







Languages
Pages
Legal


501
Dosages of ARV drugs for adults and adolescents
Generic name Dose
Nucleoside reverse-transcriptase inhibitors (NRTIs)
Abacavir (ABC) 300 mg twice daily or 600 mg once daily
Emtricitabine (FTC) 200 mg once daily
Lamivudine (3TC) 150 mg twice daily or 300 mg once daily
Zidovudine (AZT) 300 mg twice daily
Nucleotide reverse-transcriptase inhibitors (NtRTIs)
Tenofovir disoproxil fumarate (TDF)
300 mg once dailya
Tenofovir alafenamide (TAF) 10 or 25 mg once dailyb
Non-nucleoside reverse-transcriptase inhibitors (NNRTIs)
Efavirenz (EFV) 400 mg or 600 mg once daily
Etravirine (ETV) 200 mg twice daily
Nevirapine (NVP) 200 mg once daily for 14 days followed by 200 mg twice daily
Protease inhibitors (PIs)
Atazanavir/ritonavir (ATV/r) 300 mg/100 mg once daily
Darunavir + ritonavir (DRV/r) 800 mg + 100 mg once daily or 600 mg + 100 mg twice daily
Lopinavir/ritonavir (LPV/r) 400 mg/100 mg twice daily
Considerations for individuals receiving TB therapy
In the presence of rifampicin, adjusted dose of LPV/r (double-dose LPV 800 mg + ritonavir 200 mg twice daily or super boosted with LPV 400 mg/ + ritonavir 100 mg twice daily plus additional doses of RTV 300 mg twice daily), with close monitoring. In the presence of rifabutin, no dose adjustment required. Rifapentine should not be used.
Integrase strand transfer inhibitors (INSTIs)
Dolutegravir (DTG) 50 mg once dailya
Raltegravir (RAL) 400 mg twice daily
Considerations for individuals receiving TB therapy
In the presence of rifampicin, adjusted dose of DTG (50 mg twice daily) and RAL (800 mg twice daily), with close monitoring DTG and RAL dose should remain twice daily for additional two weeks after the last dose of rifampicin. In the presence of rifabutin or rifapentine, no dose adjustment is required.
a DTG 50 mg and TLD (tenofovir 300 mg, lamivudine 300 mg, dolutegravir 50 mg, fixed-dose combination) can be used once daily for adolescents living with HIV weighing at least 30 kg. DTG 50-mg film-coated tablets can be used for children and adolescents weighing at least 20 kg. TDF 300 mg can be used for adolescents weighing at least 30 kg.
b TAF 25 mg and TAF + FTC + DTG (TAF 25 mg, emtricitabine 200 mg, dolutegravir 50 mg, fixed-dose combination) can be used once daily for adolescents living with HIV weighing at least 25 kg. The TAF dose is reduced to 10 mg when administered in the context of boosted regimens.
ANNEX 1: DOSAGES FOR ARV DRUGS

502 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Weight-based dosing for ARV drug formulations for infants and children
Prescribing information and weight-based dosing of available ARV formulations for infants and childrenThis annex contains information on ARV drugs for which there are paediatric indications, formulations or sufficient information and evidence to provide guidance on prescribing and dosing for infants, children and adolescents. WHO has undertaken the work to develop and update simplified guidance on ARV drugs for children through the Paediatric Antiretroviral Working Group.1
For simplification and ease of implementation, doses are expressed by weight band rather than per kilogram or per square metre of body surface area. When this simplified weight-band dosing was developed, the expected body surface area of children from low- and middle-income countries in each weight band was carefully considered. The primary source of information for the guidance provided is the manufacturer’s package insert. This was supplemented with data from other clinical studies as well as expert paediatric pharmacology consultations. For ARV drug fixed-dose combinations, a dose-modelling tool (1) was used to predict the dose delivered for each component drug against the recommended dosing schedule. In some cases, the dose for a component in a particular weight band may be somewhat above or below the target dose recommended by the manufacturer. This is inevitable given the limitations imposed by a fixed-dose combination, but care was taken to minimize the number of children that would receive more than 25% above the maximum target dose or more than 5% below the minimum target dose. Pharmacokinetic efficacy and safety studies have also confirmed the overall safety of this dosing approach. For simplification, ARV drugs no longer considered preferred or alternative options for children have been removed from the dosing guidance.
In the context of increasing implementation of HIV virological testing at birth, and the shift towards treating infants earlier in an effort to reduce early mortality, these guidelines include additional weight-based dosing guidance for term infants less than four weeks old, including those weighing 2–3 kg. However, there is limited experience with initiating treatment for neonates living with HIV younger than two weeks and a paucity of pharmacokinetic data to fully inform accurate dosing for most drugs in neonates, who are undergoing rapid growth and maturation in renal and liver function. Limited pharmacokinetic data for preterm infants are available for AZT, NVP, 3TC and ABC; there is considerable uncertainty of appropriate dosing for NVP, RAL, 3TC and ABC for preterm and low-birth-weight infants. In addition, LPV/r solution should not be given to infants younger than two weeks old or to preterm infants until they have reached 42 weeks of gestational age, because of the risk of adverse effects that may occur in this population. The management of HIV treatment for preterm neonates remains challenging because of the lack of appropriate pharmacokinetic, safety and dosing information as well as suitable formulations.
1 Paediatric Antiretroviral Working Group members: Elaine Abrams (ICAP at Columbia University, USA); Pauline Amuge (Baylor College of Medicine Children’s Foundation, Uganda); Mo Archary (University of Kwazulu-Natal, South Africa); Adrie Bekker (University of Stellenbosch, South Africa); Brookie Best (University of San Diego, USA); David Burger (Radboud University Nijmegen Medical Centre, Netherlands); Esther Casas (MSF, South Africa); Luis Castaneda (Hospital de Ninos Benjamin Bloom, El Salvador); Diana Clarke (Boston Medical Center, USA); Polly Clayden (HIV i-Base, United Kingdom); Angela Colbers (Radboud University Nijmegen Medical Centre, Netherlands); Tim R. Cressey (PHPT-IRD Research Unit, Chang Mai University, Thailand); Roberto Delisa (European Medicines Agency); Paolo Denti (University of Cape Town, South Africa); Diana Gibb (MRC Clinical Trials Unit at University College London, United Kingdom); Rohan Hazra (National Institute of Child Health and Human Development, USA); Maria Kim (Baylor International Pediatric AIDS Initiative, Malawi); Shahin Lockman (Harvard T.H. Chan School of Public Health, USA); Fatima Mir (Agha Khan University, Pakistan); Mark H. Mirochnick (Boston Medical Center, USA); Elizabeth Obimbo (University of Nairobi/Kenyatta National Hospital); Thanyawee Puthanakit (Chulalongkorn University, Thailand); Natella Rakhmanina (Elizabeth Glazer Paediatric AIDS Foundation, USA); Pablo Rojo (Hospital de 12 Octubre Madrid, Spain); Vanessa Rouzier (GHESIKO); Ted Ruel (University of California, San Francisco, USA); Nadia Sam-Agudu (Institute of Human Virology, Nigeria); Mariam Sylla (EVA Network, Mali); and Anna Turkova (MRC Clinical Trials Unit at University College London, United Kingdom). Observers: Yodit Belew (United States Food and Drug Administration, USA); Helen Bygrave (Access Campaign MSF); Shaffiq Essajee (UNICEF, USA); Stephanie Hackett (United States Centers for Dsiease Control and Prevention, USA); Marc Lallemant (PHPT Foundation, Thailand); Linda Lewis (Clinton Health Access Initiative, USA); Lynne Mofenson (Elizabeth Glaser Paediatric AIDS Foundation, USA); Irene Mukui (Drugs for Neglected Diseases initiative, Geneva, Switzerland); Sandra Nobre (Medicines Patent Pool, Switzerland); Mary Ojoo (UNICEF, Denmark); George Siberry (United States Agency for International Development, USA); Nandita Sugandhi (ICAP at Columbia University, USA); Marissa Vicari (International AIDS Society, Switzerland); Melynda Watkins (Clinton Health Access Initiative, USA); and Hilary Wolf (Office of the United States Global AIDS Coordinator, Department of State, USA).

503Annex 1: dosages for ARV drugs
Dosing for postnatal prophylaxis for infants exposed to HIV is also included here. These guidelines provide simplified dosing to administer enhanced or extended prophylaxis with NVP 50 mg scored dispersible tablets, which provide an alternative to NVP syrup. Finally, alternative ARV drugs were considered to address special situations in which stock-outs of NVP or AZT may affect the ability to effectively provide postnatal prophylaxis (including for enhanced and extended prophylaxis).
Since the WHO ARV drug guidelines were revised in 2018, integrase strand transfer inhibitors (INSTIs) have been included more prominently among the preferred regimens recommended by WHO, and DTG-based regimens have been recommended for all children with approved DTG dosing. At the time of this update in July 2021, the United States Food and Drug Administration and the European Medicines Agency have approved DTG for treatment-naive or treatment-experienced INSTI-naive children who are at least four weeks old and weigh at least 3 kg (2,3). These approvals were granted based on data generated by the IMPAACT P1093 registration trial (4) as well as the multicountry Odyssey trial (5), which also investigated the pharmacokinetics of DTG among children co-treated for TB.
– In November 2020, the United States Food and Drug Administration approved the first generic DTG 10 mg scored dispersible tablet. DTG dispersible tablets should be ideally dispersed in water or swallowed whole. Crushing, chewing or mixing with other foods or liquids can be considered as long as the entire tablet is ingested. DTG dispersible tablets are not bioequivalent to DTG film-coated tablets; 30 mg of DTG dispersible tablet is equivalent to 50 mg of DTG film-coated tablets (6).
– For infants who received RAL-containing ART for limited duration (such as no more than three months) and without evidence or suspicion of treatment failure, the Paediatric Antiretroviral Working Group concluded that switching to standard (once-daily) weight-appropriate DTG was reasonable while encouraging the generation of direct evidence to evaluate this approach. Of note, although DTG can be dosed twice daily for treating adults with suspected INSTI resistance, this approach cannot be safely extrapolated to children given differences in pharmacokinetics. Alternative regimens should be considered and, if possible, informed by appropriate HIV drug resistance testing.
– This annex includes guidance on dose adjustment for children receiving a DTG formulation during rifampicin-based TB co-treatment. For all weights and ages with approved DTG dosing, the United States Food and Drug Administration recommended administering the weight-based DTG dose twice daily if taken with rifampicin based on its customary approach of extrapolating drug–drug interaction data from adults. Direct pharmacokinetic data for children support the use of DTG twice daily for children weighing more than 25 kg (7). The DTG dose will need to remain twice daily for two weeks after the last dose of rifampicin has been given since the enzyme-inducing effect of rifampicin slowly fades away after discontinuing the drug. The Paediatric Antiretroviral Working Group highlights the need to continue to collect confirmatory evidence in lower weight bands but, as reflected in the dosing table, endorses immediate uptake of twice-daily dosing of DTG when taken with rifampicin for all children (at least four weeks old and weighing at least 3 kg) and to be continued for two weeks after cessation of rifampicin-based TB treatment.
RAL granules were added in 2018 with the goal of providing a suitable formulation to deliver RAL to neonates. Because of concerns about the complexity of administering the granule formulation, the Paediatric Antiretroviral Working Group endorsed the 25-mg chewable tablets as dispersible tablets for infants and children older than four weeks and weighing at least 3 kg. This decision was largely based on in vitro data on solubility and bioequivalence between RAL chewable tablets and granules (8) and considering the limited availability of alternative formulations for this age group. In this update of the dosing guidance, we also recommend appropriate dose adjustment for of RAL during rifampicin-based TB treatment, to be continued for two weeks after completion of rifampicin-based TB treatment.

504 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
In this 2021 update, we confirm dosing information for children for tenofovir alafenamide (TAF), fixed-dose combinations containing TAF were included for children weighing 25 kg or more with a 25-mg dose when used with unboosted regimens. This aligns with dosing approved by United States Food and Drug Administration (9). Studies to investigate dosing for children weighing less than 25 kg are ongoing, and more information will be made available as soon as approval is extended.
This dosing annex and the simplified dosing schedule will be regularly reviewed and updated as additional data and new formulations become available. Updated information on ARV drug dosing in children and rationale for dose simplification is available on the newly developed paediatric ARV dosing dashboard (10).
ARV drugs and formulations are available from several manufacturers, and the available dosage strengths of tablets, capsules and liquid formulations may vary from the information provided here. Several optimal dosage forms for children are currently being developed but have not yet received regulatory approval at the time these updated guidelines were published. National programme managers should ensure that products planned for use have received stringent regulatory approval and are of appropriate quality and stability. The current list of WHO prequalified drugs is available (11). The United States Food and Drug Administration has a current list of approved and tentatively approved ARV drugs (12). The policy of the Global Fund to Fight AIDS, Tuberculosis and Malaria on procurement and quality assurance is available (13).
General principlesWHO followed the following principles in developing the simplified tables.
• Using an age-appropriate fixed-dose combination is preferred for any regimen if such a formulation is available.
• Oral liquid or syrup formulations should be avoided if possible (except for neonatal treatment and prevention). Dispersible tablets (or granules) are the preferred solid oral dosage forms, since these formulations can be made into liquid at the point of use.
• If suitable dispersible fixed-dose combinations are not available and oral liquids must be used, children should be switched to a solid oral dosage form as soon as possible.
• Although dosing newborns generally requires using oral liquid formulations for administrating precise dosing, switching to solid oral dosage form as soon as possible is recommended.
• If children have to use adult formulations, care must be taken to avoid underdosing and overdosing. Using scored tablets is preferred to ensure accurate dosing, especially if adult dosage forms are used. Splitting unscored tablets should be avoided since the uniform distribution of active drug product cannot be assured in tablet fragments.
• Some tablets such as LPV/r or ATV/r heat-stable tablets are made in a special embedded matrix formulation (a proprietary melt extrusion technology that stabilizes drug molecules that are normally heat labile) and should not be cut, split, dissolved, chewed or crushed, since bioavailability is significantly reduced when they are not swallowed whole.
• Among children for whom an LPV/r-based regimen remains the appropriate treatment choice, LPV/r is available in a 40 mg/10 mg pellet or granule formulation for infants and young children. However, children weighing 10 kg or more should be transitioned to LPV/r heat-stable tablets as soon as they are able to swallow tablets whole to ease administration and improve palatability and to reduce pill burden.
• After the first four weeks of life, at each clinic visit, infants and children should be weighed and doses should be adjusted based on observed growth and change in body weight.
• Country programmes should consider the national regulatory status and local availability status of specific dosage forms when developing national recommendations for treating children.
• Research is ongoing for several ARV medications to establish dosing guidance for neonates, infants and young children. The age indications for each drug mentioned in the drug pages are based on current evidence and will be updated as new recommendations become available.

505Annex 1: dosages for ARV drugs
Tabl
e A1
.1 S
impl
ified
dos
ing
of c
hild
-fri
endl
y fix
ed-d
ose
solid
for
mul
atio
ns f
or t
wic
e-da
ily d
osin
g fo
r in
fant
s an
d ch
ildre
n fo
ur w
eeks
and
old
era
Dru
gSt
reng
th o
f pa
edia
tric
tab
lets
N
umbe
r of
tab
lets
by
wei
ght
band
mor
ning
and
eve
ning
Stre
ngth
of
adul
t ta
blet
Num
ber
of t
able
ts b
y w
eigh
t ba
nd
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
AM
PMA
MPM
AM
PMA
MPM
AM
PMA
MPM
AZT
/3TC
Tabl
et (d
ispe
rsib
le)
60 m
g/30
mg
11
1.5
1.5
22
2.5
2.5
33
300
mg/
150
mg
11
ABC
/3TC
Tabl
et (d
ispe
rsib
le)
60 m
g/30
mgb
11
1.5
1.5
22
2.5
2.5
33
600
mg/
300
mg
0.5
0.5
Tabl
et (d
ispe
rsib
le)
120
mg/
60 m
g0.
50.
50.
51
11
11.
51.
51.
560
0 m
g/30
0 m
g0.
50.
5
a Fo
r inf
ants
you
nger
tha
n fo
ur w
eeks
old
, see
Tab
le A
1.4
for m
ore
accu
rate
dos
ing,
whi
ch is
red
uced
bec
ause
of t
he d
ecre
ased
abi
lity
to e
xcre
te a
nd m
etab
oliz
e m
edic
atio
ns. F
or in
fant
s w
ho a
re a
t le
ast f
our w
eeks
old
but
wei
gh le
ss t
han
3 kg
, the
imm
atur
ity
of r
enal
and
hep
atic
pat
hway
s of
elim
inat
ion
are
less
of a
con
cern
, but
unc
erta
inty
stil
l exi
sts
on t
he a
ppro
pria
te d
osin
g of
ARV
dru
gs fo
r pr
eter
m a
nd lo
w-b
irth
-wei
ght i
nfan
ts.
b Th
is fo
rmul
atio
n w
ill b
e ph
ased
out
of u
se o
ver t
ime,
and
pro
gram
mes
sho
uld
tran
siti
on t
o us
ing
the
120
mg/
60 m
g di
sper
sibl
e sc
ored
tab
lets
.

506 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Tabl
e A1
.2 S
impl
ified
dos
ing
of c
hild
-fri
endl
y so
lid f
orm
ulat
ions
for
onc
e-da
ily d
osin
g fo
r in
fant
s an
d ch
ildre
n fo
ur w
eeks
and
old
era
Dru
gSt
reng
th o
f pae
diat
ric
tabl
et
Num
ber
of t
able
ts o
r ca
psul
es b
y w
eigh
t ba
nd o
nce
daily
Stre
ngth
of
adul
t ta
blet
Num
ber
of t
able
ts o
r ca
psul
es b
y w
eigh
t ba
nd o
nce
daily
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
EFVb
Tabl
et (s
core
d) 2
00 m
g–
–1
1.5
1.5
-2
ABC
/3TC
Tabl
et (d
ispe
rsib
le) 6
0 m
g/30
mg
23
45
660
0 m
g/30
0 m
g1
Tabl
et (d
ispe
rsib
le) 1
20 m
g/60
mg
11.
52
2.5
3
TAF/
FTCc
Tabl
et 2
5 m
g/ 2
00 m
g–
––
––
25 m
g/20
0 m
g1
ATVd
Caps
ules
100
mg
––
22
230
0 m
g1e
Caps
ules
200
mg
––
11
1
DRV
fTa
blet
600
mg
––
–1
160
0 m
g1
Tabl
et 1
50 m
g–
––
44
RTVg
Tabl
et 2
5 m
g–
––
44
100
mg
1
Tabl
et 5
0 m
g–
––
22
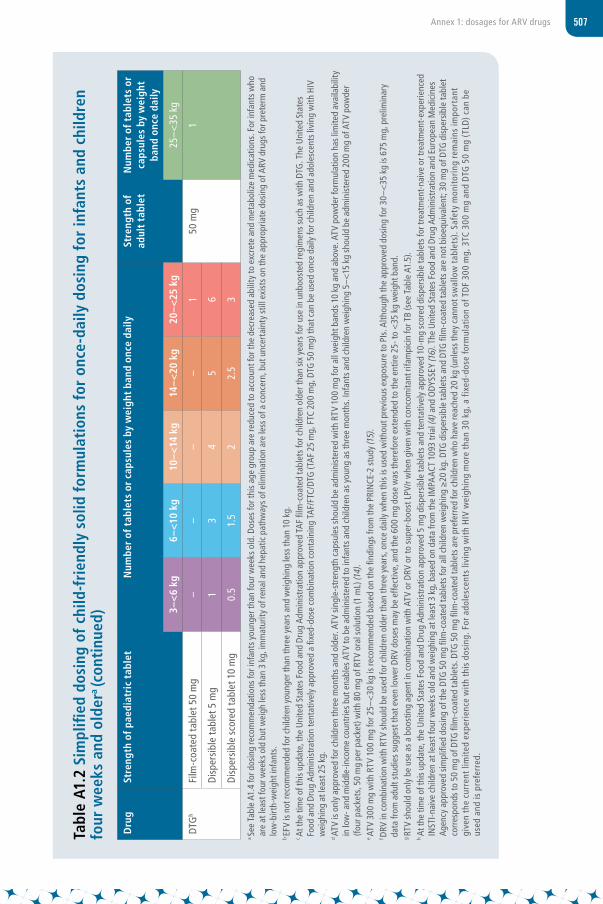
507Annex 1: dosages for ARV drugs
Tabl
e A1
.2 S
impl
ified
dos
ing
of c
hild
-fri
endl
y so
lid f
orm
ulat
ions
for
onc
e-da
ily d
osin
g fo
r in
fant
s an
d ch
ildre
n fo
ur w
eeks
and
old
era (c
onti
nued
)
Dru
gSt
reng
th o
f pae
diat
ric
tabl
et
Num
ber
of t
able
ts o
r ca
psul
es b
y w
eigh
t ba
nd o
nce
daily
Stre
ngth
of
adul
t ta
blet
Num
ber
of t
able
ts o
r ca
psul
es b
y w
eigh
t ba
nd o
nce
daily
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
DTG
hFi
lm-c
oate
d ta
blet
50
mg
––
––
150
mg
1
Dis
pers
ible
tabl
et 5
mg
13
45
6
Dis
pers
ible
sco
red
tabl
et 1
0 m
g0.
51.
52
2.5
3
a Se
e Ta
ble
A1.4
for d
osin
g re
com
men
datio
ns fo
r inf
ants
you
nger
than
four
wee
ks o
ld. D
oses
for t
his
age
grou
p ar
e re
duce
d to
acc
ount
for t
he d
ecre
ased
abi
lity
to e
xcre
te a
nd m
etab
oliz
e m
edic
atio
ns. F
or in
fant
s w
ho
are
at le
ast f
our w
eeks
old
but
wei
gh le
ss th
an 3
kg,
imm
atur
ity o
f ren
al a
nd h
epat
ic p
athw
ays
of e
limin
atio
n ar
e le
ss o
f a c
once
rn, b
ut u
ncer
tain
ty s
till e
xist
s on
the
appr
opria
te d
osin
g of
ARV
dru
gs fo
r pre
term
and
lo
w-b
irth-
wei
ght i
nfan
ts.
b EF
V is
not r
ecom
men
ded
for c
hild
ren
youn
ger t
han
thre
e ye
ars
and
wei
ghin
g le
ss th
an 1
0 kg
.c
At th
e tim
e of
this
upda
te, t
he U
nite
d St
ates
Foo
d an
d Dr
ug A
dmin
istr
atio
n ap
prov
ed T
AF
film
-coa
ted
tabl
ets
for c
hild
ren
olde
r tha
n si
x ye
ars
for u
se in
unb
oost
ed re
gim
ens
such
as
with
DTG
. The
Uni
ted
Stat
es
Food
and
Dru
g Ad
min
istr
atio
n te
ntat
ivel
y ap
prov
ed a
fixe
d-do
se c
ombi
natio
n co
ntai
ning
TA
F/FT
C/DT
G (T
AF
25 m
g, F
TC 2
00 m
g, D
TG 5
0 m
g) th
at c
an b
e us
ed o
nce
daily
for c
hild
ren
and
adol
esce
nts
livin
g w
ith H
IV
wei
ghin
g at
leas
t 25
kg.
d AT
V is
only
app
rove
d fo
r chi
ldre
n th
ree
mon
ths a
nd o
lder
. ATV
sin
gle-
stre
ngth
cap
sule
s sho
uld
be a
dmin
iste
red
with
RTV
100
mg
for a
ll w
eigh
t ban
ds 1
0 kg
and
abo
ve. A
TV p
owde
r for
mul
atio
n ha
s lim
ited
avai
labi
lity
in lo
w- a
nd m
iddl
e-in
com
e co
untr
ies
but e
nabl
es A
TV to
be
adm
inis
tere
d to
infa
nts
and
child
ren
as y
oung
as
thre
e m
onth
s. In
fant
s an
d ch
ildre
n w
eigh
ing
5–<1
5 kg
sho
uld
be a
dmin
iste
red
200
mg
of A
TV p
owde
r (fo
ur p
acke
ts, 5
0 m
g pe
r pac
ket)
with
80
mg
of R
TV o
ral s
olut
ion
(1 m
L) (1
4).
e AT
V 30
0 m
g w
ith R
TV 1
00 m
g fo
r 25–
<30
kg
is re
com
men
ded
base
d on
the
findi
ngs
from
the
PRIN
CE-2
stu
dy (1
5).
f DRV
in c
ombi
natio
n w
ith R
TV s
houl
d be
use
d fo
r chi
ldre
n ol
der t
han
thre
e ye
ars,
onc
e da
ily w
hen
this
is us
ed w
ithou
t pre
viou
s ex
posu
re to
PIs
. Alth
ough
the
appr
oved
dos
ing
for 3
0–<
35 k
g is
675
mg,
pre
limin
ary
data
from
adu
lt st
udie
s su
gges
t tha
t eve
n lo
wer
DRV
dos
es m
ay b
e ef
fect
ive,
and
the
600
mg
dose
was
ther
efor
e ex
tend
ed to
the
entir
e 25
- to
<35
kg
wei
ght b
and.
g RT
V sh
ould
onl
y be
use
as
a bo
ostin
g ag
ent i
n co
mbi
natio
n w
ith A
TV o
r DRV
or t
o su
per-
boos
t LPV
/r w
hen
give
n w
ith c
onco
mita
nt ri
fam
pici
n fo
r TB
(see
Tab
le A
1.5)
.h
At th
e tim
e of
this
upda
te, t
he U
nite
d St
ates
Foo
d an
d Dr
ug A
dmin
istr
atio
n ap
prov
ed 5
mg
disp
ersi
ble
tabl
ets
and
tent
ativ
ely
appr
oved
10-
mg
scor
ed d
ispe
rsib
le ta
blet
s fo
r tre
atm
ent-
naiv
e or
trea
tmen
t-ex
perie
nced
IN
STI-n
aive
chi
ldre
n at
leas
t fou
r wee
ks o
ld a
nd w
eigh
ing
at le
ast 3
kg,
bas
ed o
n da
ta fr
om th
e IM
PAAC
T 10
93 tr
ial (
4) a
nd O
DYSS
EY (1
6). T
he U
nite
d St
ates
Foo
d an
d Dr
ug A
dmin
istr
atio
n an
d Eu
rope
an M
edic
ines
Ag
ency
app
rove
d si
mpl
ified
dos
ing
of th
e DT
G 5
0 m
g fil
m-c
oate
d ta
blet
s fo
r all
child
ren
wei
ghin
g ≥
20 k
g. D
TG d
ispe
rsib
le ta
blet
s an
d DT
G fi
lm-c
oate
d ta
blet
s ar
e no
t bio
equi
vale
nt; 3
0 m
g of
DTG
dis
pers
ible
tabl
et
corr
espo
nds
to 5
0 m
g of
DTG
film
-coa
ted
tabl
ets.
DTG
50
mg
film
-coa
ted
tabl
ets
are
pref
erre
d fo
r chi
ldre
n w
ho h
ave
reac
hed
20 k
g (u
nles
s th
ey c
anno
t sw
allo
w t
able
ts).
Safe
ty m
onito
ring
rem
ains
impo
rtan
t gi
ven
the
curr
ent l
imite
d ex
peri
ence
wit
h th
is d
osin
g. F
or a
dole
scen
ts li
ving
wit
h H
IV w
eigh
ing
mor
e th
an 3
0 kg
, a fi
xed-
dose
form
ulat
ion
of T
DF
300
mg,
3TC
300
mg
and
DTG
50
mg
(TLD
) can
be
used
and
is p
refe
rred
.

508 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Tabl
e A1
.3 S
impl
ified
dos
ing
of c
hild
-fri
endl
y so
lid a
nd o
ral l
iqui
d fo
rmul
atio
ns f
or t
wic
e-da
ily d
osin
g fo
r in
fant
s an
d ch
ildre
n fo
ur w
eeks
of
age
and
olde
ra
Dru
gSt
reng
th o
f pa
edia
tric
tab
lets
N
umbe
r of
tab
lets
or
mL
by w
eigh
t-ba
nd m
orni
ng (A
M) a
nd e
veni
ng (P
M)
Stre
ngth
of
adul
t ta
blet
N
umbe
r of
tab
lets
by
wei
ght
band
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
AM
PMA
MPM
AM
PMA
MPM
AM
PMA
MPM
Solid
for
mul
atio
ns
AZT
Tabl
et (d
ispe
rsib
le)
60 m
g1
11.
51.
52
22.
52.
53
330
0 m
g1
1
ABC
Tabl
et (d
ispe
rsib
le)
60 m
g 1
11.
51.
52
22.
52.
53
330
0 m
g1
1
LPV/
rb Ta
blet
100
mg/
25 m
g–
––
–2
12
22
2–
33
Pelle
ts 4
0 m
g/10
mg
22
33
44
55
66
––
Gra
nule
s 40
mg/
10 m
g sa
chet
22
33
44
55
66
––
DRV
cTa
blet
75
mg
––
––
––
55
55
400
mg
11
RTVd
Tabl
et 2
5 m
g–
––
––
–2
22
210
0 m
g1
1
Tabl
et 5
0 m
g–
––
––
–1
11
1
RALe
Chew
able
tabl
ets
25 m
g1
12
23
34
46
640
0 m
g1
1
Chew
able
tabl
ets
100
mg
––
––
––
11
1.5
1.5
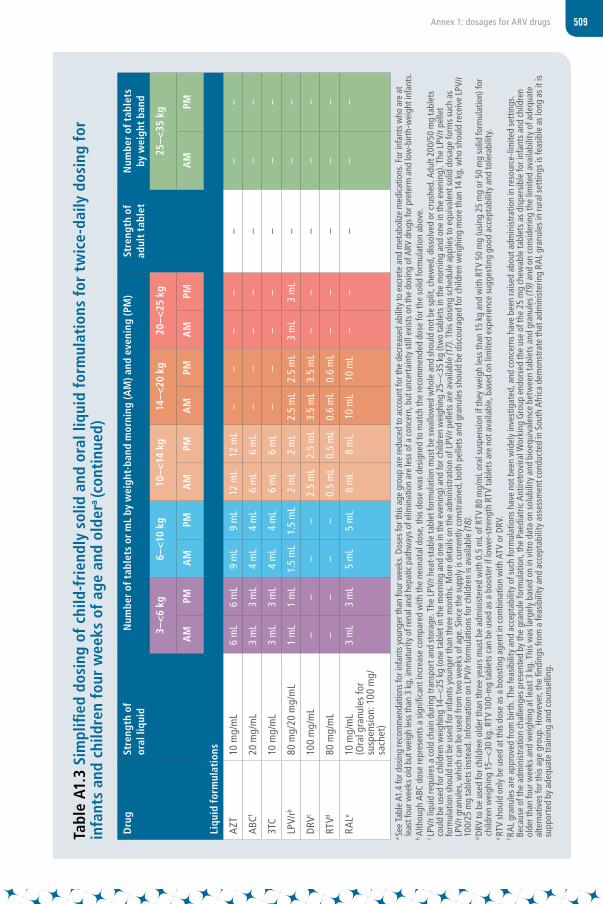
509Annex 1: dosages for ARV drugs
Tabl
e A1
.3 S
impl
ified
dos
ing
of c
hild
-fri
endl
y so
lid a
nd o
ral l
iqui
d fo
rmul
atio
ns f
or t
wic
e-da
ily d
osin
g fo
r in
fant
s an
d ch
ildre
n fo
ur w
eeks
of
age
and
olde
ra (c
onti
nued
)
Dru
gSt
reng
th o
f or
al li
quid
N
umbe
r of
tab
lets
or
mL
by w
eigh
t-ba
nd m
orni
ng (A
M) a
nd e
veni
ng (P
M)
Stre
ngth
of
adul
t ta
blet
N
umbe
r of
tab
lets
by
wei
ght
band
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
AM
PMA
MPM
AM
PMA
MPM
AM
PMA
MPM
Liqu
id f
orm
ulat
ions
AZT
10 m
g/m
L6
mL
6 m
L9
mL
9 m
L12
mL
12 m
L–
––
––
––
ABC
f20
mg/
mL
3 m
L3
mL
4 m
L4
mL
6 m
L6
mL
––
––
––
–
3TC
10 m
g/m
L3
mL
3 m
L4
mL
4 m
L6
mL
6 m
L–
––
––
––
LPV/
rb80
mg/
20 m
g/m
L1
mL
1 m
L1.
5 m
L1.
5 m
L2
mL
2 m
L2.
5 m
L2.
5 m
L3
mL
3 m
L–
––
DRV
c10
0 m
g/m
L–
––
–2.
5 m
L2.
5 m
L3.
5 m
L3.
5 m
L–
––
––
RTVd
80 m
g/m
L–
––
–0.
5 m
L0.
5 m
L0.
6 m
L0.
6 m
L–
––
––
RALe
10 m
g/m
L
(Ora
l gra
nule
s fo
r su
spen
sion
: 100
mg/
sach
et)
3 m
L3
mL
5 m
L5
mL
8 m
L8
mL
10 m
L10
mL
––
––
–
a Se
e Ta
ble
A1.4
for d
osin
g re
com
men
datio
ns fo
r inf
ants
you
nger
than
four
wee
ks. D
oses
for t
his a
ge g
roup
are
redu
ced
to a
ccou
nt fo
r the
dec
reas
ed a
bilit
y to
exc
rete
and
met
abol
ize m
edic
atio
ns. F
or in
fant
s who
are
at
leas
t fou
r wee
ks o
ld b
ut w
eigh
less
than
3 k
g, im
mat
urity
of r
enal
and
hep
atic
path
way
s of e
limin
atio
n ar
e le
ss o
f a c
once
rn, b
ut u
ncer
tain
ty st
ill e
xist
s on
the
dosin
g of
ARV
dru
gs fo
r pre
term
and
low
-birt
h-w
eigh
t inf
ants
.b
Alth
ough
ABC
dos
e re
pres
ents
a s
igni
fican
t inc
reas
e co
mpa
red
with
the
neon
atal
dos
e, th
is do
se w
as d
esig
ned
to m
atch
the
reco
mm
ende
d do
se fo
r the
sol
id fo
rmul
atio
n ab
ove.
c LP
V/r l
iqui
d re
quire
s a
cold
cha
in d
urin
g tr
ansp
ort a
nd s
tora
ge. T
he L
PV/r
heat
-sta
ble
tabl
et fo
rmul
atio
n m
ust b
e sw
allo
wed
who
le a
nd s
houl
d no
t be
split
, che
wed
, dis
solv
ed o
r cru
shed
. Adu
lt 20
0/50
mg
tabl
ets
coul
d be
use
d fo
r chi
ldre
n w
eigh
ing
14–<
25 k
g (o
ne ta
blet
in th
e m
orni
ng a
nd o
ne in
the
even
ing)
and
for c
hild
ren
wei
ghin
g 25
–<35
kg
(tw
o ta
blet
s in
the
mor
ning
and
one
in th
e ev
enin
g). T
he L
PV/r
pelle
t fo
rmul
atio
n sh
ould
not
be
used
for i
nfan
ts y
oung
er th
an th
ree
mon
ths.
Mor
e de
tails
on
the
adm
inis
trat
ion
of L
PV/r
pelle
ts a
re a
vaila
ble
(17)
. Thi
s do
sing
sch
edul
e ap
plie
s to
equ
ival
ent s
olid
dos
age
form
s su
ch a
s LP
V/r g
ranu
les,
whi
ch c
an b
e us
ed fr
om tw
o w
eeks
of a
ge. S
ince
the
supp
ly is
cur
rent
ly c
onst
rain
ed, b
oth
pelle
ts a
nd g
ranu
les
shou
ld b
e di
scou
rage
d fo
r chi
ldre
n w
eigh
ing
mor
e th
an 1
4 kg
, who
sho
uld
rece
ive
LPV/
r 10
0/25
mg
tabl
ets
inst
ead.
Info
rmat
ion
on L
PV/r
form
ulat
ions
for c
hild
ren
is av
aila
ble
(18)
.d
DRV
to b
e us
ed fo
r chi
ldre
n ol
der t
han
thre
e ye
ars
mus
t be
adm
inis
tere
d w
ith 0
.5 m
L of
RTV
80
mg/
mL
oral
sus
pens
ion
if th
ey w
eigh
less
than
15
kg a
nd w
ith R
TV 5
0 m
g (u
sing
25
mg
or 5
0 m
g so
lid fo
rmul
atio
n) fo
r ch
ildre
n w
eigh
ing
15–<
30 k
g. R
TV 1
00-m
g ta
blet
s ca
n be
use
d as
a b
oost
er if
low
er-s
tren
gth
RTV
tabl
ets
are
not a
vaila
ble,
bas
ed o
n lim
ited
expe
rienc
e su
gges
ting
good
acc
epta
bilit
y an
d to
lera
bilit
y.e
RTV
shou
ld o
nly
be u
sed
at th
is do
se a
s a
boos
ting
agen
t in
com
bina
tion
with
ATV
or D
RV.
f RA
L gr
anul
es a
re a
ppro
ved
from
birt
h. T
he fe
asib
ility
and
acc
epta
bilit
y of
suc
h fo
rmul
atio
ns h
ave
not b
een
wid
ely
inve
stig
ated
, and
con
cern
s ha
ve b
een
rais
ed a
bout
adm
inis
trat
ion
in re
sour
ce-li
mite
d se
ttin
gs.
Beca
use
of th
e ad
min
istr
atio
n ch
alle
nges
pre
sent
ed b
y th
e gr
anul
e fo
rmul
atio
n, th
e Pa
edia
tric
Ant
iretr
ovira
l Wor
king
Gro
up e
ndor
sed
the
use
of th
e 25
mg
chew
able
tabl
ets
as d
ispe
rsib
le fo
r inf
ants
and
chi
ldre
n ol
der t
han
four
wee
ks a
nd w
eigh
ing
at le
ast 3
kg.
Thi
s w
as la
rgel
y ba
sed
on in
vitr
o da
ta o
n so
lubi
lity
and
bioe
quiv
alen
ce b
etw
een
tabl
ets
and
gran
ules
(19)
and
on
cons
ider
ing
the
limite
d av
aila
bilit
y of
ade
quat
e al
tern
ativ
es fo
r thi
s ag
e gr
oup.
How
ever
, the
find
ings
from
a fe
asib
ility
and
acc
epta
bilit
y as
sess
men
t con
duct
ed in
Sou
th A
fric
a de
mon
stra
te th
at a
dmin
iste
ring
RAL
gran
ules
in ru
ral s
ettin
gs is
feas
ible
as
long
as
it is
su
ppor
ted
by a
dequ
ate
trai
ning
and
cou
nsel
ling.
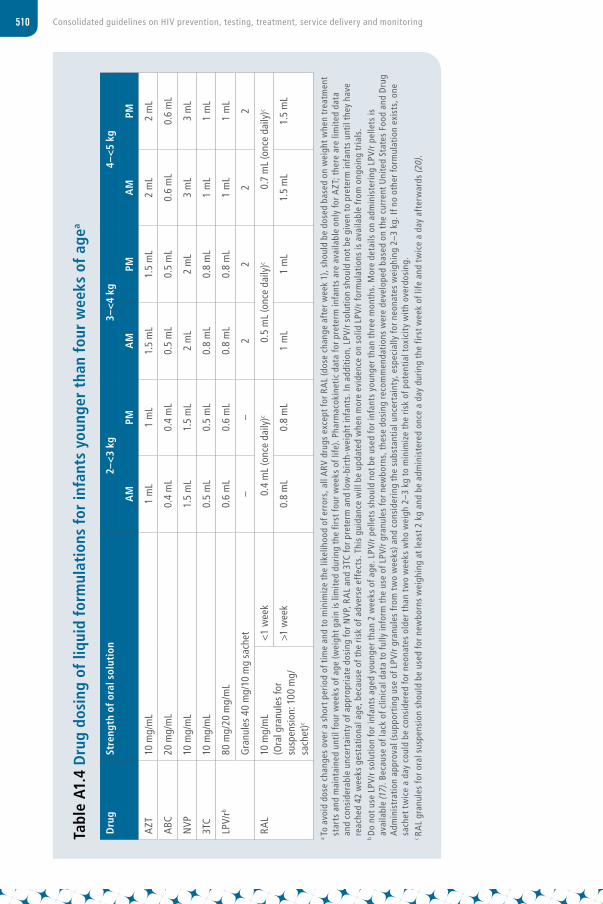
510 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Tabl
e A1
.4 D
rug
dosi
ng o
f liq
uid
form
ulat
ions
for
infa
nts
youn
ger
than
fou
r w
eeks
of
agea
Dru
gSt
reng
th o
f ora
l sol
utio
n2–
<3
kg3–
<4
kg4–
<5
kg
AM
PMA
MPM
AM
PM
AZT
10 m
g/m
L1
mL
1 m
L1.
5 m
L1.
5 m
L2
mL
2 m
L
ABC
20 m
g/m
L0.
4 m
L0.
4 m
L0.
5 m
L0.
5 m
L0.
6 m
L0.
6 m
L
NVP
10 m
g/m
L1.
5 m
L1.
5 m
L2
mL
2 m
L3
mL
3 m
L
3TC
10 m
g/m
L0.
5 m
L0.
5 m
L0.
8 m
L0.
8 m
L1
mL
1 m
L
LPV/
rb80
mg/
20 m
g/m
L0.
6 m
L0.
6 m
L0.
8 m
L0.
8 m
L1
mL
1 m
L
Gra
nule
s 40
mg/
10 m
g sa
chet
––
22
22
RAL
10 m
g/m
L (O
ral g
ranu
les
for
susp
ensi
on: 1
00 m
g/sa
chet
)c
<1
wee
k0.
4 m
L (o
nce
daily
)c0.
5 m
L (o
nce
daily
)c0.
7 m
L (o
nce
daily
)c
>1 w
eek
0.8
mL
0.8
mL
1 m
L1
mL
1.5
mL
1.5
mL
a To
avo
id d
ose
chan
ges
over
a s
hort
per
iod
of t
ime
and
to m
inim
ize
the
likel
ihoo
d of
err
ors,
all
ARV
dru
gs e
xcep
t for
RA
L (d
ose
chan
ge a
fter
wee
k 1)
, sho
uld
be d
osed
bas
ed o
n w
eigh
t whe
n tr
eatm
ent
star
ts a
nd m
aint
aine
d un
til fo
ur w
eeks
of a
ge (w
eigh
t gai
n is
lim
ited
duri
ng t
he fi
rst f
our w
eeks
of l
ife).
Phar
mac
okin
etic
dat
a fo
r pre
term
infa
nts
are
avai
labl
e on
ly fo
r AZT
; the
re a
re li
mite
d da
ta
and
cons
ider
able
unc
erta
inty
of a
ppro
pria
te d
osin
g fo
r NVP
, RA
L an
d 3T
C fo
r pre
term
and
low
-bir
th-w
eigh
t inf
ants
. In
addi
tion
, LPV
/r s
olut
ion
shou
ld n
ot b
e gi
ven
to p
rete
rm in
fant
s un
til t
hey
have
re
ache
d 42
wee
ks g
esta
tion
al a
ge, b
ecau
se o
f the
ris
k of
adv
erse
eff
ects
. Thi
s gu
idan
ce w
ill b
e up
date
d w
hen
mor
e ev
iden
ce o
n so
lid L
PV/r
form
ulat
ions
is a
vaila
ble
from
ong
oing
tria
ls.
b D
o no
t use
LPV
/r s
olut
ion
for i
nfan
ts a
ged
youn
ger t
han
2 w
eeks
of a
ge. L
PV/r
pel
lets
sho
uld
not b
e us
ed fo
r inf
ants
you
nger
tha
n th
ree
mon
ths.
Mor
e de
tails
on
adm
inis
teri
ng L
PV/r
pel
lets
is
avai
labl
e (1
7). B
ecau
se o
f lac
k of
clin
ical
dat
a to
fully
info
rm t
he u
se o
f LPV
/r g
ranu
les
for n
ewbo
rns,
the
se d
osin
g re
com
men
dati
ons
wer
e de
velo
ped
base
d on
the
cur
rent
Uni
ted
Stat
es F
ood
and
Dru
g A
dmin
istr
atio
n ap
prov
al (s
uppo
rtin
g us
e of
LPV
/r g
ranu
les
from
tw
o w
eeks
) and
con
side
ring
the
sub
stan
tial u
ncer
tain
ty, e
spec
ially
for n
eona
tes
wei
ghin
g 2–
3 kg
. If n
o ot
her f
orm
ulat
ion
exis
ts, o
ne
sach
et t
wic
e a
day
coul
d be
con
side
red
for n
eona
tes
olde
r tha
n tw
o w
eeks
who
wei
gh 2
–3 k
g to
min
imiz
e th
e ris
k of
pot
entia
l tox
icit
y w
ith
over
dosi
ng.
c RA
L gr
anul
es fo
r ora
l sus
pens
ion
shou
ld b
e us
ed fo
r new
born
s w
eigh
ing
at le
ast 2
kg
and
be a
dmin
iste
red
once
a d
ay d
urin
g th
e fir
st w
eek
of li
fe a
nd t
wic
e a
day
afte
rwar
ds (2
0).
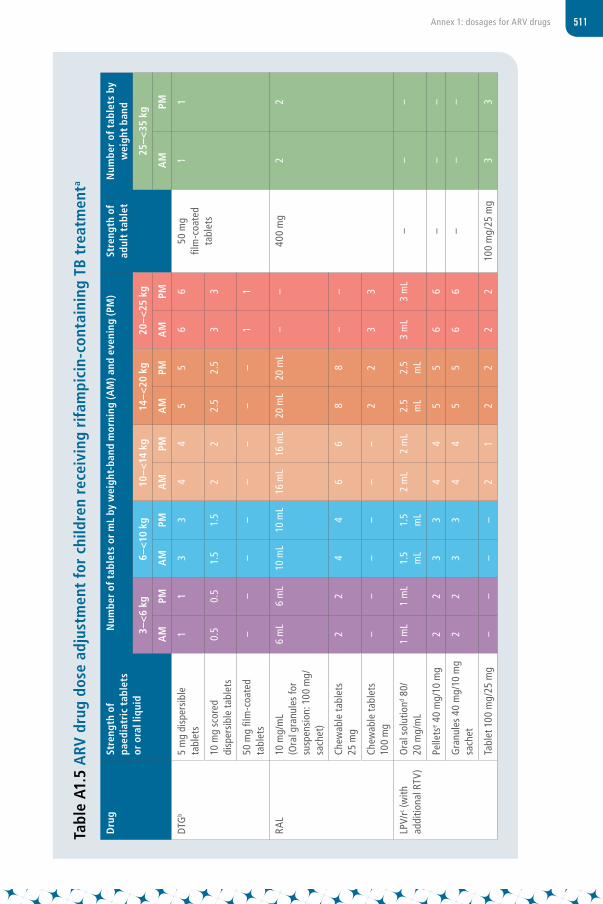
511Annex 1: dosages for ARV drugs
Tabl
e A1
.5 A
RV d
rug
dose
adj
ustm
ent
for
child
ren
rece
ivin
g ri
fam
pici
n-co
ntai
ning
TB
trea
tmen
ta
Dru
gSt
reng
th o
f pa
edia
tric
tab
lets
or
ora
l liq
uid
Num
ber
of t
able
ts o
r m
L by
wei
ght-
band
mor
ning
(AM
) and
eve
ning
(PM
)St
reng
th o
f ad
ult
tabl
et
Num
ber
of t
able
ts b
y w
eigh
t ba
nd
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
AM
PMA
MPM
AM
PMA
MPM
AM
PMA
MPM
DTG
b5
mg
disp
ersi
ble
tabl
ets
11
33
44
55
6 6
50 m
g
film
-coa
ted
tabl
ets
11
10 m
g sc
ored
di
sper
sibl
e ta
blet
s0.
50.
51.
51.
52
22.
52.
53
3
50 m
g fil
m-c
oate
d ta
blet
s–
––
––
––
–1
1
RAL
10 m
g/m
L (O
ral g
ranu
les
for
susp
ensi
on: 1
00 m
g/sa
chet
)
6 m
L6
mL
10 m
L10
mL
16 m
L16
mL
20 m
L20
mL
––
400
mg
22
Chew
able
tabl
ets
25 m
g2
24
46
68
8–
–
Chew
able
tabl
ets
100
mg
––
––
––
22
33
LPV/
rc (w
ith
addi
tiona
l RTV
)O
ral s
olut
iond 8
0/
20 m
g/m
L1
mL
1 m
L1.
5 m
L1.
5 m
L2
mL
2 m
L2.
5 m
L2.
5 m
L3
mL
3 m
L–
––
Pelle
tse 4
0 m
g/10
mg
22
33
44
55
66
––
–
Gra
nule
s 40
mg/
10 m
g sa
chet
22
33
44
55
66
––
–
Tabl
et 1
00 m
g/25
mg
––
––
21
22
22
100
mg/
25 m
g3
3
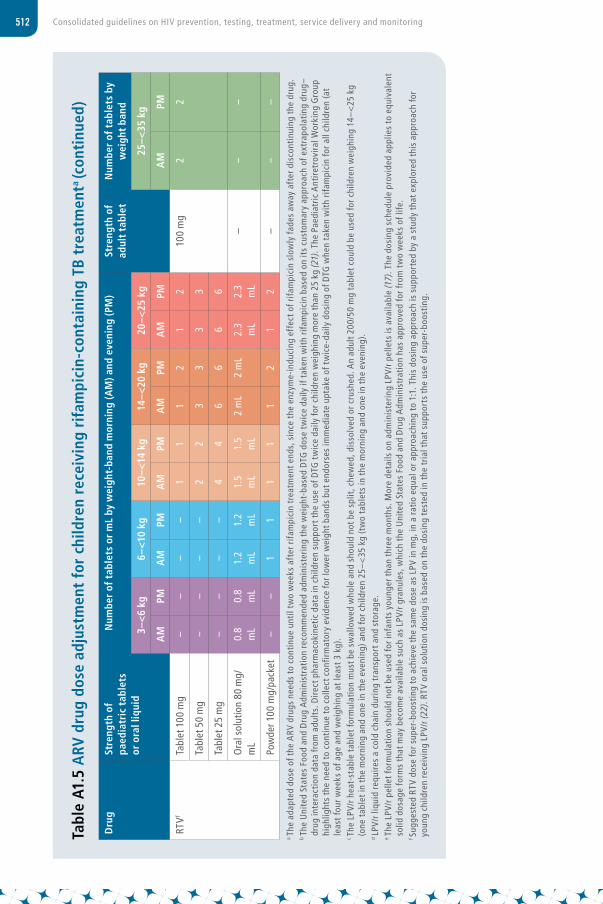
512 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Tabl
e A1
.5 A
RV d
rug
dose
adj
ustm
ent
for
child
ren
rece
ivin
g ri
fam
pici
n-co
ntai
ning
TB
trea
tmen
ta (c
onti
nued
)
Dru
gSt
reng
th o
f pa
edia
tric
tab
lets
or
ora
l liq
uid
Num
ber
of t
able
ts o
r m
L by
wei
ght-
band
mor
ning
(AM
) and
eve
ning
(PM
)St
reng
th o
f ad
ult
tabl
et
Num
ber
of t
able
ts b
y w
eigh
t ba
nd
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
AM
PMA
MPM
AM
PMA
MPM
AM
PMA
MPM
RTVf
Tabl
et 1
00 m
g–
––
–1
11
21
210
0 m
g2
2
Tabl
et 5
0 m
g–
––
–2
23
33
3
Tabl
et 2
5 m
g–
––
–4
46
66
6
Ora
l sol
utio
n 80
mg/
mL
0.8
mL
0.8
mL
1.2
mL
1.2
mL
1.5
mL
1.5
mL
2 m
L2
mL
2.3
mL
2.3
mL
––
–
Pow
der 1
00 m
g/pa
cket
––
11
11
12
12
––
–
a Th
e ad
apte
d do
se o
f the
ARV
dru
gs n
eeds
to
cont
inue
unt
il tw
o w
eeks
aft
er r
ifam
pici
n tr
eatm
ent e
nds,
sin
ce t
he e
nzym
e-in
duci
ng e
ffec
t of r
ifam
pici
n sl
owly
fade
s aw
ay a
fter
dis
cont
inui
ng t
he d
rug.
b Th
e U
nite
d St
ates
Foo
d an
d D
rug
Adm
inis
trat
ion
reco
mm
ende
d ad
min
iste
ring
the
wei
ght-
base
d D
TG d
ose
twic
e da
ily if
tak
en w
ith
rifa
mpi
cin
base
d on
its
cust
omar
y ap
proa
ch o
f ext
rapo
lati
ng d
rug–
drug
inte
ract
ion
data
from
adu
lts.
Dir
ect p
harm
acok
inet
ic d
ata
in c
hild
ren
supp
ort t
he u
se o
f DTG
tw
ice
daily
for c
hild
ren
wei
ghin
g m
ore
than
25
kg (2
1). T
he P
aedi
atri
c A
ntir
etro
vira
l Wor
king
Gro
up
high
light
s th
e ne
ed t
o co
ntin
ue t
o co
llect
con
firm
ator
y ev
iden
ce fo
r low
er w
eigh
t ban
ds b
ut e
ndor
ses
imm
edia
te u
ptak
e of
tw
ice-
daily
dos
ing
of D
TG w
hen
take
n w
ith
rifa
mpi
cin
for a
ll ch
ildre
n (a
t le
ast f
our w
eeks
of a
ge a
nd w
eigh
ing
at le
ast 3
kg)
.c
The
LPV/
r hea
t-st
able
tab
let f
orm
ulat
ion
mus
t be
swal
low
ed w
hole
and
sho
uld
not b
e sp
lit, c
hew
ed, d
isso
lved
or c
rush
ed. A
n ad
ult 2
00/5
0 m
g ta
blet
cou
ld b
e us
ed fo
r chi
ldre
n w
eigh
ing
14–<
25 k
g (o
ne t
able
t in
the
mor
ning
and
one
in t
he e
veni
ng) a
nd fo
r chi
ldre
n 25
–<35
kg
(tw
o ta
blet
s in
the
mor
ning
and
one
in t
he e
veni
ng).
d LP
V/r l
iqui
d re
quir
es a
col
d ch
ain
duri
ng t
rans
port
and
sto
rage
.e
The
LPV/
r pel
let f
orm
ulat
ion
shou
ld n
ot b
e us
ed fo
r inf
ants
you
nger
tha
n th
ree
mon
ths.
Mor
e de
tails
on
adm
inis
teri
ng L
PV/r
pel
lets
is a
vaila
ble
(17)
. The
dos
ing
sche
dule
pro
vide
d ap
plie
s to
equ
ival
ent
solid
dos
age
form
s th
at m
ay b
ecom
e av
aila
ble
such
as
LPV/
r gra
nule
s, w
hich
the
Uni
ted
Stat
es F
ood
and
Dru
g A
dmin
istr
atio
n ha
s ap
prov
ed fo
r fro
m t
wo
wee
ks o
f life
.f S
ugge
sted
RTV
dos
e fo
r sup
er-b
oost
ing
to a
chie
ve t
he s
ame
dose
as
LPV
in m
g, in
a ra
tio
equa
l or a
ppro
achi
ng t
o 1:
1. T
his
dosi
ng a
ppro
ach
is s
uppo
rted
by
a st
udy
that
exp
lore
d th
is a
ppro
ach
for
youn
g ch
ildre
n re
ceiv
ing
LPV/
r (22
). RT
V or
al s
olut
ion
dosi
ng is
bas
ed o
n th
e do
sing
tes
ted
in t
he t
rial t
hat s
uppo
rts
the
use
of s
uper
-boo
stin
g.

513Annex 1: dosages for ARV drugs
Tabl
e A1
.6 S
impl
ified
dos
ing
of is
onia
zid
and
co-t
rim
oxaz
ole
prop
hyla
xis
for
infa
nts
and
child
ren
at le
ast
four
w
eeks
old
Dru
gSt
reng
th o
f pa
edia
tric
tab
let
or o
ral l
iqui
d
Num
ber
of t
able
ts o
r m
L by
wei
ght
band
onc
e da
ilySt
reng
th o
f ad
ult
tabl
etN
umbe
r of
tab
lets
by
wei
ght
band
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
Ison
iazi
d10
0 m
g0.
51
1.5
22.
530
0 m
g1
Co-t
rimox
azol
e (s
ulfa
met
hoxa
zole
an
d tr
imet
hopr
im)
Susp
ensi
on 2
00 m
g/
40 p
er 5
mL
2.5
mL
5 m
L5
mL
10 m
L10
mL
––
Tabl
ets
(dis
pers
ible
) 10
0 m
g/20
mg
12
24
4–
–
Tabl
ets
(sco
red)
40
0 m
g/80
mg
–0.
50.
51
140
0 m
g/80
mg
2
Tabl
ets
(sco
red)
80
0 m
g/16
0 m
g–
––
0.5
0.5
800
mg/
160
mg
1
Ison
iazi
d/
(sul
fam
etho
xazo
le
and
trim
etho
prim
)/B6
Tabl
ets
(sco
red)
30
0 m
g/(8
00 m
g/
160
mg)
/25
mg
––
–0.
50.
530
0 m
g/
(800
mg/
16
0 m
g)/
25 m
g
1
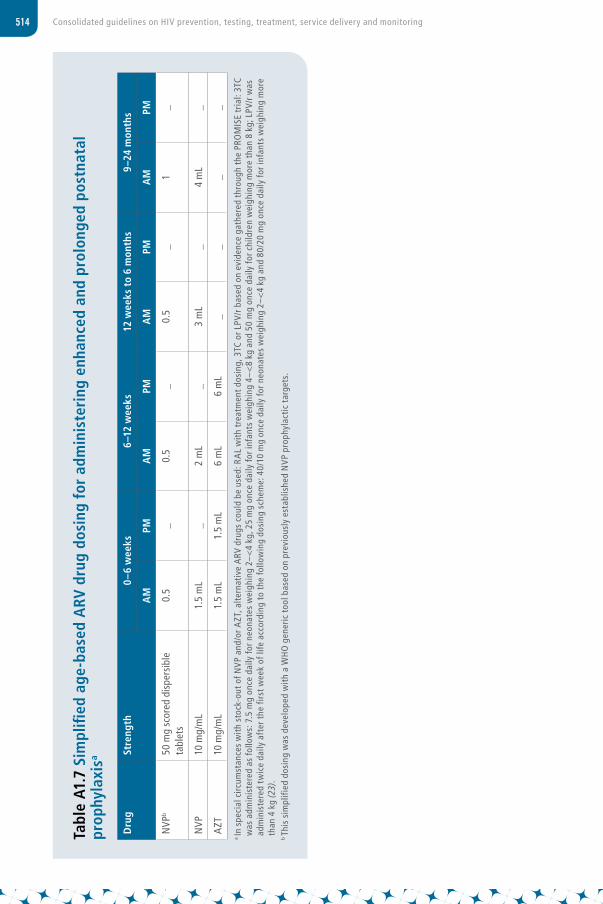
514 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Tabl
e A1
.7 S
impl
ified
age
-bas
ed A
RV d
rug
dosi
ng f
or a
dmin
iste
ring
enh
ance
d an
d pr
olon
ged
post
nata
l pr
ophy
laxi
sa
Dru
gSt
reng
th
0–6
wee
ks6–
12 w
eeks
12 w
eeks
to
6 m
onth
s9–
24 m
onth
s
AM
PMA
MPM
AM
PMA
MPM
NVP
b50
mg
scor
ed d
ispe
rsib
le
tabl
ets
0.5
_0.
5_
0.5
_1
_
NVP
10 m
g/m
L1.
5 m
L_
2 m
L_
3 m
L_
4 m
L_
AZT
10 m
g/m
L1.
5 m
L1.
5 m
L6
mL
6 m
L_
__
_
a In
spe
cial
circ
umst
ance
s w
ith
stoc
k-ou
t of N
VP a
nd/o
r AZT
, alte
rnat
ive
ARV
dru
gs c
ould
be
used
: RA
L w
ith
trea
tmen
t dos
ing,
3TC
or L
PV/r
bas
ed o
n ev
iden
ce g
athe
red
thro
ugh
the
PRO
MIS
E tr
ial:
3TC
was
adm
inis
tere
d as
follo
ws:
7.5
mg
once
dai
ly fo
r neo
nate
s w
eigh
ing
2–<
4 kg
, 25
mg
once
dai
ly fo
r inf
ants
wei
ghin
g 4–
<8
kg a
nd 5
0 m
g on
ce d
aily
for c
hild
ren
wei
ghin
g m
ore
than
8 k
g; L
PV/r
was
ad
min
iste
red
twic
e da
ily a
fter
the
firs
t wee
k of
life
acc
ordi
ng t
o th
e fo
llow
ing
dosi
ng s
chem
e: 4
0/10
mg
once
dai
ly fo
r neo
nate
s w
eigh
ing
2–<
4 kg
and
80/
20 m
g on
ce d
aily
for i
nfan
ts w
eigh
ing
mor
e th
an 4
kg
(23)
.b Th
is s
impl
ified
dos
ing
was
dev
elop
ed w
ith
a W
HO
gen
eric
too
l bas
ed o
n pr
evio
usly
est
ablis
hed
NVP
pro
phyl
actic
tar
gets
.

515Annex 1: dosages for ARV drugs
Optimal ARV drug formulary for childrenIn recent years, a number of improved ARV drug formulations have become available, such as dispersible, scored fixed-dose combination tablets that have replaced traditional liquid formulations. These products have greatly simplified the delivery of HIV treatment for children in low-income settings; however, the proliferation of options has resulted in a multiplicity of formulations across regimens and weight bands. Generic manufacturers use economies of scale to maintain affordable pricing, but fragmentation of demand across too many duplicative products creates instability in the reliable supply of ARV dosage forms for children and complicates procurement and supply chain management.
Partners of the ARV Procurement Working Group (24) and of the Global Accelerator for Paediatric Formulations Network (16) provide formulary guidance to programmes on selecting optimal ARV drugs for children, which have been defined using a robust set of criteria. The formulary was first developed in 2011 but is routinely revised to correspond to current WHO guidelines and available products. The current Optimal Formulary was revised in December 2020 and released in April 2021 (25). It now includes seven products that deliver recommended and appropriate first and second-line regimens across all weight bands for children. Programmes are encouraged to procure dosage forms for children that are included in the Optimal ARV Formulary for Children. During periods of transition or in special circumstances (neonatal treatment, TB co-treatment and third-line ART), dosage forms included on the ARV Limited-use Formulary are sufficient to provide appropriate dosing across weight bands for children (26).
The need for new formulationsAs part of the Global Accelerator for Paediatric Formulations Network, the work of the Paediatric Antiretroviral Working Group and the Paediatric ARV Drug Optimization (27,28) groups continue to highlight the urgent need for better age-appropriate formulations for infants and children living with HIV. An additional solid fixed-dose combination formulation is under the final stage of approval (ABC/3TC/LPV/r granules). In addition, the availability of co-formulated DRV/r in a heat-stable fixed-dose combination is critical to facilitate treatment sequencing and uptake of future second- and third-line regimens for children. Several formulations containing approved ARV drugs for children have been formally given priority and are listed in Table A1.6. Finally, additional formulations containing newer drugs for which there is currently no indication for children were considered, and the central future role of DTG and TAF in optimizing dose, sequencing and harmonization across age groups was highlighted.
In moving towards promoting drug optimization for children and adolescents, WHO will continue to work to simplify prescribing, dispensing and dosing guidance and work with the pharmaceutical industry (originator and generic) and other partners to develop more practical recommendations on the range of formulations required to safely accelerate the scaling up of ART for children.

516 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
Box
A1.1
Ant
icip
ated
sim
plifi
ed d
osin
g fo
r fo
rmul
atio
ns u
nder
dev
elop
men
t
Dru
gSt
reng
th o
f pae
diat
ric
tabl
ets
or
ora
l liq
uid
Num
ber
of t
able
ts o
r m
L by
wei
ght-
band
mor
ning
(AM
) and
eve
ning
(PM
)
3–<
6 kg
6–<1
0 kg
10–<
14 k
g14
–<20
kg
20–<
25 k
g25
–<35
kg
AM
PMA
MPM
AM
PMA
MPM
AM
PMA
MPM
ABC
/3TC
/LPV
/r 30
mg/
15 m
g/40
mg/
10 m
g gr
anul
es2
23
34
45
56
6–
DRV
/r12
0 m
g/20
mg
tabl
et–
––
–2
23
33
34
4
ABC
/3TC
/DTG
aD
ispe
rsib
le 6
0 m
g/30
mg/
5 m
g ta
blet
–3
45
6–
a Th
is d
osag
e fo
rm is
the
one
iden
tifie
d by
the
PA
DO
4 gr
oup
(28)
as
the
mos
t lik
ely
to d
eliv
er a
ppro
pria
te d
ose
base
d on
the
bes
t ava
ilabl
e in
form
atio
n.
517Annex 1: dosages for ARV drugs
References1. WHO ARV dosing generic tool [website]. Geneva: World Health Organization; 2021
(https://www.who.int/groups/antiretroviral-drug-optimization, accessed 1 June 2021).
2. Annex 1. Summary of product characteristics. Tivicay. Amsterdam: European Medicines Agency; 2020 (https://www.ema.europa.eu/en/documents/product-information/tivicay-epar-product-information_en.pdf, accessed 1 June 2021).
3. FDA approves drug to treat infants and children with HIV. Washington (DC): United States Food and Drug Administration; 2020 (https://www.fda.gov/news-events/press-announcements/fda-approves-drug-treat-infants-and-children-hiv?utm_campaign=061220_PR_United States Food and Drug Administration%20Approves%20Drug%20to%20Treat%20Infants%20and%20Children%20with%20HIV&utm_medium=email&utm_source=Eloqua, accessed 1 June 2021).
4. Safety of and immune response to dolutegravir in HIV-1 infected infants, children, and Adolescents. Bethesda (MD): ClinicalTrials.gov; 2020 (https://clinicaltrials.gov/ct2/show/NCT01302847, accessed 1 June 2021).
5. Turkova A. Dolutegravir-based ART is superior to NNRTI/PI-based ART in children and adolescents. 28th Conference on Retroviruses and Opportunistic Infections, virtual, 3 June–3 November 2021 (https://www.croiconference.org/abstract/dolutegravir-based-art-is-superior-to-nnrti-pi-based-art-in-children-and-adolescents, accessed 1 June 2021).
6. Dolutegravir tablet for oral suspension. Washington (DC): United States Food and Drug Administration; 2020 (https://www.accessdata.fda.gov/drugsatfda_docs/pepfar/214521PI.pdf, accessed 1 June 2021).
7. Jacobs TG, Svensson EM, Musiime V, Rojo P, Dooley KE, McIlleron H. Pharmacokinetics of antiretroviral and tuberculosis drugs in children with HIV/TB co-infection: a systematic review. J Antimicrob Chemother. 2020;75:3433–57.
8. Teppler H, Thompson K, Chain A, Mathe M, Nachman S, Clarke D. Crushing of raltegravir (RAL) chewable tablets for administration in infants and young children. International Workshop on HIV Pediatrics, Paris, France, 21–22 July 2017.
9. GENVOYA® (elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide) tablets, for oral use. Washington (DC): United States Food and Drug Administration; 2017 (https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/207561s013lbl.pdf, accessed 1 June 2021).
10. Paediatric ARV dosing dashboard [website]. Geneva: World Health Organization; 2021 (https://www.who.int/groups/antiretroviral-drug-optimization, accessed 1 June 2021).
11. World Health Organization prequalification [website]. Geneva: World Health Organization; 2021 (http://apps.who.int/prequal, accessed 1 June 2021).
12. Quick reference guide for PEPFAR Database; interactive database for antiretroviral (ARV) drugs tentatively approved or approved that are eligible for procurement. Washington (DC): United States Food and Drug Administration; 2021 (https://www.fda.gov/InternationalPrograms/PEPFAR/ucm119231.htm, accessed 1 June 2021).
13. Sourcing and management of health products [website]. Geneva: Global Fund to Fight AIDS, Tuberculosis and Malaria; 2021 (https://www.theglobalfund.org/en/sourcing-management/quality-assurance/medicines, accessed 1 June 2021.
14. REYATAZ® (atazanavir) oral powder. Washington (DC): United States Food and Drug Administration; 2018 (https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021567s042,206352s007lbl.pdf, accessed 1 June 2021).

518 Consolidated guidelines on HIV prevention, testing, treatment, service delivery and monitoring
15. Cotton MF, Liberty A, Torres-Escobar I, Gonzalez-Tome MI, Lissens J, Zaru L et al. Safety and efficacy of atazanavir powder and ritonavir in HIV-1-infected infants and children from 3 months to <11 years of age: the PRINCE-2 Study. Pediatr Infect Dis J. 2018;37:e149–56.
16. A randomised trial of dolutegravir (DTG)-based antiretroviral therapy vs. standard of care (SOC) in children with HIV infection starting first-line or switching to second-line ART. Bethesda (MD): ClinicalTrials.gov; 2020 (https://clinicaltrials.gov/ct2/show/NCT02259127, accessed 1 June 2021).
17. WHO, Interagency Task Team (IATT) on Prevention of HIV Infection in Pregnant Women, Mothers and their Children, UNICEF). Fact sheet on lopinavir and ritonavir (LPV/R) oral pellets: 40 mg/10 mg per capsule bottle pack containing 120 capsules. Geneva: World Health Organization; 2015 (https://apps.who.int/iris/handle/10665/193543, accessed 1 June 2021).
18. Lopinavir/ritonavir 40 mg/10 mg pellets and granules and 100/25 mg tablets. ARV Procurement Working Group; 2020 (https://www.arvprocurementworkinggroup.org/lpv-r-supply, accessed 1 June 2021).
19. Fillekes Q, Mulenga V, Kabamba D, Kankasa C, Thomason MJ, Cook A et al. Pharmacokinetics of nevirapine in HIV-infected infants weighing 3 kg to less than 6 kg taking paediatric fixed dose combination tablets. AIDS. 2012;26:1795–800.
20. ISENTRESS® (raltegravir) film-coated tablets, for oral use, ISENTRESS® HD (raltegravir) film-coated tablets, for oral use, ISENTRESS® (raltegravir) chewable tablets, for oral use, ISENTRESS® (raltegravir) for oral suspension. Washington (DC): United States Food and Drug Administration; 2020 (https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/022145s042,203045s016,205786s008lblrpl.pdf, accessed 1 June 2021).
21. Bollen PDJ, Moore CL, Mujuru HA, Makumbi S, Kekitiinwa AR, Kaudha E et al. Simplified dolutegravir dosing for children with HIV weighing 20 kg or more: pharmacokinetic and safety substudies of the multicentre, randomised ODYSSEY trial. Lancet HIV. 2020;7:e533–44.
22. Rabie H, Denti P, Lee J, Masango M, Coovadia A, Pillay S et al. Lopinavir-ritonavir super-boosting in young HIV-infected children on rifampicin-based tuberculosis therapy compared with lopinavir-ritonavir without rifampicin: a pharmacokinetic modelling and clinical study. Lancet HIV. 2018:S2352-3018(18)30293-5.
23. Nagot N, Kankasa C, Tumwine JK, Meda N, Hofmeyr GJ, Vallo R, et al. Extended pre-exposure prophylaxis with lopinavir–ritonavir versus lamivudine to prevent HIV-1 transmission through breastfeeding up to 50 weeks in infants in Africa (ANRS 12174): a randomised controlled trial. The Lancet. 2016 Feb 6;387(10018):566-73.
24. ARV Procurement Working Group [website]. ARV Procurement Working Group; 2021 (https://arvprocurementworkinggroup.org/en, accessed 1 June 2021).
25. Global Accelerator for Paediatric Formulations Network (GAP-f) [website]. Geneva: World Health Organization; 2021 (https://www.who.int/initiatives/gap-f, accessed 1 June 2021).
26. The 2021 optimal formulary and limited-use list for antiretroviral drugs for children. Geneva: World Health Organization; 2021 (https://www.who.int/publications/i/item/9789240023529, accessed 1 June 2021).
27. Meeting report: Paediatric Antiretroviral Drug Optimization (PADO) Meeting 4. Geneva: World Health Organization; 2018 (https://cdn.who.int/media/docs/default-source/hq-hiv-hepatitis-and-stis-library/pado4.pdf?sfvrsn=26d4169c_5, accessed 1 June 2021).
28. Penazzato M, Townsend CL, Rakhmanina N, Cheng Y, Archary M, Cressey TR et al. Prioritising the most needed paediatric antiretroviral formulations: the PADO4 list. Lancet HIV. 2019;6:e623–31.
Top Related