





Languages
Pages
Legal


Burst Abdomen
By Dr.Suhaib

Introduction
• Disruption of an abdominal wound.• it may be limited to the deep fascia with the skin
remaining intact.• When it is complete, all the layers of the abdominal
wall have burst apart with or without associated protrusion of a viscus (evisceration).
• The mean time to wound dehiscence is 8–10 postoperative days

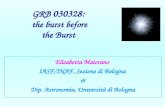
Anatomy
• Abdominal wall – Skin– Subcutaneous layers– Ext oblique with
aponeurosis.– Internal oblique forming
rectus sheath– Transverse abdominis– Transversalis fascia– Extraperitoneal fat– Peritoneum


Factors relating to the incidence of burst abdomen and
incisional hernia

Technique of wound closure
• Choice of suture material• Catgut leads to high incidence then non absorbable
sutures
• Method of closure• Interrupted sutures have low incidence• High incidence in single layer closure then two layer
closure.• Using short material and keeping the wound taut.
• Drainage • Drainage through the same wound increases the
incidence

Factors relating to incision
• Midline and vertical incisions have higher incidence.

Reasons for initial operation
• Deep wound infection is notorious for causing burst abdomen or late incisional hernia.
• Wounds –peritonitis, acute abdomen, pancreatic, hepatic ,gastric surgeries for malignancy have high incidence of disruption.

Coughing,vomiting and distension
• Any violent coughing set off by the removal of an endotracheal tube and suction of the laryngopharynx strains the sutures; likewise cough, vomiting and distension.
• Overvigorous postoperative ventilation in sedated patients can lead to wound disruption.

Poor condition of the patient
• Factors conducive to disruption of a laparotomy wound– Obesity– Diabetes mellitus– Immunosuppresion.– Uraemia – Jaundice– Malignant disease– Hypoproteinaemia and– Anaemia

Clinical features
• Sudden feeling of giving away.• Pinkish serosanguinous discharge from
wound.• Open wound with bowel contents.

Management
• Reassure the patient• Cover the contents with sterile towel• Nasogastric tube.• Intavenous fluids.• Antibiotics • Tension suturing.

Operation
• Each coil of intestine is cleaned with saline and kept back in abdominal cavity
• Fascia is strong and intact, primary closure is warranted. • If the fascia is infected or necrotic, débridement is performed. • If after débridement the edges of the fascia cannot be
approximated without undue tension, consideration needs to be given to closing the wound with absorbable mesh or the recently developed biologic prostheses
• All layers approximated by through and through sutures using nylon and applying plastic or rubber tubings to prevent cutting through.

• The abdominal wall may be supported by strips of adhesive plaster encircling the anterior two-thirds of the circumference of the trunk.
• If a partial disruption (ie, the skin is intact) is stable and the patient is a poor operative risk, treatment may be delayed and the resulting incisional hernia accepted

THANK YOU
Top Related