






Languages
Pages
Legal


ComplicatioComplications of ns of LaborLabor
( Dysfunctional Labor )( Dysfunctional Labor )

Dystocia (literally difficult labor) ► ► is characterized by abnormally slow progress in labor. It is characterized by abnormally slow progress in labor. It
is the consequence of four distinct abnormalities that is the consequence of four distinct abnormalities that may exist singly or in combination.may exist singly or in combination.
- Uterine forces that are not sufficiently strong or - Uterine forces that are not sufficiently strong or appropriately coordinated to efface and dilate the cervix. appropriately coordinated to efface and dilate the cervix.
- Forces generated by voluntary muscles during the second - Forces generated by voluntary muscles during the second stage of labor that are inadequate to overcome the normal stage of labor that are inadequate to overcome the normal resistance of the bony birth canal and maternal soft parts. resistance of the bony birth canal and maternal soft parts.
- Faulty presentation or abnormal development of the fetus of - Faulty presentation or abnormal development of the fetus of such character that the fetus cannot be extruded through the such character that the fetus cannot be extruded through the birth canal. birth canal.
- Abnormalities of the birth canal that form an obstacle to the - Abnormalities of the birth canal that form an obstacle to the descent of the fetus. descent of the fetus.

Hypotonic Uterine Contraction
► are infrequent, weak and of short duration.
General factors: - Primigravida particularly elderly. Primigravida particularly elderly. - Anaemia and asthenia. - Anaemia and asthenia. - Nervous and emotional as anxiety and fear. - Nervous and emotional as anxiety and fear. - Hormonal due to deficient prostaglandins or - Hormonal due to deficient prostaglandins or
oxytocin as oxytocin as in induced labour. in induced labour. - Improper use of analgesics. - Improper use of analgesics.
Local factors: - Overdistension of the uterus. - Overdistension of the uterus. - Developmental anomalies of the uterus e.g. - Developmental anomalies of the uterus e.g.
hypoplasia. hypoplasia. - Myomas of the uterus interfering mechanically with - Myomas of the uterus interfering mechanically with contractions. contractions. - Malpresentations, malpositions and cephalopelvic - Malpresentations, malpositions and cephalopelvic disproportion. The presenting part is not fitting in the disproportion. The presenting part is not fitting in the lower uterine segment leading to absence of reflex lower uterine segment leading to absence of reflex
uterine uterine contractions. contractions. - Full bladder and rectum. - Full bladder and rectum.

TypesTypesPrimary inertia: weak uterine contractions from the start. Primary inertia: weak uterine contractions from the start. Secondary inertia: inertia developed after a period of good Secondary inertia: inertia developed after a period of good
uterine contractions when it failed to overcome an uterine contractions when it failed to overcome an obstruction so the uterus is exhausted. obstruction so the uterus is exhausted.
Clinical PictureClinical Picture
- Labour is prolonged. - Labour is prolonged. - Uterine contractions are infrequent, weak and of short - Uterine contractions are infrequent, weak and of short duration. duration. - Slow cervical dilatation. - Slow cervical dilatation. - Membranes are usually intact. - Membranes are usually intact. - The foetus and mother are usually not affected apart from - The foetus and mother are usually not affected apart from maternal anxiety due to prolonged labour. maternal anxiety due to prolonged labour. - More susceptibility for retained placenta and postpartum - More susceptibility for retained placenta and postpartum haemorrhage due to persistent inertia. haemorrhage due to persistent inertia. - Tocography: shows infrequent waves of contractions with - Tocography: shows infrequent waves of contractions with low amplitude.low amplitude.
Hypotonic Uterine Contraction

Hypotonic Uterine Contraction
ManagementManagement
General measures:General measures: Examination to detect disproportion, malpresentation or Examination to detect disproportion, malpresentation or malposition and manage according to the case. malposition and manage according to the case. Proper management of the first stage (see normal labour). Proper management of the first stage (see normal labour). Prophylactic antibiotics in prolonged labour particularly if the Prophylactic antibiotics in prolonged labour particularly if the
membranes are ruptured. membranes are ruptured.
Amniotomy: Amniotomy: Providing that; Providing that;
vaginal delivery is amenable, vaginal delivery is amenable, the cervix is more than 3 cm dilatation and the cervix is more than 3 cm dilatation and the presenting part occupying well the lower the presenting part occupying well the lower
uterine segment. uterine segment. Artificial rupture of membranes augments the uterine Artificial rupture of membranes augments the uterine contractions by: contractions by:
release of prostaglandins. release of prostaglandins. reflex stimulation of uterine contractions when reflex stimulation of uterine contractions when the presenting the presenting part is brought closer to the lower uterine part is brought closer to the lower uterine segment. segment.

Oxytocin:Oxytocin: Providing that there is no contraindication for it, 5 Providing that there is no contraindication for it, 5 units of oxytocin (syntocinon) in 500 c.c glucose 5% units of oxytocin (syntocinon) in 500 c.c glucose 5% is given by IV infusion starting with 10 drops per minute is given by IV infusion starting with 10 drops per minute and increasing gradually to get a uterine contraction and increasing gradually to get a uterine contraction rate of 3 per 10 minutes. rate of 3 per 10 minutes.
Operative delivery: Operative delivery: Vaginal delivery: by forceps, vacuum or breech Vaginal delivery: by forceps, vacuum or breech extraction according to the presenting part and extraction according to the presenting part and
its its level providing that, level providing that, cervix is fully dilated. cervix is fully dilated. vaginal delivery is amenable. vaginal delivery is amenable.
Caesarean sectionCaesarean section is indicated in: is indicated in: failure of the previous methods. failure of the previous methods. contraindications to oxytocin contraindications to oxytocin
infusion including infusion including disproportion. disproportion. foetal distress before full cervical foetal distress before full cervical
dilatation.dilatation.
Hypotonic Uterine Contraction

Hypertonic Uterine Contraction
TypesColicky uterus: incoordination of the different parts of the Colicky uterus: incoordination of the different parts of the uterus in contractions. uterus in contractions. Hyperactive lower uterine segment: so the dominance of the Hyperactive lower uterine segment: so the dominance of the upper segment is lost. upper segment is lost.
Clinical Picture The condition is more common in primigravidae and characterised The condition is more common in primigravidae and characterised by: by:
- Labour is prolonged. - Labour is prolonged. - Uterine contractions are irregular and more painful. The - Uterine contractions are irregular and more painful. The
pain pain is felt before and throughout the contractions with marked is felt before and throughout the contractions with marked low backache often in occipito-posterior position. low backache often in occipito-posterior position. - High resting intrauterine pressure in between uterine - High resting intrauterine pressure in between uterine
contractions detected by tocography (normal value is 5-10contractions detected by tocography (normal value is 5-10 mmHg).
- Slow cervical dilatation . - Premature rupture of membranes. - Foetal and maternal distress.

Hypertonic Uterine Contraction
ManagementManagement
General measures:General measures:Examination to detect disproportion, Examination to detect disproportion,
malpresentation or malposition and manage according malpresentation or malposition and manage according to to the case. the case.
Proper management of the first stage (see Proper management of the first stage (see normal normal labour). labour).
Prophylactic antibiotics in prolonged labour Prophylactic antibiotics in prolonged labour particularly if the membranes are ruptured. particularly if the membranes are ruptured.
Medical measures:Medical measures: Analgesic and antispasmodic as Analgesic and antispasmodic as
pethidine. pethidine. Epidural analgesia may be of good Epidural analgesia may be of good
benefit. benefit.
Caesarean sectionCaesarean section is indicated in: is indicated in: Failure of the previous methods. Failure of the previous methods. Disproportion. Disproportion. Foetal distress before full cervical Foetal distress before full cervical
dilatation. dilatation.

Abnormal Labor
Nullipara Multipara
Prolonged latent phase 20 hr or more20 hr or more 14 hr or more14 hr or more
Protracted active phase 1.2 cm/hr or less1.2 cm/hr or less
Protracted descent 1 cm/hr or less1 cm/hr or less 2 cm/hr or less2 cm/hr or less
Prolonged deceleration phase 3 hr or more3 hr or more 1 hr or more1 hr or more
Secondary arrest of dilatation
Arrest 2 hr or more
Arrest of descent Arrest 1 hr or more
Failure of descent No descent in deceleration phase of second stage

Abnormal Labor
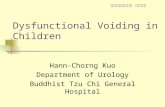
Prolonged Latent Phase
Factors that appear to be responsible for the development of prolonged Factors that appear to be responsible for the development of prolonged latent phase disorders in multiparas most often include excessive latent phase disorders in multiparas most often include excessive sedation administered during the course of the latent phase and poor sedation administered during the course of the latent phase and poor prelabor soft-tissue preparation. In addition, false labor and myometrial prelabor soft-tissue preparation. In addition, false labor and myometrial dysfunction are found but can be diagnosed only retrospectively. dysfunction are found but can be diagnosed only retrospectively.
Prolonged Latent Phase Pattern(Green Line)
* Normal Curve (Violet Line)

Abnormal LaborArrest disorders
Etiology of arrest disorders are as follows. The striking Etiology of arrest disorders are as follows. The striking association with cephalopelvic disproportion makes these association with cephalopelvic disproportion makes these disorders especially ominous; whenever encountered, arrest disorders especially ominous; whenever encountered, arrest patterns should signal the likelihood that a bony impediment patterns should signal the likelihood that a bony impediment exists. Other factors very often occur in combination with each exists. Other factors very often occur in combination with each other and with disproportion as well. other and with disproportion as well.
A.A. Secondary arrest of dilatationSecondary arrest of dilatation pattern with documented pattern with documented cessation ofcessation of progression in the active phase
B. Prolonged deceleration phase pattern with deceleration phase duration greater than normal limits
C. Failure of descent in the deceleration phase and second stage
D. Arrest of descent characterized by halted advancement of fetal station in the second stage.
* Normal dilatation and descent curves (broken lines)

PRECIPITATE LABOR
► A labour lasting less than 3 hours.
It is more common in multiparas when there are;It is more common in multiparas when there are;- strong uterine contractions, - strong uterine contractions, - small sized baby, - small sized baby, - roomy pelvis, - roomy pelvis, - minimal soft tissue resistance. - minimal soft tissue resistance.
Complications Maternal:
- Lacerations of the cervix, vagina and perineum. - Shock. - Inversion of the uterus. - Postpartum haemorrhage:
* no time for retraction, lacerations. - Sepsis due to:
* lacerations, inappropriate surroundings.

PRECIPITATE LABOR Foetal:Foetal: - Intracranial haemorrhage due to sudden compression - Intracranial haemorrhage due to sudden compression
and and decompression of the head. decompression of the head. - Foetal asphyxia due to: - Foetal asphyxia due to:
strong frequent uterine contractions strong frequent uterine contractions reducing reducing placental perfusion, lack of placental perfusion, lack of immediate resuscitation. immediate resuscitation.
- Avulsion of the umbilical cord. - Avulsion of the umbilical cord. - Foetal injury due to falling down. - Foetal injury due to falling down.
ManagementManagement Before deliveryBefore delivery
Patient who had previous precipitate labour should be Patient who had previous precipitate labour should be hospitalized before expected date of delivery as she is more hospitalized before expected date of delivery as she is more prone prone to repeated precipitate labour.to repeated precipitate labour. During delivery
Inhalation anaesthesia: as nitrous oxide and oxygen is given to slow the course of labour.
Tocolytic agents: as ritodrine (Yutopar) may be effective. Episiotomy: to avoid perineal lacerations and intracranial haemorrhage.
After deliveryExamine the mother and foetus for injuries.

CONSTRICTION (CONTRACTION) RINGCONSTRICTION (CONTRACTION) RING
► ► It is a persistent localized annular spasm of the circular uterine It is a persistent localized annular spasm of the circular uterine muscles. muscles. ► ► It occurs at any part of the uterus but usually at junction of the It occurs at any part of the uterus but usually at junction of the upper and lower uterine segments. upper and lower uterine segments. ► ► It can occur at the 1st, 2nd or 3 rd stage of labour. It can occur at the 1st, 2nd or 3 rd stage of labour.
Predisposing factors are: Predisposing factors are: - Malpresentations and malpositions. - Malpresentations and malpositions. - Clumsy intrauterine manipulations under light - Clumsy intrauterine manipulations under light
anaesthesia. anaesthesia. - Improper use of oxytocin e.g. use of oxytocin in - Improper use of oxytocin e.g. use of oxytocin in
hypertonic inertia. hypertonic inertia. - IM injection of oxytocin. - IM injection of oxytocin.
Diagnosis- The condition is more common in primigravidae and
frequently preceded by colicky uterus. - The exact diagnosis is achieved only by feeling the ring with a hand introduced into the uterine cavity.

CONSTRICTION (CONTRACTION) RINGCONSTRICTION (CONTRACTION) RING
Complications- Prolonged 1st stage: if the ring occurs at the level of Prolonged 1st stage: if the ring occurs at the level of
the internal os. the internal os. - Prolonged 2nd stage: if the ring occurs around the - Prolonged 2nd stage: if the ring occurs around the
foetal neck. foetal neck. - Retained placenta and postpartum haemorrhage: - Retained placenta and postpartum haemorrhage:
if the ring occurs in the 3rd stage (hour- glass if the ring occurs in the 3rd stage (hour- glass contraction). contraction).
Management- Exclude malpresentations, malposition and disproportion. Exclude malpresentations, malposition and disproportion. - In the 1st stage: Pethidine may be of benefit. - In the 1st stage: Pethidine may be of benefit.
- In the 2nd stage: Deep general anaesthesia and amyl - In the 2nd stage: Deep general anaesthesia and amyl nitrite nitrite inhalation are given to relax the constriction ring: inhalation are given to relax the constriction ring:
- If the ring is relaxed, the foetus is delivered - If the ring is relaxed, the foetus is delivered immediately by immediately by forceps. forceps.
- If the ring does not relax, caesarean section is carried out with lower segment vertical incision to divide the ring.
- In the 3rd stage: Deep general anaesthesia and amyl nitrite inhalation are given followed by manual removal of the
placenta.

Physiological Retraction Ring
- It is a line of demarcation between the upper and - It is a line of demarcation between the upper and lower uterine segment present during normal labor and lower uterine segment present during normal labor and cannot usually be felt abdominally.cannot usually be felt abdominally.
Pathological Retraction Ring (Bandl’s ring)Pathological Retraction Ring (Bandl’s ring)
- It is the rising up retraction ring during obstructed It is the rising up retraction ring during obstructed labour due to marked retraction and thickening of the labour due to marked retraction and thickening of the upper upper uterine segment while the relatively passive lower uterine segment while the relatively passive lower segment segment is markedly stretched and thinned to is markedly stretched and thinned to accommodate the accommodate the foetus. foetus.
- - The Bandl’s ringThe Bandl’s ring is seen and felt abdominally as a is seen and felt abdominally as a transverse groove that may rise to or above thetransverse groove that may rise to or above the umbilicus.
- Clinical picture: is that of obstructed labour with impending rupture uterus (see later).
Obstructed labour should be properly treated otherwise the thinned lower uterine segment will rupture.

Abnormalities of PlacentaAbnormalities of Placenta

Bi lobate placenta

Placenta succenturiata
• A small part of the A small part of the placenta is separate placenta is separate from the main massfrom the main mass

Battledore placenta
• The umbilical cord is The umbilical cord is attached to the attached to the periphery.periphery.

Velamentous placenta
• The umbilical vessels The umbilical vessels divide into many divide into many branches before branches before entering placentaentering placenta

Circumvallate placenta

► ► placenta implantation at the lower segment of the placenta implantation at the lower segment of the uterus.uterus.
► ► obstructing the descent of the baby’s head.obstructing the descent of the baby’s head.
► ► presented with antepartum hemorrhage. presented with antepartum hemorrhage.
Placenta Previa

Placenta Previa

End…End…Prepared by:
Eloise M. Pateño Nr-22
Top Related