



Languages
Pages
Legal


National Center for Emerging and Zoonotic Infectious Diseases
Candida auris: is it here to stay?
Shawn R. Lockhart, Ph.D., D(ABMM), F(AAM)Senior Clinical Laboratory Advisor
Senior Advisor for AMRCDC Mycotic Diseases Branch
Association of Public Health LaboratoriesSeptember 18, 2019

CBS News



Objective Points
• Candida auris is here
• Candida auris is deadly
• Candida auris can be slowed

What do we know about Candida?
Candida speciesThey are gut bugs
Mostly antifungal susceptible
Rarely causes outbreaks
Candida aurisIt is a skin bug
Mostly antifungal resistant
Frequently causes outbreaks

C. auris in 2009

C. auris in 2015

C. auris in 2019

CDC issued a clinical alert to healthcare facilities – June 2016

0
5
10
15
20
25
30
35
40
45
50
C. auris clinical cases reported — United States, June 2016
CDC’s clinical alert

0
5
10
15
20
25
30M
ay-1
3
Aug-
13
Nov
-13
Feb-
14
May
-14
Aug-
14
Nov
-14
Feb-
15
May
-15
Aug-
15
Nov
-15
Feb-
16
May
-16
Aug-
16
Nov
-16
Feb-
17
May
-17
Aug-
17
Nov
-17
Feb-
18
May
-18
Aug-
18
Nov
-18
Feb-
19
Num
ber o
f clin
ical
cas
es
New York New Jersey Maryland Illinois
C. auris clinical cases reported by state — United States, 2013–December 2016
CDC issued a clinical alert on C.
auris

05
101520253035404550
New York Illinois New Jersey FloridaMassachusetts California Maryland TexasIndiana Oklahoma Connecticut Virginia
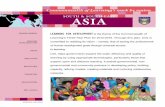
C. auris clinical cases reported by state — United States, 2013–July 2019
~800 clinical cases~2350 clinical + screening cases

Number of C. auris clinical cases
012-1011-5051-100101 or more
Clinical cases of C. auris reported in the United States as of July 31, 2019
~800 cases1550 colonized

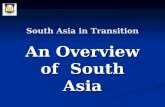
WGS relationships among C. auris isolates
East Asia
Africa
South Asia
South America
B11209 India 2013
SRR1664627 India 2013
B11218 India 2014
B11217 India 2014
B11216 India 2014
B11215 India 2014
B11214 India 2014
B11213 India 2014
B11212 India 2014
B11210 India 2013
B11096 Pakistan 2014
B11101 Pakistan 2014
B11118 Pakistan 2015
B11113 Pakistan 2015
B11114 Pakistan 2015
B11097 Pakistan 2014
B11117 Pakistan 2015
B11104 Pakistan 2015
B11105 Pakistan 2015
B11098 Pakistan 2014
B11116 Pakistan 2015
B11115 Pakistan 2015
B11103 Pakistan 2015
B11099 Pakistan 2014
B11200 India 2012
ERR899743 India
B11205 India 2013
B11201 India 2012
B11207 India 2013
B11208 India 2013
B11206 India 2013
B11112 Pakistan
B8441 Pakistan 2010
B11230 South Africa 2014
B11224 South Africa 2013
B11228 South Africa 2014
B11226 South Africa 2014
B11221 South Africa
B11222 South Africa 2012
B11223 South Africa 2013
B11225 South Africa 2014
B11227 South Africa 2014
B11229 South Africa 2014
B11220 Japan 2009
B11247 Venezuela 2012
B11244 Venezuela 2012
B11245 Venezuela 2012
B11243 Venezuela 2013
B11246 Venezuela 2012
110
19688
250
265
11226
11975
8110
27366
47473
• Very different across regions
• Nearly identical within regions

East Asia
South Asia
Africa
South America
Known introductions in the US

B17654 FL B17054 FL
B17018 FL B17656 FL
B17655 FL B16417 Kenya
B16517 Kenya B16491 Kenya
B17653 FL B17050 FL
Florida isolates
B16482 Kenya B16462 Kenya
B16500 Kenya B16454 Kenya
B16485 Kenya B11227 South Africa
B11229 South Africa B16489 Kenya
B12631 IN001 B11225 South Africa
3001643608 TX002Indiana, Texas isolates
B16515 Kenya B16328 MD
Maryland Isolate
3001643611 CA 3001643609 CA 3001643610 CA 3001643642 CA002 3001641578 CA002 Clinical 3001643643 CA
California isolates
B16425 Kenya B16518 Kenya B16501 Kenya
B16445 Kenya B16457 Kenya
B16410 Kenya B16480 Kenya
B11224 South Africa B11226 South Africa
B16407 Kenya B11223 South Africa B11221 South Africa
B11222 South Africa B16452 Kenya
B11230 South Africa
1
1
0
2
0
7
4
2
1
0
4
4
3
2
8
3
0
17
18
2
38
1
3
1
0
0
0
0
1
0
3
4
1
3
11
6
0
0
13
1
1
0
9
42
4
51
4
2
1
2
6
1
2
32
10
2
21
5
1
2
1
7
14
3
30
10
WGS proof of independent introduction of the same clade across several states

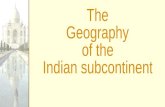
Molecular epidemiology: are there more clades?
>1000 isolates22 countries
Clade I South-East Asia
Clade IIIAfrica
Clade IIEast Asia
Clade IV South America

USPakistanIndiaSouth AfricaSouth KoreaVenezuelaJapanCanadaIsraelColombiaIran
3001716699
B12555
B12531
B12549
B11810 MD001
B13519
B13520
B11861 NY001
B12045 NY001
B11116 Pakistan
B12079
B12089
B12428
B11201 India
B13696 CA001
3001721428 GA
B14068 MD
B11096 Pakistan
B11209 India
B11214 India
B11112 Pakistan
B8441 Pakistan(Reference)
B8441 Pakistan
B12037 Canada
B11230 South Africa
B11221 South Africa
3001644584
3001716286
3001644586
3001644585
3001643608 TX002
B11225 South Africa
B12631 IN001
3001716708
B17654 FL
B17915
B16328 MD
B17834
B17833
3001717113 LongBeach
B17743
B17835
B17741
B17742
B17721 CA002
B17746
B12043 NY003
B11220 Japan
B11808 South Korea
B11809 South Korea
B11245 Venezuela
B11247 Venezuela
B11244 Venezuela
B11894 Israel
B11895 Israel
B11896 Israel
3000912664 Coata Rica
3001716760 CostaRica traveler
B11778 Colombia
B11846 Colombia
B11851 Colombia
B14303 OK002
3001620899
3001721417 IN
B11842 IL002
3001620892
3001620893
3001620900
3015352932
3015352934
B11843 IL001
B12493 MA001
NG-19339 Iran
0
1
2
39
1
0
0
4
11
0
2
0
0
3
0
0
1
1
1
0
0
0
11
2
3
52
3
7
7
0
1
24
142
17
22
0
0
41
6
2
40
3
0
1
2
28
27
4
7
17
0
6
3
23
603
1034
0
1
1
1
1
5
4
6
17
2
0
42
3
77
13
0
106153
35
77307
63
972
39
55
23151
78
35
343
14938
65586
462
15647
11141
40524
38238
20000
WGS results for Indiana, Costa Rica isolates
South America Clade
B11247
B11245
B11244Venezuela
B11895
B11894
B11896Israel
3001716760 CA (Costa Rica traveler)
3000912664 Costa Rica
B11846
B11778
B11851Colombia
B14303 OK002
3001721417 IN
3001620899
B11842 IL002
3001620893
3001620892
3001620900
3015352932
3015352934
B12493 MA001
B11843 IL001
US
0
1
3
6
3
23
39
52
2
7
17
77
4
7
1
0
0
11
0
1
2
1
263
255
15
1439
2
61
1
78
13
9
3
20

South Africa 14% of candidemia in surveillance in South Africa was due to C. auris
Van Schalkwyk (2019) EID 25:1698

C. auris can overwhelm a healthcare system
• C. auris cases are additive, increasing overall candidemia rate• Published crude mortality ranges from 25% to >60%
https://www.eccmidlive.org/#resources/how-should-we-manage-the-c-auris-outbreak

Targets the most vulnerable
Multiple healthcare stays (acute and long term)
Multiple underlying conditions, indwelling devices– Tracheostomy– Ventilator – Peg tube– Central lines– On antibiotics and antifungals

C. auris persists in the healthcare environment

Mobile equipment has been heavily implicated in transmission


Hotbed of C. auris activity
• LTACH• Long-term Acute Care Hospital
• vSNF• Ventilator Skilled Nursing Facility

Stays in certain types of post-acute care facilities is a major risk factor: vSNFs and LTACHs
0.7%
C. auris prevalence in regular nursing homes
C. auris prevalence in nursing home units with ventilator beds
7.7% Adams EH, Quinn M, Ostrowsky B, et al. The Value Added from Candida auris Point Prevalence and Environmental Studies in New York State. 2018. Available at: https://idsa.confex.com/idsa/2018/webprogram/Paper72423.html.

• Colonization means patients are:• at risk for developing invasive
infection • A source of transmission to
others• Almost 100 cases of BSI in colonized
patients who were being followed 2016-2018
C. auris colonization can precede infection

Slide courtesy of Chicago Department of Public Health.
vSNF colonization March 2017

Slide courtesy of Chicago Department of Public Health.
vSNF colonization January 2018

Slide courtesy of Chicago Department of Public Health.
vSNF colonization January 2018
C. auris colonization often associated with CRE carriage

Proactive Public Health responseCalifornia• Performing proactive urine culture identification• Discovered a case in an LTACH, performed
extensive point prevalence surveys of LTACHS and vSNFs
• Identified >100 colonized patients
• Implemented extensive infection control
• Has kept case count below 5

?What don’t we know?

Laboratory updates

Laboratory Safety• Lab coat and gloves, and eye protection if spatter or splash may occur
• Use a biological safety cabinet (BSL2) or glove box when manipulating known or suspected C. auris isolates.
• To disinfect surfaces contaminated with C. auris, use 10% bleach (made fresh daily) or other bleach-based products. Alternatively, disinfectants on the USA Environmental Protection Agency List K
• After work with C. auris is complete, decontaminate the biological safety cabinet with 10% bleach
https://www.cdc.gov/fungal/candida-auris/c-auris-lab-safety.html

Update on lab methods for detecting C. auris• FDA approvals
• VITEK MS MALDI-TOF• Bruker Biotyper MALDI-TOF• GenMark ePlex BCID-FP panel blood culture test
• Other available tests• VITEK 2 8.01 update• PCR• Bruker FungiPlex
https://www.cdc.gov/fungal/candida -auris/recommendations.html

VITEK 2 update 8.01J Clin Microbiol. 2019 Aug 14. pii: JCM.00884-19. doi: 10.1128/JCM.00884-19. [Epub ahead of print]Identification of Candida auris using the updated 8.01 VITEK®2 yeast identification system: a multi-laboratory evaluation study.Ambaraghassi G1,2, Dufresne PJ3, Dufresne SF1,2,4, Vallières É2,5,6, Muñoz JF7, Cuomo CA7, Berkow EL8, Lockhart SR8, Luong ML9,2.
• Still difficulties distinguishing between C. auris and C. duobushaemuloniiespecially for isolates from East Asia and Africa• South Asia – 74%• East Asia – 0%• Africa – 7%• South America – 100%

Resistance: C. glabrata
7/1700 resistant to fluconazole and micafungin
8%Azoles
3%Micafungin

Global C. auris antifungal resistance
0 10 20 30 40 50 60 70 80
Fluconazole
Amphotericin B
Echinocandins
% ResistanceN=912

US Resistance: C. auris
33% multidrug-resistant
1 2 3
88% 34% 3%Azoles EchinocandinsPolyenes

Pan-resistance
First 2 confirmed pan-resistant C. auris cases found in NY Identified by ARLN NE regional lab (Wadsworth/NY) Cases were unrelated Acquired resistance on treatment No transmission of resistance seen Pan-resistance has also been reported from a few other
countries

Nationally notifiable
• C. auris nationally notifiable as of 2019• In pilot testing phase for message mapping guide• Contact your local or state PHL for information on
reporting

Surveillance possibilities

Colonization screening Current recommendations are for a single swab of axilla x 2
and groin x 2– Some data that suggests also screening the nares can be
advantageous
Screening can be accomplished through culture of the swab in Sab salt dulcitol broth
PCR
https://www.cdc.gov/fungal/candida -auris/recommendations.html

Screening: Consider screening - Close healthcare contacts of patients with newly identified C. auris
infection or colonization
Patients who have had an overnight stay in a healthcare facility outside the United States in the previous one year, especially if in a country with documented C. auris cases.– Strongly consider screening patients colonized with carbapenemase-
producing Gram-negative bacteria. C. auris co-colonization with these organisms has been observed regularly.
https://www.cdc.gov/fungal/candida -auris/c-auris-screening.html

Identifying the species of Candida from urine and other non-sterile body sites Yeast from urine usually tossed out because not
considered an infection
~50%
Only about 50% of clinical C. auriscases are from blood

Periodic point prevalence surveys in LTACHs and vSNFs One state is conducting periodic PPS at LTACHs bordering a
high prevalence state Detected 4 cases of C. auris colonization within first few
rounds of screening

If you identify a C. auris, please notify your PHL and/or regional ARLN lab

More information can be found:
https://www.cdc.gov/fungal/candida-auris/
https://www.cdc.gov/drugresistance/solutions-initiative/ar-lab-network.html

For more information, contact CDC1-800-CDC-INFO (232-4636)TTY: 1-888-232-6348 www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Contact us at: [email protected]
Thank you! Questions?
Top Related