






Languages
Pages
Legal


Addressing “Stress” in the Health Addressing “Stress” in the Health Care WorkforceCare Workforce
((Human Resources for HealthHuman Resources for Health))
Thomas C. RickettsThomas C. RickettsThe University of North CarolinaThe University of North Carolina

Workforce Problems and Workforce Problems and SolutionsSolutions
The problems are usually defined as The problems are usually defined as NationalNational (e.g. a national shortage of (e.g. a national shortage of nurses).nurses).
The impacts are very The impacts are very LocalLocal (a facility (a facility cannot operate effectively, care is cannot operate effectively, care is not available).not available).
States and Institutions States and Institutions are often left are often left to find the solutions.to find the solutions.

Current Research in HRHCurrent Research in HRH
To verify the national situation and To verify the national situation and interpret it. Stress = Shortageinterpret it. Stress = ShortageShortage of numbersShortage of prestigeShortage of organization
““Inconvenient Truths” from EconomicsInconvenient Truths” from EconomicsThe same work can be done by different
professionsThere are less expensive ways to prepare
professionals

Uncomfortable truths conflict with...Uncomfortable truths conflict with...
Practice Acts for Healing ArtsPractice Acts for Healing Arts(a.k.a. “Fighting Words”)
Professional IdentitiesProfessional IdentitiesCommitment, compassion
Awkward occupational impulsesAwkward occupational impulsesHypercredentialismGrowing fluidity in labor markets

Old line of Research ProductsOld line of Research Products
Shortage of Numbers and Shortage of Numbers and organization (EngagedResearch®)organization (EngagedResearch®)
Shortage of Prestige Shortage of Prestige (AdvocacyResearch©)(AdvocacyResearch©)
Inconvenient (and frankly ugly) Inconvenient (and frankly ugly) Truths (PureResearch™)Truths (PureResearch™)

New, Needed Product LineNew, Needed Product Line
© ® ™

The missing dataThe missing data
Regularly collected inventories that Regularly collected inventories that yield timely projections of supply yield timely projections of supply and needand need
Rhetoricof Shortage
Reliability of Data

The missing policyThe missing policy
Support for independent, ongoing, Support for independent, ongoing, longitudinal research capacity in longitudinal research capacity in health workforce.health workforce.
Yes, money.Yes, money.

Questions we need to getQuestions we need to get(and sometimes do)(and sometimes do)
What is the proper mix of _______ What is the proper mix of _______ necessary to provide ______ ?necessary to provide ______ ?Practitioners .... Access; Services ..... Cost-effective CareProviders .... Capacity to Meet Demand
How will directly paying ______ affect How will directly paying ______ affect ______?______?Nurses .... Overall CostsOther professionals .... Access to Care

Questions we always getQuestions we always getWhat will a _________ cost?What will a _________ cost?
Medical SchoolDental SchoolExpanded Ph.D. Nursing Program
Part of our SiloResearch™Product Line

Questions that are emergingQuestions that are emerging
Is there a “BIG TENT” for health workforce Is there a “BIG TENT” for health workforce policy making policy making And, by extension, research.
Example Example TITLE VIITITLE VII support to health support to health workforceworkforce
NOWNOW: a mix of related programs with little : a mix of related programs with little ability to show impact.ability to show impact.
FUTUREFUTURE: Coordinated policy with : Coordinated policy with measurable outputs and impacts.measurable outputs and impacts.

The Political Economy of The Political Economy of Underservice in the Safety NetUnderservice in the Safety Net
Current system depends on rigid Current system depends on rigid definition of local underservicedefinition of local underservice
Underservice is in demand....!Underservice is in demand....!RESEARCH Question: How can we RESEARCH Question: How can we
optimally allocate resources?optimally allocate resources?Safety netSystem and organization

Questions I wish we would ask...Questions I wish we would ask...
Can we train for Can we train for efficiencyefficiency as well as as well as we train for we train for proficiencyproficiency
What makes an What makes an interdisciplinaryinterdisciplinary team work well?team work well?
How can we evaluate programs like How can we evaluate programs like Title VII and VIII in a Title VII and VIII in a Fair and Fair and Balanced™Balanced™ way. way.

And the kickers...And the kickers...
Who actually Who actually takes care of takes care of sick people?sick people?
Who actually Who actually keeps people keeps people well?well?

First steps to wisdomFirst steps to wisdom
How many practitioners are there?How many practitioners are there?When do they enter and leave When do they enter and leave
practice?practice?Where do they practice?Where do they practice?What do they practice?What do they practice?

finfin

Components of Change, Physicians, Components of Change, Physicians, 2001-20052001-2005
New to file1,681
(status change 480newly licensed 1,201)
2001 Supply16,392
Left File1,304
2002 total16,769
Net gain 377
New to file1,563
(status change 508newly licensed 1,055)
2002 Supply16,769
Left File1,242
2003 total17,090
Net gain 384
Source: NC Health Professions Data System, with data provided by the North Carolina Medical Board.Note: Newly licensed physicians are those who are new to file with a license date in the current or previous year. Status change physicians are those who were licensed in NC in an earlier year but were either inactive or active out of state in the previous year.
New to file1,413
(status change 480newly licensed 933)
2003 Supply17,090
Left File1,154
2004 total17,349
Net gain 259
New to file1,550
(status change 667newly licensed 883)
2004 Supply17,349
Left File1,004
2005 total17,895
Net gain 546

10
12
14
16
18
20
22
Year
2005
2007
2009
2011
2013
2015
2017
2019
2021
2023
2025
2027
2029
Year
Pro
vid
er P
er 1
0,00
0 P
op
ula
tio
n
Baseline, not age-adj
Baseline
Medical Grads + 30%
Recruitment + 15%
Projections: PhysiciansProjections: Physicians
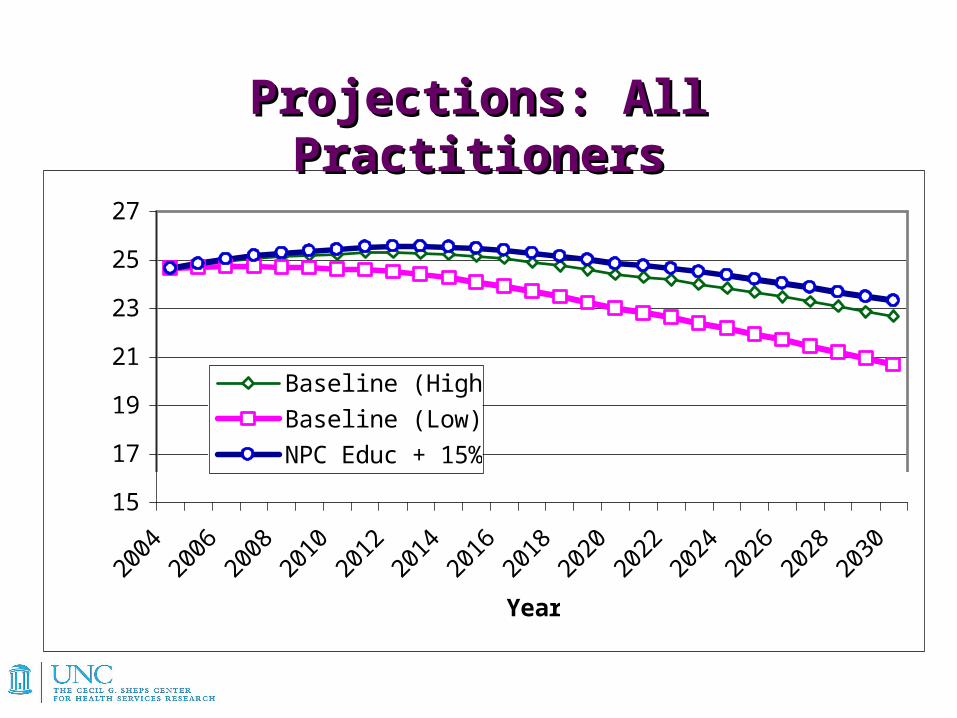
15
17
19
21
23
25
27
2004
2006
2008
2010
2012
2014
2016
2018
2020
2022
2024
2026
2028
2030
Year
Pro
vid
ers
Pe
r 1
0,0
00
Po
pu
lati
on
Baseline (High)
Baseline (Low)
NPC Educ + 15%
Projections: All PractitionersProjections: All Practitioners

Birth States of NC Physicians, 2003Birth States of NC Physicians, 2003n=17,315*n=17,315*
SC522
GA434
OH691
IL450
VA614
NY1498
NJ485
PA872
Source: AMA Masterfile, December 31, 2003. Note: Birthplace was unknown for 476 physicians. Percentages are based on 16,839 physicians for whom birthplace data were available. 2,668 physicians practicing in NC were born outside of the U.S. (16% of total).
NC301618%
NC301618%

Where NC Physicians went to Where NC Physicians went to Medical School, 2003 Medical School, 2003
n = 17,315n = 17,315
Source: AMA Masterfile, December 31, 2003. Note: 2,303 physicians practicing in NC went to medical schools outside the U.S. (13% of total).
SC524
GA520
OH652
IL430
VA807
NY900
PA817
TX435
NC477128%
NC477128%
TN463
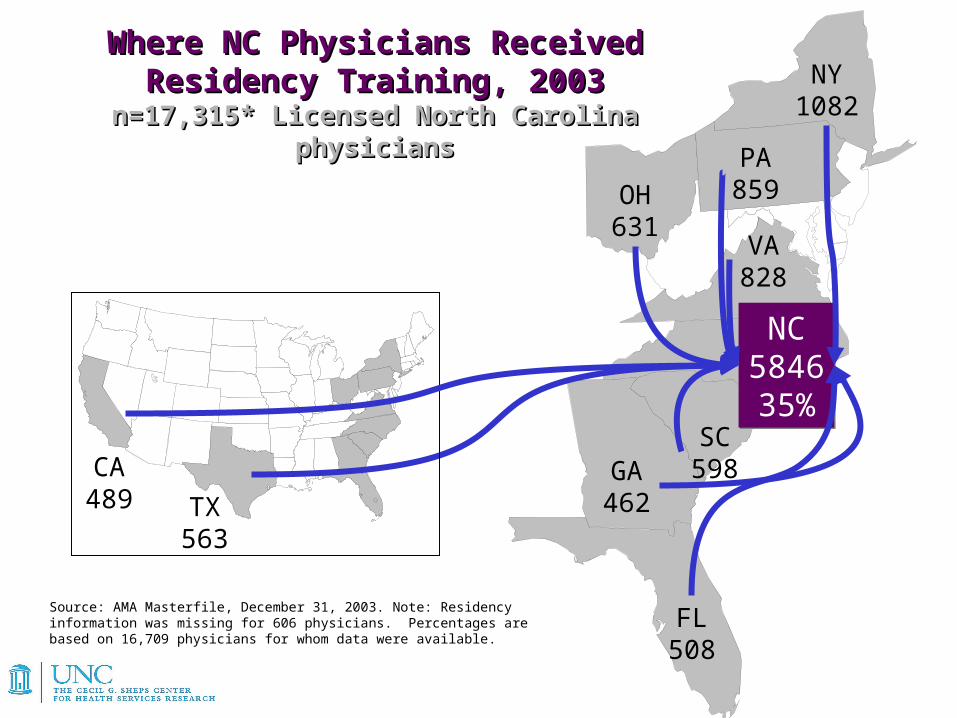
Where NC Physicians Received Residency Where NC Physicians Received Residency Training, 2003Training, 2003
n=17,315* Licensed North Carolina physiciansn=17,315* Licensed North Carolina physicians
NC584635%
NC584635%
SC598GA
462
OH631
VA828
NY1082
PA859
FL508
TX563
CA489
Source: AMA Masterfile, December 31, 2003. Note: Residency information was missing for 606 physicians. Percentages are based on 16,709 physicians for whom data were available.

39% of NC Medical 39% of NC Medical Students and 49% of NC Students and 49% of NC Post-graduate Trainees Post-graduate Trainees Remain in the State Remain in the State
NC39% / 49%retention
NC39% / 49%retention
SCGA
FL
TX
CA
TN
VA
NY
Source: AMA Masterfile, December 31, 2003.
Top Related