







Languages
Pages
Legal


Outcome of the Cervix Uteri Cancer Patients Treated with ConcurrentChemo-radiotherapy Incorporating High Dose Rate Brachytherapy
A Retrospective Single Institution Study In Saudi Arabia
Mohamed Ezzat. El Sayed, Yasir Abdulaziz Bahadur, Ashraf Hamed
Hassouna , Ehab Esmat Fawzy , Azza Mohamed Nasr , Bakr Ben Sadiq,
Reyad Dada , Khalid Husenin Sait and Nisrin Mohamed Anfinan
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Conflict of interest
The authors have no conflict of interest to declare
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Introduction
Cervix uteri cancer is the second most common cancer among women worldwide and
the most common cancer affecting women in sub- Saharan Africa, Central America and
South-central Asia [Parkin DM, etal 2005].
The incidence of cervical cancer in Saudi women is low. The current estimates indicate
that every year, 152 women will be newly diagnosed with cervical cancer and 55 will
die from the disease in Saudi Arabia [International Cancer Screening Network2008
&Cancer Incidence Report Saudi Arabia 2005].
High dose-rate intra-cavitary brachytherapy (HDR-ICBT) in combination with external
beam irradiation (EBRT) has become the standard treatment for localized cervix uteri
cancer [Toita T.etal 1999].Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Introduction
• In 1999, after publication of 5 trials, the National Cancer Institute (NCI) issued an
alert recommending that ’Concomitant chemo radiotherapy should be considered
instead of radiotherapy alone in women with cervical cancer’. This has led to a
worldwide change in the treatment cervix uteri cancer [Toita T. etal 1999 &Trimble E.
etal 2007].
• The Cochrane Gynecological Group concluded in a meta-analysis that: there is a 6%
improvement in 5-year survival rate with chemo - radiotherapy (hazard ratio (HR) =
0.81, P <0.001), and significant survival benefit for both platinum-based (HR =0.83, P
=0.017) and non-platinum based (HR=0.77,P=0.009) chemo-radiotherapy. Furthermore
chemo-radiotherapy also reduced local and distant recurrence and improved disease-
free survival (DFS) [Vale C. et al 2008].Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Aim of the study& Methods
Aim of the study: A retrospective study evaluating the survival
outcome, pattern of failure and prognostic factors of using concurrent
chemo-radiotherapy (CRT) and high dose rate brachytherapy ( HDR-
BT)in cervix uteri cancer patients.
Methods: We reviewed the data of 60 cervix uteri cancer patients
with stages IB-IVA; treated with radiotherapy with and without
concurrent Cisplatin plus HDR-BT; between January 2004 and
December 2010.
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Results
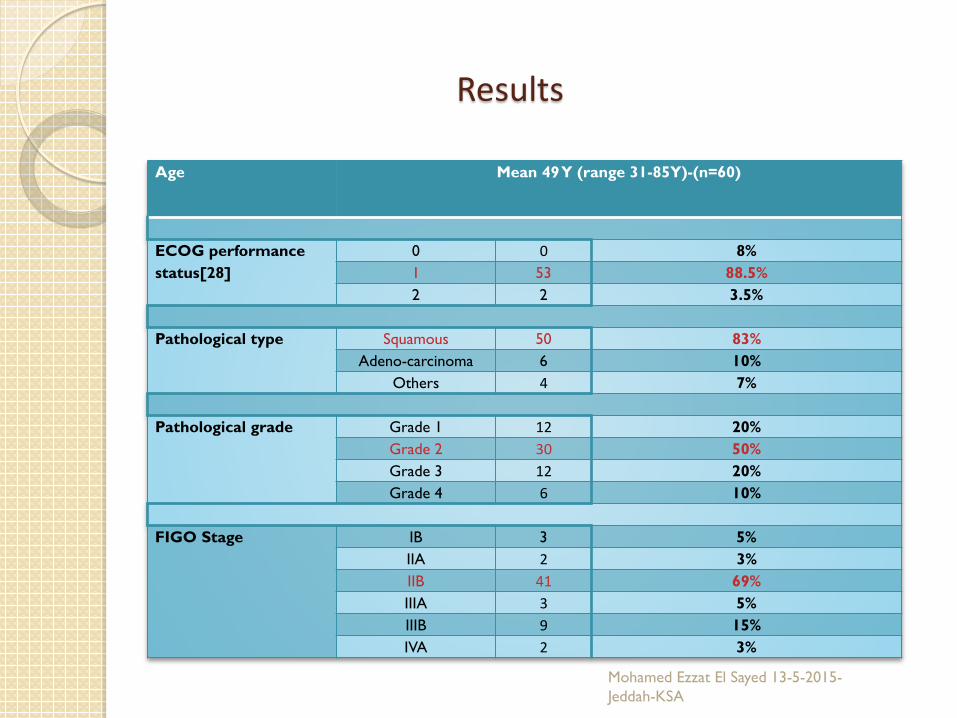
Mean 49 Y (range 31-85Y)-(n=60)Age
8%00ECOG performance status[28] 88.5%531
3.5%22
83%50SquamousPathological type 10%6Adeno-carcinoma7%4Others
20%12Grade 1Pathological grade 50%30Grade 220%12Grade 310%6Grade 4
5%3IBFIGO Stage 3%2IIA
69%41IIB5%3IIIA15%9IIIB3%2IVA
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
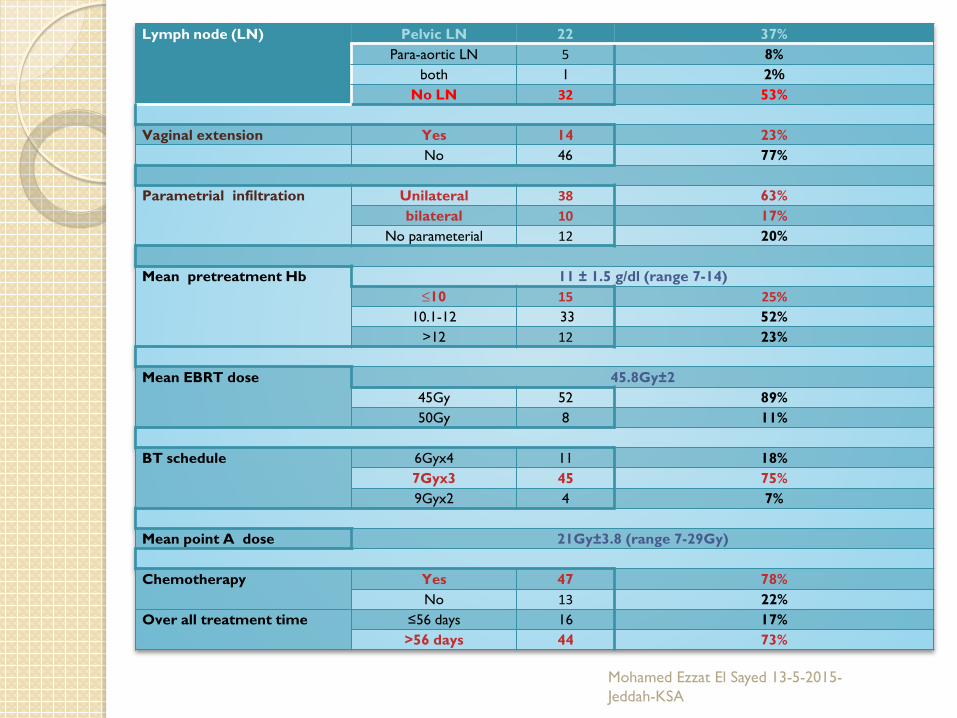
37%22Pelvic LNLymph node (LN)8%5Para-aortic LN%21both
53%32No LN
23%14YesVaginal extension77%46No
63%38UnilateralParametrial infiltration 17%10bilateral20%12No parameterial
11 ± 1.5 g/dl (range 7-14)Mean pretreatment Hb25%15≤1052%3310.1-1223%12>12
45.8Gy±2Mean EBRT dose 89%5245Gy11%850Gy
18%116Gyx4BT schedule 75%457Gyx37%49Gyx2
21Gy±3.8 (range 7-29Gy)Mean point A dose
78%47YesChemotherapy 22%13No17%16≤56 daysOver all treatment time 73%44>56 days
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Results (cont.)
For those 60 patients, 186 applications were done, the mean dose to point A was 6.5 ± 1.1 Gy
The mean total physical dose to the point A from BT was 21 ±3.8 Gy (range 7-29 Gy), with the mean
total physical dose to point A from EBRT and BT of 45.8 Gy + 21Gy = 66.8 Gy.
The mean value of the maximal point dose to the rectum from EBRT and BT was 56.2 ± 4 Gy (between
49.1- 65.2 Gy ).
The mean of the maximal point dose (ICRU) to the bladder from EBRT and BT was 57.7 ±4.3Gy(
between 49.4- 68.1Gy).
Converting these physical dose to biologically effective dose using linear quadratic model; the
isoeffective total dose (EBRT+BT) EQD2; given a total doses in 2 Gy and α/β of 10 Gy for the tumor and 3
Gy for the rectum and the bladder; was found equivalent to 74.9 Gy to point A dose,73.1 Gy as a maximal
dose to the bladder, and 67.4 as a maximal dose to the rectum (with our constraints for BT were 80% of
the fraction dose; 5.6 Gy to the bladder point/2cc volume and 70 % of the fraction dose; 4.9 Gy to the
rectal point/2 cc volume). Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
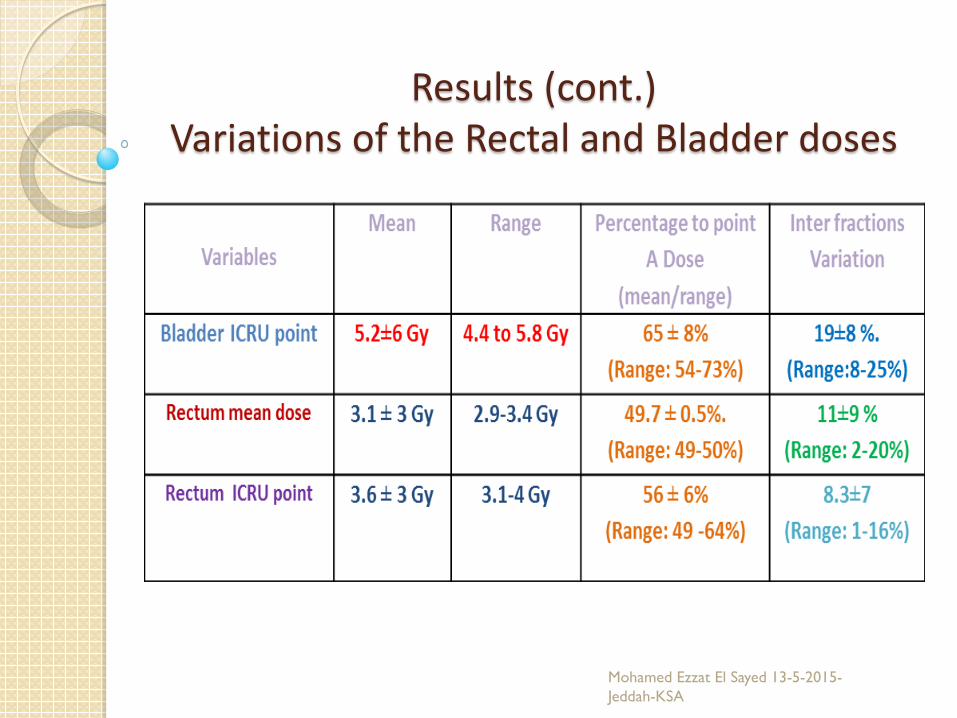
Results (cont.)Variations of the Rectal and Bladder doses
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
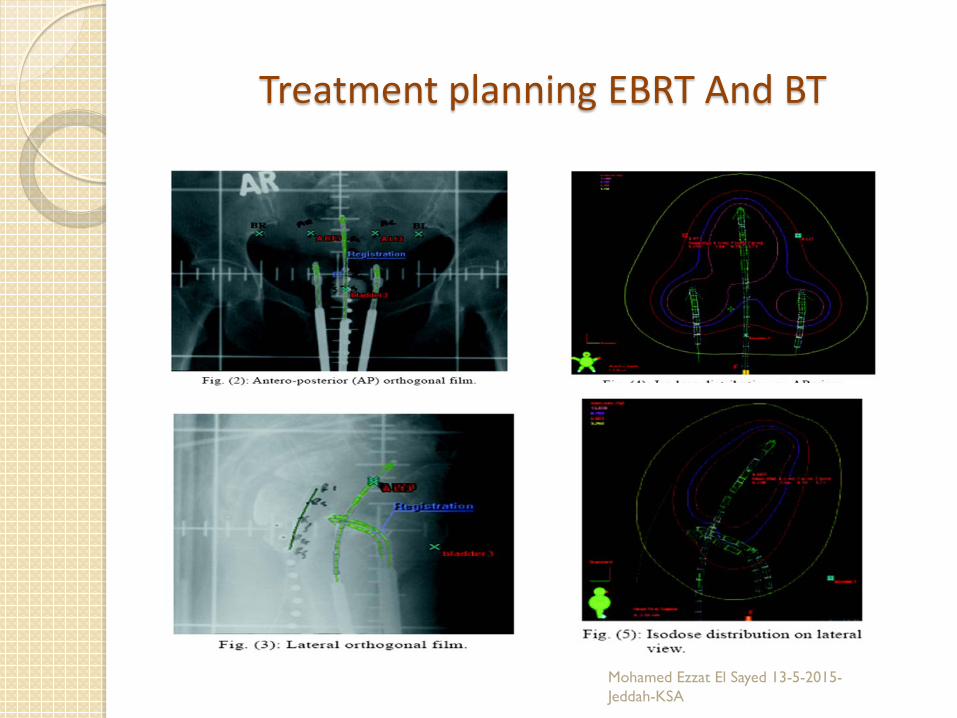
Treatment planning EBRT And BT
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
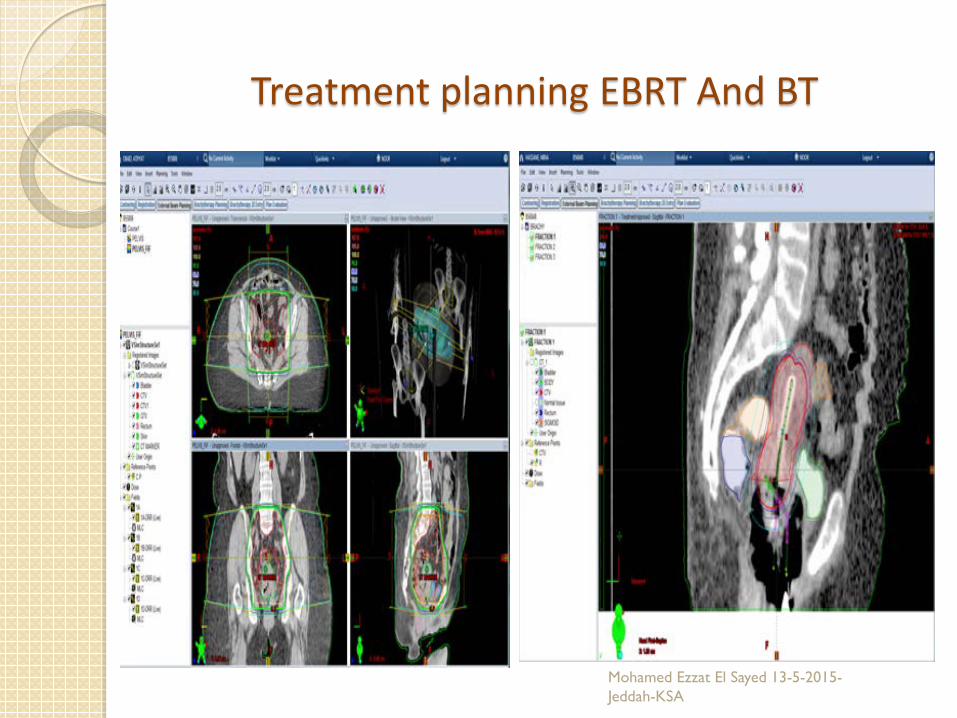
Treatment planning EBRT And BT
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Results (cont.) The median follow up period was 24 months (range,6-77
months). The 2 and 4 years overall survival(OAS) was 82%,and 79%
respectively. Prolongation of the overall treatment time(OAT) more than
56 days and the pretreatment hemoglobin(Hb)level (˂10g/dL)negatively predict the OS(p=0.039 and p=0.008 respectively).
The 2 and 4 years disease free survival(DFS)were 80% and 69% respectively, with vaginal extension as the only significant factor predicting the relapse(p=0.048).
The 2 and 4 years loco-regional and distant metastasis free survival were 78% & 70% and 82%&79% respectively.
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Results (cont.)The distribution of relapses
Type of relapse Number of patients relapsed (%)
Loco regional alone 5 (8)
Loco regional + systemic 10 (17)
Total 15 (25)
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Toxicities and side effects All patients tolerate their treatment well without reported acute grade 3 or 4 skin ,
urinary, rectal, gastro intestinal or hematological toxicities , the majority reported grade 1 or
2 reactions and treated with appropriate medical and supportive measures .
Three patients (5%) developed late urinary reactions in the form of grade 1 or 2 dysuria
and frequency of micturition together with radiological thickening of the bladder wall,
however no grade 3 or 4 late urinary bladder reactions were reported.
Six (10 %) patients had late rectal reactions, it was grade 1 or 2 in 4 patients (7%), and
grade 3 or 4 in 2 patients (3 %); one patient developed grade 3 proctitis, and the other one
developed recto-vaginal fistula (grade 4). A vaginal adhesion was reported only in one patient
(1.7%) who required frequent vaginal dilation.
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Summaries of the results of the previously published series of chemo-radiotherapy incorporating HDR-BT in cervix uteri cancer patients
Number FIGO StageOS (%) (5years unless stated)
LRC rate (%)Median follow up
in , monthsGrade
Study Country of patients I, II,III, and IV (5 years unless
stated Grade 3or 4 late
reactionpatients
Lim A and Sia S 2011[24 ]
Western Australia 69 18, 28,17,and 1 61(4 year) 70.1 (4 y) 27 4(5.8%)
Teh et al 2010 [25]
Singapore 120 7,53,36,and 4 65 81.7 50 5(4%)
Parker et al 2009 [26]
UK 92 8,63,26,and 0 55 67 26 4(4%)
Atahan et al2007 [27]
Turkey 100*/183 10,64,26,and 0 55 74 45 8(8%)
Novetsky et al 2007[(28]
United Sates 10060(I-II)and40(III
and IV)82
88% for stage I-II,65%for stage
III/IV42 5(6%)
Chen et al 2006 [29]
Taiwan 70 0,69,31,and0 74(4year) 87% 43 11(14.3%)
Current study Saudi Arabia 60 3,43,12,and2 79(4year) 70 (4Y) 24 2(3%)Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Conclusion and limitation of the study
• Although our retrospective study with its inherit bias; it display the efficacy of concomitant
cisplatin based chemo-radiotherapy incorporating HDR-BT and relevant prognostic factors for
local control and survival in accordance with the published literature.
• While local and distant failure are yet to be solved in this group of patients, ongoing research
and advances in image guided and intensity modulated radiotherapy as well as progress in
systemic therapy seem to be promising in the future.
• The limitations of this study are the small sample size with wide range of tumor stages treated
and inclusion of different methods of brachytherapy fractionation/planning. These concerns
limit the results of the multivariate analysis. National studies that include data across the
country from all the centers are highly appreciated and desired.Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Future directions & recommendations
Increase the BT by change the schedule to 8Gyx3 with attention to the critical organ doses.
Use of applicator that can deliver higher and conformal dose to the vaginal extension.
MRI guided brachytherapy
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Acknowledgement:
The authors would like to acknowledge our patients for their patience
during their course of treatment, and to our head nurse and patients
educator Mrs. Asma Adel , Mrs. Molly Kuriakose; our brachytherapy
nurse and to all our colleagues in dosimetery and physics .

Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA

THANK YOU
Mohamed Ezzat El Sayed 13-5-2015-Jeddah-KSA
Top Related