







Languages
Pages
Legal

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
1
Application for inclusion of ledipasvir/sofosbuvir (Harvoni®) tablets on the WHO Model List
of Essential Medicines
Submitted by
Gilead Sciences Inc.
November 28, 2014
Gilead Sciences Inc.
333 Lakeside Drive
Foster City
California 94404
USA
Gilead Submission Reference number:
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
2
Contents
1. Summary statement of the proposal for inclusion .................................................... 5
2. Name of the focal point in WHO submitting or supporting the application .................. 8
3. Name of the organization(s) consulted and/or supporting the application .................. 8
4. International Nonproprietary Name (INN, generic name) of the medicine .................. 8
5. Formulation proposed for inclusion ........................................................................ 8
6. International availability ...................................................................................... 10
7. Listing type requested ........................................................................................ 12
8. Information supporting the public health relevance ................................................ 12
8.1 Epidemiological information on disease burden ........................................... 12
8.2 Assessment of current use ........................................................................ 15
8.3 Target population ..................................................................................... 18
9. Treatment details ............................................................................................... 18
9.1 Indications and usage ............................................................................... 18
9.2 Dosage and administration ........................................................................ 18
9.2.1 Special populations ............................................................................ 19
9.3 Duration .................................................................................................. 20
9.4 Reference to existing WHO and other clinical guidelines .............................. 20
9.5 Special requirements ................................................................................ 21
10. Summary of comparative effectiveness in a variety of clinical settings ............. 22
10.1 Identification of clinical evidence ................................................................ 22
10.2 Summary of available data on comparative effectiveness of Harvoni® ........... 22
10.2.1 Summary of the Phase 2 clinical trial program for Harvoni® .................... 23
10.2.2 Background and design of the Phase 3 studies of Harvoni®
in HCV GT 1 ...................................................................................... 29

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
3
10.2.3 Results of the Phase 3 registration studies of Harvoni® in mono-infected
patients with HCV GT 1 ...................................................................... 31
10.2.4 Virologic failure and resistance analysis in the clinical studies ................ 40
10.2.5 Results of the Phase 3 studies of Harvoni® in patients with traditionally
hard-to-treat baseline characteristics ................................................... 46
10.2.6 Results of the studies of Harvoni® in patients with genotypes
other than GT 1 ................................................................................. 50
10.2.7 Impact of Harvoni® on patient health-related quality of life ...................... 51
10.2.8 Effect of Harvoni® therapy on long-term patient outcomes ..................... 52
10.3 Summary of available estimates of comparative effectiveness ...................... 53
11. Summary of comparative evidence on safety ................................................. 55
11.1 Estimate of total patient exposure to Harvoni® ............................................... 56
11.2 Description of adverse effects/reactions ..................................................... 57
11.2.1 Treatment-emergent adverse events in patients with HCV GT 1 ............. 57
11.2.2 Safety of Harvoni® in patients with HCV GT 1 and cirrhosis ................... 63
11.2.3 Safety of Harvoni® in patients with HIV/HCV co-infection ....................... 64
11.2.4 Safety of Harvoni® in patients with HCV GT 2, 3, 4, 5 and 6 infection ...... 65
11.2.5 Drug interactions ............................................................................... 66
11.3 Summary of comparative safety ................................................................... 70
12. Summary of available data on comparative cost and cost-effectiveness
within the pharmacologic class or therapeutic group ...................................... 72
12.1 Range of costs of the proposed medicine ................................................... 72
12.1.1 USA ................................................................................................. 72
12.1.2 Developing countries .......................................................................... 72
12.2 Cost-effectiveness of medicines for HCV ...................................................... 73
13. Summary of regulatory status of the medicine ................................................ 76

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
4
14. Availability of pharmacopoeial standards ....................................................... 76
14.1 Specifications of Harvoni® tablets............................................................... 76
15. Proposed (new/adapted) text for the WHO Model Formulary ........................... 78
15.1 Other antivirals ......................................................................................... 78
16. References ................................................................................................. 79
Appendix 1. Harvoni® Access PI ............................................................................. 88
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
5
1. Summary statement of the proposal for inclusion
Harvoni® (ledipasvir/sofosbuvir 90 mg/400 mg) is a once-daily, fixed-dose combination
tablet for oral administration for the treatment of hepatitis C virus (HCV). Harvoni®
contains ledipasvir (LDV), an HCV NS5A inhibitor, and sofosbuvir (SOF), a nucleotide
analog inhibitor of HCV NS5B polymerase. It is proposed for inclusion in the WHO Model
List of Essential Medicines as a treatment for chronic HCV infection in adult patients
(≥18 years).
The use of Harvoni® is based primarily on efficacy and safety data from three published
open-label Phase 3 studies, ION-1, ION-2 and ION-3. The ION studies evaluated
Harvoni® in 1952 patients with HCV genotype (GT) 1 and compensated liver disease,
and comprised one study in non-cirrhotic, treatment-naïve patients (ION-3), one study in
cirrhotic and non-cirrhotic treatment-naïve patients (ION-1), and one study in cirrhotic
and non-cirrhotic patients who had failed prior therapy with an interferon (IFN)-based
regimen, including regimens containing an HCV protease inhibitor (PI; ION-2). In
addition, a Phase 3 Japanese study evaluated Harvoni®, with or without ribavirin (RBV),
in 341 treatment-naïve and treatment-experienced patients with HCV GT 1.
The principal reasons for requesting inclusion in the World Health Organization (WHO)
Model List of Essential Medicines are as follows:
• Infection with HCV imposes a significant global burden, with wide-ranging personal,
societal and economic effects [WGO Guidelines, 2013]
o Up to 85% of patients infected with HCV develop chronic infection, placing
them at risk of serious sequelae, including liver fibrosis, cirrhosis,
hepatocellular carcinoma (HCC) and death [Chen and Morgan, 2006]
o Chronic HCV infection is associated with increased morbidity and mortality
from extrahepatic manifestations, including circulatory diseases, renal
diseases, autoimmune disorders, cutaneous manifestations and non-liver
cancers [Himoto et al, 2012; Lee et al, 2012]
o Chronic HCV infection significantly affects patients’ quality of life (QoL) and
ability to work, and confers high medical costs, which rise with increasing
disease severity [Vietri et al, 2013]

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
6
o Whilst the incidence of new HCV infections has fallen in many countries
following the introduction of blood product screening [CDC, 2011; EASL,
2014a], the substantial burden of chronic HCV infection is growing, as
individuals who contracted HCV in the past begin to develop long-term
complications [Davis et al, 2010; Razavi et al, 2013]
• Until recently, the standard of care for patients with chronic HCV infection consisted
of long-duration treatment regimens based on pegylated interferon (PEG-IFN) plus
RBV, with the addition of a direct-acting antiviral agent (DAA) of the PI class in
patients with HCV GT 1 [EASL, 2014a]. Such regimens are limited by the inability or
unwillingness of patients to tolerate long-duration IFN-based regimens (up to
48 weeks); medical ineligibilities to PEG-IFN + RBV (e.g. psychiatric disorders,
co-morbidities, substance use disorders); and other barriers to IFN-based treatment
(e.g. intolerance, fear of known side effects, needle phobia and contraindications due
to drug–drug interactions with other medications) [North et al, 2013]
• The recent approval of SOF (Sovaldi®; Sovaldi US PI, 2014), and its
recommendation as the backbone of the new standard of care for HCV infection
[EASL, 2014b], has improved treatment options for patients with chronic HCV
infection and offers a number of potential benefits [Jacobson et al, 2013; Lawitz et al,
2013; Afdhal et al, 2014a; WHO Guidelines, 2014; Zeuzem et al, 2014; Data on file –
Gilead Sciences EAME – (HCV1300034); Data on file – Gilead Sciences EAME –
(HCV1300042); Data on file – Gilead Sciences EAME – (HCV1300053)]:
o High rates of sustained virologic response (SVR) in treatment-naïve and
treatment-experienced patients
o Pangenotypic activity with efficacy across HCV GT 1–6
o Efficacy in patients unwilling or unable to tolerate IFN-based therapy
o Shorter duration of treatment where combination therapy including IFN is
required for optimum efficacy (e.g. those with GT 1)
o Efficacy in difficult-to-treat patients, including those with cirrhosis, human
immunodeficiency virus (HIV) co-infection and HCC awaiting liver
transplantation
o Favorable safety and tolerability profiles across all genotypes in patients with
and without cirrhosis

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
7
o High barrier to resistance
• As part of its ongoing clinical development program, SOF has been investigated in
combination with LDV, with or without RBV, to address the need for an all-oral
treatment option with a short and simple regimen that would eliminate the toxicity,
tolerability issues and contraindications associated with the use of IFN- or
RBV-based regimens. LDV and SOF (LDV/SOF) have been co-formulated as the
once-daily, oral fixed-dose single tablet regimen (STR), Harvoni®.
• A series of clinical trials have established the efficacy, tolerability and safety of
Harvoni® in treatment-naïve and treatment-experienced HCV GT 1 patients with
8–12 weeks of therapy. Exclusion of RBV from the regimen maintained efficacy and
substantially reduced the incidences of adverse events (AEs) and laboratory
abnormalities experienced by patients. In patients with compensated cirrhosis,
Harvoni® for 24 weeks or Harvoni® + RBV for 12 weeks also resulted in high rates of
response, with the shorter-duration regimen being a considerable treatment advance
in this group of patients. It is noteworthy that Harvoni® has been associated with a
low incidence of drug–drug interactions (DDIs), compared with other DAAs, and has
been studied in patients receiving a number of immunosuppressant drugs or
antiretroviral therapy (ART), supporting its use in traditionally hard-to-treat patient
populations, including those receiving concomitant therapies for complex comorbid
conditions, such as HIV. Finally, data have shown that Harvoni® is effective in
patients with resistance-associated variants (RAVs), with a high proportion of
patients with baseline RAVs and PI-resistant mutations achieving SVR [Lawitz et al,
2014; Afdhal et al. 2014b and 2014c; Kowdley et al, 2014; Data on file – Gilead
Sciences EAME – (HCV1300044); Data on file – Gilead Sciences EAME –
(HCV1300045); Data on file – Gilead Sciences EAME – (HCV1300046); Data on file
– Gilead Sciences EAME – (HCV1300047); Data on file – Gilead Sciences EAME –
(HCV1300049); Data on file – Gilead Sciences EAME – (HCV1300050); Data on file
– Gilead Sciences EAME – (HCV1300057); Data on file – Gilead Sciences EAME –
(HCV13000103); Data on file – Gilead Sciences EAME – (HCV1300074); Data on
file – Gilead Sciences EAME – (HCV13000119)].
• Harvoni® builds on the proven efficacy of SOF to offer a high chance of cure to a
wide range of patients, including those with traditionally difficult-to-treat disease, with
a short-duration, mostly IFN- and RBV-free regimen.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
8
2. Name of the focal point in WHO submitting or supporting the application
Stefan Wiktor, 20 Avenue Appia, 1211 Geneva, 27-Switzerland.
3. Name of the organization(s) consulted and/or supporting the application
World Health Alliance.
4. International Nonproprietary Name (INN, generic name) of the medicine
Ledipasvir and sofosbuvir.
5. Formulation proposed for inclusion
Harvoni® is a two-drug fixed-dose combination medication that contains 90 mg of LDV
and 400 mg of SOF in a single tablet. The recommended dosage of Harvoni® is one
tablet taken orally once daily with or without food. It is available as an orange,
diamond-shaped, film-coated tablet of dimensions 19 mm x 10 mm, debossed with ‘GSI’
on one side and ‘7985’ on the other side [Harvoni® US PI, 2014; Harvoni® SmPC, 2014].
An alternative white, film-coated tablet presentation is also available, which differs only
from the aforementioned tablet formulation in the color of the film coat applied.
The tablets are packaged in 100 mL, white, high-density polyethylene bottles containing
one gram of silica gel desiccant and a polyester fiber coil. Each bottle contains
28 tablets and is capped using a white, continuous thread, child-resistant polypropylene
screw cap with an induction-sealed, aluminum-faced liner [Harvoni® US PI, 2014].
The qualitative and quantitative composition of Harvoni® tablets is provided in Table 1.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
9
Table 1. Qualitative composition of Harvoni® (LDV/SOF) tablets
Tablet core
Colloidal silicon dioxide (E551)
Copovidone (E1201)
Croscarmellose sodium (E468)
Lactose monohydrate
Magnesium stearate (E470b)
Microcrystalline cellulose (E460[i])
Film coating (orange film coat)
FD&C yellow 6/sunset yellow FCF aluminium lake (E110)
Polyethylene glycol (E1521)
Polyvinyl alcohol (E1203)
Talc (E553b)
Titanium dioxide (E171)
Film coating (white film coat)
Polyethylene glycol (E1521)
Polyvinyl alcohol (E1203)
Talc (E553b)
Titanium dioxide (E171)
Harvoni® is indicated for use in adult patients (≥18 years). Harvoni® is not presently
recommended for patients aged <18 years because its safety and efficacy in children
and adolescents have not yet been established [Harvoni® US PI, 2014]. Thus, no
pediatric formulation is proposed for inclusion and its potential for use in this patient
population will not be discussed further in this application.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
10
6. International availability
Harvoni® is a registered trademark of Gilead Sciences, Inc, or its related companies in
the USA and other countries.
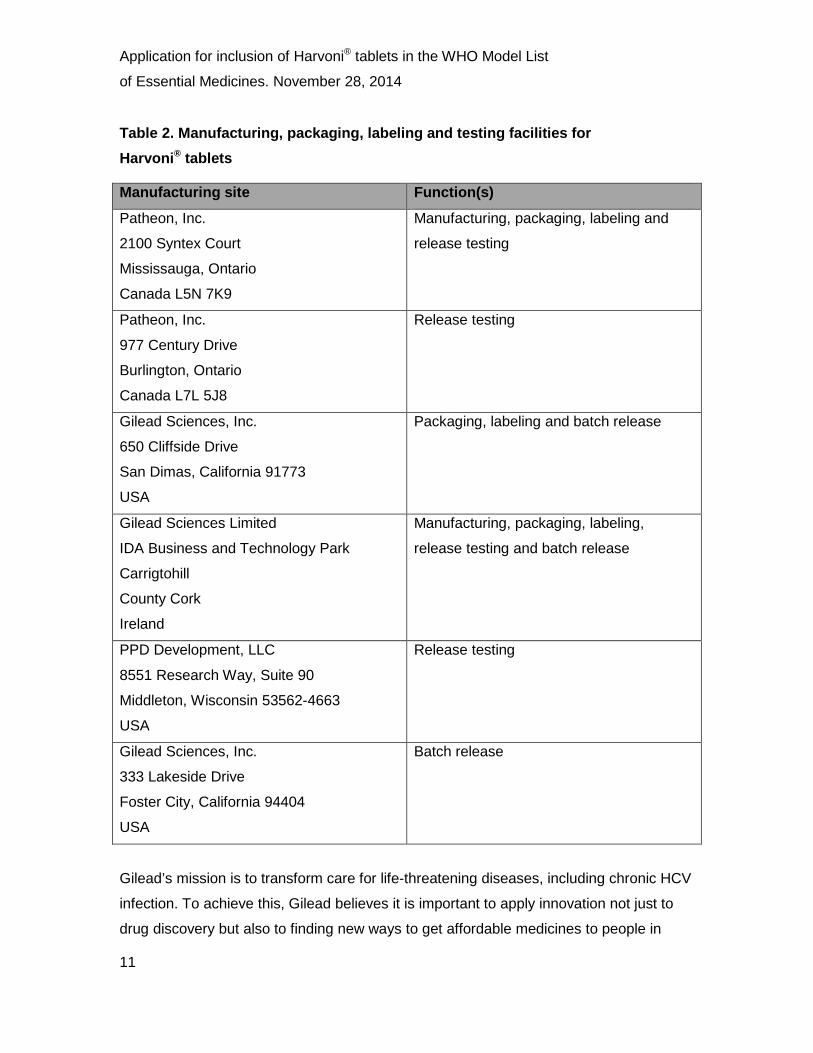
Harvoni® tablets are currently manufactured, packaged, labeled and tested for Gilead
Sciences, Inc. at the facilities listed in Table 2. All of the sites are currently approved and
listed in the US New Drug Application (NDA). The manufacturing steps conducted at all
facilities are in compliance with European Union (EU) and US Food and Drug
Administration (FDA) Good Manufacturing Practice (GMP) guidelines.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
11
Table 2. Manufacturing, packaging, labeling and testing facilities for Harvoni® tablets
Manufacturing site Function(s)
Patheon, Inc.
2100 Syntex Court
Mississauga, Ontario
Canada L5N 7K9
Manufacturing, packaging, labeling and
release testing
Patheon, Inc.
977 Century Drive
Burlington, Ontario
Canada L7L 5J8
Release testing
Gilead Sciences, Inc.
650 Cliffside Drive
San Dimas, California 91773
USA
Packaging, labeling and batch release
Gilead Sciences Limited
IDA Business and Technology Park
Carrigtohill
County Cork
Ireland
Manufacturing, packaging, labeling,
release testing and batch release
PPD Development, LLC
8551 Research Way, Suite 90
Middleton, Wisconsin 53562-4663
USA
Release testing
Gilead Sciences, Inc.
333 Lakeside Drive
Foster City, California 94404
USA
Batch release
Gilead’s mission is to transform care for life-threatening diseases, including chronic HCV
infection. To achieve this, Gilead believes it is important to apply innovation not just to
drug discovery but also to finding new ways to get affordable medicines to people in

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
12
need as quickly as possible. Gilead’s model for Harvoni® is based on its HIV treatment
provision in developing countries, which has evolved over time, in response to lessons
learned, stakeholder feedback and evidence of program effectiveness. Gilead learned
early about the importance of partnership and collaboration for increasing drug access.
Today, Gilead works with more than 70 manufacturers, regional and local distributors,
and generic licensees to expand access to marketed medicines and to plan for future
access to pipeline products (see Section 12).
7. Listing type requested
Listing is requested on the Model List of Essential Medicines as an example of the
therapeutic class of DAAs for HCV infection.
8. Information supporting the public health relevance
8.1 Epidemiological information on disease burden
Following its isolation and identification in 1989, HCV infection has been recognized
as a major cause of chronic liver disease worldwide. Estimates suggest that more than
185 million people (approximately 3% of the global population) are infected with HCV,
the majority of whom live in resource-limited settings [Mohd Hanafiah et al, 2013].
Egypt is believed to have the highest prevalence rate in the world with more than 15% of
the population infected [Sievert et al, 2011], while Africa has the highest WHO estimated
regional HCV prevalence at 5.3% [Karoney and Siika, 2013]. Each year, 3–4 million
more people become infected with HCV and more than 350,000 die from liver-related
diseases such as liver cirrhosis and HCC [WHO Fact Sheet, July 2013].
HCV is a blood-borne infection; the majority of HCV transmission in the developing world
is associated with unsafe injection practices and poor infection control. In many
resource-limited countries, the reuse of syringes and use of contaminated medical
equipment without proper sterilization are common and known risk factors for HCV
transmission [WGO Guidelines, 2013], together with the widespread use of unscreened
blood for transfusions [Hauri et al, 2004]. Lack of access to sterile injection equipment
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
13
continues to fuel the HCV epidemic in many countries, notably Pakistan, where
transmission is also influenced by community-related activities, such as traditional
healers, unqualified medical providers, tattoo parlors and barber shops [Qureshi et al,
2010; Sievert et al, 2011]. While people who inject drugs (PWID) remain the primary
route by which HCV infection is transmitted in developed countries, injection drug use is
also becoming an increasingly important risk factor for HCV transmission in developing
countries [Nelson et al, 2011]. Globally, China has the highest estimated number of
HCV-infected PWID but prevalence is also high in Mexico, Pakistan and Thailand where
more than 80% of PWID are HCV antibody-positive [Nelson et al, 2011].
A small proportion of newly infected patients will clear the virus spontaneously and do
not require treatment; however, up to 85% of acute cases become chronic and, if left
untreated, about 60–70% go on to develop chronic liver disease: approximately 5–20%
develop cirrhosis and 1–5% die from cirrhosis or HCC. HCV infection is the underlying
cause of liver cancer in approximately 25% of patients [WHO Fact Sheet, July 2013]
and, as more than 80% of HCC cases occur in sub-Saharan Africa and the Far East,
notably China [Villar et al, 2012], infection with HCV is an important driver of morbidity
and mortality in many medium- to low-resource settings.
As HIV and HCV share common routes of parenteral transmission, HIV/HCV co-infection
is relatively common, with estimates suggesting that, of the 34 million persons infected
with HIV worldwide, up to 30% are concurrently infected with HCV [UNAIDS, 2012;
Price and Thio, 2010].
Prevalence is highest in sub-Saharan Africa, where more than two-thirds of all those
infected with HIV live today [WHO Fact Sheet, June 2013]. Co-infection with HIV is
associated with persistent HCV viremia and higher HCV viral load, leading to
accelerated progression of liver disease and increased mortality among HCV-infected
patients [Mohsen et al, 2002; Operskalski and Kovacs, 2011]. HIV may also increase the
risk of mother-to-child transmission of HCV [Gibb et al, 2000]. The early use of ART
among HIV/HCV co-infected individuals has been shown to slow the progression of liver
disease and improve health outcomes [Averhoff et al, 2012].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
14
In contrast to HIV, for which infected patients require lifelong therapy, HCV is a curable
viral infection. However, because acute HCV infection is generally asymptomatic, most
individuals living with HCV infection are unaware that they are infected and, as a result,
do not receive appropriate drug therapy early in the course of infection. Such patients
are at risk of HCV-associated complications, including cirrhosis and HCC [Averhoff et al,
2012]. In addition, HCV-infected persons can serve as a reservoir for ongoing HCV
transmission within the community; therefore, antiviral treatment is a vital measure in
disease prevention to reduce the number of infected individuals.
Significant barriers exist in many low-resource countries that inhibit the widening of
access to screening and treatment for HCV infection. However, awareness is growing in
many parts of the developing world relating to the importance of managing HCV and
chronic HCV infection. In 2010, the World Health Assembly urged its Member States
“to support or enable an integrated and cost-effective approach to the prevention, control
and management of viral hepatitis considering the linkages with associated co-infection
such as HIV, as well as to collaborate with other organizations in the United Nations
system, partners, international organizations and other relevant stakeholders in
enhancing access to affordable treatments in developing countries” [World Health
Assembly, 2010].
These sentiments coincide with the advent of DAAs for the treatment of HCV. These
agents have the potential to revolutionize the management of HCV, addressing concerns
that treatment success rates with PEG-IFN/RBV are too low and that treatment is too
complex and produces troublesome side effects [Cooper et al, 2009], while outcomes in
patients with HIV/HCV co-infection are poor [Operskalski and Kovacs, 2011]. A 2012
systematic review and meta-analysis of treatment outcomes in a large number of
HCV-infected patients in low- and middle-income countries showed that rates of
treatment success with PEG-IFN/RBV were similar to those reported in high-income
countries. The meta-analysis also suggested that the availability of new DAAs “will be
particularly useful in resource-limited settings where the disease burden is greatest”
[Ford et al, 2012].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
15
Evidence that HCV-infected persons in resource-limited settings have treatment success
rates similar to those in developed countries provides a solid foundation for increasing
efforts to improve access to HCV treatment in low- and middle-income countries, as well
as providing a rationale for the inclusion of Harvoni® on the WHO Model List of Essential
Medicines.
8.2 Assessment of current use
In the USA, Harvoni® is indicated for use as a treatment for chronic HCV GT 1 infection
in adult patients (≥18 years), as illustrated in Table 3; Harvoni® is not presently
recommended for patients aged <18 years because its safety and efficacy in children
and adolescents (<18 years) have not yet been established [Harvoni® US PI, 2014].
In Europe, Harvoni® is also indicated for the treatment of chronic HCV GT 4 infection
and some GT 3 adult patients (Table 4) [Harvoni® SmPC, 2014; Gilead Press Release,
2014]. Countries in which Harvoni® is currently licensed for use are detailed in
Section 13.
Table 3. Recommended treatment duration for Harvoni® in patients with chronic HCV GT 1 infection [Harvoni® US PI, 2014]
Patient population Duration
Treatment-naïve patients with or without cirrhosis 12 weeks*
Treatment-experienced patients** without cirrhosis 12 weeks
Treatment-experienced patients** with cirrhosis 24 weeks *Harvoni® for 8 weeks can be considered in treatment-naïve patients without cirrhosis who have
pre-treatment HCV RNA of <6 million IU/mL
**Treatment-experienced patients who have failed treatment with either PEG-IFN and RBV
or an HCV PI + PEG-IFN + RBV
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
16
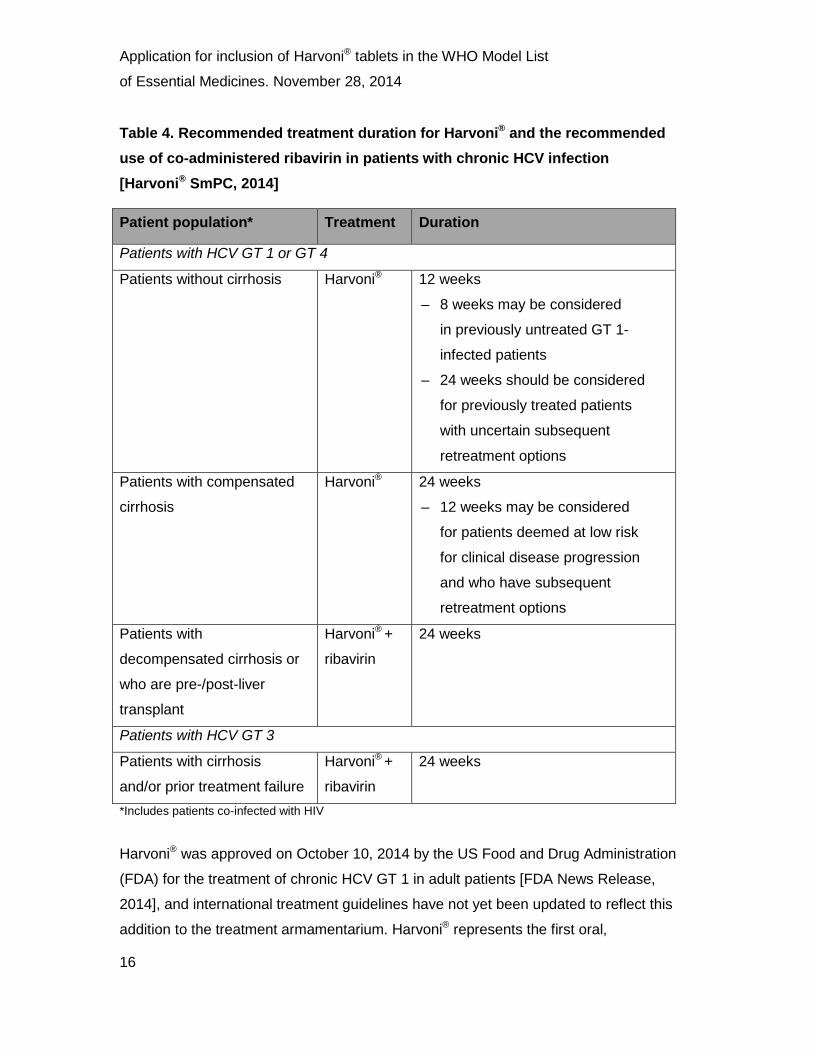
Table 4. Recommended treatment duration for Harvoni® and the recommended use of co-administered ribavirin in patients with chronic HCV infection [Harvoni® SmPC, 2014]
Patient population* Treatment Duration
Patients with HCV GT 1 or GT 4
Patients without cirrhosis Harvoni® 12 weeks
– 8 weeks may be considered
in previously untreated GT 1-
infected patients
– 24 weeks should be considered
for previously treated patients
with uncertain subsequent
retreatment options
Patients with compensated
cirrhosis
Harvoni® 24 weeks
– 12 weeks may be considered
for patients deemed at low risk
for clinical disease progression
and who have subsequent
retreatment options
Patients with
decompensated cirrhosis or
who are pre-/post-liver
transplant
Harvoni® +
ribavirin
24 weeks
Patients with HCV GT 3
Patients with cirrhosis
and/or prior treatment failure
Harvoni® +
ribavirin
24 weeks
*Includes patients co-infected with HIV
Harvoni® was approved on October 10, 2014 by the US Food and Drug Administration
(FDA) for the treatment of chronic HCV GT 1 in adult patients [FDA News Release,
2014], and international treatment guidelines have not yet been updated to reflect this
addition to the treatment armamentarium. Harvoni® represents the first oral,
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
17
short-duration combination therapy to be approved for the treatment of HCV GT 1
infection and the first approved regimen that does not require administration with either
PEG-IFN or RBV [FDA News Release, 2014]. As such, it may help to shorten and
simplify treatment regimens; reduce the incidences of AEs and drug–drug interactions;
decrease monitoring requirements; and widen patient eligibility for treatment. Edward
Cox, Director of the Office of Antimicrobial Products in the FDA’s Center for Drug
Evaluation and Research has stated, “We are changing the treatment paradigm…
Until last year, the only available treatments for hepatitis C virus required administration
with interferon and ribavirin. Now, patients and healthcare professionals have multiple
treatment options, including a combination pill to help simplify treatment regimens”
[FDA News Release, 2014]. Approval for the use of Harvoni® in Europe followed on
November 18, 2014, after the European Commission granted marketing authorization
for Harvoni® to treat the majority of chronic HCV G1 and GT 4 infections in adults
[Gilead Press Release, 2014]. As Harvoni®, like SOF, was reviewed under the FDA’s
and European Medicine Agency’s priority review programs and received breakthrough
therapy designation, it seems likely that international treatment guidelines will be revised
rapidly to reflect its availability, as they were with SOF.
Guidelines issued by a number of international associations continue to recommend
PEG-IFN/RBV as standard of care, with the addition of boceprevir or telaprevir as part of
a triple-therapy regimen, for patients with HCV GT 1. However, further revisions in line
with those from the American Association for the Study of Liver Diseases (AASLD), the
European Association for the Study of Liver Diseases (EASL) and the World Health
Organization (WHO), and following the US approval of Harvoni®, are anticipated. As the
new generation of DAAs gain wider international approval, updates can be expected
from the Asian Pacific Association for the Study of the Liver (APASL; guidance last
updated 2012) and the World Gastroenterology Organisation (WGO; guidance last
updated 2013), both of which focus on the needs of patients living in developing
countries.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
18
8.3 Target population
Harvoni® is suitable for the treatment of chronic HCV GT 1 infection in a wide range of
patient subgroups, regardless of race or gender, including geriatric patients; patients
with mild or moderate renal impairment; and post-liver transplant patients. Harvoni® has
also been approved for use in GT 4 patients and some GT 3 patients in Europe
[Harvoni® SmPC, 2014; Gilead Press Release, 2014]. The safety and efficacy of
Harvoni® have not been established in children and adolescents, pregnant women or
nursing mothers [Harvoni® US PI, 2014].
9. Treatment details
9.1 Indications and usage
Harvoni® is indicated for the treatment of chronic HCV GT 1 infection in adult patients
(aged ≥18 years) (Table 3) [Harvoni® US PI, 2014]. In Europe, Harvoni® is also indicated
for the treatment of adult patients with chronic HCV GT 4 infection and some GT 3
patients (Table 4) [Harvoni® SmPC, 2014; Gilead Press Release, 2014].
9.2 Dosage and administration
The recommended dose of Harvoni® in adult US patients with HCV GT 1 is one tablet
(90 mg of LDV and 400 mg of SOF) taken orally, once daily with or without food for the
duration shown in Table 3, depending on patient characteristics [Harvoni® US PI, 2014].
In Europe, once-daily Harvoni® is recommended as a monotherapy for the treatment of
patients with HCV GT 1 or GT 4 infection with compensated cirrhosis or without
cirrhosis; HCV GT 4 patients with decompensated cirrhosis or who are pre-/post-liver
transplant and HCV GT 3 patients with cirrhosis and/or prior treatment failure should
receive Harvoni® in combination with ribavirin (Table 4) [Harvoni® SmPC, 2014].
As Harvoni® contains LDV and SOF, any interactions that have been identified with
these agents individually may occur with Harvoni®. The concomitant use of Harvoni® and
P-glycoprotein (P-gp) inducers, such as rifampin or St John’s wort, may significantly
decrease plasma concentrations of LDV and SOF, thus potentially reducing the
therapeutic effect of Harvoni®; therefore, the use of Harvoni® is not recommended in
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
19
combination with P-gp inducers. The use of Harvoni® in combination with other products
containing SOF is also not recommended. It is noteworthy that Harvoni® does not
demonstrate significant drug interactions with immunosuppressant drugs or ART,
other than tenofovir disoproxil fumarate, and thus offers an additional treatment choice
for patient populations for whom therapeutic options have always been limited [Harvoni®
US PI, 2014]. The reader is referred to Section 11.2.5 ‘Drug interactions’ and Table 17
for more detailed information on potential drug interactions associated with Harvoni®.
No specific antidote is available for overdose with Harvoni®. If overdose occurs, the
patient must be monitored for evidence of toxicity. Treatment for overdose consists of
general supportive measures, including monitoring of vital signs and observation of the
patient’s clinical status. Hemodialysis can remove the predominant circulating metabolite
of SOF (GS-331007) with an extraction ratio of 53% but is unlikely to result in significant
removal of LDV as LDV is highly bound to plasma protein [Harvoni® US PI, 2014].
9.2.1 Special populations
Pregnancy Category B: Harvoni® should be used during pregnancy only if the potential
benefit justifies the potential risk to the fetus [Harvoni® US PI, 2014].
Nursing mothers: It is not known whether Harvoni® and its metabolites are present in
human breast milk. The health benefits of breastfeeding should be considered alongside
the mother’s clinical need for Harvoni® and any potential adverse effects on the child
from the drug or the mother’s condition [Harvoni® US PI, 2014].
Pediatric use: The safety and efficacy of Harvoni® have not been established in children
and adolescents [Harvoni® US PI, 2014].
Geriatric use: No dose adjustment is warranted for elderly patients [Harvoni® US PI,
2014].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
20
Renal impairment: No dose adjustment of Harvoni® is required for patients with mild or
moderate renal impairment. The safety and efficacy of Harvoni® have not been
established in patients with severe renal impairment (estimated glomerular filtration rate
[eGFR] <30 mL/min/1.73 m2) or end-stage renal disease (ESRD) requiring hemodialysis.
Therefore, no dose recommendation can be given for these patient populations
[Harvoni® US PI, 2014].
Hepatic impairment: No dose adjustment of Harvoni® is required for patients with mild,
moderate or severe hepatic impairment (Child–Pugh–Turcotte [CPT] class A, B or C).
The safety and efficacy of Harvoni® have not been established in patients with
decompensated cirrhosis [Harvoni® US PI, 2014].
9.3 Duration
Harvoni® should be administered once daily for a duration of 12 or 24 weeks, according
to the presence or absence of cirrhosis and the patient’s treatment experience.
Administration of Harvoni® for 8 weeks can be considered in treatment-naïve patients
without cirrhosis who have pre-treatment HCV RNA of <6 million IU/mL (Table 3)
[Harvoni® US PI, 2014].
9.4 Reference to existing WHO and other clinical guidelines
The WHO issued its first set of guidelines on the treatment of HCV infection in April
2014, with the recommendation that all adults and children with chronic HCV infection,
including persons who inject drugs (PWID), should be assessed for HCV therapy [WHO
Guidelines, 2014]. With respect to the choice of treatment, the WHO recommendations
are as follows:
• PEG-IFN/RBV is recommended for the treatment of chronic HCV, rather than
non-pegylated IFN/RBV (strong recommendation, moderate quality of evidence)
• PI-based (boceprevir or telaprevir) triple therapy is suggested for chronic HCV
GT 1, rather than PEG-IFN/RBV alone (conditional recommendation, moderate
quality of evidence)

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
21
• SOF, in combination with RBV, with or without PEG-IFN depending on genotype,
is recommended for HCV GT 1, GT 2, GT 3 and GT 4, rather than PEG-IFN/RBV
alone or no treatment in those who are intolerant to IFN (strong recommendation,
high quality evidence)
• Simeprevir, in combination with PEG-IFN/RBV, is recommended for patients with
HCV GT 1b infection and for those with HCV GT 1a without the Q80K
polymorphism, rather than PEG-IFN/RBV alone (strong recommendation, high
quality evidence).
Evidence-based guidelines have also been issued by a number of internationally
recognized bodies, including the AASLD, the Infectious Diseases Society of America
(IDSA) and the International Antiviral Society-USA (IAS-USA) [AASLD Guidelines, 2014],
as well as EASL [EASL Guidelines, 2014a] and WGO [WGO Guidelines, 2013].
While both US and European guidelines include next-generation DAAs, such as SOF,
in line with WHO recommendations, the APASL and WGO currently recommend
PEG-IFN/RBV as standard therapy for chronic HCV, with the addition of boceprevir or
telaprevir as part of a triple-therapy regimen for patients with HCV GT 1 [WGO
Guidelines, 2013]. Additionally, the WGO suggests how therapy might be modified for
specific regions and in countries where resources are very limited.
As Harvoni® has only been approved recently by the US FDA and EMA, it is not currently
included in international management guidelines for HCV. However, it seems likely that
the guidelines will be updated rapidly to include Harvoni®, reflecting its breakthrough
therapy designation by the FDA. Section 8.2, ‘Assessment of current use’, provides
further information about international guidelines for the management of HCV.
9.5 Special requirements
Treatment with Harvoni® should be initiated and monitored by a physician experienced in
the management of patients with chronic hepatitis C.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
22
10. Summary of comparative effectiveness in a variety of clinical settings
10.1 Identification of clinical evidence
In compiling evidence for this submission, a search of the Medline® database was
performed using the search criteria: ledipasvir [AND] sofosbuvir. A search of abstracts
from relevant congresses over the past 2 years was also performed using the same
search criteria. In addition, review articles on new DAAs, including Harvoni®, were
identified and the reference lists of these examined for any further articles of relevance.
The use of Harvoni® is supported principally by data from three Phase 3 studies (ION-1,
ION-2 and ION-3) [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014], following
successful completion of a Phase 2 clinical program that comprised several studies in
HCV treatment-naïve and treatment-experienced patients (see Table 5) [Data on file –
Gilead Sciences EAME – (HCV13000050); Lawitz et al, 2014; Data on file – Gilead
Sciences EAME – (HCV1300049); Data on file – Gilead Sciences EAME –
(HCV1300045); Data on file – Gilead Sciences EAME – (HCV1300044)]. The Phase 2
program continues to be reinforced by additional studies and analyses in traditionally
difficult-to-treat patient populations, including SIRIUS (PI failures), SOLAR-1
(decompensated cirrhosis and post-liver transplantation) and the LDV/SOF in
Compensated Cirrhosis post-hoc analysis (Table 5) [Data on file – Gilead Sciences
EAME – (HCV13000113); Data on file – Gilead Sciences EAME – (HCV13000101); Data
on file – Gilead Sciences EAME – (HCV13000116); Data on file – Gilead Sciences
EAME – (HCV13000100)]. Some of the analyses from the Phase 2 studies and most
results from the Phase 3 clinical program have been published in international, peer-
reviewed journals.
10.2 Summary of available data on comparative effectiveness of Harvoni®
This section will focus primarily on the outcomes of the Phase 3 clinical trials that have
formed the basis of the regulatory submissions for Harvoni®. The extensive Phase 2
clinical program that has also been undertaken for Harvoni® is overviewed in Table 5.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
23
10.2.1 Summary of the Phase 2 clinical trial program for Harvoni®
The Phase 2 clinical trial program for Harvoni® has evaluated this regimen in patients
with HCV GT 1, GT 3, GT 4 and GT 6 infection, and is ongoing.
The Phase 2 studies in GT 1 patients (LONESTAR, ELECTRON, ELECTRON-2,
SIRIUS, ERADICATE, LDV/SOF in SOF failures) demonstrated that administration of
LDV/SOF for 8, 12 or 24 weeks, with or without RBV, resulted in high rates of SVR12 in
a diverse range of patients, including those with difficult-to-treat characteristics, for
example, with HCV recurrence following liver transplantation [Lawitz et al, 2014; Data on
file – Gilead Sciences EAME – (HCV1300047); Data on file – Gilead Sciences EAME –
(HCV13000050); Data on file – Gilead Sciences EAME – (HCV1300045); Data on file –
Gilead Sciences EAME – (HCV13000113); Data on file – Gilead Sciences EAME –
(HCV13000103); Data on file – Gilead Sciences EAME – (HCV1300097)]. Of note,
patients who had relapsed following treatment with SOF-based regimens were
successfully retreated with LDV/SOF [Data on file – Gilead Sciences EAME –
(HCV1300031)].
Several Phase 2 studies have investigated the efficacy and tolerability of LDV/SOF in
patients with non-GT 1 HCV infections, and a number of these studies are ongoing.
ELECTRON-2 evaluated LDV/SOF in treatment-naïve and treatment-experienced GT 3
patients and GT 6 patients [Data on file – Gilead Sciences EAME – (HCV1300045); Data
on file – Gilead Sciences EAME – (HCV13000114], whilst patients with HCV GT 4
infection have been enrolled in the ongoing SYNERGY and SOLAR-1 studies [Data on
file – Gilead Sciences EAME – (HCV1300098); Data on file – Gilead Sciences EAME –
(HCV13000101)]. Results of the Phase 2 studies of LDV/SOF in patients with genotypes
other than GT 1 are discussed in Section 10.2.6.
Resistance monitoring was performed for all patients in the LONESTAR study in order to
detect treatment-emergent RAVs [Lawitz et al, 2014]. Virologic failure and resistance
analysis, including findings from the Phase 2 LONESTAR study, are discussed more
fully in Section 10.2.4 of this document.
The results from some of the studies in the extensive Phase 2 clinical program guided
the development of the Phase 3 studies described in the next section, and provide

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
24
preliminary evidence for the efficacy of Harvoni® in patients with HCV genotypes other
than GT 1.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
25
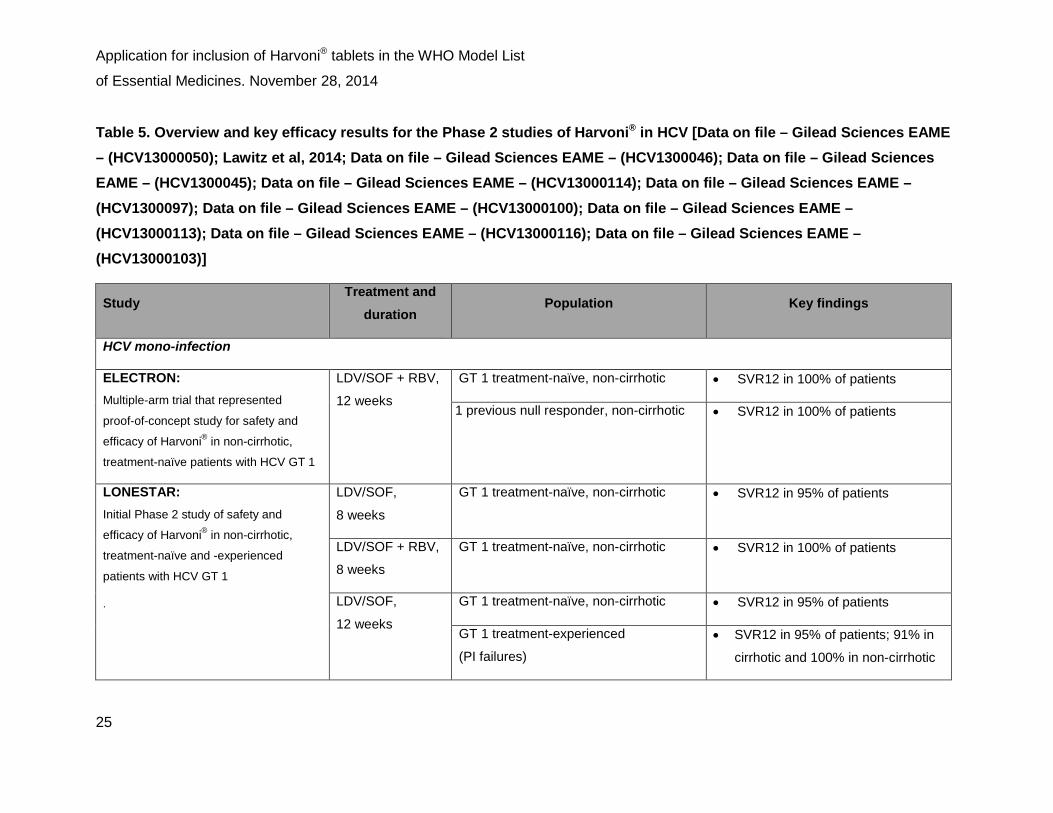
Table 5. Overview and key efficacy results for the Phase 2 studies of Harvoni® in HCV [Data on file – Gilead Sciences EAME – (HCV13000050); Lawitz et al, 2014; Data on file – Gilead Sciences EAME – (HCV1300046); Data on file – Gilead Sciences EAME – (HCV1300045); Data on file – Gilead Sciences EAME – (HCV13000114); Data on file – Gilead Sciences EAME – (HCV1300097); Data on file – Gilead Sciences EAME – (HCV13000100); Data on file – Gilead Sciences EAME – (HCV13000113); Data on file – Gilead Sciences EAME – (HCV13000116); Data on file – Gilead Sciences EAME – (HCV13000103)]
Study Treatment and
duration Population Key findings
HCV mono-infection
ELECTRON: Multiple-arm trial that represented
proof-of-concept study for safety and
efficacy of Harvoni® in non-cirrhotic,
treatment-naïve patients with HCV GT 1
LDV/SOF + RBV,
12 weeks
GT 1 treatment-naïve, non-cirrhotic • SVR12 in 100% of patients
1 previous null responder, non-cirrhotic • SVR12 in 100% of patients
LONESTAR: Initial Phase 2 study of safety and
efficacy of Harvoni® in non-cirrhotic,
treatment-naïve and -experienced
patients with HCV GT 1
.
LDV/SOF,
8 weeks
GT 1 treatment-naïve, non-cirrhotic • SVR12 in 95% of patients
LDV/SOF + RBV,
8 weeks
GT 1 treatment-naïve, non-cirrhotic • SVR12 in 100% of patients
LDV/SOF,
12 weeks
GT 1 treatment-naïve, non-cirrhotic • SVR12 in 95% of patients
GT 1 treatment-experienced
(PI failures) • SVR12 in 95% of patients; 91% in
cirrhotic and 100% in non-cirrhotic
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
26
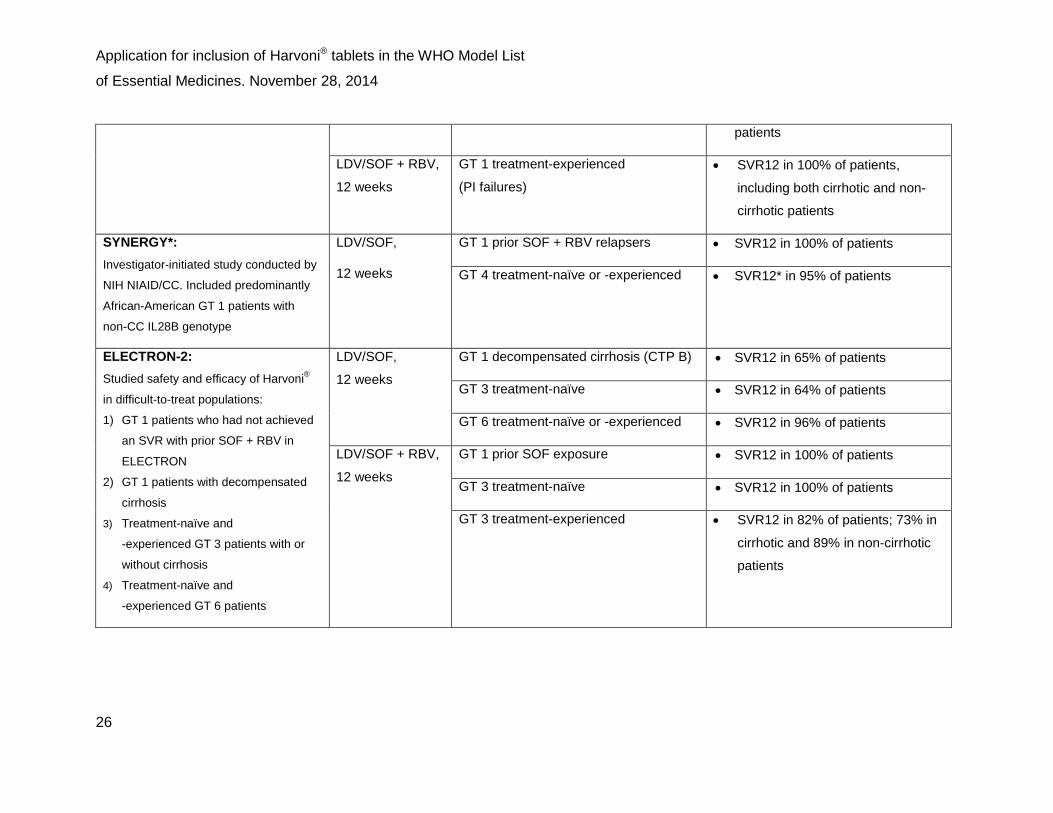
patients
LDV/SOF + RBV,
12 weeks
GT 1 treatment-experienced
(PI failures) • SVR12 in 100% of patients,
including both cirrhotic and non-
cirrhotic patients
SYNERGY*: Investigator-initiated study conducted by
NIH NIAID/CC. Included predominantly
African-American GT 1 patients with
non-CC IL28B genotype
LDV/SOF,
12 weeks
GT 1 prior SOF + RBV relapsers • SVR12 in 100% of patients
GT 4 treatment-naïve or -experienced • SVR12* in 95% of patients
ELECTRON-2: Studied safety and efficacy of Harvoni®
in difficult-to-treat populations:
1) GT 1 patients who had not achieved
an SVR with prior SOF + RBV in
ELECTRON
2) GT 1 patients with decompensated
cirrhosis
3) Treatment-naïve and
-experienced GT 3 patients with or
without cirrhosis
4) Treatment-naïve and
-experienced GT 6 patients
LDV/SOF,
12 weeks
GT 1 decompensated cirrhosis (CTP B) • SVR12 in 65% of patients
GT 3 treatment-naïve • SVR12 in 64% of patients
GT 6 treatment-naïve or -experienced • SVR12 in 96% of patients
LDV/SOF + RBV,
12 weeks
GT 1 prior SOF exposure • SVR12 in 100% of patients
GT 3 treatment-naïve • SVR12 in 100% of patients
GT 3 treatment-experienced • SVR12 in 82% of patients; 73% in
cirrhotic and 89% in non-cirrhotic
patients
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
27
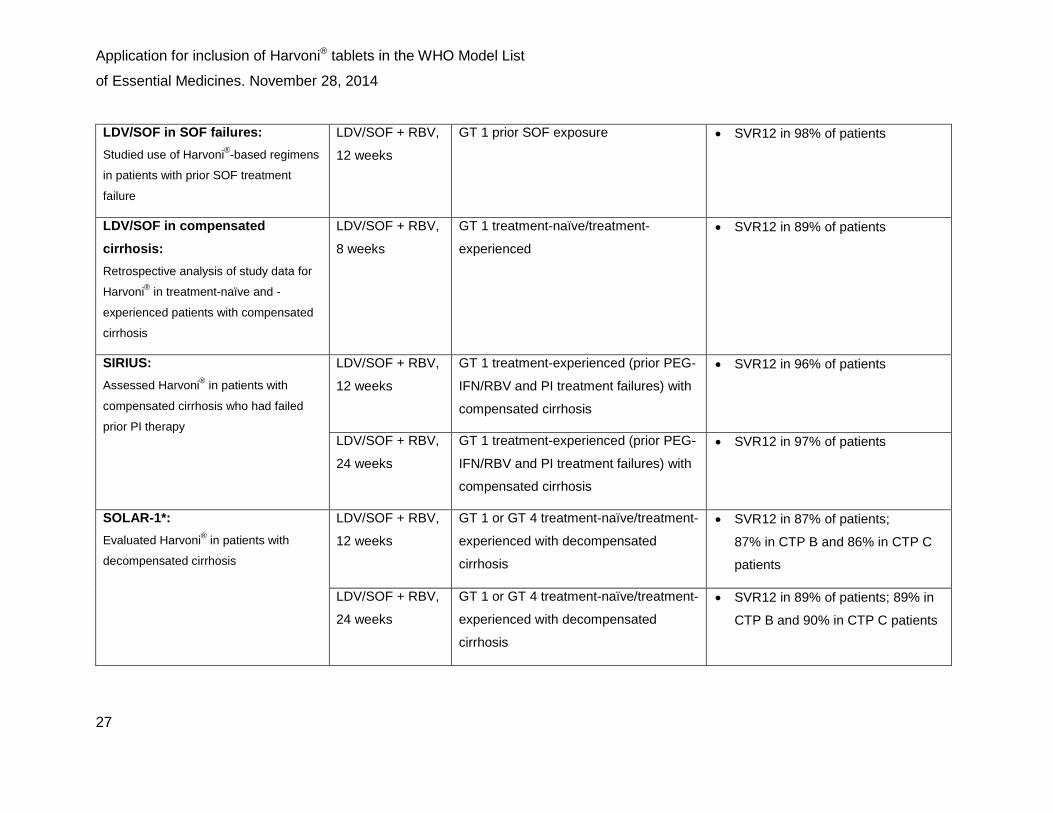
LDV/SOF in SOF failures: Studied use of Harvoni®-based regimens
in patients with prior SOF treatment
failure
LDV/SOF + RBV,
12 weeks
GT 1 prior SOF exposure • SVR12 in 98% of patients
LDV/SOF in compensated cirrhosis: Retrospective analysis of study data for
Harvoni® in treatment-naïve and -
experienced patients with compensated
cirrhosis
LDV/SOF + RBV,
8 weeks
GT 1 treatment-naïve/treatment-
experienced • SVR12 in 89% of patients
SIRIUS: Assessed Harvoni® in patients with
compensated cirrhosis who had failed
prior PI therapy
LDV/SOF + RBV,
12 weeks
GT 1 treatment-experienced (prior PEG-
IFN/RBV and PI treatment failures) with
compensated cirrhosis
• SVR12 in 96% of patients
LDV/SOF + RBV,
24 weeks
GT 1 treatment-experienced (prior PEG-
IFN/RBV and PI treatment failures) with
compensated cirrhosis
• SVR12 in 97% of patients
SOLAR-1*: Evaluated Harvoni® in patients with
decompensated cirrhosis
LDV/SOF + RBV,
12 weeks
GT 1 or GT 4 treatment-naïve/treatment-
experienced with decompensated
cirrhosis
• SVR12 in 87% of patients;
87% in CTP B and 86% in CTP C
patients
LDV/SOF + RBV,
24 weeks
GT 1 or GT 4 treatment-naïve/treatment-
experienced with decompensated
cirrhosis
• SVR12 in 89% of patients; 89% in
CTP B and 90% in CTP C patients

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
28
HIV/HCV co-infection
ERADICATE:
Investigator-initiated study conducted by
NIAID/CC that investigated Harvoni® in
HIV/HCV co-infected patients and
included ARV treatment-naïve and
-experienced patients
LDV/SOF,
12 weeks
GT 1 HIV/HCV ARV-untreated • SVR12 in 100% of patients
GT 1 HIV/HCV ARV-treated • SVR12 in 97% of patients
Special populations
SOLAR-1*: Evaluated Harvoni® in patients with
recurrent HCV infection post-liver
transplantation
LDV/SOF + RBV,
12 weeks
GT 1 or GT 4 patients, post-liver
transplant, non-cirrhotic (F0–F3) • SVR12 in 96% of patients
GT 1 or GT 4 patients, post-liver
transplant, cirrhotic (CTP A, B or C) • SVR12 in 96% in CTP A, 85% in
CTP B and 60% in CTP C patients
LDV/SOF + RBV,
24 weeks
GT 1 or GT 4 patients, post-liver
transplant, non-cirrhotic (F0–F3) • SVR12 in 98% of patients
GT 1 or GT 4 patients, post-liver
transplant, cirrhotic (CTP A, B or C) • SVR12 in 96% in CTP A, 83% in
CTP B and 97% in CTP C patients
ART, antiretroviral therapy; CTP, Child–Turcotte–Pugh; GT, genotype; HCV, hepatitis C virus; HIV, human immunodeficiency virus; LDV, ledipasvir;
LLOQ, lower limit of quantification; NIAID, National Institute of Allergy and Infectious Diseases; NIH, National Institutes of Health; PEG-IFN, pegylated interferon;
PI, protease inhibitor; RBV, ribavirin; SOF, sofosbuvir; SVR, sustained virologic response
*Study ongoing

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
29
10.2.2 Background and design of the Phase 3 studies of Harvoni® in HCV GT 1
The efficacy of Harvoni® was evaluated in four Phase 3 studies (ION-1, ION-2, ION-3,
Japanese study) in a total of 2293 patients with HCV GT 1 infection [Afdhal et al, 2014b
and 2014c; Kowdley et al, 2014; Data on file – Gilead Sciences EAME – (HCV1300057);
Data on file – Gilead Sciences EAME – (HCV13000104)].
ION-1, ION-2 and ION-3 were randomized, open-label, multicenter studies that
evaluated Harvoni®, with or without RBV, for 8, 12 or 24 weeks in patients with HCV
GT 1 infection. The Japanese study was a randomized, multicenter, Phase 3 study of
12 weeks of Harvoni®, with or without RBV, in 341 treatment-naïve and treatment-
experienced Japanese patients with HCV GT 1 infection.
The primary efficacy endpoint in all four studies was SVR12 (HCV RNA below the lower
limit of quantification [25 IU/mL] 12 weeks after the end of treatment); in ION-1, ION-3
and the Japanese study, data were compared with a prespecified historical SVR rate.
All four studies investigated safety and tolerability, virologic failure and viral resistance
associated with Harvoni® therapy. The designs of the four studies are shown in Figure 1.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
30
Figure 1. Designs of the Phase 3 studies of Harvoni® in treatment-naïve and treatment-experienced patients with HCV GT 1 [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014; Data on file – Gilead Sciences EAME – (HCV1300057)]
GT, genotype; HCV, hepatitis C virus; LDV, ledipasvir; RBV, ribavirin; SOF, sofosbuvir;
SVR, sustained virologic response
Specific and general inclusion and exclusion criteria for the ION studies are shown in
Table 6. As the table shows, the ION-1 and ION-2 studies enrolled a high proportion of
patients with cirrhosis, thus providing a strong evidence base for the use of Harvoni® in
this important patient population.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
31
Table 6. Key inclusion and exclusion criteria in the Phase 3 ION studies of Harvoni® [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014]
ION-1 ION-2 ION-3
Specific inclusion criteria
Treatment-naïve:
no prior treatment
with RBV or IFN
Prior treatment
failure with
IFN-based therapy
(including
PI failures)
Treatment-naïve:
no prior treatment
with RBV or IFN
Cirrhosis permitted?
Up to 20% 20% Not permitted
General inclusion criteria
≥18 years of age; confirmation of chronic hepatitis C by positive
anti-HCV, positive HCV RNA or positive HCV genotyping
≥6 months prior to baseline or liver biopsy with evidence of
chronic hepatitis C; serum HCV RNA ≥104 IU/mL during
screening; BMI ≥18 kg/m2 (no upper limit to age or BMI)
Exclusion criteria Co-infection with HBV or HIV; any other clinically significant
chronic liver disease; clinical hepatic decompensation; history of
major organ transplant; clinically relevant drug or alcohol abuse
Women who were pregnant or breastfeeding or men whose
partners were pregnant
BMI, body mass index; HBV, hepatitis B virus; HCV, hepatitis C virus; HIV, human immunodeficiency virus;
IFN, interferon; PI, protease inhibitor; RBV, ribavirin
10.2.3 Results of the Phase 3 registration studies of Harvoni® in mono-infected
patients with HCV GT 1
Efficacy in treatment-naïve patients: ION-1 (ClinicalTrials.gov: NCT01701401)
Of the patients enrolled in ION-1, approximately two-thirds (67%) were infected with
HCV GT 1a. The mean age of patients across the treatment arms was 52 years;
59% were male, the majority (85%) were white, and mean body mass index (BMI) was
27 kg/m2. The study included a high proportion of patients with traditional negative
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
32
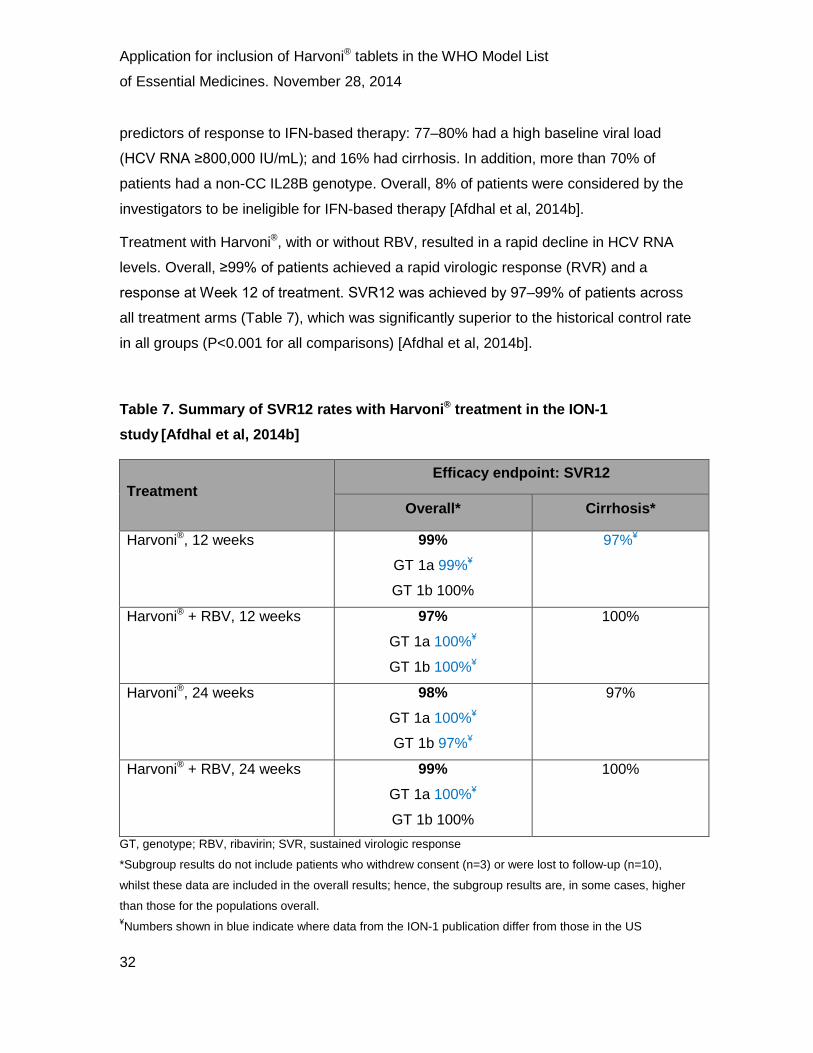
predictors of response to IFN-based therapy: 77‒80% had a high baseline viral load
(HCV RNA ≥800,000 IU/mL); and 16% had cirrhosis. In addition, more than 70% of
patients had a non-CC IL28B genotype. Overall, 8% of patients were considered by the
investigators to be ineligible for IFN-based therapy [Afdhal et al, 2014b].
Treatment with Harvoni®, with or without RBV, resulted in a rapid decline in HCV RNA
levels. Overall, ≥99% of patients achieved a rapid virologic response (RVR) and a
response at Week 12 of treatment. SVR12 was achieved by 97‒99% of patients across
all treatment arms (Table 7), which was significantly superior to the historical control rate
in all groups (P<0.001 for all comparisons) [Afdhal et al, 2014b].
Table 7. Summary of SVR12 rates with Harvoni® treatment in the ION-1 study [Afdhal et al, 2014b]
Treatment Efficacy endpoint: SVR12
Overall* Cirrhosis*
Harvoni®, 12 weeks 99% GT 1a 99%¥
GT 1b 100%
97%¥
Harvoni® + RBV, 12 weeks 97% GT 1a 100%¥
GT 1b 100%¥
100%
Harvoni®, 24 weeks 98% GT 1a 100%¥
GT 1b 97%¥
97%
Harvoni® + RBV, 24 weeks 99% GT 1a 100%¥
GT 1b 100%
100%
GT, genotype; RBV, ribavirin; SVR, sustained virologic response
*Subgroup results do not include patients who withdrew consent (n=3) or were lost to follow-up (n=10),
whilst these data are included in the overall results; hence, the subgroup results are, in some cases, higher
than those for the populations overall. ¥Numbers shown in blue indicate where data from the ION-1 publication differ from those in the US

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
33
Prescribing Information. These discrepancies have arisen as a result of patient reclassification, a lack of
available data at the appropriate time point or incorrectly captured genotype in the interim data.
Of the 16 patients who failed to achieve an SVR12 in ION-1, 13 were lost to follow-up
or withdrew consent. One patient who received 24 weeks of Harvoni® had virologic
breakthrough during treatment, which was suspected to be due to non-adherence to
therapy (documented by means of serum assays for drug levels). Only two patients
(<1%) relapsed post-treatment (one each in the Harvoni®12-week and 24-week arms);
both had NS5A resistance variants at baseline [Afdhal et al, 2014b].
Very high response rates were seen in all patient subgroups in ION-1, including patients
with characteristics historically associated with a poor response to treatment; these
patients demonstrated response rates similar to those among patients without these
characteristics (Figure 2) [Afdhal et al, 2014b].
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
34
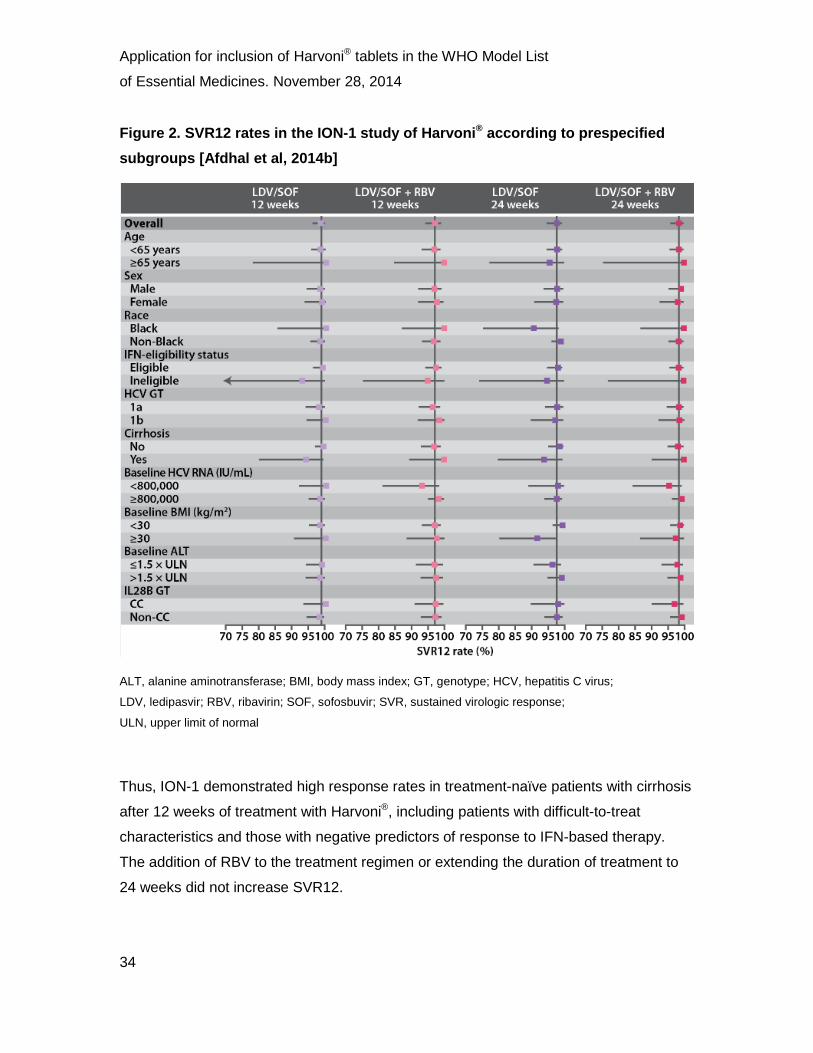
Figure 2. SVR12 rates in the ION-1 study of Harvoni® according to prespecified subgroups [Afdhal et al, 2014b]
ALT, alanine aminotransferase; BMI, body mass index; GT, genotype; HCV, hepatitis C virus;
LDV, ledipasvir; RBV, ribavirin; SOF, sofosbuvir; SVR, sustained virologic response;
ULN, upper limit of normal
Thus, ION-1 demonstrated high response rates in treatment-naïve patients with cirrhosis
after 12 weeks of treatment with Harvoni®, including patients with difficult-to-treat
characteristics and those with negative predictors of response to IFN-based therapy.
The addition of RBV to the treatment regimen or extending the duration of treatment to
24 weeks did not increase SVR12.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
35
Efficacy in treatment-naïve patients without cirrhosis: ION-3
(ClinicalTrials.gov: NCT01851330)
In the ION-3 study, 80% of enrolled patients had HCV GT 1a infection, 19% were Black,
and 6% were Hispanic, reflecting the population of patients with HCV infection in the
USA. Approximately three-quarters of the patients had a non-CC IL28B genotype and an
estimated 6% were considered to be IFN-ineligible by the study investigators [Kowdley
et al, 2014].
Treatment with Harvoni®, with or without RBV, resulted in a rapid decline in HCV RNA
levels, with all but two patients (both in the Harvoni® + RBV arm) achieving an RVR;
≥93% of patients achieved an SVR12 (Table 8) [Kowdley et al, 2014]. Of note, a
non-inferiority analysis demonstrated that the response rate in patients treated with
Harvoni® for 8 weeks was non-inferior to that in patients treated for a longer duration in
the other two groups, supporting the feasibility of a shorter treatment regimen.
Table 8. Summary of SVR12 rates with Harvoni® treatment in the ION-3 study [Kowdley et al, 2014]
Treatment Efficacy endpoint: SVR12
Harvoni®, 8 weeks 94% GT 1a 93%
GT 1b 98%
Harvoni®+ RBV, 8 weeks 93% GT 1a 92%
GT 1b 96%¥
Harvoni®, 12 weeks 95%¥ GT 1a 95%¥
GT 1b 98% GT, genotype; RBV, ribavirin; SVR, sustained virologic response ¥Numbers shown in blue indicate where data from the ION-3 publication differ from those in the US
Prescribing Information. These discrepancies have arisen as a result of patient reclassification, a lack of
available data at the appropriate time point or incorrectly captured genotype in the interim data.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
36
None of the 647 patients treated in ION-3 experienced virologic breakthrough whilst on
therapy. Overall, 23 patients (4%) had a virologic relapse after the end of therapy:
11 patients (5%) who received Harvoni® for 8 weeks, nine (4%) who received Harvoni® +
RBV for 8 weeks, and three (1%) in the 12-week group. In general, similarly high SVR
rates were observed in all prespecified patient subgroups as in the overall population in
ION-3 (Figure 3) [Kowdley et al, 2014].
Figure 3. Rates of SVR12 with Harvoni® in ION-3 according to patient subgroup [Kowdley et al, 2014]
ALT, alanine aminotransferase; BMI, body mass index; GT, genotype; HCV, hepatitis C virus;
IFN, interferon; LDV, ledipasvir; RBV, ribavirin; SOF, sofosbuvir; SVR, sustained virologic response;
ULN, upper limit of normal

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
37
Patients with characteristics historically associated with a poor response to IFN-based
treatment (e.g. non-CC IL28B genotype, high viral load at baseline, Black race, HCV
GT 1a infection) demonstrated SVR12 rates that were similar to those among patients
without these characteristics. For example, in the patient cohort receiving 8 weeks of
Harvoni® without RBV, response rates in all subgroups ranged from 89% to 100%,
irrespective of NS5A mutations or HCV RNA levels at baseline. Patients with baseline
HCV RNA <800,000 IU/mL achieved SVR12 rates of 95.5–97.1%, depending on
treatment regimen, with corresponding rates in patients with high baseline HCV RNA
of 92.4–95.3% [Kowdley et al, 2014].
Thus, in ION-3, Harvoni® therapy was associated with a high SVR12 rate in
treatment-naïve patents without cirrhosis, including those with typically hard-to-treat
characteristics. As in ION-1, the co-administration of RBV or the extension of treatment
did not substantially increase SVR12, supporting a short, simplified treatment regimen.
Efficacy in treatment-experienced patients: ION-2 (ClinicalTrials.gov: NCT01768286)
The majority of patients (79%) in the ION-2 study had HCV GT 1a infection. The mean
age of patients across the treatment arms was 55‒57 years; 65% were male; the
majority (81%) were White; and mean BMI was 28 kg/m2. As expected in a population of
patients who had not responded to prior IFN-based therapy, most patients (88%) had the
non-CC IL28B genotype. A total of 20% of patients in each of the four treatment groups
had cirrhosis. Across the treatment arms, 41‒46% were prior non-responders to
PEG-IFN/RBV therapy, with or without PIs. Overall, 52% of the enrolled patients had
failed prior treatment with a PI-based regimen [Afdhal et al, 2014c].
Treatment with Harvoni®, with or without RBV, resulted in a rapid decline in HCV RNA
levels, with ≥99% of patients in all groups in ION-2 achieving an RVR and end of
treatment response and ≥94% of patients achieving SVR12 (Table 9). Response rates
were similar between cirrhotic and non-cirrhotic patients treated for 24 weeks with
Harvoni®, with or without RBV. In general, SVR12 rates were lower in cirrhotic patients
treated for 12 weeks than those treated for 24 weeks (P=0.007). However, ION-2 was
not powered for intergroup comparisons, and no baseline or on-treatment indicators

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
38
could be identified that might predict which cirrhotic patients were most likely to benefit
from 24 weeks and which 12 weeks of treatment [Afdhal et al, 2014c].
Table 9. Summary of SVR12 rates with Harvoni® therapy in the ION-2 study
[Afdhal et al, 2014c]
Treatment Efficacy endpoint: SVR12
Overall Cirrhosis
Harvoni®, 12 weeks 94% GT 1a 95%
GT 1b 87%
86%
Harvoni® + RBV, 12 weeks 96% GT 1a 96%
GT 1b 100%
82%
Harvoni®, 24 weeks 99% GT 1a 99%
GT 1b 100%
100%
Harvoni® + RBV, 24 weeks 99% GT 1a 99%
GT 1b 100%
100%
GT, genotype; RBV, ribavirin; SVR, sustained virologic response.
Only one patient in ION-2 (in the 24-week Harvoni® + RBV group) experienced
on-treatment virologic breakthrough; however, this patient was thought not to have
adhered to the study treatment, as indicated by plasma concentrations of LDV and
GS-221007 (the predominant circulating metabolite of SOF) that were below or near the
lower level of quantification at Weeks 2, 4 and 6 during treatment. Overall, 11 patients
(2%) relapsed post-treatment, seven (6%) in the 12-week Harvoni® group and four (4%)
in the 12-week Harvoni® + RBV group [Afdhal et al, 2014c].
In all treatment arms, response rates were similar among patients with HCV GT 1a
infection and those with HCV GT 1b infection, among patients who had previously

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
39
received PEG-IFN + RBV and those who had previously received a PI-based regimen,
and among patients with no response to prior treatment and those with prior virologic
breakthrough or relapse (Figure 4). RBV had no effect on response rates, regardless of
treatment duration, and nor did baseline NS5A mutations; 14% of patients had NS5A
RAVs at baseline and 89% of these patients achieved SVR12 [Afdhal et al, 2014c].
Figure 4. Rates of SVR12 with Harvoni® therapy, according to subgroup, in the ION-2 study [Afdhal et al, 2014c]
GT, genotype; HCV, hepatitis C virus; LDV, ledipasvir; PI, protease inhibitor; PEG-IFN, pegylated interferon;
RBV, ribavirin; SOF, sofosbuvir; SVR, sustained virologic response

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
40
The ION-2 study demonstrated similarly high response rates with Harvoni® therapy
across a wide range of treatment-experienced patient subgroups, including those with
difficult-to-treat characteristics, reflecting the broad applicability of Harvoni® also
demonstrated in the ION-1 and ION-3 studies.
Efficacy in Japanese patients: Japanese Phase 3 study
(ClinicalTrials.gov: NCT01975675)
In the Japanese Phase 3 study, the mean age of treated patients was 59 years and
42% were male; all patients were infected with HCV GT 1 (97% GT 1b) and 22% were
cirrhotic [Data on file – Gilead Sciences EAME – (HCV1300057); Data on file – Gilead
Sciences EAME – (HCV13000104)].
Overall, Harvoni®, with or without RBV, resulted in an SVR12 rate of 98% in GT 1
treatment-naïve patients; SVR12 rates of 96% and 100% were demonstrated with
Harvoni®, with and without RBV, respectively. All treatment-experienced patients
achieved SVR12, irrespective of the inclusion of RBV in the treatment regimen or prior
therapy. The study met its primary endpoint of superiority compared with a predefined
historical SVR rate; only one cirrhotic patient did not achieve SVR12. Of note, 99% of
patients (75/76) with RAVs at baseline achieved SVR12, including a small number of
patients with multiple RAVs [Data on file – Gilead Sciences EAME – (HCV1300057);
Data on file – Gilead Sciences EAME – (HCV13000104)]. Thus, the study demonstrated
that Harvoni® therapy was associated with very high response rates in Japanese
patients with HCV GT 1 infection, including those with cirrhosis, prior treatment failure
and RAVs. These results are noteworthy because the high cure rates were achieved
without the need for IFN or RBV, and thus without the substantial side effects associated
with those therapies.
10.2.4 Virologic failure and resistance analysis in the clinical studies
The potential for the development of viral mutations that are resistant to treatment with
DAAs is an important consideration in patients receiving antiviral therapy for HCV
infection, and has been a limiting factor associated with the use of other drugs in this

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
41
class. Importantly, studies have shown that SOF has a high genetic barrier to resistance
[Data on file – Gilead Sciences EAME – (HCV1300023)], whilst NS5A mutations that are
resistant to LDV remain susceptible to SOF, thus indicating a lack of cross-resistance
between the two agents [Wong et al, 2013]. The non-overlapping resistance profiles of
SOF and LDV support their combined use in the treatment of HCV.
Resistance monitoring was performed for all patients in the Phase 2 LONESTAR study
in order to detect treatment-emergent RAVs [Lawitz et al, 2014]. At baseline, NS3 PI
RAVs were detected by deep sequencing in 33/100 patients and NS5A RAVs were
detected in 9/100 patients. All of the patients with NS3 RAVs and 7/9 patients with NS5A
RAVs achieved SVR12 with Harvoni®, with or without RBV; only two patients, one
treatment-naïve and one treatment-experienced, experienced post-treatment virologic
relapse. The high rate of SVR12 in patients with baseline RAVs suggested that the
presence of variants did not preclude the possibility to achieve SVR12 or predict
virologic failure [Lawitz et al, 2014].
Resistance monitoring in the Phase 3 studies
Population and/or deep sequencing of the NS5A and NS5B regions of HCV RNA were
performed for all patients at baseline in the ION studies. For those patients who
experienced virologic failure, sequences obtained at the time of failure were compared
with baseline samples and references in order to detect any treatment-emergent RAVs
[Afdhal et al, 2014b and 2014c; Kowdley et al, 2014].
Results of resistance monitoring in treatment-naïve patients
A pooled analysis of data from the ION studies demonstrated that 16% of patients had
baseline NS5A RAVs, irrespective of subtype (Table 10) [Afdhal et al, 2014b and 2014c;
Kowdley et al, 2014].
Of the treatment-naïve patients with baseline NS5A-resistant mutants in ION-1
and ION-3, 96% and 90% achieved SVR12, respectively [Afdhal et al, 2014b;
Kowdley et al, 2014]. The presence of any given NS5A RAV at baseline was not
associated with relapse.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
42
In ION-1, virologic failure was rare, occurring in only 3/865 patients [Afdhal et al, 2014b].
One patient had virologic breakthrough during treatment, which was associated with
non-adherence to therapy; this patient did not have baseline NS5A RAVs. Of the two
patients who relapsed post-treatment, both had NS5A-resistant variants at baseline.
All three patients had NS5A-resistant variants at the time of virologic failure (L31M in
the GT 1a patient and Y93H in the two GT 1b patients).
In ION-3, no patient experienced on-treatment virologic breakthrough. Of the 23 patients
who relapsed post-treatment, 15 had NS5A RAVs at the time of relapse and eight did
not. Of the 15 patients with NS5A RAVs at relapse, nine had the variants at baseline and
six did not [Kowdley et al, 2014].
The NS5B S282T variant, which is associated with reduced susceptibility to SOF,
was not detected by means of deep sequencing in any patient at baseline or at the time
of virologic failure in either ION-1 or ION-3, reflecting the high genetic barrier to
resistance that has been observed in clinical trials of SOF [Afdhal et al, 2014b;
Kowdley et al, 2014].
Results of resistance monitoring in treatment-experienced patients
In ION-2, 14% of patients with available data had variants associated with resistance to
NS5A inhibitors at baseline; of these, 89% achieved SVR12 (Table 10) [Afdhal et al,
2014c]. In addition, variants associated with resistance to NS3/4A PIs were detected at
baseline in 71% of patients who had received prior PI-based treatment; of these 98%
achieved SVR12 [Afdhal et al, 2014c].
No patient in ION-2 experienced on-treatment virologic breakthrough whilst remaining
adherent to treatment. Of the 11 patients who relapsed after treatment, six had
NS5A-resistant variants at baseline, and all had detectable NS5A-resistant variants at
the time of virologic failure (Table 10). Early reductions in HCV RNA levels were similar
in patients with and without RAVs at baseline, including those who had relapsed. The
NS5B S282T variant was not observed in ION-2 [Afdhal et al, 2014c].
Resistance analyses have been performed using pooled data from a large number of
treatment-naïve and -experienced GT 1 patients receiving Harvoni®, with or without

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
43
RBV, in the Phase 2 LONESTAR and ELECTRON studies and the Phase 3 ION studies.
The analysis evaluated the effects of baseline RAVs on treatment outcomes and
characterized NS5A and NS5B RAVs in patients with virologic failure [Data on file –
Gilead Sciences EAME – (HCV13000119)]. It was notable that pre-existing NS5A RAVs
had poor predictive value for virologic failure, while baseline NS5B NI and NS3 PI RAVs
had no effect on SVR12 rate. Furthermore, whilst virologic failure was associated with
NS5A RAVs in the majority of patients, the prevalence of virologic failure was low, at
2.4% (51/2144 patients) across the studies. Thus, SOF-containing regimens continue to
demonstrate a high barrier to SOF resistance and the efficacy of Harvoni® remains high
despite the presence of RAVs.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
44
Table 10. NS5A resistance in the Phase 3 ION studies [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014]
Study
Overall NS5A mutations at
baseline, n/N* (%)
SVR in patients with baseline
mutations, n/N (%)
Post-treatment relapse, n/N (%)
NS5A-resistant mutations in patients with post-treatment
relapses
At relapse, n/N
At relapse and baseline, n/N
Treatment-naïve
ION-1 140/861 (16) 135/140 (96) 2/865 (0.2) 2/2 2/2
ION-3 116/647 (18) 104/116 (90) 23/647 (3.5) 15/23 9/15
Treatment-experienced
ION-2 62/439 (14) 55/62 (89) 11/440 (2.5) 11/11 6/11
SVR, sustained virologic response
*Patients with available data.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
45
Summary of resistance analyses
Resistance monitoring in the Phase 2 and 3 studies of Harvoni® demonstrated that a
high proportion (92%) of patients who exhibited baseline NS5A RAVs achieved SVR12
[Data on file – Gilead Sciences EAME – (HCV1300119)]. No specific baseline NS5A
mutation was associated with relapse, although patients who experienced relapse were
more likely to have baseline NS5A mutations. No patients receiving Harvoni®
experienced virologic breakthrough other than one non-adherent patient; post-treatment
relapse was also rare, occurring in only 1.8% of patients [Afdhal et al, 2014b and 2014c;
Kowdley et al, 2014]. Response to Harvoni® therapy was not affected substantially by
the presence of either baseline NS5A mutations or, in treatment-experienced patients,
PI-resistant mutations. This latter finding is particularly important as studies of telaprevir
and boceprevir within triple-therapy regimens have detected RAVs in 50‒75% of
treatment-naïve patients not achieving SVR [Wyles et al, 2012]; patients who have failed
therapy with current PI-based therapies represent a growing population with limited
treatment options. Resistance analyses using pooled Phase 2 and 3 data endorse these
results, supporting the efficacy of Harvoni® in patients in whom prior therapies have
proven ineffective [Data on file – Gilead Sciences EAME – (HCV1300119)].
The NS5B S282T variant, which reduces susceptibility to SOF, was detected in only
one patient in the pooled resistance analysis (1/2144), confirming the high genetic
barrier to resistance observed in previous studies of SOF-based therapy; this patient
achieved SVR12 following re-treatment with Harvoni + RBV [Data on file – Gilead
Sciences EAME – (HCV1300119)]. LDV was fully active against S282T, while all
LDV RAVs were fully susceptible to SOF. Both SOF and LDV were fully active against
substitutions associated with resistance to other types of DAAs with different
mechanisms of action (i.e. NS5B non-nucleoside inhibitors and NS3 PIs). This lack
of cross-resistance between LDV, SOF and other DAAs offers an advantage over other
available treatment regimens.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
46
10.2.5 Results of the Phase 3 studies of Harvoni® in patients with traditionally hard-to-treat baseline characteristics
Patients with low albumin and platelet levels
Patients with albumin <3.5 g/dL and platelets <90,000/mm3 have been shown to have a
poor prognosis when treated with first-generation PIs [Afdhal et al, 2014b] and,
therefore, were included in subgroup analyses in the ION-1 and ION-2 studies. In ION-1,
the SVR12 rate in the seven patients with these characteristics was 86%, with the only
patient not responding having stopped treatment after a single dose [Afdhal et al,
2014b]. In ION-2, the SVR12 rate was 92% [Data on file – Gilead Sciences EAME –
(HCV1300059)]. These data support the efficacy of Harvoni® in this traditionally
hard-to-treat patient population.
Patients with HIV/HCV co-infection
Patients with HIV/HCV co-infection who require the co-administration of ART have
traditionally presented a treatment challenge to clinicians due to the potential for
drug–drug interactions between anti-HCV and anti-HIV therapies. The Phase 2
ERADICATE study evaluated the efficacy and safety of Harvoni® for 12 weeks in
patients with HIV/HCV GT 1 co-infection and demonstrated that Harvoni® can be
administered with acceptable tolerability in combination with several ART regimens, with
a low rate of AEs, no substantial changes in CD4 T-cell count or HIV RNA levels, no
renal toxicity and no patient withdrawals from treatment due to AEs; SVR12 was 97%
in those patients who received concomitant ART [Data on file – Gilead Sciences EAME –
(HCV13000103)]. These findings are significant given the previously limited treatment
options available for treating this complex patient population. Phase 3 data from ION-4
in 335 GT 1 and GT 4 patients with HIV-1 co-infection that had been virologically
suppressed for more than 6 months with emtricitabine and tenofovir disoproxil fumarate
plus efavirenz or rilpivirine or raltegravir are expected in early 2015.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
47
Patients with fibrosis or compensated cirrhosis
A considerable proportion of patients in the ION studies had fibrotic liver disease;
therefore, a post-hoc analysis investigated the impact of fibrosis stage on treatment
response [Data on file – Gilead Sciences EAME – (HCV13000105)]. Importantly,
Harvoni®-based regimens were effective in GT 1 patients, irrespective of the degree of
fibrosis or the method of determining fibrosis severity.
To date, a total of 513 patients with HCV GT 1 infection and compensated cirrhosis have
received Harvoni®, with or without RBV, as part of the Phase 2 and Phase 3 clinical trial
programs. These patients were included in a pooled analysis to determine treatment
efficacy in this patient population [Data on file – Gilead Sciences EAME –
(HCV13000100)]. The majority of patients (69%) were treatment-experienced and, of
these, 68% had received prior PI-based therapy. The overall SVR12 rate in this analysis
was 96%; 95% in patients receiving 12 weeks of therapy and 98% with 24 weeks of
therapy. High SVR rates were observed across all patient subgroups and were
increased with the addition of RBV therapy [Data on file – Gilead Sciences EAME –
(HCV13000100)]. These data support the efficacy of Harvoni® in patients with fibrotic
liver disease or cirrhosis.
Patients with negative predictors of response to IFN-based therapy
The ION study program was designed to allow the enrolment of patients with baseline
characteristics typically associated with a poor response to IFN-based therapy. A total of
308 Black patients were included in a retrospective analysis that evaluated the efficacy
of Harvoni®-based regimens in such patients [Data on file – Gilead Sciences EAME –
(HCV13000117)]. Overall, 95% of Black patients achieved an SVR12, while non-Black
patients achieved a rate of 97%, demonstrating that the all-oral regimen was highly
effective in Black patients. A further retrospective analysis investigated the impact of
age, obesity, IL28B TT genotype, uncontrolled diabetes, high viral load, opiate
replacement therapy and prior treatment failures on treatment response [Data on file –
Gilead Sciences EAME – (HCV13000106)]. This analysis demonstrated that traditional
negative predictors of response for IFN-based therapy do not predict response to

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
48
Harvoni® (Table 11). Thus, Harvoni®-based regimens achieve high response rates in
patients with negative predictors of response to IFN.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
49
Table 11. SVR12 rates in patients with traditional negative predictors of response to IFN-based therapy in the ION studies [Data on file – Gilead Sciences EAME – (HCV13000106)]
Predictor Harvoni® Harvoni® + RBV
8 weeks 12 weeks 24 weeks 8 weeks 12 weeks 24 weeks
Age ≥65 years 90% 100% 97% 92% 97% 100%
IL28B TT 92% 97% 96% 86% 98% 100%
Black 91% 99% 92% 89% 98% 100%
HCV RNA >6 million IU/mL 90% 96% – 87% – –
Opiate replacement therapy 100% 94% 91% 100% 91% 100%
HCV, hepatitis C virus; RBV, ribavirin

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
50
Summary
These study data support the efficacy of Harvoni® in a number of traditionally challenging
patient populations, including those with low albumin and platelet levels, HIV/HCV
co-infection, compensated cirrhosis and negative predictors for response to IFN therapy.
Historically, these patient populations have had limited treatment options available to
them and low cure rates. The high rates of SVR12 demonstrated with Harvoni® support
the efficacy of this therapy in these patient cohorts and the potential associated
cost-efficacy benefits to healthcare providers. The reader is referred to Section 12 for a
discussion of the cost-effectiveness of Harvoni®.
10.2.6 Results of the studies of Harvoni® in patients with genotypes other than GT 1
Data from small patient populations in the Phase 2 trials have suggested that Harvoni®
therapy is associated with high cure rates in patients with HCV GT 3, GT 4 and GT 6
infection [Data on file – Gilead Sciences EAME – (HCV1300045), Data on file – Gilead
Sciences EAME – (HCV13000114; Data on file – Gilead Sciences EAME –
(HCV1300098); Data on file – Gilead Sciences EAME – (HCV13000114)].
The Phase 2 ELECTRON-2 study evaluated Harvoni® in treatment-naïve and treatment-
experienced patients with GT 3 infection, with and without cirrhosis. All of the treatment-
naïve patients who received Harvoni® plus RBV achieved SVR12 (26/26) [Data on file –
Gilead Sciences EAME – (HCV1300045)]. Data also showed that 82% (41/50) of the
treatment-experienced patients administered Harvoni® + RBV achieved SVR12,
including 73% of cirrhotic and 89% of non-cirrhotic patients [Data on file – Gilead
Sciences EAME – (HCV13000114].
Patients with HCV GT 4 infection were enrolled in the ongoing Phase 2 SYNERGY and
SOLAR-1 studies [Data on file – Gilead Sciences EAME – (HCV1300098); Data on file –
Gilead Sciences EAME – (HCV13000101)]. Of the 20 GT 4 patients who received
Harvoni® in SYNERGY, 95% achieved SVR12 (19/20; one patient had not reached the
12-week time point at the time of analysis) [Data on file – Gilead Sciences EAME –
(HCV1300098)]. These findings are borne out by early Phase 3 trial data. Two
treatment-naïve patients with HCV GT 4 infection were enrolled in the Phase 3 ION-1

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
51
study, one of whom received Harvoni® for 12 weeks and the other Harvoni® + RBV for
24 weeks; both patients achieved SVR12 [Afdhal et al, 2014b].
There is currently no approved all-oral treatment regimen for patients with HCV GT 6.
One arm of the ELECTRON-2 study evaluated whether Harvoni® would be effective in
treatment-naïve and treatment-experienced GT 6 patients, and a high rate (96%) of
SVR12 was demonstrated in this population [Data on file – Gilead Sciences EAME –
(HCV13000114)]; currently, no data are available in patients with HCV GT 5 infection.
Further data on the efficacy of Harvoni® in non-GT 1 genotypes in the ION and other
Phase 3 trials are awaited with interest.
10.2.7 Impact of Harvoni® on patient health-related quality of life
Patients with chronic HCV infection have reduced health-related quality of life (HRQoL)
compared with the general population, and treatment with PEG-IFN-based regimens
diminishes this further, largely as a result of side effects [Bezemer et al, 2012]. Patients
in the ION study program were asked to complete several questionnaires (Chronic Liver
Disease Questionnaire-HCV, Short Form-36, Functional Assessment of Chronic Illness
Therapy-Fatigue, and Work Productivity and Activity Index: Specific Health Problem) in
order to establish the effect of Harvoni®, with and without RBV, on patient-reported
outcomes (PRO) [Data on file – Gilead Sciences EAME – (HCV13000108)]. During
treatment with RBV-containing regimens, PRO scores decreased compared with
baseline and remained below baseline levels until the end of therapy. In contrast,
PRO improved in the RBV-free treatment arms throughout the treatment period and were
significantly superior to those in the Harvoni® + RBV arms. Patients who achieved
SVR12 (irrespective of treatment regimen) showed a significant improvement in
PRO compared with baseline.
A similar analysis was conducted and stratified according to fibrosis stage [Data on file –
Gilead Sciences EAME – (HCV13000109)]. At baseline, patients with advanced fibrosis
had greater PRO impairment than those in the early stages of disease. However,
significant improvements in PRO were observed in patients who achieved SVR12,
irrespective of fibrosis stage, with those with early-stage liver disease obtaining similar
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
52
benefits to those with more advanced disease. Thus, Harvoni® therapy is associated with
significant improvements in patient HRQoL regardless of disease stage.
10.2.8 Effect of Harvoni® therapy on long-term patient outcomes
Currently, only short-term data are available from the Phase 3 studies of Harvoni® in
patients with HCV and therefore any conclusions about potential long-term outcomes,
such as the development of decompensated cirrhosis or HCC or the need for liver
transplantation, can only be derived from models. In one such analysis, using SVR12
rates from Phase 3 studies, modeled cohorts of GT 1 patients initiated treatment at
different stages of fibrosis (F0–F1, F2, F3–F4) and received either Harvoni® for 8 or
12 weeks; SOF-, PI- or PEG-IFN-based regimens; or no treatment [Data on file – Gilead
Sciences EAME – (HCV13000110)]. In the analysis, initiating Harvoni® treatment at
F0–F1 or F2 versus F3–F4 resulted in a significant decrease in liver disease progression
and related sequelae.
An additional model evaluated health outcomes associated with 12 weeks of
Harvoni® therapy in GT 1 cirrhotic patients compared with other treatment options (SOF
+
PEG-IFN + RBV for 12 weeks, or simeprevir + PEG-IFN + RBV for 12 weeks, or no
treatment) [Data on file – Gilead Sciences EAME – (HCV13000111)]. Compared with
SOF + PEG-IFN, Harvoni® conferred an anticipated 50% reduction in HCV sequelae and
increased quality-adjusted life years (QALYs). The model also evaluated the benefits of
SOF-based regimens in other genotypes, and demonstrated that they were associated
with a decrease in the incidence of liver disease complications compared with
non-SOF-based treatment options.
These models suggest that Harvoni®, in GT 1 patients, and other SOF-based regimens
in GT 2, GT 3 and GT 4 patients, are likely to yield better health outcomes than other
HCV treatment options in both cirrhotic and non-cirrhotic patients. The reader is referred
to Section 12 for further discussion on modeling of patient outcomes with Harvoni®.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
53
10.3 Summary of available estimates of comparative effectiveness
In the Phase 3 clinical trial program, 8–12 weeks of Harvoni® therapy, with or without
RBV, provided high levels of cure in treatment-naïve and treatment-experienced patients
with HCV GT 1, including those with compensated cirrhosis [Afdhal et al, 2014b and
2014c; Kowdley et al, 2014; Data on file – Gilead Sciences EAME –
(HCV13000104)].The ION studies and the Japanese Phase 3 study clearly
demonstrated that exclusion of RBV from the regimen maintained efficacy, with
subsequent analyses showing that patient HRQoL also improved with the omission of
RBV from the regimen [Data on file – Gilead Sciences EAME – (HCV13000108)]. Thus,
the studies supported the feasibility of shorter, simplified, all-oral, Harvoni®-based
regimens for HCV GT 1 patients.
Data from the Phase 2 trials have suggested that Harvoni® therapy is associated with
high rates of cure in patients with HCV GT 3, GT 4 and GT 6 infection [Data on file –
Gilead Sciences EAME – (HCV1300045), Data on file – Gilead Sciences EAME –
(HCV13000114); Data on file – Gilead Sciences EAME – (HCV1300098); Data on file –
Gilead Sciences EAME – (HCV13000114)].
The extensive Phase 2 clinical trial program demonstrated that administration of
Harvoni® for 8, 12 or 24 weeks, with or without RBV, achieved high rates of SVR12 in a
diverse range of HCV GT 1 patients, including those with difficult-to-treat characteristics,
such as HIV/HCV co-infection, recurrent HCV infection following liver transplantation and
previous non-response to PI- and SOF-based therapies [Lawitz et al, 2014; Data on file
– Gilead Sciences EAME – (HCV13000103); Data on file – Gilead Sciences EAME –
(HCV13000101); Data on file – Gilead Sciences EAME – (HCV13000113); Data on file –
Gilead Sciences EAME – (HCV1300097)]. Again, these results are endorsed by findings
from the Phase 3 studies, which showed high cure rates with Harvoni® in patients with
low albumin and platelet levels, and compensated cirrhosis, and in those with baseline
characteristics typically associated with a poor response to IFN-based therapy (i.e. Black
ethnicity, obesity, older age, IL28B TT genotype, uncontrolled diabetes, high viral load,
opiate replacement therapy and prior treatment failure) [Data on file – Gilead Sciences
EAME – (HCV1300059); Data on file – Gilead Sciences EAME – (HCV13000100); Data
on file – Gilead Sciences EAME – (HCV13000105); Data on file – Gilead Sciences
EAME – (HCV13000106); Data on file – Gilead Sciences EAME – (HCV13000117)].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
54
Resistance monitoring in the ION studies demonstrated that a high proportion (92%) of
patients who exhibited baseline NS5A RAVs achieved SVR12 [Data on file – Gilead
Sciences EAME – (HCV1300119)]. No specific baseline NS5A mutation was associated
with relapse, and post-treatment relapse was rare. In addition, no patients receiving
Harvoni® experienced virologic breakthrough, other than one non-adherent patient
[Afdhal et al, 2014b and 2014c; Kowdley et al, 2014]. Importantly, response to Harvoni®
therapy was not affected substantially by the presence of baseline NS5A mutations or
PI-resistant mutations. Furthermore, the studies confirmed the high genetic barrier to
resistance observed previously with SOF-based therapy and demonstrated a lack of
cross-resistance between LDV, SOF and other DAAs. These findings are borne out by
pooled data for a large number of treatment-naïve and -experienced patients in Phase 2
and 3 trials of Harvoni®, which demonstrated that the presence of NS5A RAVs prior to
commencing treatment were poor predictors for the risk of virologic failure, while
baseline NS5B or NS3 PI RAVs had no impact on SVR12 rate [Data on file – Gilead
Sciences EAME – (HCV1300119)].
Notably, the high cure rates achieved with Harvoni® in the Phase 3 trials were
associated with significant improvements in PRO and patient HRQoL compared with
baseline assessments [Data on file – Gilead Sciences EAME – (HCV13000108); Data on
file – Gilead Sciences EAME – (HCV13000109], which, together with the simple, all-oral
treatment regimen, may promote improved patient adherence to treatment. Furthermore,
modeling of data from the Phase 3 trials suggested that Harvoni® is likely to confer
substantial reductions in HCV sequelae and increases in QALYs in the long term, in both
cirrhotic and non-cirrhotic patients across the genotypes, compared with other available
HCV treatment options [Data on file – Gilead Sciences EAME – (HCV13000110); Data
on file – Gilead Sciences EAME – (HCV13000111)]. Such findings indicate potential
cost-efficacy benefits for healthcare providers, which may be particularly pertinent to
resource-limited regions, such as developing countries (See Section 12).
The Harvoni® STR builds on the proven efficacy of SOF to offer a wide range of patients,
including those with traditionally difficult-to-treat disease, a high chance of cure with a
short, all-oral, IFN- and, in most cases, RBV-free treatment regimen.
Overall, data from the clinical studies suggest that Harvoni®, with or without RBV, has
the potential to offer HCV patients, including those with historically difficult-to-treat

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
55
disease, significant efficacy advances over current standards of care. This is reflected in
its designation by the US FDA in October 2014 as a breakthrough therapy for HCV
[FDA News Release, 2014]. Moreover, as the next section will demonstrate, Harvoni® is
well tolerated and – as a once-daily, oral medication – a simple drug to prescribe.
11. Summary of comparative evidence on safety
The safety and tolerability of Harvoni® have been assessed in a diverse range of patients
with chronic HCV GT 1 infection. Data from these studies have demonstrated an
excellent safety and tolerability profile for Harvoni® in this patient population, with a low
rate of treatment discontinuations [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014;
Lawitz et al, 2014; Data on file – Gilead Sciences EAME – (HCV13000045); Data on file
– Gilead Sciences EAME – (HCV1300046); Data on file – Gilead Sciences EAME –
(HCV1300047); Data on file – Gilead Sciences EAME – (HCV1300050); Data on file –
Gilead Sciences EAME – (HCV1300097); Data on file – Gilead Sciences EAME –
(HCV13000101); Data on file – Gilead Sciences EAME – (HCV13000103); Data on file –
Gilead Sciences EAME – (HCV13000113); Data on file – Gilead Sciences EAME –
(HCV13000116)].
Reported incidences of anemia, headache, fatigue, rash, pruritus and insomnia were
higher among patients receiving concomitant RBV, consistent with the well-known side
effects of this therapy [Lawitz et al, 2014; Data on file – Gilead Sciences EAME –
(HCV1300045); Data on file – Gilead Sciences EAME – (HCV1300050); Data on file –
Gilead Sciences EAME – (HCV1300098); Data on file – Gilead Sciences EAME –
(HCV13000103); Data on file – Gilead Sciences EAME – (HCV13000113)]. However,
data from the ION studies indicated that the co-administration of RBV increased toxicity
without providing substantial additional efficacy benefits, supporting the use of RBV-free
regimens, and their potential for reduced patient monitoring, fewer transfusions and
improved treatment adherence [Kowdley et al, 2014].
It is noteworthy that the favorable safety profile of Harvoni® included GT 1 patients with
HIV/HCV co-infection, regardless of ART status, a population for whom treatment is
traditionally limited by the high rate of AEs and the potential for drug–drug interactions

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
56
[Data on file – Gilead Sciences EAME – (HCV1300069); Data on file – Gilead Sciences
EAME – (HCV1300103)].
Preliminary data on the safety and tolerability of Harvoni® in patients with HCV GT 3,
GT 4 and GT 6 infection suggest that the safety profile of this agent is similar to that
observed in HCV GT 1 patients [Data on file – Gilead Sciences EAME – (HCV1300045);
[Data on file – Gilead Sciences EAME – (HCV1300098); Data on file – Gilead Sciences
EAME – (HCV13000114)]. Studies are ongoing in these patient populations.
11.1 Estimate of total patient exposure to Harvoni®
More than 800 patients have participated in completed and ongoing Phase 2 trials of
Harvoni®, while over 2000 patients have been treated in the Phase 3 clinical trial
program. These studies have enrolled a broad range of chronic HCV patients, including
patients with HIV/HCV co-infection, patients with bleeding disorders, and patients from a
range of ethnicities, including Japanese patients [Data on file – Gilead Sciences EAME –
(HCV13000103); Data on file – Gilead Sciences EAME – (HCV1300047); Data on file –
Gilead Sciences EAME – (HCV1300057); Data on file – Gilead Sciences EAME –
(HCV13000104)].
Cumulative patient exposure to Harvoni® in the period following drug approval is
presented in Table 12.
Table 12. Estimated cumulative post-marketing exposure to Harvoni® in Europe and North America
Product Time period Cumulative post-marketing exposure
Harvoni® October 10 – October 31, 2014* 19,000 units
*Harvoni® was approved in Canada on October 16, 2014. Patients in the UK were treated on an
early access program.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
57
11.2 Description of adverse effects/reactions
11.2.1 Treatment-emergent adverse events in patients with HCV GT 1
Treatment-emergent adverse events in the Phase 2 studies
Harvoni® demonstrated a favorable safety profile in GT 1 patients in the Phase 2 studies.
The most commonly reported AEs in patients treated with Harvoni®, with or without RBV,
across all studies were headache (≤26%), fatigue (≤32%) and rash (≤21%) [Lawitz et al,
2014; Data on file – Gilead Sciences EAME – (HCV1300045); Data on file – Gilead
Sciences EAME – (HCV1300050); Data on file – Gilead Sciences EAME –
(HCV1300079); Data on file – Gilead Sciences EAME – (HCV1300098); Data on file –
Gilead Sciences EAME – (HCV13000103); Data on file – Gilead Sciences EAME –
(HCV13000113)]. Anemia, known to be associated with RBV, was more common in
patients treated with Harvoni® + RBV compared with Harvoni® alone [Data on file –
Gilead Sciences EAME – (HCV1300045)]. Overall, there was a low rate of Grade 3–4
AEs and serious AEs (SAEs), with few patients across all studies withdrawing from
treatment due to AEs [Lawitz et al, 2014; Data on file – Gilead Sciences EAME –
(HCV1300045); Data on file – Gilead Sciences EAME – (HCV1300050); Data on file –
Gilead Sciences EAME – (HCV1300098); Data on file – Gilead Sciences EAME –
(HCV13000103); Data on file – Gilead Sciences EAME – (HCV13000113)].
In the Phase 2 SIRIUS study in patients (N=155) with compensated cirrhosis who had
failed prior therapy (PEG-IFN/RBV or PI/PEG-IFN/RBV), treatment was well tolerated
and Harvoni® demonstrated a similar AE profile when administered for 12 weeks with
RBV and when administered for 24 weeks alone; one patient withdrew from the study
during the placebo phase due to an SAE and was excluded from the analysis [Data on
file – Gilead Sciences EAME – (HCV1300079); Data on file – Gilead Sciences EAME –
(HCV13000113)]. Reductions in hemoglobin levels, consistent with RBV-associated
anemia, were observed during treatment, while alanine aminotransferase and aspartate
aminotransferase elevations were noted during the placebo phase, consistent with the
natural history of untreated HCV infection. These safety findings are encouraging as
patients with cirrhosis are at high risk of disease progression.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
58
TEAEs in the Phase 3 trials
The favorable safety profile of Harvoni® demonstrated in the Phase 2 studies was
confirmed in the Phase 3 analyses (Tables 13, 14 and 15). Whilst the majority of patients
in the ION-1, -2 and -3 studies (67‒92%), including those with and without cirrhosis,
exhibited at least one AE, most events were of grade 1 severity; the most commonly
reported AEs were fatigue, headache, insomnia and nausea (Table 13) [Afdhal et al,
2014b and 2014c; Kowdley et al, 2014]. Patients receiving RBV demonstrated higher
incidences of fatigue, insomnia, rash, cough, pruritus and anemia – AEs known to be
associated with RBV – than those receiving Harvoni® alone.
Serious AEs were reported by ≤8% of patients with HCV GT 1 across all arms of the
three ION studies (Table 14). Overall, SAEs were reported more commonly in patients
who received Harvoni® for 24 weeks than in those receiving treatment for 8 or 12 weeks
[Afdhal et al, 2014b and 2014c; Kowdley et al, 2014].
Harvoni® was generally well tolerated, with a low rate of treatment discontinuations
across the trials (≤2% for Harvoni® alone and ≤3% for Harvoni® + RBV) (Table 14).
No patients receiving Harvoni® for 8 or 12 weeks withdrew from treatment due to AEs.
In a Phase 3 study in treatment-naïve (n=166) and treatment-experienced (n=175)
GT 1 patients in Japan, the safety profile of Harvoni® was similar to that in the pivotal
ION studies [Data on file – Gilead Sciences (HCV 1300070)]. Data from the Phase 3
Japanese study are presented in Tables 13, 14 and 15. These data demonstrate
consistency in safety findings across patients of different racial origins.
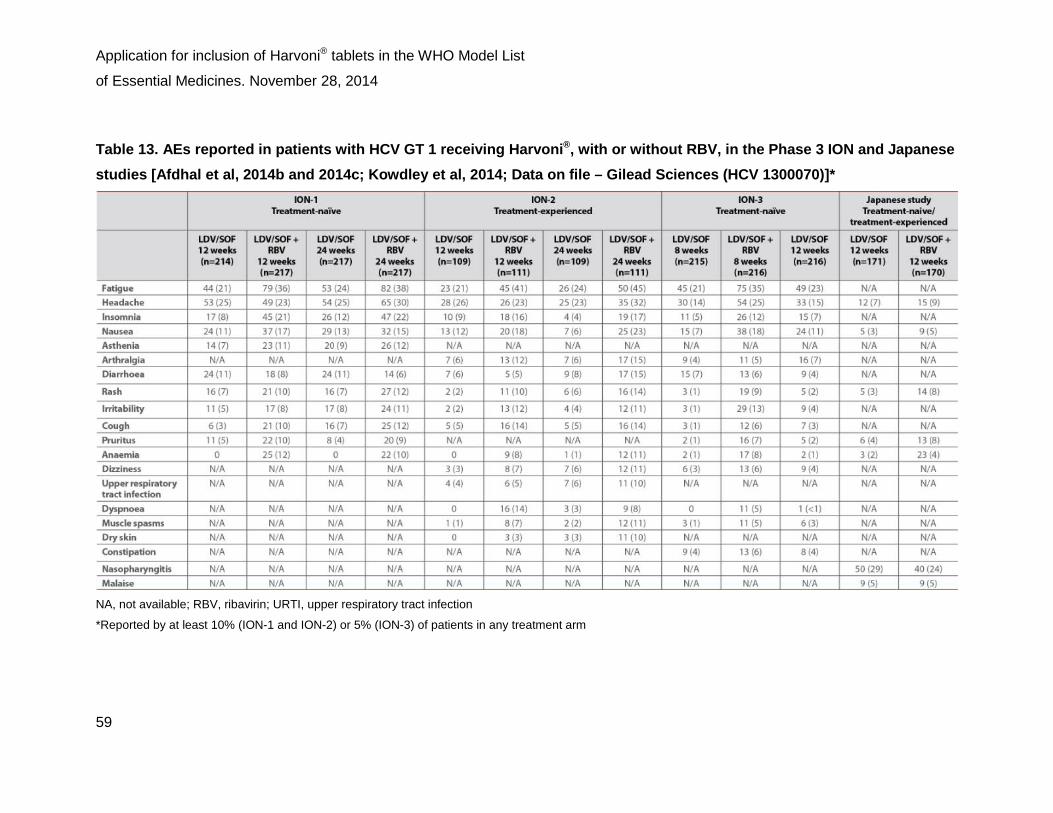
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
59
Table 13. AEs reported in patients with HCV GT 1 receiving Harvoni®, with or without RBV, in the Phase 3 ION and Japanese studies [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014; Data on file – Gilead Sciences (HCV 1300070)]*
NA, not available; RBV, ribavirin; URTI, upper respiratory tract infection
*Reported by at least 10% (ION-1 and ION-2) or 5% (ION-3) of patients in any treatment arm

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
60
Table 14. Overall safety profile and treatment discontinuations reported in patients receiving Harvoni®, with or without RBV, in the Phase 3 ION and Japanese studies [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014; Data on file – Gilead Sciences (HCV 1300070)]
AEs, adverse events; RBV, ribavirin; SAEs, serious adverse events

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
61
Treatment-emergent laboratory test abnormalities in the Phase 3 clinical trials
Hematologic abnormalities are a well-known side effect of RBV therapy and a common
reason for dose reductions [Fried, 2002]. Anemia was reported in 8‒12% of patients
treated with Harvoni® + RBV versus 0‒1% of patients treated with Harvoni® alone in the
ION studies; all but one case of reduced hemoglobin levels (<10 mg/mL) were observed
with RBV treatment (Table 15) [Kowdley et al, 2014].
Bilirubin, creatine kinase and lipase elevations
Total bilirubin elevations of more than 1.5× the upper limit of normal (ULN) were
observed in 3%, <1% and 2% of patients treated with Harvoni® for 8, 12 and 24 weeks,
respectively, in the ION trials [Harvoni® US PI, 2014].
Creatine kinase (CK) levels were not assessed in the Phase 3 ION trials of
Harvoni® [Harvoni® US PI, 2014]. However, isolated, asymptomatic CK elevations of
greater than or equal to 10×ULN have been reported previously in ≤2% of patients
receiving SOF + RBV, with or without PEG-IFN, for 12 or 24 weeks in the FISSION and
NEUTRINO trials [Sovaldi US PI, 2014].
Transient, asymptomatic lipase elevations of more than 3×ULN were observed in
<1%, 2% and 3% of patients treated with Harvoni® for 8, 12 and 24 weeks, respectively,
in the Phase 3 studies [Harvoni® US PI, 2014], reflecting similar findings to those
reported with SOF + RBV, with or without PEG-IFN, in FISSION and NEUTRINO
[Sovaldi® US PI, 2014].
No clinical significance has been reported in association with these findings in
HCV patients receiving Harvoni® to date.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
62
Table 15. Hematologic abnormalities reported in patients receiving Harvoni®, with or without RBV, in the Phase 3 ION and Japanese studies [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014; Data on file – Gilead Sciences (HCV 1300070)]
ANC, absolute neutrophil count; Hb, hemoglobin; NA, available; RBV, ribavirin
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
63
11.2.2 Safety of Harvoni® in patients with HCV GT 1 and cirrhosis
Patients with cirrhosis tend to be older and to have a lower tolerance to AEs than
patients with less advanced disease; such patients also tend to experience a greater
number of potentially treatment-limiting hematologic AEs [EASL Guidelines, 2014a].
A pooled analysis of safety and tolerability data from the three Phase 3 ION trials
demonstrated similar safety data for GT 1 patients with and without cirrhosis, although a
higher proportion of cirrhotic patients in the Harvoni® + RBV arms experienced AEs
leading to study drug modification or interruption (Table 16). Overall, no patients with
cirrhosis withdrew from treatment due to AEs [Afdhal et al, 2014b and 2014c; Kowdley et
al, 2014].
Phase 2 trial data have demonstrated that Harvoni® was well tolerated in HCV GT 1
patients with decompensated cirrhosis, with a safety profile similar to that in non-cirrhotic
patients [Data on file – Gilead Sciences EAME – (HCV1300045); Data on file – Gilead
Sciences EAME – (HCV13000116]. This is a particularly important finding as such
patients are excluded from treatment with IFN-based regimens due to AEs and,
therefore, have limited treatment options available to them.
Data have also suggested that Harvoni® + RBV is generally well tolerated in patients with
recurrent HCV infection post-transplant, with low rates of treatment discontinuation due
to AEs [Data on file – Gilead Sciences EAME – (HCV13000101)]. No drug–drug
interactions have been reported between Harvoni® and the immunosuppressants that
are critical for the management of post-liver transplant patients [Harvoni® US PI, 2014],
therefore Harvoni® may represent a valuable addition to the treatment options available
for these patients The reader is referred to Section 11.2.5 for further discussion on
potential drug interactions associated with Harvoni® therapy.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
64
Table 16. Safety profile according to cirrhosis status in the Phase 3 ION studies [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014]
n (%) Harvoni® Harvoni® + RBV
No cirrhosis (n=969)
Cirrhosis (n=111)
No cirrhosis (n=759)
Cirrhosis (n=113)
AE 715 (73.7) 85 (76.6) 646 (85.1) 99 (87.6)
Treatment-related AE
438 (45.2) 46 (41.4) 528 (69.6) 89 (78.8)
Grade ≥3 AE 39 (4.0) 7 (6.3) 35 (4.6) 10 (8.8)
SAE 29 (3.0) 5 (4.5) 14 (1.8) 3 (2.7)
Treatment-related SAE
3 (0.3) 1 (0.9) 0 1 (0.9)
AEs leading to study drug modification/ interruption
5 (0.5) 1 (0.9) 95 (12.5) 23 (20.4)
Treatment discontinuation due to AE
6 (0.6) 0 11 (1.5) 0
Death 0 0 0 0
AE, adverse event; RBV, ribavirin; SAE, serious adverse event
11.2.3 Safety of Harvoni® in patients with HIV/HCV co-infection
Traditionally, the treatment of patients with HIV/HCV co-infection has been limited due
to the high rate of AEs observed with PEG-IFN- and RBV-based regimens, and the
potential for drug–drug interactions between anti-HCV and anti-HIV therapies. While
efficacy has improved with the advent of PIs, AE profiles did not improve until the advent

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
65
of SOF; both telaprevir and boceprevir are associated with increased rates of anemia,
rash, pruritus and dysgeusia [Naggie and Sulkowski, 2012].
The Phase 2 ERADICATE study evaluated the efficacy and safety of Harvoni® for
12 weeks in patients with HCV GT 1 and HIV co-infection. Harvoni® was administered in
combination with several ART regimens, with a low rate of AEs, no significant changes in
CD4 T-cell count or HIV RNA levels, no renal toxicity and no patient withdrawals from
treatment due to AEs [Data on file – Gilead Sciences EAME – (HCV13000103)]. The
lack of significant interactions with several ART regimens suggests that Harvoni® may be
administered with acceptable safety and tolerability to some HIV co-infected patients, for
whom current treatment options are limited.
11.2.4 Safety of Harvoni® in patients with HCV GT 2, 3, 4, 5 and 6 infection
Preliminary data on the safety and tolerability of Harvoni® in HCV genotypes other
than GT 1 are available for a small group of patients.
The Phase 2 ELECTRON-2 trial [Data on file – Gilead Sciences EAME –
(HCV1300045); Data on file – Gilead Sciences EAME – (HCV13000114)] evaluated
Harvoni® for 12 weeks in patients with GT 3 infection (n=50). Results from the study
were encouraging, demonstrating a similar safety profile with Harvoni®, with or without
RBV, to that in the Phase 3 studies in GT 1 patients. Preliminary data from the trial
(n=25) also suggest that Harvoni® is well tolerated in patients with GT 6 infections
[Data on file – Gilead Sciences EAME – (HCV13000114)], representing the first
indication of a potentially safe and effective all-oral regimen in this patient population.
Two patients infected with HCV GT 4 were enrolled in the Phase 3 ION-1 study; one
patient received Harvoni® for 12 weeks and the other Harvoni® + RBV for 24 weeks
[Afdhal et al, 2014b]. To date, no specific details of the safety analysis in these two
patients have been published. Thus, studies in patients with GT 4 infection are ongoing,
while the use of Harvoni® is also under investigation in patients with HCV GT 2 and
GT 5.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
66
11.2.5 Drug interactions
As Harvoni® contains LDV and SOF, any drug interactions that have been identified with
these agents individually may occur with Harvoni®. Both LDV and SOF are substrates of
the drug transporters P-gp and breast cancer resistance protein (BCRP). Ledipasvir is
an inhibitor of both P-gp and BCRP, and may increase intestinal absorption of
co-administered substrates for these transporters. Medicinal products that are potent
P-gp inducers, such as rifampin or St John’s wort, may decrease plasma concentrations
of LDV and SOF, leading to a potential reduction in the therapeutic efficacy of Harvoni®.
Thus, co-administration of Harvoni® with potent P-gp inducers is not recommended
[Harvoni® US PI, 2014; Data on file – Gilead Sciences EAME – (HCV13000118)].
Table 17 provides a listing of established or potentially clinically significant drug
interactions with Harvoni®, based on predicted drug interactions and studies conducted
with Harvoni® or its individual components. It should be noted that this list is not
all-inclusive.
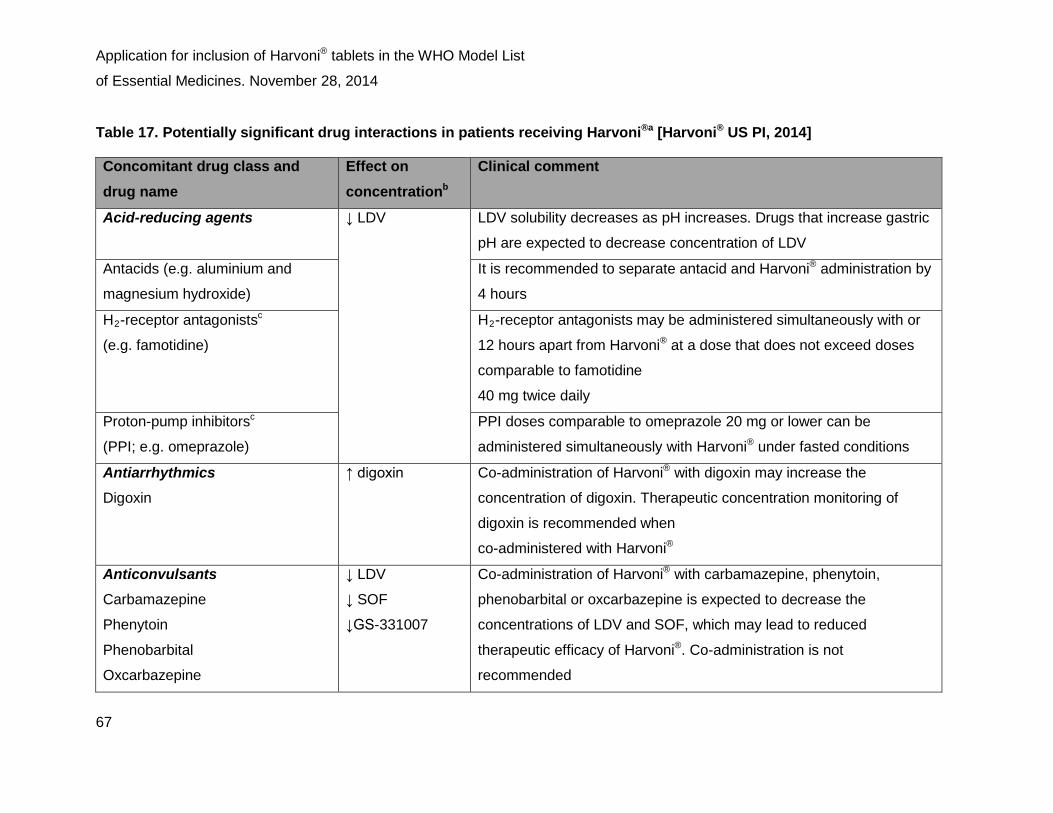
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
67
Table 17. Potentially significant drug interactions in patients receiving Harvoni®a [Harvoni® US PI, 2014]
Concomitant drug class and drug name
Effect on concentrationb
Clinical comment
Acid-reducing agents ↓ LDV
LDV solubility decreases as pH increases. Drugs that increase gastric
pH are expected to decrease concentration of LDV
Antacids (e.g. aluminium and
magnesium hydroxide)
It is recommended to separate antacid and Harvoni® administration by
4 hours
H2-receptor antagonistsc
(e.g. famotidine)
H2-receptor antagonists may be administered simultaneously with or
12 hours apart from Harvoni® at a dose that does not exceed doses
comparable to famotidine
40 mg twice daily
Proton-pump inhibitorsc
(PPI; e.g. omeprazole)
PPI doses comparable to omeprazole 20 mg or lower can be
administered simultaneously with Harvoni® under fasted conditions
Antiarrhythmics
Digoxin
↑ digoxin Co-administration of Harvoni® with digoxin may increase the
concentration of digoxin. Therapeutic concentration monitoring of
digoxin is recommended when
co-administered with Harvoni®
Anticonvulsants Carbamazepine
Phenytoin
Phenobarbital
Oxcarbazepine
↓ LDV
↓ SOF
↓GS-331007
Co-administration of Harvoni® with carbamazepine, phenytoin,
phenobarbital or oxcarbazepine is expected to decrease the
concentrations of LDV and SOF, which may lead to reduced
therapeutic efficacy of Harvoni®. Co-administration is not
recommended

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
68
Antimycobacterials Rifabutin
Rifampin
Rifapentine
↓ LDV
↓ SOF
↓GS-331007
Co-administration of Harvoni® with rifabutin or rifapentine is expected
to decrease the concentrations of LDV and SOF, leading to reduced
therapeutic effect of Harvoni®. Co-administration of Harvoni® with
rifampin, a potent P-gp inducer, is not recommended
HIV antiretrovirals
Efavirenz, emtricitabine,
tenofovir DF
↑ tenofovir Monitor for tenofovir-associated adverse reactions in patients
receiving Harvoni® concomitantly with the combination of efavirenz,
emtricitabine and tenofovir DF. Refer to Viread®, Truvada® or Atripla®
Prescribing Information for recommendations on renal monitoring
Regimens containing tenofovir DF
and an HIV PI/ritonavir
• atazanavir/ritonavir +
emtricitabine/tenofovir DFc
• darunavir/ritonavir +
emtricitabine/tenofovir DFc
• lopinavir/ritonavir +
emtricitabine/tenofovir DF
↑ tenofovir The safety of increased tenofovir concentrations in the setting of
Harvoni® and an HIV PI/ritonavir has not been established.
Consider alternative HCV or ART to avoid increases in tenofovir
exposures. If
co-administration is necessary, monitor for tenofovir-associated
adverse reactions. Refer to Viread® or Truvada® Prescribing
Information for recommendations on renal monitoring
Elvitegravir, cobicistat,
emtricitabine, tenofovir DF
↑ tenofovir The safety of increased tenofovir concentrations in the setting of
Harvoni® and the combination of elvitegravir, cobicistat, emtricitabine
and tenofovir DF has not been established. Co-administration is not
recommended

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
69
Tipranavir/ritonavir ↓ LDV
↓ SOF
↓GS-331007
Co-administration of Harvoni® with tipranavir/ritonavir is expected to
decrease the concentrations of LDV and SOF, leading to reduced
therapeutic effect of Harvoni®.
Co-administration is not recommended
HCV products Simeprevir
↑ LDV
↑ simeprevir
Concentrations of LDV and simeprevir are increased when simeprevir
is
co-administered with LDV. Co-administration of Harvoni® with
simeprevir is not recommended
Herbal supplements St. John’s wort
(Hypericum perforatum)
↓ LDV
↓ SOF
↓GS-331007
Co-administration of Harvoni® with St. John’s wort, a potent P-gp
inducer,
is not recommended
HMG-CoA reductase inhibitors
Rosuvastatin
↑ rosuvastatin Co-administration of Harvoni® with rosuvastatin may significantly
increase the concentration of rosuvastatin, which is associated with an
increased risk of myopathy, including rhabdomyolysis. Co-
administration of Harvoni® with rosuvastatin is not recommended ART, antiretroviral therapy; H2 receptor, histamine receptor; HCV, hepatitis C virus;
HIV, human immunodeficiency virus; HMG-CoA, 3-hydroxy-3-methylglutaryl coenzyme A; LDV, ledipasvir;
P-gp, P-glycoprotein; PI, protease inhibitor; PPI, proton-pump inhibitor; SOF, sofosbuvir;
tenofovir DF, tenofovir disoproxil fumarate
a. This table is not all-inclusive
b. ↓ = decrease; ↑ = increase
c. These interactions have been studied in healthy adults

11.3 Summary of comparative safety
Phase 2 and 3 studies conducted to date have demonstrated that Harvoni® is
well tolerated with an excellent safety profile in a diverse range of patients with chronic
HCV GT 1 infection [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014; Lawitz et al,
2014; Data on file – Gilead Sciences EAME – (HCV13000045); Data on file – Gilead
Sciences EAME – (HCV1300046); Data on file – Gilead Sciences EAME –
(HCV1300047); Data on file – Gilead Sciences EAME – (HCV1300050); Data on file –
Gilead Sciences EAME – (HCV1300097); Data on file – Gilead Sciences EAME –
(HCV13000101); Data on file – Gilead Sciences EAME – (HCV13000103); Data on file –
Gilead Sciences EAME – (HCV13000113); Data on file – Gilead Sciences EAME –
(HCV13000116)].
The advent of the PIs, boceprevir and telaprevir, significantly increased SVR rates in
patients with HCV GT 1 infections receiving PEG-IFN and RBV, including in patients who
had previously failed to respond to treatment [Naggie and Sulkowski, 2012]. However,
triple therapy has been associated with significant additional side effects and drug–drug
interactions, together with stringent dosing requirements and a high pill burden [Butt and
Kanwal, 2012]. The introduction of SOF provided an alternative treatment option
associated with high cure rates and a well-tolerated safety profile, although the
tolerability of SOF has been limited by the requirement for the co-administration of
PEG-IFN. It is noteworthy that very few patients treated with Harvoni® in the Phase 3
ION studies withdrew from treatment due to AEs, and most of those that did were in the
treatment arms receiving 24 weeks of treatment or concomitant RBV [Afdhal et al, 2014b
and 2014c; Kowdley et al, 2014]. The higher rates of AEs, such as anemia, headache,
fatigue, rash, pruritus and insomnia, observed in patients who were co-administered
RBV are consistent with the well-known side effects of RBV therapy. ION study data
suggest that the administration of RBV, in addition to Harvoni®, increases toxicity without
providing substantial additional efficacy benefits. Thus, by administering Harvoni®
without RBV, clinicians may decrease the risk of RBV-related toxicities, reduce the need
for hemoglobin monitoring during treatment, diminish requirements for colony-stimulating
factors and transfusions, and contribute to improved treatment adherence [Kowdley et al,
2014].
Patients with cirrhosis tend to be older, have a lower tolerance to AEs, and experience
more treatment-limiting hematological AEs than those with less advanced disease

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
71
[EASL, 2014b]. Treatment-related toxicities associated with boceprevir and telaprevir are
particularly challenging in cirrhotic patients, resulting in high discontinuation rates
(approximately 12% and 15%, respectively) in patients with HCV GT 1 [Manns and
Cornberg, 2013; Bourliere et al, 2012]. Data from Phase 2 and 3 studies in patients
receiving Harvoni® have demonstrated a low rate of treatment withdrawal due to AEs in
patients with cirrhosis [Afdhal et al, 2014b and 2014c; Kowdley et al, 2014] and a similar
safety profile in patients with decompensated cirrhosis as those without cirrhosis [Data
on file – Gilead Sciences EAME – (HCV1300045)]. Similarly, the treatment of patients
with HIV/HCV co-infection has been limited by the high rate of AEs experienced with
combination therapies and the potential for drug–drug interactions between anti-HCV
and anti-HIV therapies; telaprevir and boceprevir are associated with increased rates of
anemia, rash, pruritus and dysgeusia in this patient population [Naggie and Sulkowski,
2012]. Phase 2 trial data have shown a very low incidence of AEs with Harvoni® in
HIV/HCV co-infected GT 1 patients, regardless of ART status [Data on file – Gilead
Sciences EAME – (HCV13000103)]. These data support the use of Harvoni® in
traditionally hard-to-treat patient populations, including those receiving concomitant
therapies for complex comorbid conditions.
For patients with HCV non-GT 1 infections, safety data for Harvoni® are available for
a small number of patients. Phase 2 study findings in patients with GT 3 infection and
GT 6 infection have been encouraging, suggesting a similarly favorable safety profile to
that in GT 1 patients [Data on file – Gilead Sciences EAME – (HCV1300045); Data on
file – Gilead Sciences EAME – (HCV13000114)].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
72
12. Summary of available data on comparative cost and cost-effectiveness within the pharmacologic class or therapeutic group
12.1 Range of costs of the proposed medicine
12.1.1 USA
The US FDA approved Harvoni® in October 2014 for the treatment of chronic HCV GT 1
infection in adult patients (aged ≥18 years) [Harvoni US PI, 2014].
The monthly treatment cost of Harvoni® tablets varies among payers in the USA.
Table 18 details the wholesale acquisition cost in the USA.
Table 18. Wholesale acquisition costs of Harvoni® in the USA
Dosage form and product strength
Package size Wholesale acquisition cost (US$)
Tablet containing:
90 mg LDV
400 mg SOF
28 tablets
$31,500
LDV, ledipasvir; SOF, sofosbuvir
12.1.2 Developing countries
Gilead’s mission is to transform care for life-threatening diseases, including chronic
HCV, throughout the world. For Harvoni®, which the FDA has designated a breakthrough
therapy for HCV, Gilead is utilizing mechanisms based on the principle that underpinned
its approach to treatment expansion in developing countries, ie, tiered pricing and
voluntary generic licensing. As a result of this approach, 6.7 million people living with
HIV in developing countries are currently receiving a Gilead-based HIV medicine. In
relation to Harvoni®, Gilead has developed a system of tiered pricing based on a
country’s ability to pay. Countries are categorized within bands according to gross

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
73
national income per capita and HCV prevalence and final prices are determined on a
country-by-country needs basis.
In addition, Gilead signed an agreement with seven Indian drug manufacturers in
September 2014 to provide generic versions of Harvoni® for distribution in 91 developing
countries, including India, Egypt, Pakistan and Nigeria, which are home to more than
100 million individuals living with chronic HCV.
Lowering prices, however, is just one aspect of successfully scaling up HCV treatments,
such as Harvoni®. Also critical are in-country activities that support drug availability and
use, including product registration, medical education, demand forecasting and
collaborative research. All of these are elements of Gilead’s treatment access initiatives,
the aim of which is to introduce new medicines quickly.
12.2 Cost-effectiveness of medicines for HCV
Chronic HCV currently affects approximately 3.2 million individuals in the USA, with
17,000 new cases arising each year [CDC, 2014]. With such substantial prevalence,
chronic HCV places a considerable burden on US healthcare resources.
The economic burden of HCV is lower in treated patients compared with untreated
patients [McCombs et al, 2011]. In addition, both direct and indirect healthcare costs
increase in a stepwise fashion with disease progression, with the majority of costs
resulting from end-stage liver diseases [Galbraith et al, 2014; McAdam-Marx et al, 2011;
Gordon et al, 2012]. Treatments for HCV aim to cure patients of their infection and, in so
doing, remove the risk of long-term HCV-related complications and the associated
burden and cost to healthcare providers. The endpoint of HCV treatment is SVR12,
which correlates strongly with permanent clearance of the virus and reduced healthcare
costs. Indeed, extrapolation of modeled data over a 5-year post-treatment period in one
study showed that, among patients with chronic HCV, failure to achieve SVR was
associated with a 13-fold increase in costs and a 56-fold increase in costs in patients
who required retreatment [Backx et al, 2014]. In addition, initiation of HCV therapy at an
earlier stage (i.e. in patients without cirrhosis) yields substantially fewer cases of
HCV-related complications and an estimated reduction in total costs of approximately
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
74
39–46% [Younossi et al, 2014]. Indeed, modeling data for long-term health and
economic outcomes have demonstrated that initiation of Harvoni® therapy at earlier
stages of fibrosis (F0–F1 or F2 versus F3–F4) is associated with estimated absolute
reductions in liver disease progression and related sequelae of 82.2% and 66.1%,
respectively [Data on file – Gilead Sciences EAME – (HCV13000118)].
Until recently, the standard of care for HCV infection was PEG-IFN/RBV, with PI-based
triple therapy for patients with GT 1. However, such regimens have been limited by
variable efficacy, poor tolerability and the unsuitability or unwillingness of many patients
to receive these treatments. With the advent of the next-generation DAAs, including
Sovaldi® and Harvoni®, the potential exists to bridge current treatment gaps and,
importantly, to ®make treatment available to a wider population of chronic HCV patients,
including those who are unable or unwilling to receive IFN. This development is reflected
in recent updates to international treatment guidelines, which recommend Sovaldi® as
the new standard of care for all HCV genotypes and advise against the use of
PEG-IFN/RBV or the first-generation DAAs due to their side-effect profiles and risk of
drug–drug interactions [AASLD Guidelines, 2014].
Cost-effectiveness analyses have demonstrated that the costs of cure with
Harvoni®- and Sovaldi®-based regimens are economically efficient in the short-term
and cost-effective in the longer term compared with other available treatment options.
Harvoni®-based regimens are associated with more favorable health outcomes across
a broad spectrum of patients than comparator therapies, with 25.8–70.0% lower costs
per SVR amongst treatment-naïve patients and substantially lower costs for
treatment-experienced patients (6.5–55.4% and 8.1–48.5% lower, respectively, per
successfully treated patient amongst those who had previously received PEG-IFN/RBV
or PI + PEG-IFN/RBV) [Data on file – Gilead Sciences EAME – (HCV13000120)].
Amongst treatment-naïve patients alone, data suggest that earlier initiation of Harvoni®
therapy (i.e. fibrosis stage F0–F1 or F2 versus F3–F4) confers an estimated
9.6% reduction in the cost per SVR and 14.3–15.9% lower lifetime costs [Data on file –
Gilead Sciences EAME – (HCV13000118)]. Harvoni® therapy is also associated with
additional QALYs, relative to comparator therapies, in both treatment-naïve and
treatment-experienced patients [Data on file – Gilead Sciences EAME –

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
75
(HCV13000120)]. Such findings extend to patients with cirrhosis, in whom both Harvoni®
(GT 1 patients) and Sovaldi® (GT 2, 3 and 4 patients) have demonstrated better
long-term health outcomes, a lower incidence of liver disease complications and greater
cost-efficacy, when compared with current standards of care [Data on file – Gilead
Sciences EAME – (HCV13000111)]. Furthermore, modeling data have suggested that
reduced rates of absenteeism, alone, amongst cirrhotic and non-cirrhotic patients
receiving Harvoni® therapy, as a result of higher SVR12 rates, are associated with
significantly increased work productivity versus baseline and an anticipated economic
gain of $2 billion or more per year in the USA [Data on file – Gilead Sciences EAME –
(HCV13000112)]. Importantly, Harvoni®-based treatment has demonstrated an
incremental cost-effectiveness ratio (ICER) that remains well below $50,000 per QALY
gained, considered the willingness-to-pay threshold for payers in the USA. These
findings indicate that Harvoni® is a cost-effective strategy relative to other available
treatment options, even when variance in clinical, cost and natural history parameters is
taken into account [Data on file – Gilead Sciences EAME – (HCV13000111); Data on file
– Gilead Sciences EAME – (HCV13000120)].
As Harvoni®, like Sovaldi®, has received breakthrough therapy designation by the US
FDA, it seems likely that Harvoni® will achieve a similarly rapid adoption into national and
international treatment guidelines as Sovaldi®. In addition, given the high rates of SVR12
associated with Harvoni® across a wide patient population, including those with
traditionally difficult-to-treat characteristics, Harvoni® may offer a similar level of
cost-effectiveness, with the added benefits of short and simplified all-oral dosing
regimens that do not require the concomitant administration of IFN.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
76
13. Summary of regulatory status of the medicine Table 19. Worldwide Marketing Authorization status for Harvoni® tablets
Territory Approval date Trade name
United States of America October 10, 2014 Harvoni®
Canada October 16, 2014 Harvoni®
European Union November 18, 2014 Harvoni®
14. Availability of pharmacopoeial standards
(British Pharmacopoeia, International Pharmacopoeia, United States Pharmacopoeia)
14.1 Specifications of Harvoni® tablets
European Pharmacopoeia:
US Pharmacopoeia:
In-house standards – see Table 20.
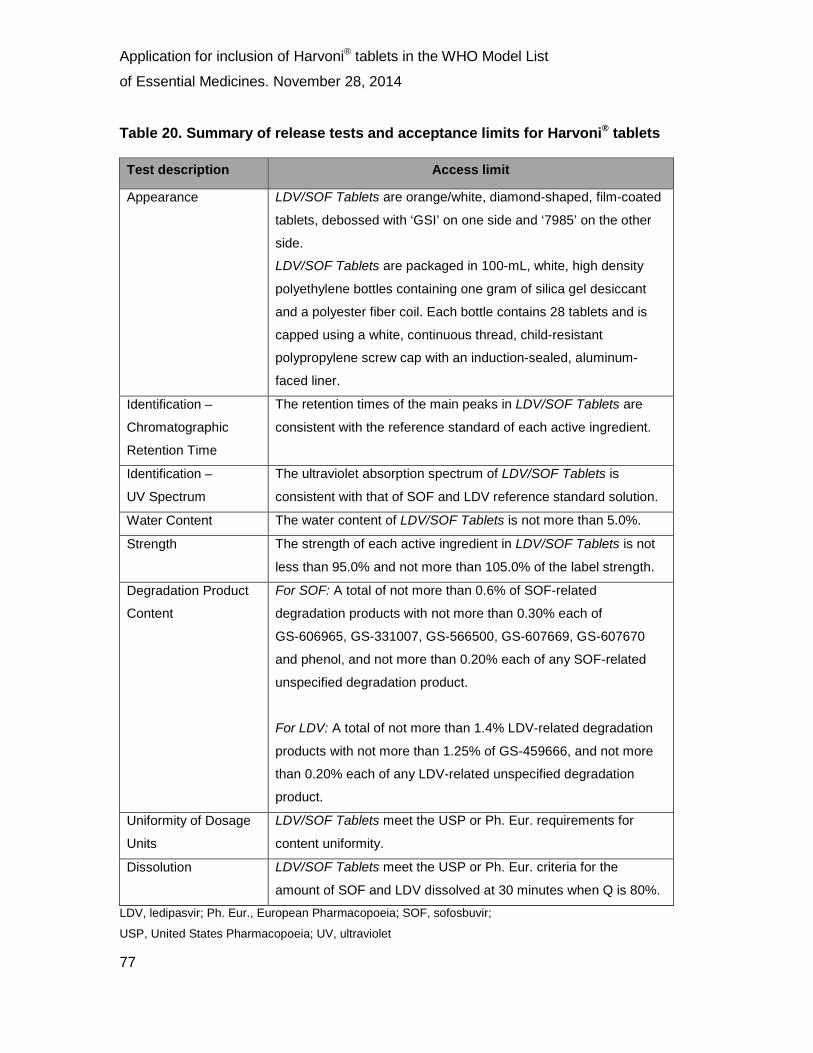
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
77
Table 20. Summary of release tests and acceptance limits for Harvoni® tablets
Test description Access limit
Appearance LDV/SOF Tablets are orange/white, diamond-shaped, film-coated
tablets, debossed with ‘GSI’ on one side and ‘7985’ on the other
side.
LDV/SOF Tablets are packaged in 100-mL, white, high density
polyethylene bottles containing one gram of silica gel desiccant
and a polyester fiber coil. Each bottle contains 28 tablets and is
capped using a white, continuous thread, child-resistant
polypropylene screw cap with an induction-sealed, aluminum-
faced liner.
Identification –
Chromatographic
Retention Time
The retention times of the main peaks in LDV/SOF Tablets are
consistent with the reference standard of each active ingredient.
Identification –
UV Spectrum
The ultraviolet absorption spectrum of LDV/SOF Tablets is
consistent with that of SOF and LDV reference standard solution.
Water Content The water content of LDV/SOF Tablets is not more than 5.0%.
Strength The strength of each active ingredient in LDV/SOF Tablets is not
less than 95.0% and not more than 105.0% of the label strength.
Degradation Product
Content
For SOF: A total of not more than 0.6% of SOF-related
degradation products with not more than 0.30% each of
GS-606965, GS-331007, GS-566500, GS-607669, GS-607670
and phenol, and not more than 0.20% each of any SOF-related
unspecified degradation product.
For LDV: A total of not more than 1.4% LDV-related degradation
products with not more than 1.25% of GS-459666, and not more
than 0.20% each of any LDV-related unspecified degradation
product.
Uniformity of Dosage
Units
LDV/SOF Tablets meet the USP or Ph. Eur. requirements for
content uniformity.
Dissolution LDV/SOF Tablets meet the USP or Ph. Eur. criteria for the
amount of SOF and LDV dissolved at 30 minutes when Q is 80%.
LDV, ledipasvir; Ph. Eur., European Pharmacopoeia; SOF, sofosbuvir;
USP, United States Pharmacopoeia; UV, ultraviolet
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
78
15. Proposed (new/adapted) text for the WHO Model Formulary
15.1 Other antivirals
Ledipasvir/sofosbuvir
Tablet: 90 mg LDV and 400 mg SOF (Table 21).
Also known as HARVONI®.
Uses: Harvoni is licensed in the USA for the treatment of chronic HCV GT 1 infection in
adult patients (aged ≥18 years). In Europe, Harvoni is also indicated for the treatment of
adult patients with chronic HCV GT 4 infection and some GT 3 patients [Harvoni® US PI,
2014; Harvoni® SmPC, 2014].
Precautions: The concomitant use of Harvoni® and P-gp inducers, such as rifampin or
St John’s wort, is not recommended. In addition, the use of Harvoni® in combination with
other drugs containing SOF, including Sovaldi®, is not recommended.
Dose: One tablet taken orally once daily, with or without food.
Table 21. Summary of drugs comprising the Harvoni® STR and the dose of each agent per tablet
Agent Dose per tablet
LDV
SOF
90 mg
400 mg LDV, ledipasvir; SOF, sofosbuvir
Adverse effects: The most common adverse reactions (incidence greater than or equal
to 10%, all grades) observed with treatment with Harvoni® for 8, 12 or 24 weeks were
fatigue and headache.
Please refer to the Prescribing Information appropriate to the Gilead Access Program
contained in Appendix 1 for further details on Harvoni®.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
79
16. References
AASLD Guidelines. Recommendations for Testing, Managing, and Treating Hepatitis C.
Available at: http://HCVguidelines.org. Accessed November 2014.
Afdhal N, Everson G, Calleja JL, et al. Sofosbuvir and ribavirin for the treatment of
chronic HCV with cirrhosis and portal hypertension with and without decompensation:
early virologic response and safety. European Association for the Study of the Liver
2014a oral #64 (Data on file – Gilead Sciences EAME – HCV1300043).
Afdhal N, Reddy R, Nelson D, et al. Ledipasvir and sofosbuvir for previously treated HCV
genotype 1 infection. N Engl J Med 2014b;370:1483–93.
Afdhal N, Zeuzem S, Kwo P, et al. Ledipasvir and sofosbuvir for previously untreated
HCV genotype 1 infection. N Engl J Med 2014c;370:1889–98.
Averhoff FM, Glass N, Holtzman D. Global burden of hepatitis C: Considerations for
healthcare providers in the United States. Clin Infect Dis 2012:55(Suppl 1):S10–15.
Backx M, Lewszuk A, White JR, et al. The cost of treatment failure: resource use and
costs incurred by hepatitis C virus genotype 1-infected patients who do or do not achieve
sustained virological response to therapy. J Viral Hepat 2014;21:208–15.
Bezemer G, Van Gool AR, Verheij-Hart E, et al. Long-term effects of treatment and
response in patients with chronic hepatitis C on quality of life. An international,
multicentre, randomized controlled study. BMC Gastroenterol 2012;12:11.
Bourliere M, Khaloun A, Wartelle-Bladou C, et al. Future treatment of patients with HCV
cirrhosis. Liver Int 2012;32 Suppl 1:113‒9.
Butt AA, Kanwal F. Boceprevir and telaprevir in the management of hepatitis C virus-
infected patients. Clin Infect Dis 2012;54:96–104.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
80
CDC. Hepatitis C FAQs for health professionals. 2014. Available
at: http://www.cdc.gov/hepatitis/hcv/hcvfaq.htm. Accessed November 2014.
CDC. Disease burden from viral hepatitis A, B, and C in the United States 2011.
Available at: http://www.cdc.gov/hepatitis/Statistics/index.htm. Accessed November
2014.
Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int J Med
Sci 2006;3:47‒52.
Cooper CL, Mills E, Wabwire BO, et al. Chronic viral hepatitis may diminish the gains of
HIV antiretroviral therapy in sub-Saharan Africa. Int J Infect Dis 2009;13:302–6.
Data on file – Gilead Sciences EAME – (HCV1300023).
Data on file – Gilead Sciences EAME – (HCV1300031).
Data on file – Gilead Sciences EAME – (HCV1300034).
Data on file – Gilead Sciences EAME – (HCV1300042).
Data on file – Gilead Sciences EAME – (HCV1300044).
Data on file – Gilead Sciences EAME – (HCV1300045).
Data on file – Gilead Sciences EAME – (HCV1300046).
Data on file – Gilead Sciences EAME – (HCV1300047).
Data on file – Gilead Sciences EAME – (HCV1300049).
Data on file – Gilead Sciences EAME – (HCV1300050).

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
81
Data on file – Gilead Sciences EAME – (HCV1300053).
Data on file – Gilead Sciences EAME – (HCV1300057).
Data on file – Gilead Sciences EAME – (HCV1300059).
Data on file – Gilead Sciences EAME – (HCV1300069).
Data on file – Gilead Sciences EAME – (HCV1300070).
Data on file – Gilead Sciences EAME – (HCV1300074).
Data on file – Gilead Sciences EAME – (HCV1300097).
Data on file – Gilead Sciences EAME – (HCV1300098).
Data on file – Gilead Sciences EAME – (HCV13000100).
Data on file – Gilead Sciences EAME – (HCV13000101).
Data on file – Gilead Sciences EAME – (HCV13000103).
Data on file – Gilead Sciences EAME – (HCV13000104).
Data on file – Gilead Sciences EAME – (HCV13000105).
Data on file – Gilead Sciences EAME – (HCV13000106).
Data on file – Gilead Sciences EAME – (HCV13000108).
Data on file – Gilead Sciences EAME – (HCV13000109).
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
82
Data on file – Gilead Sciences EAME – (HCV13000110).
Data on file – Gilead Sciences EAME – (HCV13000111).
Data on file – Gilead Sciences EAME – (HCV13000112).
Data on file – Gilead Sciences EAME – (HCV13000113).
Data on file – Gilead Sciences EAME – (HCV13000114).
Data on file – Gilead Sciences EAME – (HCV13000116).
Data on file – Gilead Sciences EAME – (HCV13000117).
Data on file – Gilead Sciences EAME – (HCV13000118).
Data on file – Gilead Sciences EAME – (HCV13000119).
Data on file – Gilead Sciences EAME – (HCV13000120).
Davis GL, Alter MJ, El-Serag H, et al. Aging of hepatitis C virus (HCV)-infected persons
in the United States: a multiple cohort model of HCV prevalence and disease
progression. Gastroenterology 2010;138:513‒21.
EASL. EASL Clinical Practice Guidelines: Management of hepatitis C virus infection. J
Hepatol 2014a;60:392‒420.
EASL. EASL recommendations on treatment of hepatitis C 2014. 2014b. Available at:
http://files.easl.eu/easl-recommendations-on-treatment-of-hepatitis-C.pdf. Accessed
November 2014.
FDA News Release. FDA approves first combination pill to treat hepatitis C. 10 October,
2014. Available at:
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
83
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm418365.htm.
Accessed November 2014.
Ford N, Kirby C, Singh K, et al. Chronic hepatitis C treatment outcomes in low- and
middle-income countries: a systematic review and meta-analysis. Bull WHO
2012;90:540–50.
Fried MW. Side effects of therapy of hepatitis C and their management. Hepatology
2002;36(5 Suppl 1):S237–44.
Galbraith JW, Donnelly JP, Franco RA, et al. National Estimates of Healthcare Utilization
by Individuals With Hepatitis C Virus Infection in the United States. Clin Infect Dis
2014;59:755–64.
Gibb DM, Goodall RL, Dunn DT, et al. Mother-to-child transmission of hepatitis C virus:
evidence for preventable peripartum transmission. Lancet 2000;356:904–7.
Gilead Press Release. European Commission grants marketing authorization for
Gilead’s Harvoni® (ledipasvir/sofosbuvir), the first single tablet regimen to treat the
majority of chronic hepatitis C patients with genotype 1 and 4. Available
at: http://www.gilead.com/news/press-releases/2014/11/european-commission-grants-
marketing-authorization-for-gileads-harvoni-ledipasvirsofosbuvir-the-first-single-tablet-
regimen-to-treat-the-majority-of-chronic-hepatitis-c-patients-with-genotype-1-and-4.
Accessed November 2014.
Gilead Sciences Inc. Harvoni® US Prescribing Information, October 2014. Available at:
http://www.gilead.com/~/media/Files/pdfs/medicines/liver-disease/harvoni/harvoni_pi.pdf.
Accessed November 2014.
Gilead Sciences Inc. Sovaldi® US Prescribing Information, November 2014. Available
at: http://www.gilead.com/~/media/Files/pdfs/medicines/liver-
disease/sovaldi/sovaldi_pi.pdf. Accessed November 2014.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
84
Gilead Sciences Ltd. Harvoni® Summary of Product Characteristics, November 2014.
Available at: https://www.medicines.org.uk/emc/medicine/29471. Accessed November
2014.
Gordon SC, Pockros PJ, Terrault NA, et al. Impact of disease severity on healthcare
costs in patients with chronic hepatitis C (CHC) virus infection. Hepatology
2012;56:1651–60.
Hauri AM, Armstrong GL, Hutin YJ, et al. The global burden of disease attributable to
contaminated injections given in health care settings. Int J STD AIDS 2004;15:7–16.
Himoto T, Masaki T. Extrahepatic manifestations and autoantibodies in patients with
hepatitis C virus infection. Clin Dev Immunol 2012;2012:871401.
Jacobson IM, Gordon SC, Kowdley KV, et al. Sofosbuvir for hepatitis C genotype 2 or 3
in patients without treatment options. N Engl J Med 2013;368:1867–77.
Karoney MJ, Siika AM. Hepatitis C virus (HCV) infection in Africa: a review. Pan Af Med
J 2013;14:44.
Kowdley KV, Gordon SC, Reddy KR, et al. Ledipasvir and sofosbuvir for 8 or 12 weeks
for chronic HCV without cirrhosis. N Engl J Med 2014;370:1879–88.
Lawitz E, Poordad F, Pang PS, et al. Sofosbuvir and ledipasvir fixed-dose combination
with and without ribavirin in treatment-naïve and previously treated patients with
genotype 1 hepatitis C virus infection (LONESTAR): an open-label, randomised, phase 2
trial. Lancet 2014;383:515–23.
Lawitz E, Lalezari JP, Hassanein T, et al. Sofosbuvir in combination with peginterferon
alfa-2a and ribavirin for non-cirrhotic, treatment-naive patients with genotypes 1, 2, and 3
hepatitis C infection: a randomised, double-blind, phase 2 trial. Lancet Infect Dis
2013;13:401–8.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
85
Lee MH, Yang HI, Lu SN, et al. Chronic hepatitis C virus infection increases mortality
from hepatic and extrahepatic diseases: a community-based long-term prospective
study. J Infect Dis 2012;206:469‒77.
Manns MP, Cornberg M. Sofosbuvir: the final nail in the coffin for hepatitis C? Lancet
Infect Dis 2013;13:378–9.
McAdam-Marx C, McGarry LJ, Hane CA, et al. All-cause and incremental per patient per
year cost associated with chronic hepatitis C virus and associated liver complications in
the United States: a managed care perspective. J Manag Care Pharm 2011;17:531–46.
McCombs JS, Yuan Y, Shin J, et al. Economic burden associated with patients
diagnosed with hepatitis C. Clin Ther 2011;33:1268–80.
Mohd Hanafiah K, Groege J, Flaxman AD, et al. Global prevalence of hepatitis C virus
infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology
2013;57:1333–42.
Mohsen AH, Easterbrook P, Taylor CB, et al. Hepatitis C and HIV-1 co-infection. Gut
2002;51:601–8.
Naggie S, Sulkowski MS. Management of patients coinfected with HCV and HIV: a close
look at the role for direct-acting antivirals. Gastroenterology 2012;142:1324‒34.
Nelson PK, Mathers BM, Corrie B, et al. Global epidemiology of hepatitis B and hepatitis
C in people who inject drugs: results of systematic reviews. Lancet 2011;378:571–83.
North CS, Hong BA, Adewuyi SA, et al. Hepatitis C treatment and SVR: the gap between
clinical trials and real-world treatment aspirations. Gen Hosp Psychiatry 2013;35:122‒8.
Operskalski EA, Kovacs A. HIV/HCV co-infection: pathogenesis, clinical complications,
treatment, and new therapeutic technologies. Curr HIV/AIDS Rep 2011;8:12–22.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
86
Price JC, Thio CL. Liver disease in the HIV-infected individual. Clin Gastroenterol
Hepatol 2010;8:1002–12.
Qureshi H, Bile KM, Jooma R, et al. Prevalence of hepatitis B and C viral infections in
Pakistan: findings of a national survey appealing for effective prevention and control
measures. East Mediterr Health J 2010;16(suppl):S15–23.
Razavi H, Elkhoury AC, Elbasha E, et al. Chronic hepatitis C virus (HCV) disease burden
and cost in the United States. Hepatology 2013;57:2164‒70.
Sievert W, Altraif I, Rezavi HI, et al. A systematic review of hepatitis C virus
epidemiology in Asia, Australia and Egypt. Liver Int 2011;31(Suppl 2):6–80.
UNAIDS. UNAIDS World AIDS Day Report 2012. Available
at: http://www.unaids.org/sites/default/files/media_asset/JC2434_WorldAIDSday_results
_en_1.pdf. Accessed November 2014.
Vietri J, Prajapati G, El Khoury, AC. The burden of hepatitis C in Europe from the
patients’ perspective: a survey in 5 countries. BMC Gastroenterology 2013;13:16.
Villar S, Ortiz-Cuaran S, Abedi-Ardekani B, et al. Aflatoxin-induced TP53 R249S
mutation in hepatocellular carcinoma in Thailand: association with tumors developing in
the absence of liver cirrhosis. PLoS One. 2012;7(6):e37707.
WGO Guidelines. Diagnosis, management and prevention of hepatitis C. April 2013.
Available
at: http://www.worldgastroenterology.org/assets/export/userfiles/WGO_Hepatitis%20C_F
inal%20Version.pdf. Accessed November 2014.
World Health Assembly – Viral hepatitis. WHA63.18. Sixty-third World Health Assembly.
Agenda item 11.12. Geneva: World Health Organization; 2010. Available
at: http://apps.who.int/gb/ebwha/pdf_files/WHA63-REC1/WHA63_REC1-en.pdf.
Accessed November 2014.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
87
WHO Guidelines. Guidelines for the screening, care and treatment of persons with
hepatitis C infection. WHO, April 2014. Available
at: http://www.who.int/hiv/pub/hepatitis/hepatitis-c-guidelines/en/. Accessed November
2014.
WHO Fact Sheet. Hepatitis C. Fact Sheet 164. July 2013. Available
at: http://www.who.int/mediacentre/factsheets/fs164/en/. Accessed November 2014.
Wong KA, Worth A, Martin R, et al. Characterization of Hepatitis C virus resistance from
a multiple-dose clinical trial of the novel NS5A inhibitor GS-5885. Antimicrob Agents
Chemother 2013;57:6333‒40.
Wyles DL. Beyond telaprevir and boceprevir: resistance and new agents for hepatitis C
virus infection. Top Antivir Med 2012;20:139‒45.
Younossi ZM, Stepanova M, Henry L, et al. Effects of sofosbuvir-based treatment, with
or without interferon, on outcome and productivity of patients with chronic hepatitis C.
Zaltron Clin Gastroenterol Hepatol 2014;12:1349–59.
Zaltron S, Spinetti A, Biasi L, et al. Chronic HCV infection: epidemiological and clinical
relevance. BMC Infect Dis 2012;12 Suppl 2:S2.
Zeuzem S, Dusheiko GM, Salupere R, et al. Sofosbuvir and ribavirin in HCV genotypes
2 and 3. N Engl J Med 2014;370:1993–2001.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 88
Appendix 1. Harvoni® Access PI

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 89
FULL PRESCRIBING INFORMATION 1 INDICATIONS AND USAGE HARVONI is indicated for the treatment of chronic hepatitis C (CHC) genotype 1 infection in adults. 2 DOSAGE AND ADMINISTRATION 2.1 Recommended Dosage in Adults HARVONI is a two-drug fixed-dose combination product that contains 90 mg of ledipasvir and 400 mg of sofosbuvir in a single tablet. The recommended dosage of HARVONI is one tablet taken orally once daily with or without food [see Clinical Pharmacology (12.3)]. Duration of Treatment Relapse rates are affected by baseline host and viral factors and differ between treatment durations for certain subgroups [see Clinical Studies (14)]. Table 1 below provides the recommended HARVONI treatment durations for treatment-naïve and treatment-experienced patients and those with and without cirrhosis [see Clinical Studies (14)]. Table 1 Recommended Treatment Duration for HARVONI in Patients with CHC Genotype 1 Patient Population Recommended Treatment Duration Treatment-naïve with or without cirrhosis 12 weeks* Treatment-experienced** without cirrhosis 12 weeks Treatment-experienced** with cirrhosis 24 weeks
* HARVONI for 8 weeks can be considered in treatment-naïve patients without cirrhosis who have pre-treatment HCV RNA less than 6 million IU/mL [see Clinical Studies (14)]. **Treatment-experienced patients who have failed treatment with either peginterferon alfa + ribavirin or an HCV protease inhibitor + peginterferon alfa + ribavirin.
2.2 Severe Renal Impairment and End Stage Renal Disease No dose recommendation can be given for patients with severe renal impairment (estimated Glomerular Filtration Rate [eGFR] <30 mL/min/1.73m2) or with end stage renal disease (ESRD) due to higher exposures (up to 20-fold) of the predominant sofosbuvir metabolite [see Use in Specific Populations (8.6) and Clinical Pharmacology (12.3)]. 3 DOSAGE FORMS AND STRENGTHS HARVONI is available as an orange colored, diamond shaped, film-coated tablet debossed with “GSI” on one side and “7985” on the other side of the tablet. Each tablet contains 90 mg ledipasvir and 400 mg sofosbuvir.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 90
4 CONTRAINDICATIONS None 5 WARNINGS AND PRECAUTIONS 5.1 Risk of Reduced Therapeutic Effect Due to P-gp Inducers The concomitant use of HARVONI and P-gp inducers (e.g., rifampin, St. John’s wort) may significantly decrease ledipasvir and sofosbuvir plasma concentrations and may lead to a reduced therapeutic effect of HARVONI. Therefore, the use of HARVONI with P-gp inducers (e.g., rifampin or St. John’s wort) is not recommended [see Drug Interactions (7.2)]. 5.2 Related Products Not Recommended The use of HARVONI with other products containing sofosbuvir (SOVALDI®) is not recommended. 6 ADVERSE REACTIONS 6.1 Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. The safety assessment of HARVONI was based on pooled data from three Phase 3 clinical trials of subjects with genotype 1 chronic hepatitis C (CHC) with compensated liver disease (with and without cirrhosis) including 215, 539, and 326 subjects who received HARVONI for 8, 12 and 24 weeks, respectively [see Clinical Studies (14)]. The proportion of subjects who permanently discontinued treatment due to adverse events was 0%, <1%, and 1% for subjects receiving HARVONI for 8, 12, and 24 weeks, respectively. The most common adverse reactions (≥10%) were fatigue and headache in subjects treated with 8, 12, or 24 weeks of HARVONI. Table 2 lists adverse reactions (adverse events assessed as causally related by the investigator, all grades) observed in ≥5% of subjects receiving 8, 12, or 24 weeks treatment with HARVONI in clinical trials. The majority of adverse reactions presented in Table 2 occurred at severity of grade 1. The side-by-side tabulation is to simplify presentation; direct comparison across trials should not be made due to differing trial designs.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 91
Table 2 Adverse Reactions (All Grades) Reported in ≥5% of Subjects Receiving 8, 12, or 24 Weeks of Treatment with HARVONI HARVONI
8 weeks HARVONI 12 weeks
HARVONI 24 weeks
N=215 N=539 N=326 Fatigue 16% 13% 18%
Headache 11% 14% 17%
Nausea 6% 7% 9%
Diarrhea 4% 3% 7%
Insomnia 3% 5% 6%
Laboratory Abnormalities
Bilirubin Elevations: Bilirubin elevations of greater than 1.5xULN were observed in 3%, <1%, and 2% of subjects treated with HARVONI for 8, 12, and 24 weeks, respectively.
Lipase Elevations: Transient, asymptomatic lipase elevations of greater than 3xULN were observed in <1%, 2%, and 3% of subjects treated with HARVONI for 8, 12, and 24 weeks, respectively.
Creatine Kinase: Creatine kinase was not assessed in Phase 3 trials of HARVONI. Isolated, asymptomatic creatine kinase elevations (Grade 3 or 4) have been previously reported in subjects treated with sofosbuvir in combination with ribavirin or peginterferon/ribavirin in other clinical trials.
7 DRUG INTERACTIONS 7.1 Potential for Drug Interaction As HARVONI contains ledipasvir and sofosbuvir, any interactions that have been identified with these agents individually may occur with HARVONI. After oral administration of HARVONI, sofosbuvir is rapidly absorbed and subject to extensive first-pass hepatic extraction. In clinical pharmacology studies, both sofosbuvir and the inactive metabolite GS-331007 were monitored for purposes of pharmacokinetic analyses. Ledipasvir is an inhibitor of the drug transporters P-gp and breast cancer resistance protein (BCRP) and may increase intestinal absorption of coadministered substrates for these transporters.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 92
Ledipasvir and sofosbuvir are substrates of drug transporters P-gp and BCRP while GS-331007 is not. P-gp inducers (e.g., rifampin or St. John’s wort) may decrease ledipasvir and sofosbuvir plasma concentrations, leading to reduced therapeutic effect of HARVONI, and the use with P-gp inducers is not recommended with HARVONI [see Warnings and Precautions (5.1)]. 7.2 Established and Potentially Significant Drug Interactions Table 3 provides a listing of established or potentially clinically significant drug interactions. The drug interactions described are based on studies conducted with either HARVONI, the components of HARVONI (ledipasvir and sofosbuvir) as individual agents, or are predicted drug interactions that may occur with HARVONI [see Warnings and Precautions (5.1) and Clinical Pharmacology (12.3)]. Table 3 Potentially Significant Drug Interactions: Alteration in Dose or Regimen May Be Recommended Based on Drug Interaction Studies or Predicted Interactiona Concomitant Drug Class: Drug Name
Effect on Concentrationb
Clinical Comment
Acid Reducing Agents
↓ledipasvir
Ledipasvir solubility decreases as pH increases. Drugs that increase gastric pH are expected to decrease concentration of ledipasvir.
Antacids (e.g., aluminum and magnesium hydroxide)
It is recommended to separate antacid and HARVONI administration by 4 hours.
H2-receptor antagonistsc
(e.g., famotidine)
H2-receptor antagonists may be administered simultaneously with or 12 hours apart from HARVONI at a dose that does not exceed doses comparable to famotidine 40 mg twice daily.
Proton-pump inhibitorsc
(e.g., omeprazole)
Proton-pump inhibitor doses comparable to omeprazole 20 mg or lower can be administered simultaneously with HARVONI under fasted conditions.
Antiarrhythmics: digoxin
↑ digoxin
Coadministration of HARVONI with digoxin may increase the concentration of digoxin. Therapeutic concentration monitoring of digoxin is recommended when coadministered with HARVONI.
Anticonvulsants: carbamazepine phenytoin phenobarbital oxcarbazepine
↓ ledipasvir ↓ sofosbuvir ↓ GS-331007
Coadministration of HARVONI with carbamazepine, phenytoin, phenobarbital, or oxcarbazepine is expected to decrease the concentration of ledipasvir and sofosbuvir, leading to reduced therapeutic effect of HARVONI. Coadministration is not recommended.
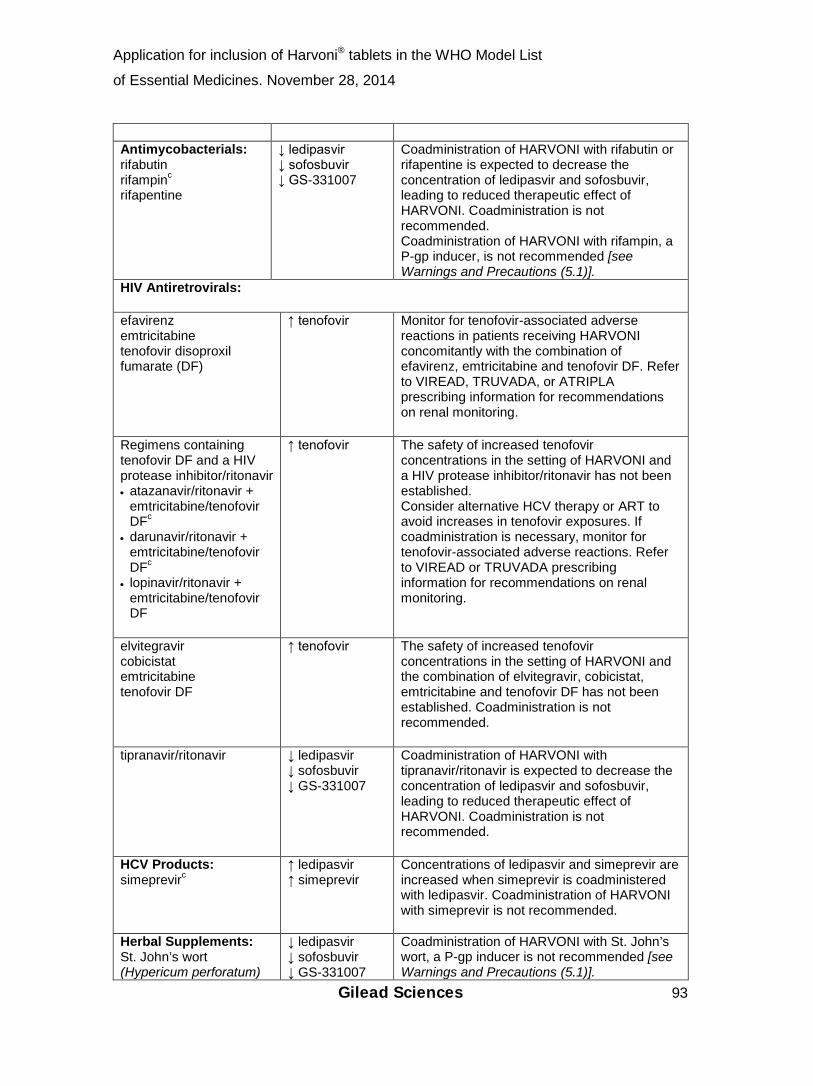
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 93
Antimycobacterials: rifabutin rifampinc
rifapentine
↓ ledipasvir ↓ sofosbuvir ↓ GS-331007
Coadministration of HARVONI with rifabutin or rifapentine is expected to decrease the concentration of ledipasvir and sofosbuvir, leading to reduced therapeutic effect of HARVONI. Coadministration is not recommended. Coadministration of HARVONI with rifampin, a P-gp inducer, is not recommended [see Warnings and Precautions (5.1)].
HIV Antiretrovirals: efavirenz emtricitabine tenofovir disoproxil fumarate (DF)
↑ tenofovir
Monitor for tenofovir-associated adverse reactions in patients receiving HARVONI concomitantly with the combination of efavirenz, emtricitabine and tenofovir DF. Refer to VIREAD, TRUVADA, or ATRIPLA prescribing information for recommendations on renal monitoring.
Regimens containing tenofovir DF and a HIV protease inhibitor/ritonavir • atazanavir/ritonavir +
emtricitabine/tenofovir DFc
• darunavir/ritonavir + emtricitabine/tenofovir DFc
• lopinavir/ritonavir + emtricitabine/tenofovir DF
↑ tenofovir
The safety of increased tenofovir concentrations in the setting of HARVONI and a HIV protease inhibitor/ritonavir has not been established. Consider alternative HCV therapy or ART to avoid increases in tenofovir exposures. If coadministration is necessary, monitor for tenofovir-associated adverse reactions. Refer to VIREAD or TRUVADA prescribing information for recommendations on renal monitoring.
elvitegravir cobicistat emtricitabine tenofovir DF
↑ tenofovir
The safety of increased tenofovir concentrations in the setting of HARVONI and the combination of elvitegravir, cobicistat, emtricitabine and tenofovir DF has not been established. Coadministration is not recommended.
tipranavir/ritonavir
↓ ledipasvir ↓ sofosbuvir ↓ GS-331007
Coadministration of HARVONI with tipranavir/ritonavir is expected to decrease the concentration of ledipasvir and sofosbuvir, leading to reduced therapeutic effect of HARVONI. Coadministration is not recommended.
HCV Products: simeprevirc
↑ ledipasvir ↑ simeprevir
Concentrations of ledipasvir and simeprevir are increased when simeprevir is coadministered with ledipasvir. Coadministration of HARVONI with simeprevir is not recommended.
Herbal Supplements: St. John’s wort (Hypericum perforatum)
↓ ledipasvir ↓ sofosbuvir ↓ GS-331007
Coadministration of HARVONI with St. John’s wort, a P-gp inducer is not recommended [see Warnings and Precautions (5.1)].
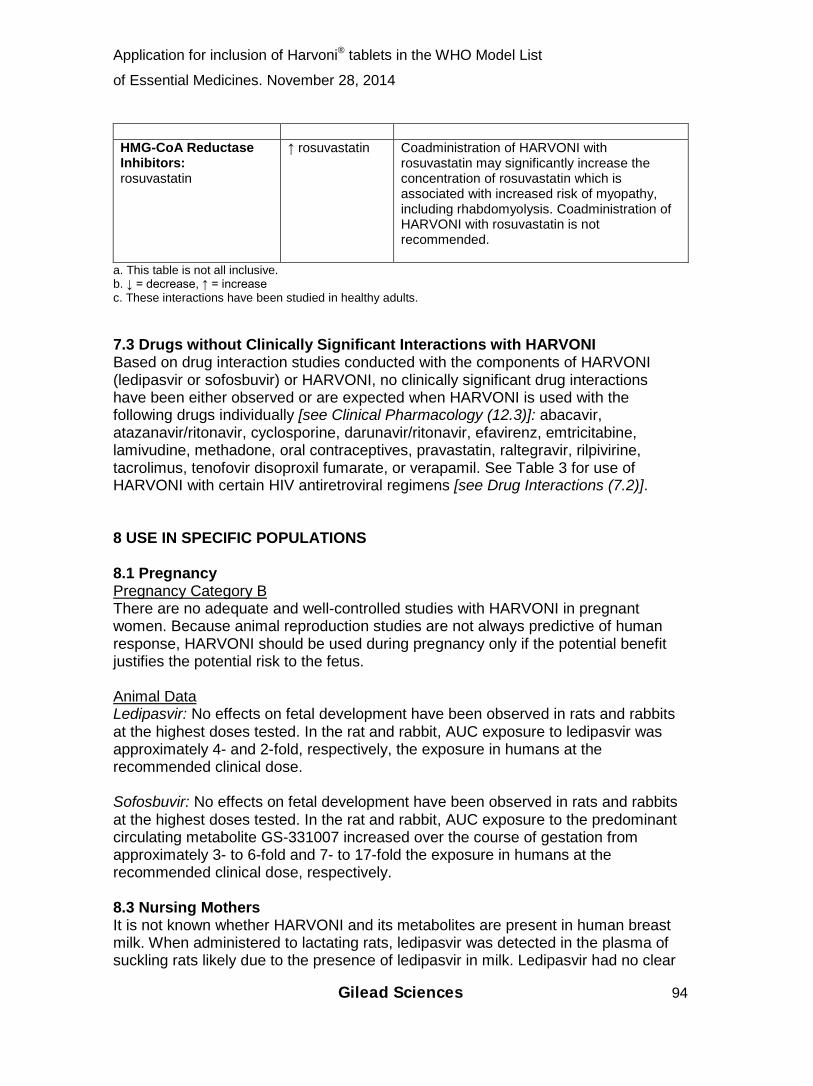
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 94
HMG-CoA Reductase Inhibitors: rosuvastatin
↑ rosuvastatin
Coadministration of HARVONI with rosuvastatin may significantly increase the concentration of rosuvastatin which is associated with increased risk of myopathy, including rhabdomyolysis. Coadministration of HARVONI with rosuvastatin is not recommended.
a. This table is not all inclusive. b. ↓ = decrease, ↑ = increase c. These interactions have been studied in healthy adults. 7.3 Drugs without Clinically Significant Interactions with HARVONI Based on drug interaction studies conducted with the components of HARVONI (ledipasvir or sofosbuvir) or HARVONI, no clinically significant drug interactions have been either observed or are expected when HARVONI is used with the following drugs individually [see Clinical Pharmacology (12.3)]: abacavir, atazanavir/ritonavir, cyclosporine, darunavir/ritonavir, efavirenz, emtricitabine, lamivudine, methadone, oral contraceptives, pravastatin, raltegravir, rilpivirine, tacrolimus, tenofovir disoproxil fumarate, or verapamil. See Table 3 for use of HARVONI with certain HIV antiretroviral regimens [see Drug Interactions (7.2)]. 8 USE IN SPECIFIC POPULATIONS 8.1 Pregnancy Pregnancy Category B There are no adequate and well-controlled studies with HARVONI in pregnant women. Because animal reproduction studies are not always predictive of human response, HARVONI should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Animal Data Ledipasvir: No effects on fetal development have been observed in rats and rabbits at the highest doses tested. In the rat and rabbit, AUC exposure to ledipasvir was approximately 4- and 2-fold, respectively, the exposure in humans at the recommended clinical dose. Sofosbuvir: No effects on fetal development have been observed in rats and rabbits at the highest doses tested. In the rat and rabbit, AUC exposure to the predominant circulating metabolite GS-331007 increased over the course of gestation from approximately 3- to 6-fold and 7- to 17-fold the exposure in humans at the recommended clinical dose, respectively. 8.3 Nursing Mothers It is not known whether HARVONI and its metabolites are present in human breast milk. When administered to lactating rats, ledipasvir was detected in the plasma of suckling rats likely due to the presence of ledipasvir in milk. Ledipasvir had no clear

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 95
effects on the nursing pups. The predominant circulating metabolite of sofosbuvir (GS-331007) was the primary component observed in the milk of lactating rats, without effect on nursing pups. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for HARVONI and any potential adverse effects on the breastfed child from the drug or from the underlying maternal condition. 8.4 Pediatric Use Safety and effectiveness of HARVONI have not been established in pediatric patients. 8.5 Geriatric Use Clinical trials of HARVONI included 117 subjects aged 65 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. No dosage adjustment of HARVONI is warranted in geriatric patients [see Clinical Pharmacology (12.3)]. 8.6 Renal Impairment No dosage adjustment of HARVONI is required for patients with mild or moderate renal impairment. The safety and efficacy of HARVONI have not been established in patients with severe renal impairment (eGFR <30 mL/min/1.73m2) or ESRD requiring hemodialysis. No dosage recommendation can be given for patients with severe renal impairment or ESRD [see Dosage and Administration (2.2) and Clinical Pharmacology (12.3)]. 8.7 Hepatic Impairment No dosage adjustment of HARVONI is required for patients with mild, moderate, or severe hepatic impairment (Child-Pugh Class A, B, or C). Safety and efficacy of HARVONI have not been established in patients with decompensated cirrhosis [see Clinical Pharmacology (12.3)]. 10 OVERDOSAGE No specific antidote is available for overdose with HARVONI. If overdose occurs the patient must be monitored for evidence of toxicity. Treatment of overdose with HARVONI consists of general supportive measures including monitoring of vital signs as well as observation of the clinical status of the patient. Hemodialysis is unlikely to result in significant removal of ledipasvir since ledipasvir is highly bound to plasma protein. Hemodialysis can efficiently remove the predominant circulating metabolite of sofosbuvir, GS-331007, with an extraction ratio of 53%. 11 DESCRIPTION HARVONI is a fixed-dose combination tablet containing ledipasvir and sofosbuvir for oral administration. Ledipasvir is an HCV NS5A inhibitor and sofosbuvir is a nucleotide analog inhibitor of HCV NS5B polymerase.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 96
Each tablet contains 90 mg ledipasvir and 400 mg sofosbuvir. The tablets include the following inactive ingredients: colloidal silicon dioxide, copovidone, croscarmellose sodium, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablets are film-coated with a coating material containing the following inactive ingredients: FD&C yellow #6/sunset yellow FCF aluminum lake, polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide. Ledipasvir: The IUPAC name for ledipasvir is Methyl [(2S)-1-{(6S)-6-[5-(9,9-difluoro-7-{2-[(1R,3S,4S)-2-{(2S)-2-[(methoxycarbonyl)amino]-3-methylbutanoyl}-2-azabicyclo[2.2.1]hept-3-yl]-1H-benzimidazol-6-yl}-9H-fluoren-2-yl)-1H-imidazol-2-yl]-5-azaspiro[2.4]hept-5-yl}-3-methyl-1-oxobutan-2-yl]carbamate. It has a molecular formula of C49H54F2N8O6 and a molecular weight of 889.00. It has the following structural formula:
Ledipasvir is practically insoluble (<0.1 mg/mL) across the pH range of 3.0–7.5 and is slightly soluble below pH 2.3 (1.1 mg/mL). Sofosbuvir: The IUPAC name for sofosbuvir is (S)-Isopropyl 2-((S)-(((2R,3R,4R,5R)-5- (2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl)-4-fluoro-3-hydroxy-4-methyltetrahydrofuran-2- yl)methoxy)-(phenoxy)phosphorylamino)propanoate. It has a molecular formula of C22H29FN3O9P and a molecular weight of 529.45. It has the following structural formula:
Sofosbuvir is a white to off-white crystalline solid with a solubility of ≥2 mg/mL across the pH range of 2–7.7 at 37°C and is slightly soluble in water.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 97
12 CLINICAL PHARMACOLOGY 12.1 Mechanism of Action HARVONI is a fixed-dose combination of ledipasvir and sofosbuvir which are direct-acting antiviral agents against the hepatitis C virus [see Microbiology (12.4)]. 12.2 Pharmacodynamics Cardiac Electrophysiology Thorough QT studies have been conducted for ledipasvir and sofosbuvir. The effect of ledipasvir 120 mg twice daily (2.67 times the maximum recommended dosage) for 10 days on QTc interval was evaluated in a randomized, multiple-dose, placebo-, and active-controlled (moxifloxacin 400 mg) three period crossover thorough QT trial in 59 healthy subjects. At the dose of 120 mg twice daily (2.67 times the maximum recommended dosage), ledipasvir does not prolong QTc interval to any clinically relevant extent. The effect of sofosbuvir 400 mg (maximum recommended dosage) and 1200 mg (three times the maximum recommended dosage) on QTc interval was evaluated in a randomized, single-dose, placebo-, and active-controlled (moxifloxacin 400 mg) four period crossover thorough QT trial in 59 healthy subjects. At a dose three times the maximum recommended dose, sofosbuvir does not prolong QTc to any clinically relevant extent. 12.3 Pharmacokinetics Absorption The pharmacokinetic properties of ledipasvir, sofosbuvir, and the predominant circulating metabolite GS-331007 have been evaluated in healthy adult subjects and in subjects with chronic hepatitis C. Following oral administration of HARVONI, ledipasvir median peak concentrations were observed 4 to 4.5 hours post-dose. Sofosbuvir was absorbed quickly and the peak median plasma concentration was observed ~0.8 to 1 hour post-dose. Median peak plasma concentration of GS-331007 was observed between 3.5 to 4 hours post-dose. Based on the population pharmacokinetic analysis in HCV-infected subjects, geometric mean steady-state AUC0-24 for ledipasvir (N=2113), sofosbuvir (N=1542), and GS-331007 (N=2113) were 7290, 1320, and 12,000 ng•hr/mL, respectively. Steady-state Cmax for ledipasvir, sofosbuvir, and GS-331007 were 323, 618, and 707 ng/mL, respectively. Sofosbuvir and GS-331007 AUC0-24 and Cmax were similar in healthy adult subjects and subjects with HCV infection. Relative to healthy subjects (N=191), ledipasvir AUC0-24 and Cmax were 24% lower and 32% lower, respectively, in HCV-infected subjects. Effect of Food Relative to fasting conditions, the administration of a single dose of HARVONI with a moderate fat (~600 kcal, 25% to 30% fat) or high fat (~1000 kcal, 50% fat) meal increased sofosbuvir AUC0-inf by approximately 2-fold, but did not significantly affect sofosbuvir Cmax. The exposures of GS-331007 and ledipasvir were not altered in

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 98
the presence of either meal type. The response rates in Phase 3 trials were similar in HCV-infected subjects who received HARVONI with food or without food. HARVONI can be administered without regard to food. Distribution Ledipasvir is >99.8% bound to human plasma proteins. After a single 90 mg dose of [14C]-ledipasvir in healthy subjects, the blood to plasma ratio of 14C-radioactivity ranged between 0.51 and 0.66. Sofosbuvir is approximately 61–65% bound to human plasma proteins and the binding is independent of drug concentration over the range of 1 μg/mL to 20 μg/mL. Protein binding of GS-331007 was minimal in human plasma. After a single 400 mg dose of [14C]-sofosbuvir in healthy subjects, the blood to plasma ratio of 14C-radioactivity was approximately 0.7. Metabolism In vitro, no detectable metabolism of ledipasvir was observed by human CYP1A2, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and CYP3A4. Evidence of slow oxidative metabolism via an unknown mechanism has been observed. Following a single dose of 90 mg [14C]-ledipasvir, systemic exposure was almost exclusively to the parent drug (>98%). Unchanged ledipasvir is the major species present in feces. Sofosbuvir is extensively metabolized in the liver to form the pharmacologically active nucleoside analog triphosphate GS-461203. The metabolic activation pathway involves sequential hydrolysis of the carboxyl ester moiety catalyzed by human cathepsin A (CatA) or carboxylesterase 1 (CES1) and phosphoramidate cleavage by histidine triad nucleotide-binding protein 1 (HINT1) followed by phosphorylation by the pyrimidine nucleotide biosynthesis pathway. Dephosphorylation results in the formation of nucleoside metabolite GS-331007 that cannot be efficiently rephosphorylated and lacks anti-HCV activity in vitro. After a single 400 mg oral dose of [14C]-sofosbuvir, GS-331007 accounted for approximately >90% of total systemic exposure. Elimination Following a single 90 mg oral dose of [14C]-ledipasvir, mean total recovery of the [14C]-radioactivity in feces and urine was approximately 87%, with most of the radioactive dose recovered from feces (approximately 86%). Unchanged ledipasvir excreted in feces accounted for a mean of 70% of the administered dose and the oxidative metabolite M19 accounted for 2.2% of the dose. These data indicate that biliary excretion of unchanged ledipasvir is a major route of elimination, with renal excretion being a minor pathway (approximately 1%). The median terminal half-life of ledipasvir following administration of HARVONI was 47 hours. Following a single 400 mg oral dose of [14C]-sofosbuvir, mean total recovery of the dose was greater than 92%, consisting of approximately 80%, 14%, and 2.5% recovered in urine, feces, and expired air, respectively. The majority of the sofosbuvir dose recovered in urine was GS-331007 (78%) while 3.5% was recovered as sofosbuvir. These data indicate that renal clearance is the major

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 99
elimination pathway for GS-331007. The median terminal half-lives of sofosbuvir and GS-331007 following administration of HARVONI were 0.5 and 27 hours, respectively. Specific Populations
Patients with Renal Impairment: The pharmacokinetics of ledipasvir were studied with a single dose of 90 mg ledipasvir in HCV negative subjects with severe renal impairment (eGFR <30 mL/min by Cockcroft-Gault). No clinically relevant differences in ledipasvir pharmacokinetics were observed between healthy subjects and subjects with severe renal impairment.
The pharmacokinetics of sofosbuvir were studied in HCV negative subjects with mild (eGFR ≥50 and <80 mL/min/1.73m2), moderate (eGFR ≥30 and <50 mL/min/1.73m2), severe renal impairment (eGFR <30 mL/min/1.73m2), and subjects with ESRD requiring hemodialysis following a single 400 mg dose of sofosbuvir. Relative to subjects with normal renal function (eGFR >80 mL/min/1.73m2), the sofosbuvir AUC0-inf was 61%, 107%, and 171% higher in mild, moderate, and severe renal impairment, while the GS-331007 AUC0-inf was 55%, 88%, and 451% higher, respectively. In subjects with ESRD, relative to subjects with normal renal function, sofosbuvir and GS-331007 AUC0-inf was 28% and 1280% higher when sofosbuvir was dosed 1 hour before hemodialysis compared with 60% and 2070% higher when sofosbuvir was dosed 1 hour after hemodialysis, respectively. A 4 hour hemodialysis session removed approximately 18% of administered dose [see Dosage and Administration (2.2) and Use in Specific Populations (8.6)].
Race: Population pharmacokinetics analysis in HCV-infected subjects indicated that race had no clinically relevant effect on the exposure of ledipasvir, sofosbuvir, and GS-331007.
Gender: Population pharmacokinetics analysis in HCV-infected subjects indicated that gender had no clinically relevant effect on the exposure of sofosbuvir and GS-331007. AUC and Cmax of ledipasvir were 77% and 58% higher, respectively, in females than males; however, the relationship between gender and ledipasvir exposures was not considered clinically relevant, as high response rates (SVR >90%) were achieved in male and female subjects across the Phase 3 studies and the safety profiles are similar in females and males.
Pediatric Patients: The pharmacokinetics of ledipasvir or sofosbuvir in pediatric patients has not been established [see Use in Specific Populations (8.4)].
Geriatric Patients: Population pharmacokinetic analysis in HCV-infected subjects showed that within the age range (18 to 80 years) analyzed, age
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 100
did not have a clinically relevant effect on the exposure to ledipasvir, sofosbuvir, and GS-331007 [see Use in Specific Populations (8.5)].
Patients with Hepatic Impairment: The pharmacokinetics of ledipasvir were studied with a single dose of 90 mg ledipasvir in HCV negative subjects with severe hepatic impairment (Child-Pugh Class C). Ledipasvir plasma exposure (AUC0-inf) was similar in subjects with severe hepatic impairment and control subjects with normal hepatic function. Population pharmacokinetics analysis in HCV-infected subjects indicated that cirrhosis had no clinically relevant effect on the exposure of ledipasvir [see Use in Specific Populations (8.7)].
The pharmacokinetics of sofosbuvir were studied following 7-day dosing of 400 mg sofosbuvir in HCV-infected subjects with moderate and severe hepatic impairment (Child-Pugh Class B and C). Relative to subjects with normal hepatic function, the sofosbuvir AUC0-24 were 126% and 143% higher in moderate and severe hepatic impairment, while the GS-331007 AUC0-24 were 18% and 9% higher, respectively. Population pharmacokinetics analysis in HCV-infected subjects indicated that cirrhosis had no clinically relevant effect on the exposure of sofosbuvir and GS-331007 [see Use in Specific Populations (8.7)].
Drug Interaction Studies Ledipasvir and sofosbuvir are substrates of drug transporters P-gp and BCRP while GS-331007 is not. P-gp inducers (e.g., rifampin or St. John’s wort) may decrease ledipasvir and sofosbuvir plasma concentrations, leading to reduced therapeutic effect of HARVONI, and the use with P-gp inducers is not recommended with HARVONI [see Warnings and Precautions (5.1)]. Coadministration with drugs that inhibit P-gp and/or BCRP may increase ledipasvir and sofosbuvir plasma concentrations without increasing GS-331007 plasma concentration; HARVONI may be coadministered with P-gp and/or BCRP inhibitors. Neither ledipasvir nor sofosbuvir is a substrate for hepatic uptake transporters OCT1, OATP1B1, or OATP1B3. GS-331007 is not a substrate for renal transporters, including organic anion transporter OAT1 or OAT3, or organic cation transporter OCT2. Ledipasvir is subject to slow oxidative metabolism via an unknown mechanism. In vitro, no detectable metabolism of ledipasvir by CYP enzymes has been observed. Biliary excretion of unchanged ledipasvir is a major route of elimination. Sofosbuvir is not a substrate for CYP and UGT1A1 enzymes. Clinically significant drug interactions with HARVONI mediated by CYP or UGT1A1 enzymes are not expected. The effects of coadministered drugs on the exposure of ledipasvir, sofosbuvir, and GS-331007 are shown in Table 4 [see Drug Interactions (7.2)].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 101
Table 4 Drug Interactions: Changes in Pharmacokinetic Parameters for Ledipasvir, Sofosbuvir, and the Predominant Circulating Metabolite GS-331007 in the Presence of the Coadministered Druga

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 102
NA = not available/not applicable, ND = not dosed. a. All interaction studies conducted in healthy volunteers. b. Administered as ATRIPLA®
(efavirenz, emtricitabine, tenofovir DF). c. This study was conducted in the presence of two other investigational HCV direct-acting agents. No effect on the pharmacokinetic parameters of ledipasvir, sofosbuvir, and GS-331007 was observed with the combination of abacavir and lamivudine, or emtricitabine, rilpivirine, and tenofovir DF, or raltegravir. Ledipasvir is an inhibitor of drug transporter P-gp and breast cancer resistance protein (BCRP) and may increase intestinal absorption of coadministered substrates for these transporters. Ledipasvir is an inhibitor of transporters OATP1B1, OATP1B3, and BSEP only at concentrations exceeding those achieved in clinic. Ledipasvir is not an inhibitor of transporters MRP2, MRP4, OCT2, OAT1, OAT3, MATE1, and OCT1. The drug-drug interaction potential of ledipasvir is primarily limited to the intestinal inhibition of P-gp and BCRP. Clinically relevant transporter inhibition by ledipasvir in the systemic circulation is not expected due to its high protein binding. Sofosbuvir and GS-331007 are not inhibitors of drug transporters P-gp, BCRP, MRP2, BSEP, OATP1B1, OATP1B3, and OCT1, and GS-331007 is not an inhibitor of OAT1, OCT2, and MATE1. Ledipasvir, sofosbuvir, and GS-331007 are not inhibitors or inducers of CYP or UGT1A1 enzymes. The effects of ledipasvir or sofosbuvir on the exposure of coadministered drugs are shown in Table 5 [see Drug Interactions (7.2)].
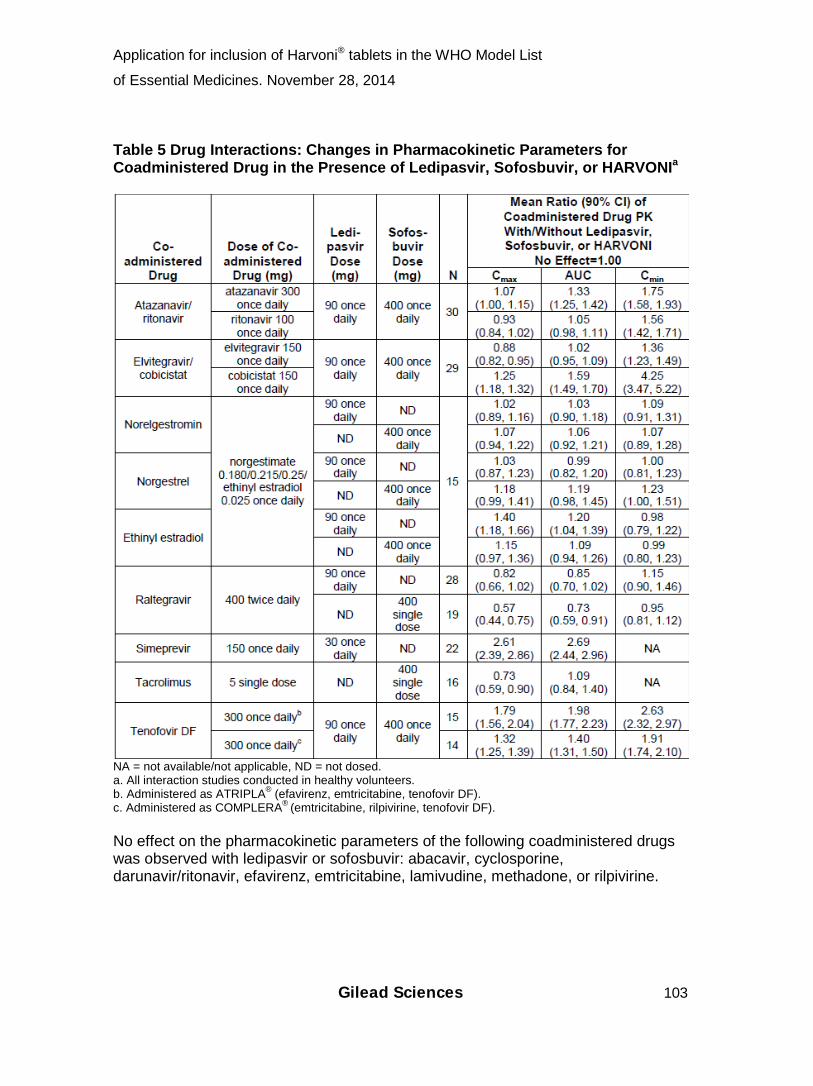
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 103
Table 5 Drug Interactions: Changes in Pharmacokinetic Parameters for Coadministered Drug in the Presence of Ledipasvir, Sofosbuvir, or HARVONIa
NA = not available/not applicable, ND = not dosed. a. All interaction studies conducted in healthy volunteers. b. Administered as ATRIPLA® (efavirenz, emtricitabine, tenofovir DF). c. Administered as COMPLERA®
(emtricitabine, rilpivirine, tenofovir DF). No effect on the pharmacokinetic parameters of the following coadministered drugs was observed with ledipasvir or sofosbuvir: abacavir, cyclosporine, darunavir/ritonavir, efavirenz, emtricitabine, lamivudine, methadone, or rilpivirine.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 104
12.4 Microbiology Mechanism of Action Ledipasvir is an inhibitor of the HCV NS5A protein, which is required for viral replication. Resistance selection in cell culture and cross-resistance studies indicate ledipasvir targets NS5A as its mode of action. Sofosbuvir is an inhibitor of the HCV NS5B RNA-dependent RNA polymerase, which is required for viral replication. Sofosbuvir is a nucleotide prodrug that undergoes intracellular metabolism to form the pharmacologically active uridine analog triphosphate (GS-461203), which can be incorporated into HCV RNA by the NS5B polymerase and acts as a chain terminator. In a biochemical assay, GS-461203 inhibited the polymerase activity of the recombinant NS5B from HCV genotypes 1b, 2a, 3a and 4a with IC50 values ranging from 0.7 to 2.6 μM. GS-461203 is neither an inhibitor of human DNA and RNA polymerases nor an inhibitor of mitochondrial RNA polymerase. Antiviral Activity In HCV replicon assays, the EC50 values of ledipasvir against full-length replicons from genotypes 1a and 1b were 0.031 nM and 0.004 nM, respectively. The median EC50 values of ledipasvir against chimeric replicons encoding NS5A sequences from clinical isolates were 0.018 nM for genotype 1a (range 0.009–0.085 nM; N=30) and 0.006 nM for genotype 1b (range 0.004–0.007 nM; N=3). Ledipasvir has less antiviral activity compared to genotype 1 against genotypes 4a, 5a, and 6a, with EC50 values of 0.39 nM, 0.15 nM, and 1.1 nM, respectively. Ledipasvir has substantially lower activity against genotypes 2a, 2b, 3a, and 6e with EC50 values of 21–249 nM, 16–530 nM, 168 nM, and 264 nM, respectively. In HCV replicon assays, the EC50 values of sofosbuvir against full-length replicons from genotypes 1a, 1b, 2a, 3a, and 4a, and chimeric 1b replicons encoding NS5B from genotypes 2b, 5a, or 6a ranged from 14–110 nM. The median EC50 value of sofosbuvir against chimeric replicons encoding NS5B sequences from clinical isolates was 62 nM for genotype 1a (range 29–128 nM; N=67), 102 nM for genotype 1b (range 45–170 nM; N=29), 29 nM for genotype 2 (range 14–81 nM; N=15), and 81 nM for genotype 3a (range 24–181 nM; N=106). In replication competent virus assays, the EC50 values of sofosbuvir against genotypes 1a and 2a were 30 nM and 20 nM, respectively. Evaluation of sofosbuvir in combination with ledipasvir showed no antagonistic effect in reducing HCV RNA levels in replicon cells. Resistance
In Cell Culture HCV replicons with reduced susceptibility to ledipasvir have been selected in cell culture for genotypes 1a and 1b. Reduced susceptibility to ledipasvir was associated with the primary NS5A amino acid substitution Y93H in both genotypes 1a and 1b. Additionally, a Q30E substitution emerged in genotype 1a replicons. Site-directed mutagenesis of the Y93H in both genotypes 1a and 1b, as well as the Q30E substitution in genotype 1a,
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 105
conferred high levels of reduced susceptibility to ledipasvir (fold change in EC50 greater than 1000-fold). HCV replicons with reduced susceptibility to sofosbuvir have been selected in cell culture for multiple genotypes including 1b, 2a, 2b, 3a, 4a, 5a, and 6a. Reduced susceptibility to sofosbuvir was associated with the primary NS5B substitution S282T in all replicon genotypes examined. Site-directed mutagenesis of the S282T substitution in replicons of 8 genotypes conferred 2- to 18-fold reduced susceptibility to sofosbuvir.
In Clinical Trials In a pooled analysis of subjects who received HARVONI in Phase 3 trials, 37 subjects (29 with genotype 1a and 8 with genotype 1b) qualified for resistance analysis due to virologic failure (35 with virologic relapse, 2 with breakthrough on-treatment due to documented non-adherence). Post-baseline NS5A and NS5B deep sequencing data (assay cutoff of 1%) were available for 37/37 and 36/37 subjects’ viruses, respectively.
Of the 29 genotype 1a virologic failure subjects, 55% (16/29) of subjects had virus with emergent NS5A resistance-associated substitutions K24R, M28T/V, Q30R/H/K/L, L31M, or Y93H/N at failure. Five of these 16 subjects also had baseline NS5A polymorphisms at resistance-associated amino acid positions. The most common substitutions detected at failure were Q30R, Y93H or N, and L31M.
Of the 8 genotype 1b virologic failure subjects, 88% (7/8) had virus with emergent NS5A resistance-associated substitutions L31V/M/I or Y93H at failure. Three of these 7 subjects also had baseline NS5A polymorphisms at resistance-associated positions. The most common substitution detected at failure was Y93H.
At failure, 38% (14/37) of virologic failure subjects had 2 or more NS5A substitutions at resistance-associated positions.
In phenotypic analyses, post-baseline isolates from subjects who harbored NS5A resistance-associated substitutions at failure showed 20- to >243-fold reduced susceptibility to ledipasvir.
Treatment-emergent NS5B substitutions L159 (n=1) and V321 (n=2) previously associated with sofosbuvir failure were detected in the Phase 3 trials. In addition, NS5B substitutions at highly conserved positions D61G (n=3), A112T (n=2), E237G (n=2), and S473T (n=1) were detected at low frequency by next generation sequencing in treatment failure subjects infected with HCV GT1a. The D61G substitution was previously described in subjects infected with HCV GT1a in a liver pre-transplant trial. The clinical significance of these substitutions is currently unknown.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 106
The sofosbuvir-associated resistance substitution S282T in NS5B was not detected in any failure isolate from the Phase 3 trials. NS5B substitutions S282T, L320V/I, and V321I in combination with NS5A substitutions L31M, Y93H, and Q30L were detected in one subject at failure following 8 weeks of treatment with HARVONI in a Phase 2 trial.
Cross Resistance Ledipasvir was fully active against the sofosbuvir resistance-associated substitution S282T in NS5B while all ledipasvir resistance-associated substitutions in NS5A were fully susceptible to sofosbuvir. Both sofosbuvir and ledipasvir were fully active against substitutions associated with resistance to other classes of direct-acting antivirals with different mechanisms of actions, such as NS5B non-nucleoside inhibitors and NS3 protease inhibitors. NS5A substitutions conferring resistance to ledipasvir may reduce the antiviral activity of other NS5A inhibitors. The efficacy of ledipasvir/sofosbuvir has not been established in patients who have previously failed treatment with other regimens that include an NS5A inhibitor. Persistence of Resistance-Associated Substitutions No data are available on the persistence of ledipasvir or sofosbuvir resistance-associated substitutions. NS5A resistance-associated substitutions for other NS5A inhibitors have been found to persist for >1 year in some patients. Effect of Baseline HCV Polymorphisms on Treatment Response Analyses were conducted to explore the association between pre-existing baseline NS5A polymorphisms at resistance-associated positions and relapse rates. In the pooled analysis of the Phase 3 trials, 23% (370/1589) of subjects’ virus had baseline NS5A polymorphisms at resistance-associated positions (any change from reference at NS5A amino acid positions 24, 28, 30, 31, 58, 92, or 93) identified by population or deep sequencing. In treatment-naïve subjects whose virus had baseline NS5A polymorphisms at resistance-associated positions in Studies ION-1 and ION-3, relapse rates were 6% (3/48) after 8 weeks and 1% (1/113) after 12 weeks of treatment with HARVONI. Relapse rates among subjects without baseline NS5A polymorphisms at resistance-associated positions were 5% (8/167) after 8 weeks and 1% (3/306) after 12 weeks treatment with HARVONI. In treatment-experienced subjects whose virus had baseline NS5A polymorphisms at resistance-associated positions, relapse rates were 22% (5/23) after 12 weeks and 0% (0/19) after 24 weeks of treatment with HARVONI. The specific baseline NS5A resistance-associated polymorphisms observed among subjects with relapse were M28T/V, Q30H, Q30R, L31M, H58P, Y93H, and Y93N in genotype 1a, and L28M, A92T, and Y93H in genotype 1b. Subjects with multiple NS5A polymorphisms at resistance-associated positions appeared to have higher relapse rates.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 107
SVR was achieved in all 24 subjects (N=20 with L159F+C316N; N=1 with L159F; and N=3 with N142T) who had baseline polymorphisms associated with resistance to NS5B nucleoside inhibitors. The sofosbuvir resistance-associated substitution S282T was not detected in the baseline NS5B sequence of any subject in Phase 3 trials by population or deep sequencing. 13 NONCLINICAL TOXICOLOGY 13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility Carcinogenesis and Mutagenesis Ledipasvir: Ledipasvir was not genotoxic in a battery of in vitro or in vivo assays, including bacterial mutagenicity, chromosome aberration using human peripheral blood lymphocytes, and in vivo rat micronucleus assays. Carcinogenicity studies of ledipasvir in mice and rats are ongoing. Sofosbuvir: Sofosbuvir was not genotoxic in a battery of in vitro or in vivo assays, including bacterial mutagenicity, chromosome aberration using human peripheral blood lymphocytes and in vivo mouse micronucleus assays. Two-year carcinogenicity studies in mice and rats were conducted with sofosbuvir. Mice were administered doses of up to 200 mg/kg/day in males and 600 mg/kg/day in females, while rats were administered doses of up to 750 mg/kg/day in males and females. No increase in the incidence of drug-related neoplasms were observed at the highest doses tested in mice and rats, resulting in AUC exposure to the predominant circulating metabolite GS-331007 of approximately 4- and 18-fold (in mice) and 8- and 10-fold (in rats), in males and females respectively, the exposure in humans at the recommended clinical dose. Impairment of Fertility Ledipasvir: Ledipasvir had no adverse effects on mating and fertility. In female rats, the mean number of corpora lutea and implantation sites were reduced slightly at maternal exposures approximately 3-fold the exposure in humans at the recommended clinical dose. At the highest dose levels without effects, AUC exposure to ledipasvir was approximately 5- and 2-fold, in males and females, respectively, the exposure in humans at the recommended clinical dose. Sofosbuvir: Sofosbuvir had no effects on embryo-fetal viability or on fertility when evaluated in rats. At the highest dose tested, AUC exposure to the predominant circulating metabolite GS-331007 was approximately 5-fold the exposure in humans at the recommended clinical dose. 13.2 Animal Toxicology and/or Pharmacology Sofosbuvir: Heart degeneration and inflammation were observed in rats following GS-9851 (a stereoisomeric mixture containing approximately 50% sofosbuvir) doses of 2,000 mg/kg/day for up to 5 days. At this dose, AUC exposure to the predominant circulating metabolite GS-331007 is approximately 17-fold higher than human exposure at the recommended clinical dose. No heart degeneration or

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 108
inflammation was observed in mice, rats, or dogs in studies up to 3 months, 6 months, or 9 months at GS-331007 AUC exposures approximately 24-, 5-, or 17-fold higher, respectively, than human exposure at the recommended clinical dose. In addition, no heart degeneration or inflammation was observed in rats following sofosbuvir doses of up to 750 mg/kg/day in the 2-year carcinogenicity study at GS-331007 AUC exposure approximately 9-fold the exposure in humans at the recommended clinical dose. 14 CLINICAL STUDIES 14.1 Overview of Clinical Trials The efficacy of HARVONI was evaluated in three Phase 3 trials of 1518 subjects with genotype 1 chronic hepatitis C (CHC) with compensated liver disease:
• Study ION-3: noncirrhotic treatment-naïve subjects [see Clinical Studies (14.2)],
• Study ION-1: cirrhotic and noncirrhotic treatment-naïve subjects [see Clinical Studies (14.2)], and
• Study ION-2: cirrhotic and noncirrhotic subjects who failed prior therapy with an interferon-based regimen, including regimens containing an HCV protease inhibitor [see Clinical Studies (14.3)].
All three Phase 3 trials evaluated efficacy of HARVONI (one fixed-dose tablet of 90 mg of ledipasvir and 400 mg of sofosbuvir administered once daily) with or without ribavirin. Treatment duration was fixed in each trial. Serum HCV RNA values were measured during the clinical trials using the COBAS TaqMan HCV test (version 2.0), for use with the High Pure System. The assay had a lower limit of quantification (LLOQ) of 25 IU/mL. Sustained virologic response (SVR) was the primary endpoint and was defined as HCV RNA less than LLOQ at 12 weeks after the cessation of treatment. Relapse was a secondary endpoint, which was defined as HCV RNA greater than or equal to LLOQ with 2 consecutive values or last available post-treatment measurement during the post-treatment period after achieving HCV RNA less than LLOQ at end of treatment. 14.2 Clinical Trials in Treatment-Naïve Subjects Treatment-Naïve Adults without Cirrhosis ─ ION-3 (Study 0108) ION-3 was a randomized, open-label trial in treatment-naïve non-cirrhotic subjects with genotype 1 CHC. Subjects were randomized in a 1:1:1 ratio to one of the following three treatment groups and stratified by HCV genotype (1a vs 1b): HARVONI for 8 weeks, HARVONI for 12 weeks, or HARVONI + ribavirin for 8 weeks. Demographics and baseline characteristics were balanced across the treatment groups. Of the 647 treated subjects, the median age was 55 years (range: 20 to 75); 58% of the subjects were male; 78% were White; 19% were Black; 6% were Hispanic or Latino; mean body mass index was 28 kg/m2 (range: 18 to 56 kg/m2);

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 109
81% had baseline HCV RNA levels greater than or equal to 800,000 IU/mL; 80% had genotype 1a HCV infection; 73% had non-C/C IL28B alleles (CT or TT). Table 6 presents the response rates for the HARVONI treatment groups in the ION-3 trial after 8 and 12 weeks of HARVONI treatment. Ribavirin was not shown to increase the response rates observed with HARVONI. Therefore, the HARVONI + ribavirin arm is not presented in Table 6. Table 6 Study ION-3: Response Rates after 8 and 12 Weeks of Treatment in Treatment-Naïve Non-Cirrhotic Subjects with Genotype 1 CHC HARVONI 8 weeks
(N=215) HARVONI 12 weeks
(N=216) SVR 94% (202/215) 96% (208/216)
Outcome for subjects without SVR
On-treatment virologic failure 0/215 0/216
Relapsea 5% (11/215) 1% (3/216)
Otherb 1% (2/215) 2% (5/216)
SVR by genotypec
Genotype 1a 93% (159/171) 96% (165/172)
Genotype 1b 98% (42/43) 98% (43/44)
a. The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. b. Other includes subjects who did not achieve SVR and did not meet virologic failure criteria (e.g., lost to follow-up). c. One subject without a confirmed subtype for genotype 1 infection was excluded from this subgroup analysis. The treatment difference between the 8-week treatment of HARVONI and 12-week treatment of HARVONI was –2.3% (97.5% confidence interval –7.2% to 2.5%). Among subjects with a baseline HCV RNA <6 million IU/mL, the SVR was 97% (119/123) with 8-week treatment of HARVONI and 96% (126/131) with 12-week treatment of HARVONI.
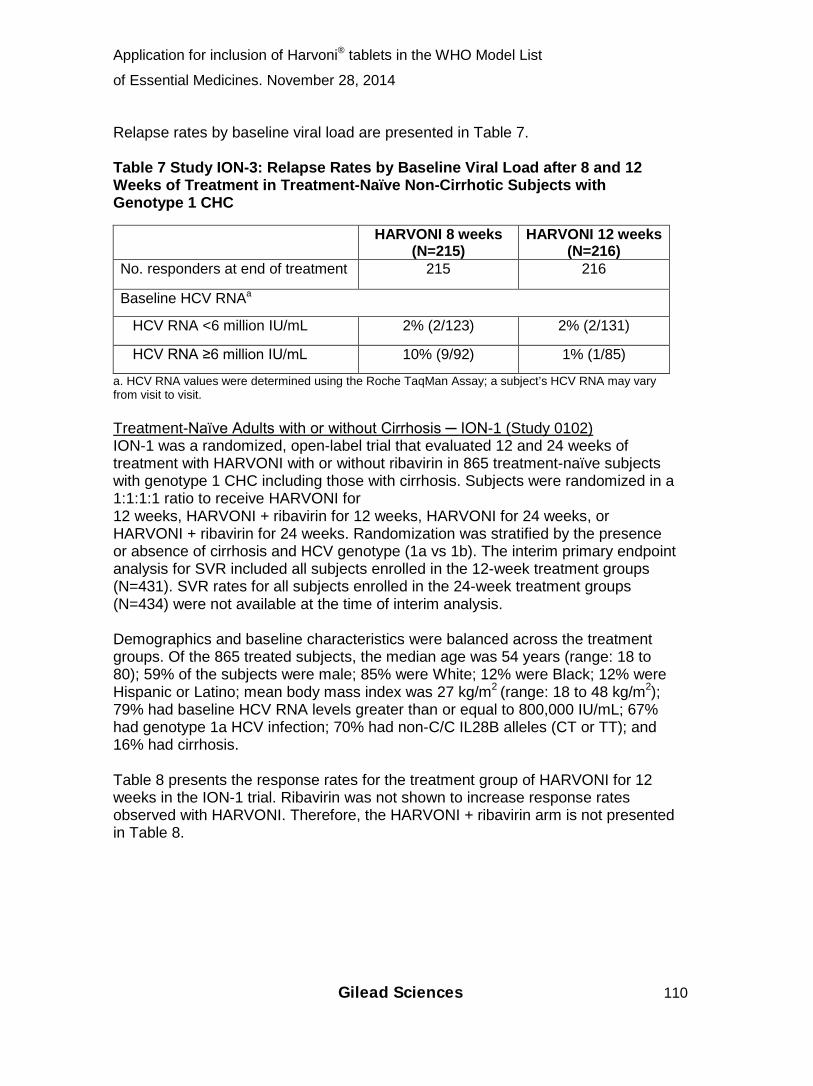
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 110
Relapse rates by baseline viral load are presented in Table 7. Table 7 Study ION-3: Relapse Rates by Baseline Viral Load after 8 and 12 Weeks of Treatment in Treatment-Naïve Non-Cirrhotic Subjects with Genotype 1 CHC HARVONI 8 weeks
(N=215) HARVONI 12 weeks
(N=216) No. responders at end of treatment 215 216
Baseline HCV RNAa
HCV RNA <6 million IU/mL 2% (2/123) 2% (2/131)
HCV RNA ≥6 million IU/mL 10% (9/92) 1% (1/85)
a. HCV RNA values were determined using the Roche TaqMan Assay; a subject’s HCV RNA may vary from visit to visit. Treatment-Naïve Adults with or without Cirrhosis ─ ION-1 (Study 0102) ION-1 was a randomized, open-label trial that evaluated 12 and 24 weeks of treatment with HARVONI with or without ribavirin in 865 treatment-naïve subjects with genotype 1 CHC including those with cirrhosis. Subjects were randomized in a 1:1:1:1 ratio to receive HARVONI for 12 weeks, HARVONI + ribavirin for 12 weeks, HARVONI for 24 weeks, or HARVONI + ribavirin for 24 weeks. Randomization was stratified by the presence or absence of cirrhosis and HCV genotype (1a vs 1b). The interim primary endpoint analysis for SVR included all subjects enrolled in the 12-week treatment groups (N=431). SVR rates for all subjects enrolled in the 24-week treatment groups (N=434) were not available at the time of interim analysis. Demographics and baseline characteristics were balanced across the treatment groups. Of the 865 treated subjects, the median age was 54 years (range: 18 to 80); 59% of the subjects were male; 85% were White; 12% were Black; 12% were Hispanic or Latino; mean body mass index was 27 kg/m2
(range: 18 to 48 kg/m2); 79% had baseline HCV RNA levels greater than or equal to 800,000 IU/mL; 67% had genotype 1a HCV infection; 70% had non-C/C IL28B alleles (CT or TT); and 16% had cirrhosis. Table 8 presents the response rates for the treatment group of HARVONI for 12 weeks in the ION-1 trial. Ribavirin was not shown to increase response rates observed with HARVONI. Therefore, the HARVONI + ribavirin arm is not presented in Table 8.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 111
Table 8 Study ION-1: Response Rates after 12 Weeks of Treatment in Treatment-Naïve Subjects with Genotype 1 CHC with and without Cirrhosis HARVONI 12 WEEKS
(n=214) SVRa 99% (210/213)
Outcome for subjects without SVR
On-treatment virologic failurea 0/213
Relapsea,b <1% (1/212)
Othera,c 1% (2/213) a. Excluding one subject with genotype 4 infection. b. The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. c. Other includes subjects who did not achieve SVR and did not meet virologic failure criteria (e.g., lost to follow-up). Response rates for selected subgroups are presented in Table 9. Table 9 Study ION-1: SVR Rates for Selected Subgroups after 12 Weeks of Treatment in Treatment-Naïve Subjects with Genotype 1 CHC with and without Cirrhosis HARVONI 12 WEEKS
(n=214)
Genotypea
Genotype 1a 98% (142/145)
Genotype 1b 100% (67/67)
Cirrhosisb
No 99% (176/177)
Yes 94% (32/34) a. One subject without a confirmed subtype for genotype 1 infection and one subject with genotype 4 infection were excluded from this subgroup analysis. b. Subjects with missing cirrhosis status were excluded from this subgroup analysis. 14.3 Clinical Trials in Subjects Who Failed Prior Therapy Previously-Treated Adults with or without Cirrhosis ─ ION-2 (Study 0109) ION-2 was a randomized, open-label trial that evaluated 12 and 24 weeks of treatment with HARVONI with or without ribavirin in genotype 1 HCV-infected subjects with or without cirrhosis who failed prior therapy with an interferon-based regimen, including regimens containing an HCV protease inhibitor. Subjects were randomized in a 1:1:1:1 ratio to receive HARVONI for 12 weeks, HARVONI + ribavirin for 12 weeks, HARVONI for 24 weeks, or HARVONI + ribavirin for 24
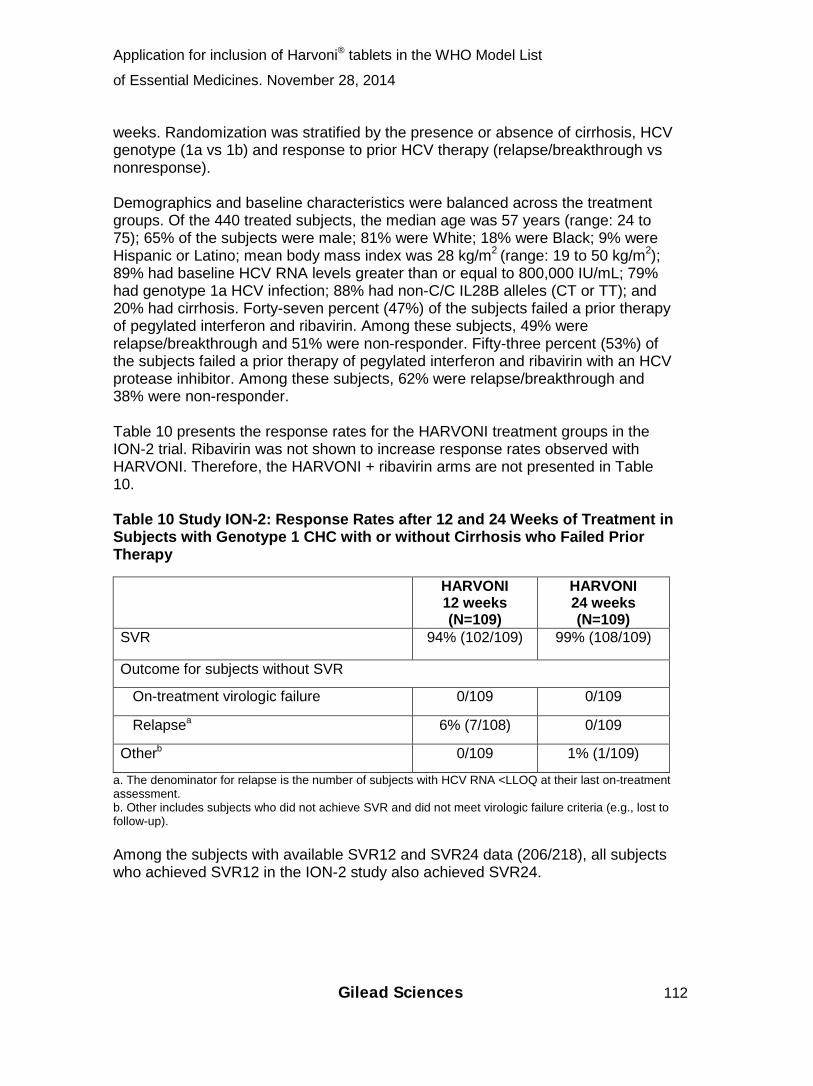
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 112
weeks. Randomization was stratified by the presence or absence of cirrhosis, HCV genotype (1a vs 1b) and response to prior HCV therapy (relapse/breakthrough vs nonresponse). Demographics and baseline characteristics were balanced across the treatment groups. Of the 440 treated subjects, the median age was 57 years (range: 24 to 75); 65% of the subjects were male; 81% were White; 18% were Black; 9% were Hispanic or Latino; mean body mass index was 28 kg/m2
(range: 19 to 50 kg/m2); 89% had baseline HCV RNA levels greater than or equal to 800,000 IU/mL; 79% had genotype 1a HCV infection; 88% had non-C/C IL28B alleles (CT or TT); and 20% had cirrhosis. Forty-seven percent (47%) of the subjects failed a prior therapy of pegylated interferon and ribavirin. Among these subjects, 49% were relapse/breakthrough and 51% were non-responder. Fifty-three percent (53%) of the subjects failed a prior therapy of pegylated interferon and ribavirin with an HCV protease inhibitor. Among these subjects, 62% were relapse/breakthrough and 38% were non-responder. Table 10 presents the response rates for the HARVONI treatment groups in the ION-2 trial. Ribavirin was not shown to increase response rates observed with HARVONI. Therefore, the HARVONI + ribavirin arms are not presented in Table 10. Table 10 Study ION-2: Response Rates after 12 and 24 Weeks of Treatment in Subjects with Genotype 1 CHC with or without Cirrhosis who Failed Prior Therapy HARVONI
12 weeks (N=109)
HARVONI 24 weeks (N=109)
SVR 94% (102/109) 99% (108/109)
Outcome for subjects without SVR
On-treatment virologic failure 0/109 0/109
Relapsea 6% (7/108) 0/109
Otherb 0/109 1% (1/109)
a. The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. b. Other includes subjects who did not achieve SVR and did not meet virologic failure criteria (e.g., lost to follow-up). Among the subjects with available SVR12 and SVR24 data (206/218), all subjects who achieved SVR12 in the ION-2 study also achieved SVR24.
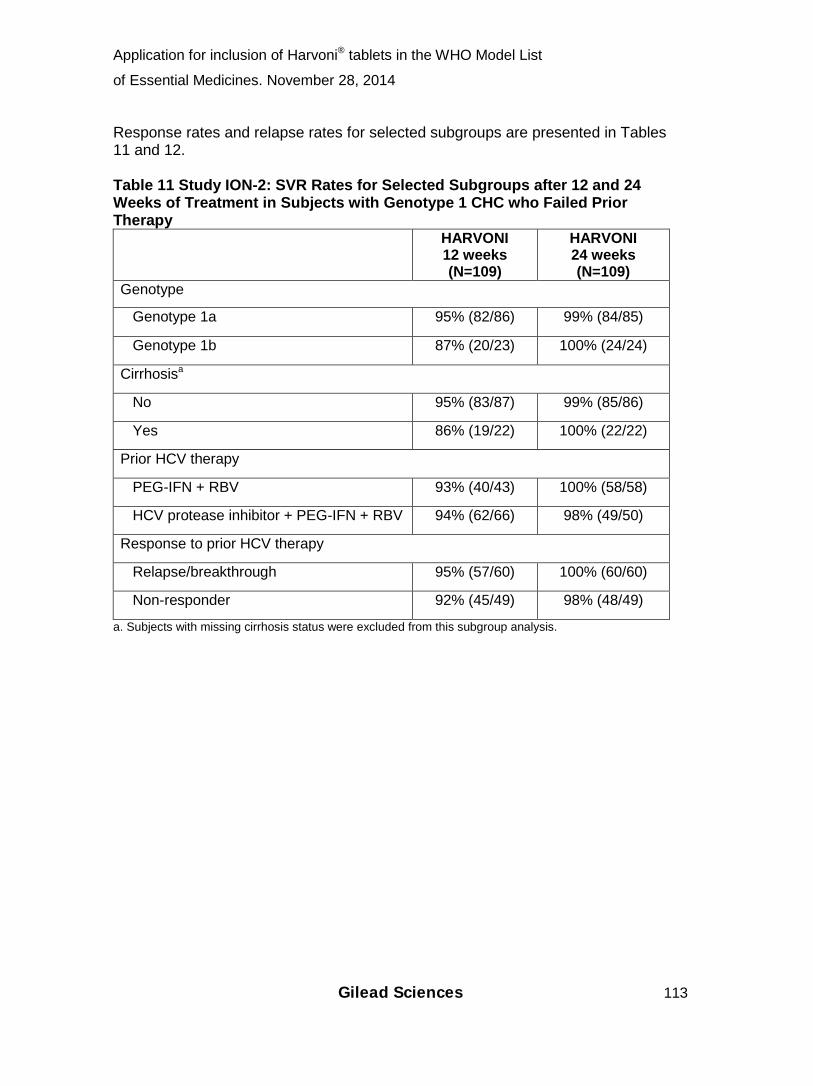
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 113
Response rates and relapse rates for selected subgroups are presented in Tables 11 and 12. Table 11 Study ION-2: SVR Rates for Selected Subgroups after 12 and 24 Weeks of Treatment in Subjects with Genotype 1 CHC who Failed Prior Therapy HARVONI
12 weeks (N=109)
HARVONI 24 weeks (N=109)
Genotype
Genotype 1a 95% (82/86) 99% (84/85)
Genotype 1b 87% (20/23) 100% (24/24)
Cirrhosisa
No 95% (83/87) 99% (85/86)
Yes 86% (19/22) 100% (22/22)
Prior HCV therapy
PEG-IFN + RBV 93% (40/43) 100% (58/58)
HCV protease inhibitor + PEG-IFN + RBV 94% (62/66) 98% (49/50)
Response to prior HCV therapy
Relapse/breakthrough 95% (57/60) 100% (60/60)
Non-responder 92% (45/49) 98% (48/49)
a. Subjects with missing cirrhosis status were excluded from this subgroup analysis.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 114
Table 12 Study ION-2: Relapse Rates for Selected Subgroups after 12 and 24 Weeks of Treatment in Subjects with Genotype 1 CHC who Failed Prior Therapy HARVONI
12 weeks (N=109)
HARVONI 24 weeks (N=109)
Number of responders at end of treatment 108 109
Cirrhosisa
No 5% (4/86)b 0% (0/86)
Yes 14% (3/22) 0 (0/22)
Presence of baseline NS5A resistance-associated polymorphismsc
No 2% (2/85) 0% (0/90)
Yes 22% (5/23) 0% (0/19)
IL28B status
C/C 0% (0/10) 0% (0/16)
Non-C/C 7% (7/98) 0% (0/93)
a. Subjects with missing cirrhosis status were excluded from this subgroup analysis. b. These 4 non-cirrhotic relapsers all had baseline NS5A resistance-associated polymorphisms. c. NS5A resistance-associated polymorphisms include any change at NS5A positions 24, 28, 30, 31, 58, 92, or 93. 16 HOW SUPPLIED/STORAGE AND HANDLING HARVONI tablets are orange, diamond-shaped, film-coated, debossed with “GSI” on one side and “7985” on the other side of the tablet. Each bottle contains 28 tablets (NDC 61958-1801-1), a silica gel desiccant, polyester coil, and is closed with a child-resistant closure. Store at room temperature below 30°C (86°F).
• Dispense only in original container. • Do not use if seal over bottle opening is broken or missing.
17 PATIENT COUNSELING INFORMATION Advise the patient to read the FDA-approved patient labeling (Patient Information). Drug Interactions Inform patients that HARVONI may interact with other drugs. Advise patients to report to their healthcare provider the use of any other prescription or nonprescription medication or herbal products including St. John’s wort [see Warnings and Precautions (5.1) and Drug Interactions (7)].

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 115
Hepatitis C Virus Transmission Inform patients that the effect of treatment of hepatitis C infection on transmission is not known, and that appropriate precautions to prevent transmission of the hepatitis C virus during treatment or in the event of treatment failure should be taken. Administration Advise patients that HARVONI should be taken once daily on a regular dosing schedule with or without food. If a patient did not take HARVONI at the regular time, it should be taken as soon as they remember on the same day. Resume the usual dosing schedule the next day. Advise the patient not to take more than 1 tablet of HARVONI in a day. Manufactured and distributed by: Gilead Sciences, Inc. Foster City, CA 94404 Harvoni, Complera, Sovaldi, Truvada and Viread are trademarks of Gilead Sciences, Inc., or its related companies. Atripla is a trademark of Bristol-Myers Squibb & Gilead Sciences, LLC. All other trademarks referenced herein are the property of their respective owners. © 2014 Gilead Sciences, Inc. All rights reserved. 205834-GS-000

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 116
Patient Information
HARVONI® (har-VOE-nee)
(ledipasvir and sofosbuvir) tablets
Read this Patient Information before you start taking HARVONI and each time you get
a refill. There may be new information. This information does not take the place of
talking with your healthcare provider about your medical condition or your treatment.
What is HARVONI?
• HARVONI is a prescription medicine used to treat chronic (lasting a long time)
hepatitis C genotype 1 infection in adults.
• HARVONI contains the prescription medicines ledipasvir and sofosbuvir
(SOVALDI®).
It is not known if HARVONI is safe and effective in children under 18 years of age.
What should I tell my healthcare provider before taking HARVONI? Before taking HARVONI, tell your healthcare provider if you:
• have liver problems other than hepatitis C infection
• have severe kidney problems or you are on dialysis
• have any other medical condition
• are pregnant or plan to become pregnant. It is not known if HARVONI will harm
your unborn baby.
• are breastfeeding or plan to breastfeed. It is not known if HARVONI passes into
your breast milk.
Tell your healthcare provider about all of the medicines you take, including
prescription and over-the-counter medicines, vitamins, and herbal supplements.
HARVONI may affect the way other medicines work, and other medicines may affect
how HARVONI works.

Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 117
You should not take HARVONI if you also take other medicines that contain
sofosbuvir (SOVALDI®).
Especially tell your healthcare provider if you take any of the following medicines:
• an antacid that contains aluminum or magnesium hydroxide. If you take an
antacid during treatment with HARVONI, take the antacid 4 hours before or 4
hours after you take HARVONI.
• carbamazepine (Carbatrol®, Epitol®, Equetro®, Tegretol®)
• digoxin (Lanoxin®)
• efavirenz, emtricitabine, tenofovir disoproxil fumarate (ATRIPLA®)
• elvitegravir, cobicistat, emtricitabine, tenofovir disoproxil fumarate (STRIBILD®)
• medicines for indigestion, heartburn, or stomach ulcers, such as nizatidine
(Axid®), famotidine (Pepcid AC®), cimetidine (Tagamet®), ranitidine (Zantac®),
esomeprazole (Nexium®), lansoprazole (Prevacid®), omeprazole (Prilosec®),
rabeprazole (Aciphex®), or pantoprazole (Protonix®)
• oxcarbazepine (Trileptal®, Oxtellar XR®)
• phenytoin (Dilantin®, Phenytek®)
• phenobarbital (Luminal®)
• rifabutin (Mycobutin®)
• rifampin (Rifadin®, Rifamate®, Rifater®, Rimactane®)
• rifapentine (Priftin®)
• rosuvastatin (Crestor®)
• simeprevir (Olysio®)
• St. John’s wort (Hypericum perforatum) or a product that contains St. John’s
wort
• tipranavir (Aptivus®) used in combination with ritonavir (Norvir®)
• tenofovir disoproxil fumarate (VIREAD®, TRUVADA®) used in combination with
atazanavir (Reyataz®) and ritonavir (Norvir®), darunavir (Prezista®) and ritonavir
(Norvir®), or used in combination with lopinavir and ritonavir (Kaletra®)
Know the medicines you take. Keep a list of your medicines and show it to your
healthcare provider and pharmacist when you get a new medicine.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 118
How should I take HARVONI?
• Take HARVONI exactly as your healthcare provider tells you to take it. Do not
change your dose unless your healthcare provider tells you to.
• Do not stop taking HARVONI without first talking with your healthcare provider.
If you think there is a reason to stop taking HARVONI, talk to your healthcare
provider before doing so.
• Take HARVONI 1 time each day with or without food.
• If you miss a dose of HARVONI, take the missed dose as soon as you
remember the same day. Do not take more than 1 tablet of HARVONI in a day.
Take your next dose of HARVONI at your regular time the next day
• If you take too much HARVONI, call your healthcare provider or go to the
nearest hospital emergency room right away.
What are the possible side effects of HARVONI? The most common side effects of HARVONI include:
• tiredness
• headache
Tell your healthcare provider if you have any side effect that bothers you or that does
not go away.
These are not all the possible side effects of HARVONI. For more information, ask your
healthcare provider or pharmacist.
Call your doctor for medical advice about side effects. You may report side effects to
FDA at 1-800-FDA-1088.
How should I store HARVONI?
• Store HARVONI at room temperature below 86°F (30°C).
• Keep HARVONI in its original container.
• Do not use HARVONI if the seal over the bottle opening is broken or missing.
Keep HARVONI and all medicines out of the reach of children.
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 119
General information about the safe and effective use of HARVONI It is not known if treatment with HARVONI will prevent you from infecting another
person with the hepatitis C virus during treatment. Talk with your healthcare provider
about ways to prevent spreading the hepatitis C virus.
Medicines are sometimes prescribed for purposes other than those listed in a Patient
Information leaflet. Do not use HARVONI for a condition for which it was not
prescribed. Do not give HARVONI to other people, even if they have the same
symptoms you have. It may harm them.
If you would like more information about HARVONI, talk with your healthcare provider.
You can ask your healthcare provider or pharmacist for information about HARVONI
that is written for health professionals.
For more information, call 1-800-445-3235 or go to www.HARVONI.com.
What are the ingredients in HARVONI? Active ingredients: ledipasvir and sofosbuvir
Inactive ingredients: colloidal silicon dioxide, copovidone, croscarmellose sodium,
lactose monohydrate, magnesium stearate, and microcrystalline cellulose.
The tablet film-coat contains: FD&C yellow #6/sunset yellow FCF aluminum lake,
polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide.
This Patient Information has been approved by the U.S. Food and Drug Administration.
Manufactured and distributed by:
Gilead Sciences, Inc.
Foster City, CA 94404
Issued: October 2014
Application for inclusion of Harvoni® tablets in the WHO Model List
of Essential Medicines. November 28, 2014
Gilead Sciences 120
Harvoni, Sovaldi, Stribild, Truvada and Viread are trademarks of Gilead Sciences, Inc.,
or its related companies. Atripla is a trademark of Bristol-Myers Squibb & Gilead
Sciences, LLC. All other trademarks referenced herein are the property of their
respective owners.
©2014 Gilead Sciences, Inc. All rights reserved.
205834-GS-000
Top Related