







Languages
Pages
Legal

Acute Renal FailureFall Medical/ Surgical Conference
Lubbock-Crosby-GarzaCounty Medical Society
Sandra Sabatini PhD, MD
Neil A Kurtzman MD
• Acute Kidney Injury now the preferred term• It's imprecise • Some forms of ARF are not associated with
tissue injury• We'll stick with ARF
An elevated serum creatinine during hospitalisation is an independent risk factor for mortality, progression to CKD, end-stage renal disease, and reduced long-term survival. Patients with chronically elevated serum creatinine (i.e., impaired baseline renal function) have a higher risk for acute kidney injury during hospital stays and are more often dialysis-dependent at hospital discharge than those without.
http://bestpractice.bmj.com/best-practice/monograph/935.html

ARF is an acute decline in the glomerular filtration rate (GFR) from baseline, with or without oliguria/anuria. It may be due to various insults such as impaired renal perfusion, exposure to nephrotoxins, outflow obstruction, or intrinsic renal disease.
Three General Mechanisms
• Pre-renal
• Renal
• Post-Renal

ARF vs CRFadaptation
• BP• Edema - fluid overload• Acid-Base• RBC• Ca• PO4• K

Pre-Renal
• Decreased renal perfusion• Contracted EABV• CHF• Blood loss• Vomiting• Diarrhea• Sweating• Decreased fluid intake• Cirrhosis• Pre-glomerular vascular disease
Evaluation
• History• PE
- Pulse and BP- Edema- Signs of other diseases
• Urine NaCl• BUN/Cr• Uric Acid
Treatment and Implications
• Depends on cause• Fluid loss different from CHF different from
Cirrhosis• Vol contraction predisposes to ATN - more soon

Post Renal
• Prostatism• Advanced Cervical Cancer• Retroperitoneal Fibrosis• Retroperitoneal Lymphoma• Bilateral Renal Calculi
Features
• Anuria if complete
• Collecting duct dysfunction

• Polyuria - NDI
• Metabolic acidosis
• Hyperkalemia
• NaCl loss
Treatment
• Relieve obstruction if possible• Dialysis and supportive care if obstruction is
irreversible

Renal
• Acute glomerulonephritis• Acute vasculitides • Acute interstitial nephritis• Toxins• Acute tubular necrosis (ATN)• Acute papilary necrosis

Toxins -Ethylene Glycol

Ethylene Glycol - Anti-Freeze
Dog kidney - polarized light

Manifestations
• CNS
• Metabolic Acidosis
• Renal failure

Diagnosis
• History
• CNS - "drunk", seizures
• Anion gap metabolic acidosis
• Oxaluria
• Acute renal failure
Treatment
• Ethanol
• Fomepizole (inhibits alcohol dehydrogenase)
• Hemodialysis
• Prognosis - good early treatment
• Prognosis - bad late treatment
Acute Interstitial Nephritis
• Can be infectious
• Usually non-infectious inflammatory
• Commonly drug induced
• Allergic reaction to a drug (acute interstitial allergic nephritis)
• Autoimmune disorders such as anti-tubular basement membrane disease, Kawasaki’s disease, Sjogren syndrome, systemic lupus erythematosus, or Wegener’s granulomatosis
• Acetaminophen, aspirin, NSAIDS
• Penicillin, ampicillin, methicillin, sulfonamide
• Furosemide, thiazide diuretics, omeprazole, triamterene, and allopurinol
• Hypokalemia
• Hypercalcemia, hyperuricemia
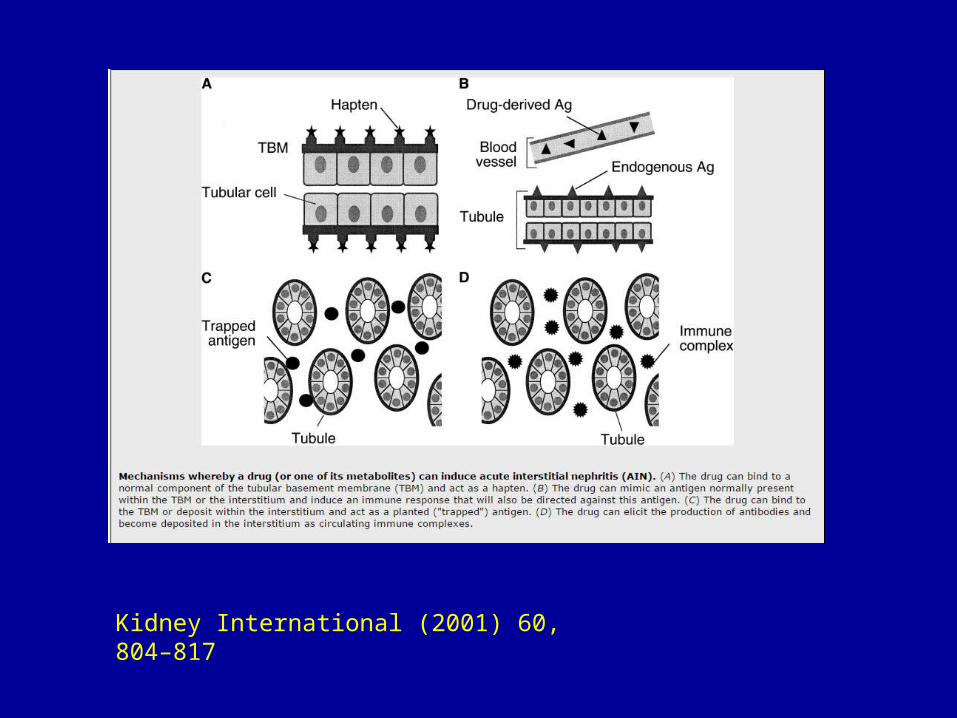
Kidney International (2001) 60, 804–817

Kidney International (2001) 60, 804–817

Kidney International (2001) 60, 804–817

Treatment
• Stop offending drug
• Treat underlying disease
• Steroids may hasten recovery
Acute Papillary Necrosis
• Chronic more common
• Diabetes
• Infection
• Often a catastrophic illness

ATN• Requires an underperfused kidney
• Nephrotoxins (Hg, Pt)
• Major surgery (due to multiple factors)
• Third-degree burns covering > 15% of BSA
• The heme pigments myoglobin and hemoglobin
• Tumor lysis or multiple myeloma
• Herbal and folk remedies, such as ingestion of fish gallbladder in Southeast Asia (uncommon)

Am J Med Sci. 2007, 334(2):115-24.
Cisplatin nephrotoxicity: a review.
Yao X1, Panichpisal K, Kurtzman N, Nugent K.
• Common nephrotoxins include the following:
• Aminoglycosides• Amphotericin B• Cisplatin and other chemotherapy drugs• Radiocontrast agents • NSAIDs• Colistimethate• Calcineurin inhibitors (cyclosporine, tacrolimus)

ATN
• ATN is more likely to develop in patients with the following:
• Preexisting hypovolemia or poor renal perfusion
• Preexisting chronic kidney disease
• Diabetes mellitus
• Older age
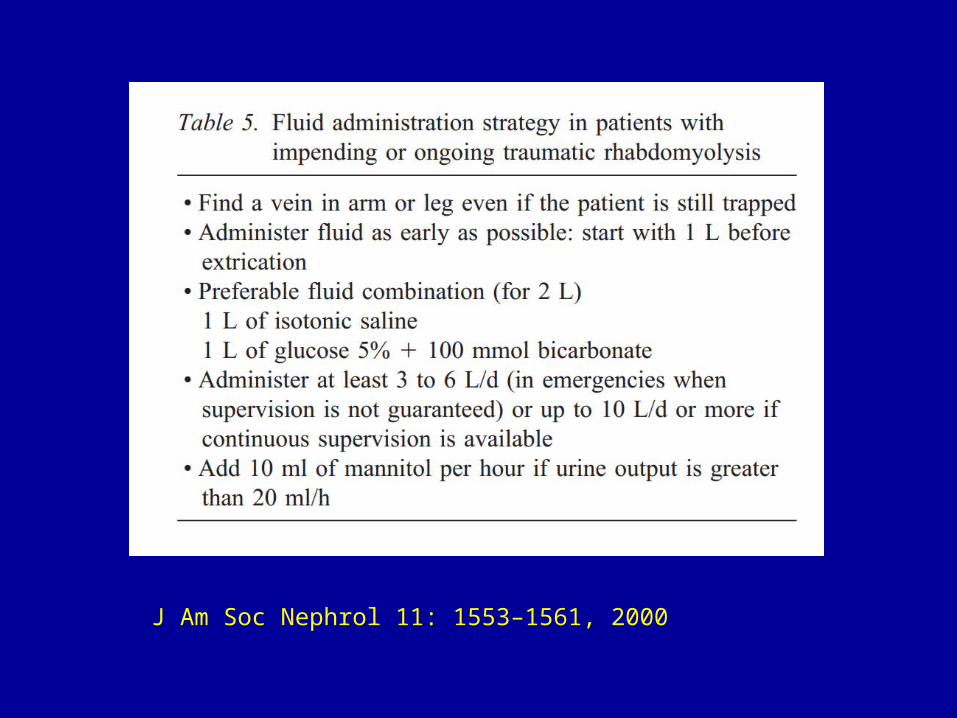
Crush Syndrome
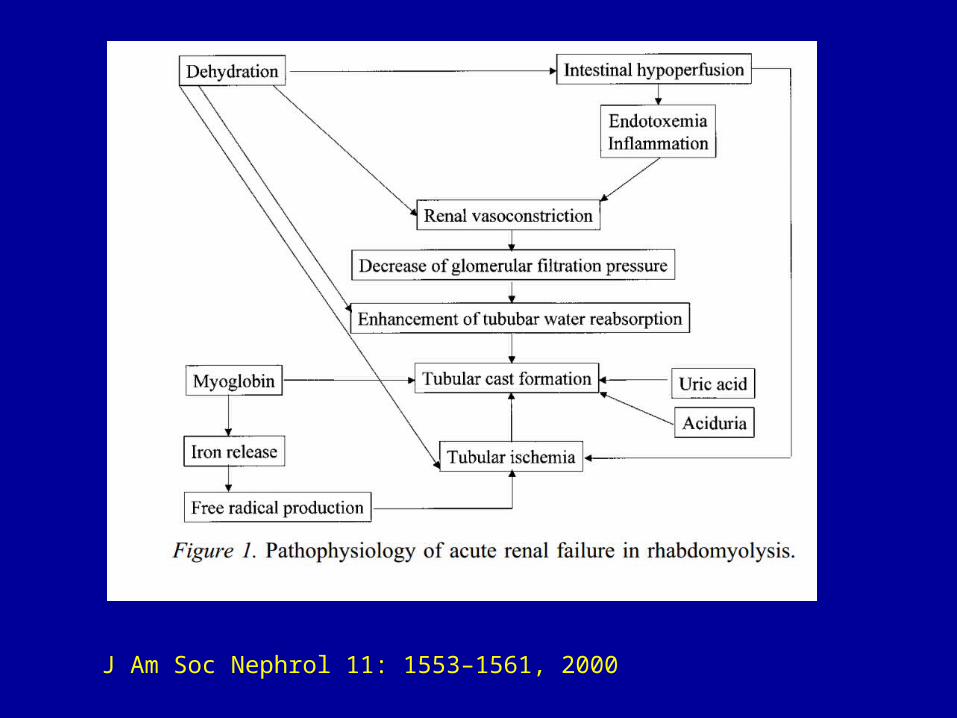
J Am Soc Nephrol 11: 1553–1561, 2000
J Am Soc Nephrol 11: 1553–1561, 2000
Contrast Induced ARF
• Systolic blood pressure <80 mm Hg • Intraarterial balloon pump • Congestive heart failure • Age >75 y • Hematocrit level <39% for men and <35% for
women
• Diabetes especially with ↑Cr• Contrast media volume • Renal insufficiency• Serum creatinine level >1.5 g/dL• Estimated Glomerular filtration rate < 60
ml/min• Gadolinium enhance MRI risks NSF and CRI

Prevention
• Avoid use in high risk patients• Isotonic saline• Saline and furosemide if CHF present
• HCO3 of uncertain utility
• N-acetylcysteine probably ineffective• Prophylactic hemodialysis not proven effective
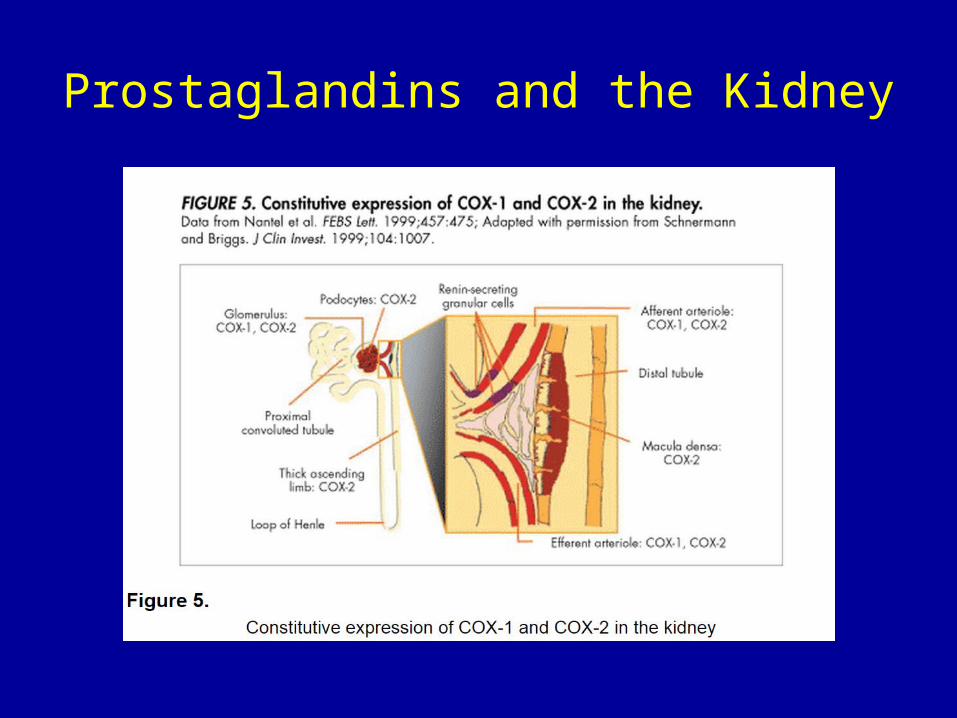
Prostaglandins and the Kidney
NSAIDS and Renal Disease
• AIN
• Pre renal azotemia
• ATN
• Nephrotic Syndrome
• Hyperkalemia
• Hyponatremia
NSAIDS and ARF
• Relatively uncommon• Incidence increases with age• ACE inhibitors and ARBs increase incidence• Volume contraction• Diuretics• Pre-existing renal disease

Prognosis
• 65% recover to baseline in 7-10 days• Dialysis needed <1% of patients• 18% who need HD remain on it
• Maioli M, Toso A, Leoncini M, Gallopin M, Musilli N, Bellandi F. Persistent renal damage after contrast-induced acute kidney injury: incidence, evolution, risk factors, and prognosis. Circulation. Jun 26 2012;125(25):3099-107

The Centre for Adverse Reactions Monitoring, NZ 2000
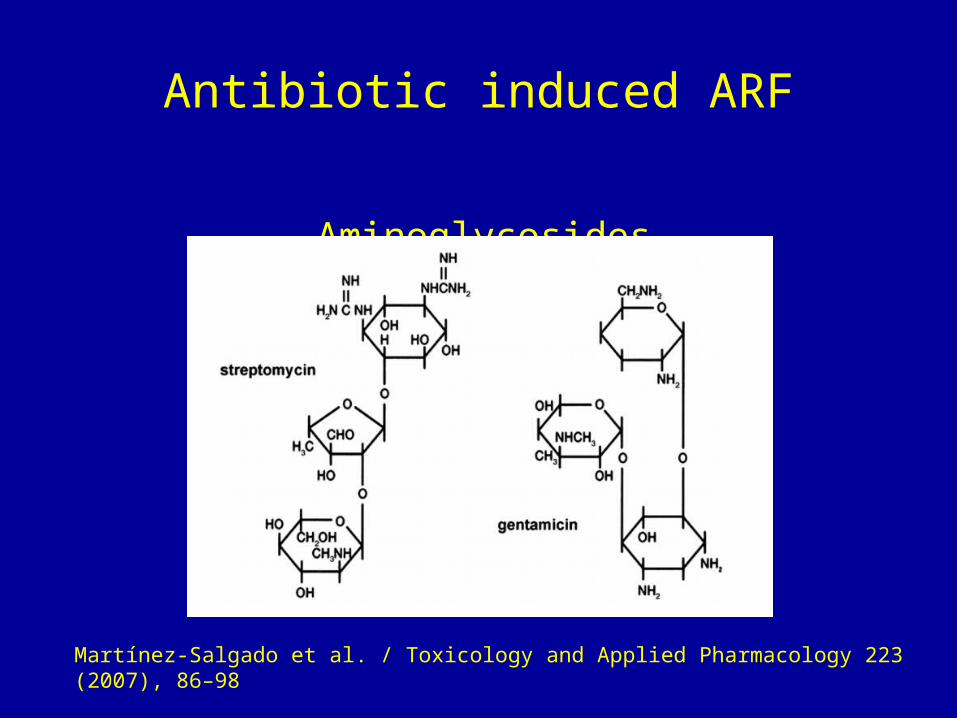
Antibiotic induced ARF
Aminoglycosides
Martínez-Salgado et al. / Toxicology and Applied Pharmacology 223 (2007), 86–98
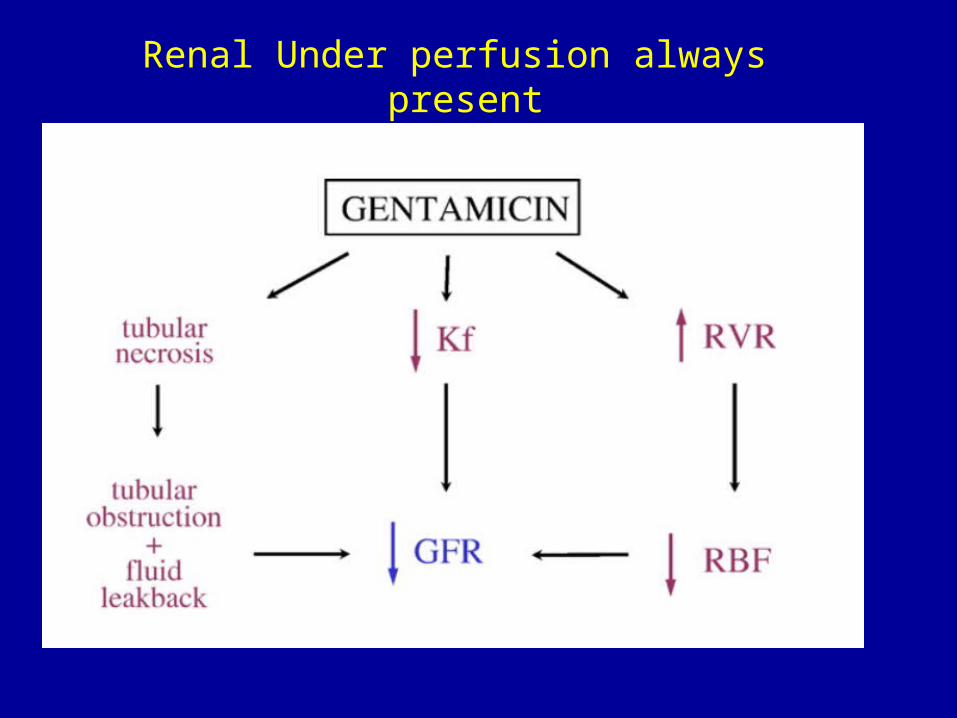
Renal Under perfusion always present
Amphotericin Nephrotoxicity
• Renal Underperfusion• Hypokalemia • Renal tubular acidosis• Liposomal formulation likely lower incidence• Acute renal failure
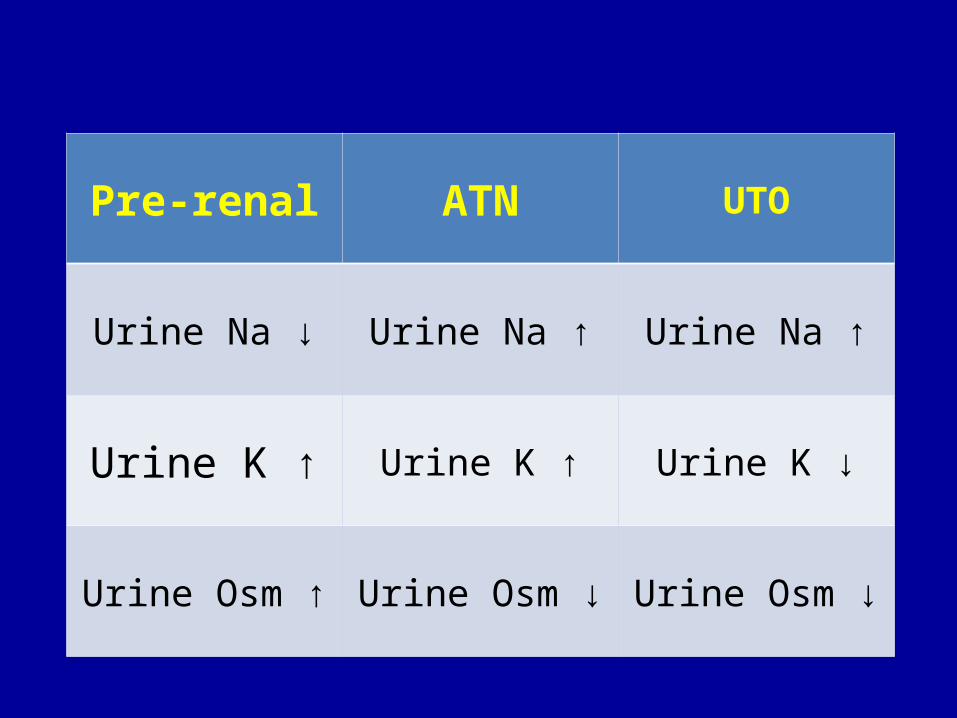
Pre-renal ATN UTO
Urine Na ↓ Urine Na ↑ Urine Na ↑
Urine K ↑ Urine K ↑ Urine K ↓
Urine Osm ↑ Urine Osm ↓ Urine Osm ↓
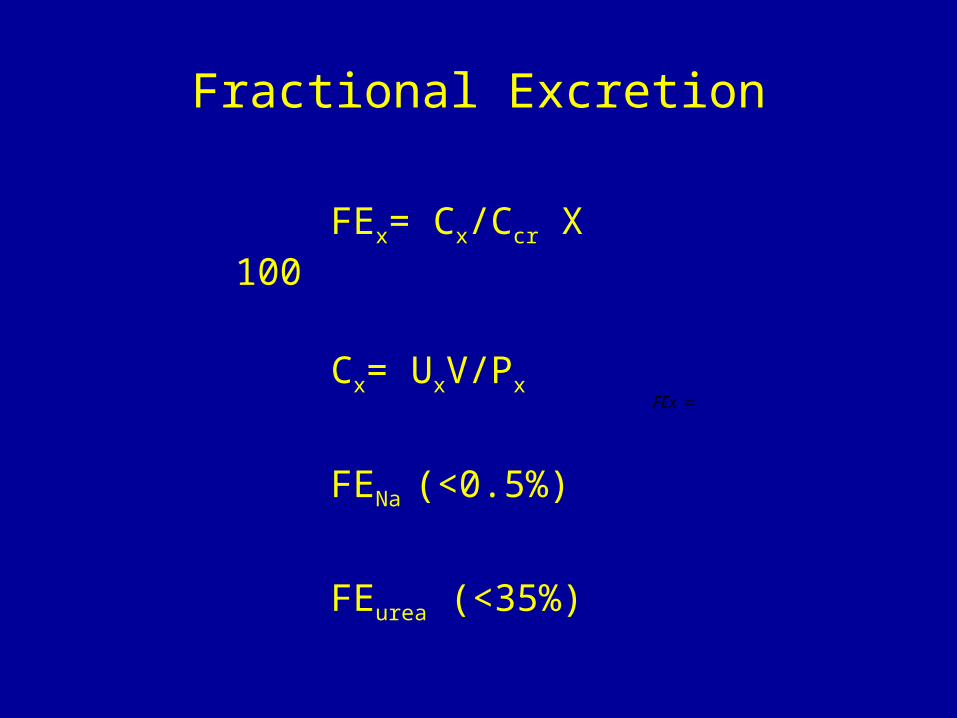
Fractional Excretion
FEx
FEx= Cx/Ccr X 100
Cx= UxV/Px
FENa (<0.5%)
FEurea (<35%)
Rx Oliguric ARF
• A fluid challenge is a substitute for thought• HD a soon as diagnosis is made• Daily until clinical status improves• Better avoided than treated

http://medicine-opera.com/2014/11/acute-renal-failure/
Top Related