




Languages
Pages
Legal


J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 6 . 0 2 . 0 4 6
STATEMENT FROM THE INTERVENTIONAL COUNCIL OF THE ACC
A Practical Approach to MechanicalCirculatory Support in Patients UndergoingPercutaneous Coronary InterventionAn Interventional Perspective
Tamara M. Atkinson, MD,a E. Magnus Ohman, MD,b William W. O’Neill, MD,c Tanveer Rab, MD,d
Joaquin E. Cigarroa, MD,a on behalf of the Interventional Scientific Council of the American College of Cardiology
ABSTRACT
Fro
Ins
Mi
refl
con
Gil
rec
Dr
tha
Ma
Percutaneous mechanical circulatory support has been used to stabilize patients in cardiogenic shock and provide
hemodynamic support during high-risk percutaneous coronary interventions for several decades. The goal of this paper is to
provide a practical approach to percutaneousmechanical circulatory support in patients undergoing percutaneous coronary
intervention with cardiogenic shock and/or high risk features to aid in decision making for interventional cardiologists.
(J Am Coll Cardiol Intv 2016;9:871–83) © 2016 by the American College of Cardiology Foundation.
P ercutaneous mechanical circulatory support(MCS) has evolved dramatically since thefirst intra-aortic balloon pump (IABP) was
used in humans in the 1960s (1,2). Although IABPhas been the mainstay of MCS devices, recentstudies have demonstrated lack of efficacy (3–5).In the setting of cardiogenic shock and high-riskpercutaneous coronary intervention (HR-PCI), theintroduction of newer devices coupled with datafrom clinical trials is challenging the role of theIABP (6–8). Mechanical circulatory support, such asImpella (Abiomed Inc., Danvers, Massachusetts),TandemHeart (CardiacAssist, Inc., Pittsburgh, Penn-sylvania), and extracorporeal membrane oxygena-tion (ECMO), all possess an ability to providegreater hemodynamic support and may improveclinical outcomes.
m the aKnight Cardiovascular Institute, Oregon Health and Science Un
titute, Duke University Medical Center, Durham, North Carolina; cDiv
chigan; and the dDivision of Cardiology, Emory University School of Me
ect the opinion of the American College of Cardiology or the JACC: Card
sultant for Abiomed, AstraZeneca, Biotie, Boehringer Ingelheim, Daiich
ead Sciences, Janseen Pharmaceuticals, Merck, Stealth Peptides, Medsca
eived research grant support from Daiichi-Sankyo, Eli Lilly & Compan
. O’Neill has served as a consultant for Medtronic, Edwards Lifesciences, a
t they have no relationships relevant to the contents of this paper to dis
nuscript received December 14, 2015; revised manuscript received Janua
MCS is used primarily in 3 populations includingHR-PCI, cardiogenic shock, and cardiac arrest. Asdefined by the 2015 Society for Cardiovascular Angi-ography and Interventions/American College ofCardiology/Heart Failure Society of America/Societyof Thoracic Surgeons Clinical Expert Consensus onthe use of percutaneous MCS in cardiovascular care,the purpose of MCS is to reduce left ventricular strokework and myocardial oxygen demand while main-taining systemic and coronary perfusion in the settingof cardiogenic shock or to provide hemodynamicsupport during complex cardiac procedures includingHR-PCI and certain high-risk ventricular tachycardiaelectrophysiology ablation procedures (9). Withmultiple treatment modalities available, the chal-lenge for the practicing interventional cardiologist isto understand which MCS offers the best use in each
iversity, Portland, Oregon; bDuke Clinical Research
ision of Cardiology, Henry Ford Hospital, Detroit,
dicine, Atlanta, Georgia. This manuscript does not
iovascular Interventions. Dr. Ohman has served as a
i-Sankyo, Eli Lilly & Company, Faculty Connection,
pe, The Medicines Company, and WebMD; and has
y, Gilead Sciences, and Janssen Pharmaceuticals.
nd St. Jude Medical. All other authors have reported
close.
ry 29, 2016, accepted February 1, 2016.

TABLE
Clinical
SBP <
Suppo
End
Coo
UOP
HR >
Hemody
Cardia
PCWP
The SHOCcriteria lis
HR ¼ hblood pre
ABBR EV I A T I ON S
AND ACRONYMS
3VD = 3-vessel disease
CPR = cardiopulmonary
resuscitation
ECMO = extracorporeal
membrane oxygenation
HR-PCI = high-risk
percutaneous coronary
intervention
IABP = intra-aortic balloon
pump
ICU = intensive care unit
MCS = mechanical circulatory
support
ROSC = return of spontaneous
circulation
VA = venoarterial
Atkinson et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
Algorithm for Mechanical Circulatory Support M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3
872
clinical scenario and to understand how pa-tient characteristics impact this choice. Thegoal of this paper is to define a practicalapproach for the interventional cardiologistregarding when to use MCS, how to selectMCS device type, and practical points toconsider when utilizing MCS devices.
POPULATIONS REQUIRING
PERCUTANEOUS MECHANICAL
CIRCULATORY SUPPORT
CARDIOGENIC SHOCK. Cardiogenic shockoccurs secondary to multiple etiologiesincluding left ventricular systolic dysfunc-tion, right ventricular systolic dysfunction,valvular heart disease, pericardial disease,and vasodilatory abnormalities. These con-
ditions, in our patient population, most often presentin patients with acute myocardial infarction, out-of-hospital cardiac arrest, and patients with a historyof congestive heart failure and/or advanced valvularheart disease. While cardiogenic shock is one of themore fatal complications of acute myocardial infarc-tion, it is relatively rare occurring in about 7% of allacute myocardial infarctions (10,11). Even withprompt reperfusion therapy with primary percuta-neous coronary intervention, mortality rates stillrange from 30% to 50% (3). The SHOCK (SHould weemergently revascularize Occluded Coronaries forcardiogenic shocK?) trial outlined clinical and hemo-dynamic criteria to define cardiogenic shock (Table 1).In clinical practice, patients with cardiogenic shockrepresent a spectrum of disease secondary todifferent etiologies, which can be classified as pre/early shock, shock, and severe shock (Table 2) (12–21).Therefore, a structured approach to determine thebest adjunctive MCS device in patients undergoingpercutaneous coronary intervention (PCI) is required.
1 Hemodynamic Criteria for Cardiogenic Shock
90 mm Hg for 30 min
rtive measures needed to maintain SBP >90 mm Hg
-organ hypoperfusion
l extremities
<30 ml/h
60 beats/min
namic
c index <2.2 ml/min/m2
>15 mm Hg
K trial defined cardiogenic shock according the clinical and hemodynamicted (11).
eart rate; PCWP ¼ pulmonary capillary wedge pressure; SBP ¼ systolicssure; UOP ¼ urine output.
HR-PCI. The evolution of PCI with advances incatheter design, creation of low profile balloons,guidewire design, stent deliverability, and develop-ment of effective antiproliferative medicationshave increased the number of patients eligible forpercutaneous revascularization. According to recentAmerican Heart Association statistics, although bothPCI and coronary artery bypass graft surgerynumbers have declined, PCI is the most commonrevascularization modality and is applied topatients with increased lesion complexity and com-orbidities with 51% of all PCI performed in patients>65 years of age (22). In addition, the advent oftranscatheter techniques for the treatment ofpatients with valvular heart disease has resultedin older patients with severe coronary disease andleft ventricular systolic dysfunction undergoingHR-PCI. Multiple variables define HR-PCI includingclinical presentation, coronary anatomy, hemody-namic status, electrical instability and end organfunction (Table 3) (23,24). PCI in patients withfactors such as impaired left ventricular systolicfunction defined as ejection fraction <35%, un-protected left main disease, severe 3-vessel disease(3VD) (SYNTAX score >33), or last remaining patentvessel are associated with in-hospital mortality ratesbetween 5% and 15% (24–30).
MCS has been used to provide stability during high-risk interventions for over 25 years. The goal of MCSduring HR-PCI is to provide sufficient forward cardiacoutput to maintain myocardial, cerebral, mesenteric,renal, and peripheral tissue perfusion. Nellis et al. (31)have demonstrated in an animal model that a40 mm Hg pressure gradient exists between coronaryarterioles and venules. Sustained hypotension withcoronary perfusion gradients <40 mm Hg can lead toprofound myocardial ischemia, which quickly de-presses an already impaired left ventricle and maylead to cardiovascular collapse and arrest. Cliniciansmust recognize this scenario and act prior to reachingthis threshold to avoid this lethal spiral. Measuring aleft ventricular end-diastolic pressure prior to PCI canhelp differentiate where the patient is on the spec-trum of cardiogenic shock and determine whetherMCS is needed prior to PCI. MCS should be institutedprior to PCI in an effort to avoid “crashing onto sup-port” and to enable the most complete revasculariza-tion feasible. In the PROTECT II (Prospective, Multi-center, Randomized Controlled Trial of the IMPELLARECOVER LP 2.5 System Versus Intra Aortic BalloonPump [IABP] in Patients Undergoing Non EmergentHigh Risk PCI) trial, hypotensive events occurred lessoften in the Impella group (11.8% vs. 17.2%; p < 0.001).Patients with the lowest major adverse events at

TABLE 2 Spectrum of Cardiogenic Shock
Pre/Early Shock
Clinical
SBP <100 mm Hg
HR 70–100 beats/min
Normal lactate
Normal mentation
Cool extremities
Hemodynamic
CI 2–2.2
PCWP <20
LVEDP <20
CPO >1 W
Vasoactive medications
0 or 1 low dose
Shock
Clinical
SBP <90 mm Hg
HR >100 beats/min
Lactate >2
AMS
Cool extremities
Hemodynamic
CI 1.5–2.0
PCWP >20
LVEDP >20
CPO <1 W
Vasoactive medications
1 moderate to high dose
Severe shock
Clinical
SBP <90 mm Hg
HR >120 beats/min
Lactate >4
Obtunded
Cool extremities
Hemodynamic
CI <1.5
PCWP >30
LVEDP >30
CPO <0.6 W
Vasoactive medications
2 or more
Cardiogenic shock can be classified as pre/early shock, shock, and severe shock, whichcan help determine the appropriate mechanical circulatory support (MCS) device.
AMS ¼ altered mental status; CI ¼ cardiac index; CPO ¼ cardiac power;LVEDP ¼ left ventricular end diastolic pressure; other abbreviations as in Table 1.
TABLE 3 High-Risk PCI
Clinical
LVEF <35%
Electrical instability
Congestive heart failure
Comorbidities
Severe aortic stenosis
Severe mitral regurgitation
Chronic obstructive pulmonary disease
Chronic kidney disease
Diabetes
Cerebrovascular disease
Peripheral vascular disease
Age >75 yrs
Acute coronary syndrome
Coronary anatomy
Last patent vessel
UPLMN
3 vessel disease, SYNTAX score >33
Target vessel providing collaterals to a territory, which supplies>40% of the myocardium
Distal left main bifurcation
High-risk percutaneous coronary intervention (PCI) is defined in multiple clinicaltrials according to several key clinical features, comorbidities, and anatomicalfeatures that have shown to cause increased morbidity and mortality during PCIAdapted with permission from Myat et al. (43).
LVEF ¼ left ventricular ejection fraction; UPLMN ¼ unprotected left maincoronary artery.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6 Atkinson et al.M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3 Algorithm for Mechanical Circulatory Support
873
follow-up were those who had 2 or more vesselsrevascularized (32).
CARDIOGENIC SHOCK AFTER CARDIAC ARREST
WITH AND WITHOUT RETURN OF SPONTANEOUS
CIRCULATION. Out-of-hospital cardiac arrest carriesa significant morbidity and mortality, with only 7% to10% surviving to hospital discharge (33–35). Initialpresentation with ventricular tachycardia or ventric-ular fibrillation is associated with improved survivaloutcomes ranging from 25% to 30% (34). While
survival rates have increased over the last decade,improvements in management of cardiac arrest arewarranted. The 2015 American Heart AssociationUpdated Guidelines for cardiac arrest defines theterm ECPR as initiation of venoarterial ECMO(VA-ECMO) for cardiac arrest patients requiringongoing cardiopulmonary resuscitation (CPR), withthe goal to provide cardiopulmonary support whilespontaneous circulation is regained and reversiblecauses are identified and treated (33). Observationalstudies have demonstrated improvements in returnof spontaneous circulation (ROSC), mortality, andneurologic outcomes with ECPR; however, no ran-domized trial data exists (36–39). While the newguidelines do not support the routine use of ECPR, itis now a Class IIb recommendation in patients withcardiac arrest with ongoing CPR after 10 min.
PERCUTANEOUS MECHANICAL SUPPORT
DEVICES AVAILABLE AND TRIAL DATA
Three main MCS strategies are commonly utilized toprovide circulatory and left ventricular support.Circulatory support increases mean arterial bloodpressure which improves vital organ perfusion whileleft ventricular support reduces myocardial oxygendemand by reducing left ventricular pressure and

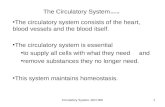
FIGURE 1 Comparison of MCS Devices
A structured approach to determine the best adjunctivemechanical circulatory support (MCS) device required involves understanding themechanisms, technical requirements,
and hemodynamic responses of each device. AO ¼ aorta; IABP¼ intra-aortic balloon pump; LA ¼ left atrium; LV¼ left ventricle; LVEDP ¼ left ventricular end diastolic
pressure; MAP ¼ mean arterial pressure; PCWP¼ pulmonary capillary wedge pressure; RA¼ right atrium; VA-ECMO ¼ venoarterial extracorporeal membrane oxygenation.
Atkinson et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
Algorithm for Mechanical Circulatory Support M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3
874
volume (Figure 1) (9,40–46). Although the mostextensive experience exists with the use of IABP, itprovides minimal hemodynamic support, which maybe insufficient to support more severe forms ofcardiogenic shock. Newer continuous flow devicessuch as Impella (left ventricle / aorta) andTandemHeart (left atrium / femoral artery) offera greater level of left ventricular support (Figure 2)(47). In the cardiovascular literature, VA-ECMO,femoral vein to femoral artery cannulation withextracorporeal oxygenation and nonpulsatile retro-grade femoral artery bypass, has been used predom-inantly in profound cardiogenic shock coupled withrespiratory failure and in cardiac arrest.
The use of MCS devices in HR-PCI and cardiogenicshock has been studied in several randomized clinicaltrials (Table 4) (7,20,23,30,39,48–57). IABP has beenstudied extensively and has not reduced mortality inpatients with cardiogenic shock or HR-PCI except in
the setting of ST-segment elevation myocardialinfarction patients treated with fibrinolysis (3,58,59).While randomized clinical trials have been too small todemonstrate a mortality benefit with Impellacompared to IABP in patients with HR-PCI and cardio-genic shock, these studies have demonstrated superiorhemodynamic support and maintenance of cardiacpower (23). Cardiac power (product of mean arterialblood pressure and cardiac output divided by 451)represents an independent predictor of mortality inthe setting of cardiogenic shock, acute myocardialinfarction and severe left ventricular systolicdysfunction (16,40). The FDA has recently approvedImpella devices for use in cardiogenic shock after acutemyocardial infarction or open heart surgery. Limitedrandomized clinical trials for TandemHeart demon-strate superior hemodynamic support compared toIABP in the setting of cardiogenic shock (48,49).Finally, while VA-ECMOprovides excellent circulatory

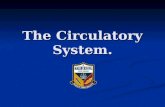
FIGURE 2 Comparison of MCS Devices and Their Impact on Cardiac Flow
Four main families of devices exist for percutaneous MCS, which includes IABP, Impella (Abiomed Inc., Danvers, Massachusetts), TandemHeart
(CardiacAssist, Inc., Pittsburgh, Pennsylvania), and VA-ECMO. Each device provides a different level of cardiac flow and device selection should
be tailored to the level of support needed. Abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6 Atkinson et al.M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3 Algorithm for Mechanical Circulatory Support
875
support, it has a higher vascular complication ratecompared to IABP; left ventricular venting is oftenrequired to prevent increased myocardial oxygen de-mand secondary to increased afterload, which canprecipitate further myocardial ischemia (55,56,60,61).Despite the lack of randomized clinical trials, registrydata with ECMO has resulted in an increased applica-tion in patients with cardiac arrest (47,62).
PRACTICAL APPROACH TO PERCUTANEOUS
MCS IN CARDIOGENIC SHOCK, HR-PCI, AND
CARDIOGENIC SHOCK AFTER CARDIAC
ARREST WITH AND WITHOUT ROSC
Cardiogenic shock, HR-PCI, and cardiac arrest patientsrepresent a wide spectrum of disease that requirestailored therapy to improve individual hemodynamicderangements. First, prompt recognition of patientswith cardiogenic shock and identification of patientswith high-risk features for PCI is essential. Onceidentified, a multidisciplinary heart team approach, aspioneered in the SYNTAX (SYNergy Between PCI WithTAXUS and Cardiac Surgery) and PARTNER (Place-ment of AoRTic TraNscathetER Valve Trial EdwardsSAPIEN Transcatheter Heart Valve) trials, with inter-ventional cardiology, cardiothoracic surgery, criticalcare, and advanced heart failure physicians should beinitiated (63,64). The next step is to identify diseaseseverity from a PCI and/or shock perspective todetermine the most appropriate level of support. Withthe advent of multiple devices, identifying which de-vice to use can be challenging for the intervention-alist. We created an algorithm to simplify decisionmaking in this challenging patient population, whichwill be outlined subsequently (Central Illustration).
IDENTIFICATION OF CARDIOGENIC SHOCK AND
HR-PCI PATIENTS. Identification of hemodynamicderangement can help define the level of shock.Multiple critical care scores exist to predict the
severity of shock with the most familiar being theAPACHE II (Acute Physiology and Chronic HealthEvaluation II) score (12). In general, signs of hypo-perfusion including altered mental status, decreasedurine output (<30 ml/h), elevated lactate, elevatedcreatinine, elevated liver function tests, cool ex-tremities, or hemodynamics refractory to medicaltherapy and/or IABP correspond to severe shockwhich requires the highest level of support (12–15).Quick classification and resuscitation is required,while consultation with the heart team and decisionfor mechanical support is made.
In the setting of HR-PCI patients, identificationof patients with significant comorbidities, ejectionfraction <35%, last patent vessel, severe 3VD(SYNTAX score >33), and unprotected left main dis-ease is critical.
HEART TEAM APPROACH. First described in theSYNTAX and PARTNER trials, the multidisciplinaryheart team has typically been comprised of inter-ventional cardiologists and cardiothoracic surgeonsto participate in clinical decision making with revas-cularization and valvular heart disease specificallysevere aortic stenosis (63–65). In the setting ofcardiogenic shock, the multidisciplinary heart teamshould expand to include advanced heart failure andintensive care physicians who will play an essentialrole in the post-procedure management. The poten-tial benefits of the heart team have not been evalu-ated or clearly defined in a clinical trial, but mayinclude improved patient outcomes and system basedoutcomes (65). Due to the emergent nature ofcardiogenic shock and requirement for quick inter-vention, a heart team approach is not always feasible.
PATIENT ASSESSMENT/TECHNICAL ASPECTS/TIPS
AND TRICKS. Several technical requirements must beconsidered prior to choosing a device for MCSincluding identifying indications, contraindications,

TABLE 4 Contemporary Outcomes for MCS Devices
First Author/Trial(Ref. #) Indication HR-PCI/Shock Definition N Devices Outcomes Complications
Burkhoff et al. (48) CS CI <2.2 l/min/m2, PCWP >15, endorgan hypoperfusion (low UOP,AMS), high dose vasopressor orinotrope, failed IABP
42 IABP versusTandemHeart
No difference in survival or30-day adverse events.
Better hemodynamics withTandemHeart (CI, MAP)
Kar et al. (49) Severe CS SBP <90 mm Hg, CI <2 l/min/m2,end organ failure despite IABP/pressors/inotropes
117 TandemHeart(82% had IABP prior
to TandemHeart)
30-day survival: 60% Bleeding aroundcannula sites 29%
Blood transfusions:59.8%
Thiele et al. (57) CS in AMI(95% PCI)
SHOCK trial definition,lactate >2, CI <2.1 l/min/m2
41 IABP ¼ 20TandemHeart ¼ 21
Superior hemodynamicsupport withTandemHeart:
[ CPI, Y lactate, PCWPSimilar 30-day mortality
Increased bleeding andlimb ischemia
Alli et al. (50) ProphylacticHR-PCI
EF <30% with a Jeopardy score >8in which occlusion of the targetvessel(s) either transient orpermanent could result incardiogenic shock, CPR, or death
54 TandemHeart 6-month survival: 87% 13% vascularcomplications
ISAR-SHOCK (51) Severe CS in AMI SHOCK trial definition 25 IABP versus Impella 30-day survival: 54%in both
Superior hemodynamicswith Impella (CI, CPI)
Hemolysis
USPella (30) ProphylacticHR-PCI
Severe 3VD, UPLMN, last patentvessel, low EF
No STEMI or shock,mean SYNTAX score 36
175 Impella 2.5 12-month survival: 88% MACE: 8%
EuroPella (52) ProphylacticHR-PCI
Severe 3VD, UPLMN, last patentvessel, EF <30%
No STEMI or shock
144 Impella 2.5 30-day survival: 94.5% MI: 0%, stroke 0.7%,bleeding 6.2%,vascularcomplication 4%
Protect I (7) HR-PCI Last patent vessel, UPLMN,EF <35%
No STEMI or shock
20 Impella 2.5 MACE 20%
PROTECT-II (23) HR-PCI UPLMN, last patent vessel,EF <35%, 3VD, and EF <30%
452 IABP (226) versusIMPELLA 2.5 (226)
Superior hemodynamicswith Impella (CPO)
No statistical difference inMAE
MAE: MAE 30 & 90days: (ITT)
Impella: 35.1%, 40.6%IABP: 40.1%, 49.3%
Nichol et al. (54) CS and/or cardiacarrest
1,49484 studies
VA-ECMO 50% survival to hospitaldischarge
Vascular injury,bleeding and stroke
ELSO registry (39) Cardiac arrest 75% cardiac disease 2,633:295 ECPR
VA-ECMO 91% 27% survival to hospitaldischarge
Neurologiccomplications 33%
Takyama et al. (53) Refractory CS,23% active CPR
SBP <90 mm Hg, CI <2.0 l/min/m2,evidence of end-organ failuredespite inotropes/vasopressorsor IABP
90 VA-ECMO 49% survival to hospitaldischarge
Bleeding and stroke:26% and 18%
LV distention andpulmonary edema
Teirstein et al. (55) HR-PCI andVA-ECMO
1) Stable or unstable angina pectoris;2) at least 1 coronary arterystenosis amenable to PCI; 3)EF <25%; or 4) angioplastytarget vessel supplying >50% ofthe viable myocardium, or both
389: prophylacticCPS
180: standby CPS
CPS [ Procedural morbidityprophylactic 41.3 versus9.4% standby, noimprovement inoutcome
7.2% required initiationof standby CPS
Standby CPS: providedexcellent supportand recommendedover prophylacticCPS
Schreiberet al. (56)
HR-PCI Low EF, culprit vessel supplying themajority of myocardium, orintended multivessel angioplasty
CPS: 58IABP: 91
IABP versus CPS No difference in MACE (MI,stroke, death, CABG)
Multivessel angioplastysuccess rates higher inCPS (40% vs. 20%)
Increased vascularrepair with CPS(14 v. 3%)
Increased transfusionwith CPS(60 versus 27%)
Sheu et al. (20) AMI and CS Profound CS: SBP <75 mm Hgdespite inotropes and IABPsupport, with AMS, oliguria, andrespiratory failure requiringmechanical ventilatory support
Group 1: 115Group 2: 219
In Group 1 ECMO:100% IABP, 25profound CS, noECMO
In Group 2: 46profound CS þECMO
60.9% 30-day survival inECMO group versus 28%30-day survival in non-ECMO group
PCI completed withstent in 70%
Mechanical circulatory support (MCS) devices have been studied in cardiogenic shock (CS) and high-risk percutaneous coronary intervention (HR-PCI) in several randomized controlled trials and observationalstudies. This is not a complete review of the literature for MCS devices in CS and HR-PCI, but highlights many of the important studies within this field.
3VD ¼ 3-vessel disease; AMI ¼ acute myocardial infarction; AMS ¼ altered mental status; CABG ¼ coronary artery bypass graft; CI ¼ cardiac index; CPI ¼ cardiac power index; CPO ¼ cardiac power;CPR ¼ cardiopulmonary resuscitation; CPS ¼ cardiopulmonary support; ECMO ¼ extracorporeal membrane oxygenation; EF ¼ ejection fraction; IABP ¼ intra-aortic balloon pump; MACE ¼ major adversecardiac events; MAP ¼ mean arterial pressure; MI ¼ myocardial infarction; PCWP ¼ pulmonary capillary wedge pressure; SBP ¼ systolic blood pressure; STEMI ¼ ST-segment elevation myocardial infarction;UOP ¼ urine output; UPLMN ¼ unprotected left main artery; VA-ECMO ¼ venoarterial extracorporeal membrane oxygenation.
Atkinson et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
Algorithm for Mechanical Circulatory Support M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3
876

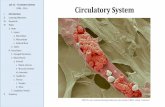
CENTRAL ILLUSTRATION Algorithm for Percutaneous MCS Device Selection in Patients with Cardiogenic Shock,Cardiac Arrest, and HR-PCI
Atkinson, T.M. et al. J Am Coll Cardiol Intv. 2016;9(9):871–83.
3VD ¼ 3 vessel coronary artery disease; AS ¼ aortic stenosis; BiV ¼ biventricular; CI ¼ cardiac index; CPO ¼ cardiac power; EF ¼ ejection fraction; HR ¼ heart rate;
HR-PCI ¼ high-risk percutaneous coronary intervention; IABP ¼ intra-aortic balloon pump; LVEDP ¼ left ventricular end-diastolic pressure; MCS ¼ mechanical
circulatory support; MR ¼ mitral regurgitation; PCI ¼ percutaneous coronary intervention; PCWP ¼ pulmonary capillary wedge pressure; ROSC ¼ return of spontaneous
circulation; RVAD ¼ right ventricular assist device; SBP ¼ systolic blood pressure; UPLMN ¼ unprotected left main artery; VA-ECMO ¼ venoarterial extracorporeal
membrane oxygenation.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6 Atkinson et al.M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3 Algorithm for Mechanical Circulatory Support
877
access site, and operator experience. Each device hasspecific contraindications, which must be noted priorto the procedure (Table 5) (9,43,66). While moderateto severe aortic regurgitation and ventricular septaldefect are listed as contraindications to Tandem-Heart, isolated case reports have used TandemHeartfor support in both settings (67,68).
Access remains a key issue with regard to technicalfeasibility as these patients not only have severe
coronary atherosclerotic disease, but often have ilio-femoral atherosclerotic disease as well, which createschallenges secondary to vessel tortuosity and heavycalcification. Pelvic angiography should be performedto assess iliofemoral vasculature, but computed to-mography pelvic angiography can be done as analternative for pre-procedural planning. If the iliofe-moral arteries are not suitable for access, thensubclavian or axillary arterial access with an 8 to

TABLE 5 MCS Device Contraindications and Complications
IABP Impella TandemHeart VA-ECMO
Contraindications Moderate to severe ARSevere PADAortic disease
LV thrombusMechanical aortic valveAortic stenosis with
AVA <0.6Moderate to severe ARSevere PADContraindication to
anticoagulation
Severe PADHITDICContraindications to
anticoagulationLA thrombusVSDModerate to severe AR
Contraindications toanticoagulation
Moderate to severe ARSevere PAD
Complications StrokeLimb ischemiaVascular traumaBalloon ruptureThrombocytopeniaAcute kidney injuryBowel ischemiaInfection
Device migrationDevice thrombosisLimb ischemiaVascular traumaHemolysisInfectionStroke
Air embolismThromboembolismDevice DislodgementCardiac tamponadeLimb ischemiaVascular traumaHemolysisInfectionStroke
BleedingVascular traumaLimb ischemiaCompartment syndromeAcute kidney injuryHemolysisThromboembolismAir embolismInfectionNeurological Injury
Bleeding/hemolysis þ þþ þþ þþVascular complications þ þþ þþþ þþþþ
Contraindications and complications must be reviewed prior to MCS device use in all patients and can vary according to device.
AR ¼ aortic regurgitation; AVA ¼ aortic valve area; DIC ¼ disseminated intravascular coagulation; HIT ¼ heparin-induced thrombocytopenia; LA ¼ left atrium; LV ¼ leftventricle; PAD ¼ peripheral arterial disease; VSD ¼ ventricular septal defect; other abbreviations as in Table 4.
Atkinson et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
Algorithm for Mechanical Circulatory Support M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3
878
10 mm � 20 cm vascular graft can be pursued tofacilitate Impella placement (69,70). Recently atranscaval approach has been performed (71). Pre-procedural planning when feasible with vascularsurgery or interventional radiology can provideexpert guidance to determine the best point of accessfor each patient (Table 6) (70,72–75).
One must also consider the learning curve that ex-ists with these devices reported by Henriques et al.(76). In a pre-specified analysis in the PROTECT II trial,which removed the operator’s placement of first IABPand first Impella treated patient at each site fromanalysis, there was a reduction of major adverse eventfrom 50% to 38% (p ¼ 0.029) at 90 days for Impellasupported patients (76). For this reason it is importantthat if Impella or TandemHeart is used, that there is anexperienced team that inserts and works on this de-vice. Institutional systems, team familiarity, post-procedure recovery and device management must allbe taken into consideration when choosing a device.
Device escalation is often required if the initialsupport device (usually IABP) does not improve he-modynamics and end organ perfusion.
DEVICE SELECTION. Pre-shock/shock . In the set-ting of pre-shock with systemic hypoperfusion with-out a blood pressure<100mmHg, itmay be reasonableto use an IABP while performing PCI (21). Quick feed-back loops incorporating patient status and hemody-namics are required to assess the need for escalation ofsupport to an Impella, TandemHeart, or VA-ECMO. Forpatients with shock, we recommendMCSwith Impella.We recommend repeat hemodynamic assessment 15 to
30 min after initial device placement. In the ISAR-SHOCK (Efficacy Study of LV Assist Device to TreatPatients With Cardiogenic Shock) trial, hemodynamicsin the IABP group noted a 0.11 increase in cardiac indexand decrease in diastolic blood pressure and meanarterial pressure within 30min while Impella 2.5 notedan increase of 0.49 in cardiac index and increase inmean arterial pressure within 30 min (51).Severe shock . In patients meeting criteria for severecardiogenic shock, initial management requiresmechanical support devices including Impella (CP or5.0) or TandemHeart, not an IABP. The Impella familyoffers 2 different sizes devices that can be insertedpercutaneously (2.5 and CP) via the arterial circulationand 5.0 which can be implanted transcavally (personalcommunication, W.W. O’Neill, December 30, 2015) orsurgically. A multidisciplinary heart team consulta-tion should be completed as further escalation forsurgical left ventricular assist devices or VA-ECMOmay be needed.
In the setting of cardiogenic shock secondary toacute right ventricular systolic dysfunction, the mainoptions for hemodynamic support include Tandem-Heart ProTek Duo (CardiacAssist, Inc., Pittsburgh,Pennsylvania), Impella RP (Abiomed Inc., Danvers,Massachusetts), and VA-ECMO (77,78). In patientswith biventricular failure, percutaneous optionsinclude VA-ECMO or combination of percutaneousright ventricular assist devices such as TandemHeartor Impella RP with an Impella CP or 5.0 (79).
Card iogen ic shock after card iac arrest with andwithout ROSC. For the patients with profound

TABLE 6 Tips and Tricks
Vascular access
Femoral
Micropuncture needle
Ultrasound guidance
Benefit: anterior stick above femoral bifurcation
Stiff wire: for sheath delivery in morbidly obese, tortuousanatomy or heavy calcification
Amplatz Extra Stiff
Amplatz Super Stiff
Backup Meier
Axillary/subclavian
Surgical placement: 8–10 mm x 20 cm vascular graft
Severe tortuosity
Lunderquist Extra Stiff Wire (if prior wires have failed)
13/14-F 30 cm Cook Check Flo Sheath
Vascular closure
Pre-close technique
Deployment of 2 Perclose ProGlide devices 90� apart (10 o’clockand 2 o’clock) prior to large bore sheath insertion
Manual
Femostop under patient prior to sheath removal for emergencyuse
45-min compression
2 physicians present at bedside
Vascular surgery
Surgical repair
Device escalation
IABP removal
Obtain contralateral access
Place Impella in contralateral artery
Place IABP on standby
Pull back balloon until it reaches the end of the sheath
Slowly remove balloon through sheath
If unable to remove through sheath, a 0.025” exchange lengthwire or 0.018” Platinum Plus wire can be placed through theballoon pump lumen.
Remove the sheath and balloon as one leaving the wire in place.
Upsize sheath by 0.5- to 1-F size
Closure device can then be deployed or sheath can be used forfurther arterial access for PCI if indicated
Meticulous access is required to limit vascular complications. Several tips andtricks are outlined to provide guidance for successful device placement.
Abbreviations as in Table 4.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6 Atkinson et al.M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3 Algorithm for Mechanical Circulatory Support
879
cardiopulmonary failure (left ventricular and/orbiventricular) including respiratory failure with dif-ficulty maintaining oxygenation/ventilation orongoing cardiopulmonary resuscitation, the use ofVA-ECMO should be considered in centers withdedicated ECMO teams. VA-ECMO provides total cir-culatory support and can achieve a circulatory flowrates up to 7 l/min. A dedicated perfusionist isrequired. However, the use of this device can beassociated with left ventricular distention andadequate techniques for venting the left ventriclemay be simultaneously required (i.e., IABP, Impella,veno-veno-arterial ECMO, biatrial cannulation)(60,80).
HR-PCI . Pre-procedural planning is key to successwhen approaching complex, high-risk interventions.With the use of MCS, the term “protected PCI” is nowthe mainstay for complex coronary revascularization.For patients undergoing protected PCI, randomizeddata and registry information has not demonstrated abenefit of IABP (Table 7) (3–5,58,59,81,82). Impellasupport, however, enhances 90-day major adverseevent free survival compared to IABP protectedpatients (23). The mechanism for this benefit appearsto be related to greater support of cardiac power andreduction in hypotensive events during PCI for Impellaprotected patients. Given the results of the PROTECT IItrial, Impella 2.5 is approved for the use in HR-PCI. Inhigher risk patients and complex anatomy requiringprolonged balloon inflations or adjunct therapies thatmay precipitate significant myocardial ischemia theImpella CP should be considered. Given that HR-PCI isoften performed electively, pre-procedural planningincluding a heart team approach is essential; ad-hocHR-PCI should be limited to unstable patients.POST-PROCEDURE CARE. A critical aspect to MCS, isdevicemanagement post-procedurewhen transferringto an intensive care unit (ICU) and weaning the devicein the setting of HR-PCI. Establishment of appro-priate training and protocols within each institution iscritical to continued hemodynamic support of patientswith cardiogenic shock or HR-PCI post device place-ment. Cardiogenic shock requires a multidisciplinaryteam approach as patients can now be supportedwith left ventricular assist devices over prolongedperiods to allow decisions regarding permanent leftventricular assist devices or cardiac transplantation.
Another important consideration is anticoagulationmanagement and hemolysis. While hemolysis is rare,platelet counts, hemoglobin and hematocrit should befollowed on a daily basis. Anticoagulation protocolsshould be implemented with appropriate bleedingreduction strategies.
The long-term use of support devices increases therisk for complications. Each device has specific com-plications that require different treatments (Table 5)(9,43,66). Device migration is one of the most com-mon issues encountered with both the Impella andTandemHeart and can be associated with pooreroutcomes. This is a less common issue with the IABP.Patient immobilization with femoral cannulation anddedicated nursing staff familiar with these issuesare essential.DEVICE WEANING AND REMOVAL. Weaning pro-tocols are at the discretion of the physician and shouldbe created for each institution. In the setting of HR-PCI, weaning may occur in the cardiac catheteriza-tion laboratory. If an IABP is in place, we recommend

TABLE 7 Contemporary Trials With IABP
Trial/First Author(Ref. #) Indication Definition N
Control or NoIABP Survival
Prophylactic orIABP Survival Routine Use
IABP-SHOCK-II (3) AMI and CS SBP <90 mm Hg for >30 minor vasoactive medicationsneeded to maintain SBP>90, pulmonary edema,end-organ dysfunction(AMS, cool extremities,UOP<30 ml/h, lactate >2)
600 41.3% 39.7% No difference in survival
TACTICs (59) AMI and CS s/p fibrinolysis 57 67% at 30 daysKillip III/IV: 20% at
6 months
73% at 30 daysKillip III/IV: 61% at
6 months
No significant differenceexcept in Killip III/IVpatients who receivedIABP
Waksman et al. (58) AMI and CS s/p fibrinolysis 45 19% 46% In-hospital survivalimproved with IABP usein patients s/pfibrinolysis
NRMI (81) AMI and CS Observational study: IABPcompared to no IABPamong patients givenfibrinolysis or primaryangioplasty
IABP ¼ 7,268No IABP ¼ 15,912
Lytics: 67%in-hospitalmortality
PTCA: 42%in-hospitalmortality
Lytics: 49% in-hospitalmortality
PTCA: 47% in-hospitalmortality
IABP provided substantialbenefit in patients withAMI and CS whoreceived fibrinolysis
CRISP-AMI (5) Anterior MI withplanned PCI
Prophylactic IABP 337 No difference insurvival
No difference insurvival
No reduction in infarct size
NCDR (82) High risk includingSTEMI and CS
UPLMN, CS, severelydepressed EF (<30%), orSTEMI
181,599 No difference inmortality
No difference inmortality
BCIS-1 (4) HR-PCI EF <30%, severe CAD:jeopardy score >8, noshock or STEMI
301 No difference insurvival
No difference insurvival
Increase minor bleeding inIABP arm
Decreased periproceduralcomplications in IABP(decreasedhypotension)
Elective IABP at 5 yrsassociated with RRR34% for all-causemortality
A nonexhaustive review of the literature for IABP use in cardiogenic shock and HR-PCI.
CAD ¼ coronary artery disease; lytics ¼ fibrinolytics; PTCA ¼ percutaneous transluminal coronary angioplasty; RRR ¼ relative risk reduction; s/p ¼ status post; other abbreviations as in Table 4.
Atkinson et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
Algorithm for Mechanical Circulatory Support M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3
880
placing the patient on 1:2 for 10min, followed by 1:3 for10 min. If stable for 10 min, the device can be removed.Abiomed provides 2 general weaning strategies with arapid and slow weaning protocol for the Impella de-vices (70,74,83). In the setting of HR-PCI, the rapidweaning protocol can be used which consists ofdecreasing the level of support by 2 levels at a timeevery 10 min until P2. If the patient remains stable onlevel P2 for 10 min, then the device can be removed. Atthe time of device removal, the device is turned downto P1 and the Impella pulled back into the descendingthoracic aorta. Once in the descending thoracic aorta,the device can be turned off completely to P0 andremoved. In most cases, the device can be removedsafely at the end of the case.
In the ICU weaning is best accomplished overseveral hours, and should begin immediately in pa-tients that demonstrate hemodynamic improvementwith MCS and have good end organ perfusion and
function. An IABP should be weaned with initialreduction in assisted beats from 1:1 to 1:2 to 1:3 overseveral hours. If stable on 1:3 for 3 h, the deviceshould be set at 1:1 and the heparin infusion should bestopped for device removal once the PTT is <50 s.Impella should be weaned over several hours withreduction in level of support by 2 levels every 2 to 3 huntil level P2. Once stable at level P2 for 2 to 3 h thedevice can be removed. After the device has beenremoved, the patient is vulnerable and may requirereinsertion of a device, which can be difficult after allaccess sheaths are removed.
Interventional cardiologists must become facilewith large bore sheath vascular closure techniques.Arterial access can be closed utilizing the pre-closetechnique, surgical closure, or manual pressure(Table 6). Although manual hemostasis can beachieved, it should not be the default technique. Thepre-close technique is the preferred strategy (72,75).

PERSPECTIVES
WHAT IS KNOWN? Mechanical circulatory support devices
have been used for decades to support patients in cardiogenic
shock or patients undergoing high-risk percutaneous coronary
intervention. Newer devices offer a greater level of hemody-
namic support, but device selection can often be challenging.
WHAT IS NEW? An algorithm was created to guide interven-
tional cardiologists in clinical decision making for choosing
mechanical circulatory support devices in patients undergoing
percutaneous coronary intervention with high risk features or
cardiogenic shock.
WHAT IS NEXT? Despite the ability to provide superior
hemodynamic support, this has not translated into improved
clinical outcomes. Further studies are needed to understand this
discrepancy.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6 Atkinson et al.M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3 Algorithm for Mechanical Circulatory Support
881
IMPLEMENTATION OF A SUCCESSFUL
PERCUTANEOUS MECHANICAL
CIRCULATORY SUPPORT PROGRAM
With multiple MCS devices available, each institutionmust develop a strategy for the preferred MCS devicefor patients with adequate training of cardiac cathe-terization and ICU staff. A critical aspect of devicemanagement involves unification of cardiac cathe-terization staff, coronary care intensivists and nurses,interventional cardiologists, advanced heart failurecardiologists, and cardiothoracic surgeons to createan operational strategy for each institution. This fa-cilitates protocols that can be used and executed in atimely manner and assist in especially for trouble-shooting issues or complications. Ideally, this teamshould also review the outcomes for all patientstreated with left ventricular support devices totabulate and evaluate complications as well as iden-tify process improvement areas.
Interventional cardiology and cardiac catheteriza-tion expertise is critical to the success of a per-cutaneous MCS program. As noted previously, asignificant learning curve exists; each institutionshould become familiar with at least 2 levels of sup-port including IABP and Impella or TandemHeart inorder to provide safe and efficient delivery of care inpatients with HR-PCI and cardiogenic shock. Invest-ment in training the interventionalist and cardiaccatheterization team will improve patient care andhemodynamic support with the use of MCS.
CONCLUSIONS
The use of mechanical support devices has undergonedramatic changes in the last decade when applied topatients undergoing HR-PCI including those pre-senting with cardiogenic shock or cardiac arrest. Cli-nicians must quickly assess clinical presentation,hemodynamics, and anatomy to determine the mostappropriate MCS device.
1. We created an algorithm to help guide interven-tional cardiologists on the appropriate clinical
scenarios for the use of various percutaneous MCSdevices in the setting of HR-PCI, cardiogenicshock, and cardiac arrest.
2. Technical considerations must be taken into ac-count with regards to access, indications, andcontraindications of each device.
3. A multidisciplinary heart team involving inter-ventional cardiology, cardiothoracic surgery,intensive care, and advanced heart failure physi-cians should be utilized for decision-making pro-cesses when time permits and for post-devicemanagement.
4. Adequate training of the interventional cardiolo-gist, cardiac catheterization laboratory staff, andICU staff must be performed for MCS program tosucceed.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Joaquin E. Cigarroa, MD, Knight CardiovascularInstitute, Cardiovascular Division, UHN-62, OregonHealth & Science University, 3181 Southwest SamJackson Park Road, Portland, Oregon 97239. E-mail:[email protected].
RE F E RENCE S
1. Moulopoulos SD, Topaz S, Kolff WJ. Diastolicballoon pumping (with carbon dioxide) in theaorta–a mechanical assistance to the failing cir-culation. Am Heart J 1962;63:669–75.
2. Kantrowitz A, Tjonneland S, Freed PS,Phillips SJ, Butner AN, Sherman JL Jr. Initial clin-ical experience with intraaortic balloon pumping incardiogenic shock. JAMA 1968;203:113–8.
3. Thiele H, Zeymer U, Neumann FJ, et al. Intra-aortic balloon support for myocardial infarctionwith cardiogenic shock. N Engl J Med 2012;367:1287–96.
4. Perera D, Stables R, Thomas M, et al. Electiveintra-aortic balloon counterpulsation during high-risk percutaneous coronary intervention: a ran-domized controlled trial. JAMA 2010;304:867–74.
5. Patel MR, Smalling RW, Thiele H, et al. Intra-aortic balloon counterpulsation and infarct size inpatients with acute anterior myocardial infarctionwithout shock: the CRISP AMI randomized trial.JAMA 2011;306:1329–37.
6. Henriques JP, Remmelink M, Baan J Jr., et al.Safety and feasibility of elective high-risk percu-taneous coronary intervention procedures with

Atkinson et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6
Algorithm for Mechanical Circulatory Support M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3
882
left ventricular support of the Impella Recover LP2.5. Am J Cardiol 2006;97:990–2.
7. Dixon SR, Henriques JP, Mauri L, et al.A prospective feasibility trial investigating the useof the Impella 2.5 system in patients undergoinghigh-risk percutaneous coronary intervention (ThePROTECT I Trial): initial U.S. experience. J Am CollCardiol Intv 2009;2:91–6.
8. Burkhoff D, O’Neill W, Brunckhorst C, Letts D,Lasorda D, Cohen HA. Feasibility study of theuse of the TandemHeart percutaneous ventricu-lar assist device for treatment of cardiogenicshock. Catheter Cardiovasc Interv 2006;68:211–7.
9. Rihal CS, Naidu SS, Givertz MM, et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statementon the Use of Percutaneous Mechanical CirculatorySupportDevices inCardiovascular Care: Endorsed bythe American Heart Assocation, the CardiologicalSociety of India, and Sociedad Latino Americana deCardiologia Intervencion;AffirmationofValueby theCanadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d’interven-tion. J Am Coll Cardiol 2015;65:e7–26.
10. Goldberg RJ, Gore JM, Alpert JS, et al.Cardiogenic shock after acute myocardial infarc-tion. Incidence and mortality from a community-wide perspective, 1975 to 1988. N Engl J Med1991;325:1117–22.
11. Hochman JS, Sleeper LA, Webb JG, et al. Earlyrevascularization in acute myocardial infarctioncomplicated by cardiogenic shock. SHOCK In-vestigators. Should We Emergently RevascularizeOccluded Coronaries for Cardiogenic Shock. N EnglJ Med 1999;341:625–34.
12. Knaus WA, Draper EA, Wagner DP,Zimmerman JE. APACHE II: a severity of diseaseclassification system. Crit Care Med 1985;13:818–29.
13. Marshall JC, Cook DJ, Christou NV, Bernard GR,Sprung CL, Sibbald WJ. Multiple organ dysfunctionscore: a reliable descriptor of a complex clinicaloutcome. Crit Care Med 1995;23:1638–52.
14. Vincent JL, Moreno R, Takala J, et al. The SOFA(Sepsis-related Organ Failure Assessment) scoreto describe organ dysfunction/failure. On behalf ofthe Working Group on Sepsis-Related Problems ofthe European Society of Intensive Care Medicine.Intensive Care Med 1996;22:707–10.
15. Samuels LE, Kaufman MS, Thomas MP,Holmes EC, Brockman SK, Wechsler AS. Pharma-cological criteria for ventricular assist deviceinsertion following postcardiotomy shock: experi-ence with the Abiomed BVS system. J Card Surg1999;14:288–93.
16. Fincke R, Hochman JS, Lowe AM, et al. Cardiacpower is the strongest hemodynamic correlate ofmortality in cardiogenic shock: a report from theSHOCK trial registry. J Am Coll Cardiol 2004;44:340–8.
17. Hasdai D, Holmes DR Jr., Califf RM, et al.Cardiogenic shock complicating acute myocardialinfarction: predictors of death. GUSTO Investi-gators. Global Utilization of Streptokinase andTissue-Plasminogen Activator for Occluded Coro-nary Arteries. Am Heart J 1999;138:21–31.
18. Torre-Amione G, Milo-Cotter O, Kaluski E,et al. Early worsening heart failure in patientsadmitted for acute heart failure: time course,hemodynamic predictors, and outcome. J Card Fail2009;15:639–44.
19. Afifi AA, Chang PC, Liu VY, da Luz PL, Weil MH,Shubin H. Prognostic indexes in acute myocardialinfarction complicated by shock. Am J Cardiol1974;33:826–32.
20. Sheu JJ, Tsai TH, Lee FY, et al. Early extra-corporeal membrane oxygenator-assisted primarypercutaneous coronary intervention improved30-day clinical outcomes in patients withST-segment elevation myocardial infarctioncomplicated with profound cardiogenic shock. CritCare Med 2010;38:1810–7.
21. Menon V, Slater JN, White HD, Sleeper LA,Cocke T, Hochman JS. Acute myocardial infarctioncomplicated by systemic hypoperfusion withouthypotension: report of the SHOCK trial registry.Am J Med 2000;108:374–80.
22. Go AS, Mozaffarian D, Roger VL, et al. Heartdisease and stroke statistics–2014 update: a reportfrom the American Heart Association. Circulation2014;129:e28–292.
23. O’Neill WW, Kleiman NS, Moses J, et al.A prospective, randomized clinical trial of hemo-dynamic support with Impella 2.5 versusintra-aortic balloon pump in patients undergoinghigh-risk percutaneous coronary intervention: thePROTECT II study. Circulation 2012;126:1717–27.
24. Levine GN, Bates ER, Blankenship JC, et al.2011 ACCF/AHA/SCAI Guideline for PercutaneousCoronary Intervention. A report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines andthe Society for Cardiovascular Angiography andInterventions. J Am Coll Cardiol 2011;58:e44–122.
25. Sarkar K, Kini AS. Percutaneous left ventricularsupport devices. Cardiol Clin 2010;28:169–84.
26. Ellis SG, Tamai H, Nobuyoshi M, et al.Contemporary percutaneous treatment of unpro-tected left main coronary stenoses: initial resultsfrom a multicenter registry analysis 1994–1996.Circulation 1997;96:3867–72.
27. Kosuga K, Tamai H, Ueda K, et al. Initial andlong-term results of angioplasty in unprotectedleft main coronary artery. Am J Cardiol 1999;83:32–7.
28. Wallace TW, Berger JS, Wang A, Velazquez EJ,Brown DL. Impact of left ventricular dysfunctionon hospital mortality among patients undergoingelective percutaneous coronary intervention. Am JCardiol 2009;103:355–60.
29. Keelan PC, Johnston JM, Koru-Sengul T, et al.Comparison of in-hospital and one-year out-comes in patients with left ventricular ejectionfractions <or¼40%, 41% to 49%, and >or¼50%having percutaneous coronary revascularization.Am J Cardiol 2003;91:1168–72.
30. Maini B, Naidu SS, Mulukutla S, et al. Real-world use of the Impella 2.5 circulatory supportsystem in complex high-risk percutaneous coro-nary intervention: the USpella Registry. CatheterCardiovasc Interv 2012;80:717–25.
31. Nellis SH, Liedtke AJ, Whitesell L. Small coro-nary vessel pressure and diameter in an intactbeating rabbit heart using fixed-position and free-motion techniques. Circ Res 1981;49:342–53.
32. Kovacic JC, Kini A, Banerjee S, et al. Patientswith 3-vessel coronary artery disease and impairedventricular function undergoing PCI with Impella2.5 hemodynamic support have improved 90-dayoutcomes compared to intra-aortic balloon pump:a sub-study of the PROTECT II trial. J Interv Car-diol 2015;28:32–40.
33. Brooks SC, Anderson ML, Bruder E, et al. Part6: Alternative Techniques and Ancillary Devicesfor Cardiopulmonary Resuscitation: 2015 AmericanHeart Association Guidelines Update for Cardio-pulmonary Resuscitation and Emergency Cardio-vascular Care. Circulation 2015;132:S436–43.
34. Daya MR, Schmicker RH, Zive DM, et al. Out-of-hospital cardiac arrest survival improving overtime: Results from the Resuscitation OutcomesConsortium (ROC). Resuscitation 2015;91:108–15.
35. Sasson C, Rogers MA, Dahl J, Kellermann AL.Predictors of survival from out-of-hospital cardiacarrest: a systematic review and meta-analysis. CircCardiovasc Qual Outcomes 2010;3:63–81.
36. Chen YS, Lin JW, Yu HY, et al. Cardiopulmo-nary resuscitation with assisted extracorporeallife-support versus conventional cardiopulmonaryresuscitation in adults with in-hospital cardiac ar-rest: an observational study and propensity anal-ysis. Lancet 2008;372:554–61.
37. Maekawa K, Tanno K, Hase M, Mori K, Asai Y.Extracorporeal cardiopulmonary resuscitation forpatients with out-of-hospital cardiac arrest ofcardiac origin: a propensity-matched study andpredictor analysis. Crit Care Med 2013;41:1186–96.
38. Sakamoto T, Morimura N, Nagao K, et al.Extracorporeal cardiopulmonary resuscitationversus conventional cardiopulmonary resuscita-tion in adults with out-of-hospital cardiac arrest: aprospective observational study. Resuscitation2014;85:762–8.
39. Thiagarajan RR, Brogan TV, Scheurer MA,Laussen PC, Rycus PT, Bratton SL. Extracorporealmembrane oxygenation to support cardiopulmo-nary resuscitation in adults. Ann Thorac Surg2009;87:778–85.
40. Burkhoff D, Naidu SS. The science behindpercutaneous hemodynamic support: a review andcomparison of support strategies. CatheterCardiovasc Interv 2012;80:816–29.
41. Werdan K, Gielen S, Ebelt H, Hochman JS.Mechanical circulatory support in cardiogenicshock. Eur Heart J 2014;35:156–67.
42. Ouweneel DM, Henriques JP. Percutaneouscardiac support devices for cardiogenic shock:current indications and recommendations. Heart2012;98:1246–54.
43. Myat A, Patel N, Tehrani S, Banning AP,Redwood SR, Bhatt DL. Percutaneous circulatoryassist devices for high-risk coronary intervention.J Am Coll Cardiol Intv 2015;8:229–44.
44. Kar B, Basra SS, Shah NR, Loyalka P. Percu-taneous circulatory support in cardiogenic shock:interventional bridge to recovery. Circulation2012;125:1809–17.

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 9 , 2 0 1 6 Atkinson et al.M A Y 9 , 2 0 1 6 : 8 7 1 – 8 3 Algorithm for Mechanical Circulatory Support
883
45. De Silva K, Lumley M, Kailey B, et al. Coronaryand microvascular physiology during intra-aorticballoon counterpulsation. J Am Coll Cardiol Intv2014;7:631–40.
46. Remmelink M, Sjauw KD, Henriques JP, et al.Effects of left ventricular unloading by Impellarecover LP2.5 on coronary hemodynamics. Cath-eter Cardiovasc Interv 2007;70:532–7.
47. Napp LC, Kuhn C, Hoeper MM, et al. Cannu-lation strategies for percutaneous extracorporealmembrane oxygenation in adults. Clin Res Cardiol2016;105:283–96.
48. Burkhoff D, Cohen H, Brunckhorst C,O’Neill WW, TandemHeart Investigators G.A randomized multicenter clinical study to eval-uate the safety and efficacy of the TandemHeartpercutaneous ventricular assist device versusconventional therapy with intraaortic balloonpumping for treatment of cardiogenic shock. AmHeart J 2006;152:469.e1–8.
49. Kar B, Gregoric ID, Basra SS, Idelchik GM,Loyalka P. The percutaneous ventricular assistdevice in severe refractory cardiogenic shock.J Am Coll Cardiol 2011;57:688–96.
50. Alli OO, Singh IM, Holmes DR Jr., Pulido JN,Park SJ, Rihal CS. Percutaneous left ventricularassist device with TandemHeart for high-riskpercutaneous coronary intervention: the MayoClinic experience. Catheter Cardiovasc Interv 2012;80:728–34.
51. Seyfarth M, Sibbing D, Bauer I, et al.A randomized clinical trial to evaluate the safetyand efficacy of a percutaneous left ventricular assistdevice versus intra-aortic balloon pumping fortreatment of cardiogenic shock caused by myocar-dial infarction. J Am Coll Cardiol 2008;52:1584–8.
52. Sjauw KD, Konorza T, Erbel R, et al. Supportedhigh-risk percutaneous coronary intervention withthe Impella 2.5 device the Europella registry. J AmColl Cardiol 2009;54:2430–4.
53. Takayama H, Truby L, Koekort M, et al. Clinicaloutcome of mechanical circulatory support forrefractory cardiogenic shock in the current era.J Heart Lung Transplant 2013;32:106–11.
54. Nichol G, Karmy-Jones R, Salerno C, Cantore L,Becker L. Systematic review of percutaneouscardiopulmonary bypass for cardiac arrest or cardio-genic shock states. Resuscitation 2006;70:381–94.
55. Teirstein PS, Vogel RA, Dorros G, et al. Pro-phylactic versus standby cardiopulmonary supportfor high risk percutaneous transluminal coronaryangioplasty. J Am Coll Cardiol 1993;21:590–6.
56. Schreiber TL, Kodali UR, O’Neill WW,Gangadharan V, Puchrowicz-Ochocki SB, Grines CL.Comparison of acute results of prophylactic intra-aortic balloon pumping with cardiopulmonarysupport for percutaneous transluminal coronaryangioplasty (PCTA). Cathet Cardiovasc Diagn 1998;45:115–9.
57. Thiele H, Sick P, Boudriot E, et al. Randomizedcomparison of intra-aortic balloon support with apercutaneous left ventricular assist device in pa-tients with revascularized acute myocardialinfarction complicated by cardiogenic shock. EurHeart J 2005;26:1276–83.
58. Waksman R, Weiss AT, Gotsman MS, Hasin Y.Intra-aortic balloon counterpulsation improvessurvival in cardiogenic shock complicating acutemyocardial infarction. Eur Heart J 1993;14:71–4.
59. Ohman EM, Nanas J, Stomel RJ, et al.Thrombolysis and counterpulsation to improvesurvival in myocardial infarction complicated byhypotension and suspected cardiogenic shock orheart failure: results of the TACTICS Trial.J Thromb Thrombolysis 2005;19:33–9.
60. Kawashima D, Gojo S, Nishimura T, et al. Leftventricular mechanical support with Impella pro-vides more ventricular unloading in heart failurethan extracorporeal membrane oxygenation.ASAIO J 2011;57:169–76.
61. Pavlides GS, Hauser AM, Stack RK, et al. Effectof peripheral cardiopulmonary bypass on leftventricular size, afterload and myocardial functionduring elective supported coronary angioplasty.J Am Coll Cardiol 1991;18:499–505.
62. Jung C, Janssen K, Kaluza M, et al. Outcomepredictors in cardiopulmonary resuscitation facili-tated by extracorporeal membrane oxygenation.Clin Res Cardiol 2015;105:196–205.
63. Serruys PW, Morice MC, Kappetein AP, et al.Percutaneous coronary intervention versuscoronary-artery bypass grafting for severe coronaryartery disease. N Engl J Med 2009;360:961–72.
64. Leon MB, Smith CR, Mack M, et al. Trans-catheter aortic-valve implantation for aortic ste-nosis in patients who cannot undergo surgery.N Engl J Med 2010;363:1597–607.
65. Coylewright M, Mack MJ, Holmes DR Jr.,O’Gara PT. A call for an evidence-based approachto the Heart Team for patients with severe aorticstenosis. J Am Coll Cardiol 2015;65:1472–80.
66. Cheng R, Hachamovitch R, Kittleson M, et al.Complications of extracorporeal membraneoxygenation for treatment of cardiogenic shockand cardiac arrest: a meta-analysis of 1,866 adultpatients. Ann Thorac Surg 2014;97:610–6.
67. Pham DT, Al-Quthami A, Kapur NK. Percuta-neous left ventricular support in cardiogenic shockand severe aortic regurgitation. Catheter Car-diovasc Interv 2013;81:399–401.
68. Gregoric ID, Kar B, Mesar T, et al. Periopera-tive use of TandemHeart percutaneous ventricularassist device in surgical repair of postinfarctionventricular septal defect. ASAIO J 2014;60:529–32.
69. Sassard T, Scalabre A, Bonnefoy E, Sanchez I,Farhat F, Jegaden O. The right axillary arteryapproach for the Impella Recover LP 5.0 micro-axial pump. Ann Thorac Surg 2008;85:1468–70.
70. Impella 2.5 with the Automated ImpellaController, Circulatory Support System: In-structions for Use and Clinical Reference Manual.Danvers, MA: Abiomed, 2015.
71. Greenbaum AB, O’Neill WW, Paone G, et al.Caval-aortic access to allow transcatheter aorticvalve replacement in otherwise ineligible patients:initial human experience. J Am Coll Cardiol 2014;63:2795–804.
72. Krajcer Z, Howell M. A novel technique usingthe percutaneous vascular surgery device to close
the 22 French femoral artery entry site used forpercutaneous abdominal aortic aneurysm exclu-sion. Catheter Cardiovasc Interv 2000;50:356–60.
73. Estep JD, Cordero-Reyes AM, Bhimaraj A, et al.Percutaneous placement of an intra-aortic balloonpump in the left axillary/subclavian position pro-vides safe, ambulatory long-term support asbridge to heart transplantation. J Am Coll CardiolHF 2013;1:382–8.
74. Impella CP. Circulatory Support System.Instructions for Use and Clinical ReferenceManual. Danvers, MA: Abiomed, 2015.
75. Toggweiler S, Leipsic J, Binder RK, et al.Management of vascular access in transcatheteraortic valve replacement: part 1: basic anatomy,imaging, sheaths, wires, and access routes. J AmColl Cardiol Intv 2013;6:643–53.
76. Henriques JP, Ouweneel DM, Naidu SS, et al.Evaluating the learning curve in the prospectiveRandomized Clinical Trial of hemodynamic supportwith Impella 2.5 versus Intra-Aortic Balloon Pumpin patients undergoing high-risk percutaneouscoronary intervention: a prespecified subanalysisof the PROTECT II study. Am Heart J 2014;167:472–479.e5.
77. Anderson MB, Goldstein J, Milano C, et al.Benefits of a novel percutaneous ventricular assistdevice for right heart failure: The prospectiveRECOVER RIGHT study of the Impella RP device.J Heart Lung Transplant 2015;34:1549–60.
78. Kapur NK, Paruchuri V, Jagannathan A, et al.Mechanical circulatory support for right ventricu-lar failure. J Am Coll Cardiol HF 2013;1:127–34.
79. Kapur NK, Jumean M, Ghuloom A, et al. Firstsuccessful use of 2 axial flow catheters forpercutaneous biventricular circulatory support as abridge to a durable left ventricular assist device.Circ Heart Fail 2015;8:1006–8.
80. Jumean M, Pham DT, Kapur NK. Percutaneousbi-atrial extracorporeal membrane oxygenationfor acute circulatory support in advanced heartfailure. Catheter Cardiovasc Interv 2015;85:1097–9.
81. Barron HV, Every NR, Parsons LS, et al. The useof intra-aortic balloon counterpulsation in patientswith cardiogenic shock complicating acutemyocardial infarction: data from the NationalRegistry of Myocardial Infarction 2. Am Heart J2001;141:933–9.
82. Curtis JP, Rathore SS, Wang Y, Chen J,Nallamothu BK, Krumholz HM. Use and effective-ness of intra-aortic balloon pumps among patientsundergoing high risk percutaneous coronaryintervention: insights from the National Cardio-vascular Data Registry. Circ Cardiovasc Qual Out-comes 2012;5:21–30.
83. Cohen HA, Henriques JPS. Percutaneousventricular support. Interv Cardiol Clin 2013;2:397–498.
KEY WORDS cardiogenic shock, high-riskpercutaneous coronary intervention,mechanical circulatory support
Top Related