







Languages
Pages
Legal

Cause for Concern Process
Guidelines for Supervisors of Midwives
North of Scotland Local Supervising Authority Consortium
2
Guideline produced by: Supervisors Quality Improvement Group (SQIG)
Guideline production date: Version 1: May 2009
Version 2: January 2013, updated August 2013
Consultation process: North of Scotland LSA Consortium
Draft reviewed by: Supervisors Quality Improvement Group
Guideline approved by: North of Scotland LSA Consortium
Guideline approval date: 26/08/2013
Guideline Implementation date: 01/09/2013
Guideline review date: January 2016
Paper copies of this guideline may not be the most recent version. The definitive version is
held at http://www.midwiferysupervision-noslsa.scot.nhs.uk
3
Contents
Introduction ............................................................................................................................ 4
Process.................................................................................................................................. 5
Local Action Plan ................................................................................................................... 6
Outcome ................................................................................................................................ 6
References ............................................................................................................................ 7
Appendix 1: Cause for Concern Flow Chart ........................................................................... 8
Appendix 2: Cause for Concern Form .................................................................................. 10
Appendix 3: Supervisory review/fact finding event chronology ............................................. 13
Appendix 3a: Example of supervisory review/fact finding event chronology - no concerns-
good practice identified .................................................................................................... 15
Appendix 3b: Example of supervisory review/fact finding event chronology - SoM
investigation not recommended but some issues identified .............................................. 18
Appendix 3b: Example of supervisory review/fact finding event chronology - SoM
investigation recommended .............................................................................................. 21
Appendix 4: Local Action Plan ............................................................................................. 24
Appendix 4a: Example of a Local Action Plan .................................................................. 25

4
Introduction
Local Supervising Authorities (LSA) are organisations within geographical areas, responsible
for ensuring that statutory supervision of midwives is undertaken according to the standards
set by the Nursing and Midwifery Council (NMC) under article 43 of the Nursing and
Midwifery Order 2001, details of which are set out in the NMC Midwives rules and standards
(NMC 2012). In Scotland, the function of the LSAs is provided by the Health Boards, which
are arranged into two Regions: the South East and West of Scotland and the North of
Scotland.
Each LSA has an appointed LSA Midwifery Officer (LSAMO) to carry out the LSA function.
The LSAMOs are practising midwives with experience in statutory supervision and provide
an essential point of contact for Supervisors of Midwives to consult for advice on aspects of
supervision. Members of the public who seek help or support concerning the provision of
midwifery care, can also contact the LSAMO directly. LSAMOs provide leadership, support
and guidance on a range of matters including professional development. They also
contribute to the wider NHS agenda by supporting public health and interprofessional
activities at Health Board level.
The Supervisor of Midwives role includes supporting midwives to develop and improve their
practice. This includes giving advice to individual midwives and/or their employers when
additional support is needed for a midwife to ensure safety for the public. For example when
a midwife
� Needs support to learn a new skill or role required for the employment
� Needs to orientate to a new organisation or department
� Has returned to the workplace after an absence and needs support to gain
confidence
� Has requested additional support to aid personal or professional development
� Has identified a problem with their own practice that they need support with
� Has made a minor mistake, with little or no risk of recurrence
Such circumstances can be corrected through a local action plan with the named supervisor
of midwives. This may include reflection on an incident or undertaking continuing
professional development relevant to the issue that caused concern.
5
The purpose of this guideline is to help Supervisors of Midwives determine when and how to
initiate the cause for concern process and when to escalate to the LSA via the LSAMO.
Raising a Cause for Concern by Supervisors of Midwives
Raising and communicating a cause for concern should primarily be viewed as a positive and
supportive procedure for the midwife concerned and an area where the primary focus of
support will be through the supervisory structure.
It is better to report an issue of concern early, waiting and hoping for an improvement may
delay effective intervention. The process should be used to structure feedback and monitor
the midwife’s progress.
The process is outlined below and summarised in appendix 1.
Process
A cause for concern should be initiated if following discussion between a midwife and her line
manager and or a Supervisor of Midwives there is no resolution regarding her
� competence
� conduct
� involvement in a clinical incident
The initiation of the cause for concern must be communicated to the midwife, her named
Supervisor of Midwives and her line manager/ team leader.
A review of the concerns raised will be undertaken by the midwife’s named Supervisor of
Midwives, or if this is not possible, another Supervisor of Midwives within the area. At this
stage a cause for concern form should be commenced (appendix 2).
If the cause for concern involves a clinical incident a supervisory review/fact finding event
chronology (appendix 3) should also be completed to determine whether a supervisory
investigation is required. If it is determined that a supervisory investigation is not required but
6
the midwife (s) has made a minor mistake, with little or no risk of recurrence then the cause
for concern process should be followed and a local action plan put in place.
In order to ensure the process encourages reflection on practice and maintains the purpose
of a supportive intervention it is imperative that midwives receive feedback via letter or email
when care and support has been found to be effective, appropriate and safe following a
critical incident.
Local Action Plan
The named Supervisor of Midwives needs to ensure that the midwife receives the necessary
support to enable, where possible, an early resolution to the situation. This might include the
following
� review of shift patterns
� review of work environment
� occupational health referral
The Supervisor of Midwives will meet with the midwife to discuss with her the concerns
raised and agree a local action plan and regular feedback times and review dates (appendix
4). It is expected that the midwife, will demonstrate that she has successfully achieved the
competencies/objectives set in the local action plan within 4 weeks of commencement.
Outcome
Once a local action plan has been put in place the Supervisor of Midwives should inform the
LSAMO of the cause for concern and progress made by the midwife.
Possible outcomes that will result from the local action plan are as follows
� cause for concern resolved – no further action required
� cause for concern unresolved
� repeated concerns raised
7
If the cause for concern remains unresolved or repeated concerns arise about the midwives
competence and/ or conduct the Supervisor of Midwives will write a report and forward this to
the LSAMO for guidance and advice about the next steps to be taken.
It is important to note that where a cause for concern involves a serious untoward clinical
incident, intractable incompetence or serious misconduct a supervisory investigation must be
carried out in accordance with the LSAMO Forum UK guideline Supervisory Investigation into
a midwife’s fitness to practise (appendix 1).
References
LSAMO Forum UK 2013 Supervisory Investigation into a midwife’s fitness to practise.
Available online @ http://www.lsamoforumuk.scot.nhs.uk/policies-guidelines.aspx
Nursing and Midwifery Council 2012 Midwives rules and standards. London: NMC
The Nursing and Midwifery Order. SI 2002 No. 253. Available online @
http://www.opsi.gov.uk/si/si2002/20020253.htm
8
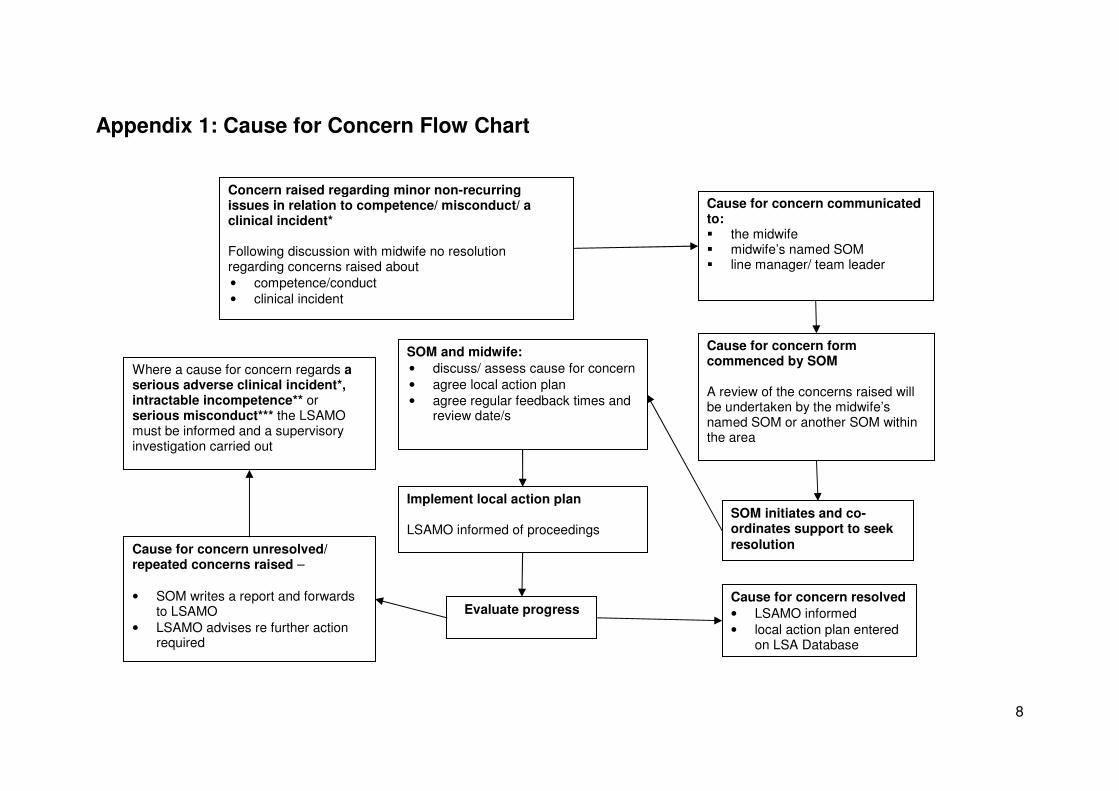
Appendix 1: Cause for Concern Flow Chart
Cause for concern form commenced by SOM
A review of the concerns raised will be undertaken by the midwife’s named SOM or another SOM within the area
Cause for concern communicated to: � the midwife � midwife’s named SOM � line manager/ team leader
SOM initiates and co-ordinates support to seek
resolution
Cause for concern resolved
• LSAMO informed
• local action plan entered on LSA Database
SOM and midwife:
• discuss/ assess cause for concern
• agree local action plan
• agree regular feedback times and review date/s
Implement local action plan LSAMO informed of proceedings
Evaluate progress
Cause for concern unresolved/ repeated concerns raised –
• SOM writes a report and forwards to LSAMO
• LSAMO advises re further action required
Concern raised regarding minor non-recurring issues in relation to competence/ misconduct/ a clinical incident* Following discussion with midwife no resolution regarding concerns raised about
• competence/conduct
• clinical incident
Where a cause for concern regards a serious adverse clinical incident*, intractable incompetence** or serious misconduct*** the LSAMO must be informed and a supervisory investigation carried out

9
*In this context, a clinical incident is any situation that raises concern that the public are being put at risk. However if the incident is serious
please refer to the Monitoring & Reporting Serious Incidents & Events Guideline
** Lack of competence is a lack of knowledge, skill or judgement of such a nature that the registrant is unfit to practise safely and effectively in any field in which the registrant claims to be qualified, or seeks to practise
Examples of lack of competence include:
� persistent lack of ability in correctly and/or appropriately calculating administering and recording the administration or disposal of medicines
� persistent lack of ability in properly identifying care needs and, accordingly, planning and delivering appropriate care
*** Misconduct is conduct, which falls short of that which can reasonably be expected of a registrant.
The most common examples of misconduct include:
� physical or verbal abuse
� theft
� deliberate failure to deliver adequate care
� deliberate failure to keep proper records
10
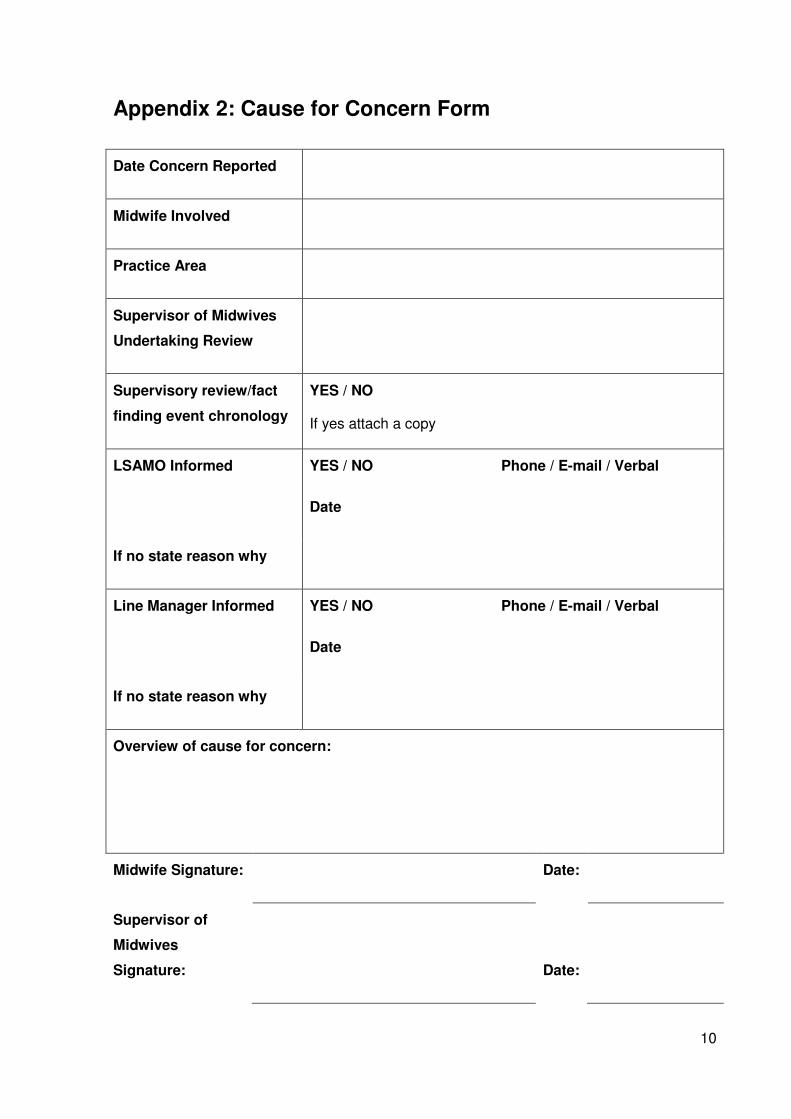
Appendix 2: Cause for Concern Form
Date Concern Reported
Midwife Involved
Practice Area
Supervisor of Midwives
Undertaking Review
Supervisory review/fact
finding event chronology
YES / NO
If yes attach a copy
LSAMO Informed YES / NO Phone / E-mail / Verbal
Date
If no state reason why
Line Manager Informed YES / NO Phone / E-mail / Verbal
Date
If no state reason why
Overview of cause for concern:
Midwife Signature:
Date:
Supervisor of
Midwives
Signature:
Date:

11
Agreed Action / Process:
Action carried out by:
Midwife Signature: Date:
Supervisor of
Midwives
Signature: Date:
12
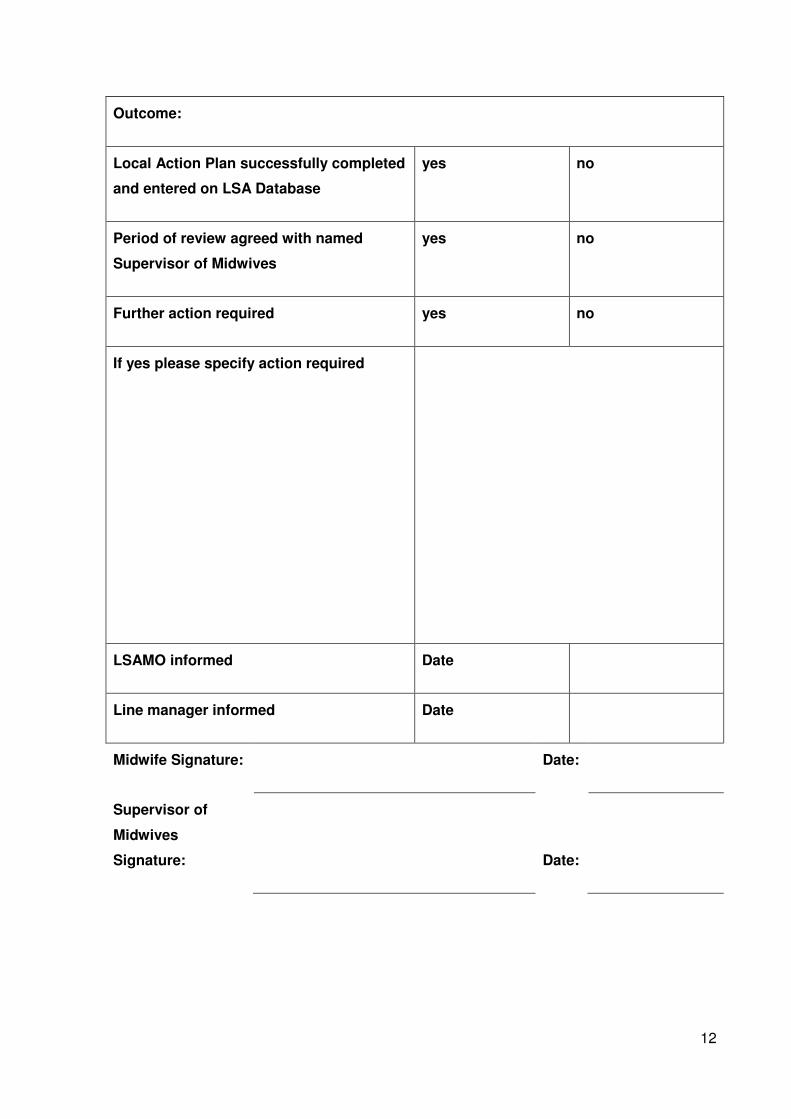
Outcome:
Local Action Plan successfully completed
and entered on LSA Database
yes no
Period of review agreed with named
Supervisor of Midwives
yes no
Further action required yes no
If yes please specify action required
LSAMO informed Date
Line manager informed Date
Midwife Signature: Date:
Supervisor of
Midwives
Signature: Date:

13
Appendix 3: Supervisory review/fact finding event chronology
Trigger:
Woman’s Name:
CHI: LSA: Maternity Unit:
Medical/Social history:
Past obstetric history:
Present pregnancy:
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
Review of antenatal care provided (please keep brief if nil of note – but highlight good practice)
Review of intranatal care provided (please keep brief if nil of note – but highlight good practice)
Review of postnatal care provided (please keep brief if nil of note – but highlight good practice)

14
Recommend Supervisory Investigation: YES NO
Reason/s for decision:
If good practice has been highlighted, please identify/detail the named SoM(s) below and inform her (them) via letter or email
Informed by letter /email Date:
Signature of Reviewing SoM: Date of review:
Copy of review to LSAMO Date:
Entered on LSA Database YES NO

15
Appendix 3a: Example of supervisory review/fact finding event chronology - no concerns- good practice
identified
Trigger: Haemorrhage
Woman’s Name: B Brown
CHI: 0101790101 LSA: A&B Maternity Unit: Local Royal Infirmary
Medical/Social history: Nil of note
Past obstetric history: Green pathway. SVD at term. Nil of note.
Present pregnancy: Green pathway. Nil of note
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
Review of antenatal care provided (please keep brief if nil of note – but highlight good practice)
070501-
241001
Booking at 13 wks
gest to 40 wk ANC
apt.
Routine antenatal green
pathway care
S Smith
G Gold
SWHMR
Pregnancy
Record
Good continuity of care
Appropriate care
High standard of documentation
Review of intranatal care provided (please keep brief if nil of note – but highlight good practice)
271001
0830-1335
Admission in
established labour
Baseline observation
normal. Green pathway
labour care provided.
G Green SWHMR Labour
and Birth Record
Appropriate care planning
Appropriate documentation
271001
1336
SVD Routine care provided.
Active 3rd
stage as
requested.
G Green As above As above
271001
1350
Sudden brisk bleed –
total blood loss
1500mls
IV access sited – FBC,
X Match, Coagulation
screen.
G Green
Dr Gray (Cons)
As above plus
MEWS chart
As above plus
Appropriate escalation
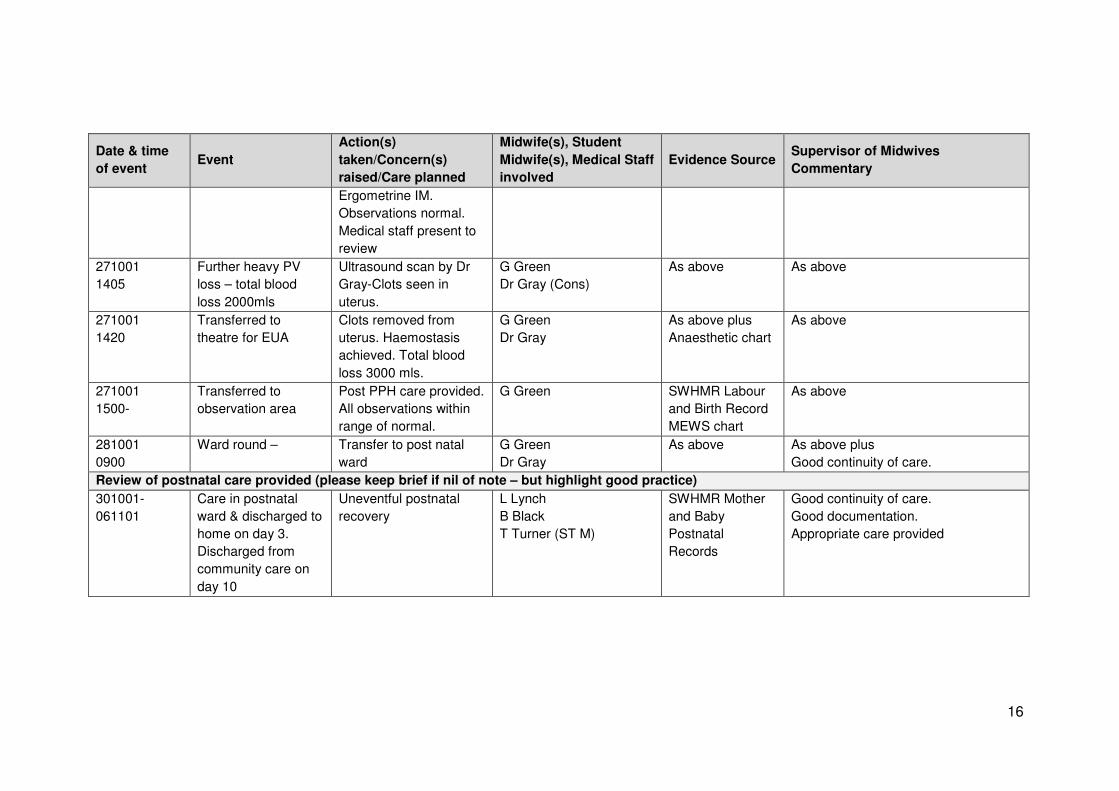
16
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
Ergometrine IM.
Observations normal.
Medical staff present to
review
271001
1405
Further heavy PV
loss – total blood
loss 2000mls
Ultrasound scan by Dr
Gray-Clots seen in
uterus.
G Green
Dr Gray (Cons)
As above As above
271001
1420
Transferred to
theatre for EUA
Clots removed from
uterus. Haemostasis
achieved. Total blood
loss 3000 mls.
G Green
Dr Gray
As above plus
Anaesthetic chart
As above
271001
1500-
Transferred to
observation area
Post PPH care provided.
All observations within
range of normal.
G Green SWHMR Labour
and Birth Record
MEWS chart
As above
281001
0900
Ward round – Transfer to post natal
ward
G Green
Dr Gray
As above As above plus
Good continuity of care.
Review of postnatal care provided (please keep brief if nil of note – but highlight good practice)
301001-
061101
Care in postnatal
ward & discharged to
home on day 3.
Discharged from
community care on
day 10
Uneventful postnatal
recovery
L Lynch
B Black
T Turner (ST M)
SWHMR Mother
and Baby
Postnatal
Records
Good continuity of care.
Good documentation.
Appropriate care provided
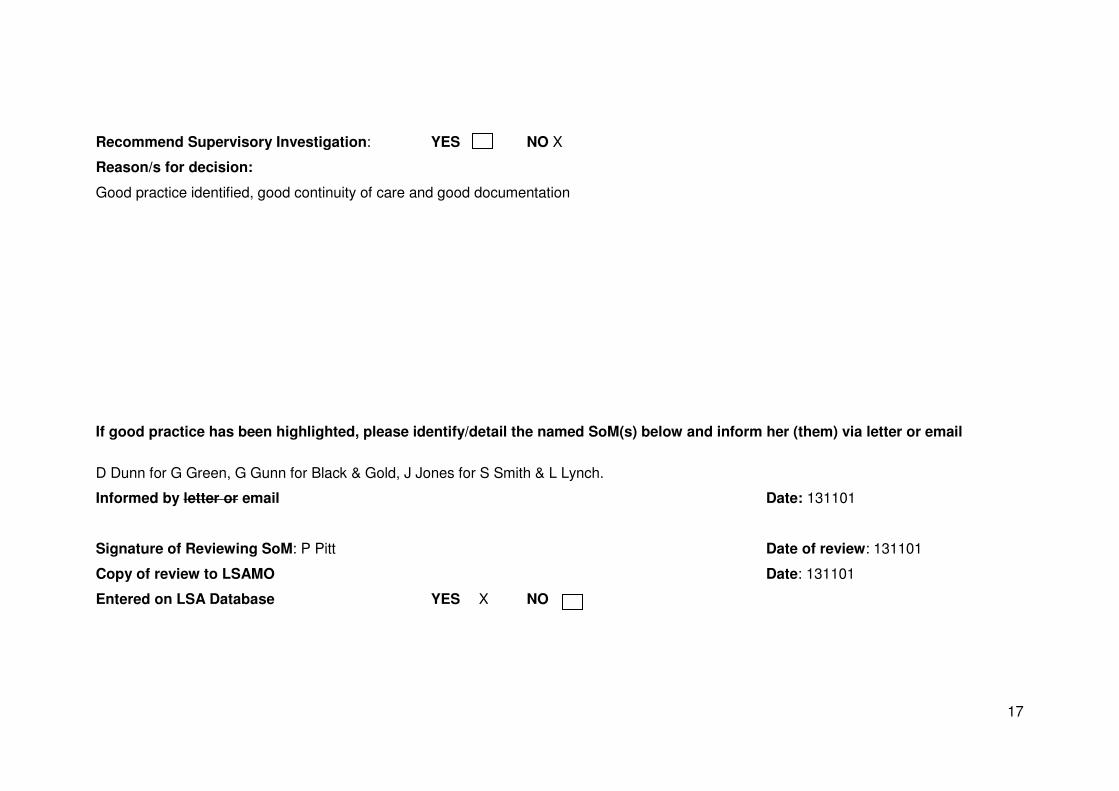
17
Recommend Supervisory Investigation: YES NO X
Reason/s for decision:
Good practice identified, good continuity of care and good documentation
If good practice has been highlighted, please identify/detail the named SoM(s) below and inform her (them) via letter or email
D Dunn for G Green, G Gunn for Black & Gold, J Jones for S Smith & L Lynch.
Informed by letter or email Date: 131101
Signature of Reviewing SoM: P Pitt Date of review: 131101
Copy of review to LSAMO Date: 131101
Entered on LSA Database YES X NO
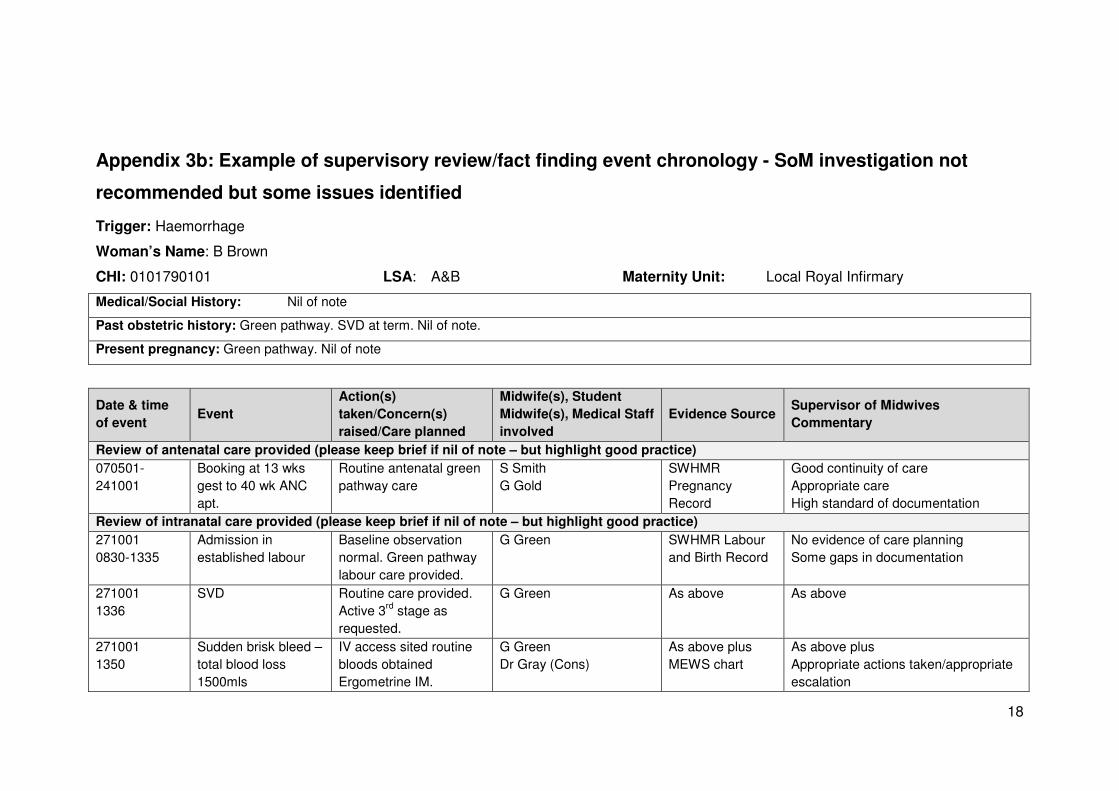
18
Appendix 3b: Example of supervisory review/fact finding event chronology - SoM investigation not
recommended but some issues identified
Trigger: Haemorrhage
Woman’s Name: B Brown
CHI: 0101790101 LSA: A&B Maternity Unit: Local Royal Infirmary
Medical/Social History: Nil of note
Past obstetric history: Green pathway. SVD at term. Nil of note.
Present pregnancy: Green pathway. Nil of note
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
Review of antenatal care provided (please keep brief if nil of note – but highlight good practice)
070501-
241001
Booking at 13 wks
gest to 40 wk ANC
apt.
Routine antenatal green
pathway care
S Smith
G Gold
SWHMR
Pregnancy
Record
Good continuity of care
Appropriate care
High standard of documentation
Review of intranatal care provided (please keep brief if nil of note – but highlight good practice)
271001
0830-1335
Admission in
established labour
Baseline observation
normal. Green pathway
labour care provided.
G Green SWHMR Labour
and Birth Record
No evidence of care planning
Some gaps in documentation
271001
1336
SVD Routine care provided.
Active 3rd
stage as
requested.
G Green As above As above
271001
1350
Sudden brisk bleed –
total blood loss
1500mls
IV access sited routine
bloods obtained
Ergometrine IM.
G Green
Dr Gray (Cons)
As above plus
MEWS chart
As above plus
Appropriate actions taken/appropriate
escalation

19
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
Observations normal.
Medical staff present to
review
271001
1405
Further heavy PV
loss – total blood
loss 2000mls
Ultrasound scan by Dr
Gray-Clots seen in
uterus.
G Green
Dr Gray (Cons)
As above As above
271001
1420
Transferred to
theatre for EUA
Clots removed from
uterus. Haemostasis
achieved. Total blood
loss 3000 mls.
G Green
Dr Gray
As above plus
Anaesthetic chart
As above
271001
1500-
Transferred to
observation area
Post PPH care provided.
All observations within
range of normal.
G Green SWHMR Labour
and Birth Record
MEWS chart
As above
281001
0900
Ward round Transfer to post natal
ward
G Green
Dr Gray
As above As above plus
Good continuity of care.
Review of postnatal care provided (please keep brief if nil of note –but highlight good practice)
301001-
061101
Care in postnatal
ward and discharged
to home on day 3.
Discharged from
community care on
day 10
Uneventful postnatal
recovery
L Lynch
B Black
T Turner (ST M)
SWHMR Mother
and Baby
Postnatal
Records
Good continuity of care.
Good documentation.
Appropriate care provided
20
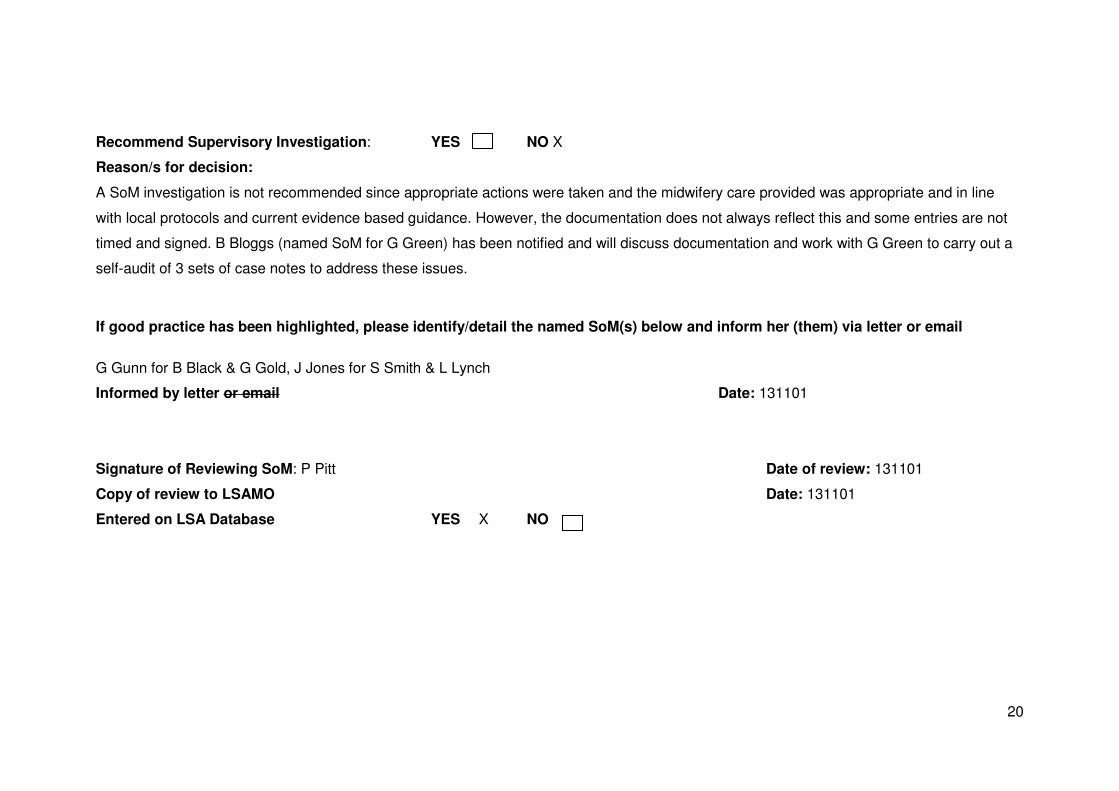
Recommend Supervisory Investigation: YES NO X
Reason/s for decision:
A SoM investigation is not recommended since appropriate actions were taken and the midwifery care provided was appropriate and in line
with local protocols and current evidence based guidance. However, the documentation does not always reflect this and some entries are not
timed and signed. B Bloggs (named SoM for G Green) has been notified and will discuss documentation and work with G Green to carry out a
self-audit of 3 sets of case notes to address these issues.
If good practice has been highlighted, please identify/detail the named SoM(s) below and inform her (them) via letter or email
G Gunn for B Black & G Gold, J Jones for S Smith & L Lynch
Informed by letter or email Date: 131101
Signature of Reviewing SoM: P Pitt Date of review: 131101
Copy of review to LSAMO Date: 131101
Entered on LSA Database YES X NO

21
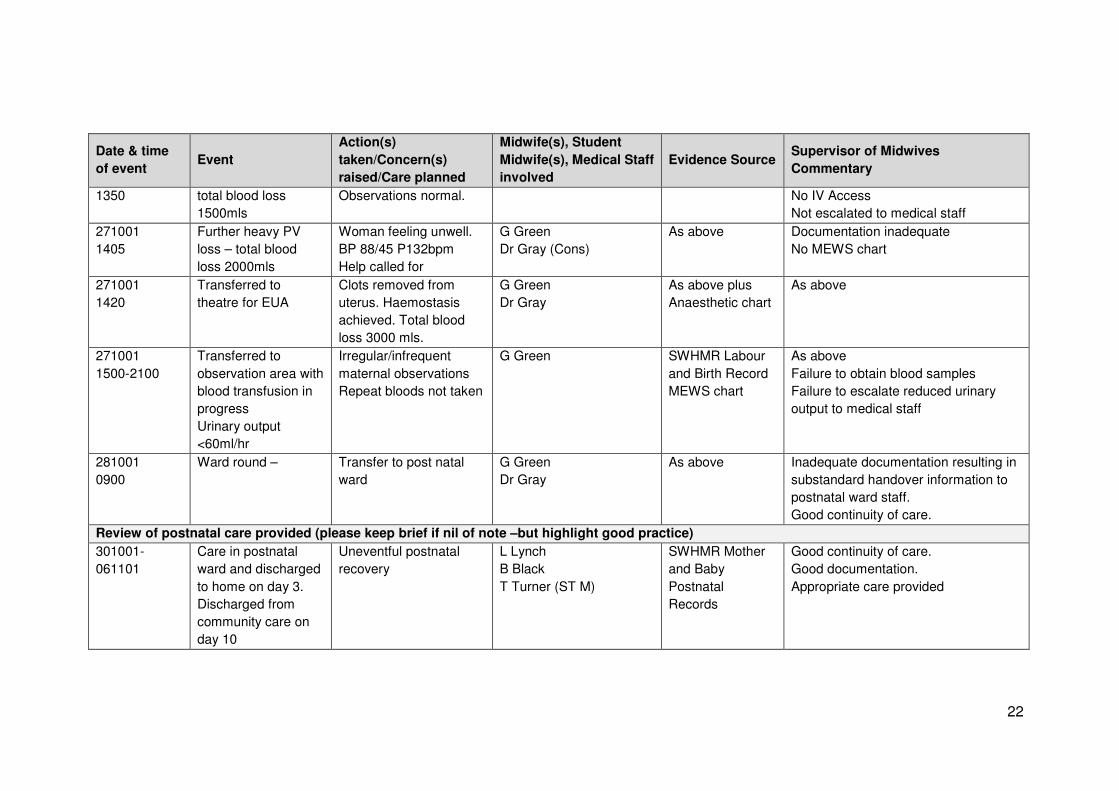
Appendix 3b: Example of supervisory review/fact finding event chronology - SoM investigation
recommended
Trigger: Haemorrhage
Woman’s Name: B Brown
CHI: 0101790101 LSA: A&B Maternity Unit: Local Royal Infirmary
Medical/Social History: Nil of note
Past obstetric history: Green pathway. SVD at term. Nil of note.
Present pregnancy: Green pathway. Nil of note
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
Review of antenatal care provided (please keep brief if nil of note –but highlight good practice)
070501-
241001
Booking at 13 wks
gest to 40 wk ANC
apt.
Routine antenatal green
pathway care
S Smith
G Gold
SWHMR
Pregnancy
Record
Good continuity of care
Appropriate care
High standard of documentation
Review of intranatal care provided (please keep brief if nil of note –but highlight good practice)
271001
0830-1335
Admission in
established labour
Baseline observation
normal. Green pathway
labour care provided.
G Green SWHMR Labour
and Birth Record
No evidence of care planning
Some gaps in documentation
271001
1336
SVD Routine care provided.
Physiological 3rd
stage
despite birth plan
documentation for active
3rd
stage
G Green As above As above
271001 Sudden brisk bleed – Ergometrine IM. G Green As above plus As above plus
22
Date & time
of event Event
Action(s)
taken/Concern(s)
raised/Care planned
Midwife(s), Student
Midwife(s), Medical Staff
involved
Evidence Source Supervisor of Midwives
Commentary
1350 total blood loss
1500mls
Observations normal.
No IV Access
Not escalated to medical staff
271001
1405
Further heavy PV
loss – total blood
loss 2000mls
Woman feeling unwell.
BP 88/45 P132bpm
Help called for
G Green
Dr Gray (Cons)
As above Documentation inadequate
No MEWS chart
271001
1420
Transferred to
theatre for EUA
Clots removed from
uterus. Haemostasis
achieved. Total blood
loss 3000 mls.
G Green
Dr Gray
As above plus
Anaesthetic chart
As above
271001
1500-2100
Transferred to
observation area with
blood transfusion in
progress
Urinary output
<60ml/hr
Irregular/infrequent
maternal observations
Repeat bloods not taken
G Green SWHMR Labour
and Birth Record
MEWS chart
As above
Failure to obtain blood samples
Failure to escalate reduced urinary
output to medical staff
281001
0900
Ward round – Transfer to post natal
ward
G Green
Dr Gray
As above Inadequate documentation resulting in
substandard handover information to
postnatal ward staff.
Good continuity of care.
Review of postnatal care provided (please keep brief if nil of note –but highlight good practice)
301001-
061101
Care in postnatal
ward and discharged
to home on day 3.
Discharged from
community care on
day 10
Uneventful postnatal
recovery
L Lynch
B Black
T Turner (ST M)
SWHMR Mother
and Baby
Postnatal
Records
Good continuity of care.
Good documentation.
Appropriate care provided

23
Recommend Supervisory Investigation: YES X NO
Reason/s for decision:
Inadequate/poor care planning
Inadequate/poor documentation
Failure to communicate/escalate to medical staff
Failure to perform regular maternal observations on high risk woman
Failure to obtain blood results
If good practice has been highlighted, please identify/detail the named SoM(s) below and inform her (them) via letter or email
G Gunn for B Black & G Gold, J Jones for S Smith & L Lynch
Informed by letter or email Date: 131101
Signature of Reviewing SoM: P Pitt Date of review: 131101
Copy of review to LSAMO Date: 131101
Entered on LSA Database YES X NO
24
Appendix 4: Local Action Plan
Midwife’s Name: Supervisor of Midwives:
By the end of this Local Action the
midwife will have:
Action Plan for Learning Resources required Assessment / Evidence
25
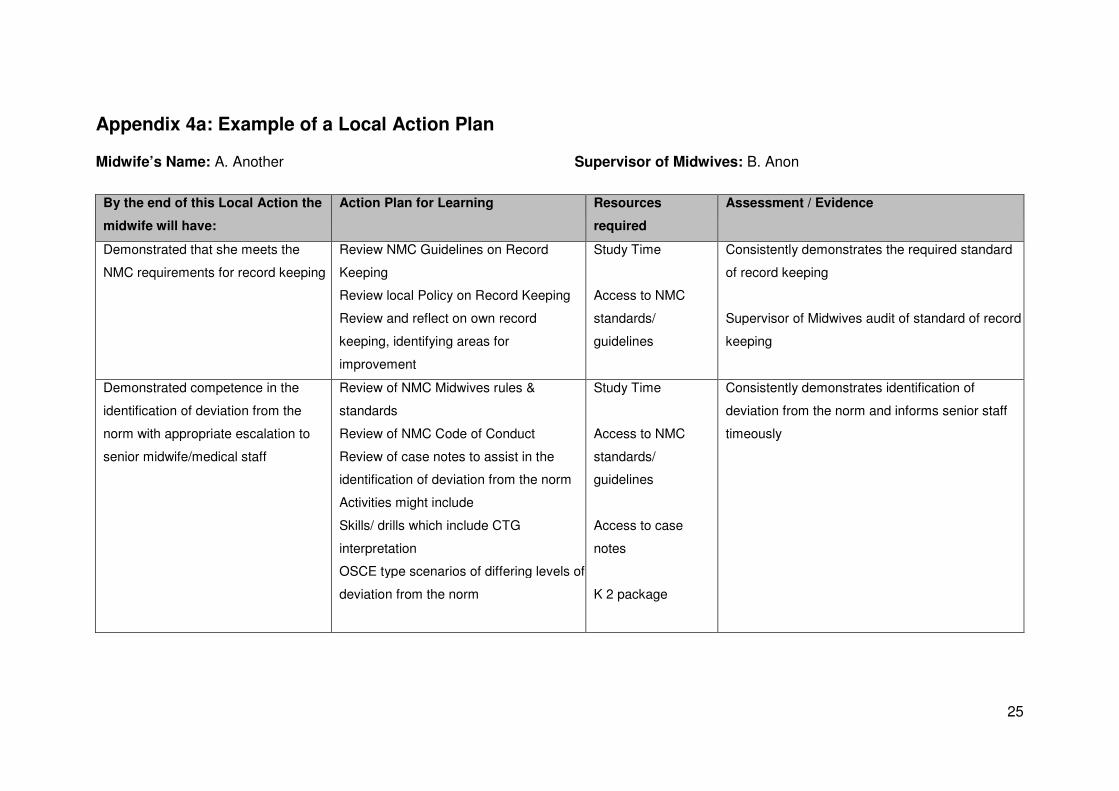
Appendix 4a: Example of a Local Action Plan
Midwife’s Name: A. Another Supervisor of Midwives: B. Anon
By the end of this Local Action the
midwife will have:
Action Plan for Learning Resources
required
Assessment / Evidence
Demonstrated that she meets the
NMC requirements for record keeping
Review NMC Guidelines on Record
Keeping
Review local Policy on Record Keeping
Review and reflect on own record
keeping, identifying areas for
improvement
Study Time
Access to NMC
standards/
guidelines
Consistently demonstrates the required standard
of record keeping
Supervisor of Midwives audit of standard of record
keeping
Demonstrated competence in the
identification of deviation from the
norm with appropriate escalation to
senior midwife/medical staff
Review of NMC Midwives rules &
standards
Review of NMC Code of Conduct
Review of case notes to assist in the
identification of deviation from the norm
Activities might include
Skills/ drills which include CTG
interpretation
OSCE type scenarios of differing levels of
deviation from the norm
Study Time
Access to NMC
standards/
guidelines
Access to case
notes
K 2 package
Consistently demonstrates identification of
deviation from the norm and informs senior staff
timeously

North of Scotland Local Supervising Authority Consortium
Top Related