







Languages
Pages
Legal


Blood TransfusionSafe
Practice
Definition
• Introduction of new matching blood into the bloodstream or/and of any specific blood components.
Blood Components Available at KAUH
• Packed RBC• Platelet• Fresh frozen plasma • Cryoprecipitate
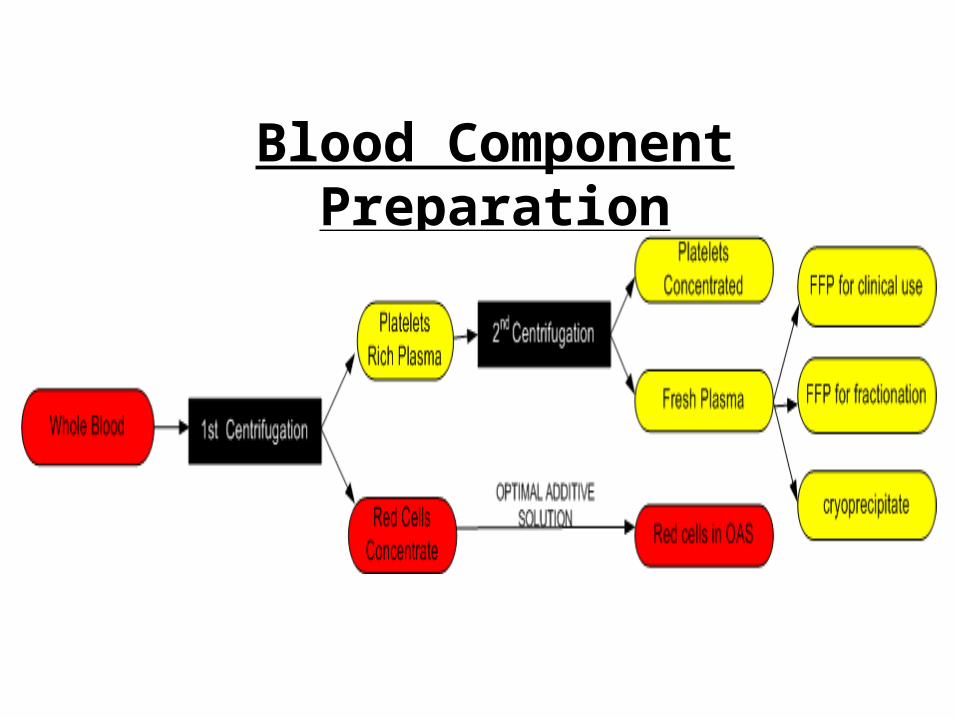
Blood Component Preparation
Red Blood Cells
(Erythrocytes )
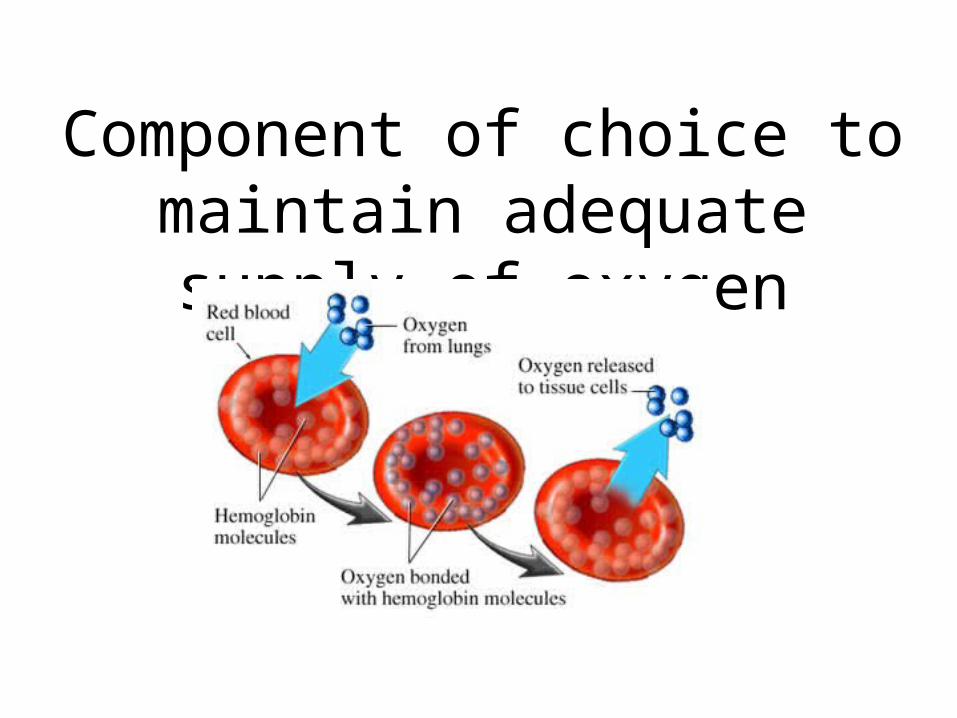
Component of choice to maintain adequate supply
of oxygen
Symptomatic anemia (Hb<8g/dl)
Acute blood loss
Preoperative (Hb<7-8g/dl)
Chronic transfusion patient (Hb<9g/dl)
Indication
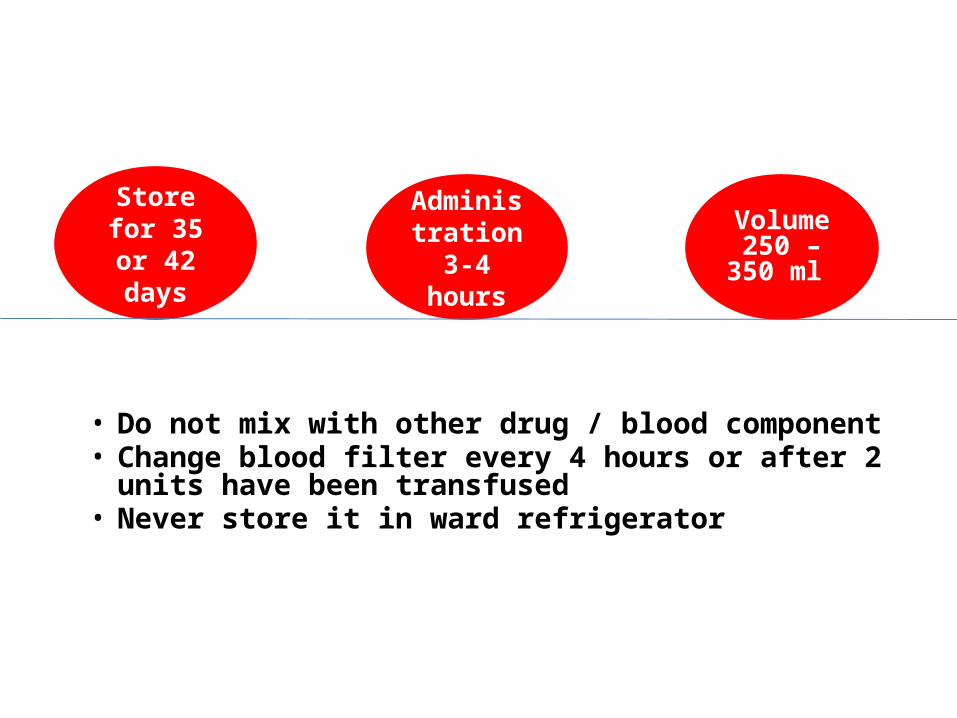
Red Cell Storage & Administration
• Do not mix with other drug / blood component• Change blood filter every 4 hours or after 2 units have
been transfused• Never store it in ward refrigerator
Store for 35 or 42
days
Administration 3-4 hours
Volume 250 – 350
ml

Platelets
Essential for Homeostasis
Prevent or Stop Bleeding
Platelets
•Bone marrow failure•Abnormalities of platelet function •Acute dissemination intravascular coagulopathy –DIC•Massive blood transfusion
Indication

Platelets Storage & Administration
within 15-30
minutesStored for
5 daysYellow in
colourGive
immediately
• Do not store in ward fridge• Do not mix with other drug / blood component• Bacterial contamination greater than with red cells• Volume 45 - 65 ml
Fresh Frozen Plasma (FFP)
FFP
Initial Treatme
nt of Massive Bleeding
Replaces Clotting Factors

Stored for 1 year
Give each unit over
30 minutes
Volume 150 – 250
ml Needs
thawing
Cryoprecipitate
Indication •fibrinogen deficiency •Hemophilia•Von will brands disease (bleeding disorder caused by a deficiency of von Willebrand factor •factor XIII deficiency• Disseminated intravascular coagulation (DIC)
Stored for 1 year
Volume 15 – 25 ml
Needs thawing

Blood Warmers
The routine warming of blood and blood component is
NOT recommended
Keeping the patient warm is probably more important than warming the infusion blood
limited benefit
potentially dangerous
Blood warmer indicated
Exchange transfusion in infant When transfusion patient with clinically significant cold agglutinationAdult receiving blood at rate greater than 50ml/kg/hrChildren receiving blood at rate greater than 15ml/kg/hrMassive transfusion ( 50% or above of body blood volume Trauma situation Cardiopulmonary bypass surgical procedure Blood and blood component should not be warmed using improvisation such as putting the pack into hot water, in microwave
Transfusion Process
1. Prescription of blood component (Doctor’s order)
2. Pre-transfusion sample collection
Prescription of Blood Component
Prescription form Should include:patient name & IDdate and timepatient diagnosisReason of transfusionnumber of unit to be administeredrate of infusionspecial procedure
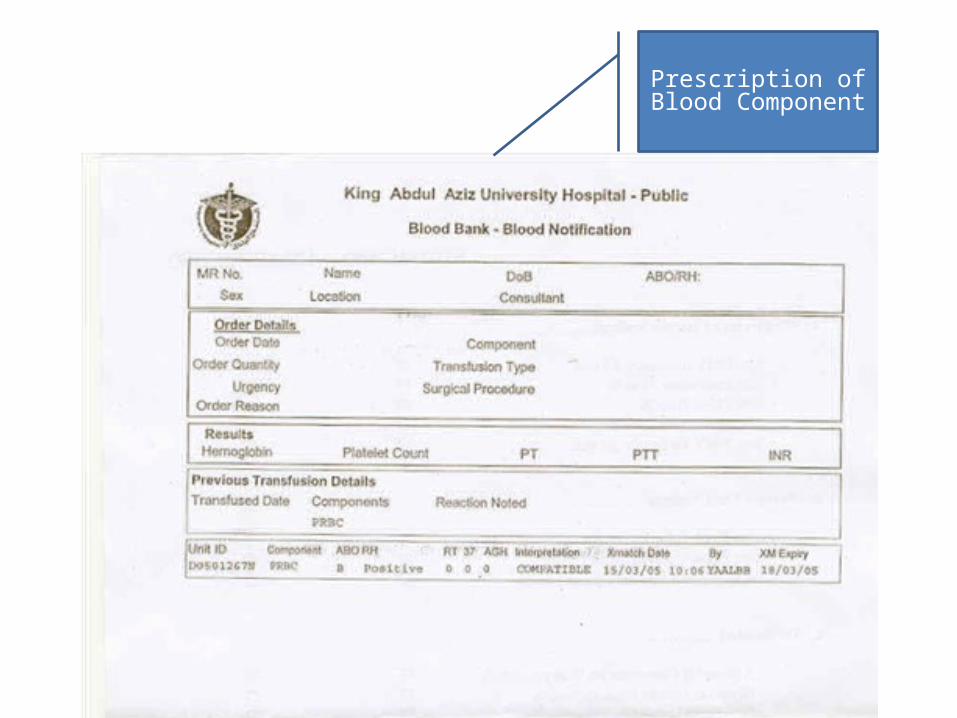
Prescription of Blood Component

Informed Consent
Signed
• Prior Transfusion• 15 to 20 Minutes After Starting• Post Transfusion.
vital signs monitoring
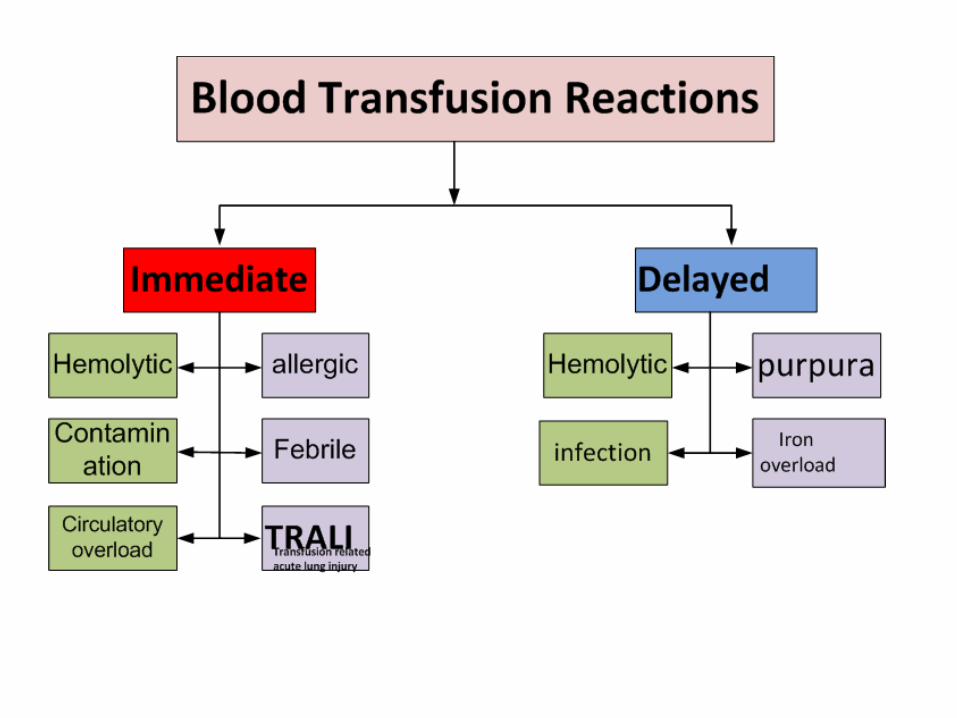
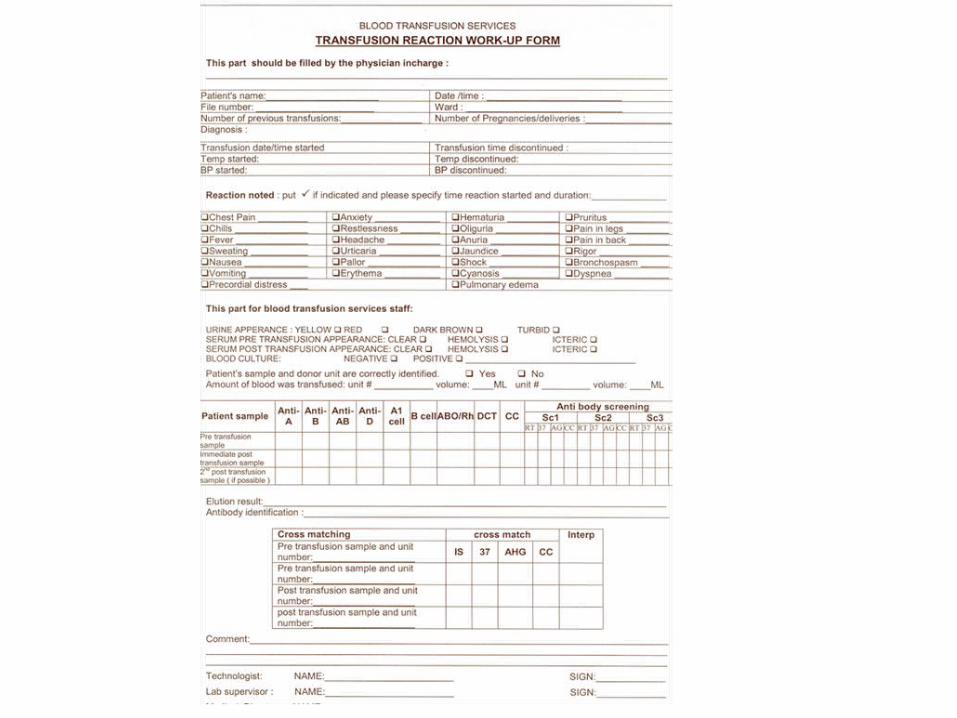
Blood Transfusi
on Reaction
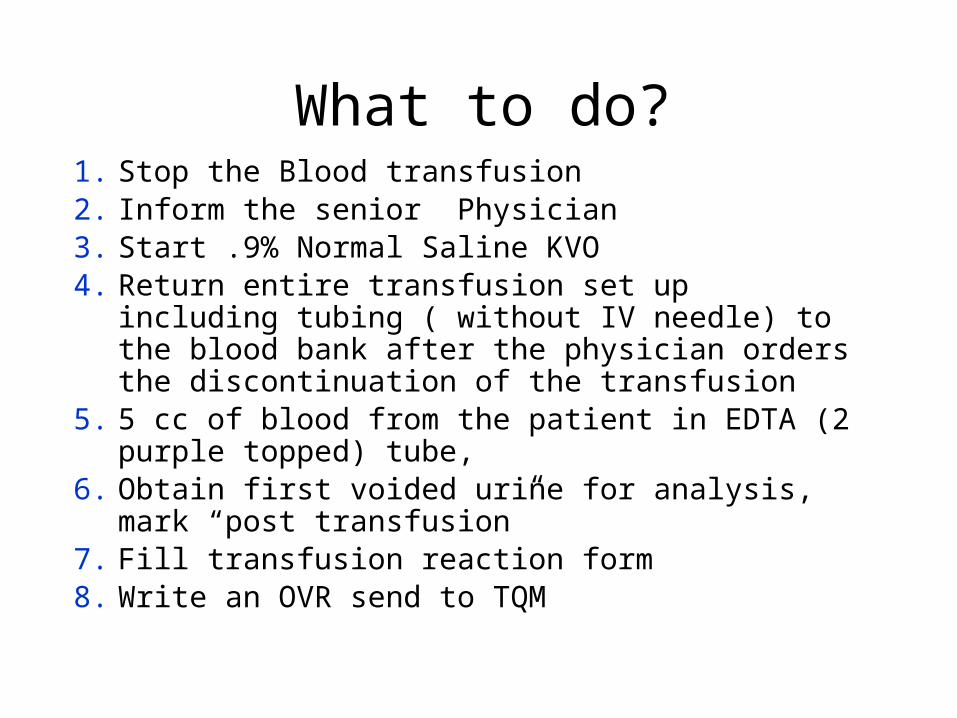
1. Stop the Blood transfusion2. Inform the senior Physician3. Start .9% Normal Saline KVO4. Return entire transfusion set up including tubing
( without IV needle) to the blood bank after the physician orders the discontinuation of the transfusion
5. 5 cc of blood from the patient in EDTA (2 purple topped) tube,
6. Obtain first voided urine for analysis, mark “post transfusion”
7. Fill transfusion reaction form 8. Write an OVR send to TQM
What to do?
Transfusion Of Incompatible Blood
1. Transfusion of incompatible blood component is regarded as an error that should be avoided
2. Some situation it is the only option available that can save patient life
3. The patients physician will always be informed of decision by director of the blood bank
Summary
• Doctors & Nurses have a major role in blood transfusion practice.
• They should follow all safety and general precautions throughout all of the steps for administering transfusions.
• They should adhere to KAUH transfusion policy & procedure
Thank youCSSC
Top Related