







Languages
Pages
Legal


Appropriate use of cephalosporin; Focusing on
ceftriaxone Apichot So-Ngern B.Sc (Pharm), Mahidol university Certified General Residency in Pharmacotherapy Infectious Disease Fellowship Training in Mahidol University Lecturer at Faculty of Pharmacy, Siam University

• Antibiotics consumption and Resistance • Mechanism of Resistance • Pharmacokinetics and Pharmacodynamics • Drug Use Evaluation of Ceftriaxone Therapeutic uses Dosage and administration; IV compatibility AND
drug interaction
Outlines

Antibiotics consumption and Resistance
Int J Antimicrob Agents. 2005 Dec;26(6):463-72.

Mechanism of Resistance
Int J Med Microbiol. 2010; 300(6): 371-9.
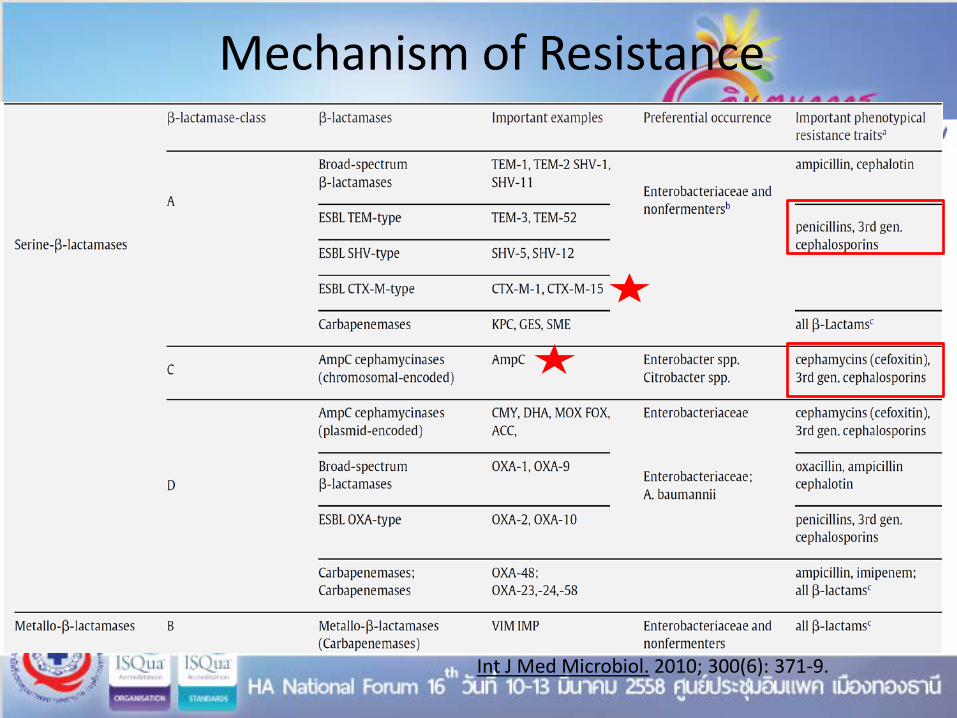
Mechanism of Resistance
Int J Med Microbiol. 2010; 300(6): 371-9.

VERSUS
Appropriate use Inappropriate use

Pharmacodynamics of ceftriaxone
Good activity No activity
Gram positive -Streptococci spp. -Staphylococcus spp. (except MRSA and MRSE) Gram negative
-Enterobacteriaceae (negative for ESBL or AmpC production ) - H.Influenzae - M.catarrhalis - N.gonorrhoeae, N.meningitidis ETC. - Leptospira spp.
Gram positive - Enterococcus spp. - L.monocytogenes Gram negative
- B.pseudomallei - P.aeruginosa (hospital) - A.baumanii (hospital)
Atypical pathogen - Mycoplasma spp., - Chlamydia spp. ETC. - Rickettsia organisms Anaerobe organism
Drugs 2002; 62 (7): 1041-1089 Goodman & Gilman's the pharmacological basis of therapeutics
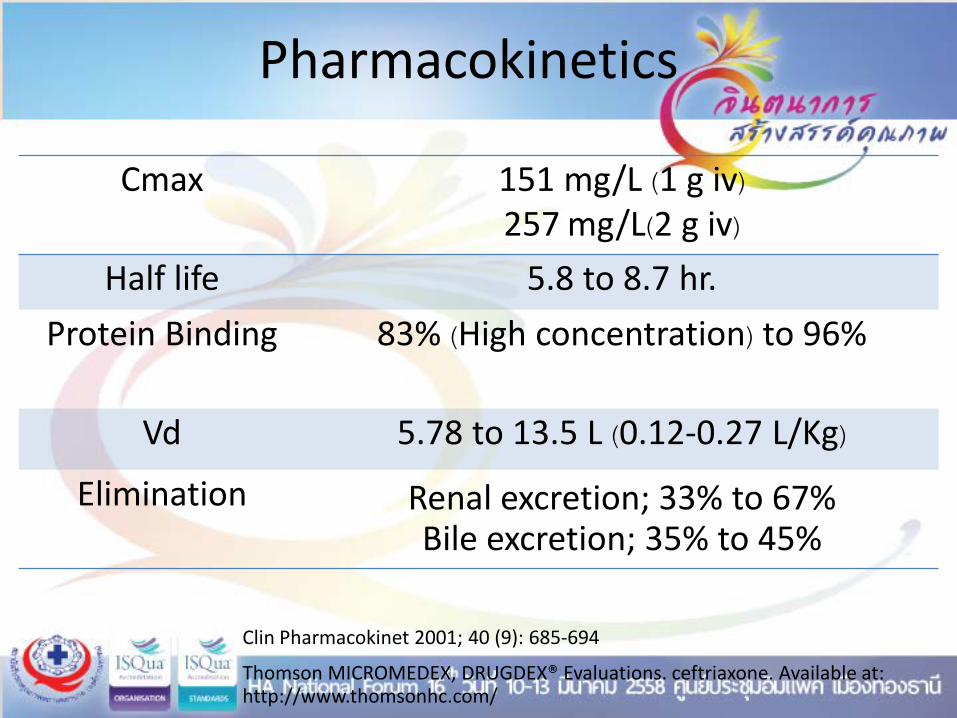
Pharmacokinetics
Cmax 151 mg/L (1 g iv)
257 mg/L(2 g iv)
Half life 5.8 to 8.7 hr. Protein Binding 83% (High concentration) to 96%
Vd 5.78 to 13.5 L (0.12-0.27 L/Kg)
Elimination Renal excretion; 33% to 67% Bile excretion; 35% to 45%
Clin Pharmacokinet 2001; 40 (9): 685-694 Thomson MICROMEDEX, DRUGDEX® Evaluations. ceftriaxone. Available at: http://www.thomsonhc.com/

Drug use evaluations of ceftriaxone

Case study
ผ ปวยชายไทย อาย 37 ป มาโรงพยาบาลดวยอาการดนไปมา ไมพด เรยกไมรสกตว มชกเกรงกระตกทงตว มไข
ประวตกอนมาโรงพยาบาล ผ ปวยบนปวดศรษะมาก อาเจยนพง 1-2 ครง ไมมประวตแพยา ไมมประวตนอนโรงพยาบาลใน 1 ปทผานมา Vital sign: T 38.7 ˚C, P 110/min, RR 20/min, BP 143/96 mmHg PE; Neurological exam; stiff neck positive • CT brain: normal • LP; Open pressure = 38 cmH2O, Closing pressure = 35 cmH2O,
Turbid; WBC =2,880 (%N= 85, %L= 11), protein = 474, sugar=13 (blood sugar =143 mg/dL )
• Culture and identification CSF gram strain: Gram positive cocci in pair Blood gram strain: Negative 2 specimen R/O; Bacterial meningitis Start ceftriaxone 2 g in NSS 100 ml iv q 12 hr.

Drug Use Evaluation of Ceftriaxone; Which Point to Concern
- Indication - Other drugs to treatment - Community acquired infection without risk of
B.pseudomallei and Enterococcus spp. - Severity of disease - Aged > 28 days - Drug interaction especially Calcium inj. - Allergy
- Dosage and administration - Adverse drug reaction
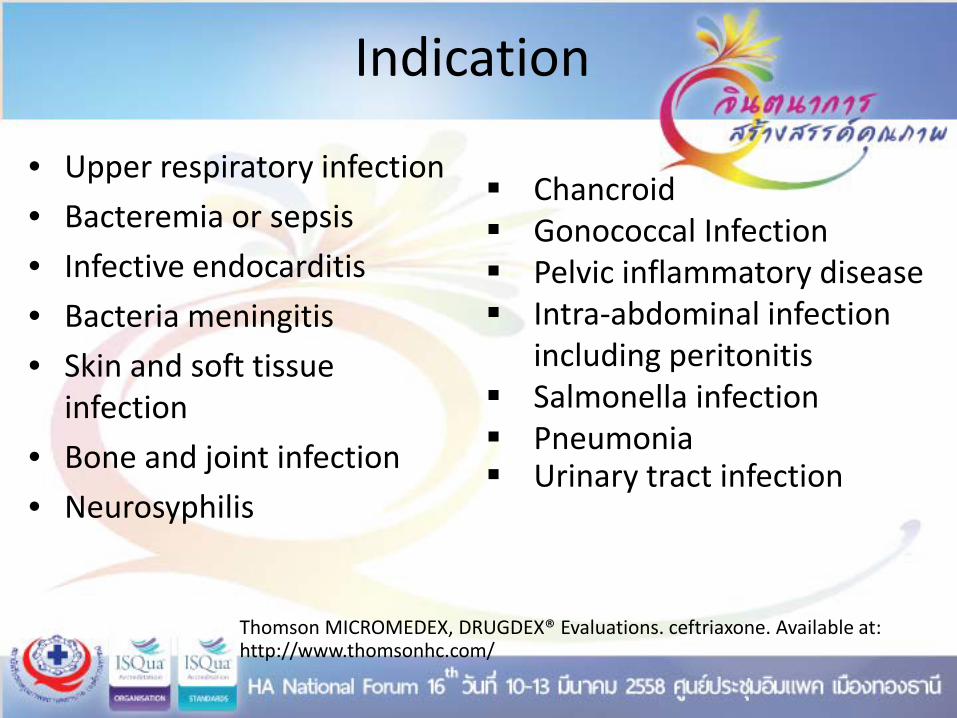
Indication
• Upper respiratory infection • Bacteremia or sepsis • Infective endocarditis • Bacteria meningitis • Skin and soft tissue
infection • Bone and joint infection • Neurosyphilis
Chancroid Gonococcal Infection Pelvic inflammatory disease Intra-abdominal infection
including peritonitis Salmonella infection Pneumonia Urinary tract infection
Thomson MICROMEDEX, DRUGDEX® Evaluations. ceftriaxone. Available at: http://www.thomsonhc.com/

Indication
• Upper respiratory infection • Bacteremia • Sepsis • Infective endocarditis • Bacteria meningitis • Skin and soft tissue
infection • Bone and joint infection • Neurosyphilis
Chancroid Gonococcal Infection Pelvic inflammatory disease Intra-abdominal infection
including peritonitis Salmonella infection Pneumonia (admitted) Urinary tract infection
Thomson MICROMEDEX, DRUGDEX® Evaluations. ceftriaxone. Available at: http://www.thomsonhc.com/

• Empiric therapy for acute bacterial meningitis ในผ ปวยอายมากกวา 1 เดอน
• Empiric therapy for bacterial brain abscess • Empiric therapy for severe community-acquired sepsis
(inflammatory response syndrome plus end organ damage eg. hypoxemia, lactic acidosis, acute renal failure)
• Empiric therapy for community-acquired intra-abdominal infection of mild-to-moderate severity
• Disseminated gonococcal infection, arthritis, pharyngitis, conjunctivitis, ophthalmic neonatorum
• Uncomplicated gonococcal infection of the cervix, urethra and rectum
ขอบงชในการสงยา ceftriaxone และ cefotaxime พฒนาโดย สาขาวชาโรคตดเชอ
ภาควชาอายรศาสตร คณะแพทยศาสตร จฬาลงกรณมหาวทยาลย โรงพยาบาลจฬาลงกรณ

• Empiric therapy for community-acquired pneumonia สาหรบ
ผ ปวยทตองนอนโรงพยาบาล • Empiric therapy for hospital-acquired pneumonia สาหรบผ ปวยท
เปน non-immunocompromised host, ตดเชอภายใน 3-5 วนแรกหลงนอน
โรงพยาบาล (early-onset HAP) • Empiric therapy for community-acquired UTI (ในกรณทมผล Cr >
2 หรอคาดวาเชอกอโรคดอตอยา aminoglycoside )
ขอบงชในการสงยา ceftriaxone และ cefotaxime พฒนาโดย สาขาวชาโรคตดเชอ
ภาควชาอายรศาสตร คณะแพทยศาสตร จฬาลงกรณมหาวทยาลย โรงพยาบาลจฬาลงกรณ

• Empiric therapy for native joint gram-negative arthritis หรอผล gram stain หรอ culture ไมพบเชอกอโรค
• Serious skin and soft-tissue infection, bone infection ทเชอกอโรคเปนเชอกรมลบ
• Gram negative bacteremia จากเชอกอโรคทไวตอยา ceftriaxone หรอ
cefotaxime • Endocarditis ในกรณทเกดจากเชอ gram-negative bacilli eg.
Enterobacteriaceae • Endocarditis ในกรณทเกดจากเชอ streptococci ทตองการรกษาโดยการใหยาฉด IV แบบ
ผ ปวยนอก
• เปลยนจาก antibiotic อนมาใช ceftriaxone หรอ cefotaxime เนองจากผลเพาะเชอได
เชอ...............................ซงไวตอยา ceftriaxone หรอ cefotaxime โดยดอตอ ampicillin และ cefazolin โปรดระบโรคของผ ปวยทใชยาในขอบงชน........................
• แพยา.............................ซงเปน first-line drug ในการรกษาโรคคอ........................................
ขอบงชในการสงยา ceftriaxone และ cefotaxime พฒนาโดย สาขาวชาโรคตดเชอ ภาควชา
อายรศาสตร คณะแพทยศาสตร จฬาลงกรณมหาวทยาลย โรงพยาบาลจฬาลงกรณ

Dosage and administration
IV compatibility AND drug interaction
IV compatibility AND drug interaction
• Do not reconstitute or mix ceftriaxone with a calcium-containing product, such as Ringer’s or Hartmann’s solution or parenteral nutrition containing calcium, or products in the same IV administration line or Y-site, including continuous calcium-containing infusions such as parenteral nutrition
• Concomitant use of ceftriaxone and intravenous calcium-containing products is contraindicated in neonates (<28 days of age).
http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafetyInformationforHeathcareProfessionals/ucm084263.htm
Thomson MICROMEDEX, DRUGDEX® Evaluations. ceftriaxone. Available at: http://www.thomsonhc.com/
IV compatibility AND drug interaction
• In patients >28 days of age, ceftriaxone and calcium-containing products may be administered sequentially, provided the infusion lines are thoroughly flushed between infusions with a compatible fluid.

Case study
• จากนน อก 3 วนหลงจากผ ปวยไดรบยา ceftriaxone 2 gm q 12 hr. ผ ปวยมแนวโนมตอบสนองตอการรกษา มอาการทางคลนกทดขน โดย
• CSF culture: Streptococcus pneumoniae • Penicillin MIC = 0.032 mcg/ml • Cefotaxime MIC = 0.047 mcg/ml • Susceptibility test: S: chloramphenicol ,
Erythromycin, Linezolid, ofloxacin, tetracycline, vancomycin
• R: Trimethoprim/Sulfamethoxazole

Case study • CSF culture: Streptococcus pneumoniae • Penicillin MIC = 0.032 mcg/ml • Cefotaxime MIC = 0.047 mcg/ml • Susceptibility test: S: chloramphenicol ,
Erythromycin, Linezolid, ofloxacin, tetracycline, vancomycin
• R: Trimethoprim/Sulfamethoxazole
De-escalation ?
Documented therapy; S.pneumoniae
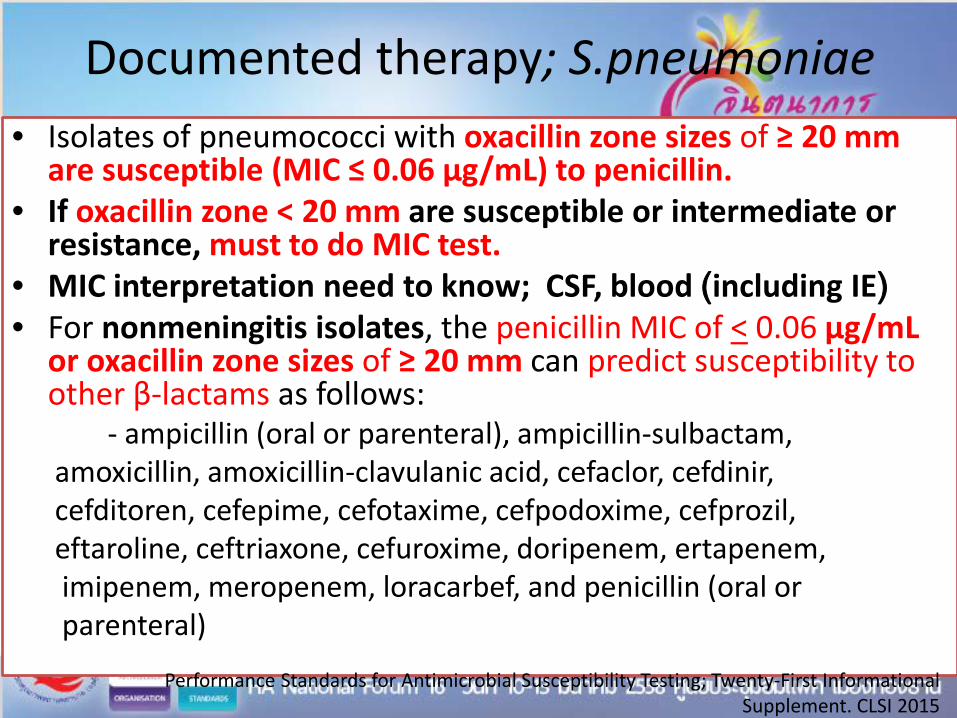
• Isolates of pneumococci with oxacillin zone sizes of ≥ 20 mm are susceptible (MIC ≤ 0.06 μg/mL) to penicillin.
• If oxacillin zone < 20 mm are susceptible or intermediate or resistance, must to do MIC test.
• MIC interpretation need to know; CSF, blood (including IE) • For nonmeningitis isolates, the penicillin MIC of < 0.06 μg/mL
or oxacillin zone sizes of ≥ 20 mm can predict susceptibility to other β-lactams as follows:
- ampicillin (oral or parenteral), ampicillin-sulbactam, amoxicillin, amoxicillin-clavulanic acid, cefaclor, cefdinir, cefditoren, cefepime, cefotaxime, cefpodoxime, cefprozil, eftaroline, ceftriaxone, cefuroxime, doripenem, ertapenem, imipenem, meropenem, loracarbef, and penicillin (oral or parenteral)
Performance Standards for Antimicrobial Susceptibility Testing; Twenty-First Informational Supplement. CLSI 2015
Documented therapy; S.pneumoniae
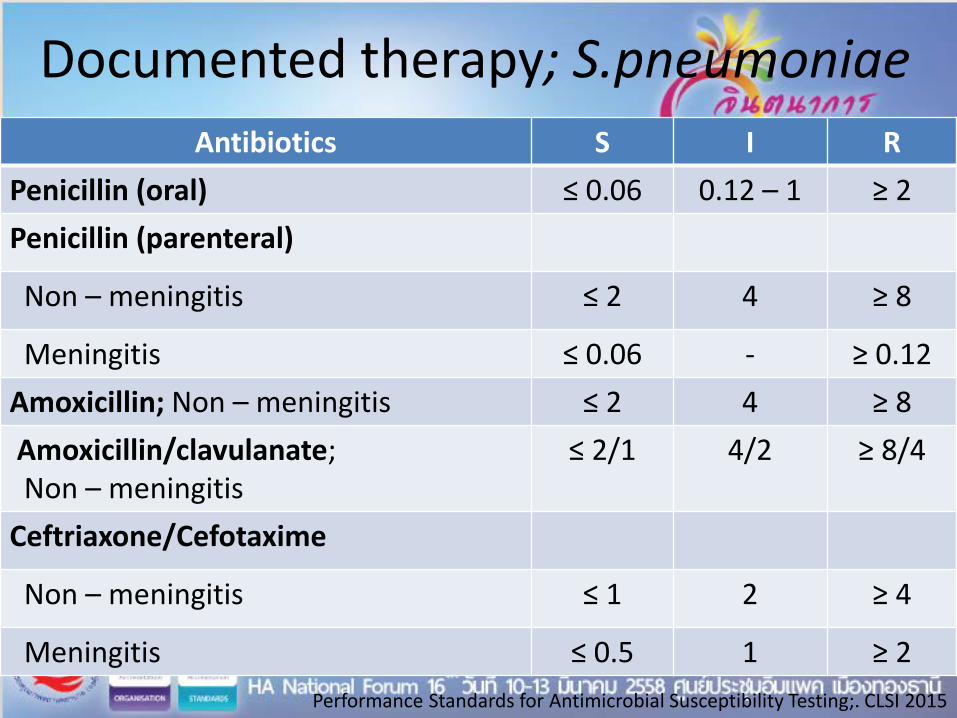
Antibiotics S I R Penicillin (oral) ≤ 0.06 0.12 – 1 ≥ 2 Penicillin (parenteral)
Non – meningitis ≤ 2 4 ≥ 8
Meningitis ≤ 0.06 - ≥ 0.12 Amoxicillin; Non – meningitis ≤ 2 4 ≥ 8 Amoxicillin/clavulanate; Non – meningitis
≤ 2/1 4/2 ≥ 8/4
Ceftriaxone/Cefotaxime
Non – meningitis ≤ 1 2 ≥ 4
Meningitis ≤ 0.5 1 ≥ 2 Performance Standards for Antimicrobial Susceptibility Testing;. CLSI 2015

Documented therapy; S.pneumoniae
Antibiotics S I R Penicillin (oral) ≤ 0.06 0.12 – 1 ≥ 2 Penicillin (parenteral)
Non – meningitis ≤ 2 4 ≥ 8
Meningitis ≤ 0.06 - ≥ 0.12 Amoxicillin; Non – meningitis ≤ 2 4 ≥ 8 Amoxicillin/clavulanate; Non – meningitis
≤ 2/1 4/2 ≥ 8/4
Ceftriaxone/Cefotaxime
Non – meningitis ≤ 1 2 ≥ 4
Meningitis ≤ 0.5 1 ≥ 2 Performance Standards for Antimicrobial Susceptibility Testing;. CLSI 2015
Penicillin MIC = 0.032 mcg/ml Cefotaxime MIC = 0.047 mcg/ml
Case study
• ผ ปวยไดรบการเปลยนการรกษาเปนยา Penicillin G 24 million units/day IV, in divided doses every 4 hours จนครบ 14 วน จากนน จาหนายออกจากโรงพยาบาล

Take home message
• Ceftriaxone has good activity to community pathogen except B.pseudomallei and Enterococcus spp.)
• Almost patients have serious and/or moderate to
severe infection need to be received empirical therapy by ceftriaxone (except severe community-acquired intra-abdominal infection)
• Susceptibility reported De-escalation
Top Related