







Languages
Pages
Legal


Antipsychotic Agents
Schizophrenia is the most common psychosis having
the following POSITIVE SYMPTOMS: Delusions: fixed constant beliefs Hallucinations (auditory/visual): false perceptions in the
absence of real external stimuli Disorganized thoughts, behavior & speech
In addition to psychotic symptoms Negative symptoms; apathy, low mood, blunted emotion, &
social withdrawal mostly are present Cognitive difficulties; attention, concentration, & memory Schizophrenia/psychosis related to DAergic hyperactivity
Dopamine Receptor Subtypes
Five types, all G-protein coupled D1 receptor subfamily - D1 and D5 receptor
subtypes D2 receptor subfamily - D2, D3 and D4 receptor
subtypes D1 receptors stimulate whereas D2 receptors
reduce, or do not change, adenylyl cyclase activity mediating the postsynaptic response to dopamine
Dopamine Receptor Subtypes
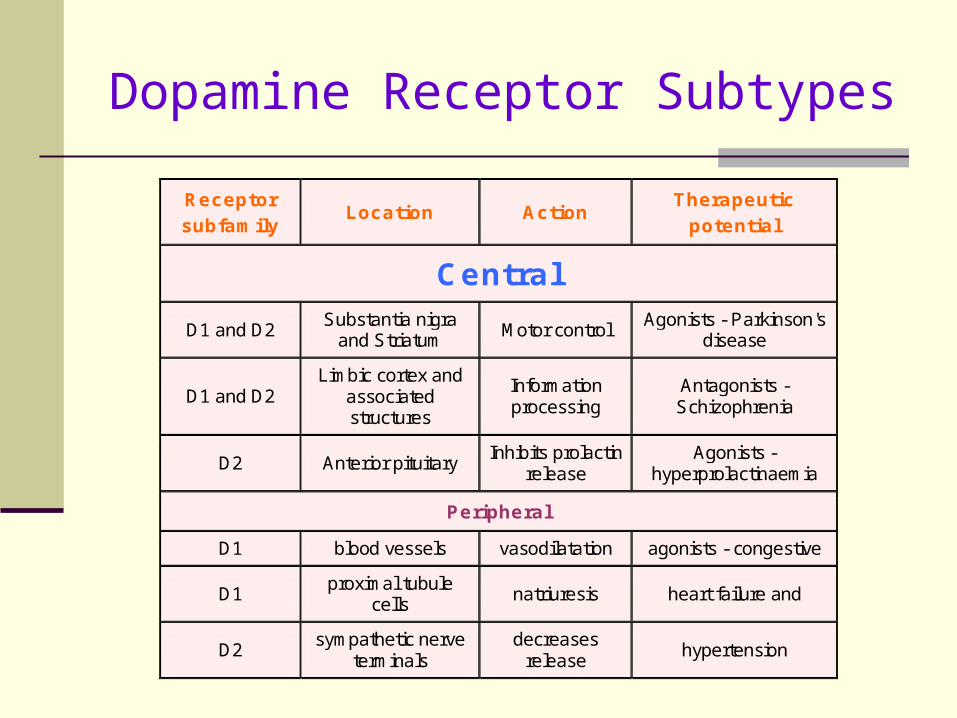
Receptor subfamily
Location Action Therapeutic
potential
Central
D1 and D2 Substantia nigra
and Striatum Motor control
Agonists - Parkinson's disease
D1 and D2 Limbic cortex and
associated structures
Information processing
Antagonists - Schizophrenia
D2 Anterior pituitary Inhibits prolactin
release Agonists -
hyperprolactinaemia
Peripheral
D1 blood vessels vasodilatation agonists - congestive
D1 proximal tubule
cells natriuresis heart failure and
D2 sympathetic nerve
terminals decreases
release hypertension
Dopamine Receptor Subtypes
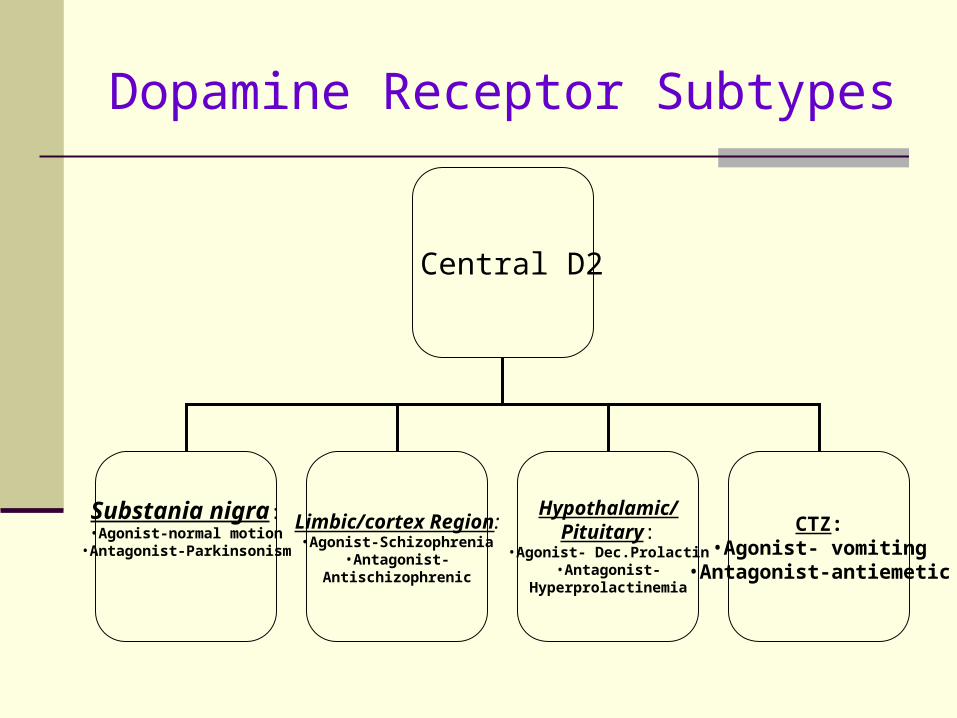
Central D2
Substania nigra:•Agonist-normal motion
•Antagonist-Parkinsonism
Limbic/cortex Region:•Agonist-Schizophrenia
•Antagonist-Antischizophrenic
Hypothalamic/Pituitary:
•Agonist- Dec.Prolactin•Antagonist-
Hyperprolactinemia
CTZ:•Agonist- vomiting
•Antagonist-antiemetic

Dopaminergic Pathways

Schizophrenia Dopaminergic Biochemical Hypothesis
Schizophrenia/psychosis related to DAergic hyperactivity in mesolimbic/mesocortical tracts
Neuroleptics antipsychotic therapeutic effects (positive signs) are via blockade of DA-2 receptors in mesolimbic & mesocortical pathways
D2 blockade in nigrostriatal pathways results in parkinsonian side effects
D2 blockade in hypothalamphseal pathway leads to hyperprolactinemia
Neuroleptic block histmainergic, α-adrenergic, and cholinergic receptors

Classes of Neuroleptics
Class Drugs D2 R M R α1 R Extrapyrimdal
Antich.
Sedatn.
Hypotsn.
Low-Potency
CPZ, Thioridazine, Perphenazine
+/++ +++ +++
High-potency
Haloperidol
Fluphenazine
+++ _ +
Atypical Clozapine
Resperidone
Ziprasiddone
+
++
+++
-
++
++
No
Low
High
Low

Antipsychotic Actions of Neuroleptics
Antipsychotic effect rely upon D2 receptor blockade in limbic system
Reduction of delusion-hallucinations-thoughts disorders (Positive symptoms)
Negative symptoms & cognitive impairment are poorly affected by typical neuroleptics
Atypical neuroleptics (clozapine) improve moderately the negative symptsoms
No effect on intellectual activity of the patient & minor motor incoordiantion (unlike other CNS depressants)
Antipsychotic effect takes several weeks to develop
Atypical Neuroleptics
Clozapine & Resperidone are characterized by low extrapyrimdal side effects & lower TD
No hyperprolctinemia They improve negative symptoms of
schizophrenia more than typical ones They have higher affinity for D4 receptors when
compared to D2 & block 5-HT2A receptors
Nigrostriatal DA pathway is under inhibitory serotoninergic modulation
Clozapine can produce agranulocytosis; frequent WBCs monitoring
Antinausea & Antivomiting Effects
CTZ is a reticular formation part in the medulla oblangata outside the BBB
Neuroleptic by D2 receptor blockade in the CTZ, can protect against nausea/vomiting induced by cancer chemotherapy, pregnancy, radiation sickness (domperidone, metoclopramide & prochloperazine)
Phenothiazines like promethazine, meclizine are effective in motion sickness

EXTRAPYRIMADAL SIDE-EFFECTS1- Neuroleptic-induced Parkinsonism
Blockade of D2 receptors in the nigrostriatal pathways by antipsychotics underlie the Parkinsonian disorder including:
o Akinesia: shorter steps, reduced arm swing, micrographia & difficulty in motion initiation
o Rigidity: Stiffnesso Temor similar to Parkinson’s disease
EXTRAPYRIMADAL SIDE-EFFECTS
2- Neuroleptic Malignant Syndrome
Rare, severe, may be fatal Cardinal signs: severe rigidity,
fever, marked autonomic disturbance, & muscle destruction (increased creatine-PK)
Can not be predicted, irregular dose-relation
Treat hyperthermia, dantrolene (central muscle relaxant), bromocriptine
3- Neuroleptic-Induced Dyskinesia/Dystonias
Occurs 1-3 days consisting of involuntary motions of lips, jaw & tongue (speech difficulty)
Acute dystonias: involuntary twisting of neck, pelvis, & eyes
4- Neuroleptic Induced Akathisia
Akathisia is a motor restlessness, usually lower limb, accompanied by feeling of restlessness
Restlessness & anxiety usually accompany schizophrenia overshadowing the akathisia
Onset of akathisia coincides with initiation of treatment complaining of “restless” legs
Patients report relief upon moving their legs
Treatment of Neuroleptic-Induced Parkinsonism, Dystonias, & Akathisia
Striatal GABAergic neural output is controlled by DAergic nigral & local cholinergic inputs
DAergic blockade by neuroleptics renders cholinergic input to be dominating resulting in parkinsonism & dystonias
Bezotropine/biperiden, by blocking cholinergic receptors, restore DA/Ach balance
L-DOPA restores DA but antagonize therapy Neuroleptic-anticholinergic combinations are
routine for children & young men Majority of adults, first treated with neuroleptics, &
anticholinergic added whenever needed
Tardive Dyskinesia (TD)
After few months-years: Involuntary oral & lingual gum chewing-like movements, in addition to dystonic neck, & trunk motions
DA receptor up-regulation from chronic blockade is not mediating TD?: fast upregulation & slow TD
Neuroleptic dose increment may improve TD Anticholinergics may worsen TD, though
improving parkinsonian side effects Neuroleptic stop is essential whenever psychotic
status is improved Atypical neuroleptic clozapine is alternative,
suppressing TD or no further worsening

Hyperprolactinemia & Galactorrhea
Neuroleptics interact with hypothalamo-hypophyseal DA system (hypothalmus-pituitary axis)
Neuroleptics antagonize D2 receptors in mammotrophs of the pituitary gland, resulting in increased prolactin
Breast swelling & galactorrhea Infertility & impotence may occur They may block FSH & LH leading to failure of
ovulation in women on antipsychotics leading to pseudopregnancy

Unwanted Sedation
It is mediated mainly via histaminergic & cholinergic receptor blockade
Low-potency agents are of highest sedation & high-potency the least
It is presented as attention & concentration difficulties, daytime drowsiness & fatigue
Orthostatic Hypotension
Some neuroleptics have α-adrenergic blockade &/or direct effect on vasomotor centre

Anticholinergic Side Effects
Low-potency neuroleptics are of potent cholinergic effects but not high-potency ones
Anticholinergic effects include: dry mouth, constipation, urinary retention, in addition to dry eyes & blurred vision
There may be decreased aqueous humor outflow leading to increased IOP & glaucoma attacks in sensitive patients
The intrinsic antimuscarinic activity of low-potency neuroleptics might be related to the low extrapyrimadal side effects

Other DA-Independent Side Effects
Jaundice Phenothiazine-induced
jaundice occurs in a very limited number of patients
Possibly hypersensitivity dose-independent reactions
Dermatitis & Photosensitivity Most frequent with low-
potency agents in a limited no. of patients
Patients become sunlight-sensitive & may develop sunburns
Possible skin & corneal hyperpigmentaion

Other side Effects & Contraindications
Significant weight gain is common with atypical neuroleptics
CPZ & clozapine are contraindicated in patients with seizure disorder, where they lower seizure threshold
Clozapine-induced agranulocytosis limit its use to refractory schizophenia
Tachycardia Sexual dysfunction

Case
W G., 19 years old when he was enrolled in university. His academic record was good, he won a place on the university sports team. When he returned to school for his second year, his roommate observed that W G. was staying by himself, avoiding the company of friends, and skipping school and athletic training, things he had never done before.
Some time later, he was heard speaking to himself as he sat isolated in his room, mumbling and smiling. Soon after, he confided to his roommate that he had uncovered a ‘grand conspiracy” to rob him of his athletic abilities and that he could hear the conspirators’ voices as they made plans to destroy him.
Finally; he accused his roommate of being a part of the conspiracy.
At this point, his friends called his parents and was taken to see a psychiatrist. The psychiatrist diagnosed him as showing early symptoms of schizophrenia, and he was admitted to the hospital. Blood and-urine tests were negative for signs of any general medical condition or the presence of any street drugs.
He was therefore treated with haloperidol at a starting dose of 10 mg per day. On the second day of his treatment, while a medical student was interviewing him, he seemed to develop a “seizure.” His neck strained backward with his face turned upward toward the ceiling. He was having difficulty speaking, But was quite conscious of his surroundings. The attending physician recognized this as an acute dystonic reaction to the medication rather than a seizure
The doctor immediately ordered an injection of benztropine, which resolved the situation in a matter of minutes. Following this experience, W.G. refused to have anything more to do with haloperidol.
However, he agreed to take loxapine instead after it was explained to him that he was less likely to have the dystonic reaction with this drug, especially if it was accompanied by benztropine.
The dose of loxapine was gradually increased to 40 mg/day He experienced sedation, blurred vision, drying of his eyes that made it difficult for him to wear contact lenses, and dry mouth. However, over the next 3 weeks his delusions and hallucinations disappeared. He developed insight into his problems, and the sedation, the dry mouth, and the dry eyes became much more bearable. He left the hospital a month later, went back to his dormitory; and resumed his academic life.

Questions
1) Relate different Dopamine Pathway to therapeutic and side effects; Mesolimbic/Mesocortical Nigrostriatal Hypothalamic/pituitary
2) Advantage of atypical neuroleptics Vs Typical regarding; Receptors, Therapeutic effects and Side effects.
3) Differentiate between: Neuroleptic-induced Parkinsonism and Neuroleptic-induced tardive dyskinesia regarding the following points
Symptoms Onset Treatment
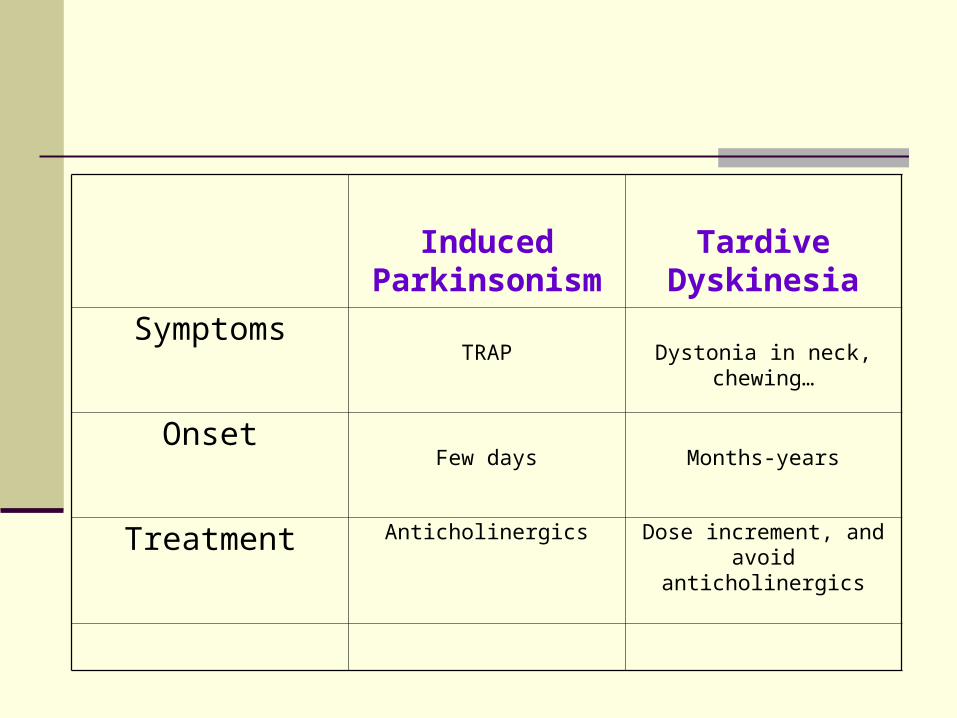
Induced Parkinsonism
Tardive Dyskinesia
SymptomsTRAP Dystonia in neck, chewing…
OnsetFew days Months-years
Treatment Anticholinergics Dose increment, and avoid anticholinergics
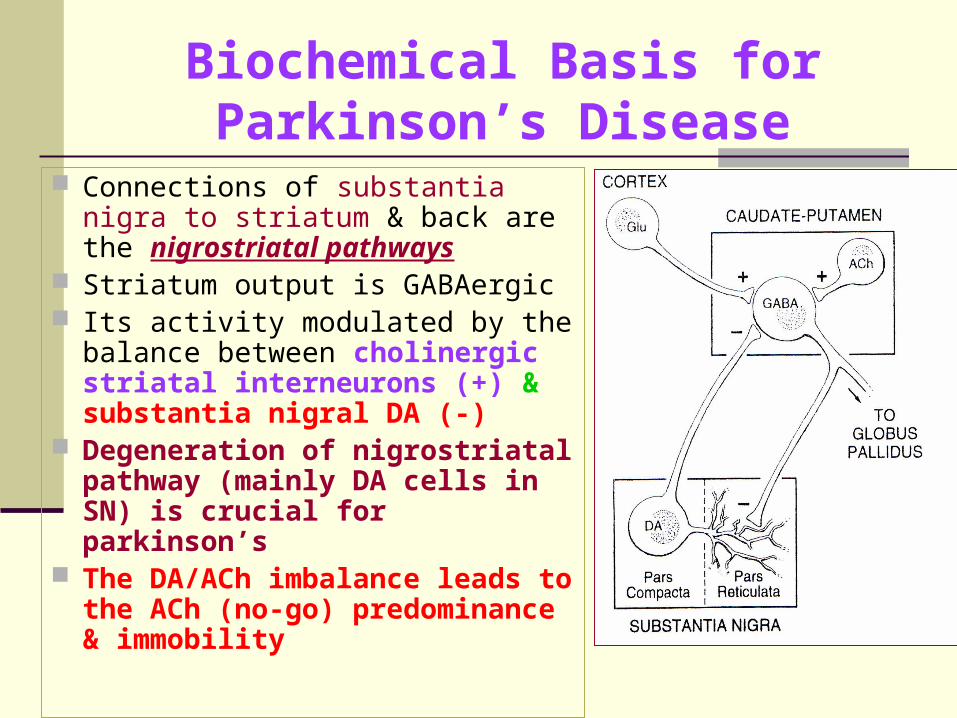
Biochemical Basis for Parkinson’s Disease
Connections of substantia nigra to striatum & back are the nigrostriatal pathways
Striatum output is GABAergic Its activity modulated by the
balance between cholinergic striatal interneurons (+) & substantia nigral DA (-)
Degeneration of nigrostriatal pathway (mainly DA cells in SN) is crucial for parkinson’s
The DA/ACh imbalance leads to the ACh (no-go) predominance & immobility
Top Related