







Languages
Pages
Legal


Becoming a “Conversation Ready” OrganizationSession 4: Respect- Meeting people where they are as illness advances
July 11, 2017
Today’s presenters have
nothing to disclose
Lauge Sokol-HessnerKate LallyKelly McCutcheon Adams

Senior Project Manager
Angela G. Zambeaux, Senior Project Manager, Institute for Healthcare Improvement, has managed a wide variety of IHI projects, including a project funded by the US Department of Health and Human Services that partnered with the design and innovation consulting firm IDEO around shared decision-making and patient-centered outcomes research; the STAAR (STateAction to Reduce Avoidable Rehospitalizations) initiative; virtual programming for office practices; and in-depth quality and safety assessments for various hospitals and hospital systems. Prior to joining IHI, Ms. Zambeaux provided project management support to a small accounting firm and spent a year in France teaching English to elementary school students.

Faculty
Kate Lally, MD, FACP, Chief of Palliative Care, Care New England Health System, also serves as Medical Director at Integra Accountable Care Organization and Hospice Medical Director of Care New England VNA Hospice. At Care New England, she developed a system-wide comprehensive, interdisciplinary palliative care program that has expanded from the hospital into the community. Dr. Lally spearheaded Care New England's role as a Pioneer Sponsor in the Institute for Healthcare Improvement's Conversation Ready initiative and helped integrate Conversation Ready principles into the health system's palliative care program. She has served on the faculty of the IHI since 2013, and as a result has developed and led a number of on-line and in-person educational initiatives for both national and international audiences. As a result of her work, she has received numerous awards including “Top Doc” in RI monthly, Providence Business News “40 under 40” and was named an “Inspiring Hospice and Palliative Medicine Leader Under 40” by the American Academy of Hospice and Palliative Medicine. She is a graduate of Yale School of Medicine and did her post-graduate training in Internal Medicine at the Hospital of the University of Pennsylvania. She currently serves as an Assistant Professor of Medicine (Clinical) at the Warren Alpert Medical School of Brown University.

Faculty
Lauge Sokol-Hessner, MD, is a hospitalist and the Associate Director of Inpatient Quality at Beth Israel Deaconess Medical Center (BIDMC) in Boston. He has worked in southern Africa on multiple occasions, completed medical school and residency at the University of Pennsylvania in Philadelphia, and worked as an attending physician at the University of Washington Medical Center in Seattle before joining BIDMC. On the wards, his work includes collaborating as a member of interdisciplinary teams of health care providers, coaching medical students and residents as they develop their communication skills, and caring for a broad variety of patients and their families. In his quality improvement role he leads several projects, including Conversation Ready at BIDMC.
Webinar Series ObjectivesAt the conclusion of this webinar series, participants will be able to:
Articulate the vision and mission of The Conversation Project and different
ways to approach end-of-life care conversations.
Describe strategies that have worked for pioneer organizations to engage
patients and families in discussions to understand what matters most to them
at the end-of-life
Explain ideas for reliably stewarding this information across the health care
system, including strategies for working with electronic health records
Teach ways to engage communities that help to activate the public in having
these conversations in advance of a potential medical crisis
Test methods to help staff engage in this work personally before exemplifying
it for their patients
Describe changes to CMS reimbursement policies for advanced care planning
conversations
Today’s Agenda
Introductions
Debrief Sessions 3-4 Actions
Respect: Meeting people where they are
as illness advances
Action Period Assignment

Conversation Ready Principles
1. Engage with our patients and families to understand what matters most to them at the end of life
2. Steward this information as reliably as we do allergy information
3. Respect people’s wishes for care at the end of life by partnering to develop shared goals of care
4. Exemplify this work in our own lives so that we understand the benefits and challenges
5. Connect in a manner that is culturally and individually respectful of each patient
Connect
Engage Steward Respect
Exemplify

Schedule of Calls
Session 1 – The Conversation Project: Reaching people where they live, work, and prayDate: Tuesday, May 23, 2017, 2:00 PM-3:00 PM Eastern Time
Session 2 – Engage: Moving from passive to proactiveDate: Tuesday, June 6, 2017, 2:00 PM-3:00 PM Eastern Time
Session 3 – Steward: Achieving the reliability of allergy informationDate: Tuesday, June 20, 2017, 2:00 PM-3:00 PM Eastern Time
Session 4 – Respect: Meeting people where they are as illness advances Date: Tuesday, July 11, 2016, 2:00 PM-3:00 PM Eastern Time
Session 5 – The Exemplify Principle in Action/ Connecting In a Culturally Respectful MannerDate: Tuesday, July 25, 2:00 PM-3:00 PM Eastern Time
Session 6 – CMS ReimbursementDate: Tuesday, August 8, 2:00 PM-3:00 PM Eastern Time
Suggested Action (spans sessions 3 and 4)
Review the charts of the last 20 patients* who died in your setting.
As you review the charts, note evidence of the following:
Advance directive documents are accessible and can be understood by the care team (i.e., not just a “Yes/No” notation that the patient has an advance directive);
Documentation of provider and patient conversation(s) — or conversation(s) with a surrogate decision maker, if the patient is not able to participate — about “What matters?” to the patient regarding end-of-life care wishes;
Location of death;
Whether patient received life-sustaining treatment;
A few details about the patient’s medical history and situation immediately prior to death; and
The presence of indicators about whether the care the patient received was aligned with their documented end-of-life care wishes.
Consider including representatives from the involved clinical services in the review, to understand their perspectives on the care provided and to engage them in the work.
* We recommend 20 for a fuller picture of your system but if that is a stopper, then do 10.
To share today:
Briefly document two stories gleaned from the review that illustrate current end-of-life care processes (to help build will among colleagues and create a clearer picture of reasons to engage in work).
For example: Mr. S had a note in his patient chart that an advance directive existed, but it was
not accessible in the patient chart. There was no documentation of discussions with providers about end-of-life care goals, and the care team was not able to determine alignment of care goals and Mr. S’s end-of-life care wishes.
Ms. W had an accessible advance directive and detailed notes about end-of-life care goals in her patient record, and she was transferred to an inpatient hospice unit in apparent alignment with her wishes.
Information from the review can be used to guide team conversations about setting an aim, selecting a subpopulation, and identifying the best location for pilot testing. Additionally, this information can help build will when discussing work with colleagues.

The Respect PrincipleMeeting people where they are as illness advances
Kate Lally, MD, FACPLauge Sokol-Hessner, MD

Retaining Hope Health Care
At Retaining Hope Health Care there is a disconnect
between anything that is known about patient wishes and
their actual care leading up to their deaths. Still not wanting
to take away hope and not wanting to declare that the end
is nigh, care planning conversations do not surface the
gravity of patient situations and opportunities to direct care
differently. Families expressed being surprised afterwards
that death was so close when they still thought treatment
would be effective.

Reliability Health Care
At Reliability Health Care, early engagement and reliable
stewarding means that there is confidence that what has
mattered most to patients over time is known and that this
information is accessible and ready to be confirmed and
adapted to current circumstances as patients get closer to
death. Patients and their loved ones are not caught off
guard about the gravity of their illnesses and have an
opportunity to take actions that have meaning to them prior
to the end of their lives.
What does it mean to respect patient wishes?
Consider three core conversation topics:
– Information about diagnoses, prognoses and treatments
– “What matters most” to the patient
– Shared decision making
What does Reliability get right?
– Conversations about serious illnesses and poor prognoses
– Recognition that hope is not inconsistent with developing a plan
– Early engagement and stewarding about “what matters most”
– Engagement in shared decision making
– Care consistent with “what matters most” to patients
– Doing it the right way, each time, with every patient

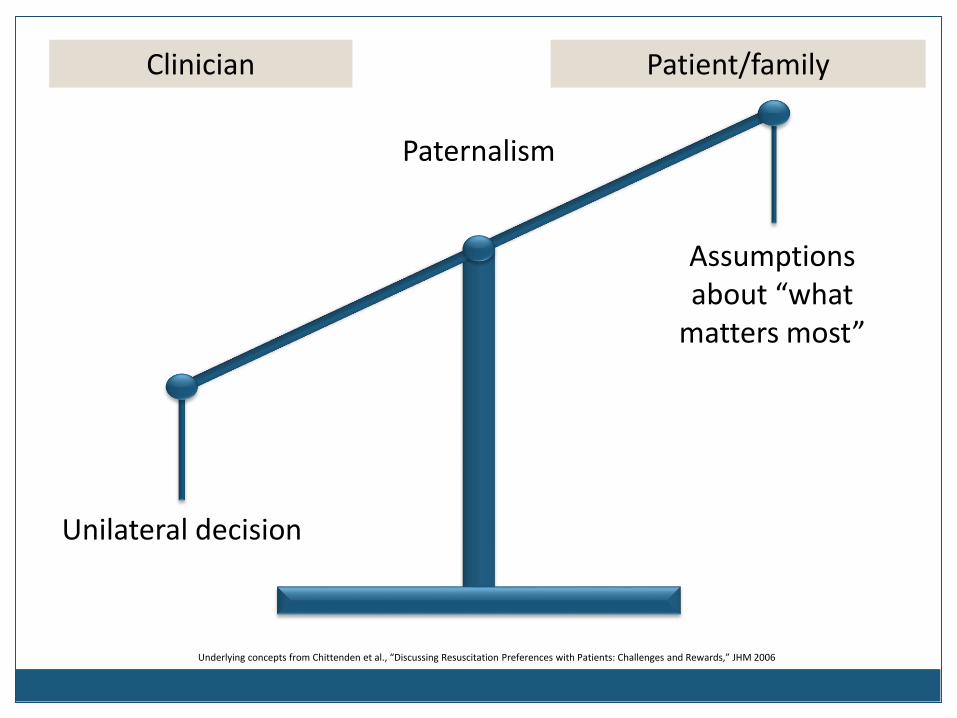
Underlying concepts from Chittenden et al., “Discussing Resuscitation Preferences with Patients: Challenges and Rewards,” JHM 2006
Clinician Patient/family
Underlying concepts from Chittenden et al., “Discussing Resuscitation Preferences with Patients: Challenges and Rewards,” JHM 2006
Assumptions about “what
matters most”
Paternalism
Unilateral decision
Clinician Patient/family
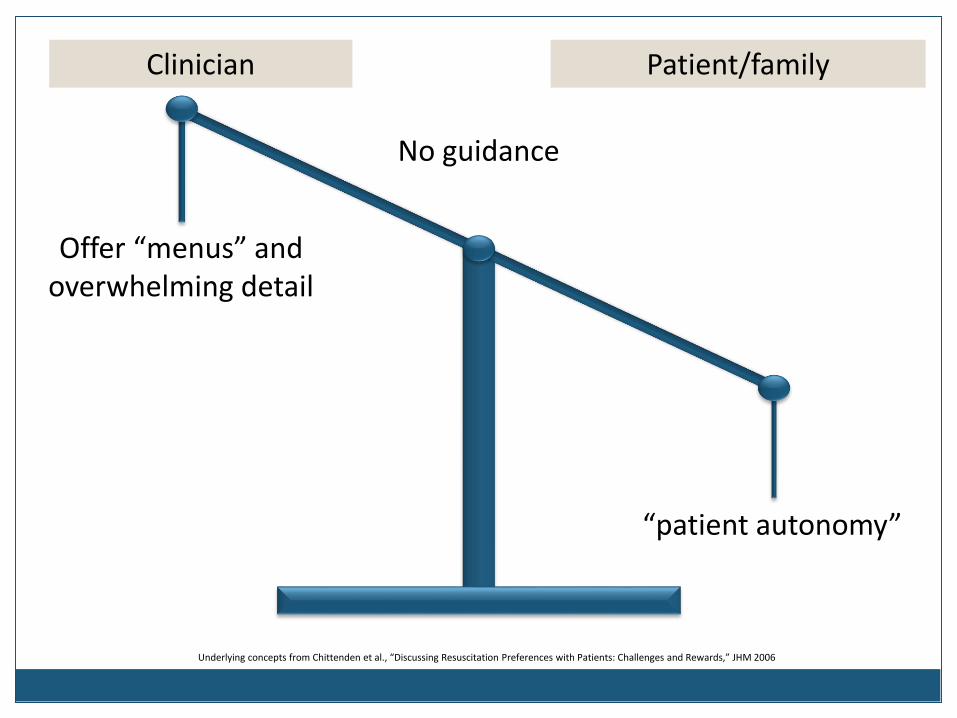
Underlying concepts from Chittenden et al., “Discussing Resuscitation Preferences with Patients: Challenges and Rewards,” JHM 2006
“patient autonomy”
Offer “menus” and overwhelming detail
No guidance
Clinician Patient/family

Underlying concepts from Chittenden et al., “Discussing Resuscitation Preferences with Patients: Challenges and Rewards,” JHM 2006
Incorporate the patient’s goals,
values, preferences
Use clinical judgment when discussing
treatments & side effects
“Co-production”through shared decision making
Clinician Patient/family


It is about providing care consistent with wishes…
Mrs. A is a woman with recurrent
cervical cancer.
She struggled with initial trials of
chemotherapy and became very
symptomatic
She understands that her cancer
is no longer curable
She no longer wants chemo,
feels that she wants to focus on
quality of life over length of life
Her goal is to stay home and go
on to hospice
She dies at home 3 months later
Mrs. B is a woman with recurrent cervical cancer.
She struggled with initial trials of chemotherapy and became very symptomatic
She understands that her cancer is no longer curable
Her daughter is getting married in 3 months and she wants to do everything to make it to her daughter’s wedding
She undergoes chemotherapy until the week before her daughter’s wedding
She goes on hospice and dies 2 weeks after her daughter’s wedding
What are the ways in which this goes wrong?
Failure to collect information about “what matters most”
and the goals of care
Health care professionals insert their own perspectives
and values, usually unconsciously and unintentionally
Lack of confidence that informed decisions have been
made
– Sometimes a lack of shared decision making
– Sometimes just a sign of poor team communication
– Either way can lead to moral distress
Dzeng et al., “Moral Distress Amongst American Physician Trainees Regarding Futile Treatments at the End of Life: A Qualitative Study,” JGIM 2015

Pause
Questions? Comments?

3 cases exploring Respect
1. When the patient cannot tell us “what
matters most”
2. When prognosis is uncertain
3. When it’s not clear that care is consistent
with “what matters most”
Case 1 – Mrs. Jones
Had a large stroke several months before her
hospitalization
Difficulty eating and with caring for herself
Daughter was her primary caretaker
Mrs. Jones found at home minimally responsive
Admitted to hospital with large stroke, unable to speak
for herself

Case 1 – Mrs. Jones
Doctors considering feeding tube vs comfort care
Daughter is tearful and anxious making decisions
“I don’t know what she would want, we never talked
about it”
How do we identify Mrs. Jones’ wishes to make sure we
are respecting them?
How do we know we are respecting
Mrs. Jones’ wishes?
In the absence of stated preferences, we can infer things
from different data sources:
– Gather info about how she lived her life
– What was important to her?
– What did she tell her daughter about her quality of life?
– What were her experiences with her parents’ deaths?
How would her prognosis affect what mattered most to
her?

Suggested language for Mrs. Jones’ daughter
“What was your mother like when she was well?
If we look back a couple of years ago, what type
of things did she like to do?”
“How did she feel about her quality of life after
her last stroke?”
“She has had a major stroke. If we place a
feeding tube she will likely need to go to a
nursing home for 24 hour care. How would she
feel about that?”

3 cases exploring Respect
1. When the patient cannot tell us “what
matters most”
2. When prognosis is uncertain
3. When it’s not clear that care is consistent
with “what matters most”

Case 2 – Mrs. Smith
Mrs. Smith is a 71 year woman with COPD
Has advance directive stating DNR/DNI
She gets very ill and goes to the hospital
Placed on BIPAP
Physicians feel she has a good chance of recovering
with a short trial of intubation

How do we make sure we are
respecting Mrs. Smith’s wishes?
We need to understand her concerns and fears around
her illness and aggressive treatments
Would she have been willing to try it for a short period of
time?
– Time limited trials
– Viewing prognosis as continuously evolving
Set a future date to re-address prognosis and goals if
she does go on a ventilator

Language to elicit what matters
“Your mother said she would not want to be on a ventilator.
That is certainly understandable. What were her concerns
about the ventilator?”
“Was she afraid of being on the ventilator for a long period of
time?”
“I think we could improve her breathing if she went on the
ventilator for a few days. Would she be willing to do that?”
“If she is not improved in 3-4 days we should discuss whether
we should continue or shift our focus to comfort at that time”

3 cases exploring Respect
1. When the patient cannot tell us “what
matters most”
2. When prognosis is uncertain
3. When it’s not clear that care is
consistent with “what matters most”

Case 3 – Mrs. Lynch
78yo woman with COPD and lung cancer
Declining for several months
Now mostly house bound, oxygen dependent
Wants to spend her remaining time with family and avoid
returning to the hospital again
Advance care planning has never been attempted
Develops pneumonia

Case 3 – Mrs. Lynch
Without advance care planning
Poor prognosis not acknowledged, even when patient asked
Admitted to the ICU with pneumonia and delirium, intubated
Unclear who should be her “voice,” contributing to family disagreements
Difficult situation, with loss and sadness, anger, confusion and moral distress
Develops complications, doesn’t regain capacity, dies in the hospital
Doesn’t complete her life in the ways that mattered most to her
Complicated bereavement
With advance care planning
Health care professionals would have talked about her prognosis in patient-centered ways and aligned around hope, but made a plan in case things didn’t go well
– Surrogate decision maker
– “What matters most”
– Enrolls in hospice
– POLST/MOLST
Pneumonia would occur, and she’d be given treatment consistent with her goals
It’d be a difficult situation, with loss and sadness, but everyone would have confidence in the decisions that had been made
She would have died surrounded by family and in the ways that mattered most to her
Improved bereavement
Mrs. Lynch (and her family) have suffered
preventable harm
If we agree that…
– It is our responsibility – as health care professionals – to
preserve patient autonomy and ensure patients are always given
the opportunity to make informed decisions
– And that in the context of serious illness, advance care planning
is the way of ensuring informed decisions are being made
Then…
– What keeps us from “seeing” this as preventable harm?
– What will it take to generate consensus that the lack of
appropriate advance care planning for seriously ill patients is
poor quality care?

Consider another story of preventable harm…
Central-line associated bloodstream infections (CLABSIs)– Used to be that “they just happen as part of care”
– Innovation led to a bundle of discrete interventions to prevent them
– Now reliable use of the bundle is considered the standard of care – the harm is largely preventable
What will it take to make these aspects of advance care planning the standard of care?– Identifying a surrogate decision maker
– Having conversations– Sharing the diagnosis, prognosis and treatment options
– Understanding “what matters most”
– Shared decision making
– Appropriately using POLST-paradigm forms

Engaging in the “practice of respect”
Capturing preventable emotional harm events, treating them
with the same rigor with which we treat physical harm events
– Assessing, categorizing, understanding, discussing
Learning about the importance of a reliable “practice of
respect” for seriously ill patients from individual cases/stories:
– Lack of indicated advance care planning
– Failure to appropriately involve surrogate
– Problems discussing serious news
– Lack of informed decision making
– Failure to anticipate future emergencies
– Problems managing limitations on life-sustaining treatment
Sokol-Hessner, Folcarelli and Sands, “Emotional harm from disrespect: the neglected preventable harm,” BMJ Quality & Safety, 2015

Pause
Questions? Comments?

Suggested Actions
Review one of the following Ethnogeriatrics modules on
https://geriatrics.stanford.edu/– African-American
– American Indian
– Asian Indian
– Chinese
– Filipino
– Native Hawaiian and Pacific Islander
– Hispanic/Latino
– Japanese
– Korean
– Pakistani
– Vietnamese
Identify at least one story in your own practice where culture
competency fell through the cracks and less than optimal care was
provided at the end-of-life
Session 5
Lauge Sokol-Hessner, MD
Hospitalist and the Associate Director of Inpatient Quality
at Beth Israel Deaconess Medical Center (BIDMC)
Tuesday, July 25, 2-3 PM Eastern
The Exemplify Principle in Action/ Connecting In a Culturally Respectful Manner
Rev. Rosemary Lloyd, BSN, MDiv
Advisor to the Faith-Based Community,
The Conversation Project

Thank You!
Please let us know if you have any questions or
feedback following today’s webinar.
Top Related