






Languages
Pages
Legal


COPD-Asthma


Risk Factors for COPD
NutritionNutrition
InfectionsInfections
Socio-economic Socio-economic statusstatus
Aging PopulationsAging Populations


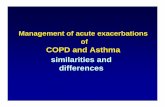
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0Proportion of 1965 Rate Proportion of 1965 Rate
1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998
–59%–59% –64%–64% –35%–35% +163%+163% –7%–7%
CoronaryHeart
Disease
CoronaryHeart
Disease
StrokeStroke Other CVDOther CVD COPDCOPD All OtherCauses
All OtherCauses
Source: NHLBI/NIH/DHHSSource: NHLBI/NIH/DHHS

Prevalence of allergies and asthma in PakistanM.Y. Noori, S.M. Hasnain, and M.A. Waqar.
World Allergy Organization Journal & November 2007
• The frequency of wheezing was found to be 15.2%, • while the diagnosed cases of asthma were 9.5%. • The frequency of allergic rhinitis was found to be 34.3%. • The frequency of those having allergic rhinitis as well as
wheezing episodes was 8%. • There was no statistically significant difference between
asthmatics and non-asthmatics by sex (P-value:0.402). • Socioeconomic status was found to affect significantly (p
value 0.001) as the prevalence of diagnosed asthma cases was 6.17% in high socioeconomic class,13.11% in the middle-class and 2.4% in the low socioeconomic class.
• Family history of atopy was also found to be significantly higher in asthmatics.

NOCTURNAL ASTHMA IN SCHOOL CHILDREN OF SOUTH PUNJAB,PAKISTANGhulam Mustafa, Pervez Akber Khan, Imran Iqbal
J Ayub Med Coll Abbottabad 2008;20(3)
• The parents reported nocturnal asthma in 177 (6%) of their children with an equal prevalence in boys and girls,

Anatomy

LUNG INFLAMMATIONLUNG INFLAMMATION
COPD PATHOLOGYCOPD PATHOLOGY
OxidativeOxidativestressstress ProteinasesProteinases
Repair Repair mechanismsmechanisms
Anti-proteinasesAnti-proteinasesAnti-oxidantsAnti-oxidants
Host factorsAmplifying mechanisms
Cigarette smokeCigarette smokeBiomass particlesBiomass particles
ParticulatesParticulates
Pathogenesis of COPD
Source: Peter J. Barnes, MD

Differences in Inflammation and its Consequences: Asthma and COPD
YYYY YY
Mast cellMast cell
CD4+ cellCD4+ cell(Th2)(Th2)
EosinophilEosinophil
AllergensAllergens
Ep cellsEp cells
ASTHMAASTHMA
BronchoconstrictiBronchoconstrictionon
AHRAHR
Alv macrophageAlv macrophage Ep cellsEp cells
CD8+ cellCD8+ cell(Tc1)(Tc1)
NeutrophilNeutrophil
Cigarette smokeCigarette smoke
Small airway narrowingSmall airway narrowingAlveolar destructionAlveolar destruction
COPDCOPD
Reversible IrreversibleAirflow LimitationAirflow Limitation
Source: Peter J. Barnes, MD

COPD airway

Asthma airway

Mucus gland hyperplasia
Goblet cellhyperplasia
Mucus hypersecretion Neutrophils in sputum
Squamous metaplasia of epithelium
↑ Macrophages
No basement membrane thickening
Little increase in airway smooth muscle
↑ CD8+ lymphocytes
Changes in Large Airways of COPD Patients
Changes in Large Airways of COPD Patients
Source: Peter J. Barnes, MD

NormalNormalInspiration
Expiration
alveolar attachments
Mild/moderateMild/moderateCOPD COPD
loss of elasticity
Severe Severe COPD COPD
loss of alveolar attachments
closure
small small airwayairway
Dyspnea↓ Exercise capacity
Air trappingAir trappingHyperinflationHyperinflation
↓ ↓ HealthHealthstatusstatus
Air Trapping in COPD
Source: Peter J. Barnes, MD

Disrupted alveolar attachments
Inflammatory exudate in lumen
Peribronchial fibrosisLymphoid follicle
Thickened wall with inflammatory cells- macrophages, CD8+ cells, fibroblasts
Changes in Small Airways in COPD Patients
Source: Peter J. Barnes, MD

Alveolar wall destruction
Loss of elasticity
Destruction of pulmonarycapillary bed
↑ Inflammatory cells macrophages, CD8+ lymphocytes
Changes in the Lung Parenchyma in COPD Patients
Source: Peter J. Barnes, MD

Cigarette smoke Cigarette smoke (and other irritants)(and other irritants)
PROTEASES PROTEASES Neutrophil elastaseNeutrophil elastaseCathepsinsCathepsinsMMPsMMPs
Alveolar wall destructionAlveolar wall destruction(Emphysema)(Emphysema)
Mucus hypersecretionMucus hypersecretion
CD8CD8+ +
lymphocytelymphocyte
Alveolar Alveolar macrophagemacrophage
EpithelialEpithelialcellscells
FibrosisFibrosis(Obstructive(Obstructivebronchiolitis)bronchiolitis)
FibroblastFibroblast
MonocyteMonocyteNeutrophilNeutrophil
Chemotactic factorsChemotactic factors
Inflammatory Cells Involved in COPD
Source: Peter J. Barnes, MD

Anti-proteases
SLPI 1-AT
Proteolysis
OO22--, H, H220022
OHOH.., ONOO, ONOO--
Mucus secretion
Plasma leak Bronchoconstriction
NF-NF-BB
IL-8IL-8
NeutrophilNeutrophilrecruitmentrecruitment
TNF-TNF-
IsoprostanesIsoprostanes
↓ ↓ HDAC2HDAC2
↑↑InflammationInflammationSteroidSteroid
resistanceresistance
Macrophage NeutrophilOxidative Stress in COPD
Source: Peter J. Barnes, MD

Chronic hypoxiaChronic hypoxia
Pulmonary vasoconstrictionPulmonary vasoconstriction
MuscularizationMuscularization
Intimal Intimal hyperplasiahyperplasia
FibrosisFibrosis
ObliterationObliteration
Pulmonary hypertensionPulmonary hypertension
Cor pulmonaleCor pulmonale
DeathEdemaEdema
Pulmonary Hypertension in COPD
Source: Peter J. Barnes, MD

Asthma

Emphysema- CT scan

Emphysema

Chronic bronchitis

PEF meters

Spirometry: Normal and Patients with COPD


Lung Volumes and Capacities

PFTsASTHMA COPD
FEV1 Decreased in active asthma Decreased-stage of disease
FVC Decreased Decreased
FEV1/FVC Decreased decreased
TLC Normal or increased Normal or increased
FRC Normal or increased Normal or increased
RV Normal or Increased Normal or increased
DLCO Normal or Increased Decreased in Emphysema

IV: Very Severe III: Severe II: Moderate I: Mild
Therapy at Each Stage of COPD
FEV1/FVC < 70%
FEV1 > 80% predicted
FEV1/FVC < 70%
50% < FEV1 < 80%
predicted
FEV1/FVC < 70%
30% < FEV1 < 50% predicted
FEV1/FVC < 70%
FEV1 < 30% predicted
or FEV1 < 50% predicted plus chronic respiratory failure
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add inhaled glucocorticosteroids if repeated exacerbations
Active reduction of risk factor(s); influenza vaccinationAdd short-acting bronchodilator (when needed)
Add long term oxygen if chronic respiratory failure. Consider surgical treatments
Top Related