








Languages
Pages
Legal


9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 1
Dilemmas in the Diagnosis & Management of Acid Base
Disorders
Paula Dennen, MD Assistant Professor of Medicine
Nephrology and Critical Care Medicine September 27, 2012
Background
Acid/Base
It’s all about…
pH
Acid Base
Balance

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 2
Acid Base Balance:
DEFINITION: Simply the maintenance of a normal hydrogen ion concentration
pH Acid Base
Balance
Acid Base Balance
What is a normal hydrogen ion concentration?
40 nMol (1/1,000,000,000 of a mole vs. mMol which is
1/1,000 of a mole)
0.00004 mEq/L (pretty small amount!)
Definitions: “emia” vs “osis”
“osis” is the process Metabolic alkalosis
Metabolic acidosis
Respiratory alkalosis
Respiratory acidosis
“emia” is the actual pH of the blood Acidemia Alkalemia

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 3
Acid Base Basics
Interpretation: need ABG (or VBG*) & Chem 7 ABG
Measured: pH, pCO2, pO2
Calculated: HCO3-, O2 sat
Chem 7 total CO2 includes dissolved CO2, H2CO3 and HCO3
- (mostly HCO3-)
About 2mmol/L difference between ABG & Chem 7
*VBG – pH ~ 0.03 lower, pCO2 ~ 6 higher “Pretty good” Underutilized for pH and pCO2
Acid Base Basics: “4” Step Approach Step 1 Calculate anion gap
IF anion gap, calculate ΔΔ (potential bicarb)
Step 2 Look at the pH (ABG or VBG) > 7.4 alkalemia < 7.4 acidemia
Step 3 Look at HCO3-
If pH & HCO3- same direction, 1° metabolic
If pH & HCO3- opposite direction, 1° respiratory
Acute or chronic
Step 4 Evaluate compensation
Compensation
HCO3- Controlled
by the kidneys CO2 Controlled by
the lungs
Normal HCO3- 24 mEq/L Normal pCO2
40 mmHg

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 4
Remember: Compensation is ALWAYS in the same direction as the primary
change!!
Compensation
Metabolic acidosis Expected pCO2 = 1.5 x HCO3
- + 8 ± 2
Metabolic alkalosis Expected pCO2 = (0.7 x HCO3
-) + 20 ± 2
Respiratory acidosis ↑ HCO3
-: ↑ pCO2, acute* 1:10, chronic** 3:10
Respiratory alkalosis ↓ HCO3
-: ↓ pCO2, acute* 2:10, chronic** 4:10
* Acute: before full renal compensation; **Chronic:after full renal compensation
Compensation:
Renal compensation 2-3 day delay…
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 5
Metabolic Acidosis
Anion Gap vs Non Anion Gap
Metabolic Acidosis
? Is it bicarbonate loss (NAGMA) or
? Is it gain of acid (AGMA) (bicarbonate
consumption)
H+ + HCO3- H2CO3 H2O + CO2
H+ + HCO3- H2CO3 H2O + CO2
Non Anion Gap Metabolic Acidosis (NAGMA)
Loss of Bicarbonate

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 6
Metabolic Acidosis: NAGMA
? Blame the kidney Or blame the gut…
The normal anion gap
=
Na – (HCO3- + Cl-) = 12*
Normally,
*Adjust downward by 2.5 for every 1 mg/dL decrease in albumin
Remember…we are electroneutral!
Daily Acid Load
Product of dietary protein & cellular metabolism
Acids produced: sulfuric & phosphoric acid, etc.
Estimated 1 mmol/kg/day (50-100mmol/day)
50-100 meq of H+ buffered daily
HCO3- lost during buffering, replaced in distal
nephron
If bicarbonate production impaired, NAGMA occurs
Anions of daily load are excreted ( IF normal kidney function) therefore AG is normal
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 7
“Blame the Kidney”: RTAs Key Points
Diagnosis: kidney function must be normal
Mechanism: disorders of impaired tubular function
Consequence: systemic metabolic acidosis due to an inability of the kidney to handle the daily acid load
UAG: unreliable when urine pH > 6.5 or when other measured
anions such as ketones or unmeasured anions (lithium) are present
Tracks unmeasured cations (like NH4+) vs. unmeasured
anions (serum anion gap)
Proximal RTA: Type II
Reduced Tm for HCO3-
Distal tubule function normal
Hypokalemia is common Lose K+ with HCO3
-
Treatment: lots and lots of bicarbonate
Acetazolamide (Diamox) essentially produces a proximal RTA
Wastes HCO3- and K+
Distal RTA: Type I
problem with urine acidification
Positive urine anion gap (UAG)
Urine pH ≥ 5.5
Defect in H+ secretion

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 8
Hyperkalemic RTA – Type 4
Problem of NH3 production Hyperkalemia Hypoaldosteronism contributes
Not a problem of acidifying the urine
Urine pH can be <5.5
Urine anion gap (UAG) is positive
Hyperkalemic RTA, secondary
Mineralocorticoid deficiency Addison disease, DM
Mineralocorticoid resistance Interstitial nephritis
Drug induced ACE-I, COX inhibitors, heparin K sparing diuretics, trimethoprim Beta-blockers
NAGMA in CKD Problem is NOT decreased tubular function
Problem is decreased functioning nephrons (tubules)
“over function” to compensate
As CKD progresses functioning nephrons increase amount of NH3 they make
Eventually (GFR ~ 30 to 40)
reduction in functioning nephrons exceeds ability of remaining nephrons to compensate
daily acid load (~ 1meq/kg/day) cannot be excreted
systemic acidosis occurs
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 9
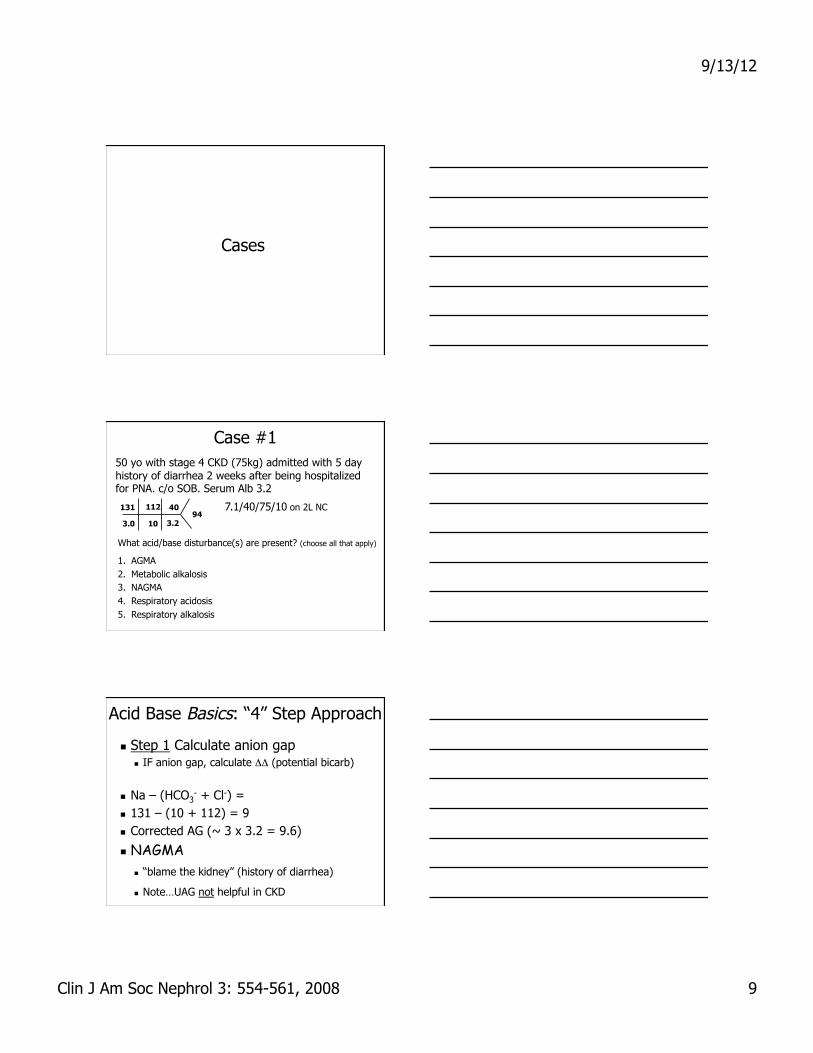
Cases
Case #1 50 yo with stage 4 CKD (75kg) admitted with 5 day history of diarrhea 2 weeks after being hospitalized for PNA. c/o SOB. Serum Alb 3.2
131 112
3.0 10
40
3.2 94
7.1/40/75/10 on 2L NC
What acid/base disturbance(s) are present? (choose all that apply)
1. AGMA 2. Metabolic alkalosis 3. NAGMA 4. Respiratory acidosis 5. Respiratory alkalosis
Acid Base Basics: “4” Step Approach
Step 1 Calculate anion gap IF anion gap, calculate ΔΔ (potential bicarb)
Na – (HCO3- + Cl-) =
131 – (10 + 112) = 9 Corrected AG (~ 3 x 3.2 = 9.6)
NAGMA “blame the kidney” (history of diarrhea)
Note…UAG not helpful in CKD

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 10
Acid Base Basics: “4” Step Approach
Step 2 Look at the pH (ABG or VBG) < 7.4 acidemia
Step 3 Look at HCO3-
If pH & HCO3- same direction, 1° metabolic
Step 4 Evaluate compensation Expected pCO2 = 1.5 x HCO3
- + 8 ± 2 Expected pCO2 = 1.5 x 10 + 8 ± 2 = 21-25 Respiratory Acidosis (pCO2 = 40 = inappropriate
respiratory compensation)
Case #1 continued… 50 yo with stage 4 CKD (75kg) admitted with 5 day history of diarrhea 2 weeks after being hospitalized for PNA. c/o SOB. Serum Alb 3.2
131 112
3.0 10
40
3.2 94
7.1/40/75/10 on 2L NC
What acid/base disturbance(s) are present? (choose all that apply)
1. AGMA 2. Metabolic alkalosis 3. NAGMA 4. Respiratory acidosis 5. Respiratory alkalosis
Case #1 Would you give bicarbonate? Why?
Symptomatic (SOB, can’t compensate) Ongoing loss Unable to “generate” bicarb with CKD
How would you give it? Calculate & replace deficit IV Continue 1meq/kg PO after repleted for CKD
What should you do before giving bicarbonate? Replace potassium Check ionized Ca++ & replace if low

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 11
Case #1: HCO3- deficit
How much HCO3- should be given to raise the
HCO3- to 15? To 20?
mEq HCO3- = weight x ∆ HCO3 x bicarb space
= 75 kg x 5 mmol/L x 0.5 = 187.5 mmol (goal 15) = 375 mmol (goal 20)
7.1 / 40 / 75 / 10 pH / pCO2 / pO2 / HCO3
Bicarb Replacement (for NAGMA)
1 amp of HCO3- is 50 mmol of Na+ & 50 mmol of HCO3
-
3 amps in a liter of D5W: Na+ of 150 mEq/1150 mL or 130 mEq/L Can leave out the D if hyperglycemic
2 amps in 1L 1/4NS: Na+ of 38 + 100 / 1100 mL or 125 mEq/L
NaHCO3- tablets – 7meq per 650mg tablet
Example – deficit ~ 200 meq (+ “losses”) = 28 tabs/day Useful for maintenance of 1meq/kg/day
Tough for replacement!
Case #2
Mr. V is a 75 yo male with a 2 day h/o N/V admitted with septic shock 2/2 aspiration pneumonia (on vasopressors), respiratory failure and oligoanuric AKI (albumin 3.3).
134
6
90
2.5
70
24
7.2/60/75/22 on 100% NRB
Lactate 6
140
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 12
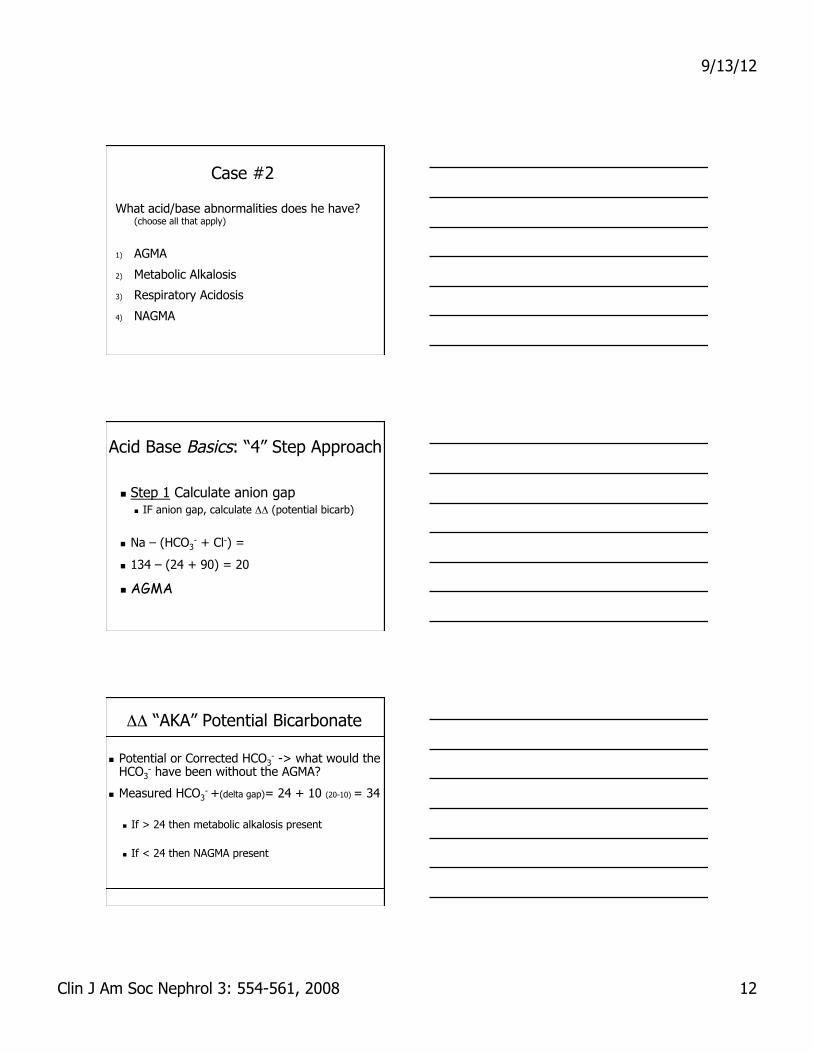
Case #2
What acid/base abnormalities does he have? (choose all that apply)
1) AGMA
2) Metabolic Alkalosis
3) Respiratory Acidosis
4) NAGMA
Acid Base Basics: “4” Step Approach
Step 1 Calculate anion gap IF anion gap, calculate ΔΔ (potential bicarb)
Na – (HCO3- + Cl-) =
134 – (24 + 90) = 20
AGMA
ΔΔ “AKA” Potential Bicarbonate
Potential or Corrected HCO3- -> what would the
HCO3- have been without the AGMA?
Measured HCO3- +(delta gap)= 24 + 10 (20-10) = 34
If > 24 then metabolic alkalosis present
If < 24 then NAGMA present
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 13
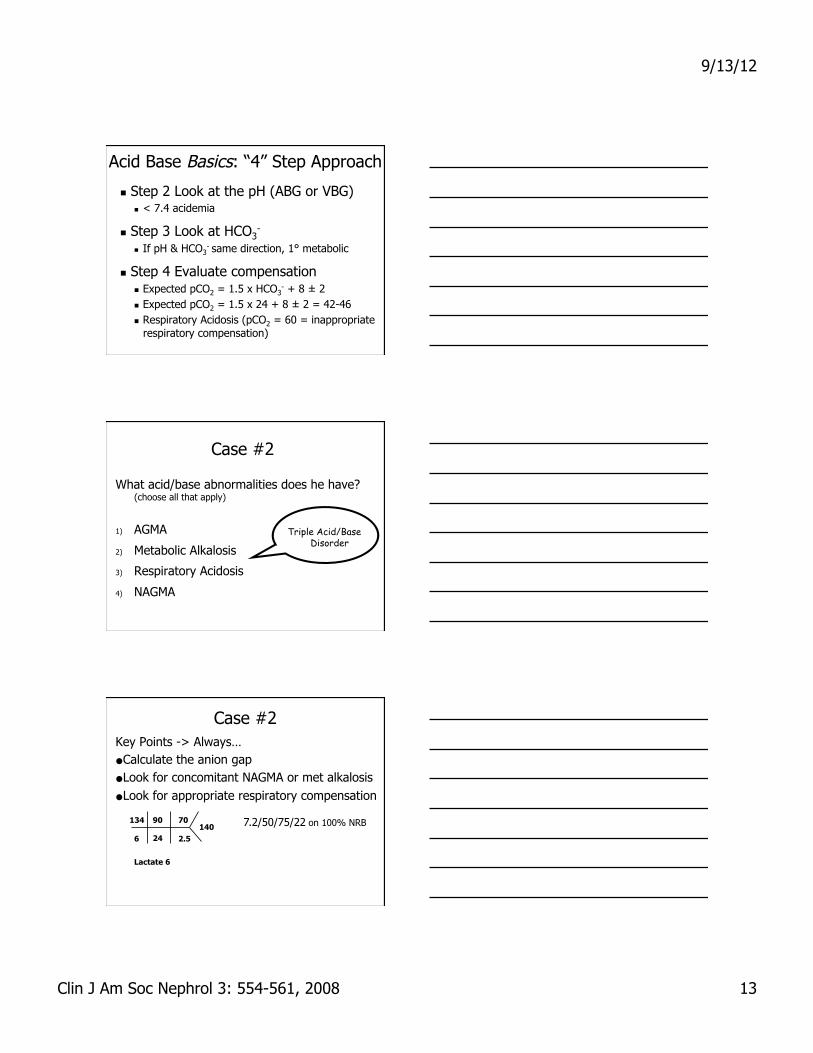
Acid Base Basics: “4” Step Approach
Step 2 Look at the pH (ABG or VBG) < 7.4 acidemia
Step 3 Look at HCO3-
If pH & HCO3- same direction, 1° metabolic
Step 4 Evaluate compensation Expected pCO2 = 1.5 x HCO3
- + 8 ± 2 Expected pCO2 = 1.5 x 24 + 8 ± 2 = 42-46 Respiratory Acidosis (pCO2 = 60 = inappropriate
respiratory compensation)
Case #2
What acid/base abnormalities does he have? (choose all that apply)
1) AGMA
2) Metabolic Alkalosis
3) Respiratory Acidosis
4) NAGMA
Triple Acid/Base Disorder
Case #2 Key Points -> Always… ● Calculate the anion gap ● Look for concomitant NAGMA or met alkalosis ● Look for appropriate respiratory compensation
134
6
90
2.5
70
24
7.2/50/75/22 on 100% NRB
Lactate 6
140

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 14
Anion Gap Metabolic Acidosis (AGMA)
Gain of Acid
What is the Acid?
AGMA: Gain of H+Anions- Metabolism
Starvation (ketones) DKA (ketones)
Ingestions Ethylene glycol (-> -> glycolic acid -> -> oxalic acid) Methanol (formaldehyde -> formic acid) Ethanol (ketones) (also lactic acid if “too much substrate”) Aspirin (Acetylsalicylic acid -> salicylic acid)
Hypoperfusion and Hypoxia (Lactic acid)
Renal failure (sulfate, urate, phosphate, hippurate…) MUDPILES or whatever works for you…
What about an AGMA is bad for you? AKA: Why do we care?
The anion?
The H+?
The disease?

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 15
“Bad” Anions: Methanol
Methanol (Sterno, shellac, varnish, de-icing)
HC3 – OH H – C – H
= O
Alcohol dehydrogenase
Methanol Formaldehyde Formic acid
H – C – OH
= O
Fomepizole or ethanol Hemodialysis Hemodialysis Rx:
“Bad” Anions: EG
Ethylene glycol (EG) (antifreeze, solvents)
H2C
Alcoho
l
dehy
drog
enas
e
Ethylene glycol
Glyco- aldehyde
Oxalic acid
Fomepizole or ethanol Hemodialysis Rx:
HO
HO
H2C
–
–
–
Glycolic acid
Glycoxalic acid
– H
= O
C
H2C
–
HO
–
– OH
= O
C
H2C
–
HO
–
H – = O
C
– OH
= O
C
–
HO – = O C
– OH
= O
C
–
Ethylene Glycol
Not itself toxic Converted to toxic metabolites Dependent on alcohol dehydrogenase Suspect in a patient with AGMA & osmolar gap
MW is 62, small amount can increase osmolar gap
Symptoms: AMS, tachypnea, pulm edema… Renal failure is a LATE finding
Toxic effects of glycolic acid on tubules Oxalic acid crystalizes in tubules

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 16
Serum Osmolality Osmolality = Osmoles/kg of water
What makes of serum osmolality?
2 (Na+) + Glucose/18 + BUN/2.8
Normal serum osmolality is 285-295 Kidney runs a pretty tight ship!
Osmolar Gap = Osmmeasured – Osmcalculated
Normal ~ 10
+ Ethanol/4.6
To convert mg/dL to mmol/L:
Divide by the molecular weight and multiply by 10
Osmolar Gap…
MW Example concentration
Contribution to osmolality
Methanol 32 80 mg/dL 25 mMol
Ethylene glycol
62 80 mg/dL 13 mMol
Salicylic acid
180 50 mg/dL 3 mMol
Ethanol 46 100 mg/dL 22 mMol
Osmolar Gap… Classic workup
Ethanol Ethylene glycol Methanol Isopropyl alcohol
What else increases it DKA or alcoholic ketoacidosis Lactic acidosis Chronic renal failure Mannitol infusion Hypertriglyceridemia
If no other explanation, or greater than 25 it is suggestive of methanol or ethylene glycol poisoning

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 17
Bad Anions: Salicylates Aspirin: acetylsalicylic acid
Active form: salicylic acid 90% protein bound 10% therapeutically active
At toxic doses: Limited protein binding Liver detoxification overwhelmed
Respiratory alkalosis (brain stimulation) Often the 1st sign
AG metabolic acidosis 50 mg/dL of salicylic acid (MW 180) is 3 mEq/L
Bad Anions: Salicylcates
Salicylate anion: S- (impermeable to cell membranes)
Salicylic acid: HS (freely crosses cell membranes)
H+ + S- HS
Ion trapping: Alkalinizing the serum and the urine increases the formation of S- which allows elimination of the drug
CAUTION: risk of bicarbonate is severe alkalemia (mixed respiratory and metabolic) (Resp alkalosis: 1st acid/base disturbance seen in salicylate toxicity)
Non-toxic Anions: Ketones
Ketones:
Alternate fuel when glucose is scarce Starvation, DKA, alcohol
Produced in the liver from triglycerides
Beta-hydroxybuterate, acetoacetate, acetone
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 18
Lactate
1400 mmol produced daily
Production of lactic acid from pyruvate via lactate dehydrogenase yields NAD+ for glycolysis
Buffered by bicarbonate to form lactate
Liver oxidizes lactate to form bicarbonate
Kidney responsible for 10 to 20% of lactate removal
Generation increases when glucose or glycogen are required to generate ATP in the absence of oxygen
Lactate Clearance Conversion to Bicarbonate
Clearance Elevated Lactate due to
Decreased metabolism
Decreased Clearance
Increased production
Combination of above
Lactic Acidosis
Absence of mitochondrial function from
Tissue hypoxia (Type A)
Impaired mitochondrial oxygen utilization (Type B) (cyanide, metformin, thiamine deficiency)
Mortality is 60 to 90%
Sepsis is most common cause

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 19
Lactic Acidosis: Causes Type B
Propylene glycol
Nitroprusside
Metformin
Malignancies
Lymphoma, leukemia
Liver failure
Ingestions…
Type A
Sepsis
Ischemia
Hypoperfusion
Seizures
Exercise
Reminder…Case #2 cont’d
Mr. V is a 75 yo male with a 2 day h/o N/V admitted with septic shock 2/2 aspiration pneumonia (on vasopressors), respiratory failure and oligoanuric AKI (albumin 3.3).
134
6
90
2.5
70
24
7.2/60/75/22 on 100% NRB
Lactate 6
140
Case #2
After 6L volume resuscitation with IVNS his ABG is 7.1/50/100/12 with AGMA 20. Mr. V becomes more obtunded, requires intubation and is initiated on CRRT. The next morning he has an increase in his vasopressor requirement.
What do you expect his pH to be on his AM ABG?
Why does he have an increased pressor requirement?

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 20
Case #2 What is his most likely pH on his AM ABG?
1. 7.15 2. 7.32 3. 7.40 4. 7.58 5. 7.7
CAUTION: Don’t forget to adjust the vent (minute ventilation) as the metabolic acidosis is being corrected!
(cuz CRRT is just that good)
Mixed respiratory and metabolic alkalosis
Case #2 Why an increased pressor requirement?
1. Worsening sepsis 2. Volume Depletion 3. Hypocalcemia 4. Tension pneumothorax 5. Bleeding
CAUTION: free or ionized calcium drops with alkalemia which can lead to clinically significant hypotension
Bicarbonate and Calcium
Data from ICU patients with lactic acidosis
Given 2 mEq/kg of NaHCO3 or saline
pH from 7.22 to 7.36 Ionized calcium fell
8.5% (from .95 to 0.87) pH correction vs.
hypocalcemia effect on cardiac contractility
Cooper, DJ et al, Annals 1990;112:492-8.

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 21
Calcium
HCO3- binds Ca++ decreasing ionized or
“available” calcium
IF Ca++ is low and patient is acidemic, IMPORTANT to correct Ca++ as reversal of acidemia will decrease free Ca++
Similar to K+, IF patient is hypokalemic and acidemic, IMPORTANT to correct hypokalemia before acidemia
Case #3 50 yo with decompensated heart failure on NIPPV for acute hypoxemic respiratory failure 2/2 volume overload and increased work of breathing. Aggressively diuresed on lasix gtt for management of pulmonary edema. After 24 hours on a lasix gtt his urine output drops to 10cc/hr.
What additional information would be helpful?
1) Hemodynamics 2) Serum sodium 3) Serum creatinine 4) Pulmonary pressures 5) All of the above
Case #3
What is the risk of metabolic alkalosis in this patient:
1) Respiratory depression
2) Hypoxia due to hypoventilation
3) Increased affinity of hemoglobin for O2
4) Hypocalcemia
5) All of the above
134
30 2.5
89 39 134
1.3 7.5/48/75/29 on 70% 12/5

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 22
Case #3 Based on the previous labs what should be your
next order (s) ? Choose all that apply:
1) Diamox 500mg IV x 1
2) Intubation
3) KCl at 20meq/hr x 6
4) Check an ionized calcium
5) Give IVF
Acetazolamide (Diamox)
Confirm alkalemic pH Contraindicated for primary respiratory acidosis
Increases bicarbonate loss in proximal tubule
CAUTION with hypokalemia Must replace BEFORE diamox
CAUTION with hypocalcemia Must replace BEFORE diamox
Important to assess volume status IVF treatment for hypovolemic (chloride
responsive metabolic alkalosis)
Case #4 54 yo female with h/o DM on metformin, schizoaffective D/O, COPD admitted with AMS, lethargy and decreased PO intake per family report. 1st chem 7:
Albumin 2
What acid/base disturbances are present? (choose all that apply)
1) AGMA 2) Metabolic alkalosis 3) NAGMA 4) Respiratory acidosis 5) Respiratory alkalosis
129 86
4.5 27
65
10.5 85

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 23
Acid Base Basics: “4” Step Approach Step 1 Calculate anion gap
IF anion gap, calculate ΔΔ (potential bicarb)
Na – (HCO3- + Cl-) =
129 – (27 + 86) = 16
AGMA Potential Bicarb
HCO3- + (delta gap) = 27 + 10 = 37
If > 24 then metabolic alkalosis present
Case #4 54 yo female with h/o DM on metformin, schizoaffective D/O, COPD admitted with AMS, lethargy and decreased PO intake per family report. 1st chem 7:
What acid/base disturbances are present? (choose all that apply)
1) AGMA 2) Metabolic alkalosis 3) NAGMA 4) Respiratory acidosis 5) Respiratory alkalosis
129 86
4.5 27
65
10.5 85
Need an ABG or VBG!
Case #4
What is the most likely cause of her acid/base disturbances?
What additional information do you want? Lactate 1 Albumin 2 Toxic Alcohol Screen Negative Salicylate negative Other?
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 24
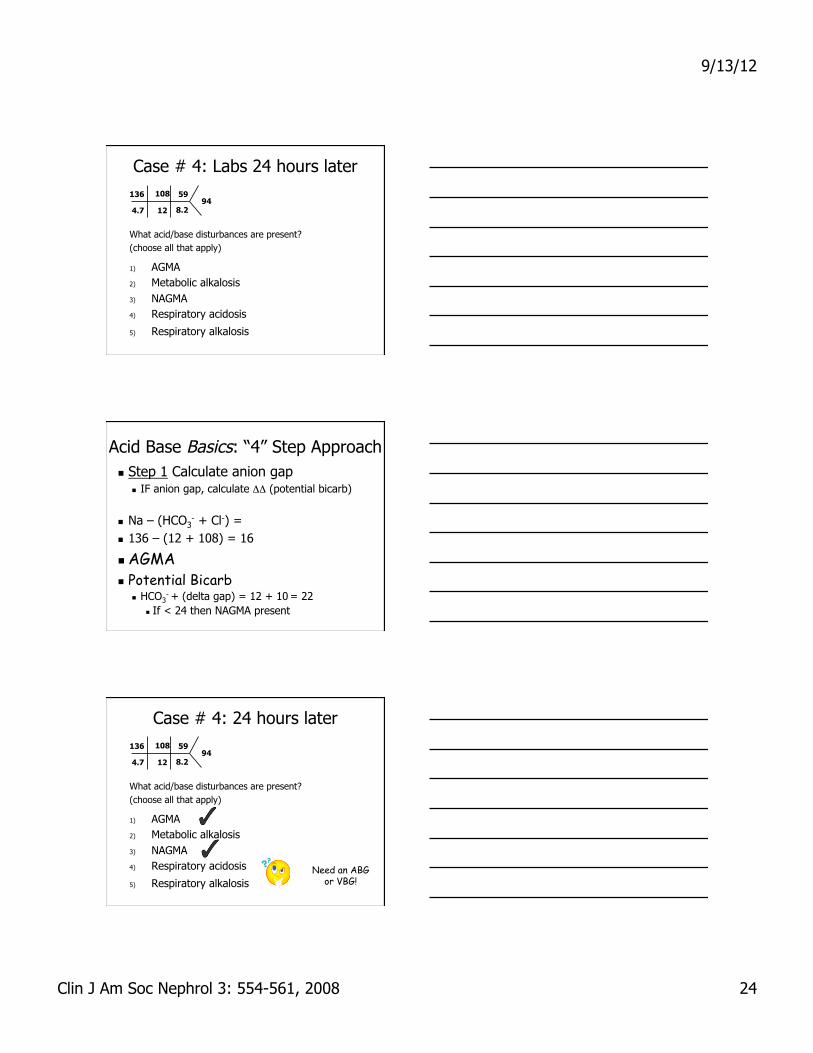
Case # 4: Labs 24 hours later
What acid/base disturbances are present? (choose all that apply)
1) AGMA 2) Metabolic alkalosis 3) NAGMA 4) Respiratory acidosis
5) Respiratory alkalosis
136 108
4.7 12
59
8.2 94
Acid Base Basics: “4” Step Approach Step 1 Calculate anion gap
IF anion gap, calculate ΔΔ (potential bicarb)
Na – (HCO3- + Cl-) =
136 – (12 + 108) = 16
AGMA Potential Bicarb
HCO3- + (delta gap) = 12 + 10 = 22
If < 24 then NAGMA present
Case # 4: 24 hours later
What acid/base disturbances are present? (choose all that apply)
1) AGMA 2) Metabolic alkalosis 3) NAGMA 4) Respiratory acidosis
5) Respiratory alkalosis
136 108
4.7 12
59
8.2 94
Need an ABG or VBG!

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 25
Case #4
What is the most likely cause of her acid/base disturbances?
What additional information do you want?
Serum KETONES Large!!!
“Normoglycemic” DKA
Don’t need hyperglycemia to be in DKA
Be complete in your workup of AGMA
Don’t let a high bicarbonate mask your AGMA ALWAYS calculate the anion gap
Don’t be fooled by “normoglycemic” DKA!
Metformin: MALA Metformin Associated Lactic Acidosis
Risk Factors AKI/CKD/elderly
Symptoms Lethargy, N/V/abd pain
Signs VERY high lactate (Note…lactate was only 1)
Can be confused with mesenteric ischemia No hypoglycemia in therapeutic doses but
hypoglycemia seen in toxic doses
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 26
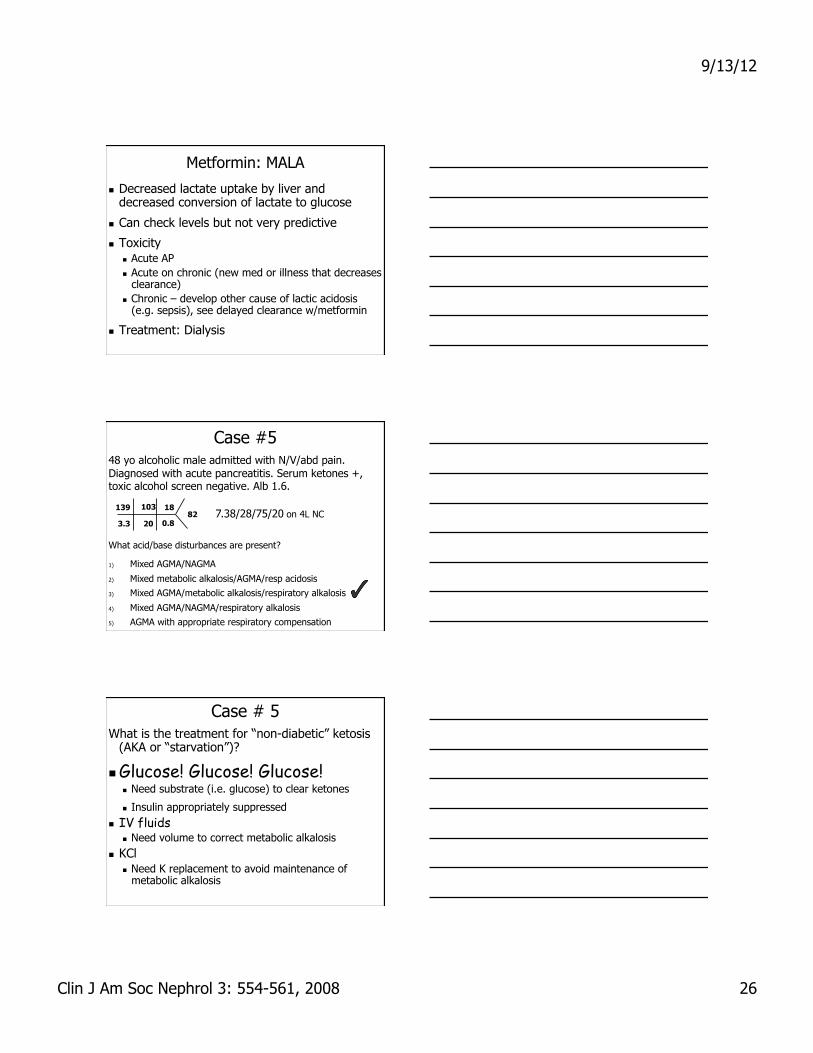
Metformin: MALA
Decreased lactate uptake by liver and decreased conversion of lactate to glucose
Can check levels but not very predictive
Toxicity Acute AP Acute on chronic (new med or illness that decreases
clearance) Chronic – develop other cause of lactic acidosis
(e.g. sepsis), see delayed clearance w/metformin
Treatment: Dialysis
Case #5 48 yo alcoholic male admitted with N/V/abd pain. Diagnosed with acute pancreatitis. Serum ketones +, toxic alcohol screen negative. Alb 1.6.
139 103
3.3 20
18
0.8 82 7.38/28/75/20 on 4L NC
What acid/base disturbances are present?
1) Mixed AGMA/NAGMA
2) Mixed metabolic alkalosis/AGMA/resp acidosis
3) Mixed AGMA/metabolic alkalosis/respiratory alkalosis
4) Mixed AGMA/NAGMA/respiratory alkalosis
5) AGMA with appropriate respiratory compensation
Case # 5 What is the treatment for “non-diabetic” ketosis
(AKA or “starvation”)?
Glucose! Glucose! Glucose! Need substrate (i.e. glucose) to clear ketones
Insulin appropriately suppressed IV fluids
Need volume to correct metabolic alkalosis KCl
Need K replacement to avoid maintenance of metabolic alkalosis

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 27
Case # 6 32 yo found down at home by roomate. Obtunded
and tachypneic but protecting airway. Foley placed with good UOP. BAL 300, tox screen negative, lactate 20. AG 16. Difficult physical exam due to obtundation. Hemodynamically stable. No other history available?
What other lab value (s) or imaging studies do you want right away?
Case #6
Which of the following causes of AGMA does NOT cause a severely elevated lactate
1. Metformin
2. Ethylene glycol
3. Methanol
4. Mesenteric Ischemia
Ethylene Glycol (EG)
Typically does NOT cause severe lactic acidosis
Acidosis due to breakdown product Major toxin is glycoaldehyde Dependent on alcohol dehydrogenase
Blocked by ethanol or fomepizole
Can be masked if elevated BAL
Don’t forget to use your serum osm
IMPORTANT: False + lactate 2/2 interference of metabolite of EG in analyzer

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 28
Bicarbonate in AGMA?
Consequences of Acidemia…
Cardiovascular Decreased cardiac contractility Arterial dilatation/venoconstriction Increased pulmonary vascular resistance Predisposition to arrhythmias Decreased response to catecholamines
Exogenous or endogenous
Respiratory Hyperventilation
Consequences of Acidemia…
Metabolic Insulin resistance Inhibition of glycolysis Reduced ATP synthesis Hyperkalemia (shfit)
Cerebral Altered mental status Coma

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 29
Acidemia Does arterial pH reflect tissue pH?
If blood flow to a tissue decreases 50% Tissue PCO2 will double Local intracellular pH will decrease (acidosis) Arterial pH and PCO2 do not change
What about mitochondrial pH? In isolated hepatocytes Mitochondrial pH gradient did not change when
extracellular pH was lowered from 7.4 to 6.9
Chest 2000; 117:260-267
Respiratory Acidosis
Elevated pCO2 dilates cerebral vessels
“Permissive” hypercapnia (e.g. in ARDS) is potentially dangerous and contra-indicated in patients with TBI or CVA Don’t need hyperventilation but should
avoid hypoventilation
Should I give Bicarbonate?

9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 30
Bicarbonate in DKA?
Can be detrimental in DKA
Ketones reduce pH, and decreased pH blocks ketogenesis, negative feedback
Increasing pH turns off the negative feedback, stimulating ketogenesis
Consensus statement from ADA 2006 recommends bicarb for pH < 6.9 (no prospective study)
Bicarbonate in Lactic Acidosis Why Not?
Causes CSF acidosis
Intracellular acidosis
Impairs oxygen delivery to tissues
Increases carbon dioxide and worsens acidosis
Increases lactic acid production
Worsens hypocalemia
Bicarbonate in Lactic Acidosis Controversial…
pH < 7.2 ?
pH < 7.15
pH < 7.1
pH < 7
Who knows?
9/13/12
Clin J Am Soc Nephrol 3: 554-561, 2008 31
Summary of Bicarbonate in Metabolic Acidosis
Reasonable/recommended to give in disorders where HCO3
- is lost RTA, diarrhea with severe acidosis
Acidemia well tolerated in permissive hypercapnea, DKA
Lactic acidosis No improvement in hemodynamics Potentially detrimental – although clinical
significance unknown
What to worry about with bicarbonate administration…
Alkalemia – know the pH 1st
Hypokalemia – replete K+ 1st
Hypocalcemia – replete Ca++ 1st
Take Home Pearls Acidemia likely better tolerated than we think
Caution with bicarbonate (watch electrolytes)
Sometimes treatment worse than condition
Appreciate integration between metabolic and respiratory physiology (e.g. vent & CRRT)
Don’t forget the osmolar gap
Think twice (or 3x) about bicarbonate in AGMA
Analyze acid/base status in all patients (can uncover other diagnoses)
Integrate clinical and laboratory data
Top Related