






Languages
Pages
Legal

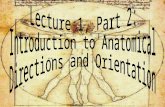
Brain Stem Anterior View Posterior View 3 4 9,10,11 5
Adducent
Facial colliculus 7 & 8th 12 Striae Medullare Case.1 A 55 year
old overweight man was brought to the emergency roomunconscious
after he had collapsed while loading a truck.After heregained
consciousness, an exam revealed a paresis of both right limbswith a
Babinski sign on the right. The patient's tongue deviated to
theleft upon protrusion, and he had no vibratory sense on the right
side ofthe body. These findings suggest. A lesion in the medial
medulla A lesion in the medial pons An infract PICA A lesion in the
lateral medulla Case cont2 A 35-year-old visits hospital because of
severe headache. The patient says that theheadache, which seems to
be localized area behind his ears, it has beenintermittent but
persistent since he was involved in the baseball game while on
hisvacation. Shortly after he returned from his vacation, he made
an appointmentwith his family physician because he was worried
about the headache and the factthat he had developed noticeable
clumsiness. When physician questioned, hementioned unusual frequent
bouts of nausea and vertigo. Physical examinationreveals mild
hoarseness of voice and some difficulty swallowing oral
secretions.The left side of his face is affected by Horners
syndrome, He has decreasedsensitivity to light touch on the left
side of his face, flattening of the left nasolabialfold, and
paresis of the left soft palate. Finger to nose testing shows left
sidedDysmetria. When asked to walk across the examining room, his
gait is ataxic andhe deviates to the left. There is diminished pain
and thermal sensation on the rightside. Reflexes are symmetric.
There is no Babinski reflex, and the remainder of themotor and
sensory examination is normal. Case Cont.3 Which one of the
following vessels should be the primary suspect? Middle cerebral
artery Internal carotid artery at the cavernous sinus Superior
cerebellar artery Posterior inferior cerebellar artery Anterior
communicating artery Case cont4 45 year-old women with a history of
high blood pressure experienced a sudden onset of Dizziness,
nausea, and vomiting. She was brought to the emergency room where a
neurological Exam revealed horizontal nystagmus, Dysphagia and
hoarseness. Absent of gag reflex on the left. Alteration of taste
sensations from the tongue. Analgesia and thermal anesthesia on the
left side of the face . Analgesia and thermal anesthesia on the
right side of the body. Homers syndrome and significant hearing
loss on the left as compared to the right Case cont5 The dysphagia
and hoarseness in this case are to due to lesion ofwhich structure?
Dorsal motor nucleus of vagus Nucleus solitarius Nucleus ambigus
Inferior salivatory nucleus Superior salivatory nucleus Case cont
6. The analgesia and thermal anesthesia on the left side of the
face inthis case most likely Resulted from a lesion of which
structure? The trigeminal nerve The Mesencephalic nucleus of
trigeminal The principal (chief) nucleus of The spinal tract of
trigeminal The trigeminal ganglia Level Nuclei Midbrain III, IV,
mesencephalic V Pons V (main nucleus) Caudal pons VI, VII
Ponto-medullary junction VIII Medulla N. of the descending tract of
V. N. ambiguus N. tractus solitarius Motor X XII Cervical cord XI
Medial Medullary Syndrome
Medial Medullary Syndrome/ InferiorAlternating Hemiplegia (branches
of anterior spinal artery occlusion) contralateral hemiplegia of
arm & leg (pyramidcorticospinal fibers) contralateral loss
position sense, vibration,discriminatory touch (medial lemniscus)
deviation of tongue to ipsilateral side whenprotruded; muscle
atrophy (CN XII hypoglossal nerve in medulla orCN XII nucleus)
Lateral medullary Syndrome (Wallenberg's)
contralateral body pain & temp loss (anterolateral
system/spinothalamic tract) ipsilateral face pain & temp loss
(spinal trigeminal tract & nucleus) dysphagia, soft palate
paralysis, hoarseness,diminished gag reflex (nucleus ambiguus,
roots of 9th and 10thnerves) ipsilateral Horners Syndrome (myosis,
ptosis,anhydrosis) (descending hypothalamospinal fibers) nausea,
diplopia, vertigo, nystagmus (vestibular nucleiCN 8) ataxia to the
ipsilateral side (restiform body & spinocerebellar fibers) Case
7.. A 46-year-old woman presents to her physician with "double
vision" and is unable to adduct her right eye on attempted left
lateral gaze. Convergence is intact. Both direct and consensual
light reflexes are normal. Which of the following structures is
most likely to be affected? Left oculomotor nerve Medial
longitudinal fasciculus Right abducent nerve Right oculomotor nerve
Right trochlear nerve Case 8.. A patient with a bullet wound to the
head is referred to you for neurological examination.Upon entering
the hospital room you find the patient on a respiratory and cardiac
monitor.You have difficulty arousing the patient and once awake you
note the following: Rightpupil is constricted; there is medial
strabismus of the right eye and upon attempted rightlateral gaze
the left eye fails to adduct; loss of pain and temperature
sensitivity on the rightside of the face and left side of the body;
deafness of the right ear; a pronounced intentiontremor in the
right arm and leg. The deep tendon reflexes on the right side are
not as briskas those on the left and there appears to be a complete
facial paralysis on the right side. The likely site for this lesion
is: The left internal capsule The right caudal pons The left
cerebellar hemisphere The left side of the midbrain at the level of
the superior colliculus The right side of the medulla at the level
of the dorsal column nuclei Pontine Syndromes (paramedian branches
of basilar artery occlusion)
Medial Pontine Syndrome/ Middle Alternating Hemiplegia (paramedian
branches of basilar artery occlusion) contralateral hemiplegia of
arm & leg (corticospinal fibers in basilar pons) contralateral
loss/decrease of proprioception, vibration, discriminative touch
(medial lemniscus) ipsilateral lateral rectus muscle paralysis
(abducens nerve fibers or nucleusCN 6) paralysis of conjugate gaze
toward side of lesion Medial Strabismus (paramedian pontine
reticular formation/pontine gaze center) Lateral Pontine Syndrome
)
. *note: combination of symptoms varies with caudal to rostral
level oflesion* ataxia, unsteady gait, fall toward side of lesion
(middle & superior cerebellar pedunclescaudal & rostral
pons lesions) vertigo, nausea, nystagmus, deafness, tinnitus,
vomiting (vestibular &cochlear nerves and nucleiCN 8)
ipsilateral paralysis of facial muscles (facial motor nucleusCN
7caudalpons lesions) ipsilateral paralysis of mastication muscles
(trigeminal motor nucleus CN 5midpontine lesions) ipsilateral
Horners Syndrome (descending hypothalamospinal fibers) ipsilateral
face pain & temp loss (spinal trigeminal tract & nucleus)
contralateral body pain & temp loss (anterolateral
system/spinothalamictract) paralysis of conjugate gaze (paramedian
pontine reticular formationmid to caudal pons lesions) (Long
circumferential branches of basilar artery occlusion) Case 9 Jones
likes to play golf.Usually he is a very competitive member of
theteam UK , but his game has been off lately.He has been unable to
maintainhis well-practiced grip on his favorite clubs (particularly
with his right hand),causing the club to slip out of alignment as
he begins his swing. Additionally, as all great golfers know,
maintaining visual contact with theball is critical to accurate
placement of the ball on the green.Peter hasbegun to complain that
he sometimes sees two balls (double vision), and thatoccasionally
he swings at the wrong one.He has been unable to keep hiseyes on
the ball as he swings and he has not been able to watch it as it
sailsto its destination.Today has been particularly hot, and the
entire teambecoming fatigued as they near the final hole.Its at
this point that one ofthe partners who is a neurologist notices
that June's left eye is crossed. On further
examinationNeurologistnoticed fallowing Case 9 Left eye is crossed
(diplopia); an inability to move the Left to the left. He has
Spastic paralysis of the rightupper and right lower limb muscles.
His left side of the body seems to be functioning normal. Case 10
60 year old woman suddenly remarked that she was seeing double and
felt a weakness in herleft arm and leg. Her husband noticed that
her right eyelid was drooping. At the hospital,she was awake,
oriented, and articulate. Her visual fields were normal but here
right eyedeviated to the right. On attempted lateral gaze to the
left only the left eye responded; onlythe left eye constructed in
response to light. Upon smiling, there was a minor weakness onthe
left. The gag, corneal, and jaw jerk reflexes were normal as were
the sensoryexaminations of the face and body. Motor strength was
normal in the extremities on theright but reduced on the left
especially in the arm where there was a heightened biceps reflexand
resistance to passive stretch. Where is the site of lesion?
a)Cerebellum b)Substantia nigra c)Mid brain d)None of above.
Mid-Brian @ Superior colliculus Mid-Brian @ Superior colliculus
Medial Midbrain (Weber) Syndrome/ Superior Alternating
Hemiplegia
(paramedian branches of P1 segment of PCA occlusion)
1.contralateral hemiplegia of arm & leg corticospinal fibers in
crus cerebri) ipsilateral paralysis of eye movement, oriented down
& out, pupil dilated & fixed (oculomotor nerveCN 3) 2.
Central Midbrain Lesion (Claude Syndrome) contralateral ataxia and
tremor of cerebellar origin (red nucleus & cerebellothalamic
fibers) 3. Benedikt Syndrome: includes both regions, both sets of
symptoms from above
Top Related