







Languages
Pages
Legal


8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 1/172
CPC I
1) Dermatomyositis
2)Erythema Multifome
3) Psuedoxanthoma
Elasticum 4) Amyloidosis
5) Gestational Pemphigus
6) Grover,s Disease
7) Pediculosis capitis
8) Steatocystoma
Multiplex
9)Lupus Rythematosis
10) Keratoacanthoma
11) Leukocytoclastic
Vasculitis 12) Bullous Pemphigoid
13) Porokeratosis
14) Hailey Hailey Disease

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 2/172
Case 1

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 3/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 4/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 5/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 6/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 7/172
Dermatomyositis: Clinical Proximal extensor myopathy
Adult and Juvenille
Females more common in adult
25% of adult with malignancy
Poikiloderma (violaceous) Heliotrope sign
Photodistribution, nailfoldtelangiectasia
Grotton¶s papules R/o CTD overlap
Anti-Jo-1 20%

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 8/172
Dermatomyositis: Histology
CPC! Non-diagnostic
Similar to SLE
Vacuolar degeneration of basallayer
Epidermal atrophy withhyperkeratosis and blunting of rete ridges
Thickening of the basementmembrane
Edema and increased dermalmucin
Sparse dermal/perivascular mononuclear cell infiltrate

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 9/172
Epidermal atrophy
Basal vacuolar
degeneration

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 10/172
Edema
Dermal mucin
Sparse perivascular infiltrate

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 11/172
Case 2

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 12/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 13/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 14/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 15/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 16/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 17/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 18/172
Erythema Multiforme: Clinical Erythematous, symmetrical, fixed
papules -> targets
HSV, Orf, Histoplasma, ?EBV
50% with clinical herpes labialis(genital rare)
Appear within 24-72h; ~100 lesions Itch or burning of lesions
Dorsal hands, forearms > palms,neck, face, trunk
Oral lesions (lips buccal tongue)
³Target´ lesions have dusky center and erythematous halo (2 or 3rings)
Resolves 2 weeks

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 19/172
Erythema Multiforme: Histology
Vacuolar degeneration of basal layer with dermaledema and sub-epidermalblister
Scattered or groupednecrotic keratinocytes
³Satellitosis´: necrotickeratinocytes surrounded bylymphocytes
Superficial perivascular lymphocytic infiltrate
Extravasated dermal RBCs

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 20/172
Vacuolization, Demal edemaVacuolization, Demal edema

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 21/172
Grouped necrotic keratinocytesGrouped necrotic keratinocytes

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 22/172
SatellitosisSatellitosis

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 23/172
Case 3

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 24/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 25/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 26/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 27/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 28/172
Pseudoxanthoma Elasticum: Clinical
Skin, eyes, cardiovascular
Yellowish ( pseudoxanthomatous)
papules -> plaques Flexural; lax and inelastic skin
ABCC6 ± transmembrane transport
protein (present in skin, eyes, arteries)

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 29/172
Inner lip lesions are mostcommon mucosal finding
Angiod Streaks
breaks in the calcified elastic
lamina of Bruch's membrane Subsequent hemorrhage
Association with B-
thalassemia Early cardiovascular disease
Hematopoietic mases

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 30/172
PXE: Histology
Distorted and fragmentedelastic fibers in the reticular dermis
Calcium deposits on elasticfibers may be visible as³purple clumps´
Silver stains for elastin(Verhoeff van Giesson) and
calcium (von Kossa) tovisualize alterations in theelastic fibers

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 31/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 32/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 33/172
Case 4

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 34/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 35/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 36/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 37/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 38/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 39/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 40/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 41/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 42/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 43/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 44/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 45/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 46/172
Macular Amyloidosis: Clinical
Cutaneous Amyloidosis:macular, lichen, nodular
Brown stippled macules;³salt and pepper´
Moderately pruritic
Interscapular region(classic); thighs, shins,arms, breasts, buttocks
Chronic Result of itching notalgia
paresthetica?

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 47/172
Primary Cutaneous Amyloidosis: ClinicalMacular
Brown stippled macules; ³salt andpepper´; moderate pruritus
Interscapular region (classic); thighs,shins, arms, breasts, buttocks
Result of itching of notalgia paresthetica?
Lichen
persistent pruritic papules/plaquesextensor extremities; shins, thighs,forearms
skin-colored to hyperpigmented papules
Moderately pruritic
Unilateral; can become bilateral
Nodular Very rare
Can progress to systemic (7%)
Paraproteinemia (40%)

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 48/172
Macular Amyloidosis: Histology
Amyloid deposits inthe papillary (andupper) dermis
Melanophages(pigment incontinence
Sparse perivascular lymphistiocytic
infiltrate Stains with congo red,
crystal violet
+birefringence
Nodular AmyloidNodular Amyloid

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 49/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 50/172
Primary Cutaneous Amyloidosis: Histology
Amyloid deposits in thepapillary (and upper)dermis
Melanophages (pigment
incontinence) Sparse perivascular
lymphistiocytic infiltrate
Stains with congo red,crystal violet
+birefringence
Nodular AmyloidNodular Amyloid

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 51/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 52/172
+ Birefringence+ Birefringence
Congo RedCongo Red
Crystal VioletCrystal Violet

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 53/172
Case 5

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 54/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 55/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 56/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 57/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 58/172
C3

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 59/172
Gestational Pemphigoid(= Herpes Gestationis)
(BP180; collagen XVII)
Direct IF demonstrating deposits of C3 along the dermo-epidermal junction
Papillary dermal edema andperivascular lymphocytic and
eosinophilic infiltrate

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 60/172
Gestational Pemphigoid

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 61/172
Gestational Pemphigoid
(= Herpes Gestationis) Sudden onset of intensely pruritic vesiculo-bullous eruption
developing during 2nd or 3rd trimester or the immediatepostpartum period
starts on abdomen in half the cases
Lesions rapidly progress to generalized bullous eruption sparingthe face, mucous membranes, palms and soles
Spontaneous resolution following delivery

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 62/172
Case 6

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 63/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 64/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 65/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 66/172
T i t th l ti d t i

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 67/172
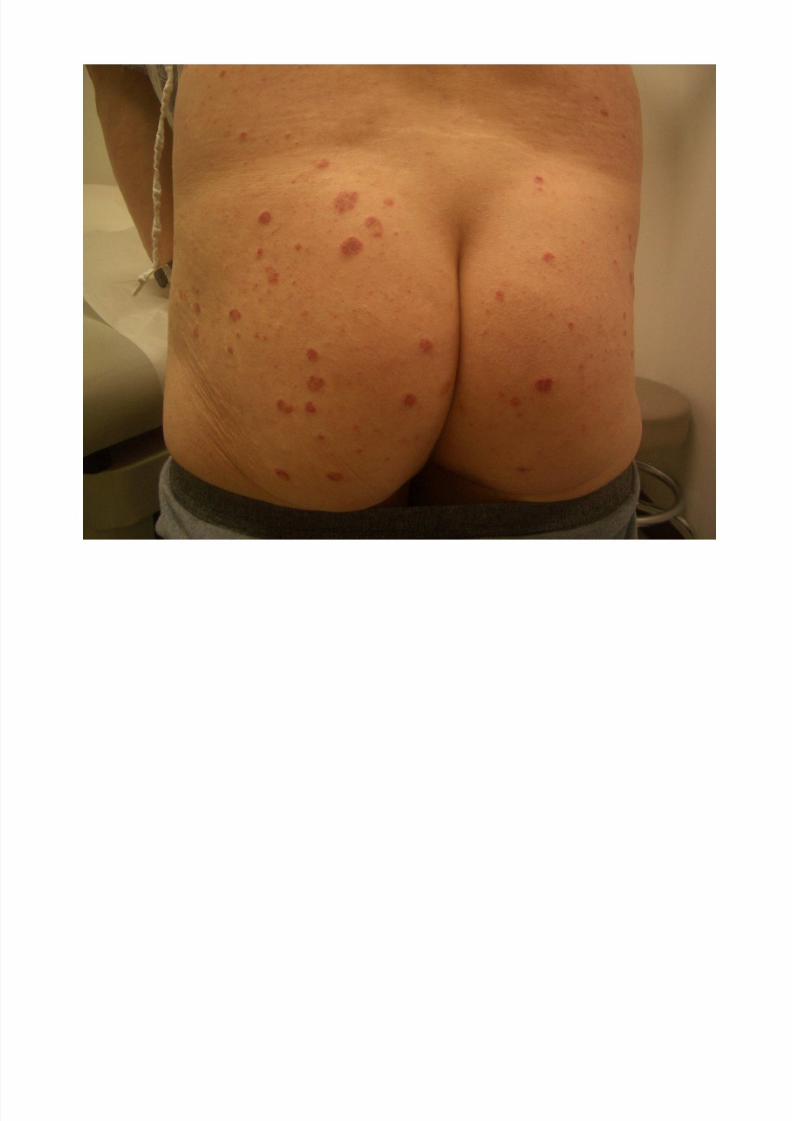
Transient acantholytic dermatosis(Grover's Disease)
four histologic patterns, resembling Darier's disease, Hailey-Hailey
disease, pemphigus and a spongiotic pattern
T i t th l ti d t i

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 68/172
Transient acantholytic dermatosis(Grover's Disease)
intensely pruritic, polymorphic, papulovesicular
dermatitis primarily of the trunk
chiefly affectsCaucasian men after the age of 40 years
transient version lasts for weeks to months
chronic variant follows a chronic, relapsing course over
years
exacerbating factors include friction, heat, sweating andsunlight exposure

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 69/172
Case 7

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 70/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 71/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 72/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 73/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 74/172
di l i i i

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 75/172
Pediculosis capitis(Head lice)
Skin findings (excoriations, erythema, pyoderma, and
scaliness) most commonly behind the ears and posterior
neck
Classic symptom is intense pruritus
Diagnosis is made by the identification of nits and/oradult lice in the scalp hair
Viable eggs are usually tan to brown in color. Hatchedeggs are clear to white and have to be differentiatedfrom hair casts, dandruff, hair gel, and white piedra

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 76/172
Case 8

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 77/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 78/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 79/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 80/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 81/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 82/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 83/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 84/172
Steatocystoma: Histology

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 85/172
Steatocystoma: Histology
Thin walled dermal cyst
Stratified squamousepithelium
Fine scant keratinousdebris
Sebaceous glandsadjacent to or arising
from cyst wall Irregular eosinophiliccuticle lines the cyst

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 86/172
Steatocystoma: Histology
Thin walled cyst
Sebaceous
glands adjacent
to cyst wall
Steatocystoma: Histology

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 87/172
Steatocystoma: Histology
stratified squamousepithelium
irregular eosinophiliccuticle lines the cyst
Fine scant keratinousdebris

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 88/172
Steatocystoma-path

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 89/172
Steatocystoma-path

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 90/172
Steatocystoma-path
Cyst with sparse keratin or hair shafts, but
frequently appears empty.
Wall of ruggated squamous epithelium
with a wrinkled eosinophilic refractile
cuticle of keratin-no granular layer.
Sebaceous glands within or adacent to the
cyst wall opening into cyst.
Steatocystoma: Clinical

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 91/172
Steatocystoma: Clinical
Steatocystoma Simplex
Steatocystoma Multiplex ± Autosomal Dominant; Keratin
17
± Association with Eruptive Vellus
Hair Cysts; PachyonychiaCongenita (also K17)
Dermal cysts
Drain oily fluid when
punctured Chest, axilla, groin
Asymptomatic/Cosmeticconcerns

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 92/172
Case 9

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 93/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 94/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 95/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 96/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 97/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 98/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 99/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 100/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 101/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 102/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 103/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 104/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 105/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 106/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 107/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 108/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 109/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 110/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 111/172
³Lupus Band´

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 112/172
p
granular Ig + C3 at the DEJ
Photo: Bhawan, Byers, & Sau. Dermatopathology Interactive Atlas.

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 113/172
Summary: Histology of LE

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 114/172
Summary: Histology of LE
Epidermal atrophy and hyperkeratosis,
follicular plugging
Vacuolar interface dermatitis
Superficial and deep perivascular
lymphocytic infiltrate
Periadnexal infiltrate
Thickened basement membrane
Dermal mucin
Andrews Classification

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 115/172
Andrews Classification
Chronic LE ± DLE ± localized
± DLE ± generalized
± Hypertrophic LE
± LE-LP overlap
± Tumid LE
± Lupus Panniculitis
± Chilblain LE
Subacute LE ± Annular
± Papulosquamous
± Drug-induced
± Neonatal
± Complement deficiency
Acute LE ± Malar rash & related
± Bullous LE
DLE Clinical Features

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 116/172
DLE ± Clinical Features
Most common form of chronic cutaneouslupus
Erythematouspapules & plaques
Scale
Atrophy
Scarring Dyspigmentation
Follicular Plugging
S d DLE

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 117/172
Sun and DLE
DLE is photosensitive, but not limited to a
photodistribution
± Experimentally reproduced by UVB and UVA
± Not as strongly photosensitive as other forms of
cutaneous lupus
± May occur on photoprotected skin (including sites of
prediliction ± scalp and conchal bowls)
DLE Scalp involvement

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 118/172
DLE ± Scalp involvement
Involved in 60%
Scarring alopecia
may result
Mucosal DLE

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 119/172
Mucosal DLE
Up to 24% in one
study
Mouth (buccal
mucosa-mostcommon)
Nose
Eye
Genitals
DLE Prognosis

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 120/172
DLE - Prognosis
Occurs in 20% of
patients with SLE
< 5-10% patients
presenting with DLEwill progress to SLE
*Caution: children
with DLE may have a
higher chance of progression
DLE

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 121/172
all patients
localized
Fewer manifestations of SLE
Less often ANA+
Greater chance of spontaneous
remission (~50%)
Higher chance of SLE
More often ANA+, leukopenia, ESR
Less chance of remission (<10%)
generalized
Lab Workup: Other serologies

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 122/172
Lab Workup: Other serologies
ANA
dsDNA, Sm
± Markers for SLE
Ro (SSA), La (SSB)
± Markers for SCLE, photosenstivity, Sjogren¶s
U1RNP
± MCTD, SLE
Treatment of Dermatologic LE

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 123/172
Treatment of Dermatologic LE
Foundation:
Sunscreen & Smoking Cessation,
Eliminate drug precipitants
Topicals
Antimalarials
Other
Treatment Topicals

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 124/172
Treatment - Topicals
Topical steroids as determined by lesions
thickness and site
ILK
Immunomodulators
± Tacrolimus, pimecrolimus
Treatment First Line Systemics

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 125/172
Treatment ± First Line Systemics
Hydroxychloroquine
± 200mg po qd to bid
Chloroquine ± 250mg po qd
Quinacrine
± 100mg po qd in addition to HCQ or CQ
± Must be compounded
Antimalarial Resistant Disease

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 126/172
Antimalarial-Resistant Disease
Review treatment foundations: ± sun protection
± smoking cessation
Immunosuppressive agents ± Methotrexate
± Azathioprine
± Mycophenolate mofetil
Oral retinoids ± Hypertrophic or palmoplantar disease
Thalidomide
Path: LE

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 127/172
Path: LE
Follicular plugging
Epidermal atrophy/hyperplasia
Colloid bodies
Liquefaction degeneration of basal layer Thickened basement membrane
Increased Mucin
Perivascular and peradnexal lymphocitic
infiltrate Immunofluorescence-granular IgM, IgG and
complement at the DEJ

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 128/172
Case 10

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 129/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 130/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 131/172
keratoacanthoma
KA-clinical

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 132/172
KA clinical
Common volcano nodule or plaque
erupting over several weeks.
Capable of spontaneous resolution.
Subtype of SCC-rarely metastasizes.
SCC-ka type, the usual designation by
pathologists.
Path: KA

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 133/172
Path: KA
Keratin filled crater
Pale, eosinophilic, glassy well
differentiated epithelial proliferation with
squamous eddies or keraitn pearls
Cytologic atypia no more than mild
Occasional perivascular or lichenoid
infiltrate

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 134/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 135/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 136/172
Case 11
8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 137/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 138/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 139/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 140/172
Leukocytoclastic vasculitis
Clinical LCV

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 141/172
Clinical LCV
Majority follow acute infection or exposure tonew medication.
Palpable purpura is the hallmark of the disease.
Annular, vesicular, bullous.
Affect mainly dependent areas-legs.
Ck-CBC, ASO, HBV, HCV, ANA. Consider SPEP, UPEP, complement, ANCA¶s, andcryoglobulins.
Path-LCV

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 142/172
Path LCV
Epidermis-normal to necrotic
Vasculitis of small venules, predominantly
neutrophils
Nuclear dust often.
RBC extravasation.
Occ. Thrombi.
Fibrin deposits may be seen.

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 143/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 144/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 145/172
Case 12

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 146/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 147/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 148/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 149/172
Bullous pemphigoid
Clinical-BP

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 150/172
Large tense blisters-groin, axilla, trunk, thighs,flexor surfaces
Bullae often occur on an urticarial base.
Age of onset-65-75 years.
Circulating antibodies to BPAg1 (230kda) andBPAg2 (180kda).
Tx: topical steroid, systemic steroids, other immunesuppression, tetracyclines plusniacinamide.
Path-BP

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 151/172
Eosinophilic spongiosis
Subepidermal blister
Viable roof over blisters-non necrotic
Immunofluorescence-linear IgG (IgG4) in
the basement membrane zone

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 152/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 153/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 154/172
Case 13

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 155/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 156/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 157/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 158/172
Porokeratosis
Clinical: porokeratosis

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 159/172
Types: ± Mibelli-usually solitary.
± DSAP-sun-exposed areas.
± Linear porokeratosis-highest risk of developing cutaneous malignancies.
± Palmaris, plantaris et disseminata-first onhands and feet, then rest of body.
± Punctate porokeratosis-limited to hands andfeet.
Path-porokeratosis

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 160/172
Coronoid lamella-a column of
parakeratosis under which there is
hypogranulosis.
Epidermis centrally may be normal. Perivascular or lichenoid lymphocytes
occasionally under coronoid lamella.

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 161/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 162/172
Case 14

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 163/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 164/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 165/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 166/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 167/172

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 168/172
Benign Familial Pemphigus
(Hailey-Hailey): Clinical

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 169/172
Autosomal Dominant, rare
ATP2C1 ± Mutation in Calcium ATPase, Golgi apparatus
Loss of cellular adhesion, stratumspinosum
Onset ages 10-50 years
Flaccid blisters, erosive plaques
Intertriginous and Neck
± Axillae, groin
Painful; Malodorous vegetations
Flares and remissions
Heals with scarring
SCCSCC
HSVHSV
Kaposi¶sKaposi¶s
varicelliformvaricelliform
eruptionseruptions
Benign Familial Pemphigus:
Histology

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 170/172
Generalizedacantholysis leads to
"dilapidated brick wall³
³Villi´: dermal papillaelined by basal cells
Rare ³corps ronds´
Negative directimmunofluorescence

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 171/172
Benign Familial Pemphigus:
Histology

8/8/2019 CPC Kurban I
http://slidepdf.com/reader/full/cpc-kurban-i 172/172
³Dilapidated brick
wall"
Acanthosis
+/- parakeratosis
(later lesions)
Top Related