





Languages
Pages
Legal


Resultaten TRIDENT-studie
Diane Van Opstal,
Laboratorium Specialist Klinische Genetica
Symposium 23 mei 2016
Stichting Prenatale Screening Zuidwest
Nederland

1 april 2014: start of NIPT in the Netherlands (until 2016) (all UMCs participate)
Trident Trial by Dutch laboratories for Evaluation of Non-invasive prenatal Testing
Patients:
-increased risk of trisomy > 1/200 based on abnormal first trimester screening
-medical indication
choice of NIPT or invasive testing (chorionic villi or amniocentesis)
Aim:
1.To study how NIPT can best be implemented in the Netherlands next to other
prenatal screening programs (FTS, US)
2. To study the performance of the test: which factors influence the performance
3. To study the choices pregnant couples make after aFTS results
TRIDENT

Het begin
“Fetus-derived Y sequences were detected in 24 (80%) of the 30 maternal
plasma samples………. may have implications for non-invasive prenatal
diagnosis…………”
-NIPT with fetal cells: expensive and time-consuming
-presence of tumour DNA in plasma of cancer patient
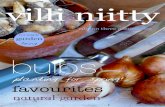
(cf)-DNA in maternal blood is partially fetal
Fetal fraction: (Wang et al., 2013, Prenat Diagn, 33,
662–666)
mean 10,2 % at 10 wks
in 2% < 4% FF
4% is theoretical cut-off value
(<->Fiorentino et al., 2016, Prenat Diagn: 2%)
Half-life very short
Uniformely distributed over the whole
genome

Gestational age
BMI
Fetal aneuploidy
Factors that influence the fetal fraction
Wang et al., 2013, Prenat Diagn, 33, 662–666) Taglauer et al., 2014, Placenta, 28, S64-S68)

1 april-1 september 2014:
1413/23232 (6%) afwijkende CT
1211 (85.7%) + 179 medical indication kozen voor NIPT:
N=1390
1386 resultaat (99.7%) (6x na herhaalde bloedafname (0.4%))
Gemiddelde TAT= 11 dagen
37/38 (97.4%) trisomies 21 (29/30), 18 (4/4) or 13 (4/4) (0.1%)
5 vals positieven (0.4%) (2x +21, 1x +18 en 2x +13)
reductie invasieve testen geschat op 62%
Submitted to Prenat Diagn
Resultaten TRIDENT: trisomie 13, 18, 21

Chromosome
aberration
sensitiviteit specificiteit PPV NPV
Trisomy 21
96.7% 99.9% 93.5% 99.9%
Trisomy 13
100% 99.9%
66.7% 100%
Trisomy 18
100% 99.9%
80% 100%
Performance NIPT
In 2/8 centra (G/U) alleen 13, 18 en 21
In 6/8: ook overige chromosoomafwijkingen
Overige chromosoomafwijkingen

bepaald door:
techniek en analyse methode
de oorsprong van het onderzochte cel-vrije DNA
Typen/aantal nevenbevindingen
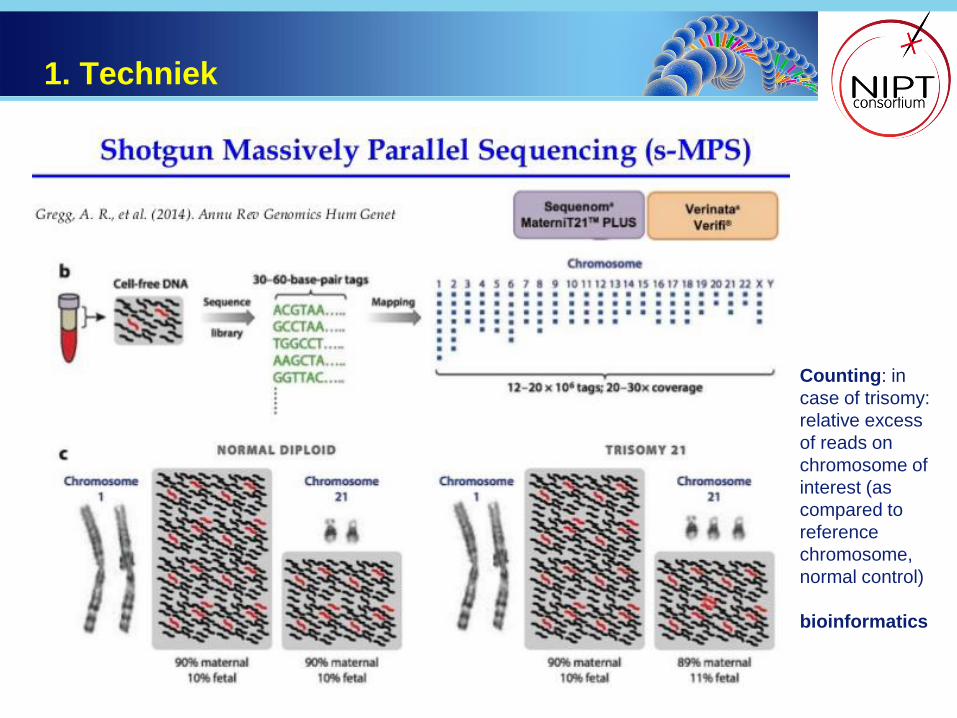
1. Techniek
Counting: in
case of trisomy:
relative excess
of reads on
chromosome of
interest (as
compared to
reference
chromosome,
normal control)
bioinformatics
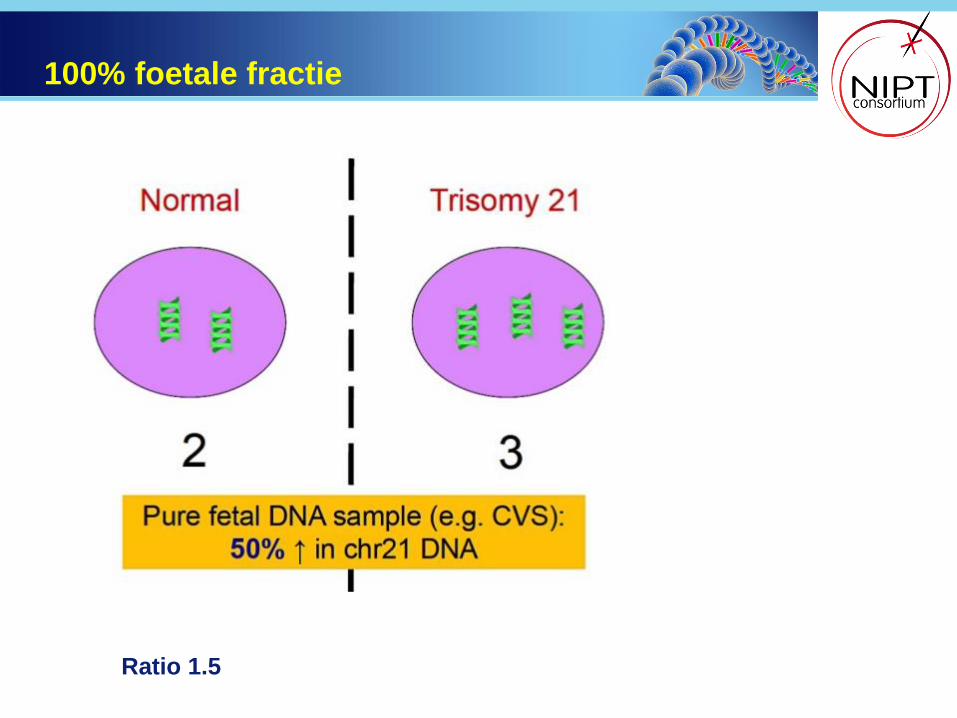
100% foetale fractie
Ratio 1.5

10-20% foetale fractie

Results expressed as
Z-score = (Chr21 fraction test sample) – (Average Chr21 fraction reference set)
Standard Deviation Chr 21 fraction reference set
Fraction = number of reads on chr n / total mapped reads
Reference set = a set of normal samples
Z-score > 3 trisomy
Calculation of z-score

Analyse methode: WISECONDOR
Onderzoek van alle autosomen! Geen geslachts-chromosomale afwijkingen en geen triploidie
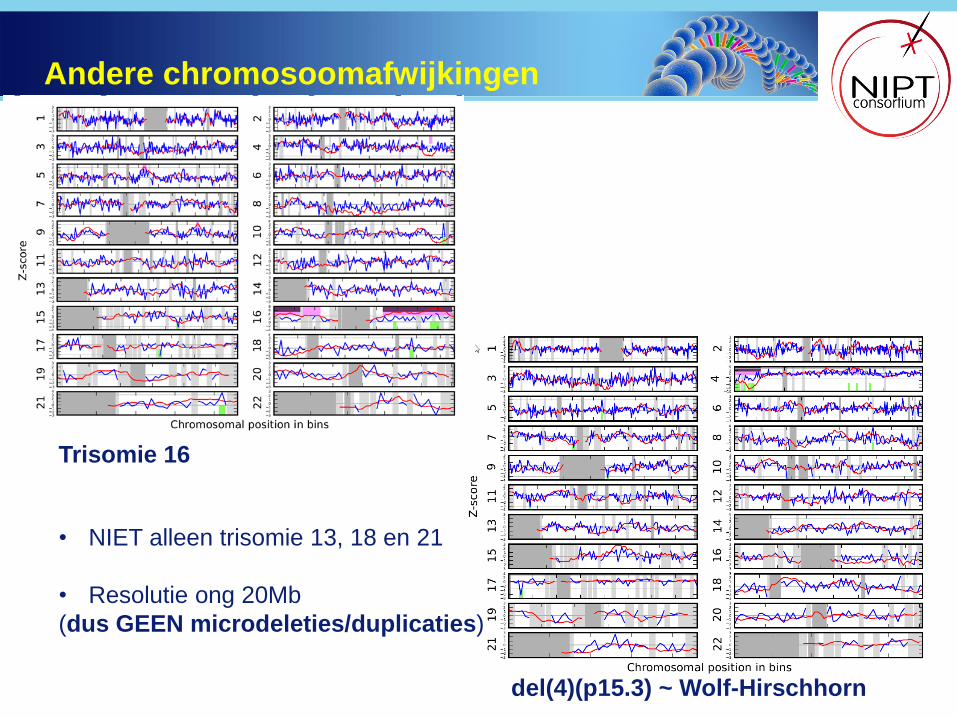
Andere chromosoomafwijkingen
Trisomie 16
del(4)(p15.3) ~ Wolf-Hirschhorn
• NIET alleen trisomie 13, 18 en 21
• Resolutie ong 20Mb
(dus GEEN microdeleties/duplicaties)
A. grotendeels van moederlijke origine (~90% maternaal/10% foetaal)
-Moederlijk mozaïek
-Moederlijke copy number variatie
-Moederlijke maligniteit
2. Oorsprong van het cel-vrije DNA

B. cel-vrije foetale fractie heeft een placentaire oorsprong
Oorsprong van het “foetale” cel-vrije DNA
Confined
placental
mosaicism
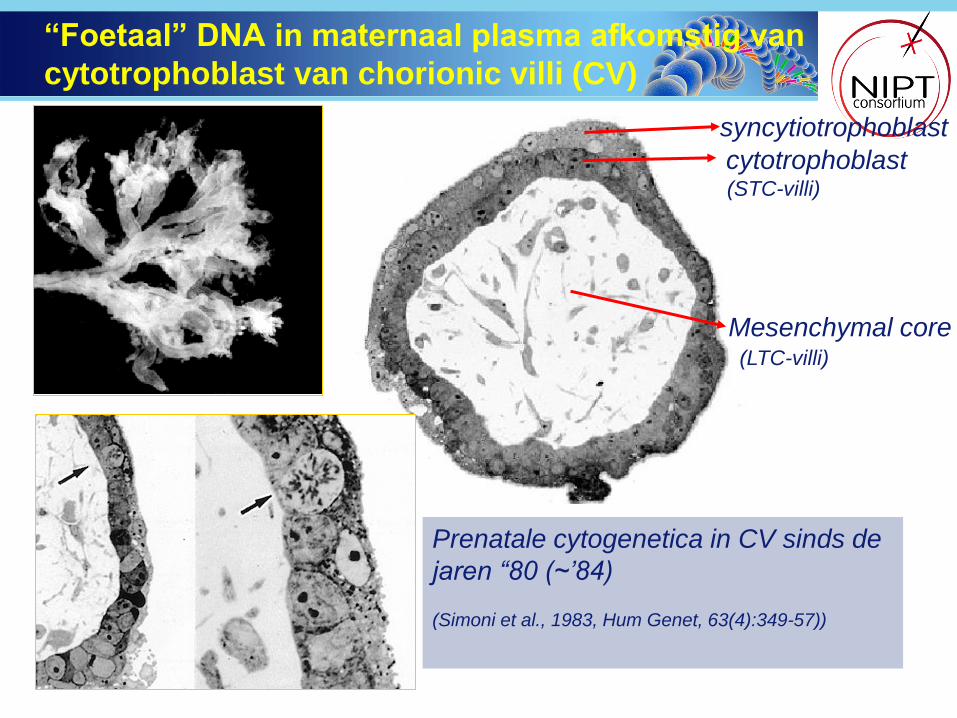
“Foetaal” DNA in maternaal plasma afkomstig van
cytotrophoblast van chorionic villi (CV)
syncytiotrophoblast
cytotrophoblast
Mesenchymal core
Prenatale cytogenetica in CV sinds de
jaren “80 (~’84)
(Simoni et al., 1983, Hum Genet, 63(4):349-57))
(STC-villi)
(LTC-villi)

Zygote
Trophoblast (STC-villi)
ICM
Fetus (amniotic fluid )
EEM (LTC-villi)
Discrepanties tussen cytotrophoblast en foetus
Syncytiotrophoblast
Cytotrophoblast STC – villi/NIPT
Mesenchymal Core LTC - villi
Early embryonic development
Crane and Cheung, Prenat Diagn, 1988 Feb;8(2):119-29; Bianchi Am J Med Genet, 1993 Jun 15;46(5):542-50.
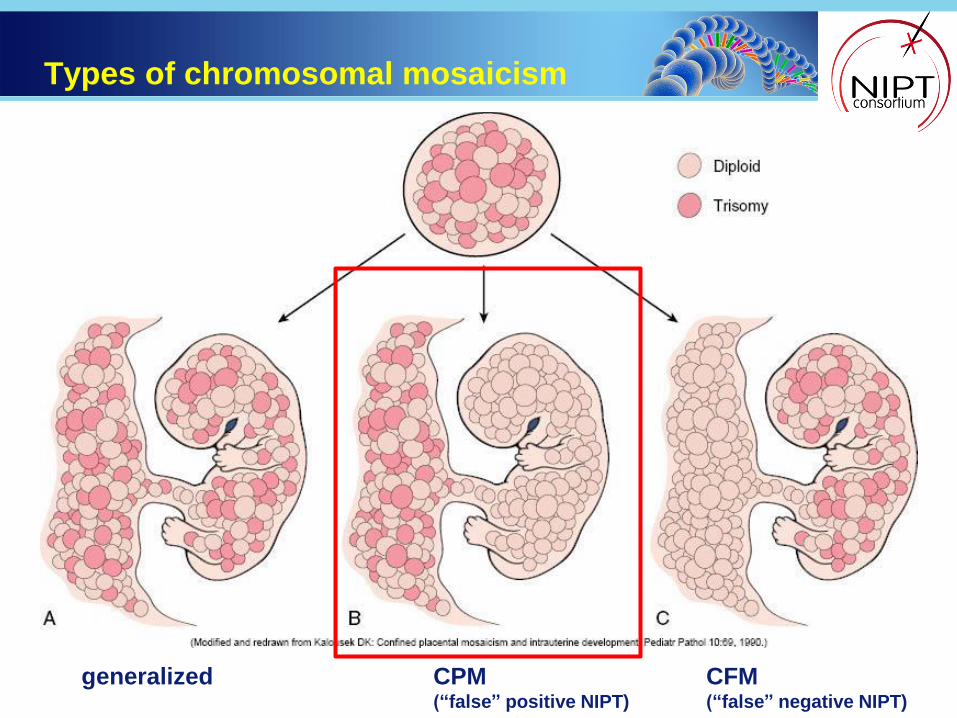
Types of chromosomal mosaicism
generalized CFM (“false” negative NIPT)
CPM (“false” positive NIPT)

“Exotic” aberrations with NIPT as with CVS
1. Foetale afwijkingen ≠ trisomie 13, 18 en 21
2. Confined placental mosaicism
3. Moederlijk mozaïek
4. Moederlijke copy number variatie
5. Moederlijke maligniteit
Typen nevenbevindingen

N=3306 getest
N=3278 (99.2%) met uitslag
107 met trisomie 13, 18 of 21 (3.3%)
51 nevenbevindingen (1.6%)
1/3 afwijkingen ≠ trisomy 13, 18, 21
Resultaten in 1e jaar TRIDENT

9 foetale afwijkingen
25 (waarschijnlijk) confined placental mosaicism
9 moederlijke CNVs
2 wrschl technisch
6 onbekend :
1 geen FU
5x foetus en placenta normaal (4 gezond; 1 neonatale dood)
51 nevenbevindingen

Chromosoomafwijking zwangerschapsuitkomst
mos +9 Levend met MCA/MR (19 ma)
mos +15 (echo g.b.) Levendgeboren 40 3/7 wkn. Geen FU.
mos +22 (geen echo) TOP (dysmorfieën)
mos +del(8)(p21.3p23.1) (echo g.b.) TOP 17 1/7 wkn (dysmorfieën,
hand/voet/anusafw)
der(9)t(2;9)(p21;p24) IUVD 30 wks (familiaire translocatie)
del dup (9p) (echo g.b.) TOP 21 3/7 wkn
del(12)(q21.2q21.33) (echo g.b.) TOP 21 3/7 wkn
der(13;18)(q10;q10) (geen echo) TOP (dysmorfieën)
del(6)(q14.1q16.1) (echo g.b.) Levendgeboren 33 5/7 wkn
(fenotype: 6q14 deletie syndroom)
1. Foetale chromosoomafwijkingen (N=9)
Case report
Patiënte 38 jaar
NIPT bij 12 2/7 wkn
Indicatie: afw ETS: risico Down syndroom: 1:149
del(6)(q14.1q16.1)
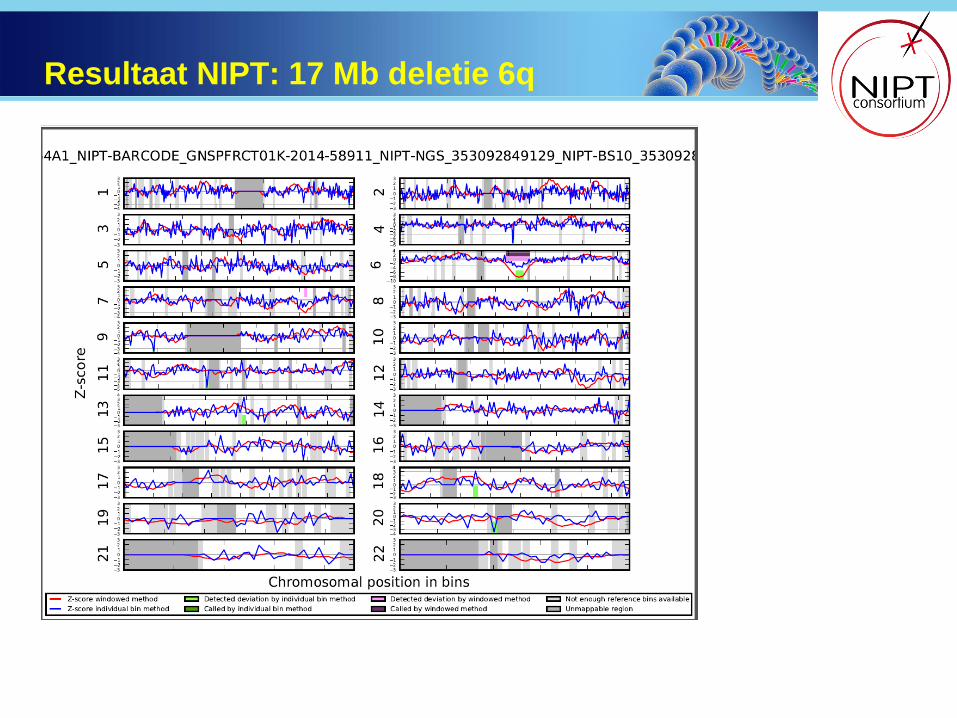
Resultaat NIPT: 17 Mb deletie 6q
Wilden geen vruchtwaterpunctie
Array ouders: normaal
FISH (uitsluiting gebalanceerde chromosoomafwijking in 1 van
ouders): normaal
Echo-onderzoek: geen bijzonderheden
Vervolgonderzoek tijdens de zwangerschap

33 5/7 weken een sectio caesarea verricht.
Kind: een goede start. De Apgarscores waren 5, 8 en 8 na
respectievelijk 1, 5 en 10 minuten.
Naar SKZ vanwege ademhalingsproblemen; beademd
Gewicht 1575 gram (-1.92 SD), schedelomtrek 29.5 cm (-1.41 SD)
Open ductus Botalli, niet geopereerd
Vertraagde ontwikkeling
Wordt vervolgd bij de chromosomenpoli in Groningen
Na geboorte

SNP array op navelstrengbloed
14.8 Mb deletie 6q14.1q16.1
overlappend met
6q14 deletie syndroom
Klinische kenmerken:
mentale en ontwikkelingsachterstand
obesitas
gedragsafwijkingen
macrocephaly
dysmorfieën

Incidentie foetale chromosoomafwijking
≠ +13, +18, +21
3/530 (0.6%*)
NIPT
9/2527 (0.4%)
Array*
* Van Opstal et al., 2015, Hum Mut, 36(3):319-26

Chromosoomafwijking aantal
+2 1
+3 1
+7 7
+8 2
+9 2
+16 9
+22 1
+7,+20 1
+2,+20 1
totaal 25
2. Confined placental mosaicism N=25

Incidentie CPM
5/530
~1%
NIPT
25/2527
~1%
Array*
* Van Opstal et al., 2015, Hum Mut, 36(3):319-26

Geassocieerd met:
IUGR
IUVD
Foetale afwijkingen (gegeneraliseerd mozaïek?)
vervolg echografisch onderzoek geïndiceerd
Kalousek, D. K., P. N. Howard-Peebles, S. B. Olson, I. J. Barrett, A. Dorfmann, S. H. Black, J. D. Schulman and R. D. Wilson. "Confirmation of
CVS mosaicism in term placentae and high frequency of intrauterine growth retardation association with confined placental mosaicism." Prenat
Diagn 1991 11(10): 743-750.
Johnson, A., R. J. Wapner, G. H. Davis and L. G. Jackson. "Mosaicism in chorionic villus sampling: an association with poor perinatal
outcome." Obstet Gynecol 1990 75(4): 573-577.
Goldberg, J. D., A. E. Porter and M. S. Golbus. "Current assessment of fetal losses as a direct consequence of chorionic villus sampling." Am J
Med Genet 1990 35(2): 174-177.
Toutain et al. Prenat Diagn 2010; 30: 1155–1164.
Klinische relevantie van CPM
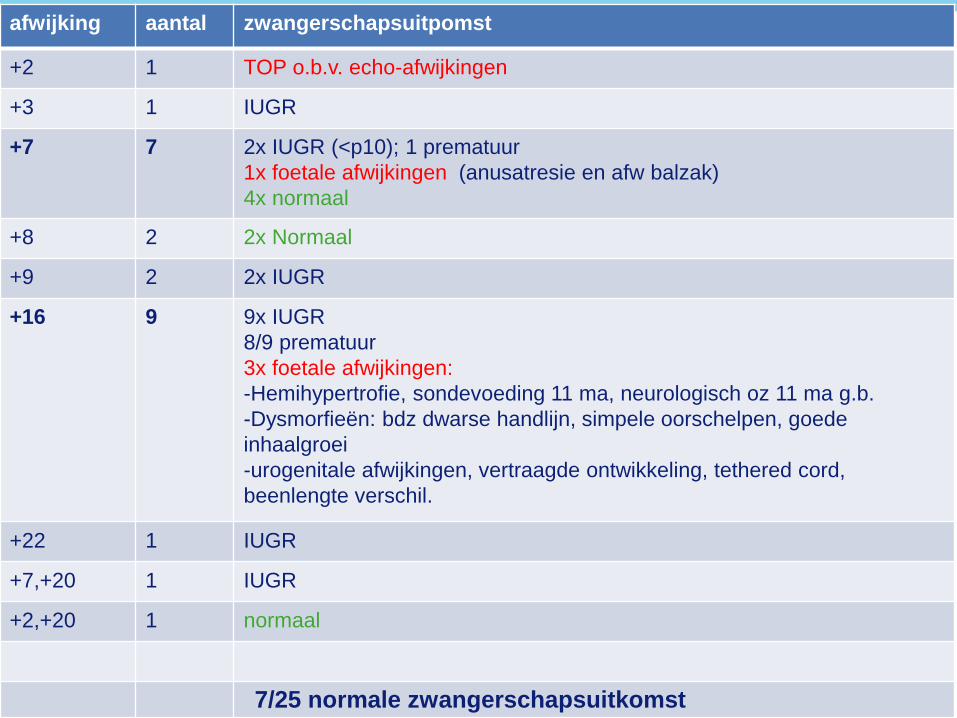
afwijking aantal zwangerschapsuitpomst
+2 1 TOP o.b.v. echo-afwijkingen
+3 1 IUGR
+7 7 2x IUGR (<p10); 1 prematuur
1x foetale afwijkingen (anusatresie en afw balzak)
4x normaal
+8 2 2x Normaal
+9 2 2x IUGR
+16 9 9x IUGR
8/9 prematuur
3x foetale afwijkingen:
-Hemihypertrofie, sondevoeding 11 ma, neurologisch oz 11 ma g.b.
-Dysmorfieën: bdz dwarse handlijn, simpele oorschelpen, goede
inhaalgroei
-urogenitale afwijkingen, vertraagde ontwikkeling, tethered cord,
beenlengte verschil.
+22 1 IUGR
+7,+20 1 IUGR
+2,+20 1 normaal
7/25 normale zwangerschapsuitkomst

20% kind/foetus met afwijkingen
~60% IUGR
* Toutain et al., 2010, 30, 1155-1164
Klinische follow-up van 25 x CPM

afwijking Follow-up tijdens de zwangerschap echo
10 Mb dup (1) (known maternal CNV from previous array) g.b.
12 Mb dup (3) (known maternal CNV 3 Mb from previous array) Array
navelstrengbloed normaal.
g.b.
15 Mb del (11p)
6 Mb del 11p in blood and wangslijmvlies mother ?
10 Mb dup(17p) Buffy coat: 1.3 Mb dup 17p12 ~ Charcot Marie Tooth
(klinisch daarmee bekend)
g.b.
dup(20) Array on maternal gDNA ?
del(13q) (spike) Buffy coat: del(13) g.b.
10 Mb dup (13)
Mat ~500 Kb dup on 13q ?
11 Mb dup (21)
Buffy coat: ~2 Mb dup= UV (geen onderzoek van foetus) IUGR
11 Mb dup (21)
AF: QF normal
Mother: array: dup 21 ?
3. Maternal CNVs (N=9)

Moederlijke duplicatie
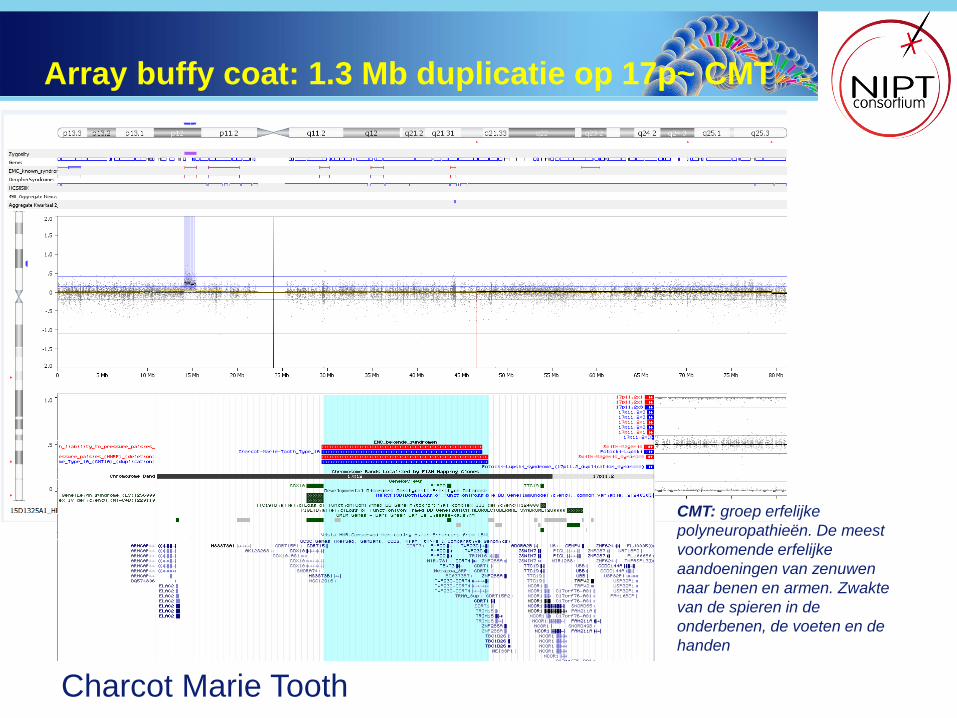
Array buffy coat: 1.3 Mb duplicatie op 17p~ CMT
CMT: groep erfelijke
polyneuropathieën. De meest
voorkomende erfelijke
aandoeningen van zenuwen
naar benen en armen. Zwakte
van de spieren in de
onderbenen, de voeten en de
handen
Charcot Marie Tooth

Maternal CNV on chr21
[
Case:
a FTS: risk trisomy 21 1:85 at 12 5/7 wks
BMI 32.2
z-scores for #21:
BS: 4.43
Lmfit: 4.63
WISECONDOR: <5

Partial duplication 21q21.1

Array op buffy coat: 2 Mb mat duplicatie
chr21:20,604,811-22,572,304: klinische relevantie onbekend
geen onderzoek foetus. Wel gerapporteerd ivm toekomstig NIPT onderzoek
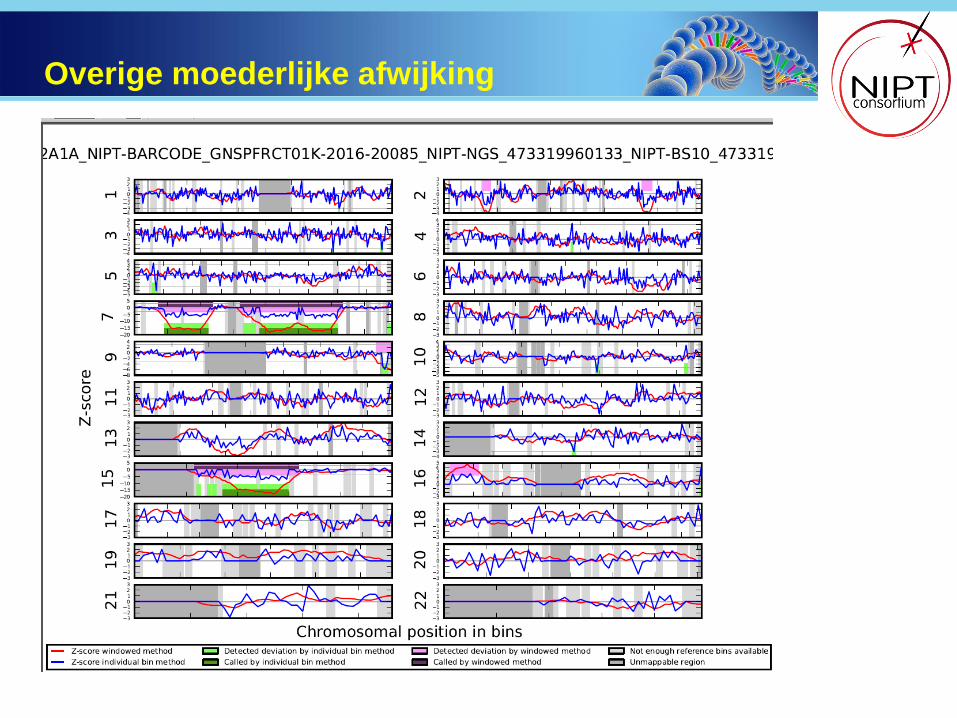
Overige moederlijke afwijking

• Buffy coat: normaal
• Overleg met aanvrager: patiënte bekend met uterus myomatosus
• Voor zekerheid: vruchtwater: normaal
Vervolgonderzoek:

Altijd vervolgonderzoek nodig
• Soms onderzoek moeder voldoende
• Indien niet-maternaal: invasief vervolgonderzoek
NIPT geen diagnostische test

Vruchtwaterpunctie of vlokkentest?
Altijd bevestging van NIPT middels diagnostische test
In praktijk meestal vruchtwaterpunctie
Vlokkentest mogelijk?
NIPT bij ~10 wkn resultaat bij ~12 wkn
vruchtwaterpunctie ~15-16 wkn??
FTS
< 12 wkn
NIPT
> 12 wkn
Resultaat
~14-15 wkn

Afhankelijk van de chromosoomafwijking is
CVS soms mogelijk
Trisomy
13, 18, 21
Trisomy
3, 72, 81, 9, 202 Trisomy
152, 16, 22, rare trisomies and sex-
chromosomal aneuploidy
Normal
fetus
Chorionic villus sampling (mesenchymal core) 3
MOS
(risk ~3%) A
Abnormal
fetus
Cordocentesis4
N A or MOS N2
Normal
fetus
Amniocentesis2, 4
(MOS)+3,
+72,+9,+202 (MOS)+81
Amniocentesis4
A or MOS N2
Normal
fetus
Abnormal
fetus2
Amniocentesis4
Placenta
biopsies
(4 quadrants)5
NIPT result
type of
invasive test
cytogenetic
results
prenatal
diagnosis
cytogenetic
follow up
investigations
Chorionic villus sampling (mesenchymal core) 3
Placenta
biopsies
(4 quadrants)5
Van Opstal and Srebniak (2016), Expert Rev Mol Diagn. 2016 Feb 29:1-8.

Chromosome
aberration
Van Opstal and
Srebniak, 2016
(N= 704)
Grati et al 2015
(N= 1512)
Trisomie 13
8.3% 22%
Trisomie 18
3.2% 4%
Trisomie 21 1.6% 2%
Totaal 3.3% 3.9%
Risico op een 2de invasieve test
• Van Opstal and Srebniak, 2016, Exp Rev Mol Diagn
• Grati et al., 2015, Prenat Diagn, 35(10): p. 994-8
= risico op chromosomaal mosaicisme

Vruchtwater normaal hoogstwaarschijnlijk confined placental mosaicism
Bevestiging van NIPT:
Onderzoek van placenta na de geboorte:
min 4 biopten uit min 4 kwadranten
Bevestiging afwijkende NIPT na de geboorte
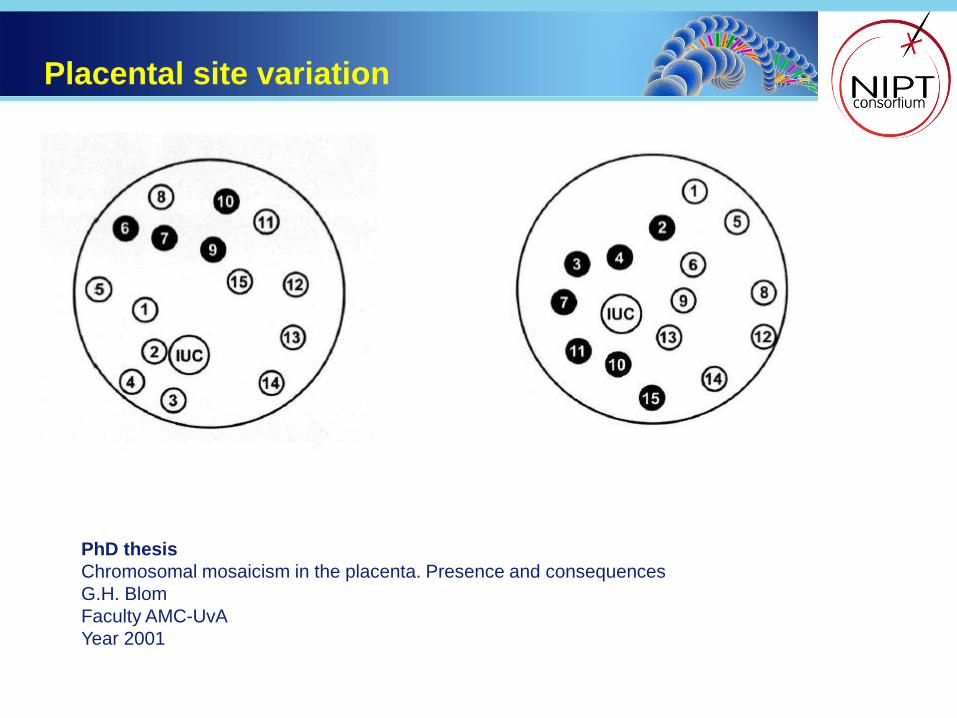
Placental site variation
PhD thesis
Chromosomal mosaicism in the placenta. Presence and consequences
G.H. Blom
Faculty AMC-UvA
Year 2001
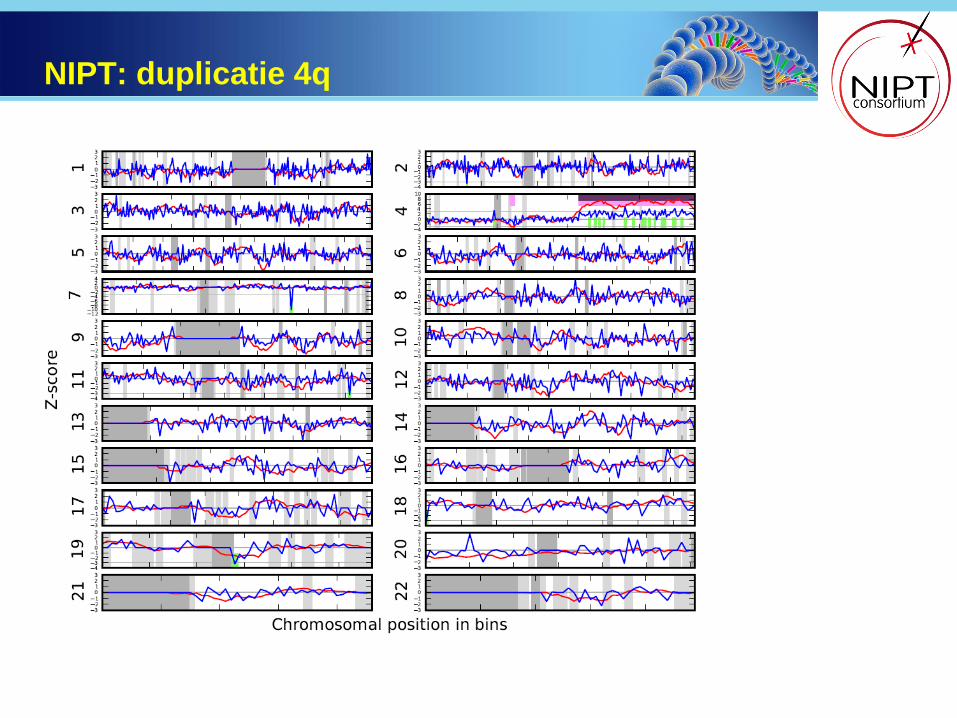
NIPT: duplicatie 4q

Vruchtwater: deletie 2

Placenta na TOP: deletie 2
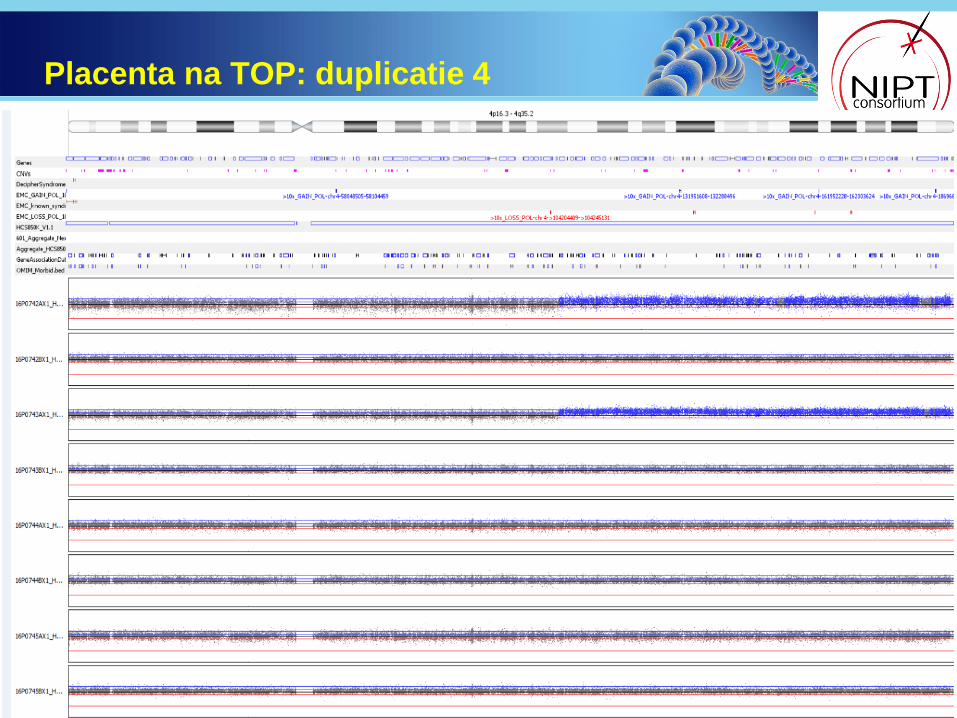
Placenta na TOP: duplicatie 4

De introductie van NIPT in Nederland heeft geleid tot een hoge uptake onder zwangeren
met een afwijkende CT (~86%) met als gevolg een reductie van invasieve ingrepen met
~62% (Oepkes et al., submitted, Prenat Diagn).
Hoge sensitiviteit en specificiteit voor detectie van tris 13, 18 en 21 (Oepkes et al.,
submitted, Prenat Diagn).
O.b.v. gebruikte techniek zijn nevenbevindingen te verwachten (1/3 van alle afwijkingen!):
Algoritme: foetale afwijkingen ≠ trisomie 13, 18 en 21
Oorsprong van het cel-vrije DNA:
-Moederlijk mozaiëk, CNV of maligniteit/benign tumor
-Confined placental mosaicism en/of vanishing twin
Vanwege de oorsprong van het gebruikte DNA is NIPT GEEN diagnostische test. Altijd
vervolgonderzoek noodzakelijk!
Vervolgonderzoek middels invasieve test: vlokkentest of vruchtwaterpunctie o.a. afhankelijk
van chromosoomafwijking
Indien vruchtwater normaal: bevestigingsonderzoek in placenta (min 4 biopten!)
•
• Indien NIPT normaal en later echo-afwijkingen -> indicatie voor invasief onderzoek
Conclusies

Acknowledgements
Janneke Weiss, VUMC
Merel van Maarle, AMC
Klaske Lichtenbelt, UMCU
Brigitte Faas, RUNMC
Voor cytogenetische FU:
Shama Bhola, VUMC
Karin Huijsdens, AMC
Mariëtte Hoffer, LUMC
Merryn Macville, MUMC
Angelique Kooper, RUNMC
Heleen Schuring-Blom, UMCU
Voor klinische FU:
Lutgarde C.P. Govaerts, Erasmus MC
Gita Tan, VUMC
Nicolette den Hollander, LUMC
Lieve Page-Christiaens, UMCU
Ilse Feenstra, RUNMC
Eramus MC, Rotterdam:
-Laboratorium van de afd Klinische Genetica
-labspecialisten klinische genetica:
Gosia Srebniak
Femke de Vries
Jeroen Knijnenburg
-Klinisch genetici:
Marieke Joosten.
Lutgarde Govaerts
Karin Diderich
Robert-Jan Galjaard
-gynaecologen: ErasmusMC, Albert Schweitzer
ZH, Reinier de Graaf ZH, Amphia ZH
Erik Sistermans, VUMC
Dick Oepkes, LUMC
Heleen Schuring – Blom, UMCU
Lieve Christiaens, UMCU
Robert-Jan Galjaard
Lidewij Henneman, VUMC
Alle consortium leden van alle disciplines
De TRIDENT studie werd mede mogelijk gemaakt door:
Nederlandse Organisatie voor Gezondheidsonderzoek en
Zorginnovatie (ZonMw) & Ministerie van Volksgezondheid,
Welzijn en Sport

Vragen?
Top Related