





Languages
Pages
Legal

8/2/2019 23172860 Liver Function
1/90
LIVER FUNCTION TESTSAND LIVER DISEASES
Prof. Fang ZhengDepartment of Laboratory MedicineSchool of Medicine, Wuhan University
8/2/2019 23172860 Liver Function
2/90
Anatomy of Liver
Functions of Liver
Tests of Liver Function
Liver Diseases
How to use biochemical tests of liverfunctions?
Content
8/2/2019 23172860 Liver Function
3/90
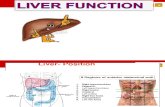
INTRODUCTION The liver is divided into four lobes.
8/2/2019 23172860 Liver Function
4/90
THE STRUCTUREOF LIVER
8/2/2019 23172860 Liver Function
5/90
The portal vein carries blood that has alreadypassed through the capillary bed of thegastrointestinal tract.
The hepatic artery carries well-oxygenatedblood to the liver. Both circulations mix in a vast network ofhepatic sinusoids and leave the liver via thehepatic vein. Sinusoids are lined byendothelial and Kupffers cells.
LOBES VASCULAR ANDBILIARY SYSTEMS
8/2/2019 23172860 Liver Function
6/90
LOBES VASCULAR ANDBILIARY SYSTEMS
In the liver the ductules merge into bileducts, hepatic ducts, and eventually thecommon hepatic ducts .Their bile drains into the right and lefthepatic ducts.
8/2/2019 23172860 Liver Function
7/90
Liver Function
1. Synthesis secretionplasma proteins,bile
2. Metabolism ofcarbohydrate
lipid, proteinvitamins, hormonebile acids, bilepigment, drug andtoxins
3. Detoxification (bio-
transformation)
8/2/2019 23172860 Liver Function
8/90
TESTS OF LIVERFUNCTION1.Tests of Protein Metabolism2. Tests of Bil irublin Metabolism3. Dye intake and Excretion4. Biochemical Serum Enzyme Tests5. Tests of Viral Hepatitis6. Other tests
8/2/2019 23172860 Liver Function
9/90
Tests of ProteinMetabolism1. Serum total protein (TP), albumin (A) and globulin(G)
2. Serum protein electrophoresis
3. Hepatic neoplasm markers
8/2/2019 23172860 Liver Function
10/90
Serum total protein (TP),albumin (A) and globulin(G)Albumin
Albumin is quantitatively the most important plasmaprotein synthesized by the liver and thus is a useful
indicator of hepatic function. Albumin has a fairly longhalf-life in serum (20 days) and hence is not a goodindicator of hepatic protein synthesis in acute liverdisease.
Serum albumin levels are depressed in alcoholiccirrhosis.A crude measure of the livers synthetic capacity
hypoalbuminaemia: advanced chronic liver diseasesevere acute liver damage
8/2/2019 23172860 Liver Function
11/90
Globulin: The main proteins in serum. Total serum globin: the severity of
liver disease
Serum total protein (TP),albumin (A) and globulin(G)
8/2/2019 23172860 Liver Function
12/90
Reference Value Alb 40-55g/L TP 60-80g/L Globulin 20-30g/L
8/2/2019 23172860 Liver Function
13/90
Densitometric scan of a normal serum protein electrophoresispattern showing the relative position of the albumin,1,2, and
regions
Serum protein electrophoresis
8/2/2019 23172860 Liver Function
14/90
Hepatic neoplasmmarkers
alpha-fetoprotein(AFP): primaryhepatocellular carcinoma
Carcinoembryonic antigen(CEA): livermetastatic carcinoma or other carcinomas ofthe gastrointestinal system.
8/2/2019 23172860 Liver Function
15/90
Normal 400ng/mL
Reference Value(AFP)
8/2/2019 23172860 Liver Function
16/90
OTHER SERUM PROTEINSPRODUCED BY THE LIVER
Coagulation factors (prothrombin time)1) The liver synthesizes six coagulation factors:
factors(fibrinogen),II(prothrombin),V,VII,and X.
Only substantial impairment in the livers ability to
synthesize these proteins can result in clotting
abnormalities
2) Prolongation of the prothrombin time is not specific
for liver disease.
8/2/2019 23172860 Liver Function
17/90
Tests of Bil irublinMetabolism Serum total bi l irubin(STB) Conjugated bil irubin Urobil inogen
8/2/2019 23172860 Liver Function
18/90
Bil irubin Metabolism1) Bilirubin is the principal degradation product of
heme.
2) Bilirubin transport and conjugation in the
hepatocyte.
3) The generally accepted reference range for normalplasma bilirubin concentrations in healthy persons,
which includes 95 per cent of all individuals values, is
1.7 to 17.1umol/L.
8/2/2019 23172860 Liver Function
19/90
Bilirubinmetabolism
8/2/2019 23172860 Liver Function
20/90
Bil irubinBilirubin is derived from the tetrapyrrole prostheticgroup found in haemoglobin and the cytochrome. It isnormally conjugated with glucuronic acid to make itmore soluble, and excreted in the bile.Both conjugated bilirubin and unconjugated bilirubinmay be present in plasma. Conjugated bilirubin iswater soluble, unconjugated bilirubin is not, and bindsto albumin. Bilirubin is neurotoxic, and if its levels risetoo high in neonates, permanent brain damage canoccur.
8/2/2019 23172860 Liver Function
21/90
BILIRUBINBilirubin metabolites are responsible for the browncoloration of faeces. If bilirubin does not reach the gut,stools become pale in color.Bilirubin in the gut is metabolized by bacteria to producestercobilinogen, which is partly reabsorbed andreexcreted in the urine as urobilinogen. When highlevels of conjugated bilirubin are being excreted , urinemay be a deep orange colour.
8/2/2019 23172860 Liver Function
22/90
High bil irubin levelHaemolysis (Haemolytic)The increased haemoglobinbreakdown produces bilirubin which overloads the
conjugating mechanism.
Unconjugated hyperbilirubinaemia is commonly
encountered in babies.
Liver disorder (Hepatocellular) Failure of theconjugating mechanism within the hepatocyte.
Obstruction in the biliary system (Cholestatic)including extrahepatic biliary obstruction, Intrahepatic
biliary obstruction is much more difficult to diagnose
than extrahepatic obstruction.
8/2/2019 23172860 Liver Function
23/90
Jaundice Whats Jaundice?
Jaundice is a yellow discoloration of the skinor sclera.Due to the bil irubin concentration in plasma ismuch greater than normal (greater than about40 mol/L)
8/2/2019 23172860 Liver Function
24/90
Causes ofjaundice
8/2/2019 23172860 Liver Function
25/90
Jaundice indicates that there is anelevated concentration of bil irubin inserum.
In neonates it is important to determinethe concentration of unconjugatedbilirubin in order to decide what treatmentis required.
In adults, the most common cause ofjaundice is obstruction, and this isconfirmed by the elevation of both
8/2/2019 23172860 Liver Function
26/90
Jaundice/More than34.2mol/L(2.0mg/100mL) Latent jaundice/17.2 34.2 mol/L Normal/ Less than 1.70~17.2 mol/L 80% is unconjugated bil irubin and 20%
is conjugated bil irubin
Serumbil irubin
8/2/2019 23172860 Liver Function
27/90
Because only conjugated bilirubin isexcreted in urine, it is indirect test forincreased concentration of conjugatedbilirubin in serum.
A fresh urine specimen is required sincebilirubin is very unstable when exposed inlight and room temperature.
The chemstrip test for bil irubin in urine.
Urine Bil irubin
8/2/2019 23172860 Liver Function
28/90
Haemolytic Cholestatic HepatocellularFeatures
1.Bil irubin usually3 upper l imit ofreference range.4.AST, ALT+LDHusually modestly
1.AST+ALT 2.Bil irubin later3.Bil irubin in urine4. ALP later
8/2/2019 23172860 Liver Function
29/90
DIFFERENTIAL DIAGNOSIS OF JAUNDICEUnconjugated hyperbilirubinemiaIncreased heme catabolismHemolytic anemiaHematoma
Impaired hepatic conjugationNeonatal jaundice
Conjugated hyperbilirubinemiaImpaired hepatic excretionHepatocellular diseasePosthepatic obstruction
8/2/2019 23172860 Liver Function
30/90
Dye intake and Excretion Indocyanine green retention rate
(ICGR): 15min
8/2/2019 23172860 Liver Function
31/90
SERUM ENZYMETESTS
AminotransferaseAminotransferase1) AST (Aspartate) and ALT (Alanine) is present in a wide
variety of tissues-including heart, skeletal muscle, kidney,and brain in addition to liver.
2) Serum levels of AST and ALT are elevated to some extent inalmost all liver diseases (viral hepatitis, obstructive jaundiceand liver cirrhosis).
3) The elevations of the enzyme levels do not correlate witheventual outcome, even though they may reflect the extent ofhepatocellular necrosis.
8/2/2019 23172860 Liver Function
32/90
AminotransferaseminotransferaseClinical value of AST and ALT
The ratio of AST to ALT
Reference Value
AST and ALT: 5~40U/L
SERUM ENZYME TESTS
8/2/2019 23172860 Liver Function
33/90
MARKERS OF CHOLESTASIS Alkaline phosphatase(ALP)An indices of a blockage of bile flow Cholestasis,which maybe intra- or extra-hepatic disease
(tumor, cirrhosis )
ADULT 25~90U/LADULT 25~90U/LCHILD 50~350U/LCHILD 50~350U/L
SERUM ENZYMETESTS
8/2/2019 23172860 Liver Function
34/90
Plasma alkaline phosphatase activity as a function of age andsex(men , women). Horizontal lines refer to multiples of the
adult upper reference limit.
8/2/2019 23172860 Liver Function
35/90
1) The reference range for ALP is dependent on age.
2) In the human body, ALP has been identified in liver,bone, intestine, kidney and leukocytes. ALPs are a
heterogeneous group of enzymes. For patients withhigh ALP levels, measurement of ALP isoenzymes isuseful for differentiating between bone and liversources.
3) The highest elevations of ALP in patients with liverdisease occur in patients with cholestasis or hepaticcarcinoma.
SERUM ENZYMETESTS
8/2/2019 23172860 Liver Function
36/90
-Glutamyl Transpeptidase ( -GT)Cholestasis
Alcohol
Drugs
Acute hepatic damage
Combining with alkaline phosphatase
Male 11-50U/LFemale 7~32U/L
SERUM ENZYME TESTS
8/2/2019 23172860 Liver Function
37/90
1) -GT has been localized to the whole hepatobiliary tree-from hepatocytes to common bile duct in the liver, andalso to pancreatic acini and ductules.
2) Serum -GT is elevated in association with a wide varietyof pathologic states in addition to hepatobiliary disease,including chronic alcoholism, pancreatic disease,myocardial infarction, renal failure, chronic obstructivepulmonary disease and diabetes.
3) In liver disease, serum -GT activity correlates wellwith serum ALP, and is the most sensitive indicator ofbiliary tract disease.
SERUM ENZYME TESTS
8/2/2019 23172860 Liver Function
38/90
5-Nucleotidase (5-NT)
1) 5-NT is present in the intestines, brain, heart, blood
vessels and endocrine pancreas in addition to the liver.
2) Elevation of 5-NT in the serum are purported to be ofhepatobiliary origin only despite the widespread localizationof the enzyme in other body tissues.
3) In clinical hepatic disease, serum 5-NT correlate closely withserum alkaline phosphatase.
4) Serum 5-NT is particularly useful in diagnosing liver diseasein childhood and in pregnancy.
SERUM ENZYMETESTS
8/2/2019 23172860 Liver Function
39/90
monoamine oxidase, MAO -Proline hydroxylase, PHIndices of hepatic f ibrosis
SERUM ENZYME TESTS
8/2/2019 23172860 Liver Function
40/90
Unlike some disorders such asacute pancreatit is (Amylase) andmyocardial infarction (MyoglobinTroponin), for which there areenzyme markers that are primari lyused for one disorder and havehigh diagnostic efficiencies, thereare no enzyme markers that arespecif ic for any single l iverdisease.
8/2/2019 23172860 Liver Function
41/90
When evaluating these disorders,therefore, it is appropriate to consider apanel of markers, sometimes called livefunction tests (LFTs). usually includes bil irubin, AST, ALT, ALP,and sometimes GGT and 5'NT although these tests can reflect various
disease processes in the liver, they donot reflect hepatic reserve for synthesisand metabolic functions
8/2/2019 23172860 Liver Function
42/90
Other tests for LiverExcretion Function Bile Acids
8/2/2019 23172860 Liver Function
43/90
Bile Acids The regulation of bile acid is a major function ofthe liver. Cholesterol homeostasis is in large partmaintained by the conversation of cholesterol to bileacids and subsequent regulation of bile acidmetabolism.
Bile acid provides surface-active detergentmolecules that facilitate both hepatic excretion ofcholesterol to bile acids and solubilization of lipids forintestinal absorption.
8/2/2019 23172860 Liver Function
44/90
The metabolism of bile acid
8/2/2019 23172860 Liver Function
45/90
8/2/2019 23172860 Liver Function
46/90
The cl inical Signif icancesof SERUM BILE ACIDS1. In the last 20 years, there have been majormethodological advances in the measurement ofserum bile acids.2. Clinical significance:1) Bile acids more specifically reflect excretoryfunction. Increase of bile acids in serum suggestimpaired hepatic uptake or secretion, or portal-systemic shunting2) The high concentration of serum bile acidsseem to occur in viral hepatitis and extrahepaticobstruction.
8/2/2019 23172860 Liver Function
47/90
SERUM BILE ACIDS3) Abnormal results of ALP, AST and rGT lackedthe specificity of bile acids abnormalities.AST determinations are more sensitive thanthose for fasting serum bile acids in detectingmild liver diseases such as fatty liver orchronic persistent hepatitis, because mild orpatchy hepatocellular injury does not impairhepatic function severely.
4) The ratio of cholic acid to chenodeoxycholicacid is between 0.5-1.0 in healthy subjects,but in extrahepatic obstruction it is increased0.96-3.6.
8/2/2019 23172860 Liver Function
48/90
SERUM BILE ACIDS Reference value:
Total Bile Acid 0~6mol/L
8/2/2019 23172860 Liver Function
49/90
Summary of Liver functionests
A request for LFTs will usually generate results forbilirubin, the aminotransferases and alkaline phosphatase.
Raised activities of the aminotransferases(AST and ALT)indicate hepatocellular damage.
Increased bilirubin concentration and increased alkalinephosphatase activity indicate the presence of cholestasis, ablockage in bile flow.
Serial use of LFTs is of most value in following theprogress or resolution of liver disease.
Measurement of GT can give an indication ofhepatocellular enzyme induction due to drugs or alcohol.
8/2/2019 23172860 Liver Function
50/90
Tests of Viral Hepatit is Hepatitis A
Hepatitis B
Hepatitis C
8/2/2019 23172860 Liver Function
51/90
Hepatitis A(HAV) is a kind of RNA virus.It is transmitted by the fecal-oral route.
It is thus implicated in most instancesof water-borne and food-transmittedinfection and in epidemics of viral
hepatitis.
Tests of Viral Hepatit is A
8/2/2019 23172860 Liver Function
52/90
Serologic markers of viralhepatit is AAgent markers definition significances
HAV Anti-HAVIgM type Antibodyto HAV Current or recentinfection of HAV
IgG type Current or previousinfection of HAV,confers immunity
8/2/2019 23172860 Liver Function
53/90
HBV is a kind of DNA virusconsisted by core and surfacecomponents. HBV transmissionoccurs most commonly via bloodand blood products, contaminatedneedles and intimate personalcontact. HBV is present in al l bodyfluids.
Tests of Viral Hepatit is B
8/2/2019 23172860 Liver Function
54/90
gent markers definition significances
HBV HBsAG HBV surfaceantigen
Positive in acute or chronic infection
HBeAG e antigen, acomponent
Transiently positive in acute hepatitisB, reflects presence of viral replication
and high infectivityAnti-HBe Antibody to e
antigen
Transiently positive, may be
persistently present in chronic cases,reflects low infectivity
Anti-HBcAntibodyto core
antigen
IgG type Positive in all acute and chronic cases,reliable marker of infection, past orcurrent
IgM type Reflects active viral replication, not
protective
hepatit is
8/2/2019 23172860 Liver Function
55/90
Agent markers definition significances
Anti-HBs Antibody to
surface
confers immunity,
8/2/2019 23172860 Liver Function
56/90
Tests of Viral Hepatit is C HCV is a kind of RNA virus and issimilar to HBV, is largely parenterallytransmitted. HCV is the main causeof post-transfusion hepatitis.
8/2/2019 23172860 Liver Function
57/90
Serologic markers of viralhepatit is
Agent markers definition significances
HCV Anti-HCV Antibody
to HCV
Positive after clinical
onset(15 weeks),
Not protective,
Persists in chronic infection
8/2/2019 23172860 Liver Function
58/90
Liver Disease
8/2/2019 23172860 Liver Function
59/90
PoisoningInfection Viral hepatitis (hepatitis B)Inadequate perfusionChronic excess alcohol ingestionAutoimmune diseaseUnusual cause of cirrhosis:1-antitrypsin deficient and Wilsons
disease
Causes for l iver disease
8/2/2019 23172860 Liver Function
60/90
Liver diseaseAcute Hepatocellular InjuryViral Hepatitis
Acute Liver failure
Cholestatic Liver DiseaseIntrahepatic ObstructionExtrahepatic Obstruction
Chronic Liver DiseaseChronic Hepatitis
Cirrhosis
Liver Cancer
Alcoholic Liver DiseaseFatty Liver
Alcoholic He atitis
8/2/2019 23172860 Liver Function
61/90
It may resolve
It may progress to acute hepatic failureIt may lead to chronic hepatic damage
OUTCOME
Acute Hepatocellular Injury
8/2/2019 23172860 Liver Function
62/90
Biochemicalfindings inhepaticfailure
8/2/2019 23172860 Liver Function
63/90
Cholestasis Cholestasis represents the demonstrableaccumulation in the blood stream of
substances normally excreted in bile(e.g., bil irubin, cholesterol, bile acids).
8/2/2019 23172860 Liver Function
64/90
Cholestatic Liver Disease Intrahepatic Obstruction
Intrahepatic cholestasis often results
from cirrhosis or hepatitis. Extrahepatic Obstruction
Extrahepatic cholestasis is usually the
result of mechanical obstruction of thecommon bile duct or hepatic duct.
8/2/2019 23172860 Liver Function
65/90
Chronic Liver Disease
Chronic Hepatitis chronic active hepatitis
chronic persistent hepatitis Cirrhosis
Liver enzyme levels in cirrhosis are variably elevatedand can be normal during the terminal stages of thedisease.
Primary biliary cirrhosis /Elevations in ALP andaminotransferases are expected along with high titers
of antimitochondrial antibody. Liver Cancer
The liver enzyme results tend to be more elevated inthe active form; however, differentiation is best made
by performing a liver biopsy.
8/2/2019 23172860 Liver Function
66/90
Fibrosis of Liver tissuesFibrosis is common to several chronic liverdiseases and as such is the leading causeof morbidity and mortality from hepaticdisease.Hepatic fibrosis may have biologic effectson cells as well as physical effects on bloodflow and is a main cause of portalhypertension.
8/2/2019 23172860 Liver Function
67/90
The most common causes of cirrhosis are chronicexcess alcohol ingestion, viral hepatitis andautoimmune diseases.Cirrhosis is not reversible. There are no goodbiochemical indicators of cirrhosis in the early andstable periodCirrhosis can develop in children as a result of a1-antitrypsin deficiency or Wilsons disease and inadult due to haemochromatosis.
Cirrhosis
8/2/2019 23172860 Liver Function
68/90
Terminal stage ofcirrhosis
Developing jaundiceEncephalopathyAscitesBleeding tendenicesTerminal l iver failure
8/2/2019 23172860 Liver Function
69/90
Alcoholic Liver DiseaseFatty LiverThe concentrations of traditional liver enzymesare typically within the normal range.Definitive diagnosis is made by a liver biopsy.The disease is considered benign and can beeffectively reversed by immediate abstinence
from ethanol intake.Alcoholic Hepatitis Liver enzyme concentrations are increased,
notably AST and ALT
8/2/2019 23172860 Liver Function
70/90
Normal Liver
8/2/2019 23172860 Liver Function
71/90
Fatty Liver
8/2/2019 23172860 Liver Function
72/90
Cirrhotic Liver
8/2/2019 23172860 Liver Function
73/90
A 49-year-old woman attend her GP with an 8-day history ofanorexia, nausea and flu-like symptom. She had noticed thather urine had been dark in colour over the past 2 days.Physical examination revealed tenderness in the right upperquadrant of the abdomen. LFTS were as follows:
Bilirubin AST ALT ALP -GT TP Albmol/L U/L(g/L)63 936 2700 410 312 68 42
Comment on these results.
What is the differential diagnosis?
Case history
8/2/2019 23172860 Liver Function
74/90
Markers For Liver Function And Disease
8/2/2019 23172860 Liver Function
75/90
Markers For Liver Function And Disease
Disease or function MarkersFunction evaluationNormal synthesis capacity Albumin, prealbumin prothrombin time,Excretory function Bil irubin, bile acids , globulinsMetabolic function Ammonia, amino acids, l ipids, serum
protein electrophoresisPathological evaluationHepatocel lular injury AST, ALTObstruction Bil irubin, alkaline phosphatase, -
GT , 5 - nucleotidosebile acids,InfectionsViral and autoimmune serologies
8/2/2019 23172860 Liver Function
76/90
ALT and AST in acute l iver injurydisease enzyme marker
acute hepatitis ALT and AST elevated>1000U/L (viral or toxic)
HAV ALT elevated in 3 to 4 weeks after infectionALT return to normal within 8 to 12 weeks
HBV preclinical incubation phase is longer and ALTand and AST may remain normal for 2 to 6monthsHCV ALT and AST return to normal within 2 to 3months
chronic activehepatitis ALT and AST elevated 5 to10 fold
end-stage ALT and AST return to normal or subnormalliver disease
8/2/2019 23172860 Liver Function
77/90
Relationship of AST and ALT toALP and GGT in Hepatit is
8/2/2019 23172860 Liver Function
78/90
Relationship of AST and ALT to ALPand GGT in Cholestasis
Multi
pli
8/2/2019 23172860 Liver Function
79/90
The best markers for intrahepatic andextrahepatic cholestas is are ALP, GGT, and 5'NT AST and ALT are generally only sl ightly elevated incholestasis, rarely more than 500 U/L. The largest elevations (four- to 10-fold) of ALP are
typically seen in obstruction owing to gallstones ormalignancy and in biliary cirrhosis . Measurement of total and direct bilirubin
are also important in making the diagnosisof obstructive jaundice.
8/2/2019 23172860 Liver Function
80/90
Ratio (AST/ALT)
8/2/2019 23172860 Liver Function
81/90
The Ratio of (AST/ALT) Further differentiation of specific liver
diseases is aided by calculating the ratioof AST to ALT levels. acute or chronic ? intra- or extrahepatic ?
recommended by the International Federation ofClinical Chemistry (IFCC) The ratio is normally approximately 1.15
ALT versus AST levels
8/2/2019 23172860 Liver Function
82/90
in various l iver diseases
8/2/2019 23172860 Liver Function
83/90
AST/ALTDiseaseST/ALT
Acute disorders of the liver 1.0alcoholic liver diseasechronic active hepatitisChronic persistent hepatitis normal
Extrahepatic obstructionacute passage of a stone 1.5intrahepatic cholestasisbiliary cirrhosis and malignancy 1.5
Relationship of AST and ALT to ALP
8/2/2019 23172860 Liver Function
84/90
and GGT in Malignancy
Mu
ltiplies
o
Relationship of AST and ALT to ALP an
8/2/2019 23172860 Liver Function
85/90
GGT in Alcoholic Live Disease
Mu
ltiplie
s
8/2/2019 23172860 Liver Function
86/90
Abnormal Liver Function TestsHepatocellular Disease Cholestatic Disease
NormalAlbumin DecreasedAlbumin NormalAlbumin DecreasedAlbuminAcuteHepatitis ChronicHepatitis AcuteCholestasis ChronicCholestasis
UltrasoundDetectionIntrahepatic Cholestasis Extrahepatic Cholestasi
8/2/2019 23172860 Liver Function
87/90
Case historyA 60-years-old female with a history of breast carcinomatreated by mastectomy three years previously is nowcomplaining of general malaise and bone pain. Biochemistryshowed that fluid and electrolyte, total protein, albuminand calcium values were all normal. LFTs were as follows:Bilirubin AST ALT Alkaline phosphatase GTmol/l U/l
7 33 38 89032Evaluate these results and suggest a likely diagnosis.
8/2/2019 23172860 Liver Function
88/90
Biochemical monitoring of liver disease is bysequential measurements of the aminotransferase,bilirubin and alkaline phosphatase. In acute liver damage there is usually intrahepaticobstruction as well as hepatocellular damage. Severe cases of acute liver damage may progressto hepatocellalur failure. Cirrhosis is the end point of both acute and chronicliver damage, as well as being caused by a numberof metabolic and autoimmune diseases. Biochemical tests may be of little value in makinga specific diagnosis. A liver biopsy is frequentlymore helpful.
Summary
8/2/2019 23172860 Liver Function
89/90
The clinical significances of each liverfunction test?
The differentiation diagnosis ofjaundice.
The evaluations of biochemical tests of
liver functions in different liverdiseases.
8/2/2019 23172860 Liver Function
90/90
Thank You for YourAttention!
Top Related