






Languages
Pages
Legal


Digestive Disease institute | fall | 2013
Digestthis
p.05
Endoscopic Submucosal Dissection
p.04
Pouch Disorders: What Have We Learned?
p.09
Refining Treatment Options for Gastroparesis
p.10
Driving Medical Advances in Gastroenterology and Hepatology
Cleveland Clinic #2 in the U.S. – Gastroenterology & GI Surgery
FEATURED ART ICLE

DIGeStIve DISeASe InStItUte CHAIR John Fung, MD, PhD
MAnAGInG eDItoR Ann Bakuniene-Milanowski
ARt DIReCtoR Michael viars
MARketInG MAnAGeR Priya Barra
ContRIBUtInG PHotoGRAPHeRS Russell Lee Cleveland Clinic Center for Medical Art & Photography
Dear Colleagues,
We’ve entered the age of
high-definition healthcare.
Breakthroughs in visual-
ization and big data allow
us to see more and do
more than ever before.
this issue of Digest This offers many examples —
from 3-D liver models to delicate endoscopic submu-
cosal dissection to gastroparesis results checked by
the SmartPill® device.
Beyond the patient at hand, our increasing store
of digital data is making it possible for us to study
everything from small cohorts to vast populations
at ever-higher levels of granularity. our cover story
describes several data-driven projects — such as a
study of the natural history of Barrett esophagus that
draws on the Digestive Disease Institute’s 3,200-
patient (and growing) Barrett esophagus Registry.
Science seeks clarity in all it does. But even as
the digital revolution makes the body increasingly
transparent, much remains hidden. What causes
Crohn disease? How can we manage and prevent
alcoholic hepatitis? Why aren’t there better treat-
ments for gastroparesis? We discuss these and
other topics as part of our GI research overview.
Finally, please join us in congratulating our Ileal
Pouch Center on its 10th anniversary of elucidating
this increasingly prevalent condition and offering
hope and care to those who have it.
Sincerely,
John Vargo, MD, PhD Chairman | Department of Gastroenterology and Hepatology
CME CalendarMedical professionals are invited to attend the following continuing education programs:
Digestive Disease Institute’s International Interdisciplinary Education Week 2014
25th Annual David G. Jagelman/ 35th Rupert B. Turnbull International Colorectal Disease Symposium Feb. 11-16 Harbor Beach Marriott Fort Lauderdale, Fla.
3rd Annual Gastroenterology and Hepatology Symposium Feb. 13-15 Harbor Beach Marriott Fort Lauderdale, Fla.
14th Annual Surgery of the Foregut Symposium Feb. 16-19 the Biltmore Hotel Coral Gables, Fla.
Visit ClevelandClinicFloridaCME.org for more information about the above events and more CME offerings from Cleveland Clinic Florida.
24/7 ReferralsReferring Physician Hotline 855.REFER.123 (855.733.3712)
Download today! Physician Referral AppContacting us is easier than ever before.
With our new free “Physician Referral”
app, you will be able to view all our specialists, transfer
a patient and get in touch immediately with one click of
your iPhone® or iPad®. Available at the App Store.
Coming soon to Android™ phone and tablet.
stay connected with us on…

clevelandclinic.org/digestive 855.ReFeR.123 {3}
Digestive Disease institute
Nizar Zein, MD 216.444.6126 [email protected]
image of the issue
Imagine you are a surgeon going to perform a resection of half of a liver for a
transplant and you are actually provided with a 3-D model of the liver you will
encounter the next day,” says nizar Zein, MD, Chief of Hepatology and Medical
Director of liver transplantation at Cleveland Clinic. “You can look at the 3-D
‘printout’ and plan your surgery.”
this technology exists. Working with Cleveland Clinic lerner Research institute’s
Medical Devices unit, Dr. Zein has built more than 20 of these liver models to date
– in a flexible resin with internal lumen geometry generated from a reconstructed
Ct scan – to improve surgical planning and training. ■

{4} Digest This Fall | 2013
Cleveland Clinic
Emre Gorgun, MD 216.444.1244 [email protected]
Case stuDYesD: endoscopic submucosal DissectionChallenging colonic lesions require advanced intraluminal surgical approach
PReSentAtIon
A 60-year-old man with
a medical history of atrial
fibrillation, hypertension
and CoPD presented
with rectal bleeding.
A colonoscopy was
performed at an outside
hospital, which revealed
a large colonic lesion.
the patient was referred
to the Digestive Dis-
ease Institute for emre
Gorgun, MD, to perform
a segmental bowel
resection.
tReAtMent
After an extensive
workup, the patient was
found to have a lesion that was confined to the colon.
therefore, it was decided to treat this high-surgical-
risk patient using an intraluminal surgical approach.
He underwent en bloc endoscopic submucosal dissec-
tion (eSD) of this large colonic lesion in the cecum.
the lesion was 3 cm away from the ileocecal valve
and involved 35 percent of the circumference of the
lumen. Using special endoluminal instruments includ-
ing a dual knife and hook knife, the lesion was marked
circumferentially with a 3 mm clear margin. this step
was followed by submucosal injection and lifting using
a concentrated hypromellose/indigo carmine solution.
once the mucosa had been scored and lifted, submu-
cosal attachments beneath the lesion were divided with
the fine endoscopic tools. The dissection was facilitated
using a distal disposable cap that was attached at the
end of the colonoscope. en bloc removal of the lesion
was successfully achieved, and the specimen measured
3.2 cm in diameter. the patient was discharged on
postoperative day 1 with no complications. The final
pathology revealed tubulovillous adenoma with clear
deep and circumferential margins.
DISCUSSIon
In the United States, the eSD method is presently
used only in a small number of centers to remove large
colonic polyps. Currently, with few exceptions, patients
with large sessile benign colonic polyps are referred by
gastroenterologists to surgeons for segmental colorec-
tal resections. the eSD technique to keep polyps and
large intraluminal lesions intact during removal may
enable precise pathological assessment of the resected
lesions. eSD is a safe and useful technique in carefully
selected patients. We expect that it will soon become
more widely used by surgeons and endoscopists for
large colonic lesions.
Dr. Gorgun is a minimally invasive-robotic and lapa-
ro-endoscopic surgeon and the quality officer in the
Digestive Disease Institute’s Department of Colorectal
Surgery. He specializes in colorectal surgery, with
a particular interest in malignant diseases of the
rectum and colon. ■
esDis a safe and useful
technique to remove
polyps and large
intraluminal lesions
in carefully selected
patients.

clevelandclinic.org/digestive 855.ReFeR.123 {5}
Digestive Disease institute
CoveR featuRe
D R i v i n g
in Gastroenterology and Hepatology
From unlocking disease mechanisms to finding
drugs with fewer toxic side effects, the Digestive
Disease institute’s Department of gastroenterology
and Hepatology is committed to advancing research
that leads to better understanding, more effective
therapies and improved outcomes.

{6} Digest This Fall | 2013
Cleveland Clinic
Pig Whipworms May Help Fight Crohn DiseaseA pivotal trial testing whether the micro-
scopic eggs of pig whipworm (trichuris
suis ova or CnDo-201) may help those
with severe-to-moderate Crohn disease
is nearing completion.
the research is based on what’s known
as the “hygiene hypothesis” of Crohn
disease and multiple animal and hu-
man studies.
“We don’t really know why people
get Crohn disease, but one theory is
based on an epidemiological observa-
tion that the disease is principally
seen in developed areas of the world
such as the United States and europe
while it is hardly ever seen in under-
developed countries that have endemic infection of parasitic worms in the gastrointestinal tract,” explains
Bret Lashner, MD, site primary investigator at Cleveland Clinic for the tRUSt-I trial. “this has led researchers
to hypothesize that this type of infection has a protective effect in the gut.”
TRUST-I, a multicenter phase 2 clinical trial sponsored by Coronado Biosciences, recently finished enrollment of
250 Crohn disease patients. the trial enrolled and randomized patients with moderate-to-severe Crohn disease to
receive either 7,500 ova or placebo once every two weeks, for 12 weeks.
“the pig whipworm, which is not pathogenic for humans, may potentially stimulate the innate immune system
enough to help certain patients with Crohn disease,” Dr. Lashner says. Preliminary data from a phase 1 clinical
study of trichuris suis ova in patients with Crohn disease were positive, and top-line data from the tRUSt-I phase
2 trial are expected in the fourth quarter of 2013. ■
“The pig whipworm, which is not pathogenic for humans, may
potentially stimulate the innate immune system enough to help
certain patients with Crohn disease.” – Bret Lashner, MD
Bret Lashner, MD 216.444.6524 [email protected]
With more than 350 active research projects that span the broad range of gi disorders,
our team is constantly collaborating with investigational partners across the u.s. and pursuing
innovative basic science and clinical research that we hope one day will improve patient care.

clevelandclinic.org/digestive 855.ReFeR.123 {7}
Digestive Disease institute
ALD: Understanding Progression and Improving TreatmentLaura E. Nagy, PhD, Pathobiology Staff and Director of Lerner Research Institute’s Center for Liver Disease
Research, has received two U01 grants from the national Institute on Alcohol Abuse and Alcoholism/national
Institutes of Health.
The first grant is a five-year, $2.1 million U01 titled “Migration inhibitory factor in progression and treatment
of alcoholic liver disease.” With this grant, Dr. Nagy will examine whether genetic variation in a specific pro-
tein — migration inhibitory factor — can predict the incidence and/or severity of alcoholic liver disease (ALD).
ninety percent of alcoholics develop fatty liver, and a subset of that population progresses to the more serious
ALD. Dr. nagy’s team will collaborate with groups in Italy and Spain to examine genetic variation in patients
with ALD. they will examine samples taken from the entire population of two Italian villages almost 30 years
ago, allowing them to observe how ALD has progressed over time.
Dr. Nagy’s second award is a five-year, $1.4 million U01 for “Novel therapeutics for alcoholic hepatitis — Cleve-
land translational component.” In this large, multi-institutional study, Dr. nagy will search for potential new drug
targets for alcoholic hepatitis (AH), one of the most serious forms of alcohol-induced liver disease. She will focus
her efforts on the role of gut integrity and inflammation in the development of the disease.
Arthur McCullough, MD, Gastroenterology and Hepatology, will lead a clinical trial component of the grant, from
which Dr. nagy will obtain human samples for her studies. For the clinical trial, Dr. McCullough and his consor-
tium of investigators at the University of Massachusetts, University of Louisville and University of texas Southwest
will receive $5.5 million over five years. AH has a high short-term mortality rate, and those who do survive have
a 70 percent probability of developing cirrhosis. ■
Investigating ELAD for Treating Acute Liver FailureA team at Cleveland Clinic led by gastroenterologist Talal Adhami, MD, has begun enrolling patients in a multi-
center trial testing the safety and efficacy of the ELAD® system (vital therapies Inc., San Diego, Calif.) in patients
with alcohol-induced liver decompensation (AILD).
eLAD is a human-cell-based liver therapy, designed to provide liver support continuously to patients with liver failure.
It uses a proprietary line of allogeneic human liver cells, originally derived from hepatoblastoma and refined, which
are incorporated in cartridges into an extracorporeal blood pumping system at the patient’s bedside. each patient is
treated with four cartridge bioreactors containing a total of 440 grams of cloned immortalized human liver cells.
“this is a novel and exciting trial because there are not only patients who need bridge-to-transplant support, but also
many whose livers — if given enough support — may regenerate enough to overcome the injury to the point that they
may never need transplantation,” says Dr. Adhami, who serves as the Cleveland Clinic site principal investigator.
the randomized, open-label, controlled study is looking to enroll about 200 patients with AILD. they will be
randomly assigned in a 1-to-1 ratio to receive either standard-of-care treatment for AILD plus treatment with the
eLAD system or standard-of-care treatment alone for up to 91 days. outcomes will be evaluated at 91 days, six
months, nine months, 1 year and 5 years. ■
Laura E. Nagy, PhD 216.444.4021 [email protected]
Talal Adhami, MD 216.839.3000 [email protected]
“This is a novel and exciting trial because there are patients who not only need
bridge-to-transplant support, but also many who – if given enough support – their
livers may regenerate enough to overcome the injury to the liver to the point that
they may never need transplantation.” – Talal Adhami, MD

{8} Digest This Fall | 2013
Cleveland Clinic
Improving Disease Progression in Barrett’s EsophagusPrashanthi Thota, MD, is evaluating
the data from Cleveland Clinic’s Barrett
esophagus Registry of more than 3,200
patients for answers to questions about
the natural history of the disease.
The Barrett’s database, first established
at Cleveland Clinic in 2002, includes
information about the patients’ medical
history, risk factor profile, and endoscopy
and histopathological findings.
“We’ve been following these patients on a
long-term basis to find out how patients
with Barrett’s esophagus progress over
time, identify risk factors for progression,
and measure the success of different
endoscopic treatments in patients with dysplasia and early esophageal cancer,” explains Dr. thota, Head of the
newly established Center for excellence for Barrett’s at Cleveland Clinic’s Digestive Disease Institute.
She and her team are also now examining whether vitamin D levels influence the disease progression in Barrett’s
as well as participating in a national multicenter registry, which ideally will improve understanding of the natural
course of the disease. ■
How LGG and Tributyrin Prevent Antibiotic-Associated DiarrheaA study led by Gail Cresci, PhD, RD, recently published in the Journal of Parenteral and Enteral Nutrition,
has demonstrated why lactobacillus GG (LGG) and tributyrin supplementation reduce antibiotic-induced
intestinal injury.
“While clinical studies have shown some benefit to giving probiotics to treat antibiotic-associated diarrhea, the
molecular mechanism behind it remained to be understood,” says Dr. Cresci, of the Digestive Disease Institute’s
Center for Human nutrition.
Her team, including Laura Nagy, PhD, and Vadivel Ganapathy, PhD, studied the effects of broad-spectrum
antibiotics on germ-free mice given broad-spectrum antibiotics and the probiotic LGG or butyrate, a short-chain
fatty acid that is a fermentation byproduct of undigested fiber and starch.
“We found broad-spectrum antibiotics decrease expression of anion exchangers, butyrate transporter and receptor,
and tight junction proteins in mouse intestine,” says Dr. Cresci, “and simultaneous oral supplementation with LGG
and/or tributyrin minimizes these losses.”
Dr. Cresci also is involved in ongoing research into the effects of antibiotics on the intestinal barrier and how
the barrier can be protected to diminish alcoholic liver disease. ■
Prashanthi Thota, MD 216.445.9552 [email protected]
Gail Cresci, PhD, RD 216.445.8317 [email protected]
Need help? Consult our experts or make a referral today by calling 855.REFER.123.

clevelandclinic.org/digestive 855.ReFeR.123 {9}
Digestive Disease institute
{8} Digest This Fall | 2013
Pouch Disorders: a quick look at our accomplishments, evolution in the field and what advances may be on the horizon.
Celebrating 10 Years of Excell
ence
ILEA
L POUCH CENTER
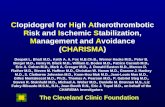
WHAT HAVE WE LEARNED? Correct classification of pouch disorders is key to appropriate therapy
RECENT BREAkTHRoUGHS
WHAT LIES AHEAD?
Pouch Disorders Surgical /Mechanical Inflammatory/
Infectious Functional Neoplastic Systemic/ Metabolic
THEN NOW
C L E V E L A N D C L I N I C C L A S S I F I C AT I o N & M A N A G E M E N T o F P o U C H D I S o R D E R S
Supercharcoal –
absorbs bacterial
toxins rather than
destroying them
Intravenous
immunoglobulin
treatment
novel endoscopic
approaches, including
endoscopic balloon and
needle knife for pouch
strictures and sinus
Ileal Pouch Center specialists are studying:
• the microbiome of the pouch
• Hepatobiliary disorders’ impact on the pouch
• new endoscopic therapies
• Cancer risk in pouch patients
• Adverse metabolic consequences of pouch and pouchitis
• Health disparity in care of patients with pouch disorders
• new surgical techniques to salvage the gastrointestinal continuity
■ Anastomotic leak
■ Pelvic sepsis
■ Sinus
■ Fistula
■ Strictures
■ Afferent/efferent limb syndromes
■ Infecundity
■ Sexual dysfunction
■ Portal veinthrombi
■ Prolapse
■ Pseudo- obstruction/ megapouch
■ twist/volvulus
■ Foreign body
■ Pouchitis
■ Cuffitis
■ Crohn disease
■ Small bowel bacterial overgrowth
■ Inflammatory polyps
■ Irritable pouch syndrome
■ Dyssynergic
■ Poor pouch compliance
■ Hypersensitive suture lines
■ Pouchalgia fugax
■ Pouch/ AtZ neoplasia
■ Lymphoma
■ Squamous cell cancer
■ Anemia
■ Bone loss
■ Renal stone
■ Vitamin deficiency (D and B12)
■ Celiac disease
■ Medical therapy■ Endoscopic therapy
■ Surgical therapy■ Combined therapy
Need help? Consult our experts or make a referral today by calling 855.REFER.123.
ToDAy, subclassification is based on
etiology, disease mechanism, clinical
presentations and disease course.
ILEAL PoUCH CENTER
World’s first and largest multidisciplinary pouch center (formerly known as the Pouchitis Clinic)
1,200 patients & 700 pouch endoscopies per year

{10} Digest This Fall | 2013
Cleveland Clinic
Raul Rosenthal, MD 954.659.5249 [email protected]
Michael Cline, Do 216.444.3192 [email protected]
Refining Treatment Options for GastroparesisDetermining the most effective approaches for your patients
With limited medical options for gastroparesis, interest in nonmedical treatments has
intensified. Cleveland Clinic Digestive Disease Institute physicians and surgeons are
refining the target populations for gastric neurostimulation and gastric bypass surgery,
while conducting research designed to gain new insight into the disease process.
their goal is to provide effective treatment for more patients.
“We see hundreds of patients with gastroparesis on a
yearly basis. Unfortunately, medical treatment options
are few and futile. We need to improve treatment mo-
dalities, because these patients have a poor quality of
life and become a burden on our healthcare system,”
says Raul Rosenthal, MD, a general surgeon on the
gastroparesis team at Cleveland Clinic Florida.
exPAnDInG neURoStIMULAtIon
For several years, Cleveland Clinic DDI physicians
have used gastric neurostimulation to improve symp-
toms that can include persistent nausea and vomit-
ing, dehydration, electrolyte imbalance, malnutrition,
significant weight loss, and diminished quality of life.
However, less than 20 percent of patients qualify for
the procedure.
In an attempt to predict individual response and
avoid unnecessary surgery, Dr. Rosenthal’s team now
places an external gastric pacemaker endoscopically
through the mouth to assess the effect of gastric pac-
ing. If symptoms improve in two or three days, the
stimulator is implanted internally by minimally inva-
sive surgical techniques. otherwise, the endoscopi-
cally placed external stimulator is removed.
In another effort to better target treatment, Dr. Rosen-
thal is measuring intragastric currents to help differen-
tiate among types of gastroparesis.
Michael Cline, Do, a DDI gastroenterologist with a
specialty interest in gastroparesis, suspects that more
extensive disease may prevent some patients with
gastroparesis from benefiting from gastric pacing. This
year, he will begin a study using the SmartPill to directly
visualize how the pacemaker affects stomach emptying.
“In our experience, 20 to 40 percent of patients with
gastroparesis have another part of the gut in addition
to the stomach that doesn’t work. A pacemaker won’t
help if the colon doesn’t function,” he says.
Dr. Cline expects the SmartPill study to disprove the
theory that the gastric pacemaker does not pace the
stomach, but rather improves communication between
the stomach and brain. “I don’t believe it, because
in my practice, all appropriately selected pacemaker
candidates get better. If they don’t, we suspect another
part of the gut is not functioning,” he says.
RoLe oF GAStRIC ByPASS SURGeRy
the population for gastric bypass surgery may be
established. At Cleveland Clinic Florida, about 1 per-
cent of patients with gastroparesis — primarily obese,
diabetic patients — are prime candidates.
“Bypassing the paralyzed stomach has been very
successful in properly selected patients,” says
Dr. Rosenthal.
“these patients may do better with bypass surgery than
with a pacemaker, because weight loss solves a variety of
other problems, such as elevated blood sugar and joint
pain, that a pacemaker wouldn’t help,” adds Dr. Cline.
CoMPReHenSIve CARe
Dr. Cline has teamed with general surgeons Mat-
thew kroh, MD, and kevin el-Hayek, MD, to care for
patients with gastroparesis. Starting this fall, they will
offer a Gastroparesis Clinic in which patients will see
Dr. Cline and a surgeon, pain management specialist
and dietitian in a single visit.
At Cleveland Clinic Florida, gastroenterologists Andrew
Ukleja, MD, and Alison Schneider, MD, evaluate and
treat patients with gastroparesis. Gastrointestinal and
bariatric surgery is performed by Dr. Rosenthal. ■
new this fallour new Gastropare-
sis Clinic can help your
patients see a gastroen-
terologist, surgeon, pain
management specialist
and dietitian in a
single visit.

DDI receives $2 million endowment for colorectal surgery chairkenneth M. Garschina and his wife, Sara Story, have pledged
$2 million to the Digestive Disease Institute to create an
endowed chair for colorectal surgery research.
Luca Stocchi, MD, head of research for the Department of
Colorectal Surgery, will be the first recipient of the Story
Garschina endowed Chair that will help fund research projects
on Crohn disease and anal cancer.
this is the Story family’s second gift to Cleveland Clinic. In
2007, Ed Story, Sara’s father, donated $1.5 million to create
an endowed chair for inflammatory bowel disease research and
education, the Ed & Joey Story Endowed Chair, first held by
Colorectal Chairman Feza H. Remzi, MD.
To reflect our team approach to patient care, the Ed & Joey Story
endowed Chair will now be held by Bo Shen, MD, Section Head
for Pouch Disorders in the Department of Gastroenterology and
Hepatology. Dr. Remzi will now hold the Rupert B. turnbull Jr.,
MD, endowed Chair in Colorectal Surgery. established in 1994,
the latter chair is named after former Colorectal Surgery Chairman
Dr. turnbull, a pioneering surgeon and authority on IBD.
Dr. kessler joins Colorectal SurgeryColorectal surgeon Herman kessler, MD, PhD, has joined the
Digestive Disease Institute. Dr. kessler’s specialty interests in-
clude laparoscopic surgery, Crohn disease, ulcerative colitis, colon
and rectal cancer, and diverticulitis. His research interests are
minimally invasive surgery, IBD, surgery for colorectal carcinoma,
and intestinal endometriosis. Dr. kessler comes to Cleveland Clin-
ic from the University of erlangen-nuremberg, Germany, where
he was professor of surgery and received his medical degree. He
completed fellowships in colorectal surgery at Cleveland Clinic
and Mount Sinai Medical Center, new york, n.y.
Dr. Wexner takes on new roleSteven D. Wexner, MD, has been appointed Digestive Disease
Center Director for Cleveland Clinic Florida. Dr. Wexner has been
with Cleveland Clinic since 1988, serving as Chairman of the
Department of Colorectal Surgery, Cleveland Clinic Florida, since
1993 and Chief of Staff there from 1997 to 2008. He is an
internationally recognized leader in colorectal surgery who will
work closely with DDI Chairman John Fung, MD, PhD, to align
the strategic vision of the Florida and ohio campuses to foster
world-class patient care, research and training.
FINDING BALANCE THRoUGH INNoVATIoN
2013 Medical Innovation Summit oct. 14-16 global Center for Health innovations Cleveland, ohio
clevelandclinic.org/summit
Cleveland Clinic’s annual Medical Innovation Summit convenes
1,100 great thinkers and leaders for a candid exchange on new
medical technology, its future, recent breakthroughs and continu-
ing challenges. Join us for:
• Detailed insights into the newest innovations in the
fast-growing metabolic markets
• Discussions with world leaders responsible for the
change in healthcare technology.
• top 10 Medical Innovations for 2014
Speakers include former Senate Majority Leader tom Daschle,
Aetna Ceo Mark Bertolini and Covidien Ceo José e. Almeida.
SCIENCE AND PRACTICE oF oBESITy MANAGEMENT
8th Annual obesity Summit oct. 16-17 interContinental Hotel and Bank of america Conference Center Cleveland, ohio ccf.cme.org/obesity
this groundbreaking summit, led by Philip Schauer, MD, Direc-
tor of Cleveland Clinic’s Bariatric and Metabolic Institute, unites
multidisciplinary leaders in clinical practice and the workplace
environment to present the latest findings in tackling key issues
surrounding the rapidly escalating obesity epidemic, including:
• the latest update on the Look AHeAD trial
• the current research on sugar-sweetened beverages
• What’s new in drug therapy
• What leaders are saying about pregnancy and obesity
inBrief}
CMe Calendar}

Digestive Disease Institutethe Cleveland Clinic Foundation9500 euclid Avenue/AC311Cleveland, oH 44195
24/7 ReferralsReferring Physician Hotline 855.REFER.123 (855.733.3712) clevelandclinic.org/refer123Live help connecting with our specialists, scheduling and
confirming appointments, and resolving service-related issues.
Hospital transfers800.553.5056
Physician Directoryview our staff online at clevelandclinic.org/staff.
Same-Day AppointmentsCleveland Clinic offers same-day appointments to help your patients get the care they need, right away. Have your patients call our same-day appointment line, 216.444.CARe (2273) or 800.223.CARe (2273).
Track your Patient’s Care onlineestablish a secure online DrConnect account for real-time information about your patients’ treatment at Cleveland Clinic at clevelandclinic.org/drconnect.
Critical Care Transport Worldwide to arrange for a critical care transfer, call 216.448.7000 or 866.547.1467. Learn more at clevelandclinic.org/criticalcaretransport.
CME opportunities: Live and onlinevisit ccfcme.org to learn about the Cleveland Clinic Center for Continuing education’s convenient, complimentary learning opportunities.
Outcomes Dataview outcomes books at clevelandclinic.org/outcomes.
Clinical TrialsWe offer thousands of clinical trials for qualifying patients. visit clevelandclinic.org/clinicaltrials.
Executive EducationLearn about the executive visitors’ Program and the two-week Samson Global Leadership Academy immersion program at clevelandclinic.org/executiveeducation.
about Cleveland ClinicCleveland Clinic is an integrated healthcare delivery system with local, national and international reach. At Cleveland Clinic, more than 3,000 physicians and researchers rep-resent 120 medical specialties and subspecialties. We are a nonprofit academic medical center with a main campus, eight community hospitals, more than 75 northern ohio outpatient locations (including 16 full-service family health centers), Cleveland Clinic Florida, Cleveland Clinic Lou Ruvo Center for Brain Health in Las vegas, Cleveland Clinic Canada, Sheikh khalifa Medical City and Cleveland Clinic Abu Dhabi.
In 2013, Cleveland Clinic was ranked one of America’s top 4 hospitals in U.S. News & World Report’s annual “America’s Best Hospitals” survey. the survey ranks Cleveland Clinic among the nation’s top 10 hospitals in 14 specialty areas, and the top in heart care for the 19th consecutive year.
ReSoURCeS FoR PHyS IC IAnS
CLEVELAND CLINIC #2 IN THE U.S. — GASTRoENTERoLoGy & GI SURGERy
Download today! Physician Referral AppContacting us is easier than ever before.
With our new free “Physician Referral”
app, you will
be able to view all our specialists,
transfer a patient and get in touch
immediately with one click of your
iPhone® or iPad®. Available at the
App Store. Coming soon to Android™
phone and tablet.
13
-DD
I-103
Top Related