






Languages
Pages
Legal


24 hr BP control
Renal aspects

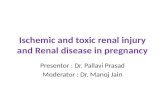
Hypertension and Chronic Renal Disease: Hemodynamic Abnormalities
Mean BPTotal Systemic
Vascular Resistance= X
Increased Cardiac Output Intravascular Volume Glomerular filtration Sodium excretion Extracellular Fluid Renal Nerve Activity Myocardial Performance Adrenergic Activity
Increased Cardiac Output Intravascular Volume Glomerular filtration Sodium excretion Extracellular Fluid Renal Nerve Activity Myocardial Performance Adrenergic Activity
IncreasedVasoconstriction Adrenergic Stimuli Angiotensin II Endothelin Endothelium-derived Contracting Factors Thromboxane
IncreasedVasoconstriction Adrenergic Stimuli Angiotensin II Endothelin Endothelium-derived Contracting Factors Thromboxane
CardiacOutput
DecreasedVasodilation Prostacyclin Nitric oxide EDHF*
DecreasedVasodilation Prostacyclin Nitric oxide EDHF*
Textor SC. Atlas of Diseases of the Kidney, 2001.
*Endothelium-derived Hyperpolarizing Factors
www.hypertensiononline.org

“ The inherent variability of the blood pressure has ledto problems in the diagnosis, treatment, and prognosis
of hypertension. Knowing how the blood pressurefluctuates with the stresses and strains of everyday lifeshould help in assessing the severity of hypertension,
the response to treatment, and the prognosis in individualcases”
Hinman et al; 1962
DIURNAL BLOOD PRESSURE VARIATION IS LONG RECOGNISED !

Diurnal blood pressure variation
Am J Hypertens 2005; 18: 149-151.

Altered Circadian rhythm in CKD
Nephrol Dial Transplant (1997) 12: 2301–2307

Consecutive patients referred for ambulatory blood pressure monitoring, Followed over 1 year
322 patients included:– 137 dippers, 185 non dippers
Mean baseline GFRs– Dippers: 80.5 mL/min per 1.73 m2 – Non dippers: 76.4 mL/min per 1.73 m2
Arch Intern Med. 2006;166:846-852

Dippers vs Non dippers - only significantly different parameters shown
- values in brackets are percentage of total
Arch Intern Med. 2006;166:846-852
Variable Dippers
(n = 137)
Non dippers
(n = 185)
Age, y 61.3 ± 12.6 65.7 ± 12.2
Diabetes mellitus 9 (6.6) 32 (17.3)
Hypertension 92 (67.2) 162 (87.6)
Coronary artery disease 17 (12.4) 47 (25.4)
Antihypertensive drugs ACEI, BB

Dippers vs Non dippers - only significantly different parameters shown
- values in brackets are percentage of total
Arch Intern Med. 2006;166:846-852
Variable Dippers
(n = 137)
Non dippers
(n = 185)
FBG, mg/dL 95.7 ± 19.2 102.4 ± 28.5
GFR at Follow-up 81.0 ± 20.7 64.7 ± 26.6
Triglyceride level, mg/dL 129.4 ± 68.9 163.8 ± 93.7
High-density lipoprotein 55.8 ± 17.3 49.5 ± 15.2

Dippers vs Non dippers
Arch Intern Med. 2006;166:846-852


Non Dipping pattern – Cause or effect ? Fifteen healthy subjects (4 men, 11 women; aged 33 to 65
years;mean age 55±2 years) who underwent unilateral nephrectomy for kidney donation were studied
Hypertens Res 2005; 28: 301–306
Results suggest that unilateral nephrectomy disturbs the circadian rhythm of BP as a function of renal dysfunction without affecting absolute levels of BP
Non dipping of BP seems to be the consequence of the loss of renal function, rather than the cause

Am J Physiol Renal Physiol 2007 293:655-659

ABPM findings in a community
The Spanish Society of Hypertension - 20000 patients - 17 219 analyzed
Remarkable discrepancy between office and ambulatory BP in high-risk hypertensive patients
The prevalence of a non-dipper BP pattern was almost 60%
Journal of Hypertension 2007, 25:977–984

ABPM findings in a community
Journal of Hypertension 2007, 25:977–984

Nocturnal BP Changes and CV Mortality: Ohasama study
0.96 1
2.56
3.69
0
0.5
1
1.5
2
2.5
3
3.5
4
Extreme dippers
Dippers Non-dippers
Risers
Risk of CV Mortality
Ohkubo et al; AJH 1997; 10: 1201

Analysis of The Influence of the Morning Surge of BP on Stroke
Incidence Cox regression analysis for clinical stroke eventsCovariates RR P value
Age (10 yrs) 1.80 (1.21-2.69) 0.004
Male gender 1.42 (0.76-2.67) 0.266
BMI 0.98 (0.90-1.07) 0.663
24 hr SBP 1.37 (1.16-1.63) 0.003
Morning BP surge* 1.29 (1.10-1.51) 0.001
Nocturnal BP fall* 0.88 (0.73-1.06) 0.167
Lowest sleep BP 1.05 (0.65-1.71) 0.837* per 10 mmHg
Kario, Pickering et al, Circ 2003; 107:1401


Cause of Circadian Rhythms - Role of the Autonomic system
212 patients with progressive autonomic failure due to familial amyloid polyneuropathy
Group I – No evidence yet of impairment of their ANS– Circadian BP and HR variations indistinguishable from controls
Group II – Variable parasympathetic, intact sympathetic – 24 hour HR was higher vs Controls but maintained– Circadian BP variation diminished - attenuation of the nocturnal BP
decline
Hypertension 2000;35;892-897

Role of the Autonomic system
Group III – parasympathetic failure and intermediate sympathetic
dysfunction– Blunted diurnal BP variation
Group IV – parasympathetic failure and severe sympathetic
dysfunction– Absent diurnal BP variation
Hypertension 2000;35;892-897

How to tackle the variations
Pharmacodynamic Pharmacokinetic
maintain blood concentration of a drug for longer periods
longer acting drugs
• Sympatholytic drugs
• RAAS system

Diuretics Convert Non-Dippers to Dippers
100
110
120
130
140
150
Systolic pressure mmHg
Day
Night
No Rx HCTZ No Rx HCTZ
Dippers Non-DippersUzu & Kimura Circ 1999; 100:1635

Diuretics Convert Non-Dippers to Dippers
100
110
120
130
140
150
Systolic pressure mmHg
Day
Night
No Rx HCTZ No Rx HCTZ
Dippers Non-DippersUzu & Kimura Circ 1999; 100:1635

Effects of Alpha-Blockade on the Morning Surge of Blood Pressure
Kario, Pickering, et al Am J Hypertens 2004;17; 668
Doxazosin
No Rx

Role of alpha blockers Type 2 DM with hypertension and nephropathy
Effects of antihypertensive therapy of combinations of angiotensin converting enzyme (ACE) inhibitor, calcium antagonists (CCB), diuretics (DU), and α blocker (AB)
At the end of the studySignificant associations among – decline of 24-hr creatinine clearance and the levels of systolic
blood pressure
– levels of systolic blood pressure and the urine excretion of protein-creatinine ratio in the morning
– Analysis of patients who had systolic blood pressure in the morning less than 140 mmHg revealed that 65% of these patients received doxazosin-averaged doses of 4.8 ± 1.5 mg daily
Clinical and Experimental Hypertension, 2005; 27:129 - 138

Pre Tx(n = 30) – CCB/DU + ARB
Tx (n = 27) – Pre Tx + AB at bedtime

Changing the timing of dosing helps Setting & Participants
– 32 CKD patients with CKD , eGFR > 90 mL/min/1.73 m2 and ABP night-day ratio greater than 0.9
– normal daytime ABP (<135/85 mm Hg)
Intervention – Shifting 1 antihypertensive drug from morning to evening
Outcomes – Percentage of patients changing the night-day ratio of mean
ABP from greater than 0.9 to 0.9 or less 8 weeks after the shift
Measurements– Office blood pressure/ABP and proteinuria at baseline and after
the shift
AJKD, 2007;50(6):908-17

Changing the timing of dosing helps
Results After shift:
– ABP N/D ratio decreased in 93.7% of patients, with normal circadian rhythm restored in 87.5%
– Was not associated with an increase in diurnal ABP and was independent from number and class of shifted drug
– Office blood pressure in the morning also decreased (from 136 ± 16/77 ± 10 to 131 ± 13/75 ± 8 mm Hg; P = 0.02)
– Urinary protein excretion decreased from 235 ± 259 to 167 ± 206 mg/dl (P < 0.001)
AJKD, 2007;50(6):908-17

Question: If you were allowed just one reading over 24 hours to predict morbidity,
which would you choose?
Gosse et al, J Hum Hypertens 2001; 15: 413
Awake AwakeSleep
Going to bed Arising
Evening BP
Lowest BP
Preawake BP
Morning BP

Masked hypertension = ↑ risk of ESRD in CKD
White coat hypertension = better outcome
AMBP = Home BP >> Clinic BP
BP obtained in triplicate twice daily for 3 days every 3 months appears appropriate
Alternatively, blood pressure obtained thrice daily for 1 week can be used
Curr Opin Nephrol Hypertens, 2006 15:309–313
Top Related