







Languages
Pages
Legal


Are we overdoing it with micronutrient supply to pre-
schoolers?Omar Dary USAID, Bureau for Global Health, Nutrition
DivisionMicro-University
Washington DCMarch 7th, 2014
OD-2014-6
2
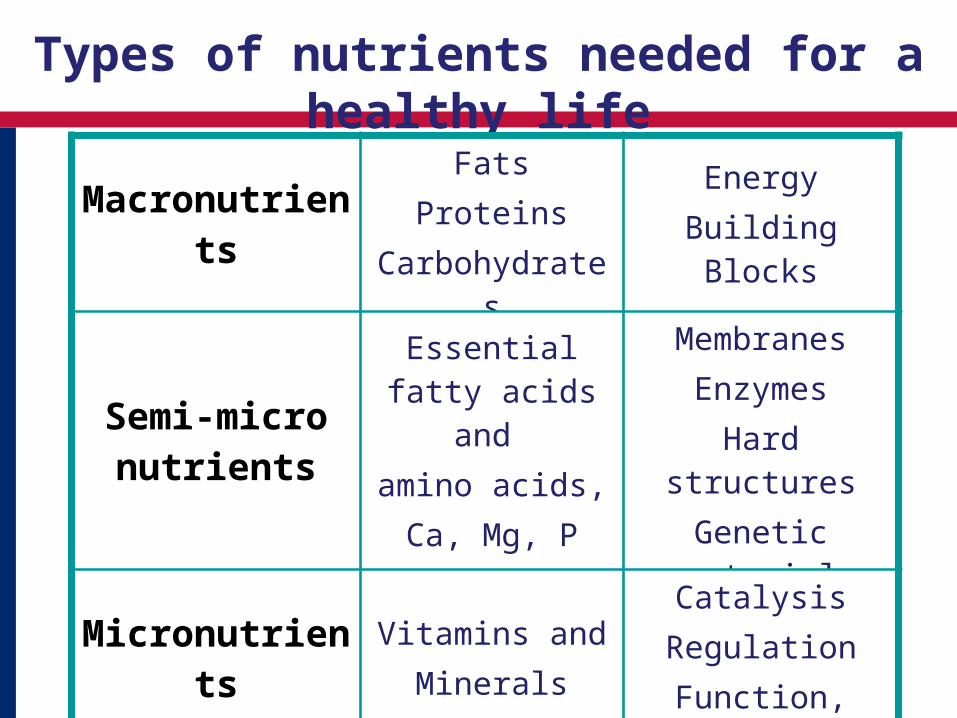
Types of nutrients needed for a healthy life
MacronutrientsFats
ProteinsCarbohydrates
EnergyBuilding Blocks
Semi-micro nutrients
Essential fatty acids and
amino acids,Ca, Mg, P
MembranesEnzymes
Hard structuresGenetic material
MicronutrientsVitamins and
Minerals
CatalysisRegulation
Function, Vision
3
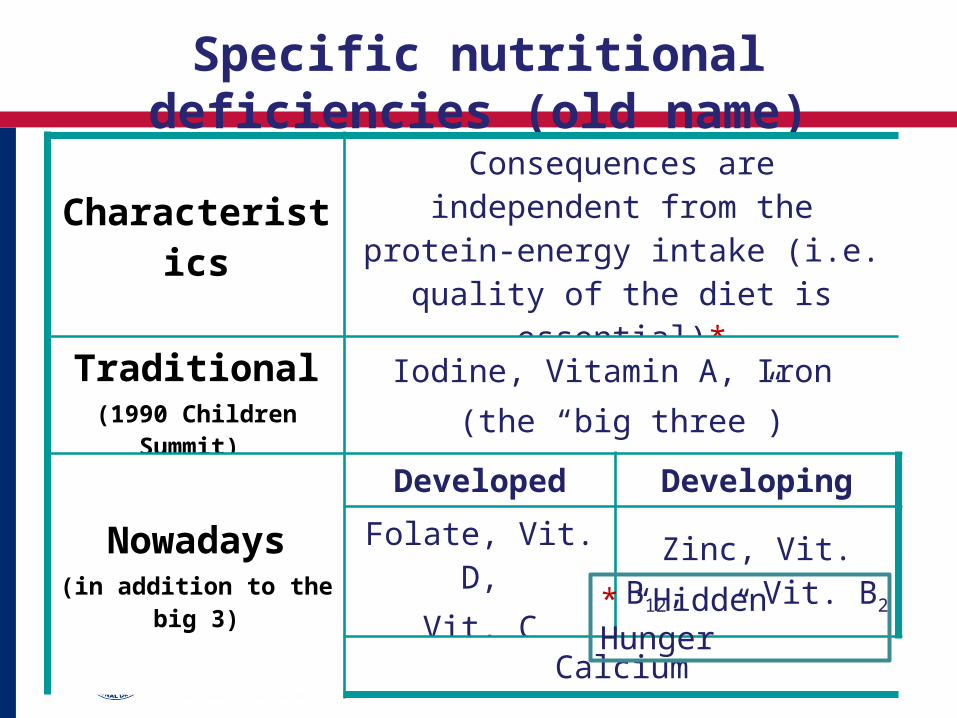
Specific nutritional deficiencies (old name)
CharacteristicsConsequences are independent from the protein-energy intake (i.e. quality
of the diet is essential)*
Traditional(1990 Children Summit)
Iodine, Vitamin A, Iron (the “big three”)
Nowadays(in addition to the big 3)
Developed Developing
Folate, Vit. D,Vit. C
Zinc, Vit. B12, Vit. B2
Calcium
* “Hidden Hunger”

Fetus Abortion Stillborn Congenital abnormalities Perinatal mortality Infant mortality Neurologic cretinism: Mutism, mental retardation – deafness Endemic cretinism: dwarfism/ mental deficiency Psychomotor impairment
Infant Hypothyroidism / Irreversible mental retardation Children and adolescent
IQ reduced / Goiter / Hypothyroidism / Impaired physical and mental development
Adult Goiter and complications Hypothyroidism
Consequences of iodine deficiency
4 4

5
Consequences of vitamin A deficiency
• Deterioration of ocular conjunctive and cornea
• Less capacity to fight infections
• Alterations in growth and development
• Impaired visual and reproductive capability
• Night blindness• Permanent blindness• Death
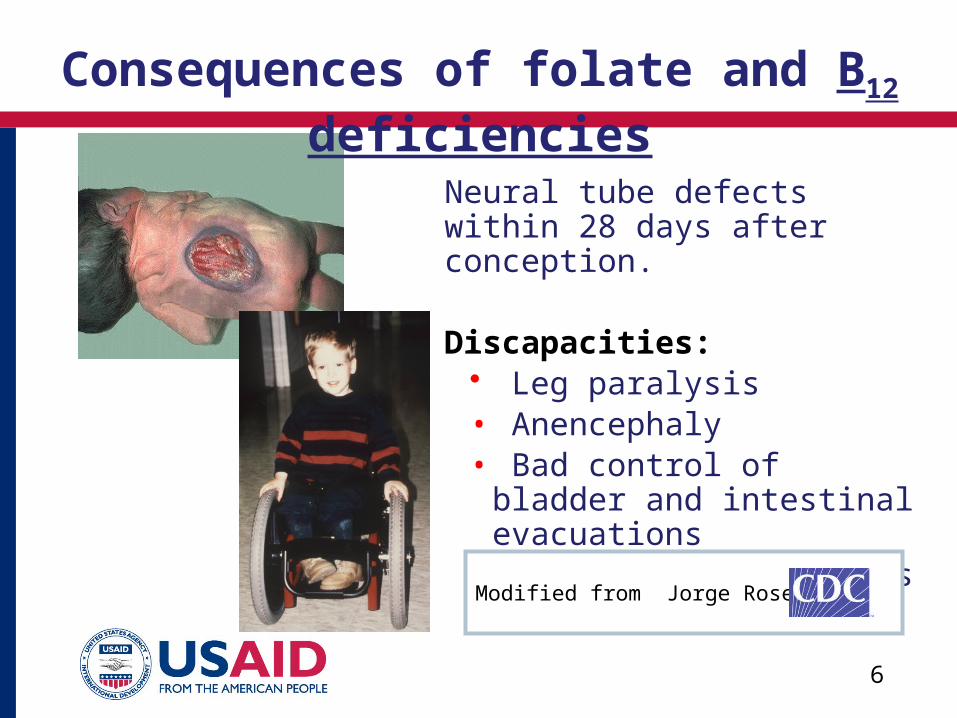
Neural tube defects within 28 days after conception.
Discapacities:• Leg paralysis• Anencephaly• Bad control of bladder and
intestinal evacuations• Learning difficulties
Modified from Jorge Rosenthal
Consequences of folate and B12 deficiencies
6 6
7
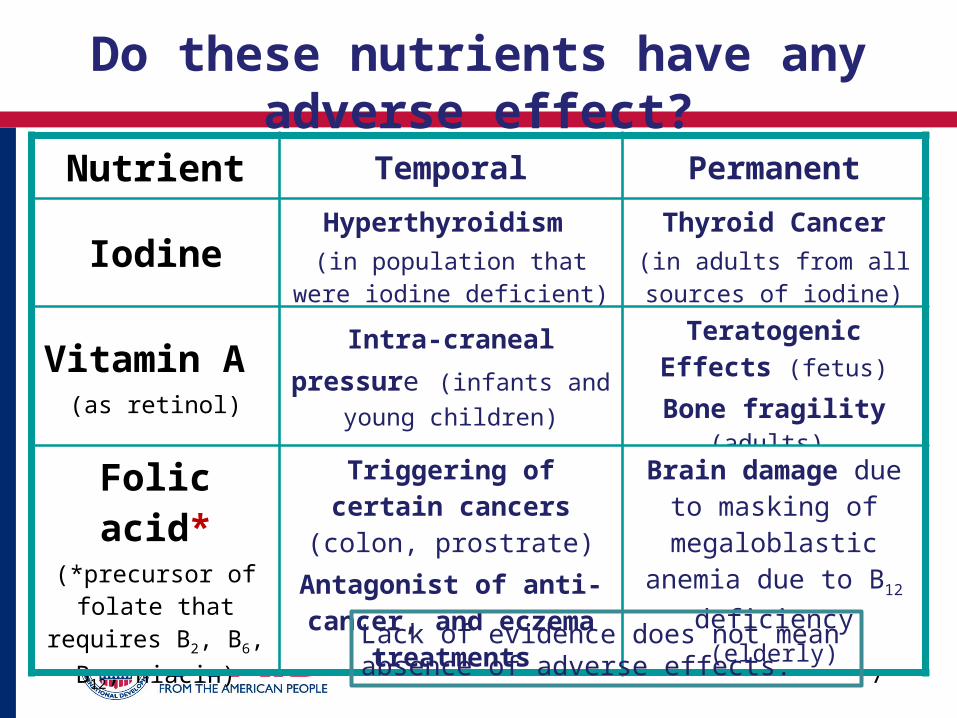
Do these nutrients have any adverse effect?
Nutrient Temporal Permanent
IodineHyperthyroidism
(in population that were iodine deficient)
Thyroid Cancer(in adults from all sources
of iodine)
Vitamin A (as retinol)
Intra-craneal pressure (infants and young children)
Teratogenic Effects (fetus)
Bone fragility (adults)
Folic acid*(*precursor of folate that requires B2, B6,
B12, niacin)
Triggering of certain cancers (colon, prostrate)
Antagonist of anti-cancer, and eczema
treatments
Brain damage due to masking of
megaloblastic anemia due to B12 deficiency
(elderly)
Lack of evidence does not mean absence of adverse effects.

8
Cumulativerisk of deficiency
Cumulativerisk of toxicity
Distributionof requirements
Distribution ofrisk of toxicity
Acceptable Rangeof Oral intake
(AROI )
Total oral intake
NormalHomeostasis
A BDose
Perc
enta
ge o
f po
pula
tion
at r
isk 100 100
50 50
EAR
RNI
LOAEL
NOAEL
UF
UL
Modified from the International Programme on Chemical Safety (IPCS), 2002.
How to estimate safety?
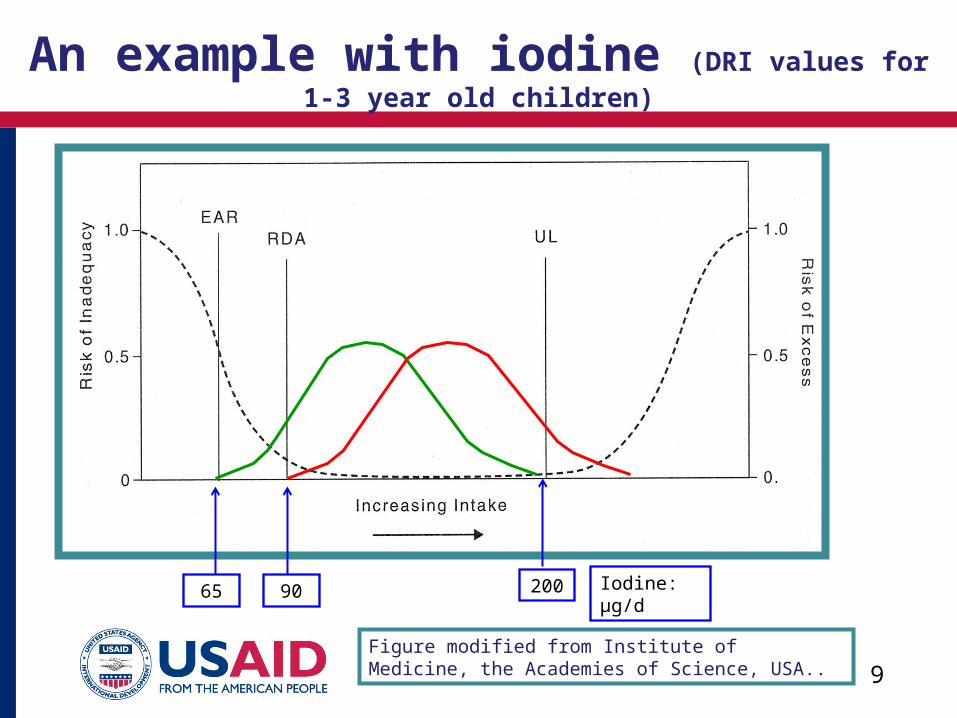
9Figure modified from Institute of Medicine, the Academies of Science, USA..
An example with iodine (DRI values for 1-3 year old children)
65 90 200 Iodine: µg/d
10
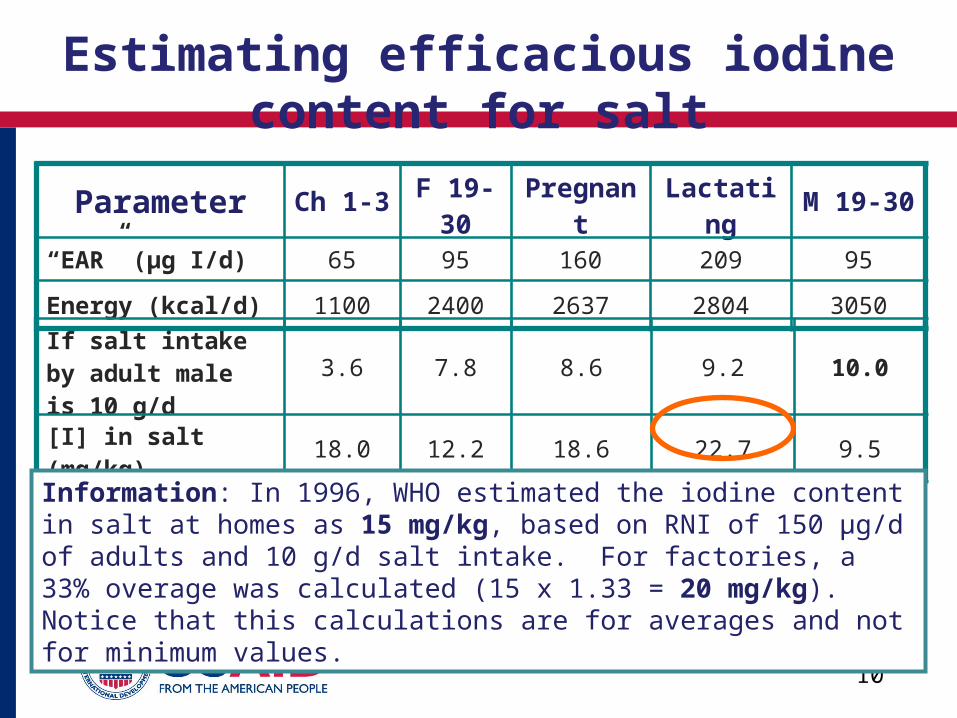
Estimating efficacious iodine content for salt
Parameter Ch 1-3 F 19-30 Pregnant Lactating M 19-30
“EAR” (µg I/d) 65 95 160 209 95
Energy (kcal/d) 1100 2400 2637 2804 3050
If salt intake by adult male is 10 g/d
3.6 7.8 8.6 9.2 10.0
[I] in salt (mg/kg) 18.0 12.2 18.6 22.7 9.5
Information: In 1996, WHO estimated the iodine content in salt at homes as 15 mg/kg, based on RNI of 150 µg/d of adults and 10 g/d salt intake. For factories, a 33% overage was calculated (15 x 1.33 = 20 mg/kg). Notice that this calculations are for averages and not for minimum values.
11
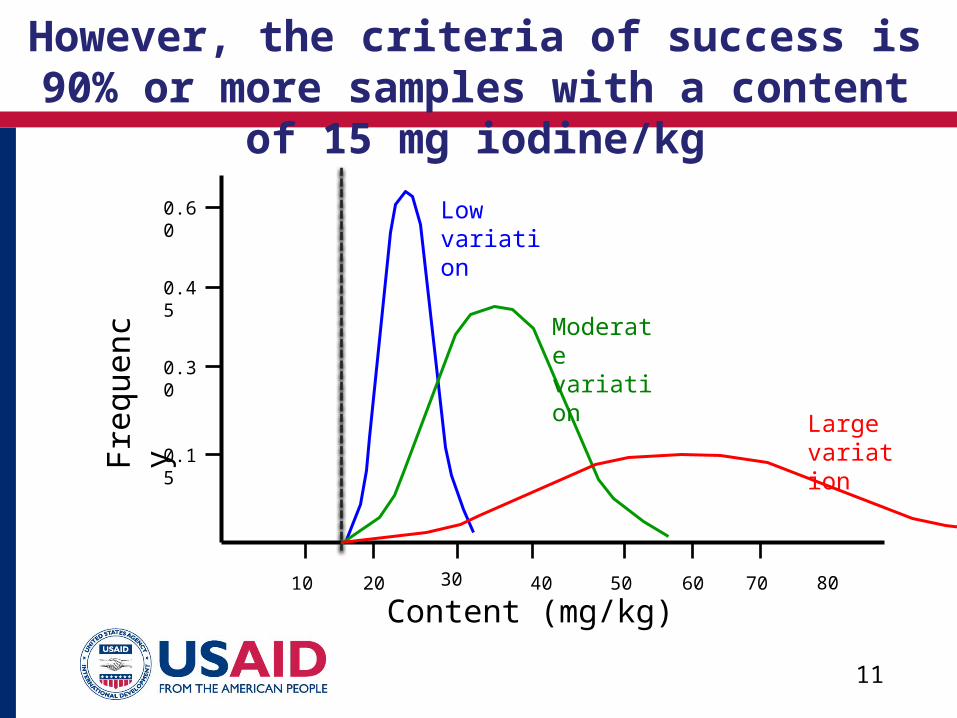
However, the criteria of success is 90% or more samples with a content
of 15 mg iodine/kg
10 40 60
0.15
0.30
0.45
0.60
Content (mg/kg)
Fre
quen
cy
20 50 70 8030
Low variation
Moderate variation
Large variation
12
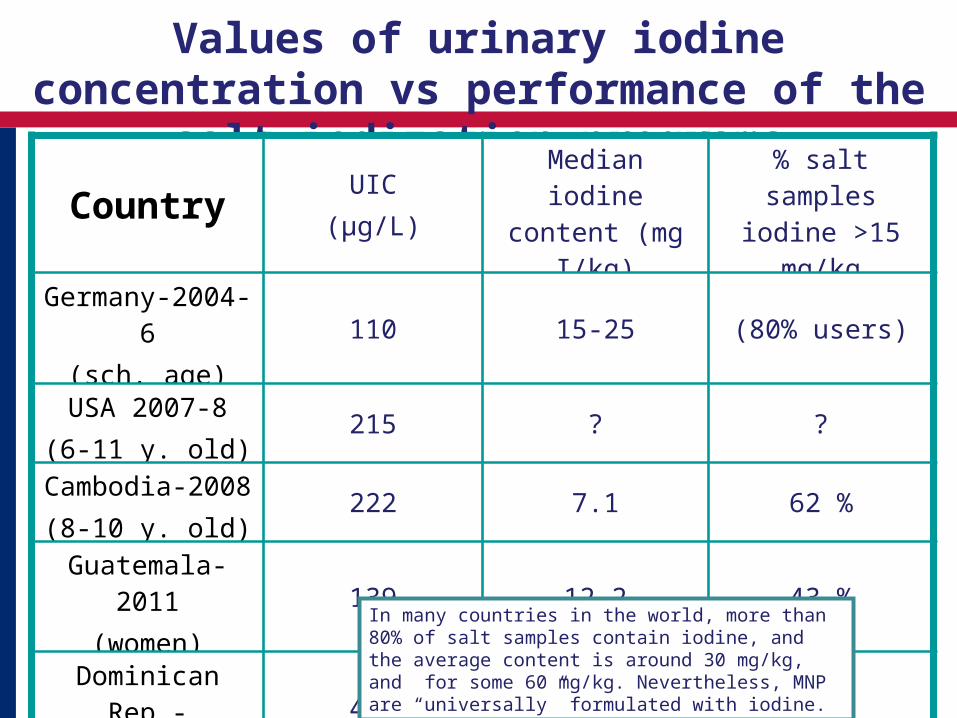
Values of urinary iodine concentration vs performance of the salt iodization
programsCountry
UIC(µg/L)
Median iodine content (mg I/kg)
% salt samples iodine >15 mg/kg
Germany-2004-6(sch. age)
110 15-25 (80% users)
USA 2007-8(6-11 y. old)
215 ? ?
Cambodia-2008(8-10 y. old)
222 7.1 62 %
Guatemala-2011(women)
139 12.2 43 %
Dominican Rep.-15-19 y women
409 21 35 %
In many countries in the world, more than 80% of salt samples contain iodine, and the average content is around 30 mg/kg, and for some 60 mg/kg. Nevertheless, MNP are “universally” formulated with iodine.

13
Source : Menchú et al. (INCAP). Estudio complementario la ENCOVI-2006 de Guatemala; 2013.
Dietary availability of vitamin A, Guatemala-2006
Diet adequacy (density)
Safety of retinol (density)

14
Source : Menchú et al. (INCAP). Estudio complementario la ENCOVI-2006 de Guatemala; 2013.
Total supply vitamin A (diet+fortified sugar 9 mg/kg)
Diet adequacy (density)
Safety of retinol (density)
15
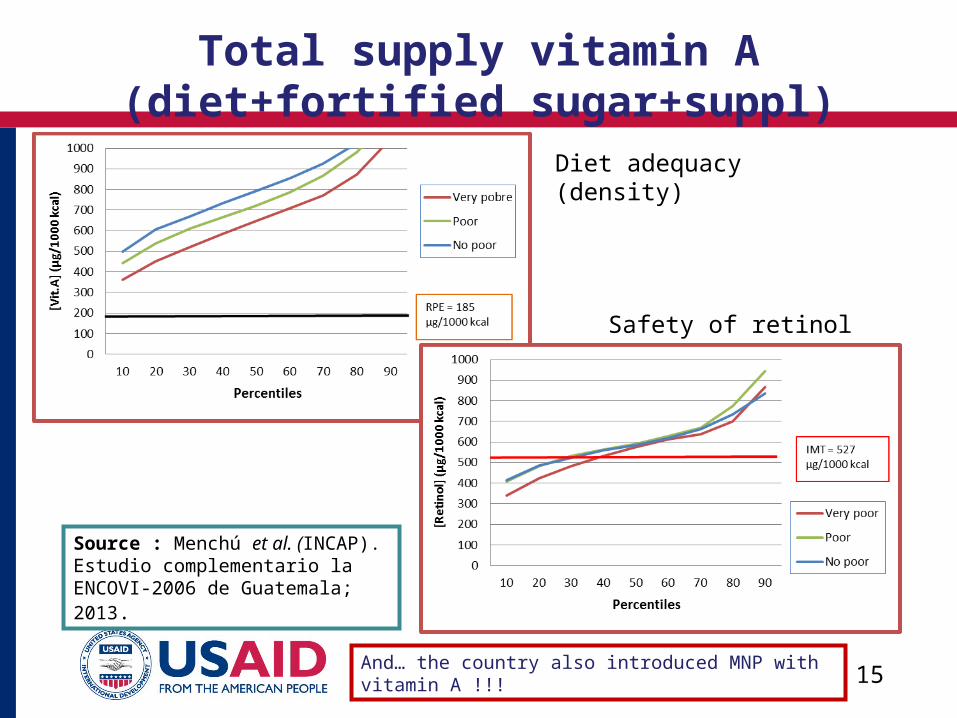
Source : Menchú et al. (INCAP). Estudio complementario la ENCOVI-2006 de Guatemala; 2013.
Total supply vitamin A (diet+fortified sugar+suppl)
Diet adequacy (density)
Safety of retinol (density)
And… the country also introduced MNP with vitamin A !!!
16
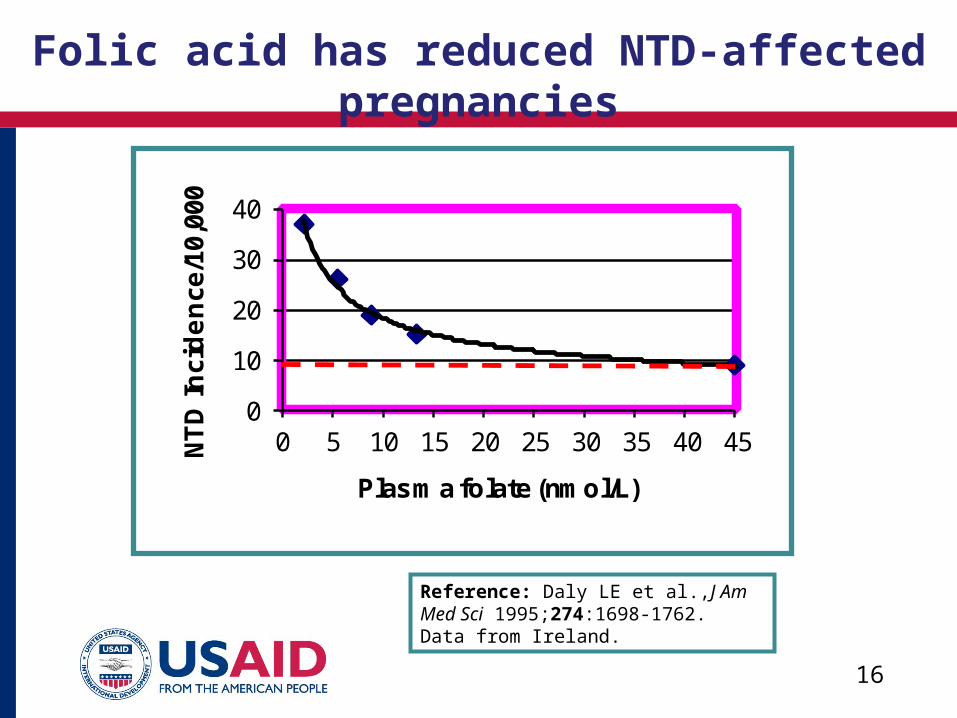
Reference: Daly LE et al.,J Am Med Sci 1995;274:1698-1762. Data from Ireland.
Folic acid has reduced NTD-affected pregnancies
0
10
20
30
40
0 5 10 15 20 25 30 35 40 45NT
D I
nci
de
nce
/10,
000
Plasma folate (nmol/L)
17
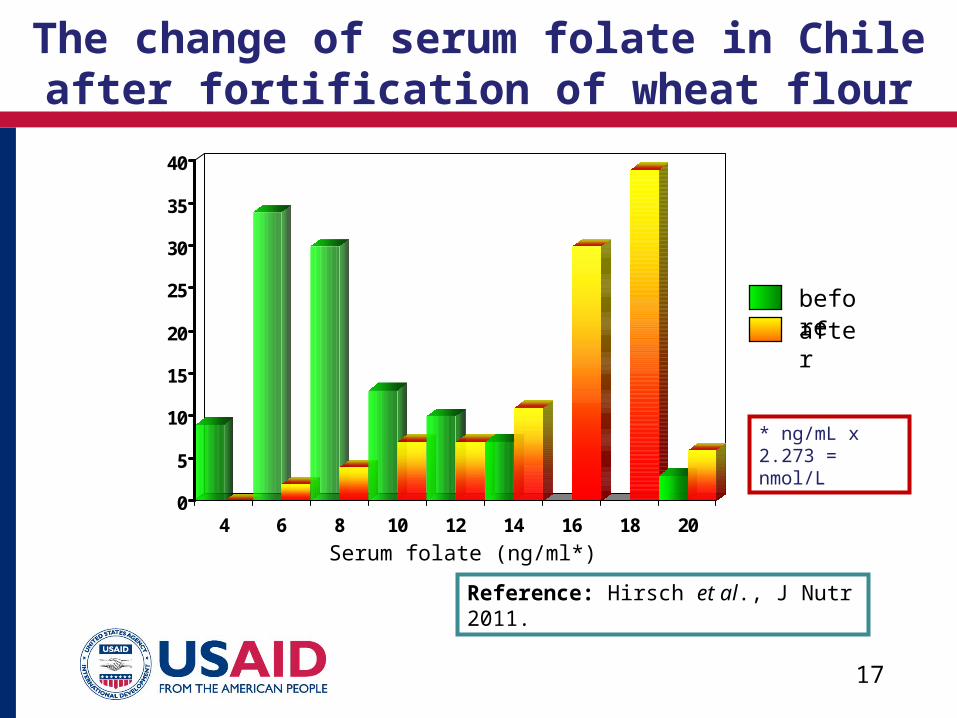
Reference: Hirsch et al., J Nutr 2011.
The change of serum folate in Chile after fortification of wheat flour
0
5
10
15
20
25
30
35
40
4 6 8 10 12 14 16 18 20
beforeafter
Serum folate (ng/ml*)
* ng/mL x 2.273 = nmol/L
18
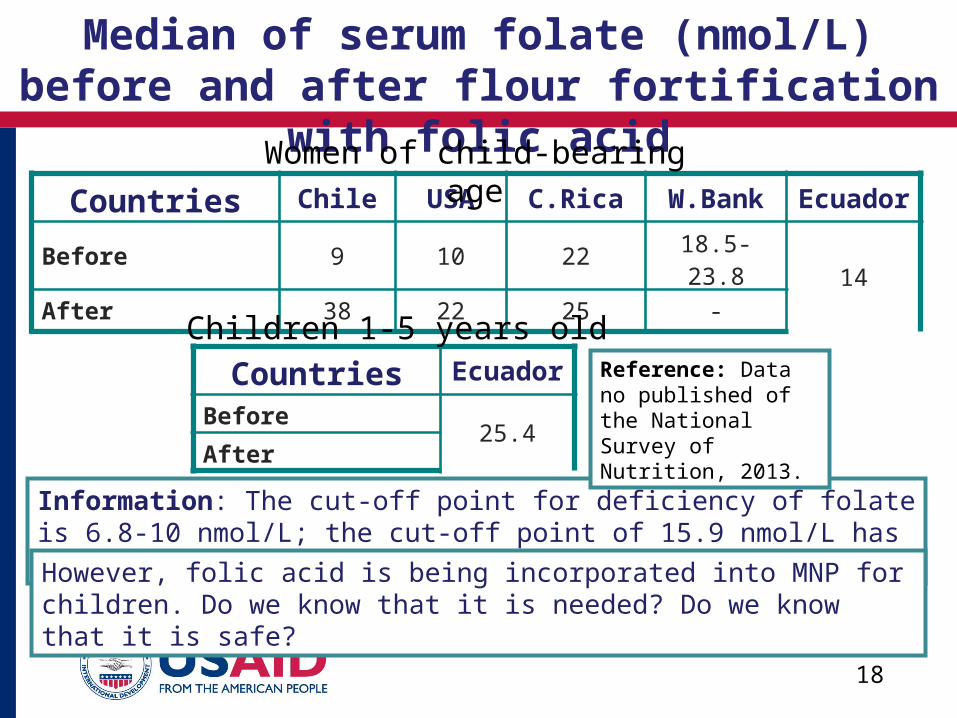
Median of serum folate (nmol/L) before and after flour fortification
with folic acidCountries Chile USA C.Rica W.Bank Ecuador
Before 9 10 22 18.5-23.814
After 38 22 25 -
Information: The cut-off point for deficiency of folate is 6.8-10 nmol/L; the cut-off point of 15.9 nmol/L has been proposed for identifying risk of NTD.
Women of child-bearing age
However, folic acid is being incorporated into MNP for children. Do we know that it is needed? Do we know that it is safe?
Countries Ecuador
Before25.4
After
Children 1-5 years oldReference: Data no published of the National Survey of Nutrition, 2013.
Next Session Room Numbers:
Please fill out an evaluation by going
to this session’s page on your mobile app OR by filling out a paper evaluation in the back of the
room.
Thank you!
Integration of Family Planning Services into MNCH Programming in Liberia 301
The Realities of Integration: NCDs and TB in Ethiopia (Continued) 302
Integrating Family Planning with Obstetric Fistula Services: Achieving Reproductive Intentions 307
Operational Research Training in the 21st Century 308
Constant Contact: Reinforcing Provider Training with Mobile Messages and Supervision in Ghana (Continued) 310
Indoor Residual Spraying: A Weapon in the Fight Against Malaria 311
Increasing District Level, Evidence-Based Decision Making in Cote d'Ivoire 405
Making Every Life Count: Strengthening Civil Registration-Vital Statistics Systems 407
How Strengthening Medicines Regulatory Authorities Can Increase Access to Medicines (Continued) 413
Child TB: No More Crying, No More Dying? 414
Creating the Next Condom: TPPs for Next Generation MPTs Betts Theatre
Sustainable Health Gain from Smart Governance of Hospitals and Health SystemsContinental Ballroom
Gender, Medicines, and the Road to Equity #AreWeThereYet?Grand Ballroom
Top Related