





Languages
Pages
Legal


Depression Care ManagementLessons from Project IMPACT
_____________________________________________________
Jürgen Unützer, MD, MPHProfessor and Vice Chair of
PsychiatryUniversity of [email protected]

IMPACT Study Methods
Design / Intervention: Randomized control trial of a collaborative care management program for depression (vs) care as usual
Participants: 1,801 older adults with major depression/ dysthymia from 8 diverse health care systems in 5 states. 400 primary care providers
Unützer et al, Med Care 2001; 39(8):785-99

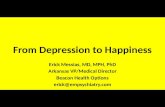
Robust reduction in depressionacross diverse health care organizations
0
10
20
30
40
50
60
70
1 2 3 4 5 6 7 8
Usual Care Intervention
> 5
0 %
red
uctio
n in
dep
ress
ion
from
bas
elin
e at
12
mon
ths
Participating Organizations
%
all p < 0.01

Better Physical Function
38
38.5
39
39.5
40
40.5
41
Baseline 3 mos 6 mos 12 mos
Usual Care
Intervention
PCS-12
P<0.01
P<0.01 P<0.01
P=0.35
Callahan et al, in Press. JAGS.

032
82
188
284
371
2561
136
201
266
0
100
200
300
400
500
600
700
Baseline 3 6 12 18 * 24 *
months
Me
an
(d
ay
s)
Intervention Group Usual Care Group
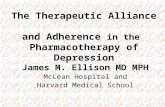
Long-term: more Depression-Free Days
IMPACT INTERVENTION NO IMPACT
*Hunkeler, et al 2004 – unpublished data.

John A. Hartford Foundation Annual Report 2002,
Photo - Courtesy of Don Battershall
IMPACT ‘Key Ingredient’: Depression care manager

Core skills for Depression Care Managers
- Educate about depression
- Clarify treatment goals, expectations, and preferences
- Convey hopefulness and encourage treatment adherence
- Support antidepressant management (side effect management)
- Teach - Problem Solving Skills- Pleasant Events Scheduling (Behavioral Activation)

Depression Care Manager: Core Skills (con’t)
- Track treatment response (PHQ-9)
- Provide updates and recommendations to PCP
- Consult with team psychiatrist
- Facilitate referrals to specialty care and community resources
- Prepare for relapse prevention

Some Practice Considerations forCare Managers
Practice Setting– Practice size: small practices, large group practices– Practice organization: primary care, multispecialty care, – Mental health on / off site
Reimbursement– Fee-for service (e.g., Medicare), capitated (HMOs, VA, other)– Mental health coverage carved in / out
Scope of Practice– National standards / professional certification– State practice acts (licensure)– Agency requirements (internal credentialing)– Third-party payor requirements (e.g., Medicare rules and
regulations; independent or incident to physician billing)– Prescriptive privileges

What is the vision for depression care management?
Program focus– ‘Freestanding’ depression care management program– Depression care as part of a broader disease management
effort? • Depression and other common mental disorders
• Depression and other chronic medical illnesses
• Geriatric care management
Setting / scope- On / off site; in person (vs) telephone
- Number of practices, providers, patients
Target Population- Age, gender, language, special needs, comorbid medical / psychiatric / substance abuse problems, insurance benefits
Top Related