the withdrawal of this drug from the
market in 2004.
• Diclofenac (Voltaren) is a relatively COX-2-selective drug and seems
to have a similar degree of COX-2 selectivity as celecoxib.
• Diclofenac was associated with increased CV events.
• In the randomized trial analysis, there was an increase in CV risk with
high-dose ibuprofen.

Based on the available data, the FDA has requested that manufacturers of
all prescription products containing nonselective NSAIDs revise their
product labeling to include
(1) a boxed warning regarding the potential serious adverse CV events
and the serious, potentially life-threatening GI adverse events
associated with the use of this class of drugs
(2) a contraindication for use in patients who have recently undergone
coronary artery bypass surgery
(3) a medication guide for patients, regarding the potential for CV and GI
adverse events associated with the use of this class of drugs.
Given this situation and reasonable alternative NSAIDs, its recommended not
considering COX-2 inhibitors for treating routine endodontic pain patients.

Limitations and Drug Interactions
• NSAIDs exhibit an analgesic ceiling that limits the maximal level of
analgesia and induces side effects, including those affecting the GI
system (3% to 11% incidence) and the CNS (1% to 9% incidenc of
dizziness and headache).
• NSAIDs are contraindicated in patients with ulcers and aspirin
hypersensitivity.
• Also associated with severe GI complications
• Risk of adverse effects increases with increasing lifetime accumulated
dose of these drugs.
• Acetaminophen and opioid combination drugs represent alternatives
for those patients unable to take NSAIDs
Acetaminophen• one of the most commonly used drugs
• found in Combination products for the relief of pain and symptoms of
cold or flu.
• considered safe when taken at normal doses, but in higher doses
causes liver toxicity and has become the most common cause of acute
liver failure
• conjugated in the liver to form inactive metabolites.

• A small portion is metabolized by the cytochrome P450 system to form N-
acetyl-p-benzoquinone imine (NAPQI), which is very toxic but is
generally detoxified by glutathione and converted into nontoxic
compounds.
• Large doses of acetaminophen saturate the main route of metabolism,
causing more acetaminophen to be converted to NAPQI.
• Liver injury occurs once glutathione becomes depleted and NAPQI is
allowed to accumulate.
• Healthy adults should not take more than 4 g (4000 mg) of
acetaminophen in a 24-hour period.

Opioid Analgesics
• potent analgesics
• used in dentistry in combination with acetaminophen, aspirin, or
ibuprofen
• activate mu opioid receptors located at several important sites in the
brain
• Activation of these receptors inhibits the transmission of nociceptive
signals from the trigeminal nucleus to higher brain regions
• opioids also activate peripheral opioid receptors located in dental pulp
• Intraligamentary injection of morphine has been shown to significantly
reduce pain in endodontic patients and other inflammatory pain states
• Adverse side effects, which can include nausea, emesis, dizziness,
drowsiness, and the potential for respiratory depression and constipation.

A combination formulation is preferred because it permits a lower dose of
the opioid, thereby reducing side effects
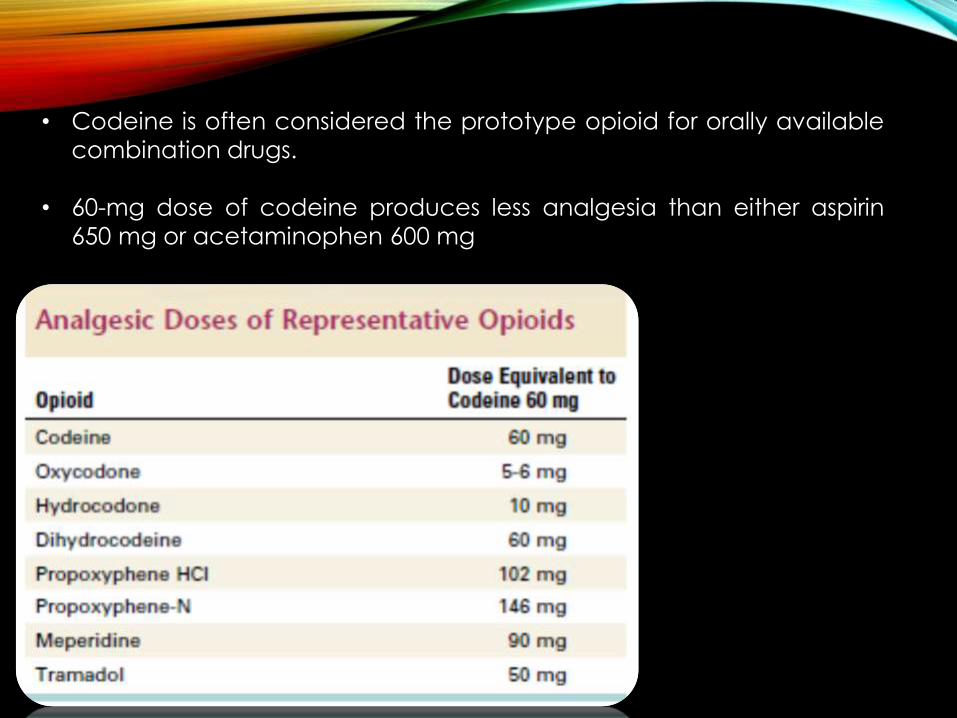
• Codeine is often considered the prototype opioid for orally available
combination drugs.
• 60-mg dose of codeine produces less analgesia than either aspirin
650 mg or acetaminophen 600 mg
PART II
CORTICOSTEROIDS
• Corticosteroids contain 21 carbon atoms in a four memberedhydrocarbon ring system.
• They comprise glucocorticoids and mineral corticoids.
• Glucocorticoids have been used in endodontics for their potent anti-inflammatory effects.
• The anti-inflammatory properties of glucocorticoids were firstappreciated and utilized as an adjunct in endodontic therapy almosthalf a century ago.
• Glucocorticoids have been used as an intracanal medication eitheralone or in combination with antibiotics/ antihistamines, and systemicallyas a means to decrease pain and inflammation in endodontic patients
• Glucocorticoids have effects on carbohydrate, protein and fat metabolism, and other activities that are inseparably linked to these.
• Actions include-
• Carbohydrate & protein metabolism- promote glycogen deposition in liver, increase uric acid secretion, maintains blood glucose levels during starvation so that brain continues to get its nutrients.
• Fat metabolism- promote lipolysis, subcutaneous tissue over extremities loses fat- moon face, fish mouth, buffalo hump
• Calcium metabolism- inhibit intestinal absorption and enhance renal excretion of calcium
• Water excretion- maintain normal GFR
• CVS- restrict capillary permeability, maintain tone of arterioles and myocardial contractility.

• Skeletal muscles- optimum level needed for normal muscular activity-
Hypocorticism- diminished work capacity and weakness due tohypodynamic circulation
Hypercorticism- muscle wasting and myopathy weakness
• CNS- pharmacological doses- mild euphoria- insomnia, anxiety or depression
• Stomach- aggrevate peptic ulcer
• Inflammatory responses- irrespective of type of injury, inflammatory response suppressed.
• Action is non-specific, reduction of increased capillary permeability, local exudation, cellular infiltration, phagocytic activity and late responses like capillary proliferation, collagen deposition, fibroblastic activity and scar formation, limits recruitment of inflammatory cells at local site.
• Post treatment pain or flare-up after endodontic treatment
inflammation, infection, or both in the periradicular tissues.
• Establishing patency and subsequently debriding and shaping theroot canal system irritate the periradicular tissues introduce
bacteria, bacterial products, necrotic pulp tissue, or caustic irrigating
solution through apical foramina.
• In response to this irritation inflammatory mediators (e.g.,
prostaglandins, leukotrienes, bradykinin, platelet-activating factor,substance P, etc.) released into the tissues surrounding the apical
area of the tooth.
• Pain fibers are directly stimulated or sensitized, and an increase in
vascular dilation and permeability results in edema and increased
interstitial tissue pressure.

Glucocorticosteroids reduce the acute inflammatory response by
• suppressing vasodilation,
• migration of polymorphonuclear (PMN) leukocytes
• phagocytosis
• inhibiting formation of arachidonic acid from neutrophil andmacrophage cell membrane phospholipids, thus blocking the COXand lipoxygenase pathways and respective synthesis of PGs andleukotrienes.

• Wolfson and Blitzer stated that hydrocortisone as an intracanalmedication resulted in reduction and elimination of inflammatoryreactions in periapical tissues.
• Ehrmann reported that ledermix (triamcinolone dimethylchlorotetracycline in a water soluble cream) stopped the painassociated with pericementitis.
• Langeland et al demonstrated that Ledermix as an intracanalmedication eliminated post-endodontic treatment pain within minutesto a few hours after placement.
• Chance et al compared the effect of intracanal meticortelone(prednisolone acetate 2.5%) vs. saline on post-treatment pain in adouble-blind study.
• The results indicated that the corticosteroid was effective significantly inreducing the incidence of pain in vital teeth when compared to saline.
• However, there was no difference between the two solutions in necroticteeth.

Ledermix• Ledermix is a paste that combines 1% triamcinolone acitonide (a
corticosteroid) and demethylchlorotetracycline(demeclocycline, a tetracycline analog).
• Used as a pulp capping agent, and as a root canal medicamentfor both vital and necrotic cases because of its anti-inflammatoryand antimicrobial properties.
• Both components of Ledermix can diffuse into dentin andthrough the apical foramen.
• The concentration of demeclocycline in the root canal wasshown to be much higher than is required to inhibit bacteria;however, this activity tends to decrease considerably by 7days.
• It may be combined with calcium hydroxide at a 50:50 ratio toenhance its antimicrobial efficacy, but this tends to reduce thediffusion of its main ingredients.
• Efficacious against pulpal pain in some earlier studies, possiblybecause of its corticosteroid content; however, pulp capping forpainful cases with pulp exposures is not currently recommendedbecause of its low long-term prognosis.
• In a randomized clinical trial to compare Ledermix withformocresol and calcium hydroxide used as interappointmentmedicaments on postinstrumentation flare-ups, no differenceswere detected among the three medicaments.
Intracanal Administration
• In 50 consecutive patients requiring nonsurgical root canal treatment of
vital teeth, one investigator alternately placed a dexamethasone
solution or saline placebo as intracanal medicaments after the root
canals had been cleaned and shaped.
Pretreatment pain ratings were collected, and at 24, 48, and 72 hours after
treatment.
Results indicated a significant reduction in pain at 24 hours but no,
significant difference at 48 and 72 hours.
Intracanal steroids appear to have significant effects for reducing
postoperative pain.
Moskow A, et al: Intracanal use of a corticosteroid solution
as an endodontic anodyne. Oral Surg Oral Med Oral Pathol
58:600, 1984.

Systemic Administration
In one double-blind, randomized, placebo-controlled study,
dexamethasone (4 mg/ml) or saline was injected intramuscularly at the
conclusion of a single-visit endodontic appointment or at the first visit of
a multivisit procedure.
Results indicated that the steroid significantly reduced the incidence
and severity of pain at 4 hours when compared with the placebo.
Pain was reduced at 24 hours, but it was not statistically significant, and
no difference in incidence or severity was seen at 48 hours
106 patients with irreversible pulpitis and acute periradicular
periodontitis were given an intraoral intramuscular injection of
dexamethasone at different doses, either on completion of a single-visit
endodontic treatment or after the first visit of a multivisit procedure.
Systemic administration of dexamethasone was shown to significantly
reduce the severity of pain at 4 and 8 hours, with an optimum dose
between 0.07 and 0.09 mg/kg.
No significant reduction in the severity of pain was noted at 24, 48, and
72 hours, and no overall effect was seen on the incidence of pain.
Another study compared the effect on intraligamentary injection of
methylprednisolone, mepivacaine, or placebo in preventing
posttreatment endodontic pain.
The results showed methylprednisolone significantly reduced
postoperative pain within a 24-hour follow-up period
In a double-blind placebo controlled study, patients with irreversible
pulpitis were given 4 mg of dexamethasone or placebo by means of a
supraperiosteal injection at the apex of the treated tooth following
pulpectomy.
This is an injection technique that most clinicians would be familiar with (as
opposed to intramuscular injection).
Posttreatment pain was significantly reduced in the steroid group during
the first 24 hours. There was no difference at 48 hours.

Collectively, these studies on systemic steroid administration indicate that
corticosteroids reduce the severity of posttreatment endodontic pain
compared with placebo treatment.
‘However, given the relative safety/efficacy relationship between steroids
and NSAIDs, most investigators choose an NSAID as the drug of first choice
for postoperative pain control.’

PART III
ANTIBIOTICS
Endodontics in the adult patient: the role of antibioticsL.P. Longmana, A.J. Preston, M.V. Martin, N.H.F. Wilson
Journal of Dentistry 28 (2000) 539–548

• The first reported local use of an antibiotic in endodontics was in1951 when Grossman used a polyantibiotic paste known as PBSC (amixture of penicillin, bacitracin, streptomycin, and caprylatesodium).
• PBSC contained penicillin to target Gram-positive organisms,bacitracin for penicillin resistant strains, streptomycin for Gram-negative organisms, and caprylate sodium to target yeasts - thesecomponents were suspended in a silicone vehicle.
• Later, Nystatin replaced caprylate sodium as an antifungal agent ina similar medicament, known as PBSN.

Bacteria are involved in endodontic cases with apical periodontitis, the
incidence of a posttreatment infection or flare-up is a concern to clinicians
providing endodontic treatment.
Use of antibiotics is controversial for several reasons.
1. overprescribing antibiotics, especially when these drugs are notindicated, has led to increased bacterial resistance and patient
sensitization.
2. antibiotics have been mistakenly prescribed for patients with
severe pain who have a vital tooth (i.e., when bacteria are
unlikely to be a causative factor in periradicular pain).
3. even when bacteria are likely to be present, data fromcontrolled clinical trials provide little or no support for the hypothesis
that antibiotics reduce pain.

• Antibiotic usage in endodontic therapy is almost totally empirical
driven by opinion and medico-legal concerns.
• The rational use of antibiotics is based upon three variables:
- a defined indication
- the appropriateness of the antibiotic, and - the adverse effects associated with the drug.
Antibiotics are prescribed in endodontic practice for either therapeutic
or prophylactic purposes.

Penicillins
• Penicillins have a short half-life, limited to about 1 hour.
• Amoxicillin is generally considered the penicillin of first choicebecause of its somewhat better absorption from the gut.
• Also used for periodontal abscesses, periapical abscesses,pericoronitis, acute suppurative pulpitis, necrotizing ulcerativegingivitis, oral cellulitis etc
• Less active against Shigella and H.influenza
• Majority of cases resolve with 250-500 mg TDS given for 5 days.

Cephalosporins
• Obtained from fungus Cephalosporium.
4 generations-
First generation- high activity against gram +ve, weak against gram –ve
• Cefazolin, cephalexin, cephradine, cefadroxil
Second generation- more active against gram -ve
• Cefaclor, cefuroxime
Third generation- highly augmented activity against gram –veenterobacteriaceae, some inhibit pseudomonas, less active on grampositive cocci and anaerobes
• Cefixime, cefdinir, cefotaxime, ceftizoxime, cefoperazone
Fourth generation- highly resistant to B-lactamases, active against manybacteria resistant to earlier drugs. P.aeruginosa and staph.aureus alsoinhibited.
• Cefepime, cefpirome
• All bactericidal, same mechanism of action as penicillin, i.e inhibition ofbacterial cell wall synthesis.
Metronidazole
• Metronidazole (Flagyl®) is also considered a bactericidal drugbecause of its fast killing time.
• It attacks the bacteria’s DNA and works against obligateanaerobes but not against facultative bacteria or aerobes.
• Metronidazole is often used in combination with anotherantibiotic, usually amoxicillin, to combat the stomach ulcer–causing Helicobacter pylori.
• Combination helps in severe dental infections
• Metronidazole shares properties with disulfiram (Antabuse®), adrug used to help alcoholics avoid alcohol by inducing violentvomiting.
Patients taking metronidazole should be cautioned about notusing alcohol for the time they are taking the drug plus 1 dayfollowing to allow the drug to be eliminated from their system.
• The half-life of metronidazole is in the 8- to 10-hour range. Sideeffects include an unpleasant, metallic taste and browndiscoloration of the urine, effects that are dose related.

Macrolides
• Erythromycins kill bacteria by slowing the manufacture of bacterialprotein but do not alter the rate of human protein synthesis.
• Alternative to penicillin
• Act by inhibiting bacterial protein synthesis
• Narrow spectrum, mostly gram +ve, few gram –ve, highly activeagainst Str.pyogens, Str.pneumonia, N.gonorrhoeae etc
• Acid labile, enteric coated tablets to protect it from gastric acid,crosses serous membranes and placenta but not blood brainbarrier.
• Plasma t1/2 is 1.5 hours
• Dose- 250-500 mg 6 hourly
• Adverse effects- GIT- diarrhoea, epigastric pain, high doses-hearing impairment, hypersensitivity
• Second choice drug to penicillins in dental infections, valuable topatients allergic to penicillins

Azithromycin- expanded spectrum, better tolerability, improvedpharmacokinetics.
• More active than other macrolides against H.influenza,Peptostreptococcus, Clostridia
• Less active against gram +ve cocci
• Acid stability, rapid oral absorption, marked tissue distribution andintracellular penetration.
• Absorption decreased by food
• Dose- azithral 500 mg once daily 1 hour before or 2 hours afterfood for 3 days is sufficient for most infections
• Mild gastric upset, abdominal pain, headache and dizziness
Clindamycin (Cleocin®)
often indicated in endodontic infections.
• It is rapidly and completely absorbed and has a good spectrum ofkilling oral pathogens, including many anaerobes.
• It was, however, the first antibiotic to be associated with causingpseudomembranous colitis, a life-threatening condition in whichlarge patches of gut slough epithelium because of toxins fromovergrowth of the nonsusceptible organism Clostridium difficile.
• The average half-life of clindamycin is about 3 hours.
Tetracyclines
• Tetracyclines, including tetracycline-HCl, minocycline,demeclocycline and doxycycline, are a group of broad-spectrumantibiotics that are effective against a wide range ofmicroorganisms.
• Bacteriostatic in nature.
• This property may be advantageous because, in the absence ofbacterial cell lysis, antigenic byproducts such as endotoxin are notreleased.
• Inhibition of mammalian collagenases, which prevent tissuebreakdown.
• Inhibition of clastic cells, which results in anti-resorptive activity
• In endodontics, tetracyclines have been used to remove the smear layer from instrumented root canal walls, for irrigation of retrograde cavities during periapical surgical procedures, and as anintracanal medicament.

• Barkhordar et al. evaluated the effect of doxycycline-HCl on thesmear layer of instrumented root canal walls. They showed thatdoxycycline-HCl eliminated smear layer in a concentrationdependent manner with 100 mg/ml doxycycline being moreeffective than lower concentrations.
• In another investigation, Haznedaroglu and Ersev used scanningelectron microscopy (SEM) to assess the effect of tetracycline-HCl asan endodontic irrigant in removing the smear layer. They reportedthat tetracycline was as effective as citric acid in removing thesmear layer.
• Barkhordar and Russell evaluated the effect of doxycycline on theapical penetration of dye through the margins of retrograde fillings.The teeth with retrograde IRM or amalgam fillings placedsubsequent to doxycycline irrigation had significantly less dyepenetration than those that were not irrigated with doxycycline.

• Carson et al. used an agar diffusion test to compare theantimicrobial activities of 6% and 3% sodium hypochlorite(NaOCl) solutions, 2% and 0.12% chlorhexidine gluconate (CHX),and 0.01% and 0.005% doxycycline (Doxy) on fourmicroorganisms associated with endodontic infections of teeththat had not been previously treated, namelyPeptostreptococcus micros, Prevotella intermedia,Streptococcus sanguis, and Lactobacillus acidophilus.
For the first three of these organisms, the general order ofantimicrobial effectiveness was
0.01% Doxy >0.005% Doxy >6% NaOCl >3% NaOCl >2% CHX > 0.12%CHX
However, for L. acidophilus, the order of effectiveness was
6% NaOCl >3% NaOCl >2% CHX > 0.01% Doxy >0.005% Doxy >0.12%CHX.
• Pinheiro et al. evaluated the antibiotic susceptibility ofEnterococcus faecalis isolates from canals of root-filledteeth with periapical lesions.
• The antibiotics were benzylpenicillin, amoxicillin, amoxicillinwith clavulanic acid, erythromycin, azithromycin,vancomycin, chloramphenicol, tetracycline, doxycycline,ciprofloxacin and moxifloxacin.
• The vast majority (85.7%) of the isolates were susceptible totetracycline and doxycycline.
• Chai et al. investigated the antimicrobial efficacy of six groups of
antibiotics (ampicillin co-trimoxazole, erythromycin,
oxytetracycline, vancomycin, and vancomycin followed b
gentamicin) and calcium hydroxide agains Enterococcus
faecalis biofilm in a membrane filter model.
• They concluded that erythromycin, oxytetracycline and Ca
(OH)2 were 100% effective in eliminating the E. faecalis biofilm,
whereas ampicillin, co-trimoxazole, vancomycin, and
vancomycin followed by gentamicin were ineffective.

Based on the hypotheses that microorganisms can reach the apicalarea of recently replanted teeth from the oral cavity (or fromcontaminated root surfaces during the extra-oral time), and thattetracyclines can potentially inhibit this route of bacterialcontamination, Cvek et al. developed a protocol for the topicaltreatment of exposed roots with doxycycline before replantation.
• Aim was to eliminate the microorganisms from the root surface ofan avulsed tooth via direct local application of the antibiotic inorder to decrease the frequency and severity of the inflammatoryresponse.
• Topical doxycycline significantly increased the chances ofsuccessful pulp revascularization and decreased the number ofmicroorganisms that could be isolated from the root canals.
• They also reported a decreased frequency of ankylosis, externalreplacement resorption and external inflammatory resorption.
• The beneficial effect of soaking a tooth in doxycycline has alsobeen confirmed by Yanpiset and Trope
Substantivity of tetracyclines
• Tetracyclines readily attach to dentine and are subsequentlyreleased without losing their antibacterial activity.
• This property creates a reservoir of active antibacterial agent, whichis then released from the dentine surface in a slow and sustainedmanner.
• Stabholz et al. compared the antibacterial substantivity of twoconcentrations of tetracyclineHCl (50 mg/ml, 10 mg/ml) and 0.12%chlorhexidine.
• Their findings showed that both concentrations of tetracyclinedemonstrated residual antibacterial activity and the antibacterialsubstantivity of the three solutions in descending order was: 50mg/ml tetracycline >10 mg/ml tetracycline > 0.12% CHX.
• Abbott et al. demonstrated that tetracyclines form a strong reversible bond with the dental hard tissues and that they exhibit slow release over an extended period of time up to at least 12 weeks.

BioPure (MTAD)
• Bio Pure (Dentsply, Tulsa Dental, Tulsa, OK, USA), otherwise known asMTAD (mixture of tetracycline, acid and detergent), is a relativelynew root canal irrigant which was introduced by Torabinejad andJohnson in 2003.
• This solution contains 3% doxycycline (at a concentration of 3%),citric acid (4.25%) and a detergent, Polysorbate 80 (0.5%).
• Several studies have evaluated the effectiveness of MTAD fordisinfection of root canals.
• Torabinejad et al have shown that MTAD is able to remove thesmear layer and is effective against E. faecalis.
• Shabahang et al. cleaned and shaped root canals of extractedhuman teeth and exposed them to human saliva. They thencompared the antibacterial efficacy of a combination of 1.3%NaOCl as a root canal irrigant and MTAD as a final rinse with that of5.25% NaOCl. Their findings showed that using MTAD in addition to1.3% NaOCl was more effective at disinfecting root canals thanusing 5.25% NaOCl alone.
• Tay et al. found that when MTAD was applied to 1.3% NaOCl-irrigated dentine, its antimicrobial substantivity was reduced. Theyattributed this to the oxidation of MTAD by NaOCl in a mannersimilar to the peroxidation of tetracycline by reactive oxygenspecies.
• Shabahang and Torabinejad compared the antibacterial effectsof MTAD with those of NaOCl and EDTA by using standard in vitromicrobiological techniques and they reported that MTAD wassignificantly more effective against E. faecalis.

• Kho and Baumgartner compared the antimicrobial efficacy of 1.3%NaOCl /MTAD against E faecalis with that of the combinedalternate use of 5.25% NaOCl and 15% EDTA for root canalirrigation.
• This investigation showed consistent disinfection of infected rootcanals when a combination of 5.25% NaOCl and 15% EDTA wasused.
• However, the combination of 1.3% NaOCl/ MTAD left nearly 50% ofthe canals contaminated with E. faecalis.
• Mohammadi and Yazdizadeh evaluated the substantivity of NaOCl,CHX and MTAD substantivity of MTAD was significantly greater thanCHX and NaOCl.
Tetraclean
• Tetraclean (Ogna Laboratori Farmaceutici, Muggiò(Mi),Italy), like MTAD, is a mixture of an antibiotic, an acid and adetergent. However, the concentration of the antibiotic,doxycycline (50 mg/ml), and the type of detergent(polypropylene glycol) differ from those of MTAD.
• Giardino et al.compared the surface tension of 17% EDTA,Cetrexidin, Smear Clear, 5.25% NaOCl, MTAD andTetraclean.
• The NaOCl and EDTA had the highest surface tension,whereas Cetrexedin and Tetraclean had the lowest values.
• In another study, they compared the antimicrobial efficacyof 5.25% NaOCl, MTAD, and Tetraclean against an E.faecalis biofilm generated on cellulose nitrate membranefilters.
• Only the NaOCl could disaggregate and remove the biofilmat every time interval tested although treatment withTetraclean caused a high degree of biofilm disaggregationat each time interval when compared with MTAD.
Combination of Ledermix and calcium hydroxide
• The combination of Ledermix paste with calcium hydroxide wasadvocated by Schroeder initially for the treatment of necroticteeth with incomplete root formation.
• A 50:50 mixture of Ledermix paste and calcium hydroxide has alsobeen advocated as an intracanal dressing in cases of infectedroot canals.
• It has been shown that the 50:50 mixture results in slower releaseand diffusion of the active components of Ledermix paste, whichmakes the medicament last longer in the canal.
• This in turn helps to maintain the sterility of the canal for longer andalso maintains a higher concentration of all components within thecanal.
• Seow showed that for Streptococcus sanguis and S. aureus, the
addition of only 25% by volume of Calyxl (a calcium hydroxide in
saline paste) (Otto and Co. Frankfurt, Germany) to Ledermix
converted the zone of complete inhibition originally seen in
Ledermix to one of only partial inhibition.
• Chu et al. compared the efficacy of disinfection of root canals
with periapical radiolucencies when treated with either
antibiotics/ steroid medicaments (Ledermix or Septomixine) or acalcium hydroxide paste (Calasept, Speiko, Darmstadt,
Germany).
• Their finding showed that in the Ledermix group, 38 strains of
bacteria were recovered. The Septomixine group had 25 strains,
and the Calasept group had 25 strains.
• Gram-positive facultative anaerobic cocci (includingstaphylococci and streptococci) were more prevalent than the
gram-negative obligate anaerobic rods after treatment in all
three groups.
Septomixine Forte• Septomixine Forte (Septodont, Saint- Maur, France) contains two
antibiotics: Neomycin and Polymixin B sulfate.
• Tang et al. who demonstrated that a routine one-week
application of Septomixine Forte was not effective in inhibiting
residual intracanal bacterial growth between appointments.
• In addition, although the anti-inflammatory (corticosteroid) agent,
dexamethasone (at a concentration of 0.05%), is clinically
effective, triamcinolone is considered to have less systemic side
effects.

Triple antibiotic paste• The infection of the root canal system is considered to be a
polymicrobial infection, consisting of both aerobic an anaerobic
bacteria.
• Because of the complexity of the root canal infection, it is unlikelythat any single antibiotic could result in effective sterilization of the
canal.
• More likely a combination would be needed to address the diverse
flora encountered.
• A combination of antibiotics would also decrease the likelihood of
the development of resistant bacterial strains.
• The combination that appears to be most effective consists of
metronidazole ciprofloxacin, and minocycline.
• Sato et al. evaluated the potential of a mixture of ciprofloxacin,metronidazole and minocycline to kill bacteria in the deep layers
of root canal dentine in situ.
• Results showed that no bacteria were recovered from the
infected dentine of the root canal wall 24 h after application of
the drug combination, except in one case in which a few
bacteria were recovered.
• Hoshino et al. investigated the antibacterial effect of a mixture of
ciprofloxacin, metronidazole, and minocycline with and without
the addition of rifampicin, on bacteria from infected dentine of
root canal walls.
• The efficacy was also determined against bacteria of carious
dentine and infected pulps, which may the precursory bacteria of
infected root dentine.
• They found that alone, none of the drugs resulted in complete
elimination of bacteria. However, in combination; these drugs
were able to consistently sterilize all samples.
• Iwaya et al. reported a necrotic immature mandibular second
premolar with periapical involvement and sinus tract.
• Instead of the standard root canal treatment protocol and
apexification, antimicrobial agents (metronidazole andciprofloxacin) were used in the canal, after which the canal was
left empty.
• Radiographic examination showed the start of apical closure five
months after the completion of the antimicrobial protocol.
• Thickening of the canal wall and complete apical closure was
confirmed 30 months after the treatment, indicating therevascularization potential of a young permanent tooth pulp into a
bacteria-free root canal space.
Takushige et al. evaluated the efficacy of polyantibiotic paste
consisted of metronidazole, ciprofloxacin, and minocycline, on the
clinical outcome of so-called “Lesion Sterilization and Tissue Repair,”
(LSTR) therapy in primary teeth with periradicular lesions.
Results showed that in all cases, clinical symptoms such as gingival
swelling, sinus tracts, induced dull pain, spontaneous dull pain, and
pain on biting disappeared after treatment, although in four cases
clinical signs and symptoms were finally resolved only after
retreatment using the same procedures.
Thus, gingival abscesses and fistulae, if present, disappeared after a
few days.

Endodontics and therapeutic antibiotics
a. Adjunct to operative treatment
In healthy patients endodontic infections can be treated solely by the
early establishment of drainage and removal of the cause of the
problem, for example, debridement of the infected root canal system or
surgical removal of extraradicular infection.
1. In acute dentoalveolar infections antibiotics may be indicated
because there is a diffuse spreading infection or evidence of systemic
involvement.
Antibiotics are not an alternative to dental intervention; they are an
adjunct to it
2. In medically compromised patients host-defence mechanisms may
be thought to be inadequate the operative treatment of acute
dentoalveolar infections may sometimes be supplemented with
therapeutic antibiotics.
3. A patient’s resistance to infection may be reduced by medication
(e.g. corticosteroids, antimetabolites), systemic disease such as
leukaemia, HIV or poorly controlled Type I diabetes
b. Contingency treatment
On rare occasions, it may not be possible to obtain drainage or remove the
cause of infection by operative treatment.
There is no evidence that the use of antibiotics in this situation is of any
benefit; definitive treatment is required.
The principle purposes of prescribing are to: limit the local spread of
infection, treat systemic infection and bring about symptomatic relief
Examples1. Patient has cellulitis associated with an acute periapical infection,originating from a tooth that has a well-retained intraradicular post
drainage of infection cannot be achieved by the incision of the soft tissues
and intracanal instrumentation.
2. Failure to achieve anaesthesia for the extraction of an abscessed tooth
can necessitate a prescription for antimicrobials in acute periapical
infection.
3. When an anxious or phobic patient presents with acute periapical
infection, and cannot accept treatment without the assistance of sedation.
4. Uncooperative patients with physical or learning disabilities may not be
amenable to immediate operative treatment.
c. Antibiotics at obturation
• Anecdotal evidence cites the use of systemic antibiotics at the time of
obturation, when pus remains in the root canal system, despite
repeated inter-appointment dressings.
• There is no scientific evidence that this practice is beneficial.
• Antibiotic therapy has also been suggested for one visit endodontics,
undertaken when there is infection present in the root canal.
• There is no evidence that antibiotics are efficacious in this situation,
the root canal is dressed rather than obturated.

d. Antibiotics for perio-endo lesions
• There are no authoritative studies to support the use of systemic
antibiotics in the management of “perio-endo” lesions.
• The treatment of combined lesions is based upon the basic principles of
endodontic and periodontal therapy, and is dependent upon the
aetiology of the condition.
• Endodontic treatment usually involves root canal treatment, or less
commonly root resection or repair of a perforation.
• Systemic antibiotics are not a substitute for effective mechanical
debridement of the root canal system and root surface.

Which antibiotic?
• At least 70 different bacterial species have been isolated from root
canals and synergistic relationships are thought to exist between them.
• Certain bacteria seem to occur in pairs and these include: Bacteroides
vulgaris and Fusobacterium necrophorum; Peptostreptococcus spp. and
Prevotella spp; P. micros and P. melaninogenica; Prevotella and
Eubacterium ssp.
• The majority of symptomatic, infected root canals contain anaerobes; it
has been proposed that the larger the number of bacterial species
present the more symptoms will be experienced.
• It has also been demonstrated that intracanal flora from teeth with failed
endodontic therapy differs markedly from the root canals of untreated
teeth.
• Empirical prescribing of anti-microbials as part of endodontic management
is problematic, given the diversity of potential pathogens and their differing
drug sensitivities.
• Culture and sensitivity testing is not routinely recommended for endodontic
procedures
The most commonly prescribed antibiotics are erythromycin,
amoxicillin, penicillin and metronidazole
Some anaerobes isolated from the endodontic lesions are resistant to
penicillin and therefore serious infections are treated empirically with a
combination of metronidazole and a penicillin

Duration of antibiotic therapy required for acute dentoalveolar
infections has never been defined precisely.
• Tendency in dental practice to use courses of antibiotics 3–5
days for the treatment of infection .
• There is increasing awareness of the value of the commensalflora in the host’s defence system both in the oral cavity and in
other body sites.
• Prolonged courses of antibiotics destroy the commensal flora
and abolish colonisation resistance.
• The prescribing of systemic antibiotics must therefore be
justifiable.
Few studies on the use of antimicrobials have supported the view that it is
not necessary to complete the course of antibiotics.
• One study has advocated that a two-dose administration of an anti-
microbial agent is as efficacious as a 5 day course in the management
of acute dentoalveolar infections; this was not a double blind placebo
controlled trial.
• Two separate investigations, compared three anti-microbial agents, and
showed that the majority of patients were asymptomatic after 2 days
therapy.
• Majority of patients 2 or 3 days of oral antibiotics, in doses
recommended by the BNF, will suffice for acute dentoalveolar
infections.
• Alternatively, a two-dose regime of 3 g amoxicillin can be used in
patients who are not allergic to penicillin.
• Fazakerley MW, McGowan P, Hardy P, et al.
A comparative study of cephradine, amoxycillin and phenoxymethylpenicillin in the
treatment of acute dentoalveolar infections. British Dental Journal1993;174:359–63.
• Martin MV, Longman LP, Hill JB, et al.
Acute alveolar infections: an investigation of the duration of antibiotic therapy.
British Dental Journal 1997;183:135–7.

Topical antibiotics and endodontics
The limited spectrum of activity of the antibiotic preparations available, the
potential for bacterial resistance, the risk of drug hypersensitivity and the
potential to mask certain aetiological factors limit their
usefulness.
PulpitisThere is no convincing evidence to justify the use of Ledermix (Lederle Lab
Gosport, Hants, UK) to sedate the pulp prior to definitive treatment.
There is no indication for the use of topical antibiotics in the treatment of
pulpitis
Pulp capping
Calcium hydroxide- most popular agent for both direct and indirect pulp
capping.
Anti-bacterial action, stimulates secondary dentine formation.
Ledermix is the most commonly used alternative to calcium hydroxide and
contains a steroid (triamcinolone) and an antibiotic
(demethylchlortetracycline).
Ledermix is a topical preparation, available as either a paste or a cement.

Root canal therapy
• The most important elements of root canal preparation are effective
access and aseptic biomechanical preparation.
• Early investigations evaluated two antibiotic-containing preparations:
Grossman’s polyantibiotic paste, which contains penicillin, bacitracin or
chloramphenicol and streptomycin
• A mixture of neomycin, polymixin and nystatin.
• Both of these had some efficacy as intracanal medicaments.
Perio-endo lesions
Topical antibiotics, such as the tetracyclines or metronidazole, may be
applied by some clinicians, to the periodontal defect as an adjunct to
root planing.

Flare-ups
• Topical antibiotics have been used to reduce post-operative pain and
swelling following root canal preparation; this is often referred to as a
flare- up.
• In the treatment of infected root canals where there is often a need to
carry out the treatment over more than one visit, with an antibacterial
intracanal medicament placed between visits; the intracanal
medicament that is commonly used is calcium hydroxide.
Tooth avulsion
Ledermix has been used as an intracanal medicament in the management
of tooth avulsion, but it is not clear whether the beneficial effect is due to
the action of the steroid or the antibiotic.

Antibiotic prophylaxis and endodontics
Healthy patient
There is no evidence that antibiotic prophylaxis, given to healthy patients
undergoing surgical endodontics is efficacious.
Despite this, antibiotics are sometimes prescribed prophylactically to
prevent infection at the site of surgery.
• Ideally, antibiotics should be given prior to reimplantation.
• Often not possible and could necessitate a delay in tooth replacement,
adversely affecting the prognosis.
• Re-implantation is therefore, one of the rare situations when
chemoprophylaxis may have to be given post-operatively, assuming
there are no medical contraindications
• The re-implantation of teeth should not be considered if the procedure
places the patient at risk from haematogenous spread of infection.
• An example would be a patient with acute leukaemia or HIV infection.
• Once the decision to re-implant has been made, the timing of antibiotic
prophylaxis is critical if serious sequelae are to be avoided.
• It would be logical to administer antibiotic prophylaxis prior to
implantation, to ensure adequate antibiotic serum levels at the time of
operation.

Prophylaxis for the medically compromised
• Patients who are susceptible to IE, or osteoradionecrosis, and those who
have endoprostheses
• Second category is patients with impaired host-defence mechanisms
• These patients are potentially at risk from opportunistic infections.
• Patients who are receiving renal dialysis or have had organ transplants
are included in this group.
Infective endocarditis
• Dental procedures that reliably cause a transient bacteraemia could
result in IE.
• The use of chemoprophylaxis is well established and necessary
medico-legally for surgical endodontics, in patients at risk from IE.

• It is unrealistic and undesirable to give systemic prophylaxis for every
endodontic procedure that may occasionally cause bleeding or a
bacteraemia, including the placement of rubber dam.
• Simple pre-operative mouthrinsing and disinfection of the gingival tissues
with chlorhexidine reduces the magnitude of a bacteraemia
• Elective endodontic procedures should be avoided wherever possible, in
patients who have a damaged endocardium and concomitant gingival
inflammation.
Radiotherapy
• After radiotherapy, there is a diminution of the vascular supply in the
irradiated area especially in the mandible.
• This is a progressive risk that does not reduce with time
• Risk of infection is much greater with exodontia than root canal therapy,
consequently non-surgical endodontics is the preferred treatment for a
necrotic pulp in irradiated patients.
Prosthetic implants• The prophylactic antibiotics should target the putative pathogens,
staphylococci and to a lesser extent oral streptococci
• Patients with cardiac pacemakers, intraocular lenses, breast implants,
penile implants and prosthetic vascular grafts are not considered to be
especially susceptible to infection from dental bacteraemias.
• The use of antibiotic prophylaxis in patients with intravascular access
devices and CSF shunts is contentious.
• Neurosurgeons are more likely to recommend prophylaxis for patients
with ventriculoatrial shunts, than for the more commonly used
ventriculoperitoneal shunts
Immunocompromised patients
• Patients who are immunocompromised, including patients who
have organ transplants or indwelling intraperitoneal catheters,
do not require antibiotic prophylaxis for dental treatment.
• It can be concluded, therefore, that endodontic treatment
does not require antibiotic prophylaxis.
Systemic antibiotics should normally only be prescribed to treat dental
infections on the basis of a defined need.
• The potential benefits of antibiotic administration should therefore
outweigh the possible disadvantages associated with their use.
• A dentist who prescribes an antibiotic for a questionable indication
may be seen as placing a patient at risk from potential adverse effects
of drugs.

PART IV
LOCAL ANESTHETICS

Local anesthetics (CLASSIFICATION): Injectable
a. Short duration (30 minutes of pulpal anesthesia)-
Procaine
b. Intermediate duration (60 minutes of pulpal anesthesia)-
Lignocaine, prilocaine
c. Long duration (over 90 minutes of pulpal anesthesia)-
Tetracaine, bupivacaine, ropivacaine, dibucaine
Surface anestheticSoluble
Cocaine
Lignocaine
Tetracaine
Benoxinate
Insoluble
Benzocaine
Butylaminobenzoate ( Butamben)

Lignocaine (lidocaine)
• Most widely used
• Surface application and injectable
• Blocks nerve conduction in 3 mins whereas procaine may takeupto 15 mins
• Overdose causes muscle twitching, convulsions, cardiacarrhythmias, fall in BP, coma, respiratory arrests
• Dental use- 2% with or without adrenaline 1:80,000
Mepivacaine
• Available in formulation containing levonordefrin, an adrenergic agonist, 1:20000 conc.
Articaine
• 4% solution containing 1:100,000 and 1:200,000 epinephrine
• Amide anesthetic that contains thiophene ring and ester linkage.
• Maximum dose is 7 catridges compared to 13 catridges of 2% lidocaine
• Potential to cause methemoglobinemia and neuropathies

Bupivacaine and etidocaine
• Prolonged pain control, long acting
• Etidocaine withdrawn from market recently
• Bupivacaine exhibits prolonged soft tissue numbness or lip sign
• Slower onset than lidocaine but twice the duration of action (around 4 hours) in mandible
Ropivacaine
• Structural homologue of bupivacaine that appears to have a lower potential for CNS and CV toxic effects.

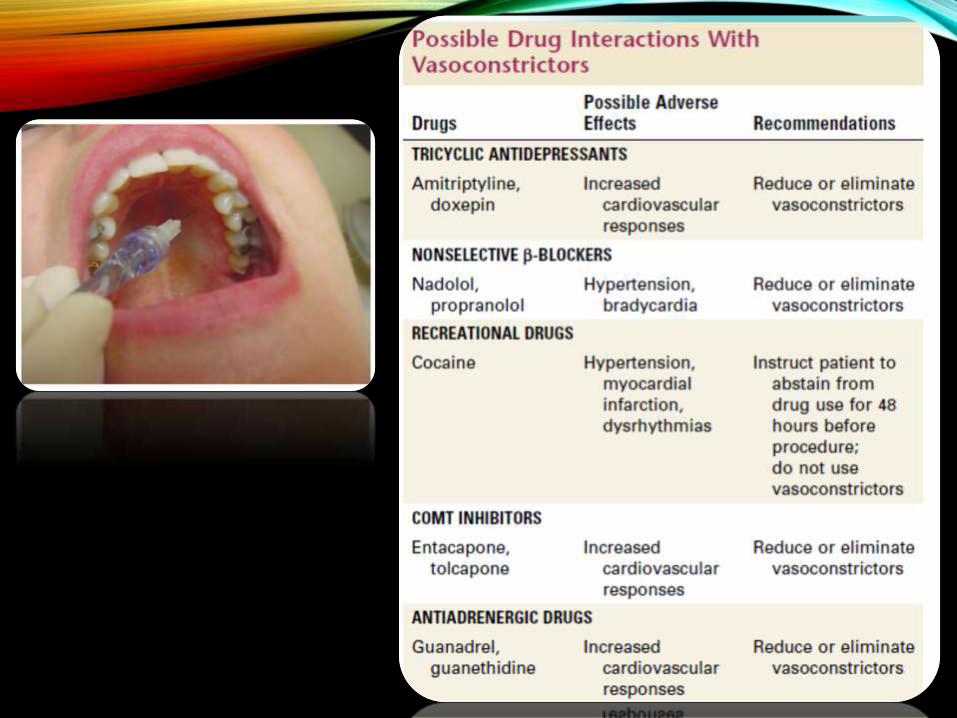
• Cardiac patients (e.g., those with unstable angina pectoris, history of
myocardial infarction or stroke within the past 6 months, severe
hypertension, uncontrolled congestive heart failure, or heart transplant)
should not receive a local anesthetic containing a vasoconstrictor and
should consult their physicians before undergoing endodontic treatment.
• Local anesthetics may interact with a patient’s medications
• Thorough review of the medical history is an absolute requirement.
• Potential drug-drug interactions occur primarily with the vasoconstrictors
in local anesthetic formulations.
• Judicious use of local anesthetic solutions without vasoconstrictors (e.g.,
3% mepivacaine) is a reasonable alternative for adult patients.

PART V
ANTIMICROBIAL AGENTS
Antimicrobial agents may be disinfectants and antiseptics that
destroy or inhibit the growth of microorganisms and thereby prevent
infection by pathogenic or potentially pathogenic microorganisms.Disinfectants are used on inanimate objects or surfaces, whilst
antiseptics are used on living tissues.
McDonnell G, Russell AD. Antiseptics and disinfectants:
activity, action, and resistance. Clinical Microbiology
Reviews 1999;12:147–79.
Conventional antiseptics 1. Alcohols – Ethyl alcohol, Isopropylalcohol
2. Phenolic Compounds – Camphorated phenol,
Monochlorophenol, Thymol, Cresol, Creosote
3. Heavy Metal Salts
4. Cationic Detergents – Quarternary ammonium compounds
5. Halogens – Hypochlorite, Chloramine T, Iodine, Iodophores
ChemotherapeuticsAntibiotics
Classification of antimicrobial agents.
• The mechanism of action of antimicrobial agents is varied as theyhave multiple sites of action except for antibiotics, which havevery specific sites of action.
• The nature of the organism, antimicrobial agent and theconcentration determine the response of the microorganisms tothe antimicrobials.
• The cell wall, cytoplasmic membrane and ribosomes ofvegetative cells, the coat and cortex of bacterial spores,envelope and capsid of viruses and proteins (structural proteins,enzymes), nucleic acids and polysaccharides are some of thesites of action of antimicrobial agents.
• These antimicrobial actions eventually result in the loss ofimportant cell functions like protein synthesis and metabolism,replication, transcription and destruction of cell membranes withleakage of cell contents
Mechanism of action
• The two most important features which determine the efficacy ofantimicrobial agents are the killing and the cleaning potential ofthe agent.
• The antimicrobial activity may vary from inhibition of metabolismto destruction of the microorganisms.
• The specific target of action of antimicrobials is difficult toelucidate as antimicrobial agents act on multiple cellcomponents, resulting in both primary and secondary effects,which in turn is hard to distinguish.
Sodium hypochlorite
• Concentrations ranging from 0.5 % to 5.25 %.
• This is due to its antimicrobial and dissolving effects onnecrotic tissues (Sodium hypochlorite is a reducing agentwith 5 % of available chlorine
• lubricant, antiseptic agent, bleach and also dissolves tissue
• Antibactericidal ability of NaOCl results from the formationof hypochlorous acid (HOCl) when in contact with organicdebris.
• HOCl exerts its effect by the oxidation of sulphydryl groupswithin bacterial enzyme systems, thereby disrupting themetabolism of the microorganism.
• Cvek M et al. in his study reported that flushing with sterilesaline had poor antibacterial action (9 %) when comparedto sodium hypochlorite (25 %)
• The antibacterial action of NaOCl is time dependent.
• In an in vivo study, Ringel et al. noted that in root canals ofpermanent teeth 2.5 % NaOCl had a more powerfulantibacterial effect than 2 % chlorhexidine gluconate, asNaOCl was a powerful solvent for necrotic and organicmaterial.
• Naenni et al reported that only sodium hypochloriteshowed effective necrotic tissue dissolution among 10 %chlorhexidine, 3 % and 30 % hydrogen peroxide, 10 %peracetic acid, 5 % dichloroisocyanurate (NaDCC), and 10% citric acid.
Chlorhexidine gluconate
• Chlorhexidine (CHX) is widely used in periodontal andendodontic treatment as an irrigant.
• There are various mechanisms of antimicrobial action forchlorhexidine.
• It attaches electrostatically to negatively charged sites onbacteria and also to its cytoplasmic membrane.
• The leakage of intracellular material is due to the loss ofosmotic balance by CHX.
• The binding of CHX to hydroxyapatite and soft tissueschanges their electrical field to compete with the binding ofbacteria
Cetrexidin♦ (Vebas, San Giuliano, Milan, Italy)
Antiseptic agent that is being evaluated.
• It consists of 0.2 % chlorhexidine gluconate and 0.2 % cetrimide.
• Cetrimide (cetiltrimethyl ammonium bromide), is a quarterneryammonium compound and a cationic detergent that is effectiveagainst many Gram positive and Gram negative bacteria

• Study on the antimicrobial effectiveness and cytotoxicity of 4irrigant solutions, viz 5.25 % sodium hypochlorite (NaOCl), 0.2 %chlorhexidine gluconate plus 0.2 % cetrimide (CetrexidinR), 2 %chlorhexidine gluconate and 0.9 % sterile saline solutiondemonstrated that NaOCl should remain in the canal for asubstantial period so that it can act upon the bacterial cellslocated in the irregularities within the canal.
• In this study, 5 minutes following the irrigation process,chlorhexidine gluconate had a more rapid and stronger actionon E. faecalis than NaOCl.
Calcium hydroxide
• Calcium hydroxide is the most commonly used inter-appointment intracanal endodontic medicament.
• The publication of research data on the antibacterial action ofcalcium hydroxide in root canal treatment by De Moor & DeWitte led to increased use of calcium hydroxide in endodontictreatment.
• The antibacterial activity is a result of free hydroxyl radicalliberation and diffusion of hydroxyl radicals resulting in a highlyalkaline environment(pH 12.5).
• These hydroxyl ions penetrate the dentinal tubules and exerttheir effect.

• These hydroxyl radicals cause bacterial cell death by threepossible mechanisms.
• The first mechanism is by splitting DNA strands and therebypreventing DNA replication and disrupting cellular activity.
• Another method is by lipid peroxidation, which leads to thedestruction of both phospholipidand cell membrane, finallyresulting in loss of unsaturated fatty acids and massive destructionof membrane.
• The third mechanism is by protein denaturation and damage ofcell metabolism.
• Calcium hydroxide also shows increased activity againstanaerobes in comparison to paramonochlorophenol andformocresol.
Hydrogen peroxide
• The mechanism of action is by the reaction of superoxide ions,resulting in formation of hydroxyl radicals.
• Hydroxyl radicals are strong oxidants and they destroy membranelipids, DNA and other essential cell components.
• The oxidation of sulphydryl groups and double bonds in proteins,lipids, and surface membranes is responsible for the antimicrobialaction.
• In addition, the chloride in the bacteria may be oxidized tohypochlorite when myeloperoxidase enzyme is present.
• Hydrogen peroxide is an oxidizing solution and is usually used incombination with sodium hypochlorite for root canal irrigation.This results in two kinds of reactive oxygen species, the superoxideanion radical (O2 -) and the hydroxyl radical (OH-).

• Root canal irrigation with NaOCl and H2O2 induces both biologicaland mechanical effects.
• The biological effect of NaClO and H2O2 owes to tissue irritationdue to the chemical reactions of O2 - and OH-, while themechanical effect results from O2 bubbling.
• The effervescent action resulting in the release of nascent oxygenresults in the agitation of the root canal contents and the debris isflushed out.
• The tissue dissolution and antimicrobial effect are the main modeof action of the combined solutions.
• The final irrigation of the canal should be done with sodiumhypochlorite, as hydrogen peroxide can form gas in the presenceof necrotic debris and blood leading to pain.
Formocresol
• Formocresol consists of formalin and tricresol in a ratio of 1:1.
• Tricresol is a combination of o-, m-, and p-cresols.
• The application time and the concentration of formocresolinfluence the histologic reaction of vital pulp.
• Formocresol is a bactericidal agent and the mode of action is byfixation, which results in inhibition of bacteria.
• Formocresol causes zones of necrosis, fixation, and inflammation.
• It results in healing with inflammation and eventual replacementwith granulation tissue, bone or osteodentin in some cases.

Ferric sulphate
• 15.5 % used as a haemostatic agent in pulpotomy procedures.
• Landau and Johnsen in 1988
• The mode of action is by the formation of a ferric ion proteincomplex in the presence of blood resulting in the mechanicalsealing of cut vessels by the membrane of this complex.
• This ultimately leads to haemostasis
• Pulpal reaction of ferric sulfate and formocresol did not differfrom each other.
• Ferric sulphate is less toxic than formocresol and hence it may beconsidered as an alternative to formocresol for pulp therapy inprimary molars.
• As ferric sulphate causes only haemostasis, it is a moreappropriate pulpotomy agent and may be considered a goodreplacement for formocresol in pulpotomy.

Peracetic Acid• Peracetic acid has a wide spectrum of antimicrobial action at low
concentration, and within short duration.
• Aqueous solution of peracetic acid (PAA) has high microbicidalactivity against a broad range of microorganisms.
• Peracetic acid is an effective germicide against bacteria, yeast,and viruses at 0.03 % or lower concentration.
• Alasri et al. state that when peracetic acid and hydrogen peroxideare used together, they have a combined action on biofilms owingto the microbicidal activity of peracetic acid and detachment ofbiofilm by hydrogen peroxide.

• The sporicidal action decreased with storage due to hydrolysis ofperacetic acid, whereas it increased with high pH concentration.
• The drawback of high pH concentration is the carcinogenicpotential of 1 % peracetic acid, as it is a tumor promotor.
• The sporicidal action in a study by Jose-Luis and Aylin was asfollows: hypochlorite > peracetic acid > copper ascorbate >glutaraldehyde > peroxide > phenol > formaldehyde.
• Ageing, pH, and temperature were found to greatly influence theorder of the efficacy of these agents
• According to Naenni N et al., among the commonly usedendodontic irrigants like 10 % chlorhexidine, 3 % and 30 %hydrogen peroxide, 10 % peracetic acid, 5 %dichloroisocyanurate (NaDCC), and 10 % citric acid, all hadlower tissue dissolution capacity in comparison to 1 % (wt/vol)sodium hypochlorite (NaOCl).
Chloramine T
• Chloramine T is N-chloro-p-toluensulphonamidesodium.
• It is used as an effective oral antiseptic agent.
• The mode of action is by the conversion of amino acids intoaldehydes, carbon dioxide, ammonia and nitriles.
• Irrigation with a combination of hydrogen peroxide andchloramine, chloramine or glutaraldehyde were moreeffective irrigants than normal saline, 1% metronidazole or3% hydrogen peroxide
Hexetidine1,3-bis(2-ethylhexyl)-5-amino-5-methyl hexahydropyrimidine.
• Hexetidine is a good antibacterial and antifungal agent with awide spectrum of activity both in vivo and in vitro.
• Hexetidine rinse is widely used as an antiplaque andantigingivitis, as it decreases supragingival plaque and gingivalinflammation.
• In vitro and in vivo action against Gram-positive and Gram-negative bacteria as well as yeasts (Candida albicans) is wellknown.
• In addition, it is also used as an astringent, local anaestheticand deodorant.
• It has not been widely used in endodontic treatment.
• Studies on in vitro oral biofilm models demonstrate thatantimicrobials like chlorhexidine, hexetidine, delmopinol,amine fluoride/stannous fluoride, triclosan, and phenoliccompounds interfere with bacterial metabolism and mayinhibit biofilm development and maturation

Aminefluoride
• 38 % diamine silver fluoride, or Ag(NH3)2F, is used as aNd:YAG laser initiator.
• Yokoyama K and co-workers reported that pulsed Nd:YAGlaser or iontophoresis following Ag(NH3)2F increased thepermeability of the root canal wall and occlusion of dentinaltubules.
• Root canals treated using irradiation with an Nd:YAG laserthat has been coated with Ag(NH3)2F solution showedimproved results compared to either iontophoresis aftercoating with Ag(NH3)2F solution, or coating alone.
Cetylpyridinium chloride
• Cetylpyridinium chloride (CPC) is a quaternary ammoniumsalt (C21H38ClN; molecular weight, 358.07) having acombination of hydrophilic and lipophilic affinities.
• CPC is commonly used as a broad-spectrum antimicrobialagainst oral bacteria and with properties and uses typical ofcationic surfactants.
• The primary mechanism of action of CPC is by cellmembrane penetration, which results in leakage of cellcontents, disturbance of bacterial metabolism and inhibitionof cell growth.
• These eventually cause cell death.
• It exhibits surface-active properties.
• Thus the long duration of action is by virtue of the binding ofCPC to the glycoproteins covering the teeth and oralmucosa.

• Cetylpyridinium chloride (CPC) is recognied as an effectiveantiplaque agent and commonly found in oral hygiene aids.
• It is less commonly used in root canal treatment.
• Several animal studies on the cytotoxicity of CPC haveshown it to be a highly safe and effective antimicrobialagent.
• CPC has the distinction of being recognized by the FDAPlaque Subcommittee after a six year review of over 40active ingredients as being one of the only three (stannousfluoride and essential oils – the remaining two safe agents)antimicrobial agents which is safe and effective(concentration range of 0.05 and 0.10 %) for the treatmentof plaque-induced gingivitis.
PART VIIANXIETY AND FEAR IN THE
ENDODONTIC PATIENT
Most common fears of man-
• Fear of height
• Fear of flying
• Fear of mice
• Fear of public speaking
• Fear of dentists
‘Our most common fears.’
Dental health advisor, Spring 1987

• Incidence of dental phobia or ODONTOPHOBIA- 10-30 % of adults,moderate to severe odontophobia
• Fear and pain are a potent combination capable of provokingsome of the most catastrophic situations imaginable in the dentaloffice, such as cardiac arrest.
• Sedation occurs as a result of CNS depression, from minimalsedation to general anesthesia.

• Minimal sedation- ‘anxiolysis’, a minimally depressed level ofconsciousness that retains the persons ability to independentlyand continuously maintain an airway and respond appropriatelyto physical stimulation or verbal command and that is producedby pharmacologic or nonpharmacologic method or acombination thereof.
• Nitrous oxide/oxygen (N2O-O2)
• Moderate sedation- ‘conscious sedation’, drug induceddepression of consciousness during which pateints respondpurposefully to verbal commands, either alone or accompaniedby light tactile stimulation.
• Deep sedation- drug induced depression of consciousness duringwhich patients cannot be easily aroused but respondpurposefully following repeated or painful stimulation.
• Sedation- Iatrosedation- ‘no drugs’ sedation, relaxation of the patient by the dentists behaviour.
• Drug sedation/ techniques-
• Inhalation sedation-
• N20-O2, rapid onset of action, level of CNS depression that can be rapidly increased if necessary, level of CNS depression that can be rapidly decreased if necessary, complete recovery following the delivery of 100% O2 at the completion of procedure- permits the patient to leave the clinic unescorted, no other route of drug administration offers this advantage.
• Because of rapid onset, it can be titrated, which increases both the safety and success of the technique.
• Only disadvantage for endodontists is the nasal hood on the way which is not a problem once experienced.
Oral conscious sedation-
• Least controllable route
• Slow onset of action usually
• Erratic absorption of the drug from the GIT
• Only advantage is easy for dentist and patient
• CNS depressants given night prior to planned appointment, in the morning 1 hr prior to the scheduled dental visit, to assist them in overcoming any last minute increase in their anxiety.
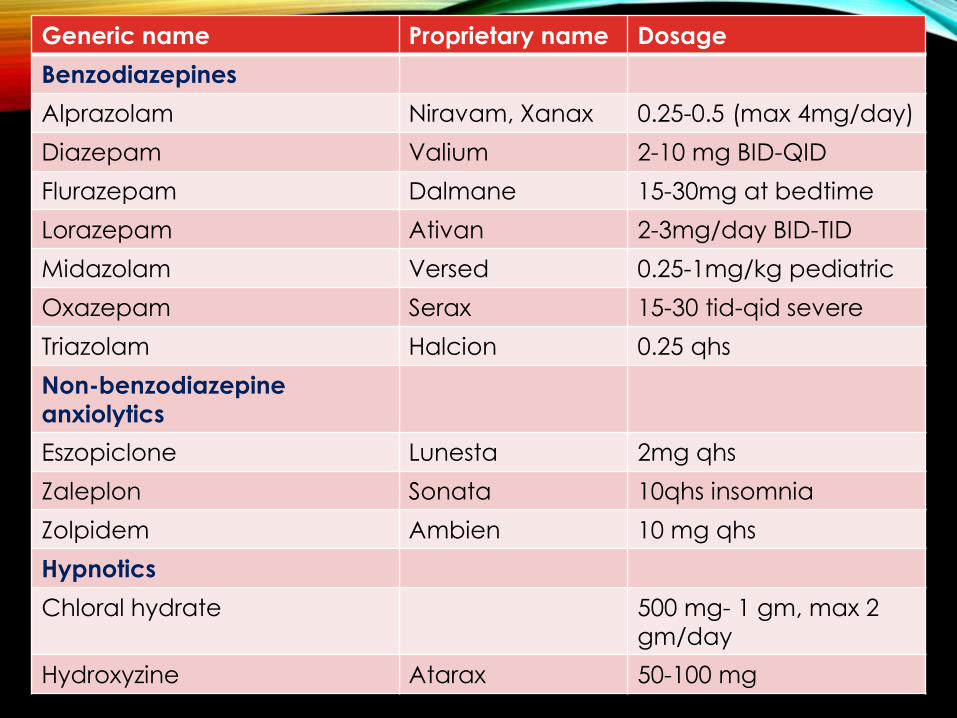
Generic name Proprietary name Dosage
Benzodiazepines
Alprazolam Niravam, Xanax 0.25-0.5 (max 4mg/day)
Diazepam Valium 2-10 mg BID-QID
Flurazepam Dalmane 15-30mg at bedtime
Lorazepam Ativan 2-3mg/day BID-TID
Midazolam Versed 0.25-1mg/kg pediatric
Oxazepam Serax 15-30 tid-qid severe
Triazolam Halcion 0.25 qhs
Non-benzodiazepine
anxiolytics
Eszopiclone Lunesta 2mg qhs
Zaleplon Sonata 10qhs insomnia
Zolpidem Ambien 10 mg qhs
Hypnotics
Chloral hydrate 500 mg- 1 gm, max 2
gm/day
Hydroxyzine Atarax 50-100 mg
Intravenous conscious sedation
• Rapid onset, titration possible to desired level, more safer than oral
• Requires fasting prior to procedure
• Inability to quickly lessen the level of CNS depression
• Inability to reverse the action of some drugs (barbiturates)
• Prolonged clinical recovery
• Benzodiazepines, midazolam, diazepam
• Venipuncture skill required
Intramuscular
• Drug by passes the GI tract, being absorbed directly into the system
• Hepatic first pass effect neglected, leading to more reliableabsorption and more rapid onset of action
• Titration not possible
• Doses decided by weight (mg/kg)
• Reversal done with iv flumazenil or naloxone
• Im not controllable like iv so sedation limited to moderate level,doctor should be trained to recognize and manage the patiententering deep sedation
Intranasal
• Newer technique in dentistry
• More rapid absorption since nasal mucosa is highly vascular
• No injection needed
• Cannot be titrated
• Dosage based on weight
• Sedation limited to moderate, not controllable
• IN midazolam commonly used
General anesthesia
Provided to dentist by an anesthetologist
PART VIIITHE MEDICALLY COMPLEX
ENDODONTIC PATIENT
‘Never treat a stranger.’
- Sir William Osler
• The value of a thorough medical and dental history of a patient
cannot be overemphasized.
• Recognition of a medical condition that requires treatment
modification prior to treatment can avert significant treatment
complications.

ASA Physical Status Classification System & therapy
modifications• ASA Physical Status 1 - A normal healthy patient
No therapy modifications, stress reduction as indicated
• ASA Physical Status 2 - A patient with mild systemic disease
Possible stress reduction and other modifications as needed
• ASA Physical Status 3 - A patient with severe systemic disease
Possible stress modifications, stress reduction and medical consultation are
priorities
• ASA Physical Status 4 - A patient with severe systemic disease that is a
constant threat to life
Minimal emergency care in office, may consist of pharmacologic
management only, hospitalize for stressful elective treatment, medical
consultation urged
• ASA Physical Status 5 - A moribund patient who is not expected to
survive without the operation
Treatment in the hospital is limited to life support only, eg:- airway and
haemorrhage management
• ASA Physical Status 6 - A declared brain-dead patient whose organs are
being removed for donor purposes
Not applicable

Antibiotic prophylaxis recommended, based on risk
stratification for infective endocarditis Highest risk of adverse outcome from infective endocarditis• Prosthetic heart valve
• Previous infective endocarditis
• Congenital heart disease (CHD)
• Unrepaired cyanotic CHD, including palliative shunts and
conduits• Completely repaired congenital heart defect with prosthetic
material or device, whether placed by surgery or catheter,
during the first six months after the procedure
• Repaired CHD with residual defects at the site or adjacent to the
site of a prosthetic patch or prosthetic device
• Cardiac transplant recipients who develop cardiac valvulopathy
Risk of dental procedure-All dental procedures that involve manipulation of gingival tissue orthe periapical region of the teeth or perforation of the oral mucosa

Antibiotic prophylaxis for dental procedures- all regimens
are a single dose given 30-60 mins before the procedureStandard oral regimen
Adults- 2 gm amoxicillin
Children- 50 mg/kg
Alternative oral regimen for patients allergic to penicillin or patients who are
currently taking a penicillin class antibiotic
Adults-
2 gm cephalexin or 600 mg clindamycin or 500 mg azithromycin
Children-
50 mg/kg cephalexin or 20 mg/kg clindamycin or 15 mg/kg azithromycin
Patients unable to take oral medication
Adults-
2 gm iv / im ampicillin or 1 gm im / iv cefazolin or ceftriaxone
Children-
50 mg/kg im or iv ampicillin or 50 mg/kg im or iv cefazolin or ceftriaxone
Alternative im/iv regimen for patients allergic to penicillin and unable to take
oral medications
Adults-
1 gm im/iv cefazolin or ceftriaxone or 600 mg im/iv clindamycin
Children
50 mg/kg im/iv cephazolin or ceftriaxone
20 mg/kg im/iv clindamycin within 30 mins before the procedure
ReferencesBOOKS• Cohen’s Pathways of the pulp- 10th edition
• Ingles Endodontics- 6th edition
• Essentials of pharmacology- KD Tripathi, 2006
• Endodontics- Arnaldo Castellucci- Vol 1 and 2
• Endodontics- principles and practise- M.Torabinejad, 4th edition
• Harty’s Endodontics in clinical practise, 6th edition
ARTICLES
• Pharmacological Strategies to Control Post-operative Endodontic Pain Zahed Mohammad, Alireza Farhad, Meisam Khalesi Dent Res J 2007; 4(2): 61-68
• Endodontics in the adult patient: the role of antibiotics L.P. Longman, A.J. Preston, M.V. Martin, N.H.F. Wilson Journal of Dentistry 28 (2000) 539–548
• Fazakerley MW, McGowan P, Hardy P, et al. A comparative study of cephradine, amoxycillin and phenoxymethylpenicillin in the treatment of acute dentoalveolar infections. British Dental Journal1993;174:359–63.
• Martin MV, Longman LP, Hill JB, et al. Acute alveolar infections: an investigation of the duration of antibiotic therapy. British Dental Journal 1997;183:135–7.

• McDonnell G, Russell AD. Antiseptics and disinfectants: activity, action, and resistance. Clinical Microbiology Reviews 1999;12:147–79.
• Anaesthetising Painful Pulp in Endodontics-A Review. Rakesh Mittal, Jamal M El- Swiah, Vandana Dahiya; JOHCD, September 2011;5(3)
• Pharmacological Strategies to Control Post-operative Endodontic PainZahed Mohammadi, Alireza Farhad, Meisam Khalesi, Dent Res J 2007; 4(2): 61-68
• An update on the antibiotic-based root canal irrigation solutions. ZahedMohammadi, IEJ Vol 3, No 2 Spring 2008
• Endodontic Consideration for the Usage of Drugs in Pregnant and Lactating Mothers AGGARWAL R, SINGLA M, MITTAL N, Journal of Clinical and Diagnostic Research. 2010 August ;(4):2974-2978
• Antimicrobial agents used in endodontic treatment. Marina George Kudiyirickal, Romana Ivančaková, ACTA MEDICA (Hradec Kralove) 2008;51(1):3–12
• Antibiotics as an intracanal medicament in endodontics: A review NeelamMittal, Jyoti Jain, indian journal of dentistry 4(2013) 29-34
• Are antibiotics effective for endodontic pain? Ashraf f. Fouad, Endodontic Topics 2002, 3, 52–66

THANK
YOU
Top Related