



Languages
Pages
Legal

Coagulation DisordersCorrina Mc Mahon
Laboratory investigationsPT: VII, X, V
APTT; XII, XI, IX, VIII
TT; Fibrinogen
D dimers; fibrin breakdown
Case 14 yr old boyURTI 2 weeks agoSudden onset bruising/petechiaePH: NilFH: NilPhysical examination:
Congenital ThrombocytopeniaDysfunctional plateletsBernard SoulierGrey platelet syndromeWiskott-Aldrich syndrome
Normal Platelet functionMay-HegglinTAR
Case 2Newborn infantIntracranial HaemorrhageNo dysmorphic features1st childNo liver/spleen palpableFBCHb 18.5g/dlWCC 10 x x 109/l /lPlatelets 10 x 109/l /l
Coagulation screenPT 15 sec. (13-16)APTT 41 sec (28-36)
Differential diagnosisInfectionDICImmune ThrombocytopeniaAlloimmuneIsoimmuneCongenital ThrombocytopeniaTAR syndromeWiscott Aldrich SyndromeVon Willebrands diseaseType 2BA-V malformations
Alloimmune ThrombocytopeniaIncidence 1:1000-5000 birthsIgG antibodiesHPA1a 80% HPA5b 15%50% occur in 1st pregnancyBleeding can be in utero or after birth
TreatmentPlateletsIVIg?Steroids
Isoimmune Thrombocytopenia Maternal anti-platelet IgGPlacental PassageThrombocytopenia nadir ~5days post-partumHistory & examination of motherTreatmentIvIg steroids
Disseminated Intravascular CoagulopathyInfection
Symptoms and SignsPetechiaeBruisingBleeding
Laboratory resultsAnaemiaThrombocytopeniaPT/ APTT/Fibrinogen/ d dimers
HaemophilaInherited Bleeding Disorder
Factor VIII/FIX deficiency
X-Linked InheritanceCarrier XX may have low levels
Spontaneous mutation
Inheritance of Haemophilia
Life Expectancy In Haemophilia
Bleeding problems in HaemophiliaFactor LevelType of Bleed5%Trauma/Surgery
Intracranial BleedsAt BirthInjury
AdmissionFactor ConcentrateScanningObservationNeurosurgery
Forearm Bleed
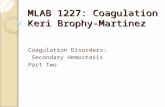
Joint bleedSynovial inflammation and hyperaemiaSynovial overgrowth and Bone resorptionFurther BleedJoint Destruction
Joint Bleeding
Chronic Joint Bleeding
The role of prophylaxis in the prevention of joint injury
Lofqvist, Nilsson et al ( Journal Int. Medicine May 1997): 34 patients aged 7-22yrs. Age at commencement of prophylaxis - 1-4.5yrs. 79% had no joint problems and the rest had no deterioration in joint abnormalities.
Liesner,Khair, Hann, ( BJH Mar 1996)27 children aged 1.3-15.9yrs. No. of bleeds/yr pre-prophylaxis-14.5 and post - 1.5. 20 children had evidence of arthropathy which improved on prophylaxis.
Prophylaxis The Irish Data (1992-1997)
Bleeds/yr, pre-prophylaxis, 9.5-106 (mean 38)
Bleeds/yr, post-prophylaxis, 0-9 (mean 3.5)
Development of inhibitors, 2 - low level (
ProphylaxisFactor VIII
T = 8 hoursFrequency three times/weekDose 20-40iu/kgFactor IX
T = 18 hoursFrequency twice/weekDose 50iu/kg
Dose AdjustmentGrowth
Break through bleeds
Management of Acute BleedsRest
Factor ConcentrateFVIII; 35-50iu/kgFIX; 70-100% (7-10iu/ml)Wt x desired rise x 1.25Continuous infusionFVIII50iu/kg bolus; infusion 4iu/kg/hrFIX100% bolus; infusion 6-8iu/kg/hr
Mild Factor VIII DeficiencyFactor VIII
DDAVP0.3mcg/kg/30 min
Antifibrinolytic therapy
Haemophilia The problems
BleedingDestructive arthropathyAddictionInfectionInhibitors
Management of InhibitorsAcute Bleeding episodesFVIIa
Immune ToleranceHigh Dose 200-300iu/kg/d x 1-3 yrsCyclophosphamide/FVIII/IVIg50iu/kg/d x 1->12m25iu/kg/d x 1->12m
Von Willebrands DiseaseAutosomal InheritanceAbnormal VWFS/S: easy bruising, mucosal bleeds, heavy periodsTreatment: antifibrinolytic agentsDDAVPPlasma derived factor (Fanhdi)Lab Investigations
FVIIIcVWF:AgVWF:RCFBleeding timeVWF Multimers
Top Related