




Languages
Pages
Legal


Assessment and
Management of Disorders of
the Knee, Shoulder, and Hip

William D. Stanish, MD, FRCS(C), FACS, AOAProfessor Emeritus, Department of Surgery
Dalhousie University, Halifax, Nova Scotia, Canada
Director, Orthopaedic and Sport Medicine Clinic of Nova
Scotia
My Disclosures


The Plan of Attack

1. Introduce the subject
2. Some facts about the area
3. Present the case profile
4. Introduce you to the actual patient
5. Offer some “Take Home Pearls”

My Philosophy
Guiding Principles
Pearl #1“Understand the natural history of
the disorder”

Pearl #2“Always be a skeptic”

Pearl #3“Form follows function”
Hippocrates – 350 BC


The Knee – Facts

1. Knee Fact - Intrinsically
unstable
2. Knee Fact - Easily injured
3. Knee Fact - Slow to heal



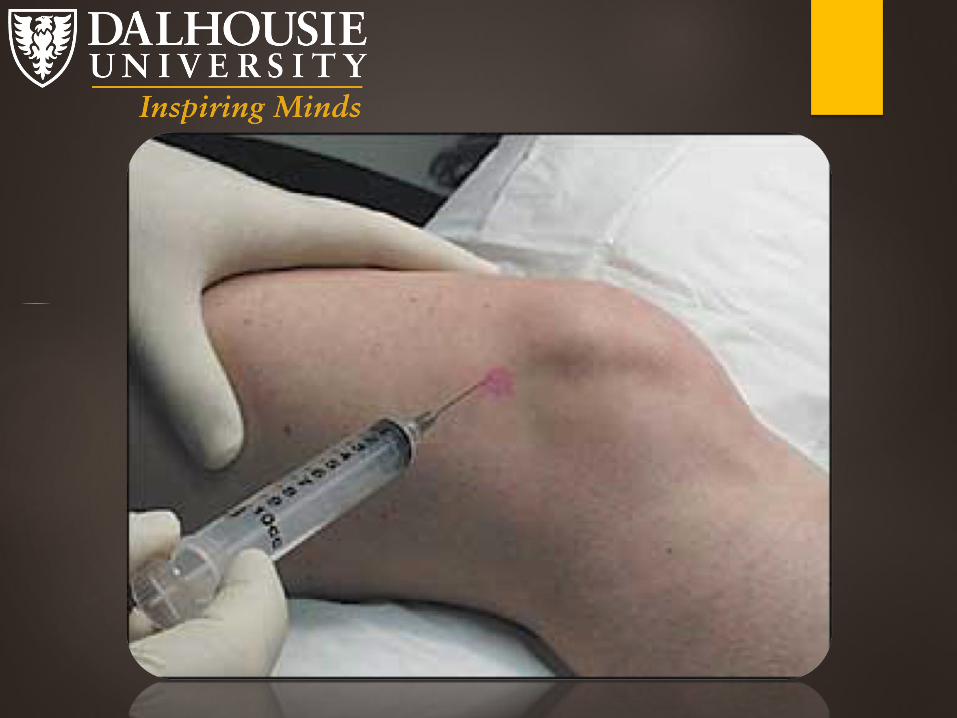
Introducing the “Knee
Patient”

Her Story
• Her Examination
33 y.o. Graduate Student
Very active
Injured her right knee in
roller derby
Persisted with “some” pain

Knee Pearls
1. If it hurts – Danger
2. If it swells – Danger
3. Surgery is not always
required
The Shoulder - Facts
1. Shoulder Fact - Intrinsically
unstable
2. Shoulder Fact - Pathology
dictated by age
3. Shoulder Fact - Slow to heal


Introducing the
“Shoulder Patient”
His Story
• His Examination
• 78 y.o. very active
gentleman
• Bilateral shoulder pain
• Difficulty with sleeping
• Rotator cuff tears


Shoulder Pearls
1. Cuff tears are common
2. Surgery is not always
required
The Hip – Facts

1. Hip Fact – Intrinsically stable
2. Hip Fact – Diagnostic Challenge
3. Hip Fact – Usually not surgical

Introducing the “Hip
Patient”

Her Story
• Her Examination
58 y.o Physiotherapist with
periodic hip pain –
sometimes severe!


Hip Pearls
1. Listen to the patient
2. Be prepared to “wait it out”
3. No rush to surgery
“THE PHILOSPHIES OF ONE AGE
HAVE BECOME THE
ABSURDITIES OF THE NEXT”
~ Sir William Osler
Top Related